







Languages
Pages
Legal


2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)www.escardio.org/guidelines
TheTaskForceforthemanagementofacutemyocardialinfarc6oninpa6entspresen6ngwithST-segmenteleva6onoftheEuropeanSocietyofCardiology
2017ESCGuidelinesforthemanagementofacutemyocardialinfarcNoninpaNentspresenNngwithST-segmentelevaNon
Chairpersons:BorjaIbanez(Spain),StefanJames(Sweden).Authors/TaskForceMembers:StefanAgewall(Norway),ManuelJ.Antunes(Portugal),ChiaraBucciarelli-Ducci(UK),HéctorBueno(Spain),AlidaL.P.Caforio(Italy),FilippoCrea(Italy),JohnA.Goudevenos(Greece),SigrunHalvorsen(Norway),GerhardHindricks(Germany),AdnanKastra6(Germany),MaSeJ.Lenzen(TheNetherlands),EvaPrescoT(Denmark),MarcoRoffi(Switzerland),MarcoValgimigli(Switzerland),ChristophVarenhorst(Sweden),PascalVranckx(Belgium),PetrWidimský(CzechRepublic).
1
2
ESC
WG - Cardiovascular Pharmacotherapy
WG - Cardiovascular Surgery
EACVI - European Association of Cardiovascular Imaging
ACCA - Acute Cardiovascular Care Association
HFA - Heart Failure Association
EHRA - European Heart Rhythm Association
Council - Cardiovascular Nursing and Allied Professions
EAPCI - European Association of PCI
WG - Myocardial and Pericardial Diseases
WG - Thrombosis
EAPC -- European Association of Preventive cardiology
Council – for Cardiology practice
v
vv30 Reviewers
v
v
vv
vv
v
v v
v
v
v
vv
v
v
v
v
v
v
v
v
v
vv
v
v
v
-1224 comments and requests
v
Task Force Members
2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)www.escardio.org/guidelines
19 Authors ESC
www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
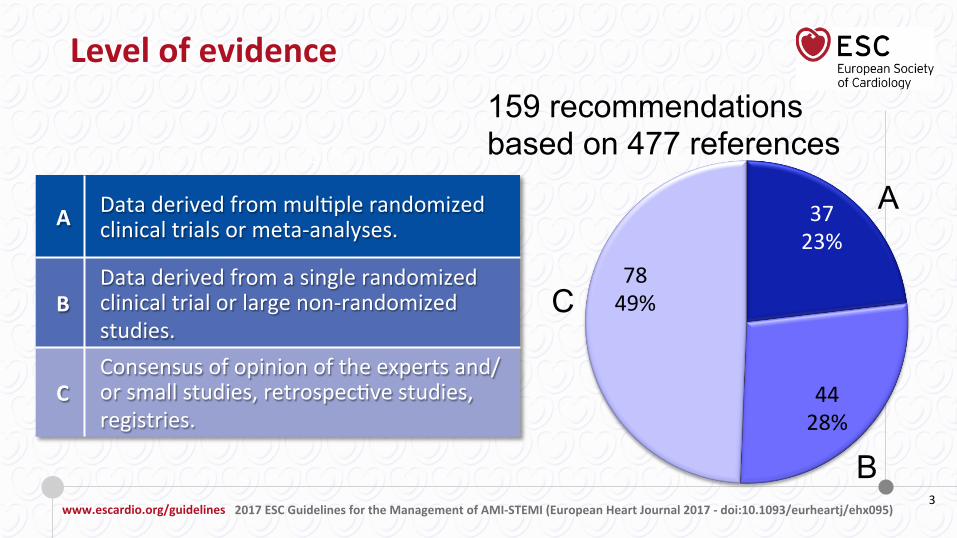
Levelofevidence
3
21%
159 recommendations based on 477 references
A
B
C
3723%
4428%
7849%
A Dataderivedfrommul6plerandomizedclinicaltrialsormeta-analyses.
BDataderivedfromasinglerandomizedclinicaltrialorlargenon-randomizedstudies.
CConsensusofopinionoftheexpertsand/orsmallstudies,retrospec6vestudies,registries.

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
2017NEW/REVISEDCONCEPTS
STRATEGYSELECTIONANDTIMEDELAYS:• Cleardefini6onoffirstmedicalcontact(FMC).• Defini6onof“6me0”tochoosereperfusionstrategy(i.e.thestrategyclockstartsatthe6meof“STEMIdiagnosis”).
• Selec6onofPCIoverfibrinolysis:whenan6cipateddelayfrom“STEMIdiagnosis”towirecrossingis≤120min.• Maximumdelay6mefrom“STEMIdiagnosis”tobolusoffibrinolysisagentissetin10min.• “Door-to-Balloon”termeliminatedfromguidelines.
ELECTROCARDIOGRAMATPRESENTATION:• Lejandrightbundlebranchblockconsideredequalforrecommendingurgentangiographyifischaemicsymptoms.
TIMELIMITSFORROUTINEOPENINGOFANIRA:• 0-12h(ClassI);12-48h(ClassIIa);>48h(ClassIII).
MINOCAANDQUALITYINDICATORS:• Newchaptersdedicatedtothesetopics.
PATIENTSTAKINGANTICOAGULANTS:• Acuteandchronicmanagementpresented.
TIMETOANGIOGRAPHYAFTERFIBRINOLYSIS:• Timeframeissetin2-24hajersuccessfulfibrinolysis.
Whatisnewin2017GuidelinesonAMI-STEMI
4

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
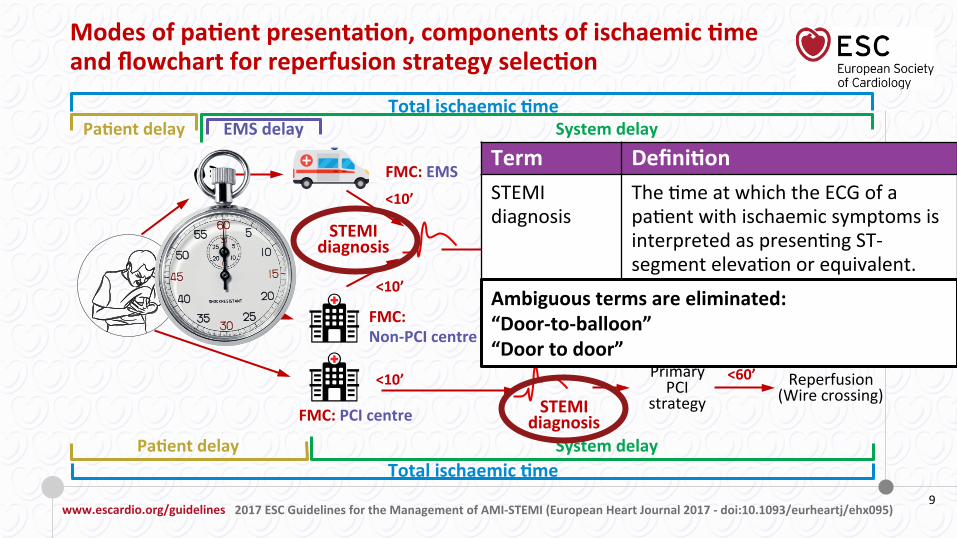
ModesofpaNentpresentaNon,componentsofischaemicNmeandflowchartforreperfusionstrategyselecNon
TotalischaemicNme
TotalischaemicNme
PaNentdelay EMSdelay
PaNentdelay
Systemdelay
Systemdelay
FMC:EMS<10’
STEMIdiagnosis
<10’
FMC:Non-PCIcentre
<10’
FMC:PCIcentre
PrimaryPCI
strategyReperfusion
(Wirecrossing)
Fibrinolysisstrategy
Reperfusion(Ly6cbolus)
PrimaryPCI
strategyReperfusion
(Wirecrossing)
<90’
<10’
<60’
STEMIdiagnosis
≤120min
>120min
TimetoPCI?
5
Term DefiniNonFMC The6mepointwhenthepa6entis
eitherini6allyassessedbyaphysician,paramedic,nurseorothertrainedEMSpersonnelwhocanobtainandinterprettheECG,anddeliverini6alinterven6ons(e.g.defibrilla6on).FMCcanbeeitherintheprehospitalseSngoruponpa6entarrivalatthehospital(e.g.emergencydepartment).



www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
ModesofpaNentpresentaNon,componentsofischaemicNmeandflowchartforreperfusionstrategyselecNon
TotalischaemicNme
TotalischaemicNme
PaNentdelay EMSdelay
PaNentdelay
Systemdelay
Systemdelay
FMC:EMS<10’
STEMIdiagnosis
<10’
FMC:Non-PCIcentre
<10’
FMC:PCIcentre
PrimaryPCI
strategyReperfusion
(Wirecrossing)
Fibrinolysisstrategy
Reperfusion(Ly6cbolus)
PrimaryPCI
strategyReperfusion
(Wirecrossing)
<90’
<10’
<60’
STEMIdiagnosis
≤120min
>120min
TimetoPCI?
9
Term DefiniNonSTEMIdiagnosis
The6meatwhichtheECGofapa6entwithischaemicsymptomsisinterpretedaspresen6ngST-segmenteleva6onorequivalent.
Ambiguoustermsareeliminated:“Door-to-balloon”“Doortodoor”

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
ModesofpaNentpresentaNon,componentsofischaemicNmeandflowchartforreperfusionstrategyselecNon
TotalischaemicNme
TotalischaemicNme
PaNentdelay EMSdelay
PaNentdelay
Systemdelay
Systemdelay
FMC:EMS<10’
STEMIdiagnosis
<10’
FMC:Non-PCIcentre
<10’
FMC:PCIcentre
PrimaryPCI
strategyReperfusion
(Wirecrossing)
Fibrinolysisstrategy
Reperfusion(Ly6cbolus)
PrimaryPCI
strategyReperfusion
(Wirecrossing)
<90’
<10’
<60’
STEMIdiagnosis
≤120min
>120min
TimetoPCI?
10
Lejandrightbundlebranchblockareconsideredequalforrecommendingurgentangiographyifischaemic
symptoms.
AtypicalECGpresentaNons§ Bundlebranchblock,§ Ventricularpacing,§ Hyper-acuteTwaves,§ Isolateddepressioninanteriorleads,§ UniversalSTdepressionwithaVRelevaNonIn
Inthepresenceofsymptoms,aprimaryPCI
strategy(urgentangiographyandPCIif
indicated)shouldbefollowed.

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
ModesofpaNentpresentaNon,componentsofischaemicNmeandflowchartforreperfusionstrategyselecNon
TotalischaemicNme
TotalischaemicNme
PaNentdelay EMSdelay
PaNentdelay
Systemdelay
Systemdelay
FMC:EMS<10’
STEMIdiagnosis
<10’
FMC:Non-PCIcentre
<10’
FMC:PCIcentre
PrimaryPCI
strategyReperfusion
(Wirecrossing)
Fibrinolysisstrategy
Reperfusion(Ly6cbolus)
PrimaryPCI
strategyReperfusion
(Wirecrossing)
<90’
<10’
<60’
STEMIdiagnosis
≤120min
>120min
TimetoPCI?
11
IntheabsenceofST-segmentelevaNon Class Level
AprimaryPCIstrategyisindicatedinpa6entswithsuspectedongoingischaemicsymptomsif:‒ haemodynamicinstabilityorcardiogenicshock,‒ recurrentorongoingchestpainrefractorytomedicaltreatment,‒ life-threateningarrhythmiasorcardiacarrest,‒ mechanicalcomplica6onsofmyocardialinfarc6on,‒ acuteheartfailure,‒ recurrentdynamicST-segmentorT-wavechanges,par6cularlywithintermiTentST-segmenteleva6on.
I C

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
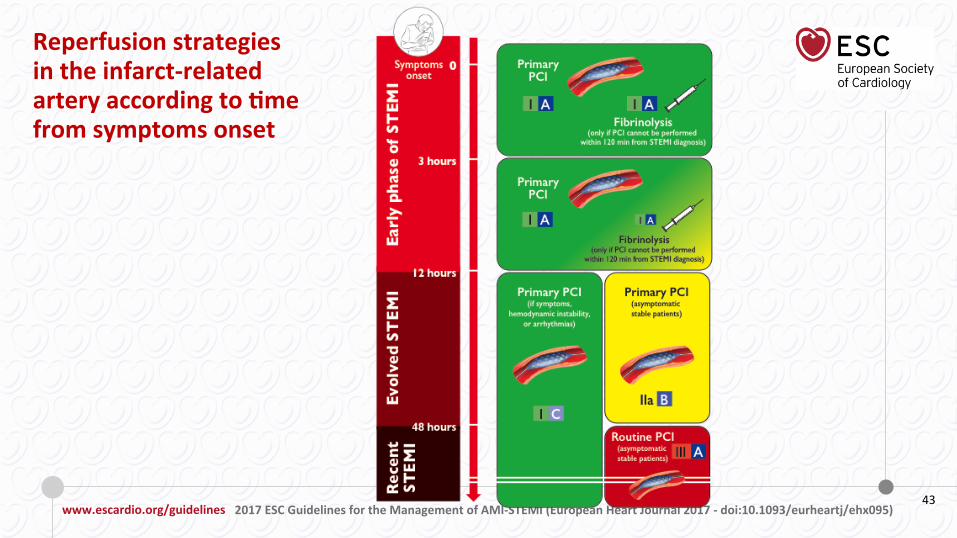
Reperfusionstrategiesintheinfarct-relatedarteryaccordingtoNmefromsymptomsonset
Early
pha
seofS
TEMI
3hours
Symptomsonset
0 PrimaryPCI
PrimaryPCI
Fibrinolysis(onlyifPCIcannotbeperformed
within120minfromSTEMIdiagnosis)
Fibrinolysis(onlyifPCIcannotbeperformed
within120minfromSTEMIdiagnosis)
I A I A
I AI A
12
12hours

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Reperfusionstrategiesintheinfarct-relatedarteryaccordingtoNmefromsymptomsonset(con&nued)
EvolvedSTEM
I
48hours
Recent
STEM
I
I C
PrimaryPCI(ifsymptoms,
hemodynamicinstabilicy,orarrhythmias)
PrimaryPCI(asymptomaNcstablepaNents)
III ARouNnePCI(asymptomaNcstablepaNents)
IIa B
12hours
13

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
14
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
15
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA
Valgimigli et al. Lancet 2015;385:2465-76

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
16
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA
Sabate et al. Lancet 2012;380:1482-90

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
17
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA
Engstrometal,Lancet2015

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
18
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA
Jollyetal,NEJM2015Frobertetal,NEJM2013

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
19
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA
Valgimiglietal,NEJM2015 Shazadetal,Lancet2014

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
20
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA
Silvainetal,BMJ2012

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
21
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
22
CHANGEINRECOMMENDATIONS2012 2017
Same dose i.V in all patients Half dose i.V. in Pts ≥75 years STREAM
Oxygen when SaO2 <95% Oxygen when SaO2 <90% AVOID, DETO2X
Radial access
PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute
TOTAL, TASTE
MATRIX, HEAT-PPCI
ATOLL, Meta-analysis
Small trials & observational data
EXAMINATION,COMFORTABLE-AMI,NORSTENT
MATRIX
DES over BMS
Complete Revascularization
Thrombus Aspiration
Bivalirudin
Enoxaparin
Early Hospital Discharge
OXYGEN
TNK-tPA
Stubbetal,Circ2015

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
• CangrelorifP2Y12inhibitorshavenotbeengiven.CHAMPION
• SwitchtopotentP2Y12inhibitors48hoursajerfibrinolysis.Expertopinion
• ExtendTicagrelorupto36monthsinhigh-riskpa6ents.PEGASUS-TIMI54
• Useofpolypilltoincreaseadherence.FOCUS
2017NEWRECOMMENDATIONS• Addi6onallipidloweringtherapyifLDL>1.8mmol/L(70mg/dL)despiteonmaximumtoleratedsta6ns.IMPROVE-IT,FOURIER
• Completerevasculariza6onduringindexprimaryPCIinSTEMIpa6entsinshock.Expertopinion
IIIIIbIIaI
• Rou6neuseofdeferredsten6ng.DANAMI3-DEFER
23

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
• CangrelorifP2Y12inhibitorshavenotbeengiven.CHAMPION
• SwitchtopotentP2Y12inhibitors48hoursajerfibrinolysis.Expertopinion
• ExtendTicagrelorupto36monthsinhigh-riskpa6ents.PEGASUS-TIMI54
• Useofpolypilltoincreaseadherence.FOCUS
2017NEWRECOMMENDATIONS• Addi6onallipidloweringtherapyifLDL>1.8mmol/L(70mg/dL)despiteonmaximumtoleratedsta6ns.IMPROVE-IT,FOURIER
• Completerevasculariza6onduringindexprimaryPCIinSTEMIpa6entsinshock.Expertopinion
IIIIIbIIaI
• Rou6neuseofdeferredsten6ng.DANAMI3-DEFER
24
BhaTetal,NEJM2013

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
Whatisnewin2017GuidelinesonAMI-STEMI
• CangrelorifP2Y12inhibitorshavenotbeengiven.CHAMPION
• SwitchtopotentP2Y12inhibitors48hoursajerfibrinolysis.Expertopinion
• ExtendTicagrelorupto36monthsinhigh-riskpa6ents.PEGASUS-TIMI54
• Useofpolypilltoincreaseadherence.FOCUS
2017NEWRECOMMENDATIONS• Addi6onallipidloweringtherapyifLDL>1.8mmol/L(70mg/dL)despiteonmaximumtoleratedsta6ns.IMPROVE-IT,FOURIER
• Completerevasculariza6onduringindexprimaryPCIinSTEMIpa6entsinshock.Expertopinion
IIIIIbIIaI
• Rou6neuseofdeferredsten6ng.DANAMI3-DEFER
25
Bonacaetal,NEJM2015

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)26
“Donotforget”intervenNonsinSTEMIpaNentsundergoingaprimaryPCIstrategy

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
DiagnosNctestflowchartinMINOCA
ACUTEINVESTIGATIONSUSPECTEDSTEMI
Coronarystenosis≥50% UrgentangiographyNoCoronarystenosis≥50%+Fulfilment
universalAMIcriteria
TreatasSTEMI MINOCAAcuteLVwallmoNonassessment(angiogram/echo)
27

www.escardio.org/guidelinesFullTextESCPocketGuidelinesAppandmuchmore…

Ιωάννινα
Λευκάδα
Πρέβεζα
Άρτα
Κέρκυρα
Φιλιάτες
STEMI in NW Greece
Διάρκεια 12 µήνες
(1/10/05 – 31/9/06)
n: 359 (άνδρες
82%) Άφιξη από την έναρξη των συµπτωµάτων
<3 h 201(55%) 3-12 59
>12 99

Primary PCI Athens area



STEMI pPCI patients Time Delays
Thrombolysis 2011 2012 2015 Symptoms – FMC 136,91 min 125,5 min 136 min FMC – needle 62,17 min 65,5 min 36 min pPCI Symptoms – FMC 142,41 min 131,26min 125 min FMC – PCI center 129,11 min 119,21 min 78 min Door – Balloon 53,41 min 53,1 min 55 min FMC – Balloon 182,52 min 172,31 min 133 min
ESCPocketGuidelinesAppAny6me-Anywhere
• AllESCPocketGuidelines• Over140interacNvetools
- Algorithms- Calculators- Charts&Scores
• SummaryCards&EssenNalMessages
• Online&Offline
Learn more on the Guidelines area

HELIOS 2005-6 Eπαναιµάτωση σε STEMI
p PCI9%
Lysis50%
No Rx41%
Mε αιµοδ/εργ. Xωρίς
35% 65%
prPCI 24%
1% Θρ/λυση 43%
54% Kαµµιά 33%
45%

2017ESCGuidelinesforthemanagementofacutemyocardialinfarcNoninpaNentspresenNngwithST-segmentelevaNon

EKAB
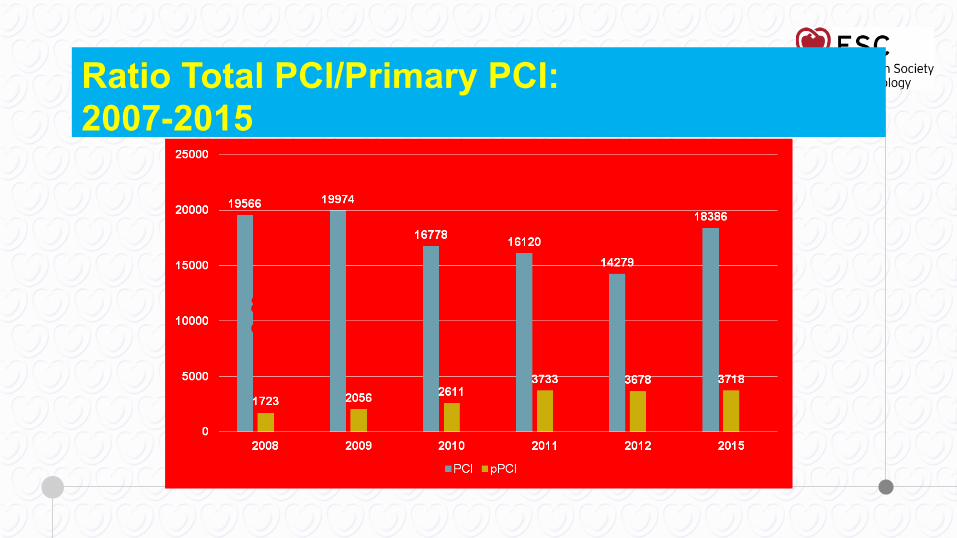
Ratio Total PCI/Primary PCI: 2007-2015
8,8%
10,2%
15,5%
23%
25%
20%


www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
ClassesofrecommendaNons
9258%38
24%
138%
1610%
I IIa
IIb III
159 recommendations Classes DefiniNon Suggested
wording
ClassI Evidenceand/orgeneralagreementthatagiventreatmentorprocedureisbeneficial,useful,effec6ve.
Recommended/isindicated.
ClassIIa Weightofevidence/opinionisinfavourofusefulness/efficacy.
Shouldbeconsidered.
ClassIIb Usefulness/efficacyislesswellestablishedbyevidence/opinion.
Maybeconsidered.
ClassIII Evidenceorgeneralagreementthatthegiventreatmentorprocedureisnotuseful/effec6ve,andinsomecasesmaybeharmful.
Notrecommended.

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
2017NEW/REVISEDCONCEPTS
STRATEGYSELECTIONANDTIMEDELAYS:• Cleardefini6onoffirstmedicalcontact(FMC).• Defini6onof“6me0”tochoosereperfusionstrategy(i.e.thestrategyclockstartsatthe6meof“STEMIdiagnosis”).
• Selec6onofPCIoverfibrinolysis:whenan6cipateddelayfrom“STEMIdiagnosis”towirecrossingis≤120min.• Maximumdelay6mefrom“STEMIdiagnosis”tobolusoffibrinolysisagentissetin10min.• “Door-to-Balloon”termeliminatedfromguidelines.
ELECTROCARDIOGRAMATPRESENTATION:• Lejandrightbundlebranchblockconsideredequalforrecommendingurgentangiographyifischaemicsymptoms.
TIMELIMITSFORROUTINEOPENINGOFANIRA:• 0-12h(ClassI);12-48h(ClassIIa);>48h(ClassIII).
MINOCAANDQUALITYINDICATORS:• Newchaptersdedicatedtothesetopics.
PATIENTSTAKINGANTICOAGULANTS:• Acuteandchronicmanagementpresented.
TIMETOANGIOGRAPHYAFTERFIBRINOLYSIS:• Timeframeissetin2-24hajersuccessfulfibrinolysis.
Whatisnewin2017GuidelinesonAMI-STEMI
41

www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)
ModesofpaNentpresentaNon,componentsofischaemicNmeandflowchartforreperfusionstrategyselecNon
TotalischaemicNme
TotalischaemicNme
PaNentdelay EMSdelay
PaNentdelay
Systemdelay
Systemdelay
FMC:EMS<10’
STEMIdiagnosis
<10’
FMC:Non-PCIcentre
<10’
FMC:PCIcentre
PrimaryPCI
strategyReperfusion
(Wirecrossing)
Fibrinolysisstrategy
Reperfusion(Ly6cbolus)
PrimaryPCI
strategyReperfusion
(Wirecrossing)
<90’
<10’
<60’
STEMIdiagnosis
≤120min
>120min
TimetoPCI?
42
www.escardio.org/guidelines 2017ESCGuidelinesfortheManagementofAMI-STEMI(EuropeanHeartJournal2017-doi:10.1093/eurheartj/ehx095)43
Reperfusionstrategiesintheinfarct-relatedarteryaccordingtoNmefromsymptomsonset
Top Related