







Languages
Pages
Legal

Antihypertensive drugs

• Primary or essential hypertension (95%)
No specific underlying cause
• Secondary hypertension (5%)Due to specific disease or drug

Blood Pressure
• Systolic blood pressure (SBP) : maximum pressure recorded during ventricular systole
• Diastolic blood pressure (DBP) : minimum pressure recorded during ventricular diastole
• Pulse pressure (PP) : SBP - DBP
• Mean arterial pressure : DBP + 1/3 PP
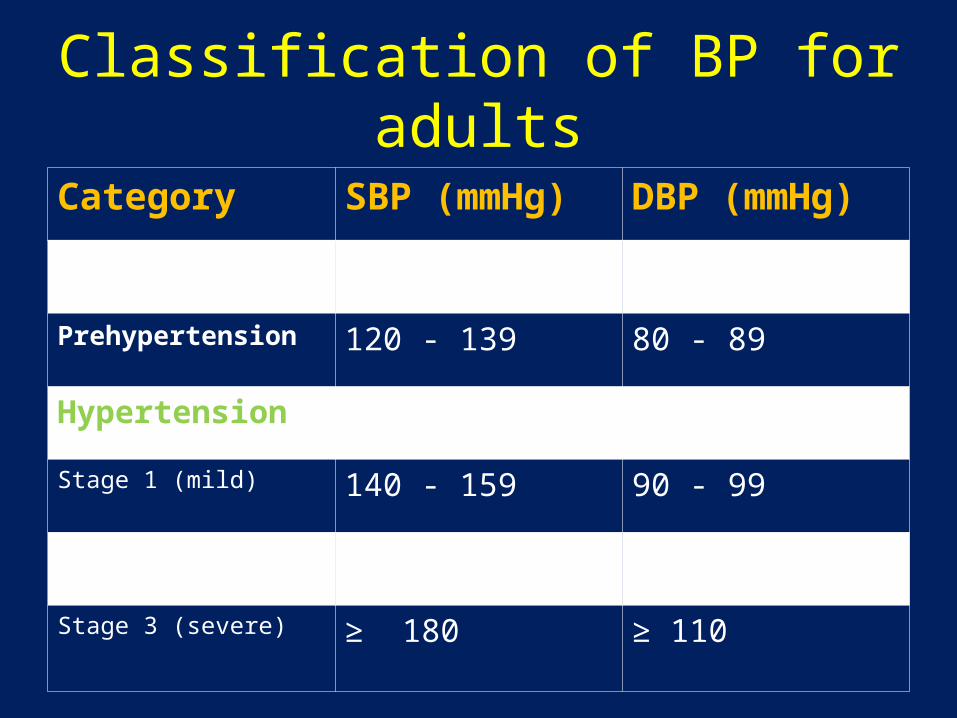
Classification of BP for adults
Category SBP (mmHg) DBP (mmHg)
Normal < 120 < 80
Prehypertension 120 - 139 80 - 89
Hypertension
Stage 1 (mild) 140 - 159 90 - 99
Stage 2 (moderate) 160 - 179 100 - 109
Stage 3 (severe) ≥ 180 ≥ 110

Classification:
1.Angiotensin Converting Enzyme inhibitors (ACEIs) :
Captopril, enalapril, lisinopril
2. Angiotensin-II receptor blockers (ARBs) : Losartan, candesartan, irbesartan
3. Calcium channel blockers (CCBs) : Verapamil, diltiazem, nifedipine, nimodipine amlodipine, felodipine

4. Diuretics : a) Thiazides & related agents –
Hydrochlorothiazide chlorthalidone b) Loop diuretics – Furosemide, bumetanide c) Potassium sparing diuretics – Amiloride triamterene spironolactone
5. Sympatholytic drugs: a) Centrally acting agents – Clonidine, α-
methyldopa b) Ganglion blockers – Trimethaphan c) Neuronal blockers – Reserpine

d) α-Adrenergic blockers: (i) Non-selective: Phenoxybenzamine phentolamine (ii) Selective: Prazosin, terazosin e) β-Adrenergic blockers: (i) Non-selective: Propranolol, timolol (ii) Selective: Atenolol, metoprolol
6. Vasodilators: a) Arteriolar – Hydralazine, minoxidil, diazoxide b) Arterial and venodilator – Sodium
nitroprusside

I. ACEIs : 1st line agents
Renin
ACE
(vasoconstriction)
BP
ACEIs
Bradykinin PG
Vasodilation
Blood vessel Aldosterone release
Cardiac hypertrophy & remodelling
Angiotensinogen
Angiotensin I
Angiotensin II
PVR Na+ & H2O retention
Inactive

Mechanism of action:• Inhibit the generation of angiotensin II – a potent
vasoconstrictor
• Inhibit the degradation of bradykinin – a potent vasodilator
• Stimulate the synthesis of PGs
• Reduce sympathetic nervous system activity
• Reduce aldosterone production
• Dilates both arteries & veins – afterload and preload

Therapeutic uses:
Hypertension
Congestive cardiac failure (CCF)
Myocardial infarction
Diabetic nephropathy
Scleroderma renal crisis

Adverse effects:• Dry cough & angioedema
• Taste alteration, proteinuria
• Teratogenicity – growth retardation & neonatal death
• Severe hypotension, neutropenia
• Hyperkalaemia
Drug interactions :
• ACEI x Potassium sparing diuretics – hyperkalaemia
• ACEI x Lithium – Li toxicityContraindicated in pregnancyPreferred drug in younger age group,
diabetics – delay or prevent the progression of renal complications

II. ARBs : MOA : competitevely inhibits the binding of angiotensin II to AT1 receptors
- do not affect bradykinin production
Therapeutic uses:• Hypertension• Diabetic nephropathy• CCF
Adverse effects: • Dry cough & angioedema - less
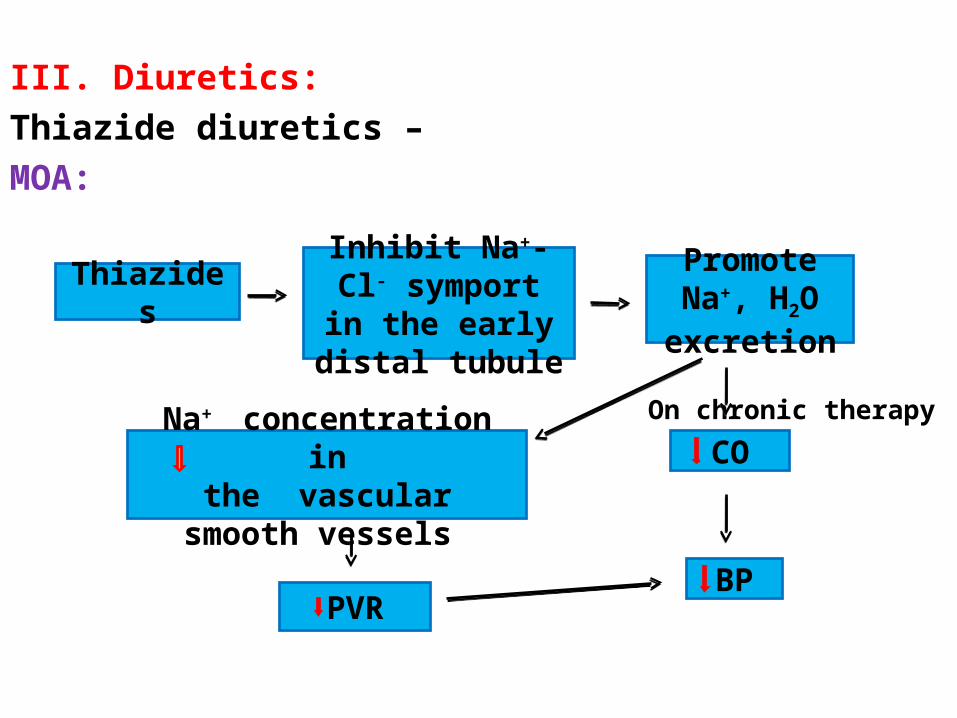
III. Diuretics:Thiazide diuretics –MOA:
On chronic therapy
ThiazidesInhibit Na+-Cl- symport in the
early distal tubule
Promote Na+, H2O excretion
CO
BP
Na+ concentration inthe vascular smooth vessels
PVR

Advantages:• Long duration of action• Cheaper• Well tolerated in elderly patients• Decreases the incidence of fracture in elderly
patients by reducing urinary calcium excretion
Can not be given in patients with gout and hyperlipidaemia

Loop diuretics: Furosemide – not preferred in uncomplicated primary HT because of shorter duration of action
- used in presence of renal failure, CCF or hypertensive emergency

IV. CCBs:• Dihydropyridines (DHPs) – preferred among CCBs -
more selective action on blood vessels• Particularly useful in elderly patients and also in
patients with angina, asthma, pvd, migraine, hyperlipidaemia, diabetes and renal dysfunction
DHPsRelaxes
vascular smooth muscle
PVR
BP

V. Sympatholytics :
a) β-adrenergic blockers – often used as 1st line agents in mild to moderate
hypertension blocks β1 receptors on heart –
HR,
FOC, CO - BP
β-blockers blocks β1 receptors on kidney –
renin release - BP sympathetic outflow - BP

β-adrenergic blockers are mainly useful in –
• Young hypertensives with high renin levels
• Patients with associated conditions such as angina, post MI, migraine and psychosomatic disorders
• Patients receiving vasodilatorsAvoided in pts with asthma, pvd,
diabetes, hyperlipidaemia
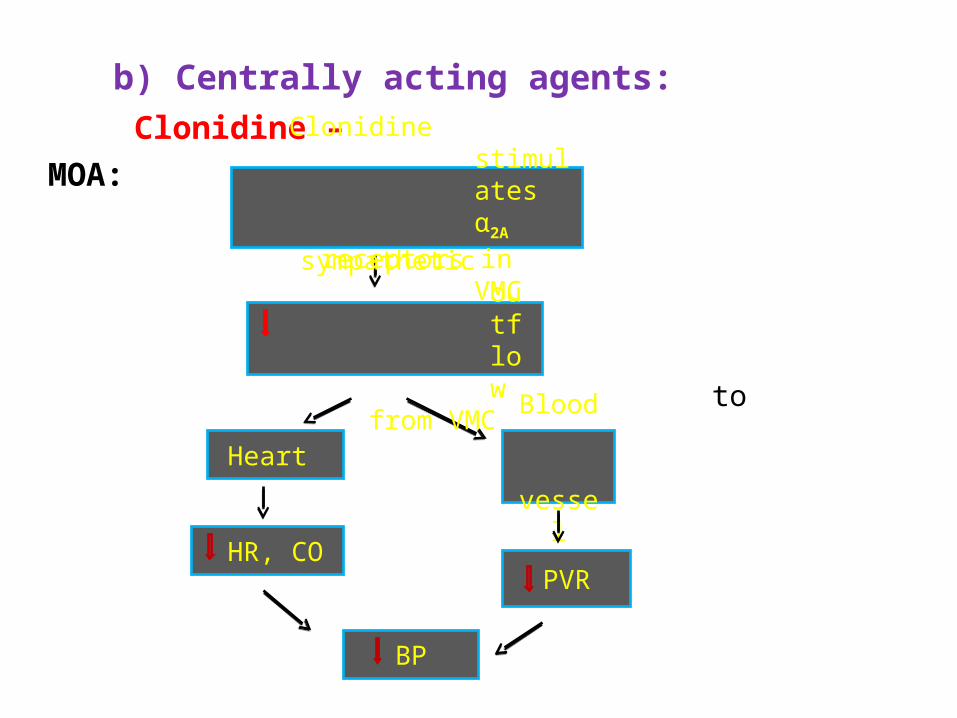
b) Centrally acting agents: Clonidine –
MOA:
to
Heart
Blood vessel
HR, COPVR
BP
Clonidine stimulates α2A
receptors in VMC sympathetic
outflow
from VMC

Adverse effects:
Dryness of mouth & eyes Sedation, depression, nausea, dizziness Bradycardia, impotence, pain Swelling of parotid gland
Sudden stoppage after prolonged use - withdrawal syndrome –
headache, nervousness, tachycardia, sweating, tremors, palpitation & rebound hypertension

α-Methyldopa:MOA – α-methyldopa
α-methyldopamine
α-methylnoradrenaline (false NT)
stimulates α2-VMC
sympathetic outflow
HR,PVR
BP

• Preferred antihypertensive during pregnancy
Adverse effects:
• Nasal stuffiness, dryness of mouth • Headache, sedation, mental depression• Bradycardia, EPS• Impotence, gynaecomastia

c) α-Adrenergic blockers:
α-blockers
Nonselective blockers Selective blockers
Block both α1 & α2- receptors Block selectively α1-
in the blood vessels vascular receptors
Vasodilation & fall in BP Arterial & venodilation(due to α1-blockade)
Noradrenaline release Fall in BP(due to presynaptic α2-blockade)
Reflex tachycardia

Non-selective drugs – not preferred for essential hypertension
Used in special conditions –• Pheochromocytoma• Clonidine withdrawal• Cheese reaction
Prazosin – first dose phenomenon – postural
hypotension after the 1st dose

VI. Vasodilators :
activates
MinoxidilDiazoxide
K+ channel (K+ channel openers)
K+ efflux
Hyperpolarization of vascular smooth
muscle
Vasodilatation
BP

Minoxidil:• Use – promote hair growth in male-type baldness
• AE – reflex tachycardia, Na+ & H2O retention with
edema
Diazoxide:• Use – treatment of hypertensive emergencies
• AE - reflex tachycardia, Na+ & H2O retention,
hyperglycaemia
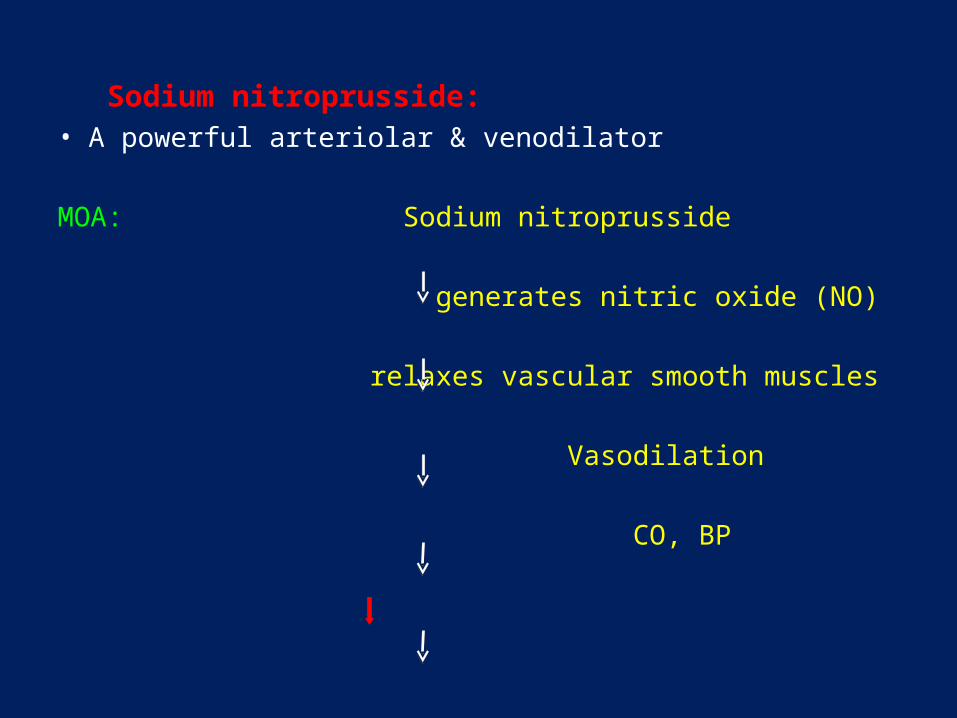
Sodium nitroprusside:• A powerful arteriolar & venodilator
MOA: Sodium nitroprusside
generates nitric oxide (NO)
relaxes vascular smooth muscles
Vasodilation
CO, BP
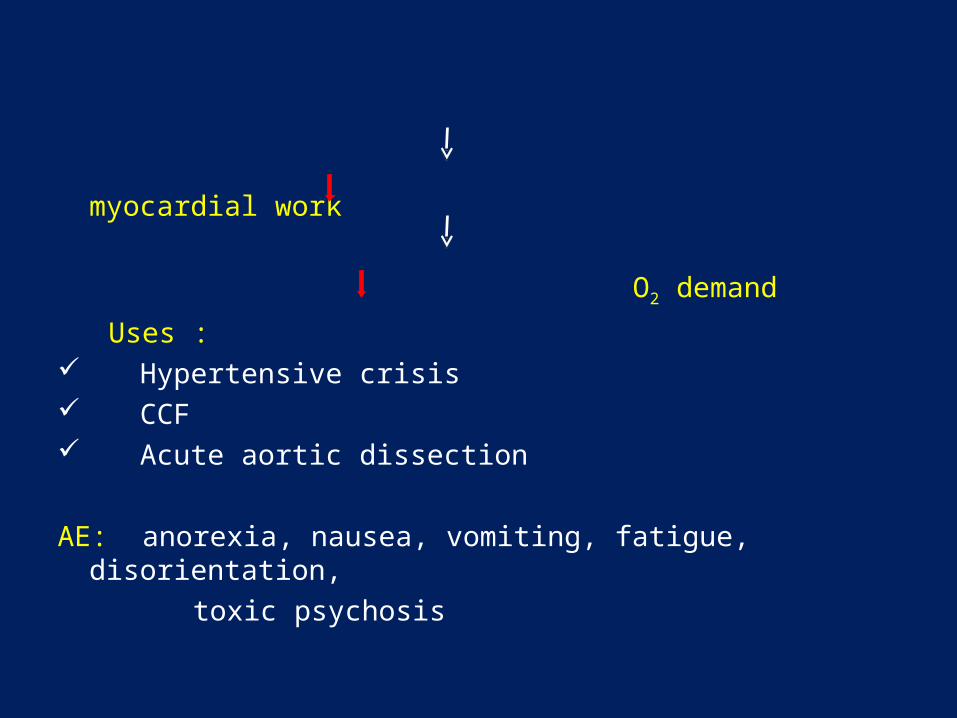
myocardial work
O2 demand
Uses : Hypertensive crisis CCF Acute aortic dissection
AE: anorexia, nausea, vomiting, fatigue, disorientation,
toxic psychosis

Treatment of Hypertension
Non-pharmacological approaches:• Weight reduction• Sodium restriction• Alcohol restriction• Aerobic exercises• Mental relaxation• Smoking cessation• Consumption of potassium-rich diet
Selection of antihypertensive drugs in individual patients depends on:
• Comorbidity• Associated complications• Age• Sex• Cost of the drug• Concomitant drugs

Combination therapy
• Hydralazine/ DHPs & beta blockers• ACEI/ ARBs & Diuretics• Vasodilators & diuretics• ACEI & clonidine/ beta blocker• CCB + ACEI + Diuretic• CCB + beta blocker + diuretic• ACEI + beta blocker + diureticUsed for severe / non responsive / malignant
HT

Thank you
Top Related