Zoom In ISSN: 1545 9616 December 2019 • Volume 18 • Issue ... · panoate (MEP) for Treating...
100
Contents | Zoom In | Zoom Out | Search Issue | Next Page JDD RESIDENT ROUNDS NEWS, VIEWS, & REVIEWS PIPELINE PREVIEWS CLINICAL TRIAL REVIEW ISSN: 1545 9616 December 2019 • Volume 18 • Issue 12 ANTI-AGING · AESTHETIC · MEDICAL DERMATOLOGY Truncal Acne Diabetic Skin Changes Acne Vulgaris in Females: Effect of Age on Efficacy and Tolerability Learning Analytics for Dermatopathology Education Derm In Review Case Studies Image credit page 1233
Transcript of Zoom In ISSN: 1545 9616 December 2019 • Volume 18 • Issue ... · panoate (MEP) for Treating...

Contents | Zoom In | Zoom Out | Search Issue | Next Page
JDD
RESIDENT ROUNDS NEWS, VIEWS, & REVIEWS PIPELINE PREVIEWS CLINICAL TRIAL REVIEW
ISSN: 1545 9616 December 2019 • Volume 18 • Issue 12
ANTI-AGING · AESTHETIC · MEDICAL DERMATOLOGY
Truncal Acne
Diabetic Skin Changes
Acne Vulgaris in Females: Effect of Age on Efficacy and Tolerability
Learning Analytics for Dermatopathology Education
Derm In Review Case Studies
Image credit page 1233
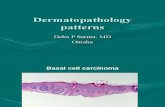
Figure 3. Diagnostic heat map showing areas of diagnostic confusion. The colors on the heat map depict the correlation of resident responses to the correct answers as determined by expert dermatopathologists. Red and blue squares correspond to high and low correlation, respectively. The central diagonal of red squares demonstrates that the majority of residents’ responses are correct. Darker blue corresponds to areas with little diagnostic confusion, and lighter blue, green, orange, and yellow squares represent areas of increasing diagnostic confusion. The most commonly confused items included: acquired fibrokeratoma for traumatic neuroma, angioleiomyoma for schwannoma, traumatic neuroma for neurothekeoma, leiomyoma for hypertrophic scar and vice versa, and Kaposi sarcoma for dermatofibroma.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
TOLERIANEULTRASOOTHING REPAIR MOISTURIZERProvides instant andlong-lasting comfort on skin
100% Preservative-Free – Airtight Packaging
to register to find out more information.
Visit
PreservativeParabenFragranceDrying Alcohol
Build a barrier for even the most sensitive skin
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1193 Volume 18 • Issue 12
Copyright © 2019 EDITORIAL BOARD Journal of Drugs in Dermatology
SENIOR ASSOCIATE EDITORSKenneth Beer MD
Martin Braun MD
Jeffrey Phillip Callen MD
Jean Carruthers MD
James Q. Del Rosso DO
Lawrence F. Eichenfield MD
Patricia Farris MD
Norman Goldstein MD
Aditya K. Gupta MD PhD
Elizabeth Hale MD
Sherry H. Hsiung MD
Leon Kircik MD
Mark Lebwohl MD
Henry W. Lim MD
Flor Mayoral MD
Maurizio Podda MD PhD
Jeffrey Orringer MD
Maritza Perez MD
Kevin Pinski MD
Luigi Rusciani Scorza MD
Ritu Saini MD
Jerome l. Shupack MD
Amy Taub MD
Danny Vleggaar MD
Brian Zelickson MD
FEATURE EDITORSKendra G. Bergstrom MD
Joel L. Cohen MD
Adam Friedman MD
James L. Griffith MD
Marissa Heller MD
Isaac Zilinsky MD
ASSOCIATE EDITORSDale M. Abadir MD
William Abramovits MD
Andrew F. Alexis MD MPH
Shawn Allen MD
Rex A. Amonette MD
Robert Anolik MD
Martha P. Arroyo MD
Robin Ashinoff MD
Marc R. Avram MD
David E. Bank MD
Jay G. Barnett MD
Eliot F. Battle Jr. MD
Richard G. Bennett MD
Diane S. Berson MD
Ronald R. Branacaccio MD
Rana Anadolu Brasie MD
Jeremy A. Brauer MD
Gary Brauner MD
Neil Brody MD PhD
Lance H. Brown MD
Isaac Brownell MD PhD
Karen E. Burke MD PhD
Mariano Busso MD
Francisco M. Camacho-Martinez MD
Marian Cantisano-Zilkha MD
Alastair Carruthers MD
Roger I. Ceilley MD
Clay J. Cockerell MD
David E. Cohen MD
Julian S. Conejo-Mir MD
Elizabeth Alvarez Connelly MD
Ira Davis MD
Calvin Day MD
Doris Day MD
Jeffrey S. Dover MD
Zoe Diana Draelos MD
Madeleine D. Duvic MD
Mohamed L. Elsaie MD
Joseph C. English III MD
Neil Alan Fenske MD
Rebecca Fitzgerald MD
Alina A. Fratila MD
Alejandro Camps Fresnada MD
Ellen C. Gendler MD
Dore Gilbert MD
David J. Goldberg MD
Leonard H. Goldberg MD
Robert H. Gotkin MD
Gloria F. Graham MD
John Hawk MD
Michael P. Heffernan MD
William L. Heimer II MD
N. Patrick Hennessey MD
Alysa R. Herman MD
George J. Hruza MD
Shasa Hu MD
Mark J. Jaffe MD
Jared Jagdeo MD
S. Brian Jiang MD
Bruce E. Katz MD
Mark D. Kaufmann MD
Amor Khachemoune MD
Poong Myung Kim MD
Christine Ko MD
David Kriegel MD
Pearon G. Lang MD
Aimee Leonard MD
Mary P. Lupo MD
Alan Matarasso MD
Alan Menter MD
Warwick L. Morison MD
Rhoda S. Narins MD
Mark Naylor MD
Kishwer S. Nehal MD
Martino Neumann MD
Nelson Lee Novick MD
Jorge J. Ocampo Candiani MD
Philip Orbuch MD
Ariel Ostad MD
Cleire Paniago-Pereira MD
Anna C. Pavlick MD
Christopher R. Payne MD
António Picoto MD
Sheldon V. Pollack MD
Babar K. Rao MD
Wendy E. Roberts MD
Amy E. Rose MD
Steven Rosenberg MD
Lidia Rudnicka MD
Bijan Safai MD
Eli R. Saleeby MD
Fitzgeraldo A. Sanchez-Negron MD
Miguel Sanchez-Viera MD
Julie Schaffer MD
Bryan C. Schultz MD
Daniel Mark Siegel MD
Arthur J. Sober MD
Nicholas A. Soter MD
Jennifer Stein MD
Fernando Stengel MD
Hema Sundaram MD
Susan C. Taylor MD
Emily Tierney MD
George-Sorin Tiplica MD PhD
Ella L. Toombs MD
Irene J. Vergilis-Kalner MD
Steven Wang MD
Ken Washenik MD PhD
Jeffrey Weinberg MD
Robert A. Weiss MD
W. Phillip Werschler MD
Ronald G. Wheeland MD
Jai Il Youn MD
John Zic MD
John A. Zitelli MD
PAST CO-EDITORS-IN-CHIEFElizabeth Hale MD (2004)
Susan H. Weinkle MD (2005-2008)Keyvan Nouri MD (2005-2008)Sherry H. Hsiung MD (2008)
James M. Spencer MD (2009-2013)
EDITOR-IN-CHIEFPerry Robins MD
CO-EDITOR-IN-CHIEFDeborah S. Sarnoff MD
Macrene Alexiades MD PhD
Robert Baran MD
Joseph B. Bikowski MD
Dee Anna Glaser MD
C. William Hanke MD
William Levis MD
Ronald L. Moy MD
Keyvan Nouri MD
Neil S. Sadick MD
Gerhard Sattler MD
James M. Spencer MD
Susan H. Weinkle MD
SENIOR EDITORS
Impact FactorImpact Factor Score: 1.394*
Normalized Eigenfactor® Score: 0.574*
Article Influence Score: 0.378*
*Clarivate Analytics, Formerly the IP & Science Business of Thomson Reuters, June 2019
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1194 Volume 18 • Issue 12
Copyright © 2019 TABLE OF CONTENTS Journal of Drugs in Dermatology
ORIGINAL ARTICLES
1198 Oral Polypodium Leucotomos Extract and Its Impact on Visible Light-Induced Pigmentation in Human SubjectsTasneem F. Mohammad MD, Indermeet Kohli PhD, Cynthia L. Nicholson MD, German Treyger DO, Suteeraporn Chaowattanapanit MD, Amanda F. Nahhas DO, Taylor L. Braunberger MD, Henry W. Lim MD, Iltefat H. Hamzavi MD
1205 Truncal Acne: A Neglected EntityJames Q. Del Rosso DO, Linda Stein-Gold MD, Charles Lynde MD, Emil Tanghetti MD, Andrew F. Alexis MD MPH
1211 Diabetic Skin Changes Can Benefit from Moisturizer and Cleanser Use: A ReviewRobert S. Kirsner MD PhD, Gil Yosipovitch MD FAAD, Shasa Hu MD FAAD, Anneke Andriessen PhD, Jason R. Hanft DPM FACFAS, Paul J. Kim DMP MS, Lawrence Lavery DPM MPH, Luigi Meneghini MD MBA, Lee C. Ruotsi MD ABWMS CWS-P UHM
1218 Tretinoin 0.05% Lotion for the Once-Daily Treatment of Moderate and Severe Acne Vulgaris in Females: Effect of Age on Efficacy and TolerabilityLinda Stein Gold MD, David M. Pariser MD, Eric Guenin PharmD PhD MPH
1226 Evaluation of Efficacy of a Skin Care Regimen Containing Methyl Estradiolpro-panoate (MEP) for Treating Estrogen Deficient SkinJoel L. Cohen MD
1231 Learning Analytics to Enhance Dermatopathology Education Among Dermatology ResidentsEuphemia W. Mu MD, Martin Pusic MD PhD, Matt Coneybeare BA MBA, Shane A. Meehan MD
1237 Hispanic Tattoo Artists Could Provide Skin Cancer Prevention via Aftercare Instructions and Social Media Cristian D. Gonzalez MD, Adrian Pona MD, Barbara J. Walkosz PhD, Robert P. Dellavalle MD PhD MSPH
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Copyright © 2019 ALASTIN Skincare®, Inc. All rights reserved.www.Alastin.comReferences: 1. Clinical data on file at ALASTIN Skincare®. 2. Widgerow AD, Fabi SG, Palestine RF, et al. Extracellular matrix modulation: optimizing skin care and rejuvenation procedures. J Drugs Dermatol. 2016;15(4)(suppl):s63-s71.
TransFORM Body Treatment with TriHex Technology® accelerates and enhances body contouring outcomes.
ACCELERATE results: After hot or cold body fat reduction procedures.1 Faster visible results
ENHANCE results: After body-skin tightening procedures or as a daily stand-alone treatment to improve the appearance of skin texture, laxity, and crepiness.2
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1196 Volume 18 • Issue 12
Copyright © 2019 TABLE OF CONTENTS Journal of Drugs in Dermatology
ORIGINAL ARTICLES (CONTD)
1244 Dietary Lycopene Protects SKH-1 Mice Against Ultraviolet B-Induced Photo- carcinogenesisKaren E. Burke MD PhD, Xueyan Zhou MD MS, Yongyin Wang PhD, Huachen Wei MD PhD
1255 Gene Expression Studies Pertaining to Extracellular Matrix Integrity and Remodeling: Nuances and Pitfalls of In Vitro InvestigationsAlan D. Widgerow MBBCh MMed (Plast) FCS FACS, John A. Garruto BS
1261 Histopathological Changes After Experimental Skin Resurfacing Using an Improved Fractional High-Power 1064-nm Q-Switched Nd:Yag LaserFernando Urdiales-Gálvez MD, Mario A. Trelles MD PhD, Sandra Martín-Sánchez MD, Mónica Maiz-Jiménez MD
1268 The Fate of Active Acne and Acne Scars Following Treatment With Fractional RadiofrequencyBruce E. Katz MD
CASE REPORTS
1276 Response of Lichen Planopilaris to Pioglitazone HydrochlorideErik L. Peterson BS, Daniel Gutierrez MD, Nooshin K. Brinster MD, Kristen I. Lo Sicco MD, Jerry Shapiro MD
1281 Methacrylate Polymer Powder Dressing for a Nasal Surgical Defect Matthew J. Lin MD, Danielle P. Dubin BA, Aaron S. Farberg MD, Hooman Khorasani MD, David A. Kriegel MD
LETTER TO THE EDITOR
1274 The Impact of Submental Deoxycholic Acid Injections on Neck SurgeryMatthew J. Lin MD, Danielle P. Dubin BA, Robert M. Schwarcz MD, Hooman Khorasani MD
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1197 Volume 18 • Issue 12
Copyright © 2019 TABLE OF CONTENTS Journal of Drugs in Dermatology
Journal of Drugs in Dermatology (JDD) is indexed in MEDLINE®/PubMed® and is published monthly by the Journal of Drugs in Dermatology115 E. 23rd Street, 3rd Floor, Unit 322, New York, NY 10010telephone: 212-213-5434 | fax: 212-213-5435 | JDDonline.com
No part of this publication may be reproduced, stored in a retrieval system, or transmitted in electrical or other forms or by any means without prior written permission from the Journal of Drugs in Dermatology (JDD). This publication has been registered with the Library of Congress (ISSN: 1545 9616). The publisher and the organizations appearing herein assume no responsibility for any injury and/or damage to persons or property as a matter of product liability, negligence, or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein. No suggested test or procedure should be carried out unless, in the reader’s judgment, its risk is justified. Because of the rapid advances in the medical sciences, we recommend that independent verification of diagnoses and drug dosages should be made. Discussions, views, and recommendations as to medical procedures, choice of drugs, and drug dosages are the responsibility of the authors. Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the editors, publisher, or staff. The editors, publisher, and staff disclaim any responsibility for such material and do not guarantee, warrant, or endorse any product or service advertised in this publication nor do they guarantee any claim made by the manufacturer of such product or service.
Although all advertising material is expected to conform to ethical and medical standards, inclusion in this publication does not constitute a guarantee or endorsement by the Journal or its staff of the quality or value of such products or of the claims of any manufacturer. The paper used in this publication meets the minimum requirements of the American National Standard for Information Sciences Permanence of Paper for Printed Library Materials, ANSI Z39.48-1992.
© 2019 Journal of Drugs in Dermatology
Journal of Drugs in Dermatology (JDD) (ISSN 1545-9616) is published monthly for $300 per year US Individual subscriptions/ $350 per year International Individual subscriptions/(Corporate and Institutional rates contact Sales for a quote) by the Journal of Drugs in Dermatology, 115 E. 23rd Street, 3rd Floor, Unit 322, New York, NY 10010. Periodicals postage paid at New York, NY and additional mailing offices.
ADVERTISING & CORPORATE & INSTITUTIONAL SALES: Contact Nick Gillespie at 646-453-5711 e-mail: [email protected]
REPRINTS & PERMISSIONS: Contact Luz Figueroa at 646-736-4338 e-mail: [email protected]
SUBSCRIPTIONS: Email [email protected] or call 212-213-5434 ext. 4
POSTMASTER: Send address changes to the Journal of Drugs in Dermatology, 115 E. 23rd Street, 3rd Floor, Unit 322, New York, NY 10010.
Publishers Shelley N. Tanner Lawrence E. Robins
Executive Editor Karin Beehler
Associate Editor Kathleen Leary RN
Associate Publisher Nick Gillespie
Scientific Publications Liaison Luz Figueroa
Design Karen Rebbe
OFFICIAL PUBLICATION OF
FEATURES
1282 ARTE Poster Competition Winner: The 5 P’s of Pyoderma Gangrenosum Brett C. Neill MD, Edward W. Seger MS, Tyler A. Hooton BS, Gabrielle Bailey BS, Anand Rajpara MD, William V. Stoecker MD MS
1285 Senior Resident Peer-To-Peer Case StudiesMisty Eleryan MD, Angelo Landriscina MD
1288 Pipeline Previews
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1198 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Oral Polypodium Leucotomos Extract and Its Impact on Visible Light-Induced Pigmentation in Human Subjects
Tasneem F. Mohammad MD,ª Indermeet Kohli PhD,B Cynthia L. Nicholson MD,B German Treyger DO,c
Suteeraporn Chaowattanapanit MD,D Amanda F. Nahhas DO,E Taylor L. Braunberger MD,a Henry W. Lim MD,ª Iltefat H. Hamzavi MDª
aDepartment of Dermatology, Henry Ford Hospital, Detroit, MIbDepartment of Dermatology, Wayne State University, Detroit, MI
cDepartment of Dermatology, Beaumont Hospital, Trenton, MIDDepartment of Medicine, Srinagarind Hospital, Khon Kaen, Thailand
EDepartment of Dermatology, Beaumont-Farmington Hills, Farmington Hills, MI
Background: Visible light (VL) has multiple effects on the skin that currently available sunscreens do not protect against. Polypodium leucotomos extract (PLE) has properties that may offer protection against VL. Objectives: To determine the effectiveness of PLE in preventing VL-induced effects. Methods: Twenty-two subjects with Fitzpatrick skin phototype IV-VI were enrolled. On day 0, subjects were irradiated with VL. Clinical Investigator’s Global Assessment (IGA) scoring and spectroscopic evaluations were performed immediately, 24 hours, and 7 days after irradiation. Subjects then received a 28-day supply of PLE (480 mg daily). Irradiation and evaluation were repeated. Three 4-mm punch biopsies were obtained for immunohistochemistry analysis: one from normal unirradiated skin and the other two twenty-four hours after irradiation, pre- and post-PLE, from sites irradiated with highest dose of VL. Results: All subjects had immediate pigment darkening, persistent pigment darkening, and delayed tanning both pre- and post-PLE. For the highest VL dose (480 J/cm²) spectroscopic assessments demonstrated a statistically significant decrease in persistent pig-ment darkening and delayed tanning post-PLE. In addition, there was a significant decrease in cyclooxygenase-2, and a trend towards decreases in the markers for cellular damage post-PLE. While there was a trend towards lower IGA scores post-PLE, statistical signifi-cance was not reached possibly due to lack of sensitivity of the visual IGA scoring system in detecting small changes. Conclusions: Spectroscopic data and immunohistochemistry indicate an effect of PLE on visible light induced effects. As such, PLE may be used as an adjuvant to traditional means of photoprotection to protect against the effects of VL. Clinical trial registration number: NCT02904798.
J Drugs Dermatol. 2019;18(12):1198-1203.
ABSTRACT
INTRODUCTION
Approximately 44% of sunlight is composed of visible light (VL).1 VL has been shown to have multiple bio-logic effects on the skin2 including DNA damage sec-
ondary to the production of reactive oxygen species (ROS), the induction of pro-inflammatory cytokines,3 worsening of photo-exacerbated conditions,4 and pigmentation in melano-competent individuals.5,6 Pigmentation caused by VL occurs in 3 stages.6 The first, immediate pigment darkening (IPD), occurs immediately after exposure and can last up to 2 hours. IPD is followed by persistent pigment darkening (PPD), which occurs between 2 to 24 hours after exposure. Both IPD and PPD are caused by the oxidation and redistribution of existing melanin in the skin. The final stage is delayed tanning (DT), which occurs 24 hours to several days after exposure and is caused by the new production of melanin.6
Disorders of pigmentation such as melasma and post-inflam-matory hyperpigmentation are relatively common in those with skin of color. Affected individuals often note worsening of cutaneous hyperpigmentation after sun exposure despite appropriate application of broad- spectrum sunscreens. This is in part because currently available organic sunscreens and micronized inorganic sunscreens primarily protect against ul-traviolet (UV) radiation, but are ineffective against VL.4 Iron oxides, which are present in make-up and tinted products, are effective against VL. However, many people are resistant to the idea of wearing “make-up” for photoprotection. They are also not water or sweat resistant. Taken together, alternative, and supplementary methods of protection against VL induced ef-fects, such as oral antioxidants, are necessary.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1199
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
T.F. Mohammad, I. Kohli, C.L. Nicholson, et al
Light Sources and IrradiationThe light source used in this study was a Fiber-Lite (Dolan-Jenner Industries, Boxborough, MA) with a 150W EKE lamp. The spectral output consisted of over 97.5% VL, with less than 0.5% and 2.0% of UVA1 and infrared radiation, respectively. The UVA1 contribution in the spectral output has been shown to be insufficient to cause pigmentation on its own based on known minimal tanning doses.13 The fluence rate was adjusted to either 250 mW/cm2 or 200 mW/cm2 using an Oriel thermopile (Oriel, Stamford, CT). A fluence rate of 250 mW/cm2 was used in most subjects. As the output of the radiation source included trace amounts of UVA1, if a subject was on photosensitizing medica-tion in the UVA1 range, a fluence rate of 200 mW/cm2 was used instead. However, the same fluence rate was used for both pre- and post-PLE irradiation for a given subject.
Clinical and Spectroscopic AssessmentsClinical photography and Investigator Global Assessment (IGA). Clinical photographs of the back were taken at each visit. The degree of pigmentation and erythema in each site was graded using an Investigator Global Assessment (IGA) scale (Table 1). The same investigator performed IGA scoring both pre- and post-PLE.
Diffuse reflectance spectroscopy. This non-invasive objective assessment technique quanti-fies the degree of melanin and hemoglobin in lesions, which corresponds to pigmentation and erythema, respectively. Dif-fuse reflectance spectroscopy was used to collect absorbance spectra at each visit within the irradiated site and at adjacent normal skin. The methodology has been described in detail in our previous publication.5 To summarize, an average of 3 mea-surements was used for analysis. The difference between the absorbance spectra of irradiated and normal skin was calculated and integrated between 400-700 nm. This integrated value (area under the curve) was referred to as the relative pigment since it included contributions from both melanin and hemoglobin, cor-responding to the overall darkness of the irradiated site. Higher values of relative pigment correspond to a darker lesion. The pre-PLE relative pigment was compared to post-PLE relative pigment for the corresponding time point. In addition, the ratio of pre-PLE relative pigment to that of post-PLE relative pigment was used to calculate the VL protection factor for a given assess-ment time point.14
PLE is an over-the-counter supplement derived from a fern native to Central and South America,7 which has multiple an-ti-inflammatory, immunomodulatory, chemoprotectant, and antioxidant properties.2 One effect of PLE is that it enhances the endogenous antioxidant system, which neutralizes superoxide anions, lipid peroxides, and hydroxyl radicals.3,8,9 PLE has also been shown to suppress UV-induced erythema, and to decrease cyclooxygenase (COX)-2, p53, cyclobutane pyrimidine dimers, epidermal proliferation, sunburn cells, and inflammatory infil-trates induced by UV radiation.10,11 More recently, PLE was shown to decrease VL-induced cell death, matrix metalloproteinase (MMP)-1 production, and other alterations of the extracellular matrix in an in-vitro model.12 Given the photoprotective effects of PLE and its antioxidant properties, this study was designed to quantify the effects of oral PLE on VL-induced pigmentation in human subjects.
MATERIALS AND METHODSStudy SubjectsTwenty-seven healthy males and females with skin pho-totypes IV-VI were enrolled in this study, with 24 subjects completing the study. This study was approved by the Insti-tutional Review Board at Henry Ford Hospital (IRB# 8385) and all guidelines from the Declaration of Helsinki were followed. Informed consent was obtained from all participants. Exclusion criteria included current or past history of skin cancer, photo-aggravated conditions, photosensitizing medications in the VL range, tanning, intention to become pregnant, pregnancy, and lactation. Subjects were willing to limit direct exposure of areas being irradiated to light during the study. Urine pregnancy tests were performed for any females of child-bearing potential with a last menstrual period of over 5 weeks.
Study DesignSubjects were irradiated with 5 doses of VL on the left side of the back at 6 sites on day 0. IPD was then assessed. The doses were 40, 80, 160, 320, and 480 J/cm2, with the dose of 480 J/cm2 being repeated for biopsy purposes. PPD and DT did not occur at 40 and 80 J/cm2 in the first 13 subjects, therefore, these doses were eliminated for the remaining subjects. On day 1, PPD was assessed and biopsies were performed of normal skin and 1 of the sites irradiated at 480 J/cm2. On day 7, DT was assessed, and suture removal performed. In addition, subjects were given a 28-day supply of oral PLE (Heliocare, Cantabria Labs, Madrid, Spain) with instructions to take 2 pills (total dose 480 mg) 1 hour apart between the hours of 8 AM and noon starting on day 8. Day 0 through 7 responses are referred to as pre-PLE in the remainder of the manuscript. On day 35, subjects returned for VL irradiation of the right back at the same doses and number of sites as was performed pre-PLE. Post-PLE IPD was assessed and the number of remaining PLE pills recorded to ensure com-pliance. Day 36 consisted of assessment of post-PLE PPD and biopsy of the second dose of 480 J/cm2. Post-PLE DT was as-sessed on day 42 in addition to suture removal.
TABLE 1.
Investigator Global Assessment Scale for Pigmentation
IGA Hyperpigmentation
0 Clear of hyperpigmentation
1 Almost clear of hyperpigmentation
2 Mild but noticeable hyperpigmentation
3 Moderate hyperpigmentation (medium brown in quality)
4 Severe hyperpigmentation (dark brown in quality)
5 Very severe hyperpigmentation (very dark brown, almost black in quality)
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1200
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
T.F. Mohammad, I. Kohli, C.L. Nicholson, et al
ImmunohistochemistryThe following stains were performed on the specimens biop-sied: COX-2, cyclin D1, MMPs 1, 2, and 9, Fontana Masson, Melan-A/Mart 1, and B-cell lymphoma (Bcl)-2. These stains as-sessed inflammation, cell cycle progression, structural integrity, pigmentation, and apoptosis, respectively.
COX-2, cyclin D1, and melanoma-associated antigen recog-nized by T cells (MART)-1 were counted for positive cells with an Olympus BX51 microscope fitted to an Olympus DP71 digital camera (Olympus America, Inc., Center Valley, PA) at 40x mag-nification. Positive cells of MART-1 were counted throughout the tissue sections while the numbers of positive cells per 100 epidermal cells of COX-2 and cyclin D1 were counted at 3 differ-ent microscope fields. Each field consisted of the edges of both sides and the centre of the tissue sections by using photographs at 40x magnification. Brown nuclear staining was considered as positive for cyclin D1, while cytoplasmic staining was consid-ered as positive for COX-2. The number of positive cells was assessed by 2 independent observers and the average number of positive cells was calculated.
MMP-1, MMP-2, MMP-9, Bcl-2, and Fontana-Masson were evalu-ated by intensity scores (Table 2). Keratinocytes, and dermal fibroblasts were evaluated for MMP-1, MMP-2 and MMP-9, and basal keratinocytes were assessed for Bcl-2. The intensity scores were assessed by 2 independent observers from 6 dif-ferent fields at 40x magnification and the average score was calculated.
Statistical AnalysisPaired t-tests were used to compare IGA scores, relative pigment intensity, and immunohistochemistry results. When the t-test assumption of distribution normality was violated, the Wilcoxon signed rank test was performed instead. Statistical significance was set at p-values less than 0.05. Immunohistochemistry find-ings of day 1, referred to as pre-PLE, were compared with those on day 36, referred to as post-PLE. For IGA and relative pigment intensity, comparisons were made for each time point IPD, PPD,
and DT. All analyses were done using SAS software (version 9.4, SAS Institute Inc., Cary, NC).
RESULTSAll subjects had an IPD response at the VL doses delivered, but PPD and DT were not consistently present or were subtle. As such, the results reported will focus on the highest VL dose (480 J/cm2). Two subjects formed blisters at the dose of 480 J/cm2during the post-PLE irradiation visit (day 35), which was like-ly secondary to fluctuations in the intensity of the lamp in the radiation source. The lamp was replaced, and the light source was recalibrated. Another course of PLE was given to 1 of the subjects who blistered, with repetition of all post-PLE visits. The subject did not form blisters post-PLE once the light source had been recalibrated, and it was concluded that PLE was not the cause of blistering. The data from the 2 subjects who blistered was excluded.
Clinical Photography and Investigator Global Assessment (IGA)At the DT assessment time point, 7 out of 22 (32%) subjects had a decrease in IGA scores post-PLE (Figure 1). Although there was a trend towards lower IGA scores post-PLE, statistical sig-nificance was not reached (p = 0.07) (Figure 2).
Diffuse Reflectance SpectroscopyAt a dose of 480 J/cm2, post-PLE there was a statistically sig-nificant decrease in the amount of relative pigment when comparing PPD and DT (P<0.05) (Figure 3). In addition, PLE ex-hibited a VL protection factor of 1.3, 1.5 and 1.5 at the IPD, PPD and DT time points, respectively.
TABLE 2.
Intensity Scoring System for Select Stains
Score Interpretation
-4 >75% decrease in intensity when compared to control
-3 51%-75% decrease in intensity when compared to control
-2 26%-50% decrease in intensity when compared to control
-1 10%-25% decrease in intensity when compared to control
0 Unchanged when comparing to control
1 10%-25% increase in intensity when compared to control
2 26%-50% increase in intensity when comparing to control
3 51%-75% increase in intensity when comparing to control
4 75% increase in intensity when comparing to control
FIGURE 1. Clinical photography and IGA scoring of a subject pre- and post-PLE. Abbreviations: IGA, Investigator Global Assessment; PLE, Polypodium leucotomos extract.
Pre=PLE Post=PLE
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1201
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
T.F. Mohammad, I. Kohli, C.L. Nicholson, et al
ImmunohistochemistryThere was a statistically significant decrease in COX-2 staining post-PLE. In addition, there was a strong trend towards reduc-tions in MMP-2, and a weak trend towards reductions in MART-1, MMP-1, MMP-9, and Bcl-2 post-PLE. No change in pigmentation was detected with Fontana Masson among control, pre-, and post- PLE sites likely because tissue specimens were obtained 24 hours after irradiation, but new pigment formation takes longer (approximately 5-7 days). As such, histologically, differ-ence in pigmentation could not be assessed. A post-PLE trend towards an increase in cyclin D1 was observed (Tables 3 and 4).
Adverse EventsTwo consecutive subjects in this study blistered at a dose of 480 J/cm2 during the post-PLE irradiation visit. However, this was unlikely to be related to PLE as when one of these patients was given a second course of PLE and re-irradiated, no blister was observed. Of note, re-irradiation was performed after lamp re-placement and recalibration of the light source. Three subjects
experienced intermittent gastrointestinal upset, 3 experienced pruritus, and 1 subject complained of dry mouth.
DISCUSSIONIn this study, a real-world relevant dose of 480 J/cm2 VL was used, which is equivalent to approximately 160 minutes of sun-light exposure.15 This study demonstrated that at this VL dose, the administration of oral PLE prior to irradiation led to a de-
FIGURE 2. Pre-PLE and post-PLE average IGA scores for pigmentation as a function visit number at a visible light dose of 480 J/cm2. Abbreviations: IGA, Investigator Global Assessment; PLE, Polypodium leucotomos extract.
FIGURE 3. Diffuse reflectance spectroscopy measured relative pigment pre-PLE and post-PLE as a function visit number at a visible light dose of 480 J/cm². Abbreviations: PLE, Polypodium leucotomos extract.
TABLE 3.
Staining Results for the Change from to Pre-PLE to Post-PLE
IGA N Mean SD Median P-value
COX post-PLE minus pre-PLE
22 -2.20 4.33 -2.833 0.0271
Cyclin post-PLE minus pre-PLE
22 3 7.43 3.67 0.072
MART post-PLE minus pre-PLE
22 -0.39 9.70 1.50 0.85
COX, cyclooxygenase; MART, melanoma-associated antigen recognized by T cells; PLE, Polypodium leucotomos extract; SD, standard deviation1P < 0.05
TABLE 4.
Other Staining Results for the Change from Pre-PLE to Post-PLE (Post - Pre)
Variable N Mean SD Median P=value
Change from pre-PLE to post-PLE for Fontana Masson
22 0.00 0.98 0.00 1.00
Change from pre-PLE to post-PLE for MMP 1
22 -0.27 0.93 0.00 0.18
Change from pre-PLE to post-PLE for MMP 2
15 -0.60 1.06 -1.00 0.07
Change from pre-PLE to post-PLE for MMP 9
22 -0.27 0.90 0.00 0.16
Change from pre-PLE to post-PLE for Bcl-2
22 -0.27 1.07 0.00 0.24
Bcl, B-cell lymphoma; MMP, matrix metalloproteinase; PLE, Polypodium leu-cotomos extract; SD, standard deviationP<0.05
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1202
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
T.F. Mohammad, I. Kohli, C.L. Nicholson, et al
crease in pigmentation at all time points, as assessed clinically via IGA scoring, though not statistically significant (Figure 2). Diffuse reflectance spectroscopy (DRS) demonstrated a statis-tically significant decreases in PPD and DT based on relative pigment intensity (Figure 3). As IGA is a visual assessment, while DRS is an objective, instrument-based measurement, these results clearly demonstrate the limitations of IGA, even when performed by experienced evaluators.
Immunohistochemistry results showed a statistically signifi-cant decrease in inflammation, and a trend toward decreases in markers for certain collagen remodelling markers post-PLE. There was also a weak trend towards a decrease in melano-cytes, other collagen remodelling markers, and apoptotic markers post-PLE. These were consistent with PLE’s previously proven antioxidant and anti-inflammatory characteristics. There-fore, while clinical improvements were not noted in all subjects, effects by PLE were observed as demonstrated by spectroscopy and immunohistochemistry. In this study, a total daily dose of 480 mg of PLE was used. PLE has been shown to have no ob-servable side effects even at daily doses as high as 1080 mg.16
Therefore, it is possible with higher doses of PLE, an even more noticeable protective effect against VL-induced changes would be observed. The non-significant increase in cyclin D1, which indicates cell cycle progression, requires further investigation. VL has multiple effects on the skin, including erythema, DNA damage secondary to ROS, pigmentation, and the induction of pro-inflammatory cytokines, as well as MMPs 1 and 9.1,3,4,6,9,17 Because PLE has antioxidant as well as anti-inflammatory prop-erties, it is likely that these mechanisms could contribute to downregulation of the deleterious effects of VL by quenching ROS and reducing inflammation. It should be noted that while multiple formulations of PLE exist, all the published studies to date have been done with PLE sourced from a single source (Heliocare, Cantabria Lab, Madrid, Spain), the preparation used in this study. In a recent in vitro study comparing the photo-protective properties of different PLE preparations, preparation sourced from the referenced lab was shown to have the most potent property.18
While down-regulating pigmentation induced by VL is important, especially in people with skin of color, the potential for carci-nogenesis induced by VL is also a concern. Oxidative damage caused by irradiation with wavelengths ranging from 312-434 nm, which partially fall into the VL spectrum, have been shown to potentially cause both melanoma and non-melanoma skin cancer in human skin cells.17 The availability of high SPF, broad-spectrum sunscreens allows people to spend greater amounts of time in direct sunlight with decreased risk of sunburn. This leads to greater exposure to VL, and possible increased DNA damage secondary to ROS contributing to the formation of skin cancer.
Currently available sunscreens are either ineffective against VL, or for those that protect on the VL spectrum, cosmetically unacceptable to most patients. While PLE is not a substitute for sunscreen, it could serve as an oral adjuvant to provide protection against VL. PLE has previously been shown to down-regulate the biologic effects of UVB and UVA.6,10,11,19,20 As such, PLE can potentially offers broad-spectrum protection that can supplement sunscreens and phototprotective clothing, espe-cially in those with photo-exacerbated conditions.
CONCLUSIONVL has multiple potential deleterious effects on the skin. The administration of oral PLE prior to light exposure offers some protection against pigmentation, inflammation, and cellu-lar damage caused by VL. As an over-the-counter supplement with an excellent safety profile, it can be used in patients as an adjuvant to, but not a substitute for, sunscreen, and other pho-toprotective measures.
DISCLOSURESDrs. Lim, Hamzavi, Kohli, Mohammad, Nicholson, Nahhas, and Braunberger are investigators for Ferndale, Allergan, Unigen, and Estee Lauder. Drs. Hamzavi and Kohli have also served as investigators for Bayer and Johnson and Johnson. Dr. Kohli has served as an investigator for Pfizer and Drs. Lim and Hamzavi have served as an investigator for Incyte. All grants paid to in-stitution. Dr. Lim has participated as a speaker in an educational session sponsored by Pierre Fabre. Drs. Treyger and Chaowat-tanapanit have no disclosures to report. Funding: This study was funded by Ferndale Laboratories.
ACKNOWLEDGMENTWe would like to thank Drs. Liaqat Ali and Darius Mehregan from Pinkus Dermatopathology Laboratory for their assistance with the histologic aspects of this study as well as Angela Parks-Miller for project management, and Andrew Clark for fi-nancial management of the research study. We would also like to acknowledge Gordon Jacobsen for his assistance with the statistical analysis.
REFERENCES1. Randhawa M, Seo I, Liebel F, Southall MD, Kollias N, Ruvolo E. Visible light
induces melanogenesis in human skin through a photoadaptive response. PLoS One. 2015;10(6):e0130949.
2. Parrado C, Mascaraque M, Gilaberte Y, Juarranz A, Gonzalez S. Fernblock (Polypodium leucotomos extract): molecular mechanisms and pleiotropic ef-fects in light-related skin conditions, photoaging and skin cancers, a review. Int J Mol Sci. 2016;17(7):E1026.
3. Liebel F, Kaur S, Ruvolo E, Kollias N, Southall MD. Irradiation of skin with visible light induces reactive oxygen species and matrix-degrading enzymes. J Invest Dermatol. 2012;132(7):1901-1907.
4. Mahmoud BH, Hexsel CL, Hamzavi IH, Lim HW. Effects of visible light on the skin. Photochem Photobiol. 2008;84(2):450-462.
5. Kohli I, Chaowattanapanit S, Mohammad TF, et al. Synergistic effects of long-wavelength ultraviolet A1 and visible light on pigmentation and erythema. Br J Dermatol. 2018;178(5):1173-1180.
6. Mahmoud BH, Ruvolo E, Hexsel CL, et al. Impact of long-wavelength UVA and visible light on melanocompetent skin. J Invest Dermatol. 2010;130(8):2092-2097.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1203
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
T.F. Mohammad, I. Kohli, C.L. Nicholson, et al
15. ASTM International. ASTM G173 - 03(2012): Standard tables for reference solar spectral irradiances: direct normal and hemispherical on 37° tilted sur-face. West Conshohocken, PA: ASTM International; 2012.
16. Winkelmann RR, Del Rosso J, Rigel DS. Polypodium leucotomos ex-tract: a status report on clinical efficacy and safety. J Drugs Dermatol. 2015;14(3):254-259.
17. Kvam E, Tyrrell RM. Induction of oxidative DNA base damage in human skin cells by UV and near visible radiation. Carcinogenesis. 1997;18(12):2379-2384.
18. González S, Lucena SR, Delgado P, Juarranz A. Comparison of several hydro-philic extracts of Polypodium leucotomos reveals different antioxidant moi-eties and photoprotective effects in vitro. J Med Plant Res. 2018;12(22):336-345.
19. Kohli I, Shafi R, Isedeh P, et al. The impact of oral Polypodium leucotomos extract on ultraviolet B response: a human clinical study. J Am Acad Derma-tol. 2017;77(1):33-41 e31.
20. Philips N, Smith J, Keller T, Gonzalez S. Predominant effects of Polypodium leucotomos on membrane integrity, lipid peroxidation, and expression of elastin and matrixmetalloproteinase-1 in ultraviolet radiation exposed fibro-blasts, and keratinocytes. J Dermatol Sci. 2003;32(1):1-9.
7. Choudhry SZ, Bhatia N, Ceilley R, et al. Role of oral Polypodium leucotomos extract in dermatologic diseases: a review of the literature. J Drugs Derma-tol. 2014;13(2):148-153.
8. Gomes AJ, Lunardi CN, Gonzalez S, Tedesco AC. The antioxidant action of Polypodium leucotomos extract and kojic acid: reactions with reactive oxy-gen species. Braz J Med Biol Res. 2001;34(11):1487-1494.
9. Gonzalez S, Pathak MA. Inhibition of ultraviolet-induced formation of reac-tive oxygen species, lipid peroxidation, erythema and skin photosensitiza-tion by polypodium leucotomos. Photodermatol Photoimmunol Photomed. 1996;12(2):45-56.
10. Middelkamp-Hup MA, Pathak MA, Parrado C, et al. Oral Polypodium leu-cotomos extract decreases ultraviolet-induced damage of human skin. J Am Acad Dermatol. 2004;51(6):910-918.
11. Zattra E, Coleman C, Arad S, et al. Polypodium leucotomos extract decreases UV-induced Cox-2 expression and inflammation, enhances DNA repair, and decreases mutagenesis in hairless mice. Am J Pathol. 2009;175(5):1952-1961.
12. Zamarron A, Lorrio S, Gonzalez S, Juarranz A. Fernblock prevents dermal cell damage induced by visible and infrared A radiation. Int J Mol Sci. 2018;19(8):E2250.
13. Kohli I, Sakamaki T, Tian WD, Moyal D, Hamzavi IH, Kollias N. The dynamics of pigment reactions of human skin to ultraviolet-A radiation. Photodermatol Photoimmunol Photomed. 2019.
14. Kohli I, Nahhas AF, Braunberger TL, et al. Spectral characteristics of visible light-induced pigmentation, and visible light protection factor. Photoderma-tol Photoimmunol Photomed. 2019.
AUTHOR CORRESPONDENCE
Iltefat H. Hamzavi MDE-mail:................…….............................. [email protected]
• Tag dermoscopic images to overview photos for efficient exams and accurate follow-ups.
• 3D cross-polarized lighting (patent pending) improves lesion assessment.
• Accurate body surface area measurements.
• Minimizes photography time and reduces patient anxiety.
Ideal for• Psoriasis • Vitiligo • Pigmented lesions • Plastic and reconstructive surgery
360° and 180° whole body imaging
www.canfieldsci.com 973.434.1201
The award winning VECTRA WB360
® ®Do Not Copy
Penalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
JDD Podcasts present the latest journal content related to advances in drugs, devices and treatment methods in dermatology, in a new convenient audio format. From article abstracts to interviews, JDD Podcasts provide a fresh perspective of the peer reviewed content you have come to rely on from JDD (Journal of Drugs in Dermatology).
Hosted by Adam Friedman, MD and released monthly, each episode will feature an interview with, and practical pearls from, the principal investigator of a high-profile JDD manuscript in a convenient audio format. Each podcast will place the selected article into a clinically useful perspective that is easy to listen to in the office or on the go.
www.jddonline.com/category/podcast
NEW EPISODE - CME AVAILABLEDon’t Go Zero to TEN: Identifying Gaps that Lead to Drug Re-exposure in Toxic Epidermal Necrolysis Drs. Helena Pasieka and Adam Friedman
We’ve all been there – that dreaded middle of the night page/call from the ER. Three simple words that send us spinning: “Rule out TEN.” Have no fear though, because the skin sloughing savoir is here. Inpatient dermatology service director Dr. Helena Pasieka joins us to discuss her recent research that elucidates opportunities to prevent offending agent re-exposure (aka first time shame on you, second time shame on us) in patients with a history of SJS/TEN. Simple steps can be taken to improve communication and prevention. Even more importantly, Dr. Pasieka walks us through her tried and true approach to that r/o call, key findings to guide your decision making, and what to when. Listening to this podcast may save someone’s life…
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1205 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Truncal Acne: A Neglected Entity James Q. Del Rosso DO,a Linda Stein-Gold MD,B Charles Lynde MD,c Emil Tanghetti MD,D
Andrew F. Alexis MD MPHE ªResearch Director/Clinical Dermatology, JDR Dermatology Research/Thomas Dermatology, Las Vegas, NV
BDirector of Clinical Research, Department of Dermatology, Henry Ford Hospital, Detroit, MIcDepartment of Medicine, University of Toronto, Canada; Lynde Institute of Dermatology and Lynderm Research
DCenter for Dermatology & Laser Surgery, Sacramento, CAEDepartment of Dermatology, Mount Sinai St. Luke’s and Mount Sinai West, Skini of Color Center, New York, NY
Truncal acne – acne vulgaris involving the chest, back, or shoulders – is thought to be present in more than half of patients with acne. Because the study of acne has been focused on the face, there are sparse data in the literature about the clinical characteristics and management options for truncal acne. It is thought that the pathogenic process is similar between the face and the back, suggesting that treatments studied on the face may be suitable for use on the back. It is not uncommon for patients to omit discussion of truncal acne with their treating physician, and it is likely that non-facial acne is under-diagnosed and under-treated. Scarring and pigmentary problems are common sequelae of acne on the trunk, underscoring the need for early and effective treatment as a preventive measure.
Truncal acne merits consideration and should be more thoroughly studied. Initiating treatment with a topical retinoid combined with an antimicrobial agent is logical for most patients with truncal acne, and mirrors recommendations for facial acne; however, there are ad-ditional considerations for truncal acne such as extension of the lesions, risk of antibiotic resistance due to large surface areas treated for a prolonged duration, accessibility of lesions, and discoloration of clothing or bedding due to topical products. Oral isotretinoin is the treatment of choice when truncal acne is severe. This article reviews available information as well as recent recommendations for treatment.
J Drugs Dermatol. 2019;18(12):1205-1208.
ABSTRACT
INTRODUCTION
CAcne vulgaris is a very common skin disease with a complex, multifaceted pathogenesis and a clinical presentation that encompasses a spectrum of lesions
which occur subsequent to inflammation of the pilosebaceous unit.1 Although most of the medical literature has focused on fa-cial acne, the disease also commonly involves skin of the chest and back, areas that also have a high density of pilosebaceous units.2 There is currently very little information in the medical literature about the entity of truncal acne.3 In addition, aware-ness of truncal acne among both the public and healthcare practitioners is low. Expert recommendations and guidelines for the management of acne have been focused on facial acne, with little, if any, attention given to truncal acne.4-7 At the time of writing, there were no treatments specifically indicated for truncal acne.
TRUNCAL ACNE: WHAT IS KNOWN ABOUT IT?EpidemiologyThe epidemiology of truncal acne has not been well character-ized. Del Rosso et al conducted clinical examinations of 300 consecutive acne patients aged 14 to 20 years, and reported the presence of at least moderate truncal acne in 47%, with a slightly higher rate found in males vs females (54% vs 43%).8 In
a study of 965 acne patients referred to dermatologists, Tan et al reported 61% had chest acne and 45% had back acne.9 In the largest study to date, Dreno et al observed a 35.6% prevalence of acne lesions on both the face and trunk among 2,926 patients with mild-to-moderate acne.10 This group also found that the fre-quency of truncal acne was significantly higher in patients who had a family history of acne (P<.0001).10
Consistent with the authors’ clinical impressions, it has been reported that many patients (25%) do not voluntarily mention torso involvement, but that the majority (78%) want treatment.3
Scarring and dyschromia are common and bothersome sequel-ae, and Graber et al report that these may be more common in males than in females and that Asians and Black patients are prone to keloidal scars.11 As with facial acne, scarring likelihood on the trunk increases with increasing acne severity.3,11 Lauer-mann et al noted scarring in 17% of those with chest acne and in 8.2% of those with anterior chest acne in a cohort of 2,201 ado-lescent males.12 The potential for scarring indicates that early diagnosis and efficacious treatment are important for preven-tion.2
Truncal acne is not limited to acne that occurs in adolescence.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1206
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
J.Q. Del Rosso, L. Stein-Gold, C. Lynde, et al
durations of oral antibiotic therapy be avoided due to the potential for antimicrobial resistance, and in some cases adverse effects are more likely with long durations of treat-ment.2
Skin CareGood skin care with the professional direction of a physician is a very important component of acne management both on the face and the trunk.19 Patients usually appreciate educa-tion and recommendations about skin care, and proper use of appropriate products can reduce the potential for cutaneous ir-ritation that can accompany topical medical therapy.19 Both the disease and some of its treatments can negatively impact skin permeability, causing increased transepidermal water loss with associated xerosis, inflammation, and skin sensitivity.19-21 Be-cause there is both a high demand for information from patients and a widespread availability of non-dermatologist information sources (eg, television, internet, and spas to name just a few), it behooves the dermatologist to be ready to have a knowledge-able discussion about the role of skin care in managing acne.19
This can reassure the patient that the physician has an encom-passing strategy for the overall management of acne. Further, Matsuoka et al showed that education about skin care and cos-metic use compared with no education can improve the quality of life in acne patients.22
A gentle cleanser and cream moisturizer are essential elements in skin care for patients with acne, and should be used both when lesions are present and during periods when the skin is mostly clear.19 Unfortunately, there are few data in the medical literature to guide recommendations for cleansers and mois-turizers in acne-prone skin.19 However, most dermatologists advocate once- or twice-daily washing with a mild cleanser.21
Overly aggressive cleaning or scrubbing should be avoided, as it could lead to increased irritation and inflammation. Moistur-izers should be non-comedogenic and non-acnegenic. Products that have sebum absorbent ingredients such as silica micro-beads and corn starch may be useful for patients with oily skin.19 Acne patients should also routinely use sun protection, particu-larly those patients with darker skin phototypes who are prone to hyperpigmentation problems.21 Additional considerations with truncal acne include wearing breathable fabrics for work-outs and using gentle laundry detergents.
Topical Therapy A few agents (BPO, azelaic acid, dapsone) have been specifically studied in truncal acne, all in small studies.23-25 The efficacy and safety of these agents in facial acne have been well character-ized.
BPO is a potent antimicrobial agent that has traditionally been an attractive option in truncal acne for decreasing acne lesions and reducing the risk of bacterial resistance to antibiotics. BPO
In a large-scale international prospective study of 374 adult fe-males, Dreno et al reported that 48.4% of the women had acne on chest, shoulders, or back, in addition to facial acne.13 Addor et al. reported a slightly lower frequency, 31.8%, of truncal acne in 262 adults with predominantly moderate acne in Brazil.14
PathophysiologyIt is generally accepted that acne has 4 major pathogenic mech-anisms: altered keratinization and blockage of pilosebaceous ducts, inflammation, increased sebum production, and coloni-zation of the pilosebaceous unit by Cutibacterium acnes.1 It is thought that these factors are generally the same with truncal involvement, although there is some evidence that sebum ex-cretion may have a smaller role in truncal acne.15 This may be because truncal skin differs from facial skin in thickness and has fewer sebaceous glands and lower pH.16 The skin of the trunk may be more affected by mechanical effects of trapped sweat/oils, pressure, friction, or occlusion by clothing or sports equip-ment.17
MANAGING TRUNCAL ACNEThere are some challenges with managing truncal as compared with facial acne. First, as has already been mentioned, there is a lower potential for patients to report truncal acne to their physi-cian and a lower potential for dermatologists to inquire about trunk involvement.3 There is also a larger skin area involved with the trunk compared with the face, and some areas are hard to reach, potentially making topical therapy more difficult. Final-ly, similar to facial acne, truncal acne is often accompanied by emotional/social aspects such as embarrassment in social situa-tions where the skin is revealed.
Although there are no data, it is reasonable to assume a com-bination treatment approach similar to that used in facial acne is warranted; thus, a rational initial approach would be a topi-cal retinoid plus an antimicrobial agent.2,3,18 Based on current standards of care for facial acne, Liu et al gave the following recommendations for truncal acne:2
• Topical therapy may be considered an appropriate initial option for mild to moderate truncal acne. Suitable agents include topical retinoids alone or in fixed combination with benzoyl peroxide (BPO) or topical antibiotics, azelaic acid, and dapsone.
• In moderate to moderately severe truncal acne, the initial therapy may include a combination of topical therapy with systemic antibiotics or hormonal therapy for females.
• With severe truncal acne, oral isotretinoin is often the op-timal treatment approach. For those who are unable or unwilling to take isotretinoin, oral antibiotics with topical therapy and hormonal therapy may be an alternative.
• Response to therapy should be evaluated after 2 to 3 months and adjusted as needed. It is recommended that prolonged
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1207
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
J.Q. Del Rosso, L. Stein-Gold, C. Lynde, et al
efficacious and was not associated with any statistically or clini-cally significant increases in plasma retinoid levels despite the large skin area treated.31 Jarratt et al later reported good efficacy and low systemic exposure among subjects with moderate-to-severe acne who applied tazarotene foam or gel formulations to the face, chest, upper back, and shoulders for 22 days.32
Systemic TherapySome clinicians feel oral medications are necessary when trun-cal acne is present, especially in cases of greater severity or when the surface area involved is widespread. However, clinical study data and management guidelines are very limited on the use of oral antibiotics for truncal acne. It is also important to note that there is a greater risk of side effects with systemic vs topical therapy.2,33
Oral antibiotics may be useful in moderate-to-severe acne, es-pecially when topical therapy does not achieve desired results.2
However, it is strongly recommended that antibiotics not be used as monotherapy and the duration of treatment should be limited as much as possible.2,6,26 Hormonal therapies includ-ing newer combined oral contraceptives (COCs) may be useful in truncal acne. Palli et al conducted a 24-week, randomized, double-blind study in 25 women aged 18 or older with 10 to 50 truncal acne lesions.34 This group reported a success rate (clear/almost clear) of 53.3% vs 20% for placebo (P=NS) at week 24; however, reductions in IL, NIL, and total lesions were all sta-tistically significant.34 Spironolactone mean improvement was 75.9% for chest acne and 77.6% for back acne in 110 patients.35
Oral isotretinoin is considered to be the most effective potential treatment for severe truncal acne, although it should be noted that this disease presentation (especially with nodulocystic le-sions) may be less responsive to treatment than facial acne.3
FUTURE PROSPECTSTargeted formulations that are easy to spread, have rapid cu-taneous penetration with low systemic exposure, and provide effective drug delivery with a lack of residue and low potential to stain clothing/bedding are being developed. Agents being studied in truncal acne include trifarotene and cortexolone 17α-propionate.
Recently, 2 large-scale randomized clinical trials evaluating the safety and efficacy of the drug-candidate trifarotene were pub-lished (PERFECT 1 and 2); these studies involved 2,420 subjects, of whom 1,214 were treated with trifarotene.36 Subjects were treated once daily with either trifarotene or vehicle for 12 weeks, and both facial and truncal acne were evaluated with the pri-mary efficacy endpoint being an IGA rating of “clear” or “almost clear” plus a ≥2-grade improvement in IGA. At week 12, facial IGA success rates were 29.4% (PERFECT 1) and 42.3% (PERFECT 2, both P<0.001); truncal success rates were 35.7% (PERFECT 1)
wash is often recommended for ease of administration to large areas; however, the use of BPO wash on the trunk has been shown to not effectively reduce C acnes counts.3,18,23,26 BPO can bleach clothing and bedding, which may be problematic when applied on the torso.2 When evaluating the effect of BPO on C acnes in truncal acne, it has been shown that effective use of BPO on the trunk is both concentration and contact time depen-dent. Leyden et al reported BPO 9.8% foam short contact therapy effectively reduced C acnes counts on the back in healthy sub-jects (no acne), but no reduction was shown with an 8% BPO wash.18,23 There is a concern with wash formulations that ad-equate contact time may not be achieved, particularly on the back which may require more time.18 Small open-label or uncon-trolled studies have suggested that both the wash and cleanser formulations reduce inflammatory lesions by 30% to 40% and non-inflammatory lesions by approximately 25%; and Del Rosso et al reported a mean total lesion count reduction of approxi-mately 70% in small scale (N=20) studies of BPO 8% creamy wash with or without clindamycin phosphate 1% foam.27,28
Azelaic acid 15% foam has been evaluated in patients (N=18) with moderate truncal acne in a 16-week, single-center, open-label study.25 In this setting, 89% of patients had a 1 grade improvement and 44% were judged clear/almost clear on trunk at week 16.25 Kainz et al reported that azelaic acid 20% cream improved acne on the face, chest, and back in a 12-week non-interventional study.29
Del Rosso et al reported a 16-week, open-label study of the ef-ficacy and safety of topical dapsone 7.5% gel (N=20, 15 of whom completed the study) in truncal acne.24 The primary endpoint was the percent of subjects with a ≥2-grade improvement on IGA plus a rating of “clear” or “almost clear” by study end-point. At baseline, 80% of the subjects were judged as having moderate truncal acne and the remaining 20% had severe truncal acne. By week 16, 45% of study participants had met the primary endpoint of clear/almost clear plus at least 2-grade improvement. Tolerability was acceptable, with 15 reports of lo-cal tolerability issues, of which 3 were mild but unresolved at study end and one lost to follow-up. Three subjects had adverse events, which were judged unrelated to study medication. The authors concluded that topical dapsone could be a viable addi-tion to therapeutic options for truncal acne, and recommended further investigation in a large-scale randomized clinical trial.24
Retinoids are recommended in facial acne due to their multiple actions on acne lesions, including decreasing inflammation and follicular keratinization abnormalities, which translate to both comedolytic and anti-inflammatory effects.2 Because topical ret-inoids reduce microcomedone formation, they are considered to be an integral component of topical management for most patients with acne.6,30 In 2001, Cunliffe et al showed that 4 weeks treatment of facial and truncal acne with topical isotretinoin was
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1208
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
J.Q. Del Rosso, L. Stein-Gold, C. Lynde, et al
and 42.6% (PERFECT 2, both P<0.001). Trifarotene was associ-ated with significantly greater reductions in inflammatory and non-inflammatory lesions on both face and trunk when com-pared with corresponding vehicle, with separation from vehicle occurring by weeks 1 to 2 for face and 2 to 4 for trunk. Tolerabil-ity was consistent with the profile of topical retinoids, and was better on the trunk than on the face. Local irritation, when it oc-curred, was mostly mild to moderate and resolved with ongoing treatment. Adverse events were primarily cutaneous in nature, occurring at the application site. Overall, safety was judged by investigators to be acceptable and manageable.36
DISCLOSURES AND ACKNOWLEDGMENTSEditorial services for this publication were provided by Galder-ma Laboratories, LP. All authors have served as consultants for Galderma. The authors wish to acknowledge Valerie Sanders, Sanders Medical Writing, for assistance with preparation of this publication.
REFERENCES1. Gollnick H, Cunliffe W, Berson D, Dreno B, Finlay A, Leyden JJ et al. Manage-
ment of acne: a report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49:s1-s37.
2. Liu C-WT, J. Understanding truncal acne: a practical guide to diagnosis and management. Skin Ther Lett. Available at: http://www.skintherapyletter.com/conditions/acne/truncal-diagnosis-management/. Accessed July 16, 2018, 2017.
3. Del Rosso JQ. Management of truncal acne vulgaris: current perspectives on treatment. Cutis. 2006;77:285-289.
4. Zaenglein AL, Pathy AL, Schlosser BJ, Alikhan A, Baldwin HE, Berson DS et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74:945-973(e33).
5. Eichenfield LF, Krakowski AC, Piggott C, Del Rosso J, Baldwin H, Friedlander SF et al. Evidence-based recommendations for the diagnosis and treatment of pediatric acne. Pediatrics. 2013;131(Suppl 3:s163-s186).
6. Thiboutot D, Gollnick H, Bettoli V, Dreno B, Kang S, Leyden JJ et al. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009;60:s1-s50.
7. Nast A, Dreno B, Bettoli V, Bukvic Mokos Z, Degitz K, Dressler C et al. Euro-pean evidence-based (S3) guideline for the treatment of acne - update 2016 - short version. J Eur Acad Dermatol Venereol. 2016;30:1261-1268.
8. Del Rosso JB, Blaum E. Prevalence of truncal acne vulgaris: a popula-tion study based on private practice experience. J Am Acad Dermatol. 2007;57(Suppl 2:AB3.)
9. Tan JK, Tang J, Fung K, Gupta AK, Thomas DR, Sapra S et al. Prevalence and severity of facial and truncal acne in a referral cohort. J Drugs Dermatol. 2008;7:551-556.
10. Dreno B, Jean-Decoster C , Georgescu V. Profile of patients with mild-to-moderate acne in Europe: a survey. Eur J Dermatol. 2016;26:177-184.
11. Graber EMA, KA. Treatment of truncal acne scarring. In: M. P. Alam, M. edi-tor. Body Rejuvenation: Springer Science+Business Media LLC; 2010.
12. Lauermann FT, Almeida HL Jr., Duquia RP, Souza PR, Breunig Jde A. Acne scars in 18-year-old male adolescents: a population-based study of preva-lence and associated factors. An Bras Dermatol. 2016;91:291-295.
13. Dreno B, Thiboutot D, Layton AM, Berson D, Perez M, Kang S et al. Large-scale international study enhances understanding of an emerging acne pop-ulation: adult females. J Eur Acad Dermatol Venereol. 2015;29:1096-1106.
14. Addor FA , Schalka S. Acne in adult women: epidemiological, diagnostic and therapeutic aspects. An Bras Dermatol. 2010;85:789-795.
15. Kim BR, Chun MY, Kim SA, Youn SW. Sebum secretion of the trunk and the development of truncal acne in women: do truncal acne and sebum affect each other? Dermatology. 2015;231:87-93.
16. Kim SA, Kim BR, Chun MY, Youn SW. Relation between pH in the trunk and face: Truncal pH can be easily predicted from facial pH. An Dermatol. 2016;28:216-221.
17. Bikowski J. Back in the spotlight: effective options for truncal acne. Practi-cal Dermatology. Available at: http://practicaldermatology.com/2010/02/back-
in-the-spotlight-effective-options-for-truncal-acne. Accessed July 17, 2018, 2010.
18. Bikowski J. A review of the safety and efficacy of benzoyl peroxide (5.3%) emollient foam in the management of truncal acne vulgaris. J Clin Aesthet Dermatol. 2010;3:26-29.
19. Del Rosso JQ, Brandt S. The role of skin care as an integral component in the management of acne vulgaris: part 2: tolerability and performance of a designated skin care regimen using a foam wash and moisturizer SPF 30 in patients with acne vulgaris undergoing active treatment. J Clin Aesthet Dermatol. 2013;6:28-36.
20. Thiboutot D, Del Rosso JQ. Acne vulgaris and the epidermal barrier: is acne vulgaris associated with inherent epidermal abnormalities that cause impair-ment of barrier functions? Do any topical acne therapies alter the structural and/or functional integrity of the epidermal barrier? J Clin Aesthet Dermatol. 2013;6:18-24.
21. Zip C. The role of skin care in optimizing treatment of acne and rosacea. Skin Ther Lett. 2017;22:5-7.
22. Matsuoka Y, Yoneda K, Sadahira C, Katsuura J, Moriue T, Kubota Y. Effects of skin care and makeup under instructions from dermatologists on the quality of life of female patients with acne vulgaris. J Dermatol. 2006;33:745-752.
23. Leyden JJ, Del Rosso JQ. The effect of benzoyl peroxide 9.8% emollient foam on reduction of Propionibacterium acnes on the back using a short contact therapy approach. J Drugs Dermatol. 2012;11:830-833.
24. Del Rosso JQ, Kircik LH, Tanghetti E. Management of truncal acne vulgaris with topical dapsone 7.5% gel. J Clin Aesthet Dermatol. 2018;11:45-50.
25. Hoffman LK, Del Rosso JQ , Kircik LH. The efficacy and safety of azelaic acid 15% foam in the treatment of truncal acne vulgaris. J Drugs Dermatol. 2017;16:534-538.
26. Thiboutot D, Dreno B, Gollnick H, Bettoli V, Kang S, Leyden JJ et al. A call to limit antibiotic use in acne. J Drugs Dermatol. 2013;12:1331-1332.
27. Del Rosso JQ. What is the role of benzoly peroxide cleansers in acne man-agement? J Clin Aesthet Dermatol. 2008;1:48-51.
28. Gold M. Survey results of compliance, preference, and satisfaction in pa-tients prescribed benzoyl peroxide 8% wash and benzoyl peroxide 9% cleanser for the treatment of acne vulgaris. American Academy of Dermatol-ogy Annual Meeting. San Francisco, California 2006.
29. Kainz JT, Berghammer G, Auer-Grumbach P, Lackner V, Perl-Convalexius S, Popa R. Azelaic acid 20 % cream: effects on quality of life and disease sever-ity in adult female acne patients. J Dtsch Dermatol Ges. 2016;14:1249-1259.
30. Thiboutot DD, Abanmi A, Alexis AF, et al. Practical management of acne for clinicians. An international consensus from the Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2018;78(2 Suppl 1):s1-s23.
31. Cunliffe WJ, Glass D, Goode K, Stables GI, Boorman GC. A double-blind investigation of the potential systemic absorption of isotretinoin, when combined with chemical sunscreens, following topical application to pa-tients with widespread acne of the face and trunk. Acta Derm Venereol. 2001;81:14-17.
32. Jarratt M, Werner CP, Alio Saenz AB. Tazarotene foam versus tazarotene gel: a randomized relative bioavailability study in acne vulgaris. Clin Drug Inves-tig. 2013;33:283-289.
33. Del Rosso JQ. Truncal acne vulgaris: the relative roles of topical and sys-temic antibiotic therapy. J Drugs Dermatol. 2007;6:148-151.
34. Palli MB, Reyes-Habito CM, Lima XT, Kimball AB. A single-center, randomized double-blind, parallel-group study to examine the safety and efficacy of 3mg drospirenone/0.02 mg ethinyl estradiol compared with placebo in the treat-ment of moderate truncal acne vulgaris. J Drugs Dermatol. 2013;12:633-637.
35. Charny JW, Choi JK , James WD. Spironolactone for the treatment of acne in women, a retrospective study of 110 patients. Int J Women's Dermatol. 2017;3:111-115.
36. Tan J, Thiboutot D, Popp G, Gooderham M, Lynde C, Del Rosso J, et al. Randomized phase 3 evaluation of trifarotene 50 mug/g cream treatment of moderate facial and truncal acne. J Am Acad Dermatol. 2019;80:1691-1699.
AUTHOR CORRESPONDENCE
James Q. Del Rosso DOE-mail:................……......................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Sanofi - 193150Project: Approved for Patients aged 12 and older
Campaign: Sept-Oct 2019
Creative: US.DAD.14993_1_ROB_5TH_6TH_Pgs
AE: Frank Brusco
Publication: Various A-Size
IO #: Havas Media
Issue: Sept - Oct
Ad Type: Singles
bleed = 8.75" X 11.25"
trim = 8.5" X 11"
safety = 7" X 10"
Various A-Size
Various
Attn: Various
t: Various f: None
Ship Info:
Contact Ad Production with any questions regarding these materialsph: (973) 952-8273 email: [email protected]
atopic dermatitis (Trial 7). The safety profile of DUPIXENT in subjects followed through Week 52 was similar to the safety profile observed at Week 16 in Trial 6. The long-term safety profile of DUPIXENT observed in adolescents was consistent with that seen in adults with atopic dermatitis.AsthmaA total of 2888 adult and adolescent subjects with moderate-to-severe asthma (AS) were evaluated in 3 randomized, placebo-controlled, multicenter trials of 24 to 52 weeks duration (AS Trials 1, 2, and 3). Of these, 2678 had a history of 1 or more severe exacerbations in the year prior to enrollment despite regular use of medium- to high-dose inhaled corticosteroids plus an additional controller(s) (AS Trials 1 and 2). A total of 210 subjects with oral corticosteroid-dependent asthma receiving high-dose inhaled corticosteroids plus up to two additional controllers were enrolled (AS Trial 3). The safety population (AS Trials 1 and 2) was 12-87 years of age, of which 63% were female, and 82% were white. DUPIXENT 200 mg or 300 mg was administered subcutaneously Q2W, following an initial dose of 400 mg or 600 mg, respectively.In AS Trials 1 and 2, the proportion of subjects who discontinued treatment due to adverse events was 4% of the placebo group, 3% of the DUPIXENT 200 mg Q2W group, and 6% of the DUPIXENT 300 mg Q2W group.Table 2 summarizes the adverse reactions that occurred at a rate of at least 1% in subjects treated with DUPIXENT and at a higher rate than in their respective comparator groups in Asthma Trials 1 and 2.Table 2: Adverse Reactions Occurring in ≥1% of the DUPIXENT Groups in Asthma Trials 1 and 2 and Greater than Placebo (6-Month Safety Pool)
a Injection site reactions cluster includes erythema, edema, pruritus, pain, and inflammation.
b Eosinophilia = blood eosinophils ≥3,000 cells/mcL, or deemed by the investigator to be an adverse event. None met the criteria for serious eosinophilic conditions [see Section 5.3 Warnings and Precautions].
Injection site reactions were most common with the loading (initial) dose. The safety profile of DUPIXENT through Week 52 was generally consistent with the safety profile observed at Week 24.Chronic Rhinosinusitis with Nasal PolyposisA total of 722 adult subjects with chronic rhinosinusitis with nasal polyposis (CRSwNP) were evaluated in 2 randomized, placebo-controlled, multicenter trials of 24 to 52 weeks duration (CSNP Trials 1 and 2). The safety pool consisted of data from the first 24 weeks of treatment from both studies.In the safety pool, the proportion of subjects who discontinued treatment due to adverse events was 5% of the placebo group and 2% of the DUPIXENT 300 mg Q2W group.Table 3 summarizes the adverse reactions that occurred at a rate of at least 1% in subjects treated with DUPIXENT and at a higher rate than in their respective comparator group in CSNP Trials 1 and 2.Table 3: Adverse Reactions Occurring in ≥1% of the DUPIXENT Group in CRSwNP Trials 1 and 2 and Greater than Placebo (24 Week Safety Pool)
a Injection site reactions cluster includes injection site reaction, pain, bruising and swelling.
b Conjunctivitis cluster includes conjunctivitis, allergic conjunctivitis, bacterial conjunctivitis, viral conjunctivitis, giant papillary conjunctivitis, eye irritation, and eye inflammation.
The safety profile of DUPIXENT through Week 52 was generally consistent with the safety profile observed at Week 24.Specific Adverse ReactionsConjunctivitis During the 52-week treatment period of concomitant therapy atopic dermatitis trial (Trial 3), conjunctivitis was reported in 16% of the DUPIXENT 300 mg Q2W + TCS group (20 per 100 subject-years) and in 9% of the placebo + TCS group (10 per 100 subject-years). Among asthma subjects, the frequency of conjunctivitis was similar between DUPIXENT and placebo. In the 52-week CRSwNP study (CSNP Trial 2), the frequency of conjunctivitis was 3% in the DUPIXENT subjects and 1% in the placebo
subjects; all of these subjects recovered [see Warnings and Precautions (5.2)]. Eczema Herpeticum and Herpes Zoster The rate of eczema herpeticum was similar in the placebo and DUPIXENT groups in the atopic dermatitis trials. Herpes zoster was reported in <0.1% of the DUPIXENT groups (<1 per 100 subject-years) and in <1% of the placebo group (1 per 100 subject-years) in the 16-week atopic dermatitis monotherapy trials. In the 52-week DUPIXENT + TCS atopic dermatitis trial, herpes zoster was reported in 1% of the DUPIXENT + TCS group (1 per 100 subject-years) and 2% of the placebo + TCS group (2 per 100 subject-years). Among asthma subjects the frequency of herpes zoster was similar between DUPIXENT and placebo. Among CRSwNP subjects there were no reported cases of herpes zoster or eczema herpeticum.Hypersensitivity Reactions Hypersensitivity reactions were reported in <1% of DUPIXENT-treated subjects. These included serum sickness reaction, serum sickness-like reaction, generalized urticaria, rash, erythema nodosum, and anaphylaxis [see Contraindications (4), Warnings and Precautions (5.1), and Adverse Reactions (6.2)]. Eosinophils DUPIXENT-treated subjects had a greater initial increase from baseline in blood eosinophil count compared to subjects treated with placebo. In subjects with atopic dermatitis, the mean and median increases in blood eosinophils from baseline to Week 4 were 100 and 0 cells/mcL respectively. In subjects with asthma, the mean and median increases in blood eosinophils from baseline to Week 4 were 130 and 10 cells/mcL respectively. In subjects with CRSwNP, the mean and median increases in blood eosinophils from baseline to Week 16 were 150 and 50 cells/mcL, respectively. Across all indications, the incidence of treatment-emergent eosinophilia (≥500 cells/mcL) was similar in DUPIXENT and placebo groups. Treatment-emergent eosinophilia (≥5,000 cells/mcL) was reported in <2% of DUPIXENT-treated patients and <0.5% in placebo-treated patients. Blood eosinophil counts declined to near baseline levels during study treatment [see Warnings and Precautions (5.3)]. Cardiovascular (CV)In the 1-year placebo controlled trial in subjects with asthma (AS Trial 2), CV thromboembolic events (CV deaths, non-fatal myocardial infarctions [MI], and non-fatal strokes) were reported in 1 (0.2%) of the DUPIXENT 200 mg Q2W group, 4 (0.6%) of the DUPIXENT 300 mg Q2W group, and 2 (0.3%) of the placebo group.In the 1-year placebo controlled trial in subjects with atopic dermatitis (Trial 3), CV thromboembolic events (CV deaths, non-fatal MIs, and non-fatal strokes) were reported in 1 (0.9%) of the DUPIXENT + TCS 300 mg Q2W group, 0 (0.0%) of the DUPIXENT + TCS 300 mg QW group, and 1 (0.3%) of the placebo + TCS group.In the 24-week placebo controlled trial in subjects with CRSwNP (CSNP Trial 1), CV thromboembolic events (CV deaths, non-fatal myocardial infarctions, and non-fatal strokes) were reported in 1 (0.7%) of the DUPIXENT group and 0 (0.0%) of the placebo group. In the 1-year placebo controlled trial in subjects with CRSwNP (CSNP Trial 2), there were no cases of CV thromboembolic events (CV deaths, non-fatal myocardial infarctions, and non-fatal strokes) reported in any treatment arm.6.2 Immunogenicity As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to dupilumab in the studies described below with the incidence of antibodies in other studies or to other products may be misleading. Approximately 5% of subjects with atopic dermatitis, asthma, or CRSwNP who received DUPIXENT 300 mg Q2W for 52 weeks developed antibodies to dupilumab; ~ 2% exhibited persistent ADA responses, and ~ 2% had neutralizing antibodies. Approximately 9% of subjects with asthma who received DUPIXENT 200 mg Q2W for 52 weeks developed antibodies to dupilumab; ~4% exhibited persistent ADA responses, and ~4% had neutralizing antibodies.Approximately 4% of subjects in the placebo groups in the 52-week studies were positive for antibodies to DUPIXENT; ~2% exhibited persistent ADA responses, and ~1% had neutralizing antibodies.Approximately 16% of adolescent subjects with atopic dermatitis who received DUPIXENT 300 mg or 200 mg Q2W for 16 weeks developed antibodies to dupilumab; ~ 3% exhibited persistent ADA responses, and ~ 5% had neutralizing antibodies.Approximately 4% of adolescent subjects with atopic dermatitis in the placebo group were positive for antibodies to DUPIXENT; ~ 1% exhibited persistent ADA responses, and ~ 1% had neutralizing antibodies.The antibody titers detected in both DUPIXENT and placebo subjects were mostly low. In subjects who received DUPIXENT, development of high titer antibodies to dupilumab was associated with lower serum dupilumab concentrations [see Clinical Pharmacology (12.3) in the full prescribing information]. Two subjects who experienced high titer antibody responses developed serum sickness or serum sickness-like reactions during DUPIXENT therapy [see Warnings and Precautions (5.1)]. 7 DRUG INTERACTIONS 7.1 Live Vaccines Avoid use of live vaccines in patients treated with DUPIXENT.
Adverse Reaction
CSNP Trial 1 and Trial 2
DUPIXENT 300 mg Q2W
N=440 n (%)
Placebo N=282 n (%)
Injection site reactionsa 28 (6%) 12 (4%)
Conjunctivitisb 7 (2%) 2 (1%)
Arthralgia 14 (3%) 5 (2%)
Gastritis 7 (2%) 2 (1%)
Insomnia 6 (1%) 0 (<1%)
Eosinophilia 5 (1%) 1 (<1%)
Toothache 5 (1%) 1 (<1%)
Adverse Reaction
AS Trials 1 and 2
DUPIXENT 200 mg Q2W
N=779 n (%)
DUPIXENT 300 mg Q2W
N=788 n (%)
Placebo
N=792 n (%)
Injection site reactionsa 111 (14%) 144 (18%) 50 (6%)
Oropharyngeal pain 13 (2%) 19 (2%) 7 (1%)
Eosinophiliab 17 (2%) 16 (2%) 2 (<1%)
HH1068880_M07_Sept19_Brief_Summary_A_Size.indd 2 7/22/19 5:19 PM
S:7"
S:10"
T:8.5"
T:11"
B:8.75"
B:11.25"
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Sanofi - 193150Project: Approved for Patients aged 12 and older
Campaign: Sept-Oct 2019
Creative: US.DAD.14993_1_ROB_5TH_6TH_Pgs
AE: Frank Brusco
Publication: Various A-Size
IO #: Havas Media
Issue: Sept - Oct
Ad Type: Singles
bleed = 8.75" X 11.25"
trim = 8.5" X 11"
safety = 7" X 10"
Various A-Size
Various
Attn: Various
t: Various f: None
Ship Info:
Contact Ad Production with any questions regarding these materialsph: (973) 952-8273 email: [email protected]
Manufactured by: Regeneron Pharmaceuticals, Inc., Tarrytown, NY 10591 U.S. License # 1760; Marketed by sanofi-aventis U.S. LLC, (Bridgewater, NJ 08807) and Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591). DUPIXENT® is a registered trademark of Sanofi Biotechnology/© 2019 Regeneron Pharmaceuticals, Inc./sanofi-aventis U.S. LLC. All rights reserved. Issue Date: June 2019 US-DUP-1104(2)
7.2 Non-Live Vaccines Immune responses to vaccination were assessed in a study in which subjects with atopic dermatitis were treated once weekly for 16 weeks with 300 mg of dupilumab (twice the recommended dosing frequency). After 12 weeks of DUPIXENT administration, subjects were vaccinated with a Tdap vaccine (Adacel®) and a meningococcal polysaccharide vaccine (Menomune®). Antibody responses to tetanus toxoid and serogroup C meningococcal polysaccharide were assessed 4 weeks later. Antibody responses to both tetanus vaccine and meningococcal polysaccharide vaccine were similar in dupilumab-treated and placebo-treated subjects. Immune responses to the other active components of the Adacel and Menomune vaccines were not assessed. 8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy Pregnancy Exposure RegistryThere is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to DUPIXENT during pregnancy.Please contact 1-877-311-8972 or go to https://mothertobaby.org/ongoing-study/dupixent/ to enroll in or to obtain information about the registry.Risk SummaryAvailable data from case reports and case series with DUPIXENT use in pregnant women have not identified a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Human IgG antibodies are known to cross the placental barrier; therefore, DUPIXENT may be transmitted from the mother to the developing fetus. There are adverse effects on maternal and fetal outcomes associated with asthma in pregnancy (see Clinical Considerations). In an enhanced pre- and post-natal developmental study, no adverse developmental effects were observed in offspring born to pregnant monkeys after subcutaneous administration of a homologous antibody against interleukin-4-receptor alpha (IL-4Rα) during organogenesis through parturition at doses up to 10-times the maximum recommended human dose (MRHD) (see Data). The estimated background risk of major birth defects and miscarriage for the indicated populations are unknown. All pregnancies have a background risk of birth defect, loss or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.Clinical ConsiderationsDisease-Associated Maternal and/or Embryo-fetal RiskIn women with poorly or moderately controlled asthma, evidence demonstrates that there is an increased risk of preeclampsia in the mother and prematurity, low birth weight, and small for gestational age in the neonate. The level of asthma control should be closely monitored in pregnant women and treatment adjusted as necessary to maintain optimal control. DataAnimal Data In an enhanced pre- and post-natal development toxicity study, pregnant cynomolgus monkeys were administered weekly subcutaneous doses of homologous antibody against IL-4Rα up to 10 times the MRHD (on a mg/kg basis of 100 mg/kg/week) from the beginning of organogenesis to parturition. No treatment-related adverse effects on embryofetal toxicity or malformations, or on morphological, functional, or immunological development were observed in the infants from birth through 6 months of age. 8.2 Lactation Risk SummaryThere are no data on the presence of dupilumab in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The effects of local gastrointestinal and limited systemic exposure to dupilumab on the breastfed infant are unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for DUPIXENT and any potential adverse effects on the breastfed child from DUPIXENT or from the underlying maternal condition.8.4 Pediatric Use Atopic DermatitisThe safety and efficacy of DUPIXENT have been established in pediatric patients 12 years of age and older with moderate-to-severe atopic dermatitis. A total of 251 adolescents ages 12 to 17 years old with moderate-to-severe atopic dermatitis were enrolled in Trial 6. The safety and efficacy were generally consistent between adolescents and adults [see Adverse Reactions (6.1) and Clinical Studies (14.2) in the full prescribing information]. Safety and efficacy in pediatric patients (<12 years of age) with atopic dermatitis have not been established.AsthmaA total of 107 adolescents aged 12 to 17 years with moderate to severe asthma were enrolled in AS Trial 2 and received either 200 mg (N=21) or 300 mg (N=18) DUPIXENT (or matching placebo either 200 mg [N=34] or 300 mg [N=34]) Q2W. Asthma exacerbations and lung function were
assessed in both adolescents and adults. For both the 200 mg and 300 mg Q2W doses, improvements in FEV1 (LS mean change from baseline at Week 12) were observed (0.36 L and 0.27 L, respectively). For the 200 mg Q2W dose, subjects had a reduction in the rate of severe exacerbations that was consistent with adults. Safety and efficacy in pediatric patients (<12 years of age) with asthma have not been established. Dupilumab exposure was higher in adolescent patients than that in adults at the respective dose level which was mainly accounted for by difference in body weight [see Clinical Pharmacology (12.3) in the full prescribing information]. The adverse event profile in adolescents was generally similar to the adults [see Adverse Reactions (6.1)]. CRSwNP CRSwNP does not normally occur in children. Safety and efficacy in pediatric patients (<18 years of age) with CRSwNP have not been established.8.5 Geriatric Use Of the 1472 subjects with atopic dermatitis exposed to DUPIXENT in a dose-ranging study and placebo-controlled trials, 67 subjects were 65 years or older. Although no differences in safety or efficacy were observed between older and younger subjects, the number of subjects aged 65 and over is not sufficient to determine whether they respond differently from younger subjects [see Clinical Pharmacology (12.3) in the full prescribing information].Of the 1977 subjects with asthma exposed to DUPIXENT, a total of 240 subjects were 65 years or older. Efficacy and safety in this age group was similar to the overall study population.Of the 440 subjects with CRSwNP exposed to DUPIXENT, a total of 79 subjects were 65 years or older. Efficacy and safety in this age group were similar to the overall study population. 10 OVERDOSE There is no specific treatment for DUPIXENT overdose. In the event of overdosage, monitor the patient for any signs or symptoms of adverse reactions and institute appropriate symptomatic treatment immediately. 17 PATIENT COUNSELING INFORMATION Advise the patients and/or caregivers to read the FDA-approved patient labeling (Patient Information and Instructions for Use).Pregnancy RegistryThere is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to DUPIXENT during pregnancy. Encourage participation in the registry [see Use in Specific Populations (8.1)].Administration InstructionsProvide proper training to patients and/or caregivers on proper subcutaneous injection technique, including aseptic technique, and the preparation and administration of DUPIXENT prior to use. Advise patients to follow sharps disposal recommendations [see Instructions for Use].Hypersensitivity Advise patients to discontinue DUPIXENT and to seek immediate medical attention if they experience any symptoms of systemic hypersensitivity reactions [see Warnings and Precautions (5.1)]. Conjunctivitis and Keratitis Advise patients to consult their healthcare provider if new onset or worsening eye symptoms develop [see Warnings and Precautions (5.2)]. Eosinophilic ConditionsAdvise patients to notify their healthcare provider if they present with clinical features of eosinophilic pneumonia or vasculitis consistent with eosinophilic granulomatosis with polyangiitis [see Warnings and Precautions (5.3)].Not for Acute Asthma Symptoms or Deteriorating DiseaseInform patients that DUPIXENT does not treat acute asthma symptoms or acute exacerbations. Inform patients to seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with DUPIXENT [see Warnings and Precautions (5.4)].Reduction in Corticosteroid DosageInform patients to not discontinue systemic or inhaled corticosteroids except under the direct supervision of a physician. Inform patients that reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy [see Warnings and Precautions (5.5)].Patients with Comorbid AsthmaAdvise patients with atopic dermatitis or CRSwNP who have comorbid asthma not to adjust or stop their asthma treatment without talking to their physicians [see Warnings and Precautions (5.6)].
HH1068880_M07_Sept19_Brief_Summary_A_Size.indd 3 7/22/19 5:19 PM
References: 1. DUPIXENT Prescribing Information. 2. Simpson EL, Bieber T, Guttman-Yassky E, et al; SOLO 1 and SOLO 2 Investigators. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2016;375(24):2335-2348. 3. Data on file, Regeneron Pharmaceuticals, Inc. 4. Blauvelt A, de Bruin-Weller M, Gooderham M, et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet. 2017;389(10086):2287-2303.
S:7"
S:10"
T:8.5"
T:11"
B:8.75"
B:11.25"
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1211 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Diabetic Skin Changes Can Benefit from Moisturizer and Cleanser Use: A Review
Robert S. Kirsner MD PhD,ª Gil Yosipovitch MD FAAD,B Shasa Hu MD FAAD,c Anneke Andriessen PhD,d Jason R. Hanft DPM FACFAS,e Paul J. Kim DMP MS,f Lawrence Lavery DPM MPH,g
Luigi Meneghini MD MBA,h Lee C. Ruotsi MD ABWMS CWS-P UHMi
aUniversity of Miami Hospital Wound Center and Chief of Dermatology, University of Miami Hospital, Miami, FL; Harvey Blank Chair in Dermatology, Dr. Phillip Frost Department of Dermatology and Cutaneous Surgery,
University of Miami Miller School of Medicine, Miami, FL BMiami Itch Center, Miami, FL; Dr. Phillip Frost Department of Dermatology and Cutaneous Surgery,
University of Miami Miller School of Medicine, Miami, FLcDr. Phillip Frost Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, FL;
Dr. Phillip Frost Department of Dermatology and Cutaneous Surgery, Sylvester Comprehensive Cancer Center, Miami, FL DAndriessen Consultants, Malden, Netherlands, and Radboud University Nijmegen Medical Centre, Netherlands
ePodiatric Surgery Specialist, Foot & Ankle Institute of South Florida, South Miami, FL; South Miami Hospital, South Miami, FL fMedStar Plastic & Reconstructive Surgery, MedStar Health Inc., Washington, DC;
Georgetown University School of Medicine, Washington, DC gUT Southwestern’s Comprehensive Wound Care Center, Dallas, TX; Plastic Surgery, Orthopaedic Surgery,
and Physical Medicine & Rehabilitation, UT Southwestern Medical Center, Dallas, TX hGlobal Diabetes Program, Parkland Health and Hospital System, Dallas, TX; Internal Medicine,
University of Texas Southwestern Medical Center, Division of Endocrinology, Dallas, TX iCatholic Health Advanced Wound Healing Centers, Buffalo, NY
Introduction: Diabetes mellitus (DM) associated skin changes, which may be the first sign of DM in undiagnosed patients. Frequently these patients present with dry skin, which may benefit from the use of gentle cleansers and moisturizers. A review paper was devel-oped to explore DM-associated skin changes and possible benefits of cleanser and moisturizer use. Methods: For this purpose, an expert panel of physicians involved in the care of patients with DM selected information from literature searches coupled with expert opinions and experience of the panel. Results: A defective skin barrier predisposes the skin to water loss leading to dryness, hyperkeratosis and inflammation. Skin changes that may benefit from the use of gentle cleansers and moisturizers are, amongst others, diabetic foot syndrome, ichthyosiform skin changes, xerosis, and keratosis pilaris. Adherence to treatment is a considerable challenge making education essential, especially about the need to keep skin clean and what skin care to use. Specifically designed diabetic skin care that contains anti-aging ingredients, urea, and essential ceramides, has demonstrated benefits for dry/itchy skin. Conclusions: Skin disorders are common complications among either diabetic patients with patients with DM and may lead to seri-ous adverse events. Evidence suggests that daily application of optimal skin care using gentle cleansers and moisturizers is one of the measures that may help improve skin barrier dysfunction, preventing complications by providing early-stage treatment of patients with diabetes.
J Drugs Dermatol. 2019;18(12):1211-1217.
ABSTRACT
INTRODUCTION
Diabetes mellitus (DM) is a common and debilitating disease that also affects the skin. Thirty percent (30%) to 70% of patients with DM have associated skin dis-
eases. The severity of skin disease may vary, ranging from benign to deforming to life-threatening.1 These diabetic skin changes may allow insight into patients’ glycemic control and may be the first signs of DM in undiagnosed patients.2 Recog-
nition and management of DM-related skin conditions are im-portant in maximizing patients’ quality of life and in avoiding serious complications.2
Maintaining an intact skin barrier by preventing and treating skin dryness may improve skin conditions in patients with diabetes.3 Currently gentle cleansers and moisturizers are un-
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1212
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
R.S. Kirsner, G. Yosipovitch, S. Hu, et al
Cutaneous manifestations in DM may be classified into four cat-egories: 1) Skin associated with DM (from strongest to weakest association include necrobiosis lipoidica, diabetic dermopathy, diabetic bullae, yellow skin, eruptive xanthomas, perforating disorders, acanthosis nigricans, oral leucoplakia, lichen planus); 2) Infections (bacterial, fungal); 3) Cutaneous manifestations of diabetic complications (microangiopathy, macroangiopathy, neuropathy); and 4) Skin reactions to diabetes treatment (ie, sulphonylurea rash or insulin lipohypertrophy).2 Additionally, hyperglycemia may lead to skin changes (Table 1), the mecha-nism of action is unclear and other factors are likely involved.2,6
In patients with DM, functional properties of the stratum cor-neum (SC) may be altered, impacting skin barrier function.4 A defective skin barrier predisposes the skin to water loss and to invasion by pathogens, which in turn may lead to dryness, hy-perkeratosis and redness from inflammation.7 The status of the permeability and antimicrobial barrier of the skin in DM remains unknown.2 In-vivo impairment of the skin barrier was observed in type 2 DM mice models, which results from impairment of skin barrier homeostasis and decreases in epidermal prolifera-tion and epidermal lipid synthesis.8
In vivo and in vitro, pre-clinical studies show that, diabetes alters epidermis histology and suppresses proliferation of ke-ratinocytes.9 Impaired keratinocyte homeostasis and epidermal barrier function, results in higher risk of chronic wounds and infection.10,11,13-15
der-utilized. Skin care is frequently lacking or overlooked as part of patients’ DM skin treatment.3
To address these unmet needs, a review paper was developed to explore DM skin changes and possible benefits of appropri-ate cleanser and moisturizer use in DM skin treatment.
METHODSAn expert panel of physicians involved in the care of patients with DM convened in Miami, FL, in March 2019, to deliberate about diabetic skin changes and the impact of cleanser and moisturizer use on skin health. For this purpose, selected infor-mation from literature searches coupled with expert opinions and experience of the panel were used. The literature review was conducted prior to the meeting; the results were presented and discussed during the meeting. The selected literature was deemed clinically relevant to DM skin changes and challenges in treating diabetic skin. Skin conditions that differ from DM skin changes, or those that would not necessarily benefit from cleanser and moisturizer use, are outside the scope of this re-view.
Diabetes Mellitus and Related Skin Changes DM-related skin changes are a common complication seen in both type 1 and type 2 DM.2 Dermatologic conditions linked with DM vary in severity and while usually benign can in certain circumstances lead to major complications, including amputa-tions.4,5
TABLE 1.
Altered Functional Properties of the Skin Barrier in Diabetes. Diabetes mellitus (DM); Stratum corneum (SC); Advanced glycation end-product (AGE); lamellar body (LB); epidermal antimicrobial peptides (AMPs).
Reference Impact on Skin Barrier Function
Campos de Macedo GM, et al2DM caused skin changes are common complications of both type 1 and type 2 DM and are usually neglected and frequently underdiagnosed.
Spravchikov N.6
Hyperglycemia and impaired insulin signaling might be directly involved in the development of chronic com-plications of diabetes by impairing glucose utilization of skin keratinocytes as well as skin proliferation and differentiation.
Kim JH, et al8
The status of the permeability and antimicrobial barrier of the skin in DM remains unknown. In-vivo (mice) im-pairment of the skin barrier was observed in type 2 DM, which results from impairment of skin barrier homeo-stasis, decreases in epidermal proliferation and epidermal lipid synthesis, and decreases in LB and AMPs.
Okano J, et al9In-vivo and in-vitro diabetes alters epidermis histology, suppresses proliferation of keratinocytes and reduces proliferation in epidermal cells.
Quondamatteo F.10 Impaired keratinocyte homeostasis and epidermal barrier function through direct and indirect mechanisms results in susceptibility to skin complications, chronic wounds and infection.
Eaglstein WH, et al11 Dermatologic comorbidities of DM and related issues.
Sakai S, et al12 Patients with DM showed a reduced hydration state of the SC together with decreased sebaceous gland activity.
Piérard GE, et al13 The most common skin changes of DM are “dry skin,” xerosis, and acquired ichthyosis, occurring predominately on the shins and feet. Moisturizers improve the feeling of well-being for diabetes patients.
Muller LM, et al14Patients with type 1 and type 2 DM are at increased risk for skin and mucous membrane infection. Studies are warranted into management of such infections.
Park HY, et al24 A long-standing hyperglycaemic condition impairs the skin barrier and accelerates the skin aging process.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1213
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
R.S. Kirsner, G. Yosipovitch, S. Hu, et al
Diabetic Foot SyndromeDiabetic foot syndrome (DFS) is a broad term denoting anatom-ic and physiologic changes in the feet resulting from DM.1,4,5 The incidence and prevalence of DFS is reported at 1% to 4%, and 4% to 10%, respectively.1 DFS is slightly more prevalent in type 1 DM compared with type 2 DM.1
Diabetic foot ulcer (DFU), the end stage of DFS, is a global pan-demic of diabetes, developing countries are especially on the frontline (Figure 1).4 Persons with DM have a 15–25% lifetime risk of DFU, and have a 50–70% recurrence rate within 5 years.4,5 Depending on size, duration and depth, healing can be difficult and take, on average, 11–14 weeks to heal. They precede ampu-tation in 85% of cases, with a 1-year amputation rate estimated at 15%.4,5 DFS and DFUs profoundly impact costs to the health system.4,5
DFS presents initially with callosities and dry skin related to diabetic neuropathy.4,5 In later stages, chronic ulcers and a va-riety of other malformations of the feet may develop.4,5 DFUs frequently present with secondary infection, diabetic neuro-os-teoarthropathy and clawing deformity (Figure 2).4,5 Neuropathic, but mostly painless, ulceration results from peripheral neuropa-thy, and is the most common type of complication. However, ulceration may be due to either ischemic changes or due to both peripheral neuropathic and ischemic disease.4,5 Dry skin of the diabetic foot is mostly due to the autonomic component of the peripheral neuropathy that may be present.4,5
The interdisciplinary, team-based approach to DFU should in-
Diabetic skin also ages faster due to inflammation triggered by both intrinsic and extrinsic factors. In diabetic skin in vitro studies showed elevated levels of MMP-1 and MMP-2, increased lysyl oxidase (LOX) expression, higher cross-linked collagens and fragmented collagen fibrils compared to healthy skin. It is thought that deterioration of dermal collagen structural integrity and mechanical properties occurs at an earlier age in those with diabetes.12 Mechanisms that alter skin surface integrity have been identified for various skin conditions that present with dry skin.6,7,13-15 The formation of the SC barrier, specifically generation of its lipophilic components, involves several pH-dependent en-zymes.7 Two key lipid-processing enzymes, β-glucocerebrosidase and acid sphingomyelinase, have pH optima of 5.6 and 4.5, re-spectively, as part of the skin’s acid mantle. They are involved in the synthesis of ceramides––critical components of the per-meability barrier.7 Activity of β-glucocerebrosidase is 10 times lower in situ at pH 7.4 than at pH 5.5. The processing of lipids secreted by lamellar bodies and the formation of lamellar struc-tures require an acidic environment.7
Skin Conditions That May Benefit from Skin Cleanser and Mois-turizer Use Examples of common skin changes in DM that may benefit from gentle skin cleansers and moisturizers are, diabetic foot syn-drome (DFS), ichthyosiform skin changes, and xerosis due to diabetes, and keratosis pilaris.
Acanthosis nigricans is mentioned as an example of a condition that may benefit from gentle skin cleansers and moisturizer use as an adjunctive measure together with treatment of the under-lying condition, for example, insulin resistance. Acanthosis Nigricans Acanthosis nigricans (AN) presents with multiple poorly de-marcated plaques with grey to dark-brown hyperpigmentation and a thickened velvety to verrucous texture. In insulin resistant states the proposed mechanism is stimulation of IGF-1 receptors in the skin by cross-reaction with insulin.16,17 Common locations for AN are posterior neck, axilla, elbows, palms, inframammary creases, umbilicus, and groin; it is typically asymptomatic.16,17
Management of AN includes lifestyle changes such as dietary modifications, increased physical activity, and weight reduction. While AN can occur in other settings, in patients with DM, medi-cation such as metformin may be recommended to improve glycemic control and reduce insulin resistance, although con-clusive evidence to support this is lacking.16,17 Topical therapies are usually ineffective in patients with generalized involvement of the condition. In those with thickened or macerated areas of skin, topical keratolytics such as ammonium lactate, retinoic acid, or salicylic acid can improve appearance of AN.16,17
FIGURE 1. Diabetic foot ulcer (DFU). DFS presents initially with callosities and dry skin related to diabetic neuropathy. In later stages, chronic ulcers and a variety of other malformations of the feet develop.18,19
FIGURE 2. Deformation and callus formation in the diabetic foot syndrome patient. Callus formation is the body’s natural response to excessive friction and pressure. Biomechanical factors may play a role in callus formation as well as an abnormal gait.20 Photograph courtesy of Dr. Sherkin.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1214
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
R.S. Kirsner, G. Yosipovitch, S. Hu, et al
TABLE 2.
Interdisciplinary Team-Based Approach for Patients With Diabetic Foot Ulcers. Adapted from Botros M, et al.19
Treat the CauseVascular – infection – pressure• Manage comorbidities• Assess risk based on health status
Address Patient-Centered Concerns
• Provide individualized patient education• Engage patient and family in care planning• Explore potential barriers to adherence
Local Wound and Skin Care
• Debridement: Remove necrotic tissue and remove callus • Infection/inflammation control: Rule out or treat localized/spreading infection• Wound moisture balance: Provide a moist, interactive wound environment• Remove dry scales • Daily use of gentle cleansers and moisturizers on dry skin areas
volve lifestyle changes such as dietary modifications, daily foot surveillance, appropriate foot hygiene, footwear and skin care (Table 2).4,5,18,19 Treatment of a patient with DFU can follow an algorithm called “VIPS,"18 to treat the cause of the ulceration. The abbreviation stands for: V = Vascular supply, which can be assessed by detecting a palpable foot pulse of ≥80 mmHg, an ankle-brachial pressure index (ABPI) of >0.5 and <1.3, a transcu-taneous oxygen tension of >30 mmHg, and toe pressure of >55 mmHg. If the ABPI is >1.3, calcifications could be present indicat-ing peripheral ischemic disease. The ABPI is to be followed by a full Doppler examination of the affected extremity, which may include the abdomen, to detect the extent of the disease and to define the healing ability of the ulcer.18
I = Inflammation and/or Infection treatment, in case there are clinical signs of an infection, such as erythema, edema, en-hanced exudate production, pus, deterioration of the ulcer, and increased pain.18 However, in those patients with neuropathy, pain sensation may not be present and erythema and warmth may likewise not be as evident due reduced sympathetic arterio-lar tone due to the autonomic component of the neuropathy.18
Abnormal blood glucose values in patients that were previously well controlled may also indicate the presence of an infection.18
P = Plantar pressure redistribution and S = Sharp Surgical serial debridement.18
Early stages of DFS include dry skin, callus formation, hyper-keratosis. While they are relatively benign compared to DFU, these skin conditions can progress into skin infections or DFU if not treated appropriately. For instance, A defective skin barrier exposes the skin to water loss and to invasion of pathogens and may lead to dry/hyperkeratotic skin and inflammation.3-5,18,19
Callus formation is the body’s natural response to excessive friction and pressure; biomechanical factors may play a role in callus formation as does an abnormal gait.18-20
Hyperkeratosis in the patients with DFS can be prevented and managed by offloading and by suitable footwear, as well as by callus removal and pressure prevention (Figure 3).18-20
It is important to debride crusts, callouses, scabs, and scales, and to restore moisture balance of the skin, by using a gentle cleanser and moisturizer on a consistent basis. Appropriate care of the skin using gentle cleansers and moisturizers and early-stage treatment of skin-barrier dysfunction may help prevent complications in the patients with DFS.3-5,18-20 Utilization of rou-tine gentle cleanser and moisturizer may also help establish a durable barrier against further drying and irritation of the skin, preventing skin cracks, and infection.3-5,18-20
FIGURE 4. Ichthyosiform skin changes related to diabetes.
FIGURE 3. Pressure areas at risk in the diabetic foot syndrome patient.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1215
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
R.S. Kirsner, G. Yosipovitch, S. Hu, et al
Ichthyosiform Skin ChangesThese ichthyosiform skin changes present as large bilateral ar-eas of dryness and scaling, and may be described as “fish scale” skin (Figure 4).21,22 Development of ichthyosiform skin changes is related to production of advanced glycosylation end products and to microangiopathic changes.21,22 Treatment of these skin changes is limited; however, topical moisturizers containing keratolytic agents may be beneficial.21,22
Xerosis Due to DMXerosis presents as abnormally dry skin that may also show scaling or fissures, and appears most commonly on the feet in patients with DM (Figure 5).3-5,18-20 Dry skin conditions result from an abnormal, persistent cohesion between corneocytes, with secondary thickening of the SC, impaired moisturization of the uppermost SC layers, increased transit time of corneocytes in the SC, and altered skin barrier function.12,23,24 The decreased sebaceous gland activity in patients with DM further contributes to a reduced hydration state of the SC. The physical characteris-tic of the SC depends on its moisture content and water holding capacity.12
Patients with dry skin may have a feeling of skin tightness, espe-cially after showering, bathing or swimming.3 The skin may feel shrunken or dehydrated and looks rough rather than smooth.3
Itching and pain may be intense and there may be slight to severe scaling or peeling, fine lines, cracks and/or fissures, ery-thema, and inflammation.3-5,18-20 Deep fissures that may bleed are frequently present in the more severe cases and pose a risk for infection (Figure 6).3-5,18-20 Skin barrier dysfunction may be compounded by excessive keratin formation resulting in hyperkeratosis.20 Xerosis and hyperkeratosis can be triggered by shoes constructed of materials, that do not allow for suf-ficient moisture evaporation, by improperly fitting shoes, socks and stockings, by excessive perspiration, and by heating or air conditioning that reduces humidity and dries the skin.20 Other factors leading to cracked skin on heels are prolonged standing, especially on hard floors, and being overweight, which increas-es the pressure on the normal fat pad under the heel.20 If the skin is not supple and flexible, the pressure to crack is high. This may be the case in open backs on shoes, which allow the fat pad under the heel to expand sideways, thereby increasing the pres-sure and causing the skin to crack.20
In dry skin, the risk for infection is enhanced. The protective acid mantle is less functional while the warm moist environment in poor footwear may predispose to the development of skin infec-tion.3-5,18-20 Xerosis in DM is often associated with pruritus, mostly localized, such as on the scalp, ankles, feet, trunk, or genitalia. Pruritus is more likely in those patients with DM who have dry skin and/or neuropathy.15,25 Involvement of the genitalia or intertriginous
areas may occur in those who have an infection (eg, candidia-sis).15,25
Keratosis PilarisKeratosis pilaris presents on the extensor surfaces of the upper arms (Figure 7) and less frequently on the thighs, face and but-tocks.21 Compared to the general population, keratosis pilaris occurs more frequently and with more extensive involvement in those patients with DM. Keratosis pilaris can be treated with various topical therapies, including salicylic acid-containing moisturizers, combined with gentle exfoliation.21
Skin Care for Diabetic Skin ChangesAdherence to treatment is a considerable challenge in people with DM,1-5 making education essential, especially about the need to keep the skin clean and with regard to what cleansers to use.3 Using cleansers with a high pH (9.0–10.0) increases skin pH, thereby causing irritation and leading to lower lipid production. However, conclusive evidence is lacking that shows lowered skin pH, using near-physiologic skin surface pH (4.0–6.0) prod-ucts, improves diabetic skin.1-5
FIGURE 6. Cracked heels in a diabetes patient.
FIGURE 7. Diabetes-related keratosis pilaris.
FIGURE 5. Diabetes-related dry skin on the foot.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1216
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
R.S. Kirsner, G. Yosipovitch, S. Hu, et al
included in the diabetic skin care line, enabling easy and effec-tive skin care.
DISCUSSIONMetabolic changes associated with DM exert a major impact on the skin, leading to skin lesions, infections, angiopathy and neu-ropathy.2,5,18 The prevalence of DM-associated skin infections is greater when compared to the normal population.2
Although there is evidence from in-vitro and in-vivo studies sup-porting that hyperglycemia and impaired insulin signaling might be directly involved in the development of chronic complications of diabetes, the mechanisms behind DM-related skin changes are not yet elucidated and clinical data are lacking.1,2 There are limited clinical data regarding early-stage skin disorders in DM patients, which consequently impede efforts to include skin care as part of prevention and treatment of diabetic skin changes.2,3
As patients encounter a broad spectrum of disorders in DM, skin conditions are usually neglected and frequently underdiag-nosed.1,2,11 Moreover, adherence to treatment is a considerable challenge in patients with diabetes1-5,18-20 For this reason, it is important to educate patients on DM skin care, as well as phy-sicians, ancillary health care professionals such as diabetes educators and nurses, who may have more extensive contact with and influence on patients with DM.18-20 For educational purposes, the authors of the current review propose the term “diabetic skin syndrome” a broad term denoting anatomic and physiologic changes in the skin of those with DM. The use of this term may support education on the various issues related to this condition, with a structured approach to its prevention, treatment and maintenance as part of the multidisciplinary total care package of these patients.
Updating knowledge on skin care is required, since classical physician training used to include the message that “one can’t add moisture to the skin.” As such, many physicians practicing today may still hold this view. Evidence supporting the use of gentle cleansers and moisturizers3,27-30 should be included in
Moisturizer use decreases trans-epidermal water loss (TEWL) through occlusive agents, which can be combined with humec-tants to attract water to the skin.26
Gentle cleansers and moisturizers are recommended for daily use to restore and preserve skin barrier integrity in dry skin conditions.27 This type of skin care was shown to improve the clinical signs and symptoms of AD, including pruritus, erythe-ma, fissuring, and lichenification.27
Products composed of ceramides, cholesterol and fatty acids aim to mimic natural lipids,7 and may reduce the need for other medications.27-29 These moisturizers help to close fissures by filling spaces, sealing moisture into the skin through the pro-duction of an occlusive barrier, thereby softening the skin (Table 3).3,20
A cream with skin-identical ceramides has been shown to ameliorate dry skin conditions, which in turn improves skin barrier function, thus reducing skin irritation.28,29 A cohort study by Vender et al28 demonstrated that daily use of a ceramides-containing cleanser and moisturizer regimen over a four-week period significantly improved dry skin conditions and subject-reported quality of life.
Specifically designed diabetic skin care might contain anti-aging ingredients, urea, and essential ceramides, and MVE (layered delivery of ingredients) technology may be of benefit to treat some of the common skin conditions seen in DM or as adjunct skin maintenance regimen. A moisturizer acts as a humectant, hydrating the SC through a hygroscopic effect, thereby increas-ing its elasticity.27,28 Moreover, aphysiological pH moisturizer has keratolytic and anti-pruritic action, providing soothing and nourishing relief for dry/itchy skin.27,28 An unpublished clinical study using products with these components demonstrated that improvement in skin hydration following product application lasted up to 48 hours.
Diabetic skin changes may benefit from the use of the products
TABLE 3.
Skin Care for Xerosis. Lactic acid (LA); glycolic acid (GA); hyaluronic acid (HA); topical corticosteroids (TCS); topical calcineurin inhibitors (TCI). Adapted from Guenther L, Lynde CW, Andriessen A, et al.3
Products Function Ingredients
Cleansing Removing pollutants and bacteria Synthetically produced detergent cleansers
‘Classic’ Moisturizers Close fissures by filling spaces and seal moisture into the skin
Mineral oils (eg. liquid paraffin, petrolatum), waxes (eg. lanolin, bees-wax, carnauba), long-chain esters, fatty acids, and mono-, di-, and triglycerides
Moisturizers With Humectants
Moisturizers act as humectants, hydrate the stratum corneum through a hygroscopic effect, increasing its elasticity
Combine humectants with ingredients of classic moisturizers, eg, alpha-hydroxy acids (LA, GA, HA), urea, glycerine, propylene glycol and ceramides
TCS Anti-inflammatory effects Combine TCS with a moisturizer, such as a ceramide containing cream
TCI Anti-inflammatory effects Combine TCI with a moisturizer such as ceramide containing cream
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1217
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
R.S. Kirsner, G. Yosipovitch, S. Hu, et al
8. Kim JH, Yoon NY, Kim DH, Jung M, et al. Impaired permeability and antimi-crobial barriers in type 2 diabetes skin are linked to increased serum levels of advanced glycation end-product. Exp Dermatol. 2018;27(8):815–23. doi: 10.1111/exd.13466.
9. Okano J, et al. Hyperglycemia induces skin barrier dysfunctions with im-pairment of epidermal integrity in non-wounded skin of type 1 diabetic mice. PLoS One. 2016; 11(11): e0166215. https://doi.org/10.1371/journal.pone.0166215
10. Quondamatteo F. Skin and diabetes mellitus: what do we know? Cell Tissue Res. 2014;355(1):1–21.
11. Eaglstein WH, Callen JP. Dermatologic comorbidities of diabetes mellitus and related issues. Arch Dermatol. 2009;145(4):467–9.
12. Sakai S, Kikuchi K, Satoh J, Tagami H, Inoue S. Functional properties of the stratum corneum in patients with diabetes mellitus: similarities to senile xe-rosis. Br J Dermatol. 2005;153(2):319–23.
13. Piérard GE, Seite S, Hermanns-Le T, Delvenne P, Scheen A, Pierard-Franchi-mont C. The skin landscape in diabetes mellitus. Focus on dermocosmetic management. Clin Cosmet Investig Dermatol. 2013;6:127–35.
14. Muller LM, Gorter KJ, Hak E, Goudzwaard WL, Schellevis FG, Hoepelman AI, et al. Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin Infect Dis. 2005 Aug 1;41(3):281–8.
15. Valdes-Rodriguez R, Mollanazar NK, González-Muro J, et al. Itch prevalence and characteristics in a Hispanic geriatric population: a comprehensive study using a standardized itch questionnaire. Acta Dermato-Venereologica. 2015;95(4):417-21.
16. Bhagyanathan M, Dhayanithy D, Parambath VA, Bijayraj R. Acanthosis nigri-cans: a screening test for insulin resistance – an important risk factor for diabetes mellitus type-2. J Family Med Prim Care. 2017;6(1):43.
17. Sinha S, Schwartz RA. Juvenile acanthosis nigricans. J Am Acad Dermatol. 2007;57(3):502-08.
18. Sibbald RG, Goodman L, Woo KY, Kasper DL, Smart H, Tarig G, et al. Special consideration in wound bed preparation 2011: an update. Adv Skin Wound Care. 2011; 24:415-36.
19. Botros M, Kuhuke J, Embil J, Goettl K, Morin K, Parsons L, et al. Best prac-tice recommendations for the prevention, diagnosis and treatment of dia-betic foot ulcers: Update 2019 01 19. Canadian Association of Wound Care 1573r5E, woundscanada.ca.
20. Sherkin KJ, Springer A, Andriessen A, Botros M, Cohen D, Guy P, Mendez C, Menzildzic S, Nesbitt L. Pathway to dry foot-skin. Canadian Association of Wound Care 2011; 9(1):1-26.
21. Pavlovic MD, Milenkovic T, Dinic M, Misovic M, Dakovic D, Todorovic S, et al. The prevalence of cutaneous manifestations in young patients with type 1 diabetes. Diabet Care. 2007;30:1964–7.
22. Patel N, Spencer LA, English JC, Zirwas MJ. Acquired ichthyosis. J Am Acad Dermatol. 2006;55(4):647-56.
23. Kalus AA, Chien AJ, Olerud JE. Diabetes mellitus and other endocrine dis-eases. In: Goldsmith L, Katz S, Gilchrest B, Paller A, Leffell D, Wolff K, edi-tors. Fitzpatrick’s Dermatology in General Medicine, 8th ed. New York, NY: McGraw-Hill; 2012:151.
24. Park HY, Kim JH, Jung M, Chung CH, Hasham R, Park CS, et al. A long-standing hyperglycaemic condition impairs skin barrier by accelerating skin ageing process. Exp Dermatol. 2011;20(12):969–74.
25. Yamaoka H, Sasaki H, Yamasaki H, et al. Truncal pruritus of unknown origin may be a symptom of diabetic polyneuropathy. Diabet Care. 2010;33(1):150-55.
26. Rawlings AV. Recent advances in skin barrier research. Br J Dermatol. 2014:171 (Suppl 3):19-28.
27. Lynde CW, Andriessen A. A cohort study on a ceramide containing cleanser and moisturizer for atopic dermatitis. Cutis. 2014;93:207-213.
28. Vender RB, Andriessen A, Barankin B, Freiman A, Kyritsis D, Mistos LM, et al. Cohort using a ceramides containing cleanser and cream with sali-cylic acid for dry, flaking, and scaling skin conditions. J Drugs Dermatol. 2019;18(1):80-85.
29. Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, Schwarzenberger K, et al. Guidelines of care for the management of atopic dermatitis. Section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71:116-32.
30. Skotnicki S, Shulgan C. Beyond Soap: The Real Truth About What You Are Doing to Your Skin and How to Fix It for a Beautiful, Healthy Glow. Penguin Canada; 2018:1-304.
AUTHOR CORRESPONDENCE
Anneke Andriessen PhDE-mail:................……......................... [email protected]
educational programs together with information about prod-ucts that should not be used on the skin (eg, harsh soaps or alcohol).30 Repeated washing with alkaline soap and the use of high pH moisturizers reduce buffer capacity by washing away inherent buffering components in the skin.30 Skin surface pH influences skin barrier homeostasis, SC integrity and cohesion, and antimicrobial defense mechanisms.30 Moreover, soaps with a high pH can aggravate or predispose patients to candidal in-tertrigo that is more common in diabetics.30
Cleansing and moisturizer use may be an important measure to sustain skin pH at physiological levels in DM-affected skin, thus improving barrier function and skin condition. Consistent routine is also important in maintaining skin hydration and poten-tially reducing the risk for progression or complications of DFS.
CONCLUSION• Skin disorders are common complications among diabe-
tes patients, yet frequently underdiagnosed and usually neglected.
• Recognition and management of diabetes-related skin con-ditions are important in maximizing the patients’ quality of life and in avoiding bothersome symptoms and serious adverse effects.
• There is evidence suggesting that daily application of a ceramides-containing moisturizing skin care regime, par-ticularly on compromised lower extremities, may control both pruritus and dry skin conditions.
• Optimal skin care using moisturizers is one of the measures that may help improve skin barrier dysfunction, preventing complications by providing early-stage treatment of pa-tients with diabetes.
DISCLOSUREThe authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this supple-ment: This work was supported by an unrestricted educational grant from L’Oreal CeraVe USA.
REFERENCES1. Rosen J, Yosipovitch G. Skin Manifestations of Diabetes Mellitus. [Updated
2018 Jan 4]. In: Feingold KR, Anawalt B, Boyce A, et al, editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK481900/
2. Campos de Macedo GM, Nunes S, Barreto T. Skin disorders in diabetes mel-litus: an epidemiology and physiopathology review. Diabetol Metab Syndr. 2016;8(1):63. doi: 10.1186/s13098-016-0176-y
3. Guenther L, Lynde CW, Andriessen A, Barankin B, et al. Pathway to dry skin prevention and treatment. J Cutan Med Surg. 2012 Jan-Feb;16(1):23–31. PMID: 22417992 doi: 10.1177/120347541201600106
4. Amin N, Doupis J. Diabetic foot disease: from the evaluation of the “foot at risk” to the novel diabetic ulcer treatment modalities. World J Diab. 2016;7(7):153-164. ISSN 1948-9358 (online).
5. Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. The Lancet. 2005;366:1719–24.
6. Spravchikov N, Sizyakov G, Gartsbein M, Accili D, Tennenbaum T, Wertheimer E. Glucose effects on skin keratinocytes: implications for diabetes skin com-plications. Diabetes. 2001;50(7):1627–35.
7. Ali SM, Yosipovitch G. Skin pH: from basic science to basic skin care. Acta Derm Venereol. 2013;93:261–7. PMID: 23322028 10.2340/00015555-1531
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1218 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Tretinoin 0.05% Lotion for the Once-Daily Treatment of Moderate and Severe Acne Vulgaris in Females:
Effect of Age on Efficacy and TolerabilityLinda Stein Gold MD,ª David M. Pariser MD,B Eric Guenin PharmD PhD MPHc
aHenry Ford Hospital, Detroit, MIbEastern Virginia Medical School and Virginia Clinical Research, Inc., Norfolk, VA
cOrtho Dermatologics, Bridgewater, NJ
Background: While it is generally considered to be a disease of adolescence, acne affects an increasing number of adults, especially women. Although data exist on the use of retinoids in adult females, there is no universal agreement as to the age of onset of adult female acne, or data on the efficacy and tolerability dependent on age. A novel tretinoin 0.05% lotion formulation has been shown to be effective and well-tolerated in acne patients with moderate or severe disease.Objective: To evaluate the safety and efficacy of once-daily tretinoin 0.05% lotion in women with moderate or severe acne categorized into different age groups (13-19, 20-29, and 30+ years).Methods: Post hoc analysis of two multicenter, randomized, double-blind, vehicle-controlled phase 3 studies. Women (aged 13-19 years, N=357; 20-29 years, N=352; 30+ years, N=156) with moderate or severe acne were randomized (1:1) to receive tretinoin 0.05% lotion or vehicle, once-daily for 12 weeks. Efficacy assessments included changes in baseline inflammatory/noninflammatory lesions and treatment success (at least 2-grade reduction in Evaluator’s Global Severity Score [EGSS] and ‘clear’/’almost clear’) and Quality of Life (QoL) using the validated Acne-QoL questionnaire. Safety and adverse events (AEs) where evaluated throughout; cutaneous toler-ability assessed at each study visit using a 4-point scale (where 0=none and 3=severe).Results: At baseline, 91.9% (N=794) of women in the post hoc analysis had moderate (EGSS=3) and 8.1% (N=70) severe (EGSS=4) acne, with the highest proportion of women (11.1%, N=39) having severe acne being aged 20-29 years. Baseline inflammatory lesion counts were similar across the three age ranges, with more comedonal lesions (44.5) in adolescent females (aged 13-19 years). Quality of life at baseline was much better in adolescent females and may be age-related for some domains (self-perception and role-social). At week 12, there appeared to be an age-related improvement in both inflammatory and noninflammatory lesion counts, and treatment success although the differences between groups were not significant. Mean percent reduction in inflammatory and noninflammatory lesion counts for each age group (13-19, 20-29, and 30+ years old respectively) were 55.3% (P=0.019 versus vehicle), 55.8% (P=0.080) and 63.5%; and 47.1% (P<0.001), 55.2% (P=0.002) and 59.0% (P=0.030). Treatment success for the 3 groups was achieved by 23.2% (P=0.023), 21.3%, and 30.7% of patients, respectively, at week 12; differences between age groups were not significant. Quality of Life improved in all age groups, although changes with tretinoin 0.05% lotion were only significant compared with vehicle in adult females aged 20-29 years (self-perception, role-emotional and acne symptoms); improvements in each domain score by week 12 were also greatest in this age group. The majority of AEs were mild and transient; the most common treatment emergent AEs were application site pain and dryness especially in the older adult females (aged 30+ years). Local cutaneous safety and tolerability assessments were generally mild and improved by week 12. There were transient increases in scaling, burning and stinging in the adolescent females, peaking at week 4; all mean scores were ≤0.6 where 1=mild.Conclusions: Tretinoin 0.05% lotion was significantly more effective than vehicle in achieving treatment success and reducing inflam-matory and comedonal lesions in adult and adolescent females with moderate or severe acne. There appear to be age-related efficacy and tolerability benefits favoring adult females.
J Drugs Dermatol. 2019;18(12):1218-1225.
ABSTRACT
INTRODUCTION
Acne vulgaris (acne) is one of the most common diseases in adolescence, affecting more than 80% of teenagers.1
Although it has been traditionally considered a disease which affects adolescents, research suggests that it is becoming more prevalent in adulthood, and especially in women.2
The reasons for an increase in adult acne are unkown with a number of endogenous and exogenous factors contributing to its clinical expression3-6; increased awareness in acne may also be driving more adult patients into dermatology offices to seek care.7,8
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1219
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
L. Stein Gold, D.M. Pariser, E. Guenin
METHODSStudy DesignA post hoc analysis of two multicenter, randomized, double-blind, vehicle-controlled, parallel group clinical studies, was conducted on adolescent and adult female subjects with moderate or severe acne. Protocols for the pivotal trials received approval before patient enrollment from the appropriate institutional review board (IRB) and were conducted in accordance with the Declaration of Helsinki and Good Clinical Practices (GCP) and in compliance with local regulatory requirements. All subjects were informed of the study details and provided written consent.
Study PopulationParticipants included in the post hoc analysis were female subjects of any race and ethnicity aged 13 years and older who presented with 20 to 40 inflammatory lesions (papules, pustules, and nodules), 20 to 100 noninflammatory lesions (open and closed comedones), and two nodules or less. A washout period of up to 1 month was required for patients who used previous prescription and over-the-counter acne treatments and 6 months for systemic retinoids.
Subjects were enrolled with an Evaluator Global Severity Score [EGSS] score of 3 (moderate) or 4 (severe); randomized (1:1) to tretinoin 0.05% lotion or vehicle applied once-daily for 12 weeks.For the purposes of the post hoc analysis, three specific age groups were evaluated: women aged 13 to 19 years, 20 to 29 years, and those 30 years and older.
Efficacy EvaluationEfficacy evaluations comprised inflammatory and non- inflammatory lesion counts and an EGSS assessment at screening, baseline, and subsequent study visits (weeks 4, 8, and 12). Efficacy endpoints included mean percent change from baseline to week 12 in inflammatory and noninflammatory lesion counts and the proportion of subjects achieving at least a 2-grade reduction from baseline EGSS at week 12 with an EGSS evaluation of ‘clear’ or ‘almost clear’.
Additional assessments included a validated acne-specific quality of life (Acne-QoL) questionnaire (Merck & Co, Inc. Whitehouse, NJ). Acne-QoL was evaluated at baseline and week 12 using a 19-item patient-reported outcome measure evaluating the impact of facial acne. The questionnaire consists of four domains: self-perception, role-emotional, role-social, and acne symptoms. Each question was evaluated using a 7-point scale (from “none” or “not at all” to “extremely” or “extensive”) and answers grouped into the appropriate domains. Higher Acne-QoL domain scores indicating better acne-related QoL.
Safety EvaluationCutaneous safety (erythema and scaling) and tolerability (itching, burning, and stinging) were evaluated on a scale from 0 (none) to 3 (severe). Adverse events (AEs) were evaluated throughout;
Female patients account for two-thirds of dermatology visits for acne, and one-third of the visits are from women who are older than 25 years.9 In a large survey of over 1000 men and women, aged 20 years and older, 73.3% (N=744) reported ever having acne. The prevalence of acne among adult women aged 20-29 years, 30-39 years , 40-49 years, and 50 years and older was 50.9%, 35.2%, 26.3%, and 15.3%. In all these age groups, the difference between women and men was statistically significant.10
Acne can have significant negative psychosocial and emotional impact with older women reporting a greater impact of acne on their quality of life (QoL) than younger sufferers.11-15
Although adult acne tends to be mild-to-moderate in severity, treatment failure, and a chronic relapsing course can increase the self perception of acne severity further impacting QoL. Disease duration may also be an important factor for its poorer perception by women.12
Many factors have to be considered when selecting appropriate treatment, including acne severity, response to previous treatment, psychosocial impact, possibility of pregnancy, slow response to treatment, and the increased risk of sensitive skin irritation. Women over the age of 25 years tend to have higher rates of treatment failure. Adult women with acne also have a higher frequency of post-inflammatory erythema, hypo and/or hyperpigmentation (PIH), and scarring causing cosmetically disfiguring changes.8
Topical retinoids are commonly used to treat acne patients with mild-to-moderate disease. They are comedolytic, resolve the precursor microcomedone lesions, and are antiinflammatory. Retinoid use may be limited by its side effects including dryness, peeling, erythema, and irritation. Older patients may be more susceptible to this skin irritation, and may benefit from formulations that are less irritating.15
Recently, data were reported on a tretinoin lotion for the treatment of moderate or severe acne.17 This novel tretinoin 0.05% lotion was formulated using polymeric emulsion technology, with the specific aim of providing more efficient delivery of retinoid into the dermal layers, with less skin irritation. Not only was tretinoin 0.05% lotion effective in treating inflammatory and comedonal lesions, but it had a highly favorable safety and tolerability profile compared with data previously reported on other tretinoin formulations.
In many clinical trials of patients with acne, the mean age of enrolled subjects is commonly between 18-19 years, suggesting a number of subjects were post-adolescent. In the pivotal studies with tretinoin 0.05% lotion, the mean age was slightly higher (20.5 years) with a broad age range (9-58 years), affording the opportunity to conduct a post hoc analysis of the impact of age on efficacy and tolerability in female acne.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1220
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
L. Stein Gold, D.M. Pariser, E. Guenin
gender differences in the proportion of subjects aged 13-19 years and 20-29 years (Figure 1).
A total of 865 female acne subjects were included in the post hoc analysis (357 aged 13 to 19 years, 352 aged 20 to 29 years, and 156 aged 30 years and older), see Table 1. The percent of subjects completing the study in each age group was 86.0%, 79.5% and 85.3%, respectively. The proportion of female subjects treated with tretinoin 0.05% lotion who completed the study was greatest in those subjects aged 30 years and older (88.7%). Reasons for discontinuation were consistent across the three age groups, predominantly ‘lost to follow-up’ or ‘subject request’. Two subjects each in the 13 to 19 (1.2%), and 20 to 29 (1.2%) years age groups treated with tretinoin 0.05% lotion discontinued due to AEs.
There were noticeable differences between treatment groups with regard to baseline lesion counts and EGSS. At baseline, the mean number of inflammatory lesions was very similar across the treatment groups, however, the mean number of comedonal lesions was greatest in the adolescent females, reducing progressively with age, from 44.5 to 35.6 (Table 1). At baseline, there were twice as many subjects with severe acne (EGSS=4) in the adult female group aged 20 to 29 years than in either of the other two groups (11.1% compared with 6.7% and 4.5%).
At baseline, Acne-QoL domain scores were highest (ie, better QoL) in the adolescent females. Baseline domain scores in the two adult female groups were similar.
EfficacyLesion CountsTretinoin 0.05% lotion resulted in statistically significant reductions in noninflammatory lesion counts compared with vehicle in each age group, and significant reductions in
severity, and relationship to study medication assessed.
Statistical AnalysisThe intent-to-treat (ITT) population comprised all subjects randomized and provided with study drug and vehicle. The safety population comprised all randomized patients who were presumed to have used the study medication or vehicle at least once and who provided at least one post-baseline evaluation. The primary method of handling missing efficacy data in the ITT analysis set was based on estimation using the Markov Chain Monte Carlo multiple imputation method. No imputations were made for missing safety data.
Percent reductions in lesion counts were presented as least square (LS) means and treatment P-values from an analysis of covariance with values adjusted for multiple imputations. Significance of EGSS reductions were obtained from logistic regression (using Firth’s Penalized Likelihood) with factors of treatment group and analysis center. For comparisons between age groups, P-values were from an analysis of covariance with factors of age groups and the respective baseline scores as a covariate. All statistical analyses were conducted using SAS®
version 9.3 or later. Statistical significance was based on 2-tailed tests of the null hypothesis resulting in P values of 0.05 or less.All AEs occurring during the studies were recorded and classified on the basis of medical dictionary for drug regulatory activities terminology (MedDRA) for the safety population. Treatment group comparisons were made by tabulating the frequency of subjects with one or more AEs during the study.
RESULTSBaseline CharacteristicsOverall, 1640 subjects were enrolled in the two studies (aged 9 to 58 years). The majority of female (78.0%) and male (93.6%) subjects were aged 13-29 years, however, there were marked
FIGURE 1. Demographics based on age: ITT population, pooled data.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1221
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
L. Stein Gold, D.M. Pariser, E. Guenin
inflammatory lesion counts in adolescent female subjects at week 12. Mean percentage change (LS mean) from baseline in inflammatory lesion counts for the adolescent, young adult, and older adult subgroups were 55.3%, 55.8%, and 63.5%, respectively compared with 45.2%, 46.6%, and 56.7% for vehicle (P=0.019, P=0.080, P=0.340, respectively). Noninflammatory lesion counts were reduced by 47.1%, 55.2%, and 59.0%, respectively compared with 27.6%, 39.3%, and 45.4% for vehicle (P<0.001, P=0.002, P=0.030, respectively).
While there was a trend towards increasing efficacy with age (see Figures 2 and 3), differences between the three age groups with respect to tretinoin 0.05% lotion treatment were not significant.
Treatment SuccessTreatment success was defined as at least a 2-grade improvement in global severity by EGSS and ‘clear’ or ‘almost clear’. By week 12, 23.2%, 21.3%, and 30.7% of the adolescent, young adult, and older adult female populations were treatment successes
Table 1: (KAREN: YOU CAN TRY USING THESE TABLES AS GRAPHICS)
Pooled Data Adolescent Female Population (13-19)
Pooled Data Adult Female Population (20-29)
Pooled Data Adult Female Population (30+)
Tretinoin 0.05%
(N=173)
Vehicle (N=184)
Total (N=357)
Tretinoin 0.05%
(N=163)
Vehicle (N=189)
Total (N=352)
Tretinoin 0.05% (N=80)
Vehicle (N=76)
Total (N=156)
Evaluator’s Global Severity Score N (%) 3 – Moderate 4 - Severe
165 (95.4%) 8 (4.6%)
168 (91.3%) 16 (8.7%)
333 (93.3%) 24 (6.7%)
142 (87.7%) 20 (12.3%)
170 (89.9%) 19 (10.1%)
312 (88.9%) 39 (11.1%)
76 (95.0%) 4 (5.0%)
73 (96.1%) 3 (3.9%)
149 (95.5%) 7 (4.5%)
Inflammatory Lesion Count- Mean (SD)
26.4 (5.46) 25.2 (4.59) 25.7 (5.06) 25.5 (5.42) 26.0 (5.20) 25.7 (5.30) 24.9 (4.88) 23.4 (3.17) 24.2 (4.19)
Noninflammatory Lesion Count- Mean (SD)
42.8 (18.27) 46.2 (19.83) 44.5 (19.14) 37.7 (15.45) 40.5 (16.93) 39.2 (16.30) 36.3 (15.18) 34.8 (12.79) 35.6 (14.04)
Self-Perception-Mean (SD) 19.5 (8.05) 18.6 (7.47) -- 16.3 (7.54) 15.3 (7.55) -- 15.8 (7.85) 15.0 (8.07) --
Role-Emotional-Mean (SD) 19.5 (8.08) 18.8 (7.50) -- 16.4 (6.92) 15.8 (7.27) -- 17.0 (7.39) 15.4 (7.56) --
Role-Social-Mean (SD) 19.2 (6.59) 18.7 (7.17) -- 16.4 (7.40) 15.4 (7.05) -- 16.2 (7.44) 14.5 (7.08) --
Acne Symptoms-Mean (SD) 20.1 (6.00) 19.3 (5.62) -- 16.7 (5.80) 17.0 (5.69) -- 17.7 (6.30) 16.4 (5.79) --
TABLE 1.
Baseline Characteristics (ITT Female Population, Pooled Data, by Age Group)
FIGURE 2. Percent change in inflammatory lesions from baseline to week 12 (ITT population, pooled data, LS mean). Comparison between age groups, female patients treated with tretinoin 0.05% lotion or vehicle.*
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1222
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
L. Stein Gold, D.M. Pariser, E. Guenin
following treatment with tretinoin 0.05% lotion compared to 13.3% (P=0.023), 13.0% (P=0.054), and 18.0% (P=0.081) of subjects on vehicle (Figure 4a).
By week 12, 24.4%, 25.9%, and 30.7% of the adolescent, young adult, and older adult female populations achieved at least a 2-grade improvement in EGSS following treatment with tretinoin 0.05% lotion compared to 17.0%, 16.8%, and 18.8% on vehicle. None of these treatment differences between active and vehicle were significant (Figure 4b).
While there was a trend to greater treatment success with increasing age, differences between the three age groups with respect to tretinoin 0.05% lotion treatment were not significant.
Quality of LifeAt baseline, QoL was much better in the adolescent females (aged 13-19 years). Absolute improvement in Acne-QoL domain scores were greatest in the younger adult females (aged 20 to 29 years), and lowest in the adolescent acne population (Figure 5). Only in the young adult females were QoL improvements significant compared with vehicle (self-perception [P=0.010], role-emotional [P=0.006], and acne symptoms [P=0.008]). Domain scores for each subgroup were similar at week 12.
SafetyOverall, tretinoin 0.05% lotion was well-tolerated in female acne subjects and most AEs were of mild or moderate severity, with only three subjects (0.6%) reporting a serious AEs (SAEs) in the
FIGURE 3. Percent change in noninflammatory lesions from baseline to week 12 (ITT population, pooled data, LS mean). Comparison between age groups, female patients treated with tretinoin 0.05% lotion or vehicle.*
FIGURE 4A. Treatment success. Patients with at least a 2-grade improvement in EGSS and ‘clear’ or ‘almost clear’ at each study visit (ITT population pooled data). Comparison between age groups, female patients treated with tretinoin 0.05% lotion or vehicle.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1223
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
L. Stein Gold, D.M. Pariser, E. Guenin
FIGURE 4B. Patients with at least a 2-grade improvement in EGSS at each study visit (ITT population pooled data). Comparison between age groups, female patients treated with tretinoin 0.05% lotion or vehicle.
tretinoin 0.05% lotion group. Ten female subjects treated with tretinoin 0.05% lotion discontinued due to treatment-emergent (TE) AEs. Most common TEAEs with tretinoin 0.05% lotion were application site dryness (5.4%, N=21), pain (4.1%, N=16), and erythema (2.1%, N=8). These TEAEs were more prevalent in the adolescent females (Table 2).
Cutaneous Safety and TolerabilityErythema and scaling were recorded by the investigator and itching, burning, and stinging severity scores were obtained from subjects. In all cases tretinoin 0.05% lotion was well-
tolerated. In each subgroup there were slight, transient increases in mean scores for scaling, burning, and stinging at week 4, but all scores remained ≤0.6 where 1=mild (Figure 6).
Post-Inflammatory HyperpigmentationAlthough there appeared to be an age-dependent severity of hyperpigmentation (with the oldest females reporting the more severe disease) at baseline, mean scores were all ≤0.7, where 1=mild (Figure 7). Mean scores did not increase with tretinoin 0.05% lotion treatment, irrespective of age.
FIGURE 5. Absolute change from baseline in Acne-QoL domain scores by age (ITT population, pooled data. Comparison between age groups, female patients treated with tretinoin 0.05% lotion).
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1224
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
L. Stein Gold, D.M. Pariser, E. Guenin
Table 2:
Adolescent Females (13-19)
Adult Females (20-29)
Adult Females (30+)
Tretinoin 0.05% Lotion (N=163)
Vehicle (N=178)
Tretinoin 0.05% Lotion (N=149)
Vehicle (N=173)
Tretinoin 0.05% Lotion (N=75)
Vehicle (N=74)
General disorders and administration site conditions reported by ≥ 1% subjects
Application site pain 7 (4.3%)** 0 (0.0%) 5 (3.4%)**** 0 (0.0%) 4 (5.3%) 2 (2.7%)
Application site dryness 9 (5.5%)* 0 (0.0%) 6 (4.0%)*** 0 (0.0%) 6 (8.0%)***** 0 (0.0%)
Application site erythema 4 (2.5%) 0 (0.0%) 2 (1.3%) 1 (1.3%) 2 (2.7%) 0 (0.0%)
Application site exfoliation 2 (1.2%) 1 (0.6%) 2 (1.3%) 2 (1.2%) 0 (0.0%) 0 (0.0%)
Application site swelling 2 (1.2%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%)
Application site irritation 2 (1.2%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 1 (1.3%) 0 (0.0%)
Application site dermatitis 0 (0.0%) 0 (0.0%) 2 (1.3%) 0 (0.0%) 0 (0.0%) 0 (0.0%)
Application site pruritus 1 (0.6%) 0 (0.0%) 1 (0.7%) 1 (0.6%) 4 (5.3%) 1 (1.4%)
Application site ulcer 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 2 (2.7%) 0 (0.0%)
Application site acne 0 (0.0%) 0 (0.0%) 0 (0.0%) 1 (0.6%) 0 (0.0%) 1 (1.4%)
P =0.001 versus vehicle,**P=0.005, ***P =0.004, ****P =0.045, *****P =0.028
TABLE 2.
Treatment-Emergent Adverse Event (AE) Characteristics Through Week 12 (Safety Population, Pooled Data)
FIGURE 6. Cutaneous safety and tolerability assessment from baseline to week 12 (safety population, pooled data).
FIGURE 7. Post-inflammatory hyperpigmentation: mean scores from baseline to week 12 (safety population, pooled data).
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1225
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
L. Stein Gold, D.M. Pariser, E. Guenin
it is more effective in adult females. It also shows greatest improvement in QoL in these subjects. Coupled with a better tolerability profile tretinoin 0.05% lotion would seem to be an appropriate topical treatment option for adult female acne.
DISCLOSUREDrs Stein Gold and Pariser are advisors and investigators with Ortho Dermatologics. Dr Guenin is an employee of Bausch Health.
ACKNOWLEDGMENTSThe authors acknowledge Brian Bulley, MSc, of Konic Limited for medical writing support. Ortho Dermatologics funded Konic’s activities pertaining to this manuscript.
REFERENCES1. Krowchuk DP. Managing adolescent acne: a guide for pediatricians. Pediatr
Rev 2005;26:250-261. 2. Holzmann R, Shakery K. Postadolescent acne in females. Skin Pharmacol
Physiol 2014; 27(Suppl. 1): 3–8. 3. Schmitt JV, Masuda PY, Miot HA. Acne in women: clinical patterns in different
age-groups. An Bras Dermatol 2009;84:349-354. 4. Schafer T, Nienhaus A, Vieluf D, et al. Epidemiology of acne in the general
population: the risk of smoking. Br J Dermatol 2001;145:100-104. 5. Capitanio B, Sinagra JL, Bordignon V, et al. Underestimated clinical features
of postadolescent acne. J Am Acad Dermatol 2010;63:782-788. 6. Albuquerque RG, Rocha MA, Bagatin E, Tufik S, Andersen ML. Could adult
female acne be associated with modern life? Arch Dermatol Res 2014; 306: 683–688.
7. Goulden V, Stables GI, Cunliffe WJ. Prevalence of facial acne in adults. Am Acad Dermatol 1999; 41: 577–580.
8. Willians C, Layton AM. Persistent acne in women. Am J Clin Dermatol 2006;7(5):281–290.
9. Yentzer BA, Hick J, Reese EL, et al. Acne vulgaris in the United States: a descriptive epidemiology. Cutis 2010;86(2):94–99.
10. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58(1):56–59.
11. Lasek RJ, Chren MM. Acne vulgaris and the quality of life of adult dermatology patients. Arch Dermatol 1998; 134: 454–458.
12. Tan JK, Li Y, Fung K et al. Divergence of demographic factors associated with clinical severity compared with quality of life impact in acne. J Cutan Med Surg 2008; 12: 235–242.
13. Preneau S, Dreno B. Female acne—a different subtype of teenager acne?. J Eur Acad Dermatol Venereol 2012;26(3):277–282.
14. Poli F, Dreno B, Verschoore M. An epidemiological study of acne in female adults: results of a survey conducted in France. J Eur Acad Dermatog Venereol 2001;15(6):541–545.
15. Marks R. Acne and its management beyond the age of 35 years. Am J Clin Dermatol 2004;5(6):459–462.
16. Kamangar F, Shinkai K. Acne in the adult female patient: a practical approach. Int J Dermatol 2012;51(10):1162–74.
17. Tyring SK, Kircik LH, Pariser DM, et al. Novel Tretinoin 0.05% lotion for the once-daily treatment of moderate-to-severe acne vulgaris: Assessment of efficacy and safety in patients aged 9 years and older. J Drugs Dermatol 2018;17(10):1084-1091.
18. Burton JL, Cunliffe WJ, Stafford L. The prevalence of acne vulgaris in adolescence. Br J Dermatol 1971;85(2):119–126.
19. GouldenV,ClarkSM,CunliffeWJ.Post-adolescent acne:a review of clinical features. Br J Dermatol 1997;136(1):66–70.
20. Zeichner JA, Baldwin HE, Cook-Bolden FE, et al. Emerging issues in adult female acne. J Clin Aesthet Dermatol 2017;10(1):37-46.
DISCUSSIONAcne is one of the most prevalent inflammatory skin diseases. It has a peak incidence in both genders in adolescence.18 Interest in adult female acne has increased recently, co-inciding with an increasing prevalence in women. Our post hoc analysis reports on data in female subjects with moderate or severe acne from two large phase 3 clinical studies. Although enrollment into clinical programs is not necessarily representative of the overall acne populations, the data highlight the importance of the female adult population in contrast to male subjects, where the majority of subjects were adolescent. A community survey of more than 700 participants older than 25 years reported clinical facial acne in 12% of women and only 3% of men.19 It has been suggested that acne severity is more mild-to-moderate in adult females. In our analysis, the young adult females (aged 20-29 years) had more severe disease, however, adolescent females had the more comedonal lesions. Interestingly, there appeared to be an age-related efficacy in both lesion count reduction and treatment success, where the older female acne subjects had better outcomes following tretinoin 0.05% lotion. Differences between the age groups were not significant. In one study of postadolescent acne, 85% of patients had mostly comedonal acne.5 In our analysis, tretinoin 0.05% lotion was significantly more effective than vehicle in reducing comedonal acne lesion counts than vehicle in all age groups.
Older women with acne have reported a greater impact of acne on their QoL than younger acne patients.11-15 This finding was borne out by our data where Acne-QoL domain scores were much higher in the adolescent females at baseline (where a lower score represents poorer QoL). Despite differences at baseline, QoL across all three age groups was very similar at week 12, however changes in mean domain scores were only significant compared with vehicle in the young adults.
Older acne patients may also be more susceptible to skin irritation,13 and in clinical practice, many adult female acne patients present with dry skin.20 Tretinoin 0.05% lotion was well-tolerated in women with moderate or severe acne. Application site reactions were uncommon, with skin dryness reported most frequently, especially in older adult females. Adult women with acne also have a higher frequency of post-inflammatory erythema, hyper and/or hypopigmentation, and scarring causing cosmetically disfiguring changes.8 There were slight, transient increases in scaling, burning, and stinging at week 4 in all groups, but mean scores remained ≤0.5, where 1-mild. Although mild, the severity of hyperpigmentation at baseline appeared to be age-related, being more common in adult women. There were no increases in hyperpigmentation with tretinoin 0.05% lotion treatment in any age group.
CONCLUSIONSTretinoin 0.05% lotion appears to provide age-related efficacy benefits in treating moderate-to-severe female acne, whereby
AUTHOR CORRESPONDENCE
Linda Stein Gold MDE-mail:................……......................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1226 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Evaluation of Efficacy of a Skin Care Regimen Containing Methyl Estradiolpropanoate (MEP) for Treating Estrogen
Deficient Skin Joel L. Cohen MD
AboutSkin Research LLC, Greenwood Village, CO
Background: Aging is a complex process due to the interplay of intrinsic factors (such as genetics and hormones) and extrinsic factors (including ultraviolet radiation and pollution). A significant cause of intrinsic aging in women is the loss of estrogen as a result of the onset of menopause. Objective: A single site experience trial to assess the efficacy of Emepelle (Biopelle, Ferndale Pharma Group, Ferndale, MI), a skin care regimen containing Methyl Estradiolpropanoate (MEP)®, for the treatment of Estrogen Deficient Skin (EDS). The secondary objective was to assess patient tolerability and satisfaction.Methods: Fourteen female subjects aged 53-68 years who were amenorrheic for 1-10 years (mean, 5 years), with at least a Grade II in Wrinkling (fine to moderate-depth wrinkles, moderate number of lines) and score of at least 5 (of 9; moderate-to-severe) in elastosis on the clinician-assessed Fitzpatrick-Goldman Classification of Wrinkling and Elastosis Scale, and a 3 or greater on the Investigator Facial Skin Hydration Scale, were included in the study. The subjects were instructed to apply the product Emepelle Serum in the morning, and the product Emepelle Night Cream in the evening to the entire freshly washed and dried face. Follow up visits were performed at 8 weeks, 14 weeks, and 20 weeks to evaluate efficacy and safety. Canfield Visia Complexion Analysis and standard photography was performed at baseline and at each follow up visit.Results: On a 0-4 Facial Hydration Scale, 100% of study participants by week 20 showed at least one-grade improvement and 93% saw two grades or more improvement in hydration. 100% of study participants showed aesthetic improvements per investigator-assessed Global Aesthetic Improvement Scale (GAIS) at week 14. By week 20, 93% of study participants responded that the combination of Emepelle Serum and Night Cream regimen helped improve wrinkles, texture, and color, and 86% of study participants responded that Emepelle helped improve sun-damage, thickness, and integrity. In the Quality of Life questionnaire, 86% responded that Emepelle helped alleviate some or all of the skin issues they developed since entering menopause. Investigator clinical assessment scored pa-tients with a 53% improvement in texture, 21% improvement in keratoses, and 15% improvement in laxity on the Alexiades-Armena-kas Comprehensive Grading Scale for Assessment of Skin Aging and Photodamage by the end of the study at week 20.Conclusions: Patients in the study indicated satisfaction with the formulations of Emepelle Serum and Night Cream. Younger patients showed significant improvement by about 8 weeks. For patients who have been in menopause longer, significant improvement was seen by week 20, suggesting MEP’s potential ability to reactivate dormant estrogen receptors.
J Drugs Dermatol. 2019;18(12):1226-1230.
ABSTRACT
INTRODUCTION
Aging is a complex process due to the interplay of in-trinsic factors (such as genetics and hormones) and extrinsic factors (including ultraviolet radiation and
pollution). A significant cause of intrinsic skin aging in women is loss of estrogen as a result of the onset of the menopause, with this change being referred to as Estrogen Deficient Skin (EDS). Women in menopause manifest characteristics of EDS with documented significant decrease in Collagen I and III and type 1 procollagen, decrease in glycosaminoglycan content, decrease in TGF-β1 expression, reduced expression of IGF-1 re-ceptors and production of IGF-1, and reduced reactive oxygen species (ROS) defense activity, resulting in skin dryness, pruri-
tis, increased wrinkles, thinning, atrophy, and impaired wound healing.1 One of the ways to treat EDS in women is through oral hormone replacement therapy (HRT). While this therapy has many potential benefits, HRT was not specifically developed or recommended for cutaneous benefits and can possibly precipi-tate in some cases significant adverse events, including breast cancer or stroke.
Studies of postmenopausal women indicate that estrogen at-tenuation is associated with hot flashes as well as cutaneous dryness, atrophy, fine wrinkling, and poor healing. Epidermal thinning, declining dermal collagen content, diminished skin
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1227
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
J.L. Cohen
expression of matrixmetalloprotease 1 (MMP-1).5
Methyl Estradiolpropanoate (MEP) is a synthetic estrogenic sterol ester, which has been shown to have estrogen-like cu-taneous effects but is metabolized in the skin to an inactive compound, thus avoiding estrogen side effects.4 Emepelle skin care regimen consists of Emepelle Serum and Night Cream containing MEP that is applied to the face to specifically target estrogen deficient skin. This skincare line takes a multifactorial approach to treat both intrinsic aging and photoaging by in-cluding a number of other cosmeceutical agents.
Emepelle SerumThe Emepelle Serum is a fast-absorbing, oil-free formulation that can be layered with sunscreen or under makeup. The se-rum contains 1% MEP to help activate estrogen receptors in the skin6,7 and is intended for use in either the morning, the evening, or both morning and evening.
The ingredient niacinamide helps induce collagen synthesis and reduce the signs of UV‐induced skin aging. Topical nia-cinamide has shown significant skin appearance improvement effects for clinical signs of photoaging, hyperpigmentation, red blotchiness, and skin sallowness.8 The formula also contains the antioxidants vitamin C, vitamin E, and ferulic acid, which help neutralize free radicals and prevent cell damage from UV radiation.9,10,11 A blend of peptides helps combat oxidative stress and helps improve the appearance of fine lines, wrinkles, and skin laxity.4 Hyaluronic acid helps hydrate and maintain the skin’s moisture barrier.12
Night CreamThe key ingredients in Emepelle Night Cream include 2% MEP that helps to restore the natural function of estrogen deficient skin while utilizing the skin’s natural nighttime repair activities. Retinol 0.1% and hydroxypinacolone retinoate 0.05% aid in nightly rejuvenation and stimulate the production of new blood vessels in the skin, which help improve skin color and reduce the appearance of wrinkles.13 The niacinamide addresses skin tone and texture to help brighten and smooth the appearance of fine lines and wrinkles and provides additional antioxidant protection.8 The inclusion of tetrapeptide-26, palmitoyl oligo-peptide, and palmitoyl tetrapeptide-7 supports cell proliferation and helps combat oxidative stress14; and emollients and humec-tants help hydrate the skin and maintain its moisture barrier.
METHODSAn open-label study was designed to evaluate the efficacy and patient perception of Emepelle’s skin care regimen containing MEP on treating Estrogen-Deficient Skin (EDS).
Fourteen female subjects aged 53-68 years (mean, 60 years) in generally good health who have been amenorrheic for at least 1
moisture, decreased laxity, and impaired wound healing have all been characterized in reports on postmenopausal women.2
Studies have shown a decrease in estrogen levels leads to a 30% loss of collagen in the first 5 years of menopause.3 Es-trogen has been found, at normal blood levels, to help retain and restore skin moisture through the promotion of sebum se-cretion, primarily by regulating the expression of insulin-like growth factor receptors and increasing the production of insu-lin-like growth factors from fibroblasts.4 Women of menopausal age seek alternatives to HRT regimens that are linked with an increase in systemic estrogen. By creating a non-hormonal es-trogen receptor activator (NERA), Ferndale Pharma Group has developed another approach to address aging in the estrogen deficient female. Emepelle (Biopelle, Ferndale Pharma Group, Ferndale, MI) is a new category of skin care. The signature in-gredient, Methyl Estradiolpropanoate (MEP), is not a hormone. It is specifically a non-hormonal compound that can activate estrogen receptors on skin cells. Thus, MEP is an estrogen ana-log that activates the cutaneous estrogen receptor. Once that estrogen receptor activation takes place, the remaining com-pound has no further activity and is found to be an inactive metabolite.5
Methyl EstradiolpropanoateFacial skin aging is accelerated in postmenopausal females due to decreased collagen, reduced hydration, and loss of skin elas-ticity constituting the characteristics of EDS. The presence of estrogen receptors on dermal fibroblasts and epidermal kera-tinocytes confirms the role of estrogen in skin health. A recent double-blind randomized pilot study evaluated the efficacy and tolerability of topical MEP as an anti-aging cosmeceutical with estrogen-like cutaneous effects in postmenopausal women who had never taken hormone replacement therapy (HRT). MEP was applied to the face twice daily for 14 weeks but was metabo-lized in the skin to an inactive compound avoiding estrogen side effects, as demonstrated by the safety study. The efficacy study investigator noted MEP induced statistically significant improvement from baseline at week 14 in dryness (P<0.001), laxity (P=0.001), atrophy (P=0.003), and dullness (P<0.001) as compared to vehicle. Four of nine subjects in the biopsy sub study demonstrated an increase in fibroblast's estrogen recep-tor staining. The novel concept of a safe and efficacious soft estrogen facial cosmeceutical may provide appearance ben-efits for postmenopausal women.
The safety of topical MEP was demonstrated by the lack of ac-tive MEP and the presence of the carboxylic acid MEP inactive metabolite in the serum of subjects who had used the formula-tion for 12 weeks. This soft effect allowed targeted delivery of the MEP to the skin without systemic side effects. Restoration of estrogen-like skin effects might induce the production of col-lagen I, responsible for the strength of the skin, and collagen III, contributing to the elastic skin properties, while reducing the
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1228
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
J.L. Cohen
ing the study period unless provided by their physician. Use of any topical products containing retinoids, hydroquinone, alpha-hydroxy acids, salicylic acid, and vitamins C or E on the face was also restricted for the duration of the study.
Follow up visits with photos were performed at 8 weeks, 14 weeks, and 20 weeks to evaluate efficacy.
Canfield Visia Complexion Analysis and standard photography were performed at baseline and at each of these follow up visits to capture ongoing and post-treatment status.
Quantitative EvaluationsQuantitative evaluations including validated Fitzpatrick-Gold-man Classification of Wrinkling and Degree of Elastosis Scale, Alexiades-Armenakas Comprehensive Grading Scale for As-sessment of Skin Aging and Photodamage, the Facial Skin Hydration Scale, a 0 to 5 scale where 0 = smooth and well-hy-drated skin and 5 = severely dry skin with moderate scaling and coarseness, and Clinician Global Aesthetic Improvement Score (C-GAIS), a 1 to 5 scale, with 1 meaning very much improved and 5 meaning worsened, were performed to assess improve-ment in facial aging. Subject Qualify of Life Questionnaire and Subject Improvement Score evaluations were used to assess tolerability.
Investigator EvaluationsInvestigator performed evaluations included the Fitzpatrick-Goldman Classification of Wrinkling and Degree of Elastosis Scale (0-9 scale) at Visit 1, 2, 3, and 4. A score of 0-4 using the Alexiades-Armenakas Comprehensive Grading Scale for (1) Rhytides, (2) Dyschromia, (3) Erythema-Telangectasia, (4) Ker-atoses, and (5) Texture. For each category, a mean percent improvement was calculated on Visit 1, 2, 3, and 4. The Facial Skin Hydration was used for evaluation on Visit 1, 2, 3, and 4.The Clinician Global Aesthetic Improvement Score (C-GAIS) was completed on Visit 2, 3, and 4. The Investigator Tolerability and Side Effects Assessment was completed at all follow-up visits to evaluate any side-effects including erythema, edema, scaling, and itching (0 to 4 scale where 0 = none and 4 = severe).
Subject EvaluationsThe Subject Global Aesthetic Improvement Score (S-GAIS) was completed on Visit 2, 3, and 4. The Subject Quality of Life Ques-tionnaire was completed by the patient on post-final treatment Visit 2, 3, and 4. The Subject Questionnaire on Quality of Skin Improvement was completed on treatment Visit 2, 3, and 4. The Subject Tolerability and Side Effects Assessment was completed at all follow-up visits (erythema, edema, scaling, and itching on a 0 to 4 scale where 0 = none and 4 = severe).
RESULTSFourteen subjects successfully completed the study.
year and no more than 10 years were enrolled in the study. Each subject enrolled in the study had at least a Grade II in wrinkles and score of 5 (of 9) in elastosis on the Fitzpatrick-Goldman Clas-sification of Wrinkling and Degree of Elastosis Scale, a validated assessment tool used to measure wrinkling and degree of elas-tosis including laxity, dyschromia, erythema, and changes in texture. Each subject enrolled also measured with a score of 3 or greater on the Facial Skin Hydration Scale.
Exclusion criteria included patients who were either currently on hormone replacement therapy, or had ever been treated in the past with hormone replacement therapy, patients using any topical cosmetic anti-wrinkle and/or skin lightening products known to affect skin aging or products containing vitamin A de-rivatives on the face within 14 days prior to or during the study period. In addition, women using any topical imiquimod, 5-fluo-rouracil, or diclofenac on their face within 12 weeks prior to or during the study period were also excluded. Subjects receiving a chemical peel, or a non-ablative laser or light-based therapy on their face must have had discontinued the specific treatment at least 3 months prior to entering the study. Subjects receiv-ing radiofrequency or ultrasound treatment on their face must have had discontinued the treatment at least 6 months prior to entering the study. Subjects receiving traditional dermabrasion (deep skin peel) such as diamond fraise, and/or ablative laser treatments on their face must have had discontinued the treat-ment at least 6 months prior to entering the study. Patients with a history of or the presence of any skin condition/disease that might interfere with the diagnosis or evaluation of study param-eters were also excluded. Other exclusion criteria were having current actinic keratoses or any skin cancer(s) in the treatment areas; significant history or current evidence of a medical, psy-chological or other disorder; prior history of cancer other than basal cell carcinoma (BCC); any active systemic disease that is not yet deemed medically stabilized; or an active bacterial, fun-gal, or viral infection.
Skin Care RegimenSubjects were instructed at the baseline visit to apply one pump of the Emepelle Serum to face in the morning (immediately after cleansing and drying) and to apply a thin layer of Eme-pelle Night Cream to the entire face at night (immediately after cleansing and drying). Subjects were told to only use the skin care products provided and to wash their face twice daily with the provided gentle cleanser (CeraVe®). Each morning, subjects were required to apply the provided facial sunscreen SPF30 (CeraVe®) 15 minutes after applying the Emepelle Serum and to reapply the sunscreen every 2 hours throughout the day if exposed to direct sunlight.
Study restrictions included avoiding excessive exposure to sun-light or sunlamps in the treatment area and not applying any lotions, creams, powders, or solutions to the treated areas dur-
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1230
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
J.L. Cohen
receptors only. Restoration of estrogen-like skin effects might induce the production of collagen.5 The ability to stimulate col-lagen and improve symptoms including dryness, dullness, and fine lines is a benefit to patients with Estrogen Deficient Skin.
In this evaluation, the efficacy of a skin care regimen contain-ing Methyl Estradiolpropanoate for the treatment of facial aging was assessed over 20 weeks. Results showed the regimen im-proved wrinkles, texture, color, and hydration. Patients in the study indicated very high satisfaction with the formulations of Emepelle Serum and the Night Cream. Younger patients in the study spectrum seemed to show significant improvement by about 8 weeks. Older patients who have been in menopause longer showed notable improvement by 20 weeks.
Further study on the effects of MEP technology may lead to bet-ter treatments for premenopausal patients and pre-juvenation skin care regimens.
DISCLOSUREJoel L. Cohen MD is a consultant for Ferndale Pharma Group, Inc., Ferndale, MI.
REFERENCES1. Mukherjee S, Date A, Patravale V et al. Clin Interv Aging. 2006;1:327-348.2. Hall G, Phillips TJ. Estrogen and skin: the effects of estrogen, menopause,
and hormone replacement therapy on the skin. J Am Acad Dermatol. 2005;53:555-68.
3. Archer DF. Postmenopausal skin and estrogen. Gynecol Endocrinol. 2012;28(suppl 2):2-6.
4. Ashcroft GS, Dodsworth J, vanBoxtel E, Tarnuzzer RW, Horan MA, Schultz GS, et al. Estrogen accelerates cutaneous wound healing associated with an increase in TGF-beta1 levels. Nat Med. 1997; 3: 1209-1215
5. Draelos ZD. A double-blind randomized pilot study evaluating the safety and efficacy of topical MEP in the facial appearance improvement of estrogen deficient females. J Drugs Dermatol. 2018:17:1186-1190
6. Guven C, Dal F, Ahbab MA et al. Low dose monoethyl phthalate (MEP) ex-posure triggers proliferation by activating PDX-1 at 1.1B4 human pancreatic beta cells. Food and Chemical Toxicology. 2016. 93:41-50)
7. Katzenellenbogen BS. Estrogen receptors: bioactivities and interactions with cell signaling pathways. 1996. Biol Reprod. 54:287-293.
8. Bissett DL, Oblong JE, Berge CA. Niacinamide: A B vitamin that improves aging facial skin appearance. Dermatol Surg. 31:7:860-865.
9. Levin J, Momin SB. How much do we really know about our favorite cosme-ceutical ingredients? J Clin Aesthet Dermatol. 3(2); 2010. 22-41.
10. Traber MG, Stevens JF. Vitamins C and E: Beneficial effects from a mecha-nistic perspective. Free Radic Biol Med. 2011. 51(5). 1000-1013.
11. Addor FAS. Antioxidants in dermatology. An Bras Dematol. 2017. 92(3): 356-363. 12. Papakonstantinou E, Roth M, Karakiulakis G. Hyaluronic acid: A key molecule
in skin aging. 2012. Dermatoendocrinol. 4:(3) 253-258.13. Kang S, Fisher GJ, Vorhees JJ. Photoaging: pathogenesis, prevention, and
treatment. Clin Geriatr Med. 2001. 17(4):643-659.14. Fisher GJ, Quan T, Purohit T, Shao Y et al. Collagen fragmentation promotes
oxidative stress and elevates matrix metalloproteinase-1 in fibroblasts in aged human skin. Am J Pathol. 2009 174:101-114.
15. Affinito (was 6) P, Palomba S, Sorrention C. Di Carlo C,Bifulco G, Arienzo MP, Nappi C. Effects of postmenopausal hypoestorgenism of skin collagen. Maturitas. 1999.15;33(3):239-47.
16. Rzepecki AK, Murase J, Juran R, Fabi S, McLellan B. Estrogen deficient skin: the role of topical therapy. Int J Womens Dermatol. 2019;5:85-90.
more estrogen receptors and turn the pathways back on. This suggests that the longer patients have been amenorrheic, the more of their estrogen receptors have been lost, or at least have become more dormant or down-regulated.
CONCLUSIONFacial skin aging in postmenopausal females is due to cumula-tive photodamage and other intrinsic factors such as decreased collagen, reduced hydration, and loss of skin elasticity constitut-ing the characteristics of Estrogen Deficient Skin. The presence of estrogen receptors on dermal fibroblasts and epidermal ke-ratinocytes seems to have a direct role in women’s skin health. This research examined the efficacy and tolerability of topical Methyl Estradiolpropanoate (MEP) as an anti-aging cosme-ceutical with estrogen-like cutaneous effects in an open-label evaluation of postmenopausal women who had never taken hormone replacement therapy (HRT).
The significance of MEP technology is that it is a non-hormonal estrogen receptor activator that specifically addresses signs and symptoms of Estrogen Deficient Skin. Estrogen attenua-tion begins to take place in perimenopause and is accelerated in menopause. Again, it is important to indicate that MEP is a non-hormonal estrogen receptor activator that is specific to the skin. It is not a hormone, yet, has specific effects on specific skin
FIGURE 3. Fifty-three-year-old female patient at baseline and week 20 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
FIGURE 4. Sixty-three-year-old female patient at baseline and week 20 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
FIGURE 4: Fifty-three-year-old female patient at baseline and week 20 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
FIGURE 5: Sixty-three-year-old female Patient at baseline and week 20 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
AUTHOR CORRESPONDENCE
Joel L. Cohen MDE-mail:................……......................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1229
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
J.L. Cohen
Week 8At week 8, 93% of patients felt that they were “more comfort-able” with the appearance of their skin compared to baseline and 50% or more of the participants reported improvement in wrinkles, thickness, integrity, dullness, texture, and color. Also, at week 8, on the 0 to 5 Facial Skin Hydration Scale, 100% of study participants documented at least one grade improvement and 64% verified two grades or more improvement.
By week 8, subjects showed a 34% improvement in texture on the Alexiades‐Armenakas Comprehensive Grading Scale for Assessment of Skin Aging and Photodamage. On the Subject Questionnaire on Quality of Life, 93% said their skin felt “more comfortable” post application of the topical products, that their skin “looked better”.
Week 14On a 0-5 Facial Skin Hydration Scale, 100% of study participants showed at least 1-step improvement and 8 of 14 (57%) saw a 2-grade or more improvement in hydration. 100% of study participants showed aesthetic improvements per Investigator Global Aesthetic Improvement Scale (GAIS) at week 14.
Baseline to Week 20By week 20, 93% of study participants responded that Emepelle helped improve the appearance of wrinkles, texture, and color.
Also, by week 20, 86% of study participants responded that Emepelle helped improve the appearance of sun damage, thick-ness, and integrity. In the Subject Questionnaire on Quality of Life, 86% of study participants responded that Emepelle helped alleviate some or all of the skin issues they have developed since entering menopause by week 20.
Overall, from baseline to end of study at 20 weeks, patients showed a 53% improvement in texture, 21% improvement in keratoses, and 15% improvement in laxity on the Alexiades-Ar-menakas Quantitative and Comprehensive Grading Scale.
DISCUSSIONWhile all patients experienced at least a 1-step improvement in hydration on a 5-point scale at 8 weeks onward, more notable hydration improvements occurred throughout the course of the study. For example, at 8 weeks, only 7% of patients experienced a 3+ step improvement in hydration whereas at 20 weeks, 64% of patients experienced a 3+ step improvement in hydration.
More notable improvements were made in terms of appearance of the skin and menopausal-related skin issues throughout the course of the study. For example, at 8 weeks, 21% of patients reported 'very' or 'extremely' to the question "Do you feel the application of the study topical products made your skin look better" vs 64% after 20 weeks.
Furthermore, at 8 weeks, 7% of patients reported 'very' or 'ex-tremely' to the question "Do you feel the study products have helped alleviate some or all of the skin issues you have devel-oped since entering menopause" compared to 64% at 20 weeks.
Studies have shown that estrogen attenuation/diminution in postmenopausal conditions accelerates many skin changes, including dryness, atrophy, fine wrinkling, and poor wound healing.15 Thus, the effects of low estrogen on the skin are an important endogenous cause of aging skin in women; yet, topi-cal strategies that target estrogen deficiency are limited.16
In this open-label experience trial, all patients expressed sat-isfaction with the formulations of Emepelle Serum and Night Cream. Patients on the younger end of the study spectrum (53-60 years) seemed to show significant improvement in about 8 weeks (See Figures 1 and 2).
In older patients (over 63 years) who presumably have been in menopause longer, significant improvement seemed to take longer, but was shown by 20 weeks (See Figures 3 and 4).
Since a subset of older trial participants took longer for their roughness and dryness to improve, it may take time to rebuild
FIGURE 1. Fifty-three-year-old female patient at baseline and week 8 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
FIGURE 2: Fifty-three-year-old female patient at baseline and week 8 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
FIGURE 2. Sixty-year-old female patient at baseline and week 8 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
FIGURE 3: Sixty-year-old female patient at baseline and week 8 after morning use of Emepelle Serum and evening use of Emepelle Night Cream. Photo Courtesy of Joel L. Cohen MD
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1231 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Learning Analytics to Enhance Dermatopathology Education Among Dermatology Residents
Euphemia W. Mu MD,a,b Martin Pusic MD PhD,c,d Matt Coneybeare BA MBA,e Shane A. Meehan MDa,f
ªThe Ronald O. Perelman Department of Dermatology, New York University (NYU) School of Medicine, New York, NYBPiedmont Plastic Surgery & Dermatology, Charlotte, NC
cThe Ronald O. Perelman Department of Emergency Medicine, NYU School of Medicine, New York, NYDDivision of Learning Analytics, Institute for Innovations in Medical Education, NYU School of Medicine, New York, NY
EDepartment of Computer Science, University of California, Berkeley, Berkeley, CAfDermatology of Pathology, NYU School of Medicine, New York, NY
Background: With the advent of digital microscopy, learning analytics can be leveraged to advance teaching of dermatopathology in dermatology residency.Objective: To analyze the acquisition and decay of dermatopathology visual recognition skills and areas of diagnostic confusion amongst residents using learning metrics generated by a web-based learning tool.Methods: This was a prospective, longitudinal study of dermatology residents who studied digital photomicrographs of 18 routine diagnostic entities using an online software platform. Residents at different years of training were given 60 minutes to complete as-sessments on three occasions (initial test with follow-ups at one and three months).Results: 4,938 responses were analyzed. Accuracy and time to diagnosis improved within each assessment and between the first and second assessments. First year residents showed knowledge decay when tested at three months (67% vs 64%; P=0.002) while third year residents retained knowledge and continued to improve upon their accuracy after three months (83% to 91%, <0.001). Learning analytics highlighted diagnostically challenging cases for residents that contradicted experts’ predictions (R=0.48).Conclusions: The use of learning analytics and interactive digital platforms enhances dermatopathology curriculum development by identifying challenging diagnostic entities, assessing mastery of subject material, and optimizing review schedules.
J Drugs Dermatol. 2019;18(12):1231-1236.
ABSTRACT
INTRODUCTION
Traditional methods for instructing dermatopathology rely heavily on approaches such as didactics and stan-dard microscopy. In response to shortcomings of con-
ventional medical education techniques, advances in learning sciences offer promising new tools for learners and instructors with a goal of more efficiently acquiring knowledge.1 Prior studies have utilized digital test-enhanced learning to evaluate proficiency in clinical dermatology,2 histology,3 and radiogra-phy.4 The use of learning analytics in dermatopathology has not been well studied.
We present a web-based dermatopathology learning applica-tion to demonstrate that resident education can be enhanced using data-driven approaches. We developed an electronic platform to assess the acquisition of dermatopathology skills by dermatology residents over time with the goal of optimizing their dermatopathologic educational curriculum.
METHODSParticipant Recruitment and Setting For this study, we recruited 24 dermatology residents in the
Ronald O. Perelman Department of Dermatology at the New York University School of Medicine. To compare with a reference standard, we also invited three board-certified dermatopatholo-gists from three separate institutions to take the survey under study conditions. All participants provided informed consent, and the study was approved by the NYU Institutional Review Board. Histologic Image Selection and Diagnostic Classification Selected histologic images of 90 different cases comprised 18 diagnostic entities in the spindle cell neoplasm differential. Each case was chosen from a slide teaching collection created by the Ronald O. Perelman Department of Dermatology, and three magnifications were captured using the Olympus DP70 camera and Aperio slide scanner. The cases included had each been previously diagnosed by an experienced board-certified dermatopathologist and included: atypical fibroxanthoma, an-giofibroma, angioleiomyoma, blue nevus, dermatofibroma, dermatofibrosarcoma protuberans, dermatomyofibroma, desmoplastic melanoma, hypertrophic scar, Kaposi sarcoma, leiomyoma, neurofibroma, neurothekeoma, nodular fasciitis, normal skin, scar, schwannoma, and traumatic neuroma.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1232
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.W. Mu, M. Pusic, M. Coneybeare, S.A. Meehan
using a generalized linear mixed-effects model with a binomial link function taking into account grouping of cases within indi-viduals. To investigate the relationship of accuracy on an item with level of training and test occasion, we use a mixed logistic regression model that again took into account grouping of cases within individuals. Training level of respondents, accuracy, and time taken to re-spond were compared by the χ2 test or ANOVA for categorical variables and Student's t-test for continuous variables. Analyses were conducted in Intercooled Stata 13.0 for Mac (Stata Corp, College Station, TX). P-values less than 0.05 were considered significant.
Ranking DifficultyThree dermatopathologists were asked to rank the 18 diagnoses by predicted difficulty for learners. The actual rank of diagnos-tic difficulty for each diagnosis was determined based on the average learner accuracy under testing conditions. A Pearson correlation plot was calculated to compare experts’ ranking of predicted difficulty compared to actual ranking of how accurate-ly the histologic cases were diagnosed by learners.
RESULTSIdentifying Areas of Diagnostic ConfusionExperts were unable to accurately predict which cases would be diagnostically challenging for learners. A Pearson correlation plot of the average expert prediction of the most challenging diagnoses vs. the accuracy of the residents’ diagnoses showed poor correlation (R=0.48) (Figure 2). Interestingly, expert pre-dictions correlated more with each other (R=0.78 and R=0.63). Points along the dotted line indicate where the experts’ aver-age ranking of a diagnosis correlates with the accuracy of the
Online Software Application for Presentation of Dermatopathol-ogy Cases We developed a website (www.dermrecall.com) using HTML (version 4, World Wide Web Consortium, Cambridge, MA) and implemented using Ruby on Rails (version 5.0). Data was safeguarded via a participant-created username and unique password. Participants were permitted to complete the three sessions at a site of their choice on specified dates. The software tracked participants’ progress through the cases and recorded their responses to a mySQL Database (version 4.0.27-max-log, MySQL AB, Uppsala, Sweden)
For each case, the participant first viewed a screen listing a low power histologic image with a multiple-choice screen listing the 18 differential diagnoses (Figure 1). Clicking on thumbnail im-ages allowed viewers to view cases at low, medium, and high power. There was a 60-minute time limitation to answer the 90 questions. When the participant submitted an answer, he or she received immediate feedback including the correct diagnosis and a histologic image with a description of the pertinent histo-logic findings. Cases were presented in a random order unique to each participant so as to minimize order effects, and his or her subsequent surveys were presented in an identical order to his or her initial survey.
Study ProcedureWe contacted all 24 residents from three residency years in the Ronald O. Perelman Department of Dermatology enrolled dur-ing the 2016 to 2017 academic year. A total of 22 residents (92% of those eligible) participated in the study. The initial survey was administered online with participants creating de-identified usernames and passwords and indicating their level of train-ing. Participants were asked to repeat the survey one month and three months after their initial session. In addition, three experienced dermatopathologists completed the survey for one iteration to confirm the diagnoses under the study conditions.
DATA ANALYSISScoringWe considered each case completed by a participant to be one item. We scored each item dichotomously (correct, incorrect) de-pending on the match between the participant’s response and the diagnosis as confirmed by three board-certified dermatopa-thologists.
Test MeasuresFor each training year and participant, we determined the ac-curacy and time taken to diagnose each case. To describe the learning improvement over cases with feedback, we compared the residents’ diagnostic accuracy on the first 30 cases to that of the final 30 cases, assessing differences for statistical signifi-cance using paired t-tests to generate 95% confidence intervals around the differences. We also plotted learning trajectories
FIGURE 1. Example interface for displaying the 90 cases. A low power image is shown with options to view the image at higher magnifications. The participant is given a static list of 18 diagnoses from which to choose their answer. The remaining time is displayed in the top right-hand corner.
FIGURES
Figure 1. Example interface for displaying the 90 cases. A low power image is shown with options to view the image at higher magnifications. The participant is given a static list of 18 diagnoses from which to choose their answer. The remaining time is displayed in the top right-hand corner.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1233
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.W. Mu, M. Pusic, M. Coneybeare, S.A. Meehan
histologic diagnoses rendered by the residents under testing conditions. Points on either side of the line show some degree of mismatch. Compared to expert predictions, learners found fibrohistiocytic and neural neoplasms to be more diagnostically challenging and melanocytic neoplasms to be less so (Figure 2).
FIGURE 2. Pearson correlation plot of the average expect prediction vs actual rank of the 18 diagnoses by difficulty under testing conditions (R=0.48). A ranking of 1 denotes the easiest or most accurately diagnosed entity, and 18 denotes the hardest or least accurately diagnosed entity. Points along the dotted line indicate that the experts’ ranking of that diagnosis correlates exactly with how accurately the histologic cases were diagnosed under testing conditions.
Figure 2. Pearson correlation plot of the average expect prediction vs actual rank of the 18 diagnoses by difficulty under testing conditions (R=0.48). A ranking of 1 denotes the easiest or most accurately diagnosed entity, and 18 denotes the hardest or least accurately diagnosed entity. Points along the dotted line indicate that the experts’ ranking of that diagnosis correlates exactly with how accurately the histologic cases were diagnosed under testing conditions.
FIGURE 3. Diagnostic heat map showing areas of diagnostic confusion. The colors on the heat map depict the correlation of resident responses to the correct answers as determined by expert dermatopathologists. Red and blue squares correspond to high and low correlation, respectively. The central diagonal of red squares demonstrates that the majority of residents’ responses are correct. Darker blue corresponds to areas with little diagnostic confusion, and lighter blue, green, orange, and yellow squares represent areas of increasing diagnostic confusion. The most commonly confused items included: acquired fibrokeratoma for traumatic neuroma, angioleiomyoma for schwannoma, traumatic neuroma for neurothekeoma, leiomyoma for hypertrophic scar and vice versa, and Kaposi sarcoma for dermatofibroma.
Figure 3. Diagnostic heat map showing areas of diagnostic confusion. The colors on the heat map depict the correlation of resident responses to the correct answers as determined by expert dermatopathologists. Red and blue squares correspond to high and low correlation, respectively. The central diagonal of red squares demonstrates that the majority of residents’ responses are correct. Darker blue corresponds to areas with little diagnostic confusion, and lighter blue, green, orange, and yellow squares represent areas of increasing diagnostic confusion. The most commonly confused items included: acquired fibrokeratoma for traumatic neuroma, angioleiomyoma for schwannoma, traumatic neuroma for neurothekeoma, leiomyoma for hypertrophic scar and vice versa, and Kaposi sarcoma for dermatofibroma.
Analyzing the 4,938 responses also allowed identification of commonly confused entities (Figure 3). The colors on the heat map depict the correlation of resident responses to the correct answers. Red and blue squares correspond to high and low correlation, respectively. The central diagonal of red squares
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1234
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.W. Mu, M. Pusic, M. Coneybeare, S.A. Meehan
demonstrates that the majority of residents’ responses are correct. Darker blue corresponds to areas with little diagnostic confusion, and lighter blue, green, orange, and yellow squares represent areas of increasing diagnostic confusion.
Improvements in Accuracy and Speed Within AssessmentsThe mean accuracy of the participants improved over the course of the 90 histologic images (Figure 4A). Across all participants, the accuracy of the first to the last 30 cases improved from 71.7% to 77.2%, with a difference of 5.5% (95% confidence interval of the difference [CID]: 2.5% to 8.4%; P<0.001). This difference was in large part due to the first-year dermatology residents, who improved on average from 57.5% (Standard Deviation [SD] 49.5%) to 66.5% (SD 47.2%), with an average difference of 8.9% (95% CID: 3.2%, 14.5%; P=0.001) and second-year residents, who improved on average from 74.0% (SD 43.9%) to 81.5% (SD 38.9%), with an average difference of 7.5% (95% CID: 2.2% to 13.8%; P=0.003) from the first third to last third of the exam. The third-year residents showed no statistical difference in av-erage accuracy between portions of the exam with an average of 82.5% (SD 37.9%) for both the first and last third of the test. Figure 4A presents the results of the predicted probability cor-rect during each case sequence across three cumulative tests by training level. For each of the test characteristics, the linear mixed model graph patterns at the group level were similar, qualitatively. Both test occasion (OR 1.85, 95% CI: 1.4, 2.4) and level of training (1.25, 1.14, 1.37) were statistically significantly associated with accuracy.
The average time per case decreased as cases progressed with-in each assessment (Figure 4B), from a mean of 24.1 seconds/case to 14.6 seconds/case in the first to last 30 cases with a dif-ference of 9.4 seconds/case (95% CI of difference: 8.2 to 10.6 seconds/case; P<0.001). Between the first and last third of the exam, first-year residents averaged 27.6 vs 15.3 seconds/case, second-year residents 24.2 vs 15.2 seconds/case, and third-year residents 20.1 vs 13.1 seconds/case, with average differences
of 12.3, 9.0, and 7.0 seconds/case among the first-, second-, and third-years, respectively.
Increased Accuracy and Speed With Higher Training LevelAs expected, more advanced learners demonstrated a higher average accuracy (Table 1A). Of note, participants of all resi-dent training levels improved after the second assessment one month later. While first-year residents’ average performance de-creased when tested three months later, second- and third-year residents appear to not only have retained knowledge but to have continued to improve their accuracy.
Successive attempts were also correlated with decreased aver-age time per case (Table 1B). On the initial assessment, there was a greater difference between first-, second-, and third-year
FIGURE 4B. Graphs showing the average time per case by training level and occasion of testing.
Figure 4A. Graphs showing the predicted average accuracy by training level and occasion of testing.
Figure 4B. Graphs showing the average time per case by training level and occasion of testing.
FIGURE 4A. Graphs showing the predicted average accuracy by training level and occasion of testing.Figure 4A. Graphs showing the predicted average accuracy by training level and occasion of testing.
Figure 4B. Graphs showing the average time per case by training level and occasion of testing.
TABLE 1A.
Average Accuracy by Residency Year and Successive Assessments
Initial Avg (95% CI)
One Month Avg (95% CI)
Three Months Avg (95% CI)
P
Residency Year
First 57% (53 - 61%) 67% (62 - 71%) 64% (60 - 68%) 0.002
Second 76% (73 - 80%) 79% (75 - 83%) 80% (76 - 84%) 0.27
Third 78% (75 - 81%) 83% (70 - 86%) 91% (88 - 94%) <0.001
Avg = average, CI = confidence interval
TABLE 1B.
Time (seconds per case) by Residency Year and Successive Assessments
Initial Avg (95% CI)
One Month Avg (95% CI)
Three Months Avg (95% CI)
P
Residency Year
First 23.2 (21.8 - 24.6) 20.6 (18.9 - 22.4) 16.6 (15.4 - 17.9) 0.001
Second 21.5 (19.5 - 23.5) 18.5 (16.3 - 20.7) 17.1 (15.7 - 18.4) 0.0039
Third 17.6 (16.4 - 18.7) 15.5 (14.3 - 16.6) 13.8 (12.7 - 14.9) <0.001
Expert 22.6 (19.5 - 25.6) -- -- -- -- --
Avg = average seconds/case, CI = confidence interval
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1235
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.W. Mu, M. Pusic, M. Coneybeare, S.A. Meehan
residents (23.2 vs. 21.5 vs 17.6 seconds/case) compared to on the third assessment (16.6, 17.1, 13.8 seconds/case, respectively). In-terestingly, expert dermatopathologists used a greater amount of average time per case (22.6 seconds/case) than second- and third-year residents during the first assessment.
DISCUSSIONResidency programs vary in their teaching of dermatopathol-ogy from weekly reviews of glass slides, to didactic lectures to observing routine cases diagnosed on a dermatopathology service. Mastery or expertise in an area of learning, such as der-matopathology, may be attained by deliberate practice whose essential elements include motivation, immediate feedback and repetition as described by Ericsson.5 Acquisition of knowledge by means of deliberate practice has been documented in the medical education literature from the interpretation of radio-graphs to simulation of surgeries,6,7 and learning analytics have been used to inform and deploy effective strategies in present-ing curricula to residents in training.
Herein, we analyzed how dermatology residents learn to di-agnose a particular subset of neoplasms in dermatopathology using a web-based approach with immediate feedback. Nota-bly, we found that our experts had difficulty predicting which cases would be more diagnostically challenging for residents. For example, experts incorrectly assumed that certain mela-nocytic neoplasms would pose the most diagnostic difficulty, but learning analytics revealed that residents were more likely to incorrectly diagnose neural and fibrohistiocytic neoplasms. In addition, analysis of answer choices allowed for identifica-tion for specific areas of diagnostic confusion between entities by residents- the most difficulty was distinguishing neural neoplasms from other fibrohistiocytic and smooth muscle neo-plasms. These results suggest that learning analytics could be used to target diagnostic areas that are particularly challenging and improve the performance of a resident group. Personalized analysis could be employed to customize learning for a specific individual.
Predictably, across all participants the average time to diagnosis decreased while their accuracy improved within each test, and the average accuracy achieved in the initial survey and at three months was greater depending on the level of experience (ie, first- vs second-year residents). These findings are comparable to those in the analysis of deliberate practice amongst trainees in other disciplines using a similar web-based bank of images, supporting the effectiveness of this mode of educational inter-vention.8
With regards to loss of knowledge, skill decay with similar learning interventions has been demonstrated in a variety of domains at 6 months but may occur in as few as 2 to 4 months.9 In our study those with the least experience (first-year resi-
dents) demonstrated the greatest knowledge decay at 3 months in comparison to 1 month after the initial survey. In contrast, the third-year residents not only retained knowledge acquired during the initial assessment, but also improved upon their performance with each survey. Decay in knowledge has been correlated with a variety of factors including the strength in which knowledge is initially attained.10 Given that first-year resi-dents demonstrated the fastest decline in their visual diagnostic skills, an earlier and more robust introduction to the diagnostic entities depicted in our survey may have resulted in a more du-rable learning of the material for this group.
Presumably, the senior residents’ exposure to the diagnostic en-tities depicted in the surveys through formal teaching sessions, routine sign-out and/or deliberate practice, formed a basis for encoding of their visual knowledge that resulted in better reten-tion than junior residents and consequently higher scores on the surveys. Other strategies to enhance retention of material include the type of practice schedule employed and the meth-od of learning intervention.11 For example, scheduled practice based on the predictability of knowledge decay depicted by for-getting curves leads to more effective retention of material.11
A web-based approach to learning dermatopathology with the application of learning analytics has a variety of advantages and implications. In addition to being readily accessible and time and resource efficient, data driven learning can be used to in-form, for example, the number of cases necessary for a group of residents to review to attain a certain level of competency. Alternatively, an analysis could be employed to monitor an individual’s learning and/or forgetting of the subject material, leading to advancement or remediation when necessary.
The study of diagnostic retention and skill decay of dermatopa-thology amongst dermatology residents could also be used to design the schedule and manner in which material is introduced during their curricula. Our study suggests that those with less experience (first-year residents) may require a more robust in-troduction to increase the likelihood that their visual diagnostic abilities are retained. Those with greater experience (third-year residents) who have demonstrated a certain level of retention may benefit from devoting more time to areas of diagnostic confusion within dermatopathology or other elements of the dermatology residency curriculum rather than “overtraining” in dermatopathology. Given a goal of dermatology residency curricula is to achieve certain competency levels, a universal web-based learning tool such as ours could be used to stan-dardize the assessment of specific milestones across programs for various disciplines.
Our study has a number of limitations. The analysis involved a small cohort of residents at one institution who were tested on a narrow set of histologic images, which may limit the generaliz-
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1236
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.W. Mu, M. Pusic, M. Coneybeare, S.A. Meehan
ability of the study. Also, there was a limited period of follow-up, hence no conclusions can be made regarding the retention of this material beyond 3 months. Informative future studies could include greater follow-up time, participants from multiple insti-tutions, and wider question banks.
In summary, we discuss the advantages of using learning analytics with a web-based tool to improve teaching of der-matopathology by dermatology residents. Learning analytics may enhance curriculum development by optimizing review schedules, identifying particularly challenging diagnoses, and assessing mastery of the subject material. Data driven learning allows one to make calculations such as the projected number of cases necessary for a junior resident to study in order to achieve the performance of a senior resident, or of a senior resident to achieve the mastery of a board certified dermatopathologist, for example. Web-based tutorials utilizing digital microscopy images allow assessment of learning metrics to provide more efficient and targeted learning than conventional methods, and such an approach may be generalizable to improve other ele-ments of the dermatology education.
DISCLOSURESThe authors have no conflicts of interest.
ACKNOWLEDGMENTThe authors would like to thank Ann Perry MD, Jeff Harvell MD, Joshua Mu, and the NYU dermatology residents for their contri-butions to this study.
REFERENCES1. Kellman PJ. Adaptive and perceptual learning technologies in medical educa-
tion and training. Mil Med 2013;178:98-106.2. Rimoin L, Altieri L, Craft N, Krasne S , Kellman PJ. Training pattern recogni-
tion of skin lesion morphology, configuration, and distribution. J Am Acad Dermatol 2015;72:489-95.
3. Krasne S, Hillman JD, Kellman PJ , Drake TA. Applying perceptual and adap-tive learning techniques for teaching introductory histopathology. J Pathol Inform 2013;4:34.
4. Pusic M, Pecaric M , Boutis K. How much practice is enough? Using learning curves to assess the deliberate practice of radiograph interpretation. Acad Med 2011;86:731-6.
5. Ericsson KA. The Cambridge handbook of expertise and expert performance. Cambridge ; New York: Cambridge University Press; 2006.
6. Boutis K, Pecaric M, Seeto B , Pusic M. Using signal detection theory to model changes in serial learning of radiological image interpretation. Adv Health Sci Educ Theory Pract 2010;15:647-58.
7. McGaghie WC, Issenberg SB, Petrusa ER , Scalese RJ. Effect of practice on standardised learning outcomes in simulation-based medical education. Med Educ 2006;40:792-7.
8. Boutis K, Cano S, Pecaric M, Welch-Horan TB, Lampl B, Ruzal-Shapiro C et al. Interpretation difficulty of normal versus abnormal radiographs using a pediatric example. Can Med Educ J 2016;7:e68-77.
9. Matterson HH, Szyld D, Green BR, Howell HB, Pusic MV, Mally PV, et al. Neonatal resuscitation experience curves: simulation based mastery learn-ing booster sessions and skill decay patterns among pediatric residents. J Perinat Med 2018;46:934-941..
10. Stothard C , Nicholson R. Skill Acquisition and retention in training: DSTO support to the army ammunition study. Defence Science & Technology Organisation 2001;DSTO-CR-0218.
11. Wolf G. Want to remember everything you’ll ever learn? Surrender to this algorithm. Wired 2008;16.
AUTHOR CORRESPONDENCE
Shane A. Meehan MDE-mail:................……......................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1237 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Hispanic Tattoo Artists Could Provide Skin Cancer Prevention via Aftercare Instructions and Social Media
Cristian D. Gonzalez MD,a Adrian Pona MD,a Barbara J. Walkosz PhD,b Robert P. Dellavalle MD PhD MSPHa,c
aDepartment of Dermatology, University of Colorado School of Medicine, Aurora, CObKlein Buendel, Inc, Golden, CO
cUS Department of Veterans Affairs Rocky Mountain Regional VA Medical Center Dermatology Service, Aurora, CO
Background: The incidence of melanoma and non-melanoma skin cancer in the Hispanic population has increased. Hispanics are more likely to present with advance-staged melanoma and worse overall prognosis. Thus, public health campaigns are necessary to target the underrepresented Hispanic population.Objective: To explore Hispanic tattoo artists’ skin cancer knowledge, sun safety recommendations, and their willingness to implement primary and secondary skin cancer prevention in their daily work routines.Methods: We conducted an in-depth semi-structured interview study with ten Hispanic tattoo artists. Interviews were conducted at multiple tattoo studios in Salt Lake City, Utah.Data was coded by a third-party. Thematic analysis identified recurrent sub-themes from the transcript.Results: Majority of Hispanic tattoo artists had a high percentage of Hispanic clientele (mean: 51%, range: 25-93%) and repeat cus-tomers (mean: 73%, range: 50-90%). All tattoo artists had suboptimal skin cancer knowledge. Most Hispanic tattoo artists provide inadequate sun protective information in their aftercare instructions including a specific Sun Protection Factor, sunscreen reapplication, and protective clothing. However, all tattoo artists were willing to provide sun protective information on their social media profiles and undergo primary and secondary skin cancer prevention training.Conclusion: Hispanic tattoo artists could serve as public health allies and influence early detection of skin cancers in the Hispanic population by implementing preventative skin cancer behaviors in their daily work routines and providing comprehensive sun safety information through aftercare instructions and social media.
J Drugs Dermatol. 2019;18(12):1237-1243.
ABSTRACT
INTRODUCTION
The incidence of melanoma and nonmelanoma skin cancers (NMSC) have grown exponentially. Although the incidence of melanoma affects 22.8 patients per
100,000 in the United States (U.S.), the incidence of melano-ma in the Hispanic population in the U.S. is 4.4 patients per 100,000.1-4 Furthermore, since Hispanics do not represent the majority of the U.S. population, per population basis, the inci-dence of melanoma in Hispanics is further underrepresented.5 To prevent the increasing melanoma and NMSC incidence, pub-lic health campaigns were introduced to prevent melanomas and NMSCs, increase melanoma and NMSC awareness, and detect early stages of melanoma and NMSC.6 Although mela-noma and NMSC public health campaigns were introduced ir-respective to a specific ethnicity, cultural and language barriers exist, and melanoma and NMSC public health campaigns tar-geting Hispanics in the U.S. are limited. Furthermore, the abil-ity of healthcare providers to convey high quality skin cancer information in a culturally sensitive approach to the Hispanic community is scarce.7
Increased melanoma and NMSC awareness has influenced medical professionals to implement skin cancer prevention into their clinical routine, although nonmedical professionals can also provide primary and secondary skin cancer preven-tion.8-10 In a survey study exploring a massage therapists role in skin cancer prevention, a majority of massage therapists have previously recognized suspicious lesions on their clients and referred them to a medical professional.8 Although some tra-ditional nonmedical professionals, including hair dressers and massage therapists, offer skin cancer prevention, tattoo artists are also cognizant of skin cancer prevention; as they refrain from tattooing suspicious lesions and refer some of their clients to a healthcare provider.11 Tattoo artists could incorporate skin cancer prevention in their daily work routine by providing full-body, comprehensive sun protection advice to their clients, and refer suspicious moles to a healthcare professional.
The purpose of this study was to investigate Hispanic tat-too artist’s knowledge of skin cancer and their willingness to
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1238
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
C.D. Gonzalez, A.Pona, B.J. Walkosz, R.P. Dellavalle
Sub-themes derived from the analysis included— lack of sun protection knowledge among tattoo artists, need for a culturally sensitive approach to aftercare instructions, need for a stron-ger connection between the medical and tattoo community, and stronger tattoo practicing regulations.
RESULTSTen Hispanic tattoo artists were interviewed (Table 1). Majority of tattoo artists were male (90%) with a mean age of 30 (stan-dard deviation, 5). Of the ten tattoo artists, six tattoo artists were born in the U.S. Furthermore, of the ten tattoo artists, seven tat-too artists have a Mexican heritage. Six tattoo artists were fully bilingual in English and Spanish. Many of them reported a high percentage of Hispanic clientele (mean, 51%; range, 25-93%) and repeat customers (mean, 73%; range, 50-90%).
Skin Cancer KnowledgeNone of the Hispanic tattoo artist knew the difference between melanoma and non-melanoma skin cancer. All tattoo artists felt they would not be able to detect an abnormal mole or skin cancer. When tattoo artists were queried about their level of skin cancer knowledge, seven subjects reported no skin cancer knowledge whereas three subjects were able to describe up to two abnormal mole features. The majority (80%) of the tat-too artists finished an apprenticeship whereas two (20%) were trained by mentors. No tattoo artist received a formal educa-tion on skin cancer prevention; however, all tattoo artists were willing to undergo skin cancer prevention training. Most tattoo artists were willing to learn more about primary (90%) and sec-ondary skin cancer prevention (100%).
Lack of Sun Protection Knowledge Among Hispanic Tattoo ArtistsAlthough no Hispanic tattoo artist reported any formal education about skin cancer prevention, all artists further acknowledged no form of sun safety training during their tattoo apprentice-ship. When queried about basic sun protection, the majority could not describe a specific Sun Protection Factor (SPF) rec-ommendation, how to properly apply sunscreen, when to reapply sunscreen, and the importance of protective clothing. Furthermore, only one tattoo artist practiced safe sun protection consistently whereas five tattoo artists rarely applied sunscreen, two tattoo artists never used sunscreen, and two did not men-tion their sun protective habits. One artist reported the use of a wide-brimmed hat during the summer to protect his face, ears, and neck from the sun. Only one artist mentioned seeking shade and use of protective clothing during the summer time to pro-tect his skin from the sun.
Need for a Stronger Connection Between the Medical and Tat-too Artist CommunityFive Hispanic tattoo artists expressed curiosity throughout the interview by asking general questions about tattoo aftercare
implement skin cancer prevention in their daily routines. We describe themes and sub-themes generated by semi-structured interviews from Hispanic tattoo artists including skin cancer knowledge, aftercare instructions, social media, and other themes influencing skin cancer prevention.
METHODSRecruitment and Participant SelectionLicensed tattoo studios in Salt Lake County were identified through Yelp and Google. Studios were contacted by telephone, social media, email, or in person and queried about any working Hispanic/Latino tattoo artists. Participants were eligible if they were 18 years or older, tattoo artist from a licensed studio, and identified as Hispanic or Latino. Ten Hispanic tattoo artists from Salt Lake County agreed to participate in an in-depth interview. At this time, we reached data collection saturation, meaning that additional interviews did not provide any more sub-themes. Six tattoo artists were recruited through social media and four tat-too artists were recruited in person.
Interviews were conducted between November 2018 to Febru-ary 2019. Written informed consent was obtained from all tattoo artists before the interview. All tattoo artists were interviewed in person and audio recorded. The consent form also contained demographic questions (See Supplemental Figure 1). Each art-ist was awarded a $50 Amazon e-gift card for participation. The Western Institutional Review Board (IRB) declared the study as IRB exempt.
Data CollectionThe investigator conducted in-depth semi-structured interviews with a set of predetermined questions; to help standardize data collection during the interview (See Supplemental Figure 2). However, open ended questions were used to allow the tattoo artist to independently introduce and discuss new topics/issues. The interviewer and tattoo artist either spoke English, Spanish, or both. Interviews lasted between 30 to 60 minutes and were conducted by CG (first author). The interviewer queried on six pre-specified categories— demographics, tattoo training and experience, skin cancer knowledge, aftercare instructions, social media use, and willingness to learn about primary and second-ary skin cancer prevention. Sub-themes were identified using a grounded, data led approach (see below in data analysis).
Data AnalysisUnblinded subject responses were transcribed into an excel sheet and manually coded by the first author. Blinded/anony-mized subject responses were independently transcribed and coded separately by a third-party. A third-party associate was used to code the data as a mean to avoid bias and verify data ac-curacy and completeness. Coding discrepancies were resolved by discussion and re-listened audio recordings. A thematic analysis identified recurrent sub-themes from the transcript.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1239
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
C.D. Gonzalez, A.Pona, B.J. Walkosz, R.P. Dellavalle
TABLE 1.
Demographic Information of Tattoo Artists (n=10) and Description of Clientele
Variable Summary
Sex, n (%)
Male 9 (90)
Female 1 (10)
Age, in years
Mean (SD) 30 (5)
Min/Max 24/37
Hispanic or Latino heritage, n (%)a
Mexican 7 (70)
South American (Venezuelan) 1 (10)
Central American (El Salvador) 1 (10)
Spanish (from Spain) 1 (10)
Race, n (%)
American Indian/Alaska native 0 (0)
Asian 0 (0)
Black/African American 0 (0)
Native Hawaiian/Other Pacific islander 0 (0)
White 2 (20)
I choose not to answer 5 (50)
Other 1 (10)
Left blank intentionally 2 (20)
US born vs non-US born, n (%)
US born 6 (60)
Non-US born 4 (40)
Bilingual, n (%)
English only 1 (0)
Spanish only 0 (0)
English and Spanish 9 (90)
Fluency, n (%)
Fully bilingual 6 (60)
Understands some Spanish and can say some words in Spanish
1 (10)
Understands some Spanish but can’t speak it 2 (20)
No Spanish at all 1 (10)
Percent of repeat clients
Mean (SD) 73% (13)
Min/Max 50/90
Percent of Hispanic clients
Mean (SD) 51% (25)
Min/Max 25/93
Skin cancer knowledge
Knew 2 or less features of abnormal mole 3 (30)
Nothing at all 7 (70)
aNo Puerto Ricans, Dominicans, or Cubans
instructions including proper wound healing instructions and sunscreen information (how often to reapply, best sunscreen brand, recommended SPF). No tattoo artist referred their client to a healthcare provider in regard to an abnormal mole; how-ever, four tattoo artists reported referring a client to a healthcare provider due to acne (10%), skin infection (10%), allergic reac-tion (10%), warts (10%), and tattoo-related complication (10%). Only one artist (10%) knew of a doctor that he could consult for general inquiries. Two tattoo artists were interested in knowing a local tattoo laser removal technician or physician to refer their clients that wanted either complete tattoo removal or lighten-ing of their tattoo for cover ups. If a mole was located where the tattoo would be placed, the tattoo artists would either tattoo over the mole (10%), around the mole (20%), or would stay away from the mole (70%). All tattoo artists felt comfortable tattooing over freckles.
Aftercare InstructionsAll Hispanic tattoo artists recommended some form of sun protection in their aftercare instructions (Table 2). However, six tattoo artists provided verbal aftercare instructions only whereas four tattoo artists provided both written and verbal aftercare in-structions. All tattoo artist specified that their recommended sun protection advice was for the actual tattoo and not the rest of the skin. Most tattoo artists (70%) recommended long-term sun protection advice to the tattooed skin, mainly to preserve the ink density and vibrant colors. Recommended sun protection behaviors implemented into the tattoo artist’s aftercare instruc-tions included sun avoidance (100%), sunscreen use (80%), and protective clothing (50%). Of the eight tattoo artists that recommend sunscreen use in their aftercare instructions, none recommended a specific SPF and five tattoo artists mentioned “the higher the SPF, the better.” No tattoo artist recommended reapplying sunscreen every 2 hours or the use of hats to protect tattoos on the head and neck in their aftercare instructions.
Need for Culturally Sensitive Approach to Aftercare InstructionsOnly one Hispanic tattoo artist provided written aftercare in-structions in Spanish upon client request. Six tattoo artists provide verbal aftercare instruction in Spanish to their Spanish speaking only clients. However, all tattoo artists agreed that pro-viding Spanish aftercare instructions was a great idea. Despite all tattoo artists having a large portion of Hispanic clientele, all tattoo studio websites and social media pages were in English only. Although home remedies are a common type of alterna-tive medicine used by Hispanics, no tattoo artist inquired if their client would use a home remedy for wound care. In addi-tion, only three artists inquired about their client’s occupation prior to tattooing. Eight tattoo artists reported having clients that were Latino men that worked in construction, roofing, and other outdoor blue-collar occupations. Tattoo artists often do not recommend sunscreen to these clients since many of them consider creams, lotions, and sunscreen feminine. Instead of
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1240
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
C.D. Gonzalez, A.Pona, B.J. Walkosz, R.P. Dellavalle
recommending sunscreen, tattoo artists recommended seeking shade and wearing loose-fitting protective clothing as the pri-mary sun safety practices in Latino men that worked outdoors in a blue-collar occupation.
Need for Tougher Tattoo Artist Regulations Although three Hispanic tattoo artists did not talk about tattoo regulations, all tattoo artists who mentioned tattoo regulations during their interview recommended more strict regulations on obtaining a tattoo license in Utah. All of them recommended
formal primary and secondary skin cancer education during an apprenticeship or pre-requisite to obtaining a license to tattoo. They also mentioned the need to standardize sun safety in-formation in aftercare instructions. However, all of them were unsure about standardizing wound care in the aftercare instruc-tions.
Social Media UseAll Hispanic tattoo artists used social media (Facebook [100%]; Instagram [100%]; Twitter [10%]; Snapchat [50%]; Pinterest [10%]; YouTube [20%]) and each tattoo studio associated with the tattoo artist had both Facebook (100%) and Instagram (100%) (Table 3). Tattoo artists reported that a majority of their clients followed them on social media after their tattoo. Most tattoo artists agree that their Hispanic clients follow them on Facebook more than all other social media platforms. Six tattoo
TABLE 3.
Social Media Use
VariableSum-
mary, n (%)
Do you use social media?
Yes 10 (100)
No 0 (0)
Types of social media (personal account)
Facebook 10 (100)
Instagram 10 (100)
Twitter 1 (10)
Snapchat 5 (50)
Pinterest 1 (10)
YouTube 2 (20)
Studio website with short-term sun protection advice
Yes 3 (30)
No 3 (30)
No tattoo studio website 4 (40)
Tattoo studio with social media page
Facebook 10 (100)
Instagram 10 (100)
Are you willing to post sun safety information on your social media profile?
Yes 10 (100)
No 0 (0)
Willing to learn more about sun protection? (Primary skin cancer preven-tion)
Yes 9 (100)
No 1 (10)
Willing to learn more about skin cancer detection? (Secondary skin cancer prevention)
Yes 10 (100)
No 0 (0)
TABLE 2.
Sun Protection Information in Aftercare Instructions
VariableSummary,
n (%)
Provide any sun protection advice with aftercare instructions?
Yes 10 (100)
No 0 (0)
Verbal, written, or both?
Written only 0 (0)
Verbal only 6 (60)
Both 4 (40)
Full-body sun recommendations or just tattoo?
Full body 0 (0)
Tattoo only 10 (100)
Long or short-term sun safety advice?
Long-term 7 (70)
Short-term 2 (10)
Does not specify 1 (40)
Recommend keeping tattoo away from the sun?
Yes 10 (100)
No 0 (0)
Recommend sunscreen?
Yes 8 (80)
No 1 (10)
Only if client asks 1 (10)
Recommend a specific Sun Protection Factor (SPF)?
Yes 0 (0)
No 4 (40)
Recommends a “high SPF” 5 (50)
Not applicable (doesn’t recommend sun screen) 1 (10)
Protective clothing? 9 (90)
Yes 5 (50)
No 4 (40)
Not consistently 1 (10)
Recommends reapplication of sunscreen every 2 hours while in the sun?
Yes 0 (0)
No 9 (90)
Not applicable (does not recommend sun screen) 1 (10)
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1241
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
C.D. Gonzalez, A.Pona, B.J. Walkosz, R.P. Dellavalle
artists affiliated with a tattoo studio had a website; of those six tattoo studio websites, only three provided short-term ultravio-let (UV) protection advice (stay out of sun for two weeks and no tanning). None provided long-term UV protection advice. All tattoo artists were willing to distribute sun protective informa-tion on their personal and tattoo studio social media accounts.
OtherNinety percent of Hispanic tattoo artists felt emotionally in-vested in their clients. Although no tattoo artist recommended sun protection involving the client’s whole body, all tattoo art-ists concur that tattoo artists could influence skin cancer safety in young adults by providing full-body sun protection in their aftercare instruction. Furthermore, all tattoo artists agreed that providing aftercare instructions in Spanish is a great idea.
DISCUSSIONAlthough Hispanics do not constitute the majority of melanoma and NMSC cases in the U.S., Hispanics are more likely to be diagnosed with advanced malignant melanoma and NMSC.12,13
Furthermore, Hispanics diagnosed with melanoma have a low-er 5-year survival rate than Whites.14-16 Factors that influence an increased risk of melanoma in Hispanics include a high preva-lence of outdoor occupation, low socioeconomic status, and inadequate awareness.17,18 Nonmedical professionals could im-prove melanoma and NMSC awareness in Hispanics by learning more about skin cancer prevention and implementing culturally sensitive sun protective behaviors in their aftercare instructions and social media.
All Hispanic tattoo artists in this study had inadequate skin cancer knowledge to recognize a suspicious lesion; however, all tattoo artists were willing to learn more about skin cancer prevention. Early suspicion and detection of a lesion could in-fluence overall survival. In a study comparing survival between Hispanics and non-Hispanics, 70% of Hispanic subjects diag-nosed with localized melanoma had greater overall survival than non-Hispanics diagnosed with melanoma (P<0.01).19 Fur-thermore, ultraviolet radiation plays a role in the development of melanoma and nonmelanoma skin cancer in Hispanics.20,21 Although other studies report White patients diagnosed with melanoma have decreased overall survival than Hispanic patients, Hispanic tattoo artists who undergo primary and sec-ondary skin cancer prevention training and educate their clients about the harmful effects of ultraviolet radiation could influence melanoma and NMSC clinical outcome in Hispanics.22-24 Many of the Hispanic tattoo artists in our study believed that primary and secondary skin cancer prevention should be included in ap-prenticeships or pre-requisite to obtaining a license to tattoo. Additionally, although it may seem that Hispanic tattoo artists only interact with a small group of Hispanic clients, 38% of all Hispanics have a tattoo; therefore, Hispanic tattoo artists may influence sun protective behaviors at a larger scale.25
Hispanic tattoo artists did not provide effective sun protective behaviors in their aftercare instructions. Additionally, the ma-jority of Hispanic tattoo artists practiced suboptimal sun safety which may have influenced their sun safety advice to their cli-ents. Sun protective behaviors including avoidance of excessive sun exposure, applying sunscreen and sun protective clothing, and performing regular skin exams are essential for early mela-noma and NMSC detection.26 Such sun protective behaviors may be simple measures for tattoo artists to apply in their aftercare instructions. It should be emphasized that full-body, compre-hensive skin cancer prevention recommendations (applying sunscreen prior to UV exposure, reapplying it when outdoors for over 2 hours, using protective clothing that physically blocks UV, wearing wide-brimmed hats that shade the head, or seeking shade when available) should be compatible with current rec-ommendations to protect new tattoos. Furthermore, failing to implement a cultural approach to Hispanic clientele could jeop-ardize effective communication between the tattoo artist and the client. Multiple studies conclude that a culturally sensitive approach in Latinos could improve melanoma and NMSC edu-cation.27-29 Additionally, 90% of Latinos aged 18 to 49 seek health information through the internet and social media.30,31 Howev-er, most minorities feel that health information on the web is not tailored towards various ethnic/cultural groups.32 Providing Hispanic tattoo artists with guideline recommendations on sun protective behaviors in a culturally sensitive approach may con-vey information to Hispanic clients more effectively.
Since all Hispanic tattoo artists in our study possess a social media account, they have the opportunity to convey their sun protective behaviors more effectively. Social media may influ-ence sun protective behaviors by improving user attention and accountability.33,34 A randomized control trial stratifying 604 His-panic and non-Hispanic adult subjects into either a mobile app group that provided sun protective information or control group reported an improvement in shade use ([mean days] 41.0% vs 33.7%; P=0.03), mean total sunburns (0.60 vs 0.62; P=0.87), sun exposure (60.4% vs 49.3%; P=0.04), and all sun protective behaviors (39.4% vs 33.8%; P=0.04) in the mobile app group compared to control; however, less sunscreen was used in the mobile app group than the control group, respectively (28.6% vs 34.5%; P=0.48).35 Further studies are needed to distinguish the benefit of tattoo artists providing sun protective behaviors through social media.
Small sample size, a young age group, and local recruitment (Salt Lake County) may jeopardize our data’s external validity. Since all interviewed subjects were young, our data underrep-resented older Hispanic tattoo artists. Furthermore, our young tattoo artists may influence our high rate of social media use by tattoo artists. In a study exploring Hispanic opinions of mela-noma education, many subjects believed melanoma education may be conveyed more effectively in the Hispanic community
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1242
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
C.D. Gonzalez, A.Pona, B.J. Walkosz, R.P. Dellavalle
through television and radio. Social media may not have been mentioned because 79.4% of the studies sample size were aged 41 to 60; however, internet use by older adults has increased and nearly doubled from 2013 to 2016.28,36 Therefore, our study may not completely represent older Hispanic tattoo artists and Hispanic clientele. Lastly, majority of Hispanic tattoo artists have a Mexican heritage; therefore, there is poor Hispanic diversity within the sample size.
CONCLUSIONHispanic tattoo artists could potentially improve melanoma and NMSC prevention and treatment outcomes by providing full-body, comprehensive skin cancer prevention in their aftercare instructions and social media. Tattoo artists providing their after-care instructions in a more culturally sensitive approach could convey their recommendations more clearly to Hispanic clients. Furthermore, Hispanic tattoo artists may feel more confident referring their clients with suspicious lesions for the possible diagnose of early melanoma and NMSCs.
DISCLOSUREThe authors have no conflicts. Funding source: Funding for this project was provided by the National Cancer Institute (Diversity Training Branch and NIH/NCI Center to Reduce Cancer Health Disparities): R01CA206569-03S1
REFERENCES1. National Cancer Institute. SEER stat fact sheets: melanoma of the skin. 2015;
https://seer.cancer.gov/statfacts/html/melan.html. Accessed April 5, 2019. 2. United States Cancer Statistics Working Group. U.S. Cancer Statistics Data
Visualization Tool, based on November 2017 submission data (1999-2015). 2017; https://gis.cdc.gov/cancer/USCS/DataViz.html. Accessed April 5, 2019.
3. Agbai ON, Buster K, Sanchez M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the pub-lic. J Am Acad Dermatol. 2014;70(4):748-762.
4. Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence Estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. popula-tion, 2012. JAMA Dermatol. 2015;151(10):1081-1086.
5. United States Census Bureau. Resident population of the United States by race from 2000 to 2017 (in millions). In: US Census Bureau; 2016.
6. Montague M, Borland R, Sinclair C. Slip! slop! slap! and sunsmart, 1980-2000: skin cancer control and 20 years of population-based campaigning. Health Educ Behav. 2001;28(3):290-305.
7. Kelly S, Miller LE, Ahn HY, Haley JE. Perceptions and portrayals of skin can-cer among cultural subgroups. ISRN Dermatol. 2014;2014:325281.
8. Loescher LJ, Howerter AL, Heslin KM, et al. A Survey of licensed massage therapists' perceptions of skin cancer prevention and detection activities. Int J Ther Massage Bodywork. 2018;11(4):4-10.
9. Bailey EE, Marghoob AA, Orengo IF, et al. Skin cancer knowledge, attitudes, and behaviors in the salon: a survey of working hair professionals in Hous-ton, Texas. Arch Dermatol. 2011;147(10):1159-1165.
10. Campbell SM, Louie-Gao Q, Hession ML, et al. Skin cancer education among massage therapists: a survey at the 2010 meeting of the American Massage Therapy Association. J Cancer Educ. 2013;28(1):158-164.
11. Mori WS, Peters KV, Ferris LK, Patton TJ. Tattoo Artists' Approach to Melano-cytic Nevi. JAMA Dermatol. 2017;153(4):328-330.
12. Hu S, Parmet Y, Allen G, et al. Disparity in melanoma: a trend analysis of melanoma incidence and stage at diagnosis among whites, Hispanics, and blacks in Florida. Arch Dermatol. 2009;145(12):1369-1374.
13. Perez MI. Skin cancer in Hispanics in the United States. J Drugs Dermatol. 2019;18(3):s117-120.
14. Reintgen DS, McCarty KM, Jr., et al. Malignant melanoma in black Ameri-can and white American populations. A comparative review. JAMA. 1982;248(15):1856-1859.
AUTHOR CORRESPONDENCE
Cristian Daniel Gonzalez MDE-mail:................……............. [email protected]
15. Wu XC, Eide MJ, King J, et al. Racial and ethnic variations in incidence and survival of cutaneous melanoma in the United States, 1999-2006. J Am Acad Dermatol. 2011;65(5 Suppl 1):S26-37.
16. Byrd KM, Wilson DC, Hoyler SS, Peck GL. Advanced presentation of mela-noma in African Americans. J Am Acad Dermatol. 2004;50(1):21-24; discus-sion 142-143.
17. LeBlanc WG, Vidal L, Kirsner RS, et al. Reported skin cancer screening of US adult workers. J Am Acad Dermatol. 2008;59(1):55-63.
18. Oliveria SA, Heneghan MK, Cushman LF, et al. Skin cancer screening by dermatologists, family practitioners, and internists: barriers and facilitating factors. Arch Dermatol. 2011;147(1):39-44.
19. Feun LG, Raub WA, Jr., Duncan RC, et al. Melanoma in a southeastern His-panic population. Cancer Detect Preven. 1994;18(2):145-152.
20. Hu S, Ma F, Collado-Mesa F, Kirsner RS. UV radiation, latitude, and melanoma in US Hispanics and blacks. Arch Dermatol. 2004;140(7):819-824.
21. McLeod MP, Ferris KM, Choudhary S, et al. Contralateral distribution of non-melanoma skin cancer between older Hispanic/Latino and non-Hispanic/non-Latino individuals. Br J Dermatol. 2013;168(1):65-73.
22. Cress RD, Holly EA. Incidence of cutaneous melanoma among non-Hispanic whites, Hispanics, Asians, and blacks: an analysis of california cancer regis-try data, 1988-93. Cancer causes & control : CCC. 1997;8(2):246-252.
23. Hu S, Soza-Vento RM, Parker DF, Kirsner RS. Comparison of stage at diagno-sis of melanoma among Hispanic, black, and white patients in Miami-Dade County, Florida. Arch Dermatol. 2006;142(6):704-708.
24. Black WC, Goldhahn RT, Jr., Wiggins C. Melanoma within a southwestern Hispanic population. Arch Dermatol. 1987;123(10):1331-1334.
25. Laumann AE, Derick AJ. Tattoos and body piercings in the United States: a national data set. J Am Acad Dermatol. 2006;55(3):413-421.
26. Kasparian NA, McLoone JK, Meiser B. Skin cancer-related prevention and screening behaviors: a review of the literature. J Behav Med. 2009;32(5):406-428.
27. Hernandez C, Kim H, Mauleon G, et al. A pilot program in collaboration with community centers to increase awareness and participation in skin cancer screening among Latinos in Chicago. J Cancer Educ. 2013;28(2):342-345.
28. Chung GY, Brown G, Gibson D. Increasing melanoma screening among Hispanic/Latino Americans: A community-based educational intervention. Health Educ Behav. 2015;42(5):627-632.
29. Gloster HM, Jr., Neal K. Skin cancer in skin of color. J Am Acad Dermatol. 2006;55(5):741-760; quiz 761-744.
30. Buchanan Lunsford N, Berktold J, Holman DM, et al. Skin cancer knowledge, awareness, beliefs and preventive behaviors among black and hispanic men and women. Preventive Medicine Reports. 2018;12:203-209.
31. Pew Researchn Center. Digital Divide Narrows for Latinos as More Spanish Speakers and Immigrants Go Online. 2016; http://assets.pewresearch.org/wp-content/uploads/sites/7/2016/07/PH_2016.07.21_Broadbank_Final.pdf. Accessed May 4, 2019.
32. Manganello JA, Gerstner G, Pergolino K, et al. Media and technology use among Hispanics/Latinos in New York: implications for health communica-tion programs. J Racial Ethn Health Disparities. 2016;3(3):508-517.
33. Suffoletto B, Callaway C, Kristan J, et al. Text-message-based drinking as-sessments and brief interventions for young adults discharged from the emergency department. Alcohol Clin Exp Res. 2012;36(3):552-560.
34. Noar SM, Harrington NG. eHealth Applications: Promising Strategies for Be-havior Change. Florence: Routledge Ltd; 2012.
35. Buller DB, Berwick M, Lantz K, et al. Smartphone mobile application deliver-ing personalized, real-time sun protection advice: a randomized clinical trial. JAMA Dermatol. 2015;151(5):497-504.
36. Stellar Transportation. Interesting New Statistics Reveal Elderly Internet Us-age is on the Rise. 2018; https://www.stellartransport.com/interesting-new-statistics-reveal-elderly-internet-usage-rise/. Accessed May 5, 2019.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1243
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
C.D. Gonzalez, A.Pona, B.J. Walkosz, R.P. Dellavalle
SUPPLEMENT FIGURE 2. Survey questions.
3
14. Have you ever referred any of your patients to see a doctor? Dermatologist? If so, how come?
15. Do you know how to identify skin cancer? (If yes - What characteristics or identifiers do you look for to suspect someone has a skin cancer? If no – Would you be interested in learning what to look for?)
Sunburns & Aftercare
16. How do you provide aftercare information to your clients? For example, written, verbal, internet?
17. Do you provide aftercare information in English, Spanish, or both?
18. Does your aftercare include sun safety? What kind? (Tattoos only or full body?) Do you recommend short-term sun protection or long-term (lifelong) sun protection?
19. Specifics of sun safety in aftercare instructions? Recommend specific SPF? Reapply every 2 hours? Protective clothing?
20. Do you feel like your clients would listen to your recommendations on sun protection? If not, how come?
21. Does sun exposure make a huge difference in the quality of the tattoo? In other words, does keeping your tattoo from the sun prevent fading and breakdown of the tattoo?
22. Do you ever notice if your clients have been sunburned or if their skin has been overexposed to the sun? If so, what do you say?
Social media use and reaching out to Latinos
23. Do you use social media? If so, what kind?
24. Do you feel like many of your clients follow you on social media after getting their tattoo?
25. Do you ever post sun protection information on social media?
26. Are you interested in learning more about primary (learning more about sun protection) and secondary skin cancer prevention (learning how to detect abnormal moles)?
27. Are you willing to post sun protection information on social media?
28. What are some effective strategies that we can use to promote sun protections and skin cancer prevention in Latinos?
29. Would your studio use posters to promote skin cancer prevention?
2 Supplemental Figure 2. Survey questions.
Artist Interview Questions
Intro: Thank you for agreeing to participate in this interview for the Sun Safety Ink! program. This interview is designed to help us learn how to best develop a full body skin protection training for artists in tattoo studios. We consider sun safety as full body skin protection from ultra violet rays by using sunscreen, reapplication, wide brimmed hats, cover up clothing, sunglasses, seeking shade and monitoring the UV index. Your answers are voluntary and will be kept confidential and reported with the responses of other participants. This interview will be audio-recorded. By answering these questions, you are giving permission for us to use your responses in this research project. This study is being conducted with funding from National Institutes of Health by Klein Buendel, Inc., Northwestern University, Harvard School of Public Health, Denver VA Medical Center and Alliance of Professional Tattoo Artist’s. If you have any questions about the study, please contact Dr. Barbara Walkosz at 303-565-4356.
We are developing a skin cancer prevention training for tattoo artists so that they can inform their clients about ways to protect themselves from harmful UV radiation by recommending full body sun protection.
Demographics
1. How old are you?
2. Where were you born?
3. Where were you raised?
4. What is your Hispanic/Latino heritage? You may select more than one group. o Mexican o Puerto Rican o Dominican o Cuban o Central American (please specify: ___________________) o South American (please specify: _____________________) o Spanish (from Spain) o I choose not to answer
5. Do you speak English, Spanish or both? Tattoo Experience
6. How did you get into tattooing?
7. How long have you been tattooing for?
8. Do you specialize in any Latino specific tattoo styles (ex. Chicano) or any other specific tattoo styles?
If so, please describe your style?
9. What percent of your clients are Latino?
10. Do you have a lot of repeat clients? Y or N. What percent of your clients are repeat clients?
11. What are some of reasons why Latinos get tattoos?
Skin Cancer Knowledge
12. What do you know about skin cancer? (Probe. Ex: Do you know the difference between Non Melanoma and Melanoma skin cancers?)
13. Have you seen a new lump or bump on a tattoo? If so, were you concerned?
2 Supplemental Figure 2. Survey questions.
Artist Interview Questions
Intro: Thank you for agreeing to participate in this interview for the Sun Safety Ink! program. This interview is designed to help us learn how to best develop a full body skin protection training for artists in tattoo studios. We consider sun safety as full body skin protection from ultra violet rays by using sunscreen, reapplication, wide brimmed hats, cover up clothing, sunglasses, seeking shade and monitoring the UV index. Your answers are voluntary and will be kept confidential and reported with the responses of other participants. This interview will be audio-recorded. By answering these questions, you are giving permission for us to use your responses in this research project. This study is being conducted with funding from National Institutes of Health by Klein Buendel, Inc., Northwestern University, Harvard School of Public Health, Denver VA Medical Center and Alliance of Professional Tattoo Artist’s. If you have any questions about the study, please contact Dr. Barbara Walkosz at 303-565-4356.
We are developing a skin cancer prevention training for tattoo artists so that they can inform their clients about ways to protect themselves from harmful UV radiation by recommending full body sun protection.
Demographics
1. How old are you?
2. Where were you born?
3. Where were you raised?
4. What is your Hispanic/Latino heritage? You may select more than one group. o Mexican o Puerto Rican o Dominican o Cuban o Central American (please specify: ___________________) o South American (please specify: _____________________) o Spanish (from Spain) o I choose not to answer
5. Do you speak English, Spanish or both? Tattoo Experience
6. How did you get into tattooing?
7. How long have you been tattooing for?
8. Do you specialize in any Latino specific tattoo styles (ex. Chicano) or any other specific tattoo styles?
If so, please describe your style?
9. What percent of your clients are Latino?
10. Do you have a lot of repeat clients? Y or N. What percent of your clients are repeat clients?
11. What are some of reasons why Latinos get tattoos?
Skin Cancer Knowledge
12. What do you know about skin cancer? (Probe. Ex: Do you know the difference between Non Melanoma and Melanoma skin cancers?)
13. Have you seen a new lump or bump on a tattoo? If so, were you concerned?
SUPPLEMENT FIGURE 1. Consent form.
1 Supplemental Figure 1. Consent form.
Sun Safety Ink! Consent and Demographic Information Thank you for agreeing to participate in this interview for the Sun Safety Ink! program. We are conducting these interviews with tattoo artist are at least 18 years old. We consider sun safety full body skin protection from ultraviolet rays by using sunscreen, reapplication, wide brimmed hats, cover up clothing, sunglasses, seeking shade and monitoring the UV index. Your answers are voluntary, confidential, and anonymous, and will be combined with the answers of all participants. Your interview will be audio-recorded (with your permission). By answering these questions, you are giving permission for us to use your responses in this research project. This study is being conducted with funding from National Institutes of Health by Klein Buendel, Inc. and the Denver VA Medical Center. If you have any questions about the study, please contact Dr. Cristian Gonzalez at 864-386-3771 or Dr. Barbara Walkosz at 303-565-4356.
Demographic Information:
1. Are you Hispanic or Latino?
� Yes � No � I choose not to answer
2. Which of the following groups best describe your race? You may select more than one group.
� American Indian / Alaskan Native � Asian � Black / African American � Native Hawaiian / Pacific Islander � White � I choose not to answer
3. Are you male or female?
� Male � Female � I choose not to answer
Signature of Participant:______________________________________________ Signature of Staff:___________________________________________________
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1244 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Dietary Lycopene Protects SKH-1 Mice Against Ultraviolet B-Induced Photocarcinogenesis
Karen E. Burke MD PhD,ª Xueyan Zhou MD MS,a,b Yongyin Wang PhD,a,c and Huachen Wei MD PhDa,d
aDepartment of Dermatology, Icahn School of Medicine at Mount Sinai, New York, NYBDepartment of Internal Medicine, Gerontology and Geriatric Medicine,Wake Forest University School of Medicine, Winston-Salem, NC
cMedtronic Diabetes MiniMed, Northridge, CA dDepartment of Dermatology, No.1 Hospital, China Medical University, Shengyang, China
Lycopene, an acyclic hydrocarbon, non-provitamin A carotenoid, is a potent antioxidant with well-documented anticancer properties. In this study, we investigated the effects of dietary lycopene on sub-acute and chronic ultraviolet B (UVB)-induced skin carcinogenesis in SKH-1 mice. Groups of three mice were fed with a nonsupplemented or 1% lycopene diet for two weeks before and throughout two weeks of UVB irradiation (30 mJ/cm2 UVB, thrice weekly). The lycopene diet significantly reduced the formation of pyrimidine dimers (PDs) and the expression of proliferative cellular nuclear antigen (PCNA) in UVB-irradiated skin. Then groups of eighteen mice were each fed with control diet or with a 0.25% or 1% (w/w) lycopene-supplemented diet for 40 weeks, beginning one week before UVB irradiation (30 mJ/cm2 UVB, thrice weekly for 23 weeks) and continuing after termination of UVB. Lycopene significantly inhibited the onset and decreased the incidence, multiplicity, and tumor weights of UVB-induced skin tumors. UVB-induced epidermal hyperplasia and PCNA expression were still remarkably inhibited by dietary lycopene, even up to 40 weeks. No significant difference in protection was detected between the low and high concentrations of lycopene. These results demonstrate that dietary lycopene does protect against UVB-induced epidermal hyperplasia and carcinogenesis.
J Drugs Dermatol. 2019;18(12):1244-1254.
ABSTRACT
INTRODUCTION
By far, the most common human malignancy is skin can-cer. The incidence is increasing at an astonishing rate, with more than 5.4 million new cases of non-melanoma
skin cancer (NMSC) diagnosed each year in the United States1 that is 925 new skin cancers diagnosed each hour awake! The most common causative factor is excessive exposure to sun-light, which cannot be avoided with our daily occupational and recreational activities. The rapid rise is enhanced not only by increased travel with vacations in sunny environments, but also by an increase in high risk groups, such as immunocompro-mised organ transplant patients.2-4 The most directly carcino-genic spectrum of sunlight is ultraviolet B (UVB) radiation,5 both a tumor initiator and promoter.6-8 Generation of reactive oxy-gen species (ROS) by UVB exposure not only induces oxidative DNA damage, leading to not only tumor initiation,9 but also to activation of many growth factors and signal transduction cascades including those involved in tumor promotion, such as tyrosine protein kinase (TPK) and mitogen activating protein (MAP) kinase pathways.10-12 UVB-induced inflammation and im-munosuppression further contribute to photocarcinogenesis.11 Therefore, topical or systemic supplementation by antioxidants may protect skin against UVB-induced photodamage and car-cinogenesis.13
With current emphasis on preventative medicine and healthy eating, recent research for new anticancer drugs focuses more on natural nutrients from the regular human diet. These com-pounds rarely cause adverse side effects, and they act on a wide range of molecular targets involved in carcinogenesis. Lycopene is a carotenoid found in tomatoes and other red-col-ored fruits and vegetables.14 This powerful dietary antioxidant has received considerable attention in recent years. A potent scavenger of oxygen radicals, lycopene has the highest singlet oxygen quenching ability when compared to 31 other anti-oxidants.15-17 Numerous epidemiological, in vitro and animal studies provide convincing evidence that lycopene prevents a variety of cancers,18 including prostate,19-21 breast,22-24 cervical,25
gastric,26 colon,27 lung,28,29 liver,30,31 bladder,32 and renal cell can-cers.33 Only recently have studies assessed whether lycopene has potential for prevention of skin cancer.34,35 Although the an-ticarcinogenic effects of lycopene are thought to be primarily due to its antioxidant properties,36 other mechanisms have also been demonstrated, such as enhancing the gap junctional com-munication (GJC),37 suppressing the growth factor receptor signaling,38,39 inducing the apoptosis of cancerous cells,34,40 reg-ulating the cell cycle.38,41 and stimulating the immune system.42
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1245
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
UVB SourceFor UVB radiation, a Daavlin phototherapy unit (Daavlin Com-pany, Bryan, OH) with eight UVB lamps (FS24T12-UVB-HO) (Voltare Company, Fairfield, CT) of predominant emitting peak at 280–320 nm was used. The intensity of UVB was calibrated every week with an IL-1700 Research Radiometer (International Light, Newburgport, MA). The distance between the UVB lamps and mouse dorsal skin was approximately 40 cm. This later se-lected UVB fluence (300 J/m2) is equivalent to approximately one hour exposure to sunlight in Central Park of New York City in summer.
UVB-Induced Photodamage and Photocarcinogenesis
1) Sub-acute Photodamage Two mice comprised each of the non-UVB irradiated controls: A) control diet, B) 1% lycopene diet. Three mice were in each of the UVB-irradiated groups: C) control diet, D) 1% lycopene diet. All mice were fed with control or lycopene diet for two weeks prior to UVB exposure. Then mice of groups C and D were irradiated with 30 mJ/cm2 UVB thrice weekly for two weeks. Twenty-four hours after the last UVB exposure, mice were sacrificed and ten skin biopsy specimens were collected from each group and fixed in formalin for immunohistochemical analyses.
2) Chronic Photocarcinogenesis Sixty mice were divided into six groups. Two mice comprised each non-UVB-irradiated group: (A) control diet, (B) 0.25% lyco-pene diet, and (C) 1% lycopene diet. Eighteen mice were in each UVB-irradiated group: (D) control diet (control/UVB), (E) 0.25% lycopene diet (Lo.Ly/UVB), and (F) 1% lycopene diet (Hi.Ly/UVB). All mice were pre-fed with their respective diets for one week prior to UVB exposure. Then mice in groups D, E and F were irradiated with 30 mJ/cm2 UVB thrice weekly until the tumor incidence of the control/UVB group reached 50% (at 23 weeks); mice were maintained until 40 weeks (eight weeks after the tu-mor incidence reached 100% in the control/UVB group).
Tumors approximately >1 mm and <2 mm in size were counted only if they were present for at least one week; tumors >2 mm were counted as soon as they were observed. The numbers and sizes of tumors on each mouse were documented once per week. When mice were sacrificed at the end of study, tumors from each mouse were excised and weighed; tumors and dorsal skin specimens were fixed in formalin for immunohistochemi-cal analyses. Ten skin biopsy specimens were taken from each group and fixed in formalin for immunohistochemcial analyses.
Immunohistochemical Staining for PCNAIn order to examine the effect of sub-acute or chronic UVB exposure on cellular proliferation, skin specimens from each experimental group were stained for PCNA and five consecu-tive fields were randomly selected from the epidermis of each
Until recently, evidence as to whether lycopene protects against UVB-induced skin cancer was lacking.13 In a human intervention trial, a decrease in the photosensitivity towards UV-induced erythema was observed in volunteers following ingestion of lycopene or tomato-derived products rich in lycopene.43 Pre-vious research in our laboratory demonstrated that topical application of lycopene to dorsal skin of SKH-1 mice inhibits UVB-induced photodamage in a dose-dependent manner, as measured by a decrease in the inflammatory response and in the activity of ornithine decarboxylase (ODC) (an enzyme asso-ciated with tumor promotion).44 In addition, topical application of lycopene maintains normal levels of epidermal proliferating cell nuclear antigen (PCNA) upon UVB exposure (thus protect-ing against the UVB-induced decrease in PCNA).44 The purpose of this study is to investigate possible protection by dietary lycopene from sub-acute and chronic UVB-induced photocar-cinogenesis in SKH-1 hairless mice.
MATERIALS AND METHODSChemicalLycopene was purchased from Chemos GmbH (Regenstauf, Germany) with a purity of 95.2%. PCNA and anti-thymine di-mer antibodies were purchased from Santa Cruz Biotechnology (Santa Cruz, CA) and Affitech (Walnut Creek, CA), respectively.
AnimalsFemale SKH-1 hairless and immunocompetent mice, (6–7 weeks old, 20-23 gm), were purchased from Charles River Laboratories (Wilmington, MA). Mice were housed (two to six mice per cage) at the Mount Sinai Animal Facility under standard conditions (12 h light–dark cycle, humidity 50 ±15%, temperature 22 ± 2°C, and 12 air changes per hour). This research project was approved by the Mount Sinai School of Medicine, and the animal care was in accordance with the institutional guidelines of the Animal Care Facility of Mount Sinai Medical Center, New York. The mice were pathogen free, as confirmed by bacteriology and parasitology. The mice were acclimated for two weeks upon arrival before experimentation. Diets and water were provided ad libitum.
DietsAll diets were prepared commercially by Purina Mills’ Test Diet Company (Richmond, IN). AIN-76A diet was used as the base diet and contained no lycopene by itself. Lycopene was mixed into this AIN-76A base diet to produce 0.25 and 1% (w/w) lyco-pene diets, respectively. These concentrations of lycopene were selected because a previous study in rats consuming up to 1% dietary lycopene levels for 90 days did not show any toxicity.45 All diets were aliquoted by weekly-consuming amount, sealed and stored at -20°C upon arrival. Body weight and dietary con-sumption were recorded weekly throughout the experiment. The mean body weight and average dietary consumption per gram of mouse body weight per day were calculated weekly throughout the experiment.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1246
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
mice from each non-UV-irradiated group to check for any toxic-ity, particularly that of the liver and spleen.
Statistical AnalysisAll statistical analyses of data were performed with SAS soft-ware (SAS 9.1 for Windows by SAS Institute Inc., Cary, NC). The tumor incidence was compared by chi-square analysis. The treat-ment effects of lycopene on tumor multiplicity, tumor weight, tumor latency, body weight, diet consumption, immunostaining of biomarkers and epidermal thickness were analyzed with t-test after normality test. A P value less than 0.05 was considered statistically significant.
RESULTSEffects of Dietary Lycopene on Food Consumption and Body WeightMean water and food consumption as well as body weights did not show any significant differences between the groups throughout the experiment. There were no statistically significant differences between control and either of the lycopene-contain-ing diets or between non UV-irradiated and UV-irradiated mice. The mean daily dietary consumption was 0.140 and 0.155 gm food/gm body weight initially and at 5 weeks, respectively. This daily consumption decreased to 0.120 gm feed/gm body weight in all groups, starting at week 10 and continuing until the termi-nation of the experiment at 40 weeks. The mean body weight was 25.7 ± 0.8 gm/mouse initially at week 0 and 28.6 ± 0.9 gm/mouse by weeks 30-40.
No systemic toxicity for either concentration of lycopene in SKH-1 mice was observed. Autopsy and histologic examination (with particular attention to the liver and spleen) revealed no systemic toxicity in any of the treatment groups.
Inhibition by Lycopene on Sub-Acute UVB-Induced Epidermal PCNA PCNA is an excellent biomarker for cell proliferation, and over-expression of PCNA is associated with tumor promotion.48 UVB exposure led to a marked increase of PCNA staining (29±4 positive cells/field) in mouse epidermis compared with the unexposed control (20±2.4 positive cells/field;P<0.05), Figure 1 shows that supplementation with 1% lycopene significantly reduced the number of PCNA-positive cells to the normal level (21±3.0 positive cells/field; P<0.05). Thus lycopene suppressed PCNA expression as early as within the first two weeks of UVB exposure (Figure 1).
Inhibition by Lycopene on Sub-Acute UVB-Induced Epidermal PD Cyclobutane pyrimidine dimers (CPDs) and “6-4” photoproducts (6-4 PPs) are specific types of DNA damage induced by UVB, which can lead to tumor initiation if not efficiently repaired.49
Sub-acute exposure to UVB irradiation significantly induced the formation of PD’s in mouse epidermis 24 hours after the last
specimen for quantitative analysis. The expression of PCNA was determined using the avidin-biotin complex immunoper-oxidase technique as described previously.46,47 Briefly, slides with paraffin-embedded tissue sections were deparaffinized in xylene, dehydrated in graded ethanol and then treated with 1% non-fat milk for 30 minutes to avoid non-specific binding. Fol-lowing three rinses in PBS, sections were incubated with PCNA antibody overnight at 4°C and then blocked with 10% normal goat serum in PBS for 40 minutes. Skin sections were placed in 0.3% hydrogen peroxide for 30 minutes to block endogenous peroxidases. The sections were then incubated with biotinylated anti-rabbit (dilution 1:200) for 30 minutes and the avidin–biotin complex (Vector, Burlingame, CA) for 40 minutes. The color was developed with 3-amino-9-ethylcarbozole (Vector, Burlingame, CA), and the samples were counter stained with methyl green. Finally, digital micrographs were taken and the epidermal layer of skin was examined. Five consecutive fields were randomly selected from each skin sample. The positively stained cells from each field were counted by two investigators independently and averaged as the representative number of each skin specimen.
Immunohistochemical Staining for PDThe assay for pyrimidine dimer (PD) was described in our previ-ous publication.47 Briefly, slides with paraffin-embedded tissue sections were heated for 30 minutes at 65°C and allowed to cool at room temperature for 20 minutes before deparaffiniza-tion and rehydration. Slides were then treated with proteinase K (Roche, Nutley, NJ) for 40 minutes, RNase A (Qiagen, Valen-cia, CA) for one hour, 4 N hydrochloric acid for 7 minutes to denature DNA and then neutralized by 50 mM Tris-base for 5 minutes at room temperature. Specimens were incubated for one hour with blocking reagent provided by M.O.M. kit (Vec-tor, Burlingame, CA) and then overnight with the anti-thymine dimers antibody at a 1:150 dilution. The sections were then incubated with biotinylated secondary antibody from M.O.M. kit (Vector, Burlingame, CA) for 15 minutes, followed by 3% hydrogen peroxide inactivation and the avidin-biotin complex (Vector, Burlingame, CA) incubation. The color was developed with 3-amino-9-ethylcarbozole (Vector, Burlingame, CA), and the samples were counter stained with methyl green. The PD positive cells were counted, photographed, and statistically an-alyzed as in PCNA analyses.
Evaluation of Epidermal ThicknessThe epidermal layer of skin was examined from the digital micrographs (200x) of the immunostaining slides. Five consec-utive fields were randomly selected from each skin specimen. The total area of epidermis from each field was quantified by Image J software (Wayne Rasband, National Institutes of Health, Washington, DC) and averaged as the representative index for epidermal thickness of each specimen.
AutopsyAutopsies and histologic examination were performed on two
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1247
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
UVB irradiation. As shown in Figure 2, UVB exposure resulted in 43±9 PD-positive epidermal cells/field as compared to 2±2 PD-positive epidermal cells/field in nonirradiated controls (P<0.01). Supplementation with 1% lycopene significantly decreased the number of post-UVB PD-positive cells by 30.2% to only 30±6 PD-positive epidermal cells/field (P<0.05). These results suggest that lycopene inhibits tumor initiation by UVB by reducing pho-todynamic DNA damage (Figure 2).
Inhibition by Lycopene on Chronic UVB-Induced Carcinogenesis No tumor was observed in any mouse not exposed to UVB. Skin tumors were induced in the mice exposed to UVB irradiation, and biopsies were taken of clinically representative tumors from each mouse in each UVB exposed group. These tumors were squamous cell carcinomas varying from well-differentiated to poorly-differentiated. The severity of atypia within each tumor was not quantified or documented. No benign papillomas per-sisted for more than one week, and no benign tumors were found upon terminal histologic examination.
FIGURE 2. Effect of dietary lycopene on sub-acute UVB-induced PD formation in the epidermis of SKH-1 mice. (A) Immunohistochemical staining of PD in the epidermis in (a) control group (no UVB), (b) control group (with UVB), (c) 1% lycopene group (no UVB), and (d) 1% lycopene (with UVB) (Lyco./UVB) group. (B) Quantitation of PD positive cells. Five consecutive fields were randomly selected from each of 10 skin biopsy specimens. The positively stained cells from each field were counted and averaged as representative number of each specimen. Data were expressed as the mean + SE obtained from the 10 specimens of each group. The statistical significance of difference between groups was calculated by TTEST; *P<0.01 (versus control group); **P<0.05 (versus control/UVB group).
FIGURE 1. Effect of dietary lycopene on sub-acute UVB-induced cell proliferation in the epidermis of SKH-1 mice. (A) Immunohistochemical staining of PCNA in the epidermis. PCNA-stained sections: from (a) control group (no UVB), (b) control group (with UVB) (control/UVB), (c) 1% lycopene group (no UVB) and (d) 1% lycopene (with UVB) (Lyco./UVB) group. (B) Quantitation of PCNA positive cells. Five consecutive fields were randomly selected from each of 10 skin biopsy specimens. The positively stained cells form each field were counted and averaged as representative number of each specimen. Data shown are mean + SE obtained from the 10 specimens of each group. The statistical significance of difference between groups was calculated by TTEST; *P<0.05 (versus control group); **P<0.05 (versus control/UVB group).
22
Figure 1
a b
c d
Aaa bb
cc dd
A
0
5
10
15
20
25
30
35
control control/UVB Lycopene Lyco./UVB
PC
NA
pos
itive
cel
ls p
er fi
eld *
**
B
0
5
10
15
20
25
30
35
control control/UVB Lycopene Lyco./UVB
PC
NA
pos
itive
cel
ls p
er fi
eld *
**
B
23
Figure 2
a b
c d
Aa b
c d
A
0
10
20
30
40
50
60
control control/UVB Lycopene Lyco./UVB
PD
pos
itive
cel
ls p
er fi
eld *
**
B
0
10
20
30
40
50
60
control control/UVB Lycopene Lyco./UVB
PD
pos
itive
cel
ls p
er fi
eld *
**
B
(A) (B)
22
Figure 1
a b
c d
Aaa bb
cc dd
A
0
5
10
15
20
25
30
35
control control/UVB Lycopene Lyco./UVB
PC
NA
pos
itive
cel
ls p
er fi
eld *
**
B
0
5
10
15
20
25
30
35
control control/UVB Lycopene Lyco./UVB
PC
NA
pos
itive
cel
ls p
er fi
eld *
**
B
(A) (B)
23
Figure 2
a b
c d
Aa b
c d
A
0
10
20
30
40
50
60
control control/UVB Lycopene Lyco./UVB
PD
pos
itive
cel
ls p
er fi
eld *
**
B
0
10
20
30
40
50
60
control control/UVB Lycopene Lyco./UVB
PD
pos
itive
cel
ls p
er fi
eld *
**
B
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1248
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
The dietary supplementation with lycopene significantly de-creased UVB-induced skin tumor incidence (the percentage of mice with one tumor or more; Figures 3A and C) and multi-plicity (the number of tumors/mouse; Figures 3B and D). Both low (0.25%) and high (1%) concentrations of lycopene supple-mentation showed a markedly decreased tumor incidence and multiplicity by 32 weeks. When the tumor (>1mm) incidence of the UVB-radiated mice on the non-supplemented control diet reached 50% (at 25 weeks) and 100% (at 32 weeks), the tumor (>1 mm) incidence in mice with 0.25% and 1% lycopene was only 27.8% and 33.3%, respectively, at 25 weeks, and 83.5% (P=0.033), and 88.9% (P=0.091), respectively, at 32 weeks (P=0.089;Figure 3A). Tumor (>1 mm) multiplicity was decreased by 42.0% (P =0.022) in 0.25% lycopene group and by 34.0% (P=0.055) in 1% lycopene group at week 32 (Figure 3B). Dietary supplementa-tion with 0.25% lycopene significantly reduced the tumor (≥2 mm) incidence at week 28 by 100% (P=0.035), week 34 by 39.8% (P=0.036), week 38 by 24.7% (P=0.041), and week 40 by 17.0% (P=0.067), while 1% lycopene significantly reduced the tumor (≥2 mm) incidence at week 33 by 45.9% (P=0.046), week 34 by 33.8% (P=0.036), and week 40 by 22.0% (P=0.035; Figure 3C). Di-etary supplementation with 0.25% and 1% lycopene significantly reduced the tumor (>2 mm) multiplicity by 70.0% (P=0.006) and 60.0% (P=0.023) at week 32 (Figure 3D).
Often in experiments, exposing mice to UVB causes premature death of up to 50% of control, nonsupplemented animals by week 32-35, thus explaining the effect that the relative differ-ences in number of tumors between control and nutrient diets decreases with extended time (since deceased animals cannot acquire more cancers!). However, in the experiments presented here, no control mice died during the 40 week experiment, and only one mouse supplemented with 0.25% lycopene and one mouse supplemented with 1.0% lycopene died at the termina-tion of the experiment (at weeks 39 and 40, respectively). The fact that mice continue to develop tumors long after exposure to UVB irradiation demonstrates the importance of not terminating this type of experiment for at least 40 weeks.
Dietary lycopene also significantly prolonged tumor latency (ie, the time delay between the initiation of UVB exposure and the appearance of the first tumor) (Figure 4) and reduced tu-mor weight (Figure 5). The latency of tumor onset in mice on non-supplemented control diet (24.9 weeks) was prolonged by 2.8 (P=0.013) and 2.0 (P=0.058) weeks in the two supplemented (0.25% and 1%) lycopene groups, respectively (Figure 4).
Dietary lycopene also decreased the average size (ie, tumor load) of UVB-induced tumors (Figure 5). After sacrifice at 40 weeks, the average tumor weight of 0.552 gm/mouse in the con-trol diet was significantly higher than those mice on lycopene diets (0.258 gm/mouse (P=0.003) and 0.272 gm/mouse (P=0.018) for 0.25% and 1% lycopene, respectively). Thus with low and
high lycopene supplementation, the UVB-induced tumors were on an average only 52% and 49% the size, respectively, of tu-mors in non-supplemented mice.
Statistical analysis showed no significant difference between the two concentrations of lycopene in the supplemented diet groups with respect to tumor incidence, multiplicity, latency, and tumor weight. Thus the higher dose of 1% lycopene supple-mentation used in this study was no more effective than the lower dose of 0.25% lycopene supplementation in timing of tu-mor onset and degree of inhibition.
Our results indicate that dietary lycopene provides protection against UVB-induced photocarcinogenesis in SKH-1 mice, espe-cially at early stages.
Inhibition by Lycopene of Chronic UVB-induced Epidermal Hy-perplasiaLong-term UVB exposure causes epithelial hyperplastia which may play a critical role in tumor development.50,51 As seen clear-ly in Figure 6A and quantified in Figure 6B, epidermal thickness was increased after UVB irradiation compared with unexposed skin (P<0.00001). Dietary supplementation with 0.25% and 1% lycopene significantly decreased this UVB-induced epidermal hyperplasia by 26.6% (P<0.01) and 23.8% (P<0.05), respectively. There was no statistically significant difference between these two lycopene diets.
Inhibition by Lycopene of Chronic UVB-induced Epidermal PCNA The number of PCNA–positive cells per field in non-irradiated control epidermis was not statistically different from the num-ber in either of the non-irradiated lycopene diet groups (data not shown). As shown in Figure 6, chronic UVB exposure resulted in a strong PCNA-positive staining (50±10.5) in the epidermis compared with the unexposed controls (P<0.00001). Dietary supplementation with 0.25% and 1% lycopene significantly reduced the number of PCNA-positive cells per field in the epi-dermis to 33 ± 6.5 and 34 ± 5.4, respectively (P<0.01). Thus there was no statistically significant difference between low and high lycopene-supplemented UVB-irradiated mice. This observation that lycopene inhibits PCNA expression in epidermis sug-gests that one of the mechanisms of photoprotection against UVB-induced skin carcinogenesis is through anti-proliferative signaling.
Effects of Lycopene on Chronic UVB-induced Epidermal PD Ex-pression In the experiments presented here, there was no prominent PD staining in any samples from the chronically UVB-irradiated mice. Possibly efficient DNA repair occurred after termination of UVB treatment at 25 weeks.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1249
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
FIGURE 3. Effect of dietary lycopene on chronic UVB-induced carcinogenesis in SKH-1 mice. (A) and (B): Tumors of diameter >1 mm; (C) and (D): Tumors of diameter >2 mm; (A) and (C) tumor incidence (% mice with tumor); (B) and (D) tumor multiplicity (number of tumors/mouse). The number of tumors were recorded weekly throughout the experiment. The statistical significance of difference between control/UVB and lycopene/UVB groups was determined by chi square analysis (incidence data) or TTEST (multiplicity data). *P<0.05 (versus control/UVB group). **P<0.01 (versus control/UVB group); #0.05<P<0.1 (versus control/UVB group, close to significance).
24
Figure 3
(A) (B)
(C) (D)
FIGURE 4. Effect of dietary lycopene on the latency of onset of tumor formation in chronic UVB-induced carcinogenesis in SKH-1 mice. The time lags between the initial UVB irradiation and the appearance of the first tumor was recorded and compared using TTEST analysis. *P<0.05 (versus control/UVB group); #P=0.058 (versus, control/VUB group, close to significance).
FIGURE 5. Effect of dietary lycopene on tumor load of the UVB-induced carcinogenesis in SKH-1 mice. The average tumor weight (g) per mouse at the end of study was recorded and compared using TTEST analysis. *P<0.05 (versus control/UVB group); **P<0.01 (versus control/UVB group).
25
Figure 4
Figure 5
26
Figure 6
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1250
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
DISCUSSIONBecause lycopene has been recognized as the most effective singlet oxygen quencher among carotenicids15,52 and has been demonstrated to inhibit carcinogenesis by several different proven mechanisms, lycopene supplementation is currently being actively investigated, especially for prevention of UV-in-duced skin cancer. A particular advantage of lycopene for skin protection is that with dietary supplementation, the concentra-tion of lycopene increases more in the skin than in the blood, and the concentration decreases far more slowly in the skin than in the blood after supplementation is terminated.53 Thus, skin maintains a reservoir of protective lycopene.
Many in vitro and in vivo (mouse and human) studies have demonstrated protection from both acute and chronic UVA- and UVB-induced damage to the skin by lycopene, including prevention of skin cancer. Incubation of human dermal fibro-blasts in vitro with lycopene ameliorated UVA-induced cell death and restored UVA-induced downregulation of precolla-gen with a dose-dependent correlation.54 Lycopene treatment also prevented UVA-induced intracellular malondialdehyde (MDA) generation, matrix metalloproteinase I (MMP-1) upregu-lation, and activation of NFKβ. In other experiments, lycopene
decreased murine carcinogenesis both in vivo and in vitro by protecting cells from hydrogen-induced DNA damage and by decreasing mutations in codon 61 of the Ha-ras oncogene.55
In research similar to that reported here, male SKh-1 male mice supplemented with tangerine or red tomato powder for 35 weeks and exposed to UVB three times per week during weeks 11-20 had only 43% and 50%, respectively, of the number of tu-mors of nonsupplemented controls, though the female SKH-1 mice similarly supplemented were not significantly protected.56
Because compounds derived from tomato glycol-alkaloids, (such as tomatidine and hydroxylated-tomatidine) are sig-nificantly different in skin after tomato suppliementation, the authors suggest that these may be the compounds responsible for the decrease in tumor multiplicity in the male mice. Erdman
27
27
27
(B)
(C)
FIGURE 6. Effect of dietary lycopene on chronic UVB-induced epidermal hyperplasia and on cell proliferation and PCNA expression in the epidermis of SKH-1 mice. (A) Histology with immunohistochemical staining of PCNA in the epidermis. PCNA-stained sections: from (a) control group (no UVB), (b) control group (with UVB), (c) 0.25% lycopene (with UVB) (Lo.ly/UVB) group and (d) 1% lycopene (with UVB) (Hi.ly/UVB) group. (B) Quantitation of epidermal hyperplasia. Five consecutive fields were randomly selected from each of 10 skin biopsy specimens. The total area of epidermis from each field was quantified and averaged as representative index for epidermal thickness of each specimen. Data shown represent the relative epidermal thickness in arbitrary units, expressed as mean + SE obtained from the 10 randomly selected tissue biopsy specimens of each group. The statistical significance of difference between control/UVB-treated and all other groups was calculated by TTEST. *P<0.05 (versus control/UVB group); **P<0.01 (versus control/UVB group). ***P<0.000001 (versus control group). (C) Quantitation of PCNA positive cells. A total of five consecutive fields were randomly selected from each of 10 skin biopsy specimens. The positively stained cells from each field were counted and averaged as representative number of each specimen. Data shown are expressed as mean + SE obtained from the 10 randomly selected specimens of each group. The statistical significance of difference between control with UVB exposure and all other groups was calculated by TTEST. *P<0.01 (versus control/UVB group; **P<0.000001 (versus control group).
(A)
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1251
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
et al57 have also postulated that metabolic products of lycopene (lycopenoids) may be also responsible for some of lycopene-reported bioactivity, including photoprotection.
Other studies demonstrated that pretreatment of female IRC mice with lycopene before inducing oxidative stress and skin carcinogenesis (with 9-,10-dimethylbenz[a]anthracene (DMBA)/12-O-tetradecanoylphorbol-13-acetate (TPA)) delayed tumor-formation and reduced tumor incidence and tumor vol-ume.58 Lycopene also inhibited the formation of reactive oxygen species (ROS) and MDA. In addition, these mice showed higher levels of translocation of nuclear-factor-erythroid-2-related fac-tor into the nucleus, thus demonstrating a further protective effect.
Studies of skin protection by lycopene in human volunteers have primarily documented a decrease in sensitivity to UVA-induced erythema. Lycopene with β-carotene supplementation prevented UVA-1 induced blistering in 60 patients with poly-morphic light eruption and significantly reduced the expression of the ICAM-1 mRNA associated with the skin lesions.59 Similar photoprotection to the skin and eyes from UV exposure was reported by Stahl & Sies60 by dietary lycopene and β-carotene, especially after 10-12 weeks of lycopene supplementation. In 65 healthy volunteers, supplementation with lycopene completely inhibited UVA-1- and UVA+B-induced upregulation of heme-oxygenase 1, intercellular adhesion molecule 1, and MMP-1 mRNA, all indicators of oxidative stress.61 Oral tomato paste, rich in lycopene, was shown to decrease acute UV-induced erythema, induction of MMP-1, and reduction of fibrillin-1 and mitochondrial DNA 3895-bp deletion in 20 healthy women vol-unteers.62 However, one study of dietary lycopene given in a capsule or as tomato paste to 20 healthy volunteers detected no clinical protection from UV-induced erythema.63
Several mechanisms contribute to the inhibitory effects of lyco-pene on carcinogenesis, as excellently reviewed by Ascenso et al64 and by Mein et al65 Using tomatoes or tomato products, nu-merous studies have demonstrated decreased DNA damage,66
decreased susceptibility to oxidative stress in lymphocytes,67
and decreased low-density lipoprotein (LDL) oxidation or lipid peroxidation.68
Another mechanism of protection might be protection of the gap-junctional communication (GJC) formed by gap junction proteins such as connexin 43 (Cx-43) which control cell growth through differentiation, proliferation, and apoptosis. A loss of GJC is a hallmark of carcinogenesis.69 Lycopene has been dem-onstrated to enhance GJC in human fetal skin fibroblasts37 and in human oral tumor cells69 and to be chemoprotective in can-cer models not only by direct reactive oxygen species (ROS) scavenging activity and activation of anti-oxidant transcrip-tion mechanisms, but also by increasing GJC.65,70,71 Lycopene
increases Cx-43 expression in human keratinocytes (as do the retinoids)65 and in human oral tumor cells.69
Lycopene derivatives may have hormone-like actions at low con-centrations by acting as ligands for a nuclear receptor, similar to retinoic acid.72 Lycopene has been shown to inhibit growth and to induce apoptosis in endometrial, mammary, and lung human cancer cells.73 Because lycopene has been reported to be the most rapidly depleted antioxidant in skin upon exposure to so-lar radiation,74 pre-UV exposure to lycopene was investigated.35 In vitro preexposure of human keratinocytes to lycopene before UVB-irradiation increased both dead and viable subpopulations with over-expression of the BAX gene, resulting in a cell cycle delay at S-phase transition and consequent decrease of cells in 60/61 phase.35 Contrasting recent research demonstrated (both in vitro and in vivo (mice)) that pretreatment with lycopene attenuates UVB-induced hyperproliferation and promotes apop-tosis by negative regulation of FOXO3a through mTORc2/AKT signaling.34 A pictoral scheme of many possible cell proliferation and apoptosis signaling pathways targeted by lycopene in dif-ferent cancer cell lines is illustrated in the review by Ascenso et al64 based on the comprehensive review by Kelkel et al.70
Lycopene has also been shown to modulate the microenviron-mental interaction between cancer cells and stromal fibroblasts. Lycopene inhibits skin fibroblast migration on gelatin and col-lagen in vitro by phosphorylating platelet-derived growth factor-beta (PDGFR-β).75 Both in vitro and in vivo, lycopene bonds to PDGFR-β. In functional studies, lycopene attenuates melanoma-induced fibroblast migration and signaling trans-duction to interfere with tumor-stromal interactions,75,76 thereby limiting tumor growth and possibly metastases.
The present study evaluated for the first time the efficacy of long-term dietary supplementation of lycopene on chronic UVB-induced skin carcinogenesis in SKH-1 mice. These experiments demonstrate that dietary lycopene protects against photocar-cinogenesis. Tumor incidence, multiplicity, latency, and weight are all decreased significantly without any observable clinical or histologic adverse effects. It is known that UVB induces skin tumors that appear decades after exposure in humans: The fact that the time of initiation of tumors is postponed with dietary lycopene is certainly advantageous. Presuming a SKH-1 female mouse’s lifetime is 1.5 years (as estimated by Charles River Lab-oratory, Wilmington, MA) and a human’s lifetime is 90 years, the postponement of onset of visible tumors in mice by 2.8 and 2.0 weeks (with 0.25% and 1% lycopene supplementation) repre-sents an inhibition of onset of human skin tumors by about 3.2 and 2.3 human years. Lycopene was effective in decreasing skin carcinogenesis long-term. Although when counting all tumors, even the smallest ones <1mm, the tumor incidence in lycopene-supplemented groups increased and reached nearly 100% by 40 weeks (as in control non-supplemented group), and the differ-
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1252
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
ence in tumor multiplicity and size between supplemented and nonsupplemented mice also diminished during this extended observation period, protection in decreasing tumor incidence and multiplicity was significant even at 40 weeks when counting tumors >2mm, as was protection in delaying tumor onset and especially in decreasing tumor size. Other evidence of protection by lycopene is decreasing UVB-induced epidermal hyperplasia and decreasing the number of PCNA-positive epidermal cells. Thus dietary lycopene certainly has a role as a safe and efficient chemopreventive when exposure to UVB is limited.
Chronic UVB exposure induces sustained epidermal hyperpla-sia. This epidermal hyperkeratosis and hyperplasia is partially responsible for the unattractive appearance of premature ag-ing of the skin with surface roughness and wrinkles. Also, this hyperplasia may, in turn, contribute to further tumorigenesis51 through activation of cell-cycle-related genes50 (with resultant release of growth factors and other cytokines that increase cel-lular hyperproliferation and inflammation) as well as by altering immune response. Darvin et al77 used optical, noninvasive, in vivo techniques to analyze skin roughness in 20 volunteers be-tween 40 and 50 years old before and after supplementation with several concentrations of lycopene. These researchers77
also measured the skin surface relative concentration of lyco-pene levels by non-invasive, in vivo Raman spectroscopy. They found that higher levels of lycopene correlated significantly with decreased skin roughness. Heinrich et al78 further showed that lycopene mitigates photo-oxidative damage to structural parameters of photoaged skin, including hyperkeratosis. The experiments described in the research presented in this publica-tion confirm that dietary lycopene does significantly decrease this UVB-induced epidermal hyperplasia.
Also in the research presented here, proliferating cell nuclear antigen (PCNA), one of the most reliable and versatile markers for cell proliferation,79 was checked. PCNA plays an essential role in nucleic acid metabolism, replication, and repair80 and is abundantly increased in malignant skin diseases.48 This en-hanced expression of PCNA by UVB was efficiently inhibited by dietary lycopene supplementation in both the sub-acute and chronic studies, thereby contributing to the decreased prolif-eration of tumor cells as evidenced by the markedly decreased tumor load.
Pyrimidine dimers (PDs) (CPDs and 6-4PPs), formed immediate-ly after UVB irradiation, are considered to be early and important biomarkers for UVB–induced carcinogenesis. Long-term ex-posure to UVB results in cumulative oxidative DNA damage with PD formation and resultant tumor initiation.12,49 In normal cells, PDs induced by UVB can be repaired by nucleotide exci-sion repair systems.81 In our short-term, sub-acute UV-radiation study, dietary lycopene remarkably inhibited UVB-induced PD formation, thereby demonstrating its potential photoprotective efficacy against UVB-induced tumor initiation.
Another study confirmed this inhibition of UVB-induced CPD’s in SKH-1 mice after one exposure to UVB.82 (This one exposure was about seven times the UVB exposure of one session of ex-posure in the experiments reported here.) The exposed mice fed a tangerine tomato (ie, lycopene-enhanced) diet had 36% (in fe-males) and 33% (in males) lower CPD levels than mice fed the nonsupplemented control diet, quite similar to the percentage reduction measured in the experiments reported here (a 30% reduction). Similarly, α-tocopherol,83,84 silibinin,85 and other anti-oxidants,84 including anthrocyadnidin in fruits and vegetables,86 and Polypadium leukotomas bacterial extracts87 have been shown to suppress UVB-induced CPD and 6-4 PP formation in mouse83,85,86 and human skin.84,86,87
Several mechanisms may be involved: (1) Although PD produc-tion is a direct result of UV energy absorption without ROS, the generation of ROS may indirectly enhance the production of PDs84 because reactive metabolites can interact with histones to modulate the nucleosome conformation, resulting in an “open” chromatin structure that increases pyrimidine accessibil-ity to UV.88,89 Thus lycopene may indirectly inhibit PD formation through its strong ROS-scavenging capacity; (2) DNA repair enzymes are susceptible to damage through oxidative stress.90 Possibly lycopene decreases oxidative protein damage to help restore normal activity of DNA repair enzymes, thereby lower-ing the numbers of PDs.
Negative staining of PD after long-term UVB exposure suggests involvement of effective repair mechanisms. In our previous research with acute UVB irradiation,47 strong PD staining was observed only 2 hours after a single high (3kJ/m2) dose of UVB. This positive PD expression continued to increase and reached a peak at 24-48 hours, then completely diminished by 7 days after UVB exposure. Probably the sixteen weeks after the termination of the long-term UVB exposure provided adequate time for cells to sufficiently repair photodynamically damaged DNA.
In summary, this research demonstrates that dietary lycopene supplementation provides effective protection against UVB-in-duced photocarcinogenesis in SKH-1 mice by suppressing (1) tumor initiation by decreasing DNA damage (PDs) and (2) tumor proliferation by inhibiting PCNA expression and by decreasing epidermal hyperplasia (which may activate genes of growth fac-tors and cytokines). Further studies may illuminate other specific mechanisms underlying lycopene’s chemopreventive activity.
DISCLOSURESNone of the authors have any financial interest or benefit that has arisen from any direct application of the research presented in this paper.
We are grateful to the American Cancer Foundation for having funded this research.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1253
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
REFERENCES1. Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate
of nonmelanoma skin cancer (keratinocyte carcinomas) in the US popula-tion. JAMA Dermatol. 2015;151:1081-1086.
2. Guy GP Jr., Machlin SR, Ekwueme DU, Yabroff KR. Prevalence and costs of skin cancer treatment in the US, 2002-2006 and 2007-2011. Am J Prev Med. 2015;48:183-187.
3. Lloyd A, Klintmalm G, Qin H, Menter A. Skin cancer evaluation in transplant patients: A physician opinion survey with recommendations. Clin Transplant. 2015;29:110-117.
4. Armstrong BK, Kricker A, English DR. Sun exposure and skin cancer. Austra-las J Dermatol. 1997;38 Suppl 1:S1-6.
5. Epstein JH. Photocarcinogenesis, skin cancer, and aging. J Am Acad Der-matol. 1983;9:487-502.
6. Ley RD. Photoreactivation in humans. Proc Natl Acad Sci USA. 1993;90:4337.7. Matsumura Y, Ananthaswamy HN. Toxic effects of ultraviolet radiation on the
skin. Toxicol Appl Pharmacol. 2004;195:298-308.8. Scharffetter-Kochanek K, Wlaschek M, Brenneisen P, Schauen M, Blaudsc-
hun R, et al. UV-induced reactive oxygen species in photocarcinogenesis and photoaging. Biol Chem. 1997;378:1247-1257.
9. Peus D, Pittelkow MR. Reactive oxygen species as mediators of UVB-induced mitogen-activated protein kinase activation in keratinocytes. Curr Probl Dermatol. 2001;29:114-127.
10. Marchese C, Maresca V, Cardinali G, Belleudi F, Ceccarelli S, et al. UVB-in-duced activation and internalization of keratinocyte growth factor receptor. Oncogene. 2003;22:2422-2431.
11. Wang H, Kochevar IE. Involvement of UVB-induced reactive oxygen spe-cies in TGF-beta biosynthesis and activation in keratinocytes. Free Radic Biol Med. 2005;38:890-897.
12. Halliday GM. Inflammation, gene mutation and photoimmunosuppression in response to UVR-induced oxidative damage contributes to photocarcinogen-esis. Mutat Res. 2005;571:107-120.
13. Wright, TI, Spencer, JM, and Flowers, FP. Chemoprevention of nonmelano-ma skin cancer. J Am Acad Dermatol. 2006;54:933-46,quiz 947-950.
14. Rao, AV, Ray, MR, and Rao, LG. Lycopene. Adv Food Nutr Res. 2006;51:99-164.
15. Di Mascio, P, Kaiser, S and Sies, H. Lycopene as the most efficient biological carotenoid singlet oxygen quencher. Arch Biochem Biophys. 1989;274:532-538.
16. Di Mascio, P, Devasagayam, TP, Kaiser, S and Sies, H. Carotenoids, tocoph-erols and thiols as biological singlet molecular oxygen quenchers. Biochem Soc Trans. 1990;18:1054-1056.
17. Stahl, W and Sies, H. Antioxidant activity of carotenoids. Mol Aspects Med. 2003;24:345-351.
18. Ono M, Takeshima M, Nakano S. Mechanism of the anticancer effect of lyco-pene (tetraterpenoids). Enzymes. 2015;37:139-166.
19. Assar, EA, Vidalle MC, Chopra, M, Hafizi, S. Lycopene acts through inhibiion of IҡB kinase to suppess NF-ҡB signaling in human prostate and breast cancer cells. Tumor Biol. 2016;37(7):9375-9385. Doi: 10.1007/s13277-016-4798-3
20. Graff, RE, Pettersson, A, Lis, RT, Ahearn, TU, Markt, SC, et al. Dietary Lyco-pene intake and risk of prostate cancer defined by ERG protein expression. Am J Clin Nutr. 2016;103:851-860.
21. Ansari, MS and Ansari, S. Lycopene and prostate cancer. Future Oncol. 2005;1:425-430.
22. Takeshima, M, Ono, M, Higuchi, T, Chen, C, Hara, T, et al. Anti-proliferative and apoptosis-inducing activity of lycopene against three subtypes of human breast cancer cell lines. Cancer Sci. 2014;105:252-257.
23. Wane, D and Lengacher, CA. Integrative review of lycopene and breast can-cer. Oncol Nurs Forum. 2006;33:127-137.
24. Huang, JP, Zhang, M, Holman, CD and Xie, X. Dietary carotenoids and risk of breast cancer in Chinese women. Asia Pac J Clin Nutr. 2007;16 Suppl 1:437-442.
25. Garcia-Closas, R, Castellsague, X, Bosch, X and Gonzalez, CA. The role of diet and nutrition in cervical carcinogenesis: a review of recent evidence. Int J Cancer. 2005;117:629-637.
26. Larsson, SC, Bergkvist, L, Naslund, I, Rutegard, J and Wolk, A. Vitamin A, retinol, and carotenoids and the risk of gastric cancer: a prospective cohort study. Am J Clin Nutr. 2007;85:497-503.
27. Sengupta, A, Ghosh, S, Das, RK, Bhattacharjee, S and Bhattacharya, S. Chemopreventive potential of diallylsulfide, lycopene and theaflavin during chemically induced colon carcinogenesis in rat colon through modulation of cyclooxygenase-2 and inducible nitric oxide synthase pathways. Eur J Can-cer Prev. 2006;15:301-305.
28. Kim, DJ, Takasuka, N, Nishino, H and Tsuda, H. Chemoprevention of lung cancer by lycopene. Biofactors. 2000;13:95-102.
29. Ruano-Ravina, A, Figueiras, A, Freire-Garabal, M and Barros-Dios, JM. Anti-
oxidant vitamins and risk of lung cancer. Curr Pharm Des. 2006;12:599-613.30. Sahin, K, Orhan, C, Tuzcu, M, Sahin, N, Ali, S, et al. Orally administered lyco-
pene attenuates diethylnitrosamine-induced hepatocarcinogenesis in rats by modulating Nrf-2/HO-1 and Akt/mTOR pathways. Nutr Cancer. 2014;66:590-598.
31. Hwang ES, Lee HJ. Inhibitory effects of lycopene on the adhesion, invasion, and migration of SK-Hep1 human hepatoma cells. Exp Biol Med (Maywood). 2006;231:322-327.
32. Hung, RJ, Zhang, ZF, Rao, JY, Pantuck, A, Reuter, VE, et al. Protective effects of plasma carotenoids on the risk of bladder cancer. J Urol. 2006;176:1192-1197.
33. Sahin K, Cross B, Sahin N, Ciccone K, Sleiman S, et al. Lycopene in the prevention of renal cell cancer in the TSC2 mutant Eker rat model. Arch Bio-chem Biophys. 2015;572:36-39.
34. Chen P, Xu S, Qu, J. Lycopene protects keratinocytes against UVB radia-tion-induced carcinogenesis via negative regulation of FOXO3a through the mTORC2/AKT signaling pathway. J Cell Biochem. 2018;119:366-377.
35. Ascenso A, Pedrose T, Pinho S, Pinho F, de Oliveira JM, et al. The ef-fect of lycopene preexposure on UV-B-irradiated human keratinocytes. Oxid Med Cell Longev. 2016;Article ID 8214631:15 pages. https://doi.org/10.1155/2016/8214631.
36. Matos HR, Di Mascio P, Medeiros MH. Protective effect of lycopene on lipid peroxidation and oxidative DNA damage in cell culture. Arch Biochem Bio-phys. 2000;383:56-59.
37. Stahl W, von Laar J, Martin HD, Emmerich T, Sies H. Stimulation of gap junc-tional communication: comparison of acyclo-retinoic acid and lycopene. Arch Biochem Biophys. 2000;373:271-274.
38. Heber, D and Lu, QY. Overview of mechanisms of action of lycopene. Exp Biol Med (Maywood). 2002;227:920-923.
39. Kanagaraj, P, Vijayababu, MR, Ravisankar, B, Anbalagan, J, Aruldhas, MM, et al. Effect of lycopene on insulin-like growth factor-I, IGF binding protein-3 and IGF type-I receptor in prostate cancer cells. J Cancer Res Clin Oncol. 2007;133:351-359.
40. Ivanov, NI, Cowell, SP, Brown, P, Rennie, PS, Guns, ES, et al. Lycopene dif-ferentially induces quiescence and apoptosis in androgen-responsive and -independent prostate cancer cell lines. Clin Nutr. 2007;26:252-263.
41. Nahum, A, Hirsch, K, Danilenko, M, Watts, CK, Prall, OW, et al. Lycopene inhibition of cell cycle progression in breast and endometrial cancer cells is associated with reduction in cyclin D levels and retention of p27(Kip1) in the cyclin E-cdk2 complexes. Oncogene 2001;20:3428-3436.
42. Wertz, K, Siler, U and Goralczyk, R. Lycopene: modes of action to promote prostate health. Arch Biochem Biophys. 2004;430:127-134.
43. Stahl, W, Heinrich, U, Aust, O, Tronnier, H and Sies, H. Lycopene-rich prod-ucts and dietary photoprotection. Photochem Photobiol Sci. 2006;5:238-242.
44. Fazekas, Z, Gao, D, Saladi, RN, Lu, Y, Lebwohl, M, et al. Protective ef-fects of lycopene against ultraviolet B-induced photodamage. Nutr Cancer. 2003;47:181-187.
45. Jonker, D, Kuper, CF, Fraile, N, Estrella, A and Rodriguez Otero, C. Ninety-day oral toxicity study of lycopene from Blakeslea trispora in rats. Regul Toxicol Pharmacol. 2003;37:396-406.
46. Moore, JO, Palep, SR, Saladi, RN, Gao, D, Wang, Y, et al. Effects of ultraviolet B exposure on the expression of proliferating cell nuclear antigen in murine skin. Photochem Photobiol. 2004;80:587-595.
47. Moore, JO, Wang, Y, Stebbins, WG, Gao, D, Zhou, X, et al. Photoprotective effect of isoflavone genistein on ultraviolet B-induced pyrimidine dimer for-mation and PCNA expression in human reconstituted skin and its implica-tions in dermatology and prevention of cutaneous carcinogenesis. Carcino-genesis. 2006;27:1627-1635.
48. Kawahira, K. Immunohistochemical staining of proliferating cell nuclear an-tigen (PCNA) in malignant and nonmalignant skin diseases. Arch Dermatol Res. 1999;291:413-418.
49. Pfeifer, GP, You, YH and Besaratinia, A. Mutations induced by ultraviolet light. Mutat Res 2005;571:19-31.
50. Marks, F and Furstenberger, G. Proliferative responses of the skin to exter-nal stimuli. Environ Health Perspect. 1993;101 Suppl 5:95-101.
51. Sisskin, EE, Gray, T and Barrett, JC. Correlation between sensitivity to tumor promotion and sustained epidermal hyperplasia of mice and rats treated with 12-O-tetra-decanoylphorbol-13-acetate. Carcinogenesis. 1982;3:403-407.
52. Stahl, W, Heinrich, U, Aust, O, Tronnier, H, and Sies, H. Lycopene-rich prod-ucts and dietary photoprotection. Photochem Photobiol Sci. 2006;5:238-242.
53. Meinke, MC, Darvin, ME, Vollert, H, and Lademann, J. Bioavailability of natu-ral carotenoids in human skin compared to blood. Euro J Pharm Biopharm. 2010;76:269-274.
54. Yang, TH, Lai, YH, Lin TP, Liu, WS, Kuan, LC, et al. Chronic exposure to Rho-
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1254
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
K.E. Burke, X. Zhou, Y. Wang, H. Weia
concentration of lycopene correlates significantly with the roughness of the skin. Eur J Pharma Biopharma. 2008;69:943-947.
78. Heinrich, U, Tronnier, H, Stahl, W, Bejot, M, Maurette, JM. Antioxidant supplements improve parameters related to skin structure in humans. Skin Pharmacol Physiol. 2006;19:224-231.
79. Iatropoulos, MJ and Williams, GM. Proliferation markers. Exp Toxicol Pathol. 1996;48:175-181.
80. Kelman, Z. PCNA: structure, functions and interactions. Oncogene. 1997;14:629-640.
81. Szymkowski, DE, Lawrence, CW and Wood, RD. Repair by human cell ex-tracts of single (6-4) and cyclobutane thymine-thymine photoproducts in DNA. Proc Natl Acad Sci U S A. 1993;90:9823-9827.
82. Kopec, RE, Schick, J, Tober, KL, Riedl, KM, Francis, DM, et al. Sex differences in skin carotenoid deposition and acute UVB-induced skin damage in SKH-1 hairless mice after consumption or tangerine tomatoes. Mol Nutr Food Res. 2015;59:2491-2501.
83. Chen, W, Barthelman, M, Martinez, J, Alberts, D and Gensler, HL. Inhibition of cyclobutane pyrimidine dimer formation in epidermal p53 gene of UV-irradiated mice by alpha-tocopherol. Nutr Cancer. 1997;29:205-211.
84. Hochberg, M, Kohen, R and Enk, CD. Role of antioxidants in prevention of pyrimidine dimer formation in UVB irradiated human HaCaT keratinocytes. Biomed Pharmacother. 2006;60:233-237.
85. Gu, M, Dhanalakshmi, S, Singh, RP and Agarwal, R. Dietary feeding of silibinin prevents early biomarkers of UVB radiation-induced carcinogenesis in SKH-1 hairless mouse epidermis. Cancer Epidemiol Biomarkers Prev. 2005;14:1344-1349.
86. Afaq, F, Syed, DN, Malik, A, Hadi, N, Sarfaraz, S, et al. Delphinidin, an an-thocyanidin in pigmented fruits and vegetables, protects human HaCaT keratinocytes and mouse skin against UVB-mediated oxidative stress and apoptosis. J Invest Dermatol. 2007;127:222-232.
87. Middelkamp-Hup, MA, Pathak, MA, Parrado, C, Goukassian, D, Rius-Diaz, F, et al. Oral Polypodium leucotomos extract decreases ultraviolet-induced damage of human skin. J Am Acad Dermatol. 2004;51:910-918.
88. Hawkins, CL, Pattison, DI and Davies, MJ. Reaction of protein chloramines with DNA and nucleosides: evidence for the formation of radicals, protein-DNA cross-links and DNA fragmentation. Biochem J. 2002;365:605-615.
89. Liu, X, Mann, DB, Suquet, C, Springer, DL and Smerdon, MJ. Ultraviolet damage and nucleosome folding of the 5S ribosomal RNA gene. Biochem-istry. 2000;39:557-566.
90. Heck, DE, Vetrano, AM, Mariano, TM and Laskin, JD. UVB light stimulates production of reactive oxygen species: unexpected role for catalase. J Biol Chem. 2003;278:22432-22436.
AUTHOR CORRESPONDENCE
Karen E. Burke MD PhDE-mail:................……......................... [email protected]
dobacter sphaeroides extract Lycogen™ prevents UVA-induced malondial-dehyde accumulation and procollagen I down-regulation in human dermal fibroblasts. Int J Mol Sci. 2014;15:1686–1699.
55. Kowalczyk, MC, Walaszek, Z, Kowalczyk, P, Kinjo, T, Hanausek, M, et al. Dif-ferential effects of several phytochemicals and their derivatives on murine keratinocytes in vitro and in vivo: implications for skin cancer prevention. Carcinogenesis. 2009;30:1008-1015.
56. Cooperstone, JL, Tober, KL, Riedl, KM, Tegarden, MD, Cichon, M, et al. Toma-toes protect against development of UV-induced keratinocyte carcinoma via metabolomic alterations. Scientific Reports. 2017;7:1-9.
57. Erdman, JW., Ford, NA, and Lindshield, BL. Are the health attributes of lycopene related to its antioxidant function? Arch Biochem Biophys. 2009;483:229-235.
58. Shen, C, Wang, S, Shan, Y, Liu, Z, Fan, F, et al. Chemomodulatory efficacy of lycopene on antioxidant enzymes and carcinogen-induced cutaneum carci-noma in mice. Food Funct. 2014;5:1422-1431.
59. Marini, A, Jaenicke, T, Grether-Beck, S, Le Floc’h, C, Cheniti, A, et al. Pre-vention of polymorphic light eruption by oral administration of a nutritional supplement containing lycopene, β-carotene, and Lactobacillus johnsonii: results from a randomized, placebo-controlled, double-blinded study. Photo-dermtol Photoimmunol Photomed. 2014;30:189-194.
60. Stahl, W and Sies, H. Carotenoids and flavonoids contribute to nutritional protection against skin damage from sunlight. Mol Biotechnol. 2007;37:26-30.
61. Grether-Beck, S, Marini, A, Jaenicke, T, Stahl, W, and Krutmann, J. Molecular evidence that oral supplementation with lycopene or lutein protects human skin against ultraviolet radiation: results from a double-blinded, placebo-con-trolled, crossover study. Br J Dermatol. 2017;176:1231-1240.
62. Rizwan, M, Roderiguez-Blanco, I, Harbottle, A., Birch-Machin, MA, Watson, REB, et al. Tomato paste rich in lycopene protects against cutaneous pho-todamage in humans in vivo: a randomized controlled trial. Br J Dermatol. 2011;164:154-162.
63. Sokoloski, L, Borges, M, and Bagatin, E. Lycopene not in pill, nor in nature has photoprotective systemic effect. Arch Dermatol Res. 2015;307:545-549.
64. Ascenso, A., Ribeiro, H., Marques, H. C., Oliveira, H., Santos, C., et al. Che-moprevention of photocarcinogenesis by lycopene. Experiment Dermatol. 2014;23:874-878.
65. Mein, JR, Lian, F, and Wang, X-D. Biological activity of lycopene metabolites: Implications for cancer prevention. Nutrition Reviews. 2008;66:667–683.
66. Bowen, P, Chen, L, Stacewica-Sapuntzakis, M, Duncan, C, Sharifi, R, et al. To-mato sauce supplementation and prostate cancer: Lycopene accumulation and modulation of biomarkers of carcinogenesis. Exp Bio Med. 2002;10:886-893.
67. Porrini, M, and Riso, P. Lymphocyte lycopene concentration and DNA protec-tion from oxidative damage is increased in women after a short period of tomato consumption. J Nutr. 2000;130:189–192.
68. Agarwal, S, and Rao, A. Tomato lycopene and low density lipoprotein oxida-tion: A human dietary intervention study. Lipids. 1998;33:981–984.
69. Livny, O, Kaplan, I, Reifen, R, Polak-Charcon, S, Madar, Z, et al. Lycopene inhibits proliferation and enhances gap-junction communication of KB-1 hu-man oral tumor cells. J Nutr. 2002;132:3754-3759.
70. Kelkel, M, Schumacher, M, Dicato, M, and Diederich, M. Antioxidant and anti-proliferative properties of lycopene. Free Radical Research. 2011;45:925-940.
71. Zefferino, R, Leone, A, Piccaluga, S, Cincione, R, and Ambrosi, L. Mercury modulates interplay between IL-1β, TNF-α, and gap junctional intercellular communication in keratinocytes: mitigation by lycopene J Immunotoxicol. 2008;5:353–360.
72. Offord, EA, Gautier, JC, Avanti, O, Scaletta, C, Runge, F, et al. Photoprotec-tive potential of lycopene, β-carotene, vitamin E, vitamin C and carnosic acid in UVA-irradiated human skin fibroblasts. Free Rad Bio Med. 2002;32:1293-1303.
73. Levy, J, Bosin, E, Feldman, B, Giat, Y, Miinster, A, et al. Lycopene is a more potent inhibitor of human cancer cell proliferation than either α-carotene or β-carotene. Nutr Cancer. 1995;24:257-266.
74. Ribaya-Mercado, JD, Garmyn, M, Gilchrest, BA, and Russell, RM. Skin lyco-pene is destroyed preferentially over β-carotene during ultraviolet irradiation in humans. J of Nutrition. 1995;125:1854-1859.
75. Chiang, HS, Wu, WB, Fang, JY, Chen, DF, Chen, BH, Wang, CC, et al. Ly-copene inhibits PDGF-BB-induced signaling and migration in human dermal fibroblasts through interaction with PDGF-BB. Life Sciences. 2007;81:1509-1517.
76. Wu, WB, Chiang, HS, Fang, JY, and Hung, CF. Inhibitory effect of lycopene on PDGF-BB-induced signalling and migration in human dermal fibroblasts: a possible target for cancer. Biochem Soc Trans. 2007;35:1377-1378.
77. Darvin, M, Patzelt, A, Gehse, S, Schanzer, S, Benderoth, C, et al. Cutaneous
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1255 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Gene Expression Studies Pertaining to Extracellular Matrix Integrity and Remodeling: Nuances and Pitfalls
of In Vitro InvestigationsAlan D. Widgerow MBBCh MMed (Plast) FCS FACS,a John A. Garruto BSB
ªCenter for Tissue Engineering, Department of Plastic Surgery, University of California, Irvine, CA; Alastin Skincare Inc., Carlsbad CA
BFree Radical Technology, Inc, Oceanside, CA
Anti-aging strategies using topicals with active agents demand validation and proof of efficacy. One investigation in this realm involves gene expression testing. This study undertakes gene expression analysis of Alastin Skincare Regenerating Skin Nectar (RSN) using an in vitro human skin model. The current study is similar to other published human skin model studies, but with additional time periods beyond 24-hours (which are more appropriate for testing peptides) and a suitable control for the Alastin non-aqueous product. Results show the Alastin product upregulates a large array of genes within areas of skin renewal, extracellular matrix remodeling, barrier func-tion, and inflammation after 72 hours. The study provides gene expression data that support the clinical success of the product. It also demonstrates the difficulty and vulnerabilities in assessing efficacies of products with certain in vitro investigations when the nuances of that product are not considered.
J Drugs Dermatol. 2019;18(12):1255-1259.
ABSTRACT
INTRODUCTION
Skin renewal and regeneration are paramount to efforts in anti-aging strategies and rejuvenation. This is particularly relevant in a milieu of extracellular matrix (ECM) distor-
tion and disruption brought about by extrinsic (photodamage) and intrinsic (aging) factors that initiate and maintain these changes.1,2 In an effort to counteract changes within the ECM and epidermis, peptides, growth factors, and other active in-gredients have been used. In particular, a new generation of peptides has provided solutions to many challenges presented by biologic materials such as growth factors. Peptides’ very low molecular weights ensure absorption, synthetic manufacturing processes generate a predictable quality and quantity of stable actives, far lower amounts of potentially cytotoxic preserva-tives are needed for shelf life maintenance, and peptides have an increased safety profile related to unexpected cellular pro-liferation.3
When comparing efficacies of growth factors versus peptides, certain functional nuances need to be borne in mind when test-ing gene responses, particularly in laboratory environments. In that context, a recent study4 attempted to compare various formulations including growth factor- and non-growth factor-based skin care products, assessing their biologic activity based on gene expression responses. Major limitations were identified related to this study, which included the following:
• A single test period was examined (24 hours), which, while
this time frame may be suited to growth factor stimulation, peptides behave differently and have been demonstrated in many cases to have maximal activity in gene expression at 48, 72, and even longer time periods.
• When selecting controls, water may be ideal for certain aqueous formulations but for non-aqueous anhydrous prep-arations such as (Alastin Regenerating Skin Nectar), this provides potential inaccuracies.
• Finally, although the skin culture EFT model selected has been successfully used as a surrogate for human studies, there are inherent limitations to testing combined cell lines. Although transcription (cell commands) signaling may be demonstrat-ed, the true proof of efficacy often resides in the translational capacity of the product, that relating to new cell and protein regeneration. This is best represented by histological assess- ments of biopsies which take into account the ability of the actives to penetrate skin in a real world environment.
In an effort to address some of the limitations addressed above, a study was designed to test Alastin Skincare Regenerating Skin Nectar, ensuring analysis at two time points, selecting appropriate baseline control comparators, and using a broad panel of genes (Genemarkers Standard Skin Panel) covering a range of important biological functions in skin rather than a few selected genes.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1256
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
A.D. Widgerow, J.A. Garruto
4. qPCR Processing: qPCR reactions were run using validated Taqman® gene expression assays. Open Arrays were run in a Life Technologies QuantStudio 12K Flex instrument. Each gene was assayed in duplicate.
Statistical Data Analysis: Statistical analysis was performed us-ing the relative quantitation (RQ) method. In the first step of an RQ analysis, the CT value of the target gene is normalized to the CT value of an endogenous control gene to generate the delta CT (dCT). dCT values are calculated in order to normal-ize for variability between the samples that may occur during the experimental procedures. Statistically significant (unpaired t-test, P<0.05, N=4) changes in gene expression are shown as RQ values.
RESULTSCytotoxicity Data LDH is a cytoplasmic enzyme released into the culture me-dium of damaged or dying cells. The Alastin Product and Alastin Base both showed <20% cytotoxicity at all 3 time points demonstrating good profiles for cellular viability (Figure 1).
Gene Expression Data For the Alastin Product vs Alastin Base, statistically significant changes in gene expression occurred with the most beneficial response at 72 hours. The Alastin Product produced beneficial changes in gene expression related to antioxidant protection, cell renewal and regeneration, extracellular matrix integrity and anti-inflammatory response. It is noteworthy that results demonstrate poor responses of gene expression at 24 hours confirming previous results of peptide studies that showed effi-cacy at 72 hours and emphasizing the importance of presenting gene expression analysis in an appropriate study design related to the nuances of the active agents being tested (Figures 2 A, B).
MATERIALS AND METHODSAs in the previous study,4 EpiDermFT™ 3D full-thickness in vitro skin culture models containing epidermal and dermal cell lay-ers (EFT-400, MatTek Corp.) were used. Gene expression was assessed in full-thickness tissues following a 24- or 72-hour exposure to the test material. The following treatment groups were included (N=4): • Alastin Skincare Regenerating Skin Nectar: (Alastin Product)• Alastin Skincare Regenerating Skin Nectar Base (non-aque-
ous control): (Alastin Base)
EFT-400 tissues were stored at 4°C. The day before treatment, tissues were equilibrated overnight at 37°C with 5% CO2 and ~95% relative humidity using a 2.5mL volume of EFT-400 culture medium. The following day, equilibration medium was removed from each EFT-400 culture well and replaced with 5.0mL fresh EFT-400 medium (the vendor-recommended volume for a 72-hour study duration). Tissues and culture media were collected after 24, 48, or 72 hours. Test medium from each well was col-lected and stored at -80°C until the lactate dehydrogenase (LDH) assay was performed. Each EFT-400 culture was cut into quar-ters and placed into a tube containing RNAlater preservative solution for a 2-hour incubation at room temperature. Tissues in RNA later were then stored at 4°C for a 2-4-day incubation prior to RNA isolation. The following sequence was adopted:
1. LDH Cytotoxicity Assay: Standard assay for cytotoxicity was performed.
2. RNA Isolation: RNA was isolated from each tissue using a Maxwell 16 Simply RNA Tissue kit (Promega) following the manufacturer’s instructions.
3. cDNA Synthesis: cDNA was generated using a High Capacity cDNA Synthesis Kit according to the manufacturer’s instruc-tions (Applied Biosystems). Standard Skin Panel gene cDNA was generated from 2000 ng RNA per sample.
FIGURE 1. Relative % cytotoxicity [LDH Activity Assay].
8. Nelson A, A O. A tripeptide/hexapeptide anti-aging regimen that targets both collagen and elastin, and improves both physician and subject scoring of facial aesthetics. Case Rep Dermatol. 2018;3(1):1-5.
9. Reivitis A, Karimi K, Griffiths C, Banayan A. A single-center, pilot study evaluating a novel TriHex peptide- and botanical-containing eye treatment compared to baseline. J Cosmet Dermatol. Jun 2018;17(3):467-470.
10. Calame A, AD W. Histological changes associated with extracellular matrix-remodeling topical therapy. Case Rep Dermatol. 2017;2(2):1000126.
11. Ono T, Miyazaki T, Ishida Y, Uehata M, Nagata K. Directin vitroandin vivoevidence for interaction between Hsp47 protein and collagen triple helix. J Biol Chem. 2012;287(9):6810-6818.
12. Oikarinen A. Connective tissue and aging. Int J Cosmet Sci. 2004;26(2):107-107. 13. Widgerow AD. Cellular/extracellular matrix cross-talk in scar evolution and control. Wound Repair Regen.
2011;19(2):117-133. 14. Chiovaro F, Chiquet-Ehrismann R, Chiquet M. Transcriptional regulation of tenascin genes. Cell Adh Migr. 2015;9(1-
2):34-47. 15. Park JS, Lee YH, Lee DH, Chung JH, Lee S-T. Expression of tenascin-C is down-regulated during intrinsic skin aging.
J Dermatol Sci. 2017/05/01/ 2017;86(2):e92-e93. 16. Sun B, Boxer L, Ransohoff J, et al. CALML5 is a ZNF750- and TINCR-induced protein that binds stratifin to regulate
epidermal differentiation. Genes Dev. 2015;29:2225–2230. 17. Torma H. Regulation of keratin expression by retinoids. Dermatoendocrinol. Jul 2011;3(3):136-140. 18. Lundstrom A, Egelrud T. Stratum corneum chymotryptic enzyme: a proteinase which may be generally present in the
stratum corneum and with a possible involvement in desquamation. (0001-5555 (Print)). 19. Chelikani P, Fita I, Loewen PC. Diversity of structures and properties among catalases. Cell Mol Life Sci.
2004;61(2):192-208. 20. Afonina IS, Muller C, Martin SJ, Beyaert R. Proteolytic Processing of interleukin-1 family cytokines: variations on a
common theme. Immunity. 2015;42(6):991-1004. AUTHOR CORRESPONDENCE Alan D. Widgerow Email: [email protected]
Figure 1: Relative % cytotoxicity [LDH Activity Assay]. Figures 2A and B: Statistically significant changes in gene expression induced by Alastin RSN at 72 hours.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1257
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
A.D. Widgerow, J.A. Garruto
FIGURE 2A AND 2B. Statistically significant changes in gene expression induced by Alastin RSN at 72 hours.
Table 1: Actions of Genes Assessed in Standard Skin Panel
GENE Detailed Function Biological Function Skin SERPINH1 Plays a role in collagen biosynthesis as a collagen-specific molecular
chaperone. It codes for heat shock protein HSP47 indispensable for the proper folding of collagen triple helix.11
Extracellular Matrix Integrity
COL1A1 Col1A1 encodes the pro-alpha1 chains of type I collagen whose triple helix comprises two alpha1 chains and one alpha2 chain. Type I is a fibril-forming collagen found in most connective tissues and is abundant in the dermis where it is the most critical structural protein.12
Extracellular Matrix Integrity
COL3A1 COL3A1 gene provides instructions for making type III collagen abundant in the skin particularly in the early phases of wound healing. Ratio conversion to increased type 1 versus type 3 collagen is sought after for controlled scar formation.12,13
Extracellular Matrix Integrity
ELN This elastin gene encodes protein components of elastic fibers in the extracellular matrix important for conferring elasticity tissues including the skin.12
Extracellular Matrix Integrity
Thus, the TriHex Technology and overall formulation of Alastin Regenerating Skin Nectar has been demonstrated to signifi-cantly up-regulate gene expression in the critical areas of cell renewal, ECM remodeling and barrier function at 72 hours. These results contrasted with a previous study that tested the product with water as the control and only at the 24-hour time point.
In particular, the array of genes tested (Table 1) involve skin function from structural support and integrity of the extracellu-lar matrix in the dermis to the cell renewal function and barrier function of the more superficial epidermis thus providing com-prehensive assessment of the entire skin layer (Table 1). The range of genes tested reflect the functional homeostasis at vari-ous levels of the skin structure. Thus, protection at the surface of the skin relates to barrier function, covering various aspects from thermoregulatory issues, transepidermal water loss, mi-crobial invasion, etc – genes measured here – calmodulins and kallikreins. Moving from surface protection to cell renewal and replacement particularly at a superficial level, relevant genes are keratins and tenascin. Then the ECM structural components are particularly important in ensuring the foundation of skin
StatisticsUnpaired t-tests were carried out using TIBCO Spotfire software. Statistically significant results (P<0.05) were reported. The sta-tistical comparison generated delta delta CT [ddCT] values (the mean dCT of the treated group – the mean dCT of the control group). The statistical software converts the ddCT values into log and linear RQ values for export [RQ = 2-ddCT]. The linear RQ values were then converted to linear fold-change values to simplify data interpretation.
DISCUSSIONThe science related to anti-aging formulations has undergone major advances in recent years. Peptides are considered reli-able and effective transformers of skin homeostasis through signaling mediations, cellular proliferation, and regenerative capacities. Validation of these effects is an important part of the proof of concept through a series of steps, often beginning with gene expression analysis. However, as demonstrated in this study, certain nuances characteristic of peptide behavior re-quire consideration when validating efficacy of these molecules. By extending the period of testing and selecting appropriate controls, significant changes in gene expression have been demonstrated.
(2A)
(2B)
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1258
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
A.D. Widgerow, J.A. Garruto
homeostasis is maintained and cross talk between fibroblasts and structural proteins is ensured – here appropriate genes measured are the collagens, elastin, and tenascin. Finally, as a general homeostatic gauge of antioxidant and anti-inflammato-ry activity, catalase and Interleukin 1 beta are representative of these functions (catalase upregulation important for mopping up reactive oxygen species and IL-1b down regulation ensur-ing balanced, controlled inflammation). This general choice of genes was felt to be representative of overall skin function and homeostasis.
The primary goal of this study was to demonstrate efficacy of the product with an appropriate test model design. These re-sults confirm the efficacy of Alastin Nectar with regards to gene expression. In addition, as has been previously noted, gene expression is the first of many validation steps, and it may be argued that histological confirmation and clinical studies are more important in assessing efficacy. This has been carried out and reported in multiple publications.2,5-10
Aside from the favorable gene expression demonstrated here by the Alastin product, the issue of preservative interplay in cel-lular well-being is an area that may deserve more attention. It is known that biologic products such as growth factors need considerably more preservatives added to preparations than active peptides, in order to ensure shelf stability. Alastin Nectar contains no preservatives, which makes it especially suited for
application to ablated and post-procedure skin. This is an ad-vantage compared to growth factor preparations, which have the potential concerns of large molecular weight, inconsistent batch quality, unpredictable biologic effects, and an unfocused targeted approach that accompany biologic/growth factor tech-nologies.
CONCLUSIONGene expression studies are a necessary first step in determining the potential for clinical efficacy of products used in anti-aging skin care. Parameters chosen for testing these formulations need to match the physical nature and behavior characteristics of the active agents involved. To this end, this study was performed in response to a previous report in JDD4 and was designed to ad-dress the inherent characteristics of a peptide-based, anhydrous Alastin Skin Nectar formulation. The same EFT model was used as in the prior study, however, additional testing time points (72 hours) and a more appropriate non-aqueous control were added to the protocol. Results convincingly demonstrated sig-nificant upregulation in gene expression of Alastin Nectar in a wide array of genes in areas of cell renewal, regeneration, ECM remodeling, and barrier function. Combined with multiple other published studies demonstrating histological changes and con-sistent clinical results, this study adds to the validity of Alastin Skin Nectar as a potent pre-conditioner, wound healing and an-ti-aging agent, reaffirming its ongoing success in clinical cases.
TABLE 1.
Actions of Genes Assessed in Standard Skin Panel
GENE Detailed Function Biological Func-tion Skin
SERPINH1 Plays a role in collagen biosynthesis as a collagen-specific molecular chaperone. It codes for heat shock protein HSP47 indispensable for the proper folding of collagen triple helix.11
Extracellular Matrix Integrity
COL1A1Col1A1 encodes the pro-alpha1 chains of type I collagen whose triple helix comprises two alpha1 chains and one alpha2 chain. Type I is a fibril-forming collagen found in most connective tissues and is abundant in the dermis where it is the most critical structural protein.12
Extracellular Matrix Integrity
COL3A1COL3A1 gene provides instructions for making type III collagen abundant in the skin particularly in the early phases of wound healing. Ratio conversion to increased type 1 versus type 3 collagen is sought after for controlled scar formation.12,13
Extracellular Matrix Integrity
ELN This elastin gene encodes protein components of elastic fibers in the extracellular matrix important for conferring elasticity tissues including the skin.12
Extracellular Matrix Integrity
TNCTenascin genes modulate cell adhesion and cellular responses to growth factors and is down regulated with skin aging.14,15
Cell Renewal/ Regeneration
CALML5 Encodes for calmodulin protein and regulates epidermal differentiation and barrier function.16 Barrier Function
KRT4KRT5KRT14
Keratins are intermediate filament proteins that have essential functions in maintaining the structural integrity of epidermis and improves barrier function.17
Cell Renewal/ Regeneration/Bar-
rier function
KLK5KLK7
Kallikrein peptidases are responsible for coordinating desquamation and renewal of epithelial layers and regulating stratum corneum and barrier function.18
Extracellular Matrix Breakdown/
Barrier function
CATCatalase is a very important enzyme in protecting the cell from oxidative damage by reactive oxygen spe-cies (ROS)very representative of anti-oxidant activity.19
Antioxidant
IL1-β This interleukin cytokine is one of the most important mediators of the inflammatory response needing constant control.20
Inflammation
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1259
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
A.D. Widgerow, J.A. Garruto
AUTHOR CORRESPONDENCE
Alan D. Widgerow E-mail:................……......................... [email protected]
DISCLOSURESDr Widgerow is Chief Medical Officer of Alastin Skincare. Mr Garruto is a paid consultant of Alastin Skincare. Genemarkers company is an independently operated company unaffiliated with Alastin Skincare.
ACKNOWLEDGMENTGenemarkers (Kalamazoo, MI) for in vitro testing and Firma Clinical Research, (Chicago, IL) for statistical analysis.
REFERENCES1. Flament F, Bazin R, Laquieze S, Rubert V, Simonpietri E, Piot B. Effect of the
sun on visible clinical signs of aging in Caucasian skin. Clin Cosmet Investig Dermatol. 2013;6:221-232.
2. Widgerow AD, Fabi SG, Palestine RF, et al. Extracellular matrix modula-tion: optimizing skin care and rejuvenation procedures. J Drugs Dermatol. 2016;15(4s):S63-S71.
3. Gorouhi F, Maibach HI. Role of topical peptides in preventing or treating aged skin. Int J Cosmet Sci. Oct 2009;31(5):327-345.
4. Kadoya K, Makino ET, Jiang LI, et al. Upregulation of extracellular matrix genes corroborates clinical efcacy of human fibroblast-derived growth fac-tors in skin rejuvenation. J Drugs Dermatol. 2017;16(12):1190-1196.
5. Robinson D, Frulla A. Randomized, split-face/décolleté comparative trial of procedure enhancement system for fractional non-ablative laser resurfacing treatment. J Drugs Dermatol. 2017;16(7):707-710.
6. Vanaman Wilson MJ, Bolton J, Fabi SG. A randomized, single-blinded trial of a tripeptide/hexapeptide healing regimen following laser resurfacing of the face. J Cosmet Dermatol. Mar 31 2017.
7. Widgerow AD, Jiang LI, Calame A. A single-center clinical trial to evaluate the efficacy of a tripeptide/hexapeptide antiaging regimen. J Cosmet Der-matol. Mar 4 2018.
8. Nelson A, A O. A tripeptide/hexapeptide anti-aging regimen that targets both collagen and elastin, and improves both physician and subject scoring of facial aesthetics. Case Rep Dermatol. 2018;3(1):1-5.
9. Reivitis A, Karimi K, Griffiths C, Banayan A. A single-center, pilot study evalu-ating a novel TriHex peptide- and botanical-containing eye treatment com-pared to baseline. J Cosmet Dermatol. Jun 2018;17(3):467-470.
10. Calame A, AD W. Histological changes associated with extracellular matrix-remodeling topical therapy. Case Rep Dermatol. 2017;2(2):1000126.
11. Ono T, Miyazaki T, Ishida Y, Uehata M, Nagata K. Directin vitroandin vivoevi-dence for interaction between Hsp47 protein and collagen triple helix. J Biol Chem. 2012;287(9):6810-6818.
12. Oikarinen A. Connective tissue and aging. Int J Cosmet Sci. 2004;26(2):107-107.
13. Widgerow AD. Cellular/extracellular matrix cross-talk in scar evolution and control. Wound Repair Regen. 2011;19(2):117-133.
14. Chiovaro F, Chiquet-Ehrismann R, Chiquet M. Transcriptional regulation of tenascin genes. Cell Adh Migr. 2015;9(1-2):34-47.
15. Park JS, Lee YH, Lee DH, Chung JH, Lee S-T. Expression of tenascin-C is down-regulated during intrinsic skin aging. J Dermatol Sci. 2017/05/01/ 2017;86(2):e92-e93.
16. Sun B, Boxer L, Ransohoff J, et al. CALML5 is a ZNF750- and TINCR-induced protein that binds stratifin to regulate epidermal differentiation. Genes Dev. 2015;29:2225–2230.
17. Torma H. Regulation of keratin expression by retinoids. Dermatoendocrinol. Jul 2011;3(3):136-140.
18. Lundstrom A, Egelrud T. Stratum corneum chymotryptic enzyme: a protein-ase which may be generally present in the stratum corneum and with a possible involvement in desquamation. (0001-5555 (Print)).
19. Chelikani P, Fita I, Loewen PC. Diversity of structures and properties among catalases. Cell Mol Life Sci. 2004;61(2):192-208.
20. Afonina IS, Muller C, Martin SJ, Beyaert R. Proteolytic Processing of in-terleukin-1 family cytokines: variations on a common theme. Immunity. 2015;42(6):991-1004.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Written for Physicians by Physicians.
@JDDonline
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1261 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
Histopathological Changes After Experimental Skin Resurfacing Using an Improved Fractional High-Power
1064-nm Q-Switched Nd:YAG Laser Fernando Urdiales-Gálvez MD,a Mario A. Trelles MD PhD,b Sandra Martín-Sánchez MD,a
Mónica Maiz-Jiménez MDa
aInstituto Médico Miramar, Málaga, SpainbVilafortuny Laser Centre, Dubai, United Arab Emirates
Background: Several studies confirm microscopic changes in the cutaneous architecture following various rejuvenation techniques using non-ablative lasers. Objective: To investigate the histological changes that occur after the application of an improved high-power 1064-nm fractional Q-switched Nd: YAG laser, using different focusing tips. Material and Methods: Experimental skin resurfacing of the retroauricular area in 15 female volunteers, in three treatment sessions of one pass each, using the Clear Lift® laser (Alma Lasers, Israel) and five different focusing tips. Biopsies were taken before and immediately after the first treatment session, one month after the first session, and one month after the third session. A total of 60 microscopic images were evaluated at a micrometric scale. Results: The five tips used caused characteristic and similar histological changes in both the dermis and the epidermis. The signs of thermal damage and the formation of new collagen were observed at different depths, in accordance with the focal length of each tip. Neo-formation of collagen with the increase, reorganization and compaction of fibers began one month after the first treatment ses-sion, and was blindly confirmed, with all the tips used, one month after the third treatment session. Conclusion: The skin takes on a new conformation, with histological signs of skin rejuvenation, concordant with previous clinical ob-servations.
J Drugs Dermatol. 2019;18(12):1261-1266.
ABSTRACT
INTRODUCTION
In 2012, the first clinical results were presented with a new fractional non-ablative Q-switched neodymium-doped YAG (Nd:YAG) 1064-nm laser, which combines the benefits of a
non-ablative and fractional laser. The facial resurfacing treat-ments were effective, practically painless, and without down-time. In three treatment sessions, fine lines and wrinkles were reduced by 11.3% without adverse effects (besides temporary edema and erythema, and some cases of pinpoint petechiae) following multiple passes using energies between 400 and 1200 mJ/pulse. The procedure was extraordinarily safe and without downtime.1 Subsequently, Gold et al presented the results of a more detailed study using the same laser, in a sample of ten women, including much higher improvement percentages: 70% for hyper-pigmentation, 80% for telangiectasia, 80% for laxity, and 60% for actinic keratosis. The maximum fluence was also 1200 mJ/pulse, but he performed four treatment sessions.2
It has been postulated that the action of this laser is due to sub-dermal heating of the skin, and of the underlying extracellular matrix, causing contraction and tightening of the skin. To argue this effect, it should be noted that the focal point of the conven-
tional Q-Switched Nd:YAG 1064-nm laser had been aimed at the surface of the skin to target melanin pigment, thereby neces-sitating its application in defocused mode to avoid crusting and splatter. Comparatively, the new laser has a focal point of 100 µm, just beneath the epidermis, with greater penetration and the absence of epidermal crusting. Since the wavelength is ap-plied directly to the skin surface instead of in defocused mode, a penetration depth of up to 3.5-4mm is expected, which may also play a role in the increased efficacy compared with prior modalities.1 On the other hand, it has been suggested, based on what is known about theoretically similar lasers, that the most important effects are due to a micro-thermal injury in the dermis that causes a proliferation of fibroblasts and stimulates new collagen formation, thickening the dermis and improving skin firmness and texture.2 Despite the extensive clinical ex-perience of results with this device, its possible effects on the cutaneous architecture at a microscopic level have not yet been investigated.
Here, we analyze biopsies taken from female volunteers treated with the same laser used by other authors,1,2 recently perfected to allow double the maximum energy per pulse. The objective
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1262
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
F. Urdiales-Gálvez, M.A. Trelles, S. Martín-Sánchez
after the first treatment session, and one month after the third treatment session.
Two-millimeter punch biopsies were taken from the right retro-auricular region of each subject and samples were embedded in 25% formalin for microscopic analysis. In this way, 60 biopsy samples were obtained, 12 for each tip. Specimens were coded for blind exam and sent off to an independent board-certified dermatopathologist for hematoxylin and eosin staining and assessment, using conventional optical microscopy. Digital mi-crophotographs were taken of all the samples for the research team's subsequent sequential evaluation of images on a com-puter screen.
The serial interpretation of micrographs for each tip was per-formed by the research team, without masking, based on the specialized reports of the dermatopathologist and previous knowledge of the interpretation of microscopic skin images.3-10
RESULTSThe 15 volunteers completed the study, attending the scheduled dates for each session, without withdrawals or mishaps. Dur-ing the laser treatment and immediate post-operative period, the majority of cases reported a mild discomfort, stinging, or burning in the treated area, which they generally reported as of minor degree. No complications, adverse effects, or macro-scopic changes of any kind were observed during the follow-up, except erythema and mild edema in the treated area, which was noted in all cases, but disappeared a few hours later.
All the pre-treatment biopsies showed epidermis and dermis without specific pathological signs, but with variable signs of skin aging as shown in Figure 1. After the successive laser ses-sions, common changes were observed in the different samples, which allowed the establishment of a sequence of effects for each of the different tips used, as shown in Figures 2-6.
is to evaluate the short- and medium-term microscopic changes that happen in human skin after experimental skin resurfacing of the retroauricular area using a high-power 1064-nm fraction-al Q-switched Nd: YAG laser at an energy of 2400mJ/pulse, the maximum level allowed with the device.
MATERIALS AND METHODS15 healthy women were recruited, between 34 and 53 years old, with Fitzpatrick phototypes II-V, who participated as volunteers in a study consisting of successive sessions of an experimen-tal laser treatment, limited to the retroauricular area, with the extraction of successive biopsies for histological study. Cases of pregnancy, lactation, and pathological or psychiatric history that could interfere with the evaluation of the results were ex-cluded. Volunteers agreed to appear at the subsequent control and follow-up visits on the set dates. All subjects signed a writ-ten informed consent before inclusion in the study and agreed to the terms and conditions for inclusion in the trial protocol. The trial was conducted according to the Declaration of Helsinki and the study protocol was approved by the Antoni de Gimber-nat Foundation Ethics Committee (Cambrils, Tarragona, Spain).
A high-power 1064-nm Q-switched Nd:YAG laser (Clear Lift®) was used, integrated into the Harmony XL-Pro platform (Alma Lasers, Caesarea, Israel). The laser was programmed to emit an energy of 2400mJ/pulse, at a discharge frequency of 3 Hz and a fixed pulse time of 20ns. The laser discharge passed through a lens, which pixelates the handset’s output beam into micro-beams arranged in a 5 x 5-pixel grid (1 cm x 1 cm). The laser energy crosses the skin's surface and is absorbed by several chromophores, such as melanin, hemoglobin, proteins, and water. The absorption of laser light is considered to cause a photo-acoustic effect, creating micro-lesions in the tissue that lead to a restorative process with the consequent formation of new collagen.
The device provides five tips of different lengths, each of which focuses the light at a different depth. Theoretically, the +2 and +1 tips have a superficial action; the 0 tip has medium penetration, and the –1 and –2 tips exert a deeper action. Three sessions of la-ser treatment were performed in the retroauricular area, spaced one month apart, at the maximum energy allowed by the device (2400mJ/pulse), and with each of the five focusing tips provided by the manufacturer (-2, -1, 0, +1, and +2, with focal distances of 25, 22, 19, 14, and 11 millimeters, respectively). A single pass was performed per session, treating only the right side retroau-ricular area, which was subsequently biopsied.
Five treatment groups were established, one for each tip, so that the effects observed with each tip were verified in three different volunteers. To check the short- and medium-term effects of in vivo irradiation, biopsies were taken before treatment, imme-diately (5 minutes) after the first treatment session, one month
FIGURE 1. Human skin micrograph of the retroauricular area of a 46-year-old volunteer. H&E x 250. Epidermis is thin, and not homogeneous in width. Keratin is not well structured. Differing numbers of cell layers are seen in the skin's superficial stratum. Small papillae are forming the epidermal-dermal junction. Non-parallel collagen in the papillary dermis, running beneath the epidermal junction is noted. The dermis appears lax, with randomly distributed fibers and wide interfibrillar spaces, with characteristic signs of photo-aged skin.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1263
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
F. Urdiales-Gálvez, M.A. Trelles, S. Martín-Sánchez
FIGURE 3. Representative micrographs of the effects obtained with the –1 tip (focal distance = 22 mm). H&E x 250. Graduated scale at intervals of 100 micrometers. (A) Immediately after first treatment session (B) One month after first treatment session: Inflammatory infiltrates (arrows). (C) One month after third treatment session: Chronic lymphocytic inflammatory infiltrate (1, 2). Epidermis is wavy and has reorganized well (3).
FIGURE 4. Representative micrographs of the effects obtained with the 0 tip (focal distance = 19 mm). H&E x 250. Graduated scale at intervals of 100 micrometers. (A) Immediately after first treatment session. Lymphocytic infiltrate and eosinophilic reaction (arrows) (B) One month after first treatment session: Lymphocytic inflammatory infiltrate (1, 2). Epidermis reorganization (3). (C) One month after third treatment session: Chronic lymphocytic inflammatory infiltrate (1, 2). Epidermis reorganization (3).
FIGURE 5. Representative micrographs of the effects obtained with the +1 tip (focal distance = 14 mm). H&E x 250. Graduated scale at intervals of 100 micrometers. (A) Immediately after first treatment session. (B) One month after first treatment session: Chronic lymphocytic inflammatory infiltrate. Papillary dermis with neo-collagen formation (1,2). Epidermis reorganization (3). (C) One month after third treatment session: Chronic lymphocytic inflammatory infiltrate in papillary dermis with neo-collagen formation (1, 2). Epidermis reorganization (3).
FIGURE 2. Representative micrographs of the effects obtained with the –2 tip (focal distance = 25 mm). H&E x 250. Graduated scale at intervals of 100 micrometers. (A) Immediately after first treatment session: Coagulation images (arrows). (B) One month after first treatment session: Lymphocytic inflammatory infiltrates (arrows). (C) One month after third treatment session: Chronic infiltrate in medium and deep reticular dermis with neo-collagen formation (1, 2). Tissue organization with a dense and parallel display of fibers in the papillary dermis (3).
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1264
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
F. Urdiales-Gálvez, M.A. Trelles, S. Martín-Sánchez
appearing well compacted. In the dermis, there was a presence of inflammatory infiltrates between 900 to 1200µm. Signs of elastosis were noted in the deep reticular dermis. One month after the third treatment session, the epidermis had reorganized well, and was slightly wavy with mini-papillae. Hyalinization was seen in the dermis, along with neo-collagen synthesis, more visible in the papillary and medium reticular dermis. Chronic lymphocytic inflammatory infiltrates were found, mostly located in the deep-medium reticular and papillary dermis, at a depth of 1500 to 1700µm, as in the example in Figure 3. Evident signs of neo-collagen synthesis were observed beneath the epidermal-dermal junction (Figure 3).
Effects Observed With the 0 Tip (focal distance = 19 mm) Immediately after the first treatment session, the epidermis was formed by a few layers of cells, presenting fine papillae and a narrow band of keratin. The collagen in the dermis was lax, with notable interfibrillar spaces. Lymphocytic infiltrates and eosinophilic reactions were found in the dermis, predominantly between 1400 to 1700μm. One month after the first treatment session, there was a multicellular epidermis with scarce keratin. Lymphocytic inflammatory infiltrates were present, mostly in the papillary dermis and medium-superficial reticular layer. Neo-collagen formation was observed in the papillary and superficial reticular dermis, especially at depths between 1000-1500µm. Tissue reaction was more noticeable in the papillary dermis. In the superficial-medium reticular layer, interfibrillar spaces were wide and maintained signs of elastosis. One month after the third treatment session, chronic lymphocytic inflammatory in-filtrates persisted in the papillary dermis. A new reorganization of epidermis, with signs of hyalinization and neo-collagen syn-thesis in the papillary dermis, was seen between 700-1000µm (Figure 4).
Effects Observed With the +1 Tip (focal distance = 14 mm)Immediately after the first treatment session, the epidermis structure, although characteristic of aged skin, was not affect-ed. The epidermis was thin and slightly wavy, presenting few cell layers. Keratin appeared dispersed and was not dense. The superficial dermis showed signs of thermal effects, noticed in the eosinophilic reaction/coagulation effect at dermis depths be-tween 300 and 500µm. There were frequent signs of elastosis in the reticular dermis. One month after the first treatment session, the epidermis was in a phase of reorganization. Chronic lympho-cytic inflammatory infiltrates were found immediately beneath the basal epidermis. Neo-collagen synthesis was clear in the papillary dermis, at depths between 400-600µm. One month af-ter the third treatment session, the epidermis was multicellular and had reorganized well. Chronic lymphocytic inflammatory infiltrates were noted in the papillary dermis and beneath the epidermal-dermal junction. Visible signs of new collagen forma-tion were noted in the papillary dermis. Collagen was especially dense at depths between 600-900μm (Figure 5).
Effects Observed With the -2 Tip (focal distance = 25mm)Immediately after the first treatment session, epidermis confor-mation was maintained. Signs of coagulation were found deep in the dermis, between 2000-2500µm, with eosinophilic reactions. Signs of elastosis and notable interfibrillar spaces were noticed. One month after the first treatment session, the epidermis was formed by multiple cell layers and the keratin layer was mini-mally visible. Dense fibers ran parallel beneath the basal layer. Inflammatory infiltrates were found between 1500-2400µm. One month after the third treatment session, the epidermis was well structured with a dense keratin layer. Lymphocytic chronic inflammatory infiltrates were observed in the deep re-ticular dermis (1600-2400µm), with neo-collagen formation and tissue organization showing a parallel display of fibers in the papillary dermis, characteristic of tissue rejuvenation (Figure 2).
Effects Observed With the -1 Tip (focal distance = 22 mm) Immediately after the first treatment session, the epidermis ap-peared thin but maintained its integrity. Keratin was dispersed and conformed of a few broken layers. The dermis presented broken-up fibers, predominantly visible between 1000-1300µm. Below this depth, interfibrillar spaces were notably open. Open spaces in the dermis could be interpreted as a possible ablative effect produced by the QS-laser pulses. One month after the first treatment session, the epidermis was formed by multiple cell layers, and fibers ran parallel beneath the epidermal basal layer,
FIGURE 6. Representative micrographs of the effects obtained with the +2 tip (focal distance = 11 mm). H&E x 250. Graduated scale at intervals of 100 micrometers. (A) Immediately after first treatment session. Inflammatory infiltrate (arrows) (B) One month after first treatment session. Lymphocytic infiltrate (arrows) (C) One month after third treatment session: Chronic lymphocytic inflammatory infiltrate in papillary dermis with neo-collagen formation (1, 2). Epidermis reorganization (3).
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1265
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
F. Urdiales-Gálvez, M.A. Trelles, S. Martín-Sánchez
Effects Observed With the +2 Tip (focal distance = 11 mm) Immediately after the first treatment session, the epidermis was thin, but its characteristics were maintained. The keratin layer was made up of few layers, which were not well compacted. The dermis presented signs of thermal effect, which was more evident beneath the epidermal-dermal junction and at depths between 500-800μm. Signs of elastosis were commonly visible in the medium and reticular dermis, where wide interfibrillar spaces existed. One month after the first session, a reorganiza-tion of the epidermis was observed. Hyalinization was noted in the dermis, as well as neo-collagen synthesis. Fibers were very well attached, running parallel beneath the basal epidermis lay-er. Most tissue reactions were seen between 300-600µm. One month after the third treatment session, multicellular epidermis presenting large papillae and dense keratin layers, which is char-acteristic of rejuvenated skin. Hyalinization and neo-collagen synthesis were more notable in the papillary dermis. The col-lagen was dense and ran parallel beneath the epidermal-dermal junction, at depths between 300-500μm (Figure 6).
The changes observed in the dermis and epidermis were similar for all the tips used, but the depth of laser energy interaction in the dermis varied by the tip used. The -2 and -1 tips have an average depth of action between 900-2500µm, while the +1 and +2 tips act at depths between 300-900µm. The effects of the 0 tip were observed between 700-1700μm. Collagen neo-formation with reorganization of fibers is already verified in samples one month after the first treatment session, and is apparently con-firmed one month after the third treatment session. The increase in the number and thickness of collagen fibers, and their greater compaction, was blindly confirmed with the five tips used.
DISCUSSIONBoth nanosecond (Q-switched) and millisecond (long-pulsed) Nd:YAG lasers have been used for non-ablative dermal remod-eling. They are thought to stimulate new collagen production by originating a thermal injury to the dermis that initiates a wound healing response. During wound healing, procollagen and collagen fibers are initially produced in the dermis and have a small diameter. In more advanced phases of the reparative process, the collagen fibers are thicker and more abundant in the dermis.11-14 The 1064 nm Nd:YAG laser has a lower absorp-tion coefficient by water than the 1320 nm Nd:YAG, which allows for deeper penetration into the dermis and could theoretically promote greater neo-collagenesis. The very short pulse of the QS Nd:YAG provides a means of limiting the thermal diffusion to adjacent structures.15
The general impression is that QS-fractional nanosecond pulses produce ablation in the dermis when they are focused toward the interior of the skin. The depth of the effect is correlated with the focal distance of the tip used for treatment. Energy ab-sorption by the target chromophore originates signs of tissue
coagulation, which can be noted in a form of eosinophilic stain-ing of affected areas. Repetition of high energy pulses could cause resonance waves which, from the target of interaction, propagate to the neighboring tissue, and also to the epidermis. In the dermis, laser microlesions initiate the wound repair pro-cess, which prompts new-collagen formation.
Despite the fact that the QS-laser pulses are only nanoseconds long, the absorption of repeated pulses each second would not only initiate effects inside the dermis, but in the vicinity of la-ser energy interaction site. Effects are also transmitted to the epidermis, following the sound wave expansion originating from the photo-acoustic mechanism of action and the thermal effect. The absence of changes in the epidermis immediately af-ter treatment indicates the viability of this skin layer; however, in control, one month after a single session, the epidermis ap-peared multi-cellular and wavy, consistent with rejuvenated skin; and dense collagen fibers were observed in the dermis. The observed reactions suggest that energy does not concen-trate in the focal point of the interaction, but rather influences reactions that appear in adjacent skin layers. More collagen bands were noticed in the papillary dermis and appeared homo-geneous. Isolated bands of collagen regeneration, reaching the basal epidermis, were a reaction to the micro-lesions produced from the three treatment sessions.
In the majority of the images obtained one month after the third treatment, in the papillary dermis, just below the epidermal-dermal junction, areas of lymphocyte infiltration and/or tissue reaction were observed. This layer of skin is greatly important in skin tightness. The collagen fibers, which run parallel beneath the epidermal-dermal junction play a supporting role that could result in improved appearance, texture, and tightness, concor-dant with the clinical results.
The confirmed histological changes suggest that by first using the deepest acting tips (–2, –1), and later the most superficial acting tips (+2, +1), better clinical results could be obtained. The tissue damage caused by the laser could have a wider distri-bution, and the formation of new, more abundant collagen at different levels could occur. It remains to be confirmed if older skin may respond better to the action of the deeper tips com-pared to the more superficial tips, or if the combination of tips could be beneficial.
In conclusion, the results of this study show significant differ-ences in the depth of the effects depending on the tip used, which confirms the manufacturer's pre-clinical research. How-ever, we do not know the clinical relevance of these differences in facial resurfacing treatments. The histological changes do not always correspond with aesthetic improvements, so it is neces-sary to verify the clinical results obtained with each tip. Future research into the aesthetic improvements achieved in patients
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1266
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
F. Urdiales-Gálvez, M.A. Trelles, S. Martín-Sánchez
undergoing facial resurfacing with various tips will determine the potential importance of using a particular tip, or possible combinations of tips, and this research will help optimize the treatment protocols with this laser device.
DISCLOSURESThe authors declare that there is no conflict of interest regarding the publication of this article.
REFERENCES1. Luebberding S, Alexiades-Armenakas MR. Fractional non-ablative Q-
Switched 1064-nm neodimyum YAG laser to rejuvenate photoaged skin: a pilot study. J Drugs Dermatol. 2012;11:1300-1304.
2. Gold MH, Sensing W, Biron J. Fractional Q-Switched 1064-nm laser for the treatment of photoaged-photodamaged skin. J Cosmet Laser Ther. 2014;16:69-76.
3. Trelles MA, Shohat M, Urdiales F. Safe and effective one-session fractional skin resurfacing using a carbon dioxide laser device in super-pulse mode: a clinical and histologic study. Aesthetic Plast Surg. 2011;35:31-42.
4. Trelles MA, Pardo L, Trelles O, Vélez M, García-Solana L, Rigau J, Chamorro TJ. Clinical and histologic effects of facial skin rejuvenation with pulsed- and continuous-wave flash-scanned CO2 lasers. Aesthet Surg J. 2001;21: 99-411.
5. Trelles MA, Allones I, Luna R. Facial rejuvenation with a nonablative 1320 Nd:YAG laser: a preliminary clinical and histologic evaluation. Dermatol Surg. 2001;27:111-116
6. Trelles MA, Alvarez X, Martín-Vázquez MJ, Trelles O, Vélez M, Levy JL, Al-lones I. Assessment of the efficacy of nonaablative long-pulsed 1064-nm Nd:YAG laser treatment of wrinkles compared at 2,4, and 6 months. Facial Plast Surg. 2005;21:145-153.
7. Trelles MA, Vélez M, Mordon S. Correlation of histological findings of single session Er.YAG skin fractional resurfacing with various passes and energies and the possible clinical implications. Lasers Surg Med. 2008;40:171-177.
8. Trelles M, Allones I, Vélez M, Mordon S. Nd:YAG laser combined with IPL treatment improves clinical results in non-ablative photorejuvenation. J Cos-met Laser Ther. 2004; 6: 69-78.
9. Levy JL, Trelles M, Servant JJ, Agopian L. Non-ablative skin remodeling: an 8-month clinical and 3D in vivo profilometric study with an 810nm diode laser. J Cosmet Laser Ther. 2004;6:11-15.
10. Trelles MA, Levy JL, Álvarez X. Efficacy of nonablative laser treatment for rhytids: a controlled study with objective evaluation via clinical, profilometric and computer assessments. Aesthetic Surg J. 2006;26:136-152.
11. Golberg DJ, Silapunt S. Histologic evaluation of a Q-switched Nd:YAG laser in the nonablative treatment of wrinkles. Dermatol Surg. 2001;27:744-746.
12. Schmults CD, Phelps R, Goldberg DJ. Nonablative facial remodeling. Arch Dermatol. 2004;140:1373-1376.
13. Karabudak O, Dogan B, Baloglu H. Histologic evidence of new collagen for-mation using a Q-switched Nd:YAG laser in periorbital rhytids. J Dermatolog Treat. 2008;19:300-304.
14. Park SR, Lee JH, Jo JH, Seo YK, Kim SM. The effects of 1064nm Nd:YAG irra-diation under the different treatment conditions for skin rejuvenation: quanti-tative and histologic analyses. Photomed Laser Surg. 2013;31:283-292.
15. Freedman JR, Greene RM, Green JB. Histologic effects of resurfacing la-sers. Facial Plast Surg. 2014;30:40-48.
AUTHOR CORRESPONDENCE
Fernando Urdiales Gálvez MDE-mail:....................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
CONTACT INFORMATION
Email: [email protected] • Call: 904-494-8389
Continuing education credits jointly provided with Creighton University Health Sciences
Perry Robins, MD
I have created a comprehensive online education and training course that will
improve the efficiency and competency
of your nurses and physician assistants. This program will save you the time and burden of initial training and increase
the skills to assist you in common office surgical and cosmetic procedures.
Advanced Training in Dermatology
www.dermtraining.com
www.dermtraining.com
• 40 hours of self-paced online training for RNs, NPs, PAs, & MAs• Certificate of Completion & 15 Continuing Education*
credits available
Optimize your practice efficiency & increase patient satisfaction through staff training & development
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1268 Volume 18 • Issue 12
Copyright © 2019 ORIGINAL ARTICLE Journal of Drugs in Dermatology
SPECIAL TOPIC
The Fate of Active Acne and Acne Scars Following Treatment With Fractional Radiofrequency
Bruce E. Katz MDJUVA Skin & Laser Center, New York, NY
Introduction: Acne vulgaris (AV) is a common skin disorder that may result in long-lasting acne scars. Techniques such as delivering fractional radiofrequency (RF) energy through miniature pins or needles have been utilized to manage active acne and acne scars. Skin restoration through dermal remodeling, neo-collagenesis, neo-elastogenesis, and epidermal re-newal are typical results of such treat-ments.Methods: 15 subjects suffering from acne received 3 sessions of facial treatments, 3-4 weeks apart, using a fractional RF device with 24 pins tip of 2500μm in length. The treatment's safety and efficacy were evaluated up to 6 months after the last treatment.Results: Facial photos and classifications of active acne, acne scars, and overall skin appearance demonstrated improve-ments in follow-up visits compared to baseline. No significant or unexpected adverse events were detected.Conclusion: The current study supports the safety and efficacy of the fractional RF treatment modality for acne condition.
J Drugs Dermatol. 2019;18(12):1268-1272.
ABSTRACT
INTRODUCTION
Acne vulgaris (AV), one of the most common skin disor-ders is a prevalent condition mostly affecting adoles-cents and young adults.1 For some patients, acne con-
tinues to be a problem beyond adolescence, persisting well into adulthood.2 Studies on the psychosocial impact of acne have documented dissatisfaction with appearance, embarrassment, self-consciousness, and lack of self-confidence.3 Furthermore, acne is associated with feelings of anxiety, depression, anger, less satisfaction with the body, lower self-esteem, and social dysfunction.4 For many patients, acne may lead to permanent scarring and disfigurement, further aggravating the existing psychosocial aspects of this condition.5,6 It is therefore crucial to effectively treat AV in order to avoid scarring. The pathogenesis of acne relates to increased sebum production in the setting of aberrant follicular keratinization, propionibacterium acnes pro-liferation and significant perifollicular inflam-mation.7 This pro-cess leads to a local tissue damage, resulting in activation of a wound healing cascade. Imbalance in col-lagen deposition and matrix degradation may result in permanent scarring.8
Various therapeutic measures such as chemical peeling, derm-abrasion, and fillers have been performed to improve acne scarring, but with sub-optimal outcomes. Various lasers, each with variable reports of success and advantages, as well as lim-itations, were also adapted to overcome acne effects.9
The potential of ablative lasers such as Er:YAG or CO2 lasers in producing significant improvement was promising; how-ever, these technologies were found to be associated with long recovery times and side effects such as post-inflammatory hy-
perpigmentation and scarring.10 More recently, newer methods have been developed to minimize adverse effects by treat-ing the skin fractionally, leaving healthy areas to promote and im-prove the healing process. Ablative fractional resurfacing, using the CO2 fractional laser system has demonstrated significant beneficial effects on atrophic acne scars and minor side effects comparing to non-fractional CO2 laser.11 Newer techniques such as delivering fractional radiofrequency (RF) energy through miniature pins or needles have been clinically proven effective for skin rejuvenation with high margins of safe-ty.12-15 Improve-ment of skin conditions such as wrinkles, lax skin, and acne scars following fractional RF treatments is achieved through dermal remodeling, neo-collagenesis, and neo-elastogenesis with controlled epidermal renewal.15
The current study was focused on evaluating a fractional RF de-vice for simultaneous treatment of acne scars and active acne and for overall skin appearance improvement.
METHODSA prospective, open label, single center clinical study was con-ducted in our clinic, following IRB approval. The study was intended to evaluate the safety and efficacy of a fractional RF applicator (Fractora, InMode Ltd., Israel) for the treatment of ac-tive acne and acne scarring.
Fifteen subjects, 13 females and 2 males, average age 27.9 years (range 13-53 years), with Fitzpatrick skin types II-VI, hav-ing active acne lesions and acne scars were recruited. Subjects signed informed consent forms prior to enrolment in the study.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1269
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
B.E. Katz
Acne scars classification was done using the following 5 scores scale: None (0) = Normal Trace (1) = Barely perceptible Mild (2) = Shallow Moderate (3) = Medium depth Severe (4) = Deep
Active acne classification was done using the following 5 scores scale: None (0) = Normal Trace (1) = Barely visible and localized Mild (2) = Somewhat visible and diffuse Moderate (3) = Visible and diffuse Severe (4) = Extremely visible and dense
Overall skin improvement was evaluated using the following 5 scores scale: None (0) = No change Mild (1) = Slight change Moderate (2) = Moderate change Good (3) = Considerable change Extreme (4) = Major change
RESULTSTwelve subjects completed the study by attending the 6 months follow-up visit. One subject withdrew after the first treatment and 2 subjects attended either 1- or 3-months follow-up visits, but did not appear for the last, 6 months follow-up visit.
Evaluations of acne scars, active acne and overall skin appear-ance demonstrated progressive improvement in follow-up visits compared to baseline.
The acne scars score was reduced from an average of 2.80 to average of 0.80, active acne score was reduced from an average of 2.93 to an average of 0.75, and overall skin appearance im-proved from a score of 1.45 after one treatment to a score of 3.50 at 6 months follow-up visit. Figure 2 demonstrates the scores reduction at follow-up visits compared to baseline.
Information on medical history, demographics, and baseline photographs were gathered at baseline screening visit.
Exclusion criteria included pacemaker or internal defibrillator, other implanted metallic or electronic devices, permanent metal or silicone implants in the treated area, current or history of can-cer, pre-malignant conditions, cardiac disorders, and any severe concurrent disease, pregnancy or lactating, impaired immune system, current or history of diseases stimulated by heat, un-controlled diabetes, active skin condition in the treatment area, skin disorders, any facial treatment or surgery performed within 3 months prior to treatment, any therapies or medications that may interfere with the use of the study device, or compromised health as determined by the study doctor.
Patients received 3 sessions of facial treatments, 3-4 weeks apart (according to individual condition and physician deci-sion), using the Fractora fractional RF tips (InMode Ltd., Israel). The tip, which is in contact with the skin, is composed of an ar-ray of 24 RF conducting pins (Figure 1) and each pin is 2500μm in length, with or without insulating coating, along 2000μm. The insulated tip was used according to therapist discretion for dark skin types. Safety and efficacy of the treat-ment were evaluated at 3 follow-up visits, 1, 3, and 6 months after the last treatment.
Treatment was conducted according to the instructions in the device operator manual. A test spot was performed in a non-conspicuous area of the treatment site, prior to each session. Topical anesthesia was applied for the desired time and the area was then cleaned and dried. Fractional RF energy levels ranged between 15-38, starting with the low values, and in-creasing gradually as the treatment protocol proceeded. Lower param-eters were applied on sensitive or bony areas and on darker skin types. One or two stacks were performed in each site and 1-2 passes were applied to the full treatment area. Parameters were adjusted according to individual condition, skin response and tolerance.
Safety was evaluated after each treatment and at follow-up sessions. Frontal and 450 left and right-side photographs were taken at standard conditions before and after each treatment and at follow-up time points. Evaluation goals were rating the degree of active acne, acne scars, and overall skin appearance improvement.
FIGURE 1. Fractora 24 pin tip.
FIGURE 2. Histogram representing progress of changes in scores of acne scars, active acne and overall skin improvement as treatment progresses and at 1, 3, and 6-month follow-up visits, compared to baseline.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1270
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
B.E. Katz
FIGURE 4. Acne treatment photos and classifications of a 41 years subject, skin type IV, at baseline (left) and at 6 months post 3 treatments with 24 pins insulated tip (right).
FIGURE 5. Acne treatment photos and classifications of a 25 years subject, skin type III, at baseline (left) and at 6 months post 3 treatments with 24 pins non-insulated tip (right).
FIGURE 6. Acne treatment photos and classifications of an 18 years subject, skin type II, at baseline (left) and at 6 months post 3 treatments with 24 pins non-insulated tip (right).
FIGURE 3. Acne treatment photos and classifications of a 31 years subject, skin type IV at baseline (left), and at 6 months post 3 treatments with 24 pins non-insulated tip (right).
Classification Baseline 6 months follow-up
Acne scars 2 = Moderate 1 = Trace
Active acne 3 = Moderate 0 = None
Overall skin improvement 4 = Extreme
Classification Baseline 6 months follow-up
Acne scars 3 = Moderate 0 = None
Active acne 3 = Moderate 0 = None
Overall skin improvement 4 = Extreme
Classification Baseline 6 months follow-up
Acne scars 2 = Moderate 0 = None
Active acne 3 = Moderate 2 = Mild
Overall skin improvement 3 = Good
Classification Baseline 6 months follow-up
Acne scars 4 = Severe 1 = Trace
Active acne 3 = Moderate 2 = Mild
Overall skin improvement 4 = Extreme
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1271
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
B.E. Katz
advantages were the minimally invasive nature of the proce-dure, the relatively very short downtime and safety.
The current study further demonstrates the progress of simul-taneous active acne and acne scars improvement, following Fractora 24 pins tip treatment. Patients were treated with the coated or non-coated pins tip according to their Fitzpatrick skin type. Patients were followed for up to 6 months post 3 treat-ments. The treatment was found to be safe with no cases of significant or unexpected adverse events. Average scoring dem-onstrated a clear pattern of improvement in active acne, acne scars, and overall skin appearance. Improvement was progres-sive as collagen and elastin regeneration and the result-ant skin renewal is a process that occurs over time.
In summary, results of the current study further support the safety and efficacy of fractional RF technology for the simul-taneous treatment of active acne and acne related scars.
DISCLOSURESDr Bruce Katz has received funding for the clinical study referred to in this article.
REFERENCES1. Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity, and severity risk
factors of acne in high school pupils: a community-based study. J Invest Dermatol. 2009;129(9):2136-2141.
2. Collier CN, Harper JC, Cantrell WC, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58(1):56-59.
3. Zaraa I, Belghith I, Ben Alaya N, Trojjet S, Mokni M, Ben Osman A. Severity of acne and its impact on quality of life. Skinmed. 2013;11(3):148-53.
4. Magin P, Adams J, Heading G, Pond D, Smith W. Psychological sequelae of acne vulgaris: results of a qualitative study. Can Fam Physician. 2006;52:978-979.
5. Rivera, A.E. Acne Scarring: A review and current treatment modali-ties. J Am Acad Dermatol. 2008;59:659-676. http://dx.doi.org/10.1016/j.jaad.2008.05.029
6. Thomas, D.R. Psychosocial effects of acne. J Cutan Med Surg. 2004;8:3-5. http://dx.doi.org/10.1007/s10227-004-0752-x
7. Del Rosso, J.Q. and Kircik, L.H. The sequence of inflammation, relevant biomarkers, and the pathogenesis of acne vulgaris: what does recent re-search show and what does it mean to the clinician? J Drugs Dermatol. 2013;12:s109-s115.
8. Fabbrocini, G., Annunziata, M.C., D’Arco, V. et al. Acne scars: pathogenesis, classification and treatment. dermatology research and practice, 2010, Ar-ticle ID: 893080. http://dx.doi.org/10.1155/2010/893080
9. Goodman, G.J. Treatment of acne scarring. Int J Dermatol. 2011;50:1179-1194. http://dx.doi.org/10.1111/j.1365-4632.2011.05029.x
10. Kutlubay, Z. and Gokdemir, G. Treatment of atrophic facial acne scars with the Er:YAG laser: a Turkish experience. J Cosmet Laser Ther. 2010; 12, 65-72. http://dx.doi.org/10.3109/14764171003706141
11. Manuskiatti, W., Triwongwaranat, D., Varothai, S., et al. Efficacy and safety of a carbon-dioxide ablative fractional resurfacing device for treatment of atrophic acne scars in Asians. J Am Acad Dermatol. 2010; 63274-283. http://dx.doi.org/10.1016/j.jaad.2009.08.051
12. Taub, A.F. and Garretson, C.B. Treatment of acne scars of Skin Types II to V by sublative fractional bipolar radiofrequency and bipolar radiofrequency combined with diode laser. J Cosmet Dermatol. 2011;4:18-27.
13. Hruza G, Forman T.A, Collier S.L, Mulholland S.R. Skin rejuvenation and wrin-kle reduction using a fractional radiofrequency system. J Drugs Dermatol. 2009;8(3):259-265
14. Elman, M. and Harth, Y. Novel multi-source phase-controlled radiofrequency technology for non-ablative and micro-ablative treatment of wrinkles lax skin and acne scars. Laser Ther. 2011;20:139-144. http://dx.doi.org/10.5978/islsm.20.139
15. Mulholland RS, Ahn DH, Kreindel M, Paul M. Fractional ablative radio-fre-
. Figures 3-6 demonstrate examples of patients' photos at 6 months follow-up compared to baseline. Improved acne condi-tion, acne scars, and overall skin appearance post fractional RF treatment is noticeable in follow-up photos and classifica-tions.
Assessments of safety of the Fractora treatment after each treat-ment and at follow-up visits indicated high safety profile with no unexpected or significant adverse events. Skin responses such as mild to moderate erythema and edema, a few pinpoint bleedings and acne flare up were transient and resolved spon-taneously with no intervention.
DISCUSSIONFractional RF skin treatments are well accepted as a safe and effective modality for skin resurfacing, tightening and rejuve-nation.16-20 Various skin conditions such as wrinkles, macropores, sagging and lax skin in face, neck, and décolletage areas are successfully treated, resulting in a gradual skin renewal process with minimal down time. The fractional treatment principle is creating thermally ablated and coagulated microscopic zones of the dermal layer. The non-ablated zones in the uninjured sur-rounding tissue serve as a reservoir of cells that accelerate and promote rapid healing.
Clinical studies have shown that acne scars are an additional major skin problem, that greatly improved following faction-al RF treatments.21-25
The fractional handpiece tips composed of an array of 24 RF pins is designed to deliver RF energy to the skin surface in a fractional manner. The energy is delivered to the skin through bipolar arrays of 24 insulated or non- insulated pins and results in localized heating and ablation of the skin that is in direct con-tact with the pins. Ablation and the resultant coag-ulation of the treated skin promotes skin renewal while untreated skin be-tween the pins enables faster healing of the tis-sue. There is also the contribution of sub-necrotic, non-ablative, non-coagulative dermal matrix heating that promotes volumetric expansion of the dermis, as well as regeneration of fibers, leading to clini-cally apparent skin contraction. The InMode System with the Fractora Handpiece with the 24-pin tip has been cleared by the FDA (K151273).
Previous articles published about these treatments present clini-cal, histological and long-term results from the simultane-ous treatment of active acne and acne related scarring.26-29 Patients were treated with the 24 pins tip, while for dark skin types, the tips used featured the insulating coating to provide additional epidermal protection for a high level of safety.29
Results were followed for long term of up to three years and demonstrated clinically and histologically significant ad-vantag-es in treating simultaneously acne scars and active acne.27,28 The
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1272
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
B.E. Katz
quency resurfacing in asian and caucasian skin: a novel method for deep radiofrequency fractional skin rejuvenation. J Cosmet Dermatol Sci App. 2012;2:144-150.
16. Dahan S, Rousseaux I, Cartier H. Multisource radiofrequency for fractional skin resurfacing-significant reduction of wrinkles. J Cosmet Laser Ther. 2013 Apr;15(2):91-97.
17. Gold M, Taylor M, Rothaus K, Tanaka Y. Non-insulated smooth motion, micro-needles RF fractional treatment for wrinkle reduction and lifting of the lower face: International study. Lasers Surg Med. 2016;48(8):727–733 .
18. Tanaka Y. Long-term nasal and peri-oral tightening by a single fractional non-insulated microneedle radiofrequency treatment. J Clin Aesthet Dermatol. 2017;10(2):45–51.
19. Kaplan H, Kaplan L. Combination of microneedle radiofrequency (RF), fractional RF skin resurfacing and multi-source non-ablative skin tighten-ing for minimal downtime full face skin rejuvenation. J Cosmet Laser Ther. 2016;18(8):438-441.
20. Lyons A, Roy J, Herrmann J, Chipps L. Treatment of décolletage photo-aging with fractional microneedling radiofrequency. J Drugs Dermatol. 2018;17(1):74-76.
21. Elman M, et al. Effective treatment of atrophic and icepick acne scars using deep non-ablative radiofrequency and multisource fractional RF skin resur-facing. J Cosmet Dermatol. 2012;2:267-272.
22. Harth Y, Elman M, Ackerman E, Frank I. Depressed acne scars—effective, minimal downtime treatment with a novel smooth motion non-insulated mi-croneedle radiofrequency technology. J Cosmet Dermatol. 2014;4:212-218.
23. Elawar A, Dahan S. Non-insulated fractional microneedle radiofrequency treatment with smooth motor insertion for reduction of depressed acne scars, pore size, and skin texture improvement: a preliminary study. J Clin Aesthet Dermatol. 2018;11(8):41–44
24. Chandrashekar, B.S., Sriram, R., Mysore, R., et al. Evaluation of micronee-dling fractional radiofrequency device for treatment of acne scars. J Cutan Aesthet Surg. 2014;7, 93-97. http://dx.doi.org/10.4103/0974-2077.138328
25. Ibrahimi OA, Weiss RA, Weiss MA, Halvorson CR et al. Treatment of acne scars with high intensity focused radio frequency. J Drugs Dermatol. 2015;14(9):1066-1069.
26. Hellman J. Retrospective study of the use of a fractional radio frequency ablative device in the treatment of acne vulgaris and related acne scars. J Cosmet Dermatol Sci App. 2015;5:311-316.
27. Hellman J. Long term follow-up results of a fractional radio frequency abla-tive treatment of acne vulgaris and related acne scars. J Cosmet Dermatol Sci App. 2016;6:100-104.
28. Hellman, J. and Yao. J. Novel histological evidence of collagen and elastin regeneration in fractional RF-treated acne scars. J Cosmet Dermatol Sci App. 2019;9:155-164. https://doi.org/10.4236/jcdsa.2019.92013
29. Battle EF, Battle S. Clinical evaluation of safety and efficacy of fractional radiofrequency facial treatment of skin type VI patients. Drugs Dermatol. 2018;17(11):1032-1035.
AUTHOR CORRESPONDENCE
Bruce Katz MDE-mail:................……......................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Derm In- Review Pop Quiz – Each Friday, a new Pop Quiz question is posted to the Next Steps in Derm website, courtesy of Derm In-Review! Test your knowledge each week with these questions!
Patient Buzz Series - Do you ever field odd-ball patient questions and wonder where the information they presented came from? The monthly “Patent Buzz” series addresses recent dermatology news from the consumer press and provides background on the conditions and treatments your patients may ask about at their next office visit. Find the latest in the series under the Derm Topics section on NextStepsinDerm.com
JDD Editorial Highlights – Editorial highlights each month from the Journal of Drugs in Dermatology (JDD), as well as podcasts and the “Ask the Investigator” series.
Genoderms Made Ludicrously Easy: Tumor Syndromes Webinar: Dr. Finch brings a special webinar presentation from his wildly popular book, Genoderms Made Ludicrously Easy. In this webinar, Dr. Justin Finch reviews the clinical spectrum of genetic disorders with malignant potential and examines key dermatologic clues to the diagnosis of genetic tumor syndromes, including PTEN hamartoma syndromes, Reed syndrome, Gardner syndrome, Rombo syndrome and others. The discussion of important clinical features is facilitated by high-yield visual mnemonic cartoons.
A top practice management and career building resource for Residents and Young Dermatologists
Next Steps in Derm Content Highlights
NextStepsInDerm.com @NextSteps_Derm @nextstepsinderm @NextStepsinDerm
If you would like to contribute to Next Steps in Derm, visit https://nextstepsinderm.com/contributor/ or email us at
[email protected] and a team member will get back with you as soon as possible!
Next Steps in Derm Features
Blog-style newsfeed featuring the latest derm news and advice from mentors and peers
Next Steps in Derm Guidebook and eGuide
Online Resource Center
Bi-Monthly eNewsletters
Live Webinars
“Best of ” Booklet
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1274 Volume 18 • Issue 12
Copyright © 2019 CASE REPORT Journal of Drugs in Dermatology
SPECIAL TOPIC
The fusion of technology and medicine has led to the advent of advanced wound healing techniques that may be adapted to the man-agement of surgical defects. Shortened duration of healing and ease-of-use are two potential benefits under investigation. Here we describe a 65-year-old male with a nasal alar wound that was allowed to heal with secondary intention, assisted by a novel methacrylate polymer powder dressing.
J Drugs Dermatol. 2019;18(12):1274-1275.
ABSTRACT
BACKGROUNDAdvances in technology have recently contributed to the de-velopment of innovative wound healing modalities that hold promise for the management of surgical defects.
CASEA 65-year-old Caucasian man presented with a biopsy-proven nodular basal cell carcinoma on the left nasal alar. The tumor was cleared after 2 stages of Mohs Micrographic Surgery with excision down to the nasalis muscle. The resultant defect mea-sured 12mm x 14mm in area and 5mm in depth (wound size 840mm3). Reconstructive options were discussed, including random pattern flap repair, skin graft and secondary intention healing with the aid of a novel methacrylate powder dressing.The patient preferred to proceed with secondary intention heal-ing assisted by the methacrylate powder dressing.
After achieving hemostasis, 10mg of a sterile, biologically inert polymerized methacrylate powder dressing (Altrazeal™, Uluru Inc., TX) was poured over the wound in a uniform layer to fill and seal the entire surface. 0.1ml of sterile ionic saline was sprayed onto the powder to activate the dressing. The single dressing was left intact for 3 weeks. A post-operative follow-up visit at 3 weeks found the wound completely epithelialized and reduced in size to 9 x 10mm in area and 1mm in depth (wound size volume 90mm3). This represented a 90% reduction in wound (Figure 1). The dressing was easy to maintain, non-painful, and there were no reported adverse effects.
DISCUSSIONPolymerized methacrylate powder dressings are a novel, sophisticated dressing modality with great potential in the man-agement of wounds following cutaneous surgery. The dressing
used in this case was a lyophilized, sterile powder consisting of 84.8% poly-2-hydroxyethylmethacrylate, 14.9% poly-2-hydroxy-propylmethacrylate (pHPMA), and 0.3% sodium deoxycholate. These hydrophilic polymers have a covalent methacrylate backbone with a hydroxyl aliphatic side chain. When saline or wound exudate contacts the powder, the spheres hydrate and non-reversibly aggregate to form a moist, flexible dressing that conforms to the topography of the wound and seals it (Figure 2).1
Methacrylate Polymer Powder Dressing for a Nasal Surgical Defect
Matthew J. Lin MD,ª Danielle P. Dubin BA,B Aaron S. Farberg MD,B Hooman Khorasani MD,ª David A. Kriegel MDª
aDivision of Dermatologic Surgery, Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, NYBDepartment of Dermatology, Icahn School of Medicine at Mount Sinai, New York, NY
FIGURE 1. Patient before, during, and after. (A) Post-operative defect on the left nasal alar. (B) Single application of methacrylate polymer powder dressing on wound. (C) Wound after 3 weeks.
FIGURE 2. Polymerized methacrylate powder forms. (A) Methacrylate polmer powder. (B) Aggregation following application of ionic saline medium.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1275
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
M.J. Lin, D.P. Dubin, A.S. Farberg, H. Khorasani, D.A. Kriegel
Once the spheres have aggregated, they are designed to orien-tate in a honeycomb formation with 4-10nm openings (Figure 3) that serve as capillary channels. This porous architecture of the polymer is essential for adequate moisture management, as it allows for vapor transpiration at a rate of 12 l/m2 per day. This ensures the capillary flow from the moist wound surface is distributed evenly through the dressing, which contributes to its 68% water content. Notably, this approximately 3/5 wa-ter composition is similar to the water makeup of human skin. Optimized moisture management is theorized to enhance epi-thelial migration, stimulate angiogenesis, retain growth factors, promote autolytic debridement, and maintain ideal voltage and oxygen gradients for wound healing. The risk of infection is not increased by the existence of these pores, as their small size does not allow for bacterial migration.1
CONCLUSIONThis case demonstrates the effectiveness of a polymerized meth-acrylate powder dressing to promote timely wound healing of a nasal alar defect. This low maintenance, single-application, user-friendly dressing spared the patient the inconvenience and pain associated with more conventional primary and second-ary dressings. The dressing was well tolerated and resulted in a 90% reduction in wound size.
Further studies are needed to investigate the utility of this prom-ising technology.
DISCLOSURESThe authors have no conflicts of interest to declare.
REFERENCES1. Fitzgerald RH, Bharara M, Mills JL, Armstrong DG. Use of a Nanoflex pow-
der dressing for wound management following debridement for necrotising fasciitis in the diabetic foot. Int Wound J. 2009;6(2):133–9.
AUTHOR CORRESPONDENCE
Matthew J. Lin MDE-mail:................……................. [email protected]
FIGURE 3. Mechanism of methacrylate powder. When saline is added to methacrylate polymer powder, the particles form an aggregated, organized honeycomb structure with pores 4-10nm in diameter that serves as capillary channels. The small size allows for wound moisture management but does not permit bacterial transmigration.
A SUPPLEMENT TO
JDDTherapeutic Insights in
Melasma and Hyperpigmentation Management
Therapeutic Insights in Melasma and
Hyperpigmentation Management
STILLAVAILABLE
This journal-based enduring activity is funded through an educational grant
provided by Galderma Laboratories, L.P.
Available now in the JDDonline CME Library: www.JDDonline.com/CME
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Response of Lichen Planopilaris to Pioglitazone Hydrochloride Erik L. Peterson BS, Daniel Gutierrez MD, Nooshin K. Brinster MD,
Kristen I. Lo Sicco MD, Jerry Shapiro MDThe Ronald O. Perelman Department of Dermatology, New York University School of Medicine, New York, NY
December 2019 1276 Volume 18 • Issue 12
Copyright © 2019 CASE REPORT Journal of Drugs in Dermatology
SPECIAL TOPIC
Lichen planopilaris (LPP) is a cicatricial alopecia that often causes permanent hair loss. Pioglitazone, a peroxisome proliferator activated receptor-gamma (PPAR- γ) agonist, has demonstrated immunomodulatory properties that may offer an effective treatment modality. This retrospective analysis describes 23 patients with LPP treated with adjunctive pioglitazone. Most (18/25) demonstrated significant reduction in patient-reported symptoms and clinical signs of inflammation. No adverse effects were reported.
J Drugs Dermatol. 2019;18(12):1276-1279.
ABSTRACT
INTRODUCTION
Lichen planopilaris (LPP) is a cicatricial alopecia character-ized by perifollicular hyperkeratosis, erythema, perma-nent hair loss, and pruritus, pain or burning in affected
areas. LPP demonstrates four clinical variants that share similar histologic findings: frontal fibrosing alopecia (FFA), Graham-Little-Picardi-Lasseur syndrome (GLPL) and fibrosing alopecia in a pattern distribution (FAPD).1,2 Together, these represent the most common primary scarring alopecias.1,2 Histopathology re-veals lymphocytic infiltrates centered around the follicular in-fundibulum, interface dermatitis, and progressive perifollicular hyperkeratosis and fibrosis.7 Treatment centers on reducing dis-ease symptomatology and decreasing inflammation to prevent scarring. Most therapeutic regimens consist of high potency topical glucocorticoids and immunosuppressants, topical min-oxidil, intralesional glucocorticoids, and systemic anti-inflam-matory agents such as doxycycline and hydroxychloroquine.3 While the pathogenesis of LPP is poorly understood, disease activity likely involves a combination of hormonal and andro-genetic factors with autoinflammatory destruction of the hair follicle.4
The perioxisome proliferator-activated receptor gamma (PPAR- γ) pathway has been of interest as an additional tool in the treatment of LPP. One study demonstrated a reduction in PPAR- γ tissue expression in LPP,5 although these results were not reproducible in another study.6 Decreased PPAR- γ expression results in increased inflammatory lipids, local in-flammation, and destruction of the pilosebaceous unit.5 Thus,
PPAR- γ agonists may be efficacious in addressing the under-lying pathology of LPP. This study represents single-center retrospective analysis of 23 patients with LPP who were treated with pioglitazone at a Hair and Scalp Disorders Clinic at New York University Langone Health (NYULH).
METHODSA retrospective review of all patients with LPP who presented to NYULH between October 1, 2007 and August 18, 2018 was performed. A total of 252 unique patients were identified using International Classification of Disease billing codes and natural language corresponding to LPP, FFA, or GLPL. All individuals age 18 to 89 years of age with diagnosis of LPP, FFA, or GLPL were included. When necessary, biopsy was performed for di-agnostic guidance. A total of 23 patients who were treated with pioglitazone were identified. All patients were started on 15 mg orally once daily and increased to 30mg if well-tolerated.
These patients were evaluated for clinical changes in degree of inflammation and progression of alopecia. Hairline measure-ments from bilateral outer canthi and glabella to the frontal and temporoparietal hairline were utilized as a means of tracking progression of disease. Improvement was defined as stabi-lization of disease (lack of further progression of hair loss or recession of hair line) and resolution of symptoms as assessed by the patient perception. This study was approved by the NYULH Institutional Review board.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1277
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.L. Peterson, D. Gutierrez, N.K. Brinster, et al
treatment duration on pioglitazone was 10.68 months (range 2-20 months). The mean time to improvement after initiation of pioglitazone was 4 months (range 1-12 months). All those biop-sied had histopathologic features consistent with LPP including inflammatory lymphocytic infiltrates, interface dermatitis, and progressive perifollicular fibrosis and hyperkeratosis. None had concurrent oral or nail lichen planus. Concomitant disorders included: androgenetic alopecia (4/23), hypothyroidism (3/23), alopecia areata (2/23), and dyslipidemia (2/23).
Prior to initiating therapy with pioglitazone, all were treated with one or more other agents. However, no patients were controlled with these treatments alone or in combination. The average number of medications employed during the stabilizing regimen was 7 (range 4-10). The average number of medications employed for the maintenance regimen was 4 (range 2-7). First and second line medications are listed in Table 2. Patients with significant symptoms, rapid progression of disease, or marked activity on trichoscopy were also initiated on systemic immuno-suppression, such as hydroxychloroquine and doxycycline. As part of the therapeutic ladder for LPP, pioglitazone was added after first and second line medications failed to achieve stabi-lization.
Response to treatment was recorded at baseline and all fol-lowing visits. Patients were evaluated by the investigators and assessed via objective measures of hairline measurements, photographs, and subjective measure of symptoms of pruritus, pain, or burning. In our cohort, 18 patients (78%) achieved im-provement or stabilization of disease activity while 5 patients (22%) did not report benefits. One patient achieved minor re-growth. Mean time to stabilization after initiation of pioglitazone was 4 months (range, 1-12 months), with a mean treatment duration of 10.68 months (range, 4-20 months). No patient experienced significant adverse effects with either topical, in-tralesional, or systemic therapies. Several patients exhibited significant improvement with the addition of pioglitazone, after being refractory to other first line therapies. One such patient demonstrated improvement after 1 month of pioglitazone, complete cessation of disease activity after 2 months, and was stabilized on pioglitazone monotherapy for 12 months. Despite initial improvement on pioglitazone, three patients discontinued therapy citing concerns regarding the medication’s black box warning of increased risk of bladder cancer.
TABLE 1.
Characteristics of 23 Patients With Lichen Planopilaris and Their Clinical Response to Pioglitazone Hydrochloride
Baseline Characteristics
Gender, F:M 21:2
Age, year (mean, range) 46.8 (39-69)
Caucasian 23
Diagnosis
FFAFrontal Fibrosing Alopecia 9
LPPLichen planopilaris 13
Write this one out: GLPL 1
Top comorbidities
Androgenetic alopecia 4
Hypothyroidism 3
Alopecia areata 2
Dyslipidemia 2
Treatment Regimen
Concurrent use of topical medications
Clobetasol 0.05% solution 19
Minoxidil 5% solution 13
Tacrolimus 0.3% in Cetaphil cleanser 12
Hydrocortisone butyrate lotion 2
Clobetasol shampoo 4
Concurrent use of intralesional triamcinolone acetonide 12
Concurrent use of systemic medications
Hydroxychloroquine 200mg twice daily 17
Doxycycline 100mg twice daily 11
Naltrexone 3-4.5mg/day 6
Finasteride 1-5mg/day 10
Mycophenylate mofetil 1
Methotrexate 15mg/week 2
Prednisone 40mg, tapered 1
Response to Pioglitazone Hydrochloride
Complete resolution* 0
Improvement, stabilization** 18
No change*** 5
Progression**** 0
Time to improvement after pioglitazone (months) 4
Total treatment duration with pioglitazone (months) 10.68*Resolution of alopecia, complete regrowth**Improvement or stabilization in subjective and objective measures***No change in subjective or objective measures****Worsening of condition, in objective or subjective measuresSubjective measures = patient-reported symptoms, clinical findingsObjective measures = hairline measurements, photographs
RESULTSTable 1 summarizes the characteristics of 23 patients with LPP who were treated with pioglitazone hydrochloride. All patients were referred from an outside dermatologist for specialty evaluation and care. The average age at diagnosis was 46.8, (range, 39-69 years). All patients were Caucasian. The mean
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1278
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.L. Peterson, D. Gutierrez, N.K. Brinster, et al
TABLE 2.
Therapeutic Ladder for the Treatment of Lichen Planopilaris
Intervention Type Medication Line Dosage Notes
Topical Tacrolimus 0.3% compounded in
Cetaphil cleanser1st BIDtwice
dailyPatient applies thin layer to affected areas first. Compounded in Cetaphil cleanser as an effective, convenient, and inexpensive delivery mechanism.
Topical Clobetasol solution 1st BIDtwice daily Patient applies thin layer to affected areas second.
Topical Minoxidil 5% solution 1st BIDtwice daily
Patient applies third, creating 5 parts in the hair and applying 5 drops per part, equivalent to 1mL
Systemic Finasteride 1st 1mg/day 5α-reductase inhibition has shown efficacy in the treatment of FFA, as well as concurrent androgenetic alopecia.18,19
Intralesional Triamcinolone acetanide 1st 2.5mg/cc 3 cc applied intralesionally 1cm behind frontal hairline. 0.5cc applied to each
eyebrow. Maximum of 20mg per month.
Systemic Hydroxychloroquine 2nd 100-200mg BID
Therapy starts at 100mg BID and can increase to 200mg BID as needed. Care is taken to ensure patient follows with ophthalmology for yearly retinal exams,
Systemic Doxycycline 2nd 50-200mg BID
Therapy starts at 50mg BID and can increase to 200mg BID. Counseling regarding possible gastrointestinal and photosensitive side effects is recom-mended.
Systemic Naltrexone 3rd 3mg/day Low dose naltrexone has shown efficacy in reducing symptoms and inflam-mation in LPP.10
Systemic Pioglitazone 3rd 15-30mg/day
Low dose pioglitazone has shown efficacy in reducing symptoms and inflam-mation in LPP.8
Systemic Mycophenylate mofetil 3rd 500-1000mg
BIDMycophenylate mofetil has shown efficacy as an adjunctive anti-inflammato-ry therapy in FFA.12
Systemic Dapsone 3rd 50-100mg/day
Dapsone inhibits neutrophilic and lymphocytic inflammatory responses and may therefore provide adjunctive benefit in LPP.16
1, 78% of patients achieved stabilization or significant improve-ment with the addition of pioglitazone. While these patients were also receiving intralesional glucocorticoids and systemic and topical immunosuppression, their disease was recalcitrant prior to initiation of pioglitazone, suggesting that PPAR- γ ago-nism can be a beneficial tool in the therapeutic armamentarium for LPP via other pathways implicated in disease pathogenesis. Two studies, of 24 and 22 patients with LPP, found pioglitazone to be effective in controlling symptoms, disease progression, and inflammation in a majority of patients.8,9 However, these conclu-sions differ from another study of 22 patients in which only a minority of patients benefited from pioglitazone in recalcitrant LPP.5 Variable response rates to pioglitazone have been well de-scribed in literature for the treatment of diabetes mellitus, with response rates ranging from 57.1%-71.4% for responders and 28.6%-42.9% for non-responders.11,12 A majority of studies found an average non-responder rate of 20-30%,14 corresponding to our findings of 22% of patients who did not achieve stabilization with pioglitazone therapy. While some have postulated that the insulin resistance index may be a useful predictor of response rates to pioglitazone, no significant differences were found be-tween responder and non-responder groups in terms of age, sex, body mass index, fasting plasma glucose, or the homeostatsis model assessment for evaluating insulin resistance.11,13 Further
DISCUSSIONThe proposed mechanism and efficacy of pioglitazone hydro-chloride in the treatment of LPP is debated.5,6 Diminished tissue expression the peroxisome proliferator-activated receptor gam-ma (PPAR- γ) has been shown to result in toxic accumulation of lipids and fibrotic destruction of the pilosebaceous unit.6 Stud-ies of PPAR- γ-deficient mice demonstrated progressive hair loss, cutaneous hyperkeratosis, erythema, and complete loss of follicular ostia, as well as scratching behavior, all reminiscent of the clinical presentation and symptomotology of LPP.5,6 On histology, these mice had interstitial lymphocytic infiltrates, dys-trophic hair follicles, and destruction of sebaceous glands with follicular fibrosis, while microarray analysis revealed significant increase in gene expression of chemokines and apoptosis-re-lated genes, resulting in increased activation of macrophages and T-lymphocytes. Such findings underscore the importance of PPAR- γ in the clinical and histologic presentation of LPP, con-firming that decreased PPAR- γ expression results in activation of pro-inflammatory pathways that lead to aberrant lipid metab-olism and ultimately contribute to a cicatricial alopecia. Thus, as a PPAR- γ agonist, pioglitazone hydrochloride may be an effec-tive means of combating the underlying pathogenesis of LPP. 8,9
This single-center retrospective analysis of 23 patients supports the utility of pioglitazone for treatment of LPP. As shown in Table
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1279
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
E.L. Peterson, D. Gutierrez, N.K. Brinster, et al
investigation found that the two most common polymorphisms of the PPAR- γ gene, Pro12Ala and Pro12Pro, are not associat-ed with differing response rates to pioglitazone in vivo.14 Thus, while it is clear that some individuals demonstrate decreased response to therapy with pioglitazone, factors determining re-sponse remain uncertain. Further randomized controlled trials are necessary to understand the true mechanism and efficacy of this therapeutic modality.
The findings of this study are limited by several factors. This was a retrospective study, without a control population, which evaluated patients on several concurrent immunosuppressive therapies. Therefore, patient improvement may not be due sole-ly from pioglitazone itself, but rather a function of continued use of concurrent medications on other medications or spontaneous resolution. Furthermore, patient evaluation and assessment of disease activity was based on one provider’s clinical expertise.
CONCLUSIONPioglitazone is a beneficial adjunctive therapy in the treatment of LPP, as supported by 78% of patients who demonstrated significant improvement in disease activity with the addition of pioglitazone to their therapeutic regimen. For a subset of patients, the addition of pioglitazone to their therapeutic regi-men represented a key step toward stabilization, after being recalcitrant to all other first line therapies. These findings, in ac-cordance with current literature supporting the role of PPAR- γ in cicatricial alopecia, suggest that pioglitazone’s mechanism of action may combat a key contributor in the pathogenesis of LPP. However, given mixed evidence in current literature re-garding pioglitazone’s efficacy, a prospective, randomized trial evaluating the treatment of LPP with pioglitazone as the sole therapeutic agent is necessary to confirm or refute its potential beneficial effect.
DISCLOSURESThe authors have no conflict of interest to declare.
REFERENCES1. Saceda-Corralo, D, Fernández-Crehuet, P, Fonda-Pascual, P, Pindado-Ortega,
C, Moreno-Arrones, OM, Vañó-Galván, S. Clinical description of frontal fi-brosing alopecia with concomitant lichen planopilaris. Skin Appendage Dis-ord. 2018;4(2):105-107.
2. Olsen, EA, Bergfeld, WF, Cotsarelis, G, Price, VH, Shapiro, J, Sinclair, R, Whiting, DA. Summary of North American Hair Research Society (NAHRS)-sponsored workshop on cicatricial alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003;48(1):103-110.
3. Cevasco NC, Bergfeld WF, Remzi BK, de Knott HR. A case-series of 29 pa-tients with lichen planopilaris: the Cleveland Clinic Foundation experience on evaluation, diagnosis, and treatment. J Am Acad Dermatol. 2007;57(1):47-53.
4. Vañó-Galván, S, Molina-Ruiz, AM, Serrano-Falcón, C, Arias-Santiago, S, Ro-drigues-Barata, AR, Garnacho-Saucedo, et al. Frontal fibrosing alopecia: a multicenter review of 355 patients. J Am Acad Dermatol. 2014;70(4):670-678.
5. Karnik P, Tekeste Z, McCormick TS, Gilliam AC, Price VH, Cooper KD, et al. Hair follicle stem cell-specific PPARgamma deletion causes scarring alope-cia. J Invest Dermatol. 2009;129:1243-57.
6. Spring, P, Spanou, Z, de Viragh, PA. Lichen planopilaris treated by the per-oxisome proliferator activated receptor-γ agonist pioglitazone: Lack of last-
ing improvement or cure in the majority of patients. J Am Acad Dermatol. 2013;69(5):830-832.
7. Harries MJ. The immunopathobiology of lichen planopilaris [PhD thesis]. Manchester, United Kingdom: University of Manchester; 2011.
8. Baibergenova, A, Walsh, S. Use of pioglitazone in patients with lichen plano-pilaris. J Cutan Med Surg. 2012;16(2):97-100.
9. Mesinkovska, NA, Tellez, A, Dawes, D, Piliang, M, Bergfeld, W. The use of oral pioglitazone in the treatment of lichen planopilaris. J Am Acad Dermatol. 2015;72(2): 355-356.
10. Strazzulla, LC, Avila, L, Lo, KS, Shapiro, J. Novel treatment using low-dose naltrexone for lichen planopilaris. J Drugs Dermatol. 2017;16(11): 1140-1142.
11. Satoh N, Ogawa Y, Usui T, Tagami T, Kono S, Uesugi H, et al. Antiatherogenic effect ofpioglitazone in type 2 diabetic patients irrespective of the respon-siveness to its antidiabetic effect. Diabetes Care. 2003;26:2493-2499.
12. Gavin LA, Barth J, Arnold D, Shaw R. Troglitazone add-on therapy to a com-bination of sulfonylureas plus metformin achieved and sustained effective diabetes control. Endocr Pract. 2000;6:305-310.
13. Araki T, Emoto M, Yokoyama H, et al. Insulin resistance index as a predictor for pioglitazone treatment in type 2 diabetes. Osaka City Med J. 2005;51:19-25.
14. Blüher, M, Lübben, G, Paschke, R. Analysis of the relationship between the Pro12Ala variant in the PPAR-γ2 gene and the response rate to therapy with pio-glitazone in patients with type 2 diabetes. Diabetes Care. 2003;26(3):825-831.
15. Zhu, YI, Stiller, MJ. (2001). Dapsone and sulfones in dermatology: overview and update. J Am Acad Dermatol. 2001;45(3):420-434.
AUTHOR CORRESPONDENCE
Jerry Shapiro MDE-mail:................……...................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Clinical Insights About the Role of Skin pH in Inflammatory Dermatological Conditions
Supported by an unrestricted educational grant from the International Dermatology Education Foundation
www.jddonline.com/supplement_library
A SUPPLEMENT TO
JDDClinical Insights About the Role
of Skin pH in Inflammatory Dermatological Conditions
NOWAVAILABLE
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1281 Volume 18 • Issue 12
Copyright © 2019 LETTERS TO THE EDITOR Journal of Drugs in Dermatology
To the Editor: Non-invasive procedures targeting the submen-tal fat or “double chin” have undergone a surge in popularity. Injections of deoxycholic acid, a secondary bile acid, have re-cently received FDA-approval for fat reduction in this area. With appropriate patient selection, this preparation of 10 mg/mL of sodium deoxycholate (Kybella®, Kythera Biopharmaceuticals, Westlake Village, CA) leads to aesthetic improvement of moder-ate-to-severe convexity or fullness associated with submental fat in adults.
Treatment is generally safe and well tolerated. The most com-monly reported transient adverse effects include injection site pain, swelling, bruising, erythema, hematoma, induration, numbness, nausea, and dizziness. There have been uncommon reports of marginal mandibular nerve paresis, dysphagia, and urticaria.
The proposed mechanism of action for the lipolysis properties of these bile acids is not fully elucidated. Current evidence sug-gests that sodium deoxycholate acts as a biological detergent that disrupts the adipocyte phospholipid bilayer, which leads to cellular lysis and necrosis. Laboratory investigations of cul-tured cells confirmed the deoxycholic acid-induced cellular lysis and also noted histological evidence of inflammation and neovascularization.
The trifecta of adipolysis, inflammation, and neovascularization may alter the texture of the subdermis, as the subcutaneous tis-sue may become firmer due to the formation of new adhesions and blood vessels. This unintended side effect of deoxycholic
acid injections is not commonly reported because, for most pa-tients, it is unproblematic; however, this change in skin makeup of the submental region does have implications when perform-ing open surgery on the anterior neck. In response to sodium deoxycholate, the submental fat may become contracted and excessively firm. The adhesions formed by the injections may also obscure the surgical planes, which complicates the dis-section process. Neovascularization also increase the risk of bleeding in the surgical field, necessitating meticulous hemo-stasis and surgical drains.
We have found that these changes in subdermal characteris-tics secondary to deoxycholic acid injections pose a challenge when performing neck lifts, platysmoplasty, submentoplasty, neck liposuction, and neck dissection. Surgeons operating on the neck should, therefore, collect a comprehensive medical history and be familiar with deoxycholic acid injection adip-loysis. This allows the surgeon to appropriately prepare for the operative challenges and counsel the patient on their individual risk profile as it pertains to the neck region.
Disclosure: No conflicts of interest to disclose.
The Impact of Submental Deoxycholic Acid Injections on Neck Surgery
Matthew J. Lin MD,a Danielle P. Dubin BA,a Robert M. Schwarcz MD,b Hooman Khorasani MDa
ªDivision of Dermatologic Surgery, Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, NYbDivision of Ophthalmic Plastic Surgery, Department of Ophthalmology, NYU Langone Health, New York, NY
AUTHOR CORRESPONDENCE
Matthew J. Lin MD E-mail:................……......................... [email protected]
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1282 Volume 18 • Issue 12
Copyright © 2019 FEATURE Journal of Drugs in Dermatology
SPECIAL TOPIC
The diagnosis of pyoderma gangrenosum (PG) is often difficult to establish based on a clinical presentation, which can mimic other dermatologic conditions. The formation of a mnemonic that incorporates the most prevalent clinical features of PG could aid in accu-racy and speed of diagnosis. The 5 P's of PG: Painful, Progressive, Purple, Pretibial, Pathergy, and systemic associations, incorporate parameters recognizable on the first encounter with a patient with PG without reliance on histopathology and laboratory findings or treatment response. We postulate that this simple mnemonic will have the most utility with non-dermatology clinicians encountering a lesion suspicious for PG. By assisting in differential diagnosis formation, this mnemonic may lead to timelier biopsies and treatment initiation. The limitations of this approach mirror those of other studies and include lower sensitivities in patients with an atypical PG presentation. In conclusion, the 5 P's of PG offer a useful mnemonic for the diagnosis of PG, particularly in the initial clinical diagnosis prior to skin biopsy and treatment.
J Drugs Dermatol. 2019;18(12):1282-1283.
ABSTRACT
INTRODUCTIONPyoderma gangrenosum (PG) is an inflammatory neutrophilic dermatosis which is often difficult to diagnose because of a clini-cal presentation which frequently mimics conditions such as infections, vascular diseases, and malignancies.1 Recently, sev-eral studies have attempted to define the prevalence of clinical manifestations of PG in order to improve diagnostic accuracy.2-4 Utilizing these reports, we offer for consideration a mnemonic of the clinical features of PG, the 5 P's of PG: Painful, Progressive, Purple, Pretibial, Pathergy, and systemic associations (Table 1).
The 5 P's of Pyoderma Gangrenosum FeatureBrett C. Neill MD,ª Edward W. Seger MS,ª Tyler A. Hooton BS,ª Gabrielle Bailey BS,ª Anand Rajpara MD,ª
William V. Stoecker MD MSb
ªDivision of Dermatology, University of Kansas Medical Center, Kansas City, KS BDepartment of Dermatology, University of Missouri, Columbia, MO
*This work won First Place in the 9th Annual ARTE Poster Competition at ODAC.
TABLE 1.
The 5 P's in the Clinical Diagnosis of Pyoderma Gangrenosum. Numbers reported as percentage of cases expressing each clinical finding; Data reported for any location on the legs for Binus et al and Maverakis et al (most PG lesions on the legs are pretibial); 55% of cases had multiple ulcers with at least one on anterior lower leg; Maverakis et al criterion definition: Papule, pustule, or vesicle that rapidly ulcerates.
FindingLiterature Source
Binus Maverakis Jockenhöfer Ahronowitz Ashchyan Brooklyn Kridin Xia
Purple (undermined) borders -- 91% 98% -- -- -- -- --
Painful 64% 91% 88% -- 86.2% -- -- --
Pretibial2/ Peristomal 77.7%/-- -- -- 61.8%/18.3% --/15% -- --
Progressive -- 42% 98% -- 42% -- -- --
Pathergy 31.1% 35% 73% 28.1% -- 16.3%
Gut 34% -- -- 29.6% 41.0% -- 17.6% 44.6%
Arthritis 29.1% -- -- 22% 20.5% -- 12.8% 27.7%
Neoplasm of blood 10.7% -- -- 5.6% 5.9% -- 8.9% 13.3%
This set of key clinical parameters is recognizable on the first en-counter with a patient with PG and is modeled after the widely used 6 P’s of lichen planus (planar, purple, polygonal, pruritic, papules, and plaques).5 Our mnemonic incorporates the most sensitive features from compressive diagnostic algorithms and does so without reliance on histopathology and laboratory find-ings, co-morbidities, or treatment response.4,6 Moreover, the addition of “pretibial” reminds us of the most common location of PG: 78% of patients reported by Binus et al7 and 62% of pa-tients reported by Ashchyan et al8 had lesions on the legs.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
1283
Journal of Drugs in DermatologyDecember 2019 • Volume 18 • Issue 12
B.C. Neill, E.W. Seger, T.A. Hooton
Due to the complex nature of PG diagnosis, we postulate that this simple mnemonic will have the most utility with non-dermatology clinicians encountering a lesion suspicious for PG. By assisting in differential diagnosis formation, this mne-monic may lead to timelier biopsies and treatment initiation. At that time, the utilization of the more precise criteria set forth by Jockenhöfer et al will allow for the dermatologist to more definitively establish a diagnosis of PG.4 The limitations of this concept mirror those of other studies and include lower sensi-tivities in patients with an atypical PG presentation. In addition, by omitting some histopathologic and treatment response crite-ria in the proposed mnemonic, the specificity, inadvertently, will be reduced. However, most of the omitted criteria are not avail-able on initial evaluation. Despite these limitations, we believe this is a useful approach with simplicity that facilitates adoption into clinical practice.
CONCLUSIONThe 5 P’s of PG offers a useful mnemonic for the diagnosis of PG, particularly in the initial clinical diagnosis prior to skin bi-opsy and treatment.
DISCLOSURESNo author has conflicts of interest relevant to the manuscript. There are no funding sources to disclose.
REFERENCES1. Gortel K. Recognizing pyoderma: more difficult than it may seem. Vet Clin
North Am Small Anim Pract. 2013;43(1):1-18. [PMID: 23182321].2. Ahronowitz I, Harp J, Shinkai K. Etiology and management of pyoderma gan-
grenosum: a comprehensive review. Am J Clin Dermatol. 2012;13(3):191-211. [PMID: 22356259].
3. Xia FD, Liu K, Lockwood S, et al. Risk of developing pyoderma gangrenosum after procedures in patients with a known history of pyoderma gangreno-sum-A retrospective analysis. J Am Acad Dermatol. 2018;78(2):310-4 e1. [PMID: 28947285].
4. Jockenhofer F, Wollina U, Salva KA, et al. The PARACELSUS score: a novel diagnostic tool for pyoderma gangrenosum. Br J Dermatol. 2018. [PMID: 29388188].
5. Le Cleach L, Chosidow O. Clinical practice. Lichen planus. N Engl J Med. 2012;366(8):723-32. [PMID: 22356325].
6. Maverakis E, Ma C, Shinkai K, et al. Diagnostic criteria of ulcerative pyo-derma gangrenosum: a Delphi consensus of international experts. JAMA Dermatol. 2018;154(4):461-6. [PMID: 29450466].
7. Binus AM, Qureshi AA, Li VW, Winterfield LS. Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol. 2011;165(6):1244-50. [PMID: 21824126].
8. Ashchyan HJ, Butler DC, Nelson CA, et al. The association of age with clini-cal presentation and comorbidities of pyoderma gangrenosum. JAMA Der-matol. 2018;154(4):409-13. [PMID: 29450453].
AUTHOR CORRESPONDENCE
Brett C. Neill MDE-mail:................……...................... [email protected]
JDDFacial Skin Tightening With Microfocused
Ultrasound and Dermal Fillers :
Considerations for Patient Selection and Outcomes
STILLAVAILABLE
Facial Skin Tightening With Microfocused Ultrasound
and Dermal FillersConsiderations for Patient Selection
and Outcomes
This continuing education enduring activity is supported by an educational grant provided by
Merz North America, Inc.
Available now in the JDD CME Library: www.JDDonline.com/CME
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Thank you also to our
educational partner
Aurora Diagnostics for their
continued support of the
Dermpath components of
Derm In-Review.
DermInReview.com
Derm In-Review welcomes our
advertising supporters and thanks
them for their commitment to
resident education.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Senior Resident Peer-to-Peer Case Studies
A 56-year old Hispanic female is referred by her PCP for evaluation of a new suspicious, dark lesion on her right plantar foot. She initially noticed the lesion 6 months ago but was told that the lesion was a benign nevus. Dermoscopy shows the following pattern. An excisional biopsy is performed and the patient is subsequently diagnosed with Stage 2A acral lentiginous melanoma. This type of melanoma is more likely to show a mutation in which gene?
3)
For more practice Q&A and Board prep study tools—visit DermInReview.com
Case Studies authored by our educational partner GW School of Medicine and Health Sciences Dermatology Residency Program
A 22-year old male presents to clinic for evaluation of a changing lesion on the posterior shoulder. He reports possible trauma to the area several months prior, and recently noticing that the lesion has increased in size. A biopsy was performed and histopathology revealed the following diagnosis. What is the treatment of choice?
2)
Wide local excision with 4mm marginsMohs micrographic surgeryWide local excision with 1cm marginsDo nothing. Explain to the patient that this lesion is benign and has a low risk of malignant transformation.
NRASGNAQC-KITBRAF
A.B.C.D.
A.B.C.D.
A 72-year-old male with a recent biopsy that showed a nodular basal cell carcinoma on the left nasal ala presents for Mohs micrographic surgery. Due to the location of the surgical defect after two stages, a flap was chosen for closure. What is not a disadvantage of this type of flap?
1)
Risk of pincushioning (trapdoor effect)Requires tacking suturesHeavy flap causing secondary tension vectorsBlunting of nasal alar crease
A.B.C.D.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
Senior Resident Peer-to-Peer Case Studies
Misty Eleryan, MDGW School of Medicine and Health Sciences, Department of Dermatology
Angelo Landriscina, MDGW School of Medicine and Health Sciences, Department of Dermatology
Answers
1)
The content of these case studies, ideal to review during peer study groups, was developed by Misty Eleryan, MD and Angelo Landriscina, MD under the guidance of dermatologist Adam Friedman, MD, FAAD, Associate Professor of Dermatology, Residency Program Director, Director of Translational Research, Department of Dermatology GW University.
Explanation/Literature Review
This is an illustration of a nasolabial (melolabial) transposition flap. Transposition flaps are complex and technically challenging because they recruit tissue from donor sites that are incised and lifted over intact (uninvolved) skin and placed into the primary defect. These flaps redirect primary tension vectors onto the donor site which results in a primary defects closed under minimal to no tension. Examples of the most commonly used transposition flaps in Mohs micrographic surgery are rhombic, bilobed, Z-plasty, and nasolabial (melolabial) transposition flaps. They are all considered single-stage transposition flaps.
Rhombic transposition flaps are most useful for medial and lateral canthi, cheeks, and upper 2/3rd of the nose. Bilobed transposition flaps can be used on the distal nose. Nasolabial flaps are useful for medium-sized defects on the lateral and central nasal ala. Z-plasty is utilized for improving the cosmetic appearance of scars crossing relaxed skin tension lines or releasing contractures by redistributing tension over the wound.
Advantages of these flaps include the ability to displace tension away from the primary defect and nearby free margins. Transposition flaps also are able to reorient tension vectors in favorable directions. Disadvantages of this type of flap are blunting of the alar crease and pincushioning (also known as “trapdoor effect”). A trapdoor deformity occurs when you have an elevated tissue deformity within a U-, C-, or V-shaped flap. The trapdoor effect can be minimized with tacking sutures to decrease the dead space between the flap and recipient site, thinning of the flap, undersize the flap, and wide undermining of the recipient site widely. Other possible complications include edema, postoperative infection, flap necrosis, hematoma, and hypertrophic scar or keloid.
The correct answer is C: Heavy flap causing secondary tension vectors.
2)Explanation/Literature Review
Dermatofibrosarcoma protuberans (DFSP) is a relatively uncommon soft tissue tumor with intermediate to low-grade malignancy potential. Fewer than 5 percent of cases metastasize; however, all variants have an increased potential for local recurrence. It presents as a slow-growing pink or violaceous large plaque or nodule that evolves into a multinodular lesion in young to middle-aged adults. The most commonly affected location is the trunk, followed by the extremities.
The characteristic cytogenic features of DFSP is a reciprocal chromosomal translocation t(17;22)(q22;q13), resulting in a fusion of the platelet-derived growth factor B (PDGFB) gene at 22q13 and the collagen type 1 alpha 1 (COL1A1) at 17q22. Imantinib is the target therapy for PDGFB, which is the basis for its use in the treatment of metastatic DFSP tumors.
On histology, you will see monotonous spindle cells in a storiform appearance in the dermis and subcutaneous fat, with a characteristic “honeycomb” infiltration of fat. Cells are strongly positive for CD34 but negative for Factor XIIIa, stromelysin-3, and D2-40.
Mohs micrographic surgery is the treatment of choice, but wide local extension with 2 cm margins is also acceptable. Treatment with mms is associated with a much lower risk of locoregional recurrence when compared to WLE (1% vs. up to 15%, respectively).
The correct answer is B. Mohs micrographic surgery.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
3)
Explanation/Literature Review
Superficial spreading melanoma and nodular melanoma are the most common types of melanoma seen in fair-skinned individuals; however, acral lentiginous melanoma (ALM) is the most common subtype of cutaneous melanoma in skin of color patients. It often presents as a brown or black patch with irregular borders on acral sites. Ultraviolet radiation (UVR) does not seem to play a major role in the development of ALM. Multiple studies have reported a steady incidence of ALM in the United States in contrast the other subtypes of cutaneous melanoma, which have shown a slight increase over time. Unfortunately, patients typically present with increased tumor thickness and more advanced stage at the time of diagnosis. On dermoscopy, a parallel ridge pattern (pigmentation predominantly on the ridges) is indicative of an acral melanoma.
There are known patterns of genetic alterations within the various melanoma subtypes, which include varying chromosomal aberrations and gene mutations. BRAF and NRAS mutations are the most common aberrations in cutaneous melanoma. KIT mutations are associated with acral and mucosal melanomas. BRAF mutations are associated with superficial spreading melanomas, while nodular melanomas demonstrate NRAS mutations. Uveal melanomas can show mutations in both GNAQ/GNA11. Chronically sun-damaged skin may also be more prone to NRAS and KIT mutations, as opposed to BRAF mutations in non-chronically sun-damaged skin.
The correct answer is C. C-KIT.
Senior Resident Peer-to-Peer Case Studies
References Question 11. Alikhan A, et al. Review of Dermatology. Elsevier. 2017. ISBN: 978-0-323-29672-42. Bednarek RS, Ramsey ML. Transposition flaps. 2019 Jan. PMID: 297632043. Koranda FC and Webster, RC. Trapdoor effect in nasolabial flaps: causes and corrections. Arch Otolaryngol.
1985;111(7):421-424. doi:10.1001/archotol.1985.00800090035002
Image Sources:1. Bayer J, Schwarzmannová K, Dušková M, Novotná K, Kníže J, Sukop A. The nasolabial flap: The most versatile method in
facial reconstruction. Acta Chir Plast. Spring 2018;59(3-4):135-141. 2. Hale CS. Skin nonmelanocytic tumor: Fibrous, fibrohistiocytic and myofibroblastic neoplasms. Dermatofibrosarcoma
protuberans (DFSP). Pathology outlines. 1 Sept 2012 (online)3. Ashman N. Acral lentiginous melanoma dermoscopy. DermNet NZ. June 2019
References Question 21. Larbcharoensub N, et al. Cinicopathological features of dermatofibrosarcoma protuberans. Oncology Letters 2016;11:661-7.2. Jain S. Dermatology: Illustrated study guide and comprehensive board review. Second edition. Benign and malignant
tumors. ISBN: 978-3-319-47393-2
References Question 31. Hafliger, EM, et al. Metastatic acral lentiginous melanoma in a tertiary referral center in Switzerland: a systematic
analysis. Melanoma Res. 2018; 28(5):442-450. 2. Whiteman DC, Pavan WJ, Bastian BC. The melanomas: a synthesis of epidemiological, clinical, histopathological, genetic,
and biological aspects, supporting distinct subtypes, causal pathways, and cells of origin. Pigment Cell Melanoma Res 2011; 24:879–897.
3. Alikhan A, et al. Review of Dermatology. Elsevier. 2017. ISBN: 978-0-323-29672-4
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
December 2019 1288 Volume 18 • Issue 12
Copyright © 2019 FEATURED CONTENT Journal of Drugs in Dermatology
PIPELINE PREVIEWS
The Skin Cancer Foundation Raises More Than $700,000 at Annual Champions for Change Gala
On October 17, The Skin Cancer Foundation held its 23rd annual Gala at The Plaza Hotel in New York City. The Champions for Change Gala is the Foundation’s signature fundraising event, and more than $700,000 was raised to support the organization’s educational campaigns, community programs and research initiatives.
More than 400 guests attended the event, including Skin Cancer Foundation donors, industry and physician allies, celebrity supporters and members of the media. Skin Cancer Foundation President Deborah S. Sarnoff, MD, reflected on the Foundation’s 40th birthday and its plans for the future. “The challenges we face today are different from those we faced forty years ago,” said Dr. Sarnoff. “There have been many changes in how we approach our work, but our goal has stayed the same: to change behaviors and save lives.” The Gala was chaired by Susan Manber (chief strategy officer, Digitas Health) and Stephanie and Adam Schweitzer (partner/board member, ICM Partners). The honorary chair was Marcia Robbins-Wilf, EdD. The Gala Committee included Chris G. Adigun, MD, Jeremy Brauer, MD, Kim Campbell, Amy Conway, Doris Day, MD, Andrew Donovan, Megan Driscoll, Jennifer and Joseph A. Dussich, Dendy Engelman Thomas, MD, April Franzino, Adele Haimovic, Elizabeth K. Hale, MD, Rob Hoxie, Julie K. Karen, MD, Jesse M. Lewin, MD, Melissa Lovy, Celine Mactaggart, Kim Nichols, MD, Ariel Ostad, MD, Isabelle Raymond, PhD, Maral Skelsey, MD, Mary L. Stevenson, MD, Shelley N. Tanner, Brian Underwood and Kit Wallace. The Skin Cancer Foundation is the only global organization solely devoted to the prevention, early detection and treatment of skin cancer. The mission of the Foundation is to decrease the incidence of skin cancer through public and professional education and research. Since its inception in 1979, the Foundation has recommended following a complete sun protection regimen that includes seeking shade and covering up with clothing, including a wide-brimmed hat and UV-blocking sunglasses, in addition to daily sunscreen use. For more information, visit SkinCancer.org.
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
BRIEF SUMMARY OF PRESCRIBING INFORMATIONThis Brief Summary does not include all the information needed to prescribe DUOBRII safely and effectively. See full Prescribing Information for DUOBRII.
DUOBRII™ (halobetasol propionate and tazarotene) Lotion, 0.01%/0.045% for topical useINDICATIONS AND USAGE DUOBRII (halobetasol propionate and tazarotene) Lotion, 0.01%/0.045% is indicated for the topical treatment of plaque psoriasis in adults.CONTRAINDICATIONSPregnancy DUOBRII Lotion is contraindicated in pregnancy [see Warnings and Precautions and Use in Specific Populations].WARNINGS AND PRECAUTIONSEmbryofetal RiskBased on data from animal reproduction studies, retinoid pharmacology, and the potential for systemic absorption, DUOBRII Lotion may cause fetal harm when administered to a pregnant female and is contraindicated during pregnancy. Tazarotene is teratogenic, and it is not known what level of exposure is required for teratogenicity in humans [see Contraindications and Clinical Pharmacology]. Tazarotene elicits teratogenic and developmental effects associated with retinoids after topical or systemic administration in rats and rabbits [see Use in Specific Populations]. Advise pregnant females of the potential risk to a fetus. Obtain a pregnancy test within 2 weeks prior to DUOBRII Lotion therapy. Initiate DUOBRII Lotion therapy during a menstrual period. Advise females of reproductive potential to use effective contraception during treatment with DUOBRII Lotion therapy [see Use in Specific Populations]. Hypothalamic-Pituitary-Adrenal (HPA) Axis Suppression and Other Unwanted Systemic Glucocorticoid EffectsDUOBRII Lotion contains halobetasol propionate, a corticosteroid, and has been shown to suppress the hypothalamic-pituitary-adrenal (HPA) axis. Systemic effects of topical corticosteroids may include reversible HPA axis suppression with the potential for glucocorticosteroid insufficiency. This may occur during treatment or upon withdrawal of treatment of the topical corticosteroid. The potential for hypothalamic-pituitary-adrenal (HPA) axis suppression with DUOBRII Lotion was evaluated in a study of 20 adult subjects with moderate to severe plaque psoriasis involving ≥20% of their body surface area. The subjects were treated once daily for 8 weeks and assessed for HPA axis suppression at Weeks 4 and 8. HPA axis suppression occurred in 3 out of 20 (15%) subjects at Week 4 and none (0%) of these 20 subjects had HPA axis suppression at Week 8 [see Clinical Pharmacology in full Prescribing Information]. Because of the potential for systemic absorption, use of topical corticosteroids, including DUOBRII Lotion, may require that patients be evaluated periodically for evidence of HPA axis suppression. Factors that predispose a patient using a topical corticosteroid to HPA axis suppression include the use of more potent corticosteroids, use over large surface areas, occlusive use, use on an altered skin barrier, concomitant use of multiple corticosteroid-containing products, liver failure, and young age. An adrenocorticotropic hormone (ACTH) stimulation test may be helpful in evaluating patients for HPA axis suppression. If HPA axis suppression is documented, attempt to gradually withdraw the drug or reduce the frequency of application. Manifestations of adrenal insufficiency may require supplemental systemic corticosteroids. Recovery of HPA axis function is generally prompt and complete upon discontinuation of topical corticosteroids. Systemic effects of topical corticosteroids may also include Cushing’s syndrome, hyperglycemia, and glucosuria. Use of more than one corticosteroid-containing product at the same time may increase the total systemic exposure to topical corticosteroids. Pediatric patients may be more susceptible than adults to systemic toxicity from the use of topical corticosteroids because of their larger surface-to-body mass ratio [see Use in Specific Populations]. Local Adverse ReactionsLocal adverse reactions may include atrophy, striae, telangiectasias, folliculitis and contact dermatitis. Some local adverse reactions may be irreversible. If these adverse reactions occur, discontinue the medication at least until the integrity of the skin is restored; do not resume treatment if allergic contact dermatitis is identified. Avoid use of DUOBRII Lotion on eczematous skin, as it may cause severe irritation. Photosensitivity and Risk for SunburnBecause of heightened burning susceptibility, exposure to sunlight (including sunlamps) should be avoided unless deemed medically necessary, and in such cases, exposure should be minimized during the use of DUOBRII Lotion. Patients must be instructed to use sunscreens and protective clothing when using DUOBRII Lotion. Patients with sunburn should be advised not to use DUOBRII Lotion until fully recovered. Patients who may have considerable sun exposure due to their occupation and those patients with inherent sensitivity to sunlight should exercise particular caution when using DUOBRII Lotion. DUOBRII Lotion should be administered with caution if the patient is also taking drugs known to be photosensitizers (e.g., thiazides, tetracyclines, fluoroquinolones, phenothiazines, sulfonamides) because of the increased possibility of augmented photosensitivity. Ophthalmic Adverse Reactions Use of topical corticosteroids may increase the risk of posterior subcapsular cataracts and glaucoma. Cataracts and glaucoma have been reported postmarketing with the use of topical corticosteroid products. Advise patients to report any visual symptoms and consider referral to an ophthalmologist for evaluation. Concomitant Skin Infections Use an appropriate antimicrobial agent if a skin infection is present or develops. If a favorable response does not occur promptly, discontinue use of DUOBRII Lotion until the infection has been adequately treated.
ADVERSE REACTIONSClinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. In randomized, double-blind, multicenter, vehicle-controlled clinical trials, 410 adults with plaque psoriasis were treated with DUOBRII Lotion or vehicle lotion and had post-baseline safety data. Subjects applied DUOBRII Lotion or vehicle lotion once daily for up to eight weeks. The adverse reactions occurring in ≥1% of the subjects treated with DUOBRII through Week 8 were contact dermatitis (7%), application site pain (3%), folliculitis (2%), skin atrophy (2%), and excoriation (2%). USE IN SPECIFIC POPULATIONSPregnancyRisk SummaryBased on data from animal reproduction studies, retinoid pharmacology, and the potential for systemic absorption, DUOBRII Lotion may cause fetal harm when administered to a pregnant female and is contraindicated during pregnancy. Safety in pregnant females has not been established. The potential risk to the fetus outweighs the potential benefit to the mother from DUOBRII Lotion during pregnancy; therefore, DUOBRII Lotion should be discontinued as soon as pregnancy is recognized [see Contraindications, Warnings and Precautions, Clinical Pharmacology].Observational studies suggest an increased risk of low birthweight in infants with the maternal use of potent or very potent topical corticosteroids (see Data).In animal reproduction studies with pregnant rats, reduced fetal body weights and reduced skeletal ossification were observed after topical administration of a tazarotene gel formulation during the period of organogenesis at a dose 11 times the maximum recommended human dose (MRHD) (based on AUC comparison). In animal reproduction studies with pregnant rabbits, single incidences of known retinoid malformations, including spina bifida, hydrocephaly, and heart anomalies were observed after topical administration of a tazarotene gel formulation at 116 times the MRHD (based on AUC comparison) (see Data).In animal reproduction studies with pregnant rats and rabbits, malformations, fetal toxicity, developmental delays, and/or behavioral delays were observed after oral administration of tazarotene during the period of organogenesis at doses 9 and 228 times, respectively, the MRHD (based on AUC comparison). In pregnant rats, decreased litter size, decreased numbers of live fetuses, decreased fetal body weights, and increased malformations were observed after oral administration of tazarotene prior to mating through early gestation at doses 9 times the MRHD (based on AUC comparison) (see Data).In animal reproduction studies, increased malformations, including cleft palate and omphalocele, were observed after oral administration of halobetasol propionate during the period of organogenesis to pregnant rats and rabbits (see Data). The available data do not support relevant comparisons of systemic halobetasol propionate exposures achieved in the animal studies to exposures observed in humans after topical use of DUOBRII Lotion.The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. The background risk in the U.S. general population of major birth defects is 2 to 4%, and of miscarriage is 15 to 20%, of clinically recognized pregnancies.DataHuman DataAvailable observational studies in pregnant women did not identify a drug-associated risk of major birth defects, preterm delivery, or fetal mortality with the use of topical corticosteroids of any potency. However, when the dispensed amount of potent or very potent topical corticosteroids exceeded 300 g during the entire pregnancy, maternal use was associated with an increased risk of low birth weight in infants.Animal DataHalobetasol propionate has been shown to cause malformations in rats and rabbits when given orally during organogenesis at doses of 0.04 to 0.1 mg/kg/day in rats and 0.01 mg/kg/day in rabbits. Halobetasol propionate was embryotoxic in rabbits but not in rats. Cleft palate was observed in both rats and rabbits. Omphalocele was seen in rats but not in rabbits.In an embryofetal development study in rats, a tazarotene gel formulation, 0.5% (0.25 mg/kg/day tazarotene) was topically administered to pregnant rats during gestation days 6 through 17. Reduced fetal body weights and reduced skeletal ossification occurred at this dose (11 times the MRHD based on AUC comparison). In an embryofetal development study in rabbits, a tazarotene gel formulation, 0.5%, 0.25 mg/kg/day tazarotene) was topically administered to pregnant rabbits during gestation days 6 through 18. Single incidences of known retinoid malformations, including spina bifida, hydrocephaly, and heart anomalies were noted at this dose (116 times the MRHD based on AUC comparison).When tazarotene was given orally to animals, developmental delays were seen in rats; malformations and post-implantation loss were observed in rats and rabbits at doses producing 9 and 228 times, respectively, the MRHD (based on AUC comparisons).In female rats orally administered 2 mg/kg/day of tazarotene from 15 days before mating through gestation day 7, classic developmental effects of retinoids including decreased number of implantation sites, decreased litter size, decreased numbers of live fetuses, and decreased fetal body weights were observed at this dose (16 times the MRHD based on AUC comparison). A low incidence of retinoid-related malformations was observed at that dose.In a pre- and postnatal development toxicity study, topical administration of a tazarotene gel formulation (0.125 mg/kg/day) to pregnant female rats from gestation day 16 through lactation day 20 reduced pup survival but did not affect the reproductive capacity of the offspring. Based on data from another study, the systemic drug exposure in the rat at this dose would be equivalent to 5 times the MRHD (based on AUC comparison).LactationRisk SummaryThere are no data on the presence of tazarotene, halobetasol propionate or its metabolites in human milk, the effects on the breastfed infant, or the effects on milk production after treatment with DUOBRII Lotion.After single topical doses of a 14C-tazarotene gel formulation to the skin of lactating rats, radioactivity was detected in rat milk.
It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in human milk.The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for DUOBRII Lotion and any potential adverse effects on the breastfed child from DUOBRII Lotion.Clinical ConsiderationsAdvise breastfeeding women not to apply DUOBRII Lotion directly to the nipple and areola to avoid direct infant exposure.Females and Males of Reproductive PotentialPregnancy TestingDUOBRII Lotion is contraindicated in women who are pregnant. Females of reproductive potential should be warned of the potential risk and use adequate birth-control measures during treatment with DUOBRII Lotion. The possibility that a female of reproductive potential is pregnant at the time of institution of therapy should be considered. A negative result for pregnancy should be obtained within 2 weeks prior to DUOBRII Lotion therapy, which should begin during menstruation.ContraceptionBased on animal studies, DUOBRII Lotion may cause fetal harm when administered to a pregnant female [see Use in Specific Populations]. Advise females of reproductive potential to use effective contraception during treatment with DUOBRII Lotion. Pediatric UseSafety and effectiveness of DUOBRII Lotion in pediatric patients under the age of 18 years have not been evaluated.Because of higher skin surface area to body mass ratios, pediatric patients are at a greater risk than adults of HPA axis suppression and Cushing’s syndrome when they are treated with topical corticosteroids. They are therefore also at greater risk of adrenal insufficiency during or after withdrawal of treatment. Adverse reactions including striae have been reported with use of topical corticosteroids in infants and children [see Warnings and Precautions].HPA axis suppression, Cushing’s syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in children receiving topical corticosteroids. Manifestations of adrenal suppression in children include low plasma cortisol levels and an absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema [see Warnings and Precautions].Geriatric UseOf the 270 subjects exposed to DUOBRII Lotion in clinical trials, 39 subjects were 65 years or older. Clinical trials of DUOBRII Lotion did not include sufficient numbers of subjects age 65 years and older to determine whether they respond differently from younger subjects. NONCLINICAL TOXICOLOGYCarcinogenesis, Mutagenesis, Impairment of FertilityLong-term animal studies have not been performed to evaluate the carcinogenic potential of halobetasol propionate.A long-term study of tazarotene following oral administration of 0.025, 0.050, and 0.125 mg/kg/day to rats showed no indications of increased carcinogenic risks. Based on pharmacokinetic data from a shorter term study in rats, the highest dose of 0.125 mg/kg/day was anticipated to give systemic exposure in the rat equivalent to 1.4 times the MRHD (based on AUC comparison).A long-term study with topical application of up to 0.1% of tazarotene in a gel formulation in mice terminated at 88 weeks showed that dose levels of 0.05, 0.125, 0.25, and 1 mg/kg/day (reduced to 0.5 mg/kg/day for males after 41 weeks due to severe dermal irritation) revealed no apparent carcinogenic effects when compared to vehicle control animals. Tazarotenic acid systemic exposure at the highest dose was 35 times the MRHD (based on AUC comparison).Halobetasol propionate was not genotoxic in the Ames assay, in the sister chromatid exchange test in Chinese hamster somatic cells, in chromosome aberration studies of germinal and somatic cells of rodents, and in a mammalian spot test. Positive mutagenicity effects were observed in a mouse lymphoma gene mutation assay in vitro and in a Chinese hamster micronucleus test.Tazarotene was non-mutagenic in the Ames assay and did not produce structural chromosomal aberrations in human lymphocytes. Tazarotene was non-mutagenic in the CHO/HGPRT mammalian cell forward gene mutation assay and was non-clastogenic in an in vivo mouse micronucleus test.Studies in rats following oral administration of halobetasol propionate at dose levels up to 0.05 mg/kg/day, approximately 0.53 times the MRHD based on BSA comparisons, indicated no impairment of fertility or general reproductive performance.No impairment of fertility occurred in rats when male animals were treated for 70 days prior to mating and female animals were treated for 14 days prior to mating and continuing through gestation and lactation with topical doses of a tazarotene gel formulation up to 0.125 mg/kg/day. Based on data from another study, the systemic drug exposure in the rat at the highest dose was 5 times the MRHD (based on AUC comparison).No impairment of mating performance or fertility was observed in male rats treated for 70 days prior to mating with oral doses of up to 1 mg/kg/day tazarotene, which produced a systemic exposure 17 times the MRHD (based on AUC comparison).No impairment of mating performance or fertility was observed in female rats treated for 15 days prior to mating and continuing through gestation day 7 with oral doses of tazarotene up to 2 mg/kg/day. However, there was a significant decrease in the number of estrous stages and an increase in developmental effects at that dose, which produced a systemic exposure 30 times the MRHD (based on AUC comparison).Manufactured for:Bausch Health Americas, Inc. Bridgewater, NJ 08807 USABy:Bausch Health Companies Inc. Laval, Quebec H7L 4A8, Canada U.S. Patent Numbers: 6,517,847; 8,809,307 and 10,251,895 DUOBRII is a trademark of Ortho Dermatologics’ affiliated entities.©2019 Bausch Health Companies Inc. or its affiliates. DUO.0039.USA.18 Based on 9645601
VALE4457 DuobriiLaunch JDD B/WPage Live: .125"fromTrim Fileformat:PDF/X-1a CarlingCommunications 7/15/19Trim: 8.25"x10.875"Bleed: 8.5"x11.125”
Do Not CopyPenalties Apply

Previous Page | Contents | Zoom In | Zoom Out | Search Issue | Cover | Next Page
The only FDA-approved treatment with a potent-to-superpotent steroid that can be used until control is achieved
The effi cacy and safety of DUOBRII Lotion was investigated in two 8-week clinical trials and an additional 1 year safety study.1,3
Discontinue treatment with DUOBRII Lotion when control is achieved or if atrophy, striae, telangiectasias, or folliculitis occurs.1
Halobetasol (0.01%) Provides powerful
antiinfl ammatory effects and reduces skin irritation, which is
often associated with retinoids1,4,5
The fi rst and only steroid/retinoid therapy, allowing halobetasoland tazarotene to work together in an advanced, once-daily lotion that can be dosed to clearance1-3
American Academy of Dermatology (AAD) Guidelines give the combination of a corticosteroid and a retinoid an A rating with Evidence Level I for the treatment of psoriasis4
®/TM are trademarks of Ortho Dermatologics’ affi liated entities. ©2019 Ortho Dermatologics’ affi liated entities. DUO.0052.USA.18
Please see Brief Summary of full Prescribing Information on the following page.
References 1. DUOBRII Lotion [prescribing information]. Bridgewater, NJ: Bausch Health US, LLC. 2. Food and Drug Administration. Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. https://www.accessdata.fda.gov/scripts/cder/ob/index.cfm. Accessed April 29, 2019. 3. Data on fi le. 4. Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 3. Guidelines of care for the management and treatment of psoriasis with topical therapies. J Am Acad Dermatol. 2009;60(4):643-659. 5. Orfanos CE, Schmidt HW, Mahrle G, et al. Retinoic acid in psoriasis: its value for topical therapy with and without corticosteroids: clinical, histological and electron microscopical studies on forty-four hospitalized patients with extensive psoriasis. Br J Dermatol. 1973;88(2):167-182. 6. Lesnik RH, Mezick JA, Capetola R, Kligman LH. Topical all-trans-retinoic acid prevents corticosteroid-induced skin atrophy without abrogating the anti-infl ammatory e� ect. J Am Acad Dermatol. 1989;21(2 Pt 1):186-190. 7. Weinstein GD, Krueger GG, Lowe NJ, et al. Tazarotene gel, a new retinoid, for topical therapy of psoriasis: vehicle-controlled study of safety, e� cacy, and duration of therapeutic e� ect. J Am Acad Dermatol. 1997;37(1):85-92.
Learn more at DUOBRII.com
IndicationDUOBRII™ (halobetasol propionate and tazarotene) Lotion, 0.01%/0.045%, is indicated for the topical treatment of plaque psoriasis in adults.
Important Safety InformationContraindication DUOBRII Lotion is contraindicated in pregnancy.
Warnings and Precautions• Women of child-bearing potential should be warned of the
potential risk of fetal harm from DUOBRII and use adequate birth-control. A negative result for pregnancy should be obtained within 2 weeks prior to treatment. If the patient becomes pregnant during treatment, discontinue DUOBRII Lotion and advise patient of the potential hazard to the fetus.
• DUOBRII Lotion has been shown to suppress the hypothalamic-pituitary-adrenal (HPA) axis during or after treatment and may require that patients be evaluated periodically during treatment.
• Predisposing factors for HPA axis suppression include: use of more potent corticosteroids, use on large areas, use under occlusive dressings, use on altered skin barrier, concomitant use of other steroids, liver failure and young age.
• Systemic e� ects of topical corticosteroids may also include Cushing’s syndrome, hyperglycemia, and glucosuria.
• Local adverse reactions may include atrophy, striae, telangiectasias, folliculitis and contact dermatitis. If these e� ects occur, discontinue until the integrity of the skin has been restored. Do not resume treatment if contact dermatitis is identifi ed. DUOBRII Lotion should not be used on eczematous skin, as it may cause severe irritation.
• Avoid exposure to sunlight, sunlamps and weather extremes. Patients with sunburn should be advised not to use DUOBRII Lotion until fully recovered. DUOBRII Lotion should be administered with caution if the patient is also taking drugs known to be photosensitizers because of the increased potential for photosensitivity.
• Topical corticosteroids may increase the risk of cataracts and glaucoma; advise patients to report any visual symptoms and refer to an ophthalmologist if needed.
Adverse Events • The most common adverse events in clinical trials were contact
dermatitis (7%), application site pain (3%), folliculitis (2%), skin atrophy (2%), and excoriation (2%).
To report SUSPECTED ADVERSE REACTIONS, contact Ortho Dermatologics at 1-800-321-4576 or FDA at 1-800-FDA-1088 or visit www.fda.gov/medwatch.
bettertogetherFor adults with plaque psoriasis
Tazarotene (0.045%) Regulates cell growth and specialization to reduce hyperproliferation, increases collagen, and extends remission post treatment4,6,7
The only FDA-approved treatment with a potent-to-superpotent steroid that can be used until control is achieved
Tazarotene (0.045%) Regulates cell growth and specialization to reduce hyperproliferation, increases collagen, and extends remission post treatment
mechanisms of change
VALE4457 DuobriiLaunch JDD 4/CPage Live: .125"fromTrim Fileformat:PDF/X-1a CarlingCommunications 7/15/19Trim: 8.25"x10.875"Bleed: 8.5"x11.125”
Do Not CopyPenalties Apply