Your Benefits - Three Options All of the benefits provided ...
19
-
Upload
maxisurgeon -
Category
Documents
-
view
204 -
download
2
description
Transcript of Your Benefits - Three Options All of the benefits provided ...

Your Benefits - Three Options
Basic Basic Plus Flex
Who provides services?
Delta Dental PPO Dentists
Delta Dental PPO Dentists
Delta Dental PPO Dentists or any other dentist you choose
What services are covered?
Preventive and basic care including cleanings, x-rays, fluoride treatments, sealants, fillings and extractions.
All of the benefits provided under the Basic Option plus major services including bridges, dentures, crowns, periodontics, endodontics and orthodontics for children (up to age 19 only).
All of the benefits provided under the Basic Plus option plus the availability to use ANY dentist.The Flex Option also includes a higher level of benefits on many services and adult orthodontic benefits.

Delta Networks
800 Local PPO dental offices
1700 Local Premier dental offices
Basic and Basic Plus members use the PPO network exclusively while Flex Option members can choose
Premier and non-participating dentists as well.

Delta Dental PPO Network• No balance billing• Dentist submits claim paperwork• Minimal out of pocket expenses• Over 600 general dentists to
choose from in the St. Louis area
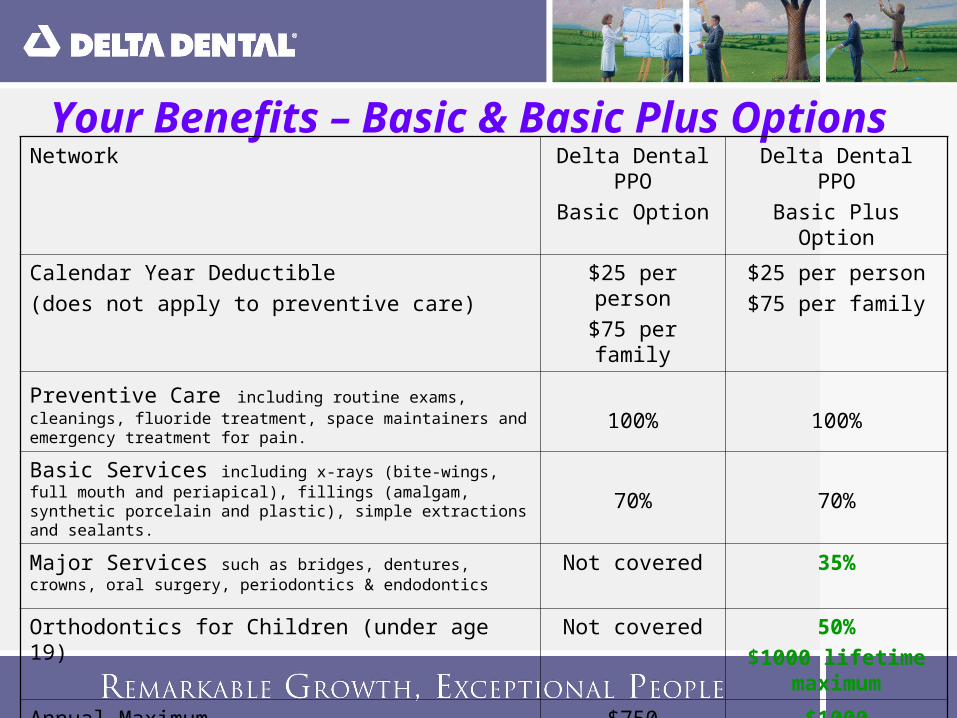
Your Benefits – Basic & Basic Plus OptionsNetwork Delta Dental
PPOBasic Option
Delta Dental PPOBasic Plus Option
Calendar Year Deductible (does not apply to preventive care)
$25 per person$75 per family
$25 per person$75 per family
Preventive Care including routine exams, cleanings, fluoride treatment, space maintainers and emergency treatment for pain.
100% 100%
Basic Services including x-rays (bite-wings, full mouth and periapical), fillings (amalgam, synthetic porcelain and plastic), simple extractions and sealants. 70% 70%
Major Services such as bridges, dentures, crowns, oral surgery, periodontics & endodontics
Not covered 35%
Orthodontics for Children (under age 19) Not covered 50%$1000 lifetime
maximum
Annual Maximum $750 $1000

Your Benefits – Flex OptionNetwork Delta Dental PPO Out of PPO
network dentists (including Delta Premier dentists)
Calendar Year Deductible (does not apply to preventive care)
$50 per person$150 per family
$50 per person$150 per family
Preventive Care including routine exams, x-rays, cleanings, fluoride treatment, space maintainers and emergency treatment for pain.
100% 100%
Basic Services including , fillings, sealants, simple and surgical extractions, oral surgery, periodontics and endodontics. 90% 80%
Major Services such as bridges, dentures, and crowns.
60% 50%
Orthodontics for Adults and Children 50%; $1000 lifetime maximum
50%; $1000 lifetime maximum
Annual Maximum $1000 $1000
• Claims finalized in 3.3 days (average)
• 99.9% accuracy
Outstanding Speed and Accuracy

Procedure code 2150 – two surface amalgam filling
Submitted DPO scheduled Delta Dental pays Patient paysamount amount (70% of $65) (30% of $65)
$136.00 $65.00 $45.50 $19.50
Example: a Delta Dental PPO dentist installs a two surface amalgam filling on a patient. Patient has 70% coverage for basic services.
Delta Dental PPO Network – Basic Options
This calculation is for illustration purposes only, it does not reflect actual fees.

Procedure code 2150 – two surface amalgam filling
Submitted DPO scheduled Delta Dental pays Patient paysamount amount (90% of $65) (10% of $65)
$136.00 $65.00 $58.50 $6.50
Example: a Delta Dental PPO dentist installs a two surface amalgam filling on a patient. Patient has 90% coverage for basic services.
Delta Dental PPO Network – Flex Option
This calculation is for illustration purposes only, it does not reflect actual fees.
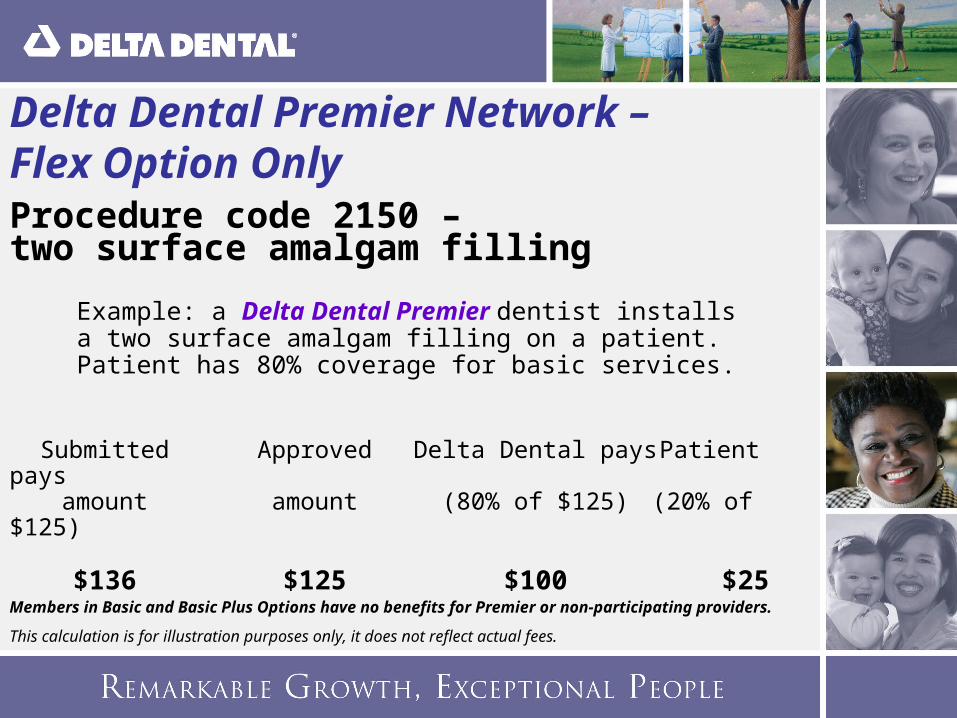
Procedure code 2150 – two surface amalgam filling
Submitted Approved Delta Dental pays Patient paysamount amount (80% of $125) (20% of
$125)
$136 $125 $100 $25
Example: a Delta Dental Premier dentist installs a two surface amalgam filling on a patient. Patient has 80% coverage for basic services.
Members in Basic and Basic Plus Options have no benefits for Premier or non-participating providers.
This calculation is for illustration purposes only, it does not reflect actual fees.
Delta Dental Premier Network – Flex Option Only

Procedure code 2150 – two surface amalgam filling
Submitted Approved Delta Dental pays Patient pays
amount amount (80% of $128) *$136 $128 $102.40 $33.60
* 20% of $128 ($25.60) - plus the difference between the approved amount and the dentist’s charges ($8)
Example: a nonparticipating dentist installs a two surface amalgam filling on a patient. Patient has 80% coverage for basic services.
Members in Basic and Basic Plus Options have no benefits for Premier or non-participating providers.
This calculation is for illustration purposes only, it does not reflect actual fees.
Delta Dental Nonparticipating – Flex Option Only
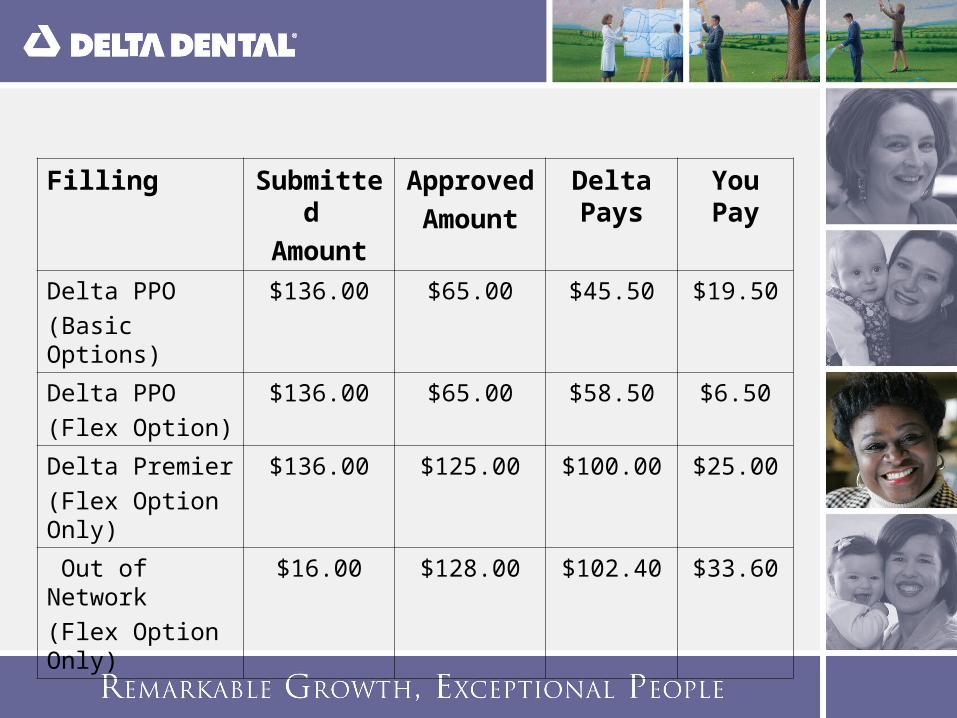
Filling Submitted
Amount
Approved
Amount
Delta Pays
You Pay
Delta PPO(Basic Options)
$136.00 $65.00 $45.50 $19.50
Delta PPO(Flex Option)
$136.00 $65.00 $58.50 $6.50
Delta Premier(Flex Option Only)
$136.00 $125.00 $100.00 $25.00
Out of Network(Flex Option Only)
$16.00 $128.00 $102.40 $33.60

• 99.8% - solutions on first call
• Over 98% of customers satisfied with service
• Average speed of answer: 8 seconds
• 96% answered in 30 seconds
• Abandon rate: 0.6%
• Average 14 years experience
• Minimal turnover
Unrivaled Customer Service
1-800-335-8266
• 24/7 access to benefit and claims information:
– Benefit24 online at www.deltadentalmo.com
– Benefit24 VRU • Faxback – summary of benefits
Ease and Convenience
For members and dentists:
–Participating dentists–Claims status and history–Copy of EOB–Benefit design–Track use of maximums–Print ID cards
State-of-the-art Web-based Service

Find a Dentist . . .

Benefits OPTION 1Flex Option
OPTION 2Basic Plus Option
OPTION 3Basic Option
Type of Plan Delta Dental PPO Delta Dental PPO(with no out of
network benefit)
Delta Dental PPO(with no out of
network benefit)
Network Considerations In PPO Network
Out of PPO Network
(Delta Premier Network or Non-participating providers)
In Delta Dental PPO Network Only
In Delta Dental PPO Network Only
Co-Insurance (Plan Pays)
Type A: Preventive Care 100% 100% 100% 100%
Type B: Basic Restorative Services
90% 80% 70% 70%
Type C: Major Restorative Services
60% 50% 35% Not Covered
Type D: Orthodontics 50% 50% 50% Not Covered
Deductible
Applies to: B & C Services B & C Services B & C Services B Services
Per Person $50 $50 $25 $25
Per Family $150 $150 $75 $75
Annual Maximum Per Person $1000 $1000 $1000 $750
Lifetime Orthodontia Maximum
$1000Adult & Child
$1000Adult & Child
$1000Child Only
Not Covered
Rates:
Employee $25.14 $16.41 $11.63
Employee + 1 $49.21 $31.15 $22.76
Family $84.24 $52.98 $40.72

Questions?