Year 1 Mh linical Skills Session · Dividing lines for the nine regions of the abdomen Upper border...
18
Year 1 MBChB Clinical Skills Session Gastrointestinal examination Wrien by: The Clinical Skills Lecture Team Reviewed & rafied by: Professor C Halloran (Gastroenterology System Lead) and Dr P Collins Consultant Gastroenterologists August 2019
Transcript of Year 1 Mh linical Skills Session · Dividing lines for the nine regions of the abdomen Upper border...

Year 1 MBChB
Clinical Skills Session
Gastrointestinal examination
Written by: The Clinical Skills Lecture Team
Reviewed & ratified by: Professor C Halloran (Gastroenterology System Lead) and Dr P Collins Consultant Gastroenterologists
August 2019

Gastrointestinal Examination
Learning objectives
o To revise the anatomy and physiology of the gastrointestinal system
o To link anatomy and physiology to the practical skill
o To understand reasons for undertaking gastrointestinal examination
o To be able to carry out elements of a gastrointestinal examination
Theory and background
A full gastrointestinal (G.I.) examination may include examination of the groins, external genitalia and rectum,
depending on the patient presentation and findings.
If a swelling or enlargement of an organ (organomegaly) is suspected or if you find a pulsatile swelling, please seek
immediate advice from a qualified professional.
Indications for abdominal examination
The following list of reasons is by no means exhaustive, a patient may present with;
o Vomiting
o Trauma
o Abdominal pain
o Change in bowel habit
o Abdominal distension
o Change in appetite
o Anaemia
o Swelling
o Weight loss
o Tenesmus (a continual or recurrent inclination to evacuate the bowels).
o Jaundice (when your skin and the whites of your eyes turn yellow. It can be a sign of something serious,
such as liver disease)
Dividing the abdomen into regions
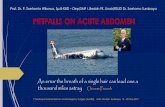
Conventionally the abdomen is divided into 9 regions, there are 4 dividing lines:
midclavicular (2) - vertical
subcostal - upper horizontal
Trans-tubercular - lower horizontal

The 9 regions will each contain their own important organs helping to make diagnosis easier. Think about what
organs are in each of the 9 regions? Answers are at the end of the presentation.
Dividing lines for the nine regions of the abdomen
Upper border of abdomen
The costal margin (rib margin)
demarcates the chest from the
abdomen superiorly
Lower border of abdomen
This is delineated by the
transtubercular line

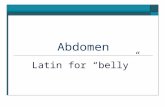
Alternative to 9 regions is to split abdomen into quadrants
The right environment
The room that the examination is taking place in should be private, with the examination couch off set from the
centre of the room. Within the room there should be a further area with curtains / screens around, offering privacy
to the patient whilst they disrobe and wear a clean gown or cover with a blanket to preserve modesty, while they
are examined. There should be a good light source that will adequately illuminate the area being examined.
As this is an intimate examination a chaperone will be present.
o There should be handwashing facilities.
Ideally the patient should be relaxed and in a warm environment, they should lie flat on their back, with hands by
their sides or a single pillow under their head. Hips and knees may be flexed to relax abdominal muscles if
necessary.
The abdomen should be exposed (the whole upper torso to the suprapubic area – inguinal and genital areas are
covered until they are to be examined).
The examiner should position him/herself to be on a level with the abdominal surface.

Patient safety
WHO (2009) http://www.who.int/infection-prevention/tools/hand-hygiene/en/
Prior to any clinical examination a detailed history should be taken from the patient, this will enable you to tailor
the examination to the patients presenting complaint and additional symptoms the patient may elude to when you
elicit a full history. For guidance on history taking please click MBCHB students – Year 1 – History taking.
General Inspection
This can be undertaken with the patient upright, check the patient’s general appearance (demeanour, pallor,
jaundice, cachexia (weakness and wasting of the body due to severe chronic illness), etc)
Include vital signs, check RR, SPO2, temperature, as appropriate. (See vital signs study guide).
Specific inspection
Check the patient’s mouth, teeth, tongue and breath, for example for hydration status, any bleeding, ulcerations,
redness, or any oral or dental infections.
Inspection of the torso should be done with the patient supine, observe for;
o Look for spider naevi [see prep but covered in more detail in 2nd year]
o Gynaecomastia in males [see prep but covered in more detail in 2nd year]
o Scars

o Rashes
o Distension
o Swellings
o Visible peristalsis
o Abdominal wall movement
o Dilated veins [covered in more detail in 2nd year]
Causes of abdominal distension
Flatus (gas) – taut abdomen which is compressible
Faeces – firm to hard mass take note of position as may be normal finding
Fluid (ascites) – taut abdomen which may be non-compressible dependant on volume
Fat – soft and compressible
Foetus – obstetric palpation will be taught in later year
Fairly big tumours - firm to hard mass (Need to be pretty big!)
Percussion
When percussing the general abdomen all areas should be percussed and should sound resonant.
When you percuss over the abdominal organs you would expect the liver, spleen and bladder to be dull. The
kidneys will be resonant due to being retroperitoneal with air filled bowel lying over them.
Palpation
There are 3 elements of abdominal palpation:
o Superficial palpation
o Deep palpation
o Specific organ palpation
When palpating, movement of the examining
hand should be slow and deliberate (no ‘wiggling’
as this would cause pain).
Palpation is performed with the flat of the
fingers, using the knuckles or (metacarpal
pharyngeal) joints as a pivot on the abdomen.

Superficial Palpation
Always start palpation away from any site of pain and always observe patient’s face for signs of discomfort.
Palpate the abdominal regions systematically, preferably at the same height as the patient’s abdomen.
Superficial palpation is using a light pressure to assess for tone, tenderness and any obvious abnormalities.
Assessing muscle tone with superficial palpation
During superficial palpation gentle pressure is
applied to the abdominal wall allowing the examiner
to depress the anterior wall of the abdomen as the
muscles relax, assessing the patient for abdominal
pain and other abnormalities.
Deep palpation
Deep palpation is using firm pressure to assess for
swellings or abnormalities. This must be done with
the palmar aspect of the fingers and you should be
on the same level as the abdomen.
Specific Organ Palpation
These organs are routinely palpated;
o Liver
o Spleen
o Kidneys
This is from the furthest direction enlargement can
occur, towards the position the organ normally lies to
detect enlargement, as explained below.
Palpation of organs

When palpating organs feel for the edges, the edges provide a better contrast between surrounding organs/tissues
and the organ.
Palpation of organs may be assisted by assessment of mobility in relation to respiration, this is because the
diaphragm moves down on inspiration, pushing abdominal organs downwards. If the liver or spleen are enlarged
they may be felt below the costal margin.
o The liver descends towards right iliac fossa on inspiration
o The spleen descends inferio-medially on inspiration towards the right iliac fossa
o The kidneys descend on inspiration








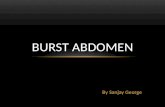
Differentiating kidneys from other organs/masses
The kidneys can be “balloted” this a technique where by a structure that is not fixed can be patted between the
examining hands.

Percussion
Once the liver has been percussed, routinely percuss all other areas of the abdomen to note if there is any pain or
tenderness on percussion.
Report any abnormalities.
Auscultation
Bowel sounds – Borborygmus
Bowels sounds are gurgling noises made by air/ liquid moving through the bowel.
Listen in any area of the abdomen and bowel sounds should be heard, but when examining a patient, listen for 2-3
minutes (or until sounds heard) in the lower right quadrant.
If no sound is heard listen elsewhere on the abdomen for a further 2-3 minutes.
If no sound is heard report the absent bowel sounds immediately to a qualified health care professional.
Answers to the question - what organs are in the 9 regions?
Right hypochondrium – small intestine, right kidney, gallbladder, liver
Left hypochondrium – pancreas, left kidney, colon, spleen
Epigastrium – spleen, pancreas, duodenum, liver, stomach
Right lumbar region – right colon, liver gallbladder
Left lumbar region – left kidney, descending colon

Umbilical – duodenum, ileum, jejunum, umbilicus
Right iliac – caecum, appendix
Left iliac – sigmoid colon, descending colon
Suprapubic – female reproductive organs, sigmoid colon, urinary bladder
Glossary
Borborygmus – Bowel sounds
Cachexia - weakness and wasting of the body due to severe chronic illness
Distension – Swelling
G.I. – Gastrointestinal
Jaundice -when your skin and the whites of your eyes turn yellow. It can be a sign of something serious, such as
liver disease
Left lower quadrant – LLQ
Left upper quadrant – LUQ
Organomegaly – Swelling or enlargement of an organ
Right lower quadrant – RLQ
Right upper quadrant – RUQ
Tenesmus – a continual or recurrent inclination to evacuate the bowels.