Yadral1ko Ducic, FResc - facetransplants.com · I 286 The Journal of Otolaryngology. Volume 28....
3
• Th e Journal of Ot olaryngology, VO/llme 2 8, Number 5, 1999 Case Repo rt s Nasal Glio .................................................................................... .................. . ....... .... .. ... ......... .................. ............. ............................................. ... ........ ... ...... .. ...... . .. .............................. ........... ......... .. ............ ............. ..... ....... Yadral1ko Ducic , MD, FResc N asal encephaloceles and gliomas pres ent along a broad spectrum of severity and deformity. A com- bination of transfacial and intracranial approac h es is often required for the safe and definitive treatment of these anomalies. As a group, congenital midline nasal masses are unusual lesions, having an in cidence of 1 in 20 , 000 to 4 0,000 live births. I Nasa l gliomas, both intranasal and exte rnal, represe nt the l east co mm on subset of these patients with less than 170 cases described in the litera- ture. 2 Th e vaSt ma jo rity of these Ic sions are diagnosed at birth o r in ea rl y c hildh ood . O nl y a h andf ul of g li omas have remained undetected until <ldulthood. 1 - 5 They are thoug ht to share a common cmbryogenesis with encep haloceles. The se le sions ar e dini cally rele- vant prim ar il y as a consequence of their pot enrial for c om munication with the ce ntral nervous system. Hi sto- logica ll y, gliomas are c har acte ri zed by unencapsulated co ll ec ti ons of astrocyt ic eosinophilic glial ce ll s in a con- nective tissue ma tri x that ma y ret ain so me fibro us attachments to the dura. Encephaloceles re pr esent her- niation of the mening es ( with or wi th o ut associated brain par enchyma ) through the skull base. Unlike most g lioma s, e ncephaloceles wi ll commu n icate with the s ubarachn oid space cerebrospinal fluid comp art me nt . In this arric le , a previously undescribed lesion wi th tw o distin ct, well-defined tracts leading from the floor of each anterio r cranial fo ssa into a single intrana sal glioma presenting in ad ulth ood will be used to hi gh· li ght the diagnosis and tr e atment of this clinical e ntit y. Case Report H C is 42· year-old African-American male who pre- sent ed to the Oto laryngology and Facial Plastic Su r ge ry service with a long-standing hi stor y of r ig ht -sided nasa l .......................................... ... .... ................ ... .... .. ..... ............................................................................. Received 8/23/99. Received revised 10/27/99. Ac ce pted for publi- ca t io n 10/27/99. Yadrank o Duc ic: Department of Otola ryngology, University of So uthWestern Medic al Center, Dallas, Texas and the Di vision of Ot ola ryngology and Facial Plasric S ur ger y, Jo hn Peter Smi th Ho spital, Fort Worth, Texas. Addre ss rep ri nt requests to: Dr. Yadranko Duci c, Director, Oto- laryngology and Facial Plastic Su rgery, John Peter Smith Hosp i- tal, 1500 South Main Street, F on Worth, TX 76104. 285 ob struction. The pat ie nt had no antecede nt hi s tor y of facial trauma an d was in good overall health. Initial intranasal e xam ination revealed the presence of a 3-cm smoot h, soft submucosal ma ss . Ri gi d endoscopic exam - ina ti on revealed that the mass was not separable from its attachment to the se ptum or the undersurface of the nasal bones. The le sion was distinct from the lateral nasal wall. T he ma ss was not comp ressible and did not ap pear to tran sillu mi nat e or change in size with Val- salva maneuvers. There was no evidence of prese nt or past cere br ospinal fluid l eakage or meningitis. The po s- sibility of intracranial co m muni cation or origin was entertained at this point and confirmed by subsequent comp uted tom ography (CT ) and magne t ic r es onance imaging ( MRI ) scans ( Fi g. 1 ). A dehiscence in the fl oo r of the ri g ht ant erior cranial fossa in cont inuity with the inrranasa lle si on was n ote d on th es e studies. Thu s, the patient was broug ht to the operating room for definiti ve resection of t hi s l es ion. An initial frontal cr a ni otomy confirmed the presence of a l. S-c m defect in the floor of the right an te ri or crania l fossa with a fibrou s connection extend ing from the dura to the intr anasa l l es io n. A transfacial lateral rhinotomy was then used to gai n access to the nasal ma ss (Fig. 2 ). Du e to its intimate attachment to bot h the posterior se ptum and the under- surface of the nasal bones, ostectomies were performed at t hese l evel s to allow for complete and safe removal of the les ion. Once fu ll y mobilized, the tract leading to the flo or of the right anterior cranial fossa floor was identified and Figure 1 Co ronal cr sca n dem ons tra ting inrr acrania l com · m unicat ion between nasal ma ss and floor of right ant erior cranial fo ss a. •
Transcript of Yadral1ko Ducic, FResc - facetransplants.com · I 286 The Journal of Otolaryngology. Volume 28....

•
The Journal of Otolaryngology, VO/llme 28, Number 5, 1999
Case Reports
Nasal Glio .................................................................................................................................................................................................................................. ..................................................................................................
Yadral1ko Ducic, MD, FResc
N asa l encephaloceles and gliomas present along a broad spectrum of severity and deformity. A com
bination of transfacial and intracranial approaches is often required for the safe and definitive treatment of these anomalies.
As a gro up, congenital midline nasa l masses are unusual lesions, having an incidence of 1 in 20,000 to 40,000 live births. I Nasal gliomas, both intranasal and external, represent the least common subset of these patients with less tha n 170 cases descr ibed in the literature.2 The vaSt ma jority of these Icsions are diagnosed at birth o r in ea rl y childh ood . O nl y a handful of gliomas have remained undetected until <ldulthood.1- 5
They are tho ught to share a common cmbryogenesis with encephaloceles. These lesions are dinically relevant primarily as a consequence of their potenrial for communication with the central nervous system. Hi stologically, gliomas are characte rized by unencapsulated collec tions of astrocyt ic eosinophilic gl ial cells in a connective tissue matrix that ma y re tain so me fibro us attachments to the dura. Encephaloceles represent herniation of the meninges (with or wi tho ut associated brain parenchyma ) through the skull base. Unlike most gliomas, encephaloceles wi ll communicate with the subarachnoid space cerebrospinal fluid compartment.
In this arric le, a previously undescribed lesion wi th two distinct, well-defined tracts leading from the floor o f each anterior cranial fossa into a single intranasal glioma presenting in adulthood will be used to high· light the diagnosis and treatment of this clinical entity.
Case Report
H C is 42·year -old African-American male w ho presented to the Otolaryngology and Facial Plastic Surgery service with a long-standing history of right-sided nasa l
.......................................... ... ........................... .. ..................................................................................
Received 8/23/99. Received revised 10/27/99. Accepted for publ ica tion 10/27/99.
Yadranko Ducic: Department of Otola ryngology, University of SouthWestern Medical Center, Dallas, Texas and the Division of Otola ryngology and Facial Plasric Surgery, John Peter Smith Hospital, Fort Worth , Texas.
Address repri nt requests to : Dr. Yadranko Ducic, Director, Otolaryngology and Facial Plastic Surgery, John Peter Smi th Hospita l, 1500 South Main Street, Fon Worth, TX 76104.
285
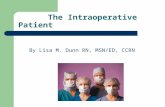
obstruction. The patient had no antecedent history of facial trauma and was in good overall health. In itial intranasal examination revea led the presence of a 3-cm smooth, soft submucosal mass. Rigid endoscopic examination revealed that the mass was not separable from its attachment to the septum or the undersurface of the nasal bones. The lesion was distinct from the lateral nasal wa ll. T he mass was not compressible and did not appear to transilluminate or change in size with Valsalva maneuvers. There was no evidence of present or past cerebrospinal fluid leakage o r meningitis. The possib ility of intracranial communica tion o r o rigin was entertained at this point and confirmed by subsequent computed tomography (CT ) and magnet ic resonance imaging (MRI) scans (Fig. 1). A dehiscence in the floor o f the right anterior cranial fossa in continuity with the inrranasa llesion was noted on these studies.
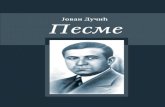
Thus, the patient was brought to the operating room for definitive resection of this lesion. An initia l frontal craniotomy confirmed the presence of a l.S-cm defect in the floor of the right anterior crania l fossa with a fibrou s connection extend ing from the dura to the intranasal lesion. A transfacial lateral rhinotomy was then used to gain access to the nasal mass (Fig. 2 ). Due to its intimate attachment to both the posterior septum and the undersurface of the nasal bones, ostectomies were performed at these levels to allow for complete and safe removal of the lesion. Once fu lly mobilized, the tract leading to the floor of the right anterior cranial fossa floor was identified and
Figure 1 Coronal cr scan demonstrat ing inrracranial com· m unicatio n between nasal mass and floo r o f right anter ior cra nial fossa.
•

I
286 The Journal of Otolaryngology. Volume 28. Nllmber 5, 1999
., •• , ,
Figure 2 Intraope rative photograph taken via lateral rhinotomy approach. N ote elevator between caudal m:lfgi n of nasal hone and nasal mass.
removed in continuity with the main specimen. Further dissection more posteriorly revealed the presence of a second distinct tract measuring 1.0 cm in diameter leading to the floor of the left anterior cranial fossa (Fig. 3) . This, toO, was removed in continuity with the nasal les ion after intracranial exposure of the left side was ohtained (Fig. 4 ). Pathologic analysis revealed the pn:sence of benign asrrocytic neuroglial cells in a fibrou s stroma, pathognomic of intranasal gliomas. The patient's nasal dorsum was reconstructed with a split calvarial bone graft. The patient has done well postoperatively with no evidence of intranasal disease or cerebrospin::d fluid leakage (Fig. 5).
Discussion
Gliomas and encephaloceles appea r to be developmentally related, with gliomas likely representing encephaloceles that were amputated at the level of the skull
'.
- .
Figure 3 Following disarticulation and infe rior displacement of nasal root (with glioma attached ro its deep aspect ), two distinct t races JeJding to the anterior crania! fossa are demonstrated with elevators.
base during development. Failure of normal migration of neural crest ce lls into the anterior cranial region would result in an area devoid of the mesenchyme necessary for skull base formation, resulting in a protrusion of intracranial contents, form ing an encephalocele. If neural crest cell migration is delayed, subseq uent osseous skull base formation would result in amputation of the intracran ial communication, resulting in the formation of a nasal glioma. Incomplete skull base closu re may give rise to persistence of a fibrous stalk that may be intimately associated with the dura.
Nasal gliomas are generally noted in infancy or early childhood and have only very rarely been diagnosed in adulthood. There is no recognized fa milial tendency, mal ignant potentia l, or sex predilection and, for the most part, they are not associated with other developmenta l anomali es.6 They are generally firm, noncompressible masses that do not transilluminate or expand with Valsalva or crying. Sixty percent of these lesions present externally, 30% present intranasally, and 10 % ha ve both components. ? External gliomas may, most often, be fo und at the level of the gla bella. Int ranasal gliomas are almost universally noted to arise ~1 long the lateral nasa l wall at or above the level of the middle turbinate, Overall, only 10 to 15% of gliomas h:wc a connection to the dura.s It should be noted that intranasa l gliomas are two to th ree times as likely to
have such a connection as compared to their external counterparts. Commun ication with the intracrania l space may lead to meningitis, on occasion.
The possibi lity of nasal glioma may be entertained based upon clinical evaluation and the use of adjunctive studies (CT and MRI scans); however, definitive diagnosis is often only possible after complete surgical excision. Incisional biopsies should be performed with caurion, if at all, under controlled circumstances in the operating room, due to the risk of serious cerebrospinal fluid leak
Figure 4 Surgica l spec imen.
,

•
,
with subsequent intracranial infection risk. A CT and/or MRI scan should be obtained in each patient to determine the presence of intracranial communication. These ill l;lging modalities arc often complementary when used ill the evaluation of gliomas and encephaloceles.
Adequate surgical (reatment of gliomas is associ:Hcd with a recurrence rate of less than 10% .6 If there is 110 evidence of intracranial communication, extecIl:dltr:l l1sfacial approaches are adequate. Neurosurgical l."ollsLllr:1tion may occasionally still be necessary if a prev iously unrecognizable tract is identified inrraoperarivl:'ly to be coursing to the skull base. Otherwise, external gl iomas are genera lly excised in an elliptical Llshion directly over the lesion's centre. An external rhinoplasty approach may provide for excellent visualiZJtion of the lesion as well as direct access (0 the nasal hones, which may be transgressed by fibrou s stalks connecting to the dura. Median osteotomies tlt this level (if required to gain transfacial access ro ;1 fibrous stalk) will a llow for controlled, compkte ksion exci sion. Intranasal gliomas, if small J nd LIcking intracrania l communication, may be exci sed endoscopically. Larger lesions or those with inrracranial communication are often best approached via a lateral rhinotomy as in the illustrative case presented. In case of suspected intracranial communica tion, based eithet on clinical examination or radiograph ic examination, initial frontal craniotomy is suggested to allow for safe, subsequent transfacial excision.
The case presented in this article is unique in a number of ways. It is unusual for a gl ioma to have remained undetected and to have presented in adulthood. Furthermore, its attachment to the septum and undersurface of nasal bones and lack of any distinct o rigin at the level of the lateral nasal wall is unusual. ' I 'hL' presence of two distinct stalks arising from a single gli oma and extending to the floors of both anterio r craIl i;ll fossae has been a previously unrecognized variant I d I his lesion. This dual communication is significant in I h.1I it was not identifiable on preoperative imaging or \ lllli .. :;ll examination. Diligent circumferential dissection ,d [hl'sL' les ions is necessa ry to a llow for clear visualizaIlel ll of any tracts communicating with the dura. One ·.hollkl 1l1;linr~l in such vigilance even in the presence of wILl ! Ill i! i;lll y appea rs to be a strictly exrracrani a l "I',h, JIIl.I. ;IS imaging studies are not infallible and the l'n''''''"lIn' of Illulti ple tracts is possible. Failure to ade-1/11.1I1"h" I·Xl"j..,e ,111 such tracts would, in theory, increase tlH' r .... k III rn"lI ITClll"l' of these lesions.
Conclusion
NaS;ll gl io11la s gl'ller ,IlI y present 3S congeni tal masses that ;1re detected ill l';lrl y infancy or childhood. PresentJtion u f a unilateral, firm, llOlKompressible intranasal mass in an adult should ;llso lead one to consider the
Dt,cic, Nas.11 Gliomas 2 87
Figure 5 Pat ient 's 2-monrh postoperative appearance.
possibiliry oi rhis emiry. Alrhough CT and/or MRI scanning is suggested to determine the presence of any
intracranial communication, the absence of such a con
nection does not rule out the presence of single or mul
tiple tracts leading from the lesion to the dura. Such tracts should be excised with a combined intracranial
transfacial approach.
References
1. Hughes G, Sharp ina G, Hum W. Tucker H. Mamgement of
the congenital midline nasal mass: a review. Head Neck
Surg 1980; 2:222-223. 2. PasqUin i E, ElJ'neti G, Giausa G, Biaviti M. A rare case of
nasa l glioma in adult :lge. Otolaryngol Head Neck Surg
1998; 6,90i-906. 3. Ogura JH, S..::henk NL. Unusual nasal tumors. Orolaryngol
Clin Norrh Am 1973; 6:8 13-837.
4. Ka rm~ P, Rasancll 0 , Ka raj a J. Nasal gliomas: a review :lnd
repOrt of two Clses . L.Hyngoscope 1976; 87: 1169-11 79"
5" PoJtard K, Carter DA. A case of nasal glioma :md neurofi
brom:ltosis. J LHyngol Oto11987; 10L497-499.
6. Katz A, Lewis ]S. Nasa l gliomas. Arch Otob ryngol 1971;
94:351-355.
7. Hengere.r A. Congenital anomalies of the nose [monograph] .
Alexandria . VA: AmeriC:ln Academy of Otola ryngo logy
Held and Ne..:k Surgery, 198 7.
8. Frodel J. Llrrabee \'(1, R:1i sis J. The nasal dermoid . Oto
bryngol HC.ld Neck Surg 1989; 101:393-394.