
Xavier Valle: Rectus Femoris
43
MLG-R A Muscle Injuries Classification Proposal
-
Upload
muscletech-network -
Category
Health & Medicine
-
view
521 -
download
0
Transcript of Xavier Valle: Rectus Femoris
MLG-RA Muscle Injuries Classification Proposal

Rectus Femoris Anatomy
Proximal MTJ

Moraux, A., et al. "An anatomical study of the indirect tendon of the rectus femoris using ultrasonography." European radiology 25.12 (2015): 3614-3619.
Proximal MTJ
• Direct head arises from the anterior inferior iliac spine (AIIS).
• Indirect head arises from the superior acetabular ridge and the posterolateral aspect of the hip joint capsule.
• The two heads form a conjoined tendon about 2 cm distal to their origin.
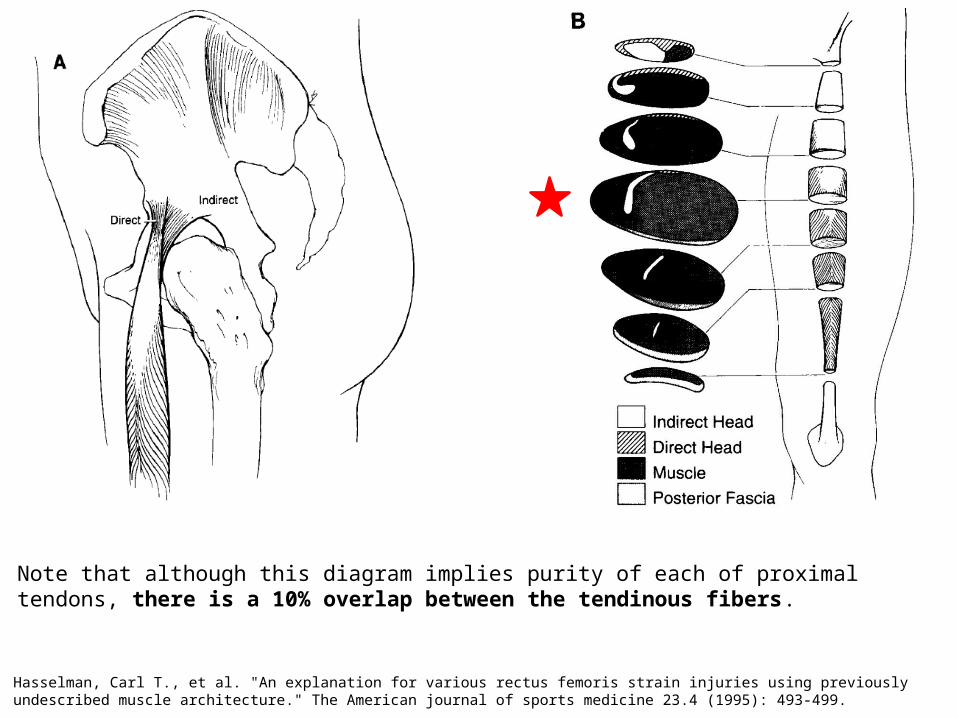
Hasselman, Carl T., et al. "An explanation for various rectus femoris strain injuries using previously undescribed muscle architecture." The American journal of sports medicine 23.4 (1995): 493-499.
Note that although this diagram implies purity of each of proximal tendons, there is a 10% overlap between the tendinous fibers.
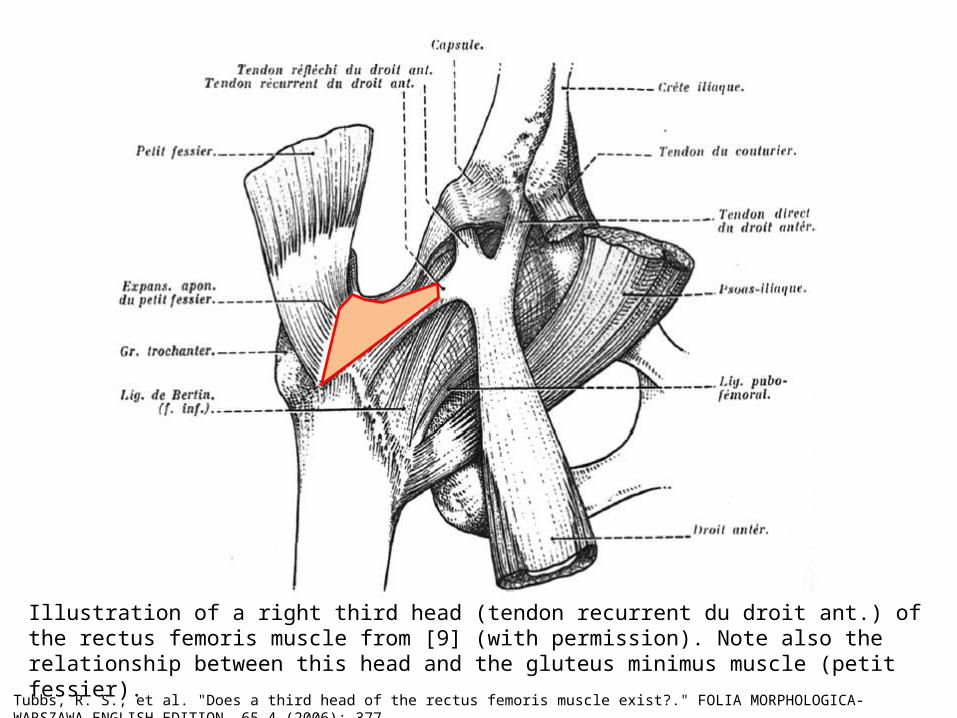
Tubbs, R. S., et al. "Does a third head of the rectus femoris muscle exist?." FOLIA MORPHOLOGICA-WARSZAWA-ENGLISH EDITION- 65.4 (2006): 377.
Illustration of a right third head (tendon recurrent du droit ant.) of the rectus femoris muscle from [9] (with permission). Note also the relationship between this head and the gluteus minimus muscle (petit fessier).

Rectus Femoris Anatomy
Distal MTJ
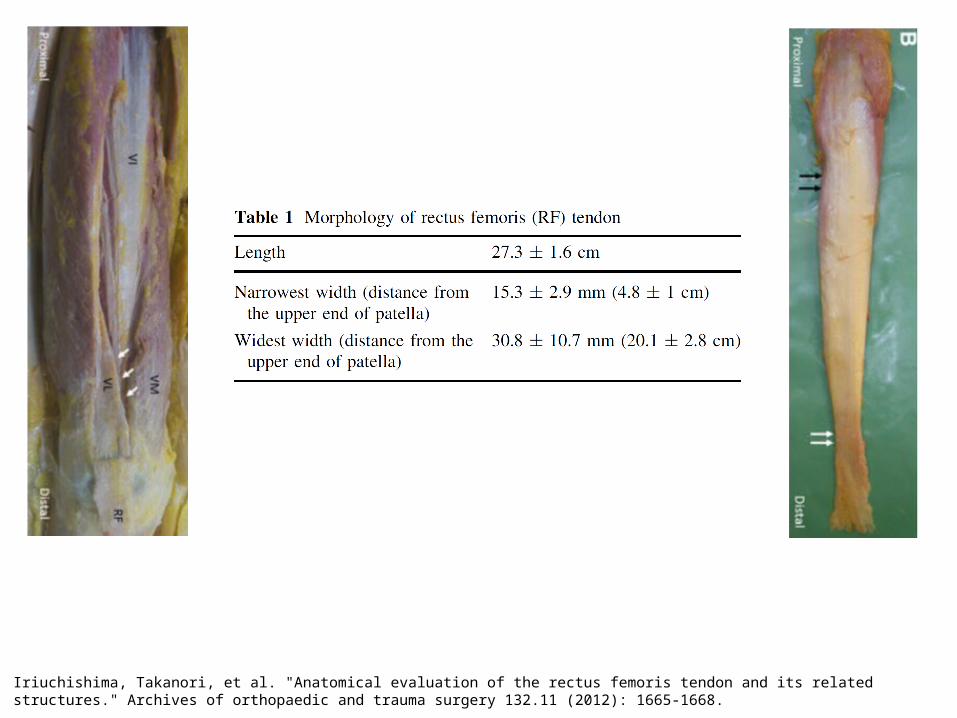
Iriuchishima, Takanori, et al. "Anatomical evaluation of the rectus femoris tendon and its related structures." Archives of orthopaedic and trauma surgery 132.11 (2012): 1665-1668.
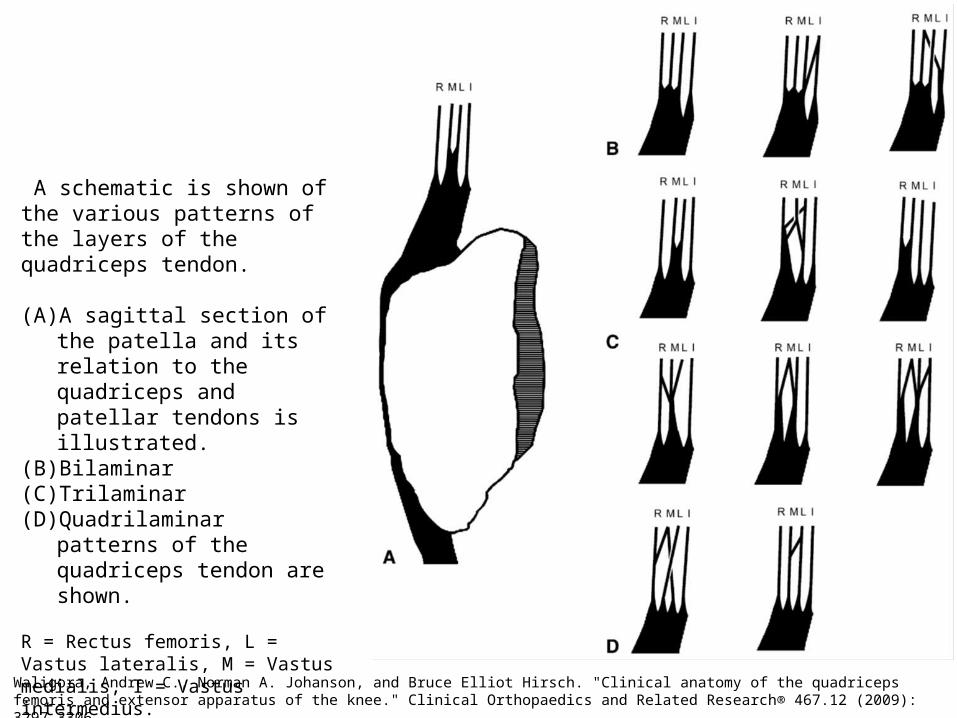
Waligora, Andrew C., Norman A. Johanson, and Bruce Elliot Hirsch. "Clinical anatomy of the quadriceps femoris and extensor apparatus of the knee." Clinical Orthopaedics and Related Research® 467.12 (2009): 3297-3306.
A schematic is shown of the various patterns of the layers of the quadriceps tendon.
(A) A sagittal section of the patella and its relation to the quadriceps and patellar tendons is illustrated.
(B) Bilaminar(C) Trilaminar(D) Quadrilaminar patterns of the
quadriceps tendon are shown.
R = Rectus femoris, L = Vastus lateralis, M = Vastus medialis, I = Vastus intermedius.
Classification• Our classification system for RF
injuries:• Capable to describe injuries location
and chronology,
• easy clinical application,
• adequate grouping of injuries with similar functional impairment, and provide potential prognostic value,
• to enhance communication between professionals and facilitate rehabilitation and RTP.
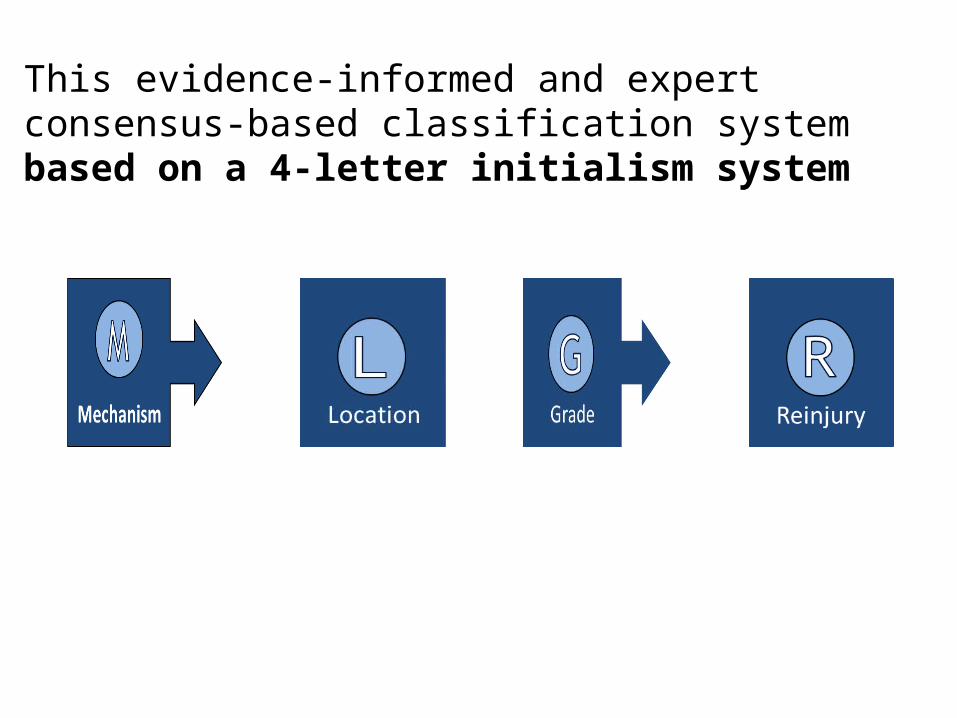
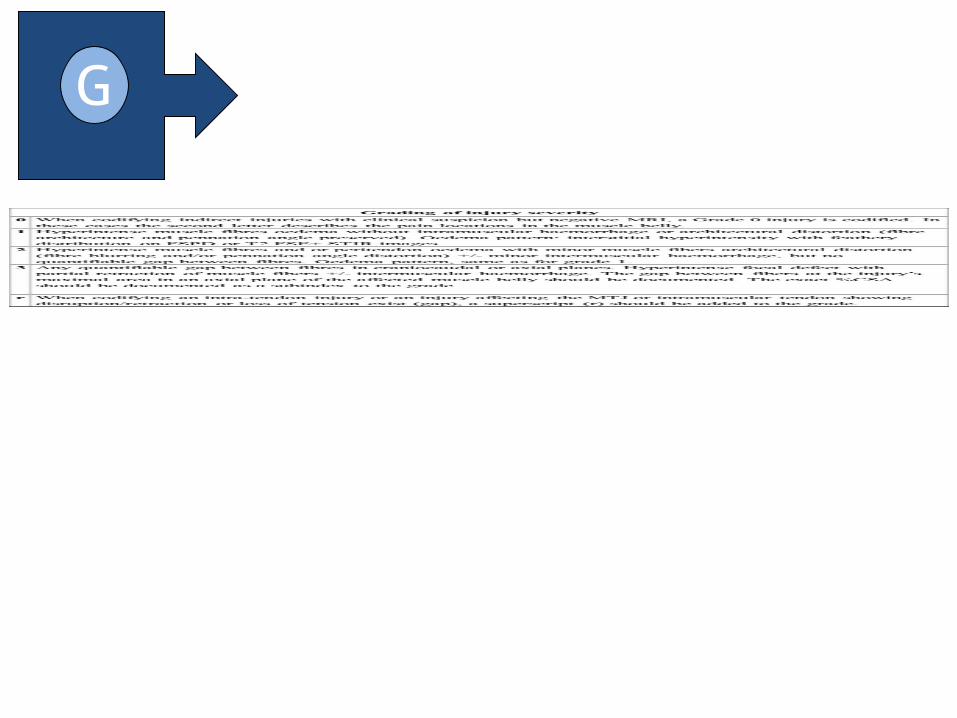
This evidence-informed and expert consensus-based classification system based on a 4-letter initialism system


Direct Injuries
• Severity depends on the site of impact, the activation status of the muscles involved (Hayashi 2012).
• Size of direct muscle injuries is not well correlated with clinical signs and functional impairment (Lee 2012).
• Better evolution with shorter time to recovery in comparison to indirect injuries (Thorsson 1997).
(Hayashi 2012).


Garrett, William E., et al. "The effect of muscle architecture on the biomechanical failure properties of skeletal muscle under passive extension." The American Journal of Sports Medicine 16.1 (1988): 7-12.
“Our results demonstrate that all four muscle types tested show injury and rupture at the MTJ whether pulled from proximal or distal attachment, regardless of muscle structure and rate of strain”

Balius, Ramon, et al. "Central aponeurosis tears of the rectus femoris: practical sonographic prognosis." British journal of sports medicine 43.11 (2009): 818-824.


Cross, Thomas M., et al. "Acute quadriceps muscle strains magnetic resonance imaging features and prognosis." The American journal of sports medicine 32.3 (2004): 710-719.
aa
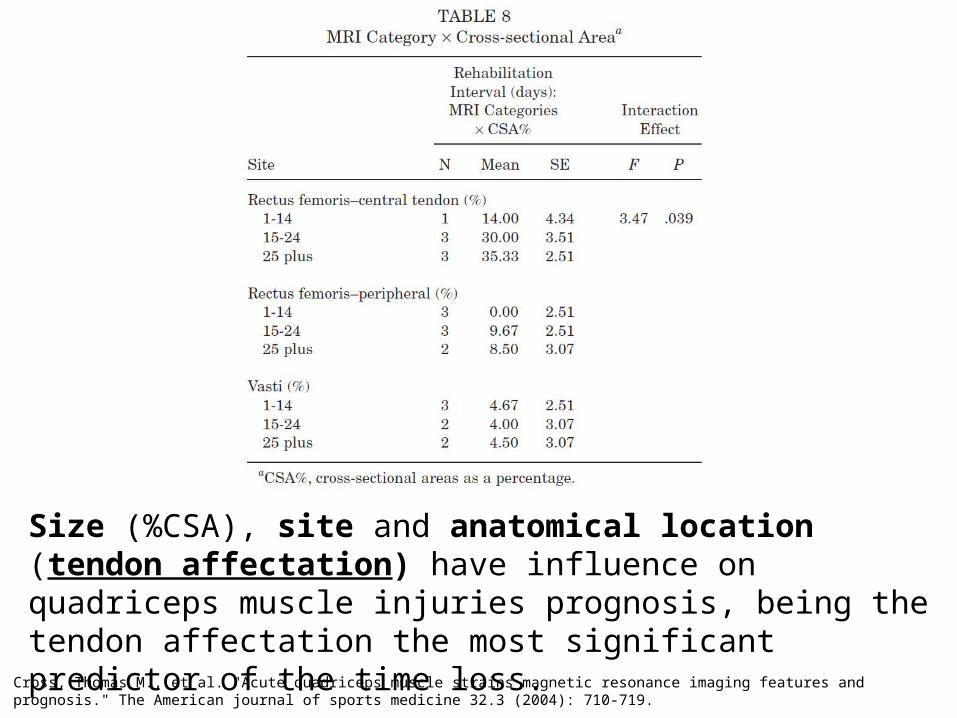
Cross, Thomas M., et al. "Acute quadriceps muscle strains magnetic resonance imaging features and prognosis." The American journal of sports medicine 32.3 (2004): 710-719.
Size (%CSA), site and anatomical location (tendon affectation) have influence on quadriceps muscle injuries prognosis, being the tendon affectation the most significant predictor of the time loss.


Mechanism Location Grade Reinjury
Name the muscle and ...

M (Mechanism)
• Describes the mechanism of injury:
• Direct injuries T
• Indirect injuries I
» Negative MRI injuries N
Mechanism

L (Location)
• Is a letter regarding the anatomical location:
• P, M or D For injuries located at the proximal, middle or distal anatomical third of the muscle belly.
• We also describe the injury relation with the proximal or distal MTJ adding a subindex P or D.
» For MRI negative injuries we will describe pain location.
Location

Kerr, R. M. MRI Web Clinic—May 2014.
• For the proximal MTJ we describes if the injury locates • conjoined tendon P
• at the direct P1
• indirect P2




R (Re-injury)
• Describes the injury chronology (first episode or a re-injury):
• R0: First episode,
• R1: First re-injury, R2: Second re-injury… and so on.
• A re-injury (R) is defined as an injury of the same type and location as the index injury occurring during the first 2 months after return to full competition (Ekstrand 2011).
• Injuries affecting the same MTJ, its intramuscular tendon or fibers associated with it (even in a different location), will also be considered a re-injury.
Examples Direct RF Injuries
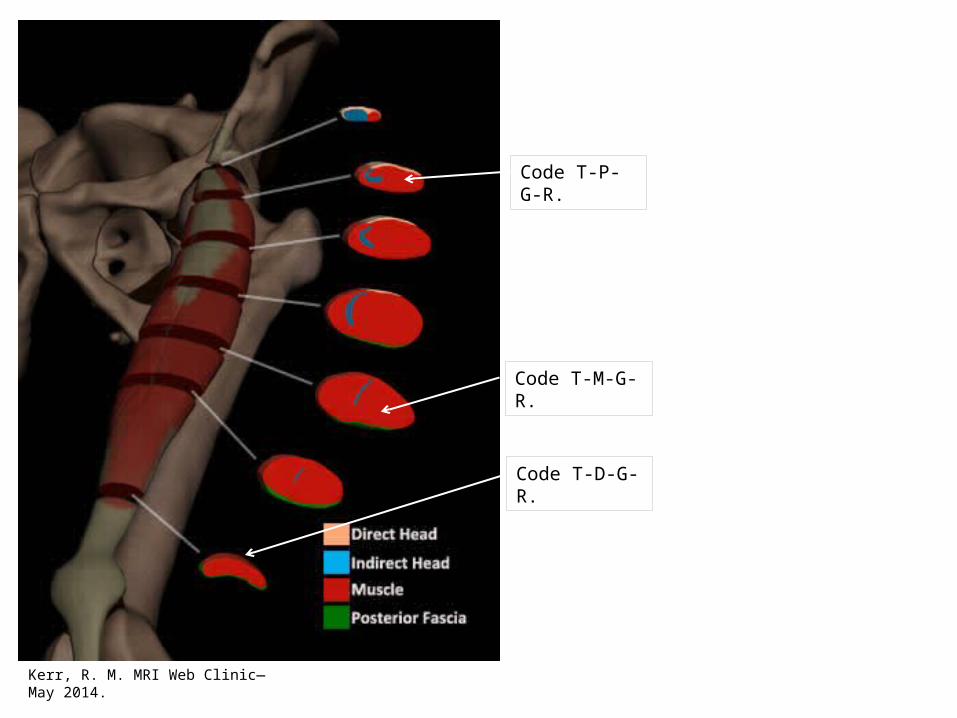
Kerr, R. M. MRI Web Clinic—May 2014.
Code T-D-G-R.
Code T-P-G-R.
Code T-M-G-R.

Examples Indirect RF Injuries with Negative MRI
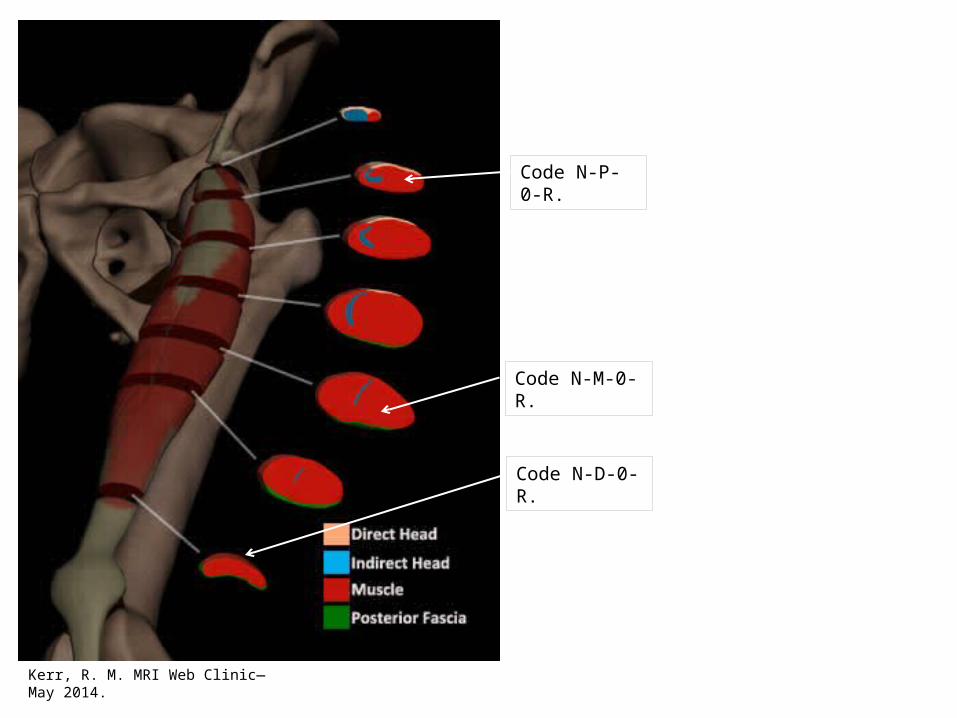
Kerr, R. M. MRI Web Clinic—May 2014.
Code N-D-0-R.
Code N-P-0-R.
Code N-M-0-R.
Examples of Indirect RF Injuries Around the Proximal MTJ
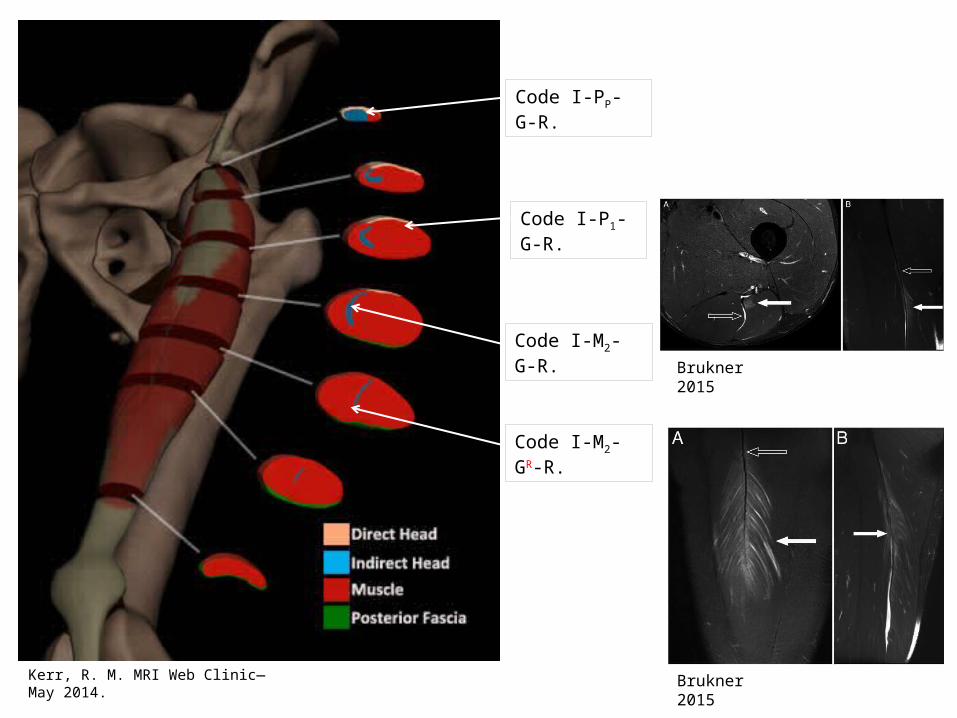
Kerr, R. M. MRI Web Clinic—May 2014.
Code I-PP-G-R.
Code I-P1-G-R.
Code I-M2-G-R.
Code I-M2-GR-R.
Brukner 2015
Brukner 2015
Examples Indirect RF Injuries Around the Distal MTJ

Kerr, R. M. MRI Web Clinic—May 2014.
Code I-MD-G-R.
Code I-DD-G-R.
Balius R
Balius R
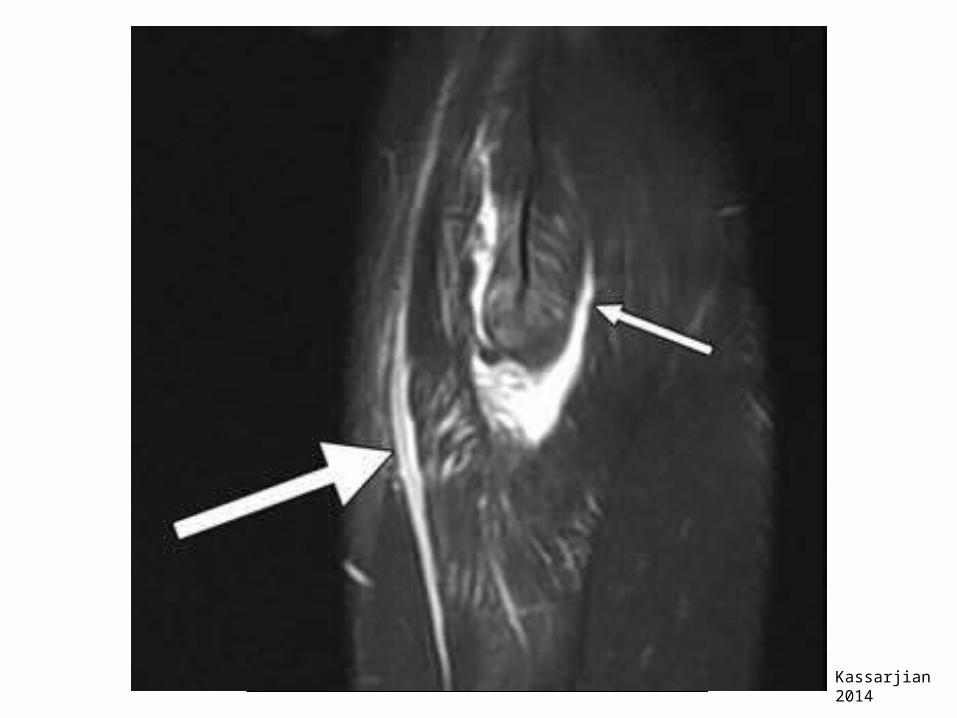
Kassarjian 2014

Hasselman, Carl T., et al. "An explanation for various rectus femoris strain injuries using previously undescribed muscle architecture." The American journal of sports medicine 23.4 (1995): 493-499.
Schematic representation of the pathophysiology in strain injury involving the deep intramuscular tendon of the indirect head.
A note the normal pattern of fibers arising from the deep intramuscular tendon of the indirect head.
B acutely, muscle fibers tear from the tendon and retract distally, with hemorrhage into the space created.
C chronically, this area organizes into a fibrous encasement of the deep tendon with muscle fibers attaching to the scar and serous fluid envelops the tendon and its encasement. The tendon remains intact throughout this injury site.
Kerr, R. M. MRI Web Clinic—May 2014.

Kerr, R. M. MRI Web Clinic—May 2014.
Code I-DD-G-R.

Kerr, R. M. MRI Web Clinic—May 2014.
Code I-DD-GR-R.

Mechanism of injury (M) Locations of injury (L) Grading of severity (G) Number of muscle re-injuries (R)
RF direct injuries
T (direct) P Injury located in the proximal third of the muscle belly
0-3
0 1st episode1 1st re-injury2 2nd re-injury, and so on.
M Injury located in the middle third of the muscle bellyD Injury located in the distal third of the muscle belly
RF indirect injuries
I (indirect) P Injury located in the proximal third of the muscle belly. The second letter is a subindex p or d to describe the injury relation with the proximal or distal MTJ respectively.
0-30 1st episode1 1st re-injury2 2nd re-injury, and so on.
M Injury located in the middle third of the muscle belly, plus the corresponding subindex.
D Injury located in the distal third of the muscle belly, plus the corresponding subindex.
Negative MRI injuries (location is pain related)
N N p proximal third injury
0-3
0 1st episode1 1st re-injury2 2nd re-injury, and so on.
N m middle third injuryN d distal third injury

Practice and Research Gaps• With a 4-letter initialism system we can
describe the injury anatomical location and relation with ECM.
• Easy to use, and avoid confusing
terminology.
• Allows communication among medical staff.
• Flexible structure allowing to incorporate new knowledge in the future.


















