

Www.saferhealthcarenow.ca Go the Distance with MedRec Emerging Ideas and Success Stories To Keep You...
23
www.saferhealthcarenow.c Go the Distance with MedRec Emerging Ideas and Success Stories To Keep You Going March 3, 2011 Alice Watt, ISMP Canada
-
Upload
may-allison -
Category
Documents
-
view
214 -
download
0
Transcript of Www.saferhealthcarenow.ca Go the Distance with MedRec Emerging Ideas and Success Stories To Keep You...

www.saferhealthcarenow.ca
Go the Distance with MedRec
Emerging Ideas and Success Stories To Keep You Going
March 3, 2011Alice Watt, ISMP Canada
www.saferhealthcarenow.ca
Outline
1. MedRec is the right thing to do2. Doing MedRec the right way3. Measurement – quality vs. quantity4. Pass the Baton

www.saferhealthcarenow.ca
3 Elements of Safer Care
1. Identifying what works (efficacy)2. Ensuring that the patient receives it
(appropriate use)3. Delivering it flawlessly (no errors)
What practices will most improve safety? Evidence-based Medicine Meets Patient Safety Leape, L. JAMA July24/31 2002 – Vol 288, No.4
www.saferhealthcarenow.ca
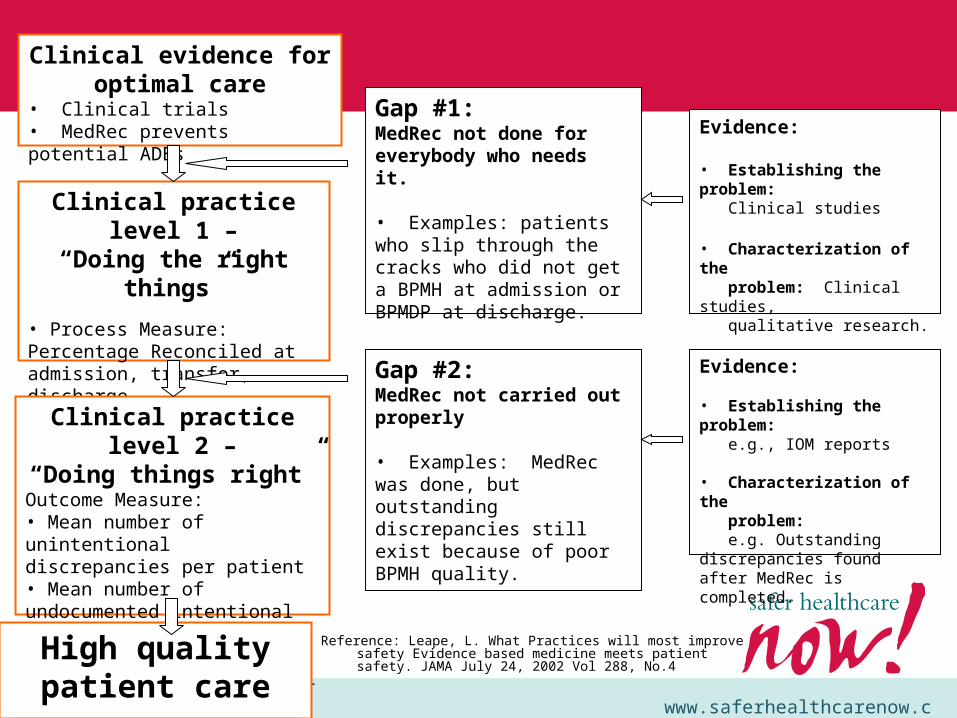
Clinical evidence for optimal care
• Clinical trials• MedRec prevents potential ADEs
Clinical practice level 1 –“Doing the right things”
• Process Measure: Percentage Reconciled at admission, transfer, dischargeGoal: Target population
Clinical practice level 2 –“Doing things right”
Outcome Measure:• Mean number of unintentional discrepancies per patient• Mean number of undocumented intentional discrepancies per patient.• Number of patients with at least one unintentional discrepancy.
Gap #1: MedRec not done for everybody who needs it.
• Examples: patients who slip through the cracks who did not get a BPMH at admission or BPMDP at discharge.
Gap #2: MedRec not carried out properly
• Examples: MedRec was done, but outstanding discrepancies still exist because of poor BPMH quality.
Evidence:
• Establishing the problem: Clinical studies
• Characterization of the problem: Clinical studies, qualitative research.
High quality patient care
Evidence:
• Establishing the problem: e.g., IOM reports
• Characterization of the problem: e.g. Outstanding discrepancies found after MedRec is completed.
Reference: Leape, L. What Practices will most improve safety Evidence based medicine meets patient safety. JAMA July 24, 2002 Vol 288, No.4

www.saferhealthcarenow.ca
Question
To determine the quality of MedRec you would measure the discrepancies found:
A. During the MedRec ProcessB. After the MedRec Process is complete.C. I don’t know

www.saferhealthcarenow.ca
Question
To determine the quality of MedRec you would measure the discrepancies found:
B. After the MedRec Process is complete.

www.saferhealthcarenow.ca
Question
To determine the impact of MedRec you would measure the discrepancies found:
A. During the MedRec ProcessB. After the MedRec Process is complete.C. I don’t know

www.saferhealthcarenow.ca
Question
To determine the impact of MedRec you would measure the discrepancies found:
A. During the MedRec Process

www.saferhealthcarenow.ca
“Reconciliation means that you recognize that there are differences. If there weren’t any differences there would be no need for reconciliation. So because there are differences, we are very well aware of the necessity for reconciliation.” Ref: Aung San Suu Nobel Laureate who has become an international symbol of peaceful
resistance in the face of oppression in Burma. Press conference Yangon, Myanmar. (14-11-2010)

www.saferhealthcarenow.ca
Ideal
BPMH – Gold Standard
Admission Orders
GAP-Reconciliation
of discrepancies
RetroactiveProactive
Quality

www.saferhealthcarenow.ca
What’s Reality
BPMH
Admission Orders
Reconciliation - discrepancies
found during MedRec
RetroactiveProactive
QualityBPMH (Clinician)
What’s the Gap? – Outcome Measures
www.saferhealthcarenow.ca
When to Measure
• Everyday reconciliation process andmeasurement process are actually distinct and different activities
• After baseline, team needs to measure after reconciliation in order to measure the improvement
www.saferhealthcarenow.ca
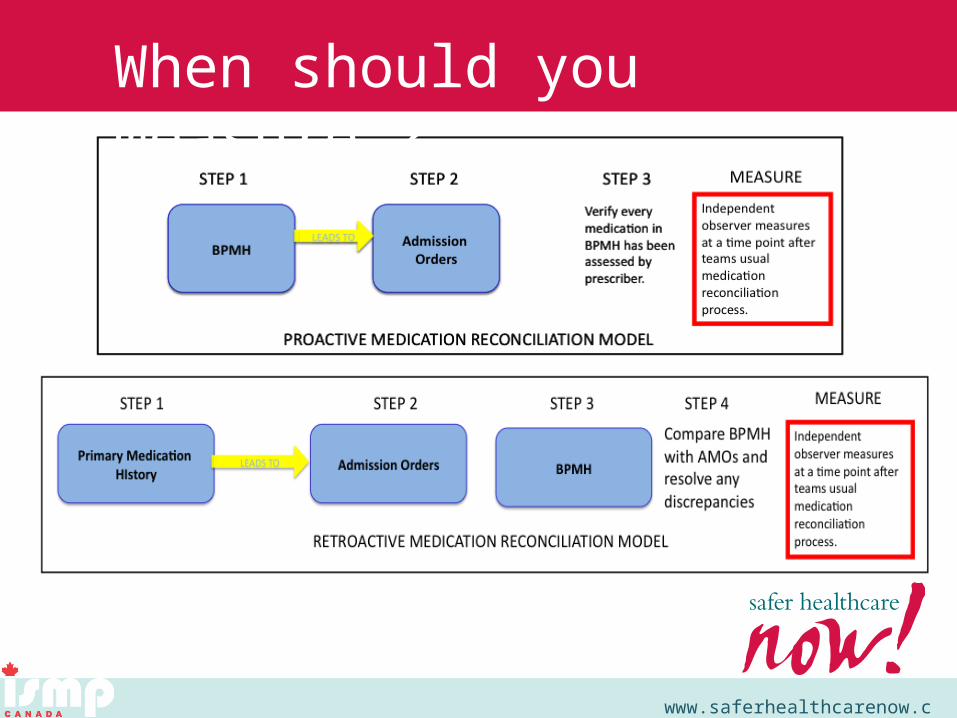
When should you measure ?

www.saferhealthcarenow.ca
– Independent of clinician who has done the main reconciliation
– Resource requirements - meant to be low intensity
– Performed on a small sample monthly for a finite period of time only .
Who Measures?

www.saferhealthcarenow.ca
–Can be from same clinical area, different clinical area, quality / patient safety staff member
–Aim is to measure the quality of medication reconciliation • To ensure medication discrepancies have all been identified
• No need to count discrepancies team has identified and are in the process of being resolved.
Who Measures?

www.saferhealthcarenow.ca
Its like an independent double check
Look at all available patient information - no need to repeat BPMH, clarify with MedRec team as necessary

www.saferhealthcarenow.ca
• Reached its 1) measurement goal (original relative target definition) or 2) reached 0.3 unintentional discrepancies per patient (absolute target- average 75th percentile for MedRec 2 for calendar 2008)
• Held its gains for 3 consecutive data points (months) in a 3-6 month period is considered to be “At Goal”.
• Teams at goal can start/ continue to measure % of patients with formal reconciliation at admission (regularly)
• Should then ensure quality is maintained by reinstituting discrepancy measurement quarterly or bi-annually.
When to Stop/ Change Frequency of Measuring?

www.saferhealthcarenow.ca
• Added to align / synchronize with Accreditation Canada performance indicators (same definitions)
• % patients receiving formal medication reconciliation on admission
• Denominator is total admissions (can be by unit or institution)
• Sampling now allowed for AC (20 patients)
Measure for Admission Medication Reconciliation
www.saferhealthcarenow.ca
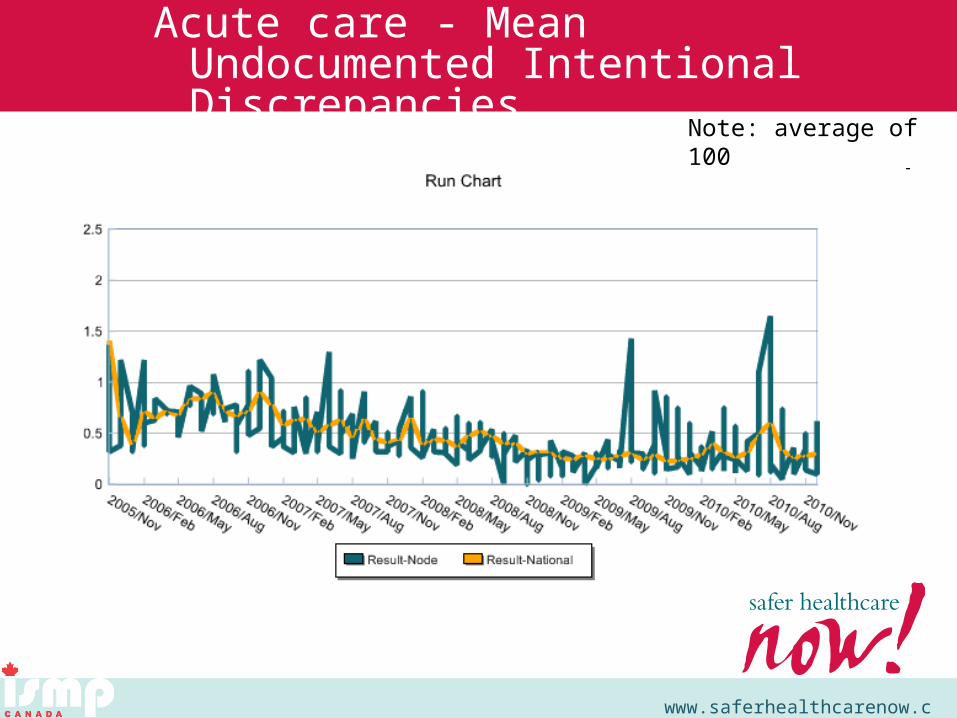
Note: average of 100 Teams reporting data/month
Measure: MedRec - 1.0 Mean Number of Undocumented Intentional Discrepancies per Patient
Measure: MedRec - 1.0 Mean Number of Undocumented Intentional Discrepancies per Patient
Acute care - Mean Undocumented Intentional Discrepancies

www.saferhealthcarenow.ca
Acute Care – Mean Unintentional Discrepancies
per patient

www.saferhealthcarenow.ca
Pass the Baton
• Silo mentality must change.• It is our responsibility to pass the
baton and ensure that our patients and their care providers have the baton and can run with it.

www.saferhealthcarenow.ca
Spring Training begins March 22Register today!


















