Wu Wei - Binnenwerk - complete proef DIGI PDF tissue and the... · Wu Wei. The printing of this...
1
Transcript of Wu Wei - Binnenwerk - complete proef DIGI PDF tissue and the... · Wu Wei. The printing of this...

A D I P O S E
T I S S U E
A N D T H E
K N E EA
DI
PO
SE
TI
SS
UE
AN
D T
HE
KN
EE
Role of inflammation on joint
degeneration and cartilage repair
Wu Wei
Wu
We
i


A D I P O S E
T I S S U E
A N D T H E
K N E E
AD
IP
OS
E T
IS
SU
E A
ND
TH
E K
NE
E
Role of inflammation on joint
degeneration and cartilage repair
Wu Wei
Wu
We
i
A D I P O S E
T I S S U E
A N D T H E
K N E E
AD
IP
OS
E T
IS
SU
E A
ND
TH
E K
NE
ERole of inflammation on joint
degeneration and cartilage repair
Wu Wei
Wu
We
i

The printing of this thesis was financially supported by:
• DepartmentofOrthopedics,ErasmusMCUniversityMedicalCenter,
Rotterdam
• NederlandseOrthopaedischeVereniging(NOV),‘sHertogenbosch
• AnnaFonds,Leiden
• CentrumOrthopedieRotterdamb.v.,Rotterdam
• LivitOrthopedie,Amsterdam
• Chipsoftb.v.Amsterdam
Coverdesign:NiekDekker,Amsterdam,niekdekker.com
Layoutandprintedby:OptimaGrafischeCommunicatie,Rotterdam,theNether-
lands
ISBN:978-94-6361-004-9
CopyrightWuWei,Rotterdam,TheNetherlands,2017.
Nopartofthisthesismaybereproduced,storedortransmittedinanyformorby
anymeanswithoutpriorpermissionoftheauthor.
DedigitaleversievanditproefschriftistevindenindeYourThesisappenkanwor-
dengelezenoptabletofsmartphone.DeappkanwordengedownloadindeApp
storeendeGooglePlaystore,ofmiddelshetscannenvanonderstaandeQR-code

ADIPOSE TISSUE AND THE KNEERoleofinflammationonjointdegeneration
and cartilage repair
Vetweefsel en de knieRolvanontstekingopgewrichtsdegeneratie
enkraakbeenherstel
Proefschrift
terverkrijgingvandegraadvandoctoraande
ErasmusUniversiteitRotterdam
opgezagvande
rectormagnificus
Prof.dr.H.A.P.Pols
envolgensbesluitvanhetCollegevoorPromoties.
Deopenbareverdedigingzalplaatsvindenop
vrijdag20oktober2017om13:30uur
door
Wu Wei
geborenteHubei,China

PROMOTIECOMMISSIE
Promotoren: Prof.dr.G.J.V.M.vanOsch
Prof.dr.J.A.N.Verhaar
Overige leden: Prof.dr.J.M.W.Hazes
Prof.dr.S.K.Bulstra
Dr.P.J.Emans
Copromotor: Dr.Y.M.Bastiaansen-Jenniskens

Voormijnouders
致我的父母


CONTENTS
Chapter1 Generalintroduction,aimsandoutlineofthethesis 11
Part I Local effects of adipose tissue
Chapter2 The size of infrapatellar fat pad adipocytes is not influenced by obesity
27
Chapter3 Stimulationoffibroticprocessesbytheinfrapatellarfatpadinculturedsynoviocytesfrompatientswithosteoarthritis: apossibleroleforprostaglandinF2α
37
Chapter4 Theinfrapatellarfatpadfromdiseasedjointsinhibitschondrogenesisofmesenchymalstemcells
59
Chapter5 Anti-chondrogenicandpro-cataboliceffectofinfrapatellarfatpadanditsresidingmacrophagescanbemodulatedbytriamcinoloneacetonide
79
Part II Systemic effects of adipose tissue
Chapter6 StatinsandfibratesdonotaffectdevelopmentofspontaneouscartilagedamageinSTR/Ortmice
99
Chapter7 HighfatdietacceleratescartilagerepairinDBA/1mice 119
Epilogue
Chapter8 Summaryandgeneraldiscussion 137
Addendumfigures 153
Nederlandsesamenvatting 155
中文简介 159
PhDportfolio 161
Listofpublications 165
Abouttheauthor 169
Dankwoord 171


CHAPTER 1
General introduction, aims and outline of the thesis


General introduction, aims and outline of the thesis 13
1GENERAL INTRODUCTION
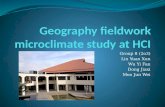
The normal knee
Thekneejointisoneofthecomplexandheavilyloadedjointsofthehumanbody.
Itisabicondylarsynovialjointwhichisformedbyarticulationsbetweenthetibia,
femurandpatella.Thekneejointallowsflexion,extensionandsomedegreesof
internalandexternalrotations.Tendonsconnectthebonestothemusclesand
togetherwiththeligamentscreatestabilitytothejoint.Thearticulatingendsof
thebonesarecoveredbyarticularcartilageandthefibrocartilaginousmeniscilie
betweenthetibiaandthefemur.
Femur
Tibia
Cartilage
Meniscus Infrapatellar fat pad
Patella
Synovial fluid
Synovial fibroblast
Blood vesselAdipocyte
Macrophage
Collagen fiber
Figure 1 ThenormalkneeThekneejointisformedbyarticulationsbetweenthetibia,femurandpatella.Theinfrapatellarfatpadislocat-edinsidethejointcapsulebutoutsidethesynovialmembrane.Thesynovialmembraneisrichlyvascularized.Itconsistsofalayeroffibroblastsandmacrophagesfollowedbyalayerofconnectivetissue.Theinfrapatellarfatpadconsistsmainlyofadipocytes.
Articular cartilage allows smooth gliding movements and acts as a shock ab-
sorber.Itisaspecializedtissuethatisavascularandaneuralandonlyharborsa
smallnumberofcells.Thesecellsarecalledchondrocytesandtheyproduceand
maintainthearticularcartilageextracellularmatrix(ECM).Thearticularcartilage
ECMconsistsmainlyofcollagentype2fibersandproteoglycans.Thenegatively
chargedglycosaminoglycans(GAG)sidechainsontheproteoglycansattractwa-
ter.TheseGAGsattractwaterinsuchextentthat65%-80%ofthecartilageconsists
ofwater.Duetoitsavascularnature,thearticularcartilagereceivesitsnutrients

14 CHAPTER 1
fromthesynovialfluidor fromthesubchondralboneunderneath thecartilage
through diffusion1.
Thesynoviumfluidisencapsulatedbythesynovialmembrane,whichisalsoan
integralpartofthejoint.Thesynovialmembraneisarichlyvascularizedconnec-
tivetissuethatisresponsiblefortheproductionofsynovialfluidandforfiltering
ofdebrisoutofthesynovialfluid.Themembraneismainlycomposedoftwocell
types:macrophagesandsynovialfibroblasts2.
Macrophagesareatypeofcellsthatcanphagocytizeforexamplecellulardebris,
foreignmaterialandmicrobes.Macrophagesplayanimportantroleininflamma-
tionandwoundhealing.Inreactiontostimulifromtheirmicroenvironmentthese
macrophagescanbecomeactivatedintoaspectrumofdifferenttypes.Roughly,
macrophagescanbecategorizedintopro-inflammatory(oftenreferredtoasM1)
macrophages and anti-inflammatory/wound healing (often referred to as M2)
macrophages3.
SynovialfibroblastsarecellsthatcansynthesizeECMsuchascollagentype1,but
alsohyaluronicacidandlubricinforthesynovialfluid.Duringinflammation,these
synovialfibroblastscanalsobetriggeredtosecreteinflammatoryandcatabolic
factors.Outsidethesynovialmembranebutinsidethejointcapsuleseveralfatde-
potsarelocalizedofwhichtheinfrapatellarfatpad(IPFP)isthelargest.TheIPFP
isalsocalledHoffa’sfatpad,namedafterdr.AlbertHoffawhofirstdescribedit
in19044.TheIPFPfillstheanteriorkneecompartmentanditsposteriorsurfaceis
coveredwithsynovialmembrane.TheIPFPprovidesmechanicalcushioningand
facilitatesthedistributionofsynovialfluids.TheIPFPisrichlyvascularizedand
innervated. Furthermore, it containsmany immune cells such asmacrophages
andstemcells5;6.These immunecellscouldplayanrole in thepathogenesisof
kneeosteoarthritis(OA)andthestemcellscouldbeusedfortissueengineering
purposes.
The diseased knee
ThekneejointisvulnerabletotraumaandthedevelopmentofOA.Accordingto
theUnitedStatesBoneand Joint Initiative, thesocioeconomicburdenof joint
diseasesin2014wasveryhighwithmorethan50%ofpeopleaged18yearsand
olderintheUSreportingamusculoskeletalconditionandallcostsassociatedwith
musculoskeletalconditionwasabout5.7%ofthegrossdomesticproduct7.OAis
themostcommondegenerativejointdisorderandaffects1.1millionintheNeth-
erlands8.KneeOAisadiseaseofthewholejointandismorethan‘wearandtear’

General introduction, aims and outline of the thesis 15
1ofthecartilagealone.ThesymptomsofkneeOAarepain,reducedmovementand
disability.ThereareseveralriskfactorsforthedevelopmentofkneeOA,which
includeage,sex,obesityandpreviousjointinjury.Structurally,thereiscartilage
damage,subchondralbonesclerosis,osteophytesformationandsynovialinflam-
mationandfibrosis9.SomeofthestructuralchangesinOAareassociatedwiththe
degreeofsymptoms.IthasbeenshownthatinflammationoftheIPFPisassociated
tokneepainandthatsynovialfibrosiswithreducedjointmovement.Currently,
thereisnocureforOA.Thereareonlytreatmentsagainstthesymptomsofknee
OA,includingreplacementbyarthroplastyinend-stagekneeOA9.
Itisgenerallyassumedthatarticularcartilagedamageifleftuntreated,eventually
couldleadtoOA.Articularcartilagenormallydoesnothealspontaneouslyoronly
partiallyduetoitsavascularandaneuralnature.Furthermore,itharborsonlya
relativelysmallnumberofchondrocytesthatcouldpotentiallyproducematrix.In
thecaseofcartilagedamage,thesechondrocytesreactbyproducingproteolytic
enzymesat the siteof injury thatdestroy theECMand therebyworsening the
damage10.
Cartilage repair
Treatment strategies
Successful treatment of these cartilage defects remains a challenging clinical
problembecausenoneofthecurrentregenerationoptionsareabletocompletely
restore theoriginalstructuralandbiomechanicalpropertiesof thecartilage. In
theknee,surgicaltreatmentoptionsaremarrowstimulationtechniques,suchas
microfracture,forsmallsymptomaticcartilagelesionsandautologouschondro-
cyteimplantation(ACI)andmosaicplastyforlargerlesions10.
The microfracture procedure, first introduced by Steadman11, is a simple and
low cost method to stimulate the body’s own repair response. In the original
technique, during knee arthroscopy, the cartilage defect is debrided down till
thesubchondralbonelayerandsmallholesare‘fractured’intothesubchondral
bone11;12.Thisinturncreatesa‘bleeding’fromtheunderlyingbonemarrowand
thusstimulationofarepairresponsebybioactivefactorsandmesenchymalstem
cells(MSC)fromtheunderlyingbonemarrow13.Thisprocedurecanpotentiallybe
enhancedbyaddinggrowthfactorsorscaffolds,orbychangingthetechniqueof
creatingtheholesorthesize,numberanddepthoftheholes14-16.Themicrofrac-
turetreatmentisgenerallyusedforsingledefectssmallerthan2.5cm2 and leads
toclinicalimprovementinfunctionandpain16-18,butnottohyalinecartilagerepair.

16 CHAPTER 1
Instead,afibrocartilaginoustissuefillsthedefect,whichisofinferiorbiomechani-
cal properties13;19;20.
TheACIprocedureuseslaboratoryexpandedautologousarticularchondrocytes
harvestedfromhealthypartof the jointtofillupthedefect21.These implanted
articular chondrocytes can potentially repair the defect by laying down a new
hyalinecartilageECM.Itisalsopossibletoenhancetherepairprocessbyaddinga
(bio)scaffold22;23.TheACIprocedureisgenerallyusedforcartilagedefectsgreater
than4cm2ormultipledefectsandthelongtermresultsaregood24.Comparedto
microfracture, theACIprocedure is expensive and requires two surgeries. Fur-
thermore,thereismuchdiscussiononthesuperiorityofthistechniquecompared
tothecheapermarrowstimulationtechniquessuchasmicrofracture17;25;26
BesidesmicrofractureandACIprocedure,anosteochondraltransplantationcan
beperformed.Inthisprocedure,alsocalledmosaicplasty,autologousosteochon-
dralgrafts fromhealthy, lessdemandingpartsof the jointare transplanted.Al-
logenousgraftcanalsobeused.Noevidenceisyetavailableaboutthesuperiority
ofthisprocedureversusmicrofractureandpatientsareleftwithanewdefectat
thedonorsitethatcausesdonorsitemorbidity25;27.
Nexttotheseinterventions,currentresearchisalsofocusedontransplantation
ofspecificengineeredMSC-basedconstructs.Inthesestrategies,anovelgraftis
engineeredin-vitrousingMSCs,scaffoldsandgrowthfactors10.Thesestrategies
couldpotentiallyreducedonorsitemorbidityandleadtoimplantationofahya-
linecartilageimplant28.However,theseareonlyexperimentaltreatmentsandcur-
rentlynorandomizedcontrolledtrialhasbeenpublishedyetonthesestrategies.
Effect of inflammation
Cartilagerepairresultscanbeinfluencedbyseveralfactors.Twentyfourhours
afterjointtrauma,thereisapeakinpro-inflammatorycytokinesintheknee,in-
cludingtumornecrosisfactoralpha(TNF-α),interleuking-1beta(IL-1β),aswellas
matrixmetalloproteinase(MMP)-1andMMP-1329-32. Ithasbeenshownthatthese
pro-inflammatorycytokinescaninhibitchondrogenesisandthereforepotentially
inhibit successful hyaline cartilage repair33-35.
Althoughthelevelofthesepro-inflammatorycytokinesdropsovertime,thelevel
ofinflammatorycytokinesininjuredkneesisstillhigherthaninnon-injuredknees
oneyearafterinjury36.Anycartilagerepairprocedureinthekneethereforetakes
placeinanenvironmentwithsomedegreeof inflammation. Inflammationisnot

General introduction, aims and outline of the thesis 17
1alwaysdetrimentaltosuccessfulwoundhealing,becausesomedegreeofinflam-
mationisnecessaryto initiateandmaintainanyhealingresponse37.Controlling
theamountof inflammationandreducingtheamountofpro-inflammatoryanti-
chondrogeniccytokinesinthekneeisthereforeimportant.
Obesity and adipose tissue inflammation
Obesityisanotherfactorthatcouldinfluencecartilagerepairresultsintheknee.
Obesityisdefinedbyabodymassindex(BMI)above30.Studieshavesuggested
thatahigherBMIcouldadverselyaffecttheclinicaloutcomeofmicrofracture18;38
andACI39inthekneeandpatientswithaBMIabove30arenowgenerallyexcluded
fromtreatment40.
Obesityisawell-knownriskfactorforthedevelopmentofOA41.Atypicalstruc-
turalchange inobesity is the increase inadiposetissuesize.Excessivedietary
intakeoflipidsandcarbohydratesleadstoadipocytehypertrophy,deathandsub-
sequentlyinfluxofinflammatorycellsintotheadiposetissue.Thisinturnleads
toincreasedinflammatorycytokinesecretionbytheadiposetissueandsystemic
inflammation.Theseinflammatorychangesleadstosystemicmetabolicchanges
such as hyperglycemia, hyperinsulinemia and dyslipidemia42-44. Combined with
obesity,thesechangesarecalledmetabolicsyndromeandareallriskfactorsfor
thedevelopmentofOA41.BesidesincreasingtheriskofdevelopingOA,obesityalso
couldexaggeratespost-traumaticarthritis45;46anddecreaseskinwoundrepair46.
Mostoftheadiposetissueinthebodyislocatedsubcutaneously.Therearealso
adiposetissuelocatedintra-articularly.Inthekneejoint,theIPFPisthebiggest.
TheIPFPishowevernotthesameassubcutaneousadiposetissue.OnMRI,total
IPFPvolumeisnotassociatedtoBMI47;48and IPFPadipocytesize inmice isnot
influenced by high fat feeding49.TheIPFPdoesplayanroleinjointhomeostasis.
MRIstudieshaveshownthatalargerIPFPisevenassociatedwithlessOA47;50-52.
Previouslywehaveshownthatthesecretionofpro-inflammatorycytokinesbythe
IPFPcanbeincreasedbyaninflammatorystimulus53andthattheIPFPsecretes
factors that could influence the cartilage in degenerative joint disease54.Other
authors report that the IPFP containsmany inflammatory cells and that it is a
sourceofinflammatoryfactors55;56.

18 CHAPTER 1
AIMS AND OUTLINE OF THE THESIS
Adiposetissuebecomesinflamedinobesityandsecretesfactorsthataffectthe
kneejoint.Thesefactorsoriginatefromadiposetissuelocatedoutsidetheknee
joint and thus influence the knee through systemically secreted factors. There
ishoweveralsotheintra-articularly locatedIPFPthatcandirectly locallyaffect
thekneejoint.Therefore,themainaimofthisthesisistoinvestigatetheeffectof
inflammationinadiposetissueondegenerativejointdiseaseandcartilagerepair.
Morespecifically,weinvestigate:
1. whetheradiposetissueinandoutsidethekneeinfluencesdegenerativejoint
diseaseandcartilagerepairintheknee
2. whattheroleisofadiposetissueresidentmacrophagesindegenerativejoint
diseaseandcartilageintheknee
3. whetherwecanmodulateadiposetissueandmacrophageswithmedicationto
reducedegenerativejointdiseaseandtoimprovecartilagerepair.
Adipocytesizeinsubcutaneousandvisceraladiposetissueisincreasedinobesity.
This increase inadipocyte size is associatedwithadipose tissue inflammation.
However,thereisnoinformationyetavailableaboutwhetherobesityinfluences
theadipocytes inthe IPFP inhumans. InChapter 2we investigatewhetherthe
adipocytes inthe IPFPare increased inobesepatients.Theposterioraspectof
theIPFPiscoveredbysynovialmembraneandthesynovialmembraneisheavily
influencedbyfactorssecretedbythe IPFP.Synovialfibrosis iscommoninknee
OAandcausesjointstiffness.InChapter 3wedeterminewhetherIPFPsecretes
factors that influence fibrotic processes in synovial fibroblasts. Previously, we
haveshownthattheIPFPsecretesfactorsthatinfluencecartilage.InChapter 4 we
examinewhethertheIPFPsecretesfactorsthatalsoinfluenceMSC-basedcartilage
repair.Furthermore,inChapter 4wedescribetheroleofmacrophagesresiding
intheIPFPonMSC-basedcartilagerepair.Toimprovethejointenvironmentfor
cartilagerepair,inChapter 5wefocusontheeffectofdifferentanti-inflammatory
medicationontheIPFPandmacrophagesintheIPFP.
TheIPFPisanintra-articularadiposedepotandmostadiposetissuearelocated
extra-articular.Subcutaneousandvisceraladiposetissuedepotsarelocatedout-
sidethejointandobesityleadstochangesinthesedepots.Thisresultsinsystemic
metabolicandinflammatorychangesthatcouldinfluencedegenerativejointdis-
easeandcartilagerepair.Thesesystemiceffectsarecomplexandthereforein-vivo
studies aremore suitable. InChapter 6 we testwhether commonly used lipid
modifyingmedicationscanpreventdegenerativejointdiseaseandcartilagedam-

General introduction, aims and outline of the thesis 19
1ageinamousemodelofspontaneouscartilagedamagewithmetabolicsyndrome.
However,whencartilagedamagedoesoccurinobesepatientsacartilagerepair
treatmentmightbeneeded.Currently,therearenostudiesavailableexaminingthe
structuralcartilagerepairoutcomeinobesepatientsorexplaininghowobesity
influencescartilagerepair.InChapter 7weinvestigatewhetherahighfatdietcan
influencecartilagerepairinamousemodelofcartilagerepair.Inthisway,Ihope
tofindnewtreatmentstoimprovethejointenvironmenttoreducecartilagedam-
ageandimprovecartilagerepair.Finally,inChapter 8Iwillsummarizeanddiscuss
ourmostimportantfindings.Iwillendwithmyperspectiveonfutureresearch.

20 CHAPTER 1
REFERENCES
1. SophiaFoxAJ,BediA,RodeoSA.2009.Thebasicscienceofarticularcartilage:structure,composi-
tion,andfunction.SportsHealth1:461-468.
2. SmithMD.2011.Thenormalsynovium.OpenRheumatolJ5:100-106.
3. MurrayPJ,AllenJE,BiswasSK,etal.2014.Macrophageactivationandpolarization:nomenclature
andexperimentalguidelines.Immunity41:14-20.
4. HoffaA.1904.Influenceofadiposetissuewithregardtothepathologyofthekneejoint.JAMA:795–
796.
5. ClockaertsS,Bastiaansen-JenniskensYM,RunhaarJ,etal.2010.Theinfrapatellarfatpadshould
beconsideredasanactiveosteoarthriticjointtissue:anarrativereview.OsteoarthritisCartilage
18:876-882.
6. DragooJL,JohnsonC,McConnellJ.2012.Evaluationandtreatmentofdisordersoftheinfrapatellar
fatpad.SportsMed42:51-67.
7. USBJ.2014.UnitedStatesBoneandJointInitiative:TheBurdenofMusculoskeletalDiseasesinthe
UnitedStates
8. ChorusAMDFS.2011.NationalePeilingvanhetBewegingsapparaat2010.
9. LaneNE,BrandtK,HawkerG,etal.2011.OARSI-FDAinitiative:definingthediseasestateofosteo-
arthritis.OsteoarthritisCartilage19:478-482.
10. HunzikerEB,LippunerK,KeelMJ,etal.2015.Aneducationalreviewofcartilagerepair:precepts&
practice--myths&misconceptions--progress&prospects.OsteoarthritisCartilage23:334-350.
11. SteadmanJR,MillerBS,KarasSG,etal.2003.Themicrofracturetechniqueinthetreatmentoffull-
thicknesschondrallesionsofthekneeinNationalFootballLeagueplayers.JKneeSurg16:83-86.
12. MithoeferK,McAdamsT,WilliamsRJ,etal.2009.Clinicalefficacyofthemicrofracturetechnique
forarticularcartilagerepairintheknee:anevidence-basedsystematicanalysis.AmJSportsMed
37:2053-2063.
13. ShapiroF,KoideS,GlimcherMJ.1993.Celloriginanddifferentiationintherepairoffull-thickness
defectsofarticularcartilage.JBoneJointSurgAm75:532-553.
14. GomollAH.2012.Microfractureandaugments.JKneeSurg25:9-15.
15. OrthP,DuffnerJ,ZurakowskiD,etal.2016.Small-DiameterAwlsImproveArticularCartilageRepair
AfterMicrofractureTreatmentinaTranslationalAnimalModel.AmJSportsMed44:209-219.
16. Fischer S, Kisser A. 2016. Single-step scaffold-based cartilage repair in the knee: A systematic
review.JOrthop13:246-253.
17. ErggeletC,VavkenP.2016.Microfractureforthetreatmentofcartilagedefectsinthekneejoint-A
goldenstandard?JClinOrthopTrauma7:145-152.
18. MithoeferK,WilliamsRJ,3rd,WarrenRF,etal.2005.Themicrofracturetechniqueforthetreatment
ofarticularcartilagelesionsintheknee.Aprospectivecohortstudy.JBoneJointSurgAm87:1911-
1920.
19. FrisbieDD,OxfordJT,SouthwoodL,etal.2003.Earlyeventsincartilagerepairaftersubchondral
bonemicrofracture.ClinOrthopRelatRes:215-227.
20. Kaul G, CucchiariniM, Remberger K, et al. 2012. Failed cartilage repair for early osteoarthritis
defects:abiochemical,histologicalandimmunohistochemicalanalysisoftherepairtissueafter
treatmentwithmarrow-stimulationtechniques.KneeSurgSportsTraumatolArthrosc20:2315-2324.
21. BrittbergM.2008.Autologouschondrocyteimplantation--techniqueandlong-termfollow-up.Injury
39Suppl1:S40-49.

General introduction, aims and outline of the thesis 21
122. BendersKE,BootW,CokelaereSM,etal.2014.MultipotentStromalCellsOutperformChondrocytes
onCartilage-DerivedMatrixScaffolds.Cartilage5:221-230.
23. BrittbergM.2010.Cellcarriersasthenextgenerationofcelltherapyforcartilagerepair:areview
ofthematrix-inducedautologouschondrocyteimplantationprocedure.AmJSportsMed38:1259-
1271.
24. PareekA,CareyJL,ReardonPJ,etal.2016.Long-TermOutcomesafterAutologousChondrocyte
Implantation:ASystematicReviewatMeanFollow-Upof11.4Years.Cartilage7:298-308.
25. GracitelliGC,MoraesVY,FrancioziCE,etal.2016.Surgicalinterventions(microfracture,drilling,
mosaicplasty,andallograft transplantation) for treating isolatedcartilagedefectsof theknee in
adults.CochraneDatabaseSystRev9:CD010675.
26. KnutsenG, Drogset JO, Engebretsen L, et al. 2016. A RandomizedMulticenter Trial Comparing
AutologousChondrocyteImplantationwithMicrofracture:Long-TermFollow-upat14to15Years.J
BoneJointSurgAm98:1332-1339.
27. AndradeR,VastaS,PereiraR,etal.2016.Kneedonor-sitemorbidityaftermosaicplasty-asystem-
aticreview.JExpOrthop3:31.
28. AnzAW,BapatA,MurrellWD.2016.Conceptsinregenerativemedicine:Past,present,andfuturein
articularcartilagetreatment.JClinOrthopTrauma7:137-144.
29. BigoniM,SacerdoteP,TuratiM,etal.2013.Acuteandlatechangesinintraarticularcytokinelevels
followinganteriorcruciateligamentinjury.JOrthopRes31:315-321.
30. CatterallJB,StablerTV,FlanneryCR,etal.2010.Changesinserumandsynovialfluidbiomarkers
afteracuteinjury(NCT00332254).ArthritisResTher12:R229.
31. IrieK,UchiyamaE,IwasoH.2003.Intraarticularinflammatorycytokinesinacuteanteriorcruciate
ligamentinjuredknee.Knee10:93-96.
32. SwardP,FrobellR,EnglundM,etal.2012.Cartilageandbonemarkersandinflammatorycytokines
areincreasedinsynovialfluidintheacutephaseofkneeinjury(hemarthrosis)--across-sectional
analysis.OsteoarthritisCartilage20:1302-1308.
33. Heldens GT, Blaney Davidson EN, Vitters EL, et al. 2012. Catabolic factors and osteoarthritis-
conditionedmediuminhibitchondrogenesisofhumanmesenchymalstemcells.TissueEngPartA
18:45-54.
34. WehlingN,PalmerGD,PilapilC,etal.2009.Interleukin-1betaandtumornecrosisfactoralphain-
hibitchondrogenesisbyhumanmesenchymalstemcellsthroughNF-kappaB-dependentpathways.
ArthritisRheum60:801-812.
35. YangKG,SarisDB,VerboutAJ,etal.2006.Theeffectofsynovialfluidfrominjuredkneejointsonin
vitrochondrogenesis.TissueEng12:2957-2964.
36. LieberthalJ,SambamurthyN,ScanzelloCR.2015.Inflammationinjointinjuryandpost-traumatic
osteoarthritis.OsteoarthritisCartilage23:1825-1834.
37. KohTJ,DiPietroLA.2011.Inflammationandwoundhealing:theroleofthemacrophage.ExpertRev
MolMed13:e23.
38. NegrinL,Kutscha-LissbergF,GartlehnerG,etal.2012.Clinicaloutcomeaftermicrofractureofthe
knee:ameta-analysisofbefore/after-dataofcontrolledstudies.IntOrthop36:43-50.
39. JaiswalPK,BentleyG,CarringtonRW,etal.2012.Theadverseeffectofelevatedbodymassindex
onoutcomeafterautologouschondrocyteimplantation.JBoneJointSurgBr94:1377-1381.
40. GomollAH,FarrJ,GilloglySD,etal.2010.Surgicalmanagementofarticularcartilagedefectsofthe
knee.JBoneJointSurgAm92:2470-2490.
41. BerenbaumF,GriffinTM,Liu-BryanR.2017.Review:MetabolicRegulationofInflammationinOsteo-
arthritis.ArthritisRheumatol69:9-21.

22 CHAPTER 1
42. ApovianCM,BigorniaS,MottM,etal.2008.Adiposemacrophage infiltration isassociatedwith
insulin resistance andvascular endothelial dysfunction in obese subjects.ArteriosclerThromb
VascBiol28:1654-1659.
43. GrantRW,DixitVD.2015.Adiposetissueasanimmunologicalorgan.Obesity(SilverSpring)23:512-
518.
44. OuchiN,ParkerJL,LugusJJ,etal.2011.Adipokinesininflammationandmetabolicdisease.NatRev
Immunol11:85-97.
45. Louer CR, Furman BD, Huebner JL, et al. 2012. Diet-induced obesity significantly increases the
severityofposttraumaticarthritisinmice.ArthritisRheum64:3220-3230.
46. WuCL,JainD,McNeillJN,etal.2015.Dietaryfattyacidcontentregulateswoundrepairandthe
pathogenesisofosteoarthritisfollowingjointinjury.AnnRheumDis74:2076-2083.
47. CaiJ,XuJ,WangK,etal.2015.AssociationBetweenInfrapatellarFatPadVolumeandKneeStruc-
turalChangesinPatientswithKneeOsteoarthritis.JRheumatol42:1878-1884.
48. ChuckpaiwongB,CharlesHC,KrausVB, et al. 2010.Age-associated increases in the sizeof the
infrapatellarfatpadinkneeosteoarthritisasmeasuredby3TMRI.JOrthopRes28:1149-1154.
49. BarbozaE,HudsonJ,ChangWP,etal.2017.Pro-fibroticinfrapatellarfatpadremodelingwithout
M1-macrophage polarization precedes knee osteoarthritis in diet-induced obesemice. Arthritis
Rheumatol.
50. DuranS,AksahinE,KocadalO,etal.2015.Effectsofbodymassindex,infrapatellarfatpadvolume
andageonpatellarcartilagedefect.ActaOrthopBelg81:41-46.
51. HanW,CaiS,LiuZ,etal.2014.Infrapatellarfatpadintheknee:islocalfatgoodorbadforknee
osteoarthritis?ArthritisResTher16:R145.
52. PanF,HanW,WangX,etal.2015.Alongitudinalstudyoftheassociationbetweeninfrapatellarfat
padmaximalareaandchangesinkneesymptomsandstructureinolderadults.AnnRheumDis
74:1818-1824.
53. ClockaertsS,Bastiaansen-JenniskensYM,FeijtC,etal.2012.Cytokineproductionbyinfrapatellar
fatpadcanbestimulatedbyinterleukin1betaandinhibitedbyperoxisomeproliferatoractivated
receptoralphaagonist.AnnRheumDis71:1012-1018.
54. Bastiaansen-JenniskensYM,ClockaertsS,FeijtC,etal.2012.Infrapatellarfatpadofpatientswith
end-stageosteoarthritisinhibitscatabolicmediatorsincartilage.AnnRheumDis71:288-294.
55. Klein-Wieringa IR,deLange-BrokaarBJ,YusufE,etal.2016. InflammatoryCells inPatientswith
EndstageKneeOsteoarthritis:AComparisonbetweentheSynoviumandtheInfrapatellarFatPad.
JRheumatol43:771-778.
56. Klein-WieringaIR,KloppenburgM,Bastiaansen-JenniskensYM,etal.2011.Theinfrapatellarfatpad
ofpatientswithosteoarthritishasaninflammatoryphenotype.AnnRheumDis70:851-857.



PART I
Local effects of adipose tissue


CHAPTER 2
The size of infrapatellar fat pad adipocytes is not
infl uenced by obesity
John GarciaWu Wei
Jos RunhaarKarina Wright
Gerjo J.V.M. van OschYvonne M. Bastiaansen-Jenniskens
The data presented in this chapter is accepted as part of the manuscript “Lack of high BMI-related features in adipocytes and infl ammatory cells in the infrapatellar fat pad”
by A.J. De Jong et al in Arthritis Research & Therapy

28 CHAPTER 2
ABSTRACT
Adipocytehypertrophyandtheresultingadiposetissueinflammationarekeyfea-
turesofobesity.However,itisstillunclearwhetherobesitycausestheadipocytes
intheinfrapatellarfatpad(IPFP)tocontributetojointinflammation.Theaimof
thisstudywastodeterminetheeffectofobesityonthesizeofIPFPadipocytes.
IPFPwasobtainedfromend-stageosteoarthritispatientswithameanbodymass
index(BMI)of29.7kg/m2(range21.5-48.47kg/m2).Subcutaneousfatwasobtained
from12 end-stageosteoarthritisdonorswith ameanBMIof 33.0 kg/m2 (range
24.2-48.5kg/m2).Fat tissueswerecryosectionedandstainedwithhaematoxylin
and eosin.The cross-sectional areaof adipocyteswasdeterminedusing image
analysissoftware.NorelationshipbetweenadipocytesizeandBMIwasobservedin
IPFPadipocytes(r=-0.06,p=0.82),whereassubcutaneousadipocytesizepositively
correlateswithdonorBMI(r=0.63,p=0.028).Fornon-obesedonors,sizeof IPFP
adipocyteswasnot significantlydifferent tosubcutaneousadipocytes (p>0.99).
Subcutaneous adipocytes fromobesedonorswere significantly larger than the
IPFPadipocytesfromotherobesedonors(p=0.03).Ourresultsdemonstratethat
obesity does not affect the size of adipocytes in the IPFP,which suggests that
inflammationoftheIPFPisnotinfluencedbyobesityassociatedadipocytehyper-
trophy.

The size of infrapatellar fat pad adipocytes is not influenced by obesity 29
2
INTRODUCTION
Ahighbodymassindexasaresultofexpansionofadiposetissueisawell-known
risk factor in the development of knee osteoarthritis (OA)1. During expansion,
adipocytesinadiposetissuebecomehypertrophic.Largeadipocyteshavebeen
showntoproducesubstantiallymorepro-inflammatorycytokinesandadipokines
thansmalleradipocytes2Thisincreasedsecretionofpro-inflammatorymolecules
such IL-6andtumornecrosis factoralpha(TNF-α)promotestherecruitmentof
macrophagesand theirdifferentiation intoapro-inflammatoryphenotype.This
leadstolow-gradesystemicinflammationandmetabolicchanges,bothofwhich
havebeenassociatedwithOA1.Besidesmechanicaloverloading,obesityrelated
inflammationandmetabolicchangeshavealsobeenassociatedwithOA1.
The infrapatellar fat pad (IPFP) is an adipose tissue located intracapsular yet
extra-synovial.IPFPisapotentialsourceofinflammatoryfactorsinthekneejoint3.
Duetoitsintra-articularlocationandbecauseadiposetissuesgenerallybecomes
inflamedinobesity,ithasbeenlongthoughtthattheIPFPcouldplayamajorrole
in obesity related joint inflammation.Unlike subcutaneous adipose tissue,MRI
studies have suggested that total IPFP volume is not associated to bodymass
index(BMI)4.However,theseMRIstudiesdidnotinvestigatethesusceptibilityof
theIPFPtoobesityrelatedeventsthatleadtoinflammation,suchasadipocytehy-
pertrophy.Theaimofthisstudywastoinvestigatewhetherincreasedadipocyte
size,whichcontributestoadiposetissueinflammation,isassociatedwithBMIin
theIPFP.
METHODS
Tissue sample preparation
Eighteen IPFPs were obtained from end stage OA patients with a mean body
mass index (BMI) of 29.7 kg/m2 (range 21.5-48.47 kg/m2) undergoing total knee
arthroplasty.Subcutaneousadipose tissuewasobtained fromtwelveendstage
OAdonorswithameanBMIof33.0kg/m2(range24.2-48.5kg/m2)undergoingtotal
hiporknee replacement.Consentwasgiven inaccordancewith theguidelines
oftheFederationofBiomedicalScientificSocieties(http://www.federa.org)after
approvalbythe localethicalcommittee(MEC2008-181andMEC2012-267).Do-
norsweresubdividedintoobese(BMI≥30)andnon-obese(BMI<30)foreachof
theadiposetissues(atotalof4groups).Tissuesampleswerecryosectionedand

30 CHAPTER 2
stainedwithhaematoxylinandeosin(H&E)andimagedusinganOlympusSC30
camera(Olympus,Zoeterwoude,Netherlands).
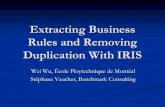
Measurement of adipocyte size
Thecross-sectionalareaoftheimagedadipocyteswascalculatedusingFijiIsJust
ImageJ softwarewith the additionalAdiposoft plugin. Three separate sections,
withaminimumof25adipocytesineachsectionweremeasuredperdonor.The
Adiposoft applicationwas calibrated to identify cellswith a diameter between
30-130µm.Ameasuringscaleof0.33µm/pixelwasalsousedbytheapplication
todetermine the cross-sectional area (size)of eachadipocyte identified in the
images.Amanualinspectionofoutputdatawasperformedtoconfirmtheconsis-
tencyofthemeasurements(Figure1).
Figure 1 IdentificationofadipocytesusingtheAdiposoftpluginforFIJI.A)Haematoxylin and eosin stainingof adipose tissue imaged at 100xmagnification.B) Imageprocessed inAdiposoft,C)Correctedimageaftermanualinspectionofprocessedimaged.Theyellowcontours(BandC)representthecross-sectionalareaofanadipocyte.Scalebar=100µm.
Statistical analysis
TheShapiro-Wilktestwasconductedtoassessthedistributionoftheadipocyte
sizesforeachdonor.Thesizeofadipocytesfromindividualdonorswasnotnor-

The size of infrapatellar fat pad adipocytes is not infl uenced by obesity 31
2
mallydistributed.Spearman’srhowasdeterminedtorelateBMItoadipocytesize
in IPFPandsubcutaneousadipose tissue.TheKruskal-Wallis testwithmultiple
comparisonswasusedtocomparethemediansizeofadipocytesfromIPFPand
subcutaneousfatfrombothnon-obeseandobesedonors.Statisticalsignificance
wasconsideredforp-values<0.05.
RESULTS
Amicroscopicobservationoftheadiposetissuesshowednodistinctdifference
betweenadipocytesintermsofgeneralmorphologyanddistributionacrossdonor
groups,howeverrelativelylargeradipocyteswerenoticeableinsubcutaneousfat
ofobesedonorscomparedtootherdonorgroups(Figure2).Thesizeofadipocytes
in subcutaneous adipose tissuewas correlated todonorBMI (r=0.63,p=0.028),
whichwasnotthecaseintheIPFP(r=-0.06,p=0.82)(Figure3A,B).Fornon-obese
donors(BMI<30), IPFPadipocytesize(1765μm2±163.5)wasnotsignificantly
differenttosubcutaneousadipocytesize(2157μm2±835.6,p>0.99).Howeverthe
sizeofadipocytesfromtheIPFPofobese(1732μm2±292.4)andnon-obesedonors
(1765μm2±163.5)weresignificantlysmallerthansubcutaneousadipocytesfrom
obesedonors(3195μm2±833.9,p=0.03andp=0.04respectively)(Figure3C).
Figure 2 RepresentativeimagesofH&EstainedcryosectionsofadiposetissuefromtheIPFPandsubcutaneousfat(SCF)ofnon-obeseandobesedonors.IPFP:infrapatellarfatpad,SCF:subcutaneousfat.Scalebar=100µm.

32 CHAPTER 2
IPFP
BMI
Adip
ocyt
eSi
ze(µ
m2 )
0 20 40 600
1000
2000
3000
4000
5000A
r=-0.06p=0.82
SCF
BMI
Adip
ocyt
eSi
ze(µ
m2 )
0 20 40 600
1000
2000
3000
4000
5000
B
r=0.63p=0.028
Adip
ocyt
eSi
ze(µ
m2 )
IPFP SCF IPFP SCF0
1000
2000
3000
4000
5000p=0.03
p=0.04C
Non-obese Obese
Figure 3 ObesitydoesnotaffectIPFPadipocytesize.Spearman’stest forcorrelationbetweendonorBMIandadipocytesize intheA) infrapatellar fatpad(IPFP)andB)subcutaneousfat(SCF).Eachdotrepresentsanindividualdonor.C)ComparisonofsizeofadipocytesbetweenIPFPandSCFinobeseandnon-obesedonor.Valuesaremean±SD
DISCUSSION
Theobesity-relatedalterationsthatoccur inadiposetissues,suchas increased
adipocyte size5,arenotwellcharacterisedintheIPFP. Inthecurrentstudy,we
haveshownthatunlikesubcutaneousadiposetissueadipocytes,thesizeofIPFP
adipocyteswasnotassociatedwithBMI.
OurobservationsinhumantissuesprovideevidencethattheIPFPadipocytesdo
notundergothemetabolicalterationsthatoftenengenderscellularhypertrophy6,
andconfirmsapreviousinvestigationthatshowedtheabsenceofhypertrophic
adipocytesintheIPFPofobesemice.7 Subcutaneous adipose tissue is considered
asbothanenergystorageandanendocrineorganthatissusceptibletoinflam-
matorymacrophageinfiltrationduringobesity.TheIPFPisapotentialcontributor
tolocaljointinflammationviatheproductionofadipokinesandcytokines3 that
exacerbatejointdegeneration.IthasbeenshownthatinflammationoftheIPFPis

The size of infrapatellar fat pad adipocytes is not influenced by obesity 33
2
associatedwithkneepainanddisabilityinobeseOApatients.8 Since the adipo-
cytesoftheIPFPitselfarenotaltered,atleastnotinsizeasaresultofobesity,it
couldbeinferredthattheIPFPderivedadipocytesdonotpossessthesamepro-
inflammatoryphenotypeassubcutaneousadipocytes.Hence,ourfindingscould
highlightnovelfunctionaldifferencesbetweentheIPFPandsubcutaneousadipose
tissueinobesity.PerhapstheinflammatoryroleoftheIPFPinthepathogenesis
ofobesityrelatedOAisseparatetothatofsubcutaneousfat.Thecellular,genetic
ormolecularmechanismsthatcausesthisdifferenceinsensitivitytoobesityin
theIPFPandotheradiposetissuesisnotfullyunderstoodandwarrantsfurther
investigation.
It is noteworthyhowever, that recentMRIbased studieshave associated large
IPFPwithareducednumberofabonemarrowlesions,lowwalkingpainandhigher
totalcartilagevolumeinOApatients. 9Furthermore,conditionedmediaof IPFP
adipocytesfromobeseOApatientswasfoundtohavenoeffectonthesecretion
ofTNF-αinlipopolysaccharidestimulatedmacrophagesin vitro,butinterestingly
inhibitedtheproductionofIL-12p40inthesestimulatedmacrophages.10Wehave
alsoshownthattherewerenodifferencesbetweentheamountofsecretedfactors
in conditionedmediaof IPFP fromobeseandnon-obeseOAdonors11, and that
conditionedmedia from OA IPFP explants have a chondroprotective effect on
cartilage.12Inaratmodelforageing,onlysynovialthicknessasoneofthemany
OA features was correlated with IPFP adipocyte size and this correlation was
independentofage.Thesecretionofthepro-inflammatorycytokineTNF-α from
IPFPwasassociatedwithage,butnoassociationbetweenIPFPadipocytesizeand
cytokinesreleasewasreported13.Theprogressiveage-dependantdownregulation
ofgenesrelated toanti-inflammatorymacrophages in IPFPexplants fromthese
ratssuggests thatashift towardsapro-inflammatoryphenotype is likely tobe
mediatedbyimmunecellsratherthanadipocytes.Takingthistogether,itisclear
thatfurtherinvestigationsarerequiredtoclarifywhetherandhowobesityinflu-
encestheIPFP,andifso,whattheimplicationsareforOA.
The use of unmatched IPFP and subcutaneous fat is a limitation to this study.
Assessingabiggersamplesizewithmatched IPFPandsubcutaneous fatwould
further confirm the differences in adipocyte size in the two tissues within a
particular donor. A recent study reported considerably larger adipocyte sizes
forbothIPFP(3708±976µm2)andsubcutaneousfat(6082±628µm2)compared
to our results14. This couldbe attributed to thedifference inmethodsused to
measurecellsize.Analysisofthesecretoryprofilesofindividualadipocyteswould
alsoprovidevaluable insightconcerningthe inflammatorystatusof the IPFP in

34 CHAPTER 2
obeseandnon-obesepatients. Interestingly,ourpreviousexperimentsrevealed
thatthesecretoryprofileofIPFPexplantsandthepresenceofmacrophagesinthe
IPFParenotinfluencedbydonorBMI.3,11Thisprovidessupportingevidencefor
ourhypothesisthatperhapsanincreasedBMIdoesnothavesignificantinfluence
ontheadipocytesintheIPFP.Furthermore,wedidnothavesamplesfromnon-OA
IPFPdonors.We thereforecannotexclude thepossibility that theOAcouldal-
readyhaveinfluencedtheadipocytesizeinourdonors.TheIPFPcanalsobecome
fibroticwhichcouldpossiblylimittheenlargementofadipocytes.
Inconclusion,toourknowledge,thisisthefirstevidencethatIPFPadipocytesdo
notbecomehypertrophicwithobesity.Adifferenceinthephysiologicalrolesof
theIPFPandsubcutaneousfatcouldpossiblyaccountforthedifferenceinsuscep-
tibilityoftheiradipocytestohypertrophy.Thedatapresentedhereaddstothe
growingbodyofliteratureinvestigatingthephysiologicalfunctionoftheIPFPand
itsroleinthedevelopmentOA.

The size of infrapatellar fat pad adipocytes is not influenced by obesity 35
2
REFERENCES
1. ThijssenE,vanCaamA,vanderKraanPM.Obesityandosteoarthritis,morethanjustwearand
tear:pivotalrolesforinflamedadiposetissueanddyslipidaemiainobesity-inducedosteoarthritis.
Rheumatology(Oxford).2015;54(4):588-600.doi:10.1093/rheumatology/keu464.
2. SkurkT,Alberti-huberC,HerderC,HaunerH.RelationshipbetweenAdipocyteSizeandAdipokine
ExHpression and Secretion. J Clin Endocrinol Metab. 2007;92(3):1023-1033. doi:10.1210/jc.2006-
1055.
3. ClockaertsS,Bastiaansen-JenniskensYM,RunhaarJ,VanOschGJVM,VanOffelJF,VerhaarJAN,et
al.Theinfrapatellarfatpadshouldbeconsideredasanactiveosteoarthriticjointtissue:anarra-
tivereview.OsteoarthritisCartilage.2010;18(7):876-882.doi:10.1016/j.joca.2010.03.014.
4. TeichtahlA,WulidasariE,BradyS,WangY,WlukaA,DingC, et al.A large infrapatellar fatpad
protectsagainstkneepainandlateraltibialcartilagevolumeloss.ArthritisResTher.2015;17:318.
doi:10.1016/j.joca.2015.02.517.
5. Hirsch J, Batchelor B. Adipose tissue cellularity in human obesity. Clin Endocrinol Metab.
1976;5(2):299-311.doi:10.1016/S0300-595X(76)80023-0.
6. DeFerranti S,MozaffarianD.Theperfect storm:Obesity, adipocytedysfunction,andmetabolic
consequences.ClinChem.2008;54(6):945-955.doi:10.1373/clinchem.2007.100156.
7. ChangW,DeMoeJ,KentC,KovatsS,GarteiserP,DoblasS,etal.Infrapatellarfatpadhypertrophy
without inflammation in a diet-inducedmousemodel of obesity and osteoarthritis. Osteoarthr
Cartil.2011;19:66.doi:10.1016/S1063-4584(11)60157-X.
8. BallegaardC,RiisRGC,BliddalH,ChristensenR,HenriksenM,BartelsEM,etal.Kneepainandin-
flammationintheinfrapatellarfatpadestimatedbyconventionalanddynamiccontrast-enhanced
magneticresonanceimaginginobesepatientswithosteoarthritis:Across-sectionalstudy.Osteo-
arthrCartil.2014;22(7):933-940.doi:10.1016/j.joca.2014.04.018.
9. HanW,CaiS,LiuZ,JinX,WangX,AntonyB,etal.Infrapatellarfatpadintheknee:islocalfatgood
orbadforkneeosteoarthritis?ArthritisResTher.2014;16(4):R145.doi:10.1186/ar4607.
10. Klein-WieringaIR,AndersenSN,KwekkeboomJC,GieraM,deLange-BrokaarBJE,vanOschGJVM,
etal.Adipocytesmodulatethephenotypeofhumanmacrophagesthroughsecretedlipids.J Im-
munol.2013;191(3):1356-1363.doi:10.4049/jimmunol.1203074.
11. ClockaertsS,Bastiaansen-JenniskensYM,FeijtC,DeClerckL,VerhaarJAN,ZuurmondA-M,etal.
Cytokine production by infrapatellar fat pad can be stimulated by interleukin 1β and inhibited
by peroxisome proliferator activated receptorα agonist. Ann RheumDis. 2012;71(6):1012-1018.
doi:10.1136/annrheumdis-2011-200688.
12. Bastiaansen-JenniskensYM,ClockaertsS,FeijtC,ZuurmondA-M,Stojanovic-SusulicV,BridtsC,
etal.Infrapatellarfatpadofpatientswithend-stageosteoarthritisinhibitscatabolicmediatorsin
cartilage.AnnRheumDis.2012;71:288-294.doi:10.1136/ard.2011.153858.
13. FuY,Huebner JL, KrausVB,GriffinTM. Effect of Aging onAdiposeTissue Inflammation in the
KneeJointsofF344BNRats.JournalsGerontolSerABiolSciMedSci.2015;00(00):1-11.doi:10.1093/
gerona/glv151.
14. MacchiV,PorzionatoA,SarasinG,PetrelliL,GuidolinD,RossatoM,etal.TheInfrapatellarAdipose
Body:AHistotopographicStudy.CellsTissuesOrgans.2016.doi:10.1159/000442876.


CHAPTER 3
Stimulation of fi brotic processes by the infrapatellar
fat pad in cultured synoviocytes from patients
with osteoarthritis: a possible role for prostaglandin F2α
Yvonne M Bastiaansen-Jenniskens Wu Wei
Carola Feijt Jan H Waarsing Jan AN Verhaar
Anne-Marie Zuurmond Roeland Hanemaaijer
Reinout Stoop Gerjo JVM van Osch
Arthritis Rheum. 2013 Aug;65(8):2070-80

38 CHAPTER 3
ABSTRACT
Objective
Stiffeningofthejointisafeatureofkneeosteoarthritis(OA)thatcanbecaused
byfibrosisofthesynovium.Theinfrapatellarfatpad(IPFP)presentintheknee
jointproducesimmune-modulatoryandangiogenicfactors.Thegoalofthepres-
entstudywastoinvestigatewhethertheIPFPcaninfluencefibroticprocessesin
synovialfibroblasts, and todetermine the roleof transforminggrowth factorβ
(TGFβ)andprostaglandinF2α(PGF2α)intheseprocesses.
Methods
Batchesoffat-conditionedmedium(FCM)weremadebyculturingpiecesofIPFP
obtainedfromthekneesof13patientswithOA.HumanOAfibroblast-likesynovio-
cytes(FLS)(frompassage3)wereculturedinFCMwithorwithoutinhibitorsof
TGFβ/activinreceptor–likekinase5orPGF2αfor4days.TheFLSwereanalyzed
for production of collagen and expression of the gene for procollagen-lysine,2-
oxoglutarate5-dioxygenase2(PLOD2;encodinglysylhydroxylase2b,anenzyme
involvedincollagencrosslinking)aswellasthegenesencodingα-smoothmuscle-
actin and type I collagen α1chain.Inparallel,proliferationandmigrationofthe
synoviocyteswereanalyzed.
Results
CollagenproductionandPLOD2geneexpressionbytheFLSwereincreased1.8-
fold(p<0.05)and6.0-fold(p<0.01),respectively,inthepresenceofFCM,relative
tocontrolcultureswithoutFCM.Moreover,themigrationandproliferationofsyn-
oviocyteswerestimulatedbyFCM.Collagenproductionwaspositivelyassociated
withPGF2αlevelsintheFCM(r=0.89,p<0.05),andinhibitionofPGF2αlevelsreduced
theextentofFCM-inducedcollagenproductionandPLOD2expression.Inhibition
ofTGFβsignalinghadnoeffectonthepro-fibroticchanges.
Conclusion
TheseresultsindicatethattheIPFPcancontributetothedevelopmentofsynovial
fibrosis in theknee jointby increasingcollagenproduction,PLOD2expression,
cell proliferation, and cellmigration. In addition,whereas the findings showed
thatTGFβisnotinvolved,themorerecentlydiscoveredpro-fibroticfactorPGF2α
appearstobepartiallyinvolvedintheregulationofpro-fibroticchanges.

Infrapatellar fat pad and synovial fibrosis 39
3
INTRODUCTION
Osteoarthritis(OA)isamultifactorialdiseaseofthearticularjoints,withaninci-
dencethatishigherinwomen,obesesubjects,andolderindividuals1;2.Therole
ofthesynoviuminOApathologyisbecomingmoreevident.Inconjunctionwith
cartilagedamageandbonealterations,thepathologic featuresof inflammation,
hyperplasia,andextensivefibrosisarealsooftenobservedinthesynoviumofOA
joints3-5.
Fibrosis can be seen as an abnormal healing process that is characterized
byexcessivedepositionof extracellularmatrixproteins, inparticular collagen,
which,inturn,resultsinalterationofthestructureofthetissueand,finally,even
lossof functionof this tissue.Fibroticprocessesarearesponse toavarietyof
insults,suchasinfection,trauma,autoimmunity,orinflammation,resultinginan
inflammatoryreactionwithrapidrecruitmentofmonocytesfromthecirculation
ormacrophages resident in the tissue.Thesecells are important sourcesof fi-
broticcytokines,suchastransforminggrowthfactorβ(TGFβ)andplatelet-derivedgrowthfactor,that,inturn,recruitfibroblaststothesiteofinjuryandstimulate
themtoproliferate6.
Fibroblastscanalsodifferentiate towardmyofibroblasts.Myofibroblasts,which
are characterized by the presence of α-smoothmuscleactin,arepresentduring
normaltissuerepair,butwhenthewoundisclosed,theydisappearfromthesite.In
thecaseoffibrosis,myofibroblastspersistinthedamagedtissue7-9.Anadditional
hallmarkoffibrosisistheincreasedlevelofhydroxyallysinecollagencrosslinks,
which is regulatedby lysylhydroxylase2b (LH2b), anenzymeencodedby the
gene for procollagen-lysine, 2-oxoglutarate 5-dioxygenase 2 (PLOD2)10. These
hydroxyallysinecollagencrosslinksare found infibrotic tissuesandareassoci-
atedwithirreversibleaccumulationofcollagen11.Recently,itwasdemonstrated
thatPLOD2expressionandthepresenceofLH2bareup-regulatedinthefibrotic
synoviumofmicewithOA12.
TGFβisapotentinducerofPLOD2expressionandLH2bactivity12;13,makingTGFβ
averypotentfibroticgrowthfactorinvolvedinalloftheprocessesseeninfibro-
sis. Inaddition toTGFβ,prostaglandinF2α (PGF2α)wasrecentlydiscoveredasa
cytokinethatfacilitatespulmonaryfibrosisindependentofTGFβ.Micelackingthe
PGF2αreceptordidnotdeveloppulmonaryfibrosisinresponsetobleomycin,and
cellsstimulatedwithPGF2αproducedmorecollagen14;15.

40 CHAPTER 3
Inadditiontocartilage,menisci,ligaments,andsynovium,thekneejointcontains
fatpads.Oneofthelargestofthefatpadsistheinfrapatellarfatpad(IPFP).The
mainroleofthe IPFPisto facilitatedistributionofsynovialfluidanddistribute
mechanicalforcesthroughthekneejoint.Severaladipokinesandcytokines,such
astumornecrosisfactorα,interleukin-6(IL-6),IL-10,leptin,andvascularendothe-
lialgrowthfactor,areknowntobeproducedbytheIPFP16-20.TheIPFPislocated
incloseproximitytothesynoviallayersandcartilagesurfaces,makingtheIPFP
abletoinfluenceinflammatoryprocessesintheknee21.Manysecretedproteinsare
derivedfromthenon-adipocytefractionofadiposetissue(macrophages,Tcells,
andBcells)18;22,andit issuggestedthatmostofthecytokinesproducedbythe
adiposetissuearemacrophage-derived23;24.
Sincesynovialfibrosisisoftenseeninend-stageOA,thegoalofthepresentstudy
was to investigate whether the IPFP and its secreted factors influence fibrotic
processesinsynovialfibroblasts,andtodeterminetheroleof2potentfibroticin-
ducers,TGFβandPGF2α,intherelationshipbetweentheIPFPandsynovialfibrosis.
MATERIALS AND METHODS
Preparation and analysis of fat-conditioned medium
Samples of IPFP were derived from anonymized leftover knee tissue material
obtainedfrompatientswithOAwhohadundergonetotalkneearthroplasty.The
IPFP sampleswereused toproduce FCM.Thepatients implicitly consented to
theuseofthesetissuesforscientificresearch,inaccordancewiththeguidelines
oftheFederationofBiomedicalScientificSocieties(http://www.federa.org),with
approval from the local ethics committee in Rotterdam, The Netherlands (ap-
provalno.MEC2008-181).Themeanageofthedonorswas67.9years(range54–81
years)andthemeanbodymassindex(BMI)ofthedonorswas30.52kg/m2(range
19.6–44.5kg/m2).Theinnerpartsofthefatpads,wherenosynoviumispresent,
werecutintosmallpiecesof±10mgandculturedinsuspensionfor24hoursina
concentrationof50mgtissue/mlinDulbecco’smodifiedEagle’smedium(DMEM)
withGlutamax(GibcoBRL),containinginsulin,transferrin,selenicacid,andalbu-
min(ITS+)(dilution1:100;BDBiosciences)aswellas50µg/mlgentamicinand1.5
µg/mlFungizone(bothfromGibcoBRL).Asacontrolmedium,weusedidentically
composedculturemediumthatdidnotcontainpiecesofIPFP,culturedinparallel.
After24hours,themediumwasharvested,centrifugedat300gfor8minutesto
remove(immune)cells,andfrozenat -80°Cinaliquotsof1.5ml,resultingin29

Infrapatellar fat pad and synovial fibrosis 41
3
differentbatchesofFCM.Thisincubationtimewaschosenarbitrarily,sinceeach
mediatorhasitsownoptimumregardingreleasekinetics22;25-27.
Isolation and culture of fibroblast like synoviocytes (FLS)
Samples of human synoviumwere also obtained as anonymized leftovermate-
rialfrompatientswithOAwhohadundergonetotalkneearthroplasty(approval
no.MEC2004-322).Onthebasisofitsspecificstructure,thesynoviumcouldbe
distinguishedandremovedfromtheadjacenttissue.Thesynoviumsampleswere
thendigestedinPronase(2mg/ml;Sigma)for2hoursandincollagenaseB(1.5
mg/ml;RocheDiagnostics)overnight.Digestedcellswereplatedoutas3,500cells
per cm2 and expanded in Iscove’smodifiedDulbecco’smediumwith 10% fetal
calfserum(FCS),50µg/mlgentamicin,and1.5µg/mlFungizone(all fromGibco
BRL).Cells frompassage 3were allowed to adhere at adensityof 50,000 cells
percm2inDMEMwithGlutamax,10%FCS,andantibiotics(allfromGibcoBRL).
Afterovernightattachment,theculturemediumwasremovedandthecellswere
washedcarefully3timeswithsaline.FCMwasmixed1:1withfreshDMEMwith
Glutamax,supplementedwith50µg/mlgentamicin,1.5µg/mlFungizone,andITS+
(dilution1:100),andappliedtotheattachedFLS.Thereafter,theFLSwerecultured
for4days.ThemeanageoftheFLSdonorswas67years(range60–81years)and
themeanBMIwas32.4kg/m2(range24.2–42.5kg/m2).
ToinvestigatetheinvolvementofTGFβ1orPGF2α,1µMSB505124(Sigma),an
inhibitorofTGFβ1signaling,or10µMAL8810(CaymanChemical),aninhibitorof
PGF2αsignaling,wasadded1hourpriortoaddingtheFCM;aspositivecontrolfor
theinhibition,1ng/mlTGFβ1or1µMPGF2αwasadded.Concentrationsandtiming
werebasedonthosepreviouslydescribedinastudybyOgaetal14.
Analysis of collagen deposition
CollagenwasdeterminedusingtheQuickzymesolublecollagenassayaccordingto
themanufacturer’sguidelines(QuickZymeBiosciences,Leiden,theNetherlands).
Briefly,culturemediumwasremovedandthecell/matrixfractionwassolubilized
byovernightincubationin0.5Maceticacidat4°C.Theassayisbasedonbinding
ofcollagenwithSiriusRed.
Analysis of gene expression
After culture,monolayers of synoviocyteswere suspended in 350µl RLT buffer
(Qiagen,Venlo,theNetherlands)supplementedwith1%β-mercaptoethanol.RNA
wasextractedandcomplementaryDNAwasanalyzedforgeneexpressionusing
previously described methods28. The primer sequences for the genes were as
follows: for the GAPDH reference gene, forward GTCAACGGATTTGGTCGTATT-

42 CHAPTER 3
GGG, reverse TGCCATGGGTGGAATCATATTGG, and probe FAM-CGCCCAATAC-
GACCAAATCCGTTGAC-TAMRA;forthetypeIcollagenα1chaingene(COL1A1),
forward CAGCCGCTTCACCTACAGC, reverse TTTTGTATTCAATCACTGTCTTGCC,
and probe FAM-CCGGTGTGACTCGTGCAGCCATC-TAMRA; for PLOD2, forward
CCCTCCGATCAGAGATGATTandreverseAATGTTTCCGGAGTAGGGGAGTCTTTTT;
and for the gene encoding α-smoothmuscleactin(ASMA),forwardCGTTGCCCCT-
GAAGAGCATandreverseCCGCCTGGATAGCCACATACA.PrimersforthetypeIIIcol-
lagengene(COL3)werepurchasedfromQiagenAssays-on-Demand(QT00058233).
For analysis of GAPDH and COL1A1, TaqMan 2x Universal Polymerase Chain
Reaction(PCR)MasterMix(AppliedBiosystems)wasused in thereaction.For
analysis of PLOD2 and ASMA, quantitative PCRMasterMix Plus SYBRGreen I
(Eurogentec)wasusedinthereaction.Indeterminingtheoptimalhousekeeping
gene,wecomparedGAPDH,18SRNA,2-microglobulin,andhypoxanthineguanine
phosphoribosyltransferase,andobservedthatGAPDHwasthemoststablehouse-
keepinggeneinourexperiments.
Migration assay
Toinvestigatethemigrationofthesynoviocytesinresponsetosolublefactors,a
scratchwoundassaywasperformed.Synoviocytesfrompassage3wereseededat
100,000cellspercm2in12-wellplatesandallowedtoadhereovernightinDMEM
containing10%FCS.A10-µlpipettetipwasusedtomakeascratchintheconfluent
monolayerofthesynoviocytes,aftermarkingthescratchlocationonthebottom
of the well. When applicable, SB505124 or AL8810 was added 1 hour prior to
makingthescratch.Celldebriswasremovedbywashingwithsaline,andthecell
culturewascontinued inDMEM–1%ITS+mixedwithFCM(1:1)withorwithout
SB505124orAL8810.
Photographic imageswereobtaineddirectlyafterscratchingandat14,16,and
19hoursafter scratching.These timepointswerechosenon thebasisofpilot
experimentsshowingthat,from14hoursonward,migrationofthesynoviocytes
isbestvisualized(resultsnotshown)without interferencefromproliferationof
thecells.ClosurewasmeasuredusingTScratchsoftware(ComputationalScience
&EngineeringLaboratory).Theextentofmigrationispresentedasthepercentage
ofclosureafterwounding.
Proliferation assay
Toanalyzeproliferation,synoviocytesfrompassage3wereseededatadensityof
10,000cellspercm2in12-wellplatesandallowedtoadhereovernightinDMEM
containing10%FCS.ToarrestcellsintheS1phase(whichwasnecessaryinorder

Infrapatellar fat pad and synovial fibrosis 43
3
toreducevariation),cellswereculturedinDMEMcontaining0.1%FCSfor24hours
afteradherence.Following24hoursofstarvation, theculturewascontinued in
DMEM–1%ITS+mixedwithFCM(1:1)withorwithouttheadditionofSB505124or
AL8810.Whenapplicable,SB505124orAL8810wasadded1hourpriortoadding
theFCM.SamplesforDNAmeasurementwereobtainedafter1,2,3,and4days
bysuspendingthemonolayerinphosphatebufferedsalinewith0.1%Triton.The
amountofDNAineachsamplewasdeterminedusingethidiumbromide,withcalf
thymusDNA(Sigma)asstandard.
Enzyme-linked immunosorbent assay (ELISA) for TGFβ1
TodeterminetheactivityofTGFβ1intheFCM,ahumanTGFβ1QuantikineELISA
kit(R&DSystems)wasusedaccordingtothemanufacturer’sguidelines.Toacti-
vatelatentTGFβ1totheimmunoreactiveform,acidactivationwith1NHCland
neutralizationwith1.2NNaOH/0.5MHEPESwasperformed.
PGF2α measurements using mass spectrometry
TodeterminethelevelsofPGF2αintheFCMsamplesthatremained(n=7),samples
wereanalyzedwith liquidchromatographytandemmassspectrometry(LC-MS/
MS)asdescribedpreviously29.Briefly,topreparethesamplesformeasurement,
FCM samples,with deuteratedPGF2α -d4 (CaymanChemical) added as internal
standard, were extracted with LC-MS–grade methanol (Riedel-de-Ha¨en). The
methanol extract was loaded on an HLB SPE column (Oasis), after which the
sampleswerereconstitutedin100µlethanolcontainingCUDA(CaymanChemi-
cal)asasecondinternalstandard,andimmediatelyusedforLC-MS/MSanalysis
onanAcquityC18BEHUltraPerformanceliquidchromatographycolumncoupled
toaXevoTQ-Smassspectrometer (Waters).Conevoltageandcollisionenergy
wereoptimizedforeachcompoundindividually.Parentandproductmass/charge
(m/z) values of PGF2α were 353.1 and 193.0. Parent and productm/z values of
PGF2α-d4were357.1and313.4.Parentandproductm/zvaluesofCUDAwere339.1
and214.1.Identificationandquantificationofpeakvalueswereperformedusing
MassLynxsoftwareversion4.1.
Statistical analysis
Experimentsexamining theeffectof FCMwereperformedwith samples from3
differentFLSdonorsand13differentFCMbatchesrepresenting13differentIPFP
donors.ExperimentsexaminingtheeffectofinhibitionofTGFβ1orPGF2α together
withFCMstimulationwereperformedwithsamplesfrom2differentFLSdonors
and8differentFCMbatchesrepresenting8differentIPFPdonors.Allexperiments
wereperformedwithtriplicatesamplespercondition,whichwastakenintoac-

44 CHAPTER 3
countinthestatisticalanalysis.Amixedlinearmodel,followedbyaBonferroni
posthoctest,wasusedtoanalyzegeneexpression,collagendeposition,andcell
migration.Aunivariategenerallinearmodelwasusedtoanalyzetheresultsfrom
theproliferationassays.SincenoteveryFCMbatchwastestedonFLSfromevery
donor,weallowedforthisinthestatisticalanalysisbyaddingasubjectvariable
indicatingtheFLSdonor.Spearman’srhocorrelationsweredeterminedtoexam-
ineassociationsbetweenTGFβ1orPGF2αlevelsandotherparameters.Datawere
analyzedwithIBMSPSSstatisticalsoftware(version20.0).
RESULTS
Induction of fibrotic processes with medium conditioned
by IPFP
Incultureconditionswith8ofthe13FCMbatches(derivedfrom13differentOA
IPFPdonors),collagenproductionbyFLSwas increased1.8-foldafter4daysof
culture, fromamean1.9µg/monolayer in control conditionswithout FCM toa
mean3.4µg/monolayer incultureswithFCM(Figure1A [all 13 included in the
figure]).Inaddition,geneexpressionoftheenzymeinvolvedintheformationof
pyridinolinebasedcollagencrosslinks,PLOD2,wasincreased6.0-foldinthepres-
enceofFCM.Surprisingly,COL1A1expressiononday4was2.5-fold lowerthan
Figure 1 The effect of fat conditionedmedium (FCM)onA) total collagenprodutionby FLSsinmonolayerafter4daysofcultureandB)geneexpressionafter4daysofculturerelativetothecontrolwithoutFCM(setat1)ofgenesdescribingafibroticprocess:Col1(coll1,α1chain),procollagen-lysine,2-oxoglutarate5-dioxygenase2(Plod2)andαsmoothmuscleactin(Asma).Atotalof13differentFCMbatcheswastestedonFLSofthreedifferentdonors.Barsrepresentthemean±standarddeviation.Box-whiskerplotsindicatethe75thand25thpercentilewiththemedian(boxes)andthemaximumandtheminimum(whiskers).*indicatesp<0.05,**indicatesp<0.01.

Infrapatellar fat pad and synovial fibrosis 45
3
thatincontrolconditionswithoutFCM,andASMAexpressionwas1.7-foldlower
(Figure1B).COL3expressionwasunalteredbytheadditionofFCM(resultsnot
shown).Theobservedincrease incollagenproductionbutdecrease inCOL1A1
expressionmightbeexplainedbythehypothesisthatalteredprocessingofthe
collagenwouldleadtomoreefficienttranslation,butwouldnotalterexpression
ofCOL3.Also,thecollagendepositionrepresentsaccumulationinthetotalculture
for4days,whereasthecollagengeneexpressionisthespecificexpressionatthe
momentofharvest.
Since TGFβ1 is known to be a potent inducer of collagen deposition and of
COL1A1,PLOD2,andASMAexpression,wealsoincluded,asapositivecontrola
cultureconditioninwhichTGFβ1wasaddedinalloftheexperiments.Indeed,irre-
spectiveofwhichFLSdonorwasused,TGFβ1inducedthesamefibroticprocesses
asseeninFLScultureswithFCM(resultsnotshown).
To investigatewhether theBMIof the IPFPdonor influenced theeffectof FCM
onFLSs,weperformedapost hocsubgroupanalysiscomparingtheFCMbatches
madefromIPFPsofdonorswhohadaBMIlowerthan30kg/m2(n=5)withFCM
batchesmadefromIPFPsofdonorswhohadaBMIequaltoorhigherthan30kg/
m2(n=8).NodifferencesincollagendepositionorexpressionofCOL1A1,PLOD2,
orASMAwereobservedbetweenthe2BMIsubgroups.Bothgroupsstillshowed
significantdifferencesingeneexpressionwhencomparedwiththecontrolcondi-
tionwithoutFCM(Figure2).
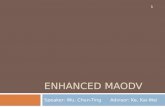
TodeterminetheeffectsonFLSmigration,weperformedascratchwoundassay
(typicalexamplesrightafterscratchingand19hoursafterscratchingareshown
in Figures3AandB).MigrationofFLS(p=0.005)andproliferationofFLS(p=0.002)
werestimulatedinthepresenceofFCM(Figures3CandD).
Association of FCM effects with the presence of TGFβ1 or PGF2α.
TGFβ1andPGF2αarebothknownaspotentpro-fibroticmediatorsandcandidates
tobe involved in theprocessesseen in theFLS inresponse toFCM.Themean
TGFβ1contentoftheFCMwas37.3pg/ml,rangingfrom0.1pg/mlto74.9pg/ml.
ThemeanPGF2αcontentintheFCMwas6,204pg/ml,rangingfrom560pg/mlto
29,718pg/ml.ThelevelofPGF2αwaspositivelycorrelatedwiththeextentofcol-
lagendepositionbytheFLS(Figure4A)andnegativelyassociatedwithCOL1A1
expression(Figure4B).

46 CHAPTER 3
Figure 2 TheeffectofFCMsubdived innonobese(BMI<30,n=5,1maleand4 female)andobese(n≥30,n8,1maleand7female)donorsonA)collagendepositionB)collagentype1geneexpression,C)Plod2geneexpression,andD)Asmageneexpressionbysynoviocytes.ThedottedlineindicatesthelevelsinthecontrolconditionwithoutFCM.**indicatessignificantlydifferentfrom control conditionwithp<0.01, ***indicates significantly different from control conditionwith p<0.005.Barsrepresentthemean±standarddeviation.
ThelevelofTGFβ1waspositivelyassociatedwithCOL1A1expression(Figure
4C).Nootherassociationswereseen.
To evaluate the effect of TGFβ1 and PGF2α on FLS in our culture system,we
addedthesecompoundstoFLScultureswithoutthepresenceofFCM.Theaddi-
tionof1ng/mlTGFβ1increasedtotalcollagendeposition,COL1A1expression,and
ASMAexpression.Theadditionof1µMPGF2α increasedPLOD2expressionand
totalcollagendeposition(Figures5AandD-F).TGFβ1andPGF2α both increased
themigrationof theFLS,buthadnoeffectonproliferationof theFLS (Figures
5BandC).TheeffectsofPGF2αbestsimulatedtheeffectsofFCMasseeninour
experiments(asdescribedinFigures1and2).

Infrapatellar fat pad and synovial fibrosis 47
3
Counteraction of the pro-fibrotic effect of FCM via inhibition of PGF2α signaling.
ToexaminetheinvolvementofTGFβ1andPGF2αinthepro-fibroticeffectofFCM,
theFLSwereculturedwithFCMwithorwithoutaTGFβ1receptortypeIkinaseinhibitor, SB505124, or a selective PGF receptor antagonist, AL8810. First, we
verifiedwhetherSB505124couldindeedinhibittheeffectof1ng/mlTGFβ1,andwhetherAL8810couldindeedinhibittheeffectof1µMPGF2α.SB505124blocked
Figure 3 TheeffectofFCMonmigrationandproliferationofFLSdeterminedbyascratch-woundassay.(A)Picturesofthescratchweretakendirectlyaftermakingthescratchand(B)aftermigrationfor19hours.ThelinesatthetopofAandBmarkthebottomofthewellasreferencepointfortakingpicturesduringmigra-tion.TheeffectofFCMon(C)migrationaspercentageopenand(D)proliferationasµgDNApermonolayerwastested.Atotalof9differentFCMbatcheswastestedonFLSofthreedifferentdonors.*indicatesp<0.05regard-ingthetotalmigrationandproliferationcurves.Dataareshownasmeanmigrationorproliferation±standarddeviationof9FCMbatches.
Figure 4 AssociationsbetweenconcentrationofTGFβ1andPGF2αintheFCMandtheeffectofFCMontheFLSinculture.A)apositiveassociationbetweenthelevelofPGF2αintheFCMandcollagendepositionbytheFLS(R=0.89,p=0.028)B)anegativeassociationbetweenPGF2αintheFCMandCol1geneexpression(R=-0.82,p=0.023),andC)apositiveassociationbetweenTGFβ1intheFCMandCol1geneexpression(R=0.77,p=0.012).Thep-valueswerecorrectedformultipletesting.

48 CHAPTER 3
theeffectofTGFβ1oncollagenproduction,COL1A1expression,andASMAexpres-
sion,confirmingtheefficacyoftheinhibitor.AL8810inhibitedtheeffectofPGF2α
oncollagenproductionandtherewasatrendtowardnormalizationofPLOD2
expression(p=0.08)(Figures5AandD–F).Thepresenceof1µMSB505124or10
µMAL8810aloneseemedtohavenoinfluenceoncollagendepositionorCOL1A1,
PLOD2,andASMAexpression(Supplementaryfigure1).
Inhibition of TGFβ/activin receptor–like kinase 5 signalingwith SB505124 did
notalter theFCM-inducedeffectsonFLS, indicating that theeffectofFCMwas
notcausedbyTGFβ.BlockingthePGFreceptorwithAL8810,ontheotherhand,
inhibitedtheincreaseincollagendepositionthathadbeeninducedbyFCM,bring-
ingthecollagendepositionbacktothelevelsseenincontrolconditionswithout
FCM(Figure6A).TheincreaseinPLOD2expressioninducedbyFCMwassimilarly
abrogated,with a return to the levels seen in control conditionswithout FCM,
whentheFLSwereco-incubatedwithFCMandAL8810(Figure6E).
Figure 5 Theeffectof1ng/mlTGFβ1and1µMPGF2αandtheirinhibitorsSB505124andAL8810intheabsenceofFCMonA)collagenproduction,B)migration,andC)proliferationandgeneexpressionofC)Col1α1,D)Plod2andE)AsmabyFLSsrelativetothecontrolwithoutthesead-ditions(setat1).AllanalysesweredoneintriplicatewiththreeFLSdonors.*indicatesp<0.05,**indicatesp<0.01.Barsordotsrepresentthemean±standarddeviation.

Infrapatellar fat pad and synovial fibrosis 49
3
TheeffectsofFCMonthemigrationandproliferationofsynoviocytesandon
thelevelofASMAexpressionwerenotcounteractedbytheadditionofthePGF
receptorinhibitorAL8810(Figures6B,C,andF).COL1A1expression,whichhad
beendecreasedinFLScultureswithFCM,wasdecreasedevenmoreincultures
withAL8810(Figure6D).ThisisconsistentwiththeminimaldecreaseinCOL1A1
expressionthatwasobservedwhenonlyAL8810wasaddedtotheFLScultures
(Figure5D).
DISCUSSION
OAisadiseaseofthearticularjointsinwhichsynovialfibrosisisoftenseen3,4,12.
Accumulatingdatahavebeenpresented tosuggest thatOA isan inflammatory
Figure 6 TheeffectoftheTGFβ/ALK5(SB505124)orPGF2αsignalling(AL8810)inhibitionontheeffectofFCMinFLSculturesonA)collagenproduction,B)migrationandC)proliferationandD)Col1α1geneexpression,E)Plod2geneexpressionandF)Asmageneexpressionbysynoviocytes.Atotalof8differentFCMbatcheswastestedusingFLSoftwodifferentdonors.Thecontrolwith-outFCMwassetat1andindicatedwithadottedlineforthegeneexpressionanalyses.*indicatesp<0.05,***indicatesp<0.005.Barsordotsrepresentthemean±standarddeviationof8differentFCMbatches.

50 CHAPTER 3
disease inwhichcytokinesand immunecellsplaya role30.Adipose tissuecan,
ingeneral,beconsideredtobeanendocrineorganthatsecretescytokinesand
growthfactorsandthatexhibitssignificantinfiltrationofimmunecells,including
macrophages31-33.Inearlierstudiesconductedbyourgroupandotherinvestiga-
tors, itwas shown that the IPFP is able toproduce cytokines, adipokines, and
growthfactors,andtherebycontributestotheirlevelsinthesynovialfluid18-20;34.
In the current study, we demonstrate thatmedium conditioned by samples of
IPFPobtained from the joints of patientswith end-stageOA stimulates fibrotic
processesinFLS.
Culturing theFLSwithFCM increasedcollagenproduction, theexpressionof
PLOD2encoding for the enzymeLH2b (involved inpyridinoline-basedcollagen
crosslinks),andthemigrationandproliferationofFLS,whicharehallmarksofa
fibrotic process11;13;35.TheseeffectswereindependentoftheBMIoftheIPFPdonor
(BMI<30kg/m2versusBMI>30kg/m2).
TGFβ1,andmorerecently,PGF2α14,havebeensuggested toactaspro-fibrotic
factorsinthejoints.WefoundthatbothTGFβ1andPGF2αwerepresentintheFCM
batchesusedforculturewiththeFLS;thisfindingisinadditiontothepreviously
describedpresenceofmanyother cytokines, adipokines, and growth factors17.
WhenwecomparedthelevelsofTGFβ1andPGF2αintheFCMwithourfunctional
parameters,we foundapositiveassociationbetweenPGF2α levelsandcollagen
deposition,anegativeassociationbetweenPGF2αlevelsandCOL1A1expression,
andapositiveassociationbetweenTGFβ1levelsandCOL1A1expression.These
associations indicate that PGF2αwas responsible for someof the effects of the
FCM.The absenceof associationsbetweenPGF2α levels andPLOD2expression
andbetweenTGFβ1levelsandASMAexpressionmightbeexplainedbythefact
thattheFCMcontains,inadditiontoPGF2αandTGFβ1,manyotherunknownfac-
torsthatcouldalsohaveinfluencedthefibroticprocessesinFLS.
Furthermore,ourexperimentsindicatethattheeffectsofFCMonFLSarecom-
parabletotheeffectsofaddingPGF2αtoFLScultureswithoutFCM,againindicat-
ingthatthepresenceofPGF2αcontributestotheFCMeffect.Theprofibroticeffect
ofFCMmaybeattributablenotonlytothePGF2αpresentintheFCM,butalsoto
thePGF2αthatisproducedbyFLSinresponsetoFCM.Fibroblasts,ingeneral,are
knowntoproducePGF2α36;37.Thismayexplainthediscrepancybetweenourfind-
ingsofPGF2αincreasingPLOD2expressionandAL8810bringingPLOD2expression
backtocontrol levelsandourfindingsoftheabsenceofacorrelationbetween
PGF2αlevelsintheFCMandPLOD2expression.
MessengerRNA(mRNA)andproteinlevelsare,ingeneral,associatedwitheach
other.ThiswastruefortheCOL1A1mRNAandproteinlevelsinthisstudy,when
we cultured the FLSwith TGFβ1.However, collagen deposition is regulated on

Infrapatellar fat pad and synovial fibrosis 51
3
manylevels,anditsregulationthroughvariationintheamountofmRNAisonly
thebeginning.Forexample,aftersynthesisofthedifferentcollagenchains,post-
translationalmodificationthroughenzymessuchasthelysylandprolylhydroxy-
lasesandlysyloxidasescanoccur,whilecorrectfoldingofthecollagenmolecules
requirestheinvolvementofchaperonessuchasHsp47.Thesechangesnotonly
aredirectlyinvolvedincollagensynthesisbutalsocanindirectlyregulatecollagen
content.Thelevelofcollagencrosslinking,forexample,canhaveaneffectonthe
sensitivityofcollagentodegradationbymatrixmetalloproteinases38.Ofcourse,
degradationofcollagencanhaveamajorroleindeterminingtowhatextentcol-
lagencontentincreasesovertime.Inthisrespect, it isveryexcitingtoseethat
despiteareductionintypeIcollagenmRNA,thepresenceofFCMorPGF2α does
result in increasedcollagendeposition, and that therearedifferencesbetween
stimulationwithPGF2α andstimulationwithTGFβ1.Unfortunately,wewerenot
abletoquantifydepositionofspecifictypesofcollagen.
TofurtherexaminetheinvolvementofTGFβ1andPGF2αpresentintheFCMin
thedifferentfibroticprocesses,weusedaTGFβ1receptortypeIkinaseinhibitor,SB505124, anda selectivePGF2α receptorantagonist,AL8810, togetherwith the
FCMincubation.BlockadeofPGF2αwithAL8810broughtcollagendepositionand
PLOD2expressionbacktothelevelsincontrolconditionswithoutFCM,whereas
thepresenceoftheTGFβ1inhibitorSB505124didnotaltertheFCMeffectonFLS.
Since theadditionofAL8810decreasedPLOD2expression,our results indicate
indirectly that PGF2α levels are associated with PLOD2 expression, in addition
to the already-shown association between PGF2α and collagen production. The
latterisconfirmedbythefactthatinhibitionofthePGF2αreceptorwithAL8810
normalizedcollagendepositioninFCM-treatedFLS.InhibitionofTGFβ1signalingwithSB505124incombinationwithFCMdidnotnormalizecollagendepositionor
PLOD2expression.Fromtheseresults,weconcludethatPGF2αmightbeamore
importantfactorthanTGFβ1intheFCM-inducedfibroticprocessesinFLS.
NoeffectoftheinhibitorswasseenontheFCM-inducedmigrationandprolifera-
tionofsynoviocytes,andco-incubationofFCMwithAL8810decreasedCOL1A1
expressionevenmorethanthatwithFCMalone.Thus,nexttoPGF2α,otherfactors
alsoinfluencedtheparametersoffibrosis,sincenotallprocessesinducedbyFCM
werecounteractedbyAL8810.Inaddition,theextrainhibitionofCOL1A1expres-
sionthatoccurredwhentheFLSwereculturedwithFCMandAL8810couldbe
explainedbythefactthat,inourculturesystem,thereisnodirecteffectofPGF2α
onCOL1A1expressionandthatotherfactorsareinvolvedinthisrelationship.
Likeotherorgans,adiposetissuecontainsaresidentpopulationofcellsofthe
innate immune system, in particular macrophages and T lymphocytes. In our
earlierstudy,wedemonstratedthatmacrophageswerepresentintheIPFP,many

52 CHAPTER 3
ofwhichhaveanM2phenotype39.AlternativelyactivatedM2macrophageshave
ananti-inflammatoryorrepairphenotypeandproduce,predominantly,IL-10but
also growth
factorssuchasTGFβ1andinsulin-likegrowthfactor1,andalmostnoIL-12or
IL-2340.ThepresenceofM2macrophages in the IPFPofpatientswithend-stage
OAmightcontributetotheprofibroticeffectoftheFCMonFLSdescribedinthe
presentstudy.Earlierstudiesalsofoundthatmacrophagesareabletoproduce
PGF2α41;42.Inadditiontomacrophages,adipocytes,Tlymphocytes,orothercells
fromthestromalvascularfractionmightalsocontributetoPGF2α production in
theIPFP43.
Prostaglandins,includingPGD2,PGE2,PGF2α,andPGI2,areproducedwhenphos-
pholipidsarecleavedinresponsetostimuli,resultinginthereleaseofarachidonic
acid,which is thenmetabolizedbycyclooxygenase toproduceprostaglandins.
PGF2α isconsideredtobeamajorandstablemetaboliteofPGE244.Reductionin
PGE2productionistheclassicmodeofactionofanti-inflammatoryagentssuch
asnonsteroidalanti-inflammatorydrugs(NSAIDs),whicharecommonlyusedin
medicalmanagementofOA,andnumerousstudieshavedemonstrateda lower
PGE2concentrationinsynovialfluidfollowingNSAIDtreatment45;46.Morerecently,
PGF2αwasalsofoundinthesynovialfluidofhorses,thelevelsofwhichincreased
afterstimulationofacute inflammationandwhichwereshowntobedecreased
after thetreatmentof inflamedkneeswithanNSAID47.NSAIDsmight, therefore,
alsobeusefulinthepreventionofthesynovialfibrosisseeninOA.
Toourknowledge,thisisthefirststudytoexaminetheeffectofadiposetissue
onthesynoviumandtoassessthepotentialinvolvementoftheIPFPonthedevel-
opmentofthesynovialfibrosisoftenseeninOA3.Theresultsofthisstudyindicate
thattheIPFPinthekneesofpatientswithend-stageOAnotonlyinhibitscatabolic
mediatorsincartilage39butalsoexertspro-fibroticeffectsonthesynovium,and
thesepro-fibroticeffectscanbepartiallyexplainedbythepresenceofPGF2α.How-
ever,sincenotallofthefibroticeffectscanbeexplainedbythepresenceofPGF2α,
otherfactorsmayalsoplayarole.Additionalexperimentsarerequiredtoexamine
theeffectofFCMontheentireOAfibroticprocess,andtoinvestigatewhetherthe
effectthatwefoundisspecifictotheIPFPinend-stageOAorwhethertheIPFP
fromanearlierstageofOAwouldhavethesamepro-fibroticeffect.Futurestud-
iesshouldalsoinvestigatewhetherFLSfrompatientswithOAinanearlierstage
wouldrespondinamannercomparabletothatofFLSfrompatientswithend-stage
OA.Inaddition,itshouldbeexaminedwhetherOApatientshaveincreasedlevels
ofPGF2αintheirsynovialfluidandwhetherthisisassociatedwithseverechanges
intheirsynovium.Thecontinuingexpansionofthisknowledgemighteventually
contributetomoreoptimaltreatmentoreventhepreventionofOA.

Infrapatellar fat pad and synovial fibrosis 53
3
REFERENCES
1. Yusuf E, Bijsterbosch J, SlagboomPE, Rosendaal FR,Huizinga TW,KloppenburgM. Bodymass
indexandalignmentandtheirinteractionasriskfactorsforprogressionofkneeswithradiographic
signsofosteoarthritis.OsteoarthritisCartilage2011;19:1117–22.
2. ReijmanM,PolsHA,BerginkAP,HazesJM,BeloJN,LievenseAM,etal.Bodymassindexassociated
withonsetandprogressionofosteoarthritisofthekneebutnotofthehip:theRotterdamStudy.
AnnRheumDis2007;66:158–62.
3. Revell PA,MaystonV, Lalor P,MappP.The synovialmembrane in osteoarthritis: a histological
studyincludingthecharacterisationofthecellularinfiltratepresentininflammatoryosteoarthritis
usingmonoclonalantibodies.AnnRheumDis1988;47:300–7.
4. HuttonCW,HintonC,DieppePA.Intra-articularvariationofsynovialchangesinkneearthritis:bi-
opsystudycomparingchangesinpatellofemoralsynoviumandthemedialtibiofemoralsynovium.
BrJRheumatol1987;26:5–8.
5. Loeuille D, Chary-Valckenaere I, Champigneulle J, Rat AC, Toussaint F, Pinzano-Watrin A, et al.
Macroscopicandmicroscopicfeaturesofsynovialmembraneinflammationintheosteoarthritic
knee: correlating magnetic resonance imaging findings with disease severity. Arthritis Rheum
2005;52:3492–501.
6. Gharaee-KermaniM,PhanSH.Roleofcytokinesandcytokinetherapyinwoundhealingandfibrotic
diseases.CurrPharmDes2001;7:1083–103.
7. Gabbiani G. The myofibroblast in wound healing and fibrocontractive diseases. J Pathol
2003;200:500–3.
8. DesmouliereA,GeinozA,GabbianiF,GabbianiG.Transforminggrowthfactor-1induces-smooth
muscleactinexpression ingranulation tissuemyofibroblastsand inquiescentandgrowingcul-
turedfibroblasts.JCellBiol1993;122:103–11.
9. Ronnov-JessenL,PetersenOW.Inductionof-smoothmuscleactinbytransforminggrowthfactor-1
inquiescenthumanbreastglandfibroblasts:implicationsformyofibroblastgenerationinbreast
neoplasia.LabInvest1993;68:696–707.
10. VanderSlotAJ,ZuurmondAM,BardoelAF,WijmengaC,PruijsHE,SillenceDO,etal. Identifica-
tionofPlod2astelopeptidelysylhydroxylase,animportantenzymeinfibrosis.JBiolChem2003;
278:40967–72.
11. VanderSlotAJ,ZuurmondAM,vandenBogaerdtAJ,UlrichMM,MiddelkoopE,BoersW,etal.
Increasedformationofpyridinolinecross-linksduetohighertelopeptidelysylhydroxylaselevels
isageneralfibroticphenomenon.MatrixBiol2004;23:251–7.
12. RemstDF,BlaneyDavidsonEN,VittersEL,BlomAB,StoopR,SnabelJM,etal.Osteoarthritis-related
fibrosisisassociatedwithbothelevatedpyridinolinecross-linkformationandlysylhydroxylase2b
expression.OsteoarthritisCartilage2013;21:157–64.
13. VanderSlotAJ,vanDuraEA,deWitEC,DeGrootJ,HuizingaTW,BankRA,etal.Elevatedformation
ofpyridinolinecross-linksbyprofibroticcytokinesisassociatedwithenhancedlysylhydroxylase
2blevels.BiochimBiophysActa2005;1741:95–102.
14. Oga T,Matsuoka T, Yao C, NonomuraK, Kitaoka S, SakataD, et al. Prostaglandin F2α receptor
signalingfacilitatesbleomycininducedpulmonaryfibrosisindependentlyoftransforminggrowth
factor-β.NatMed2009;15:1426–30.
15. OlmanMA.BeyondTGF-β:aprostaglandinpromotesfibrosis.NatMed2009;15:1360–1.

54 CHAPTER 3
16. ChenWP,BaoJP,FengJ,HuPF,ShiZL,WuLD. Increasedserumconcentrationsofvisfatinand
its production by different joint tissues in patients with osteoarthritis. Clin Chem Lab Med
2010;48:1141–5.
17. ClockaertsS,Bastiaansen-JenniskensYM,FeijtC,DeClerckL,Verhaar JA,ZuurmondAM,etal.
Cytokineproductionby infrapatellar fatpadcanbestimulatedby interleukin1and inhibitedby
peroxisomeproliferatoractivatedreceptoragonist.AnnRheumDis2012;71:1012–8.
18. Klein-Wieringa IR, Kloppenburg M, Bastiaansen-Jenniskens YM, Yusuf E, Kwekkeboom JC, El-
BannoudiH, et al.The infrapatellar fatpadofpatientswithosteoarthritishasan inflammatory
phenotype.AnnRheumDis2011;70:851–7.
19. PresleN,PottieP,DumondH,GuillaumeC,LapicqueF,PalluS,etal.Differentialdistributionof
adipokinesbetweenserumandsynovialfluidinpatientswithosteoarthritis:contributionofjoint
tissuestotheirarticularproduction.OsteoarthritisCartilage2006;14:690–5.
20. UshiyamaT,ChanoT,InoueK,MatsusueY.Cytokineproductionintheinfrapatellarfatpad:another
sourceofcytokinesinkneesynovialfluids.AnnRheumDis2003;62:108–12.
21. ClockaertsS,Bastiaansen-JenniskensYM,RunhaarJ,vanOschGJ,VanOffelJF,VerhaarJA,etal.
Theinfrapatellarfatpadshouldbeconsideredasanactiveosteoarthriticjointtissue:anarrative
review.OsteoarthritisCartilage2010;18:876–82.
22. FainJN,MadanAK,HilerML,CheemaP,BahouthSW.Comparisonofthereleaseofadipokinesby
adiposetissue,adiposetissuematrix,andadipocytesfromvisceralandsubcutaneousabdominal
adiposetissuesofobesehumans.Endocrinology2004;145:2273–82.
23. Fain JN. Release of interleukins and other inflammatory cytokines by human adipose tissue is
enhancedinobesityandprimarilyduetothenonfatcells.VitamHorm2006;74:443–77.
24. FainJN,TichanskyDS,MadanAK.Mostoftheinterleukin1receptorantagonist,cathepsinS,mac-
rophagemigrationinhibitoryfactor,nervegrowthfactor,andinterleukin18releasebyexplantsof
humanadiposetissueisbythenon-fatcells,notbytheadipocytes.Metabolism2006;55:1113–21.
25. FainJN,CheemaPS,BahouthSW,LloydHilerM.Resistinreleasebyhumanadiposetissueexplants
inprimaryculture.BiochemBiophysResCommun2003;300:674–8.
26. FainJN,MadanAK.Regulationofmonocytechemoattractantprotein1(MCP-1)releasebyexplants
ofhumanvisceraladiposetissue.IntJObes(Lond)2005;29:1299–307.
27. FainJN,TageleBM,CheemaP,MadanAK,TichanskyDS.Releaseof12adipokinesbyadiposetissue,
nonfatcells,andfatcellsfromobesewomen.Obesity(SilverSpring)2010;18:890–6.
28. Bastiaansen-JenniskensYM,deBartAC,KoevoetW,JansenKM,VerhaarJA,vanOschGJ,etal.
Elevatedlevelsofcartilageoligomericmatrixproteinduring invitrocartilagematrixgeneration
decreasecollagenfibrildiameter.Cartilage2010;1:200–10.
29. BalversMG,VerhoeckxKC,Meijerink J, Bijlsma S, RubinghCM,WortelboerHM, et al. Time-de-
pendenteffectofinvivoinflammationoneicosanoidandendocannabinoidlevelsinplasma,liver,
ileumandadiposetissueinC57BL/6micefedafish-oildiet.IntImmunopharmacol2012;13:204–14.
30. Pelletier JP,Martel-Pelletier J, Abramson SB.Osteoarthritis, an inflammatory disease: potential
implicationfortheselectionofnewtherapeutictargets[review].ArthritisRheum2001;44:1237–47.
31. KershawEE,FlierJS.Adiposetissueasanendocrineorgan.JClinEndocrinolMetab2004;89:2548–
56.
32. FraynKN,KarpeF,FieldingBA,MacdonaldIA,CoppackSW.Integrativephysiologyofhumanadi-
posetissue[review].IntJObesRelatMetabDisord2003;27:875–88.INFRAPATELLARFATPADAND
SYNOVIALFIBROSIS2079
33. GalicS,Oakhill JS,SteinbergGR.Adiposetissueasanendocrineorgan.MolCellEndocrinology
2010;316:129–39.

Infrapatellar fat pad and synovial fibrosis 55
3
34. DistelE,CadoudalT,DurantS,PoignardA,ChevalierX,BenelliC.Theinfrapatellarfatpadinknee
osteoarthritis: an important source of interleukin-6 and its soluble receptor. Arthritis Rheum
2009;60:3374–7.
35. ShiQ,LiuX,BaiY,CuiC,LiJ,LiY,etal.Invitroeffectsofpirfenidoneoncardiacfibroblasts:prolif-
eration,myofibroblastdifferentiation,migrationandcytokinesecretion.PLoSOne2011;6:e28134.
36. HarksEG,PetersPH,vanDongenJL,vanZoelenEJ,TheuvenetAP.Autocrineproductionofpros-
taglandinF2αenhancesphenotypictransformationofnormalratkidneyfibroblasts.AmJPhysiol
CellPhysiol2005;289:C130–7.
37. OlsonDM,TanswellAK.ProductionofprostaglandinsbyfetalratlungtypeIIpneumonocytesand
fibroblasts.BiochimBiophysActa1989;1003:327–30.
38. VanderSlot-VerhoevenAJ,vanDuraEA,AttemaJ,BlauwB,DegrootJ,HuizingaTW,etal.Thetype
ofcollagencross-linkdeterminesthereversibilityofexperimentalskinfibrosis.BiochimBiophys
Acta2005;1740:60–7.
39. Bastiaansen-JenniskensYM,Clockaerts S, FeijtC,ZuurmondAM,Stojanovic-SusulicV,BridtsC,
etal.Infrapatellarfatpadofpatientswithend-stageosteoarthritisinhibitscatabolicmediatorsin
cartilage.AnnRheumDis2012;71:288–94.
40. VerreckFA,deBoerT,LangenbergDM,vanderZandenL,OttenhoffTH.Phenotypicandfunctional
profilingofhumanproinflammatorytype-1andanti-inflammatorytype-2macrophagesinresponse
tomicrobialantigensandIFN-γ-andCD40Lmediatedcostimulation.JLeukBiol2006;79:285–93.
41. NorwitzER,LopezBernalA,StarkeyPM.Tumornecrosisfactor-αselectivelystimulatesprostaglan-
dinF2αproductionbymacrophagesinhumantermdecidua.AmJObstetGynecol1992;167:815–20.
42. O’Sullivan MG, Chilton FH, Huggins EM Jr, McCall CE. Lipopolysaccharide priming of alveolar
macrophagesforenhancedsynthesisofprostanoidsinvolvesinductionofanovelprostaglandinH
synthase.JBiolChem1992;267:14547–50.
43. IyerA,FairlieDP,PrinsJB,HammockBD,BrownL.Inflammatorylipidmediatorsinadipocytefunc-
tionandobesity.NatRevEndocrinol2010;6:71–82.
44. SamuelssonB.Prostaglandinsandthromboxanes.RecentProgHormRes1978;34:239–58.
45. DeGrauwJC,vandeLestCH,vanWeerenPR.Inflammatorymediatorsandcartilagebiomarkers
insynovialfluidafterasingleinflammatoryinsult:alongitudinalexperimentalstudy.ArthritisRes
Ther2009;11:R35.
46. MastbergenSC,MarijnissenAC,VianenME,ZoerB,vanRoermundPM,BijlsmaJW,etal. Inhibi-
tionofCOX-2bycelecoxibinthecaninegroovemodelofosteoarthritis.Rheumatology(Oxford)
2006;45:405–13.
47. DeGrauw JC, vande LestCH, vanWeerenPR.A targeted lipidomics approach to the studyof
eicosanoidreleaseinsynovialjoints.ArthritisResTher2011;13:R123.

56 CHAPTER 3
Supplementary figure 1TheeffectofTGFβ/ALK5(SB505124)orPGF2αsignalling(AL8810)inhibi-tiononFLSculturesonA)collagenproduction,B)Col1α1geneexpression,C)Plod2geneexpres-sion,andD)Asmageneexpression.AllanalysesweredoneintriplicateononeFLSdonor.Barsrepresentthemean+standarddeviation.



CHAPTER 4
The infrapatellar fat pad from diseased joints
inhibits chondrogenesis of mesenchymal stem cells
Wu Wei Resti Rudjito Niamh Fahy
Jan A.N. Verhaar Stefan Clockaerts
Yvonne M. Bastiaansen-Jenniskens Gerjo J.V.M. van Osch
Eur Cell Mater. 2015 Dec 02;30:303-14

60 CHAPTER 4
ABSTRACT
Cartilagerepairbybonemarrowderivedmesenchymalstemcells(MSCs)canbe
influencedbyinflammationintheknee.Nexttosynovium,theinfrapatellarfatpad
(IPFP)hasbeendescribedasasourceforinflammatoryfactors.Here,weinves-
tigatedwhetherfactorssecretedbytheIPFPaffectchondrogenesisofMSCsand
whetherthisisinfluencedbydifferentjointpathologiesorobesity.Furthermore,
weexaminedtheroleofIPFPresidentmacrophages.First,wemadeconditioned
medium from IPFP obtained fromosteoarthritic joints, IPFP from traumatically
injuredjointsduringanteriorcruciateligamentreconstructionandsubcutaneous
adiposetissue.Additionally,wemadeconditionedmediumofmacrophagesiso-
latedfromosteoarthriticIPFPandofpolarisedmonocytesfromperipheralblood.
WeevaluatedtheeffectofdifferenttypesofconditionedmediumonMSCchon-
drogenesis.Conditionedmedium from IPFPdecreasedcollagen2 andaggrecan
geneexpressionandthioninandcollagentype2staining.Thisanti-chondrogenic
effectwasthesameforconditionedmediumfromIPFPofosteoarthriticandtrau-
matically injured joints. Furthermore, IPFP from obese (BodyMass Index >30)
donorsdidnotinhibitchondrogenesismorethanthatoflean(BodyMassIndex
<25)donors.Finally,conditionedmediumfrommacrophagesisolatedfromIPFP
decreased the expression of hyaline cartilage genes, as did peripheral blood
monocytesstimulatedwithpro-inflammatorycytokines. The IPFPandtheresi-
dentpro-inflammatorymacrophagescouldthereforebetargets for therapiesto
improveMSC-basedcartilagerepair.

Anti-chondrogenic effect of IPFP on MSCs 61
4
INTRODUCTION
Articularcartilagehas limitedself-healingcapabilitiesandsurgical intervention
usingbonemarrowstimulationtechniques,suchasthemicrofractureprocedure,
canbeusedtoactivatemesenchymalstemcells(MSCs)fromtheunderlyingbone
marrow to repair the defect1;2. However, instead of a normal hyaline cartilage
matrix,afibrocartilaginouscartilagematrixfillsupthedefect1;3;4.Anexplanation
why hyaline cartilage production is inhibited could be that the cartilage defect
islocatedinapost-traumaticinflammatoryenvironment5.Inthispost-traumatic
inflammatory environment, circulating inflammatory factors stimulate matrix
degradation and inhibit chondrogenic differentiation6.
Besidessurgicalintervention,researchiscurrentlyfocusedonMSC-basedtissue-
engineered cartilage repair strategies7. In these strategies, repair tissues are
engineered in-vitro using a combination ofMSCs, scaffolds and growth factors
andsubsequentlyimplantedintothecartilagedefect.Whenimplanted,theMSCs
in thesepre-engineeredconstructswillbeexposed to the samepost-traumatic
inflammatory environment as the MSCs after the microfracture procedure. An
inflammatoryenvironmentcaninhibithyalinecartilagematrixproduction8.
AnotherfactorthatcouldinfluenceMSCchondrogenicdifferentiationisobesity.
Theclinicalresultsafterthemicrofractureprocedurearereportedtobeworsein
patients with obesity9.Obesityisknowntocausesystemicmetabolicandinflam-
matorychanges,withincreasedcirculatinginflammatoryfactors10.
Inflammatoryfactorscanbeproducedbydifferenttissuesofthekneejoint,the
mostwelldescribedbeingthesynoviumandcartilage.Theinfrapatellarfatpad
(IPFP) is an adipose tissue located extra-synovially and intra-capsularly. It is
richlyvascularised,innervatedandknowntoalsosecretemanyadipokinesand
cytokines11;12.Adiposetissueinobesepatientshasbeenshowntohaveaninflam-
matoryphenotypewithabundantimmunecellinfiltrationandsecretionofinflam-
matory cytokines13. Furthermore, joint trauma and joint degradation can both
increaseinflammationintheIPFPandthesecretionofinflammatoryfactors12;14-16.
TheIPFPcontainsimmunecellssuchasmacrophages15;17.Macrophagesplayan
importantroleininflammationandwoundhealing.Macrophagescanbecatego-
rizedintopro-inflammatorymacrophagesandanti-inflammatoryorwoundhealing
macrophages18;19.Inflammationorobesityoftenresultinincreasednumbersofin-

62 CHAPTER 4
flammatorymacrophages.Previouslywehaveshownthatonlypro-inflammatory
andnotanti-inflammatorymacrophagesinhibitMSCchondrogenesisinvitro20.
SincetheIPFPfromend-stageOApatientsisasourceofinflammatoryandcata-
boliccytokines12, it istobeexpectedthat IPFPsecretedfactors influenceother
jointtissues.AgainstourexpectationthatthefactorsreleasedfromIPFPwould
stimulate tissue degradation, our previous studies demonstrated that factors
releasedfromIPFPfromend-stageOApatientsinhibitcatabolicmediatorsincarti-
lage15andstimulatefibroticprocessesinsynovialfibroblasts21.Thisindicatesthat
thefactorsreleasedbytheIPFPnotonlyhaveapro-inflammatoryeffectonjoint
environmentandthatthiseffectcouldbedifferentineachtypeofjointtissue.
ConsideringtheIPFP’spotentialtoproducefactorsthatinfluencethejointenviron-
ment,andtheknowledgethatthejointenvironmentinfluencescartilagerepair,we
hypothesizedthatfactorssecretedbytheIPFPaffectMSC-basedcartilagerepair.
Inthisstudy,weinvestigatedwhetherandhowfactorssecretedbytheIPFPaffect
thechondrogenesisofMSCsinvitroandwhetherthiscouldbeinfluencedbyjoint
pathologyorobesity.Furthermore,weevaluatedwhethermacrophagespresentin
theIPFPcouldberesponsiblefortheeffectseenonMSCchondrogenesis.
METHODS
Preparation of adipose tissue conditioned medium (CM)
IPFP tissue was obtained as leftover material from patients with OA who had
undergonea total knee replacement (Age66.1years (53.9-80.2);BMI29.3 (21.5-
43.7)),orfrompatientsduringanteriorcruciateligament(LR)reconstruction(Age
29.3 (17.6-48.0); BMI 22.8 (19.3-29.0)),with time from trauma to reconstruction
5.4 months (2-12 months). Subcutaneous adipose tissue (SAT) from patients
undergoingtotalhipreplacementwasused(Age63.0(50.2-79.1);BMI31.3(24.0-
35.8)). Consentwas given in accordancewith the guidelines of the Federation
of Biomedical Scientific Societies (http://www.federa.org) after approval by the
localethicalcommittee(MEC2012-267).Allculturemediafromnowonwardswere
supplementedwith1.5μg/mLfungizoneand50μg/mLgentamicin(bothGibco).
Togenerateadipose tissueCM,adipose tissuewascut intosmallpiecesofap-
proximately9mm2,washedfortwotimeswithsalineandculturedataconcentra-
tionof100mg/mlinDulbecco’sModifiedEagleMediumwithGlutamax(DMEM-HG;
Gibco)supplementedwith1%insulin-transferrin-selenium(ITS+;BDBiosciences)
for24hoursat37ºC.Afterwards,themediumwasharvested,centrifugedat250G

Anti-chondrogenic effect of IPFP on MSCs 63
4
for8minutesandthesupernatantwasstoredat-80ºCforcultureexperiments.
UnconditionedmediumwasgeneratedbyincubationofDMEM-HGsupplemented
withITS+for24hoursat37ºC,centrifugedat250Gfor8minutesandstoredat-80
ºC.
Isolation of macrophages from adipose tissue and preparation of IPFP macrophage CM
Toisolatemacrophagesfromthestromalvascularfractionofadiposetissue,six
OAIPFPsamples(Age66.6(54.1-80.2),BMI28.9(21.9-33.9))wereused.Adipose
tissuesampleswerecutintopiecesofaround9mm2andincubatedovernightat
37ºCwith1mg/mlcollagenaseB(Roche,Germany) inDMEM-HGwith10%FCS.
After centrifugation, the supernatant containing thefloatingadipocytesand fat
was removed, cellpelletwas re-suspendedandfiltered througha100µmfilter
followedbya40µmfilter.Theresultingcellsuspensionwaslayeredontopof15
mlFicoll(Ficoll-Paque™PLUS,GEHealthcare)andseparatedbydensitygradient
following centrifugation at 1,000g for 15minutes. The interphasewas removed
andwashedwithphosphatebufferedsaline(PBS;Gibco)containing2%FCSfol-
lowedbyincubationwithCD45-PE(BDBiosciences)for1hourandincubationin
20µlofanti-mouse-IgGmagneticbeads(MiltenyiBiotec)per10.000.000cellsfor
30minutes inthedarkat4 ºC.CD45positivecellswereseparatedbymagnetic
activatedcellsorting(MACS,MACSSeparationcolumnsLSandMidiMACS™Sepa-
rator,MiltenyiBiotec)accordingtomanufacturer’sinstructions.Flowcytometric
analysiswasperformedtoconfirma>90%CD45+populationpurity.CD45reduced
fractioncontained<10%CD45+cells. IsolatedCD45+cellswereseededatacell
densityof100.000cells/cm2in24wellsplatesandculturedovernightat37ºCin
DMEM-HGsupplementedwith10%FCS.Cellswere thencarefullywashed twice
withPBStoremovenon-attachedcellsandDMEM-HGwith1%ITS+wasadded.
After24hours,IPFPCD45+CMwasharvested,centrifugedat250gfor8minutes
andstoredat-80ºCforfurtherexperiments.
Human monocyte isolation, differentiation and CM preparation
Peripheral blood monocytes were isolated from buffy coats with CD14+ mag-
neticbeads(MiltenyiBiotec)andMACSaccordingtomanufacturer’sinstructions.
Monocyteswerethenseededat500.000cells/cm2,stimulatedtoM(LPS+IFN-ɣ)with
100ng/ml lipopolysaccharide(LPS;SigmaAldrich)and10ng/ml IFN-ɣ (PeproT-
ech)orM(IL-4)with10ng/mlIL-4(Preprotech)19.Subsequently,M(LPS+IFN-ɣ)andM(IL-4)CMweremadeaspreviouslydescribed20;22.Samplesoftheseexperiments
werepreviouslyusedinFahyetal20,butadditionalgeneexpressionanalysiswere
performedforthecurrentstudy.

64 CHAPTER 4
Human dermal fibroblast expansion and CM preparation
Human dermal fibroblast from adult donors (HDFa)were acquired fromGibco
(Cat.no.C-013-5C)andwereseededat5000cells/cm2inDMEM-HGcontaining10%
FCS.Afterreachingsub-confluency,HDFasweretrypsinizedandseededagain.For
HDFaCMpreparation,P4cellswerecultureduntil subconfluency,washedwith
PBSforthreetimesandDMEM-HGwithITS+wasadded.After24hours,CMwas
harvested,centrifugedat250gfor8minutesandstoredat-80ºCforfurtherexperi-
ments.
Isolation and culture of human MSCs
MSCswereisolatedfromheparinizedbonemarrowaspiratesofpatientswithOA
undergoingtotalhipreplacement(9donors;Age61years(32-78)).Patientsgave
informed consent and the studywas approved by the local ethical committee
of theErasmusMC,Rotterdam(MEC2004-142)andAlbertSchweitzerHospital,
Dordrecht(MEC2011-07).Bonemarrowaspirateswereplatedandwashedafter
24hourswithPBS containing 2% fetal calf serum (FCS; Lonza).MSCswere ex-
pandedinMinimumEssentialMedium-Alpha(α-MEM;Gibco)supplementedwith
10%FCS,1ng/mLfibroblastgrowthfactor2(FGF2;R&DSystems)and25μg/mL
ascorbicacid-2-phosphate(Sigma-Aldrich).Afterreachingsub-confluency,MSCs
weretrypsinisedandseededagainatadensityof2500cells/cm2.MSCsofpassage
3or4wereused.
Chondrogenic differentiation of MSCs
MSCs were encapsulated in 1.2% alginate (CP Kelco) in saline at a density of
4.000.000 cells/ml. Beads were formed by purging the MSC-alginate solution
througha23Gneedleandallowingdropletstofallinto102mMCaCl2solution.
Pelletsweremadebycentrifugationof200.000cellsinpolypropylenetubes.Beads
andpelletswereculturedwithDMEM-HGwith ITS+containing25% IPFPCMor
unconditioned medium. As chondrogenic supplements, we used 0.1 µM Dexa-
methasone(Sigma–Aldrich),10ng/mlTGFβ1(R&Dsystems),25μg/mLascorbic
acid-2-phosphate (Sigma-Aldrich),40µg/mlL-Proline (Sigma-Aldrich)and1mM
sodiumpyruvate(Gibco).MSCbeadswereculturedin100µLofmediumperbead
andpelletswereculturedin500µLofmediumperpellet.Mediumwasrefreshed3
timesaweek.Beadsandpelletswereharvestedafter28days.
Fortheexperimentswithmacrophages,obeseversusleanIPFP,osteoarthriticver-
suspost-jointtraumaIPFPandSATversusIPFP,beadswerefirstculturedinDMEM-
HGcontainingITS+andchondrogenicsupplementsfor14days.Fromday14-17,
partsoftheDMEM-HGwithITS+wasreplacedbyconditionedmediumoranequal

Anti-chondrogenic effect of IPFP on MSCs 65
4
percentageofunconditionedmedium.FortheexperimentswithIPFPandSATCM,
wereplaced25%oftheDMEM-HGcontainingITS+.Forthemacrophagesexperi-
ments,wereplaced50%oftheDMEM-HGcontainingITS+withCD45CMor20%
withM(LPS+IFNɣ)/M(IL-4)CM.FortheCD45experiments,thelowestcellnumber
usedtogenerateCM(0.23µgDNA)wassetat50%andfortheM(LPS+IFNɣ)/M(IL-4)
experiments,theaveragecellnumberusedtogenerateCM(1.64µgDNA)wasset
at20%.Allsubsequentdonorswerecorrectedaccordinglytoassurethatmedium
conditionedbyanequalnumberofcellswasadded.Chondrogenicsupplements
werealwaysaddedaftermixingthemediumwithCMorunconditionedmedium.In
thisway,allconditionshadthesamefinalconcentrationofallsupplements.Beads
wereharvestedatday17.Allmediawererefreshed24hourspriortoharvest.
Gene expression analysis
MSC alginate beadswere harvested in ice-cold 55mM sodium citrate and dis-
solvedaftergentleagitationat4 ºC.Thesolutionwas thencentrifugedat400g
for8minutesat4ºCandcellpelletswerere-suspendedin650µlRNA-Bee(TelT-
est, USA) per bead. Chloroform (Sigma-Aldrich) was added to all samples at
200µL/mLRNA-Bee.RNAwasfurtherpurifiedusingRNeasyMicroKit(Qiagen).
RNA concentration and quality wasmeasured using NanoDrop ND1000 UV-Vis
Spectrophotometer(IsogenLifeScience).RNAwasreverse-transcribedtocDNA
using theRevertAid First StrandcDNASynthesisKit (Fermentas,Germany) ac-
cordingtomanufacturer’sinstructions.qRT-PCRwasperformedin10µLreactions
on cDNAusing theCFX96Touch™Real-TimePCRDetection System (BIO-RAD,
USA). Expression of glyceraldehyde-3-phosphate dehydrogenase (GAPDH), hy-
poxanthinephosphoribosyltransferase1(HPRT1),collagentype IIa1(COL2A1),
aggrecan(ACAN),collagentypeI(COL1A1)andversican(VCAN)weredetermined
with qRT-PCR. The genesGAPDH and HPRT were used as housekeepers. Gene
expressionwasanalyzedaccordingtotheΔΔCtmethod,withtheconditiontreated
withunconditionedmediumusedascontrolandsetat1.0.Expressionlevelsof
otherconditionsareexpressedrelativetothethiscontrolcondition.Theprimer
efficiency for GAPDHwas1.06,forHPRT0.96,forCOL2A11.02,forACAN0.95,for
COL1A10.97andVCAN0.95.ThemeanCtvalueforGAPDHwas22.9andforHPRT
28.8.DifferenceinCtvaluesbetweenthesampleswithineachexperimentwasless
than1Ctandtherewerenosignificantdifferencesbetweentheconditions(data
notshown).Geneexpressionvaluesafternormalizationtohousekeepersareused
to calculate COL2A1/COL1A and ACAN/VCANratios.
Primer sequences were as followed: GAPDH, forward: GTCAACGGATTTGGTC-
GTATTGGG, reverse: TGCCATGGGTGGAATCATATTGG and probe Fam: TGGC-

66 CHAPTER 4
GCCCCAACCAGCC.HPRTforward:TATGGACAGGACTGAACGTCTTG,reverse:CA-
CACAGAGGGCTACAATGTGandprobeFam:CGCCCAATACGACCAAATCCGTTGAC.
COL2A1 forward: GGCAATAGCAGGTTCACGTACA, reverse: CGATAACAGTCTT-
GCCCCACTTandprobeFam:CCGGTATGTTTCGTGCAGCCATCCT.ACAN forward:
TCGAGGACAGCGAGGCC,reverse:TCGAGGGTGTAGCGTGTAGAGAandprobeFam:
ATGGAACACGATGCCTTTCACCACGA. COL1A1 forward: CAGCCGCTTCACCTA-
CAGC, reverse: TTTTGTATTCAATCACTGTCTTGCC and probe Fam: CCGGTGT-
GACTCGTGCAGCCATC. VCAN forward: TGGAATGATGTTCCCTGCAA, reverse:
AAGGTCTTGGCATTTTCTACAACAG,probe:CTGGCCGCAAGCAACTGTTCCTTT.
Quantification of DNA and GAG content
Alginatebeadsweredissolvedinsodiumcitrateanddigestedwithpapain.(Sigma
Aldrich).PelletsweredigestedwithproteinaseK(SigmaAldrich).DNAwassubse-
quentlyquantifiedbyspectrophotometricdetectionofethidiumbromide(Gibco)
bindingat340and590nm.GAGcontentwasdeterminedwithdimethylmethylene
blue(Polysciences)spectrophotometricallyat530nmand590nm23andatapHof
1.75.
Histological evaluation of MSC chondrogenesis in pellet culture
6µm thickparaffinsectionsweremadeof thepelletsand thioninstainingwas
performed. For immunohistochemical staining, sections were incubated with
monoclonalantibodyagainstcollagentype2(DSHB,#II-II6B3)andcollagentype1
(Abcam,#6308)orIgG1isotypecontrol(DakoCytomation,#X0931).Sectionswere
thenincubatedwithLinkandLabel(Biogenex,HK-321-UK)andfreshlyprepared
new-fuchsinwasusedassubstrate.
Evaluation of macrophage subtypes in adipose tissue
10µmcryosectionsweremadeof13samplesofOAIPFP(Age65.3(54.3-74.1),BMI
28(21.5-35.8)),7samplesofLRIPFP(Age29.9(21.3-48),BMI25.6(19.3-38.5))and
9samplesofSAT(Age63.1(±50.2-79.1),BMI32.3(25.9-47.2)).Afterfixationinac-
etone,sectionswereincubatedwithmonoclonalantibodiesagainstCD68(DAKO,
#EMB11),CD11c(Chemicon,#EP1347Y)andCD206(Abcam,#64693).MouseIgG
(Dako)wereusedasisotypecontrols.Subsequently,sectionswereincubatedwith
linkandlabel(BioGenex)andfreshlypreparednew-fuchsinwasusedassubstrate.
Acellwasconsideredpositivewhenstainedred.Sampleswererankedbasedon
theirrelativenumberofpositivecellsinthreesectionspersamplebytwoblinded
observers as previously described15. Ranking was performed for each marker
separatelyandforeachsample,theaveragerankofthetwoobservers(WWand
RR)wasusedintheanalysis.

Anti-chondrogenic effect of IPFP on MSCs 67
4
Statistical analysis
IBMSPSS statistics 21 (IBMCorporation)wasused for statistical analysis.The
Shapiro-Wilk testwasused to testdata fornormalityand theLevene’s test for
homogeneityofvariance.Nodatawerenormallydistributed.Forgeneanalysis
andGAGmeasurement,ifnototherwisestated,theKruskal-Wallistestwasused
followedbyapost-hocBonferronicorrection.Forimmunohistochemicalranking,
theMann-WhitneyUtestwasused.p<0.05wasconsideredstatisticallysignificant.
RESULTS
IPFP negatively impacts chondrogenic differentiation of MSCs
COL2A1 and ACANwereonlydetectableafterTGFβ1wasadded(Figure1).IPFP
fromOAdonorsstatisticallysignificantlyloweredthegeneexpressionofMSCsfor
COL2A1 (p<0.001),ACAN (p<0.001)andVCAN, without affecting COL1A1 (Figure
1A). This resulted in a lowerCOL2A1/COL1A1 (p<0.001) andACAN/VCAN ratio
(p<0.05)(Figure1A).ThiseffectwasabsentwhenCMwasheatedto95°Cfor10
minutesbeforeuse,indicatingthattheeffectsarecausedbyproteinsproduced
by IPFP(Figure1B).GAGcontentof thealginatebeadswere increasedby IPFP
(Figure2A).TofurtherinvestigatetheeffectsofIPFPonmatrixproduction,pellet
culturewasused. IPFPdecreasedthioninand immunohistochemicalstainingof
collagentype2,whereascollagentype1stainingwasnotinfluenced(Figure2C).
Furthermore,IPFPdecreasedGAGcontentofpellets(Figure2D-E).
Effect of obese versus lean IPFP and osteoarthritic versus traumatic joint IPFP on MSC chondrogenesis
Obesity increasesthereleaseof inflammatory factorsbyadiposetissue.There-
fore,wehypothesizedthatCMfromobeseIPFPdonors(BMI33.1(30-35.8))would
reduceMSCchondrogenesismore thanCM from lean IPFP (BMI 23.1 (21.5-24))
donors. However, chondrogenicmarkers were notmore inhibited by CM from
obesethanbyCMfromleandonors(Figure3A).Next,wecomparedtheeffectof
CMfromLRIPFP(BMI22.9(22.0-25.0))withBMImatchedOAIPFP(BMI23.1(21.5-
24.0)).Chondrogenicgeneexpressionwasnotstatisticallysignificantlydifferent
betweenMSCsexposedtoCMfromLRIPFPandCMfromOAIPFP.InterestinglyLR
IPFPCMstatisticallysignificantlyincreasedCOL1A1comparedtocontrolandOA
IPFPCM(p=0.023)(Figure3B).

68 CHAPTER 4
VCAN
0.0
0.5
1.0
1.5
2.0 p<0.05
TGFb1 --
+-
++IPFP CM
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL2A1
0.0
0.5
1.0
1.5 p<0.001
TGFb1 --
+-
++IPFP CM
Gen
eex
pres
sion
com
pare
dto
cont
rol
ACAN
0.5
1.0
1.5 p<0.05
TGFb1 --
+-
++IPFP CM
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL1A1
0.5
1.0
1.5
TGFb1 --
+-
++IPFP CM
p<0.001
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL2A1 / COL1A1
0.01
0.1
1
10 p<0.001
Control IPFP
Com
pare
dto
cont
rol
ACAN / VCAN
0.0
0.5
1.0
1.5 p<0.05
Control IPFP
Com
pare
dto
cont
rol
COL2A1
0.0
0.5
1.0
1.5
TGFb1 +-
++
+- IPFP CM
++
- - +Heating +
p<0.05
ns
Gen
eex
pres
sion
com
pare
dto
cont
rol
ACAN
0.0
0.5
1.0
1.5
2.0
TGFb1 +-
++
+-
++
- - +Heating +
p<0.05 ns
IPFP CM
Gen
eex
pres
sion
com
pare
dto
cont
rol
A
B
Figure 1 IPFPinhibitschondrogenicdifferentiationofMSCs.A)MSCalginatebeadsweretreatedwith25%IPFPCMfor28daysofculture inchondrogenicmediumwithTGFβ1.Thecontrolconditionwastreatedwith25%unconditionedmediumwithchondrogenicmediumwithTGFβ1.RelativegeneexpressionCOL2A1,ACAN,COL1A1andVCANnormalizedtothecontrolconditionandCOL2A1/COL1A1andACAN/VCANratio.CMwerepooledfrom3-5differentIPFPdonorsandusedtotreat3MSCdonors,witheachconditionperformedintriplicate.B)MSCalginatebeadsweretreatedwith25%CMfromIPFPfromday14-17ofchondrogenicstimulation.CMorunconditionedmediumwereheatedfor10minutesat95°CandallowedtocooldowntoroomtemperaturebeforeadditiontoMSCalginatebeads.RelativegeneexpressionofCOL2A1andACANinMSCsaftertreatment,normalizedtothecontrolcondition.OnepoolofCMfrom3IPFPdonorswasusedtotreat1MSCdonorwitheachconditionperformedintriplicate.ThemeanCtvalueinthecontrolconditionforCOL2A1was23.2,forACAN27.3,forCOL1A119.7andforVCAN24.3.Valuesrepresentthemean±SD.

Anti-chondrogenic effect of IPFP on MSCs 69
4
Chondrogenic differentiation of MSCs is more affected by IPFP than by SAT
Toinvestigatewhethertheeffectofadiposetissueofthejoint(IPFP)isdifferent
fromsubcutaneousadiposetissue(SAT),weaddedCMmadefromSATtoMSCs
duringchondrogenicdifferentiation. SATstatistically significantly loweredgene
expression of COL2A1 and ACAN (p<0.01), but did not influence the COL2A1/
COL1A1 and ACAN/VCANratio(Figure4A).Toinvestigatewhetherthisisduetoa
differenceintheconcentrationoffactorsreleasedbyIPFPandSAT,weincreased
thepercentageofSATCMaddedtocultureupto50%.Incontrasttotheeffectof
IPFP,theeffectofSATonchondrogenesiswasnotdosagedependent(Figure4B).
Figure 2 IPFPinhibitschondrogenicdifferentiationofMSCs.AllconditionswerechondrogenicallystimulatedwithTGFβ1duringtheentirecultureperiod. MSCalginatebeadsandpelletsweretreatedwith25%IPFPCMwhereasthecontrolconditionwastreatedwith25%uncondi-tionedmediumfor28days.A)TotalGAGcontentandB)totalDNAcontentofalginatebeads.C)Representativeimagesofpelletsfrom1MSCdonorstainedforglycosaminoglycanswiththioninorcollagentype2andcollagentype1usingimmunohistochemistry.D)TotalGAGcontentandE)totalDNAcontentofpellets.DifferentpoolsofCMfrom3differentIPFPdonorswereusedforeachexperiment.FortotalGAGandDNAcontentinbeads(PanelA),3MSCdonorswereusedwitheachconditionperformedintriplicate.Forthepelletcultureexperi-ment(PanelC-E),2MSCdonorwereusedwith5pelletspercondition.Valuesrepresentmean±SD.TheMann-WhitneyUtestwasusedtodeterminestatisticalsignificance.

70 CHAPTER 4
Difference between IPFP and SAT in number and phenotype of macrophages
WehypothesizedthatthedifferenceineffectsofIPFPandSATonexpressionof
chondrogenicandfibroustissuegenescouldbeduetothetypeofmacrophages
in the adipose tissue.We therefore first characterized themacrophages in the
differentadiposetissues. IPFPsamples fromOAdonorsrankedhigheronCD68
(p=0.007andp=0.03)andCD206 (p=0.02andp=0.049)positive staining thanLR
IPFPandSATsamples(Figure5BandD).Wecouldnotdetectdifferencesbetween
obeseandleandonors.
Macrophages in IPFP contribute to the effects seen on MSC chondrogenesis
ToinvestigatewhethermacrophagespresentintheIPFPwereresponsibleforthe
effectseenonMSCchondrogenesis,weaddedCMfrommacrophagesisolatedfrom
IPFPtoMSCsduringchondrogenesis.IPFPmacrophagesstatisticallysignificantly
lowered the COL2A1 and ACANgeneexpression(Figure6A).Sinceweapplieda
verystrictselectionforCD45+cells,theremainderfractionstillcontainedasmall
numberofCD45+cells.ThisCD45reducedfractionappearedtobeabletoinhibit
COL2A1 and ACAN geneexpressionaswell (Figure6B).To investigatewhether
thiseffectwasspecificforcellsisolatedfromtheIPFP,weaddedCMfromhuman
dermalfibroblasts(HDFA)toMSCsduringchondrogenesis.CMfromHDFAsdid
notinfluenceMSCchondrogenesis(Figure6B).
COL2A1
Control IPFP obese IPFP lean0.0
0.5
1.0
1.5 p<0.01
ns
Gen
eex
pres
sion
com
pare
dto
cont
rol
ACAN
Control IPFP obese IPFP lean0.0
0.5
1.0
1.5 p<0.01
ns
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL2A1
Control OA IPFP LR IPFP0.0
0.5
1.0
1.5 p<0.01
nsGen
eex
pres
sion
com
pare
dto
cont
rol
ACAN
Control OA IPFP LR IPFP0.0
0.5
1.0
1.5 p<0.01
nsG
ene
expr
essi
onco
mpa
red
toco
ntro
l
COL1A1
Control IPFP obese IPFP lean0
1
2
3
4
Gen
eex
pres
sion
com
pare
dto
cont
rol
VCAN
Control IPFP obese IPFP lean0
1
2
3
4
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL1A1
Control OA IPFP LR IPFP0
5
10
15p<0.05
Gen
eex
pres
sion
com
pare
dto
cont
rol
VCAN
Control OA IPFP LR IPFP0.0
0.5
1.0
1.5p<0.05
ns
Gen
eex
pres
sion
com
pare
dto
cont
rol
A
B
Figure 3 EffectofobeseversusleanIPFPandosteoarthriticversustraumaticjointIPFPonMSCchondrogenesis.AllconditionswerechondrogenicallystimulatedwithTGFβ1duringtheentirecultureperiod.MSCalginatebeadsweretreatedwith25%IPFPCMfromday14-17.Thecontrolconditionwastreatedwith25%unconditionedme-dium.RelativegeneexpressionofCOL2A1,ACAN,COL1A1andVCANinMSCsaftertreatmentwithCMfromA)obese(BMI>30)orlean(BMI<25)OAIPFPdonorsandB)OAorBMImatchedLRIPFPdonors.GeneexpressionwasnormalizedtothecontrolconditionperMSCdonor.CMfrom6obeseOAIPFP,6leanOAIPFPand6LRIPFPdonorswereused.ThreedifferentpoolsofCMwasmadewitheachpoolaselectionofthreedifferentIPFPdonors.ThreeMSCdonorswereused,witheachconditionperformedintriplicate.Valuesrepresentthemean±SD.

Anti-chondrogenic effect of IPFP on MSCs 71
4
FinallyweinvestigatedwhetherthenegativeeffectsofIPFPderivedmacrophages
onMSCchondrogenesiscouldbeexplainedbythephenotypeofthemacrophage.
DuetothelownumberofmacrophageswecouldobtainfromIPFP,weusedPBMCs
that were stimulate to pro- or anti-inflammatory phenotype. MSCs exposed to
CMofM(LPS+IFNɣ)macrophageshad lowerhyalinecartilagegenesexpression
comparedtocontrolandCMofM(IL-4)macrophages(Figure6C)
COL2A1
Control IPFP SAT
0.5
1.0
1.5 p<0.01
p<0.01
Gen
eex
pres
sion
com
pare
dto
cont
rol
ACAN
Control IPFP SAT
0.5
1.0
1.5p<0.01
p<0.05
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL1A1
Control IPFP SAT0
5
10
15
Gen
eex
pres
sion
com
pare
dto
cont
rol
VCAN
Control IPFP SAT0.0
0.5
1.0
1.5p<0.01
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL2A1 / COL1A1
Control IPFP SAT0.0
0.5
1.0
1.5
2.0
2.5
p<0.05
Com
pare
dto
cont
rol
ACAN / VCAN
Control IPFP SAT0.0
0.5
1.0
1.5
2.0
2.5 p<0.05
Com
pare
dto
cont
rol
COL2A1
Control
12.5%
IPFP
25%
IPFP
50%
IPFP
12.5%
SAT
25%
SAT
50%
SAT1
10
100
a
a
a
Gen
eex
pres
sion
com
pare
dto
hous
ekee
pers
ACAN
Control
12.5%
IPFP
25%
IPFP
50%
IPFP
12.5%
SAT
25%
SAT
50%
SAT0.01
0.1
1
10
a a
a
Gen
eex
pres
sion
com
pare
dto
hous
ekee
pers
A
B
Figure 4 MSCchondrogenesisismoreinfluencedbyIPFPthansubcutaneousadiposetissue(SAT).MSCalginatebeadsweretreatedwithCMfromIPFPorSATfromday14-17ofculture.Thecontrolconditionwastreatedwith25%unconditionedmedium.AllconditionswerechondrogenicallystimulatedwithTGFβ1duringtheentirecultureperiod.A)25%ofCMwasusedandCMwerepooledfrom3poolsofdifferent3IPFPor3poolsofdifferent3SATdonorsandusedtotreat3MSCdonors.Eachexperimentwasperformedintriplicate.RelativegeneexpressionofCOL2A1,ACAN,COL1A1,VCAN,COL2A1/COL1A1ratioandACAN/VCANratioinMSCsaftertreatment.GeneexpressionwasnormalizedtothecontrolconditionperMSCdonor.B)DifferentpercentagesofCMwereusedandCMwerepooledfrom3IPFPor3SATdonorsandusedtotreat1MSCdonor,witheachconditionperformedintriplicate.RelativegeneexpressionofCOL2A1andACANcomparedtohousekeepersinMSCsaftertreatmentAllconditionsreceivedthesamefinalconcentrationofallchondrogenicsupplements.Valuesrepresentthemean±SD.ap<0.05versusControlusingtheMann-Whitney-Utest.

72 CHAPTER 4
Figure 5 Macrophageswithdifferentphenotypesarepresentinadiposetissuesamples.13samplesofOA IPFP,7samplesofLR IPFPand9samplesofSATwereused.A)Representative imagesofimmunohistochemcalstainingofCD68,CD11candCD206positivecellsinOAIPFPsamples.Positivecellsarestainedredandindicatedwitharrows.RankingofpositivestaininginadiposetissuesamplesforB)CD68,C)CD11candD)CD206.
COL2A1
Control CD45 positive0.0
0.5
1.0
1.5 p<0.05
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL2A1
Control CD45 HDFa 20% HDFa 10%0.0
0.5
1.0
1.5
2.0
reduced
p<0.05
Com
pare
dto
cont
rol
COL2A1 / COL1A1
Control CD45 HDFa 20% HDFa 10%0.0
0.5
1.0
1.5
2.0p<0.05
reduced
Com
pare
dto
cont
rol
ACAN/VCAN
Control CD45 HDFa 20% HDFa 10%0.0
0.5
1.0
1.5
2.0 p<0.05
reduced
Com
pare
dto
cont
rol
COL2A1
0.0
0.5
1.0
1.5
2.0p<0.05
Control M(LPS+IFNg) M(IL-4)
Gen
eex
pres
sion
com
pare
dto
cont
rol
ACAN
0.0
0.5
1.0
1.5
p<0.05
p<0.05
Control M(LPS+IFNg) M(IL-4)
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL2A1 / COL1A1
0
1
2
3 p<0.05
Control M(LPS+IFNg) M(IL-4)
Com
pare
dto
cont
rol
ACAN / VCAN
0.0
0.5
1.0
1.5 p<0.05
Control M(LPS+IFNg) M(IL-4)
Com
pare
dto
cont
rol
A
B
C
ACAN
Control CD45 HDFa 20% HDFa 10%0.0
0.5
1.0
1.5
2.0p<0.05
reduced
Com
pare
dto
cont
rol
ACAN
Control CD45 positive0.0
0.5
1.0
1.5 p<0.05
Gen
eex
pres
sion
com
pare
dto
cont
rol
COL2A1 / COL1A1
Control CD45 positive0.0
0.5
1.0
1.5
Com
pare
dto
cont
rol
ACAN / VCAN
Control CD45 positive0.0
0.5
1.0
1.5p<0.05
Com
pare
dto
cont
rol
Figure 6 MacrophagesinIPFPcontributetotheeffectsseenonMSCchondrogenesis.MSCalginatebeadsweretreatedwithCMfromday14-17.Thecontrolconditionwastreatedwith25%uncondi-tionedmedium.AllconditionswerechondrogenicallystimulatedwithTGFβ1duringtheentirecultureperiod.A)Effectof50%CMfromCD45+cellsfromIPFPonMSCchondrogenesis;B)Effect50%CMfromCD45reducedfractionfromIPFPorCMfromadulthumandermalfibroblasts(HDFa)onMSCchondrogenesis;C)Effectof20%CMfromM(LPS+IFNɣ)orM(IL-4)macrophagesonMSCchondrogenesis.RelativegeneexpressionofCOL2A1,ACAN,COL2A1/COL1A1ratioandACAN/VCANratioinMSCsaftertreatment.GeneexpressionwasnormalisedtothecontrolconditionperMSCdonor.CMwerefrom6IPFPdonors,1HDFadonoror3blooddonorsandusedtotreat1MSCdonor.ConditionswithCMderivedfromIPFPwereperformedinsinglewellandallothercondi-tionswereperformedintriplicate.Valuesrepresentthemean±SD.

Anti-chondrogenic effect of IPFP on MSCs 73
4
DISCUSSION
IPFPsecretescytokines,growthfactorsandadipokineswhichcouldinfluencethe
jointenvironment11. Inthisstudywehaveshownthatthe IPFPreleasedfactors
that inhibitchondrogenicdifferentiationofMSCsandtheproductionofhyaline
cartilagematrix.Thisanti-chondrogeniceffectwasthesameforpatientswithend
stageOAandpatientswithjointtrauma.Furthermore,theIPFPofobesepatients
didnotinhibitchondrogenesismorethanIPFPofleanpatients.Finally,wehave
indicationsthatmacrophagesresidingintheIPFPmightplayanimportantrolein
thisanti-chondrogeniceffect.
Repairtissueformedaftermarrowstimulationtechniques,suchasthemicrofrac-
tureprocedure,ismainlyfibrocartilagewhichisoflessbiomechanicalqualitythan
nativehyalinecartilage24. Inthepresentstudy,thedecreaseinCOL2A1/COL1A1
and ACAN/VCANratiossuggeststhatIPFPnotonlyinhibitschondrogenesis,but
alsoshiftstheproductionfromhyalinetofibro-cartilage.Fibrocartilagealsocon-
tainsproteoglycans,butinsteadofaggrecanthisisversican.Thiscouldbeanex-
planationwhywefoundnoreductioninglycosaminoglycanproductioninalginate
beadsafterIPFPCMtreatment,despiteadecreaseinaggrecancore-proteingene
expression.However,thiscouldalsobecausedbyinterferenceoftheDMMBassay
byalginateespeciallywhenlowamountofGAGisinvolved23;25.Analysesonmatrix
withDMMBand immunohistochemistrycanbeusedmore reliablyonpellets26.
Thereducedthioninstainingandimmunohistochemicalstainingforcollagentype
2inpelletstreatedwithIPFPCMsupportsthegeneexpressionresultsinalginate
beads.OurfindingsindicatethatfibrocartilageproductionbyMSCs,takingplace
aftermicrofractureprocedure,couldbepartlyduetofactorssecretedbytheIPFP.
ThesecretionoffactorsbyIPFPcouldbeinfluencedbythediseasestateofthe
joint.ThemicrofractureprocedureandMSCbasedtreatmentsarerecommended
forthetreatmentofpost-traumatic,ratherthanend-stageOAcartilagedefects27.
Higherlevelsof inflammatorycytokineswerefoundinpost-traumaticthanend-
stageOAknees28;29.Gandhiet al 16 reported thatpost-traumatic IPFPexpresses
morepro-inflammatorygenescompared to end-stageOA IPFP.We founddiffer-
encesinmacrophagenumberandinparticularCD206positivecellsbetweenIPFP
fromOAandLRknees,albeitfactorssecretedbybothOAandLRIPFPinhibited
chondrogenesis.However,wecannotexcludethattheseeffectsareduetodiffer-
entcytokinesoradipokines.

74 CHAPTER 4
AnotherfactorthatcouldinfluencebothIPFPandtheresultsofmicrofractureis
obesity9.Inobesepatients,macrophagesinadiposetissuearechangedtowardsa
chronicinflammatoryphenotypewithincreasedproductionofpro-inflammatory
cytokines10. An inflamed obese IPFP would possibly be an explanation for the
worseresultsofmicrofractureinobesepatients.Incontrasttothishypothesis,we
didnotdetectanincreasedanti-chondrogeniceffectofIPFPfromobesecompared
toleandonors.ToinvestigatewhethertheOAprocesscouldbeofmoreinfluence
tothefactorssecretedbyIPFPthanbeingobese,experimentswithIPFPdonors
withaloworhighBMIbutwithoutOAwouldberequired.Itishoweverdifficultto
obtainsufficientIPFPfromnon-OAdonors.
Independent from joint pathology or obesity, differences have been reported
betweenIPFPandotheradiposetissue.IPFPexpressesmoreinflammatorygenes,
releasemore inflammatory factorsandcontainsmore immunecells thanSAT17.
Inourstudy,theanti-chondrogeniceffectof IPFPwasstrongerthanthatofSAT
and even after increasing the dosage of SAT CM, the anti-chondrogenic effect
wasnotincreasedtothelevelofIPFP.ThissuggeststhattheIPFPreleasesanti-
chondrogenicfactorsnotproducedbysubcutaneousadiposetissues.
IPFPsecretespro-inflammatoryfactorsandadipokines,suchasTNF-α,IL1β,IL6andadipokines,suchasleptin,resistinandadiponectin12.Thesefactorscouldbe
producedby thefibroblasts, adipocytesand immunecells residing in the IPFP.
A largeproportionof the immunecells in the IPFParemacrophages15;17. Immu-
nohistochemical analysis on IPFP and SAT indicated that IPFP containedmore
macrophages than SAT. Previously we have shown that only pro-inflammatory
macrophages inhibit chondrogenesis20 and in the current study, only the pro-
inflammatory macrophages shifts MSCs to produce fibrocartilage matrix. As a
proofofprinciple,weshowedthatisolatedmacrophagesfromtheIPFPwereanti-
chondrogenic.AlthoughwecouldnotexcludethatothercellsintheIPFPcould
alsosecreteanti-chondrogenicfactors,ourstudydoessuggestthatmacrophages
intheIPFPplayavitalroleininhibitingproductionofhyalinecartilageandthe
shifttowardsfibrocartilagematrixproduction.
NexttodirectlynegativelyaffectingchondrogenesisofMSCs,IPFPcaninfluence
other joint structures and thereby indirectly influence chondrogenesis. IPFP
factors have been shown to stimulate fibrotic processes21 and production of
pro-inflammatoryfactorsinsynovialfibroblasts30.Inthisway,synoviumcanthen
inhibit chondrogenesis20.Incontrasttotheeffectonsynovium,theIPFPinhibits
catabolicmediatorsincartilageexplantsstimulatedwithorwithoutIL1β15.This
showsthatdifferenttissuesinthejointcanreactdifferentlytofactorssecreted

Anti-chondrogenic effect of IPFP on MSCs 75
4
bytheIPFPandtheinterplaybetweenalljointtissueswilldeterminetheeventual
effect on cartilage repair. The use of co-cultures of several joint tissueswould
berequiredtoelucidatethisinfuturestudiesandtoshowthepotentialeffectof
modulation.
Insummary,wehaveshownthattheIPFPisasourceoffactorsthatinhibitchon-
drogenicdifferentiationofMSCsandshiftedtheproductionfromhyalinetofibro-
cartilagematrix.Thisanti-chondrogeniceffectofadiposetissuewasspecificfor
IPFPandnotsubcutaneousadiposetissue.Furthermore,thisanti-chondrogenic
effectwasnotmoreinobesedonorsthanleandonorsandwasnotdifferentbe-
tweendonorswithpost-jointtraumaorend-stageOA.Finally,theIPFPandspecifi-
callythemacrophagesinthetissuecouldthereforebetargetsforfuturetherapies
toimprovethejointenvironmentforMSCchondrogenesisandtherebyimprove
theoutcomeofmicrofractureprocedureandfutureMSC-basedtreatmentsforthe
repairofcartilagedefects.

76 CHAPTER 4
REFERENCES
1. ShapiroF,KoideS,GlimcherMJ.1993.Celloriginanddifferentiationintherepairoffull-thickness
defectsofarticularcartilage.JBoneJointSurgAm75:532-553.
2. SteadmanJR,MillerBS,KarasSG,etal.2003.Themicrofracturetechniqueinthetreatmentoffull-
thicknesschondrallesionsofthekneeinNationalFootballLeagueplayers.JKneeSurg16:83-86.
3. FrisbieDD,OxfordJT,SouthwoodL,etal.2003.Earlyeventsincartilagerepairaftersubchondral
bonemicrofracture.ClinOrthopRelatRes:215-227.
4. Kaul G, CucchiariniM, Remberger K, et al. 2012. Failed cartilage repair for early osteoarthritis
defects:abiochemical,histologicalandimmunohistochemicalanalysisoftherepairtissueafter
treatmentwithmarrow-stimulationtechniques.KneeSurgSportsTraumatolArthrosc20:2315-2324.
5. IrieK,UchiyamaE,IwasoH.2003.Intraarticularinflammatorycytokinesinacuteanteriorcruciate
ligamentinjuredknee.Knee10:93-96.
6. Heldens GT, Blaney Davidson EN, Vitters EL, et al. 2012. Catabolic factors and osteoarthritis-
conditionedmediuminhibitchondrogenesisofhumanmesenchymalstemcells.TissueEngPartA
18:45-54.
7. HunzikerEB,LippunerK,KeelMJ,etal.2015.Aneducationalreviewofcartilagerepair:precepts&
practice--myths&misconceptions--progress&prospects.OsteoarthritisCartilage23:334-350.
8. WehlingN,PalmerGD,PilapilC,etal.2009.Interleukin-1betaandtumornecrosisfactoralphain-
hibitchondrogenesisbyhumanmesenchymalstemcellsthroughNF-kappaB-dependentpathways.
ArthritisRheum60:801-812.
9. MithoeferK,WilliamsRJ,3rd,WarrenRF,etal.2005.Themicrofracturetechniqueforthetreatment
ofarticularcartilagelesionsintheknee.Aprospectivecohortstudy.JBoneJointSurgAm87:1911-
1920.
10. LumengCN, SaltielAR. 2011. Inflammatory linksbetweenobesity andmetabolicdisease. JClin
Invest121:2111-2117.
11. ClockaertsS,Bastiaansen-JenniskensYM,RunhaarJ,etal.2010.Theinfrapatellarfatpadshould
beconsideredasanactiveosteoarthriticjointtissue:anarrativereview.OsteoarthritisCartilage
18:876-882.
12. ClockaertsS,Bastiaansen-JenniskensYM,FeijtC,etal.2012.Cytokineproductionbyinfrapatellar
fatpadcanbestimulatedbyinterleukin1betaandinhibitedbyperoxisomeproliferatoractivated
receptoralphaagonist.AnnRheumDis71:1012-1018.
13. GrantRW,DixitVD.2015.Adiposetissueasanimmunologicalorgan.Obesity(SilverSpring).
14. GiermanLM,WopereisS,vanElB,etal.2013.Metabolicprofilingrevealsdifferencesinconcentra-
tionsofoxylipinsand fattyacidssecretedby the infrapatellar fatpadofdonorswithend-stage
osteoarthritisandnormaldonors.ArthritisRheum65:2606-2614.
15. Bastiaansen-JenniskensYM,ClockaertsS,FeijtC,etal.2012.Infrapatellarfatpadofpatientswith
end-stageosteoarthritisinhibitscatabolicmediatorsincartilage.AnnRheumDis71:288-294.
16. GandhiR,TakahashiM,VirtanenC,etal.2011.Microarrayanalysisoftheinfrapatellarfatpadin
kneeosteoarthritis:relationshipwithjointinflammation.JRheumatol38:1966-1972.
17. Klein-WieringaIR,KloppenburgM,Bastiaansen-JenniskensYM,etal.2011.Theinfrapatellarfatpad
ofpatientswithosteoarthritishasaninflammatoryphenotype.AnnRheumDis70:851-857.
18. MosserDM,EdwardsJP.2008.Exploringthefullspectrumofmacrophageactivation.NatRevIm-
munol8:958-969.
19. MurrayPJ,AllenJE,BiswasSK,etal.2014.Macrophageactivationandpolarization:nomenclature
andexperimentalguidelines.Immunity41:14-20.

Anti-chondrogenic effect of IPFP on MSCs 77
4
20. FahyN,deVries-vanMelleML,LehmannJ,etal.2014.Humanosteoarthriticsynoviumimpacts
chondrogenicdifferentiationofmesenchymalstemcellsviamacrophagepolarisationstate.Osteo-
arthritisCartilage22:1167-1175.
21. Bastiaansen-JenniskensYM,WeiW, Feijt C, et al. 2013. Stimulation of fibrotic processes by the
infrapatellarfatpadinculturedsynoviocytesfrompatientswithosteoarthritis:apossiblerolefor
prostaglandinf2alpha.ArthritisRheum65:2070-2080.
22. GrotenhuisN,VdToomHF,KopsN,etal.2014.Invitromodeltostudythebiomaterial-dependent
reactionofmacrophagesinaninflammatoryenvironment.BrJSurg101:983-992.
23. EnobakhareBO,BaderDL,LeeDA.1996.Quantificationofsulfatedglycosaminoglycansinchondro-
cyte/alginatecultures,byuseof1,9-dimethylmethyleneblue.AnalBiochem243:189-191.
24. Furukawa T, Eyre DR, Koide S, et al. 1980. Biochemical studies on repair cartilage resurfacing
experimentaldefectsintherabbitknee.JBoneJointSurgAm62:79-89.
25. Zheng CH, Levenston ME. 2015. Fact versus artifact: avoiding erroneous estimates of sulfated
glycosaminoglycan content using the dimethylmethylene blue colorimetric assay for tissue-
engineeredconstructs.EurCellMater29:224-236;discussion236.
26. YangIH,KimSH,KimYH,etal.2004.Comparisonofphenotypiccharacterizationbetween“alginate
bead”and“pellet”culturesystemsaschondrogenicdifferentiationmodelsforhumanmesenchy-
malstemcells.YonseiMedJ45:891-900.
27. GomollAH,FarrJ,GilloglySD,etal.2011.Surgicalmanagementofarticularcartilagedefectsofthe
knee.InstrCourseLect60:461-483.
28. BeekhuizenM,GiermanLM, van SpilWE, et al. 2013.An explorative study comparing levels of
solublemediatorsincontrolandosteoarthriticsynovialfluid.OsteoarthritisCartilage21:918-922.
29. TsuchidaAI, BeekhuizenM,RutgersM, et al. 2012. Interleukin-6 is elevated in synovial fluid of
patientswithfocalcartilagedefectsandstimulatescartilagematrixproductioninaninvitroregen-
erationmodel.ArthritisResTher14:R262.
30. Eymard F, Pigenet A, CitadelleD, et al. 2014. Induction of an inflammatory and prodegradative
phenotypeinautologousfibroblast-likesynoviocytesbytheinfrapatellarfatpadfrompatientswith
kneeosteoarthritis.ArthritisRheumatol66:2165-2174.


CHAPTER 5
Anti-chondrogenic and pro-catabolic effect of
infrapatellar fat pad and its residing macrophages can be modulated by triamcinolone
acetonide
Wu Wei Serdar Capar
Nicole Kops Jan A.N. Verhaar Stefan Clockaerts
Gerjo J.V.M. van Osch Yvonne M. Bastiaansen-Jenniskens
Submitted

80 CHAPTER 5
ABSTRACT
Background
Prolongedinflammationinhibitssuccessfulcartilagerepair.Aninflamedinfrapa-
tellarfatpad(IPFP),andinparticulartheresidingpro-inflammatorymacrophages,
secrete factors that inhibit chondrogenic differentiation and stimulate tissue
degradation.Weaimed to reduce inflammation in the IPFP therebycreating an
environmentmoresuitableforcartilagerepair
Hypothesis
Theanti-chondrogenicandcataboliceffectofIPFPcanbereducedbyinfluencing
macrophagephenotypewithanti-inflammatorymedication
Study design
Controlledlaboratorystudy
Methods
IPFPexplantsobtainedfrom12donorsduringtotalkneearthroplastywerecul-
turedwithcelecoxib,triamcinoloneacetonide(TAA),pravastatinandfenofibrate
for24hours.TheeffectofthemedicationsonIPFPgeneexpressionandmacro-
phagesurfacemarkerswasevaluated.Theeffectsofconditionedmedium(CM)
fromIPFPexplantstreatedwithmedicationsonchondrogenesisofhumanbone
marrowmesenchymalstemcells(MSC)andcatabolicprocessesinosteoarthritic
synovialfibroblastswereevaluated.
Results
TAA significantly decreased gene expression of tumor necrosis factor-alpha
(TNFA),interleukin(IL)-1β(IL1B) and IL6andincreasedexpressionofIL10, cluster
of differentiation (CD)206(CD206) and CD163inIPFPexplants,whereascelecoxib,
pravastatin,andfenofibratehadnoeffectonIPFPinflammation.TAAalsosignifi-
cantlyincreasedanti-inflammatoryCD14+/CD163+andCD14+/CD206+cellsinthe
IPFP.Thedecreaseofcollagentype2(COL2A1)expressioninchondrogenicMSCs
asaresultofCMfromIPFPexplantscouldbereducedbytreatingIPFPwithTAA
duringtheproductionoftheCM.Theincreasedmatrixmetalloproteinase(MMP)1
and MMP13expressioninMSCsandosteoarthriticsynovialfibroblastsasresultof
CMfromIPFPexplantscouldbesignificantlyreducedbytreatingIPFPwithTAA.

Triamcinolone affects infrapatellar fat pad and macrophages 81
5
Conclusions
TAA decreases IPFP inflammation by increasing the anti-inflammatory macro-
phagesinIPFP.TAAcanbeusedtodecreasetheanti-chondrogeniceffectofIPFP
onMSCchondrogenesis.Furthermore,TAAdecreasesthecataboliceffectofIPFP
onMSCsandsynovialfibroblasts.
Clinical relevance
TAAmightbeusedtomodulatetheIPFPandthereforeimprovethejointenviron-
mentforcartilagerepairprocedures.

82 CHAPTER 5
INTRODUCTION
Jointinjuriesarecommonandoftenresultincartilagedefectsandinflammation
of the joint. Joint inflammation in turnmayprevent successful cartilagedefect
repairandwithoutsuccessfulrepair,cartilagedefectscaneventuallyleadtothe
developmentofosteoarthritis(OA)1.Toimprovecartilagerepairandpreventthe
developmentofOA,restorationofthejointhomeostasisisnecessary.
Currently,non-steroidanti-inflammatorydrugssuchascelecoxibandglucocorti-
coidssuchastriamcinoloneacetonide(TAA)areusedtoreduceinflammationand
reduce thesymptomsofOA2.Furthermore, statinsandfibratesarealsoshown
tohaveanti-inflammatorypropertiesbesidestheirmetabolicmodulatoryproper-
ties3-5. The effect of anti-inflammatorymedication on the synoviummembrane,
cartilage and bone are often studied6;7.However,theinfrapatellarfatpad(IPFP)
alsoseemstoplayanimportantroleinjointhomeostasis8.
TheIPFPisanadiposetissuelocatedextra-synovially,butintracapsularlywithin
thekneejoint.TheIPFPsecretesfactorsthatinhibitchondrogenicdifferentiation
ofmesenchymalstemcells(MSCs)9andstimulatefibroticandcatabolicprocesses
insynovialfibroblasts10;11.Furthermore,cytokinesecretionbytheIPFPincreases
in response to inflammation4 and IPFPaggravates furtherdegenerationof trau-
matized cartilage12.The IPFP contains many pro- and anti-inflammatory macro-
phages9;13. Pro-inflammatoryorM1macrophages are indicated to contribute to
theanti-chondrogeniceffectoftheIPFP9.M2macrophagesontheotherhandcan
haveananti-inflammatoryortissuerepairphenotypeandtheydidnotinhibit9;14
andcouldevenenhanceMSCchondrogenesis15.
Toimprovethejointenvironmentforcartilagerepairprocedures,wehypothesized
thatmedicationcanbeusedtomodulatetheIPFPanditsresidentmacrophages.
Inthisway,secretionofanti-chondrogenicfactorsbytheIPFPmightreduce.Fur-
thermore,catabolicandanti-chondrogenicprocessesinsynoviummightalsobe
reducedsincetheIPFPinfluencesthesynovium5;10;11.
Inthecurrentstudy,weinvestigatedtheeffectofcelecoxib,TAA,pravastatinand
fenofibrateonIPFPinflammation.Wechoosethesefourmedicationsduetotheir
wide-spreadclinicaluse.DuetothepresenceofmanymacrophagesintheIPFP
and the importance ofmacrophages in inflammation, we investigatedwhether
macrophagephenotypewithin the IPFPwasmodulatedby themedications. Fi-
nally,weinvestigatedwhethertheanti-chondrogeniceffectofIPFPonMSCsand

Triamcinolone affects infrapatellar fat pad and macrophages 83
5
thepro-fibroticandpro-cataboliceffectonsynovialfibroblastscouldbereduced
bytreatingtheIPFPwiththesemedications.
MATERIALS AND METHODS
Treatment of infrapatellar fat pad and preparation of conditioned medium (CM)
IPFPtissuewasobtainedasleftovermaterialfrom12patientswithOAwhohad
undergoneatotalkneearthroplasty.Consentwasgiveninaccordancewiththe
guidelinesoftheFederationofBiomedicalScientificSocieties(http://www.federa.
org),withapprovalbythelocalethicalcommittee(ErasmusMCUniversityMedi-
calCenter,TheNetherlands,MEC2012-267).TheinnerpartoftheIPFPwascut
into small pieces of approximately 9 mm2, washed two times with saline and
culturedataconcentrationof100mg/ml.Asaresult,eachsamplecontained0.5g
IPFPtissuedividedover10explants.ExplantswereculturedinDulbecco’sModi-
fiedEagleMediumwithGlutamax(DMEM-HG;Gibco™,ThermoFisherScientific,
Waltham,Massachusetts,USA)supplementedwith1% insulin-transferrin-seleni-
um(ITS+;BDBiosciences,FranklinLakes,NewJersey,USA)at37ºC.Allculture
mediawere supplementedwith 1.5 μg/mL fungizone and 50 μg/mL gentamicin
(both Gibco™). Triamcinolone acetonide (TAA; #T6501), celecoxib (#PZ0008),
pravastatin(#P4498)andfenofibrate(#F6020)wereacquiredfromSigma-Aldrich
(St.Louis,Missouri,USA). Dimethylsulfoxide(DMSO;Sigma-Aldrich)wasused
to dissolve all four medications. Used end-concentration are indicated in the
respectivegraphs.Medicationswere furtherdiluted inDMEM-HGandaddedto
IPFPexplantsdirect fromthestartofculture.Theusedendconcentrations for
themedicationswerebasedonliterature16andourpreviouswork17;18.Totakeinto
account anypossible effect ofDMSO,we added extraDMSO to the conditions
where themedicationsweremorediluted.As a result, all conditionshad 0,1%
DMSOintheculturemedium.After24hoursofculture,mediumwasharvested,
centrifugedat250gfor8minutesandsupernatantwasstoredinaliquotsof1ml
at-80ºCforanalysisandcultureexperiments.IPFPexplantswerefurtherusedfor
fluorescence-activatedcellsorting(FACS)analysisorweresnap-frozeninliquid
nitrogenforgeneanalysis.Unconditionedmediumwasgeneratedbyincubation
ofDMEM-HGsupplementedwithITS+for24hoursat37ºC,centrifugedat250g for
8minutesandstoredat-80ºC.

84 CHAPTER 5
Analysis of macrophage phenotype in IPFP
CulturedIPFPexplantsweredigestedfor3hoursat37°CinHanks’BalancedSalt
solution(Gibco™)withCa2+andMg2+,containing2mg/mlCollagenaseIV(Gibco™)
and0.2mg/mlDispaseII(Roche,Penzberg,UpperBavaria,Germany).Weused0.5
gofculturedIPFPpercondition.Afterincubation,thedigestwasneutralizedby
adding fetal calf serum(FCS;Lonza,Basel, Switzerland) toafinal solutioncon-
centrationof5%.Subsequently,thesolutionwasfilteredthrougha100µmfilter
followedbytwicea40µmfilter.Cellswerethencentrifugedfor8minutesat250g,
re-suspendedinFACSflow(#342003BDBiosciences)andcounted.Approximately
200.000cellswerestainedforeachcondition.Cellswerere-suspendedin40μL
ofFACSflowandincubatedfor15minutesatroomtemperatureinthedarkwitha
mixtureofthefollowingantibodiesagainstCD14(APC-H7,#561384),CD206(FITC,
#551135),CD163(PerCP-Cy™5.5,#563887),CD80(PECy™7,#561135),andCD86
(PE, #560957, all BD Biosciences). Cells were fixed in 1.8% paraformaldehyde
for20minutesinthedark.Subsequently,paraformaldehydewasremoved,cells
weresuspendedinFACSflow,andanalyzedwithFACSJazz™(BDBiosciences)and
FlowJoV.10(FlowJoLLC,Ashland,Oregon)
Isolation and culture of human MSCs
HumanMSCswereisolatedfrombonemarrowaspiratesfrom3end-stagehipOA
patientsundergoingtotalhiparthroplasty.Writteninformedconsentwasattained
andthestudywasapprovedbythelocalethicalcommittee(ErasmusMCUniver-
sityMedicalCenter,TheNetherlands,MEC2004-142)andAlbertSchweitzerHos-
pital,TheNetherlands(MEC2011-07).Aspirateswereplatedinexpansionmedium
consistingofMinimumEssentialMedium-Alpha(α-MEM;Gibco™)supplemented
with10%FCS,1ng/mlfibroblastgrowthfactor2(FGF2;R&DSystems)and25μg/
mLascorbicacid-2-phosphate(Sigma-Aldrich).After24hours,plateswerewashed
with PBS containing 2% FCS.MSCswere then expanded in expansionmedium,
trypsinisedafterreachingsub-confluencyandseededagainatadensityof2500
cells/cm2.MSCsofpassage4wereencapsulated in1.2%alginate (CPKelco,At-
lanta,Georgia,USA)insalineatadensityof4.000.000cells/ml.Beadswereformed
bypurgingtheMSC-alginatesolutionthrougha23Gneedleallowingdropletsto
fallinto102mMCaCl2solution.Beadswerefirstculturedfor14dayswith100µL
ofDMEM-HGwithITS+peralginatebeadsupplementedwith0.1µMDexametha-
sone (Sigma-Aldrich), 25 μg/mL ascorbic acid-2-phosphate (Sigma-Aldrich), 40
µg/ml L-Proline (Sigma-Aldrich), and 1mM sodium pyruvate (Gibco™). 10 ng/
mlofTGFβ1(R&Dsystems;Minneapolis,Minnessota,USA)wasusedto induce
chondrogenesis.Mediumwasrefreshed3timesaweek.After14days,beadswere
culturedwith25% IPFPCMorunconditionedmedium.SupplementsandTGFβ1

Triamcinolone affects infrapatellar fat pad and macrophages 85
5
werealwaysaddedaftermixingthemediumwithCMorunconditionedmedium.
Thisway,alltheconditionshadthesamefinalamountofsupplementsandTGFβ1.Beadswereharvestedafter3additionaldaysofcultureandmediumwasrefreshed
24hourspriortoharvest.
Isolation and culture of human fibroblast like synoviocytes
Human synoviumwas obtained as leftovermaterial from 3 end-stage kneeOA
patientswhohadundergonea totalkneearthroplasty (ErasmusMCUniversity
MedicalCenter,TheNetherlands,MEC2008-181).Thesynoviumwasseparated
fromtheunderlyingfat,cutintosmallpiecesanddigestedovernightwith1mg/ml
collagenaseB(Roche,Germany)inIscove’smodifiedDulbecco’smedium(IMDM;
Gibco™)containing10%FCS.Thecellsuspensionwasthenfilteredthrougha100
µmfilter,followedbycentrifugationat250gfor8minutes.Theresultingcellpellet
wasre-suspendedandcellswereplatedat3500cells/cm2inIMDMwith10%FCS.
After reaching sub-confluency, cellswere trypsinised and re-seeded. Fibroblast
like synoviocytes (FLS) of passage 3wereplated asmonolayer at 50.000 cells/
cm2 in IMDM with 10% FCS and allowed to attach. After 72 hours, cells were
washed3timeswithsalineandDMEM-HGcontainingITS+with25%IPFPCMor
unconditioned medium were added. 25 μg/mL ascorbic acid-2-phosphate was
alsoaddedtotheculturemedium.After4daysofculture,mediumwasremoved
andcellswereharvest inRLTbuffer (Qiagen,Venlo,TheNetherlands)with1%
β-mercaptoethanol.Mediumwasrefreshed24hourspriortoharvest.
RNA extraction and gene expression analysis
FrozenIPFPexplantswerehomogenizedwithaMikro-Dismembrator(BraunBio-
techInternationalGmbH,Melsungen,Germany)re-suspendedin1.8mlRNA-Bee
(TelTest,Friendswood,Texas,USA).MSCalginatebeadsweredissolvedinice-cold
55mMsodiumcitrateat4 ºC.Thesolutionwasthencentrifugedat400g for8
minutesat4ºCandcellpelletswerere-suspendedin600µlRNA-Beeperbead.
Chloroform(Sigma-Aldrich)wasaddedtoallsamplesat200µL/mLRNA-Bee.FLS
wereharvestedinRLTbuffer.
RNAfromIPFPexplants,MSCsandFLSwasfurtherpurifiedusingRNeasyMicro
Kit (Qiagen) according to manufacturer’s instructions. RNA concentration and
qualitywasmeasuredusingNanoDropND1000UV-VisSpectrophotometer(Isogen
LifeScience,Veldzicht,TheNetherlands).RNAwasreverse-transcribedtocDNA
usingtheRevertAidFirstStrandcDNASynthesisKit(ThermoFisher)accordingto
manufacturer’sinstructions.qRT-PCRwasperformedin10µLreactionsoncDNA
usingtheCFX96Touch™Real-TimePCRDetectionSystem(Biorad,Hercules,Cali-
fornia,USA).Expressionofglyceraldehyde-3-phosphatedehydrogenase(GAPDH),

86 CHAPTER 5
tumor necrosis factor alpha (TNFA), interleukin-1β (IL1B), IL6, cluster of differ-
entiation (CD)206, CD163 matrix metalloproteinase (MMP)-1, MMP-13, collagen
typeII(COL2A1),aggrecan(ACAN),collagentypeI(COL1A1),procollagen-lysine
2-oxoglutarate5-dioxygenase2(PLOD2),andα-smoothmuscleactin(ASMA)were
determinedwithqRT-PCR.GeneexpressionwascalculatedaccordingtotheΔΔCt
method andGAPDHwas used as housekeeper. Ct values between the samples
withineachexperimentdifferlessthan1Ctandtherewerenosignificantdiffer-
encesbetweentheconditions.0.1%DMSOandtreatmentwithmedicationdidnot
interferewithGAPDHlevel.Unlessotherwisestated,theconditiontreatedwith
unconditionedmediumandDMSOwasusedascontrolandsetat1.0.Expression
levelsofotherconditionsareexpressedrelativetothecontrolcondition.Primer
sequencescanbefoundinthesupplementarymethods,
Statistical analysis
IBMSPSSstatistics21(IBMCorporation,Armonk,NewYork,USA)wasusedfor
statisticalanalysis.AlldatawasnotnormallydistributedaccordingtotheShapiro-
WilktestandLevene’stestforhomogeneityofvariance.
Ifnototherwisestated,statisticalsignificancebetweenconditionswasdeter-
minedusingtheMann-WhitneyUtest.p<0.05wasconsideredstatisticallysignifi-
cant.
RESULTS
Triamcinolone acetonide reduces IPFP inflammation
Of the four medications tested, only 100 µM TAA significantly reduced TNFA
(p<0.001), IL1B (p<0.001) and IL6 (p<0.001) and increased the expression of
genesencodingforproteinsrelatedtoanti-inflammatoryprocesses,namelyIL10
(p<0.05),CD206(p<0.001)andCD163(p<0.001)inIPFPexplants(Figure1).DMSO
asdiluentof themedicationsdidnot significantly influencegeneexpression in
IPFPexplants(Supplementaryfigure1).
Triamcinolone acetonide reduces IPFP inflammation, even at lower concentrations
BecauseTAAwastheonlymedicationthatsignificantlydecreasedtheexpression
of genes encoding for pro-inflammatory proteins and increased the expression
of genes associatedwith anti-inflammatory processes,we decided to focus on
theeffectsofthismedication.Toreducepossiblenegativeeffectsof100µMTAA,
weinvestigatedwhetheralowerconcentrationofTAAwouldgivethesameanti-

Triamcinolone affects infrapatellar fat pad and macrophages 87
5
inflammatoryresults.Ataconcentrationof0.1µM,TAAstillsignificantlyreduced
TNFA(p<0.05)andIL1B(p<0.05)andincreasedCD206(p<0.05)andCD163(p<0.05)
(Figure2).10and1µMofTAAalsosignificantlyincreasedIL10(p<0.05).IL6expres-
sionwasonlysignificantlyreducedwith10µMofTAAorhigher.TNFA and IL1B
expressionwerenotsignificantlydifferentbetweenthefourconcentrationtested.
TNFA
DMSO0.1
%
Celeco
xib10
mM
Triam. a
cetonide 10
0 mM
Pravas
tatin
50mM
Fenofib
rate 10
0 mM0.0
0.5
1.0
1.5
2.0
2.5
Gen
eex
pres
sion
com
pare
dto
DM
SO
*
IL1B
DMSO0.1
%
Celeco
xib10
mM
Triam. a
cetonide 10
0 mM
Pravas
tatin
50mM
Fenofib
rate 10
0 mM0
1
2
3
4
Gen
eex
pres
sion
com
pare
dto
DM
SO
*
IL6
DMSO0.1
%
Celeco
xib10
mM
Triam. a
cetonide 10
0 mM
Pravas
tatin
50mM
Fenofib
rate 10
0 mM0.0
0.5
1.0
1.5
2.0
Gen
eex
pres
sion
com
pare
dto
DM
SO
*
IL10
DMSO0.1
%
Celeco
xib10
mM
Triam. a
cetonide 10
0 mM
Pravas
tatin
50mM
Fenofib
rate 10
0 mM0
1
2
3
4
Gen
eex
pres
sion
com
pare
dto
DM
SO
*CD206
DMSO0.1
%
Celeco
xib10
mM
Triam. a
cetonide 10
0 mM
Pravas
tatin
50mM
Fenofib
rate 10
0 mM0
2
4
6
8
10
Gen
eex
pres
sion
com
pare
dto
DM
SO *
CD163
DMSO0.1
%
Celeco
xib10
mM
Triam. a
cetonide 10
0 mM
Pravas
tatin
50mM
Fenofib
rate 10
0 mM0
2
4
6
8
10
Gen
eex
pres
sion
com
pare
dto
DM
SO *
Figure 1 TriamcinoloneacetonidereducesIPFPinflammationIPFPexplantsweretreatedfor24hourswithDMSO,celecoxib,triamcinoloneacetonide,pravastatinorfenofi-brate.GeneexpressionofTNFA, IL1B, IL6, IL10, CD206, and CD163inIPFPexplantsaftertreatment,comparedtotheDMSO0.1%treatedcondition.ThegeneexpressionofDMSO0.1%treatedsamplewassetat1.IPFPfrom3donorswereculturedwith2samplesperdonor(n=6).Valuesaremean±SD.*p<0.05versusDMSOtreatedcondition.
Triamcinolone acetonide modulates macrophage phenotype in IPFP
NextweinvestigatedwhetherTAAmodulatesthephenotypeofthemacrophages
in the IPFP,sincemacrophagesareknowntobe important in inflammation.We
investigatedtheeffectof10and1µMonmacrophagesbecausethesetwocon-
centrationsalreadydecreasedpro-inflammatoryandincreasedanti-inflammatory
genesexpression.10µMofTAAsignificantlyincreasedthepercentageofCD14+/
CD206+andCD14+/CD163+cellsintheIPFP,indicatingmacrophageswithanM2-
likephenotype(Figure3).However,TAAdidnotalterthepercentageofCD14+/
CD80+andCD14+/CD86+cellsintheIPFP(Figure3),indicatingthatthepercentage
ofmacrophageswithanM1-likephenotypedidnotchange.

88 CHAPTER 5
TNFA
0.0
0.5
1.0
1.5
Gen
eex
pres
sion
com
pare
dto
DM
SO
10 mM 0.1 mM100 mM 1 mM
+ triamcinolone acetonide
* ** *
0.1%DMSO
IL1B
0.0
0.5
1.0
1.5
Gen
eex
pres
sion
com
pare
dto
DM
SO
10 mM 0.1 mM100 mM 1 mM
+ triamcinolone acetonide
* ** *
0.1%DMSO
IL6
0.0
0.5
1.0
1.5
Gen
eex
pres
sion
com
pare
dto
DM
SO
10 mM 0.1 mM100 mM 1 mM
+ triamcinolone acetonide
**
0.1%DMSO
IL10
0
1
2
3
Gen
eex
pres
sion
com
pare
dto
DM
SO
10 mM 0.1 mM100 mM 1 mM
+ triamcinolone acetonide
**
0.1%DMSO
*
*
CD206
0
2
4
6
8
10
Gen
eex
pres
sion
com
pare
dto
DM
SO
10 mM 0.1 mM100 mM 1 mM
+ triamcinolone acetonide
**
*
*
0.1%DMSO
CD163
0
2
4
6
8
10
Gen
eex
pres
sion
com
pare
dto
DM
SO
10 mM 0.1 mM100 mM 1 mM
+ triamcinolone acetonide
* * * *
0.1%DMSO
Figure 2 TriamcinoloneacetonidereducedIPFPinflammationindoserangeof0.1-100µMIPFPexplantsweretreatedfor24hourswithtriamcinoloneacetonideintheconcentrations0.1µM-100µM.GeneexpressionofTNFA, IL1B, IL6, IL10, CD206, and CD163inIPFPexplantsaftertreatment,comparedtothecondi-tiontreatedwith0.1%DMSOonly.Geneexpressionin0.1%DMSOonlywassetat1.IPFPfrom2donorswereculturedwith3samplesperdonor(n=6).Valuesaremean±SD.*p<0.05versus0.1%DMSOtreatedsamples
CD80
Perc
enta
geof
CD
14+
cells
com
pare
dto
DM
SO
0
1
2
3
0.1% DMSO 10 mM
+ triamcinolone acetonide
1 mM
CD86
Perc
enta
geof
CD
14+
cells
com
pare
dto
DM
SO
0.0
0.5
1.0
1.5
10 mM
+ triamcinolone acetonide
1 mM0.1% DMSO
CD163
Perc
enta
geof
CD
14+
cells
com
pare
dto
DM
SO
0
2
4
6
8
10
*
10 mM
+ triamcinolone acetonide
1 mM0.1% DMSO
*CD206
Perc
enta
geof
CD
14+
cells
com
pare
dto
DM
SO
0.0
0.5
1.0
1.5
2.0
2.5
*
10 mM
+ triamcinolone acetonide
1 mM0.1% DMSO
Figure 3 TriamcinoloneacetonidemodulatesmacrophagesinIPFP.IPFPexplantsweretreatedfor24hourswithtriamcinoloneacetonideintheconcentrations10µMand1µM.Intheseexplants,percentageofCD80,CD86,CD206andCD163positivecellswithintheCD14positivepopulation(indicatingmacrophages)wasdeterminedusingflowcytometry.Relativepercentageofpositivecellsaftertreatment,comparedtotheconditiontreatedwith0.1%DMSOonly.Conditiontreatedwith0.1%DMSOonlywassetat1.Valuesarefrom5IPFPdonorswith1-3samplesperdonor(n=12).Valuesaremean±SD.*p<0.05versus0.1%DMSO.

Triamcinolone affects infrapatellar fat pad and macrophages 89
5
Triamcinolone acetonide reduces anti-chondrogenic and pro-catabolic effects of IPFP
Finally,we investigatedwhetherTAAcan reduce thenegativeeffectof IPFPon
chondrogenesisofMSCsandthefibroticandcatabolicprocessesinfibroblastlike
synoviocytes (FLS). Factors secretedby untreated IPFP significantly decreased
COL2A1(p<0.05)inchondrogenicallystimulatedMSCs(Figure4A).Treatmentof
theIPFPwith1µMand10µMTAAwhilemakingtheCMsignificantlyreducedthisef-
fect,althoughnotentirely.FactorsproducedbyIPFPsignificantlyincreasedMMP1
and MMP13inMSCs(p<0.05)(Figure4A)andFLS(p<0.05)(Figure4B).Treatment
oftheIPFPwithTAAduringmakingoftheCMsignificantlyreducedtheexpres-
sionofthesegenesinMSCsandFLS.SinceTAAwasalsopresentinthemedium
conditionedbyIPFP,wealsoaddedTAAdirectlytothechondrogenicstimulated
MSCalginatebeadsandtheFLS.COL2A1 and ACAN were significantly reduced in
MSCsbyTAA.COL1A1,ASMA,MMP1, and MMP13 were significantly reduced and
PLOD2significantlyincreasedinFLSbyTAAtreatment(Supplementaryfigure2).
Thissuggests thatTAAmainlyactsbyreducing theanti-chondrogeniceffectof
othercellsonMSCsandnotthroughstimulationofchondrogenesisinMSCs.
COL2A1
TGFb1only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0.0
0.5
1.0
1.5
**
*#
#
Gen
eex
pres
sion
com
pare
dto
TGF b
1on
ly
ACAN
TGFb1only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0.0
0.5
1.0
1.5
* *
MMP1
TGFb1only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0
2
4
6
8
10
*
**#
#
*
MMP13
TGFb1only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0
1
2
3
*
* *#
#
COL1A1
FLS only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0.0
0.5
1.0
1.5
Gen
eex
pres
sion
com
pare
dto
FLS
only
*
* *##
ASMA
FLS only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0.0
0.5
1.0
1.5
* * *
PLOD2
FLS only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0
1
2
3
4
5
* **
*
MMP1
FLS only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0
1
2
3
4
*
* *##
MMP13
FLS only
+0.1%
DMSO+C
M
+CM
+10mM
TAA
+CM
+1mM
TAA0
5
10
15*
* *##
A
B
Figure 4 Triamcinolone acetonide reduces the anti-chondrogenic and pro-catabolic effects ofIPFP.FLSandchondrogenicstimulatedMSCalginatebeadsweretreatedwithCMfromIPFPtreatedwithoutorwithTAAintheconcentrations10µMand1µM.A)COL2A1, ACAN, MMP1, and MMP13expressioninchondrogenicstimulatedMSCalginatebeadsrelativetotheconditiontreatedwithTGFβ1only.B)COL1A1, PLOD2, ASMA, MMP1, and MMP13expressioninFLSrelativetotheconditionwithonlyFLSinculture.GeneexpressioninTGFβ1onlyandFLSonlyconditionsweresetat1.3differentpoolsofCMofeachfrom3IPFPdonorswereusedtotreat3MSCdonorsand3FLSdonors,witheachconditionperformedintriplicate(n=9).Valuesrepresentmean±SD.*p<0.05versusnon-treatedcontrols(TGFb1onlyorFLSonly).#p<0.05versustreatedwithCMonly.

90 CHAPTER 5
DISCUSSION
Inthisstudy,weinvestigatedwhetheranti-inflammatorymedicationscanreduce
IPFP inflammationand therebyprevent thenegativeeffectof IPFPonchondro-
genic MSCs9 and synovial fibroblasts10;11. We have tested four commonly used
medications and found that TAA, a glucocorticoid, reduced IPFP inflammation
andmodulatedIPFPmacrophagephenotype.Furthermore,TAAreducedtheanti-
chondrogeniceffectofIPFPonMSCsandthepro-cataboliceffectonFLS.
Inflammationplaysamajorinhibitoryroleinjointrepair1andmacrophagesplay
animportantroleininflammation19.Nexttothesynovium,whichisoftenstudied
inrelationtojointinflammation,theIPFPcanbecomeinflamed.TheIPFPcontains
a largenumberofmacrophages,andwasproposed tostimulatesynovialfibro-
sis10 and inhibit of chondrogenesis during cartilage repair9.Inthecurrentstudy
study,TAAnotonlydecreasedexpressionofgenesencodingforpro-inflammatory
proteins in IPFPbut also increased the percentage ofmacrophages expressing
CD163andCD206proteinontheirsurfaceintheIPFP.Anti-inflammatoryorM2-like
macrophagesexpressCD163andCD206.Furthermore,theyexpressfactorsthat
reduce inflammationor stimulate tissue repair, such as IL10orCCL1818; 20. The
increaseofM2-likemacrophagesinIPFPcouldeitherdirectlyorindirectlyaffect
theM1-likemacrophages.Asaresult,thechangeinfavourofM2-likemacrophages
mighthavecontributedtothealteredgeneexpressionofinflammatorycytokines.
Inthisway,theanti-chondrogeniceffectofIPFPonMSCandpro-cataboliceffect
onFLScanbereduced.
Theusedmedicationwaschoosenfortheiranti-inflammatoryeffects.However,
celecoxib,pravastatinandfenofibratedidnotinfluenceIPFPinflammationfocus-
ing on genes known to be expressedbydifferentmacrophagephenotypes.We
thereforedecidednottocontinuewithcelecoxib,pravastatin,andfenofibratein
the current study, as inflammation driven by themacrophages seem to play a
large role in the negative effect of IPFP on joint tissues9; 10.We cannot exclude
however that celecoxib, pravastatin and fenofibrate might have an effect on
anti-chondrogenic and catabolic properties of IPFP through inhibition of other
pathwayslessrelatedtoinflammationandviaothercellsthanthemacrophages.
TAAiscurrentlyinjectedintra-articularlyastreatmentofpainandinflammation
inearly-OA.Althoughsymptomaticreliefdoesoccur,nostructuralmodifyingef-
fect on cartilage is seen6.TAAdoesreducecatabolicprocessesinOAsynovium
explantsco-culturedwithcartilageexplants17andin-vivoratstudieshaveshown

Triamcinolone affects infrapatellar fat pad and macrophages 91
5
thatintra-articularinjectionofTAAcanreducepost-traumaticarthrofibrosis21;22.
TAAinjectedintra-articularlydirectlyafterjointtraumacouldalsoreducesyno-
vitis23. Furthermore, unlike other glucocorticoids, it is not toxic to cartilageor
synovium24-26. There are cases of adipose tissue atrophy described after TAA
injection27.AsystematicreviewbyBrinksetalshowedthattheseadverseevents
arerareandifpresent,arerelativelymild28.RepeatedinjectionsofTAAhowever,
increasedcollagentype2andaggrecanreleaseandturnoverinkneecartilageof
horses29.ToreducethenegativeeffectsofTAAoncartilage,adosageaslowaspos-
sibleispreferred.Inourcurrentstudy,expressionofGAPDH was not influenced
bytreatmentwithanyoftheconcentrations,suggestingthattheconcentrations
ofTAAweusedhadnogrossoveralleffectoncellmetabolism.Furthermore,TAA
influencedIPFPinflammationataconcentrationof0.1µM,andreducedtheanti-
chondrogenicandpro-cataboliceffectsofIPFPat1µM.Thissuggeststhatalower
doseofTAissufficienttomodulatetheIPFP.
Inrabbits,asingleintra-articularinjectionoftheglucocorticoiddexamethasone
reducesIPFPcellularityandfibrosis48hoursafterjointtrauma.Howeveritdidnot
reduce IL1BexpressionnorwereeffectsonIPFPcellularityandfibrosisstillpresent
after9weeks30.Therefore,ahigherdosageand/ormultipleintra-articularinjec-
tionsofmedicationmightbeneededbeforeaprolongedeffectivelevelisreached
intheIPFP.MultipleinjectionsthatresultinahigherconcentrationofTAA,might
however,benegativeforcartilageandMSCs31.Toreducethenumberofinjections
andtheside-effectsofahighdosage,aslow-releasedrugdeliverysystemdirectly
in the IPFPcouldbeasolution. Besidesasustaineddeliverysystem, the time
ofdeliveryisalsocrucial.Directlyafterjointtrauma,levelsofpro-inflammatory
factorsinthesynovialfluidpeak32;33.Thelevelofthesepro-inflammatoryfactors
dropsovertime,butarestillhigherininjuredkneesthaninuninjuredkneesupto
1yearafterinjury34.ThetimingofadditionofTAAisthereforeimportantaswell
astherequireddosage,whichcouldchangeovertimedependingontheexpected
levelofinflammation.
Taken together, TAA reduces IPFP inflammation and the anti-chondrogenic and
pro-cataboliceffectoftheIPFPonthejoint.Thisispossiblycausedbymodulation
ofmacrophagesintheIPFP.ThereforeTAAisapromisingmedicationtomodulate
thejointenvironment,therebycreatingabetterenvironmentforsuccessfulcar-
tilagerepair.

92 CHAPTER 5
REFERENCES
1. ZhangY,PizzuteT,PeiM.2014.Anti-inflammatorystrategiesincartilagerepair.TissueEngPartB
Rev20:655-668.
2. BannuruRR,SchmidCH,KentDM,etal.2015.Comparativeeffectivenessofpharmacologicinter-
ventionsforkneeosteoarthritis:asystematicreviewandnetworkmeta-analysis.AnnInternMed
162:46-54.
3. AbeM,MatsudaM,KobayashiH, et al. 2008. Effectsof statinson adipose tissue inflammation:
theirinhibitoryeffectonMyD88-independentIRF3/IFN-betapathwayinmacrophages.Arterioscler
ThrombVascBiol28:871-877.
4. ClockaertsS,Bastiaansen-JenniskensYM,FeijtC,etal.2012.Cytokineproductionbyinfrapatellar
fatpadcanbestimulatedbyinterleukin1betaandinhibitedbyperoxisomeproliferatoractivated
receptoralphaagonist.AnnRheumDis71:1012-1018.
5. vanEekerenIC,ClockaertsS,Bastiaansen-JenniskensYM,etal.2013.Fibratesastherapyforosteo-
arthritisandrheumatoidarthritis?Asystematicreview.TherAdvMusculoskeletDis5:33-44.
6. EvansCH,KrausVB,SettonLA.2014.Progressinintra-articulartherapy.NatRevRheumatol10:11-
22.
7. ScottiC,GobbiA,KarnatzikosG,etal.2016.CartilageRepairintheInflamedJoint:Considerations
forBiologicalAugmentationTowardTissueRegeneration.TissueEngPartBRev22:149-159.
8. ClockaertsS,Bastiaansen-JenniskensYM,RunhaarJ,etal.2010.Theinfrapatellarfatpadshould
beconsideredasanactiveosteoarthriticjointtissue:anarrativereview.OsteoarthritisCartilage
18:876-882.
9. WeiW,RudjitoE,FahyN,etal.2015.Theinfrapatellarfatpadfromdiseasedjointsinhibitschondro-
genesisofmesenchymalstemcells.EurCellMater30:303-314.
10. Bastiaansen-JenniskensYM,WeiW, Feijt C, et al. 2013. Stimulation of fibrotic processes by the
infrapatellarfatpadinculturedsynoviocytesfrompatientswithosteoarthritis:apossiblerolefor
prostaglandinf2alpha.ArthritisRheum65:2070-2080.
11. Eymard F, Pigenet A, CitadelleD, et al. 2014. Induction of an inflammatory and prodegradative
phenotypeinautologousfibroblast-likesynoviocytesbytheinfrapatellarfatpadfrompatientswith
kneeosteoarthritis.ArthritisRheumatol66:2165-2174.
12. He J, Jiang Y, Alexander PG, et al. 2017. Infrapatellar fat pad aggravates degeneration of acute
traumatizedcartilage:apossibleroleforinterleukin-6.OsteoarthritisCartilage25:138-145.
13. Bastiaansen-JenniskensYM,ClockaertsS,FeijtC,etal.2012.Infrapatellarfatpadofpatientswith
end-stageosteoarthritisinhibitscatabolicmediatorsincartilage.AnnRheumDis71:288-294.
14. FahyN,deVries-vanMelleML,LehmannJ,etal.2014.Humanosteoarthriticsynoviumimpacts
chondrogenicdifferentiationofmesenchymalstemcellsviamacrophagepolarisationstate.Osteo-
arthritisCartilage22:1167-1175.
15. SesiaSB,DuhrR,MedeirosdaCunhaC,etal.2015.Anti-inflammatory/tissuerepairmacrophages
enhance the cartilage-forming capacity of human bone marrow-derived mesenchymal stromal
cells.JCellPhysiol230:1258-1269.
16. ToyodaT,KameiY,KatoH,etal.2008.Effectofperoxisomeproliferator-activatedreceptor-alpha
ligandsintheinteractionbetweenadipocytesandmacrophagesinobeseadiposetissue.Obesity
(SilverSpring)16:1199-1207.
17. BeekhuizenM,Bastiaansen-JenniskensYM,KoevoetW,etal.2011.Osteoarthriticsynovialtissue
inhibitionofproteoglycanproductioninhumanosteoarthritickneecartilage:establishmentand
characterizationofalong-termcartilage-synoviumcoculture.ArthritisRheum63:1918-1927.

Triamcinolone affects infrapatellar fat pad and macrophages 93
5
18. UtomoL,vanOschGJ,BayonY,etal.2016.Guidingsynovialinflammationbymacrophagepheno-
typemodulation:an invitrostudytowardsatherapyforosteoarthritis.OsteoarthritisCartilage
24:1629-1638.
19. HamidzadehK,ChristensenSM,DalbyE,etal.2017.MacrophagesandtheRecoveryfromAcute
andChronicInflammation.AnnuRevPhysiol79:567-592.
20. MurrayPJ,AllenJE,BiswasSK,etal.2014.Macrophageactivationandpolarization:nomenclature
andexperimentalguidelines.Immunity41:14-20.
21. ClarkDD,WeckesserEC.1971.Theinfluenceoftriamcinoloneacetonideonjointstiffnessintherat.
JBoneJointSurgAm53:1409-1414.
22. EfirdW,KellamP,YeazellS,etal.2014.Anevaluationofprophylactictreatmentstopreventpost
traumaticjointstiffness.JOrthopRes32:1520-1524.
23. SiekerJT,AyturkUM,ProffenBL,etal.2016.ImmediateAdministrationofIntraarticularTriamcino-
loneAcetonideAfterJointInjuryModulatesMolecularOutcomesAssociatedWithEarlySynovitis.
ArthritisRheumatol68:1637-1647.
24. ShermanSL,JamesC,StokerAM,etal.2015.InVivoToxicityofLocalAnestheticsandCorticoste-
roidsonChondrocyteandSynoviocyteViabilityandMetabolism.Cartilage6:106-112.
25. ShermanSL,KhazaiRS,JamesCH,etal.2015.InVitroToxicityofLocalAnestheticsandCorticoste-
roidsonChondrocyteandSynoviocyteViabilityandMetabolism.Cartilage6:233-240.
26. SolaM,DahnersL,WeinholdP,etal.2015.Theviabilityofchondrocytesafteraninvivoinjectionof
localanaestheticand/orcorticosteroid:alaboratorystudyusingaratmodel.BoneJointJ97-B:933-
938.
27. ImagawaK,OhkumaS.2010.Acaseoffatinjectionfortreatingsubcutaneousatrophycausedby
localadministrationofcorticosteroid.TokaiJExpClinMed35:66-69.
28. BrinksA,KoesBW,VolkersAC,etal.2010.Adverseeffectsofextra-articularcorticosteroidinjec-
tions:asystematicreview.BMCMusculoskeletDisord11:206.
29. CelesteC,IonescuM,RobinPooleA,etal.2005.Repeatedintraarticularinjectionsoftriamcinolone
acetonidealtercartilagematrixmetabolismmeasuredbybiomarkersinsynovialfluid.JOrthop
Res23:602-610.
30. HeardBJ,SolbakNM,ChungM,etal.2016.Theinfrapatellarfatpadisaffectedbyinjuryinduced
inflammationintherabbitknee:useofdexamethasonetomitigatedamage.InflammRes65:459-470.
31. WylesCC,HoudekMT,WylesSP,etal.2015.Differentialcytotoxicityofcorticosteroidsonhuman
mesenchymalstemcells.ClinOrthopRelatRes473:1155-1164.
32. BigoniM,SacerdoteP,TuratiM,etal.2013.Acuteandlatechangesinintraarticularcytokinelevels
followinganteriorcruciateligamentinjury.JOrthopRes31:315-321.
33. CatterallJB,StablerTV,FlanneryCR,etal.2010.Changesinserumandsynovialfluidbiomarkers
afteracuteinjury(NCT00332254).ArthritisResTher12:R229.
34. LieberthalJ,SambamurthyN,ScanzelloCR.2015.Inflammationinjointinjuryandpost-traumatic
osteoarthritis.OsteoarthritisCartilage23:1825-1834.

94 CHAPTER 5
TNFAIL1B IL6
IL10
CD206
CD163
0
1
2
3
4
Gen
eex
pres
sion
rela
tive
toco
ntro
l
Control+ DMSO 0.1%+ DMSO 0.01%
Supplementary figure 1DMSOdoesnotsignificantlyaffectgeneexpressioninIPFPexplants.IPFPexplantsweretreatedfor24hourswithDMSO.GeneexpressionofTNFA, IL1B, IL6, IL10, CD206 and CD163 comparedtocontrol.Geneexpressionofcontrolwassetat1.Resultsarefrom3donorswith2samplesperdonor(n=6).Valuesaremean±SD.*p<0.05versuscontrol.
COL2A1
TGFb1only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
* *
Gen
eex
pres
sion
com
pare
dto
TGF b
1on
ly
MMP1
TGFb1only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
2.0
*
MMP13
TGFb1only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
COL1A1
FLS only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
Gen
eex
pres
sion
com
pare
dto
FLS
only
* *
ASMA
FLS only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
* *
PLOD2
FLS only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0
1
2
3
4
* **
MMP1
FLS only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
2.0
* *
MMP13
FLS only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
2.0
* *
ACAN
TGFb1only
+0.1%
DMSO
+10mM
TAA
+1mM
TAA0.0
0.5
1.0
1.5
* *
A
B
Supplementary figure 2TriamcinoloneacetonidehasaneffectonMSCandFLS.FLSandchondrogenicstimulatedMSCalginatebeadsweretreatedwithTAAintheconcentrations10µMand1µM.A)COL2A1, ACAN, MMP1, and MMP13expressioninchondrogenicstimulatedMSCalginatebeadsrelativetotheconditiontreatedwithTGFβ1only.B)COL1A1, PLOD2, ASMA, MMP1, and MMP13inFLSrelativetotheconditionwithonlyFLSinculture.GeneexpressioninTGFβ1onlyandFLSonlyconditionsweresetat1.TAAwasusedtotreat3MSCdonorsand3FLSdonors,witheachconditionperformedintriplicate(n=9).Valuesrepresentmean±SD.*p<0.05versusnon-treatedcontrols(TGFb1onlyorFLSonly).



PART II
Systemic effects of adipose tissue


CHAPTER 6
Statins and fi brates do not affect development
of spontaneous cartilage damage in STR/Ort mice
Wu Wei Stefan Clockaerts
Yvonne M. Bastiaansen-Jenniskens Lobke M. Gierman
Sander M. Botter Sita M.A. Bierma-Zeinstra
Harrie Weinans Jan A.N. Verhaar
Margreet KloppenburgAnne-Marie Zuurmond
Gerjo J.V.M. van Osch
Osteoarthritis Cartilage. 2014 Feb;22(2):293-301

100 CHAPTER 6
ABSTRACT
Objective
Sincestatinsandfibratesarecapableof improving themetabolicprofileofpa-
tientsaswellasdecreasinginflammation,theyareconsideredaspotentialdrugs
forpreventingOA.Thegoalofthepresentstudywastoinvestigatetheeffectof
thesedrugsintheSTR/OrtspontaneousOAmousemodel.
Design
MaleSTR/Ortmicereceivedcontroldietorcontroldietcontainingtwodifferent
dosages of simvastatin or fenofibrate or a combination of both.Micewere eu-
thanizedafter16weeksoftreatmentattheageof24weeks.Serumanalysisfor
metabolicandinflammatorymarkers,histologicOAgradingandμCTanalysisof
subchondralboneplatewereperformed.
Results
Simvastatintreatmentdidnothaveastatisticallysignificanteffectonanyofthe
measuredparameters.Fenofibratetreatedmicegainedlessbodyweightandhad
lowerserumamyloidA(SAA)levels,buthigherIL1αandMIP1αthanothermice.
Micetreatedwith200mg/kgBW/dayfenofibratehadlesssubchondralboneplate
volume thancontrol,butno statistically significant reduction incartilagedam-
age.Inthecombinationtreatmentgroup,bodyweightandSAAwerelowerthan
control.
Overall,bodyweight,synoviummembranecelllayersandSAAlevelscorrelated
to subchondral bone plate changes and subchondral bone plate changes corre-
latedtocartilagedamage.
Conclusions
StatinsandfibratesdidnotaffectdevelopmentofcartilagedamageintheSTR/Ort
spontaneousosteoarthritismousemodel.Fenofibrateshowever,hadaneffecton
bodyweight,seruminflammationmarkersandsubchondralboneplatemorphol-
ogy.

Statins and fibrates in the STROrt mouse model 101
6
INTRODUCTION
Thecurrentnonsurgicaltreatmentoptionsforosteoarthritis(OA)arelimitedto
nonpharmacologicalinterventionssuchaslifestylechanges,exerciseorweight
reduction,withpharmacological treatmentofsymptomsifneeded.Noeffective
diseasemodifyingdrugiscurrentlyonthemarketforOA1.OAisacommonjoint
diseasethataffectstheentirejoint,includingthearticularcartilage,subchondral
boneandthesynovialmembrane.Highageandobesityarebothmajorriskfactors
ofOA.Prevalenceandincidencefiguresareexpectedtorisewithincreasinglife
expectancyandgrowingobesity2;3.
Themetabolic syndrome is a concurrenceofobesity,hyperinsulinemia,dyslip-
idemia and hypertension4.Metabolic OA is considered one of the subtypes of
OAandisassociatedwiththemetabolicsyndrome.Besideshyperglycaemiaand
increasedserumlipids,alsothevascularpathologyassociatedwiththemetabolic
syndromemighthavenegativeeffectsonthecartilage5.
Statins are hydroxylmethylglutaryl coenzyme-A reductase inhibitors that de-
creaseserumcholesterollevels,reducesystemicinflammation,anddecreasethe
amountofcardiovascularevents6;7.FibratesareligandsofPeroxisomeProliferator
ActivatedReceptor(PPAR)α.Thesedrugsdecreaseserumtriglyceridesandalso
exert anti-inflammatory effects on different tissues. Like statins, they decrease
inflammatoryprocessesincartilage,synoviumandintra-articularadiposetissue
inin-vitrostudies8-14.Chroniclowgradeinflammationplaysanimportantrolein
thepathogenesisofOAandmetabolicsyndrome4.Sincestatinsandfibratescan
potentially inhibit inflammatory processes in the joint as well as improve the
metabolicprofileofpatients,theymightofferapotentialtherapeuticorpreven-
tive strategy forOA.Recently,weassociated theuseof statinswithdecreased
incidenceandslowerprogressionofkneeOAintheRotterdamStudyonx-rays15.
KadametalassociatedtheuseofstatinwithdecreasedincidenceofclinicalOA
intheGeneralPracticeResearchDatabasefromtheUnitedKingdoms16.Nodirect
associationbetweentheuseoffibratesandincidenceofOAhasbeendescribed
yet17.Beforestartingaclinicaltrialthatdirectlyaddressesthequestionwhether
statinsandfibratesareabletopreventOAorOAprogression,anin-vivoanimal
studyshouldbeperformed.
IntheSTR/Ortmousestrain,80%ofthemalemicespontaneouslydevelopOAin
thetibiofemoraljointattheageof6month,particularlyatthemedialcondyleswith
similarhistopathologicallesionsasinhumans18.STR/Ortmicealsospontaneously

102 CHAPTER 6
develop obesity19. Furthermore, serum levels of total cholesterol, high density
lipoprotein(HDL)cholesterol,LDLcholesterol, triglycerides,nonesterified fatty
acids,glucoseandinsulinarereportedtobeincreasedinSTR/Ortmicecompared
toC57BL/6Jmice19.InadditionithasbeensuggestedthatSTR/Ortmicedevelop
OAspontaneouslyduetothereductionofendogenousPPARαorPPARγsignalling,andthuspossiblyincreasinginflammationandalteringosteoblastphenotype20.
Forthesereasons,theSTR/Ortmousemodelseemseminentlysuitedtoinvesti-
gatetheeffectsofstatinsandfibratesonOAdevelopment. Inthisstudy,wein-
vestigatedwhetheradministrationofsimvastatinorfenofibrateoracombination
ofbothwouldpreventordelaythedevelopmentofOAinthetibiofemoraljoint.
Weevaluatedtheeffectofthistreatmentonserumcholesterol,triglyceride,the
inflammationmarkerserumAmyloidA(SAA)andtheinflammatorycytokinesin
theblood.Cartilagedamagewasevaluatedwithhistologyandjointbonemorphol-
ogywithmicrocomputedtomography(μCT).
METHODS
Animals
Four-week-oldmaleSTR/Ortmice(n=72)acquiredfromHarlanItaly(Udine,Italy)
were maintained at the animal testing facilities of the ErasmusMC University
MedicalCenter,TheNetherlands.Micewerehousedingroupsofthreemiceper
cageunderstandardconditionsandhadaccesstowaterandfoodadlibitum.The
studyprotocolwasapprovedbytheinstitutionalAnimalCareandUseCommittee
(ErasmusMCUniversityMedicalCenter,TheNetherlands,AEC116-10-01)
Diets and drug intake
Mice were fed semi-synthetic non-irradiatedmice reference diet (AbDiets,Wo-
erden,TheNetherlands)for4weeksbeforefeedingtheexperimentaldiets.Body
weight(BW)wasmeasuredeverytwoweeksandfoodwasreplaced2-3timesper
week.AverageBWpermouseandaverage food intakeper cageperday could
thusbedeterminedandwecouldcalculatetheamountofdrugs(mg/kg)needed
tobemixedwithreferencedietforthemicetoreceivetheintendedtargetdosage
(mg/kgBW/day).Attheageof8weeks,themiceweredividedinto6experimental
groupsofn=12.Group1(control)continuedtoreceivethenon-supplemented
referencediet.Group2and3receivedreferencedietmixedwitheither300or750
mg/kgsimvastatin(Eurogenerics,Brussel,Belgium),whichcorrespondstodos-
agesof40and100mg/kgBW/day.Groups4and5receivedreferencedietmixed

Statins and fibrates in the STROrt mouse model 103
6
witheither600or1500mg/kgfenofibrate(Eurogenerics,Brussel,Belgium),which
correspondstodosagesof80and200mg/kgBW/day.Finally,group6receiveda
combinationofsimvastatin(300mg/kg)andfenofibrate(600mg/kg)withdosages
40and80mg/kgBW/dayrespectively.Targetdosagesofeachdrugwerebased
uponwhatisoftenusedintheliteraturetostudytheanti-inflammatoryorlipid
lowering effects of these drugs 21.Allexperimentaldietswereprovidedandmixed
byABDiets(Woerden,TheNetherlands)andwerestoredat4ºCforamaximumof
26weeks.Attheageof6monthsthemiceweresacrificedviaisofluraneanesthesia
andheartpuncturing.
Onemouse in the simvastatin 40mg/kg BW/day treatment group rapidly lost
weight andwaseuthanized2weeksbefore theendof the study.Nevertheless,
havingcompleted>90%ofthestudyperiod,wedecidedtoincludethedatafrom
thismouseinallanalyses.
Serum analysis
Bloodwascollectedthroughacheekpuncturepriortothestartofexperimental
diet.Atendpoint,bloodwascollectedthroughaheartpuncture.Bloodwasstored
for1houratroomtemperature,followedby30minutesat4ºC,thencentrifuged
for5minutesat12.000rpmandserumwasremovedandimmediatelystoredat
-80ºC. Total plasma cholesterol (RocheDiagnostics kit no.1489437) andplasma
triglyceride(Rochediagnosticskitno.1488872)weredeterminedafterdefrosting.
SerumAmyloidA(SAA)wasalsodeterminedineachsamplebyELISA(Tridelta
development, Maynooth, Ireland) according to the manufacturer’s instruction.
Mouseinflammatorycytokines(FGFbasic,GM-CSF,IFN-γ,Interleukin(IL)-1α,IL-1β,IL-2,IL-4,IL-5,IL-6,IL-10,IL-12p40/p70,IL-13,IL-17,IP-10,KC,MCP-1MIG,MIP-1α,TNF-αandVEGF)weremeasuredusingamagnetic20-plexbeadassay(Invitrogen,
Frederick,MD,USA)accordingtomanufacturer’sinstructions.
Duetotechnicalproblemsduringsampleprocessing,theserumsamplesofone
mouseinthecontrolgroupandtwoofthesimvastatin40mg/kgBW/daytreatment
groupwerelost.
µCT analysis
Thelefthindlegsofallanimalswereexcisedandfixedin4%bufferedformalinfor
µCTandhistology.WeusedtheSkyscan1176X-raymicrotomographandcomple-
mentarydedicatedsoftware(Brukermicro-CT,Kontich,Belgium)toanalyzethe
subchondralbonemorphologyintheproximaltibiaoftheleftknee.Thefollowing
scansettingswereused:voltage100kV;current100µA;filter0.5mmaluminium;
imagepixel size 17.92 μm; exposure time 2360ms; frame averaging 3;with 0.4
degree rotation through 180degrees. Following scanning, datasetswere recon-

104 CHAPTER 6
structedusingNRecon(Bruker-Skyscan).Segmentationwasperformedwithalo-
calthresholdalgorithm22andusingCTAnalyser(Bruker-Skyscan),themedialand
lateralsubchondralboneplate(regionofinterestdepth:1.61mmventro-dorsal,
starting fromtheanterior intercondylararea; regionof interestwidth:adjusted
accordingtototalmedio-lateralwidthineachtibia,thensplitinhalfinthemiddle
oftheintercondylareminence,yieldingalateralandamedialpart)wereselected
asregionsofinterest.Finally,CTAnalyserwasusedtocalculatesubchondralbone
plate bone volume (BV) and subchondral bone plate thickness, as described
previously23.
Histological analysis
AfterμCTscanning,thelegsweredecalcifiedin10%formicacidindistilledwater
for10daysandembeddedinparaffinand6µmthickcoronal(frontal)histological
sectionswere cut at 100µm intervals through the joint. Sectionswere stained
with thionine. Two independent blinded observers scored cartilage damage
atthemedialandlateralsidesofboththefemurandthetibiaaccordingtothe
semi-quantitativescoringsystemdevisedbytheOsteoarthritisResearchSociety
International(OARSI)histopathologyinitiative24.Briefly,thisscoringsystemhas
arangefrom0to6,with0meansnormalcartilage,1smallfibrillationswithout
lossofcartilageand3-6erosionstothecalcifiedcartilageextendingfrom<25%
to>75%.Onlyslideswhereallfour(i.e.themedialandlateralsidesofboththe
femurandtibia) locationswerevisiblewereused.Themeanscoreof threedif-
ferentslideswasdeterminedandincaseofa>0.5scorediscrepancybetweenthe
firstobservers,athirdindependentobserverrescoredtheslides.Todetermine
whether treatment has an effect on synovial inflammation, the number of cell
layersofthesynoviummembraneonthemedialsideofthepatellawascounted.
Themeannumberofcelllayersofthreedifferentslideswasusedinthestatistical
analysis.
Duetotechnicalerrorduringanalysis,thekneesofonecontrolmouseandone
combinationtreatedmousewerelost.
Data analysis
Statistical analysis was performed in IBM SPSS statistics 20 (IBM Corporation,
Armonk,NewYork,USA)andR:Alanguageandenvironmentforstatisticalcom-
puting 3.0.2 (R Development Core Team, Vienna, Austria). Data was tested for
normalityusingtheShapiro-Wilktestandforhomogeneityofvarianceusingthe
Levene’stest.TheonewayANOVAwithpost-hocBonferronicorrectionwasthen
usedforBWatendpoint,serumtotalcholesterolandboneparametersbecause
theseparameterswerenormallydistributedandhadhomogeneityof variance.

Statins and fibrates in the STROrt mouse model 105
6
Forotherserumparameters,foodintakeandhistologicaldata,theKruskal-Wallis
withpost-hocBonferronicorrectionwasused.The95%confidenceinterval(CI)
ofthedifferencebetweenconditionswhentheKruskal-Wallistestwasused,was
calculatedusingthebootstrapmethod.ToassesstherelationshipbetweenBWat
endpoint,serumtotalcholesterolandμCTdata,thePearson’scorrelationcoeffi-
cientwasusedbecausetheseparameterswerenormallydistributed.Forallother
associationanalyses,theSpearman’scorrelationcoefficientwasused.p<0.05was
consideredstatisticallysignificant.
RESULTS
Simvastatin treatment had no statistically significant effect on serum parameters or OA characteristics
Body weightAsexpected,themeanBWofthemiceinthecontrolgroupincreased
during the study, reaching ameanof 36.8 (± 3.2) gramsafter 16weeks (Figure
1). Inthesimvastatinonlytreatedgroups,BWatendpointdidnotstatistically
significantlydifferfromcontrol(95%CI:-3.4to4.0and-2.6to4.7forthedifference
betweencontroland40or100mg/kgBW/dayofsimvastatinrespectively).Food
intakewasnotstatisticallysignificantlyinfluencedbytheadditionofsimvastatin
tothefoodandthemicereceivedamedianof77%oftheintendeddosageofdrug
(Table1).
SerumNostatisticalsignificantdifferencewasobservedinserumtotalcholes-
terol(95%CI:-0.7to0.4and-0.6to0.6),serumtotaltriglyceride(95%CI:-2.4to
1.1and-1.0to1.6)andSAAlevels(95%CI:-286.4to680.1and-570.0to728.4)after
bothdosagesofsimvastatinonlytreatments(Figure2).Usingthemultiplexassay,
IL1α,MIP1αandIL10weredetectableintheserumandcomparedtocontrolmice,
thesewerenotstatisticallysignificantlydifferentaftersimvastatintreatment.
OA cartilage damage Microscopic evaluation demonstrated variability in
cartilage lossandtheamountofsubchondralboneinall thegroups(Figure3).
Cartilagedamagewasmostprofoundinthemedialcompartmentofthejoint.The
medianOARSIscoresinthesimvastatin100mg/kgBW/daytreatedgroupatthe
medialfemurandtibiawerelowerthantheuntreatedcontrolgroup,althoughthis
differencewasnotstatisticallysignificant(95%CI:-0.6to3.8formedialfemurand
-1.8 to4.6 formedial tibiaOARSIscore).Wecouldnotdetectastatisticallysig-
nificantreductionofsynovialhyperplasiainthemiceaftersimvastatintreatment
comparedtocontrols(95%CI:-0.7to1.0and-0.7to1.0forthedifferencebetween
controland40or100mg/kgBW/dayofsimvastatinrespectively;Figure3).

106 CHAPTER 6
Figure 1 Effectoftreatmentonbodyweightandserummetabolicmarkers.T=0weeksrepresentstartofexperimentaltreatmentattheageof8weeks.Controlgroupreceivedreferencedietfor16weeks.Treatmentgroupsreceivedsimvastatinand/orfenofibratemixedintotheirdietfor16weeks.Indicateddosagesareintendeddrugintake/kgbodyweight/day.Combinationgroupreceivedsimvastatin40mgandfenofibrate80mg.A)Bodyweight,B)Serumtriglyceride,C)Serumtotalcholesterol.Valuesindicatemean+SD(n=11-12micepergroup).Horizontaldashedline:meanvalueofT=0.*p<0.01versusControlgroup.**p<0.001versusControlgroup
Table 1 Totalfoodintakeanddrugintakepermouse*
Treatment Group(Intended drug intake)
Average total food intake per mouse in grams**
P Value Actual drug intake per kg body weight per day in mg (% of intended drug intake)
Control 492.1±15.7
Simvastatin40mg 467.1±13.8 1.000 30.7±1.8(77)
Simvastatin100mg 460.2±4.2 0.265 76.2±2.6(76)
Fenofibrate80mg 557.5±18.8 0.009 74.5±2.0(93)
Fenofibrate200mg 524.9±8.6 0.265 189.3±5.5(95)
Combination 484.3±11.8 1.000 33.5±1.4(84)$67.0±2.8(84)#
*Treatmentgroupsreceivedsimvastatinand/orfenofibratemixedwiththeirdietfor16weeks.Indicateddosag-esareintendeddrugintake/kgbodyweight/day.Combinationgroupreceivedsimvastatin40mgandfenofibrate80mg.Dataaremean±SD;Kruskal-Wallistestwithpost-hocBonferonnicorrectionwasperformed;Pvaluesindicatethestatisticaldifferencebetweentreatmentandcontrolgroup;**Averagetotalfoodintakepermousefor16weeks$Simvastatin40mg#Fenofibrate80mg

Statins and fibrates in the STROrt mouse model 107
6
Figure 2 Effectofsimvastatinand/orfenofibrateonseruminflammatorymarkers.Controlgroupreceivedreferencediet.Treatmentgroupsreceivedsimvastatinand/orfenofibratemixedwiththeirdiet for16weeks. Indicateddosagesare intendeddrug intake/kgbodyweight/day.Combinationgroupreceivedsimvastatin40mgandfenofibrate80mg.A)SerumIL1α,B)SerumMIP1α,C)SerumIL10andD)SerumAmyloidAlevels.T=0:valuesbeforetreatmentattheageof8weeks.Horizontaldashedlineindicatesthemeanvalueatthestartoftreatment(T=0).Valuesindicatemean+SD(n=11-12micepergroup)
Twentyonepercentofthemicedevelopedpatellasubluxationandtheprevalence
ofsubluxationwasnotdifferentbetweengroups.Excludingthemicewithpatella
dislocationfromtheanalysesdidnotaltertheresults(Supplementarytable1).
μCT analysisBoththesubchondralbonevolume(95%CI:-0.1to0.1and-0.1to
0.2)andplatethickness(95%CI:-40.6to42.1and-24.3to60.2)didnotstatistically
significantlydifferbetweenmicetreatedwithsimvastatinandcontrolmice(Figure
4).

108 CHAPTER 6
Figure 3 Histologicalanalysisofeffectofsimvastatinand/orfenofibratetreatmentoncartilagedamageinSTR/Ortmice.Thecoronalsectionsofcartilageintheweight-bearingareaofthetibiofemoralcompartmentoftheleftkneewerestainedwiththionineandseverityofcartilagedamagewasscoredonascaleof0-6usingtheOARSIhis-tologicalscoringscale.Controlgroupreceivedreferencedietfor16weeks.Treatmentgroupsreceivedsimvas-tatinand/orfenofibratemixedwiththeirdietfor16weeks.Indicateddosagesareintendeddrugintake/kgbodyweight/day.Combinationgroupreceivedsimvastatin40mgandfenofibrate80mg.A)Representativepictureofscore0:normalcartilageB)Representativepictureofscore6:Verticalclefs/erosiontothecalcifiedcartilageextendingto>75%ofthesurface.Picturesaretakenat40xmagnification.C)QuantificationofOARSIscoresofthemedialfemur.D)QuantificationofOARSIscoresofthemedialtibia.E)Numberofcelllayersinthesynovialmembrane.Eachdotrepresentsanindividualmouse(n=11-12micepergroup)HorizontallineindicatesmedianvaluepergroupinCandD.Mean±SDisshowninE.

Statins and fibrates in the STROrt mouse model 109
6
Figure 4 Effectofsimvastatinand/orfenofibratetreatmentonsubchondralboneplatebonevol-umeandthicknessofthetibiaplateauinSTR/Ortmice.Control group receivedreferencedietfor16weeks.Treatmentgroupsreceivedsimvastatinand/orfenofibratemixedwiththeirdietfor16weeks.Indicateddosagesareintendeddrugintake/kgbodyweight/day.Combinationgroupreceivedsimvastatin40mgandfenofibrate80mg.A)Sub-chondralboneplatebonevolumeB)Subchondralboneplatethickness,Valuesindicatemean+SD(n=11-12micepergroup)
Fenofibrate treatment reduced body weight, SAA and subchondral bone
Body weightMicetreatedwith200mg/kgBW/dayfenofibratehadthelowestmean
BWatendpointcomparedtothecontrolgroup(p<0.001;Figure1).Allfenofibrate
treatedmiceatemorecomparedtothecontrolgroup,althoughonlythefenofi-
brate80mg/kgBW/daytreatedgroupatestatisticallysignificantlymore(Table1).
Nosignsofdiarrhoeawereobserved.Themicereceivedamedianof94%ofthe
intendeddrugdosage.
Serum markersWedidnotdetectastatisticallysignificanteffectoffenofibrate
treatmentonserumtotaltriglyceride(95%CI:-0.5to2.2and-0.8to2.0forthedif-
ferencebetweencontroland80or200mg/kgBW/dayoffenofibraterespectively)
andonserumtotalcholesterol(95%CI:-0.9to0.3and-0.8to0.4;Figure2).SAA
levels in fenofibrate treatedgroupsdidnotchangeafterstartof treatmentand
at end pointwere significantly lower than in the control group (95%CI: 9.5 to
828.0 and10.8 to 829).On themultiplex assayonly IL1α,MIP1α and IL10were
detectableintheserum(Figure2).IL1αandMIP1αlevelsweresignificantlyhigher
infenofibratetreatedmicethanincontrolmice.
OA cartilage damageWecouldnotdetectastatisticallysignificantreductionof
medialfemur(95%CI:-2.8to3.4and-3.5to2.6)andtibia(95%CI:-4.3to4.6and-3.4
to4.3)OARSIscoresandsynovialhyperplasia(95%CI:-1.7to1.8and-0.6to1.3)in
thefenofibratetreatedmicecomparedtocontrols(Figure3).
μCT analysisMicetreatedwith200mg/kgBW/dayfenofibratehadalowersub-
chondralbonevolumeandplatethicknessthanthecontrolgroupalthoughonly
thelowersubchondralbonevolumewasstatisticallysignificant(Figure4).

110 CHAPTER 6
Effects of combination treatment of simvastatin and fenofibrate
ThemeanBWofthemicetreatedwithacombinationofsimvastatinandfenofi-
brateattheendofthestudywaslowerthanthemeanBWinthecontrolgroup
(p=0.003,Figure1).Themicereceived84%oftheintendeddosagesimvastatinand
fenofibrate(Table1).
Only serum amyloid A was statistically significantly different between mice
treatedwithacombinationofsimvastatinandfenofibrateandcontrols(Figures
2,3and4)
Correlation between body weight, serum markers, cartilage damage, synovial hyperplasia and bone changes.
Bodyweight at end point correlatedwith serum total triglyceride (p<0.001), IL1α
(p<0.001)andMIP1α(p=0.001)andsubchondralbonevolume(p=0.01).Innoneofthe
treatmentgroups,seruminflammationmarkerscorrelatedstatisticallysignificantly
withOAcartilagedamage(Table2).SAAlevelsdidnotdifferbetweenmicewithand
without cartilage damage. SAA levels correlated to subchondral bone volume
(p=0.008) Bothsubchondralbonevolume(p=0.002),platethickness(p<0.001)and
synovialhyperplasia(p<0.001)correlatedwithcartilagedamage.(Table2)
Table 2 Correlationbetweenbodyweightserummarkers,OARSIcartilagescores,synovialhyper-plasiaandµCTdata.
Body Weight(end point)
OARSI Score Synovium cell layers
Subchondralbone plate volume
Subchondralbone plate volume
Total Femur Tibia
Body weight (endpoint)
0.14 0.04 0.19 0.32 0.31 0.22
Serum
Total cholesterol 0.09 0.07 0.02 0.05 0.04 -0.26 -0.23
Total triglyceride 0.45 0.12 0.10 0.10 0.28 0.03 0.04
AmyloidA 0.21 -0.01 -0.08 0.08 0.12 0.34 0.19
IL1α -0.52 -0.07 -0.09 -0.04 -0.09 -0.09 -0.13
MIP1α -0.44 -0.09 -0.13 -0.02 -0.05 -0.01 -0.06
IL10 0.11 -0.08 -0.14 0.03 -0.01 -0.01 -0.11
Synoviumcelllayers 0.33 0.62 0.32 0.42
Subchondral bone platevolume
0.31 0.37
Subchondral bone platethickness
0.22 0.49
Serummarkersweremeasuredatendpointafter16weeksoftreatment;OARSIscoresforthetotaljoint,bothfemurandtibialcompartments;Correlationsbetweenbodyweightatendpoint,serumtotalcholesterolandµCTdatawerecalculatedusingthePearsoncorrelationcoefficient;CorrelationsbetweenallotherparameterswerecalculatedusingtheSpearmancorrelationcoefficient;Significantcorrelations(p<0.05)areshowninbold.

Statins and fibrates in the STROrt mouse model 111
6
DISCUSSION
Inthisstudyweinvestigatedwhetherdrugsoftenusedtoreducethemorbidity
andmortality ofmetabolic syndrome and obesity could serve as a therapy to
preventortreatOA.Wedidnotfindastatisticallysignificantlyreductionofthe
severityofcartilagedamageinSTR/Ortmicewithneithersimvastatin,fenofibrate
northecombinationtreatment,althoughfenofibratetreatmentpreventedahigh
subchondralbonevolume.
TheSTR/Ortstrainwascarefullychosenforthisstudybecausethesemicehave
been described to develop OA and metabolic syndrome spontaneously at a
relativelyyoungage19,thusresemblingpatientswithmetabolicOA4.Sincestatins
andfibratesareusedtoimprovethemetabolicprofileofpatients,theuseofthis
strainseemedtomatchthesubgroupofmetabolicOApatientsthatcouldbenefit
fromtreatmentwiththesedrugs.Inadditiontohyperlipidemiaandobesity,other
possiblecausesforOApredispositionintheSTR/Ortstrainhavebeendiscussed,
suchastheroleofpatellasubluxation18;25.Whenpatellasubluxationoccurs,itis
amajorbiomechanicalriskfactoranddiseasemodifyingeffectsofsimvastatinor
fenofibratewouldbehighlyunlikely. Inourstudy,patellasubluxationoccurred
in 21% of the mice throughout all the groups. Although all mice with patella
subluxationhadextensivecartilagedamage,notallmicewithextensivecartilage
damagehadpatellasubluxation.Thissuggeststhatpatellasubluxationisnotthe
maincauseofOAinthesemiceandisnotlikelytomasktheeffectsofsimvastatin
orfenofibrate.
Inaprevioushumancohortstudywefoundthatstatinusewasassociatedwitha
lowerincidenceandreducedprogressionofkneeOAonx-rays15.Inanotherstudy
statinusewasassociatedwithlowerincidenceofclinicalOA16.Inthepresentstudy
withSTR/Ortmice,simvastatindidnotlowertheserumtotalcholesterollevel.This
couldbeexplainedbyadifferentcholesterolmetabolismpathwayinmicethanin
humans26-28.TheabsenceofastatisticallysignificanteffectofsimvastatinonOA
inourstudycouldindicatethatcholesterolandOAmightbelinkedtoeachother
andthatloweringcholesterolbystatinsisimportanttoreduceOAdevelopment.
Furthermore,differenttypesofstatinswereincludedinthehumanclinicalstudies.
Thesedifferenttypesofstatinshavebeendescribedtohavedifferenttherapeutic
effects29.Theserum levelsof totalcholesterol in thecontrolmice inourstudy
werecomparabletoapreviousstudy19.Serumcholesterolcanbeincreasedwitha
highfatdietinmiceanddecreasesaftertreatmentwithstatin30;31.Inaddition,we
havepreviouslyreportedthatstatintreatmentdecreasedthedevelopmentofOA

112 CHAPTER 6
inmiceonahighfatdiet32.Thissuggeststhattheeffectofstatintreatmentcould
alsodependonthetypeofdiet.However,thisconclusionshouldbedrawnwith
caution,becausethestudiesofFraulob31andGierman32usedrosuvastatinandthe
studyofParaskevast30atorvastatin,whereasweadministeredsimvastatin.Aswith
humans, thesedifferent typesof statinshavebeendescribed tohavedifferent
therapeuticeffectsinmice21.
Theresultofourstudythatsimvastatincouldnotstatisticallysignificantlyreduce
OAcartilagedamage is alsonot consistentwith aprevious studybyYudohet
al14,whoreportedastatisticallysignificantdecreaseinOAcartilagescoreinSTR/
Ort mice after 12 and 24 weeks of simvastatin (40 mg/kg BW/day) treatment.
Thisinconsistencycouldbeduetodifferencesinstrains:Yudohandcolleagues
usedSTR/OrtCrljmiceobtainedfromCharlesRiverJapanwhereasweusedSTR/
OrtOlaHsdmiceobtainedfromHarlan,Italy.Responsetosimvastatincouldhave
beendifferentbetweenthesetwopopulationsofmice.Furthermore,inthestudy
byYudohetal,thecartilagedamageintheuntreatedgroupattheageof24weeks
waslessseverethaninthecontrolgroupinourstudy.Thisindicatesthatsimvas-
tatinmightbemoreeffectiveinslowlydevelopingorlesssevereOA.Lastly,Yudoh
etaladministratedthedrugsbydailygavageinsteadofmixingitwiththefoodand
thereforeadifferenttherapeuticlevelmightbereachedinthemice.
Fenofibrateisanotherlipidloweringdrug,widelyusedtolowerserumlipidsin
patientswithhypertriglyceridemia.Serumtriglyceridewasnotloweredaftertreat-
mentwithfenofibrateinourstudy,butthetreatedmicegainedlessweight.BW
washowevermoderatelycorrelatedtoserumtriglyceridesuggestingthatweight
reductioncould reduceserum triglyceride.Controlmicecontinued togainBW
overtime,reachingameanweightof36.8±3.2gramsattheageof24weeks.This
is comparable toprevious studies19;33.The reduction inBWgainby fenofibrate
treatmenthowever,didnotprotectthemicefromdevelopingcartilagedamage.
ThisabsenceofcorrelationbetweenBWandincidenceofcartilagedamagecon-
firmsourearlierfindings32thatobesitydoesnotincreaseOAcartilagedamageby
biomechanicaloverloading.
Inourstudy,serumcholesterolandserumtriglyceridewerebothnotcorrelated
withcartilagedamage.ThissuggeststhatintheSTR/Ortmicelipidmetabolism
isnottheprimarycauseofspontaneousOAcartilagedamagedevelopment.Next
totheireffectonlipidmetabolism,statinsandfibratesareknowntohaveanef-
fectoninflammation8;9;11-13.SAA,amarkerforsystemicinflammation,increasedin
controlmicewithaging.SAAhasbeenassociatedwithinflammatoryprocessesin

Statins and fibrates in the STROrt mouse model 113
6
artherosclerosisandrheumatoidarthritis34-36,isincreasedinobesity37 and clinical
studieshaveshownthatSAAcanbeloweredbyfenofibrateandsimvastatintreat-
ment38-40. InthepresentstudywithSTR/Ortmice,SAAlevelswereonlylowered
after fenofibrate treatment. SAA is described to be induced by the cytokines
IL1β, IL6 andTNF-α and it canactivate theNF-ĸB pathway34;35;41.Kyostio-Moore
et al42 reportedelevated inflammatory cytokines in the serumof STR/Ortmice
includingIL1β,IL12p70andIL5,andthesechangeswerecorrelatedwithcartilage
damage.WewereabletodetectIL1α,MIP1αandIL10intheserumofthemice,
butothercytokineswerenotdetected.Surprisingly,IL1α,andMIP1αlevelswere
significantlyhigherinmicethatreceivedfenofibratetreatment.Thissuggeststhat
differentaspectsofinflammationmightoccurthatpossiblycounteracteachother.
Furthermore, we found no correlation between individual serum inflammatory
markersandsynovialhyperplasia,suggestingthatsystemicinflammationisnot
directlyrelatedtolocalinflammatorychangesinthekneeinourSTR/Ortmice
Fenofibrate lowers lipid levelsby activatingPPARα. It hasbeen suggested thatSTR/Ort mice have reduced endogenous PPARα signalling. This reduction ofPPARα signalling could be associated with increased osteogenic differentiation
andreducedadipogenicandchondrogenicdifferentiationofbonemarrowderived
mesenchymalstemcellsandthusbeassociatedwiththedevelopmentofOAin
thesemice20. Inour study,PPARα activationwith200mg/kgBW/day fenofibrate
did indeed reduce the total bone volume in the subchondral bone. We could
however, not detect a significant reduction of cartilage damage in our study.
ChangesincartilageandsubchondralboneduringOAdevelopmentarethought
to be correlated to each other43andwedidfindamoderatecorrelationbetween
cartilagedamageandsubchondralboneparameters.Theabsenceofastatistically
significantreductionofcartilagedamagemightbeduetothelimitedsensitivity
ofthehistologicalcartilagedamagescoringortothehighvariationinincidence
ofspontaneousOAcartilagedamageinthesemice.Inthepresentstudy,60%of
theanimalshaddevelopedOAcartilagedamageat24weeksofage,whichisless
thanthe80%reportedinotherstudiesthatweusedforourpowercalculation18.
Moreover, since we used a spontaneousmodel of OA development, individual
micedevelopedOAatadifferentspeed25whichmightexplainthelargevariation
incartilagedamageinthecontrolgroup.
Alternatively,itispossiblethatthemicetreatedwithfenofibrateareatadifferent
phaseinOAdevelopment.DuringOAdevelopmentinmice,abiphasicsubchon-
dralboneturnoverprocessistakingplace,withinitiallossofsubchondralbone,
followedbyincreasedvolumeandthickeningofthesubchondralboneplate23;44.

114 CHAPTER 6
Inthefenofibratetreatedmice,initialOAdevelopmentcouldhavebeendelayed
asdemonstratedbythelowersubchondralbonevolumewhereastheothermice
alreadyprogressedtoathickeningofthesubchondralplate.Furtherinvestigation
withtimeseriesisneededtoconfirmthishypothesis.
Possiblesideeffectsofstatinsandfenofibratesaremusclepainandelevatedliver
enzymes. Furthermore, toxicology studies performed onmice showed that ad-
ministrationofveryhighdosagesofsimvastatinorfenofibratefor72weekscould
possiblyinducelivercarcinomas45;46.Inourstudy,wedidnotanalysethelivers
ofourmiceatage20weeksforthepresenceoflivercarcinomas,sowecannot
excludethepresenceofthesetumours.Weincludedonegroupofmicethatwas
treatedwithacombinationofsimvastatinandfenofibrate.Thiscombinationhas
beenshowninclinicalstudiestobemoreeffectiveindecreasingcardiovasculair
mortality47, treating dyslipidemia48 and decreasing inflammation49 compared to
monotherapy.Becausethecombinationisdemonstratedtobemoreeffective47-49,
a lower dose of both drugs can be used and therefore less side effects will occur50.
Unfortunately,we did not see synergistic effects of the combination treatment
inourstudy.Simvastatinand fenofibratearebothmetabolised in the liverand
therebyloweringthelevelsthatarereachedlocallyinthekneeorsubchondral
bone.Methodstoincreasethelevelsofbothdrugslocally,suchasintra-articularly
orsubcutaneouslyinjectionsmightprovideoptionstoincreasethelocaleffects
andreducethesystemicsideeffects.
Insummary,wecouldnotdetectastatisticallysignificantlydecreaseofsimvas-
tatinorfenofibratetreatmentonthedevelopmentofcartilagedamagein6months
old STR/Ortmice.On theotherhand, the effect of fenofibrateon subchondral
bonemorphologyandthecorrelationbetweensubchondralbonemorphologyand
cartilagedamagesuggeststheremightbeamildeffectonOAdevelopmentthatis
maskedbytheinsensitivityofthecartilagescoreorthehighvariationincartilage
damageinmiceof6monthsold.Furthermore,ourdatasuggestthatbiomechani-
calchangesduetooverweightorpatellasubluxationandspontaneousmetabolic
changesarenottheprimarycauseofOAintheSTR/Ortmouse.Complexinflam-
matoryprocessesoccurinthesemicethatdidnotaffectthecartilagedirectly.
Nonetheless,wedonotexcludethatlipidloweringdrugscanstillbebeneficialin
othersubtypesofOAsuchashighfatdietinducedmetabolicOAasindicatedby
ourpreviousstudies.ThisemphasizestheimportanceoffurthersubtypingOAto
findpossibilitiesforpharmacologicaltreatmentofOA.

Statins and fibrates in the STROrt mouse model 115
6
REFERENCES
1. BijlsmaJW,BerenbaumF,LafeberFP.2011.Osteoarthritis:anupdatewithrelevance forclinical
practice.Lancet377:2115-2126.
2. Aspden RM, Scheven BA, Hutchison JD. 2001. Osteoarthritis as a systemic disorder including
stromalcelldifferentiationandlipidmetabolism.Lancet357:1118-1120.
3. OliveriaSA,FelsonDT,ReedJI,etal.1995.Incidenceofsymptomatichand,hip,andkneeosteoar-
thritisamongpatientsinahealthmaintenanceorganization.ArthritisRheum38:1134-1141.
4. ZhuoQ,YangW,ChenJ,etal.2012.Metabolicsyndromemeetsosteoarthritis.NatRevRheumatol
8:729-737.
5. HoevenTA,KavousiM,ClockaertsS,etal.2012.Associationofatherosclerosiswithpresenceand
progressionofosteoarthritis:theRotterdamStudy.AnnalsoftheRheumaticDiseases.
6. DevarajS,ChanE,JialalI.2006.Directdemonstrationofanantiinflammatoryeffectofsimvastatin
insubjectswiththemetabolicsyndrome.JClinEndocrinolMetab91:4489-4496.
7. AbeM,MatsudaM,KobayashiH, et al. 2008. Effectsof statinson adipose tissue inflammation:
theirinhibitoryeffectonMyD88-independentIRF3/IFN-betapathwayinmacrophages.Arterioscler
ThrombVascBiol28:871-877.
8. BakerJ,WalshP,ByrneD,etal.Pravastatinsuppressesmatrixmetalloproteinaseexpressionand
activityinhumanarticularchondrocytesstimulatedbyinterleukin-1β.JournalofOrthopaedicsand
Traumatology:1-5.
9. Clockaerts S, Bastiaansen-JenniskensYM, Feijt C, et al. 2011. Peroxisomeproliferator activated
receptor alpha activation decreases inflammatory and destructive responses in osteoarthritic
cartilage.OsteoarthritisCartilage19:895-902.
10. ClockaertsS,Bierma-ZeinstraSM.2011.Commenton:Statinsandthe joint:multipletarget fora
globalprotection?SeminArthritisRheum40:588.
11. DombrechtEJ,VanOffelJF,BridtsCH,etal.2007.Influenceofsimvastatinontheproductionofpro-
inflammatorycytokinesandnitricoxidebyactivatedhumanchondrocytes.ClinExpRheumatol
25:534-539.
12. LazzeriniPE,CapecchiPL,NerucciF,etal.2004.SimvastatinreducesMMP-3level in interleukin
1betastimulatedhumanchondrocyteculture.AnnRheumDis63:867-869.
13. LazzeriniPE,LorenziniS,SelviE,etal.2007.Simvastatininhibitscytokineproductionandnuclear
factor-kB activation in interleukin 1beta-stimulated synoviocytes from rheumatoid arthritis pa-
tients.ClinExpRheumatol25:696-700.
14. YudohK,KarasawaR.2010.Statinpreventschondrocyteaginganddegenerationofarticularcarti-
lageinosteoarthritis(OA).Aging(AlbanyNY)2:990-998.
15. ClockaertsS,VanOschGJ,Bastiaansen-JenniskensYM,etal.2012.Statinuse isassociatedwith
reducedincidenceandprogressionofkneeosteoarthritisintheRotterdamstudy.AnnRheumDis
71:642-647.
16. KadamUT, BlagojevicM, Belcher J. 2013. Statin Use and Clinical Osteoarthritis in the General
Population:ALongitudinalStudy.JGenInternMed.
17. vanEekerenIC,ClockaertsS,Bastiaansen-JenniskensYM,etal.2013.Fibratesastherapyforosteo-
arthritisandrheumatoidarthritis?Asystematicreview.TherAdvMusculoskeletDis5:33-44.
18. MasonRM,ChambersMG,FlannellyJ,etal.2001.TheSTR/ortmouseanditsuseasamodelof
osteoarthritis.OsteoarthritisandCartilage9:85-91.
19. UchidaK,UrabeK,NaruseK,etal.2009.Hyperlipidemiaandhyperinsulinemiainthespontaneous
osteoarthritismousemodel,STR/Ort.ExpAnim58:181-187.

116 CHAPTER 6
20. WattersJW,ChengC,PickarskiM,etal.2007.Inverserelationshipbetweenmatrixremodelingand
lipidmetabolismduringosteoarthritisprogressionintheSTR/Ortmouse.ArthritisRheum56:2999-
3009.
21. ZadelaarS,KleemannR,VerschurenL,etal.2007.Mousemodelsforatherosclerosisandpharma-
ceuticalmodifiers.ArteriosclerThrombVascBiol27:1706-1721.
22. Waarsing JH,Day JS,WeinansH. 2004. An improved segmentationmethod for in vivomicroCT
imaging.JBoneMinerRes19:1640-1650.
23. Botter SM, van Osch GJ, Clockaerts S, et al. 2011. Osteoarthritis induction leads to early and
temporalsubchondralplateporosityinthetibialplateauofmice:aninvivomicrofocalcomputed
tomographystudy.ArthritisRheum63:2690-2699.
24. GlassonSS,ChambersMG,VanDenBergWB,etal.2010.TheOARSIhistopathologyinitiative-rec-
ommendationsforhistologicalassessmentsofosteoarthritisinthemouse.OsteoarthritisCartilage
18Suppl3:S17-23.
25. NaruseK,UrabeK,JiangSX,etal.2009.OsteoarthriticchangesofthepatellofemoraljointinSTR/
OrtCrljmicearetheearliestdetectablechangesandmaybecausedbyinternaltibialtorsion.Con-
nectTissueRes50:243-255.
26. KleemannR,PrincenHM,EmeisJJ,etal.2003.Rosuvastatinreducesatherosclerosisdevelopment
beyond and independent of its plasma cholesterol-lowering effect inAPOE*3-Leiden transgenic
mice:evidenceforantiinflammatoryeffectsofrosuvastatin.Circulation108:1368-1374.
27. SparrowCP,BurtonCA,HernandezM,etal.2001.Simvastatinhasanti-inflammatoryandantiath-
eroscleroticactivitiesindependentofplasmacholesterollowering.ArteriosclerThrombVascBiol
21:115-121.
28. EndoA,TsujitaY,KurodaM,etal.1979.EffectsofML-236Boncholesterolmetabolisminmiceand
rats:lackofhypocholesterolemicactivityinnormalanimals.BiochimBiophysActa575:266-276.
29. WengTC,YangYH,LinSJ,etal.2010.Asystematicreviewandmeta-analysisonthetherapeutic
equivalenceofstatins.JClinPharmTher35:139-151.
30. ParaskevasKI,PantopoulouA,VlachosIS,etal.2011.Comparisonoffibrate,ezetimibe,low-and
high-dosestatintherapyforthedyslipidemiaofthemetabolicsyndromeinamousemodel.Angiol-
ogy62:144-154.
31. Fraulob JC, Souza-Mello V, Aguila MB, et al. 2012. Beneficial effects of rosuvastatin on insulin
resistance,adiposity,inflammatorymarkersandnon-alcoholicfattyliverdiseaseinmicefedona
high-fatdiet.ClinSci(Lond)123:259-270.
32. GiermanLM,vanderHamF,KoudijsA,etal.2012.Metabolicstress-inducedinflammationplaysa
majorroleinthedevelopmentofosteoarthritisinmice.ArthritisRheum64:1172-1181.
33. SokoloffL,MickelsenO,SilversteinE,etal.1960.Experimentalobesityandosteoarthritis.AmJ
Physiol198:765-770.
34. OkamotoH,KatagiriY,KiireA, et al. 2008. SerumamyloidAactivatesnuclear factor-kappaB in
rheumatoidsynovialfibroblaststhroughbindingtoreceptorofadvancedglycationend-products.
JRheumatol35:752-756.
35. McNiffPA,StewartC,SullivanJ,etal.1995.Synovialfluidfromrheumatoidarthritispatientscon-
tainssufficientlevelsof IL-1betaandIL-6topromoteproductionofserumamyloidAbyHep3B
cells.Cytokine7:209-219.
36. KingVL,ThompsonJ,TannockLR.2011.SerumamyloidAinatherosclerosis.CurrOpinLipidol
22:302-307.
37. TrayhurnP,Wood IS. 2004. Adipokines: inflammation and the pleiotropic role ofwhite adipose
tissue.BrJNutr92:347-355.

Statins and fibrates in the STROrt mouse model 117
6
38. GervoisP,KleemannR,PilonA,etal.2004.GlobalSuppressionof IL-6-inducedAcutePhaseRe-
sponseGeneExpressionafterChronicinVivoTreatmentwiththePeroxisomeProliferator-activated
Receptor-αActivatorFenofibrate.JournalofBiologicalChemistry279:16154-16160.
39. HoriuchiY,HirayamaS,SodaS,etal.2010.Statintherapyreducesinflammatorymarkersinhyper-
cholesterolemicpatientswithhighbaselinelevels.JAtherosclerThromb17:722-729.
40. HuY,TongG,XuW,etal.2009.Anti-inflammatoryeffectsofsimvastatinonadipokinesintype2
diabeticpatientswithcarotidatherosclerosis.DiabVascDisRes6:262-268.
41. RamadoriG,VanDammeJ,RiederH,etal.1988.Interleukin6,thethirdmediatorofacute-phase
reaction,modulateshepaticproteinsynthesisinhumanandmouse.Comparisonwithinterleukin1
betaandtumornecrosisfactor-alpha.EurJImmunol18:1259-1264.
42. Kyostio-MooreS,NambiarB,HuttoE,etal.2011.STR/ortmice,amodel forspontaneousosteo-
arthritis, exhibit elevated levels of both local and systemic inflammatorymarkers. CompMed
61:346-355.
43. MahjoubM,BerenbaumF,HouardX.2012.Whysubchondralboneinosteoarthritis?Theimpor-
tanceofthecartilageboneinterfaceinosteoarthritis.OsteoporosInt23Suppl8:841-846.
44. BotterSM,GlassonSS,HopkinsB,etal.2009.ADAMTS5-/-micehavelesssubchondralbonechanges
afterinductionofosteoarthritisthroughsurgicalinstability:implicationsforalinkbetweencarti-
lageandsubchondralbonechanges.OsteoarthritisCartilage17:636-645.
45. Drugs.com.2013.FenofibrateOfficialFDAinformation,sideeffectsanduses,fromDrugs.com.
46. Drugs.com.2013.SimvastatinorallydisintegratingtabletOfficialFDAinformation,sideeffectsand
uses,fromDrugs.com.
47. TenenbaumA,MedvedofskyD,FismanEZ,etal.2012.Cardiovasculareventsinpatientsreceived
combinedfibrate/statin treatmentversusstatinmonotherapy:AcuteCoronarySyndrome Israeli
Surveysdata.PLoSOne7:e35298.
48. DerosaG,MaffioliP,SalvadeoSA,etal.2009.Fenofibrate,simvastatinandtheircombinationinthe
managementofdyslipidaemiaintype2diabeticpatients.CurrMedResOpin25:1973-1983.
49. WagnerAM,Sanchez-QuesadaJL,BenitezS,etal.2011.Effectofstatinandfibratetreatmenton
inflammationintype2diabetes.Arandomized,cross-overstudy.DiabetesResClinPract93:e25-28.
50. FranssenR,VergeerM,StroesES,etal.2009.Combinationstatin-fibratetherapy:safetyaspects.
DiabetesObesMetab11:89-94.


CHAPTER 7
High fat diet accelerates cartilage repair in
DBA/1 mice
Wu Wei Yvonne M. Bastiaansen-Jenniskens
Mathijs Suijkerbuijk Nicole KopsPieter K. Bos
Jan A.N. Verhaar Anne-Marie Zuurmond
Francesco Dell’AccioGerjo J.V.M. van Osch
J Orthop Res. 2017 Jun;35(6):1258-64.

120 CHAPTER 7
ABSTRACT
Obesity isawell-knownrisk factor forosteoarthritis,but it isunknownwhat it
doesoncartilagerepair.Hereweinvestigatedwhetherahighfatdiet(HFD)influ-
encescartilagerepairinamousemodelofcartilagerepair. WefedDBA/1mice
controlorHFD(60%energyfromfat).Aftertwoweeks,afullthicknesscartilage
defectwasmadeinthetrochleargroove.Miceweresacrificed,1,8and24weeks
after operation. Cartilage repair was evaluated on histology. Serum glucose,
insulinandamyloidAweremeasured24hbeforeoperationandatendpoints.Im-
munohistochemicalstainingwasperformedonsynoviumandadiposetissueto
evaluatemacrophageinfiltrationandphenotype.Oneweekafteroperation,mice
onHFDhaddefect fillingwith fibroblast-like cells andmore cartilage repair as
indicatedbyalowerPinedascore.After8weeks,miceonaHFDstillhadalower
Pinedascore.After24weeks,nomicehadcompletecartilagerepairandwedid
notdetectasignificantdifferenceincartilagerepairbetweendiets.Bodyweight
wasincreasedbyHFD,whereasserumglucose,amyloidAandinsulinwerenotin-
fluenced.Macrophageinfiltrationandphenotypeinadiposetissueandsynovium
werenot influencedbyHFD. Incontrast tocommonwisdom,HFDaccelerated
intrinsiccartilagerepairinDBA/1miceontheshortterm.ResistancetoHFDin-
ducedinflammatoryandmetabolicchangescouldbeassociatedwithaccelerated
cartilagerepair.

High fat diet accelerates cartilage repair 121
7
INTRODUCTION
Traumatic articular cartilage injury, a common pathology of the knee1, results
inconsiderablemorbidityanddisabilitiesandcouldeventuallyleadtoosteoar-
thrithis (OA).Articularcartilagehas lowself-repaircapabilities2andthemicro-
fractureprocedure isused to induce intrinsiccartilage repairbymesenchymal
stemcells(MSCs)3Themicrofractureprocedureleadstosignificantsymptomatic
improvements inmostpatients4;5Theclinical improvementsarereportedtobe
less in patients with obesity6andthesepatientsarenowoftenexcludedfromtreat-
ments7.However,thereisnoinformationaboutthestructureofthenewlyformed
cartilageormechanismsexplainingtherelationshipbetweenobesityandworse
clinicaloutcome.
ObesityisamajorhealthproblemintheWesternsocietyandthenumberofpersons
withobesityisincreasing.Obesitycouldleadtosystemicmetabolicandinflamma-
torychangessuchashyperglycemia,hyperinsulinemia,increasedserumamyloid
Aandinfiltrationofadiposetissuebypro-inflammatorymacrophages8.Obesityis
awell-knownmajorriskfactorforthedevelopmentofOA9.Furthermore,obesity
exaggeratedpost-traumaticarthritis10andrheumatoidarthritis11 and could lead
toimpairedwoundhealingafteranoperation12.However,itisunknownwhatthe
preciseeffectisofobesityonintrinsiccartilagedefectrepair.
Tooptimizecartilagerepairtreatmentresultsinobesepatients,itisthereforees-
sentialtoinvestigatewhetherandhowobesitynegativelyinfluencescartilagere-
pair.Toanswerthisquestion,weperformedanin-vivomousestudytoinvestigate
thedirecteffectofobesityonintrinsiccartilagerepair.Inourstudy,ahighfatdiet
(HFD)wasusedtoincreaseweightandmimichumanobesityinmice13.HFDhas
beenshowntoincreaseweightandtobedetrimentaltocartilageandcauseOA
intheC57/BL6strainofmice12;14.Furthermore,HFDdecreasesthechondrogenic
differentiationpotentialofMSCsfromC57/BL6mice15
OurhypothesiswasthatHFDwouldnegativelyinfluenceintrinsiccartilagerepair.
SinceC57/BL6micehadbeenshownnottopossessintrinsicrepaircapabilitiesof
cartilage defects16,theywereunsuitableforourstudy.Therefore,weusedmale
DBA/1micewhichpossesscapabilitiestorepairafullthicknesscartilagedefect16
andgainweightonaHFD17.Thisstrainofmiceisthereforesuitabletostudythe
possiblenegativeeffectsofaHFDoncartilagerepair.

122 CHAPTER 7
METHOD
Animals and diet
Eight-weeks-old male DBA/1OlaHsd mice were acquired from Harlan UK and
maintainedattheanimaltestingfacilitiesoftheErasmusMCUniversityMedical
Center,TheNetherlands.Micewerehousedingroupsofthreeorfourmiceper
cageunder12hourslight-darkcycleandhadaccesstowaterandfoodadlibitum.
ThestudyprotocolwasapprovedbytheinstitutionalAnimalCareandUseCom-
mittee(ErasmusMCUniversityMedicalCenter,TheNetherlands,AEC116-12-05).
Micewereallowedtoacclimatize,werefedregularchowfortwoweeksandwere
allocatedrandomlytothedietgroups.Attheageof10weeks,micewerefedwith
aHFD(D12492;ResearchDiets,60%kcalfromfat)orcontroldiet(D12450B;Re-
searchDiets,10%kcalfromfat).Bothdietscontained4057kcalperkilogramdry
weight.Micewereweightedeverytwoweeksandthemicecontinuedtoreceive
theirrespectivedietsuntiltheywerekilled.
Operative procedure
Attheageof12weeksmicewereanesthetizedwithanisoflurane/O2mixtureand
afullthicknesscartilagedefectwascreatedaspreviousdescribed16.Thelefthind
legwasshavedanddisinfectedusingalcohol.Anincisionusinganr11microsur-
gicalscalpelwasmademediallyandproximally fromthe insertionof thepatel-
lar tendonon the tibia towards the attachmentof thequadricepsmuscle.The
jointcapsulewasopenedwithasmallincisionandthejointwasfullyextended
todislocatethepatella laterally.Theknee jointwasthen fullyflexedtoexpose
thetrochleargroovearticularsurface.Afullthicknesscartilagedefectwasthen
madeusinga25Gneedlebyscratchingthearticularsurface.Thejointwasflushed
withsalineandclosedusing6-0Vicryl(Ethicon).Theskinwasclosedusing6-0
Ethilon (Ethicon). Themice were given one dose of analgesic subcutaneously
preoperatively(Temgesic,0.05mg/kg).Micewereallowedtomovefreelypostop-
erationandtobefullweightbearing.Miceweresacrificed1,8and24weeksafter
operationwithaheartpunctureunderisoflurane/O2anesthesia.Allmicereached
end-pointwithoutdisease.34%oftheoperatedmicehadapatelladislocationand
wereexcludedfromtheanalysis.Thesemicewereequallydistributedoverboth
groups:patelladislocation ratewas35% for thecontrolgroupand32% for the
HFD fed group.We continued to operatemice until therewere at least 5mice
pergroup.Thetimepointsandminimumnumberofmicepergroupneededwere
basedonpreviousstudybyEltawiletal16.Thefinalnumberofmiceonacontrol
dietincludedforanalysiswas8miceat1week,9miceat8weeksand6miceat24

High fat diet accelerates cartilage repair 123
7
weeks.ForthemiceonaHFD,thenumberofmiceincludedwas6miceat1week,
9miceat8weeksand6miceat24weeks.
Serum collection and analysis
Bloodwascollectedthroughacheekpunctureonedaybeforetheoperationand
throughaheartpunctureatendpoints.Wecollectedthreedropsofbloodduring
thecheekpunctureand1mlofbloodthroughtheheartpuncture.Therewasno
noticeabledifferenceinbleedingtendencybetweenanimals.Micewerefastedfor
4hoursbeforebloodcollection.Bloodwasstoredfor1houratroomtemperature,
followedby30minutesat4°C,thencentrifugedfor5minutesat250g.Serumwas
removedandimmediatelystoredat-80°C.Serumglucosewasdeterminedusinga
bloodglucosemeter(FreeStyleFreedomLite,AbbottLaboratories).Seruminsulin
(Alpco,#80-INSMS-E01)andserumamyloidA(SAA,Alpco,#41-SAAMS-E01)were
determinedbyEnzyme-Linked ImmunoSorbentAssay(ELISA)according to the
manufacturer’sinstructions.
Tissue preparation for histological analysis
Theskinofbothhindlegsofallanimalswasopened.Thepatellawithsurrounding
synoviumwasremoved,placedinTissueTek®(SakuraFinetek,theNetherlands)
andsnapfrozeninliquidnitrogen.6µmthickcryosectionsweremadeofthepa-
tellawithsurroundingsynovium.Subcutaneousadiposetissueof5miceperdiet
attimepoint8weeksaftertheoperationwerefixedin4%bufferedformalinfor1
hour,embeddedinparaffinand6µmthickparaffinsectionsweremade.Theknees
ofallanimalswereexcisedandfixedin4%bufferedformalinfor7days,decalcified
in10%formicacidindistilledwaterfor7daysandembeddedinparaffin.6µm
thickparaffinsectionsweremadeofthekneesasdescribedbyEltawiletal16.
Evaluation of cartilage repair
Paraffin sections were stained with thionin or immunohistochemically stained
withamonoclonal antibodyagainst collagen type2. For immunohistochemical
staining, collagen type 2 antibody (DSHB, # II-II 6B3) or IgG1 isotype control
(DakoCytomation#X0931)werefirstpre-coupledwithbiotin-SPF(ab)2(Jackson,
#115-066-062).Sectionswerethenincubatedwiththecoupledantibodycomplex,
followedbyLabel(Biogenex,HK-321-UK)andfreshlypreparednew-fuchsinwas
usedassubstrate.PicturesweretakenusinganOlympusSC30camera.Thesize
ofthedefectandpercentageofdefectfilledwasquantifiedusingImageJsoftware
(National Institutes ofHealth, Bethesda,MD,USA). The number of cells in the
defectwasdeterminedinImageJandexpressedasper100µm2.Cartilagerepair
wasassessedusingthescoringsystemdevisedbyPinedaetal18,inwhichfilling,

124 CHAPTER 7
reconstruction of osteochondral junction,matrix staining and cellmorphology
were taken into account.ThePineda scoring systemhasa rangeof 0 to 14, in
which0meanscompleterepairand14norepairatall.Osteoarthriticdamagein
thecartilagesurroundingthedefectwasassessedusingamodifiedMankinscor-
ingsystem19.Bothscoringsystemswereperformedbytwoindependentobserv-
ers(WWandMS)whilebeingblindedtothegroupassignment.Themeanscore
of threedifferent slideswasdeterminedand in caseof a >1 scorediscrepancy
betweenthetwoobservers,rescoringwasperformedtogetherbythetwoobserv-
ers.
Evaluation of local and systemic inflammation
Cryosectionofthepatellawithsurroundingsynoviumwerefixedinacetoneand
stainedwith hematoxylin and eosin (H&E). For immunohistochemical staining,
sectionswere incubatedwithmonoclonal antibody against F4/80 (eBioscience,
#14-4801),polyclonalantibodiesagainst iNOS (Abcam,#15323)andCD206 (Ab-
cam,#64693).RatIgG2aantibody(eBioscience,#14-4321-82)wereusedasisotype
controlforF4/80andrabbitIgGantibody(DakoCytomation#X0903)wereusedas
isotypecontrolforiNOSandCD206.Subsequently,F4/80sectionswereincubated
withbiotinylatedrabbit-anti-ratIgG(Vector,#BA-4000)andiNOsandCD206sec-
tionswere incubatedwithRabbit-Link(Biogenex,HK-326-UR).Allsectionswere
afterwards incubated with Label (BioGenex, HK-321-UK) and freshly prepared
new-fuchsinwasusedassubstrate.Acellwasconsideredpositivewhenstained
red.
Synovialinflammationwasevaluatedusingthehistologicalscoringsystemdevised
byKrennetal20.TodeterminewhetherHFDhadaneffectonsynovialmacrophage
phenotype,immunohistochemicallystainedsampleswererankedbasedontheir
relativenumberofpositivecellsinthreesectionspersamplebytwoindependent
observers (WWandMS).Scoringandrankingwereperformed foreachmarker
separatelyandtheaveragerankforeachsamplebetweenthetwoobserverswas
usedintheanalysis.
Paraffinsectionsofsubcutaneousadiposetissueweredeparafinized,treatedwith
proteinase k solution (Sigma-Aldrich) for antigen retrieval and followedby the
same immunohistochemicalstainingprocedure forF4/80asthesynovium.Two
independentobservers (WWandMS)counted thenumberofcrown likestruc-
turesperareaofrandom100adipocytesfor3sectionspersampleandtheaverage
numberbetweenthetwoobserverswasusedintheanalysis.

High fat diet accelerates cartilage repair 125
7
Statistical analysis
Statistical analysis was performed in IBM SPSS statistics 20 (IBM Corporation,
Armonk,NewYork,USA).TheShapiro-Wilktestwasusedtotestdatafornormality
andtheLevene’stestforhomogeneityofvariance.Histologicaldatawasanalyzed
usingtheMann-Whitney-Utest.Weight,serumdataanddefectfillingwerenormally
distributedandunlessotherwisestated,statisticaldifferencesbetweendietswere
determined using an unpaired T-test. Differences were considered statistically
significant when p<0.05.
RESULTS
High fat diet accelerates cartilage repair early after cartilage damage
Oneweekafterthecreationofthedefect,inmiceonaHFD,spindleshapedcells
hadpartiallyfilledthedefect(Figure1A).Ahigherpercentageofthedefectwas
filledinthemiceonaHFDthanoncontroldiet(Figure1AandD),althoughthis
Cartilage Repair
Control High fat Control High fat Control High fat0
2
4
6
8
10
12
14P = 0.01
Worst
Best
1 week 8 weeks
P < 0.05
24 weeks
Pine
da
Filling of defect
Control High fat Control High fat Control High fat0
20
40
60
80
100
120
1 week 8 weeks 24 weeks
%of
defe
ct
A B
D F
Control
High fat
Non-operatedknee
1 week afteroperation
8 weeks afteroperation
Collagentype 2
Control
High fat
Control
High fat
Non-operatedknee
24 weeks afteroperation
C
Cells in defect
Control High fat0
1
2
3
4
5
Cells
/100
µm2
P < 0.05
1 week
E
Figure 1 Highfatdietfeedingimprovescartilagerepair.10weeksoldmaleDBA/1micewerefedwithcontrolorhighfatdiet.After2weeksoffeeding,fullthicknesscartilagedefectswerecreated.A)Representativepicturesofthioninstainedknees;non-operated,1weeksand8weeksafterdefectcreation,B)immunohistologicalstainingwithantibodiesagainstcollagentype2,8weeksafterdefectcreation.Thisisthefromthesamekneeasthethioninstaining.Thereisanartifactshowninthestaining.C)Representativepicturesofthioninstainedknees;24weeksafterdefectcreationandcorrespondingnon-operatedknees,D)percentageofdefectfilled,E)numberofcells inthedefectper100µm2,F)cartilagerepairevaluatedusingthePinedascoringmethod.Valuesaremean±SD(n=6-9micepergroup).

126 CHAPTER 7
wasnotstatisticallysignificant(Figure1D;95%CI:63-91%versus38-77%;p=0.15).
After8weeks,almostallthemicehadfillingofthedefect(Figure1D),however
onlytheHFDfedmicehaddefectsfilledwithchondrocyte-likecellssurrounded
withpositivethioninandcollagentype2staining(Figure1AandB).Inaddition,
thenumberofcells in thedefectwashigher inHFD fedmicecompared to the
controlmice(Figure1E).Finally,thePinedascorewaslower1week(p=0.04)and8
weeks(p=0.01)afteroperationinmiceonaHFDcomparedtocontroldiet(Figure
1FandTable1).
Table 1 Highfatdietimprovescartilagerepair
Controldiet Highfatdiet
F R M C Total F R M C Total
1week 2.0(±1.1)
2.0(±0.0)
3.4(±0.7)
3.1(±0.9)
10.5(±1.4)
1.3(±0.5)
2.0(±0.0)
2.7(±0.8)
2.3(±0.5)
8.5 (±0.7)
8weeks 0.8(±0.8)
1.9(±0.3)
3.1(±0.3)
2.8(±0.4)
8.7(±1.3)
0.8(±1.3)
1.3(±0.7)
2.0 (±1.1)
2.1(±1.3)
5.3 (±3.0)
24weeks
0.8(±0.8)
1.2(±0.4)
1.9(±0.9)
2.1(±1.0)
6.0(±2.4)
0.8(±0.8)
1.8(0.4)
2.2(0.8)
2.2(0.8)
7.0(±2.0)
CartilagerepairevaluatedusingthePinedascoringmethod.ThedifferentcomponentsofthePinedascoringmethodareshowed.Lowerscorerepresentsbettercartilagerepairresults.F:Fillingofthedefect(-1-4),R:Re-constructionofosteochondraljunction(0-2),M:Matrixstaining(0-4)andC:Cellmorphology(0-4).Valuesaremean(±SD).Boldindicatesp<0.05versusControldiet.
High fat diet does not cause major systemic or local metabolic and inflammatory changes in DBA/1 mice
24hoursbefore theoperation,high fatdiet fedmicewereheavier (26.2grams
versus23.3grams;p=0.004)andhadhigherserumglucose(p=0.01)thanmicere-
ceivingacontroldiet(Figure2A-B).Seruminsulinandamyloidwerenotdifferent
betweenthetwogroups.EightweeksaftertheoperationthemiceonHFDwere
stillheavierandhadhigherfastingserumglucose,althoughtheglucoselevelwas
notdifferentfrom1weekafteroperation.(Figure2B).Seruminsulinandamyloid
AwerenotaffectedbyHFD(Figure2CandD).Asseenonhistology,HFDinduced
adipocytehypertrophy(Figure2E).Therewaslessthanonecrownlikestructure
(CLS)per100adipocytesandtherewasnosignificantdifferencebetweencontrol
andHFDfedmice.Finally,weinvestigatedwhetherHFDinfluencedlocalinflamma-
tioninthejointandspecificallythesynovium.Thesynoviumwasmoreinflamed1
weekaftertheoperationcomparedto8weeks(Figure3A-B).Therewasnodetect-
ablesynovialinflammationinthenon-operatedknees.Nostatisticallysignificant
effectoftheHFDonsynovitisandrankofF4/80,iNOSorCD206positivecellswas
detected(Figure3B-E).

High fat diet accelerates cartilage repair 127
7
Long term effects of high fat diet and cartilage damage in DBA/1 mice
LongtermfeedingwithHFDsignificantlyincreasedtheweightofthemice(Figure
2A,41.1gramsversus30.3grams;p=0.008),butdidnotinfluenceserummetabolic
and inflammatorymarkers(Figure2B-D).Asmall lossof thioninstainingof the
cartilage surrounding thedefect in theoperatedkneeswasvisible (Figure1C).
Therewashowevernomajorcartilagelossorstructuralchangesindicatingos-
teoarthritisafter24weeksintheoperatedknees,notevenincombinationwitha
HFD(Table2,Figure1C).Therewasnocartilagelossinthenon-operatedknees
(Figure1C,Table2)
Body weight
0 10 2020
30
40
50ControlHigh fat diet
24-2Weeks
Gra
ms
** *
* * * ** * * *
E
F4/80
Control High fat
A B
C D
Fasting serum glucose
0
5
10
15
20 ControlHigh fat diet
-2Weeks
mm
ol/L
*
0 1 8
*
24
**
Fasting serum insulin
0
2
4
6 ControlHigh fat diet
-2Weeks
mm
ol/L
0 1 8 24
Fasting serum amyloid A
40
50
60
70
80
90 ControlHigh fat diet
-2Weeks
mg/m
l
0 1 8 24
Figure 2 Highfatdietincreasesbodyweight,butdoesnotcausemajorsystemicmetabolicandinflammatorychangesinDBA/1mice.Micewerefastedfor4hourspriortoserumcollection.A)Bodyweightofthemice.FastingserumB)glucose,C)insulinandD)amyloidAat1,8and24weeksafteroperation.Timepoint0represents24hoursbeforeoperation.E)RepresentativepicturesofsubcutaneousadiposetissuestainedwithantibodiesagainstF4/80at8weeksaf-teroperation.Positivecellsareindicatedwitharrows.Barvaluesaremean±SD(n=6-9micepergroup).*p<0.01versuscontroldiet.**p<0.05versuscontroldiet.

128 CHAPTER 7
DISCUSSION
Obesity,amajorrisk factor for jointdiseases9,hasbeenreportedtonegatively
influence the clinical results of cartilage repair procedures6;21.Thepresentstudyis
toourknowledgethefirstonethatinvestigatedthedirecteffectofaHFDinduced
weight gain on intrinsic repair of cartilage defects in an experimental mouse
model for cartilage repair. In contrast toourhypothesis,miceonaHFDhada
betterPinedascorethanthemiceonacontroldiet.Thisdifferencewasalready
detectable1weekaftermakingthedefect,butbecamemoreobviousafter8weeks.
Wecouldnotdetectasignificantdifferenceincartilagerepairanymorebetween
thetwodietgroupsafter24weeks,suggestingthatHFDonlyacceleratedandnot
improvedcartilagerepair.
Synovitis
Control High fat Control High fat0
2
4
6
8
1 week 8 weeks
P<0.01
##
# #Scor
e
Nonoperated
F4/80
Control High fat Control High fat10
20
30
40
P<0.01
1 week 8 weeks
# #
# #
Rank
ing
Nonoperated
iNOS
Control High fat Control High fat10
20
30
40
1 week 8 weeks
P<0.05
# #
##
Rank
ing
Nonoperated
CD206
Control High fat Control High fat10
20
30
40
1 week 8 weeks
P<0.01
# #
# #
Rank
ing
Nonoperated
F4/80 iNOS CD206A H&E
1 weekafter
operation
8 weeksafter
operation
B C D E
Figure 3 Highfatdietdoesnotinfluenceoperationinducedsynovialinflammation.A)RepresentativepicturesofsynoviumwithimmunohistochemicalstainingwithantibodiesagainstF4/80,iNOSandCD206,1and8weeksafteroperation.B)SynovitisscoreandrankingscoreofpositivecellsforC)F4/80,D)iNOSandE)CD206.Barvaluesaremean±SD(n=6-9pergroup).#p<0.01versusnon-operatedknees
Table 2: Longtermeffectsofhighfatdietonosteoarthritisdevelopment.
Controldiet Highfatdiet P-Value
ModifiedMankinscore(non-operatedknee)
0(NoOA) 0(NoOA) 1.0
ModifiedMankinscore(operatedknee)
1.5(±0.5) 1.7(±0.5) 1.0
P-Value p<0.01 p<0.01
Osteoarthritisscores24weeksafteroperation.Valuesaremean(±SD)(n=6micepergroup)

High fat diet accelerates cartilage repair 129
7
PreviousreportsonHFDhaveallshowndetrimentaleffectsofanHFDoncartilage.
Wuetal12showedthatHFDreducedearwoundhealingandacceleratedthepro-
gressiontoOAafterdestabilizationofthemedialmeniscus.Loueretal10 showed
thatHFDacceleratedpost-traumaticarthritis.However,thesestudiesusedyoung
adultC57BL/6miceandthisstrainofmice,incontrasttoDBA/1mice,doesnot
possess cartilage repair capabilities16;22;23NexttoDBA/1mice,MRL/MpJmiceare
knowntopossesscartilagerepaircapabilities24;25.Interestingly,thesemicegained
weightand fatmass,butdidnotdevelop themajormetabolicchangesseen in
C57BL/6miceafterbeingfedaHFD17;26.Ourmicegainedweight,evenonlyafter2
weeksofHFDandcontinuedtoincreaseweightduringthe24weeksofthestudy,
butdidnotdevelopmajormetabolicchanges.Thissuggests that thedegreeof
metabolicresponsetoHFDandabilitytorepaircartilagedamagemightbeassoci-
ated.
Individualdifferences in response tobeingobeseare alsoknown inhumans.
Accumulationofmacrophagesincrownlikestructures(CLS)inobesesubjectsis
associatedwithhyperinsulinemiaand increasedsystemic inflammation27; 28 and
metabolicallyhealthyobesesubjectsdonothavetheseCLSintheiradiposetis-
sue.TheabsenceofCLSintheadiposetissueoftheDBA/1miceonaHFDagain
indicatesthattheDBA/1miceareresistanttoHFD-inducedmetabolicandinflam-
matorychanges.
PreviouslywehaveshownthatthelevelofinflammatoryresponsetoaHFDwas
associatedwiththedevelopmentofOA29.Aninitialhigherinflammatoryresponse
inCRP-C57BL/6micetoaHFDwithincreasedserumlevelsofhumanC-reactive
protein(hCRP)wascorrelatedtoOAdevelopment.Furthermore,rosiglitazone,a
peroxisomeproliferator-activatedreceptors(PPAR)γagonistwithanti-inflamma-
tory properties, decreasedHFD associated inflammation andOAdevelopment,
eventhoughitincreasedweightgaininthesemice.Inthepresentstudy,HFDdid
notinducesystemicandlocalinflammatorychangesinmaleDBA/1micebasedon
theserumamyloidAmeasurementsandimmunohistologicalstainingformacro-
phagesinthesynoviumandadiposetissue.Thesemicealsodidnotdevelopmore
OA,eveninthepresenceofacartilagedefect.Thisagainsuggeststhatsusceptibil-
itytodevelopinginflammatorychangesmightbeassociatedtothedevelopment
ofOA.However,thismayonlyaccountforHFDinducedinflammatorychanges,be-
causeinhibitionofspontaneousoccurringobesityrelatedinflammatorychanges
inSTR/OrtmicewithfenofibratesdidnotinhibitthedevelopmentofOA30.
ThemaleDBA/1miceonacontroldietinourstudyshowedcartilagerepairafter
8weeks,albeitnottothesamedegreeasdescribedbyEltawiletal16.Although

130 CHAPTER 7
themiceusedwereofthesameDBA/1OlaHsdstrainfromthesamecompany,we
havemadethedefectsattheageof12weeksinsteadof8weeks,asinthestudy
byEtawiletal.Intrinsiccartilagerepaircapabilitiesmighthavebeenreducedwith
increasingage,howeveryoungerDBA/1micewouldverylikelyhaveadaptedto
aHFDandnotgainedweight11.Thechoicetouse12weeksoldDBA/1micemight
maketranslationoftheresultsofourstudytoolderindividualsdifficult.However,
thecurrentmodelhaslimitedusnottouseoldermice.Finally,weusedD12450B
as the control diet as advisedby thedietmanufacturer (ResearchDiets).This
controldietcontains10%kcal fromfatand35%kcal fromsucrose.Eltawiletal
usedchowwhichhasloweramountofkcalfromsucrose.Wecannotexcludethat
thehighsucrosecouldhavereducedcartilagerepair.
Furthermore,cartilagerepaircouldbeinfluencedbyweightbearingactivities
after surgery31.AlthoughithasbeenshownthatHFDdoesnotinfluenceactivity
levelinC57BL/6mice,wecannotexcludethatHFDcouldhaveinfluencedactivity
levelofthemiceinourstudy12.
Although HFD had no effect on inflammation, it slightly increased the serum
glucosebeforecreationofthedefectandserumglucoselevelsremainedhigher
8weeksafterthedefectwasmade.Thishigherglucoselevelmayhaveimproved
theinitialcartilagerepairprocessaftercartilagedamage,becausedifferentiation
to chondrocytes and synthesis of extracellularmatrix requires a large amount
of nutrients.An abundanceof nutrientsmight alsohave increased the activity
ofmammaliantargetofrapamycin(mTOR),whichisknowntosupportskeletal
growthandextracellularmatrixproduction32.
However,ahighermTORexpressionincartilageisalsocorrelatedtocartilage
damage and mTOR inhibition by rapamycin could prevent post-traumatic OA
development33. IncreasedmTOR expression could have played a role in initial
cartilagerepairinDBA/1mice,butinthelongtermmTORmighthavebeensup-
pressedtoincreaseautophagyandprotectthecartilage.
Nexttohyperglycemia,aHFDcanleadtohypercholesterolemia.Recentlyithas
beenshown thatcholesterolmetabolismandcartilagedevelopmentandrepair
couldberelated.Statinsareusedtoreduceserumcholesterolthroughinhibition
oftheenzymeHMG-CoAandstatinscouldbeapotentialtherapyfordevelopmen-
taldiseasessuchasachondroplasiaandmightstimulatechondrogenicpotential
ofintervertebraldisccells.34;35However,itisknownthataHFDdoesnotincrease
serumtotalcholesterolinmaleDBA/1mice17.ItcouldbethattheenzymeHMG-
CoAoranotherenzymeinthemevalonatepathwayislessactiveinDBA/1mice
andthatthiscouldberelatedtoincreasedcartilagerepairinthismousestrain.

High fat diet accelerates cartilage repair 131
7
Besides serum metabolic changes, cartilage repair could also be directly
influencedbythefatcontentofHFD.HFDcontainsmainlysaturatedandmono-
unsaturatedfattyacidswhichreduces,ratherthanstimulates,thechondrogenic
potentialofMSCsfromC57BL/6mice15.However,MSCsisolatedfromDBA/1mice
havebeenreportedtohaveabetterchondrogenicpotentialthanthoseisolated
fromC57BL/6mice36.TheeffectofHFDonMSCchondrogenesiscouldthereforebe
differentindifferentstrainofmice.
Inconclusion,ourstudyshowsthatHFDandincreasedbodyweightintheDBA/1
mice do not negatively impair cartilage repair, but can even accelerate it. The
precisemechanisminhowHFDinfluencescartilagerepairinDBA/1isunknown.
However, our data suggests that resistance to HFD induced inflammatory and
metabolic changes could be associated with accelerated cartilage repair and
reducedOAsusceptibility.Furtherresearchisnecessarytoelucidatethecomplex
relationshipsbetweenahighfatdiet,metabolicandinflammatorychanges,carti-
lagedegenerationandregeneration.Fortheclinicalpractice,ourstudysuggests
thatnotallobesepatientsshouldbeexcluded fromtreatment. Investigationof
theirmetabolicandinflammatorystatecouldbehelpfulinmakingthedecisionto
startcartilagerepairtreatments.

132 CHAPTER 7
REFERENCES
1. WiduchowskiW,WiduchowskiJ,TrzaskaT.2007.Articularcartilagedefects:studyof25,124knee
arthroscopies.Knee14:177-182.
2. NewmanAP.1998.Articularcartilagerepair.AmJSportsMed26:309-324.
3. ShapiroF,KoideS,GlimcherMJ.1993.Celloriginanddifferentiationintherepairoffull-thickness
defectsofarticularcartilage.JBoneJointSurgAm75:532-553.
4. MithoeferK,McAdamsT,WilliamsRJ,etal.2009.Clinicalefficacyofthemicrofracturetechnique
forarticularcartilagerepairintheknee:anevidence-basedsystematicanalysis.AmJSportsMed
37:2053-2063.
5. NegrinL,Kutscha-LissbergF,GartlehnerG,etal.2012.Clinicaloutcomeaftermicrofractureofthe
knee:ameta-analysisofbefore/after-dataofcontrolledstudies.IntOrthop36:43-50.
6. MithoeferK,WilliamsRJ,3rd,WarrenRF,etal.2005.Themicrofracturetechniqueforthetreatment
ofarticularcartilagelesionsintheknee.Aprospectivecohortstudy.JBoneJointSurgAm87:1911-
1920.
7. GomollAH,FarrJ,GilloglySD,etal.2010.Surgicalmanagementofarticularcartilagedefectsofthe
knee.JBoneJointSurgAm92:2470-2490.
8. LumengCN, SaltielAR. 2011. Inflammatory linksbetweenobesity andmetabolicdisease. JClin
Invest121:2111-2117.
9. ZhuoQ,YangW,ChenJ,etal.2012.Metabolicsyndromemeetsosteoarthritis.NatRevRheumatol
8:729-737.
10. Louer CR, Furman BD, Huebner JL, et al. 2012. Diet-induced obesity significantly increases the
severityofposttraumaticarthritisinmice.ArthritisRheum64:3220-3230.
11. HamaguchiK,ItabashiA,KuroeY,etal.2012.Analysisofadiposetissuesandstromalvascularcells
inamurinearthritismodel.Metabolism61:1687-1695.
12. WuCL,JainD,McNeillJN,etal.2014.Dietaryfattyacidcontentregulateswoundrepairandthe
pathogenesisofosteoarthritisfollowingjointinjury.AnnRheumDis.
13. BuettnerR,ScholmerichJ,BollheimerLC.2007.High-fatdiets:modelingthemetabolicdisordersof
humanobesityinrodents.Obesity(SilverSpring)15:798-808.
14. GriffinTM,HuebnerJL,KrausVB,etal.2012.Inductionofosteoarthritisandmetabolicinflamma-
tionbyaveryhigh-fatdietinmice:effectsofshort-termexercise.ArthritisRheum64:443-453.
15. WuCL,DiekmanBO,JainD,etal.2013.Diet-inducedobesityaltersthedifferentiationpotentialof
stemcellsisolatedfrombonemarrow,adiposetissueandinfrapatellarfatpad:theeffectsoffree
fattyacids.IntJObes(Lond)37:1079-1087.
16. EltawilNM,DeBariC,AchanP,etal.2009.Anovelinvivomurinemodelofcartilageregeneration.
Ageandstrain-dependentoutcomeafterjointsurfaceinjury.OsteoarthritisCartilage17:695-704.
17. SvensonKL,VonSmithR,MagnaniPA,etal.2007.Multipletraitmeasurementsin43inbredmouse
strains capture the phenotypic diversity characteristic of human populations. J Appl Physiol
(1985)102:2369-2378.
18. Pineda S, PollackA, Stevenson S, et al. 1992.A semiquantitative scale for histologic gradingof
articularcartilagerepair.ActaAnat(Basel)143:335-340.
19. vanderSluijsJA,GeesinkRG,vanderLindenAJ,etal.1992.ThereliabilityoftheMankinscorefor
osteoarthritis.JOrthopRes10:58-61.
20. KrennV,MorawietzL,HauplT,etal.2002.Gradingofchronicsynovitis--ahistopathologicalgrading
systemformolecularanddiagnosticpathology.PatholResPract198:317-325.

High fat diet accelerates cartilage repair 133
7
21. JaiswalPK,BentleyG,CarringtonRW,etal.2012.Theadverseeffectofelevatedbodymassindex
onoutcomeafterautologouschondrocyteimplantation.JBoneJointSurgBr94:1377-1381.
22. MatsuokaM,OnoderaT,SasazawaF,etal.2015.AnArticularCartilageRepairModelinCommon
C57Bl/6Mice.TissueEngPartCMethods.
23. RaiMF,SandellLJ.2014.Regenerationofarticularcartilageinhealerandnon-healermice.Matrix
Biol39:50-55.
24. FitzgeraldJ,RichC,BurkhardtD,etal.2008.EvidenceforarticularcartilageregenerationinMRL/
MpJmice.OsteoarthritisCartilage16:1319-1326.
25. MakJ,LeonardC,FoniokT,etal.2015.Evaluatingendogenousrepairoffocalcartilagedefectsin
C57BL/6andMRL/MpJmiceusing9.4Tmagneticresonance imaging:Apilotstudy.MagnReson
Imaging33:690-694.
26. MullAJ,BerhanuTK,RobertsNW, et al. 2014.TheMurphyRothsLarge (MRL)mouse strain is
naturallyresistanttohighfatdiet-inducedhyperglycemia.Metabolism63:1577-1586.
27. ApovianCM,BigorniaS,MottM,etal.2008.Adiposemacrophage infiltration isassociatedwith
insulin resistance andvascular endothelial dysfunction in obese subjects.ArteriosclerThromb
VascBiol28:1654-1659.
28. vanBeekL,LipsMA,VisserA, et al. 2014. Increasedsystemicandadipose tissue inflammation
differentiatesobesewomenwithT2DMfromobesewomenwithnormalglucosetolerance.Metabo-
lism63:492-501.
29. GiermanLM,vanderHamF,KoudijsA,etal.2012.Metabolicstress-inducedinflammationplaysa
majorroleinthedevelopmentofosteoarthritisinmice.ArthritisRheum64:1172-1181.
30. WeiW,ClockaertsS,Bastiaansen-JenniskensYM,etal.2014.Statinsandfibratesdonotaffectdevel-
opmentofspontaneouscartilagedamageinSTR/Ortmice.OsteoarthritisCartilage22:293-301.
31. HowardJS,MattacolaCG,RomineSE,etal.2010.ContinuousPassiveMotion,EarlyWeightBear-
ing,andActiveMotion followingKneeArticularCartilageRepair:Evidence forClinicalPractice.
Cartilage1:276-286.
32. LaplanteM,SabatiniDM.2009.mTORsignalingataglance.JCellSci122:3589-3594.
33. ZhangY,VasheghaniF,LiYH,etal.2015.Cartilage-specificdeletionofmTORupregulatesautophagy
andprotectsmicefromosteoarthritis.AnnRheumDis74:1432-1440.
34. BushJR,BerubeNG,BeierF.2015.Anewprescriptionforgrowth?Statins,cholesterolandcartilage
homeostasis.OsteoarthritisCartilage23:503-506.
35. ZhangH,LinCY.2008.Simvastatinstimulateschondrogenicphenotypeofintervertebraldisccells
partiallythroughBMP-2pathway.Spine(PhilaPa1976)33:E525-531.
36. PeisterA,MelladJA,LarsonBL,etal.2004.Adultstemcellsfrombonemarrow(MSCs)isolated
fromdifferentstrainsofinbredmicevaryinsurfaceepitopes,ratesofproliferation,anddifferentia-
tionpotential.Blood103:1662-1668.


EPILOGUE


CHAPTER 8
Summary and general discussion


Summary and general discussion 139
8
SUMMARY AND GENERAL DISCUSSION
Themostcharacteristicchangesinobesityareanincreaseinadiposetissuemass
andadipose tissue inflammation.This in turn leads to increased loadingof the
jointsandsystemicmetabolicandinflammatorychanges.Becauseadiposetissue
is amajor contributor to the inflammation in obesity,wehave focusedon the
effectofadiposetissueondifferenttissueinthekneejointandcartilagerepair.
LOCAL EFFECTS OF ADIPOSE TISSUE
The infrapatellar fat pad, an adipose tissue not changed by obesity
Theinfrapatellarfatpad(IPFP)isanintra-articularadiposetissueindirectcontact
withthesynoviummembraneandcanthereforeinfluencethekneejointenviron-
ment. Itcanplayanrole inbiomechanicsof theknee,actasashockabsorber
andisareservoirofinflammatoryandregenerativecells1-3.Adiposetissueingen-
eralfunctionsasareservoirforexcessnutrientsandincreasesinsizeinobesity.
However,MRIstudiessuggestthat,unlikemostotheradiposetissuesinthebody,
IPFPsizeisnotcorrelatedtobodymassindex(BMI)4-6.Furthermore,unlikeinsub-
cutaneousandvisceraladiposetissue,theadipocytesizeinosteoarthritic(OA)
IPFPwasnotcorrelatedtoBMI(Chapter 2).Besidesadipocytehypertrophy,an
increased infiltrationofpro-inflammatorymacrophagesand formationofcrown
likestructuresinadiposetissuearegenerallyconsideredtobecharacteristicsfor
obesity7.However,wecouldnotdetectadifferenceinmacrophageinfiltrationin
IPFPbetweenobeseandnon-obesedonorsinourpreviouswork8 nor in Chapter
4.Anin-vivostudyinhighfatdietfedC57BL/6micehasconfirmedourfindingthat
adipocytesizeandinfiltrationofmacrophagesarenotchangedbyweightgain9.
Obesity increases secretion of pro-inflammatory factors such as TNFα, IL1β,MCP-1,IL6andleptinbyadiposetissue10.However,wehavepreviouslyshownby
multiplexELISAanalysisthatsecretionofcytokinesbyOAIPFPisnotassociated
toBMI11.Finally,alltheeffectstheIPFPhadoncartilage,synovialfibroblastsand
MSCswerenotcorrelatedtoBMI(Chapter 3 and 4)8,.ThisallsuggeststhatIPFP,
unlikesubcutaneousandvisceraladiposetissue,isnotinfluencedbyobesity.
The IPFP and inflammation
Although the IPFPseemsnot tobe influencedbyobesity, it couldstillbecome
inflamedafterjointtraumaandsurgery12-14.InflammatorycytokinessuchasIL1β
canincreasethesecretionofinflammatoryfactorsbyIPFP11.Withmoreinflamma-
torystimuli,thereisanincreasedsecretionofinflammatoryfactorsbytheIPFP.

140 CHAPTER 8
Becausethesynoviumdoesnothaveabasalmembrane,theonlybarrierformol-
eculesbetweenthesynovialfluidandtheIPFPistheextracellularmatrix(ECM)
of thesynovial interstitium. Inthiscase, thesmaller themolecule, theeasier it
canfreelydiffusethroughthesynovialinterstitium15.WeinvestigatedinChapter
4theeffectofIPFPsecretedfactorsoncartilagerepair,andfoundthattheycould
inhibitMSC-basedcartilagerepair.Nexttodirectlyinfluencingtherepairprocess,
factorssecretedby IPFPalso influencethesynoviummembranebystimulating
pro-fibrotic processes (Chapter 3)andpro-catabolicprocessesinsynovialfibro-
blasts16( Chapter 5).Inturn,thiscanleadtoanincreaseininflammatoryfactors
inthesynovialfluidandfurtherdeteriorationofthejointenvironmentforrepair.
Studies have shown an increased amount of pro-inflammatory cytokines such
as IL1α/β, IL6, IL8, andTNFα, in synovial fluids of patientswith focal cartilage
defects17; 18, ACL rupture19-21 or OA22 knees compared to healthy knees. Pro-
inflammatorycytokinessuchasIL1α/β,IL6,IL17,IFNƴ,TNFα,MCP1canallinhibit
MSCchondrogenesis23-26 andincreasecatabolicprocesses inthesynoviumand
cartilage27.ReductionofthesecretionofthesecytokinesbytheIPFPorinhibiting
theeffectsofthesecytokinescouldbepromisingstrategiestoimprovethejoint
environmentandcartilagerepair.Oneshouldbecarefulhoweverwithinhibition
ofinflammation.StudiesinMRL/MpJmice,whopossesssuperhealingcapacities,
haveshownthatinflammationisnecessaryforsuccessfulwoundhealing28;29.Find-
ing the rightbalancebetweensufficient inflammation to initiatewoundhealing
andreducechronicinflammationtoinhibitcatabolicprocessesisnecessaryfor
successfulcartilagerepair.
TheIPFPconsistsmainlyofadipocytes,stemcellsandinflammatorycellssuchas
macrophages.InChapter 4wehaveshownthatpro-inflammatorymacrophages
in IPFPcontributetotheanti-chondrogeniceffectof IPFP.Macrophagesplayan
importantroleininflammationandtissuerepair.Pro-inflammatorymacrophages
secreteTNFα,IL1βandIL630andcouldthereforeinhibitcartilagerepairinvitro,in-
duce catabolic processes in cartilage31andpro-fibroticprocessesinsynovialfibro-
blasts (Addendum figure 1).Ananimalstudyreportsthatablationofallsynovial
macrophagescouldinhibitdevelopmentofOA32.Anti-inflammatorymacrophages
however,donotinhibitcartilagerepair(Chapter 4)33andmightbeevenbeneficial
tocartilagerepairinvitro34.Furthermore,Axolotls,whichareknowntobeable
toregenerate limbs,cannotregeneratewithout thepresenceofmacrophages35.
Therightbalancebetweenpro-andanti-inflammatorymacrophagesseemstobe
crucialforsuccessfulcartilagerepair.InChapter 5weuseddifferentmedications
tomodulatethemacrophagesinsidetheIPFPtowardsamoreanti-inflammatory
phenotype.Ofthemedicationswetested,onlytriamcinoloneacetonide(TAA)was

Summary and general discussion 141
8
able to reduce inflammation in IPFPandmodulate themacrophages towardsa
anti-inflammatoryphenotype.Theanti-chondrogenicandpro-cataboliceffectsof
theIPFPwerealsoreducedbyTAA.Thissuggeststhatmodulationofmacrophage
phenotypebymedicationmight improve the joint environment to reduce joint
diseaseandbebettersuitableforcartilagerepair.
Although the adipocyte size, macrophage phenotype in and the secretion of
inflammatorycytokinesbyIPFParenotinfluencedbyobesity,theIPFPremains
alargesourceofinflammatoryfactorsthataffectsthejointenvironment.Nextto
inflammatorycytokines,theadipocytesinIPFPsecretemanyadipokinessuchas
leptin36,adiponectin36,resistinandvisfatin11.Leptin,resistinandvisfatinstimulates
catabolic processes in cartilage1,synovium1andmeniscus37.Theroleofadiponec-
tinisnotyetfullyunderstood.AdiponectinincreasesATDC5-cellproliferationand
chondrogenesis38,howeveritisalsoassociatedwithcartilagedamageinOAand
couldincreaseMMP13activityandPGE2releaseinOAchondrocytes39.However
blockingadiponectinand leptindidnot inhibit thepro-cataboliceffectsof IPFP
on OA chondrocytes and synovial fibroblasts36. The effect of these adipokines
onMSCchondrogenesisisstillunknown,butreductionofcatabolicprocessesin
generalwouldeventuallybenefitthejointenvironment.Glucocorticoidsmodulate
adipokinessecretionbyadiposetissue40-42.Therefore,thereductionofcatabolic
processes in Chapter 5by treatmentwithTAAcouldalsohave takenplacevia
modulationofadipokinesecretionbytheIPFP,nexttomodulationofmacrophages
andtheirsecretionprofile.
TheIPFPandadipocytesalsoreleaseprostaglandins.Prostaglandinsareagroup
oflipidsthatplayanimportantroleininflammation43,cartilagemetabolism44;45 and
pathogenesisofOA46;47.InChapter 3wedescribethatprostaglandinF2α(PGF2α)
secreted by IPFP is involved in pro-fibrotic processes in synovial fibroblasts.
However,PGF2αdoesnotinhibitMSCchondrogenesis(Addendum figure 2),but
evenenhanceschondrogenesisinATDC5cells45andmatrixdepositionbyarticular
chondrocytes44.NexttoPGF2α,theIPFPalsosecretesprostaglandinE2(PGE2)48;49,
which stimulatespro-catabolic processes in synovial fibroblasts48. Inhibitionof
prostaglandinsecretion ispossiblethroughinhibitionofcyclooxygenase(COX)
activity.Non-specificCOXinhibitorssuchasnon-steroidanti-inflammatorydrugs
(NSAIDs) and specificCOX-2 inhibitors such as celecoxib are already clinically
usedtoreduceinflammationandthesymptomsofOA.AlthoughCOXinhibition
could be beneficial to reduce pro-fibrotic and catabolic processes47,non-specific
COX-inhibitionalsoinhibitsMSCchondrogenesis50.Ontheotherhand,aspecific
COX-2inhibitorislessdetrimentaltochondrogenesis50-52.Therefore,specificCOX-2

142 CHAPTER 8
inhibitorssuchascelecoxibarepossiblecandidatestoimprovethejointenviron-
mentforcartilagerepair.Surprisingly,celecoxibdidnotreduceIPFPinflammatory
genesexpressioninChapter 5andbecausereductionofgeneralIPFPinflammation
isimportanttoimprovethejointenvironment,wedidnotfurtherinvestigatethe
effectsofcelecoxiboncartilagerepair. InChapter 5wedemonstratedareduc-
tion inanti-chondrogenicandpro-cataboliceffectsof IPFPafter treatmentwith
TAA.TAAisanoftenusedglucocorticoidandglucocorticoidsareknowntoinhibit
prostaglandin synthesis53.However,italsoinhibitsotherpro-inflammatorypath-
waysandthereforetargetingprostaglandinsynthesisalonemightbeinsufficient
toimprovethejointenvironmentforcartilagerepair.
Nexttoprostaglandins,therearealsootherlipidsinthesynovialfluidoftheknee
joint49;54.Onegroupof lipidsare the fattyacidsand these fattyacidsarebeing
extensivelystudied.Fattyacidscanstimulateorinhibitinflammatoryprocesses55
and influence cartilage loss in OA cartilage56. An increased intake of omega-3
fattyacidscoulddecreasechronicinflammation57 and dietary fatty content could
regulatewoundhealinginmice58.Itisthereforeinterestingtoinvestigatewhether
changingdietisapossiblestrategytomodulateIPFPinflammationandthereby
improvecartilage repairprocedures. Furthermore, future researchcouldbe fo-
cusedonusingmedicationstomodifythelevelsofspecifictypesoffattyacidsand
inthatwayinfluencecartilagerepair.InChapter 5weusedstatinsandfibrates,
twooftenusedserumlipidloweringdrugs,toreduceIPFPinflammation.However,
wedidnotseeaneffectonIPFPinflammatorygenesexpression.Thesemedica-
tionsareknowntoreducesystemicinflammationsotheycouldstillbeusefulin
improving thegeneral jointhealthduringcartilagerepairprocedures,although
moreinvestigationisnecessary.
Removal of the IPFP
InsteadofmodulationoftheIPFP,itisalsopossibletosurgicallyremovetheIPFP2.
Duringtotalkneearthroplasty,theIPFPisoftenremovedtoimprovevisibilitydur-
ing the surgical procedure59;60.HowevertheremovaloftheIPFPduringtotalknee
arthroplasty is under debate61 because it is associated with shortened patellar
tendonandanteriorkneepain.Evensubtotalremovalof the IPFPwitharthros-
copy could lead to patellar tendon shortening60;62-64.Thissupportsthetheorythat
theIPFPhasamechanicalfunctionthatisnecessaryforproperjointmovement.
Besidesadipocytesandmacrophages,therearealsoMSCsintheIPFP65-67.These
MSCshavebeenshowntohavechondrogenic66;67aswellasimmunomodulatory68
capacities and some authors have proposed to use theseMSCs inMSC-based

Summary and general discussion 143
8
cartilage repair procedures66;69.ItmightalsobepossiblethatMSCsfromtheIPFP
migratetoacartilagedefectandcontributetorepair,althoughcurrentlythereis
nostudythathaveshownthis.MSCsfromthebonemarrow70andsynovialmem-
brane71couldmigratetowardsacartilagedefect.Peripheralmononucleatedcells
migratefromthebloodcirculationtoacartilagedefectinrats72,sofutureresearch
mightshowthatMSCsfromIPFPcouldalsodothis.
Furthermore,wehavepreviouslyshownthatOAIPFPconditionedmediuminhib-
itscatabolicmediatorsinbovinecartilage8.ThismeansthattheeffectofIPFPon
theseparatejointstructurescouldbedifferent.Hence,completeremovalofthe
IPFPcouldchangethejointenvironmenttoomuchandremovethebeneficialcells
intheIPFPthatmightcontributetosuccessfulcartilagerepairintheknee.
Other intra-articular adipose tissues
Mostsynovialjointshaveadiposetissuefillingthesynovialfoldsaroundthear-
ticularmargin.Thesefatdepotspossiblyactascushionsduringjointmovement73.
AlthoughtheIPFPisthelargestintra-articularadiposetissue,itisnottheonlyone
intheknee.Inthekneetherearealsothesupra-patellarfatpad,locatedbeneath
thequadricepstendon74;75,andthepre-femoralfatpad,locatedattheanteriorside
ofthefemur.SignalalterationsonMRIofthesefatpadsareassociatedtosynovi-
tis,anteriorkneepainandstructuralabnormalities74;76;77.Duetotheirproximity
totheIPFPandbecausetheyareincontactwiththesamesynovialsynovialfluid,
itmightbeexpectedthatthesameinflammatorysignalsthatwouldinfluencethe
IPFPwouldalsoinfluencethesefatpaddepots.
Besides the knee, the ankle and the hip also have an intra-articular adipose
tissue.IntheankleitiscalledtheKager’sfatpadandislocatedposteriortothe
anklejoint,anteriortotheAchillestendon78.TheKager’sfatpadisalsoknownas
thepre-Achilles fatpad.Traumato thecalcaneusorAchilles tendinopathycan
influencetheKager’sfatpad78;79.Theintra-articularadiposetissueinthehiphas
only been recently described80andissimilartotheIPFPintissularphenotype81.
Notmuch isknownaboutthisadiposetissue,but itcanbecome impingedand
causepainduringhipmovement80.
Withmoreunderstandingoftheroleoftheseotherintra-articularadiposetis-
sues,wemightimproveourunderstandingoftheroleoftheIPFPinthekneejoint.
Furthermore,theseotherintra-articularadiposetissuemightalsobetargetedto
modifythejointenvironment.

144 CHAPTER 8
SYSTEMIC EFFECTS OF ADIPOSE TISSUE
Besidesthelocaleffectsofadiposetissueonjointdiseaseandrepair,thesystemic
effects has alsobeen a focus of investigation. Especially the systemic changes
thatoccurinobesityisbeingextensivelystudied.Obesityincreasesthechance
of developing the metabolic syndrome, which is characterized by low grade
systemicinflammation,dyslipidemia,hyperinsulinemiaandhyperglycemia.Meta-
bolicsyndromehasbeenshowntobeariskfactorforthedevelopmentofOA82;83.
Obesityandtheresultingmetabolicsyndromearecausedbyaninterplaybetween
behavioral, environmental and genetic factors84; 85. Althoughourwork suggests
that the IPFP is possibly not influencedby obesity, subcutaneous and visceral
adiposetissuesbecomeinflamedduetoobesity86.Inadiposetissueinflammation,
there ismore infiltrationofpro-inflammatorymacrophages, formationofcrown
likestructuresandthereisanincreaseinsecretionofinflammatoryfactorssuch
asTNFα,IL1β,MCP-1,IL6andleptin86.Toinvestigatetheeffectofmetabolicandin-
flammatorysystemicchangesonjointdiseaseandcartilagerepair,weperformed
twoin-vivostudieswithmice.
Obesity related metabolic and inflammatory changes on cartilage damage
In Chapter 6weusedtheSTR/Ortstrainofmice.Thesemicedevelopmetabolic
and inflammatorychangesspontaneouslyonanormaldiet (Chapter 6,87).This
isnotcausedbyovereatingascomparedtotheOB/OBstrainofmice,whichdue
totheirleptindeficiency,doesnotstopeating88.Nexttodevelopingspontaneous
metabolicsyndrome89,maleSTR/Ortmicearealsoknowntodevelopspontaneous
cartilagedamage90.Thismousemodel therefore seemed tousverywell suited
to investigate whether development of spontaneous metabolic syndrome and
cartilagedamagearelinkedandwhethercartilagedamagecouldbeprevented.In
Chapter 6wefedmaleSTR/Ortmicechowmixedwithsimvastatinandfenofibrate.
Thesetwolipid loweringmedicationsarecommonlyusedtotreatdyslipidemia
and to reduce cardiovascularmorbidity andmortality91;92. Statin use has been
associatedwithdecreasedincidenceandprogressionofkneeOA93.Furthermore,
statinsandfibratesalsoreducesystemicinflammation94;95.InChapter 5wehave
shownthatstatinsandfibratesdidnotreduceIPFPinflammation,suggestingthat
thesemedicationsmightonlyhavesystemiceffects.Inourin-vivostudy,TheSTR/
Ortmicedevelopeddyslipidaemiaandsimvastatinandfenofibratedidnothave
aneffectondyslipidaemia in thesemice.Fenofibrate reducedweight, systemic
inflammationandvolumeofsubchondralbone,whereassimvastatindidnothave
aneffect.However, incontrast towhatweexpected,cartilagedamagewasnot
reducedbythesetwomedications.Ourresultssuggestthatdevelopmentofcar-

Summary and general discussion 145
8
tilagedamageinSTR/Ortmiceisnotprimarilylinkedtometabolicinflammation,
butismulti-factorial.Thisshowsthatacombinationofmetabolicinflammatory
changes andgeneticpredisposition are the causeof cartilagedamage in these
mice.Thisalsosuggestthatbeingobesedoesnotalwaysleadtocartilagedamage.
Obesity and cartilage repair
Whencartilagedamagehaveoccurredinobesepatients,weneedtorepairitto
preventthedevelopmentofOA.Theclinicalresultsofcartilagerepairinobesepa-
tientsisworse,butthereisnoinformationonthestructuraloutcomes.InChapter
7weinvestigatedwhetherahighfatdiet(HFD)inducedobesityreducescartilage
repairinDBA/1mice.Surprisingly,theHFDdidnotnegativelyinfluencecartilage
repair,butevenacceleratedit.Thiswasincontrasttocommonknowledgeand
whatwehypothesized.Furthermore,althoughthesemiceareknowntoberesistant
toOAdevelopmentaftercartilagedamage,theydidnotevendevelopOAaftercar-
tilagedamageincombinationwithaHFD.TheDBA/1miceonaHFDgainedweight,
butdidnothaveseruminflammatoryandmetabolicchanges.Furthermore,the
subcutaneousadipocytesofthesemiceonaHFDbecamehypertrophic,butthere
wasnoincreasedinfiltrationofmacrophagesnorformationofcrownlikestruc-
tures.ThisisinstarkcontrasttotheSTR/OrtmiceweusedinChapter 6,which
developed metabolic and inflammatory changes spontaneously. This suggests
thatresistancetoHFDinducedinflammatoryandmetabolicchangesisassociated
withacceleratedcartilagerepairandreducedOAsusceptibility.Inhumans,some
individuals are prone to development ofmetabolic syndrome84, but some also
gainweightandbecomeobese,butdonotdeveloptheaccompanyingmetabolic
and inflammatorychanges.Thisgroupofobese individuals, alsoknownas the
metabolic healthy obese, are often characterized by less serum inflammation,
lessvisceralfat,lessmacrophageinfiltrationinadiposetissueandlessadipocyte
hypertrophy96;97.Itremainsinconclusivewhethertheriskofcardiovascularheart
diseaseisdifferent inthisgroupof individuals97comparedtoobeseindividuals
withmetabolicchanges.Furthermore,itisunknownwhethertheseindividualsare
protectedfromjointdiseaseorhaveimprovedrepaircapabilities.Futureresearch
investigatingwhethertheseindividualsareprotectedagainstjointdiseaseorhave
improvedrepairmightprovideuswithnewtreatmenttargets.
The results of our two in-vivo studies indicate that the link between obesity
relatedmetabolicandinflammatorychanges,degenerativejointdiseaseandcar-
tilagerepair iscomplex.Furthermore,thereisheterogeneityin individualswho
areobese.AstudybyGreenetalhasshownthattherearemultipletypesofobese
individuals,whoallhavetheirspecificcausesforobesityandrelateddiseases98.

146 CHAPTER 8
Theauthorshaveconcludedthattreatmentstrategiesforobesityshouldnottar-
getobeseindividualsasawhole,butsubgroupspecificstrategiesshouldbeused.
Tobetterunderstandhowobesityinfluencesthejoint,itisthereforeimportantto
takeintoaccountthisheterogeneityofobesity.Repetitionofourin-vivostudies
usingdifferentanimalmodelsshouldtakethisheterogeneityintoaccount.
FUTURE PERSPECTIVES
Obesity, adipose tissue and the joint environment
Adiposetissueisnotonlyastoragesiteforexcessenergy,butisalsoanendocrine
organ,whichsecreteslargeamountsofimmunological,endocrineandhormonal
factors.Adiposetissueinflammationplaysanimportantroleinthepathophysi-
ologyofmetabolicdysregulation inobesity.Much isknownabout thechanges
thatoccurinsubcutaneousandvisceraladiposetissueinobesity.Lessisknown,
however,aboutobesityrelatedchangesinintra-articularadiposetissue.Obesity
isawell-knownriskfactorforjointdiseasesandhasbeenextensivelystudiedin
animalandclinicalstudies.Duetotheintra-articularlocationofIPFP,ithaslong
been thought that the IPFPwouldplayan important role inobesityassociated
jointinflammation.However,wehaveshownthattheIPFPmightnotbeinfluenced
byobesityandthatobesitycausesdegenerativejointdiseasesviaotherpathways
andnotviaIPFPinflammation.Thiscouldbethroughincreasedsystemicinflam-
mationormetabolicdysregulationduetoinflammationofthebiggersubcutane-
ousandvisceraladiposetissuedepots.
However,theeffectsofobesitycouldvarybetweenindividuals.Wehavenowshown
inanimalstudiesthatobesityisnotalwaysnegativeortherelationshipbetweenthe
changescausedbyobesityondegenerativejointdiseaseisnotalwayscompletely
clear.Theobesityepidemicwillonlyincreaseinthefutureandresearchwillcon-
tinue inthisfield.Newtargets forstrategiesto improvethe jointenvironment in
obesitymightbefoundinresearchfocusingonsubgroupsofindividualswhoare
lesssusceptibletodevelopingobesityrelatedchanges.Itwouldbeinterestingto
investigatewhethertheseindividualsarealsoprotectedagainstjointdiseases.
Modulation of the infrapatellar fat pad to improve the joint environment for cartilage repair
Irrespectivelytotheeffectsofadiposetissuerelatedsystemicchangeshaveonthe
local jointenvironment, the IPFPsecretesa largeamountofdifferentadipokines
andfattyacids.Theseindividualfactorsmighthaveanabolicorcataboliceffectson

Summary and general discussion 147
8
differentjointstructures.Within-vitroexperimentsusingIPFPconditionedmedium,
wehaveshownwhattheeffectsareofIPFPsecretedfactorsonthejoint.Further-
more,wehaveshownthatwecanmodulatein-vitrothesecretionoffactorsbythe
IPFPandtheresidentmacrophageswithacommonlyusedglucocorticoid.Thenext
stepcouldbeanin-vivoanimalstudytotestthehypothesisthatusingTAAtheIPFP
canbemodulated tobebeneficial for the joint environment.Most experimental
studiesontheeffectofinflammatorymodulationonjointdiseasearefirstperformed
in rodents.However, due to the small sizeof the rodent knee, specific targeting
theIPFPisdifficult,althoughnotimpossible.Futureexperimentsusingcanineor
ovinemodelscouldbeconsideredtoinvestigatewhetherIPFPmodulationwouldbe
feasibletoimprovethejointenvironmentforcartilagerepair.Itwouldalsobepos-
sibletodirectlyperformahumanstudy,becauseTAAiscurrentlyalreadyinjected
intra-articularly as an anti-inflammatory treatment.Thenext stepwouldonlybe
injectionofadosageofTAAintheIPFPfollowingmicrofracturesurgery.
Currently, theeffectofdifferent intra-articularstrategiesusingpharmacological
drugsandimmunomodulatorcellsisbeingstudiedforusetoimprovethejoint
environmentforcartilagerepairordirectlyinfluencecartilagerepairitself99.Next
to theeffectoncartilage repair, theeffectof these intra-articular strategieson
synoviumisalsoimportant.Thesynoviumcanbecomeinflamedandisasourceof
catabolicandanti-chondrogenicfactors.Ontheotherhand,withtheexperiments
performedinthisthesis,wehaveshownthattheIPFPisanimportanttissuein
thejointenvironmentaswell.TheIPFPcanstimulatecatabolicprocessesinthe
synovium,althoughthiscouldalsobevice-versa,wheresynoviuminflammation
couldstimulatecatabolicprocessesintheIPFP.Nevertheless,itispossiblethat
anyfutureintra-articulartherapyadministeredcouldinfluencetheIPFPandvia
the IPFP influence the synovium. Therefore, IPFP changes should be carefully
monitoredduringexperimentaltreatmentsandreductionofinflammationinthe
IPFPcouldbeconsideredasoneofthesecondaryoutcomes.
Concluding remarks
Inconclusion,thisthesisshowsthattheIPFPisnotanordinaryadiposetissueand
thatitsecretesspecificfactorsthatlocallyinfluencethekneejointandcartilage
repair.Inthefuture,itispossibletousemedicationtospecificallymodulatethe
IPFPtoimprovethejointenvironmentforcartilagerepair.Furthermore,thisthesis
providesevidencethatthereisvariabilityinhowobesityrelatedsystemiceffects
canaffectdegenerative jointdiseaseandcartilagerepair.Futurestudiesonthe
relationshipbetweenobesity,adiposetissueandcartilagerepaircouldfocuson
thisvariabilitytouncovernoveltherapeutictargets.

148 CHAPTER 8
REFERENCES
1. ClockaertsS,Bastiaansen-JenniskensYM,RunhaarJ,etal.2010.Theinfrapatellarfatpadshould
beconsideredasanactiveosteoarthriticjointtissue:anarrativereview.OsteoarthritisCartilage
18:876-882.
2. DragooJL,JohnsonC,McConnellJ.2012.Evaluationandtreatmentofdisordersoftheinfrapatellar
fatpad.SportsMed42:51-67.
3. FontanellaCG,CarnielEL,FrigoA,etal.2016.InvestigationofbiomechanicalresponseofHoffa’sfat
padandcomparativecharacterization.JMechBehavBiomedMater67:1-9.
4. CaiJ,XuJ,WangK,etal.2015.AssociationBetweenInfrapatellarFatPadVolumeandKneeStruc-
turalChangesinPatientswithKneeOsteoarthritis.JRheumatol42:1878-1884.
5. ChuckpaiwongB,CharlesHC,KrausVB, et al. 2010.Age-associated increases in the sizeof the
infrapatellarfatpadinkneeosteoarthritisasmeasuredby3TMRI.JOrthopRes28:1149-1154.
6. DuranS,AksahinE,KocadalO,etal.2015.Effectsofbodymassindex,infrapatellarfatpadvolume
andageonpatellarcartilagedefect.ActaOrthopBelg81:41-46.
7. ApovianCM,BigorniaS,MottM,etal.2008.Adiposemacrophage infiltration isassociatedwith
insulin resistance andvascular endothelial dysfunction in obese subjects.ArteriosclerThromb
VascBiol28:1654-1659.
8. Bastiaansen-JenniskensYM,ClockaertsS,FeijtC,etal.2012.Infrapatellarfatpadofpatientswith
end-stageosteoarthritisinhibitscatabolicmediatorsincartilage.AnnRheumDis71:288-294.
9. ChangWDC,KentC,KovatsS,GarteiserP,DoblasS,TownerR,GriffinTM.2011.Infrapatellarfat
padhypertrophywithoutinflammationinadiet-inducedmousemodelofobesityandosteoarthri-
tis.OsteoarthritisCartilage19:S53–S236.
10. GrantRW,DixitVD.2015.Adiposetissueasanimmunologicalorgan.Obesity(SilverSpring)23:512-
518.
11. ClockaertsS,Bastiaansen-JenniskensYM,FeijtC,etal.2012.Cytokineproductionbyinfrapatellar
fatpadcanbestimulatedbyinterleukin1betaandinhibitedbyperoxisomeproliferatoractivated
receptoralphaagonist.AnnRheumDis71:1012-1018.
12. AbreuMR,ChungCB,TrudellD, et al. 2008.Hoffa’s fatpad injuries and their relationshipwith
anteriorcruciateligamenttears:newobservationsbasedonMRimaginginpatientsandMRimag-
ingandanatomiccorrelationincadavers.SkeletalRadiol37:301-306.
13. GandhiR,TakahashiM,VirtanenC,etal.2011.Microarrayanalysisoftheinfrapatellarfatpadin
kneeosteoarthritis:relationshipwithjointinflammation.JRheumatol38:1966-1972.
14. SolbakNM,HeardBJ,AchariY,etal.2015.AlterationsinHoffa’sfatpadinducedbyaninflammatory
responsefollowingidealizedanteriorcruciateligamentsurgery.InflammRes64:615-626.
15. EvansCH,KrausVB,SettonLA.2014.Progressinintra-articulartherapy.NatRevRheumatol10:11-
22.
16. EymardF,PigenetA,CitadelleD,etal.2017.Kneeandhipintra-articularadiposetissues(IAATs)
comparedwithautologoussubcutaneousadiposetissue:aspecificphenotypeforacentralplayer
inosteoarthritis.AnnRheumDis.
17. TsuchidaAI, BeekhuizenM,RutgersM, et al. 2012. Interleukin-6 is elevated in synovial fluid of
patientswithfocalcartilagedefectsandstimulatescartilagematrixproductioninaninvitroregen-
erationmodel.ArthritisResTher14:R262.
18. TsuchidaAI,BeekhuizenM,tHartMC,etal.2014.Cytokineprofilesinthejointdependonpathol-
ogy,butaredifferentbetweensynovialfluid,cartilagetissueandculturedchondrocytes.Arthritis
ResTher16:441.

Summary and general discussion 149
8
19. BigoniM,SacerdoteP,TuratiM,etal.2013.Acuteandlatechangesinintraarticularcytokinelevels
followinganteriorcruciateligamentinjury.JOrthopRes31:315-321.
20. IrieK,UchiyamaE,IwasoH.2003.Intraarticularinflammatorycytokinesinacuteanteriorcruciate
ligamentinjuredknee.Knee10:93-96.
21. MarksPH,DonaldsonML.2005.Inflammatorycytokineprofilesassociatedwithchondraldamage
intheanteriorcruciateligament-deficientknee.Arthroscopy21:1342-1347.
22. BeekhuizenM,GiermanLM, van SpilWE, et al. 2013.An explorative study comparing levels of
solublemediatorsincontrolandosteoarthriticsynovialfluid.OsteoarthritisCartilage21:918-922.
23. HarrisQ,SetoJ,O’BrienK,etal.2013.Monocytechemotacticprotein-1inhibitschondrogenesisof
synovialmesenchymalprogenitorcells:aninvitrostudy.StemCells31:2253-2265.
24. JagielskiM,WolfJ,MarzahnU,etal.2014.TheinfluenceofIL-10andTNFalphaonchondrogenesis
ofhumanmesenchymalstromalcellsinthree-dimensionalcultures.IntJMolSci15:15821-15844.
25. KondoM,YamaokaK,TanakaY.2014.Acquiringchondrocytephenotypefromhumanmesenchymal
stemcellsunderinflammatoryconditions.IntJMolSci15:21270-21285.
26. WeiH,ShenG,DengX,etal.2013.TheroleofIL-6inbonemarrow(BM)-derivedmesenchymalstem
cells(MSCs)proliferationandchondrogenesis.CellTissueBank14:699-706.
27. LieberthalJ,SambamurthyN,ScanzelloCR.2015.Inflammationinjointinjuryandpost-traumatic
osteoarthritis.OsteoarthritisCartilage23:1825-1834.
28. CanhameroT,GarciaLV,DeFrancoM.2014.AcuteInflammationLociAreInvolvedinWoundHealing
intheMouseEarPunchModel.AdvWoundCare(NewRochelle)3:582-591.
29. GourevitchD,KossenkovAV,ZhangY,etal.2014.InflammationandItsCorrelatesinRegenerative
WoundHealing:AnAlternatePerspective.AdvWoundCare(NewRochelle)3:592-603.
30. MosserDM,EdwardsJP.2008.Exploringthefullspectrumofmacrophageactivation.NatRevIm-
munol8:958-969.
31. UtomoL,Bastiaansen-JenniskensYM,VerhaarJA,etal.2016.Cartilage inflammationanddegen-
erationisenhancedbypro-inflammatory(M1)macrophagesinvitro,butnotinhibiteddirectlyby
anti-inflammatory(M2)macrophages.OsteoarthritisCartilage24:2162-2170.
32. BlomAB,vanLentPL,LibregtsS,etal.2007.Crucialroleofmacrophages inmatrixmetallopro-
teinase-mediatedcartilagedestructionduringexperimentalosteoarthritis:involvementofmatrix
metalloproteinase3.ArthritisRheum56:147-157.
33. FahyN,deVries-vanMelleML,LehmannJ,etal.2014.Humanosteoarthriticsynoviumimpacts
chondrogenicdifferentiationofmesenchymalstemcellsviamacrophagepolarisationstate.Osteo-
arthritisCartilage22:1167-1175.
34. SesiaSB,DuhrR,MedeirosdaCunhaC,etal.2015.Anti-inflammatory/tissuerepairmacrophages
enhance the cartilage-forming capacity of human bone marrow-derived mesenchymal stromal
cells.JCellPhysiol230:1258-1269.
35. GodwinJW,PintoAR,RosenthalNA.2013.Macrophagesarerequired foradultsalamander limb
regeneration.ProcNatlAcadSciUSA110:9415-9420.
36. GrossJB,GuillaumeC,Gegout-PottieP,etal.2016.Theinfrapatellarfatpadinducesinflammatory
anddegradativeeffectsinarticularcellsbutnotthroughleptinoradiponectin.ClinExpRheumatol.
37. NishimutaJF,LevenstonME.2015.Meniscusismoresusceptiblethancartilagetocatabolicand
anti-anaboliceffectsofadipokines.OsteoarthritisCartilage23:1551-1562.
38. ChallaTD,RaisY,OrnanEM.2010.EffectofadiponectinonATDC5proliferation,differentiationand
signalingpathways.MolCellEndocrinol323:282-291.
39. FrancinPJ,AbotA,GuillaumeC,etal.2014.Associationbetweenadiponectinandcartilagedegra-
dationinhumanosteoarthritis.OsteoarthritisCartilage22:519-526.

150 CHAPTER 8
40. FainJN,MadanAK,HilerML,etal.2004.Comparisonofthereleaseofadipokinesbyadiposetissue,
adiposetissuematrix,andadipocytesfromvisceralandsubcutaneousabdominaladiposetissues
ofobesehumans.Endocrinology145:2273-2282.
41. FardetL,Antuna-PuenteB,VatierC,etal.2013.Adipokineprofileinglucocorticoid-treatedpatients:
baselineplasmaleptinlevelpredictsoccurrenceoflipodystrophy.ClinEndocrinol(Oxf)78:43-51.
42. HeardBJ,SolbakNM,ChungM,etal.2016.Theinfrapatellarfatpadisaffectedbyinjuryinduced
inflammationintherabbitknee:useofdexamethasonetomitigatedamage.InflammRes65:459-470.
43. RicciottiE,FitzGeraldGA.2011.Prostaglandinsandinflammation.ArteriosclerThrombVascBiol
31:986-1000.
44. JakobM,DemarteauO,SuetterlinR,etal.2004.Chondrogenesisofexpandedadulthumanarticular
chondrocytesisenhancedbyspecificprostaglandins.Rheumatology(Oxford)43:852-857.
45. KimJ,ShimM.2015.ProstaglandinF2alphareceptor(FP)signalingregulatesBmpsignalingand
promoteschondrocytedifferentiation.BiochimBiophysActa1853:500-512.
46. AtturM,Al-MussawirHE,PatelJ,etal.2008.ProstaglandinE2exertscataboliceffectsinosteoar-
thritiscartilage:evidenceforsignalingviatheEP4receptor.JImmunol181:5082-5088.
47. ZweersMC,deBoerTN,vanRoonJ,etal.2011.Celecoxib:considerationsregardingitspotential
disease-modifyingpropertiesinosteoarthritis.ArthritisResTher13:239.
48. Eymard F, Pigenet A, CitadelleD, et al. 2014. Induction of an inflammatory and prodegradative
phenotypeinautologousfibroblast-likesynoviocytesbytheinfrapatellarfatpadfrompatientswith
kneeosteoarthritis.ArthritisRheumatol66:2165-2174.
49. GiermanLM,WopereisS,vanElB,etal.2013.Metabolicprofilingrevealsdifferencesinconcentra-
tionsofoxylipinsand fattyacidssecretedby the infrapatellar fatpadofdonorswithend-stage
osteoarthritisandnormaldonors.ArthritisRheum65:2606-2614.
50. PountosI,GiannoudisPV,JonesE,etal.2011.NSAIDSinhibitinvitroMSCchondrogenesisbutnot
osteogenesis: implications formechanismof bone formation inhibition inman. J CellMolMed
15:525-534.
51. WeltingTJ,CaronMM,EmansPJ,etal.2011.Inhibitionofcyclooxygenase-2impactschondrocyte
hypertrophicdifferentiationduringendochondralossification.EurCellMater22:420-436;discus-
sion436-427.
52. CaronMM,EmansPJ,SanenK,etal.2016.TheRoleofProstaglandinsandCOX-EnzymesinChon-
drogenicDifferentiationofATDC5ProgenitorCells.PLoSOne11:e0153162.
53. Goppelt-StruebeM,WolterD,ReschK.1989.Glucocorticoidsinhibitprostaglandinsynthesisnot
onlyatthelevelofphospholipaseA2butalsoatthelevelofcyclo-oxygenase/PGEisomerase.BrJ
Pharmacol98:1287-1295.
54. KimIC,CohenAS.1966.Synovialfluidfattyacidcompositioninpatientswithrheumatoidarthritis,
goutanddegenerativejointdisease.ProcSocExpBiolMed123:77-80.
55. Soto-VacaA,LossoJN,McDonoughK,etal. 2013.Differentialeffectof14 free fattyacids in the
expressionofinflammationmarkersonhumanarterialcoronarycells.JAgricFoodChem61:10074-
10079.
56. Bastiaansen-JenniskensYM,SiawashM,vandeLestCH,etal.2013.MonounsaturatedandSatu-
rated,butNotn-6PolyunsaturatedFattyAcidsDecreaseCartilageDestructionunderInflammatory
Conditions:APreliminaryStudy.Cartilage4:321-328.
57. SimopoulosAP.2002.Omega-3fattyacidsininflammationandautoimmunediseases.JAmCollNutr
21:495-505.
58. WuCL,JainD,McNeillJN,etal.2015.Dietaryfattyacidcontentregulateswoundrepairandthe
pathogenesisofosteoarthritisfollowingjointinjury.AnnRheumDis74:2076-2083.

Summary and general discussion 151
8
59. VanBeeckA,ClockaertsS,SomvilleJ,etal.2013.Doesinfrapatellarfatpadresectionintotalknee
arthroplastyimpairclinicaloutcome?Asystematicreview.Knee20:226-231.
60. WhiteL,HolyoakR,SantJ,etal.2016.Theeffectof infrapatellarfatpadresectiononoutcomes
post-totalkneearthroplasty:asystematicreview.ArchOrthopTraumaSurg136:701-708.
61. BosPK.2014.CORRInsights(R):Theeffectofinfrapatellarfatpadexcisiononcomplicationsafter
minimallyinvasiveTKA:arandomizedcontrolledtrial.ClinOrthopRelatRes472:702-703.
62. Pinsornsak P, NaratrikunK, Chumchuen S. 2014. The effect of infrapatellar fat pad excision on
complicationsafterminimallyinvasiveTKA:arandomizedcontrolledtrial.ClinOrthopRelatRes
472:695-701.
63. TakatokuK,SekiyaH,HayashiM,etal.2005.Influenceoffatpadremovalonpatellartendonlength
duringgrowth.KneeSurgSportsTraumatolArthrosc13:706-713.
64. YeC,ZhangW,WuW,etal.2016.InfluenceoftheInfrapatellarFatPadResectionduringTotalKnee
Arthroplasty:ASystematicReviewandMeta-Analysis.PLoSOne11:e0163515.
65. GarciaJ,WrightK,RobertsS,etal.2016.Characterisationofsynovialfluidandinfrapatellarfatpad
derivedmesenchymalstromalcells:Theinfluenceoftissuesourceandinflammatorystimulus.Sci
Rep6:24295.
66. NeriS,GuidottiS,LilliNL,etal.2016.Infrapatellarfatpad-derivedmesenchymalstromalcellsfrom
osteoarthritispatients:Invitrogeneticstabilityandreplicativesenescence.JOrthopRes.
67. WickhamMQ, Erickson GR, Gimble JM, et al. 2003.Multipotent stromal cells derived from the
infrapatellarfatpadoftheknee.ClinOrthopRelatRes:196-212.
68. MaumusM,ManferdiniC,ToupetK,etal.2013.Adiposemesenchymalstemcellsprotectchondro-
cytesfromdegenerationassociatedwithosteoarthritis.StemCellRes11:834-844.
69. TangchitphisutP,SrikaewN,NumhomS,etal.2016.InfrapatellarFatPad:AnAlternativeSourceof
Adipose-DerivedMesenchymalStemCells.Arthritis2016:4019873.
70. ShapiroF,KoideS,GlimcherMJ.1993.Celloriginanddifferentiationintherepairoffull-thickness
defectsofarticularcartilage.JBoneJointSurgAm75:532-553.
71. Hunziker EB, Rosenberg LC. 1996. Repair of partial-thickness defects in articular cartilage: cell
recruitmentfromthesynovialmembrane.JBoneJointSurgAm78:721-733.
72. OkanoT,WakitaniS,OkabeT,etal.2014.Nucleatedcellscirculatingintheperipheralbloodcon-
tributetotherepairofosteochondraldefectsonlyintheearlyphaseofhealing.JTissueEngRegen
Med8:414-420.
73. FontanellaCG,CarnielEL,FrigoA,etal.2017.InvestigationofbiomechanicalresponseofHoffa’sfat
padandcomparativecharacterization.JMechBehavBiomedMater67:1-9.
74. SchweitzerME,FalkA,PathriaM,etal.1993.MRimagingoftheknee:canchangesintheintracap-
sularfatpadsbeusedasasignofsynovialproliferationinthepresenceofaneffusion?AJRAmJ
Roentgenol160:823-826.
75. StaeubliHU,BollmannC,KreutzR,etal.1999.Quantificationofintactquadricepstendon,quadri-
cepstendoninsertion,andsuprapatellarfatpad:MRarthrography,anatomy,andcryosectionsin
thesagittalplane.AJRAmJRoentgenol173:691-698.
76. TsavalasN,KarantanasAH.2013.Suprapatellarfat-padmasseffect:MRIfindingsandcorrelation
withanteriorkneepain.AJRAmJRoentgenol200:W291-296.
77. WangJ,HanW,WangX,etal.2014.Masseffectandsignalintensityalterationinthesuprapatellar
fatpad:associationswithkneesymptomsandstructure.OsteoarthritisCartilage22:1619-1626.
78. LyJQ,Bui-MansfieldLT.2004.AnatomyofandabnormalitiesassociatedwithKager’sfatPad.AJR
AmJRoentgenol182:147-154.
79. PingelJ,PetersenMC,FredbergU,etal.2015.InflammatoryandMetabolicAlterationsofKager’s
FatPadinChronicAchillesTendinopathy.PLoSOne10:e0127811.

152 CHAPTER 8
80. JayasekeraN,ApratoA,VillarRN.2014.Fatpadentrapmentatthehip:anewdiagnosis.PLoSOne
9:e83503.
81. EymardF,PigenetA,CitadelleD,etal.2016.Kneeandhipintra-articularadiposetissuessharea
commonphenotypeinosteoarthritis.OsteoarthritisCartilage24(2016)S63-S534.
82. BerenbaumF,GriffinTM,Liu-BryanR.2017.Review:MetabolicRegulationofInflammationinOsteo-
arthritis.ArthritisRheumatol69:9-21.
83. ZhuoQ,YangW,ChenJ,etal.2012.Metabolicsyndromemeetsosteoarthritis.NatRevRheumatol
8:729-737.
84. AlbuquerqueD,SticeE,Rodriguez-LopezR,etal.2015.Currentreviewofgeneticsofhumanobesity:
frommolecularmechanismstoanevolutionaryperspective.MolGenetGenomics290:1191-1221.
85. BouchardC.2007.Thebiologicalpredispositiontoobesity:beyondthethriftygenotypescenario.
IntJObes(Lond)31:1337-1339.
86. AbranchesMV,OliveiraFC,ConceicaoLL,etal.2015.Obesityanddiabetes:thelinkbetweenadi-
posetissuedysfunctionandglucosehomeostasis.NutrResRev28:121-132.
87. UchidaK,SatohM,InoueG,etal.2015.CD11c(+)macrophagesandlevelsofTNF-alphaandMMP-3
areincreasedinsynovialandadiposetissuesofosteoarthriticmicewithhyperlipidaemia.ClinExp
Immunol180:551-559.
88. PelleymounterMA,CullenMJ,BakerMB,etal.1995.Effectsoftheobesegeneproductonbody
weightregulationinob/obmice.Science269:540-543.
89. UchidaK,UrabeK,NaruseK,etal.2009.Hyperlipidemiaandhyperinsulinemiainthespontaneous
osteoarthritismousemodel,STR/Ort.ExpAnim58:181-187.
90. MasonRM,ChambersMG,FlannellyJ,etal.2001.TheSTR/ortmouseanditsuseasamodelof
osteoarthritis.OsteoarthritisCartilage9:85-91.
91. FulcherJ,O’ConnellR,VoyseyM,etal.2015.EfficacyandsafetyofLDL-loweringtherapyamong
menandwomen:meta-analysisofindividualdatafrom174,000participantsin27randomisedtrials.
Lancet385:1397-1405.
92. KeeneD,PriceC,Shun-ShinMJ,etal.2014.Effectoncardiovascularriskofhighdensitylipoprotein
targeteddrugtreatmentsniacin,fibrates,andCETPinhibitors:meta-analysisofrandomisedcon-
trolledtrialsincluding117,411patients.BMJ349:g4379.
93. ClockaertsS,VanOschGJ,Bastiaansen-JenniskensYM,etal.2012.Statinuse isassociatedwith
reducedincidenceandprogressionofkneeosteoarthritisintheRotterdamstudy.AnnRheumDis
71:642-647.
94. IzadpanahR,SchachteleDJ,PfnurAB,etal.2015.Theimpactofstatinsonbiologicalcharacteris-
ticsofstemcellsprovidesanovelexplanationfortheirpleiotropicbeneficialandadverseclinical
effects.AmJPhysiolCellPhysiol309:C522-531.
95. ZhangO,ZhangJ.2015.Atorvastatinpromoteshumanmonocytedifferentiationtowardalterna-
tive M2 macrophages through p38 mitogen-activated protein kinase-dependent peroxisome
proliferator-activatedreceptorgammaactivation.IntImmunopharmacol26:58-64.
96. DenisGV,ObinMS.2013. ‘Metabolicallyhealthyobesity’:originsand implications.MolAspects
Med34:59-70.
97. NavarroE,FuntikovaAN,FitoM,etal.2015.Canmetabolicallyhealthyobesitybeexplainedbydiet,
genetics,andinflammation?MolNutrFoodRes59:75-93.
98. GreenMA,StrongM,RazakF,etal.2016.Whoaretheobese?Aclusteranalysisexploringsubgroups
oftheobese.JPublicHealth(Oxf)38:258-264.
99. ZhangY,PizzuteT,PeiM.2014.Anti-inflammatorystrategiesincartilagerepair.TissueEngPartB
Rev20:655-668.

Addendum figures 153
8
ADDENDUM FIGURES
COL1A1
FLS only +M1 CM +M2 CM0.0
0.5
1.0
1.5
2.0
Rel
ativ
eto
FLS
only
ASMA
FLS only +M1 CM +M2 CM0.0
0.5
1.0
1.5
Rel
ativ
eto
FLS
only
PLOD2
FLS only +M1 CM +M2 CM0
20
40
60
80
Rel
ativ
eto
FLS
only
*
Addendum figure 1Pro-inflammatoryM1macrophagessecretepro-fibroticfactors.Humanperipheralbloodmonocytes(pBMC)werestimulatedtoM1orM2phenotypeandconditionedmedium(CM)wasmade.Synovialfibroblasts(FLS)weretreatedwithM1orM2macrophageCMfor4days.RelativeexpressionofCOL1A1,ASMAandPLOD2inFLStreatedwith25%CM.GeneexpressionwasnormalizedtotheFLSonlyconditionperdonor.CMfrom3pBMCdonorswereusedtotreat3FLSdonors,witheachconditionperformedintriplicate(n=9).Valuesrepresentmean±SD.*p<0.05versusFLSonly.
COL2A1
TGFb1only
+PGF2a+AL8810
+CM +CM +AL8810
0.0
0.5
1.0
1.5
Rel
ativ
eto
TGF b
1on
ly
*
**
ACAN
TGFb1only
+PGF2a+AL8810
+CM +CM +AL8810
0.0
0.5
1.0
1.5
Rel
ativ
eto
TGF b
1on
ly
* **
MMP1
TGFb1only
+PGF2a+AL8810
+CM +CM +AL8810
0
2
4
6
8
Rel
ativ
eto
TGF b
1on
ly
*
*
*
MMP13
TGFb1only
+PGF2a+AL8810
+CM +CM +AL8810
0.0
0.5
1.0
1.5
2.0
2.5
Rel
ativ
eto
TGF b
1on
ly **
*
Addendum figure 2EffectofPGF2αonMSCchondrogenesis.ChondrogenicstimulatedMSCalginatebeadsweretreatedwithPGF2α,AL8810inhibitororCMfromIPFP.Rela-tive expressionofCOL2A1,ACAN,MMP1andMMP13 in chondrogenic stimulatedMSCalginatebeadsaftertreatment.TwopoolsofCMfrom3differentIPFPdonorseachpoolwereusedtotreat2MSCdonors,witheachconditionperformedintriplicate(n=6).Valuesrepresentmean±SD.*p<0.05versusnon-treatedcontrols.


Nederlandse samenvatting 155
NEDERLANDSE SAMENVATTING
Deknieheeftgewrichtsvlakkendiebedektwordendoorkraakbeen.Kraakbeenis
eenbindweefselmeteenelastischekarakter,hetzorgtervoordatdegewrichtsvlak-
kensoepeloverelkaarheenkunnenglijdenenhetgeeftschokdemping.Kraakbeen
kanbeschadigdrakenenindiendekraakbeenschadeniethersteldwordt,kandit
uiteindelijkleidentotartrose.Desymptomenvanartrosezijnonderanderepijn
enverminderdebewegelijkheid.Bijartroseisnietalleenhetkraakbeenaangetast
maarde gehele knie, inclusief het bot, ligamenten enhet synovium.Artrose is
niettegenezen;alleendesymptomenzijntebehandelen.Inheteindstadiumvan
artrosekanhetgehelekniegewrichtvervangenwordendooreenprothese.
Kraakbeenhersteltuitzichzelfnauwelijks.Ditkomtdoordathetgeenzenuwenen
geenbloedvatenbevat.Daarnaastbestaathetkraakbeenvooraluittussencelstof
enmaarvooreenkleingedeelteuitkraakbeencellen.Indienersprakeisvaneen
kraakbeendefect,isermomenteeleenaantalmethodesomhetdefectteherstel-
len.Demeest gangbare isdemicrofractureprocedure.Tijdensdezeprocedure
worden er gaten gemaakt in het bot onder het kraakbeen.Hiermeewordende
mesenchymalestamcelleninhetbeenmerggestimuleerdomhetkraakbeendefect
optevullenmetlittekenweefsel.
De resultaten van deze operaties kunnen door ontsteking negatief beïnvloed
worden.Ineenontstokenkniezijnerveelontstekingsfactorendieervoorzorgen
datstamcellennietgoedveranderennaarkraakbeencellenendaaromnietgoed
nieuwkraakbeenkunnenproduceren.De resultatenvandekraakbeenoperaties
kunnenooknegatiefbeïnvloedwordendoorobesitas.Bijobesitaszijndevetcel-
len vergroot. Daarnaast is ermeer infiltratie van ontstekingscellen, waaronder
macrofagen. Macrofagen zijn witte bloedcellen die een belangrijk rol spelen
inonsafweersysteem.Er zijn inhet lichaampro-inflammatoiremacrofagen en
weefselherstellende/anti-inflammatoiremacrofagen.Hetvetweefselisbijobesitas
ontstoken door onder andere een verhoogde infiltratie van pro-inflammatoire
macrofagenenscheidtdanookmeerontstekingsfactorenuit.Hetmeestevet in
hetlichaambevindtzichonderdehuid.Deontstekingsfactorenbereikendeknie
systemischviadebloedbaan.Echterindekniezelfbevindtzichookvetweefsel.
Hetgrootstevetweefsel indeknieishetinfrapatellairvetweefsel,ofwelHoffa’s
vetweefsel.HetHoffa’svetweefsel ligtdirect tegenhetsynoviumaan.Hetheeft
alsfunctieschokdempingenhethelpenverspreidenvansynovialevloeistof.Het
Hoffa’s vetweefsel kan ontstoken raken en daarbij stoffen uitscheiden die het
kraakbeenbeïnvloeden.

156 Nederlandse samenvatting
In Hoofdstuk 2beschrevenwijofhetHoffa’svetweefselookdaadwerkelijkveran-
derdisdoorobesitas.WijhebbendaarbijstukjesHoffa’svetweefselgebruiktvan
patiënten die een totale knieprothese kregen en stukjes onderhuids vetweefsel
vanpatiëntendieeen totaleheupprothesekregen.Wijanalyseerdendegrootte
vandevetcellenmethistologie.Obesitasleidttotvergrotingvandeonderhuidse
vetcellenenditiseenaanwijzingvoorvetweefselontsteking.Wijkondengeenver-
schilingroottevindentussenvetcellenvanhetHoffa’svetweefselvanpatiënten
met een body mass index (BMI) van <25kg/m2 en >30 kg/m2. Wij concluderen
hieruitdatdevetcelleninhetHoffa’svetweefselwaarschijnlijknietdoorobesitas
beïnvloedworden.DitsuggereertverderdathetHoffa’svetweefselniethetzelfde
isalsonderhuidsvetweefsel.
Obesitas iseenrisicofactorvoorartrose.Eenvandekenmerkenvanartrose is
stijfheid van het gewricht. Dit wordt deels veroorzaakt door fibrosering, ofwel
verlittekening van het synovium. Dit proces ontstaat doordat fibroblasten in
het synoviummeer fibrotischweefsel gaat produceren. De fibroblasten produ-
cerenmeerfibrotischweefseldooraanwezigheidvanontstekingsfactorenofeen
overdaadaangroeifactoren.HetHoffa’svetweefselligtindekniedirecttegenhet
synovium aan. Het synoviumwordt dusmogelijk continue beïnvloed door het
Hoffa’svetweefsel. InHoofdstuk 3hebbenwijbeschrevendat factorendiehet
Hoffa’svetweefseluitscheidtsynovialefibrosekanveroorzaken. Dithebbenwij
onderzochtdooreerstdefactorendiehetHoffa’svetweefseluitscheidtoptevan-
geninkweekmedium.Daarnahebbenwijfibroblastenuithetsynoviumgeïsoleerd
endeze gekweektmethet kweekmedium.Wij zagenhierbij datdefibroblasten
meer fibrotische eigenschappenontwikkelden.Wemerktenookopdat er geen
verschilwas ineffect tussenkweekmediumgemaaktvanHoffa’svetweefselvan
obese en van niet-obese donoren. Verder ontdekten we dat prostaglandine F2a
(PGF2a)uitgeschedendoorhetHoffa’svetweefselmedeverantwoordelijkisvoor
deze reactie.Ditbetekentdusdat eenprostaglandine remmer, zoals celecoxib,
mogelijkgebruiktzoukunnenwordenomontstaanvansynovialefibroseterem-
men.
WewetennudathetHoffa’svetweefselstoffenuitscheidtdathetkraakbeenen
synoviumbeïnvloeden.Indekliniekzijnderesultatenvankraakbeenherstelopera-
tiesnietoptimaal,wanterontstaateensoortlittekenkraakbeen.In Hoofdstuk 4
hebbenwijexperimentenuitgevoerdomtekijkenofhetHoffa’svetweefselook
stoffenuitscheidtdiedekraakbeenvormendecapaciteitvanstamcellenremmen.
Wijgebruiktenhetzelfdesoortkweekmediumwelkeweeerdergebruikthebben
voordesynovialefibroseexperimenteninHoofdstuk 3.Wijzagendatditkweek-

Nederlandse samenvatting 157
mediumkraakbeenvormendecapaciteitvanstamcellenremde.Verdervondenwij
geenverschilinhetremmendeeffectvanHoffa’svetweefseltussenobeseenniet-
obesedonoren,nochtussenartrotischeenpost-traumatischedonoren.Diteffect
waswelHoffa’svetweefselspecifiek,wantsubcutanevetweefselhadgeeneffect
opdestamcellen.Tenslottetoondenweaandatpro-inflammatoiremacrofagenin
hetHoffa’svetweefselbijdragenaanhetkraakbeenvormingremmendeeffectvan
hetHoffa’svetweefsel.Ditbetekentdusdatalswedenegatieveeffectenvanhet
Hoffa’svetweefselwillenverminderen,datweeenmedicijnmoetengebruikendat
depro-inflammatoiremacrofageninhetHoffa’svetweefselbeïnvloedt.
In Hoofdstuk 5probeerdenwevervolgensmetmedicijnenontstekinginhetHoffa’s
vetweefselteremmen.Wegebruiktencelecoxibentriamcinoloneacetonide,twee
vaak gebruikte ontstekingsremmers, en pravastatine en fenofibraat, twee vaak
gebruiktecholesterol-entriglyceridegehalteverlagersmetontstekingsremmende
effecten.WekweektenstukjesHoffa’svetweefselmetdeverschillendemedicijnen.
WevondendatalleentriamcinoloneacetonideontstekinginhetHoffa’svetweefsel
konverlagen.Daarnaastremdehetookspecifiekdepro-inflammatoiremacrofagen.
HierdoorwerdhetHoffa’svetweefselmindernegatiefvoorkraakbeenvormende
capaciteitvandestamcellen.VerderzagenwijookheteffectvanHoffa’svetweefsel
opsynovialefibroblastenveranderde.Ertradennamelijkkraakbeenafbraakpro-
cessenopsynovialefibroblasten.Hetlijkterdusopdattriamcinoloneacetonide
gebruiktkanwordenomspecifiekhetHoffa’svetweefseltemodulerennaareen
meervoorkraakbeenherstelgeschiktestaat.
Hetmeeste vetweefsel in het lichaambevindt zich onder de huid. Bij obesitas
isditonderhuidsevetweefselontstokenendeontstekingsfactorenwordensys-
temischuitgescheidenenbereikendanviadebloedbaandeknie.Hierdoorkan
kraakbeenschadeenuiteindelijkartroseontstaan.Daarnaastisditontstokenmi-
lieumogelijkmindergeschiktvoorkraakbeenhersteloperaties.Naastontsteking
speeltookmetaboleontregelingeenrolbijobesitasenhetontstaanvanartrose.
Omdecomplexeverschillendeveranderingeninobesitasteonderzoeken,ishet
noodzakelijkdierproevenuittevoeren.InHoofdstuk 6gebruiktenwijdeSTR/Ort
muizenstam,diespontaanobesitasenmetabole-eninflammatoireveranderingen
ontwikkelt.Dezemuizenkregengedurendeeenhalfjaardagelijkssimvastatineof
fenofibraatofeencombinatiehiervan.Ditzijntweevaakgebruiktecholesterol-en
triglyceridegehalteverlagersmetontstekingsremmendeeffecten.Naeenhalfjaar
kondenwe geen effect op kraakbeenschade vinden. Fenofibraat voorkwamwel
obesitas,verlaagdesystemischeontstekingenbotsclerose,maarkonkraakbeen-
schadenietvoorkomen.Tenslottewarenmetaboleinflammatoireveranderingen

158 Nederlandse samenvatting
indemuizennietgeassocieerdmethetontstaanvankraakbeenschade.Wijcon-
cludeerdenuitdezemuizenstudiedatobesitasenobesitasgerelateerdemetabole
eninflammatoireveranderingennietdirectdeoorzaakzijnvankraakbeenschade
indezemuizen.Voordepatiënt suggereertdit dat obesitasniet altijd leidt tot
kraakbeenschade.
Alseenobesepatiënteenmaalwelkraakbeenschadeheeft,ishetnoodzakelijkeen
kraakbeenhersteloperatieuittevoerenomdeprogressietotartrosetevoorkomen.
Op ditmomentworden obese patiënten in principe niet geopereerd omdat de
klinischeresultatenminderzijnbijdezepatiënten.Echterishetnognietduidelijk
ofdaadwerkelijkdekwaliteitvanhersteldekraakbeenbeïnvloedwordtdoorobe-
sitasenhoeditgebeurt.Wijhebbengeprobeerddezevraagtebeantwoordenin
Hoofdstuk 7.IndithoofdstukgebruiktenwijDBA/1muizen,waarvanbekendis
datzekraakbeenschadekunnenherstellen.Wijhebbendezemuizeneenhoogvet
dieetgevoerdwaar60%vandeenergieuitvetkomt.Daarnaastmaaktenweeen
kraakbeendefectinhunknie.Dezemuizenwerdendikker,maartegendeverwacht-
ingin,hersteldedegroepdieeenhoogvetdieetkregenbeterdandemuizendie
eencontroledieetkregen.Daarnaastontwikkeldedegroepdieeenhoogvetdieet
kregenookgeenartroseenhaddendemuizengeenmetaboleof inflammatoire
veranderingenopdelangetermijn.Wijconcludeerdennaaraanleidingvandeze
resultatendatresistentietegenhoogvetdieetgeïnduceerdemetaboleeninflam-
matoireveranderingenmogelijkgelinktisaanbeterkraakbeenherstel.Wijweten
nietprecieswelkemechanismeshierineenrolspelen,daarvoorismeeronderzoek
nodig.
Concluderend heb ik met het onderzoek beschreven in dit proefschrift aan-
getoonddathetHoffa’svetweefselniethetzelfde isalsonderhuidsevetweefsel.
HetHoffa’svetweefselvanpatiëntenmetartroseofknieschadescheidtfactoren
uitdiehetkniegewrichtenkraakbeenherstelkunnenbeïnvloeden.Indetoekomst
is het mogelijk met medicijnen het Hoffa’s vetweefsel te moduleren om zo de
gewrichtsomgeving te optimaliseren voor kraakbeenherstel. Verder hebbenwij
aanwijzingengevondendatobesitasnietaltijdleidttotartroseennietperdefinitie
negatiefisvoorkraakbeenherstel.Ombetertebegrijpenwaaromditverschillend
istussenobesepatiëntenzijnermeeronderzoekennodig.Wellichtkunnenwijin
detoekomsthierdoorooknieuwetherapieënvindenomartroseteverminderen
enkraakbeenherstelteverbeteren.

159
中文简介
盖软骨作为减震器,可以使膝盖平滑无痛的运动。软骨可能会受损,一旦受损就不
能恢复,最终可能导致膝关节骨性关节炎。膝关节骨关节炎不能治愈,但通过治疗
可以缓解其症状。在骨性关节炎末期,需要施行关节置换手术更换整个关节。
软骨损伤可以通过软骨修复手术来治疗。但是,炎症会影响手术的效果。在肥胖人
群的脂肪组织多于常人,大多数脂肪组织位于皮下,而且会发炎。在膝盖内部有不
小的一片脂肪组织,称为髌下脂肪垫或霍法氏脂肪垫。本论文的研究表明,这种脂
肪垫与皮下脂肪不同。霍法氏脂肪垫分泌因子可能对膝关节和软骨的修复具有负面
影响。这可能是PGF2α 因子的分泌和促炎性巨噬细胞的存在引起的。添加曲安奈德可
以部分抵消这种负面作用。这意味着将来可以使用药物来调节霍法氏脂肪垫,从而
改善膝关节软骨修复的环境。
除了研究霍法氏脂肪垫引起的炎症之外,本论文还研究了额外关节脂肪组织炎症对
关节疾病和软骨修复的影响。通过小鼠活体实验发现,肥胖和肥胖相关的代谢和炎
症变化并不总是导致软骨损伤,也不总是对软骨修复具有负面作用。研究实验提供
的证据表明,肥胖相关的全身效应对退行性关节疾病和软骨修复影响具有变化性。
关于肥胖,脂肪组织和软骨修复之间的关系的未来研究可以侧重于这种变化性以揭
示新的治疗靶点
中文简介


PhD portfolio 161
PHD PORTFOLIO
NamePhDStudent: WuWei
ErasmusMCDepartment: Orthopedics
ResearchSchool: Postgraduate SchoolMolecularMedicine (Mol-
Med)
PhDTime-span: February2012–December2015
Promotors: Prof.dr.G.J.V.M.vanOsch
Prof.dr.J.A.N.Verhaar
Co-promotor: Dr.Y.M.Bastiaansen-Jenniskens
PhD Training
Year Workload
(ECTS)
In-depth courses
Laboratoryanimalscience(ErasmusMCGraduateSchool)
BiostatisticalmethodsI:Basicprinciples(NIHES)
BiomedicalEnglishwritingcourse(MolMed)
Researchintegritycourse(ErasmusMCGraduateSchool)
BiomedicalEnglishWritingandCommunication(ErasmusMC
GraduateSchool)
ICRSFocusMeeting–TheKnee(ICRS)
Podium presentations
Statinsandfibratestopreventspontaneousosteoarthritis:an
invivostudyinmice
NVMB Meeting, Lunteren
Pro-inflammatorymacrophagesinHoffa’sfatpadreduces
chondrogenicpotentialofmesenchymalstemcells
NOV Jaarcongres, Rotterdam
The infrapatellar fat pad inhibits chondrogenesis of
mesenchymalstemcells
Molecular Medicine Day, Rotterdam
Obesitydoesnotnegativelyinfluencecartilagerepairinmice
NOV Jaarcongres, Rotterdam
2012
2013
2013
2014
2014
2014
2013
2014
2014
2015
4.02.02.00.34.0
1.0
1.0
1.0
1.0
1.0

162 PhD portfolio
PhD Training
Year Workload
(ECTS)
Theinfrapatellarfatpadfromdiseasedjointsinhibits
chondrogenesisofmesenchymalstemcells
ICRS World conference, Chicago, USA
Award for excellence in cartilage research
Theinfrapatellarfatpadofdiseasedjointsinhibits
chondrogenesisofmesenchymalstemcells
SEOHS 2015, Leiden
Best abstract nominee
Anti-chondrogenicandpro-cataboliceffectoftheinfrapatellar
fatpadcanbemodulatedbytriamcinoloneacetonide
ICRS World conference, Sorrento, Italy
Poster presentations
Statinsandfibratestopreventspontaneousosteoarthritis:
aninvivostudyinmice
Molecular Medicine Day, Rotterdam
Statinsandfibratesdonotaffectdevelopmentofspontaneous
osteoarthritisinSTR/Ortmice
OARSI World conference, Philadelphia, USA
PPARαsignallingreducessubchondralbonethickeningandinflammation,butdoesnotpreventcartilagedamageinSTR/
Ortmice
OARSI World conference, Philadelphia, USA
The infrapatellar fat pad inhibits chondrogenesis of
mesenchymalstemcells
Matrix Biology Europe Meeting, Rotterdam
HighfatdietacceleratescartilagerepairinDBA/1mice
Molecular Medicine Day, Rotterdam
Theinfrapatellarfatpadfromdiseasedjointsinhibits
chondrogenesisofmesenchymalstemcells
OARSI World conference, Seattle, USA
2015
2015
2016
2013
2013
2013
2014
2015
2015
1.0
1.0
1.0
1.0
1.0
1.0
1.0
1.0
1.0

PhD portfolio 163
PhD Training
Year Workload
(ECTS)
HighfatdietacceleratescartilagerepairinDBA/1mice
OARSI World conference, Seattle, USA
HighfatdietacceleratescartilagerepairinDBA/1mice
ICRSWorldconference,Chicago,USA
Teaching
Tutoraatfirstyearmedicalstudents
Supervisingthirdyearmedicalstudentsattendingtheminor
“OrthopedicSportsTraumatology”
SupervisingMasterstudentMolecularMedicine
Supervisingmedicalstudent
SupervisingJuniorMedSchoolStudents
Winner best presentation
Other
AnnaFondsgrant
Reviewerforinternationaljournals
Cartilage (2x)
Osteoarthritis and cartilage (2x)
Rheumatology
Journal of Biomedical Materials Research Part A
VisitingresearcherAOResearchInstitute
Davos, Switzerland
2015
2015
2012
2012-
2014
2014
2014
2014
2012
2013-
2015
2015
1.0
1.0
1.5
1.0
5.0
0.5
1.0
0.2
4.0
Total 43.3


List of publications 165
LIST OF PUBLICATIONS
1. Wei W,CaparS,KopsN,VerhaarJAN,ClockaertsS,VanOschGJVM,Bastiaan-
sen-JenniskensYM.Anti-chondrogenicandpro-cataboliceffectofinfrapatellar
fat pad and its residing macrophages can be modulated by triamcinolone
acetonide.Submitted.2017.
2. Wei W,Bastiaansen-JenniskensYM,SuijkerbuijkM,KopsN,BosPK,Verhaar
JAN,ZuurmondAM,Dell’AccioF,vanOschG.Highfatdietacceleratescartilage
repairinDBA/1mice.JOrthopRes.2017Jun;35(6):1258-64.
3. DeJongA,Klein-WieringaI,AndersenS,KwekkeboomJ,Herb-vanToornL,De
Lange-BrokaarB,VanDelftD,GarciaJ,Wei W,VanderHeideH,Bastiaansen-
JenniskensY,VanOschG,ZuurmondA,Stojanovic-SusulicV,NelissenR,Toes
R,KloppenburgM, Ioan-FacsinayA.LackofhighBMI-related features inadi-
pocytesandinflammatorycellsintheinfrapatellarfatpad.AcceptedArthritis
ResTher2017.2017.
4. RezaieW,Wei W,CleffkenBI,vanderVliesCH,RoukemaGR.InternalFixation
VersusHemiarthroplastyforDisplacedIntra-CapsularFemoralNeckFractures
inASA3-5GeriatricPatients.OpenOrthopJ.2016;10:765-71.
5. Wei W, RudjitoE, FahyN,Verhaar JA,Clockaerts S,Bastiaansen-Jenniskens
YM,vanOschGJ.Theinfrapatellarfatpadfromdiseasedjointsinhibitschon-
drogenesisofmesenchymalstemcells.EurCellMater.2015Dec02;30:303-14.
6. Siebelt M, Korthagen N,Wei W, Groen H, Bastiaansen-Jenniskens Y, Muller
C, Waarsing JH, de Jong M, Weinans H. Triamcinolone acetonide activates
ananti-inflammatoryand folate receptor-positivemacrophage thatprevents
osteophytosisinvivo.ArthritisResTher.2015Dec05;17:352.
7. Wei W, Clockaerts S, Bastiaansen-Jenniskens YM, Gierman LM, Botter SM,
Bierma-ZeinstraSM,WeinansH,Verhaar JA,KloppenburgM,ZuurmondAM,
vanOschGJ.Statinsandfibratesdonotaffectdevelopmentofspontaneous
cartilagedamageinSTR/Ortmice.OsteoarthritisCartilage.2014Feb;22(2):293-
301.

166 List of publications
8. FahyN,deVries-vanMelleML,LehmannJ,Wei W,GrotenhuisN,FarrellE,van
derKraanPM,MurphyJM,Bastiaansen-JenniskensYM,vanOschGJ.Human
osteoarthriticsynoviumimpactschondrogenicdifferentiationofmesenchymal
stem cells viamacrophage polarisation state. Osteoarthritis Cartilage. 2014
Aug;22(8):1167-75.
9. Bastiaansen-JenniskensYM,Wei W,FeijtC,WaarsingJH,VerhaarJA,Zuurmond
AM,HanemaaijerR, StoopR,vanOschGJ. Stimulationoffibroticprocesses
by the infrapatellar fat pad in cultured synoviocytes frompatientswith os-
teoarthritis:apossiblerole forprostaglandin f2alpha.ArthritisRheum.2013
Aug;65(8):2070-80.
10.Wei W, Akkersdijk GP. Spontaneous aneurysm of the superficial temporal
artery.Lancet.2011Jul09;378(9786):168.
11.Damen TH,Wei W, MureauMA, Tjong-Joe-Wai R, Hofer SO, Essink-BotML,
HoviusSE,PolinderS.Medium-termcostanalysisofbreastreconstructionsin
asingleDutchcentre:acomparisonofimplants,implantsprecededbytissue
expansion, LD transpositions andDIEPflaps. J PlastReconstrAesthet Surg.
2011Aug;64(8):1043-53.



About the author 169
ABOUT THE AUTHOR
WuWei(韦芜)wasbornonMay28th1986inSongzi,
Hubei,China. In1993hemoved to theNetherlands.
AfterobtaininghisVWOdiploma(ChristelijkLyceum
Delft,Delft),hestartedmedicalschoolattheErasmus
UniversityRotterdamin2004.Duringmedicalschool,
he spent a year as full time board member of the
Medical Student Association of Rotterdam (MFVR)
and was active in various other committees of the
study.HealsoworkedasanErasmusambassadorand
attheEmergencyDepartmentasastudent-assistant.
Furthermoreheparticipatedforseveralyearsinthe
ErasmusAnatomyResearchProject,whichincreased
hisenthusiasmforOrthopedics.
In2012heobtained thedegreeofMedicalDoctor. Subsequentlyhe startedhis
PhDprojectentitled‘Adiposetissueandtheknee:roleof inflammationonjoint
degeneration and cartilage repair’ at thedepartmentof orthopedicsunder the
supervisionofprof.dr.GerjoJ.V.M.vanOsch,prof.dr.JanA.N.Verhaaranddr.
YvonneM.Bastiaansen-Jenniskens.
FromJanuary2016tillJune2017,Wuworkedasaresident(VAIOS)attheDepart-
mentofSurgeryattheReinierdeGraafGasthuisinDelft(underthesupervision
ofdr.MaartenvanderElstanddr.MarkR.deVries).FromJuly2017onwardshe
isaresident(AIOS)attheDepartmentofOrthopedicsinErasmusMCUniversity
MedicalCenterinRotterdam(supervisionbydr.PieterK.Bos)
Besideshiswork,Wuenjoysrunning,cycling,foodandcooking.


Dankwoord 171
DANKWOORD
Erwordtaltijdgevraagdofjeietsopnieuwhadwillendoenalsjewederomvoor
dezelfdekeuzestaat.Mijnantwoordopdevraagofikopnieuwvooreenpromo-
tietrajectzouhebbengekozen,isvolmondig“JA!”.Devierjareninhetlabopde
16ezijnvoorbijgevlogen.Ditproefschriftwasnooittotstandgekomenzonderde
steunvananderen.Hierbijwilikinhetbijzondereenaantalpersonenbedanken.
Allereerstmijneerstepromotorprof.dr.VanOsch.BesteGerjo,alinhetvoorjaar
van2010liepikbijjenaarbinnenomtekomenpratenovermijnkeuzeonderzoek.
Ikhadnauwelijkseenideewatfundamenteelwetenschappelijkonderzoekinhield,
nochwatertedoenwasophet lab.Naeenhalfjaar intensievebegeleidingvan
jouenYvonne,wasikheelblijdatjemijdekansboodomeenpromotietrajectte
starten.Jewasaltijdheellaagdrempeligtebereikenvooroverleg,hoedrukjehet
ookhad.Daarnaastwasernogietswaarjeookaltijdtijdvoorvrijmaakte:jouw
goudvissen.Tijdens jeafwezigheidwerdencompleteschema’sopgesteldomte
zorgendatzenietovervoerdwerden.IkvondhetleukdatjeonzegoudvisSep(je
noemdehemmini-Wu)wildeadopteren.Helaasheefthijdefinishvanditboekniet
gehaald.Gerjo,ikbenblijendankbaarjoualspromotortehebben.
Daarnaastmijntweedepromotor,prof.dr.Verhaar.BesteprofessorVerhaar,dank
udatumijdekansgegevenhebtompromotieonderzoektedoenopdeafdeling
orthopedie.Metuwuitgebreidekennisuitdekliniek,hadualtijdkritischevragen
overmijnonderzoek.Uheeftmijgeleerdénuitgedaagdbasaalwetenschappelijk
onderzoekzoklinischrelevantmogelijktemaken.Ikkijkernaaruitommeervan
utelerenindekliniek.
Dr. Bastiaansen-Jenniskens,mijn co-promotor Yvonne. Door de zeer intensieve
begeleidinghebikveelvandefundamenteletechnischezakenvanhetlabvanjou
geleerd.Veelvanjouwwerkvormdedebasisvanditboek.ZelfsviadeWhatsApp
kondenwijhetvaakhebbenoverversedata.Ookbuitenhetwerkhebikveellol
metjegehadmetdedoorjougeliefdeslechteHousemuziek.Naalhetintensief
samenwerkenbenikblijdatiknietjouwvoorkeurvoorrozehebovergenomenen
datjijnietAziaatbentgeworden.
Besteprof.dr.Hazes,prof.dr.Bulstraendr.Emans,ledenvandekleinecommissie.
Hartelijk dank voor het kritisch lezen en beoordelen van dit proefschrift. Dear
prof.dr.Dell’Accio,thankyoufortakingtimetovisitusfromtheUK.Ithankyoufor
teachingmethecartilagedefectmodelandforyourinputandsharingyourview

172 Dankwoord
oncartilagerepair.Prof.dr.VanSaase,prof.dr.Kleinrensinkendr.VanLent,dank
vooruwbereidheidomplaatstenemenindegrotecommissie.
Dr.Clockaerts, beste Stefan, jouwwerk vormde samenmetdat vanYvonnede
basisvoormijnproefschrift.Dankvoorjevoorwerkzodatikdirectkoninstromen.
Wiekonbedenkendaternogzoveelonderzoekuitgevoerdzouwordenoverdat
enestukjevetindeknie?DefilosofeersessiestijdensdeICRScongressenwaren
zeerinspirerendenhopelijkkunnenweindetoekomstnogietssamenopstarten.
Daarnaastwilikdeanderesenioronderzoekersenstafledenvandeafdelingortho-
pediegraagbedanken.Julliewarenaltijdbereidkritischnaarmijnonderzoekte
kijkenenactiefweefselteverzamelen.Devolgendepersonenwilikhierbijspeciaal
benoemen.Bestedr.Bos,vanafhetbeginhebbenwevaakmetGerjogebrainstormd
overmijnpromotieonderzoek.Dankvoorjeideeënhierbij.Max,trouweAjacied,
dankvoorjekritischeblikopmijnmaniervanpresenteren.Erwin,statistiekblijft
bijzonder.Ikwaardeerheelergjevisiehierin.
Graagwilikalleco-auteursbedankenvoorhunexpertiseeninzet,waarbijikde
volgendespeciaalwilbenoemen.LobkeGiermanenAnne-MarieZuurmond,jullie
warenmijngroteTNO-hulplijnen.Jullieexpertise inhigh-fat-dietheeftonverwa-
chteinzichtenopgeleverd.Ikkijknooitmeerhetzelfdenaardikkemuizen.Sander
Botter,bedanktvoorhetdelenvanjeexpertiseinmicro-CTensubchondraalbot
bijvroegartrose.DearNiamh,talkingaboutresearch,macrophagesandgingers
came‘handinhand’withyou.GoodtoseeyouinHollandagain!Resti,youwereso
organizedandpreciseinyourwork.YourMasterprojectmadechapter4possible.
GoodluckinSwedenwithfinishingyourownPhD.Mathijs,ikhebnooitbegrepen
waarjealletijdvandaanhaaldeomallestegelijktedoen,maarhetisjeallemaal
gelukt.Wesprekenelkaarnog indekliniek.Dear John, fellowHoffaenthusiast!
Maybeinthefuturewecanreallystartafanclub?Thankyouforyourcontribu-
tion!Serdar,thanksforculturingtheHoffaandperformingtheFACSanalysisand
goodluckwithfinishingyourownPhD!
Het‘analistentrio’Nicole,WendyenJanneke.Julliezijndevastekrachtenvanhet
lab.Altijdontspannendevenbij tepraten in julliekantoor/kamer/hok.Janneke,
bedanktvoordegezelligemomentenindeML2tijdenshetveleverversen.Wendy,
jijhebtditgroentjeveelbegeleidtijdenshetpipetteren.Aanheteindkonikhet
bestgoed,alzegikhetzelf.Nicole!Hetisjammerdatjenietinhethistologiehok
kuntsnijden,terwijljeaanhetinternetshoppenbentbijdeBijenkorf,zonderde

Dankwoord 173
cakevandeweektemissen,voordeparaffinemachine.Dankvoorhetsnijdenvan
aldieknietjesenuitvoerenvanvelekleuringen.
Sandra,altijdvrolijk.Zonderjouwashetquaformulierennietgoedgekomenbij
mij.Ikbendankbaardatjijmijviademailstructuurhebtgegevenaandeafgelopen
periode.
Theforeignseniorsofthelab.Roberto,Iwastherewhenyoudidyourfirstmara-
thonandonedayyou,MaartenandIwilldoanotheronetogether!Keepupthe
goodworkanddon’tforgettoeatlesswhennotrunning.Eric,thankyouforyour
wisdomaboutFACS,bone,wineandcuredham.Kavitha,gratefulforyouradvice
inthelastmonthsofmytimeinthelab.
Aanallecollegapromovendiopde16e:Callie,Johannes,Marloes,Nienke,Mieke,
Johan,Jasper,Michiel,Anna,Panithi,Rintje,Marjan,Mairéad,Marianne,Lizette,
Caoimhe, Shorouk, Simone, Sohrab en Laurie. Bedankt voor de samenwerking,
koffiedrinken,labdays,cakevandeweek,cursussen,borrels,inpakkenvanmijn
bureau inaluminium folie, selfies,collages,congressen inAmerikaen leerzame
tijd.Deklinischecollega’sookbedanktvoordegezelligheid.
Collega’svandechirurgieinDelft,gedurendedevooropleidingbenikeenéchte
doktergeworden.Hetwaseenwarmbadomintestarten.Ikhebmetpleziermet
julliegewerkt,inclusiefdevoetenpolienproctopok.Dankvoordezeerleerzame
tijdendeskireis.
TeamWhiskey,mijnstudievrienden,waarvaneenkleinedelegatieuiteindelijkook
indetorengepromoveerdisofgaatpromoveren.Ikhoopdatweonzevriendschap
zullenblijvenvoortzettenmetregelmatigetentjes,reizen,festivalsenfietsen.De
SV-mannenenoud-CLD’ersvandeKEB-groep:jullievormdeneenbelangrijkebron
vanafleidingtussenhetschrijvenenpipetterendoor.Niek,denkendeaanhetoude
Sintineltijdperk,wilikjehierbijspeciaaldankenvoordemooieomslag.
ChrisenMaarten:deeenkonzijnbenen inzijnnek leggen,deanderhadhaar
totzijnschoudersenikhadietsmeerwekedelen.Vroegerstondenwemetveel
bierbijGoldfishvooraan,tegenwoordiggewoonrustigmeteenwijntjeaantafel.
Maarten,metjoubenikin2011tegelijkmetdatpipetterenbegonnen,destartvan
eengeweldigeperiode.Eenmuurwasnietdikgenoegomonstescheiden.ikben
blijdatweookdevolgendestapvanonzecarrièretotorthopedischchirurgsamen
kunnenvolgen.Bedanktdatjemijnparanimfwilzijn.

174 Dankwoord
MijnschoonzussenLisaenMalou.Lisa,altijdaanhetlachenengeïnteresseerdin
watikaanhetdoenben.Onzediscussieszijnsomsfel,maardatmaaktmijook
weerscherp.JijenJoosthebbeneenprachtigdochter,Evi.Ikbenblijdatikvoor
heteerstoomgewordenben!Malou,dekleinesportieveling.Jewordtonderschat
doorjelengte,maarzwemmendinhetwater,rennendophetlandenrijdendopde
fiets,benjesupersnel.MisschienzelfsietssnellerdanMichiel?Datpromoveren
gaatjounatuurlijkmakkelijklukken!
Lieve schoonvader Jos, op geneeskundig vlak ben jemisschien een leek,maar
desondanksvindikdatjetochveelvanhetmedischeafweet.Misschienookwel
doordatweaantafelalleenmaarhieroverkunnenpraten.Omditgoedtemaken
zijnerweltweeinjegeliefdestadgepromoveerd,echterdederdemoetjehelaas
aandeconcurrentoverlaten.Jebenteenfijnenzachtpersoonenaltijdwelkom
bijons.LieveschoonmoederJosé,jewasaltijdgeïnteresseerdinwatikdeeden
vroegmijdeorenvanhetlijf.Doorjebetrokkenheidvoeldeikmealsnelthuisbij
jullie.Ikzaljeblijvenherinnerenalseenliefdevolpersoon.
Mijn lieveouders,omdatChineesbinnenonsgezindevoertaal is,zal ikverder
gaan in het Chinees.我亲爱的爸妈,谢谢你们让我成长在这么温暖又充满爱的家庭
里。你们俩一直希望我能够生活幸福事业顺利。妈,你经常说作为一个中国父母,
孩子是最重要的。一直到现在,无论我做什么你们都无条件地支持和帮助我。爸,
我现在跟你一样也是博士了,能够引用你的论文并且由你来当我的paranimf,我十
分高兴也非常很骄傲。 除了你们,我也想用这个机会感谢我的全部家人和其他好
友。谢谢你们一直以来对我的照顾与关心,以及对我完成博士论文的支持与鼓励。
MijnallerliefsteMyrthe.Jijbentdemeestveerkrachtigeensterkstepersoondie
ikken.Naalleswatdeafgelopenjarengebeurdisenhoegestrestenchagrijnigik
ookwas,jijbleefaltijdsuperliefengeduldig.Alsstelzijnwijsomseencomplete
chaos,maarmeestalvoelenwijelkaarheelgoedaan.Watweooksamendoen,de
tijdvliegtveeltesnelvoorbij.Ikbenheelgelukkigdatjijinmijnlevenbentenik
weetdatwijeraltijdvoorelkaarzullenzijn.Ikhouvanje.


A D I P O S E
T I S S U E
A N D T H E
K N E E
AD
IP
OS
E T
IS
SU
E A
ND
TH
E K
NE
E
Role of inflammation on joint
degeneration and cartilage repair
Wu Wei
Wu
We
i