Wrist/Hand Sports med 2. Articulations Radiocarpal – Flexion, extension, abduction, and...
28
Wrist/Hand Sports med 2
-
Upload
georgia-lewis -
Category
Documents
-
view
228 -
download
1
Transcript of Wrist/Hand Sports med 2. Articulations Radiocarpal – Flexion, extension, abduction, and...

Wrist/Hand
Sports med 2

Articulations• Radiocarpal
– Flexion, extension, abduction, and circumduction• Carpal
– Gliding joints– Stabilized by anterior, posterior, and connecting
ligaments• Metacarpal
– Flexion, extension, abduction, adduction, circumduction
• Phalangeal– Hinge joints– Proximal interphalangeal (PIP), Distal
interphalangeal (DIP)

Ligaments
• Wrist– Ulnar Collateral ligament• Ulna to pisiform
– Radial collateral ligament• Radius to scaphoid
– Transverse carpal ligament• Roof of the “carpal tunnel”
• Phalanges – Collateral ligaments

Muscles• Flexors– Palmar surface– Flexor digitorum superficialis, flexor
digitorum profundus• Extensors– Dorsal surface– Extensor digitorum longus,
• Intrinsics– Abduction and adduction

Blood/Nerve Supply
• Nerves– Ulnar, radial– Median• Enters palm through carpal tunnel
• Arteries– Radial– ulnar

Assessment
• History– MOI– Location and type of pain?– Increases or decreases pain?– History of trauma or overuse?– Any therapy given in the past?

Assessment
• Observations– Hand usage like writing, unbuttoning shirt– Open and close hand• Fully? Rythmically?
– Touch thumb to each fingertip– Flat knuckle– Color of fingernails• Pale= poor circulation

Assessment• Palpations– Bony
• Scaphoid (anatomical snuffbox)
• Lunate• Hamate (hook)• Metacarpals• Phalanges (proximal,
middle, and distal)
– Soft• Triangular fibrocartilage
(TFCC)• Collateral ligaments of
phalanges• Flexor and extensor musclesUse hand flashcards for palpation practice

MMTs• Flexion• Extension• Ulnar deviation
– 5th digit moves towards ulna
• Radial Deviation– Thumb moves towards
radius
• Finger Abduction – Fingers spread out
• Finger Adduction– Fingers back together
Perform Active, passive, resistive of all movements on ALL fingers

Tenosynovitis
• MOI– Repetitive use and overuse of tendons and their
sheaths• S/S– Pn with use, pn w/passive stretching– Tenderness, swelling over tendon
• TX– Ice massage, NSAIDS, rest– ROM, contrast baths, US, PRE

Carpal Tunnel Syndrome
• MOI– Inflammation in the carpal tunnel, compresses
median nerve– Repeated flexion, or direct blow
• S/S– Tingling, numbness, weakness
• TX– Rest, immobilization, NSAIDS– Possible surgery

Finkelsteins Testtests for de Quervain’s disease
• Procedure– Athlete is sitting, forms a
fist around the thumb.– Examiner grasps the
athlete's forearm and fist and ulnarly deviates
• Positive Test– Pn. = Possible
tenosynovitis (de Quervain’s disease)
– Pn. At carpal tunnel = carpal tunnel syndrome
http://youtu.be/lXV_UV62USc

Phalens Test
• Procedure– Have athlete flex both
wrists as far as possible and press together for 1 minute
• Positive Test– Pn. At the carpal tunnel
= carpal tunnel syndrome
http://youtu.be/DZ9UGuA8oAE

Wrist Sprains (most common)
• MOI– Falling on hyperextended wrist– Violent flexion or torsion
• S/S– Pn, swelling, decreased AROM
• TX– RICE, splinting, analgesics– Tape, strengthening

Gamekeepers Thumb
• MOI (skiiers, tacklers)– Sprain of UCL ligament of MCP joint of thumb– Forceful abduction with hyperextension
• S/S– Pn, weak pinch, – Tenderness and swelling
• TX– Refer– Splint 3 weeks

Glide Test
• Procedure– Grasp the athletes wrist
with one hand and their carpals with the other
– Move anterior/posterior and radial/ulnar directions
– Can also do on each phalange/metacarpal joint
• Positive Test– Pn./laxity = sprain
http://youtu.be/YrJ98IYsgBw

Valgus/Varus
• Procedure– Examiner maintains
stabilization of the proximal bone between the thumb and forefinger and grasps the distal bone
– Examiner provides a valgus/varus force
• Positive Test– Pn./laxity = collateral
ligament tear/sprain

Triangular Fibrocartilage Complex Injury (TFCC)
• MOI– Forced hyperextension
• S/S– Pn along the ulnar side of wrist– Extension = pn, difficulty– Swelling later on
• TX– refer
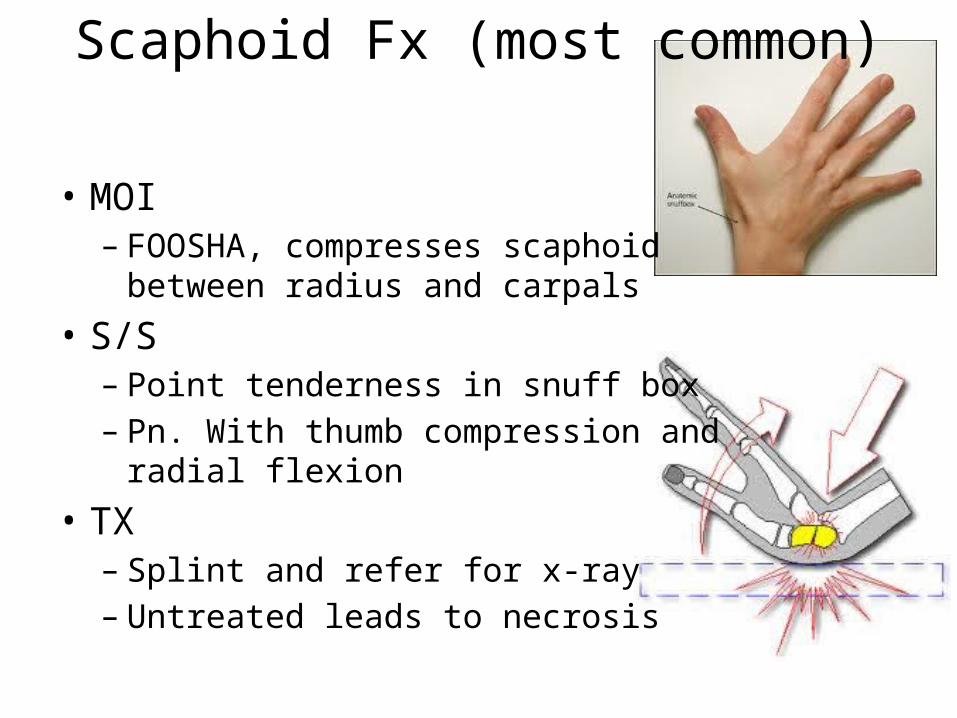
Scaphoid Fx (most common)
• MOI– FOOSHA, compresses scaphoid between radius
and carpals• S/S– Point tenderness in snuff box– Pn. With thumb compression and radial flexion
• TX– Splint and refer for x-ray– Untreated leads to necrosis

Hamate (hook) Fx
• MOI– Direct blow from racket, bat, sports stick, club
• S/S– Wrist pn and weakness– Point tender
• TX– Refer for x-ray– Doughnut pad

Colles Fx
• MOI– Fx to distal end of radius or ulna– FOOSHA, or hyperextension
• S/S– Visible deformity– Swelling and pn
• TX– Ice and splint– refer

Boxers (5th metacarpal) Fx
• MOI– Direct axial force (punching)– Getting stepped on
• S/S– Pn and swelling
• TX– RICE, analgesics, refer– Splint 4 weeks, early ROM

Compression Test
• Procedure– Athlete has finger extended– Examiner holds the distal
phalanx and applies compression along the axis of the bone of the finger being tested
– Can also be done on metacarpal in fist position
• Positive Test– Pn at injury site = possible
fx

Allens Test
• Procedure– Athlete squeezes hand into a
fist and fully opens hand 3-4 times
– With athlete holding the last fist the evaluator puts pressure over radial and ulnar artery
– Athlete opens hand (appears white), evaluator releases 1 artery and the hand should become red
• Positive Test– Not turning red instantly =
radial or ulnar artery compromise
http://youtu.be/jq0ai5uXx68

Mallet Finger
• MOI– Direct blow to extended finger
• S/S– Pn at DIP– unable to extend finger
• TX– RICE– Splinted 24 hr/day, 6-8 weeks

Boutonniere Deformity
• MOI– Trauma forcing the DIP into extension and PIP into
flexion• S/S– Pn and inability to extend the DIP– Swelling, obvious deformity
• TX– Ice– Splint PIP in extension5-8 weeks– Flex distal phalanx
Jersey Finger
• MOI– Most often in the ring finger– Grabs a jersey, ruptures flexor tendon
• S/S– DIP joint cant be flexed– Finger stuck in extension
• TX– No surgery = never flex DIP again– Surgery = 12 weeks of rehab

Tap/Percussion Test• Procedure– Athlete extends affected
finger– Evaluator applies a firm
tap to the end of the finger
• Positive Test– Pn. At injury site =
possible fx