
(WP)HIN/ICP/IER/3.4/001/HIN English only - WHO … · 2012-03-01 · duplications result in data...
64
-
Upload
nguyenkhuong -
Category
Documents
-
view
213 -
download
0
Transcript of (WP)HIN/ICP/IER/3.4/001/HIN English only - WHO … · 2012-03-01 · duplications result in data...

(WP)HIN/ICP/IER/3.4/001/HIN English only
Report series number: RS/2006/GE/24(PHL)
REPORT
WORKSHOP ON DEVELOPING INTEGRATED NATIONAL HEALTH INFORMATION SYSTEMS
Convened by:
WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR THE WESTERN PACIFIC
Manila, Philippines 6 to 8 September 2006
Not for sale
Printed and distributed by: World Health Organization
Regional Office for the Western Pacific Manila, Philippines
November 2006

SUMMARY
The Workshop on Developing Integrated National Health Information Systems was held in Manila, the Philippines from 6 to 8 September 2006.
The objectives of the workshop were:
(1) to review the content and flow of data collected by different programme-specific information systems; and
(2) to agree on common platforms to integrate programme-specific information, for sharing and use.
Thirty participants from Cambodia, China, the Lao People’s Democratic Republic, Mongolia, the Philippines and Viet Nam, participated in the workshop. The participants represented a variety of health system disciplines and programmes such as planning and health information; communicable disease control; Expanded Programme on Immunization; tuberculosis control; sexually transmitted infections including HIV/AIDS; malaria; maternal and child health; and hospital services. In addition, three resource persons from the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM), the Global Alliance for Vaccine Immunization (GAVI), and the Health Metrics Network (HMN) also participated.
The activities conducted during the workshop included presentations on HIS integration and a framework for it, country presentations covering seven different programmes, group work, and plenary sessions. For the group work sessions, participants were arranged by country and were asked to identify issues related to the integration of data collection, sharing and use, as well as the integration of resources and the development of the corresponding policies and regulations. At the third group work session, each country developed an action plan for prioritized activities.
Outputs of the workshop identified HIS functional areas for integration and issues that countries faced. Key steps for countries to plan and implement integration of HIS were identified as:
(1) the establishment of a mechanism to coordinate HIS integration. The importance of leadership and commitment to this process was emphasized;
(2) integration of information between sub systems (between different public health programmes), and with information pertaining to finance were identified at each of the HIS functions , data collection, data management, data analysis and use;
(3) the need for HIS units/division to use opportunities offered by initiatives like GFATM and GAVI to collaborate in the integration of information that is used for these activities, given their substantial interest to enhance the M&E of their programmes in country. Some activities in country for this work are:
a. Involvement of HIS units (and those responsible for monitoring and evaluation) very early in the proposal building stage for GFATM as well as in proposal negotiations. Likewise, HIS should be involved in developing the proposals for GAVI.

b. Inclusion/incorporation of the HMN assessment in countries and subsequent strategic plans into existing HIS development plans funded by other donors. This would reduce overlap and duplication of efforts.
c. Integration of country HIS proposals to GFATM, GAVI and HMN. This is best done under a country NHIS strategic plan.
At the workshop, the outputs of the country action plans indicated high priority given to integration of data collection and sharing. Countries identified a number of areas for opportunity to integrate HIS such as:
(1) Integration of data collection methods especially where data collection occurs at a single site (facility or outpost) or for the same target groups.
(2) Data sharing, at district, provincial and national levels were identified to be opportunities for integration of resources, skilled staff in data management, analysis and interpretation. Technology, where available could enhance such integration, especially the use of data warehousing.
(3) Integration in the use of information was not given high priority by country groups. But in the country presentations, opportunities for such activity were mentioned. For example, in Cambodia the annual forum, for joint review of performance (JAPR) provides such an opportunity.
(4) A gap in the HIS in many countries, discussed in the plenary, was the lack of integration of information from the private health sector. As the private sector is expanding in a number of countries in the region, this was seen as an area of concern for NHIS.
(5) The integration of information from population surveys to supplement routine information provides means to reduce the load of data collection.
(6) Opportunities for HIS integration also occur in situations where service delivery is integrated.
As a first step to the integration process, it was agreed that it is important for countries to identify on their own priorities, obtain commitment to initiate integration, plan for such activities (using the NHIS strategic plans to be developed) and pursue it given the resources and opportunities currently available.

CONTENTS
Page 1. INTRODUCTION................................................................................................................. 1
1.1 Objectives ..................................................................................................................... 1 1.2 Participants and resource persons ................................................................................. 1 1.3 Organization ................................................................................................................. 1 1.4 Opening remarks........................................................................................................... 2 1.5 Appointment of Chairperson, Vice-Chairperson and Rapporteur ................................ 2
2. PROCEEDINGS ................................................................................................................... 2
2.1 Rationale for the development of an integrated national
health information system (NHIS)................................................................................ 2 2.2 Framework for the development of integrated NHIS ................................................... 3 2.3 Country experiences on integration .............................................................................. 7 2.4 Integrating the information needs of global initiatives............................................... 10 2.5 The Health Metrics Network and its role in the development
of an integrated NHIS................................................................................................. 10 2.6 Integrating demographic data, vital statistics, special studies
and sample surveys..................................................................................................... 11 2.7 Identification of issues related to integration.............................................................. 11 2.8 Country Action Plans.................................................................................................. 12
3. CONCLUSIONS................................................................................................................. 12
ANNEX 1 - LIST OF PARTICIPANTS, TEMPORARY ADVISER, CONSULTANTS, OBSERVERS AND SECRETARIAT...................15
ANNEX 2 - PROGRAMME OF ACTIVITIES........................................................21 ANNEX 3 - PRESENTATION OF DR ROHAN JAYASURIYA,
CONSULTANT FOR THE WORKSHOP ON DEVELOPING INTEGRATED NATIONAL HEALTH INFORMATION SYSTEMS................................................................23
ANNEX 4 - OUTPUTS OF GROUP WORK SESSION 1.......................................31 ANNEX 5 - OUTPUTS OF GROUP WORK SESSION 2.......................................41 ANNEX 6 - OUTPUTS OF GROUP WORK SESSION 3.......................................51

1. INTRODUCTION
The Workshop on Developing Integrated National Health Information Systems (NHIS) was convened by the World Health Organization, Regional Office for the Western Pacific in Manila, the Philippines from 6 to 8 September 2006. The workshop focused on the integration of data collection, sharing and use by health and information subsystems. The weak integration of data has long been identified as a problem in developing countries, and has often led to the development of several parallel data collection and reporting systems in a country. Such duplications result in data inconsistency, increased reporting burden for staff, inefficient use of resources, and poor sharing and use of information across programmes.
The workshop was identified as a key component of the Regional Strategic Plan for Health Information Systems for 2006–2010, which was endorsed in November 2006.
1.1 Objectives
(1) To review the content and flow of data collected by different programme-specific information systems.
(2) To agree on common platforms to integrate programme-specific information for sharing and use.
1.2 Participants and resource persons
Thirty participants from Cambodia, China, the Lao People's Democratic Republic, Mongolia, the Philippines and Viet Nam participated in the workshop. The participants represented a variety of health system disciplines and programmes including planning and health information, communicable disease control, Expanded Programme on Immunization (EPI), tuberculosis (TB) control, sexually transmitted infections (STI) including HIV/AIDS, malaria control, maternal and child health (MCH), and hospital services.
Representatives from the Global Alliance for Vaccine Immunization (GAVI); the Global Fund to Fight Aids, Tuberculosis and Malaria (GFATM); and the Health Metrics Network (HMN) also participated in the workshop. Other attendees included the WHO secretariat from the Regional Office and country office staff in charge of health information systems (HIS). The list of participants is in Annex 1.
1.3 Organization
The workshop included presentations on the need for HIS integration and a framework for it, country presentations covering seven different programmes, group work sessions, and plenary sessions. For the group work sessions, participants were arranged by country and were asked to identify issues related to the integration of data collection, sharing and use, as well as the integration of resources and the development of the corresponding policies and regulations. During the third group work session, each country developed an action plan for prioritized activities. The programme of activities is presented in Annex 2.

- 2 -
1.4 Opening remarks
Dr Richard Nesbit, Acting Regional Director for the Western Pacific Region, welcomed the participants to the workshop. Dr Shigeru Omi, Regional Director, was on leave.
In his message, Dr Nesbit stressed that WHO has prioritized the integration of information systems in its Regional Strategic Plan for Health Information Systems for 2006–2010. He cited the following reasons for integration: the advent of global initiatives such as GFATM, GAVI and HMN, all of which share the same goal of promoting better use of information and knowledge in decision-making; the greater interest in closely monitoring country programmes that address cross-cutting issues such as equity, gender and poverty alleviation; and the proliferation of country-level data collection systems that have their own data collection tools, require their own software, and set their own reporting requirements that are often not coordinated with one another.
He likewise underscored the difficulties in integrating information systems, especially since the challenges were not purely technical, but were more political and organizational. He identified three important challenges that need to be addressed in integrating information systems: (1) the design of the system itself; (2) constant and open communication among the integrated units; and (3) the funding mechanism.
He closed his message by expressing his confidence that the workshop objectives would be achieved, given the expertise and experience of the participants, but stressed the need for follow-up actions at country level.
1.5 Appointment of Chairperson, Vice-Chairperson and Rapporteur
Ms Charity Tan of the Philippines was appointed Chairperson, Dr Sao Sovanratnak of Cambodia as Vice-Chairperson, and Dr Cheng Shiming from China as Rapporteur of the workshop.
2. PROCEEDINGS
2.1 Rationale for the development of an integrated national health information system
Dr YC Chong, Regional Adviser on Health Information, made a presentation on the rationale for the development of an integrated NHIS. He began by defining HIS integration as the process of combining different components of HIS so that they function in a more coordinated and unified manner. Integration can occur among various information subsystems, e.g. between nutrition and MCH (for breastfeeding data), or between TB control, communicable disease control, STI including HIV/AIDS, and hospital or curative services (for tuberculosis data). Integration can take place in any of the following areas: contents (indicators/information); data management (use of information technology); organization support; training/capacity-building; data dissemination (use of a central repository); and donor inputs (resource sharing).
Dr Chong identified the following reasons for integration:
(1) The emergence of several forms of monitoring and evaluation (M&E), often a result of donor funded projects, can lead to a plethora of indicators and duplication of data collection activities.

- 3 -
(2) The lack of awareness of health workers and programme managers concerning the information other programmes are collecting can hinder the sharing of information.
(3) There is a growing interest in comparative performance assessments in health, such as benchmarking or performance-based assessment.
(4) Concern is growing about data availability and data quality within and between countries.
(5) There are challenges in collecting, evaluating and interpreting indicator data to guide policy-making.
Four key challenges of HIS integration work were identified:
(1) matching up the policies, requirements and resources of donors with those of the country supported;
(2) networking among related stakeholders for active process of collaboration;
(3) contributing to an HIS comprehensive plan, and responding to the information needs of all concerned under one organization; and
(4) implementing a consistent, coherent and non-redundant HIS.
Dr Chong further emphasized that integration involves not only negotiating, discussing and working with many stakeholders and partners over time, but also building alliances where interests are articulated. At the same time, constraints and diverse perspectives must be acknowledged and addressed.
A key component for success is the establishment of leadership and policy to direct the activities.
2.2 Framework for the development of integrated NHIS
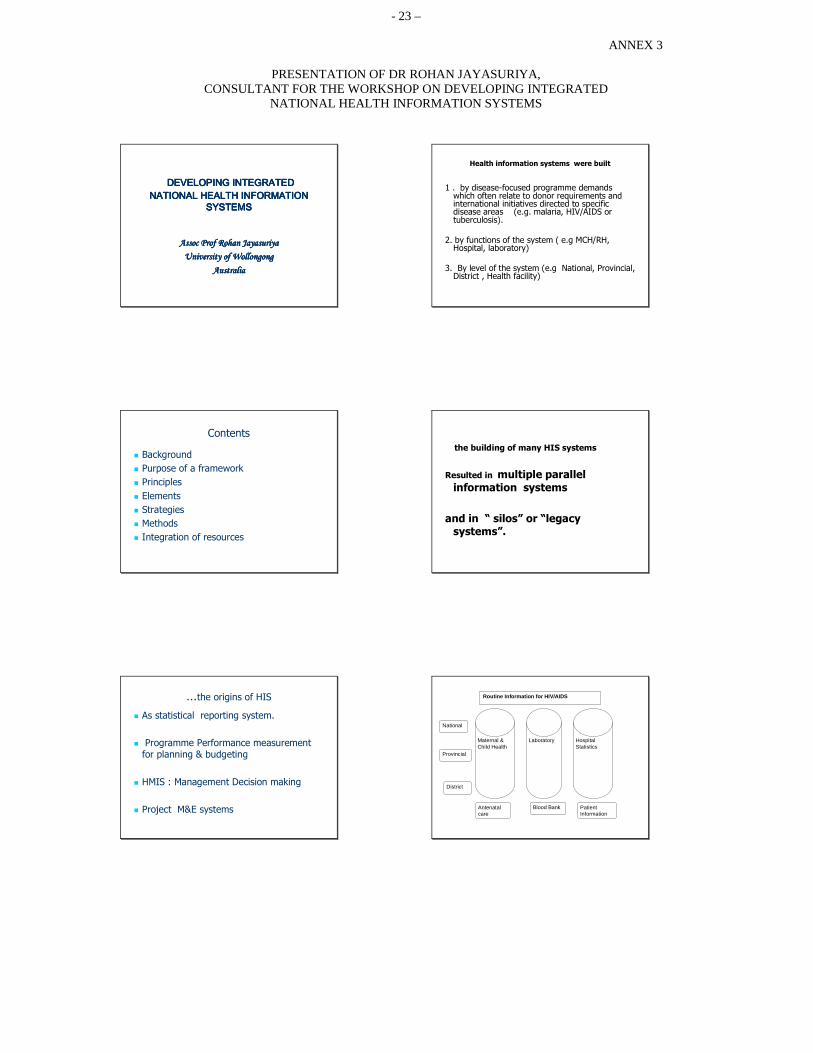
Dr Rohan Jayasuriya, WHO consultant on health information systems, presented a framework for the development of an integrated NHIS.
He stated that a framework is needed for informing interested groups (stakeholders) of the complexities of HIS integration within NHIS development, thereby preventing the spread of limited views. A framework also helps in identifying key dimensions and factors that relate to HIS integration. It provides direction for interested parties of elements that need to be considered for HIS integration and a process for implementation. He emphasized that the framework is not prescriptive and needs to be adapted to the country context and situation.
2.2.1 Framework components
The framework for HIS integration consists of principles, elements, strategies and methods (process).
One of the most important principles is that HIS integration does not aim at building new systems and applications. It focuses on building upon existing systems of health information with a “flexible” approach to allow for future changes. HIS integration must be planned. Any plans for change should consider resources for wider implementation (scalability) and resources for continuity (sustainability).

- 4 -
The elements of the HIS integration framework are illustrated in Figure 1. They consist of:
(1) external and internal forces that initiate or stimulate HIS integration as well as impact on the nature and process of integration;
(2) contents and levels of integration that identify functions of an HIS and levels for integration;
(3) strategies and methods that describe processes for implementation;
(4) resources that need to be considered; and
(5) outcomes of the process of integration.
Figure 1. Elements of the HIS integration framework
Identifying the needs for integrating HIS is complex because of the number of dimensions of a health system. The dimensions consist of levels of care, professional groups, specialities, and levels of service delivery.
Government Policy and Regulations Ex: Vital Registration, Census, ICT
Donor agencies, United Nations bodies, private sector
National Health System
National
Programmes
Hospitals
Decentralized
Units
Health Outcomes
Equity Effectiveness
Efficiency Quality
NHIS Development
HIS Integration Content
Subsystems Functions
Levels
Resources and Training
Review and Feedback
Strategy
Methods
- 5 -
A useful way to look at HIS for purposes of integration is by its functions. Using these functional areas, integration could be identified to be:
(1) integration of data collection and sources;
(2) integration of data management and sharing; and
(3) integration of information use and dissemination.
The case for integrating programs and services that target the same groups (e.g. mothers) has been well argued. Integration of formats and processes are more accepted when the activities and procedures are similar. Subsystems for support services (e.g. financial, human resources, logistics) are much easier to integrate as they use the same definitions, data formats and processes.
Integration of data management has been enhanced by the use of information communication technology (ICT). Information from many subsystems has been integrated to form district health information systems for efficient data management. More sophisticated approaches for integration include the use of data warehousing technology to achieve similar results.
Past experience has shown that integrated programme monitoring mechanisms and integrated supervisory arrangements have provided opportunities for integrating information from a number of HIS subsystems.
Most times, the denominator information required for key indicators used at national and subnational level requires population estimates. Since population estimates are not readily available in the health sector, data from census and sample surveys are integrated into the system.
2.2.2 Strategies and methods for HIS integration
The standardization strategy is a cost-effective approach to HIS integration that is commonly used in developed countries. The strategy involves the standardization of data definitions, data formats, data transmission protocols, etc.
A similar method is the use of “core or minimal essential datasets”. In cases where the HIS design is indicator led, a core indicator set provides standardization. Countries that use this strategy have found that resistance to integration is often reduced if interested parties are also allowed to collect and transmit additional data/indicators that they require.
The “data repository” approach is another successful method of integration. In most cases, data repositories are developed at national level and follow the design principles of data warehousing. In other cases, the use of a common database at district/provincial levels for sharing information has provided the impetus for subsystems to integrate their information systems and resources. A common or standardized format for data is a prerequisite for such data sharing to occur.
Integration of core processes of work is at the heart of process integration strategies. Many of these strategies depend on ICT for process integration. Global Funds are focusing on the development of tools and techniques to monitor and evaluate health programmes in developing countries. The load on HIS in countries would be substantially reduced if M&E activities of many of these agencies were integrated as a process.

- 6 -
Two common methods for implementing HIS integration are: (1) use of minimum datasets; and (2) integrated data management.
2.2.2.1 The use of minimum datasets
This method is based on the identification of essential information needed by health managers and health workers to carry out their functions. The concept of essential datasets contains the concept of integration. In a typical case, an essential set of indicators or dataset is agreed upon at national level for reporting by all facilities. This is then implemented with the proviso that additional indicators useful for management at each level (provincial, district and facility) can be added.
A number of benefits result from integrating HIS in this manner. First, the use of the minimum dataset/indicator reduces the burden in data collection and reporting, which has an impact on the quality of the data. Second, the use of standardized reports and indicators allows the comparison of information across provinces and districts. And third, the process of getting many programmes to discuss the essential dataset creates a platform for discussions on integrating HIS.
2.2.2.2 Integrated data management
In this method, datasets from all or most programmes are combined and streamlined by sorting out overlaps, gaps and inconsistencies. The advantage for the users is that the information is then made available from a single source, e.g. the district health information system. Programme-specific software applications are linked electronically to the district health information system, thus providing a shared data repository.
2.2.3 Integration of HIS resources
Isolated and fragmented human resource policies and practices have in most cases resulted in countries duplicating resources for HIS. There is the need for common training programs and support for all personnel in the health systems in developing their information skills. There are no integrated policies and activities for skill development of staff from organizations and agencies outside the health sector (such as departments of statistics and surveys) for HIS related activities.
Many resource-poor countries have multiple donors for the health sector. In most countries, donors provide financial and technical resources for development of information systems to a specific programme. Pooling of funds that relate to HIS development will enable more resources to be available for NHIS development. Some mechanisms such as SWAPs have created the platform for coordination of donor aid for HIS developments.
NHIS developments require regular reviews to ascertain progress and future needs. In most cases, reviews of HIS have been donor driven and focused on identified specialist systems (e.g. EPI or TB). Regular integrated review, using the NHIS secretariat for coordination would benefit capacity-building on a wider scale.
A copy of the presentation of Dr Jayasuriya is in Annex 3.

- 7 -
2.3 Country presentations
In order to share country experiences on integration, each country was assigned a specific programme to present. China was asked to present its experiences on two programmes, namely the TB and MCH programmes.
2.3.1 Stop Tuberculosis Programme (China)
China relies on two main sources of information for tuberculosis surveillance: (1) the National Tuberculosis Epidemiological Random Sample Survey, and (2) the National Tuberculosis Surveillance Reporting System.
The National TB Epidemiological Random Sample Survey was conducted for the first time in 1978. Since then, it has been conducted in 1984/1985, 1990 and 2000. The survey’s main indicators are: active prevalence rate, smear-positive prevalence rate, TB infection rate, TB mortality rate, and drug resistance rate.
In the case of the National TB Surveillance Reporting System, data are collected and reports are submitted monthly, quarterly and annually. The annual reporting system was the country’s first surveillance system, and was launched in a few provinces in 1984. Since 1987, it has been expanded to cover 31 provinces. This system is considered to be the national legal communicable disease reporting system, with the province as the lowest level of aggregation of the reports.
The quarterly reporting system was a more recent undertaking. It was piloted in five counties in Hebei province in 1991. From 1992 to 2001, the quarterly reporting system was expanded to 13 TB control project provinces, funded under a World Bank loan. Since 2002, this system has been implemented in all directly observed treatment, short-course (DOTS) counties in China. The system’s indicators include: DOTS coverage, pulmonary tuberculosis registration, treatment and management. The cohort analysis of treatment outcome is also done using data generated from this system. The lowest level of aggregation under this reporting system is the county.
The most recent information system launched in China is the nationwide Internet-based communicable disease surveillance system, which was launched in 2004. This system was developed to improve the quality and timeliness of reporting communicable diseases, to increase the number of cases reported by general hospitals and TB dispensaries at all levels, and to increase case finding through the tracing of cases reported by hospitals through the Internet.
The fifth National Tuberculosis Epidemiological Random Survey will be conducted in 2010. Other HIS-related plans include the sharing and integration of data generated from different subsystems.
2.3.2 Hospital information system (Mongolia)
The hospital information system in Mongolia covers three major types of information: inpatient data, outpatient data, and hospital morbidity and mortality. Inpatient and outpatient data include: (1) resource (input) indicators such as the number of health personnel by type; (2) service utilization indicators such as the average length of hospital stay, or the average number of outpatient visits per doctor; and (3) outcome indicators such as the number of deaths within 24 hours after admission.

- 8 -
Data are collected from hospital registration forms and monthly information sheets and then shared through quarterly reports and annual health reports. The monthly reports include data on births, deaths and infectious diseases, in addition to inpatient and outpatient data. The annual report has a much wider coverage since it includes data on: noncommunicable diseases; information, education and communication (IEC) activities; HIV/AIDS; TB and other infectious diseases. It includes reports of hospitals in lower administrative levels like the districts, aimags, and suoms. Since 2002, the annual report has been made available to the public on the Ministry of Health’s website.
In terms of integration, the hospital information system in Mongolia links with the information system of programmes such as GFATM and EPI. It also accesses the population data from the National Statistics Office (NSO), as well as the results of prevalence studies for various diseases and conditions like diabetes, obesity and STI including HIV/AIDS.
From 2002 to 2004, a pilot project was conducted to establish a local area network and to use electronic medical records in hospitals. The pilot study integrated inpatient and outpatient data, as well as data from different hospital departments and units. Mongolia’s hospital information system development strategy for 2006–2010 covers the development of the hospital service management information system, which includes the hospital pharmacy, laboratory, and hospital service claims and billing systems.
2.3.3 Expanded Programme on Immunization (Philippines)
In the Philippines, EPI data are collected through three information systems: (1) the National Epidemic Sentinel Surveillance System (NESS), (2) the Notifiable Disease Reporting System (NDRS), and (3) the Field Health Service Information System (FHSIS). The first two information systems generate data on immunizable diseases such as polio, measles and neonatal tetanus. NESS is hospital based, while NDRS is community based. FHSIS, on the other hand, is the official information system of the Department of Health and provides summary data on health service delivery including immunization coverage.
The Department of Health also makes use of the National Demographic Survey and the census, both of which collect data useful for immunization coverage. EPI-related information is disseminated through Philippines Health Statistics, an annual publication of the Department of Health that includes morbidity and mortality data on notifiable diseases.
The country’s future plans include the integration of NESS and NDRS into a single system called the Philippine Notifiable Disease Surveillance System. The first phase of the development of the Philippine Health Information System is in progress.
2.3.4 Maternal and child health (China)
The national monitoring system for maternal and child mortality involves the monitoring of under-five mortality, maternal mortality and birth defects. It is implemented through a three-level monitoring network covering the village, township and county in rural areas and residential blocks, districts and cities in urban areas.
At the national level, the MCH Surveillance Office implements data quality control mechanisms including sample surveys to validate records, sponsors annual conferences for information dissemination, and participates in provincial training activities.
- 9 -
Future plans include the continuous conduct of training courses on data collection and quality control, the expansion of monitoring activities to include the provincial level, and computerization.
2.3.5 Malaria control programme (Lao People’s Democratic Republic)
The malaria information system of the Lao People’s Democratic Republic is one of nine programme information systems in the country. It covers two major types of data: epidemiological data related to malaria (morbidity, mortality), and data on bednets (number of nets provided, number treated, etc.). The Epidemiology Unit of the Centre for Malaria, Parasitology and Entomology (CMPE) manages the data. The key users of these data are the Ministry of Health, WHO, the Malaria Control Project, and other related projects.
In addition to the routine system of data collection, the malaria information system accesses data from other sources such as malariometric surveys, drug use surveys, insecticide susceptibility tests and antimalarial drug resistance studies.
The malaria information system is integrated with other subsystems such as Roll Back Malaria, the Regional Information System, and the Malaria Control Project supported by GFATM. Sharing information across these related initiatives is done in consonance with national policy. In addition, important indicators related to malaria are incorporated within the NHIS.
2.3.6 HIV/AIDS (Cambodia)
The national HIV/AIDS programme in Cambodia dramatically expanded its coverage and activities from 2000 to 2006. A dual complementary approach to STI care uses both specialized STI clinics targeted to high-risk cases and where laboratory facilities are available (30 clinics in 21 provinces) and integrated clinics at health centres. Facility-based services include voluntary counselling and confidential testing (VCCT), management of opportunistic infections (OIs) and antiretroviral therapy (ART), and prevention of mother-to-child transmission. About 36% (366) of health centres also have home-based services.
Cambodia has integrated its TB and HIV programmes. It is estimated that 5%–22% of TB cases (depending on the type of infection) have HIV. Drugs and logistics are managed at national level and are distributed through a vertical system.
Given that the current NHIS cannot provide the necessary information on HIV/AIDS in the detail and time required, a parallel system of information was established by the programme. The pivotal position for the information system is the Provincial AIDS Office. Paper-based records are sent by health facilities to the provincial data manager, who enters the data into a computer, conducts data analysis, and reports to the national level.
The use of ICT is increasing as some health centres have computers. All specialized clinics and those facilities that manage OIs and ART are capable of sending electronic reports.
Sample surveys and sentinel surveillance are likewise conducted, allowing the verification of data on incidence/prevalence rates.
2.3.7 Communicable disease control (Viet Nam)
The preventive medicine system for communicable disease control in Viet Nam includes 64 provincial preventive medicine centres, 669 district preventive medicine centres, the National Institute of Hygiene and Epidemiology, the Pasteur Institute and others.

- 10 -
Data on communicable diseases are disseminated through weekly, monthly and emergency reports. Weekly reports cover the number of cases and deaths due to cholera, typhoid fever, haemorrhagic fever, viral encephalitis and plague. Monthly reports cover morbidity and mortality data on 24 communicable diseases. Emergency reports are prepared whenever outbreaks occur in an area. Morbidity and mortality data on communicable diseases are included in the Annual Statistics of Health, which is published by the Department of Planning and Finance of the Ministry of Health.
The information system for communicable diseases has not been integrated with those of other programmes. Future plans for HIS development in Viet Nam include better HIS coordination, with involvement of relevant stakeholders; updating and standardizing the basic list of indicators according the Statistics Law, the National Statistics Indicator System and other current initiatives related to health information at the national and global levels; strengthening of staff capacity for data collection, reporting, analysis and use; expanding information technology applications; and the formulation of a comprehensive HIS development plan.
2.4 Integrating the information needs of global initiatives
The reporting requirements of special projects often impose an added burden on the HIS of countries, especially if they establish a separate and parallel project-specific information system. Hence, it is important that the information subsystems of these projects be integrated into the NHIS to minimize duplication of data collection activities, ensure the consistency of data, and ensure the efficient use of resources.
Several countries implement the global initiatives of GFATM and GAVI. Representative of these two organizations presented the efforts they have exerted in countries towards integration of information systems. Both GFTAM and GAVI share the principle that parallel information systems should be avoided. Likewise, they both emphasize the importance of data quality. GAVI has implemented a Quality Audit to achieve this.
Countries participating in the workshop were strongly encouraged to avail of the funding opportunities offered by GFATM and GAVI for HIS strengthening, when developing proposals for M&E systems. The representative of GFATM stated that countries should take a more consultative approach in the development of indicators for M&E by including the NHIS in the consultations. He also stated that at project negotiation, a representative from NHIS should also be present.
Both GFATM and GAVI expressed openness to collaboration, as well as their willingness to receive feedback on their M&E tools.
2.5 The Health Metrics Network and its role in the development of an integrated NHIS
The Health Metrics Network (HMN) is a global initiative developed specifically to address the various challenges of health information systems in the resource poor countries. HMN has developed standard tools and techniques that would help countries in assessing, planning and strengthening their HIS. A number of these mechanisms and tools when operationalized would greatly facilitate the integration process within countries. Among these are:
(1) partnership between a wide range of statistical bodies;
(2) consensus building among donors; bringing-out synergies between partners;
(3) working with the whole HIS instead of individual components; and
(4) use of a unifying framework for integration of the HIS.

- 11 -
In the discussion that followed the presentation, issues raised by countries that have already received HMN support, especially in the application of the HMN assessment and monitoring tool were addressed.
2.6 Integrating demographic data, vital statistics, special studies and sample surveys
Dr G Shantakumar, WHO technical adviser, presented on the integration of demographic data, vital statistics, special studies and sample surveys into the NHIS. He described five main demographic data sources namely the population and housing census, vital registration system, population or pseudo-population registers, sample surveys and retrospective studies, and the application of indirect estimation methods developed by the United Nations.
To facilitate the integration between the various demographic data sources and the NHIS, Dr Shantakumar emphasized the need for interface between the health personnel at the Ministry of Health and the demographers and statisticians in other agencies producing demographic and other health-related data. The conduct of training programmes on demographic methods was likewise suggested to enhance the interface.
Dr Shantakumar recommended that countries should strive to have a register-based population database, similar to that in Singapore. This is a relational computer-based database combining the census, the vital registration system, the people registration and identification system, and data from sample surveys. The advantages of having a relational database are reduction in administrative costs, enhanced data retrieval and compilation.
2.7 Group work sessions
2.7.1 Identification of issues related to integration
The first two group work sessions addressed the identification of issues related to integration. In the first session, participants were asked to identify issues related to the integration of the three main HIS functions, i.e. data collection, sharing and use. In the second group work session, participants were asked to identify issues related to regulations, as well as the integration of resources. Guiding questions and worksheets were provided for each group to document the results of the group discussions.
The first topic discussed in the group work was the identification of HIS subsystems that need to be integrated. All groups concluded that integration should take place between the public health and disease control programmes, or between the preventive and curatives services. None of the groups identified the integration between health programmes and other subsystems like human resource, logistics and finance information, or between health subsystems and other data sources like the NSO. The integration of information with academic and research organizations (scientific research) and the private sector was also not identified. This may be a reflection of the composition of participants from the country.
Some of the issues identified by the participants as obstacles for integration were:
(1) decision-making/consensus-building process (Who should make the decisions on integration-related matters? How can it be done? How and to what extent should stakeholders be involved?);
(2) logistics (Who supplies the forms, data collection tools and equipment?);
(3) ICT (hardware procurement and maintenance; software design and standardization);
- 12 -
(4) human resources (capability building especially in the area of data analysis, interpretation and use; staff displacement resulting from integration; proliferation of training programmes);
(5) donors (coordination; reporting requirements especially in the area of indicators and M&E systems and tools; fund sharing); and
(6) other issues (denominator issue, confidentiality of information).
The outputs for group work sessions 1 and 2 are presented in Annex 4, and Annex 5, respectively.
2.7.1 Country action plans
Group work session 3 required the participants to develop country-specific action plans for HIS integration. Groups were first asked to rank the key HIS components and functions for integration, which were identified in the first two sessions, based on perceived impact and feasibility. They were asked to consider their countries’ HIS strategic plan and HMN work plan, if these have already been developed.
The HIS components and functions identified by countries as belonging to the three highest priorities for integration were related to data collection. Specific activities include the consolidation and standardization of forms, identification of core/essential data elements and indicators, and data quality assurance. All countries except Cambodia assigned a low rank to data utilization. This may be reflection of the current level of focus of HIS development of the countries.
Among the strategies identified in action plans, the most common were negotiation with donors, advocacy, capability building, data warehousing, and development of integrated software. Technical and financial supports were the most commonly identified resources needed to implement the various strategies.
The country outputs for group work session 3 are presented in Annex 6.
3. CONCLUSIONS
The main conclusions of the workshop were as follows:
3.1 General
3.1.1 The workshop provided a forum for country delegates and development partners to discuss the issues related to integration of health information systems in developing countries.
3.1.2 The presence of representatives from GFATM, GAVI and HMN contributed to the exchange of information on the ways to access funds to develop the HIS and health systems more broadly. Participants also learned of the development of an integrated tool for M&E by GFATM and a Quality Audit by GAVI. Both organizations encouraged countries to submit proposals that would enhance their NHIS, which would benefit information use for programme planning and evaluation.
3.2 HIS integration

- 13 -
3.2.1 During the group work sessions, participants identified functional areas for HIS integration and issues that countries need to overcome. The following key steps for countries to plan and implement integration of HIS were identified:
(1) Establish a mechanism to coordinate HIS integration. This process requires leadership and commitment and therefore should be led by a senior official. In a number of countries, an NHIS steering committee has been established; in others, in response to the HMN requirement, the Planning and Information Division or its equivalent carries out this task.
(2) Integrate information between subsystems (between different public health programmes), and with information pertaining to finance. This pertains to each of the HIS functions: data collection, management, analysis and use.
(3) Take advantage of the funding opportunities provided by GFATM and GAVI for M&E activities. Specifically, countries should do the following:
(a) HIS units (and those responsible for M&E) should be involved in developing and negotiating proposals for GFATM and GAVI.
(b) The HMN assessment and subsequent strategic plans should be incorporated into existing HIS development plans funded by other donors to reduce overlap and duplication of efforts.
(c) Integration of country HIS proposals to GFATM, GAVI and HMN. This is best done under a country NHIS strategic plan.
3.2.2 In their country action plans, participants identified a number of ways to integrate health information systems. Data collection and sharing were viewed as the highest priorities.
(1) Data collection methods should be integrated if it occurs at a single site (e.g. facility or outpost) or if it targets the same groups. For example, EPI data could be collected with other data during outreach visits to villages. The obstacles were identified to be how decisions can be taken for integration and who would be responsible for the system of data collection and reporting.
(2) Data sharing at district, provincial and national levels was identified as an opportunity for integration of resources, skilled staff in data management, analysis and interpretation. Technology, especially the use of data warehousing, could enhance such integration.
(3) Integration in the use of information was not given high priority by country groups. However, opportunities for such activity were mentioned in the country presentations. For example, in Cambodia the annual forum for joint review of performance provides such an opportunity.
(4) A gap in the HIS of many countries is the lack of integration of information from the private health sector. The lack of regulation and poor implementation of such regulation in most countries was identified as the reason for this. As the private sector is expanding in a number of countries in the Region, this was seen as an area of concern for NHIS.
(4) The integration of information from population surveys, to supplement routine information, provides means to reduce the load of data collection. In some countries, such surveys could supply information in a regular manner for essential indicators.
- 14 -
(5) Opportunities for HIS integration also occur in situations where service delivery if integrated. For example at health facilities where integrated STI services are provided, information on VCCT, ART, and reproductive health can be integrated. The other example is when integrated supervisory visits are conducted from the province/district to heath centres.
3.2.3 As a first step to the integration process, it was agreed that it is important for countries to identify their own priorities, obtain commitment to initiate integration, plan for such activities (using the NHIS strategic plans to be developed) and pursue integration given the resources and opportunities currently available..

- 15 -
ANNEX 1
LIST OF PARTICIPANTS, TEMPORARY ADVISER, CONSULTANTS, OBSERVERS/REPRESENTATIVE AND SECRETARIAT
1. PARTICIPANTS
CAMBODIA Dr Sao Sovanratnak, Deputy Director, Department of Planning and Health Information, Ministry of Health, No. 151-153 Avenue Kampuchea Krom, Phnom Penh Tel. No.: (855-23)427-368/(855-12)859-134 Fax No.: (855-23)880-262
Dr Hong Rathmony, Deputy Director, Center for Communicable Diseases Department, Ministry of Health, No. 151-153 Avenue Kampuchea Krom, Phnom Penh, Tel. No.: (855-23)722 933, Fax No.: (855-23)426-034
Dr Huot Chanyuda, Deputy Director, National Tuberculosis Center, Ministry of Health, No. 151-153 Avenue Kampuchea Krom, Phnom Penh Tel. No.: (855-23)722 933, Fax No.: (855-23)426-034
Dr Ly Penh Sun, Deputy Director, National Center for HIV/AIDS Ministry of Health, No. 151-153 Avenue Kampuchea Krom, Phnom Penh Tel. No.: (855-23) 722 933, Fax No.: (855-23) 426-034
Dr Khol Khemrary, Chief of Health Information Bureau, Ministry of Health, No. 151-153 Avenue Kampuchea Krom, Phnom Penh Tel. No.: (855-23) 722 933, Fax No.: (855-23) 426-034
CHINA Mr Yao Deming, Division of HSI/HIV/AIDS, Ministry of Health 1 Nanlu, Xishimenwai, Xicheng District, Beijing, Tel. No.: (8610) 68792375, Fax No.: (8610) 68792362, Email: [email protected]
Mr Wang Wei, Department of Communicable Disease Control, Ministry of Health, 1 Nanlu, Xishimenwai, Xicheng District, Beijing, Tel. No.: (8610) 68792338, Fax No.: (8610) 68792514
Dr Cheng Shiming, Department of Tuberculosis Control, Ministry of Health, No. 27 Nanwei, Xuanwu, Beijing, Tel. No.: (8610) 83136107, Fax No.: (8610) 83135306
Mr Wang Kerang, Department of Maternal and Child Health, Ministry of Health, 1 Nanlu, Xishimenwai, Xicheng District, Beijing Tel. No.: (8610) 68792309, Fax No.: (8610) 68792321
Dr Cheng Jianpeng, Department of Planning and Health Information, Ministry of Health, 1 Nanlu, Xishimenwai, Xicheng District, Beijing, Tel. No.: (8610) 68792467, Fax No.: (8610) 68792418

Annex 1
- 16 -
LAO PEOPLE'S Dr Panome Vilayhong, Statistics and Planning, Mother and Child Health Centre, DEMOCRATIC Ministry of Health, 3rd Kilometre, Thadena Road, Vientiane Capital, REPUBLIC Tel. No.: (856)20-241-7176, Fax No.: (856)21-312-120
Dr Phonenaly Chittamany, National Tuberculosis Centre, Ministry of Health, Vientiane, Tel. No.: (856) 21-414-259, Fax No.: (856) 21-452-855, Email: [email protected]
Dr Bounfeng Phoummalaysith, Deputy Director of Cabinet and Chair of the Committee of Coordination for, Health Information System in Laos, Ministry of Health, Vientiane, Tel. No.: (856) 21 95-1094, Fax No.: (856) 21-21-4003, Email: [email protected]
Dr Swady Kingkeo, Chief of Health Statistical Division, Ministry of Health, Vientiane, Tel. No: 856-20-2418363, Email: [email protected]
Dr Khamsovang Kham Sy, Center of Malariology, Parasitology and Entomology, Vientiane, Tel. No.: (856) 21-21-4040, Fax No.: (856) 20-5705572
MONGOLIA Mr G. Bayasgalan, Director, Second Clinical Hospital, Blk 22 Suohbaatar District Ulaanbaatar, Tel. No.: 976-11-953181, Fax No.: 976-11-453181
Dr Purev Oyuntsetseg, Officer-in Charge of Health Information Ministry of Health, Government Building, 8 Olympic Street 2, Ulaanbaatar 21068 Tel. No.: 976-51-261742, Fax No.: 976-51-260808, Email: [email protected]
Dr N. Tsogzolmaa, Officer, Information, Monitoring and Evaluation Department Ministry of Health, Government Building, 8 Olympic Street 2, Ulaanbaatar 21068 Tel. No.: 976-51-263681, Email: [email protected]
Ms D. Nyamkhorol, Head, Health Statistical Department, National Center for Health Development, Street 138, Ulaanbaatar 219648, Tel. No.: 976-11-521485 Fax No.: 976-11-520633, Email: [email protected]
Ms Ts. Oyunchimeg, General Director, National Center for Communicable Diseases, Bayanzurich District, Nam Yan Ju Street, 210-648 Ulaanbaatar City, Tel. No.: 976-11-458699, Fax No.: 976-11-458699, Email: [email protected]
PHILIPPINES Dr Ma. Joyce Ducusin, Medical Specialist IV, Family Health Office, National Centre for Disease Prevention and Control, Department of Health, Manila
Mr Ferdinand L. La Puebla, Senior Health Programme Officer, Infectious Disease Office, 3rd Floor, National Centre for Disease Prevention and Control, Department of Health, Manila, Tel. No.: (632) 534-50-73, Email: [email protected]

Annex 1
- 17 -
Dr Marlow O. Niñal, Medical Officer VII, Chief, Public Health Surveillance and Informatics Division, National Epidemiology Center, Department of Health Manila, Tel. No. (632) 741-70-48, Email: [email protected]
Dr Angeles T. De Leon, Quirino Memorial Medical Center, Project 4, Quezon City Tel. No.: (632) 421-92-89, Fax No.: (632) 421-92-89, Email: [email protected], [email protected]
Ms Charity Tan, Chief, Knowledge Management Division, Information Management Service, Department of Health, Manila, Tel. No.: (632) 743-83-01 local 1910 Fax No.: (632) 711-67-44, Email: [email protected]
VIET NAM Ms Thanh Tu Phung Thi, Vice-Director of Nha Trang Pasteur Institute Nha Trang Pasteur Institute, 8 Tran Phu, Nha Trang, Tel. No.: 84 58 811856 Fax No.: 84 58 824058, Email: [email protected]
Dr Thi Minh Dinh, Expert of Therapy Department, Department of Therapy Ministry of Health, 138A Giang Vo Street, Ha Noi, Tel. No.: 84-4-8464414 Fax No.: 84-4-8460966
Mrs Lan Phuong Do Thi, Health Statistics, 3 Ton Duc Thang, Dong Da Ha Noi, Tel. No.: 84-4-8464416
Dr TRAN Anh Dung, Medical Officer, Viet Nam Administration of Preventive Medicine, Ministry of Health, 138 A. Giang Vo Street Ha Noi, Tel. No.: 84-4-8464415, Fax No.: 84-4 7366241 Email: [email protected]
Dr Son Vo Hai, Expert of the Viet Nam Administration of HIV/AIDS Control Ministry of Health, 138 A. Giang Vo Street, Ha Noi, Tel. No.: 84-4-8465731 Fax No.: 84-4 8465732
2. TEMPORARY ADVISER
Dr G. Shantakumar, Associate Professor (Retired), National University of Singapore Consultant Demographer/Statistician/Market Researcher, 119 Jalan Dermawan, Singapore 669068 Tel. No.: (65) 67605697, Fax No.: (65) 68922110, Email: [email protected]
3. CONSULTANTS
Dr Rohan Jayasuriya, Associate Professor, University of Wollongong, School of Public Health Wollongong NSW 2500, Australia, Tel. No.: 61-42-213344, Mobile : 61-413-195448, Email: [email protected]
Dr Ophelia Mendoza, 47 Pook Dagohoy, U.P. Campus, Diliman, Quezon City, Philippines Tel. No.: (632)436-9332, Email : [email protected]
4. OBSERVERS
Annex 1
- 18 -
Global Alliance for Dr Anshu Banerjee, Senior Programme Officer/Country Support Vaccine Immunization Team, GAVI Alliance, GAVI Alliance Secretariat, c/o UNICEF
Palais des Nations , CH-1211 Geneva, 10 Switzerland Tel. No.: +41 22 909 6546, Fax No: +41 22 909 6550 Email: [email protected], Web: www.gavialliance.org
Global Fund to Fight Mr Chrishan Thuraisingham, Fund Portfolio Manager AIDS, Tuberculosis Global Fund to Fight AIDS, Tuberculosis and Malaria and Malaria in Indonesia, the Pacific Islands, Thailand and Lao People's
Democratic Republic, Bangkok, Thailand Email: [email protected]
Health Metrics Network Dr Lene Mikkelsen, Health Metrics Network, c/o WHO Headquarters, 20 Avenue Appia, 1211 Geneva 27, Switzerland Email: [email protected]
United Nations Dr Nicholas Alipui, UNICEF Representative, 31th Floor, Children's Fund Yuchengco Tower, RCBC Plaza, Makati City
Tel. No.: (632) 901-01-24
5. SECRETARIAT
Dr Soe Nyunt-U, Director, Health Sector Development, WHO Western Pacific Regional Office United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289851, Fax No.: (632) 5211036 Email: [email protected]
Dato' Dr Tee Ah Sian, Director, Combating Communicable Diseases, WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289701, Fax No.: (632) 5211036, Email: [email protected]
Dr Y.C. Chong (Responsible Officer), Regional Adviser in Health Information, Health Sector Development Division, WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289812, Fax No.: (632) 5211036, Email: [email protected]
Dr Marianna Trias, Medical Officer in Child and Adolescent Health Development, Building Health Communities and Populations Division, WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289868, Fax No.: (632) 5211036, Email: [email protected]
Dr Takeshi Kasai, Regional Adviser in Communicable Disease Surveillance and Response, Combating Communicable Diseases Division, WHO Western Pacific Regional Office, United Nations Avenue Manila, Philippines, Tel. No.: (632) 5289730, Fax No.: (632) 5211036, Email: [email protected]
Dr Yang Baoping, Regional Adviser in Expanded Programme on Immunization, Combating Communicable Diseases Division, WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289747, Fax No.: (632) 5211036, Email: [email protected]

Annex 1
- 19 -
Dr Bernard Fabre-Teste, Regional Adviser in Sexually Transmitted Infections including HIV/AIDS, Combating Communicable Diseases Division, WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289725, Fax No.: (632) 5211036, Email: [email protected]
Dr Eva-Maria Christophel, Medical Officer, Malaria, Vectorborne and other Parasitic Diseases Combating Communicable Diseases Division, WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289723, Fax No.: (632) 5211036, Email: [email protected]
Dr Pang Ruyan, Regional Adviser in Reproductive Health, Building Health Communities and Populations Division, WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289876, Fax No.: (632) 5211036, Email: [email protected]
Dr Reijo Salmela, Medical Officer, Situation Analysis for Policy, Health Sector Development Division WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289835, Fax No.: (632) 5211036, Email: [email protected]
Dr Pieter Van Maaren, Medical Officer, Stop TB and Leprosy Elimination, Combating Communicable Diseases Division, WHO Western Pacific Regional Office, United Nations Avenue Manila, Philippines, Tel. No.: (632) 5289706, Fax No.: (632) 5211036, Email: [email protected]
Dr Paul Weelen, Medical Officer, Health Systems Development, WHO office in Cambodia No. 177-179 corner Pasteur (51) and 254, Sangkat Chaktomouk, Khan Daun Penh, Phnom Penh, Cambodia Tel. No.: (855)23-216610, Fax No.: (855)23-216211, Email: [email protected]
Mr Yang Hongwei, National Programme Officer, WHO Office in China, 401, Dongwai Diplomatic Office Building, 23, Dongzhimenwai Dajie, Chaoyang District, Beijing 1000600, China, Tel. No.: (8610)6532-7189, Fax No.: (8610)6532-2359, Email.: [email protected]
Dr Dean Shuey, Technical Officer, Health Systems Development, WHO Office in Lao People's Democratic Republic, Ban Phonxay, That Luang Road, Vientiane, Lao People's .Democratic Republic, Tel. No.: (856)21413-341, Fax No: (856)21413-432, Email: [email protected]
Dr Salik Govind, Medical Officer, Health Systems Development, WHO Office in Mongolia, Ministry of Health, Government Building-8, Ulaanbaatar, Mongolia, Tel. No.: (976)11-32 78 70, Fax No.: (976)11-32 46 83, Email: [email protected]
Ms Lucille Nievera, Programme Officer, WHO Office in the Philippines, National Tuberculosis Centre Building, Second Floor, Bldg. 9, Department of Health, San Lazaro Hospital Compound, Sta. Cruz, Manila, Tel. No.: (632)338-7479, Fax No.: (632)731-3914, Email: [email protected]
Dr Lokky Wai, Technical Officer, Health Systems Development, WHO Office in Viet Nam, 63 Tran Hung Dao Street, Hoam Kiem District, Ha Noi, Socialist Republic of Viet Nam, Tel.No.: (844)943-3734, Fax No. (844)943-3740, Email: [email protected]
Mrs Rose Azcuna, Acting Assistant, Health Information, Health Sector Development Division WHO Western Pacific Regional Office, United Nations Avenue, Manila, Philippines, Tel. No.: (632) 5289837, Fax No.: (632) 5211036, Email: [email protected]

Annex 1
- 20 -

WORKSHOP ON DEVELOPING INTEGRATED NATIONAL HEALTH INFORMATION SYSTEMS
6 TO 8 SEPTEMBER 2006, Manila, Philippines
PROGRAMME OF ACTIVITIES
ACTIVITY PRESENTOR TIME
ACTIVITY PRESENTOR ACTIVITY PRESENTOR TIME
Wednesday, 6 September Thursday, 7 September
TIME
Friday, 8 September
8:30–9:00 1. Opening ceremony
8:00–9:00 7. Integrating information needs of global initiatives into the NHIS
(a) The Global Funds to Fight AIDS Tuberculosis and Malaria (GFATM)
(b) Global Alliance for Vaccine Immunization (GAVI)
8. The Health Metrics Network (HMN) and its role in the development of an integrated NHIS
9. Integrating demographic data, vital statistics, and special studies and sample surveys
Representatives of Global Initiatives
Mr C. Thuraisingham
Dr A. Banerjee
Dr L. Mikkelsen
Dr G. Shantakumar
9:00-10:00 2. Rationale for the Development of Integrated National Health Information Systems
3. Framework for the Development of Integrated National Health Information Systems
4. Discussions on the presentations
Dr Y.C. Chong
Dr R. Jayasuriya
9:00-10:00 10. Discussions on the framework for integrating national health information systems
8:00-10:00 14. Workshop 3: Prioritization of components and strategies, and formulation of country action plan
Consultants, Secretariat
10:00-10:30 C O F F E E B R E A K
10:30-12:00 5. Integrating information needs of health programmes into the national health information systems (NHIS): Country experiences (a) Stop Tuberculosis Programme
(China) (b) The Hospital Information System
(Mongolia) (c) Expanded Programme on
Immunization (Philippines)
Country Presentors
10:30-12:00 11. Workshop 1: Identification of issues (data collections, sharing and use) for the development of an integrated NHIS
Consultants, Secretariat
10:30-12:00 Continuation of Workshop 3
Consultants, Secretariat
12:00-1:30 L U N C H B R E A K
1:30–3:30 Continuation of country presentations
(d) Maternal and Child Health (China) (e) Malaria Control Programme (Lao
People's Democratic Republic) (f) HIV/AIDS (Cambodia) (g) Communicable Disease Control
(Vietnam)
Country Presentors
1:30–3:00 12. Workshop 2: Identification of issues (resources and regulations) for the development of an integrated NHIS
Consultants, Secretariat
1:30-3:00 15. Plenary 2: Presentation and discussion of outputs of workshop 3
16. Closing ceremony
3:30–4:00 Coffee Break 3:00–3:30 Coffee Break
4:00–5:00 6. Discussions on the country presentations Dr R. Jayasuriya 3:30– 5:00 13. Plenary 1: Presentation and discussion of outputs of workshops 1 and 2
Consultants, Secretariat
6:00-8:00 Informal Get Together
AN
NE
X 2
- 21 -

- 22 –
Annex 2
DEVELOPING INTEGRATED DEVELOPING INTEGRATED DEVELOPING INTEGRATED DEVELOPING INTEGRATED NATIONAL HEALTH INFORMATION NATIONAL HEALTH INFORMATION NATIONAL HEALTH INFORMATION NATIONAL HEALTH INFORMATION
SYSTEMSSYSTEMSSYSTEMSSYSTEMS
Assoc Prof Assoc Prof Assoc Prof Assoc Prof RohanRohanRohanRohan JayasuriyaJayasuriyaJayasuriyaJayasuriya
University of WollongongUniversity of WollongongUniversity of WollongongUniversity of Wollongong
AustraliaAustraliaAustraliaAustralia
Contents
� Background
� Purpose of a framework
� Principles
� Elements
� Strategies
� Methods
� Integration of resources
…the origins of HIS
� As statistical reporting system.
� Programme Performance measurement for planning & budgeting
� HMIS : Management Decision making
� Project M&E systems
Health information systems were built
1 . by disease-focused programme demands which often relate to donor requirements and international initiatives directed to specific disease areas (e.g. malaria, HIV/AIDS or tuberculosis).
2. by functions of the system ( e.g MCH/RH, Hospital, laboratory)
3. By level of the system (e.g National, Provincial, District , Health facility)
the building of many HIS systems
Resulted in multiple parallel
information systems
and in “ silos” or “legacy systems”.
Maternal & Child Health
Laboratory Hospital Statistics
National
Provincial
District
Antenatal care
Blood Bank
Routine Information for HIV/AIDS
Patient Information
Source: Chilundo & Aaanestad , 2004
- 23 –
ANNEX 3
PRESENTATION OF DR ROHAN JAYASURIYA, CONSULTANT FOR THE WORKSHOP ON DEVELOPING INTEGRATED
NATIONAL HEALTH INFORMATION SYSTEMS
Annex 3
- 24 -
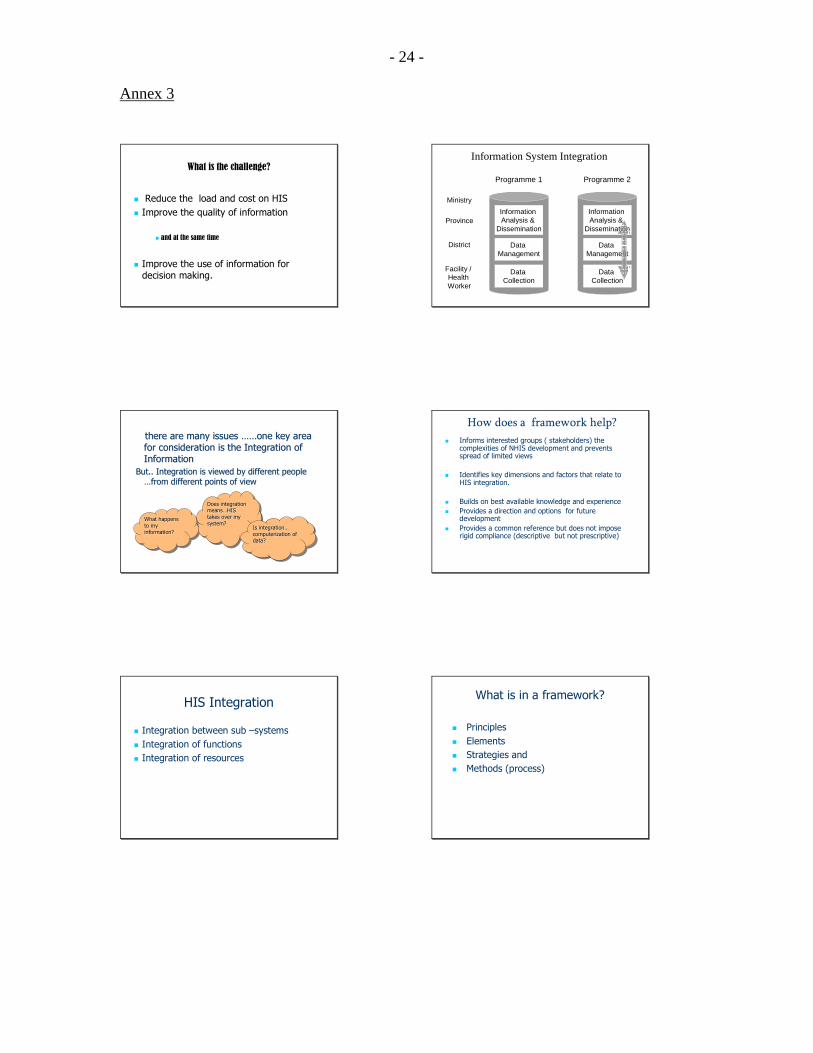
What is the challenge?
� Reduce the load and cost on HIS
� Improve the quality of information
� and at the same time
� Improve the use of information for decision making.
there are many issues there are many issues …………one key area one key area
for consideration is the Integration of for consideration is the Integration of
InformationInformation
But.. Integration is viewed by different people But.. Integration is viewed by different people
……from different points of viewfrom different points of view
What happens
to my information?
What happens What happens
to my to my
information?information?
Does integration
means…HIS takes over my
system?
Does integration Does integration
meansmeans……HIS HIS
takes over my takes over my
system?system?Is integration…
computerization of data?
Is integrationIs integration……
computerization of computerization of
data?data?
HIS Integration
� Integration between sub –systems
� Integration of functions
� Integration of resources
Information Analysis &
Dissemination
Data Management
Data Collection
Programme 1
Information Analysis &
Dissemination
Data Management
Data Collection
Programme 2
Ministry
Province
District
Facility / Health Worker
Information System Integration
How does a framework help?
� Informs interested groups ( stakeholders) the complexities of NHIS development and prevents spread of limited views
� Identifies key dimensions and factors that relate to HIS integration.
� Builds on best available knowledge and experience
� Provides a direction and options for future development
� Provides a common reference but does not impose rigid compliance (descriptive but not prescriptive)
What is in a framework?
� Principles
� Elements
� Strategies and
� Methods (process)

Annex 3
- 25 -
Key principles
� HIS integration does not necessarily lead to building new systems and applications.
� It aims to build on existing systems and developments as reasonably as possible.
� HIS integration uses “ flexible” approaches to ensure that these developments are not rigid (ie cannot be changed) and can accommodate future developments.
� HIS integration should capitalize on available opportunities that can build knowledge and capacity in the system.
� For HIS Integration to be successful plans for change should at the outset ( during the planning phase) consider resources for wider implementation (scalability) and continuity (sustainability).
Elements of the framework
� External and Internal forces
� Contents and levels of integration
� Strategies
� Methods
� Implementation ( resources & training)
� Outcome.
Elements of HIS Integration
Government Policy and RegulationsEx: Vital Registration, Census, ICT
Donor Agencies; UN Bodies; Private Sector
NationalHealth System
National
Programmes
Hospitals
Decentralized
Units
HealthOutcomes
Equity
Effectiveness
Efficiency
Quality
National Health Info System Development
HIS IntegrationContent
Routine HIS
Surveys, Census
Administrative IS
Levels
Resources& Training
Review and
Feedback
HIS IntegrationStrategy
Approach /
Methods
External and internal forces
� External stakeholders ( eg. Donors)
� Health sector reform/Decentralization
� Program changes ( eg. ART)
� Infrastructure changes ( eg. ICT)
� Policy changes
� Level of development of NHIS
Elements of HIS Integration
Government Policy and RegulationsEx: Vital Registration, Census, ICT
Donor Agencies; UN Bodies; Private Sector
NationalHealth System
National
Programmes
Hospitals
Decentralized
Units
HealthOutcomes
Equity
Effectiveness
Efficiency
Quality
National Health Info System Development
HIS IntegrationContent
Routine HIS
Surveys, Census
Administrative IS
Levels
Resources& Training
Review and
Feedback
HIS IntegrationStrategy
Approach /
Methods
Annex 3
- 26 -
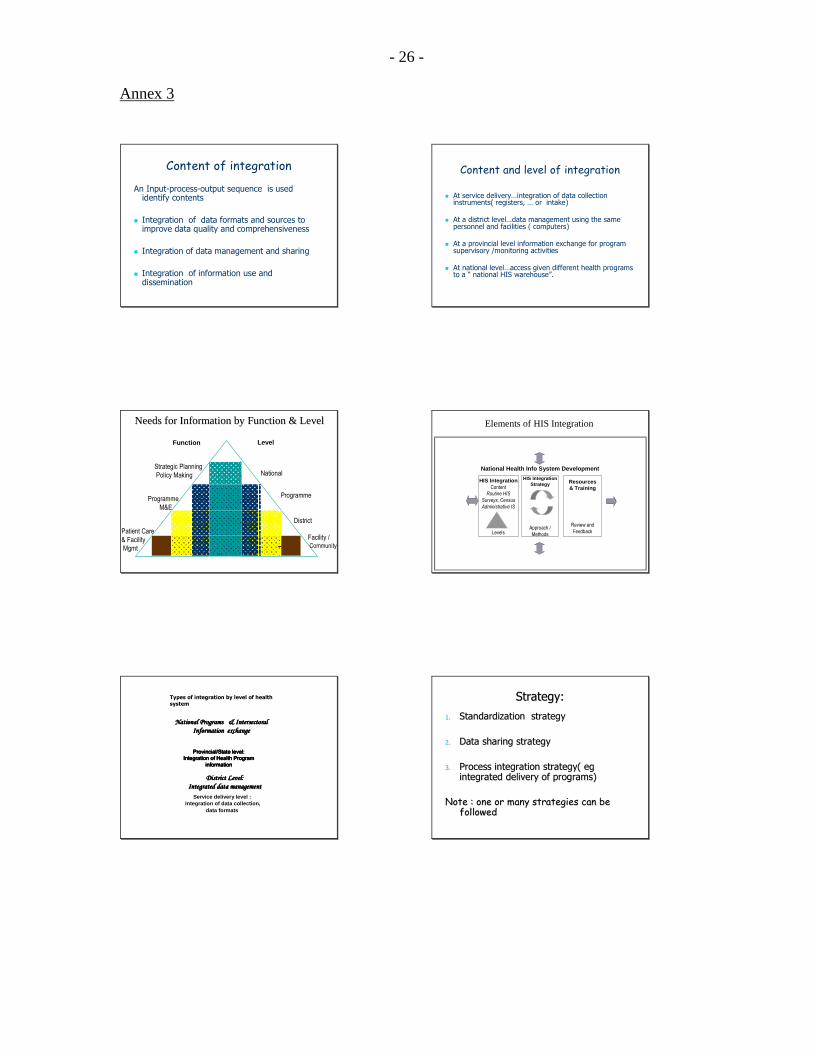
Content of integration
An Input-process-output sequence is used identify contents
� Integration of data formats and sources to improve data quality and comprehensiveness
� Integration of data management and sharing
� Integration of information use and dissemination
Needs for Information by Function & LevelNeeds for Information by Function & Level
Strategic Planning
Policy Making
Programme
M&E
Patient Care
& Facility
Mgmt
National
Programme
District
Facility / Community
Function Level
Service delivery level :Integration of data collection,
data formats
District Level: District Level: District Level: District Level:
Integrated data managementIntegrated data managementIntegrated data managementIntegrated data management
Provincial/State level: Provincial/State level: Provincial/State level: Provincial/State level: Integration of Health Program Integration of Health Program Integration of Health Program Integration of Health Program
information information information information
National Programs & National Programs & National Programs & National Programs & IntersectoralIntersectoralIntersectoralIntersectoral
Information exchangeInformation exchangeInformation exchangeInformation exchange
Types of integration by level of health
system
Content and level of integration
� At service delivery…integration of data collection instruments( registers, … or intake)
� At a district level…data management using the same personnel and facilities ( computers)
� At a provincial level information exchange for program supervisory /monitoring activities
� At national level…access given different health programs to a “ national HIS warehouse”.
Elements of HIS Integration
National Health Info System Development
HIS IntegrationContent
Routine HIS
Surveys, Census
Administrative IS
Levels
Resources& Training
Review and
Feedback
HIS IntegrationStrategy
Approach /
Methods
Strategy:Strategy:
1.1. Standardization strategyStandardization strategy
2.2. Data sharing strategyData sharing strategy
3.3. Process integration strategy( Process integration strategy( egegintegrated delivery of programs) integrated delivery of programs)
Note : one or many strategies can be Note : one or many strategies can be followedfollowed

Annex 3
- 27 -
Standardization strategy
� Standardizing strategy involves, having common data definitions, data formats, data transmission protocols etc.
� e.g. event/episode of care; length of stay
� Where data interchange is from computer to computer ( electronic data exchange) there are standards that have been developed for health data such as HL7.
Data sharing strategy
� Integration has also been successful in a number of countries that have used a shared “data repository”approach.
� Usually such repositories have been developed at national levels and follow the design principles of data warehousing.
� In other cases, data sharing, using a common data base at district/provincial levels have provided the impetus for sub systems to integrate their information systems and resources. Eg HISP
Data Warehouse DesignData Warehouse Design
Extract
Clean
Transform Data Warehouse
MCH
HIV
TB
Malaria
Data Capture
Data View
Process integration strategy
� This often occurs when integration of programmes for service delivery occurs .
� for example
integration of Reproductive Health /Sexual health and HIV VCT.
� processes of service delivery are integrated…common points of access and ..common protocols of assessment.
Implementation methods
� Examples
� Using minimum data sets/core indicators
� Integration of data management
Minimum data set approach
1. A national ministry determines an essential indicator/data set — this is the minimum reporting requirement for all facilities and health service providers in the country.
2. The next levels of management (regions, provinces, districts) adds indicators ( and data sets) that they believe they should collect in order to be able to manage their services efficiently

Annex 3
- 28 -
4. A facility develops an essential data set which includes indicators from the ministry, region and district, as well as their own indicators.
The type of information important for a facility management committee, and possibly for a district, is not necessarily relevant at the national or regional levels.
Pros and cons
� The use of minimum data sets/indicators reduces the burden in data collection and reporting
� As the indicators are the same….the data is common and reporting is standardized.
� Comparisons across, provinces, districts, facilities is possible
� An important outcome is that the process creates a
“ platform “ for integration.
Integration of data management: an example
� The Health Information Systems Project (HISP) has undertaken current efforts to establish integrated data sets in contexts as different as Addis Ababa (Ethiopia), Botswana, Zanzibar (United Republic of Tanzania), Andhra Pradesh (India) and Ho Chi Minh City (Viet Nam).
Here data sets from all or most programmes are combined and streamlined by sorting out overlaps, gaps and inconsistencies.
Programme-specific software applications are linked electronically to the District Health Information System, thus providing a shared data repository. (Braa, 2005)
DATA ELEMENT GROUPINGDATA ELEMENT GROUPING
Elements of HIS Integration
National Health Info System Development
HIS IntegrationContent
Routine HIS
Surveys, Census
Administrative IS
Levels
Resources& Training
Review and
Feedback
HIS IntegrationStrategy
Approach /
Methods

Annex 3
- 29 -
Integration of resources for HIS : personnel
and HIS skill development
This is an important component of NHIS development.
Isolated and fragmented Human Resource policies and practices have in most cases resulted in countries neglecting this issue.
There is the need for common training programs and support for all personnel in the health systems in developing their information handling capacity.
�� HIS personnel resources development also HIS personnel resources development also
required integration with organizations and required integration with organizations and
agencies outside the health sector such as agencies outside the health sector such as
Departments of Statistics and surveys and Departments of Statistics and surveys and Information Technology organizationsInformation Technology organizations in the in the
public and private sectors.public and private sectors.
�� The integration of positions for staff working in The integration of positions for staff working in
health and Department of statistics will build health and Department of statistics will build
institutionalized links between the organizations.institutionalized links between the organizations.
Integrating financial resources for HIS , including donor support.
� Many resource poor countries have multiple donors for the health sector.
� Some mechanisms such as SWAPs have created platforms for coordination of donor aid
� These mechanisms need to be explored for HIS developments.
Integration of HIS review and evaluation
� NHIS developments require regular reviews to ascertain developments and needs for the future.
� In most cases reviews on HIS , have been donor driven and focused identified health programme systems only.
� Regular integrated review, using the NHIS secretariat for coordination are required.
Elements of HIS Integration
National Health Info System Development
HIS IntegrationContent
Routine HIS
Surveys, Census
Administrative IS
Levels
Resources& Training
Review and
Feedback
HIS IntegrationStrategy
Approach /
Methods
Thank youThank youThank youThank you
Questions !!!Questions !!!Questions !!!Questions !!!

Annex 3
- 30 -

- 31 -
ANNEX 4
OUTPUTS OF WORKSHOP 1

Annex 4.1
- 32 - -
Workshop 1: Identification of Issues (Data Collection, Sharing and Use)
Country: Cambodia
Information System
Function Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
• Data items/ indicators:
− Demographic variables (age, especially for under 5, sex, location …)
− Geographic variables
− Case definition
− Denominator (population, target …)
• Vital statistic
• ICD-10
• HIV
• Child Survival
• DHF
• Core variables essential for specific stakeholders
• Minimized duplication of variables
• Diminished work load
• Better validated information
• Data collection/tools (ex., forms and registers used): electronic vs hard copy
• EPI (surveillance)
• HIV (surveillance)
• How will consensus be reached?
• Who will supply forms?
• Minimized duplication of forms
• Reports:
− Means of reporting
− Regularity, timeliness, accuracy, completeness
• EPI
• HIV
• Vertical linkage and support
• Ownership
• Partnership
• Improved planning
• Efficient budget used
• Data quality assurance
− Regular support
− Regular supervision
− Timely feedback and actions
• Vital statistic
• ICD-10
• HIV
• Child Survival
• DHF
• System set up
• Availability of qualified supervisory team members
• Improved planning
• Efficient budget used
• Better motivated staff
• Better policy setting and decision making
Data collection
• Resource
− Human: number, capacity, motivation
− Financial
• Recruitment / capacity building
• Donor contribution / allocation of budget
• Adequate workforce / resources
• Data management • All concerned stakeholder at all level
• Recruitment / capacity building
• Donor contribution / allocation of budget
• Improved efficiency of data processing
• Better information
• Facilities and infrastructures • All concerned stakeholder at all level
• Improved efficiency of data processing
• Better information
Data management and sharing
• Dissemination • All users • Improved accessibility and availability
• User friendly
• Service planning • Priority setting
• Additional information required
Data use
• M&E
• All concerned stakeholder
• Technical M&E sub-system required
• Improved effectiveness of service provision

Annex 4.1
- 33 -
Information System
Function Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
• Resources Allocation • Donor/Government contribution
• Equitable allocation
• Policy formulation • Enhanced use of information for policy formulation
• MTEF • Transparency and Predictability

Annex 4.2
- 34 -
Workshop 1: Identification of Issues (Data Collection, Sharing and Use) Country: China
Information System Function
Aspects Involved/Affected HIS subsystem
Involved Issues that are envisaged in integration
Key benefits
Data items/ indicators Health indicators system and National Health data dictionary
Agreed and being implemented. Further Coordination is required.
• Share
• Decrease duplication
Data collection tools (ex., forms and registers used)
Public Health information system(infectious disease, MCH, Chronic diseases, risk factors, environment surveillance) Health facility information system VR
How will consensus be reached? Who will supply forms?
• Minimize duplication of forms
Reports Year Book of Health Statistics
General and special reporting system should be further coordinated.
Promoting sharing of information
Data collection
Data quality assurance Special units are responsible for data quality assurance; units at higher level are responsible for the quality of data from the units at the lower level
Capacity of the local agencies is not enough, which should be improved.
Improve the liability of data.
Data storage Construction of national data centre is under the consideration of MOH.
Technically, data safety is the major concern.
It is helpful for a centralized management and improve the safety of the whole data system
Data sharing
Data retrieval The authorization to different agencies varies according to their different functions and levels.
Rationalizing the authorization is being studied with the consideration of the functions of different agencies.
The data in the centre could be used more efficiently.

Annex 4.2
- 35 -
Information System Function
Aspects Involved/Affected HIS subsystem
Involved Issues that are
envisaged in integration Key benefits
Data Analysis CHSI will make a general and comprehensive analysis. The related line technical departments will make a more detailed analysis in their own technical areas.
Weak in data analysis is a common problem at all levels in China.
Providing preliminary findings for policy-making.
Data sharing (con't)
Dissemination Year Book, publications, press conference, internet and other means of dissemination.
Identifying the most effective dissemination methods for different users of information should be further studied.
Improving the transparency of health information.
Data use Service planning M&E Resources Allocation Policy formulation
Based on health information, 11th 5-year national health development plan was developed.
Making full use of data for planning at the lower level governments should be improved.
Serving to the policy-making.
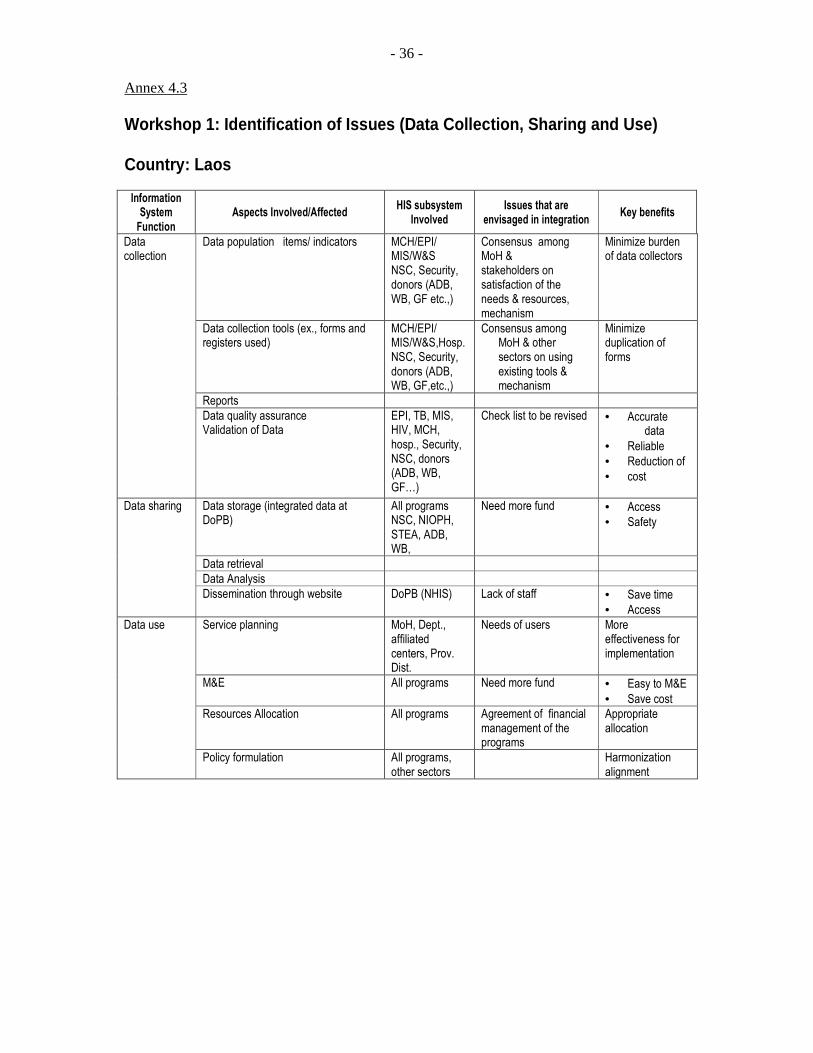
Annex 4.3
- 36 -
Workshop 1: Identification of Issues (Data Collection, Sharing and Use) Country: Laos
Information System
Function Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
Data population items/ indicators MCH/EPI/ MIS/W&S NSC, Security, donors (ADB, WB, GF etc.,)
Consensus among MoH & stakeholders on satisfaction of the needs & resources, mechanism
Minimize burden of data collectors
Data collection tools (ex., forms and registers used)
MCH/EPI/ MIS/W&S,Hosp. NSC, Security, donors (ADB, WB, GF,etc.,)
Consensus among MoH & other sectors on using existing tools & mechanism
Minimize duplication of forms
Reports
Data collection
Data quality assurance Validation of Data
EPI, TB, MIS, HIV, MCH, hosp., Security, NSC, donors (ADB, WB, GF…)
Check list to be revised • Accurate data
• Reliable
• Reduction of
• cost
Data storage (integrated data at DoPB)
All programs NSC, NIOPH, STEA, ADB, WB,
Need more fund • Access
• Safety
Data retrieval
Data Analysis
Data sharing
Dissemination through website DoPB (NHIS) Lack of staff • Save time
• Access
Service planning MoH, Dept., affiliated centers, Prov. Dist.
Needs of users More effectiveness for implementation
M&E All programs Need more fund • Easy to M&E
• Save cost
Resources Allocation All programs Agreement of financial management of the programs
Appropriate allocation
Data use
Policy formulation All programs, other sectors
Harmonization alignment
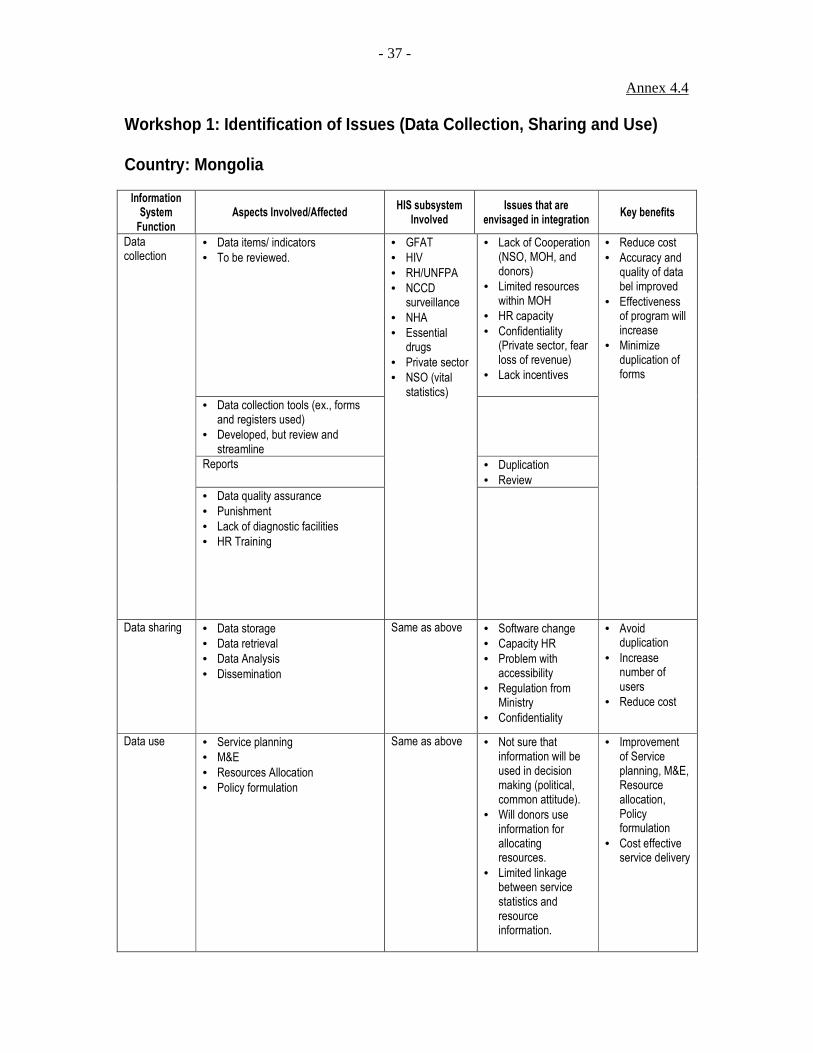
Annex 4.4
- 37 -
Workshop 1: Identification of Issues (Data Collection, Sharing and Use) Country: Mongolia
Information System
Function Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
• Data items/ indicators
• To be reviewed.
• Lack of Cooperation (NSO, MOH, and donors)
• Limited resources within MOH
• HR capacity
• Confidentiality (Private sector, fear loss of revenue)
• Lack incentives
• Data collection tools (ex., forms and registers used)
• Developed, but review and streamline
Reports
• Duplication
• Review
Data collection
• Data quality assurance
• Punishment
• Lack of diagnostic facilities
• HR Training
• GFAT
• HIV
• RH/UNFPA
• NCCD surveillance
• NHA
• Essential drugs
• Private sector
• NSO (vital statistics)
• Reduce cost
• Accuracy and quality of data bel improved
• Effectiveness of program will increase
• Minimize duplication of forms
Data sharing • Data storage
• Data retrieval
• Data Analysis
• Dissemination
Same as above • Software change
• Capacity HR
• Problem with accessibility
• Regulation from Ministry
• Confidentiality
• Avoid duplication
• Increase number of users
• Reduce cost
Data use • Service planning
• M&E
• Resources Allocation
• Policy formulation
Same as above • Not sure that information will be used in decision making (political, common attitude).
• Will donors use information for allocating resources.
• Limited linkage between service statistics and resource information.
• Improvement of Service planning, M&E, Resource allocation, Policy formulation
• Cost effective service delivery

Annex 4.5
- 38 -
Workshop 1: Identification of Issues (Data Collection, Sharing and Use) Country: Philippines Information
System Function
Aspects Involved/Affected HIS subsystem
Involved
Issues that are envisaged in integration
Key benefits
Data items/ indicators Who/which body will decide/say what minimum indicators to collect?
• Lessen the load of the data collector
• Efficient use of resources
• Data collection tools (ex., forms and registers used)
• Detection of outbreaks (national level)
• Human resource
A. PUBLIC HEALTH 1. Surveillance Systems - EPI, Influenza, HIV/AIDS, Salmonella, NESSS, Avian Influenza Notifiable Diseases 2. Registries - Disability - tumor/cancer 3. FHSIS B. Hosp/clinic mngmt is C. Corporate/administrative D. Regulatory is E. Social health insurance
• Duplication in data collection
• No common denominator (population count) --- NSO, CBMIS, LGU count, etc.)
--- projected vs actual --- political issue
• Vital statistics – from LGU vs NSO
• varied data collection tools at different levels
• Health programs have different info systems
• How will consensus be reached?
• Who will supply forms?
• Minimize duplication of forms
• Minimize load of health workers who are collecting data
Reports
Data collection
Data quality assurance Completeness of data
Data storage Confidentiality in data sharing
Data retrieval Accessibility of data from a central source/ point/warehouse
Will facilitate data retrieval and analysis
Data Analysis Lack of skill in analysis, fast turnover of personnel
Data sharing
Dissemination • No institutionalized feedback mechanism
• No full time staff specializing on data analysis & dissemination
Service planning
M&E • Varied M & E tools at different levels/at different programs
• Institutionalization of successful initiatives – e.g M & E tools which are project-based
Resources Allocation
Data use
Policy formulation Policies may not be applicable/appropriate at the local level
[

Annex 4.6
- 39 -
Workshop 1: Identification of Issues (Data Collection, Sharing and Use) Country: Viet Nam
Information System
Function Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
Data items/ indicators Hospital Information System and Public Health Information System
• Integrated Indicators • Save money and time
Data collection tools (ex., forms and registers used)
Hospital Information System and Public Health Information System
• A lot of forms issued by various programs and bodies
• Identification of a department who will supply forms
• Minimize duplication of forms
Reports Hospital Information System and Public Health Information System
• Poor coordination between relevant health sectors
• Low staff capacity
• Minimize of duplication of reports
Data collection
Data quality assurance Hospital Information System and Public Health Information System
• Data overlap
• Incomplete data
• Improve data quality
Data storage Hospital Information System and Public Health Information System
• Many data storages • Minimize risk of data loss
Data retrieval Hospital Information System and Public Health Information System
• Difficult to access data
• Easier to access data
Data sharing
Data Analysis Hospital Information System and Public Health Information System
• Low staff capacity • Easier to make comparison and link data
Service planning Hospital Information System and Public Health Information System
• Most of data has not been used for service planning
• Comprehensive planning for delivery of preventive and curative services
M&E Hospital Information System and Public Health Information System
• Easier to monitor and evaluate
Data use
Resources Allocation Hospital Information System and Public Health Information System
• Most of data has not been used for Resources Allocation
• Easier to allocate resources

Annex 4.6
- 40 -
- 41 -
ANNEX 5
OUTPUTS OF WORKSHOP 2

Annex 5.1
- 42 -
Workshop 2: Identification of Issues (Resources and Regulations for HIS) Country: Cambodia Information System
Component Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
• Number and type of staff needed at different levels
• Availability of positions
• Recruitment
• Staff turnover/ brain drain
• Mix of skills needed • Capacity building
• Capability building
HIS workforce
• Motivation
• All concerned stakeholders at all levels
• Performance based incentive
• Sharing of manpower involved in report generation
• acquisition of facilities/ communication infrastructure
• Funding
• MoH communication network
• software development
• DPHI/MoH
• Funding/Capacity
ICT
• maintenance of machines/ equipment • All levels • Maintenance system/guideline
• Resource (human and financial)
• Funding • ? • Predictability and transparency
• Equitable allocation according to country priority
• Commitment
Donor resources
• Technical assistance • Long term vs Short term
• Advocacy with proper bodies Regulations
• Development of policies, regulations and implementing guidelines
1. Bottlenecks/inhibiting factors in implementing the integration process in the country: Commitment of all concerned stakeholders (commitment of donors; political will of the government and implementers) 2. Facilitating factors that can hasten the process of integration in the country: Facilitating political environment, coordination
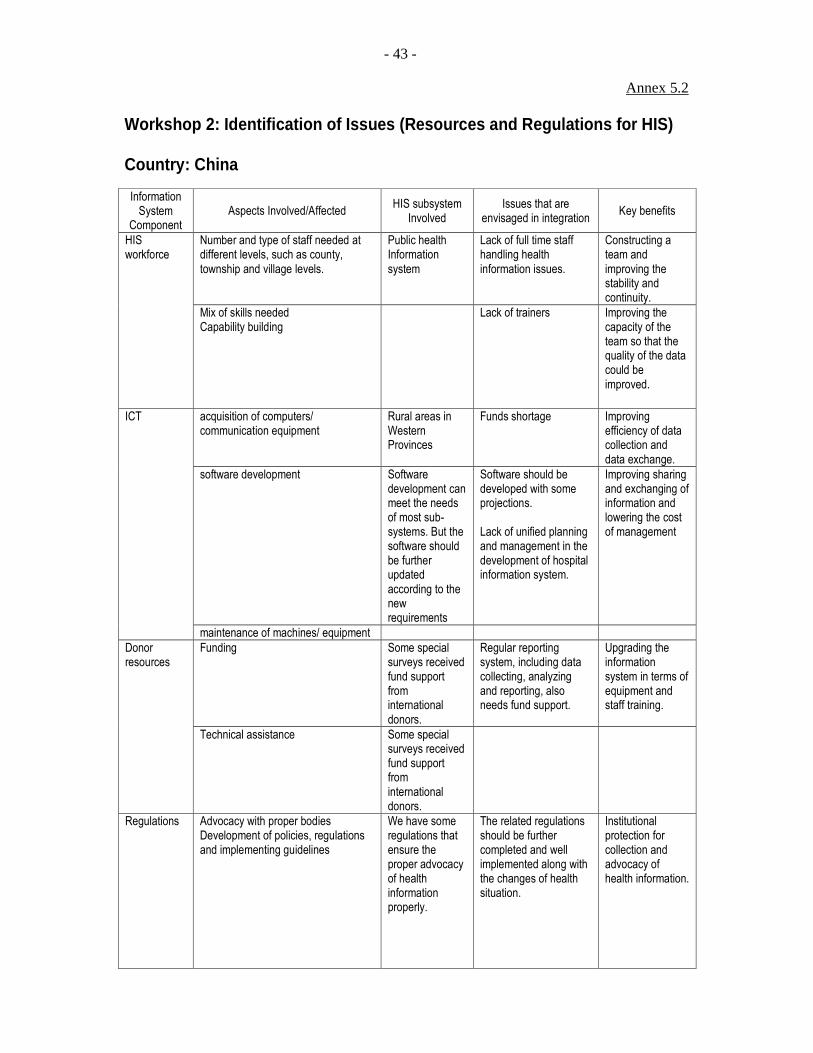
Annex 5.2
- 43 -
Workshop 2: Identification of Issues (Resources and Regulations for HIS) Country: China
Information System
Component Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
Number and type of staff needed at different levels, such as county, township and village levels.
Public health Information system
Lack of full time staff handling health information issues.
Constructing a team and improving the stability and continuity.
HIS workforce
Mix of skills needed Capability building
Lack of trainers Improving the capacity of the team so that the quality of the data could be improved.
acquisition of computers/ communication equipment
Rural areas in Western Provinces
Funds shortage
Improving efficiency of data collection and data exchange.
software development Software development can meet the needs of most sub-systems. But the software should be further updated according to the new requirements
Software should be developed with some projections. Lack of unified planning and management in the development of hospital information system.
Improving sharing and exchanging of information and lowering the cost of management
ICT
maintenance of machines/ equipment
Funding Some special surveys received fund support from international donors.
Regular reporting system, including data collecting, analyzing and reporting, also needs fund support.
Upgrading the information system in terms of equipment and staff training.
Donor resources
Technical assistance Some special surveys received fund support from international donors.
Regulations Advocacy with proper bodies Development of policies, regulations and implementing guidelines
We have some regulations that ensure the proper advocacy of health information properly.
The related regulations should be further completed and well implemented along with the changes of health situation.
Institutional protection for collection and advocacy of health information.
Annex 5.2
- 44 -
1. Bottlenecks/inhibiting factors in implementing the integration process in the country: Coordination among the ministries and line departments within MOH. Poor technical capacity in lower level agencies and in western provinces. 2. Facilitating factors that can hasten the process of integration in the country: The government attached great attention to the health development and reform. We have constructed relatively completed health information system. What we should do is to integrate the system properly. We have done something on integration and accumulated some experiences, such as Health Data
Dictionary.
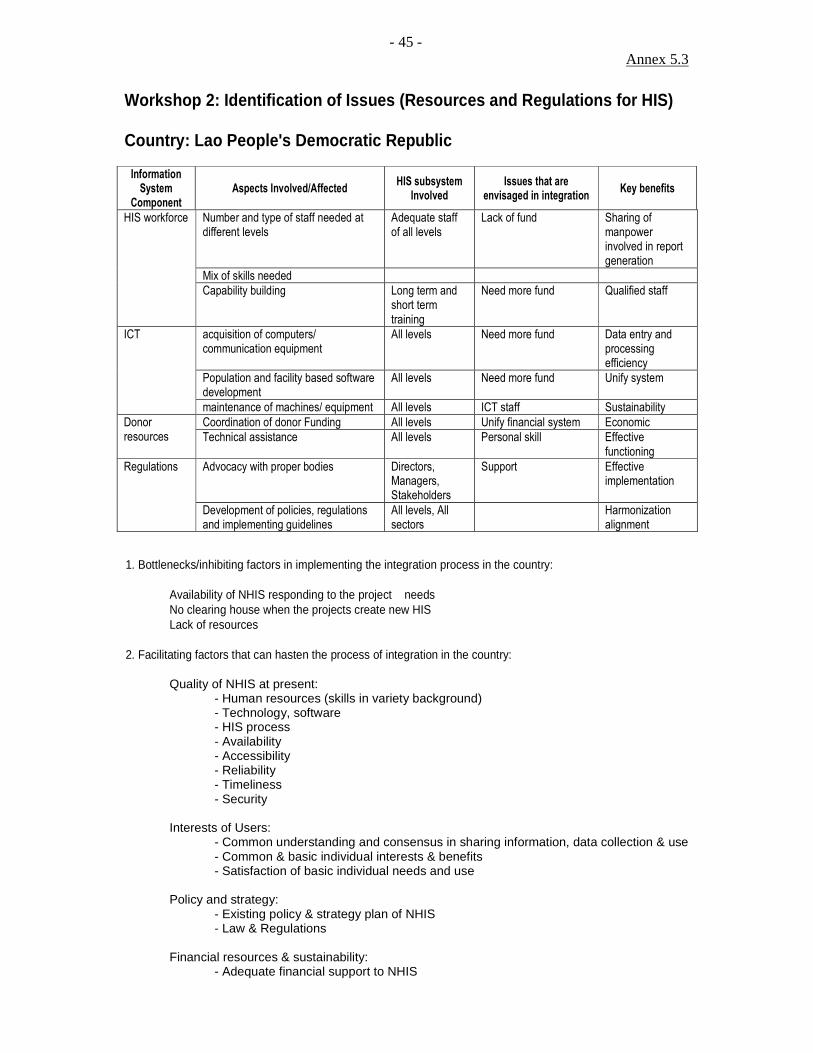
Annex 5.3
- 45 -
Workshop 2: Identification of Issues (Resources and Regulations for HIS) Country: Lao People's Democratic Republic
Information System
Component Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
Number and type of staff needed at different levels
Adequate staff of all levels
Lack of fund Sharing of manpower involved in report generation
Mix of skills needed
HIS workforce
Capability building Long term and short term training
Need more fund Qualified staff
acquisition of computers/ communication equipment
All levels Need more fund Data entry and processing efficiency
Population and facility based software development
All levels Need more fund Unify system
ICT
maintenance of machines/ equipment All levels ICT staff Sustainability
Coordination of donor Funding All levels Unify financial system Economic Donor resources Technical assistance All levels Personal skill Effective
functioning
Advocacy with proper bodies Directors, Managers, Stakeholders
Support Effective implementation
Regulations
Development of policies, regulations and implementing guidelines
All levels, All sectors
Harmonization alignment
1. Bottlenecks/inhibiting factors in implementing the integration process in the country: Availability of NHIS responding to the project needs No clearing house when the projects create new HIS Lack of resources 2. Facilitating factors that can hasten the process of integration in the country: Quality of NHIS at present: - Human resources (skills in variety background) - Technology, software
- HIS process - Availability - Accessibility - Reliability - Timeliness - Security
Interests of Users:
- Common understanding and consensus in sharing information, data collection & use - Common & basic individual interests & benefits - Satisfaction of basic individual needs and use
Policy and strategy: - Existing policy & strategy plan of NHIS - Law & Regulations Financial resources & sustainability: - Adequate financial support to NHIS

Annex 5.4
- 46 -
Workshop 2: Identification of Issues (Resources and Regulations for HIS) Country: Mongolia
Information System
Component Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
Number and type of staff needed at different levels
Mix of skills needed
HIS workforce
Capability building
• GFAT • RH/UNFPA • NCCD surveillance
• Reassignment of staff
• Assessment of staff needs
• Number of staff will be reduced and save resources
• Quality of staff will improve
acquisition of computers/ communication equipment
• Limited resources
software development • Standard operating software
•
ICT
maintenance of machines/ equipment
• Capacity building (difficulty recruiting good specialist)
• Improvement of data collection, transfer and dissemination
• Cost saving in long term
• Ease of maintenance
Funding • GFAT • WHO • UNFPA • ADB • HMN
• Pooling of funds
• Donors acceptability
• Ministries accountability
• Lack of duplication
• Cost saving
• Standardization and harmonization of supply
Donor resources
Technical assistance
Advocacy with proper bodies Regulations
Development of policies, regulations and implementing guidelines
• GFAT • HIV • RH/UNFPA • NCCD surveillance
• NHA • Essential drugs
• Private sector
• NSO (vital statistics
• Enforcement regulations by of programs
• Accessibility of regulation by donors
• Support implementation
• Coordination of stakeholders
1. Bottlenecks/inhibiting factors in implementing the integration process in the country:
Although number of HR is adequate capacity for integration needs to be strengthened Resistance from Donor Funded Projects Resistance in cooperation within MOH and other Departments Lack of adequate resources within Government
2. Facilitating factors that can hasten the process of integration in the country:
Existing well developed infrastructure for HIS. Good mechanisms for consultation with partners Ownership of system rest with country Sufficiency in HR
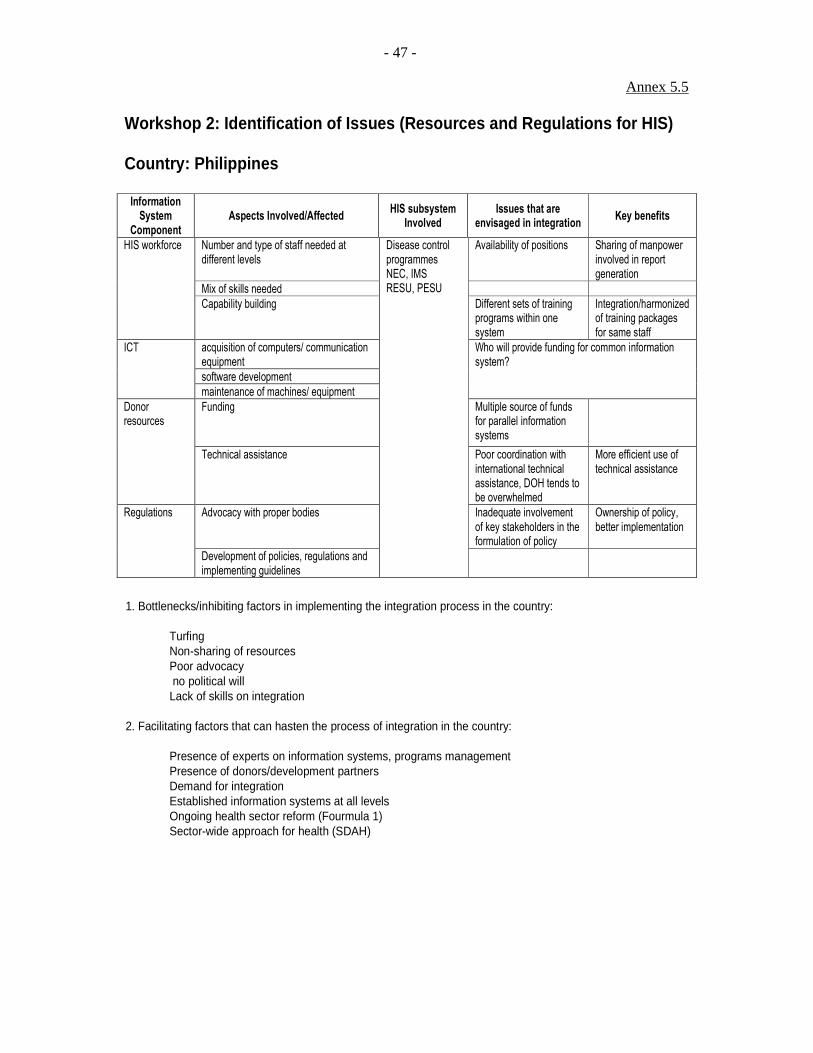
Annex 5.5
- 47 -
Workshop 2: Identification of Issues (Resources and Regulations for HIS) Country: Philippines
Information System
Component Aspects Involved/Affected
HIS subsystem Involved
Issues that are envisaged in integration
Key benefits
Number and type of staff needed at different levels
Availability of positions Sharing of manpower involved in report generation
Mix of skills needed
HIS workforce
Capability building Different sets of training programs within one system
Integration/harmonized of training packages for same staff
acquisition of computers/ communication equipment
software development
ICT
maintenance of machines/ equipment
Who will provide funding for common information system?
Funding Multiple source of funds for parallel information systems
Donor resources
Technical assistance Poor coordination with international technical assistance, DOH tends to be overwhelmed
More efficient use of technical assistance
Advocacy with proper bodies Inadequate involvement of key stakeholders in the formulation of policy
Ownership of policy, better implementation
Regulations
Development of policies, regulations and implementing guidelines
Disease control programmes NEC, IMS RESU, PESU
1. Bottlenecks/inhibiting factors in implementing the integration process in the country:
Turfing Non-sharing of resources Poor advocacy no political will Lack of skills on integration
2. Facilitating factors that can hasten the process of integration in the country:
Presence of experts on information systems, programs management Presence of donors/development partners Demand for integration Established information systems at all levels Ongoing health sector reform (Fourmula 1) Sector-wide approach for health (SDAH)

Annex 5.6
- 48 -
Workshop 2: Identification of Issues (Resources and Regulations for HIS) Country: Viet Nam
Information
System
Component
Aspects Involved/Affected HIS subsystem
Involved
Issues that are
envisaged in integration Key benefits
Number and type of staff
needed at different levels
Hospital Information
System and Public
Health Information
System (HIV/AIDS, TB,
CDs, Therapy Dept.,
EPI, MCH…)
Lack of trained staffs
under integrated system
Sharing of
manpower
involved in report
generation
Mix of skills needed Hospital Information
System and Public
Health Information
System
Lack of staffs with
needed skills
Make the data
collection easier
HIS workforce
Capability building Hospital Information
System and Public
Health Information
System
Lack of professional
trainers
Make the data
collection easier
acquisition of computers/
communication equipment
Hospital Information
System and Public
Health Information
System
Not enough (provincial
and district levels)
Make the data
collection and
data analysis
easier
software development Hospital Information
System and Public
Health Information
System
Has not been designed Make the data
collection and
data analysis
easier
ICT
maintenance of machines/
equipment
Hospital Information
System and Public
Health Information
System
Sharing responsibility for
maintenance (including
fund)
Make the system
work well
Donor
resources
Funding Hospital Information
System and Public
Health Information
System
Lack of fund for
development and
maintenance for
integration
Make the system
work well
Technical assistance Hospital Information
System and Public
Health Information
System
Lack of technical
supports at provincial
and district levels
Make the data
collection and
data analysis
easier

Annex 5.6
- 49 -
Regulations Development and enforcing
implementing guidelines
Hospital Information
System and Public
Health Information
System
Training and monitoring
at provincial and district
levels
Make the data
collection and
data analysis
easier
1. Bottlenecks/inhibiting factors in implementing the integration process in the country: Lack of human resource, equipment and fund 2. Facilitating factors that can hasten the process of integration in the country: The government knows the benefits of integration and is willing to make support activities for integration process.

Annex 5.6
- 50 -

- 51 -
ANNEX 6
OUTPUTS OF WORKSHOP 3

Annex 6.1
- 52 -
Workshop 3: Prioritization of HIS Components and Strategies, and Formulation of Country Action Plan
Country: Cambodia
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2 Strategies for Implementation Time-frame Resources needed
Data collection/ sharing
• Core variables essential for specific stakeholders
1 1 1 • Focusing on Child Survival, HIV/STI
• Technical & financial assistance (gov & health partner)
• Vertical linkage and support, Ownership, Partnership
1 3 1 • National Integrated HIS Policy
• Coordination
• Political will
• System set up 1 1 2 • Guideline on standard quality of data and system
• Technical & financial assistance (gov & health partner)
• Recruitment / capacity building
1 3 3 • Human resource mobilization and development
• Technical & financial assistance (gov & health partner)
• Donor contribution / allocation of budget
1 2 2 • Annual Forum (JAPR) for priority setting and proper resource mobilization/allocation
• Negotiation with donors
• Financial assistance (gov & health partner)
Data Use
• Priority setting (planning), enhanced use of information for policy formulation
1 1 3 • Encourage use of data for planning: information for actions
•
• Additional information required
1 1 3 • Review and minimized un-necessary indicators
•
• Transparency and Predictability
1 2 2 • Annual Forum (JAPR) for priority setting and proper resource mobilization/allocation
• Negotiation with donors
• Technical & financial assistance (gov & health partner)
1 Ranks for perceived impact and feasibility (columns 2 and 3) were assigned using a 3-point scale as follows:
1- High Priority 2 - Medium Priority
3 - Low priority
2 The overall priority rating (column 4) was assigned by ranking vertically according to impact, feasibility and other factors based on the key information functions/components listed in column (1).

Annex 6.1
- 53 -
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2 Strategies for Implementation Time-frame Resources needed
HIS Workforces
• Staff turnover, brain drain
1 2 2 • Performance based incentive
• Continue capacity building
• Technical & financial assistance (gov & health partner)
ICT
• MoH communication network
1 2 3 • Advocacy on the need with stakeholders
• Communication network development & establishment (data management unit)
•
• Funding/Capacity 1 2 2 • Annual Forum (JAPR) for priority setting and proper resource mobilization/allocation
• Financial assistance (gov & health partner)
• Maintenance system
1 2 4 • Maintenance & operational guideline
• Technical & financial assistance (gov & health partner)

Annex 6.2
- 54 -
Workshop 3: Prioritization of HIS Components and Strategies, and Formulation of Country Action Plan
Country: China
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2
Strategies for Implementation
Time-frame Resources needed
Data collection Developing Health Data Dictionary
1 1 1 Consolidate data into a single form
10 Months Technical support for develop-ment of consoli-dated form funds for printing of consoli-dated form
Standardized the Statistical Forms
1 1 2 The Forms will be approved and confirmed by the NBS and those form the base of the institutional health statistics, which is in conformity with the Law of Statistics Technical and administrative coordination is required.
6 Month Technical experts are required.
Data Quality Assurance
2 1 3 Developing data quality standard and data quality control procedures. Staff training.
3 Month 6 Month
Technical and financial assistance is required
Data use: Promoting integrated utilization of health information for health policy-making
1 2 4 Strengthening the communications between policy-makers and data managers. Improving researchers’ capacity in comprehensive analyzing data. Borrowing foreign advanced research and analyzing technologies. Using the basic principles of Knowledge Management.
Long term issue
The technical and financial requirements will be proposed once the implementation plan is finalized.
Data Sharing
1 1 5 Establishing a mechanism for data sharing; Constructing unified National Health Data Centre that can be shared Ensuring the use of historical data
2 years Technical and financial assistance is required.
1 Ranks for perceived impact and feasibility (columns 2 and 3) were assigned using a 3-point scale as follows:
1- High Priority 2 - Medium Priority
3 - Low priority
2 The overall priority rating (column 4) was assigned by ranking vertically according to impact, feasibility and other factors based on the key information functions/components listed in column (1).

Annex 6.3
- 55 -
Workshop 3: Prioritization of HIS Components and Strategies, and Formulation of Country Action Plan
Country: Laos
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2 Strategies for Implementation Time-frame Resources needed
Population� items/ indicators Data collection tools New NHIS�
1 1 1 Forms /Training Implement the new HIS
2 years Local staff
Data quality assurance � Validation of Data�
2 1 8 Training within and out side country
1 month Recruitment of local and external staff
Integrated data storage�
2 2 11 Creation the data ware house
15 days External assistant
Dissemination through website��
1 1 4 Creation network in website, training
1 month Local assistant
Data use Service planning�
1 1 5 Training Center, Provincial, District Staff
3 months External, Local assistant
Data use M & E� 1 1 6 Set up standard of M & E Training Center, Provincial, District Staff
3 months External, Local assistant
Resources Allocation ��
1 1 10 Recruitment and budget 5 years
Donors Budget
HIS workforce/ capacity building ��
1 1 2 Long term and short term training of basics statistics, data analysis and data management
5 years Donors Budget
ICT development��
1 1 3 Install computers equipments maintenance. training
2 years Donors Budget and local assistant
Coordination of Donor Funding��
1 1 9 Regular meeting with stakeholder partner
5 years
Cleaning House 2 1 12 Creation of Cleaning mechanism
1 month
Regulations & policy �
1 1 7 Policy formulation 1 year
1 Ranks for perceived impact and feasibility (columns 2 and 3) were assigned using a 3-point scale as follows:
1- High Priority 2 - Medium Priority
3 - Low priority
2 The overall priority rating (column 4) was assigned by ranking vertically according to impact, feasibility and other factors based on the key information functions/components listed in column (1).

Annex 6.4
- 56 -
Workshop 3: Prioritization of HIS Components and Strategies, and Formulation of Country Action Plan
Country: Mongolia
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2 Strategies for Implementation Time-frame Resources needed
Data collection 1 1 1 • Add Stakeholders to steering committee (GFATM, GAVI, NHA, PHI)
• Develop data dictionary for integrated HIS.
• Improve capacity of all level information providers and users
1 month 1 year 1 year
USD 15,000 USD 50,000
Data sharing 1 2 6 • Minister order
• Establish center data warehouse
• Developing and integrated software
• Develop guidelines for sharing information.
• Building capacity for all health statisticians
1 month 1 year 2 year 1 year 3 years
USD 10,000 USD 10,000+ technical support USD 5,000
Data use 1 2 5 • Advocacy for all stakeholders
• Regular consultation for donors
• Develop Executive management system for decision making
On going On going 2 years
USD 1,000 USD 1,000 Technical support + USD 20,000
HIS workforce 1 3 4 • Capacity building for integrated system for providers and users.
• Reasignment of staff
3 years 3 years
USD 100,000 0
ICT. 2 2 3 • Standard software
• Develop guidance
2 years 1 year
USD 5,000 USD 5,000
Donor resources 1 3 2 • Advocacy for all donor On going USD 1,000
• Persuade donors to pool funds to support integrated HIS work plan
• Prepare transfer rant financial and technical report
On going Annually
0 USD 5,000
Summary of resources
Financial Technical support
USD 250,000 Several STC
We will be request support from HMN above all resources
1 Ranks for perceived impact and feasibility (columns 2 and 3) were assigned using a 3-point scale as follows:
1- High Priority 2 - Medium Priority
3 - Low priority
2 The overall priority rating (column 4) was assigned by ranking vertically according to impact, feasibility and other factors based on the key information functions/components listed in column (1).

Annex 6.5
- 57 -
Workshop 3: Prioritization of HIS Components and Strategies, and Formulation of Country Action Plan
Country: Philippines
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2
Strategies for Implementation Time-frame Resources needed
DATA COLLECTION, SHARING & USE
Q4 2006-Q1 2007
Funds for workshop/meeting and consultant
Who/which body will decide/say what minimum indicators to collect?
1 1 1 Same
No common denominator (population count) --- NSO, CBMIS, LGU count, etc.) --- projected vs actual ( political issue)
2 2 12
Duplication in data collection due to varied data collection tools, specific program info systems, M & E systems at different
levels→ results to different sets of training programs
1 2 4
• Create TWG to address the issues on core indicators and denominators and duplication
• Develop standards and protocols for data generation (e.g. who will generate IMR, what population data to use, etc), data sharing, data security and confidentiality and access
• Assess info systems and recommend solutions to eliminate duplication and address submission issues
Incomplete data 1 2 5 See above Same
Non-confidentiality in data sharing
2 1 11 See above Same
Accessibility of data from a central source/point/warehouse
1 1 2 See above Q2 2007 Funds for ICT and Data warehouse
1 Ranks for perceived impact and feasibility (columns 2 and 3) were assigned using a 3-point scale as follows:
1- High Priority 2 - Medium Priority
3 - Low priority
2 The overall priority rating (column 4) was assigned by ranking vertically according to impact, feasibility and other factors based on the key information functions/components listed in column (1).

Annex 6.5
- 58 -
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2
Strategies for Implementation Time-frame Resources needed
Lack of skill in analysis, dissemination and feedback/ No institutionalized feedback mechanism on data analysis
1
2
8
Training needs assessment.
Q2 2007 Training funds
Fast turnover of personnel/ No full time staff specializing on data analysis & dissemination
1
3
10
Outsource contractual staff
Q3 2007 Funds for contractual personnel
No Institutionalization of successful initiatives – e.g M & E tools which are project-based
1
1
3
Develop functional benchmarking mechanisms for maximizing best practices and learning and integrate with DOH KM Plan.
Q2-Q4 2007 Study tours and best practices visits
Policies may not be applicable/ appropriate at the local level; Inadequate involvement of key stakeholders in the formulation of policy
1
2
7
Institute a policy audit system that would address the issue of implementation
Q3 2007 Funds for system development
RESOURCES AND REGULATIONS FOR HIS
• Focus on MCH and EPI programmes as starting point
• Consolidate data into a single form
3 months Technical support for development of consolidated form funds for printing of consolidated form
Who will provide funding for common information system/ Multiple source of funds for parallel information systems
1 2 6 Source out funding for a central information system
Funding for a central HIS
Poor coordination with international technical assistance, DOH tends to be overwhelmed
2 1 7 Request assistance from WHO in managing donors
Fund for capability development on donor management
No available positions
1 3 13 Killer problem
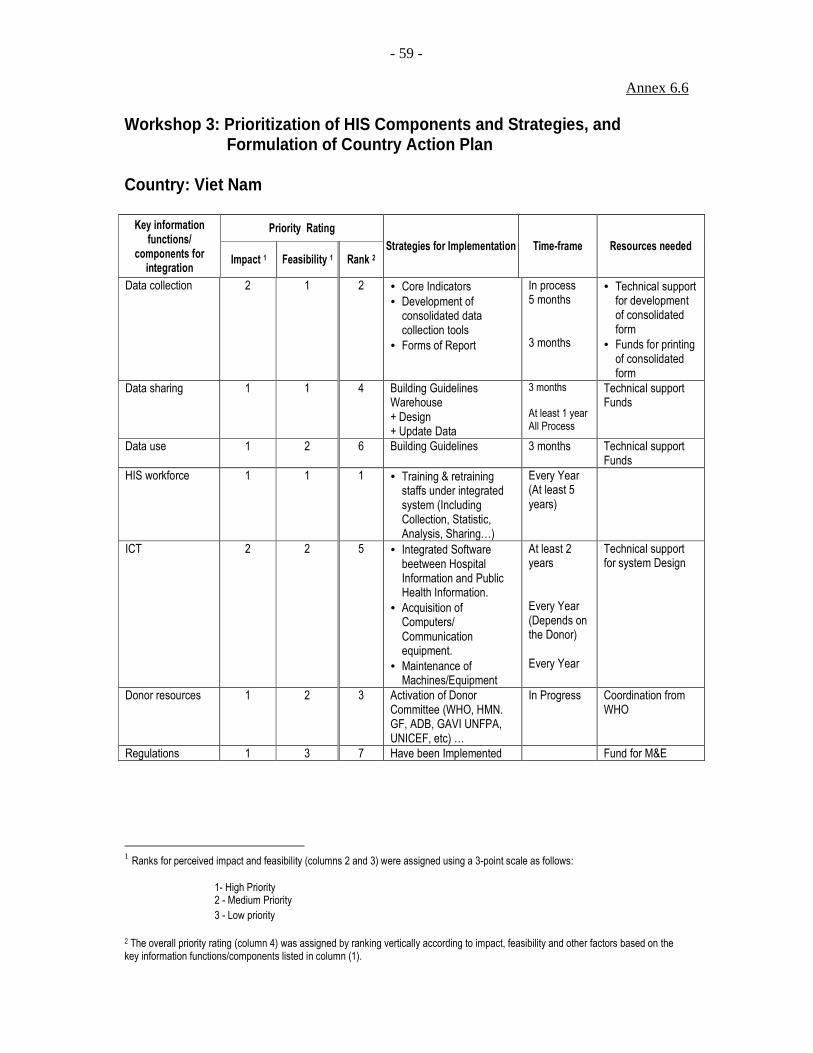
Annex 6.6
- 59 -
Workshop 3: Prioritization of HIS Components and Strategies, and Formulation of Country Action Plan
Country: Viet Nam
Priority Rating Key information functions/
components for integration
Impact 1 Feasibility 1 Rank 2 Strategies for Implementation Time-frame Resources needed
Data collection 2 1 2 • Core Indicators • Development of consolidated data collection tools
• Forms of Report
In process 5 months 3 months
• Technical support for development of consolidated form
• Funds for printing of consolidated form
Data sharing 1 1 4 Building Guidelines Warehouse + Design + Update Data
3 months At least 1 year All Process
Technical support Funds
Data use 1 2 6 Building Guidelines 3 months Technical support Funds
HIS workforce 1 1 1 • Training & retraining staffs under integrated system (Including Collection, Statistic, Analysis, Sharing…)
Every Year (At least 5 years)
ICT 2 2 5 • Integrated Software beetween Hospital Information and Public Health Information.
• Acquisition of Computers/ Communication equipment.
• Maintenance of Machines/Equipment
At least 2 years Every Year (Depends on the Donor) Every Year
Technical support for system Design
Donor resources 1 2 3 Activation of Donor Committee (WHO, HMN. GF, ADB, GAVI UNFPA, UNICEF, etc) …
In Progress Coordination from WHO
Regulations 1 3 7 Have been Implemented Fund for M&E
1 Ranks for perceived impact and feasibility (columns 2 and 3) were assigned using a 3-point scale as follows:
1- High Priority 2 - Medium Priority
3 - Low priority
2 The overall priority rating (column 4) was assigned by ranking vertically according to impact, feasibility and other factors based on the key information functions/components listed in column (1).


















