Wound Assessment and Treatment
17
10/10/2016 1 Wound Assessment and Treatment Holly Kirkland-Walsh, PhD, FNP, GNP, CWCN The Nurses Domain • Reasons for admission • Review co-morbidities/systemic factors affecting wound healing • Nutritional status • Social determinants of health Overall Assessment Patient History • Reason for Admission • Disease processes • Medications • Nutritional Status • Vascular studies- ABI • Body habitus • Previous wound history • Therapies received • Radiation • Functional support • Discharge home?
Transcript of Wound Assessment and Treatment
10/10/2016
1
Wound Assessment and Treatment
Holly Kirkland-Walsh, PhD, FNP, GNP, CWCN
The Nurses Domain
• Reasons for admission
• Review co-morbidities/systemic factors
affecting wound healing
• Nutritional status
• Social determinants of health
Overall Assessment
Patient History
• Reason for Admission
• Disease processes
• Medications
• Nutritional Status
• Vascular studies- ABI
• Body habitus
• Previous wound history
• Therapies received
• Radiation
• Functional support
• Discharge home?

10/10/2016
2
Physical Exam
• Head to toe skin assessment:
– Rashes
– Pressure points
– Scars
– Edema, capillary refill, hemosiderin
staining
– Callus formation in DM
– BMI
Cause of wound
• Surgical
• Traumatic
• Neuropathic
• Vascular
• Mixed
• Pressure related
• Fungating
Wound Assessment
• Location
• Age of wound
• Size and Shape
• Tunneling, undermining, fistulas
• Exudate color, amount, consistency
• Surrounding skin discolored, edema, erythema
• Wound edges: attached or rolled

10/10/2016
3
Wound assessment (cont’d)
• Maceration of edges
• Erythema, epithelialization, eschar
• Necrotic tissue: yellow, black or brown %
• Odor of wound
• Wound bed: granulation tissue
• Tenderness to touch, temperature, tautness
Measurement
• Linear measurements of greatest length 12 o'clock to 6 o'clock or nearest
• Width perpendicular
• Depth, undermining, tunnels
TIME Framework

10/10/2016
4
T is for Tissue
• Description: wound bed
• Color: Pink, yellow, grey, brown, green
• Thickened?
• Normal for this anatomical site?

10/10/2016
5
I- is for infection/Iatro/Inflammation
• Differentiate infection from normal granulation tissue
• Odor: mostly pseudomonas smells like ammonia
• Do not culture: The only way to know is to
take a deep tissue sample
• Gold standard for r/o osteomyelitis is bone biopsy

10/10/2016
6
Infection and inflammation
M- Moisture Balance
• For those wounds that fall between the cracks
• For those wounds that are way too wet
• In wounds the treatment rule is:
• If it is too wet, dry it- and if it is too dry, wet it
10/10/2016
7
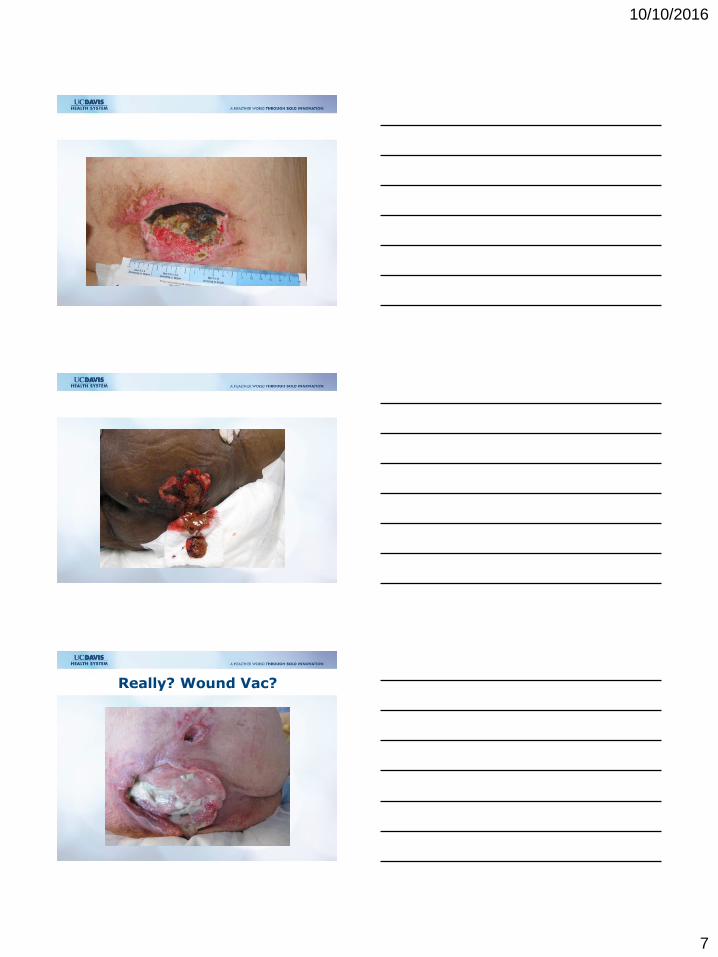
Really? Wound Vac?

10/10/2016
8
Challenges with New Anatomy
Managing Moisture
E- Edges
• Thickened? Thin? Discolored? Scarring? Discrete? Defined?
• Wounds heal from the edges
• If a signal goes to the wound saying edges are healed- wound will be stalled
• The treatment involves debridement

10/10/2016
9
Bonus photo: edges & moisture
Concepts to Promoting Healing
• Important Aspects of Wound Healing or goals of care
– Wound cleansing/odor control
– Wound debridement strategies
– Treatment of infection/ bioburden
– Maintaining moisture balance for epithelialization
– Management of wound pain
10/10/2016
10
Goals for Product Choice
• Regular assessment entire patient-engage pt
• TIME assessment of wound
• Keep wound bed clean and moist
• Keep surrounding skin clean and dry
• Few dressing changes as will allow-(no wet-
dry)
• Decrease pain and edema
• Change plan of care every 2 weeks if stalled
• Keep it simple
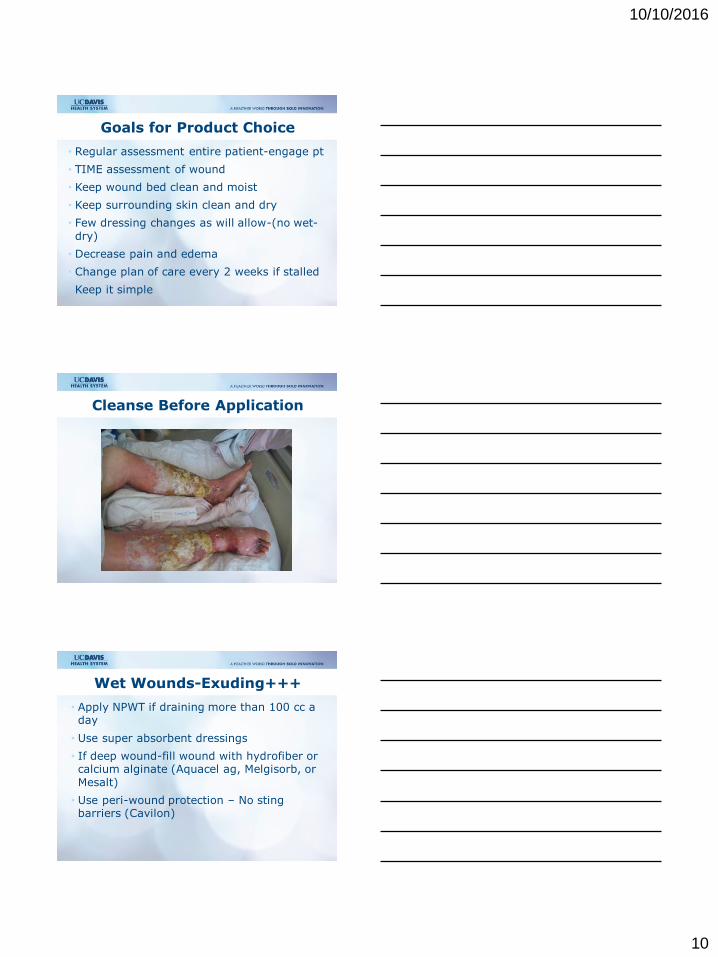
Cleanse Before Application
Wet Wounds-Exuding+++
• Apply NPWT if draining more than 100 cc a day
• Use super absorbent dressings
• If deep wound-fill wound with hydrofiber or calcium alginate (Aquacel ag, Melgisorb, or
Mesalt)
• Use peri-wound protection – No sting barriers (Cavilon)
10/10/2016
11

10/10/2016
12
Dry wounds
• Need debridement
• Autolytic- cover with a hydrocolloid , honey,
etc
• Surgical- may not be suitable
• Enzymatic- Santyl
• May wet and add bio (maggots)
Indications for use
Debridement of non-healing soft tissue and necrotic wounds, these include:
• Pressure Ulcers
• Neuropathic Foot Ulcers
• Chronic Leg Ulcers
• Post-Operative/Traumatic Wounds
• FDA approved uses as of 2004

10/10/2016
13
Honey Dressing
Promotes autolysis of wounds and the removal of slough and
dead tissue
Creates a moist, healing environment in which new
cells can flourish
Neutralizing malodor (within
12 to 24 hours)
Options: Iodosorb or Hydrogel
• Must wet the eschar
• Possibly score it
• Cover with NPWT drape and let it cook
Case Study 1- Evolution

10/10/2016
14
Case Study 2-Evolution
10/10/2016
15
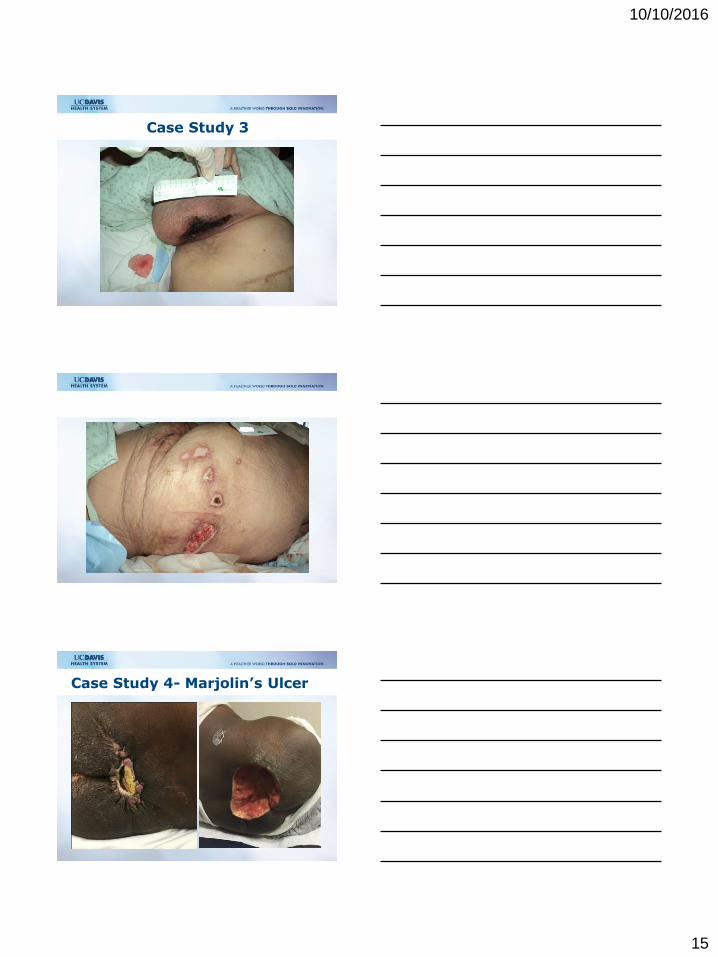
Case Study 3
Case Study 4- Marjolin’s Ulcer

10/10/2016
16
Research
Group
#of
pts Age Sex LOS
PU
present SBP DBP Braden Hct
BM
I Shock Dialysis
Surgery
time for
all
Surger
y time
surgica
l pts
Pressor
use
General 76 58.9
m=46
f=30 12.8
10.5%
(8=yes) 121 66 14
30.
7 30 9.2% 14.5% 2.46 5.83 15.8%
HAPU 43 54.95
m=28
f=15 24.9 100% 89 46 13
25.
4 31 60.5% 51.2% 11.3 13.2 60.5%
Comparison: general ICU population vs HAPU patients
Pressure Mapping
Low-air-loss bed

10/10/2016
17
Low-air-loss bed w seat cushion
Questions?