Would a radiologic examination be useful ?
8
description
Would a radiologic examination be useful ?. In short; there is insufficient evidence to support or refute the utility of MRI to identify neurovascular compression in classic TN, or to indicate the most reliable MRI technique But…. - PowerPoint PPT Presentation
Transcript of Would a radiologic examination be useful ?


Would a radiologic examination be useful?
In short; • there is insufficient evidence to support or refute the utility of MRI to identify
neurovascular compression in classic TN, or to indicate the most reliable MRI technique
But….• Neuroimaging with head CT or MRI is useful for identifying the small
proportion of patients who have a structural lesion (eg, tumor in the cerebellopontine angle, demyelinating lesions including multiple sclerosis) as the cause of secondary TN.
• In addition, high resolution MRI and magnetic resonance angiography (MRA) may be useful for identifying vascular compression as the etiology of classic TN, but the utility of these studies has not been established.
It is suggested to obtain brain MRI for patients in the following groups to rule out a causative structural brain lesion:• Patients with trigeminal sensory loss• Patients with bilateral symptoms• Young patients (under the age of 40)

How is this conditioned managed?
carbamazepine controlled-release 100 mg orally, once or twice daily; increase as tolerated and according to response every 7 days up to a maximum of 600 mg twice daily.• After pain relief has been maintained for several weeks, the dose should be gradually
reduced to establish the minimum dose that will provide good pain control.
If carbamazepine is ineffective, options include referral to a neurosurgeon or trial of other drugs alone or in combination with carbamazepine.
Murtagh suggests these as options for alternative drug therapy:• Gabapentin• Phenytoin• Clonazepam• Baclofen
Surgery• Possible procedures include:
Decompression of the trigeminal nerve root (eg. Gel foam packing between the nerve and blood vessels
Thermocoagulation/radiofrequency neurolysis Surgical division of the peripheral branches

THE REST OF THIS DOC IS A GOOD CONCISE SUMMARY OF TRIGEMINAL NEURALGIA FROM MURTAGHS

Trigeminal neuralgia Trigeminal neuralgia (tic
douloureux) is a condition of often unknown cause that typically occurs in patients over the age of 50, affecting the second and third divisions of the trigeminal nerve and on the same side of the face.
Brief paroxysms of pain, often with associated trigger points, are a feature.

Typical clinical features Site: sensory branches of the trigeminal nerve almost always unilateral (often right side) Radiation: tends to commence in the mandibular division and spreads to the maxillary
division and (rarely) to the ophthalmic division Quality: excruciating, searing jabs of pain like a burning knife or electric shock Frequency: variable and no regular pattern Duration: 1 - 2 minutes (up to 15 minutes) Onset: spontaneous or trigger point stimulus Offset: spontaneous Precipitating factors: talking, chewing, touching trigger areas on face (e.g. washing,
shaving, eating), cold weather or wind, turning onto pillow Aggravating factors: trigger points usually in the upper and lower lip, nasolabial fold or
upper eyelid Relieving factors: nil Associated features:
• rarely occurs at night• spontaneous remissions for months or years
Signs: there are no signs, normal corneal reflex Causes:
• unknown• local pressure on the nerve root entry zone by tortuous pulsatile dilated small vessels (probably up to
75%)• multiple sclerosis• neurosyphilis• tumours of the posterior fossa
Note: Precise diagnosis is essential.

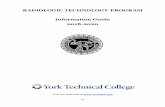
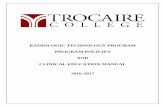
Typical cutaneous sensory distribution of the trigeminal
nerve and its branchesTrigeminal neuralgia: typical
trigger points

Treatment Patient education, reassurance and empathic support is very important
in these patients. Medical therapy:
• carbamazepine (from onset of the attack to resolution)4 50 mg (elderly patient) or 100 mg (o) bd initially, gradually increase the dose to avoid drowsiness every 4 days to 200 mg bd (maintenance); testing serum levels is unnecessary; higher dosage may be necessary
• alternative drugs if carbamazepine not tolerated or ineffective (but question the diagnosis if lack of response) gabapentin 300 mg daily initially, then increase phenytoin 300 - 500 mg daily clonazepam baclofen
Surgery:• refer to a neurosurgeon if medication ineffective• possible procedures include:
decompression of the trigeminal nerve root (e.g. gel foam packing between the nerve and blood vessels)
thermocoagulation/radiofrequency neurolysis surgical division of peripheral branches