WORRIED ABOUT AUDITS? · Agenda Are you asking your organization about RAC audits? Why that is the...
64
WORRIED ABOUT AUDITS? Why it’s more than just RAC. Presentation by Jill A Medley, MS, CHC, CHPC
Transcript of WORRIED ABOUT AUDITS? · Agenda Are you asking your organization about RAC audits? Why that is the...

WORRIED ABOUT AUDITS? Why it’s more than just RAC. Presentation by Jill A Medley, MS, CHC, CHPC

Agenda ■ Are you asking your organization about RAC
audits? Why that is the wrong question.
■ How OVHS&E got its third party medical record audits under control.

ASKING ABOUT RAC AUDITS?

Common Questions How much money have we lost to RAC audits? How many RAC audits have we had in 2016? What is the annual RAC audit impact on our financials? What is the dollar amount of RAC take backs in a given period of time? What is the RAC impact to our organization? What is the dollar amount of RAC denials during an audited fiscal year?

ARE YOU REALLY ASKING ABOUT RAC AUDITS?

Medicare FFS Auditors Medicare Administrative Contractors (MACs) Comprehensive Error Rate Testing (CERT) Zone Program Integrity Contractors (ZPICs) Supplemental Medical Review Contractor (SMRC) Recovery Auditors (RACs, RAs) Quality Improvement Organizations (QIO)

MEDICARE ADMINISTRATIVE
CONTRACTORS MACs

Medicare Administrative Contractors (MACs) Process claims submitted by physicians, hospitals and other health care professionals and pay those providers according to Medicare rules and regulations. The MACs role includes identifying and correcting underpayments and overpayments.

MACs are the Money
Medicare Administrative Contractors (MACs)

Process Medicare FFS Claims Limited authority to set payment policy
Interpret Medicare Policy Local Coverage Determinations (LCDs)
Educate providers on Medicare payment rules Conduct audits to ensure appropriate payment
Post Payment Reviews Prepayment Reviews
Medicare Administrative Contractors (MACs)

Medicare Administrative Contractors Current MAC Audit Targets (Palmetto GBA): 66984 Outpatient Cataract Removal J9310 Rituximab J1745 Infliximab DRG 460 Spinal Fusion DRG 470 Major Joint Replacement

COMPREHENSIVE ERROR RATE TESTING
CERTs

Comprehensive Error Rate Testing (CERT)
Collect documentation and perform reviews on a statistically valid random sample of Medicare FFS claims to produce an annual improper payment rate.

CERT Determines Medicare Payment Error Rate Random audits Audit results are used to calculate payment error rate Issues reports on payment error patterns Identified errors sent to MAC for payment adjustment
Comprehensive Error Rate Testing CERT is the only Medicare auditor
that does RANDOM audits. The other auditors do targeted or
focused audits. That means that most auditors target problem prone areas where payment
errors are likely.

0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
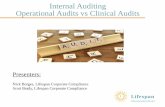
CERT Improper Payment Rate

Comprehensive Error Rate Testing (CERT) In 2009, an “improved” review methodology was implemented in the CERT program. This change included more strict enforcement of Medicare payment policies, resulting in a corresponding increase in the improper payments identified during subsequent years. Most of the increase is due to strict adherence to Medicare policy regarding documentation and signature requirements, the removal of claims history as a valid source for review information, and the determination that medical record documentation received only from a supplier, as opposed to an ordering provider, is insufficient to substantiate a claim.

ZONE PROGRAM INTEGRITY CONTRACTORS
ZPICs

Zone Program Integrity Contractors (ZPICs) Perform investigations that are unique and tailored to specific circumstances and occur only in situations where there is potential fraud and take appropriate corrective actions.


SUPPLEMENTAL MEDICAL REVIEW CONTRACTORS
SMRCs

Supplemental Medical Review Contractor (SMRC) Conducts nationwide medical reviews as directed by CMS (includes identifying underpayments and overpayments).
Performs reviews in accordance with the CMS Program Integrity Manual. Audit projects may include items identified by CERT audits, OIG audits and PEPPER report findings.



RECOVERY AUDIT CONTRACTORS
RACs or RAs

RAC or RA Focused reviews of paid Medicare claims Review issues approved by CMS Complex and automated reviews
Complex—with review of medical record Automated—no medical record—claims data only
Paid on a contingency fee basis (9%-12.5%) Identified errors sent to MAC for payment adjustment
Recovery Audit Contractors

Why are RACs so controversial? Paid on a contingency fee basis History of focus on overpayments History of focus on inpatient medical necessity denials
Inpatient v/s observation—entire payment is at risk DRG denials—only part of payment is at risk
Program changes limit the RACs ability to audit and profit from inpatient medical necessity denials.
Recovery Audit Contractors


Patient Status versus DRG Audits Patient Status Reviews: Take back is the entire payment amount. Providers originally had no recourse outside of appeal. Program improvements have added Part A to Part B billing. Program improvements have reduced look back period for patient status reviews to 6 months.
DRG Reviews: Take back is the difference between the DRG billed and the DRG determined on audit. Providers are able to appeal.


$-
$500.0
$1,000.0
$1,500.0
$2,000.0
$2,500.0
$3,000.0
$3,500.0
$4,000.0
2010 2011 2012 2013 2014 2015
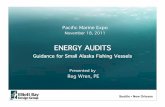
RAC Improper Payment Corrections
Overpayments Underpayments Net Overpayments


Increased use of observation by hospitals leading to the implementation of the 2 midnight rule.
The large number of provider appeals in response to RAC denials has “clogged” up the Medicare appeals process.
As a result, CMS offered a 68% settlement to providers for appealed short stay inpatient denials.
RAC findings have prompted MACs to increase prepayment audit activity.
The RAC Effect

Current RAC Activities CMS is in active procurement process for next round of RAC contracts. Current contractors are closing existing reviews. Last date current contractors can send request for medical record: May 16, 2016 Last date current contractors can send notification of improper payment: July 29, 2016 Last date that current contractors can send a payment adjustment to the MACs: October 1, 2016


Recovery Audit Contractors
RACs Have Rules RAC Scope of Work

Summary of RAC Program Enhancements Accuracy Rate of Audits: Overturn rate of less than 10% at first level of appeal.
95% accuracy rate as determined by validation contractor.
Lookback Period: Reduced to 6 months for patient status reviews.
Number of claims audited: Record request limits must be applied to all claim types.
Providers with low denial rates will have lower claim request limits.

New Medical Record Request Limits Annual Baseline: Calculated by multiplying the total number of paid Medicare claims from a previous 12 month period by 0.5%. This number is divided by 8 to establish the maximum number of records that can be requested during each 45 day audit cycle.
Adjusted Record Request Limit: After three 45-day audit cycles, CMS will calculate (or recalculate) the provider’s Denial Rate. The denial rate is used to determine the provider’s adjusted record request limit. This may result in a higher or lower medical record limit.
If the RACs choose to use the adjusted limit, the lookback period is limited to 6 months. If the RACs choose to use the baseline limit, the lookback period is 3 years. All patient status reviews are limited to a 6 month lookback period.

Summary of RAC Program Enhancements Timeliness of Reviews: Audit review period to be reduced from 60 days to 30 days.
RAC must give providers 30 days for discussion before sending denials to the MAC for payment adjustment.
Contingency Fee: RAs will not receive contingency fee until after second level of appeal.
RAs will not receive contingency fee for complex reviews not completed within 30 days.

QUALITY IMPROVEMENT ORGANIZATIONS
QIOs

Quality Improvement Organizations (QIO) The 2 midnight rule became effective on October 1, 2013. CMS initially instructed the MACs to do short stay reviews for compliance with the 2 midnight rule. On October 1, 2015, CMS instructed the Beneficiary and Family Centered Care (BFCC) Quality Improvement Organizations (QIO) to take over the “probe and educate” process. (KEPRO in WV) On May 4, 2016, CMS suspended the QIO probe and educate process. On June 6, 2016, CMS instructed the QIOs to review previously reviewed short stay claims. On July 28, 2016, CMS stated that any claims outside of the six month look back period will be removed from the audit process and paid under Part A, even if previously denied. On September 12, 2016, CMS announced that the QIOs will resume probe and educate audits.


OTHER AUDITORS

What we have reviewed so far are Medicare FFS Auditors….. Medicaid Audits
Medicaid Integrity Program Audits (MICs) Medicaid RACs Payment Error Rate Measurement (PERM) Permedion
Managed Medicare Audits Humana Aetna/Coventry United Healthcare
Commercial Audits


Top Auditors by Rank Year First Second Third Fourth Fifth 2012 Connolly
Medicare RAC Humana Permedion
Medicaid CGS MAC CGI Blue
Cross
2013 Connolly Medicare RAC
Humana CGI Blue Cross Palmetto MAC/ CGI Medicare RAC
Permedion Medicaid
2014 Humana Palmetto MAC CGI Blue Cross Permedion Medicaid
CGI RAC
2015 Humana Connolly RAC CGI Blue Cross Permedion Medicaid
Palmetto MAC
2016 Humana CGI Blue Cross Aetna/Coventry HDI Managed Medicare
CGS MAC

Audit Questions to Ask Who are our highest volume auditors? What is our current denial rate?
Before appeal? After appeal?
What is our appeal success rate? Are we seeing prepayment audits? If so, what types of services are being audited? How many claims are currently in the appeal process? What trends are we seeing?

AUDIT COORDINATION ISSUES

§ Lost Letters § Missed Deadlines § Submission of Incomplete Records § Reluctance to Query Independent Physicians for
Needed Records § Process Silos § Too Much Focus on Medical Record Submission § Too Much Focus on Billing Reconciliation § Who Owns the Appeal Process? § Failure to Fix the Front End
Common Audit Process Issues

Departments involved in the third party medical record audit process Billing Office HIM Department Utilization Review Clinical Departments Coding Department Independent Physician Offices Finance/Legal Department

Who owns the process?

Issues resulting from perspective… Billing Office Focus on payment reconciliation Limited clinical knowledge Issues related to the medical record submission
HIM Department Focus on medical record submission Little understanding of appeal process Little understanding of the payment reconciliation process


Medical Record Audit Best Practices Claims Audit Coordinator
Revenue Cycle Experience Clinical Experience Detail Oriented “Big Picture” View Inserted in “Right” Department
Tracking System Centralized System Create Reports Communicate Reminders
Department Buy-In Clinical Departments Senior Management Billing Office HIM Department Coding Department Utilization Review

CASE STUDY Blepheroplasty

Blepharoplasty 100% Denial Rate Functional v/s Cosmetic Missing Documentation:
Visual field testing Photographs showing degree of impairment
Documentation was obtained from physician office and denials appealed All denials were overturned

Blepharoplasty But……….. The physician office was cooperative. This is not always the case. Payment for each denied claim was taken back and it took months to get the money back.
Appeal process is resource intensive, taking away time from other audit processes. We knew that addressing this on the backend was not a best practice.

Blepharoplasty Objective: Fix the Front End Created check lists:
Physician Office For Surgery Department
List of documentation that was needed at the time the surgery was scheduled. Goal: All documentation needed to support the medical necessity of the service is contained in the hospital medical record.

Office Check List

Hospital Check List
Check List integrated in hospital EHR

EXAMPLE DASHBOARDS
Tools to see the BIG Picture…….




Questions