World Journal for Pediatric and Congenital Heart Surgery
23
http://pch.sagepub.com/ Congenital Heart Surgery World Journal for Pediatric and http://pch.sagepub.com/content/1/3/364 The online version of this article can be found at: DOI: 10.1177/2150135110380239 2010 1: 364 World Journal for Pediatric and Congenital Heart Surgery Richard Van Praagh Normally and Abnormally Related Great Arteries : What Have We Learned? Published by: http://www.sagepublications.com On behalf of: World Society for Pediatric and Congential Heart Surgery can be found at: World Journal for Pediatric and Congenital Heart Surgery Additional services and information for http://pch.sagepub.com/cgi/alerts Email Alerts: http://pch.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: by Jose-Antonio Quibrera on October 30, 2010 pch.sagepub.com Downloaded from
Transcript of World Journal for Pediatric and Congenital Heart Surgery

http://pch.sagepub.com/
Congenital Heart SurgeryWorld Journal for Pediatric and
http://pch.sagepub.com/content/1/3/364The online version of this article can be found at:
DOI: 10.1177/2150135110380239
2010 1: 364World Journal for Pediatric and Congenital Heart SurgeryRichard Van Praagh
Normally and Abnormally Related Great Arteries : What Have We Learned?
Published by:
http://www.sagepublications.com
On behalf of:
World Society for Pediatric and Congential Heart Surgery
can be found at:World Journal for Pediatric and Congenital Heart SurgeryAdditional services and information for
http://pch.sagepub.com/cgi/alertsEmail Alerts:
http://pch.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Invited Lecture
Normally and Abnormally Related GreatArteries: What Have We Learned?
Richard Van Praagh, MD1
AbstractThe conus arteriosus or infundibulum was the site of the major cardiovascular evolutionary and developmental adaptation thatmade possible air-breathing and permanent land-living for vertebrates, including mammals such as ourselves. The subarterial conalfree walls perform an embryonic aortic switch procedure by 35 to 44 days of age in utero, based on growth of the left-sidedsubpulmonary conal free wall and resorption of the right-sided subaortic conal free wall, i.e., complete right-left asymmetry inthe development of the subarterial conal free walls. There is only one way of doing the developmental aortic aortic switchprocedure right (one way in situs solitus, and its mirror-image in situs inversus), and there are many ways of doing it wrong,resulting in the conotruncal anomalies. The proximal or apical part of the conus arteriosus, the septal band, was the motherof the right ventricular sinus (the lung pump). The conus transformed the single (systemic) circulation of fish into our double(systemic and pulmonary) circulations. The right ventricle (RV) is only about 36% as old as the left ventricle (LV). Mostcongenital heart disease involves anomalies of the more recently developed RV, congenital heart disease being the mostfrequent anomaly in liveborn children — almost 1 percent (0.8%).
Keywordscardiac anatomy/pathological anatomy, congenital heart disease, embryology, great vessel anomaly
Submitted May 21, 2010; Accepted July 8, 2010.Presented at the Joint Meeting of The World Society for Pediatric and Congenital Heart Surgery Honoring Dr Aldo Castaneda; July 15-17, 2010;Antigua, Guatemala.
Introduction: the Developmental AorticSwitch
The distal or subsemilunar part of the infundibulum or conus
arteriosus performs an arterial switch procedure during cardio-
genesis. Normally, the straight heart tube loops or folds to the
right. D-loop formation places the developing right ventricle
(the bulbus cordis) to the right of the developing left ventricle
(the ventricle) of the bulboventricular D-loop. D-loop forma-
tion also places the developing ascending aorta to the right of
the developing main pulmonary artery of the truncus arteriosus.
This developmental stage is reminiscent of the Taussig-Bing
malformation; that is, potentially, there is a double-outlet right
ventricle {S,D,D} with a bilateral conus, the subaortic part to
the right and the subpulmonary part to the left, closer to the
developing ventricular septum, the interventricular foramen
(the ventricular septal defect), and the developing left ventricle.
The structural problem at this critical developmental stage is
how to avoid the Taussig-Bing type of double-outlet right
ventricle. Asymmetrical conal free wall development is the
solution. On the left side, growth of the subpulmonary conal
free wall elevates the pulmonary valve superiorly and protrudes
it anteriorly, above the anterior and right-sided right ventricle,
moving the pulmonary valve and artery away from the ventri-
cular septal defect (VSD). On the right side, resorption of the
subaortic conal free wall carries the developing aortic valve
inferiorly, posteriorly, and leftward into and partly through the
interventricular foramen, resulting in aortic-mitral approxima-
tion and direct fibrous continuity. The last step in this normal
arterial switch procedure is closure of the interventricular
foramen at its rightmost end, between the anterior and septal
leaflets of the tricuspid valve and beneath the right coronary-
noncoronary commissure of the aortic valve, by atrioventricu-
lar endocardial cushion tissue that is intimately associated with
the tricuspid valve, thereby forming the membranous septum.
1 Children’s Hospital Boston, Boston, Massachusetts
Corresponding Author:
Richard Van Praagh, MD, Children’s Hospital Boston, 300 Longwood Avenue,
Boston, MA 02115
Email: [email protected]
World Journal for Pediatric andCongenital Heart Surgery1(3) 364-385ª The Author(s) 2010Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/2150135110380239http://pch.sagepub.com
364 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Abbreviations and Acronyms
ACM anatomically corrected malposition of the greatarteries
AP aortopulmonary
AV atrioventricular
DORV double-outlet right ventricle
DOLV double-outlet left ventricle
D-TGA D-transposition of the great arteries
TGA transposition of the great arteries
TOF tetralogy of Fallot
VA ventriculoarterial
VSD ventricular septal defect
There are several ways in which the developmental arterial
switch procedure can be performed incorrectly:
1. Growth of the subaortic conal free wall and resorption of
the subpulmonary conal free wall result in transposition
of the great arteries (TGA).
2. Continued persistence and growth of both the subaortic
and the subpulmonary conal free walls, that is, failure of
subsemilunar conal free wall resorption, can result in a
double-outlet right ventricle (DORV).
3. Resorption of both the subaortic and the subpulmonary
conal free walls can rarely result in double-outlet left ven-
tricle (DOLV).
4. Abnormal development of the subaortic and subpulmonary
conal free walls, combined with ventricular loop formation
in one direction (eg, to the right) and twisting of the infun-
dibuloarterial (conotruncal) segment in the opposite direc-
tion (eg, to the left), rarely can result in anatomically
corrected malposition of the great arteries (ACM).
It is infrequently possible to have DORV with a normal type
of infundibulum and great arteries, for example, with the hypo-
plastic left heart syndrome (such as mitral atresia with a
diminutive or absent left ventricle): the subpulmonary infundi-
bulum can be well developed, and the subaortic conal free wall
can be resorbed, permitting aortic-tricuspid fibrous continuity.
Abnormally related great arteries usually have a subsemilu-
nar conal free wall malformation, but not always. Occasionally,
the atrioventricular (AV) canal (eg, the mitral valve) and the
left ventricle can be the site of the primary anomaly.
Truncus arteriosus and aortopulmonary (AP) window are
the only anomalies of which I am aware in which the great
arteries themselves are the site of primary malformation. In tet-
ralogy of Fallot (TOF), TGA, DORV, DOLV, and ACM, the
great arterial anomalies are secondary to a primary malforma-
tion of the subarterial part of the conus.
In a broader perspective, it should be understood that we are
really talking about the most important cardiovascular adapta-
tion of vertebrates to air breathing and land living. For our ver-
tebrate ancestors living in the water, a single, straight tube type
of heart was satisfactory. However, to breathe air and live
permanently on land, a double heart became advantageous. The
straight heart tube looped to the right. To avoid DORV, the
developing aorta was switched into the left ventricle by resorp-
tion of the subaortic conal free wall and by growth of the sub-
pulmonary conus to elevate the pulmonary artery superiorly
and protrude it anteriorly, getting the pulmonary artery out of
the way, that is, getting the pulmonary artery away from the
interventricular foramen (the VSD), making it possible for the
aorta to pass into the VSD and to achieve fibrous continuity
with the mitral valve. The ventricle of the bulboventricular
D-loop became the systemic ventricle. Beneath the septal band
of the proximal part of the bulbus cordis, the lung pump
evaginated or pouched out, creating the right ventricular
sinus or inflow tract and making the ventricle of the
D-bulboventricular loop the left ventricle. Hemodynamic
separation of this double heart (systemic and pulmonary) was
achieved by successful septation at all levels.
Hence, this study of normally and abnormally related great
arteries is concerned with one of the most important evolution-
ary adaptations of vertebrates to air breathing and land living:
the developmental aortic switch procedure, done by a combina-
tion of cardiac loop formation and by asymmetrical develop-
ment of the free walls of the subarterial conus arteriosus.
Normally related great arteries illustrate how the developmen-
tal aortic switch procedure is done successfully. Abnormally
related great arteries document the many ways in which the
developmental aortic switch procedure can be done
unsuccessfully.
Normally, in the developmental or biological aortic switch
procedure, as opposed to the surgical arterial switch operation,
only one great artery, the aorta, is switched, not both. This is
because developmentally, the starting position (preswitch) is
potentially a DORV of the Taussig-Bing type, which has trans-
position of the circulations because the developing pulmonary
artery is adjacent to the interventricular foramen (the VSD).
Why DORV? Because at the early straight tube stage, both
developing great arteries (the truncus arteriosus) are located
above the developing right ventricle (the bulbus cordis). How-
ever, in the normal developmental aortic switch process, both
great arteries are moved, if not switched. The pulmonary artery
has to be gotten ‘‘out of the way,’’ that is, away from the inter-
ventricular foramen (the VSD), so that the aortic valve can pass
partly through the interventricular foramen to achieve fibrous
continuity with the mitral valve. The normal growth of the sub-
pulmonary conus elevates the pulmonary valve superiorly and
protrudes it anteriorly on the left side of the developing great
arteries, thereby getting the pulmonary outflow tract ‘‘out of
the way,’’ making it physically possible for the aortic valve
to be switched partly through the interventricular foramen and
into the left ventricle. The normally related aorta sits partly
above the ventricular septum and partly above the left ventricu-
lar cavity.
So, the normal biological or developmental arterial switch
process involves both great arteries, but only one, the aorta,
is switched into the left ventricle. The normal morphogenetic
movements of both developing semilunar valves are
Van Praagh 365
365 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

reciprocals of each other: As the pulmonary valve moves super-
iorly, anteriorly, and rightward above the growing subpulmon-
ary conal free wall, the aortic valve moves inferiorly,
posteriorly, and leftward, partly through the interventricular
foramen and above the ventricular septum and the left ventricu-
lar cavity, atop the resorbed subaortic conal free wall, thereby
achieving aortic-mitral fibrous continuity via the intervalvar
fibrosa. These normal morphogenetic movements of the semi-
lunar valves and great arteries have usually been completed by
35 to 44 days of intrauterine life, when the membranous septum
typically is completed, thereby separating the morphologically
right and left ventricles. Thus, this is truly an embryonic aortic
switch procedure.
This presentation is really about our most important cardio-
vascular evolutionary adaptation that made possible air breath-
ing and land living. The evolution of the subarterial conus
arteriosus and of the right ventricular sinus made possible our
terrestrial prehistory, history, culture, and science—our
‘‘everything.’’ The many different anatomical types of abnor-
mally related great arteries document the many different ways
in which the embryonic aortic switch procedure can be done
wrong. There are only 2 ways in which this procedure can be
done right, as in solitus normally related great arteries and its
mirror image, inversus normally related great arteries.
Probably the biggest lesson that we have learned is that
abnormal relations between the great arteries have nothing pri-
marily to do with the great arteries themselves. For example, in
TGA, DORV, and DOLV, the great arteries per se typically are
normal (Figure 1). The anomaly usually involves the free walls
of the subsemilunar infundibulum or conus arteriosus (Figure
1),1,2 not the aorticopulmonary septum of the great arteries.
Abnormally related great arteries are abnormally connected
great arteries. The subsemilunar infundibulum (funnel, Latin)
or conus arteriosus (arterial cone, Latin) is the crucial connec-
tion between the great arteries above and the ventricles, ventri-
cular septum, and the AV canal and valves below.
Normally Related Great Arteries
The subsemilunar conus normally performs ‘‘Mother Nat-
ure’s’’ arterial switch operation. Here is what happens nor-
mally: At the straight tube stage and at the early D-loop
stage, a bilateral conus (subaortic and subpulmonary) is present
(Figure 2).1 Both developing great arteries are located above
the developing right ventricle, similar to the Taussig-Bing mal-
formation.3 Why? Because the truncus arteriosus, from which
the great arteries develop, is located above (cephalad to) the
bulbus cordis, from which the conus and the right ventricular
sinus develop (Figure 2). So, as ventricular D-loop formation
occurs, one potentially has DORV of the Taussig-Bing type,3
with a bilateral conus, and a subpulmonary interventricular
foramen (or VSD).
So, the developmental problem at this stage essentially is
how to avoid the Taussig-Bing malformation. The conal con-
nection holds the answer. Let us consider a bulboventricular
D-loop first (Figure 3, left panel). At the straight tube stage, the
developing subpulmonary part of the conus (main pulmonary
artery) is thought to be posterior (dorsal) relative to the subaor-
tic part of the developing conus (ascending aorta) (Figure 3).4
But looping to the right places the developing subaortic part of
the conus to the right, on the greater curvature of the D-loop,
and leaves the developing subpulmonary part of the conus to
the left, in the lesser curvature of the bulboventricular D-loop
(Figure 3).4
Then, in normal development, the subpulmonary infundibu-
lar free wall grows and expands, carrying the overlying pul-
monary valve superiorly and protruding the pulmonary valve
and main pulmonary artery anteriorly, on the left-hand side
of the great arterial outflow tracts. At the same time, on the
right-hand side of the great arterial outflow tracts, the subaortic
infundibular free wall normally undergoes resorption, permit-
ting the developing aortic valve to sink inferiorly (caudad),
posteriorly (dorsally), and to the left into the interventricular
foramen. Because of normal resorption of the subaortic infun-
dibular free wall, the noncoronary leaflet of the aortic valve and
a portion of the adjacent left coronary leaflet of the aortic valve
normally come into direct fibrous continuity with the develop-
ing mitral valve via the intervalvar fibrosa, resulting in solitus
normally related great arteries (Figure 2).1 Then, the final step
is closure of the interventricular foramen at its rightmost end,
between the anterior and septal leaflets of the tricuspid valve
and beneath the noncoronary–right coronary commissure of the
aortic valve, thereby forming the membranous septum.
The hemodynamic result of these developmental events is
that the posterior and left-sided left ventricle can eject only
through a posterior and right-sided aortic valve into an ascend-
ing aorta that proceeds upward (cephalad) on the right and
passes over (cephalad to) the pulmonary bifurcation because
aortic arch 4 is ventral and cephalad relative to pulmonary
arch 6. This is the fixed distal AP relationship that always
pertains (as long as an aortic arch and a pulmonary bifurcation
are present) because of this constant aortic arch 4–to–pulmonary
arch 6 relationship.
So, do you see that the development of the subsemilunar
conal free walls is performing an essential aortic switch oper-
ation? Growth of the subpulmonary conal free wall elevates the
pulmonary valve superiorly and protrudes it anteriorly, moving
it away from the interventricular foramen (the VSD). Conver-
sely, resorption of the subaortic conal free wall causes the aor-
tic valve to move in a reciprocally inferior, posterior, and
leftward direction, into the interventricular foramen, thereby
permitting normal aortic-mitral fibrous continuity. Then, the
interventricular foramen (the VSD) is closed by AV endocar-
dial cushion tissue beneath the right rim of the aortic valve and
between the anterior and septal leaflets of the tricuspid valve,
forming the membranous septum.
Conal development, growth and resorption, literally acts
like a switch in a railway track. Development of the subpul-
monary free wall switches the pulmonary valve anterosuper-
iorly, away from the interventricular foramen. Resorption of
the subaortic conal free wall switches the aortic valve into and
partly through the interventricular foramen. Growth of the
366 World Journal for Pediatric and Congenital Heart Surgery 1(3)
366 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

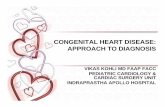
Figure 1. Types of human heart, with emphasis on segmental sets (or combinations), alignments, and spatial relations. Heart diagrams are viewedfrom below, as visualized with subxiphoid 2-dimensional echocardiography. Cardiotypes depicted in broken lines had not been documented whenthe diagram was made; cardiotypes shown in solid lines have all been documented. The aortic valve is indicated by the coronary ostia; thepulmonary valve is indicated by the absence of the coronary ostia. Braces {} mean ‘‘the set of.’’ Ant ¼ anterior; Inf ¼ infundibulum; LA ¼morphologically left atrium; L ¼ left; LV ¼ morphologically left ventricle; Post ¼ posterior; R ¼ right; RA ¼ morphologically right atrium; RV ¼morphologically right ventricle. The columns (1-4) are arranged in terms of atrioventricular (AV) concordance or discordance. Column 1 has AVconcordance between the situs solitus of the viscera and atria {S,-,-} and D-loop ventricles {S,D,-}. Column 2 has AV discordance between thesolitus viscera and atria {S,-,-} and L-loop ventricles {S,L,-}. Column 3 has AV concordance between the visceroatrial situs inversus {I,-,-} and L-loopventricles {I,L,-}. Column 4 has AV discordance between situs inversus of the viscera and atria {I,-.-} and D-loop ventricles {I,D,-}. Situs ambiguus{A,-,-} of the viscera and atria in the heterotaxy syndromes with congenital asplenia and polysplenia with D-loop ventricles {A,D,-} and with L-loopventricles {A,L,-} has been omitted for reasons of accuracy: when the atrial situs is uncertain or unknown {A,-,-}, one cannot say whether D-loopventricles {A,D,-} or L-loop ventricles {A,L,-} have AV concordance or discordance. To make the diagnosis of AV concordance or discordance, onemust know both the atrial situs and the ventricular situs. The rows (1-8) are arranged according to the types of ventriculoarterial (VA) alignmentthat are present. Normally related great arteries are depicted in rows 1 to 4 inclusively. Solitus normally related great arteries {-,-,S} and inversusnormally related great arteries {-,-,I} are both shown. In row 5, some types of transposition of the great arteries (TGA) are shown but by no meansall: D-TGA, that is, TGA {-,-,D} in which the transposed aortic valve lies to the right (dextro or D) relative to the transposed pulmonary valve, andL-TGA, that is, TGA {-,-,L} in which the transposed aortic valve lies to the left (levo or L) relative to the transposed pulmonary valve, are both
Van Praagh 367
367 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

subpulmonary conal free wall and resorption of the subaortic
conal free wall both are essential to the morphogenetic move-
ments of the semilunar valves. Note that truncoconal septation
appears not to be the primary development mechanism;
instead, it is subsemilunar conal free wall growth and resorption
(Figure 3).1,4
The great arteries normally do not twist around each other,
contrary to what we often say. Instead, the ascending aorta and
the main pulmonary artery normally are untwisting about each
other. Why untwisting? Because of the torsion that normally is
introduced at the semilunar valve level by the combination of
(1) ventricular D-loop formation and (2) asymmetric conal free
wall growth (subpulmonary) and resorption (subaortic).
Note how different the normal AP spatial relationship is
proximally compared with the AP spatial relationship distally.
Proximally, at the semilunar valves, the aortic valve is poster-
ior, inferior, and rightward, whereas the pulmonary valve is rel-
atively anterior, superior, and leftward. Distally, at the aortic
arch and pulmonary bifurcation, the aorta is anterior and super-
ior, while the pulmonary artery bifurcation is posterior and
inferior (Figure 2). Therefore, the fibroelastic great arteries
must untwist as they go from the semilunar valve relationship
proximally to the aortic arch–to–pulmonary bifurcation rela-
tionship distally. The latter relationship distally is fixed by the
embryonic branchial or aortic arch 4/6 relationship. This is why
the aortic arch is ‘‘always’’ anterior and superior to the pulmon-
ary bifurcation because this is the relationship of the embryonic
branchial or aortic arch 4 relative to branchial or aortic arch 6.
(The adverb ‘‘always’’ is between quotes because it is assumed
that an aortic arch and a pulmonary bifurcation are present; if
either is absent, ‘‘always’’ does not apply.) The untwisting of
the great arteries equals (in degrees) the difference between the
proximal and distal AP spatial relationships, which normally
equals approximately 150� (Figure 2).1
Transposition of the Great Arteries
Now, let us briefly consider what happens in typical D-
transposition of the great arteries (D-TGA) (Figure 3, left
panel).4 The wrong arterial switch operation is performed.
The asymmetrical conal free walls develop ‘‘backward,’’ that
is, the opposite of normal. The subpulmonary conal free wall
undergoes resorption (Figure 3), permitting pulmonary-mitral
fibrous continuity (Figure 2), and the subaortic infundibular
free wall grows, elevating the developing aortic valve super-
iorly and protruding it anteriorly (Figure 3). As a result of
reversed development of the subsemilunar conal free walls, the
aortic valve remains anteriorly above the anterior and right-
sided right ventricle, while the pulmonary artery arises poster-
iorly above the left ventricle. Thus, the arterial switch operation
of the subsemilunar conus has been done incorrectly: the pul-
monary artery (instead of the aorta) has been switched into the
left ventricle, and the aorta (instead of the pulmonary artery)
remains above the right ventricle.
This reversed or ‘‘backward’’ subsemilunar conal free wall
development may be regarded as inverted development of the
subarterial conal free walls, that is, right-left reversal or mirror
imagery, without anteroposterior or superoinferior change
(Figure 3). The concept of subsemilunar conal free wall
inverted development applies accurately after the cardiac loop
stage has been reached (Figure 3); but the concept of subsemi-
lunar infundibulum free wall developmental inversion may not
apply accurately at the straight tube stage, when these 2 devel-
oping conal free walls are thought (but not definitely known) to
be anteroposterior (Figure 3) rather than right-left. Anteropos-
terior reversal is not called inversion, whereas right-left rever-
sal is.
In D-TGA, why are the great arteries relatively parallel, or
straight and uncrossed, whereas normally great arteries are
twisted about each other, or really, untwisting above each other
(Figure 2)? Compare the proximal and distal AP relationships.
In D-TGA, proximally, the aortic valve is anterior and some-
what to the right, and the pulmonary valve is posterior and
somewhat to the left (Figure 2). Distally, the aortic arch is also
anterior and superior, and the pulmonary bifurcation is also
posterior and inferior (Figure 2). Thus, in D-TGA, both proxi-
mally at the valves and distally at the aortic arch/pulmonary
bifurcation, the aorta is anterior, and the pulmonary artery is
posterior. Consequently, in D-TGA, the great arteries are rela-
tively parallel, straight, and uncrossed because the fibroelastic
great arteries have little untwisting to do as they proceed from
the valves proximally to the aortic arch and pulmonary bifurca-
tion distally. This lack of necessary untwisting is because the
proximal and distal AP relationships are similar.
If one measures the semilunar interrelationship relative to
the sagittal plane in D-TGA, the semilunar valves often display
only about 30� dextrorotation, compared with about 150� dex-
trorotation for solitus normally related great arteries at the
Figure 1 continued. depicted. A-TGA, in which the transposed aortic valve lies directly anterior (antero or A) relative to the transposedpulmonary valve, is omitted for simplicity and clarity. In row 6, anatomically corrected malposition of the great arteries (ACM) is presented. Notethat in all anatomical types of ACM, the ventricles have looped in one direction and the infundibuloarterial segment has twisted in the oppositedirection. In ACM, the subsemilunar conus is either bilateral (subaortic and subpulmonary) or subaortic only (with pulmonary-tricuspid fibrouscontinuity). In ACM, although the great arteries are very malpositioned, nonetheless, there is VA alignment concordance by definition, hence, thename ‘‘anatomically corrected malposition of the great arteries.’’ ACM may be physiologically corrected, as in ACM {S,D,L}, because all segmentshave alignment concordance; or ACM can be physiologically uncorrected, as in ACM {S,L,D}, because there is one intersegmental alignmentdiscordance at the AV level. VA concordance is not synonymous with normally related great arteries because ACM also has VA alignmentconcordance, but the great arteries are very abnormally related in space, and the conal VA connections are also very abnormal. Row 7 depictssome anatomical types of double-outlet right ventricle (DORV), but by no means all. Similarly, row 8 shows some anatomical types of double-outletleft ventricle (DOLV) but not all. In DOLV, both parts of the subsemilunar conus may, or may not, be very deficient (absorbed or involuted).11,19,27
Reproduced with permission from Foran and colleagues.24
368 World Journal for Pediatric and Congenital Heart Surgery 1(3)
368 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

semilunar valves (Figure 2).1 Thus, D-TGA is characterized by
a major failure of dextrorotation at the semilunar valves
because of reversed or inverted development of the subsemilu-
nar infundibular free walls. With bulboventricular L-loops, the
same processes occur, but in mirror image, resulting in inverted
normally related great arteries or L-TGA (Figure 3, right
panel).
To generalize, normally, what happens both with ventricular
D-loops and L-loops, the initially posterior subpulmonary
conal free wall should grow. Following loop formation, the
subpulmonary conal free wall is in the lesser curvature, both
with D-loops and with L-loops (Figure 3); this is the
subpulmonary conal free wall that normally grows and
expands. The greater curvature, both of D-loops and L-loops,
is the subaortic conal free wall that normally undergoes resorp-
tion. If this subsemilunar conal free wall development is
reversed or inverted, that is, with growth of the greater curva-
ture part and resorption of the lesser curvature part, then, TGA
results, with pulmonary-mitral fibrous continuity and a right
ventricular aorta with no aortic-AV fibrous continuity because
of the presence of an interposed subsemilunar muscular conal
free wall.
So, the first big lesson that we have learned is that the classic
truncoconal malseptation hypothesis, initially proposed by
Figure 2. The morphogenesis of normally and abnormally related great arteries. In the top row, the straight heart tube, the bulboventricularD-loop, and the bulboventricular L-loop are shown from the front (a ventral view). In the second row, the truncus arteriosus and the derivativeascending aorta (Ao) and main pulmonary artery (PA) are shown both with ventricular D-loops and L-loops, as seen from the front (a ventralview). Also depicted are the various anatomical types of conus arteriosus or infundibulum (crosshatching) that can be located beneath the PAand/or the Ao. In the third row, the aortic valve (with coronary ostia), the pulmonary valve (without coronary ostia), the subsemilunar conalmusculature (crosshatching), the mitral valve (bicuspid), and the tricuspid valve (3 leaflets) are shown as seen from below (an inferior view, ie,from caudad looking cephalad), both with ventricular D-loops and L-loops. The bottom row lists some of the relations between the greatarteries that are associated with the 4 main anatomical types of conus: subpulmonary, subaortic, bilateral (subaortic and subpulmonary), andbilaterally absent or very deficient (neither subaortic nor subpulmonary). The diagrams of the great arteries and the conus are deliberately‘‘diagrammatic’’; that is, definitive anatomy rather than developmental stages are shown, for clarity of understanding. A ¼ common (undivided)atrium; Ant ¼ anterior (ventral); AoV-TV ¼ aortic valve–to–tricuspid valve (fibrous continuity); BC ¼ bulbus cordis (from which the conusarteriosus and the right ventricular sinus develop); D-loop ¼ a bulboventricular loop that has looped or folded in a rightward (dextral or D)direction, placing the developing right ventricle to the right of the developing left ventricle; D-MGA¼ dextromalposition of the great arteries inwhich the malposed aortic valve lies dextral (or to the right) of the malposed pulmonary valve: D-MGA occurs in the double-outlet rightventricle (DORV), doublet-outlet left ventricle (DOLV), and in anatomically corrected malposition of the great arteries (ACM); D-TGA ¼dextrotransposition of the great arteries in which the transposed aortic valve lies to the right (dextro or D) relative to the transposedpulmonary valve; Inf¼ infundibulum (also known as the conus arteriosus); Lt¼ left; L-MGA¼ levomalposition of the great arteries in which themalposed aortic valve lies to the left (levo or L) relative to the malposed aortic valve: L-MGA occurs in the DORV, DOLV, and ACM (seeFigure 1); L-TGA¼ levotransposed aortic valve is to the left (levo or L) of the transposed pulmonary valve; LV¼morphologically left ventricularsinus; Post¼posterior (dorsal); PV-MV¼ pulmonary valve–to–mitral valve (fibrous continuity); RT¼ right; RV¼morphologically right ventricularsinus; Sup ¼ superior (above or cephalad); TA ¼ truncus arteriosus (from which the great arteries develop in part); V ¼ ventricle of thebulboventricular loop (from which the LV develops). Reproduced with permission from Van Praagh and colleagues.1
Van Praagh 369
369 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Figure 3. The embryonic aortic switch procedure: how to do it right and how to do it wrong. At the straight tube stage, the future subpulmonaryconal area (stippled) is thought to be posterior (dorsal) relative to the future subaortic conal area (clear, ie, not stippled). Following D-loopformation, the future subpulmonary conal area occupies the lesser curvature of the D-loop (stippled), and the future subaortic conal area occupiesthe greater curvature of the D-loop (not stippled); the future subpulmonary conal region lies to the left, and the future subaortic conal region lies tothe right. Now, let us focus on the subsemilunar conal free walls (not the conal septum). Normally, the subpulmonary conal free wall grows andexpands, carrying the overlying developing pulmonary valve and main pulmonary artery superiorly (cephalad) and anteriorly (ventrally) on the left-hand side of the great arterial outflow tracts. At the same time, the subaortic conal free wall undergoes resorption or involution (indicated by thebroken circular line). Resorption of the subaortic infundibular free wall causes the overlying developing aortic valve and ascending aorta to sinkinferiorly (caudad), posteriorly (dorsally), and leftward. The aortic valve passes partly through the interventricular foramen and comes into fibrouscontinuity with the mitral valve via the intervalvar fibrosa. The last step in the normal morphogenesis of crossing the circulations is closure of theinterventricular foramen at its rightmost side, adjacent to the tricuspid valve. This is how the developmental arterial switch procedure is performedcorrectly in normal development. The pulmonary valve is carried up and away from the interventricular foramen, and the aortic valve passesdownward and to the left into the interventricular foramen. Formation of the membranous septum by endocardial cushion tissue of theatrioventricular canal completes the normal aortic switch procedure. D-loop formation and asymmetrical development of the subsemilunar conalfree walls result in about 150� of rotation of the semilunar valves to the right (in a counterclockwise direction), when viewed from below.Consequently, the fibroelastic ascending aorta and main pulmonary artery normally must untwist through about 150� in the opposite direction,leftward or clockwise as viewed from below, because of the fixed aortopulmonary relationship distally, where the aorta always arches anteriorly(ventrally) and superiorly (cephalad) relative to the bifurcation of the main pulmonary artery, because these are the fixed spatial relations betweenaortic arches 4 and pulmonary arches 6 in the embryonic branchial aortic arch system. So, normally related great arteries really are untwistingabout each other (not twisting about each other). D-loop formation and asymmetrical conal subsemilunar free wall development are the ‘‘engines’’that perform the aortic switch procedure, thereby normally crossing the systemic venous and the pulmonary venous circulations and achievingsolitus normally related great arteries. But look what happens when the wrong subsemilunar conal free wall grows and expands (the nonstippledsubaortic conal free wall on the greater curvature of the D-loop) and when the wrong subsemilunar conal free wall undergoes resorption (thestippled subpulmonary conal free wall in the lesser curvature of the D-loop). When subsemilunar conal free wall development is the opposite ofnormal, then, it is the aortic valve that is carried superiorly and protruded anteriorly on the right side of the great arterial outflow tracts, and it is thepulmonary valve and main pulmonary artery on the left that sink inferiorly and posteriorly, passing partly through the interventricular foramen andcoming into fibrous continuity with the mitral valve, which is made possible by the abnormal involution of the subpulmonary conal free wall (circularbroken line), resulting in D-TGA. Why are the great arteries relatively parallel, straight, or uncrossed in D-TGA? Because the aortopulmonaryrelationships both proximally at the semilunar valves and distally at the aortic arch/pulmonary artery bifurcation are very similar. Both proximallyand distally, the aorta is anterior (ventral), and the main pulmonary artery is posterior (dorsal). Consequently, in D-TGA, the great arteries haverelatively little untwisting to do as they pass from the semilunar valves proximally to the aortic arch/pulmonary bifurcation distally. An arterialswitch procedure has been performed, resulting in D-TGA, but the embryonic arterial switch procedure has been done wrong because the wrong
370 World Journal for Pediatric and Congenital Heart Surgery 1(3)
370 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Quain5 (1844) and subsequently espoused by many other
authors, is not quite right.6 According to this hypothesis, nor-
mally related great arteries result from spiral downgrowth of
the truncoconal septum, whereas TGA results from straight
downgrowth of the truncoconal septum. What made us realize
that the classic malseptation hypothesis is wrong? First of all, it
was anatomically obvious that in TGA and DORV, there is
much more wrong than just an abnormally straight, relatively
nonspiral AP septum. The great arterial free walls are also ana-
tomically very abnormal. How could we tell? The coronary
arteries. The origins of the right and left coronary arteries are
very abnormally located in TGA and in DORV (Figure 2),
and the coronary arteries are the first branches of the aortic
free wall.
So, we realized that from an anatomical standpoint, TGA
and DORV are much more than just an abnormality of AP sep-
tation. The great arterial free walls are just as abnormal anato-
mically as is the AP septum. This was my first realization that
something might be wrong with the widely accepted truncal
malseptation hypothesis.5
Between 1961 and 1963, I had the good fortune to be a fel-
low in the Department of Cardiology at the Hospital for Sick
Children in Toronto, in the department headed by Dr John D.
Keith, who is widely regarded as the Canadian ‘‘father’’ of
pediatric cardiology. Dr Keith asked Dr Peter Vlad and me to
prepare the chapter on TGA for the second edition of the
renowned Keith, Rowe, and Vlad textbook on heart disease
in infancy and childhood, which would be published in
1967.7 It was my job to study all of the autopsied cases of TGA
that had been retained in their collection of pathological anat-
omy of congenital heart disease. I did so, with one question
in mind: Amid all the many differences displayed by these
heart specimens, is there a feature that they all share in com-
mon? I thought that if I could find a ‘‘common denominator,’’
this might reveal what TGA really is anatomically and
developmentally.
Then, it gradually dawned on me. All these cases of TGA do
have one feature in common, amid their myriad differences:
they all have a malformation of the subsemilunar infundibulum
or conus arteriosus.7 So, the seed of understanding had been
planted. I also had the very good fortune to spend 6 fascinating
months doing observational and experimental cardiovascular
embryology at the Carnegie Institution of Washington in the
Department of Embryology under the guidance of Dr Robert
H. DeHaan in 1966.
Also, in 1966, with Dr Stella Van Praagh, we published one
of our first discoveries in congenital heart disease: isolated ven-
tricular inversion, with a consideration of the morphogenesis,
definition, and diagnosis of nontransposed and transposed great
arteries.8 This case was an illuminating natural experiment.
The segmental anatomy was {S,L,S}. So, here was a rare
patient who had situs solitus of the viscera and atria, with a dis-
cordant ventricular L-loop with AV alignment discordance: a
right-sided right atrium opening into right-sided morphologi-
cally left ventricle, and a left-sided left atrium opening into a
left-sided morphologically right ventricle. But this patient did
not have the usual congenitally physiologically corrected TGA.
Instead, this patient had a solitus normal type of conotruncus: a
left-sided, well-developed subpulmonary muscular conus
above a left-sided and left-handed right ventricle; and on the
right side, a posterior, inferior, and right-sided aortic valve in
direct fibrous continuity with a right-sided mitral valve and
right-handed left ventricle.
So, why did this patient not have the expected corrected
TGA? An important part of the answer appeared to be
because a well-developed solitus normal type of muscular
subpulmonary conus, with resorption of the subaortic conal
free wall, was present in this patient. This was an amazing
spectacle: a solitus normal type of infundibulum and great
arteries that was related as normally as possible to the under-
lying L-loop ventricles and the inverted AV valves. Suffice it
to say that the discovery of isolated ventricular inversion
{S,L,S} strengthened our hypothesis that the subsemilunar
conus is a very important determinant of whether the great
arteries are normally or abnormally related. This case seemed
to say the following: if the conus is of the solitus normal
type, then, the great arteries are solitus normally related, even
if the ventricular loop is inverted.
There were other clues also. TGA is associated almost never
with an AP septal defect (an AP ‘‘window’’). If TGA were
really caused by an anomaly of AP septation, then, definite
malformations of the AP septum, such as an AP window,
should be relatively common with TGA; in fact, an AP window
in association with TGA is so infrequent as to be reportable.
The conal maldevelopment hypothesis also could explain
the variations in semilunar valve heights, whereas the truncal
(or truncoconal) straight septum hypothesis could not. Propo-
nents of the classic straight AP septum hypothesis tried to say
that the transposed aortic valve is higher than the transposed
pulmonary valve because the conus (beneath the transposed
Figure 3 continued. subsemilunar conal free wall grew and expanded (the subaortic) and the wrong subsemilunar conal free wall underwentresorption (the subpulmonary). When L-loop formation occurs, inverted normally related great arteries also result from subpulmonary conal freewall growth and subaortic conal free wall resorption but in a mirror image when compared with what happens to produce solitus normally relatedgreat arteries with a ventricular D-loop. Similarly, typical L-TGA results from subaortic conal free wall growth and from subpulmonary conal freewall resorption (but again, in a mirror image compared with D-TGA and a ventricular D-loop). Ao¼ ascending aorta; D-loop¼ a bulboventricularheart tube that has looped or folded in a rightward (dextral or D) direction, placing the developing right ventricle (RV) to the right of the developingleft ventricle (LV), the RV being right handed and the LV being left handed; D-TGA ¼ transposition of the great arteries in which the transposedaortic valve is to the right (dextro or D) relative to the transposed pulmonary valve; L¼ left; L-loop¼ a bulboventricular heart tube that has loopedor folded in a leftward (levo or L) direction, placing the developing RV to the left of the developing LV, RV being left handed and the LV being righthanded; PA ¼ main pulmonary artery; R ¼ right. Reproduced with permission from Van Praagh.25
Van Praagh 371
371 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

aortic valve) is part of the right ventricle and is not part of the
left ventricle. We had long known that this contention is wrong
because the semilunar part of the conus can override the ventri-
cular septum to any degree, and the subsemilunar conus can be
located mostly, if not entirely, above the morphologically left
ventricle, for example, as in ACM (Figure 1)9,10 and in DOLV
(Figure 1).11 The conal connector is not an intrinsic, insepar-
able part of either the right ventricle or the left ventricle.
Instead, the conal connector forms part of the outflow tract
of both ventricles.
The subsemilunar conus, that is, the conal septum, the par-
ietal band, and the subsemilunar free walls, ‘‘belong’’ to the
great arteries, not to the ventricles. That is why the embryolo-
gists speak of the conotruncus (ie, the subsemilunar infundibu-
lum and the great arteries). It is in this sense that the
subsemilunar conus should be regarded as ‘‘belonging to’’ the
great arteries, not to the ventricles.
Finally, we (Stella and I and our colleagues) were starting to
understand the so-called conotruncal or infundibuloarterial
anomalies such as D-TGA and typical DORV. It was a shock
for us to learn that these are infundibular anomalies, not great
arterial malformations. In D-TGA and typical DORV, the great
arteries per se are normal, just as in TOF, which is another
infundibular anomaly, not primarily a great arterial
malformation.
One of the great lessons was this: Abnormally related great
arteries typically are abnormally connected great arteries.
Another lesson was as follows: The abnormality involves the
subsemilunar infundibular free wall(s), not the AP septum.
The great arteries are not attached to and do not arise from
the ventricles (meaning from the ventricular sinuses). Instead,
the great arteries arise from the subsemilunar conus, be it well
developed or absorbed, and it is the conus that connects the
great arteries with the underlying ventricular sinuses, ventricu-
lar septum, AV canal, and AV valves. It is helpful to under-
stand that if the great arteries originated directly from the
ventricular sinuses or main pumping chambers, rather than
from the infundibulum or conus arteriosus, then, the many
abnormal ventriculoarterial (VA) spatial relations and connec-
tions would be developmentally impossible. The arterioventri-
cular alignments are secondary, not primary. How the great
arteries are aligned with the ventricles is secondary to infundib-
ular development and hence can be highly variable (Figure 1).
The great arteries typically arise above the ventricles, not from
the ventricles.
TOF is particularly instructive. According to the truncal
malseptation hypothesis, it used to be thought that TOF results
from truncoconal malseptation, creating an abnormally small
subpulmonary infundibulum, pulmonary valve, and main pul-
monary artery and reciprocally cutting off an abnormally large
aortic valve and ascending aorta. The disproof of this malsep-
tation hypothesis as applied to TOF is supplied by TOF with
absent pulmonary valve leaflets. In the latter anomaly, although
subpulmonary infundibular stenosis (typically moderate) is
present, the main pulmonary artery is huge, for hemodynamic
reasons (very large systolic to diastolic excursional variations,
resulting in an abnormally large main pulmonary artery). As far
as the classic malseptation hypothesis as an explanation of the
morphogenesis of TOF is concerned, we think one cannot have
it both ways, that is, infundibular stenosis favoring the aortic
outflow tract, at the expense of the pulmonary outflow tract, but
at the great arteries favoring the size of the pulmonary artery, at
the expense of the ascending aorta. We think that the size of the
great arteries in TOF is determined by hemodynamics, that is,
by the degree of obstruction of the subpulmonary conus,12 not
by truncoconal malseptation.
In TOF, why is the pulmonary valve too leftward, too pos-
terior, and too inferior compared with normal? And why is the
aortic valve reciprocally too rightward (overriding), too ante-
rior, and too superior compared with normal? We think that the
answer is because the subpulmonary conus (free wall and sep-
tum) has not grown and expanded to a normal extent. Hypopla-
sia of the subpulmonary conus is the essence of the ‘‘monology
of Stensen.’’12 This anomaly, first described by Stenson in
1671, causes the 4 malformations so well described by Fallot
in 1888 as a tetralogy. This is why, in tetralogy, the normal
developmental arterial switch procedure has been done subnor-
mally. The pulmonary valve is not as anterior, superior, and
rightward as it normally is. And reciprocally, the aortic valve
is not as posterior, inferior, and leftward as it normally is. In
TOF, resorption of the subaortic conal free wall usually is well
done, whereas subpulmonary conal expansion is subnormal,
resulting in pulmonary outflow tract stenosis or atresia. In TOF,
the subpulmonary conal septum is a variable: it can be a little
longer than normal, or normal in length, or unusually short,
or even absent (with pulmonary valve–to–aortic valve fibrous
continuity).
The aorticopulmonary septum is not always normally
formed. Truncus arteriosus13 with its AP window comes imme-
diately to mind. However, the main point is that subarterial
conal free wall development typically appears to be the princi-
pal problem in TOF, in D-TGA {S,D,D}, and in DORV
{S,D,D} (Figure 1).
It should be understood that there are 2 main parts to the
infundibulum or conus arteriosus: (1) the subsemilunar or ‘‘par-
ietal band’’ part (Figure 4A and 4B, component 4), and (2) the
‘‘septal band’’ part (Figure 4A and 4B, component 3).14,15
Component 4, the subsemilunar part of the conus, is the part
that is involved in normally and abnormally related and con-
nected great arteries. The ‘‘septal band’’ or apical part of the
conus or infundibulum can be important in anomalies such as
double-chambered right ventricle (also known as anomalous
muscle bundles of the right ventricle).
The true right ventricle is the right ventricular sinus, body,
or inflow tract, the main pumping portion of the right ventricle.
The right ventricle normally is limited by the tricuspid valve
proximally and by the conal or infundibular ring distally that
is formed by the conal septum, parietal band, septal band, and
moderator band (Figure 4A). The right ventricle sinus or inflow
tract normally is composed of 2 components: (1) the AV canal
(Figure 4A, component 1), and (2) the right ventricle sinus
(Figure 4A, component 2).14,15
372 World Journal for Pediatric and Congenital Heart Surgery 1(3)
372 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Thus, both ventricles are composed of 4 developmental
components (Figure 4A and 4B). The subsemilunar or distal
part of the conus (component 4) is the ‘‘architect,’’ responsible
for crossing the circulations. But what is the proximal or apical
part (component 3) of the conus doing? What is it there for?
The lower or apical part of the conus is the ‘‘mother’’ of the
right ventricular sinus (which is, of course, the lung pump). The
septal and moderator bands never dissociate from the right ven-
tricular sinus. In other words, the right ventricle sinus always
evaginates or pouches out just beneath the septal band. By con-
trast, the conal septum and the parietal band can be ‘‘any-
where,’’ as DOLV and ACM illustrate (Figure 1).
The right ventricle is our major cardiovascular evolutionary
adaptation to air breathing and land living.16 The subsemilunar
conus normally crosses the circulations by performing the aor-
tic switch, and the right ventricle sinus is the lung pump.
Single left ventricle17,18 results from the absence of the right
ventricle sinus (Figure 4A, component 2). The associated
infundibular outlet chamber consists of components 3 and 4
in Figure 4A. Absence of the right ventricle sinus results in a
single or unpaired left ventricle, often with double-inlet left
ventricle because there is no right ventricular sinus for the tricus-
pid valve to open into. Common-inlet left ventricle also occurs,
when a common AV canal and a common AV valve coexist.
Because the anatomically right ventricle is composed partly
of the right ventricle sinus or inflow tract (Figure 4A, compo-
nents 1 and 2) and partly of the infundibulum, or conus, or out-
flow tract (Figure 4A, components 3 and 4), the composite
Figure 4. What is the subsemilunar part of the conus? Anatomically, what are we talking about? (A) This is a diagram of a normal, opened,morphologically right ventricle (RV) that shows the 4 main anatomical and developmental component of the RV. The RV inflow tract consistsof 2 components: component 1 is the atrioventricular (AV) canal contribution (the interventricular part of the AV septum, and the tricuspidvalve); and component 2 is the RV sinus, the main pumping portion of the RV. The RV outflow tract also consists of 2 components:component 3 is the proximal or apical part of the conus, which consists of the septal band and the moderator band, which is not involved in theconotruncal malformations (such as TGA, DORV, DOLV, and ACM shown in Figure 1); and component 4 is the distal or subsemilunar part ofthe conus that is involved in the above-mentioned infundibuloarterial anomalies and that consists of the conal septum, the parietal band, andthe subsemilunar conal free wall, which may be well developed, or resorbed, and which may prevent or permit semilunar-AV fibrouscontinuity, respectively. (B) This is a diagram of a normal, opened, morphologically left ventricle (LV), showing that it too consists of 4anatomical and developmental components: 1, the AV canal contribution; 2, the finely trabeculated LV sinus portion; 3, the smooth superiorleft ventricular septal surface component that is confluent with the septal band of the RV (component 3 in A); and 4, the immediately subaorticconal septum, as seen from within the LV. Again, component 4 is the subsemilunar part of the conus that we are focusing on concerninginfundibuloarterial malformations. Note the approximation of the aortic valve and the mitral valve, which is made possible by the normalresorption of the subaortic infundibular free wall. So, it is what one does not see that is most important: no subaortic conal free wallmyocardium (because it has been resorbed), making possible the normal aortic-mitral fibrous continuity. Reproduced with permission fromVan Praagh and colleagues.15
Van Praagh 373
373 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

nature of the normally right-sided ventricle often is not well
understood and hence is delineated here. Thus, normally
related and connected great arteries illustrate how the develop-
mental arterial switch should be done by the subsemilunar
infundibular free wall. Abnormally related and connected great
arteries illustrate the consequences of alterations in this devel-
opmental process.
TOF illustrates what happens when the developmental arter-
ial switch procedure is done subnormally: The pulmonary
valve remains too leftward, posterior, and inferior; the
Figure 5. The 4 main anatomical types of subsemilunar infundibulum or conus arteriosus: subpulmonary, subaortic, bilateral (subaortic andsubpulmonary), and absent or very deficient. The upper row of diagrams shows the infundibulum (crosshatched) and great arteries as seenfrom the front (frontal view). The lower row of diagrams shows the infundibulum (crosshatched), the semilunar valves—the aortic valve (AoV),indicated by the coronary arteries, and the pulmonary valve (PV), indicated by the absence of coronary arteries—and the atrioventricularvalves—the mitral valve (MV), being a 2-leaflet valve, and the tricuspid valve (TV), being a 3-leaflet valve—as seen from below (inferior view),similar to a subxiphoid 2-dimensional echocardiogram. In all diagrams, a ventricular D-loop is assumed to be present. The subpulmonary conusis normal. Resorption of the subaortic conal free wall permits aortic-mitral fibrous continuity. The presence of a subpulmonary infundibulumprevents pulmonary valve–atrioventricular valve fibrous continuity. A subpulmonary conus is associated with solitus normally related greatarteries (diagrammed here), inversus normally related great arteries (diagrammed in Figures 1-3), and in tetralogy of Fallot, both with solitusnormally related great arteries12 and with inversus normally related great arteries. A subpulmonary conus can also be associated with double-outlet right ventricle with the hypoplastic left heart syndrome (eg, with mitral atresia) and with aortic-tricuspid fibrous continuity. Thesubaortic conus is characterized by resorption of the subpulmonary conal free wall, permitting pulmonary-mitral direct fibrous continuity. Thepresence of a complete muscular subaortic conus prevents aortic-atrioventricular fibrous continuity. The subaortic conus and great arteriesshown here are associated with typical D-transposition of the great arteries, that is, TGA {S,D,D} (Figures 1-3). A subaortic conus also occurswith L-TGA, that is, TGA {S,L,L}, and with TGA {I,L,L} (Figures 1-3). A bilateral conus, being both subaortic and subpulmonary, preventssemilunar-atrioventricular fibrous continuity. A bilateral conus is associated with typical double-outlet right ventricle, both with D-loopventricles and with L-loop ventricles (Figures 1 and 2). A bilateral conus can also be associated with TGA when there is a muscularsubpulmonary outflow tract obstruction (stenosis or atresia).26 Rarely, it is possible for solitus normally great arteries to be associated with abilateral conus if the subpulmonary part of the conus is well developed and if the subaortic conal free wall is present but poorly developed, just1 or 2 mm in height between the aortic valve above and the mitral valve below; I have seen only 1 such case in my life, in a patient with theincomplete form of common AV valve canal with an ostium primum defect at the atrial level, no ventricular septal defect, and a cleft mitralvalve. So, what matters most morphogenetically is not just the anatomical type of conus that is present but rather how much the subsemilunarconal free wall is present or has been resorbed. In the rare case that I am referring to, a small amount of the subaortic conal free wall had notbeen resorbed, but not enough to disrupt the normal type of aortic valve–to–left ventricular approximation. The bilaterally absent or verydeficient conus can be associated with double-outlet left ventricle (DOLV) with aortic-mitral and pulmonary-mitral fibrous continuity, evenwith an intact ventricular septum.19 However, DOLV does not always have a bilaterally absent or very deficient conus.27 Figure 2 shows thediagram of a rare type of D-TGA with a bilaterally deficient conus, but with aortic valve–to–tricuspid valve fibrous continuity and withpulmonary valve–to–mitral valve fibrous continuity. It is also noteworthy in Figure 2 that a bilaterally absent or very deficient conus is notdiagrammed in association with L-loop ventricles. Why not? Because we have never seen this. It may occur (but I do not know that). Figure 2 isevidence based (not hypothetical, except where indicated by broken lines). AD ¼ anterior descending (coronary artery); Ant ¼ anterior(ventral); Inf ¼ inferior (caudad); Lt ¼ left; Post ¼ posterior (dorsal); Rt ¼ right; Sup ¼ superior (cephalad). Reproduced with permission fromVan Praagh.28
374 World Journal for Pediatric and Congenital Heart Surgery 1(3)
374 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Figure 6. The 4 main hypotheses concerning the morphogenesis of transposition of the great arteries. (1) Malseptation of the great arteries,that is, straight (as opposed to spiral) development of the aortopulmonary septum, first proposed (to our knowledge) by Quain5 in 1844 andsubsequently espoused by many authors. Ao ¼ aorta; AoV ¼ aortic valve; PA ¼ pulmonary artery; PV ¼ pulmonary valve. The semilunar valvesare designated by conventional numbers for clarity because their relative positions are highly variable. There are 4 septal semilunar leaflets,adjacent to the aortopulmonary septum: aortic and pulmonary leaflets 1, and aortic and pulmonary leaflets 3. Pulmonary leaflet 2 is nonseptal,remote from the aortopulmonary septum. Aortic leaflet 4 is also nonseptal and normally is noncoronary. The nonseptal semilunar leaflets arealso known as the intercalated leaflets. Comparison of the semilunar leaflet numbers with normally related great arteries (NRGA) as opposedto those with transposition of the great arteries (TGA) indicates (in degrees) the morphogenetic movement that has occurred with NRGA andhas not occurred with TGA. Both with NRGA and with TGA, the distal aortopulmonary relations at the aortic arch and pulmonary bifurcationare the same: the Ao arch is ventral and cephalad to the PA bifurcation because this is the fixed aortic arch 4–to–pulmonary arch 6 relationshipdistally. The straight aortopulmonary septum hypothesis is considered to be wrong for several reasons: (a) In TGA, the free walls of the greatarteries are just as abnormal as is the aortopulmonary septum. This is indicated by the abnormal locations of the coronary ostia in TGA, the
Van Praagh 375
375 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Figure 6 continued. coronary arteries being the first branches of the aortic free wall. So, TGA is more than an anomaly ofthe aortopulmonary septum because the great arterial free walls are also very abnormally located. (b) Definite evidence of abnormality of theaortopulmonary septum, such as AP window, is very rare in TGA. (c) The straight aortopulmonary septum hypothesis cannot explain thevariations in semilunar valve heights in the so-called conotruncal malformations, such as the aortic valve sitting high above the morphologicallyleft ventricle in anatomically corrected malposition of the great arteries {S,D,L} (Figure 1, row 6, column 1).10 (2) Conal maldevelopment. In1909, Keith23 was the first to propose that TGA results from persistence and development of the subaortic part of the conus (in white) andinvolution of the subpulmonary part of the conus (in black). In 19668 and 1967,7 we independently reached the same conclusion andsubsequently have extended the conal maldevelopment hypothesis to include all of the conotruncal anomalies (Figure 1).1-4,6-13 Note thatKeith23 and Cardell32 and many others thought that the normal semilunar relationships are pulmonary valve anterior, superior, and to the rightof the aortic valve, a frequent preangiocardiographic error. (3) Atavism. In 1923, Spitzer29,30 proposed a hypothesis of evolutionary(phylogenetic) regression to explain TGA in man, back to the cardiovascular state that is normal in higher reptiles such as crocodiles andalligators. One might suppose that such a hypothesis would strike investigators as hilariously funny. Instead, it mesmerized a generation.30,33 Myreaction (with a wink) was that our patients with TGA did not have tails, their smiles were not unusually wide, and they almost never hadichthyosis or any other features that suggested reverse evolution back to the crocodilian stage. So, I decided to study Spitzer’s theory29,30 withgreat care. Lev and Vass’s30 translation into English was very helpful. Finally, I understood what was wrong with this hypothesis in terms ofpathological anatomy. The dotted line indicates where the true ventricular septum was in TGA but has disappeared, according to Spitzer29,30
(left lower panel). Spitzer’s bicuspid, apparently stenotic, transposed pulmonary valve sits above the morphologically right ventricularmyocardium, to the right of the disappeared ventricular septum in D-loop ventricles. His diagram suggests that there is a ventricular septaldefect. Spitzer29,30 also states that the apparent ventricular septum is a hugely hypertrophied crista supraventricular (supraventricular crest),not the true interventricular septum (which has disappeared). So, in terms of pathological anatomy, what is wrong with Spitzer’sinterpretation? The anteroseptal region of the left-sided ventricle from which the transposed pulmonary artery arises in typical TGA consistsonly of the morphologically left ventricular myocardium. There is no morphologically right ventricular myocardium there to the right ofSpitzer’s dotted line. Spitzer does not explain how or why the ventricular septum routinely disappears in TGA. Crocodiles and alligatorsnormally have both a left ventricular aorta and a right ventricular aorta. Spitzer hypothesizes that human TGA represents reopening of theright ventricular aorta of the higher reptiles, plus closure of the left ventricular aorta of the higher reptile and mammals. So, Spitzer’s problemwas not to explain the right ventricular aorta in human TGA: all higher reptiles have a right ventricular aorta, as Spitzer knew. However,Spitzer’s real problem was the left ventricular pulmonary artery of human TGA because there is no animal known in which the pulmonaryartery normally originates above the morphologically left ventricle. This seems to be why Spitzer29,30 contended that the ventricular septum, tothe left of the ‘‘transposed’’ pulmonary artery, has disappeared. In this way, the pulmonary artery can be diagrammed as arising above the rightventricular myocardium, which is essential in any atavistic explanation of human TGA, because there is no animal known in which thepulmonary artery normally arises above the morphologically left ventricle. This hypothesis denies the reality of human TGA and asserts thatthe double-outlet right ventricle (DORV) is really present. The fatal flaw in Spitzer’s hypothesis29,30 of evolutionary regression to explain themorphogenesis of TGA is that in human TGA, the pulmonary artery really does arise above the morphologically left ventricle, the trueventricular septum is present and has not disappeared, and TGA (ventriculoarterial alignment discordance) really is present, not DORV. Infairness to Spitzer, it must be added that at his time (1923), what we now call DORV was then regarded as a form of TGA. Previousinvestigators have attempted to assess Spitzer’s hypothesis.30,33 It has been regarded with some doubt and skepticism. We may have been thefirst to indicate that Spitzer’s hypothesis29,30 is wrong because it is not supported by the morphological anatomical data of human TGA (asabove). (4) Fibrous malattachment. In 1962, Grant31 proposed that normally, there is a fibrous tract of low growth potential that tethers thedeveloping aortic valve (A) to the developing mitral valve (M), resulting in aortic-mitral fibrous continuity; the pulmonary valve (P) is nottethered either to the mitral valve (M) or to the tricuspid valve (T), and consequently, the pulmonary valve is normally anterior to the aorticvalve, the pulmonary valve being in communication with the anterior and right-sided ventricle (right lower panel). The fibrous tract betweenthe normally related aortic valve and the mitral valve is known as the intervalvar fibrosa. Grant’s31 hypothesis is that in TGA, this fibrous tractis shifted leftward, such that the developing pulmonary valve (P) is tethered to the developing mitral valve (M), resulting in pulmonary-mitralfibrous continuity and a left ventricular pulmonary artery. The aortic valve (A) is now untethered, and consequently, the aortic valve (A) isanterior to the pulmonary valve (P), with the aorta being above the anterior and right-sided right ventricle, as in typical TGA in man. So, thequestion becomes the following: Is there anything wrong with Grant’s31 hypothesis? Why could a fibrous tract of low growth potentialbetween the mitral valve (M) and the wrong semilunar valve, the pulmonary valve (P), not be the primary morphogenetic mechanismunderlying human TGA? This fibrous malattachment hypothesis31 cannot explain TGA with a bilateral conus (subaortic and subpulmonary).26
The presence of subpulmonary conal musculature would prevent the hypothesized abnormal pulmonary-mitral fibrous continuity that occurswhen TGA has a subaortic conus only. This fibrous malattachment hypothesis31 also cannot explain those rare cases of TGA with asubpulmonary conus,26 that is, short subpulmonary muscular conus with aortic valve–to–tricuspid valve fibrous continuity, in which thetransposed aortic valve can be posterior and inferior to the transposed pulmonary valve. This fibrous malattachment hypothesis, asproposed,31 cannot explain TGA with aortic-tricuspid fibrous continuity and a short subpulmonary conus. Grant’s hypothesis31 also does noteasily explain those rare cases of TGA with aortic-tricuspid and pulmonary-mitral fibrous continuity with a bilaterally deficient or absent conusbeneath both great arteries.26 Consequently, we prefer the view that regards subarterial conal free wall development—growth orresorption—as the primary morphogenetic mechanism. We think that semilunar-atrioventricular fibrous continuity or noncontinuity issecondary to subarterial conal free wall development (resorption or growth, respectively). The latter hypothesis can explain all of theanatomical data. The infundibuloarterial (conotruncal) anomalies (Figure 1) are appropriately named in terms of their pathological anatomy.Anatomically, both the infundibulum or conus arteriosus and the great arteries are malformed. Embryologically, or developmentally, however,the infundibuloarterial (conotruncal) anomalies are importantly misnamed. They are all infundibular or conal anomalies, like tetralogy of Fallot.The great arteries per se are normally formed. The real problem is the little hollow ‘‘platforms,’’ the coni arteriosi (arterial cones) orinfundibula (funnels) on which the great arteries stand, and which connect the great arteries above to the underlying ventricles, ventricularseptum, and atrioventricular valves below. Reproduced with permission from Van Praagh.6
376 World Journal for Pediatric and Congenital Heart Surgery 1(3)
376 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

subpulmonary infundibulum is obstructive (stenotic or atretic);
the aortic valve remains too rightward, anterior, and superior
(‘‘overriding’’); and a large subaortic conoventricular
malalignment type of ventricular septal defect typically results.
The fourth feature of Fallot’s tetrad, right ventricular hypertro-
phy, is not present at birth in tetralogy because right and left
ventricular pressures are essentially equal prenatally. Postna-
tally, however, right ventricular ‘‘hypertrophy’’ (compared
with normal) develops because the normal thinning of the right
ventricular free wall fails to occur, in turn because of the per-
sistence of systemic pressures in the right ventricle related to
the large subaortic VSD and right ventricular outflow tract
obstruction that are parts of the TOF. Subnormal performance
of the normal embryonic arterial switch process is what TOF
really is.
TGA {S,D,D} illustrates what happens if the arterial switch
operation is done in reverse, that is, if the pulmonary valve and
artery are approximated to the mitral valve and if the aortic
valve remains above the right ventricle. DORV {S,D,D} with
a bilateral conus illustrates what happens if the embryonic aor-
tic switch by the subsemilunar conus is not performed at all,
that is, if neither semilunar valve is switched into the left ven-
tricle and if both semilunar valves remain above the right ven-
tricle because subsemilunar conal free wall absorption has
failed to occur.
DOLV {S,D,D} (Figure 1) illustrates what can happen if
both the subaortic and the subpulmonary parts of the conus
undergo resorption, resulting in aortic-mitral and pulmonary-
mitral direct fibrous continuity.11,19 In this situation, the devel-
opmental arterial switch procedure performed by the resorption
of both parts of the subsemilunar conal free walls results in
‘‘overdoing’’ of the arterial switch procedure. Rarely, both
great arteries can come to overlie the left ventricle only, even
with an intact ventricular septum.19
Thus, there are 4 ways in which the distal or subsemilunar
infundibulum can perform the embryonic arterial switch
procedure:
1. normally;
2. in reverse (typical D-TGA);
3. not at all (typical DORV); or
4. in excess (rarely DOLV) (Figure 1).
Truncus arteriosus13,20,21 is the only infundibuloarterial
(conotruncal) anomaly in which the great arteries themselves
are primarily malformed. Again, the classic AP malseptation
hypothesis was used to explain the embryogenesis of truncus
arteriosus communis (common arterial trunk, Latin). The
classic hypothesis was that the AP septum fails to grow down-
ward (caudad) from the aortic arch 4/6 junction. Conse-
quently, it was hypothesized that the ascending aorta and
the main pulmonary artery were not completely separated
from each other and hence remained in common. Also, the
common semilunar valve was not divided into aortic and pul-
monary valves, and the conus was not septated, resulting in a
large subsemilunar VSD.
When I was working at the Congenital Heart Disease
Research and Training Center in the Hektoen Institute for Med-
ical Research at Chicago (1963-1965) with Dr Maurice Lev,
I was given truncus arteriosus as a research project. Dr Lev asked
me to figure it out: What is truncus arteriosus really? As usual,
I collaborated with Dr Stella Van Praagh.13 Fortunately, some
cases of ‘‘pseudotruncus,’’ that is, TOF with pulmonary outflow
tract atresia, had been misfiled along with the cases of ‘‘true’’ or
‘‘genuine’’ truncus arteriosus. So, I examined them all.
Then, it struck me. I realized that I could not tell pseudotruncus
from so-called true truncus by examining the right ventricular
outflow tract anatomy unless I let myself look at the great arteries.
In other words, I was astonished to find that the right ventricular
outflow tract anatomy in truncus was identical with, or exceed-
ingly similar to, that found in typical tet-atresia (TOF with right
ventricular outflow tract atresia). I realized that was not the
way it was supposed to be in truncus. According to the classic
truncoconal malseptation hypothesis, truncus was thought to
result from absence of truncoconal septation, but the truncoconal
free walls were thought to be normal (uninvolved).
But that is not what I saw in truncus. The whole semilunar
infundibulum was involved: the conal septum and free wall
were both anomalous. Very similar to tet-atresia, the conus in
truncus appeared to be atretic, unexpanded, with no infundibu-
lar lumen. I realized that if the classic nonseptation hypothesis
were correct in truncus, at the level of the right ventricular out-
flow tract, I should be looking at an infundibular or conal septal
defect only, with a normally formed infundibular free wall.
Instead, in truncus arteriosus, the whole subsemilunar infundi-
bulum appeared to be involved, septum and free wall, resulting
in an unexpanded, or very poorly expanded, subpulmonary
infundibulum, as in TOF with pulmonary outflow tract atresia.
I realized that if the problem in truncus were just a conal septal
defect (at the level of the right ventricle outflow tract), then,
there should be no right ventricle outflow tract obstruction
(no stenosis nor atresia), and the overlying semilunar valve (the
pulmonary valvar component of a common semilunar valve)
should be uninvolved. I should find the expected 4-leaflet,
undivided, common semilunar valve. So, I then examined the
semilunar valves in truncus. Never was the predicted
4-leaflet semilunar valve present. Typically, the semilunar valve
in truncus arteriosus was tricuspid and tricommissural, very
similar to, if not identical, with an aortic valve.
What did the anatomical findings suggest? Typical so-called
truncus arteriosus looked like pulmonary infundibular atresia
with consequent partial or complete absence of the overlying
pulmonary valve, associated with an AP septal defect of vari-
able size, often with a right aortic arch.13 In other words, typ-
ical truncus arteriosus appears to be TOF with pulmonary
outflow tract atresia, with partial or total absence of the pul-
monary valvar leaflets, and an AP window, that is, an anomaly
closely akin to the most severe form of TOF, only even worse.
Typically, truncus arteriosus maintains a tenuous truncal
valve (ie, aortic valve)–to–mitral valve direct fibrous continu-
ity, very similar to TOF. Rarely, however, truncus arteriosus
can originate exclusively above the right ventricle, with a
Van Praagh 377
377 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

well-developed subtruncal muscular infundibulum that pre-
vents semilunar-AV fibrous continuity. We also think that in
truncus arteriosus type A213 (type A means that a VSD is pres-
ent, and type 2 means there is little or no AP septal remnant),
the main pulmonary arterial component may well be absent
(hence, no AP septal remnant).
Why do we think that? Because we have seen 2 rare cases,21
with normal {S,D,S} segmental anatomy, which had the fol-
lowing: no VSD; a main pulmonary artery arising from the
right ventricle, giving off no pulmonary artery branches and
passing through a slightly narrowed patent ductus arteriosus
into the descending thoracic aorta; and an aorta arising nor-
mally from the left ventricle, giving off coronary arteries nor-
mally and then part way up the ascending aorta, giving origin
to the right and left pulmonary artery branches, then forming
an aortic arch and giving off the brachiocephalic arteries nor-
mally, and continuing through the aortic isthmus into the des-
cending thoracic aorta.21
When one of our colleagues, an eminent cardiovascular
radiologist, saw these angiocardiograms, he quipped the fol-
lowing: ‘‘Get rid of it. It’s impossible.’’ But why is this anom-
aly21 relevant to truncus arteriosus type 2? Because the
pulmonary artery branches originate from the aorta (ie, from
the aortic sac part of the distal truncus arteriosus). In normal
development, the pulmonary artery branches then migrate
somewhat to the left, where the pulmonary artery branches then
become confluent with the main pulmonary artery. But rarely,
this normal leftward migration of the pulmonary artery
branches can fail to occur, resulting in a nonbranched main pul-
monary with both pulmonary artery branches arising from the
ascending aorta.21
Now, consider truncus type 2: there is no AP septal remnant,
and both pulmonary artery branches arise from the so-called
common arterial trunk. Is it really a common arterial trunk?
Our hypothesis is that in truncus type 2, the main pulmonary
artery component may be absent21; hence, there is no AP septal
remnant in truncus type 2. In the case of the nonbranched main
pulmonary artery described above, if there had been subpul-
monary infundibular atresia, the overlying pulmonary valve,
main pulmonary artery, and ductus arteriosus might well have
been atretic and have undergone involution. In truncus arterio-
sus type 2, we conventionally assume that a main pulmonary
artery component must be present, even though we cannot see
it and there is no AP septal remnant to indicate where this
hypothetical main pulmonary arterial component is located.
Why do we make this assumption? Because most people do
not know that the pulmonary artery branches initially arise from
the aorta (the aortic sac), and most do not wonder why there is
no AP septal remnant. In view of the hypothesis that the main pul-
monary artery component is really absent in type 2, we talk about
truncus arteriosus; that is, we omit the communis adjective. We
think that truncus arteriosus type 2 may very well be a truncus aor-
ticus solitarius, that is, a solitary aortic trunk, not a truncus arter-
iosus communis, that is, a common (AP) arterial trunk.
When we measured the right-left width of the truncus, we
found that in type 1 (that does have a main pulmonary artery
component), low down (just above the semilunar valve level),
the truncus is wider than higher up, above the origins of the pul-
monary artery branches where the truncus becomes distinctly
narrower. But in truncus type 2, the truncus is about the same
width, just above the semilunar valve level, and above the ori-
gins of the pulmonary artery branches. Why this difference in
truncal transverse dimensions between types 1 and 2? We think
that the answer is because there is a demonstrable main pul-
monary artery component in type 1 (which makes it wider low
down) but not in type 2 (hence, little or no difference between
low-down and higher-up dimensions in type 2). Were we sur-
prised by the anatomical findings in truncus arteriosus? Yes.
Briefly, truncus arteriosus is a much more interesting form of
congenital heart disease than has been generally understood.
The 5 diagnostically and surgically important cardiac seg-
ments consist of the 3 main cardiac segments (Figure 1): (1) the
visceroatrial situs, important for atrial localization; (2) the ven-
tricular loop, important for ventricular localization; and (3) the
great arteries, important hemodynamically; and 2 connecting
cardiac segments: (4) the AV canal or junction, important for
the AV valves and the AV septum; and (5) the conus arteriosus
or infundibulum, important concerning the right and left ventri-
cular outflow tracts and the alignments and connections of the
great arteries.
These 5 cardiac segments consist of 4 independent variables
and 1 dependent variable. The 4 independent variables are
(1) the visceroatrial situs, (2) the ventricular loop, (3) the conus
arteriosus, and (4) the great arteries (truncus arteriosus). The
1 dependent variable is the AV canal, in the sense that the situs
of the AV valves typically corresponds to that of the ventricular
loop and ventricles of entry, not to that of the atria of exit.
This presentation has thus far focused primarily on the sub-
semilunar part of the infundibulum and on the great arteries.
Although these 2 cardiac components are very important con-
cerning the understanding of abnormally related great arteries,
they are not the whole story. We must now widen our focus to
consider what may be called (with a wink) ‘‘the segmental situs
salad’’ of complex congenital heart disease (Figure 1). A few
examples will suffice as illustrations.
Classic congenitally physiologically corrected TGA,22 that
is, TGA {S,L,L} (Figure 1, row 5, column 2), has not only the
subsemilunar maldevelopment discussed above but also a dis-
cordant ventricular L-loop with AV and VA discordance, as is
now quite well understood.
ACM9,10 (Figure 1, row 6) is far rarer and is consequently
less well understood. In all anatomical cases of ACM that we
have examined, the ventricles have looped in one direction, and
the great arteries have twisted in the opposite direction. For
example, in ACM {S,D,L} (Figure 1, row 6, column 1), the
ventricles have looped to the right, but the infundibuloarterial
part of the heart (the conotruncus) has twisted to the left. These
opposite morphogenetic movements have resulted in the rare
VA alignments known as anatomically corrected malposition.
In ACM {S,D,L}, although the great arteries are very malposi-
tioned, they nonetheless originate above the anatomically cor-
rect ventricles: aorta above the left ventricle, and pulmonary
378 World Journal for Pediatric and Congenital Heart Surgery 1(3)
378 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

artery above the right ventricle (Figure 1). It is in this sense that
these malposed great arteries are anatomically corrected. ACM
{S,D,L} is also physiologically corrected because there is both
AV and VA concordance. By contrast, ACM {S,L,D} (Figure 1,
row 6, column 2) is anatomically corrected but physiologically
uncorrected because there is one intersegmental alignment
discordance, at the AV level.
It is noteworthy that ACM always has VA concordance, by
definition. Thus, VA concordance is not synonymous with nor-
mally related great arteries. In ACM, the VA alignments are
concordant, but the VA connections (the anatomical types of
conus) are always very abnormal; hence, the malposition of the
great arteries. In ACM, the conal connector is either bilateral
(subaortic and subpulmonary) or subaortic (only).
The 4 anatomical types of conus are presented in Figure 5 2:
1. subpulmonary (only), with normally related great arteries;
2. subaortic (only), with typical TGA (and other VA
alignments);
3. bilateral, that is, subaortic and subpulmonary, with DORV
and TGA (and other VA alignments); and
4. absent or very deficient, with DOLV, and rarely with TGA.
Why the ventricles loop in one direction and the great
arteries twist in the opposite direction in ACM is unknown at
present.
Is it possible to have a normal type of infundibulum and
great arteries in association with abnormally related great
arteries such as DORV? The answer is yes. For example,
when DORV is associated with mitral atresia and a diminu-
tive left ventricle, one can have DORV {S,D,‘‘S’’} with
aortic-tricuspid fibrous continuity and a well-developed
subpulmonary infundibulum. Often, the atretic mitral valve
cannot be identified anatomically, and the left ventricle may
also be unidentifiable. DORV with a unilateral conus (sub-
pulmonary only or subaortic only) is a specific anatomical
type of DORV that is associated with the hypoplastic left
heart syndrome (such as mitral atresia with a diminutive
or apparently absent left ventricle).
In the designation DORV {S,D,‘‘S’’}, the quotation marks
about the ‘‘S’’ save it from anatomical inaccuracy. Logically,
can one really have DORV if the infundibulum and great
arteries are of the normal type? Logically, one might think not.
But anatomically, it does happen. How can that be? Remember,
we are considering the spatial relations, alignments, and con-
nections between the infundibulum and great arteries above
and the ventricular septum and the AV canal and valves below.
Usually, the anomalies involve the infundibulum and occasion-
ally the great arteries above. But important malformations can
also involve the underlying ventricles and the AV valves. So,
abnormally related great arteries are not always about the
infundibulum and great arteries.
Hence, in the situation of DORV {S,D,‘‘S’’} mentioned
above, we think that the excusing quotation marks about the
‘‘S’’ are necessary to avoid anatomical inaccuracy. The spatial
relations, alignments, and connections between the solitus
normal infundibulum and great arteries cannot be entirely nor-
mal because of the anomalies involving the mitral valve and
left ventricle, which is why DORV is present (rather than nor-
mally related great arteries).
Others may prefer to designate this as DORV {S,D,D} and
state that there is aortic-tricuspid fibrous continuity with a sub-
pulmonary conus. We prefer DORV {S,D,‘‘S’’} to indicate that
the infundibulum and the great arteries really are of the normal
type and to suggest that the cause of the DORV lies elsewhere,
that is, because of the coexistence of the hypoplastic left heart
syndrome.
Perhaps the biggest lesson that we have learned is that
the classic AP malseptation hypothesis that used to be
invoked to explain the abnormal development and the
pathological anatomy of abnormally related great arteries
is incorrect, as explained above. Instead, the subsemilunar
infundibulum or conus arteriosus, which normally performs
the embryonic aortic switch procedure by growth of the sub-
pulmonary infundibular free wall and by resorption of the
subaortic infundibular free wall, is usually where the anom-
aly is located. The only relatively frequent exception of
which I am aware is truncus arteriosus, in which the great
arteries per se are also primarily malformed, as summarized
above.
Arthur Keith23 (later to become Sir Arthur Keith) was, to
my knowledge, the first to report in 1909 the concept that
TGA results from persistence and development of the subaor-
tic part of the conus and involution of the subpulmonary part
of the conus. However, the conal maldevelopment hypothesis
was subsequently ‘‘forgotten’’ in favor of the classic
AP malseptation concept.6 Based on the study of many post-
mortem cases of congenital heart disease (TGA7 and others8),
I had decided by 1967 that conal maldevelopment was the
right idea. Then, in reviewing the literature on this topic, I was
delighted to find Keith’s Hunterian lecture23 that confirmed
our conclusions.7
Discussion
What we and others have learned concerning normally and
abnormally related great arteries amounts to a general princi-
ple. As mentioned previously, the most important points are the
following. The great arteries per se are seldom the primary site
of malformation; exceptions in which the great arteries them-
selves are anomalously formed include truncus arteriosus and
AP ‘‘window.’’
In essentially all other cases, when the great arteries appear
to be malformed and anatomically are malpositioned (Figure 1),
the primary site of malformation is the subsemilunar infundibu-
lum, the hollow conical ‘‘platforms’’ on which the semilunar
valves and great arteries stand, which connect the great arteries
above to the underlying ventricles, ventricular septum, AV
canal, and AV valves.
The general principle is that both normal and abnormal rela-
tionships of the great arteries are largely determined by ventri-
cular loop formation and by asymmetrical development of the
Van Praagh 379
379 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

subsemilunar conal free walls. Normally, asymmetrical conal
development involves growth of the subpulmonary conal free
wall and resorption of the subaortic conal free wall (Figures
1-5). Abnormally, the subsemilunar conal free walls can
develop in reverse, with growth of the subaortic infundibular
free wall and resorption of the subpulmonary conal free wall,
resulting in TGA (Figures 1-3 and 5). Or both the subaortic
and the subpulmonary conal free walls can grow and expand,
typically resulting in a DORV (Figures 1, 2, and 5). Or the
opposite can happen: resorption of both the subaortic and the
subpulmonary conal free walls, which can result in a DOLV
(Figures 1 and 5).
Morphogenesis
For many years, there has been considerable interest in the
morphogenesis of TGA. Four main hypotheses have emerged
(Figure 6):
1. straight development of the AP septum, also known as the
truncal malseptation hypothesis, first proposed by Quain5
in 1844;
2. conal maldevelopment, first presented by Keith23 in 1909;
3. atavism, outlined by Spitzer29,30 in 1923; and
4. maldevelopment of the intervalvar fibrosa between the
semilunar and the AV valves, proposed by Grant31 in 1962.
Why do we think that maldevelopment of the subsemilunar
conal free walls is the correct concept concerning the morpho-
genesis of all the forms of abnormally related great arteries (not
just for TGA)? Because abnormally related great arteries
always have a malformation of the subsemilunar infundibular
free walls (Figure 1), whereas normally related great arteries8
(solitus and inversus normally related great arteries) do not
(Figure 1). This was our realization in discovering and describ-
ing isolated ventricular inversion {S,L,S}8 (Figure 1, row 3,
column 2). The lesson of this case was and still is the following:
if the subsemilunar conus is of the solitus normal type, that is, a
subpulmonary muscular conus preventing pulmonary-AV val-
var fibrous continuity, with a resorbed subaortic conal free wall
permitting aortic-mitral fibrous continuity (Figure 5), then, the
great arteries are solitus normally related, even if the ventricles
are inverted because of the coexistence of L-loop ventricles.8
This was our ‘‘ah ha!’’ moment.8 Two principles had
become clear:
1. When the great arteries are abnormally related, an anomaly
of the subsemilunar conal free walls is almost always pres-
ent (Figure 1).
2. When the great arteries are normally related, a full-blown
malformation of the subsemilunar conal free walls is never
present (Figure 1).
The above-mentioned pathological anatomical data strongly
suggest that embryological investigations should focus on the
development of the subsemilunar conal free walls (rather than
on the development of the AP septum).6
What is wrong with the straight AP septum hypothesis of
Quain5 and many subsequent investigators (Figure 6)?6 As
noted heretofore, TGA is much more than just a relatively
straight, nonspiral AP septum. In TGA, the great arterial
free walls are also very much involved, that is, positionally
abnormal anatomically. What is the proof of that? The
answer is the coronary arteries. The first branches of the
aortic free wall are the coronary arteries. The locations of
the coronary ostia in TGA are very abnormally related (Fig-
ure 6, upper left). Thus, anatomically, TGA is an anomaly
of both the AP septum and of the free walls of both great
arteries, not of the AP septum only.
If TGA were caused by anomalous septation of the great
arteries, then, definite evidence of malformation of the AP sep-
tum, such as AP septal defect (AP ‘‘window’’), would be rela-
tively common in association with TGA. In fact, however, the
association of AP window with TGA is vanishingly rare. The
straight AP septum hypothesis also cannot explain the varia-
tions in semilunar valve heights, for example, why in TGA the
aortic valve is high and the pulmonary valve is low, which is
the opposite of normally related great arteries.
Aficionados of the classic straight AP septum hypothesis
have tried to explain away this weakness of the straight AP sep-
tum concept as follows: Of course, the transposed aortic valve
is high and the transposed pulmonary valve is low (which is the
opposite of normal) because the transposed aortic valve sits on
the conus, which is a part of the morphologically right ventri-
cle, whereas the transposed pulmonary valve is low, having no
conus to sit on, and consequently, the transposed pulmonary
valve is in fibrous continuity with the mitral valve. The prob-
lem with this ‘‘explanation’’ is the assumption that the subse-
milunar part of the conus is part of the morphologically right
ventricle. In fact, it is not.
Experience has taught us that the distal or subsemilunar part
of the conus can straddle the ventricular septum, to virtually
any degree. In ACM {S,D,L}10 (Figure 1, row 6, column 1) and
in DOLV,11 for example, the subsemilunar conus arteriosus can
be mostly above the morphologically left ventricle. The first
time that one sees a well-developed left-sided left ventricle sur-
mounted by a well-formed crista supraventricularis (conal mus-
culature) leading to an L-malposed aorta10 may come as quite a
shock. Many cardiac radiology textbooks define a morphologi-
cally right ventricle as the ventricle with a crista supraventricu-
laris (supraventricular crest). The problem is that the foregoing
definition of the right ventricle is not true. Usually, the crista is
above the right ventricle, but not always.
Exceptions do not prove the rule, except in a statistical sense
of indicating what is common. Exceptions really indicate that
there is something wrong with the rule, and one better find out
what it is. This kind of case taught us that the subsemilunar
conus ‘‘belongs to’’ the great arteries and is not an intrinsic,
inseparable part of either ventricle. The conotruncus concept
of the embryologists is correct. The conal maldevelopment
hypothesis can explain the variations in semilunar valve
380 World Journal for Pediatric and Congenital Heart Surgery 1(3)
380 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

heights (without invoking erroneous assumptions). The subpul-
monary and the subaortic parts of the conus act as little hollow
platforms on which the great arteries stand. The better devel-
oped the subsemilunar conus (subpulmonary, or subaortic, or
both, or neither) (Figure 5) happens to be, then, the higher and
the more anterior that semilunar valve is (Figures 2, 4, and 5).
Although Keith’s23 conal maldevelopment hypothesis was,
we think, essentially correct (as above), it is noteworthy in Fig-
ure 6 (top right) that he did not get the normal semilunar inter-
relationship quite right. His drawing shows the normally
related pulmonary valve as being anteriorly and to the right
of the normally related aortic valve. As all of us who grew
up in the catheterization laboratory know, the normally related
pulmonary valve should be anterior, superior, and to the left of
the normally related aortic valve. Also, the subpulmonary part
of the conus (shown in black, Figure 6) normally ends up some-
what further to the right than it should be.
What is wrong with Spitzer’s atavistic hypothesis to explain
the morphogenesis of TGA (Figure 6, lower left)?29,30 He
called his hypothesis a phylogenetic theory. It will be recalled
that phylogeny has to do with evolution, that is, the evolution-
ary development of a phylum, for example, of a species or
genus (Greek phule, tribe, clan), whereas ontogeny has to do
with the development of an individual organism (Greek, from
on [stem ont-], the present participle of einai, to be). Thus, the
prefix onto- indicates being or existence. Consequently, phylo-
geny means evolutionary development, whereas ontogeny
denotes individual development (embryology).
In 1923, Spitzer29,30 proposed a hypothesis of evolutionary
regression, back to the stage that is normally found in higher
reptiles such as crocodiles and alligators. Such higher reptiles
have both a left ventricular aorta and a right ventricular aorta.
Spitzer’s hypothesis29,30 is that the transposed aorta of human
TGA represents the reopened right ventricular aorta of the
higher reptiles and the closure of the left ventricular aorta of
higher reptiles and mammals. However, the fatal flaw in this
atavistic hypothesis involves the transposed pulmonary artery.
Spitzer states that the anterior portion of the true interventricu-
lar septum has disappeared: the location of the absent true ven-
tricular septum he indicates by a broken line. The apparent
ventricular septum anteriorly in TGA, Spitzer says, is a false
ventricular septum, a hugely hypertrophied crista supraventri-
cularis. In this way, Spitzer claims that the transposed pulmon-
ary valve and artery are arising from above the right ventricular
myocardium, that is, originating to the right of the vanished
true ventricular septum.
Why is this contention important? Because there is no ani-
mal known in which the pulmonary artery normally originates
above the morphologically left ventricle. Unfortunately for
Spitzer’s atavistic hypothesis,29,30 and indeed for any hypoth-
esis of phylogenic regression, the left-sided ventricle above
which the transposed pulmonary artery typically arises is com-
posed entirely of morphologically left ventricular myocardium.
There is no morphologically right ventricular myocardium
anteroseptally in this left-sided ventricular chamber. The
apparent ventricular septum is indeed the true ventricular
septum. There has been no ventricular septal disappearance,
contrary to Spitzer’s diagram (Figure 6, lower left). The anato-
mical data do not support Spitzer’s hypothesis.29,30
What is wrong with Grant’s31 fibrous malattachment
hypothesis, first proposed in 1962? Grant proposed that nor-
mally, there is a fibrous tract of low growth potential that
tethers the developing aortic valve to the developing mitral
valve (Figure 6, lower right). This causes the normal aortic-
mitral fibrous continuity and permits the pulmonary valve to
be anterior to the aortic valve, and the pulmonary valve is nor-
mally not in continuity with either the mitral valve or the tricus-
pid valve (Figure 6, lower right).
In TGA, Grant proposed that this fibrous tract of low growth
potential is shifted to the left so that it lies between the mitral
valve and pulmonary valve (not between the mitral valve and
aortic valve, which is normal). This left shift of the fibrous tract
tethers the pulmonary valve to the mitral valve but leaves the
aortic valve free and not in fibrous continuity with either AV
valve (mitral valve or tricuspid valve), as in typical TGA.
What is wrong with this fibrous malattachment hypoth-
esis?31 It cannot explain all of the conal anatomical types that
are found in association with TGA.26 Specifically, it cannot
explain those cases of TGA with a bilateral subsemilunar conus
(subaortic and subpulmonary) in which there is no pulmonary-
mitral fibrous continuity.
What anatomical types of subsemilunar conus are associated
with D-loop TGA in which a VSD is present? In 1993, Pasquini
and colleagues26 tried to answer this question, based on a study
of 119 cases of D-loop TGA with VSD:
1. a subaortic conus (with no subpulmonary conal free wall)
in 88.2%;
2. a bilateral (subaortic and subpulmonary) conus in 6.7%;
3. a subpulmonary conus (with no or minimal subaortic
conus) in 3.4%; and
4. a bilateral absent conus (neither subaortic nor subpulmon-
ary) in 1.7%.
We think that semilunar-AV fibrous continuity or disconti-
nuity results from the resorption or lack of resorption of the
subsemilunar conal free walls, respectively (Figure 3).
The conal development hypothesis, ‘‘development’’ includ-
ing both subsemilunar conal free wall growth and resorption,
appears able to explain all of the above-mentioned anatomical
types of conus associated with normally and abnormally related
great arteries (Figures 1-5).
What do we still not understand concerning normally and
abnormally related great arteries? Again, the answer is much.
The development (growth and resorption) of the subsemilunar
conal free walls is not the whole story. For example, why do the
ventricles loop in one direction, while the infundibuloarterial
segment (the conotruncus) twists in the opposite direction,
resulting, admittedly rarely, in ACM (Figure 1, row 6)? At
present, we do not know.
One of our next great challenges will be to gain a much bet-
ter understanding of the molecular genetic abnormalities and
Van Praagh 381
381 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

perhaps the environmental factors that control or influence the
development of the subsemilunar conal free walls that we have
been focusing on. This type of etiological understanding may
make possible the prediction and prevention of abnormally
related great arteries.
From a currently practical diagnostic and surgical perspec-
tive, in view of its great anatomical and developmental signif-
icance, the state of the subsemilunar conus arteriosus should be
described routinely in diagnostic imaging studies and reports
and in surgical operative notes. We need to start to understand
the subsemilunar conus arteriosus. We need to learn that the
subarterial conus is really not part of the right ventricle.
We need to understand that abnormally related great arteries
are abnormally connected great arteries; that the subsemilunar
conus is how the great arteries connect with the underlying ven-
tricles, ventricular septum, and AV valves; and that if the conal
connector has developed abnormally, the VA alignments and
other spatial relationships involving the great arteries will also
be abnormal.
Evolution and the Great Arteries
Thus far, we have considered normally and abnormally related
great arteries in terms of their normal and pathological anatomy
and embryology (ontogeny). We have barely mentioned the
probably great importance of vertebrate evolution (phylo-
geny).16 Pathological anatomy is important because it makes
possible accurate diagnosis and successful surgery; embryol-
ogy is important because it makes possible the understanding
of pathological anatomy; and evolution is important because
it makes possible the understanding of embryology.
The right ventricle (Figure 4A) is our major cardiovascular
adaptation to air breathing and land living.16 The subsemilunar
part of the conus arteriosus (Figure 4A, component 4), espe-
cially the subsemilunar conal free walls (Figure 3), normally
crosses the systemic venous and pulmonary venous circulations
by performing an embryonic aortic switch by a simultaneous
combination of subpulmonary conal free wall growth and sub-
aortic conal free wall resorption. The right ventricular sinus
(Figure 4A, component 2) evolved by evaginating or pouching
out beneath the proximal or apical portion of the conus arterio-
sus, the septal band (Figure 4A, component 3); thus, the right
ventricular sinus became the lung pump.
Who discovered evolution?16 Was it really Darwin and
Wallace, as is usually said? Fascinating to relate, the answer
is no. Evolution was in fact discovered by Empedocles, a
brilliant pre-Socratic physicist who lived from 495 to 435 BC
in Acragas (now Agrigento) in Sicily, which at that time was
part of Magna Graecia (Great Greece). Evolution may have
been understood even earlier by the Syrian brothers, who,
because of skeletal similarities, worshipped fish as the ancestor
of man. But Empedocles realized not only the existence of
evolution but how it works: by the chance occurrence of
favorable changes that then persist. Some 2300 years later, this
is what Darwin called natural selection (in 1859) and that
somewhat later Herbert Spencer termed survival of the fittest.
Homo sapiens sapiens, our modest scientific name for our-
selves (meaning ‘‘man wise wise’’), belongs to the phylum
Chordata, which includes all animals with a notochord (back
cord, Greek). The notochord early marks the long axis of the
embryo, indicating where the brain and the vertebrae will
later develop. The chordates are synonymous with the
vertebrates.
Phylogeny16
From an evolutionary (phylogenetic) standpoint, our remote
ancestors were the ancient fish of the Ordovician period and the
upper Devonian period, 500 million to 345 million years ago. In
craniate vertebrates, the heart began as a specialized part of the
primary longitudinal ventral blood vessel that pumped venous
blood from the ducts of Cuvier and the hepatic veins forward and
upward through the gills, where oxygenation took place. As long
as our vertebrate ancestors ‘‘breathed’’ water, there was a single
systemic circulation and no need for lungs or a right ventricle.
However, about 325 million years ago in the early Carboni-
ferous period, amphibians evolved. These animals evolved
lungs and so could breathe air, but they still had to breed in the
water like modern frogs. From these primitive amphibians, not
only modern amphibians evolved but also fully terrestrial ani-
mals that did not need to breed in the water. These were the
Amniota, all animals with an amniotic sac. The amniotic sac
surrounds a ‘‘mare internum’’ (internal sea) of amniotic fluid
in which the embryo and later the fetus floats, like our aquatic
vertebrate ancestors. The terrestrial Amniota then evolved into
reptiles, birds (feathered reptiles), and mammals (furry or hairy
reptiles). Mammals evolved during the Jurassic period, some
180 million years ago, when reptiles, including the giant dino-
saurs, were the lords of the earth.
Although fish and amphibians do not have a right ventricle,
higher reptiles (such as crocodiles and alligators), birds, and
mammals do. The evolution of the right ventricle was part of
the development of a double circulation—pulmonary and sys-
temic—in fully terrestrial vertebrates. In aquatic and semiaqua-
tic vertebrates, there is only a single circulation, the systemic,
that also supplies the organs of respiration (gills, lungs, and
skin).
But why is the right ventricle the right-sided ventricle?
Because D-loop formation (Figures 2 and 3), which is normal
in higher vertebrates, places the conus arteriosus, from which
the right ventricular sinus develops, to the right of the ventricle
of the bulboventricular loop, which therefore becomes the left-
sided ventricle and remains the systemic pump.
Ontogeny16
From the embryological (ontogenetic) standpoint, the salient
stages of normal human cardiogenesis are as follows:
1. The cardiogenic crescent of the precardiac mesoderm
occurs from 16 to 20 days following ovulation.
382 World Journal for Pediatric and Congenital Heart Surgery 1(3)
382 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

2. The straight tube or preloop stage follows from 20 to 22
days of age (Figure 2).
3. D-loop formation then occurs from 22 to 24 days of age
(Figure 2). This is when the human heart beat is thought
to begin. There is a single, in-series circulation, reminis-
cent of the circulation of a fish: from right atrium, to left
atrium, to future left ventricle, to future right ventricle,
to future great arteries. Left-sided juxtaposition of the
atrial appendages is present. The developing ventricular
apex points to the right; that is, dextrocardia is present. The
circulation resembles that in tricuspid atresia and in
double-inlet or common-inlet left ventricle. Both develop-
ing great arteries are above the future right ventricular
sinus; that is, DORV is potentially present. The aortic
switch process has not as yet occurred.
4. By 26 to 28 days of age in utero, both ventricular sinuses
are beginning to evaginate or pouch out from the greater
curvature of the bulboventricular D-loop. The left ventri-
cular sinus develops faster than the right ventricular sinus.
The right ventricular sinus is still somewhat posterior to
the left ventricular sinus because the developing ventricu-
lar apex is still pointing rightward. The right atrial appen-
dage is starting to bulge out to the right of the great arterial
outflow tracts; that is, left-sided juxtaposition of the atrial
appendages is beginning to be ‘‘cured.’’
5. By 30 to 32 days of age, much more evagination or out-
pouching of both the ventricular sinuses has occurred.
Although the right ventricular sinus is still smaller than the
left ventricular sinus, the growth of the right ventricular
sinus is catching up to that of the left ventricular sinus. The
ventricles are swinging horizontally leftward so that the
developing ventricular septum now occupies an approxi-
mately sagittal plane; that is, mesocardia is now present.
Left-sided juxtaposition of the atrial appendages has now
completely disappeared because the right atrial appendage
now lies entirely to the right of the great arterial outflow
tracts.
6. By 32 to 34 days of age, the ostium primum has almost
been closed by growth of the endocardial cushions of the
AV canal. The ostium primum normally is closed com-
pletely between 34 and 36 days of age. The tricuspid valve
is now opening into the right ventricle. The right ventricu-
lar sinus is now almost as large as the left ventricular sinus.
But mesocardia is still present.
7. By 38 to 40 days of age in utero, the ventricular apex nor-
mally points leftward; that is, levocardia has been
achieved. The right ventricular sinus is now as large as the
left ventricular sinus. The normal aortic switch procedure
has been performed developmentally (as described hereto-
fore). Cardiac morphogenesis normally is now largely
complete, except that the interventricular foramen (the
VSD) is still open.
8. Between days 38 to 45, the interventricular foramen nor-
mally is closed at its rightmost end, adjacent to the tricus-
pid valve. However, the interventricular foramen can
remain patent until after birth. Postnatal closure of the
membranous septum is so-called spontaneous closure, if
it occurs without interventional or surgical assistance. The
membranous septum is superior endocardial cushion tissue
of the AV canal that is intimately related to the tricuspid
valve (between the anterior and septal leaflets) and is also
closely related to the recently switched aortic valve
(beneath the right coronary-noncoronary commissure of
the normally located aortic valve).
As was stated by Ernst Haeckel of Jena (1834-1919) in his
biogenic law, the developmental history of the individual (onto-
geny or embryology) does tend to recapitulate the developmen-
tal history of our phylum Chordata (phylogeny or evolution).
Thus, the approximately 29-day history of human cardiac devel-
opment, from day 16 when the cardiogenic crescent is appearing
to day 45 when the interventricular foramen usually is closing,
does indeed recapitulate or summarize the 500 million–year
cardiovascular history of our phylum Chordata. The genes, with
their many favorable mutations, have an amazingly long and
accurate ‘‘memory.’’
But our genetic ‘‘memory’’ is far from perfect because of
mutations (copying errors). Now, have another look at Figure 1,
which documents many, but not all, of the unsuccessful ways in
which the embryonic aortic switch procedure can be per-
formed. This is what abnormally related great arteries really
are: unsuccessful attempts to perform the embryonic aortic
switch from the developing right to the developing left
ventricle.
Phylogeny and Ontogeny of Congenital Heart Disease16
Examining the normal morphologically right ventricle (Figure
4A) and solitus normally related great arteries (Figure 2), many
well-informed observers may not realize that they are looking
at the cardiovascular adaptations that made possible air breath-
ing and permanent land living for vertebrates, including mam-
mals such as ourselves. Just imagine that! The evolution
(phylogeny) and the embryology (ontology) of the right ventri-
cle (both parts of the conus arteriosus) and the great arteries
made possible ‘‘everything’’ for Homo sapiens sapiens—our
terrestrial prehistory, history, culture, and science.
In our phylum Chordata, the morphologically left ventricle
is the ancient professional pump. It is at least 500 million years
old and is seldom involved in primary malformation. By con-
trast, the right ventricle, including its 4 component parts (Fig-
ure 4A), is a ‘‘Johnny-come-lately,’’ a relative newcomer, only
about 180 million years old. The right ventricle is only about
36% as old as the left ventricle. Or, to say it another way, the
right ventricle is 64% younger than the left ventricle. As pedia-
tric cardiologists and congenital heart surgeons know, the right
ventricle is much more prone to malformation than is the left
ventricle. Congenital heart disease, that is, the structural heart
disease that one can be born with, is composed almost entirely
of right ventricular anomalies (congenital, from Latin congeni-
tus, born together with: com-, together þ genitus, born, past
participle of gignere, to beget).
Van Praagh 383
383 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

Consequently, we are still experiencing serious problems
with the phylogenetically younger part of our cardiovascular
system, that is, with the lung pump, the aortic switch, and the
septation mechanisms, examples of which follow: tricuspid
atresia; congenitally unguarded tricuspid orifice (ie, absence
of tricuspid leaflets, but with a patent tricuspid orifice); com-
mon AV canal (with or without common AV valve, with or
without AV septal defect); absence of the right ventricular
sinus (with double-inlet or common-inlet into a single or
unpaired left ventricle, with an infundibular outlet chamber);
VSDs; Ebstein anomaly of the tricuspid valve and right ventri-
cular sinus; Uhl disease (ie, parchment right ventricle); hypo-
plasia of the right ventricle sinus (with straddling tricuspid
valve, or double-outlet right atrium, or superoinferior ventri-
cles, or with crisscross AV relations); double-chambered right
ventricle (also known as anomalous muscle bundles of the right
ventricle); TOF; truncus arteriosus; TGA (Figure 1); DORV
(Figure 1); DOLV (Figure 1); ACM (Figure 1); other rare seg-
mental anatomical sets (Figure 1) such as situs inversus totalis
{I,L,I}, ventricular inversion with inverted normally great
arteries in visceroatrial situs solitus {S,L,I}, isolated ventricu-
lar inversion {S,L,S}, isolated ventricular noninversion
{I,D,I}, and isolated infundibuloarterial inversion {S,D,I} with
or without TOF; and AP septal defect (also known as AP
window).
The foregoing list is not complete but does indicate the mag-
nitude of the problem posed by malformations of the right ven-
tricle and its 4 component parts, the phylogenetically ‘‘recent’’
part of the human cardiovascular system. Primary anomalies of
the great arteries themselves, such as AP window, are relatively
rare. So, too, are primary anomalies of our ancient systemic
pump, the left ventricle.
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the
authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or
authorship of this article.
References
1. Van Praagh R, Layton WM, Van Praagh S. The morphogenesis of
normal and abnormal relationships between the great arteries and
the ventricles: pathologic and experimental data. In: Van
Praagh R, Takao A, eds. Etiology and Morphogenesis of Conge-
nital Heart Disease. Mt Kisco, New York: Futura Publishing Co
Inc; 1980:271-316.
2. Van Praagh R. Segmental anatomy. In: Selke FW, del Nido PJ,
Swanson SJ, eds. Sabiston & Spencer Surgery of the Chest. 8th
ed. Philadelphia: Saunders Elsevier; 2010:1651-1664.
3. Van Praagh R. What is the Taussig-Bing malformation? Circula-
tion. 1968;38:445-449.
4. Van Praagh R, Weinberg PM, Smith SD, Foran RB, Van Praagh S.
Malpositions of the heart. In: Adams FH, Emmanouilides GC,
Riemenschneider TA, eds. Moss’ Heart Disease in Infants,
Children, and Adolescents. 4th ed. Baltimore: Williams & Wilkins;
1968:530-580.
5. Quain R. Cited by: Peacock TB. On Malformations, Etc of
the Human Heart With Original Cases. London: Churchill;
1856: 116. Birmingham, Alabama: Gryphon Editions Lim-
ited; 1981.
6. Van Praagh R. Transposition of the great arteries: history, patho-
logic anatomy, embryology, etiology, and surgical considerations.
Cardiac Surgery: State of the Art Reviews. Philadelphia: Hanley
& Belfus Inc; 1991:7-82.
7. Van Praagh R, Vlad P, Keith JD. Complete transposition of the
great arteries. In: Keith JD, Rowe RD, Vlad P, eds. Heart Disease
in Infancy and Childhood. 2nd ed. New York: Macmillan Publish-
ing Co; 1967:682-744.
8. Van Praagh R, Van Praagh S. Isolated ventricular inversion:
a consideration of the morphogenesis, definition, and diagnosis
of nontransposed and transposed great arteries. Am J Cardiol.
1966;17:395-406.
9. Van Praagh R, Van Praagh S. Anatomically corrected transposi-
tion of the great arteries. Br Heart J. 1967;29:112-119.
10. Van Praagh R, Durnin RE, Jockin H, et al. Anatomically corrected
malposition of the great arteries {S,D,L}. Circulation.
1975;51:20-31.
11. Van Praagh R, Weinberg PM. Double-outlet left ventricle. In:
Adams FH, Emmanouilides GC, eds. Moss’ Heart Disease in
Infants, Children, and Adolescents. 3rd ed. Baltimore: Williams
& Wilkins; 1983:370-385.
12. Van Praagh R, Van Praagh S, Nebesar RA, Muster AJ,
Sinha SN, Paul MH. Tetralogy of Fallot: underdevelopment
of the pulmonary infundibulum and its sequelae. Report of a
case with cor triatriatum and pulmonary sequestration. Am J
Cardiol. 1970;26:25-33.
13. Van Praagh R, Van Praagh S. The anatomy of common aortico-
pulmonary trunk (truncus arteriosus communis) and its embryolo-
gic implications: a study of 57 necropsied cases. Am J Cardiol.
1965;16:406-425.
14. Van Praagh R, Van Praagh S. Morphologic anatomy. In:
Fyler DC, ed. Nadas’ Pediatric Cardiology. Philadelphia: Hanley
& Belfus Inc Philidelphia and St Louis: Mosby Year Book Inc;
1992:17-26.
15. Van Praagh R, Geva T, Kreutzer J. Ventricular septal defects: how
shall we describe, name and classify them? J Am Coll Cardiol.
1989;14:1298-1299.
16. Van Praagh R. The evolution of the right ventricle and its relation
to the surgical management of congenital heart disease. Rev
Argentina Cardiol. 1995;63:417-434.
17. Van Praagh R, Ongley PA, Swan HJC. Anatomic types of single
or common ventricle in man: morphologic and geometric aspects
of 60 necropsied cases. Am J Cardiol. 1964;13:367-386.
18. Van Praagh R, Plett JA, Van Praagh S. Single ventricle: pathol-
ogy, embryology, terminology, and classification. Herz. 1979;
4:113-150.
19. Paul MH, Muster AJ, Sinha SN, Cole RB, Van Praagh R. Double-
outlet left ventricle with an intact ventricular septum: clinical and
autopsy diagnosis and developmental implications. Circulation.
1970;41:129-139.
384 World Journal for Pediatric and Congenital Heart Surgery 1(3)
384 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from

20. Van Praagh R, Matsuoka R, Van Praagh S. Anatomic variations in
truncus arteriosus. In: Takahashi M, Wells WJ, Lindesmith GG,
eds. Challenges in the Treatment of Congenital Cardiac Anoma-
lies. Mt Kisco, New York: Futura Publishing Co; 1986:199-211.
21. Vizcaino A, Campbell J, Litovsky S, Van Praagh R. Single origin
of right and left pulmonary artery branches from ascending aorta
with nonbranching main pulmonary artery: relevance to a new
understanding of truncus arteriosus. Pediatr Cardiol. 2002;
23:230-234.
22. Van Praagh R, Papagiannis J, Grunenfelder J, Bartram U,
Martanovic P. Pathologic anatomy of corrected transposition of
the great arteries: medical and surgical implications. Am Heart
J. 1998;135:772-785.
23. Keith A. The Hunterian lectures on malformations of the heart.
Lancet. 1909;2:433-435.
24. Foran RB, Belcourt C, Nanton MA, et al. Isolated infundibuloar-
terial inversion {S,D,I}: a newly recognized form of congenital
heart disease. Am Heart J. 1988;116:1337-1350.
25. Van Praagh R. The importance of segmental situs in complex
congenital heart disease. Seminars in Roentgenol. 1985;20:
254-271.
26. Pasquini L, Sanders SP, Parness IA, et al. Conal anatomy in 119
patients with D-loop transposition of the great arteries with
ventricular septal defect: an echocardiographic and pathologic
study. J Am Coll Cardiol. 1993;21:1712-1721.
27. Van Praagh R, Weinberg PM, Srebro J. Double outlet left ventricle.
In: Adams FH, Emmanouilides GC, Riemenschneider TA, eds.
Moss’ Heart Disease in Infants, Children, and Adolescents. 4th
ed. Baltimore: Williams & Wilkins; 1989:461-485.
28. Van Praagh R, Van Praagh S. Morphologic anatomy. In:
Keane JF, Lock JE, Fyler DC, eds. Nadas’ Pediatric Cardiology.
2nd ed. Philadelphia: Saunders Elsevier; 2006:27-37.
29. Spitzer A. Uber den Bauplan des normalen und missbildeten
Herzens: Versuch einer phylogenetischen Theorie. Virchows Arch
f Path Anat. 1923;243:81-201.
30. Spitzer A. The Architecture of Normal and Malformed Hearts: A
Phylogenic Theory of their Development, With a Summary and
Analysis of the Theory by M Lev and A Vass. Springfield, Illi-
nois: Charles C. Thomas; 1951.
31. Grant RP. The morphogenesis of transposition of the great ves-
sels. Circulation. 1962;26:819-840.
32. Cardell BS. Corrected transposition of the great vessels. Br Heart
J. 1956;18:186-192.
33. Harris JS, Farber S. Transposition of the great cardiac vessels with
special reference to the phylogenetic theory of Spitzer. Arch
Pathol. 1939;28:427-502.
Van Praagh 385
385 by Jose-Antonio Quibrera on October 30, 2010pch.sagepub.comDownloaded from