World Distribution, Population Genetics, and Health Burden of the...
15
World Distribution, Population Genetics, and Health Burden of the Hemoglobinopathies Thomas N. Williams 1 and David J. Weatherall 2 1 Kenya Medical Research Institute/Wellcome Trust Programme, Centre for Geographical Research, Kilifi District Hospital, PO Box 230, Kilifi, Kenya 2 Weatherall Institute of Molecular Medicine, University of Oxford, John Radcliffe Hospital, Oxford OX39DU, United Kingdom Correspondence: twilliams@kilifi.kemri-wellcome.org Although information about the precise world distribution and frequency of the inherited hemoglobin disorders is still limited, there is no doubt that they are going to pose an increas- ing burden on global health resources in the future. Their high frequency is a reflection of natural selection combined with a high frequency of consanguineous marriages in many countries, together with an epidemiological transition; whereby, as public health measures improve in the poorer countries of the world, more babies with these disorders are surviving to present for treatment. T he inherited disorders of hemoglobin are by far the most common monogenic diseases. Recent surveys suggest that between 300,000 and 400,000 babies are born with a serious he- moglobin disorder each year and that up to 90% of these births occur in low- or middle-income countries (Christianson et al. 2006). Here we will discuss the world distribution of these con- ditions and what is known about the mecha- nisms that have led to their extremely high fre- quency in many tropical countries. DISTRIBUTION AND FREQUENCY OF THE HEMOGLOBIN DISORDERS An estimate of the annual births of the important hemoglobin disorders is shown in Table 1. These figures are only a very approximate assessment and are based, in many cases, on only relatively small samples from localized regions of different countries. It has been found recently that the distribution of all the important hemoglobin disorders is extremely heterogeneous within different countries, even within small geograph- ical distances (Weatherall 2010). Hence, a great deal more work needs to be done to provide anything like an accurate estimate of their true frequency. Maps showing the world distribution of the sickle cell disorders, hemoglobin (Hb)E and the different forms of thalassemia are shown in Fig- ures 1 and 2. Sickle cell anemia occurs through- out sub-Saharan Africa and in small pockets in the Mediterranean region, the Middle East, and the Indian subcontinent. By the use of haplo- type analysis, that is the pattern of single nucle- otide polymorphisms in the b-globin gene clus- ter, it has been determined that the sickle cell Editors: David Weatherall, Alan N. Schechter, and David G. Nathan Additional Perspectives on Hemoglobin and Its Diseases available at www.perspectivesinmedicine.org Copyright # 2012 Cold Spring Harbor Laboratory Press; all rights reserved; doi: 10.1101/cshperspect.a011692 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692 1 www.perspectivesinmedicine.org on January 19, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/ Downloaded from
Transcript of World Distribution, Population Genetics, and Health Burden of the...

World Distribution, Population Genetics, andHealth Burden of the Hemoglobinopathies
Thomas N. Williams1 and David J. Weatherall2
1Kenya Medical Research Institute/Wellcome Trust Programme, Centre for Geographical Research,Kilifi District Hospital, PO Box 230, Kilifi, Kenya
2Weatherall Institute of Molecular Medicine, University of Oxford, John Radcliffe Hospital,Oxford OX39DU, United Kingdom
Correspondence: [email protected]
Although information about the precise world distribution and frequency of the inheritedhemoglobin disorders is still limited, there is no doubt that they are going to pose an increas-ing burden on global health resources in the future. Their high frequency is a reflection ofnatural selection combined with a high frequency of consanguineous marriages in manycountries, together with an epidemiological transition; whereby, as public health measuresimprove in the poorer countries of the world, more babies with these disorders are survivingto present for treatment.
The inherited disorders of hemoglobin are byfar the most common monogenic diseases.
Recent surveys suggest that between 300,000and 400,000 babies are born with a serious he-moglobin disorder each year and that up to 90%of these births occur in low- or middle-incomecountries (Christianson et al. 2006). Here wewill discuss the world distribution of these con-ditions and what is known about the mecha-nisms that have led to their extremely high fre-quency in many tropical countries.
DISTRIBUTION AND FREQUENCY OFTHE HEMOGLOBIN DISORDERS
An estimate of the annual births of the importanthemoglobin disorders is shown in Table 1. Thesefigures are only a very approximate assessmentand are based, in many cases, on only relatively
small samples from localized regions of differentcountries. It has been found recently that thedistribution of all the important hemoglobindisorders is extremely heterogeneous withindifferent countries, even within small geograph-ical distances (Weatherall 2010). Hence, a greatdeal more work needs to be done to provideanything like an accurate estimate of their truefrequency.
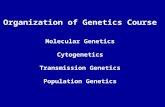
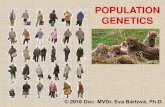
Maps showing the world distribution of thesickle cell disorders, hemoglobin (Hb)E and thedifferent forms of thalassemia are shown in Fig-ures 1 and 2. Sickle cell anemia occurs through-out sub-Saharan Africa and in small pockets inthe Mediterranean region, the Middle East, andthe Indian subcontinent. By the use of haplo-type analysis, that is the pattern of single nucle-otide polymorphisms in theb-globin gene clus-ter, it has been determined that the sickle cell
Editors: David Weatherall, Alan N. Schechter, and David G. Nathan
Additional Perspectives on Hemoglobin and Its Diseases available at www.perspectivesinmedicine.org
Copyright # 2012 Cold Spring Harbor Laboratory Press; all rights reserved; doi: 10.1101/cshperspect.a011692
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

gene arose at least twice, once in Africa and oncein India or the Middle East (Kulozik et al. 1986).Similar evidence suggests that the gene mayhave also arisen on several different occasionsin sub-Saharan Africa although these data haveto be reviewed with caution because it is possi-ble that the different haplotype patterns couldhave resulted from gene conversion events (Flintet al. 1998). Hemoglobin SC disease is morerestricted to parts of west and north Africawhereas HbS b thalassemia occurs in localizedparts of sub-Saharan Africa and sporadicallythroughout the Middle East and Indian subcon-tinent. Unlike some forms of a thalassemia andHbE, which are discussed below, the gene fre-
quency for HbS rarely rises much above 20%–25% of a particular population although thereare occasional exceptions.
Hemoglobin E, the other particularly com-mon structural hemoglobin variant, occurswidely throughout the eastern half of the Indiansubcontinent, Bangladesh, Myanmar, and eastand southeast Asia. It occurs at varying fre-quencies but in some parts of Asia, notably thenorthern parts of Thailand and Cambodia,called the “hemoglobin E triangle,” up to 70%of the population are carriers (see Fucharoenand Weatherall 2012).
The mild forms of a thalassemia (see Higgs2012), which result from a single a gene dele-tion (2a/aa), occur in a broad tropical beltstretching from sub-Saharan Africa through theMediterranean regions and Middle East to theIndian subcontinent and the whole of east andsoutheast Asia. In this band, they occur at afrequency of 10%–25%, although in a few lo-calized populations such as those of north Indiaand Papua New Guinea, they are found in up to80% of the population and the gene appears tobe going to fixation. The more severe forms of athalassemia due to loss of both a chain genes—a0 thalassemia (–/aa)—have a much more re-stricted occurrence, reaching high frequencies
HbE HbS
Figure 1. The world distribution of the origins of hemoglobin S and hemoglobin E. (From Weatherall and Clegg2001; reprinted, with permission, from the author.)
Table 1. A breakdown of the annual number of birthswith the different hemoglobin disorders
Annual births with major hemoglobin disorders
b-thalassemia major 22,989HbE b thalassemia 19,128HbH disease 9568Hb Bart’s hydrops (a0/a0) 5183SS disease 217,331S b thalassemia 11,074SC disease 54,736
From available data (Modell and Darlison 2008; Weathe-
rall 2010).
T.N. Williams and D.J. Weatherall
2 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

only in southeast Asia and in some of theMediterranean islands. They occur sporadicallythroughout other populations, however, al-though their true frequency has not been deter-mined.
Although the hemoglobinopathies all occurat particularly high frequencies in these tropicalregions, they have been transported to mostcountries of the world by population migra-tions over many years. For example, the sicklecell gene is extremely common in many of theCaribbean Islands and in parts of North Amer-ica, and occurs in most countries to a varyingdegree. The same phenomenon has occurred inthe case of all the common forms of thalasse-mia. Interestingly, there are no common hemo-globin disorders among the American Indianpopulation, probably because these conditionswere not established in Asia at the time of the
early population movements across the BeringStrait.
WHY ARE THE INHERITED DISORDERSOF HEMOGLOBIN SO COMMON?
There are several reasons why the hemoglobindisorders have reached such extraordinarilyhigh gene frequencies in many tropical coun-tries. First and foremost, it appears that theirfrequency reflects natural selection through pro-tection of heterozygotes against severe malaria,a mechanism first suggested by Haldane (1949)and later confirmed independently in the caseof sickle cell anemia by Allison (1954a,b,c). Wewill consider the possible mechanisms later inthis work.
Natural selection is not the only mecha-nism involved in maintaining these high gene
α and β thalassemia
Figure 2. The world distribution of the origins of the a and b thalassemias. (From Weatherall and Clegg 2001;reprinted, with permission, from the author.)
Epidemiology of the Hemoglobinopathies
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

frequencies. Another important factor is the rel-atively high frequency of consanguineous mar-riages in many of the high frequency countries;this mechanism has an important effect on in-creasing the gene frequency of any recessivelyinherited disorder. Although accurate data onthe frequency of consanguineous marriage arelacking, there is no doubt from such that areavailable that this is an important factor in help-ing to maintain the global health problem posedby these conditions. Another important factoris the epidemiological transition, whereby aspublic health and nutritional standards improvein the poorer countries, babies with these con-ditions who would otherwise have died in earlylife are now living long enough to present fordiagnosis and management. As evidenced bywhat happened in Cyprus after it went throughthis transition after the Second World War, thereis no doubt that this mechanism will cause amajor increase in the number of patients withthe more severe hemoglobin disorders in the fu-ture (Weatherall and Clegg 2001). Finally, thevarying distribution of some of the hemoglobindisorders in different populations reflects strongfounder effects by their original inhabitants.This mechanism is clearly illustrated in someof the Pacific Island populations (O’Shaugh-nessy et al. 1990).
It should be emphasized that even if some ofthe selective factors are reduced—the eradica-tion of malaria, for example—it will take manygenerations before the frequency of these dis-eases starts to decline; a period during whichthere will be a tendency for their increase be-cause of the epidemiological transition outlinedabove.
NATURAL SELECTION AND THEHEMOGLOBIN DISORDERS
During the six decades since Haldane first pro-posed the malaria hypothesis (Haldane 1949),evidence has steadily grown to confirm that ma-laria is indeed the primary force behind the highfrequency of inherited hemoglobin disordersthat is seen in many tropical and subtropicalpopulations. The evidence supporting this as-sertion comes from four main sources: the sim-
ilarity between the distributions of malaria andspecific hemoglobin disorders at local, regional,and global scales; from population genetic pre-dictions of their historic age; from clinical stud-ies conducted in malaria-endemic areas; andfrom mechanistic studies conducted both in-vi-tro and ex-vivo. Although such evidence isstrongest for HbS and for the a thalassemias,which have been the focus of the most research,there can now be little doubt that malaria is re-sponsible for the current distributions of all themajor hemoglobin disorders. In the followingsections we will review the evidence as it standsfor each hemoglobin disorder individually. Theproposed mechanisms for malaria protection bythese conditions are summarized in Table 2.However, later in this work we will also discussemerging data that suggest that selection for he-moglobin disorders may be competitive, andmight be influenced by negative effects wheninherited in combination with one another.
Hemoglobin S
The heterozygous state for hemoglobin S (HbAS)is the best described of all malaria-protectivetraits and is used as the classic example ofbalanced polymorphism in schools and col-leges throughout the world. The close resem-blance between the geographic distribution ofHbAS and that of malaria, documented by anumber of different investigators more than 60years ago (Beet 1946, 1947; Brain 1952; Foy et al.1952, 1954), gave the first clues. But it is Allisonwho first articulated the malaria hypothesiswith regard to HbS most definitively (Allison1954a,b,c). Not only, as others before him(Beet 1946, 1947; Brain 1952), did he note that“sicklers” were significantly less likely than“non-sicklers” to carry malaria parasites underconditions of natural exposure but he also show-ed that, when inoculated intravenously withlarge volumesofparasite-infectedblood, sicklerswere less likely to develop a clinical malaria in-fection. Many studies have since been conductedthat put the malaria hypothesis with regard toHbS beyond reasonable doubt. First, the closecorrespondence between the frequencies of thebs allele and the historic prevalence of malaria
T.N. Williams and D.J. Weatherall
4 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

has been confirmed through a growing numberof surveys at both the local (Enevold et al. 2007)and global scales (Livingstone 1973, 1985; Cav-alli-Sforza et al. 1994). Recently, this relation-ship has been quantified statistically, an analysisthat found strong geographical support for the
malaria hypothesis in Africa but not in eitherthe Americas or in Asia (Piel et al. 2010). He-moglobin S is absent from indigenous popula-tions in the Americas, probably because malariadid not reach the continent until relatively re-cently, whereas in Asia it follows a rather
Table 2. Summary of some proposed mechanisms of action of the malaria-resistance polymorphisms involvingthe inherited hemoglobin disorders
Hemoglobin
disorder
Potential mechanisms for
malaria protection Key references
Sickle cell trait(HbAS)
Impairment of P. falciparum red cellinvasion and growth under conditions oflow oxygen tension
Friedman 1978; Pasvol et al. 1978; Friedmanet al. 1979
Enhanced removal of parasite-infectedHbAS red blood cells
Luzzatto et al. 1970; Friedman 1978; Rothet al. 1978; Shear et al. 1993; Ayi et al. 2004
Reduced pathogenicity of P. falciparuminfected red blood cells because ofreduced expression of PfEMP1
Cholera et al. 2008; Cyrklaff et al. 2011
Improved acquisition of malaria-specificimmunity
Edozien et al. 1960; Cornille-Brogger et al.1979; Guggenmoos-Holzmann et al.1981; Marsh et al. 1989; Bayoumi et al.1990; Abu-Zeid et al. 1992; Odegbemiand Williams 1995; Le Hesran et al. 1999;Cabrera et al. 2005; Williams et al. 2005a;Verra et al. 2007b
Hemoglobin C(HbAC andHbCC)
Impairment of P. falciparum red cellinvasion and growth under conditions oflow oxygen tension
Friedman et al. 1979; Pasvol and Wilson1982; Olson and Nagel 1986; Fairhurstet al. 2003
Improved acquisition of malaria-specificimmunity
Ringelhann et al. 1976; Verra et al. 2007b
Reduced pathogenicity of P. falciparuminfected red blood cells because ofreduced expression of PfEMP1
Fairhurst et al. 2005; Brittain et al. 2007;Cyrklaff et al. 2011
Hemoglobin E(HbAE andHbEE)
Impairment of P. falciparum red cellinvasion and growth
Chotivanich et al. 2002
a thalassemia Specific protection against malaria-inducedanaemia
Allen et al. 1997; Williams et al. 2005d;Wambua et al. 2006; May et al. 2007;Fowkes et al. 2008; Veenemans et al. 2008
Reduced pathogenicity through reducedcytoadherence or rosetting
Udomsangpetch et al. 1993; Carlson et al.1994; Cockburn et al. 2004
Immuological priming through cross-species immunity between P. vivaxand P. falciparum
Williams et al. 1996; Veenemans et al. 2011
b thalassemia Enhanced removal of parasite-infectedred blood cells
Ayi et al. 2004
Reduced invasion and growth ofP. falciparum parasites
Kaminsky et al. 1986; Senok et al. 1997
Reduced pathogenicity through reducedcytoadherence or rosetting
Udomsangpetch et al. 1993; Carlson et al.1994
Epidemiology of the Hemoglobinopathies
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

restricted distribution, being confined to a smallnumber of tribal populations in India (Piel et al.2010).
Direct clinical support for a protective ef-fect of HbAS has been provided by case con-trol, cohort, and family-based association stud-ies conducted in multiple populations over thelast 30 years (for summary, see Williams et al.2005b; Jallow et al. 2009). In general, such stud-ies have shown that HbAS is �50% protectiveagainst uncomplicated and .80% protectiveagainst severe P. falciparum malaria. Althoughfew individual studies have been powered todetect an effect on malaria-specific mortality,HbAS was associated with 55% protectionagainst all-cause mortality in children 6–16months old in a single cohort study conductedin Western Kenya (Aidoo et al. 2002). Intrigu-ingly, HbAS has also been associated with pro-tection against invasive bacterial infectionsin two studies conducted in different parts ofAfrica (Eeckels et al. 1967; Scott et al. 2011).This observation appears to be explained bythe protective effect of HbAS against malariaand provides evidence for a causal associationbetween malaria and bacterial infections, indi-cating that in malaria-endemic environments,genetic factors like HbAS may confer an addi-tional benefit of protection against death frombacterial diseases (Scott et al. 2011). Recently,Gouagna and colleagues working in BurkinaFaso, made an additional intriguing observationregarding the malaria-protective effect of HbS(Gouagna et al. 2010). Although HbAS protectsagainst clinical malaria infections, parasite-in-fected blood from HbAS subjects is several timesmore infectious to the Anopheles vector thanthat of normal subjects (Gouagna et al. 2010).This observation, which is echoed by a similarobservation from Senegal (Lawaly et al. 2010),suggests that the personal advantage of HbAS isnot only balanced by the cost of potential homo-zygosity in offspring but also by that of increasedmalaria transmission to the general population.
Whereas the malaria-protective effect ofHbAS is clear, the effect of the homozygousstate, HbSS, on malaria risk is more controver-sial. Biologically, there are hypothetical reasonswhy subjects with HbSS might either enjoy a
greater degree of protection than those withHbAS or, conversely, might be at more increasedrisk than normal subjects (Williams and Obaro2011). Few controlled studies of this questionhave been reported but the balance of evidencesuggests that both scenarios might be true. Sub-jects with HbSS appear to be less susceptiblethan normals to developing malaria infections(Makani et al. 2010; McAuley et al. 2010) butare highly susceptible to the catastrophic conse-quences of malaria, particularly severe anemia,if they do become infected with the disease (Ma-kani et al. 2010; McAuley et al. 2010; Williamsand Obaro 2011). The net result is that malariais almost certainly a major cause of prematuremortality in children born with HbSS in malar-ia-endemic areas and that the early detection ofHbSS in association with active malaria preven-tion could have a major impact on survival (Ser-jeant 2005).
The Mechanism of Malaria ProtectionAfforded by HbAS
Although the fact that HbAS confers malariaprotection is now well established, the mecha-nism by which it does so remains a matter ofsome speculation. Through early studies, con-ducted soon after it became possible to growmalaria parasites in culture, investigators con-verged on the general hypothesis that protectionresulted from impairment in the invasion andgrowth of P. falciparum parasites into HbAS redcells under conditions of low oxygen tensionthat were physiologically representative of invivo conditions (Friedman 1978; Pasvol et al.1978; Friedman et al. 1979). However, a numberof alternative hypotheses have subsequently de-veloped. Several investigators have suggestedthat the mechanism may relate to the enhancedremoval of parasite-infected HbAS red bloodcells. Some have proposed that this may relateto the fact that such cells sickle under low oxy-gen tension (Luzzatto et al. 1970; Friedman1978; Roth et al. 1978) and that this leads totheir premature destruction in the spleen(Friedman 1978; Shear et al. 1993), whereasAyi and colleagues have proposed a mechanismthat is generic to a number of red cell disorders
T.N. Williams and D.J. Weatherall
6 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

and involves the enhanced opsonization of redcells infected with ring-stage parasites through aprocess that involves increased oxidative stress(Ayi et al. 2004).
An alternative hypothesis has emerged morerecently. Cholera and colleagues have shown thatin vitro, relative to parasitized normal HbAA redblood cells, the binding of parasitized HbAS redblood cells to both microvascular endothelialcells and to blood monocytes was significantlyreduced and that this correlated with altered sur-face display of the parasite-encoded proteinP. falciparum Erythrocyte Protein-1 (PfEMP1)(Cholera et al. 2008). Because the PfEMP1-me-diated sequestration of mature parasites inthe post-capillary venules of critical tissuessuch as the brain have been implicated in boththe pathogenesis of severe malaria and the eva-sion of parasite-infected red cells from immuneclearance by the spleen, this provides an attrac-tive explanation for the protective effect ofHbAS. Very recently, Cyrklaff and colleagueshave elaborated on this hypothesis by showing,again in vitro, that HbAS affects the traffickingsystem that directs PfEMP1 to the surface of in-fected erythrocytes. Using cryo-electron tomog-raphy they showed that within the cytoplasm ofnormal red blood cells the parasite proteins aretransported to the surface via a parasite-gener-ated host-derived actin cytoskeleton but that he-moglobin oxidation products disrupted thisprocess in HbAS red cells (Cyrklaff et al. 2011).
Whereas all the hypotheses discussed so farimply that HbAS protects against malaria en-tirely through innate mechanisms, data fromboth epidemiological and clinical studies sug-gest that this may not be the entire story. Theprotective effect of HbAS in naturally exposedpopulations increases with age (Cornille-Brog-ger et al. 1979; Guggenmoos-Holzmann etal. 1981; Le Hesran et al. 1999; Williams et al.2005a), indicating that the mechanism mightnot be entirely innate but might also includean acquired, immunological component. Thishypothesis is supported by a number of studiesthat have reported enhanced malaria-specificimmune responses in HbAS individuals (Edo-zien et al. 1960; Marsh et al. 1989; Bayoumi etal. 1990; Abu-Zeid et al. 1992; Odegbemi and
Williams 1995; Cabrera et al. 2005; Verra et al.2007a), and potentially by recent studies using amouse model that suggest an immuno-modula-tory mechanism mediated through hemoxygen-ase-1 (Ferreira et al. 2011). However, the mousemodel of the sickling disorders is metabolicallyvery different to the human sickle-cell traits.Furthermore, whereas such studies appear tosupport an immune component to the malariaprotective effects of HbAS they are balancedby others that show no apparent differences be-tween HbAS and normal subjects with regard toa range of immunological responses (Cornille-Brogger et al. 1979; Storey et al. 1979; Le Hesranet al. 1999; Tan et al. 2011), leaving the balancebetween innate and acquired mechanisms unre-solved.
From the above discussion, it is clear thatHbAS is associated with strong protectionagainst all forms of clinical P. falciparum malariabut that the mechanism for this protection re-mains somewhat speculative. Although manyplausible mechanisms have been proposed dur-ing the last 40 years, which (if any) providesthe true explanation remains unresolved. Onepossibility is that there is no single mechanismfor the protective effect of HbAS but that pro-tection results from the composite of many ofthe mechanisms described or by different mech-anisms in different populations; more work willbe required, both in vitro and ex vivo, to resolvethis question definitively.
Hemoglobin C
Fewer studies have focused on the malaria-pro-tective effects of HbC than for HbS. The geo-graphic range of HbC is considerably more lim-ited than that of HbS, being centered on Westand North-West Africa with the exception of alow-frequency corridor between West Africa andEgypt that appears to reflect patterns of humanmigration (FB Piel, AP Patil, RE Howes, et al.,unpubl.). Although historically HbC has beenrestricted to malaria-endemic communities, tothe best of our knowledge the relationship be-tween the population frequency of HbC and theendemicity of malaria has not been formallytested. Early studies investigating the association
Epidemiology of the Hemoglobinopathies
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

between HbC and clinical protection were eitherinconclusive (Thompson 1962, 1963; Gilles et al.1967; Guinet et al. 1997) or suggested only a mar-ginal effect of HbC in comparison to the markedprotection afforded by HbS (Ringelhann et al.1976). This was confirmed most recently inboth a large cross-sectional survey (Danquahet al. 2010) and in a birth cohort study (Kreuelset al. 2010), both conducted among children liv-ing in areas of high malaria transmission in Gha-na. This may well be explained by more recentstudies suggesting that protection might be spe-cific to particular categories of strictly defin-ed severe malaria (May et al. 2007) and that itis greater in homozygotes (with HbCC) thanin heterozygotes (with HbAC) (Agarwal et al.2000; Modiano et al. 2001; Mockenhaupt et al.2004a). The strongest evidence for a homozygousadvantage of HbC comes from a large case-con-trol study conducted by Modiano and colleaguesin Burkino Faso, in which they found a 29% re-duction in the risk of clinical malaria among chil-dren with HbAC compared to a 93% reductionamong children with HbCC (Modiano et al.2001). Finally, like HbS, it appears that HbC hasa marked effect on the transmissibility of malariaby the Anopheles vector (Gouagna et al. 2010).
Mechanistically, similar hypotheses havebeen pursued for HbC as for HbS. As forHbAS, early studies suggested that the protectiveeffect of HbC might result from a reduced abilityof P. falciparum parasites to grow and multiply inred blood cells containing HbC (Friedman et al.1979; Pasvol and Wilson 1982; Olson and Nagel1986; Fairhurst et al. 2003). Subsequently, how-ever, it has been suggested that the mechanismmight involve an immunological component(Ringelhann et al. 1976). This is supported bythe finding of higher immune responses toPfEMP1 and various malaria antigens amongchildren expressing the HbC allele in a low trans-mission urban area of Burkina Faso (Verra et al.2007b), although no differences were found in ahigher transmission rural population in thesame study or in a more recent study conductedin Mali (Tan et al. 2011). As for HbAS, an alter-native hypothesis has recently been developed:that HbC exerts its protection through a specificeffect on cytoadherence, mediated by the altered
display of surface-expressed parasite proteins(Fairhurst et al. 2005; Brittain et al. 2007; Cyr-klaff et al. 2011).
Hemoglobin E
Much less is known about the effects of HbE onmalaria than for the other common structuralvariants of hemoglobin. Like most of the otherdisorders, HbE is restricted to populations thathave traditionally been endemic for malaria andthere is some evidence for a correlation betweenthe prevalence of the two conditions (Flatz et al.1965; Kar et al. 1992; Win et al. 2005). Moreover,in one Thai population, it has recently been es-timated on the basis of genetic linkage analysisthat the most frequent variant, HbE b26 Glu !lys, has reached its current frequency in ,5000years, a period compatible with the malaria hy-pothesis (Ohashi et al. 2004). Nevertheless, fewclinical studies have reported the relative risk ofclinical malaria in subjects with HbE. In onesuch study, conducted in adults with malariawho were admitted to the hospital in Thailand,the manifestations of malaria were less severe inpatients with HbE trait (HbAE) (Chotivanichet al. 2002). However, in a similar study, Oo andcolleagues found no significant relationship be-tween either HbAE or HbEE and the severityof malaria in adults admitted to the hospitalin Burma (Oo et al. 1995). Similarly, a smallrecent study found no relationship betweenHbE and the risk of cerebral malaria in Thaiadults (Naka et al. 2008). To the best of ourknowledge, the relative risk of malaria in suchsubjects has not been reported through case-control or cohort studies, although a single re-port from Sri Lanka found subjects with theclinically significant condition HbE/b thalasse-mia to be at greater risk than normals fromP. vivax malaria. This observation, which maybe explained by the rapid turnover of red cellsseen in patients with this condition—as P. vivaxfavors the youngest, most metabolically activered blood cells—suggests that patients withHbE/b thalassemia should be actively protect-ed from malaria (O’Donnell et al. 2009).
Very few studies have examined the poten-tial mechanisms by which HbE might confer
T.N. Williams and D.J. Weatherall
8 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

malaria protection. In one such study, Chotiva-nich et al. (2002) found that compared to nor-mal subjects, a smaller proportion of red cellsfrom subjects with HbAE were susceptible toinvasion by P. falciparum parasites in culture,raising the possibility that HbAE might protectagainst severe malaria by limiting the ability ofinfections to achieve high parasite densities. Thedegree to which HbE protects against differentforms of malaria and any potential mechanismsremain, therefore, a subject for further investi-gation.
THE THALASSEMIAS
There is strong evidence from population datathat malaria selection explains the current dis-tribution of the thalassemias. First, at a globalscale, both a and b thalassemia follow remark-ably similar distribution to that of malaria (Liv-ingstone 1973, 1985; Cavalli-Sforza et al. 1994),an observation that also holds true at a micro-epidemiological scale. For example, in earlystudies, Siniscalco and colleagues noted a strongcorrelation between the population prevalenceof b thalassemia and the historic incidence ofmalaria among villages in Sardinia in southernItaly (Siniscalco et al. 1961), whereas Hill andcolleagues drew similar conclusions in Melane-sia (Hill et al. 1988). Similar observations havesubsequently been made regarding the distri-bution of a thalassemia in South Asia (Modi-ano et al. 1991), Tanzania (Enevold et al. 2007),and the Pacific (Flint et al. 1986), where in somepopulations these conditions have virtuallyreached fixation (Flint et al. 1998). Second, un-like many of the other disorders of hemoglobin,the molecular defects that result in the thalasse-mias are extremely diverse (see Higgs 2012),having arisen separately and been locally ampli-fied, in multiple populations throughout themalaria-endemic regions of the world. Theone notable exception is South America, wherein evolutionary terms malaria was introducedonly relatively recently.
Despite the overwhelming epidemiologicalevidence for malaria selection, the protectiveeffect of b thalassemia has been the subject offew clinical studies. Nevertheless, in one case-
control study conducted in northern Liberia,Willcox and colleagues estimated a protectiveeffect of �50% (Willcox et al. 1983). Whereasmany more studies have recorded, the clinicalrelationship between a thalassemia and malar-ia, the results have not been entirely consistent.The incidence of uncomplicated clinical malar-ia has been lower in a thalassemic than normalsubjects in some cohort studies (Wambua et al.2006; Enevold et al. 2008), whereas in others theincidence has either been equal (Lin et al. 2010;Veenemans et al. 2011) or even higher (Williamset al. 1996; Veenemans et al. 2011). Conversely,studies focused on severe malaria have shownconsistent evidence for a strongly protectiveeffect that is generally more marked in homo-zygous than heterozygous subjects (Allen et al.1997; Mockenhaupt et al. 2004b; Williams et al.2005d; Wambua et al. 2006; May et al. 2007).Available data, therefore, provide good evidencefor a protective effect of a thalassemia againstsevere and fatal malaria, but the data on uncom-plicated malaria are somewhat perplexing. Itseems likely that these observations are point-ing to important clues about the mechanismby which a thalassemia protects against severemalaria.
Several studies suggest that, as opposed toprotecting against all forms of clinical malaria,a thalassemia might specifically protect againstthe anemia that commonly complicates infec-tions caused by P. falciparum malaria (Allenet al. 1997; Williams et al. 2005d; Wambuaet al. 2006; May et al. 2007). Furthermore, unlikeHbAS, there is little evidence that a thalassemiahas any effect at the level of malaria parasitedensity (Allen et al. 1997; Mockenhaupt et al.2004b; Migot-Nabias et al. 2006; Wambua et al.2006; Enevold et al. 2008; Veenemans et al. 2008,2011). Such clinical observations suggest thatthe mechanisms by which a thalassemia pro-tects against malaria might well be differentfrom those involved in HbAS. Two possible ex-planations for a specific effect against malaria-induced anemia have been put forward: first,that the higher red cell counts that are associatedwitha thalassemia may buffer against the devel-opment of anemia during P. falciparum infec-tions (Fowkes et al. 2008), and second, that this
Epidemiology of the Hemoglobinopathies
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

protection might be im-munologically mediat-ed (Veenemans et al. 2008). With regard to thelatter, Veenemans and colleagues found that intwo cohorts of children in East Africa, the great-est falls in hemoglobin occurred when malariaparasitemia was associated with inflammationin the form of a raise C-reactive protein concen-tration in blood and that a thalassemia wasstrongly protective against this “inflammatory”form of the disease (Veenemans et al. 2008). Afurther characteristic of a-thalassemic redblood cells may provide an alternative explana-tion. In studies conducted in Papua New Guin-ea, Cockburn and colleagues noted that the ex-pression of complement receptor-1 (CR1) isreduced on the surface of a-thalassemic redblood cells (Cockburn et al. 2004). CR1 is aligand for rosetting in which uninfected redblood cells adhere to parasite-infected red cellsin vitro (Figs. 3 and 4). Because rosetting hasbeen associated with severe forms of malaria,including severe anemia, the reduced expressionof CR1 might be relevant in the protection af-forded by a thalassemia. Finally, it is also possi-ble that immune factors might be involved. Intwo clinical studies, the incidence of uncompli-cated clinical malaria has been paradoxicallyhigher in the youngest a-thalassemic children(Williams et al. 1996; Veenemans et al. 2011),raising the possibility that a thalassemia might
be acting like a natural vaccine, boosting expo-sure and immunity to malaria during earlychildhood. As for all the hemoglobin disorders,the story is more complicated than one mighthave thought at one point.
EPISTATIC INTERACTIONS BETWEENTHE HEMOGLOBIN DISORDERS
If, as discussed above, malaria is responsible forthe Mendelian selection of many of the inherit-ed disorders of hemoglobin, a question remainsabout why they have not all become commonthroughout the whole of the malaria-endemicworld. This is a question that has been askedparticularly from the perspective of pairs of he-moglobin disorders by a number of differentinvestigators. Studies conducted both in Kenyaand in Ghana have recently shown that wheninherited alone, both HbAS and a thalassemiaare strongly protective against P. falciparum ma-laria but that the protective effects of each arelost when both conditions are inherited togeth-er (Williams et al. 2005c; May et al. 2007). Fromthe perspective of HbAS, this may be explainedby the changes in the intracellular concentrationof HbAS that accompany the coinheritance of athalassemia (Brittenham et al. 1980). This neg-ative interaction between the two malaria-protective phenotypes could well explain whyboth are held at intermediate frequencies in
Figure 3. Three-dimensional photograph of normalred cells aggregating around a malaria-infected redcell to form a rosette. (Image supplied by D.J.P. Fer-guson, Oxford University.)
Figure 4. A cross-sectional photograph of a rosette asshown in Figure 3. (Image supplied by D.J.P. Fergu-son, Oxford University.)
T.N. Williams and D.J. Weatherall
10 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

populations where both occur together (Wil-liams et al. 2005c; Hedrick 2011; Penman et al.2011). A similar hypothesis has more recentlybeen advanced to explain the relative frequen-cies of HbAS and the a and b thalassaemiaswithin the Mediterranean region (Penman etal. 2009).
CONCLUSION
There is no doubt that Haldane’s “malaria hy-pothesis” has been fully vindicated over theyears, although his suggested mechanisms formalaria protection in thalassemia carriers, thatis, the small size of their red cells, has not stoodthe test of time. Further work is still requiredtoward a better understanding of the protectivemechanisms, information which is of potentialvalue not just in the field of evolutionary biologybut also for its potential in directing approachesfor the better prevention and management ofthe different forms of malaria. Similarly, furtherwork on the remarkable epistatic interactionsbetween various malaria-protective polymor-phisms should provide invaluable informationabout the mechanisms for the distribution of thedifferent forms of inherited hemoglobin disor-ders, in particular high-frequency populations.
ACKNOWLEDGMENTS
We are extremely grateful to Liz Rose for herhelp in the preparation of this manuscript. Wealso thank D.J.P. Ferguson of Oxford Universityfor supplying the photographs shown in Figures3 and 4.
REFERENCES�Reference is also in this collection.
Abu-Zeid YA, Theander TG, Abdulhadi NH, Hviid L, SaeedBO, Jepsen S, Jensen JB, Bayoumi RA. 1992. Modulationof the cellular immune response during Plasmodium fal-ciparum infections in sickle cell trait individuals. Clin ExpImmunol 88: 112–118.
Agarwal A, Guindo A, Cissoko Y, Taylor JG, Coulibaly D,Kone A, Kayentao K, Djimde A, Plowe CV, Doumbo O,et al. 2000. Hemoglobin C associated with protectionfrom severe malaria in the Dogon of Mali, a West Africanpopulation with a low prevalence of hemoglobin S. Blood96: 2358–2363.
Aidoo M, Terlouw DJ, Kolczak MS, McElroy PD, ter KuileFO, Kariuki S, Nahlen BL, Lal AA, Udhayakumar V. 2002.Protective effects of the sickle cell gene against malariamorbidity and mortality. Lancet 359: 1311–1312.
Allen SJ, O’Donnell A, Alexander ND, Alpers MP, Peto TE,Clegg JB, Weatherall DJ. 1997. aþ-Thalassemia protectschildren against disease caused by other infections as wellas malaria. Proc Natl Acad Sci 94: 14736–14741.
Allison AC. 1954a. The distribution of the sickle-cell trait inEast Africa and elsewhere, and its apparent relationshipto the incidence of subtertian malaria. Trans R Soc TropMed Hyg 48: 312–318.
Allison AC. 1954b. Notes on sickle-cell polymorphism. AnnHum Genet 19: 39–51.
Allison AC. 1954c. Protection afforded by sickle cell traitagainst subtertian malarial infection. Br Med J 1: 290–295.
Ayi K, Turrini F, Piga A, Arese P. 2004.Enhanced phagocytosisof ring-parasitized mutant erythrocytes. A commonmechanism that may explain protection against falcipa-rum-malaria in sickle-trait andb-thalassemia-trait. Blood104: 3364–3371.
Bayoumi RA, Abu-Zeid YA, Abdulhadi NH, Saeed BO, The-ander TG, Hviid L, Ghalib HW, Nugud AH, Jepsen S,Jensen JB. 1990. Cell-mediated immune responsesto Plasmodium falciparum purified soluble antigens insickle-cell trait subjects. Immunol Lett 25: 243–249.
Beet EA. 1946. Sickle cell disease in the Balovale District ofNorthern Rhodesia. East Afr Med J 23: 75–86.
Beet EA. 1947. Sickle cell disease in northern Rhodesia. EastAfr Med J 24: 212–222.
Brain P. 1952. Sickle-cell anaemia in Africa. Br Med J 2: 880.
Brittain NJ, Erexson C, Faucette L, Ward J, Fujioka H, Well-ems TE, Fairhurst RM. 2007. Non-opsonising aggregatesof IgG and complement in haemoglobin C erythrocytes.Br J Haematol 136: 491–500.
Brittenham G, Lozoff B, Harris JW, Kan YW, Dozy AM,Nayudu NV. 1980. a globin gene number: Populationand restriction endonuclease studies. Blood 55: 706–709.
Cabrera G, Cot M, Migot-Nabias F, Kremsner PG, DeloronP, Luty AJ. 2005. The sickle cell trait is associated withenhanced immunoglobulin G antibody responses toPlasmodium falciparum variant surface antigens. J InfectDis 191: 1631–1638.
Carlson J, Nash GB, Gabutti V, al-Yaman F, Wahlgren M.1994. Natural protection against severe Plasmodium fal-ciparum malaria due to impaired rosette formation.Blood 84: 3909–3914.
Cavalli-Sforza LL, Menozzi P, Piazza A. 1994. The history andgeography of human genes. Princeton University Press,Princeton, NJ.
Cholera R, Brittain NJ, Gillrie MR, Lopera-Mesa TM, Dia-kite SA, Arie T, Krause MA, Guindo A, Tubman A, Fu-jioka H, et al. 2008. Impaired cytoadherence of Plasmo-dium falciparum-infected erythrocytes containing sicklehemoglobin. Proc Natl Acad Sci 105: 991–996.
Chotivanich K, Udomsangpetch R, Pattanapanyasat K,Chierakul W, Simpson J, Looareesuwan S, White N.2002. Hemoglobin E: A balanced polymorphism protec-tive against high parasitemias and thus severe P falcipa-rum malaria. Blood 100: 1172–1176.
Epidemiology of the Hemoglobinopathies
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

Christianson A, Howson CP, Modell B. 2006. March ofDimes global report on birth defects. March of Dimes BirthDefects Foundation, New York.
Cockburn IA, Mackinnon MJ, O’Donnell A, Allen SJ,Moulds JM, Baisor M, Bockarie M, Reeder JC, RoweJA. 2004. A human complement receptor 1 polymor-phism that reduces Plasmodium falciparum rosettingconfers protection against severe malaria. Proc NatlAcad Sci 101: 272–277.
Cornille-Brogger R, Fleming AF, Kagan I, Matsushima T,Molineaux L. 1979. Abnormal haemoglobins in the Su-dan savanna of Nigeria. II: Immunological response tomalaria in normals and subjects with sickle cell trait. AnnTrop Med Parasitol 73: 173–183.
Cyrklaff M, Sanchez CP, Kilian N, Bisseye C, Simpore J,Frischknecht F, Lanzer M. 2011. Hemoglobins S and Cinterfere with actin remodeling in Plasmodium falcipa-rum-infected erythrocytes. Science 334: 1283–1286.
Danquah I, Ziniel P, Eggelte TA, Ehrhardt S, MockenhauptFP. 2010. Influence of haemoglobins S and C on predom-inantly asymptomatic Plasmodium infections in north-ern Ghana. Trans R Soc Trop Med Hyg 104: 713–719.
Edozien JC, Boyo AE, Morley DC. 1960. The relationship ofserum g-globulin concentration to malaria and sickling.J Clin Pathol J 13: 118–123.
Eeckels R, Gatti F, Renoirte AM. 1967. Abnormal distribu-tion of haemoglobin genotypes in Negro children withsevere bacterial infections. Nature 216: 382.
Enevold A, Alifrangis M, Sanchez JJ, Carneiro I, Roper C,Borsting C, Lusingu J, Vestergaard LS, Lemnge MM,Morling N, et al. 2007. Associations between aþ-thalas-semia and Plasmodium falciparum malarial infection innortheastern Tanzania. J Infect Dis 196: 451–459.
Enevold A, Lusingu JP, Mmbando B, Alifrangis M, LemngeMM, Bygbjerg IC, Theander TG, Vestergaard LS. 2008.Reduced risk of uncomplicated malaria episodes in chil-dren withaþ-thalassemia in northeastern Tanzania. Am JTrop Med Hyg 78: 714–720.
Fairhurst RM, Fujioka H, Hayton K, Collins KF, Wellems TE.2003. Aberrant development of Plasmodium falciparumin hemoglobin CC red cells: Implications for the malariaprotective effect of the homozygous state. Blood 101:3309–3315.
Fairhurst RM, Baruch DI, Brittain NJ, Ostera GR, WallachJS, Hoang HL, Hayton K, Guindo A, Makobongo MO,Schwartz OM, et al. 2005. Abnormal display of PfEMP-1on erythrocytes carrying haemoglobin C may protectagainst malaria. Nature 435: 1117–1121.
Ferreira A, Marguti I, Bechmann I, Jeney V, Chora A, PalhaNR, Rebelo S, Henri A, Beuzard Y, Soares MP. 2011. Sicklehemoglobin confers tolerance to Plasmodium infection.Cell 145: 398–409.
Flatz G, Pik C, Sringam S. 1965. Haemoglobin E and b-thalassaemia: Their distribution in Thailand. Ann HumGenet 29: 151–170.
Flint J, Hill AV, Bowden DK, Oppenheimer SJ, Sill PR, Ser-jeantson SW, Bana-Koiri J, Bhatia K, Alpers MP, Boyce AJ,et al. 1986. High frequencies of a-thalassaemia are theresult of natural selection by malaria. Nature 321:744–750.
Flint J, Harding RM, Boyce AJ, Clegg JB. 1998. The popu-lation genetics of the haemoglobinopathies. BaillieresClin Haematol 11: 1–51.
Fowkes FJ, Allen SJ, Allen A, Alpers MP, Weatherall DJ, DayKP. 2008. Increased microerythrocyte count in homozy-gous aþ-thalassaemia contributes to protection againstsevere malarial anaemia. PLoS Med 5: e56.
Foy H, Kondi A, Rebello A, Martins F. 1952. The distributionof sickle cell trait and the incidence of sickle cell anaemiain the Negro tribes of Portuguese East Africa. East AfrMed J 29: 247–251.
Foy H, Kondi A, Timms GL, Brass W, Bushra F. 1954. Thevariability of sickle-cell rates in the tribes of Kenya andthe Southern Sudan. Br Med J 1: 294–297.
Friedman MJ. 1978. Erythrocytic mechanism of sickle cellresistance to malaria. Proc Natl Acad Sci 75: 1994–1997.
Friedman MJ, Roth EF, Nagel RL, Trager W. 1979. The role ofhemoglobins C, S, and Nbalt in the inhibition of malariaparasite development in vitro. Am J Trop Med Hyg 28:777–780.
� Fucharoen S, Weatherall DJ. 2012. The hemoglobin E thal-assemias. Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a011734.
Gilles HM, Fletcher KA, Hendrickse RG, Lindner R, ReddyS, Allan N. 1967. Glucose-6-phosphate-dehydrogenasedeficiency, sickling, and malaria in African children inSouth Western Nigeria. Lancet 1: 138–140.
Gouagna LC, Bancone G, Yao F, Yameogo B, Dabire KR,Costantini C, Simpore J, Ouedraogo JB, Modiano D.2010. Genetic variation in human HBB is associatedwith Plasmodium falciparum transmission. Nat Genet42: 328–331.
Guggenmoos-Holzmann I, Bienzle U, Luzzatto L. 1981.Plasmodium falciparum malaria and human red cells.II: Red cell genetic traits and resistance against malaria.Int J Epidemiol 10: 16–22.
Guinet F, Diallo DA, Minta D, Dicko A, Sissoko MS, KeitaMM, Wellems TE, Doumbo O. 1997. A comparison of theincidence of severe malaria in Malian children with nor-mal and C-trait hemoglobin profiles. Acta Trop 68:175–182.
Haldane JBS. 1949. The rate of mutation of human genes.Hereditas 35: 267–273.
Hedrick PW. 2011. Selection and mutation fora thalassemiain nonmalarial and malarial environments. Ann HumGenet 75: 468–474.
� Higgs DR. 2012. Molecular basis of a thalassemia. ColdSpring Harb Perspect Med doi: 10.1101/cshperspect.a011718.
Hill AV, Bowden DK, O’Shaughnessy DF, Weatherall DJ,Clegg JB. 1988. b Thalassemia in Melanesia: Associationwith malaria and characterization of a common variant(IVS-1 nt 5 G----C). Blood 72: 9–14.
Jallow M, Teo YY, Small KS, Rockett KA, Deloukas P, ClarkTG, Kivinen K, Bojang KA, Conway DJ, Pinder M, et al.2009. Genome-wide and fine-resolution associationanalysis of malaria in West Africa. Nat Genet 41:657–665.
Kaminsky R, Kruger N, Hempelmann E, Bommer W. 1986.Reduced development of Plasmodium falciparum in b-thalassaemic erythrocytes. Z Parasitenkd 72: 553–556.
T.N. Williams and D.J. Weatherall
12 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

Kar S, Seth S, Seth PK. 1992. Prevalence of malaria in AoNagas and its association with G6PD and HbE. Hum Biol64: 187–197.
Kreuels B, Kreuzberg C, Kobbe R, Ayim-Akonor M, Apiah-Thompson P, Thompson B, Ehmen C, Adjei S, LangefeldI, Adjei O, et al. 2010. Differing effects of HbS and HbCtraits on uncomplicated falciparum malaria, anemia, andchild growth. Blood 115: 4551–4558.
Kulozik AE, Wainscoat JS, Serjeant GR, Kar BC, Al-AwamyB, Essan GJF, Falusi AG, Haque SK, Hilali AM, Kate S,et al. 1986. Geographical survey of bs-globin gene haplo-types: Evidence for an independent Asian origin of thesickle-cell mutation. Am J Hum Genet 39: 239–244.
Lawaly YR, Sakuntabhai A, Marrama L, Konate L, Phimpra-phi W, Sokhna C, Tall A, Sarr FD, Peerapittayamongkol C,Louicharoen C, et al. 2010. Heritability of the humaninfectious reservoir of malaria parasites. PLoS ONE 5:e11358.
Le Hesran JY, Personne I, Personne P, Fievet N, Dubois B,Beyeme M, Boudin C, Cot M, Deloron P. 1999. Longitu-dinal study of Plasmodium falciparum infection and im-mune responses in infants with or without the sickle celltrait. Int J Epidemiol 28: 793–798.
Lin E, Tavul L, Michon P, Richards JS, Dabod E, Beeson JG,King CL, Zimmerman PA, Mueller I. 2010. Minimal as-sociation of common red blood cell polymorphisms withPlasmodium falciparum infection and uncomplicatedmalaria in Papua New Guinean school children. Am JTrop Med Hyg 83: 828–833.
Livingstone FB. 1973. Data on the abnormal hemoglobin andglucose-6-phosphate dehydrogenase deficiency in humanpopulations. Museum of Anthropology, University ofMichigan, Ann Arbor, MI.
Livingstone FB. 1985. Frequencies of hemoglobin variants.Oxford University Press, New York.
Luzzatto L, Nwachuku-Jarrett ES, Reddy S. 1970. Increasedsickling of parasitised erythrocytes as mechanism of re-sistance against malaria in the sickle-cell trait. Lancet 1:319–321.
Makani J, Komba AN, Cox SE, Oruo J, Mwamtemi K, Ki-tundu J, Magesa P, Rwezaula S, Meda E, Mgaya J, et al.2010. Malaria in patients with sickle cell anemia: Burden,risk factors, and outcome at the outpatient clinic andduring hospitalization. Blood 115: 215–220.
Marsh K, Otoo L, Hayes RJ, Carson DC, Greenwood BM.1989. Antibodies to blood stage antigens of Plasmodiumfalciparum in rural Gambians and their relation to pro-tection against infection. Trans R Soc Trop Med Hyg 83:293–303.
May J, Evans JA, Timmann C, Ehmen C, Busch W, Thye T,Agbenyega T, Horstmann RD. 2007. Hemoglobin vari-ants and disease manifestations in severe falciparum ma-laria. JAMA 297: 2220–2226.
McAuley CF, Webb C, Makani J, Macharia A, Uyoga S, OpiDH, Ndila C, Ngatia A, Scott JA, Marsh K, et al. 2010.High mortality from Plasmodium falciparum malaria inchildren living with sickle cell anemia on the coast ofKenya. Blood 116: 1663–1668.
Migot-Nabias F, Pelleau S, Watier L, Guitard J, Toly C, DeAraujo C, Ngom MI, Chevillard C, Gaye O, Garcia A.2006. Red blood cell polymorphisms in relation to Plas-
modium falciparum asymptomatic parasite densities andmorbidity in Senegal. Microbes Infect 8: 2352–2358.
Mockenhaupt FP, Ehrhardt S, Cramer JP, Otchwemah RN,Anemana SD, Goltz K, Mylius F, Dietz E, Eggelte TA,Bienzle U. 2004a. Hemoglobin C and resistance to severemalaria in Ghanaian children. J Infect Dis 190: 1006–1009.
Mockenhaupt FP, Ehrhardt S, Gellert S, Otchwemah RN,Dietz E, Anemana SD, Bienzle U. 2004b. aþ Thalassemiaprotects African children from severe malaria. Blood 104:2003–2006.
Modell B, Darlison M. 2008. Global epidemiology of hae-moglobin disorders and derived service indicators. BullWorld Health Organ 86: 480–487.
Modiano G, Morpurgo G, Terrenato L, Novelletto A, DiRienzo A, Colombo B, Purpura M, Mariani M, Santa-chiara-Benerecetti S, Brega A, et al. 1991. Protectionagainst malaria morbidity: Near-fixation of the a-thalas-semia gene in a Nepalese population. Am J Hum Genet48: 390–397.
Modiano D, Luoni G, Sirima BS, Simpore J, Verra F, KonateA, Rastrelli E, Olivieri A, Calissano C, Paganotti GM,et al. 2001. Haemoglobin C protects against clinical Plas-modium falciparum malaria. Nature 414: 305–308.
Naka I, Ohashi J, Nuchnoi P, Hananantachai H, Looareesu-wan S, Tokunaga K, Patarapotikul J. 2008. Lack of asso-ciation of the HbE variant with protection from cerebralmalaria in Thailand. Biochem Genet 46: 708–711.
Odegbemi JO, Williams AI. 1995. Immunoglobulin levels inmalaria infected Nigerians with and without abnormalhaemoglobin. Afr J Med Med Sci 24: 21–25.
O’Donnell A, Premawardhena A, Arambepola M, Samara-nayake R, Allen SJ, Peto TE, Fisher CA, Cook J, CorranPH, Olivieri NF, et al. 2009. Interaction of malaria with acommon form of severe thalassemia in an Asian popula-tion. Proc Natl Acad Sci 106: 18716–18721.
Ohashi J, Naka I, Patarapotikul J, Hananantachai H, Brit-tenham G, Looareesuwan S, Clark AG, Tokunaga K. 2004.Extended linkage disequilibrium surrounding the hemo-globin E variant due to malarial selection. Am J HumGenet 74: 1198–1208.
Olson JA, Nagel RL. 1986. Synchronized cultures of P. fal-ciparum in abnormal red cells: The mechanism ofthe inhibition of growth in HbCC cells. Blood 67: 997–1001.
Oo M, Tin S, Marlar T, O’Sullivan WJ. 1995. Genetic red celldisorders and severity of falciparum malaria in Myanmar.Bull World Health Organ 73: 659–665.
O’Shaughnessy DF, Hill AVS, Bowden DK, Weatherall DJ,Clegg JB. 1990. Globin genes in Micronesia: Origins andaffinities of Pacific Island peoples. Am J Hum Genet 46:144–155.
Pasvol G, Wilson RJ. 1982. The interaction of malaria par-asites with red blood cells. Br Med Bull 38: 133–140.
Pasvol G, Weatherall DJ, Wilson RJ. 1978. Cellular mecha-nism for the protective effect of haemoglobin S againstP. falciparum malaria. Nature 274: 701–703.
Penman BS, Pybus OG, Weatherall DJ, Gupta S. 2009.Epistatic interactions between genetic disorders ofhemoglobin can explain why the sickle-cell gene is
Epidemiology of the Hemoglobinopathies
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

uncommon in the Mediterranean. Proc Natl Acad Sci 106:21242–21246.
Penman BS, Habib S, Kanchan K, Gupta S. 2011. Negativeepistasis between aþ thalassaemia and sickle cell trait canexplain interpopulation variation in South Asia. Evolu-tion 65: 3625–3632.
Piel FB, Patil AP, Howes RE, Nyangiri OA, Gething PW,Williams TN, Weatherall DJ, Hay SI. 2010. Global distri-bution of the sickle cell gene and geographical confirma-tion of the malaria hypothesis. Nat Commun 1: 104.
Ringelhann B, Hathorn MK, Jilly P, Grant F, Parniczky G.1976. A new look at the protection of hemoglobin AS andAC genotypes against Plasmodium falciparum infection:A census tract approach. Am J Hum Genet 28: 270–279.
Roth EF Jr, Friedman M, Ueda Y, Tellez I, Trager W, NagelRL. 1978. Sickling rates of human AS red cells infected invitro with Plasmodium falciparum malaria. Science 202:650–652.
Scott JA, Berkley JA, Mwangi I, Ochola L, Uyoga S, MachariaA, Ndila C, Lowe BS, Mwarumba S, Bauni E, et al. 2011.Relation between falciparum malaria and bacteraemia inKenyan children: A population-based, case-control studyand a longitudinal study. Lancet 378: 1316–1323.
Senok AC, Li K, Nelson EA, Yu LM, Tian LP, OppenheimerSJ. 1997. Invasion and growth of Plasmodium falciparumis inhibited in fractionated thalassaemic erythrocytes.Trans R Soc Trop Med Hyg 91: 138–143.
Serjeant GR. 2005. Mortality from sickle cell disease in Af-rica. BMJ 330: 432–433.
Shear HL, Roth EF Jr, Fabry ME, Costantini FD, Pachnis A,Hood A, Nagel RL. 1993. Transgenic mice expressinghuman sickle hemoglobin are partially resistant to rodentmalaria. Blood 81: 222–226.
Siniscalco M, Bernini L, Latte B. 1961. Favism and thalas-saemia in Sardinia and their relationship to malaria. Na-ture 190: 1179–1180.
Storey J, Fleming AF, Cornille-Brogger R, Molineaux L,Matsushima T, Kagan I. 1979. Abnormal haemoglobinsin the Sudan savanna of Nigeria. IV: Malaria, immuno-globulins and antimalarial antibodies in haemoglobinAC individuals. Ann Trop Med Parasitol 73: 311–315.
Tan X, Traore B, Kayentao K, Ongoiba A, Doumbo S, Wais-berg M, Doumbo OK, Felgner PL, Fairhurst RM, Cromp-ton PD. 2011. Hemoglobin S and C heterozygosity en-hances neither the magnitude nor breadth of antibodyresponses to a diverse array of Plasmodium falciparumantigens. J Infect Dis 204: 1750–1761.
Thompson GR. 1962. Significance of haemoglobins S and Cin Ghana. Br Med J 5279: 682–685.
Thompson GR. 1963. Malaria and stress in relation to hae-moglobins S and C. Br Med J 5363: 976–978.
Udomsangpetch R, Sueblinvong T, Pattanapanyasat K,Dharmkrong-at A, Kittikalayawong A, Webster HK.1993. Alteration in cytoadherence and rosetting of Plas-modium falciparum-infected thalassemic red blood cells.Blood 82: 3752–3759.
Veenemans J, Andang’o PE, Mbugi EV, Kraaijenhagen RJ,Mwaniki DL, Mockenhaupt FP, Roewer S, Olomi RM,Shao JF, van der Meer JW, et al. 2008. aþ-Thalassemia
protects against anemia associated with asymptomaticmalaria: Evidence from community-based surveys inTanzania and Kenya. J Infect Dis 198: 401–408.
Veenemans J, Jansen EJ, Baidjoe AY, Mbugi EV, Demir AY,Kraaijenhagen RJ, Savelkoul HF, Verhoef H. 2011. Effectof aþ-thalassaemia on episodes of fever due to malariaand other causes: A community-based cohort study inTanzania. Malar J 10: 280.
Verra F, Bancone G, Avellino P, Blot I, Simpore J, Modiano D.2007a. Haemoglobin C and S in natural selection againstPlasmodium falciparum malaria: A plethora or a singleshared adaptive mechanism? Parassitologia 49: 209–213.
Verra F, Simpore J, Warimwe GM, Tetteh KK, Howard T,Osier FH, Bancone G, Avellino P, Blot I, Fegan G, et al.2007b. Haemoglobin C and S role in acquired immunityagainst Plasmodium falciparum malaria. PLoS ONE 2:e978.
Wambua S, Mwangi TW, Kortok M, Uyoga SM, MachariaAW, Mwacharo JK, Weatherall DJ, Snow RW, Marsh K,Williams TN. 2006. The effect of aþ-thalassaemia on theincidence of malaria and other diseases in children livingon the coast of Kenya. PLoS Med 3: e158.
Weatherall DJ. 2010. Thalassemia as a global health prob-lem: Recent progress towards its control in the developingcountries. Ann NY Acad Sci 1202: 17–23.
Weatherall DJ, Clegg JB. 2001. The thalassaemia syndromes.Blackwell Science, Oxford.
Willcox M, Bjorkman A, Brohult J. 1983. Falciparum ma-laria and b-thalassaemia trait in northern Liberia. AnnTrop Med Parasitol 77: 335–347.
Williams TN, Obaro SK. 2011. Sickle cell disease and ma-laria morbidity: A tale with two tails. Trends Parasitol 27:315–320.
Williams TN, Maitland K, Bennett S, Ganczakowski M, PetoTE, Newbold CI, Bowden DK, Weatherall DJ, Clegg JB.1996. High incidence of malaria in a-thalassaemic child-ren. Nature 383: 522–525.
Williams TN, Mwangi TW, Roberts DJ, Alexander ND,Weatherall DJ, Wambua S, Kortok M, Snow RW, MarshK. 2005a. An immune basis for malaria protection by thesickle cell trait. PLoS Med 2: e128.
Williams TN, Mwangi TW, Wambua S, Alexander ND, Kor-tok M, Snow RW, Marsh K. 2005b. Sickle cell trait and therisk of Plasmodium falciparum malaria and other child-hood diseases. J Infect Dis 192: 178–186.
Williams TN, Mwangi TW, Wambua S, Peto TEA, Weath-erall DJ, Gupta S, Recker M, Penman BS, Uyoga S, Ma-charia A, et al. 2005c. Negative epistasis between the ma-laria-protective effects of aþ-thalassemia and the sicklecell trait. Nat Genet 37: 1253–1257.
Williams TN, Wambua S, Uyoga S, Macharia A, MwacharoJK, Newton CR, Maitland K. 2005d. Both heterozygousand homozygous aþ thalassemias protect against severeand fatal Plasmodium falciparum malaria on the coast ofKenya. Blood 106: 368–371.
Win N, Lwin AA, Oo MM, Aye KS, Soe S, Okada S. 2005.Hemoglobin E prevalence in malaria-endemic villages inMyanmar. Acta Med Okayama 59: 63–66.
T.N. Williams and D.J. Weatherall
14 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011692
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from

2012; doi: 10.1101/cshperspect.a011692Cold Spring Harb Perspect Med Thomas N. Williams and David J. Weatherall HemoglobinopathiesWorld Distribution, Population Genetics, and Health Burden of the
Subject Collection Hemoglobin and Its Diseases
The Natural History of Sickle Cell DiseaseGraham R. Serjeant Hemoglobin Synthesis
Transcriptional Mechanisms Underlying
Nathaniel J. Pope, et al.Koichi R. Katsumura, Andrew W. DeVilbiss,
Current Management of Sickle Cell Anemia
WarePatrick T. McGann, Alecia C. Nero and Russell E. Disease
Iron Deficiency Anemia: A Common and Curable
Jeffery L. Miller
TherapiesTargetedNew Disease Models Leading the Way to
Cell-Free Hemoglobin and Its Scavenger Proteins:
Dominik J. Schaer and Paul W. Buehler
Management of the ThalassemiasNancy F. Olivieri and Gary M. Brittenham
-ThalassemiaαClinical Manifestations of Elliott P. Vichinsky
-ThalassemiaβThe Molecular Basis of Swee Lay Thein
Erythroid Heme Biosynthesis and Its DisordersHarry A. Dailey and Peter N. Meissner
Erythropoiesis: Development and DifferentiationElaine Dzierzak and Sjaak Philipsen
Clinical CorrelatesHemoglobin Variants: Biochemical Properties and
Gell, et al.Christopher S. Thom, Claire F. Dickson, David A.
ErythropoietinH. Franklin Bunn
The Prevention of ThalassemiaAntonio Cao and Yuet Wai Kan
Classification of the Disorders of HemoglobinBernard G. Forget and H. Franklin Bunn
The Switch from Fetal to Adult HemoglobinVijay G. Sankaran and Stuart H. Orkin
-ThalassemiaαThe Molecular Basis of Douglas R. Higgs
http://perspectivesinmedicine.cshlp.org/cgi/collection/ For additional articles in this collection, see
Copyright © 2012 Cold Spring Harbor Laboratory Press; all rights reserved
on January 19, 2021 - Published by Cold Spring Harbor Laboratory Presshttp://perspectivesinmedicine.cshlp.org/Downloaded from