Workshop 2 Business of Leading Residency HO Shell 2_Business of... · Business of Leading Residency...
39
PRACTICE MODEL TRANSFORMATIONS: Achieving excellence through accountability and innovation Business of Leading Residency Program Development and Growth Steve Rough, M.S., Director, Pharmacy Services University of Wisconsin Health System Madison, Wisconsin Todd W. Nesbit, Pharm.D., MBA Associate Director, Department of Pharmacy The Johns Hopkins Hospital Baltimore, Maryland Introductions • Steve Rough and the University of Wisconsin Hospital and Clinics • Todd Nesbit and The Johns Hopkins Hospital Agenda • Overview of our departments and residency training programs • Why is this issue important? – Trends, PPMI, Stakeholder Conference • Model business case framework for justifying residency program development and growth • Break • Integrating residents into your practice model – As a means of advancing your practice model • Feedback and debate 6
Transcript of Workshop 2 Business of Leading Residency HO Shell 2_Business of... · Business of Leading Residency...

PRACTICE MODEL TRANSFORMATIONS:Achieving excellence through accountability and innovation
Business of Leading Residency Program Development
and Growth
Steve Rough, M.S., Director, Pharmacy Services
University of Wisconsin Health System
Madison, Wisconsin
Todd W. Nesbit, Pharm.D., MBA
Associate Director, Department of Pharmacy
The Johns Hopkins Hospital
Baltimore, Maryland
Introductions
• Steve Rough and the University of Wisconsin Hospital and Clinics
• Todd Nesbit and The Johns Hopkins Hospital
Agenda
• Overview of our departments and residency training programs
• Why is this issue important?
– Trends, PPMI, Stakeholder Conference
• Model business case framework for justifying residency program development and growth
• Break
• Integrating residents into your practice model
– As a means of advancing your practice model
• Feedback and debate
6

What this is not
• Residency Learning System (RLS) overview
• Accreditation review
• How to start a residency
What Systems are Represented?
<100 beds
101 300 b d101‐300 beds
>300 beds
What Systems are Represented?
Academic
Non‐academic
7

What Systems are Represented?
Urban
Rural
Do You Have a Residency Training Program at your Site?
Do not have a program
Have a PGY1 programHave a PGY1 program
Have a PGY1 and PGY2 program
Overview of our Departments and ProgramsDepartments and Programs
Steve and Todd
15 minutes
8

UW Hospital and ClinicsFacts and Figures FY12
Beds 491
Average daily census 388
ICU beds‐pediatric & adult 83
Inpatient admissions 27,323
Patient days 144,649
Total OR cases 25,368
Emergency dept visits 44,776
Operating revenues $1.3 billion
Clinics 95
Clinic visits 605,682
Staff 7,814
Medical residents & fellows 509
Service Lines
• Transplant – >500 solid organs per year
• Oncology – 3,000 discharge per year
• Heart and Vascular – 3,500 discharges per year
• Neurosciences 2000 discharges per year• Neurosciences – 2000 discharges per year
• Orthopedics – 2,500 discharge per year
• Children’s Hospital – 3,000 discharge per year
• General surgery – 2,200 discharges per year
9

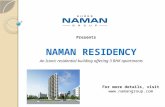
UW Health Integrated Pharmacy Care Network
Automation and robotic technologyClinical and translational research
Education and trainingElectronic health record/information technology systems
Entrepreneurial business expansionFinancial management (utilization, contracting)
Medication use policy programN l h i
Community (Retail) Pharmacy
Services Network
i h /
Management of CorporatePharmacy Network
Specialty Care/Mail Service
Pharmacy
Nuclear pharmacy serviceOperations and medication use systems management
Patient care services/practice advancementPersonnel management
Purchasing contract network (Novation/UHC)Quality and safety
Regulatory complianceRevenue cycle optimizationSupply chain management
UW Health Acute and Ambulatory Care Core Pharmacy Services
(UW Hospital, UWMF, DFM)
Unity Pharmacy Program/Prescription Benefit
Management Services
Rural Hospital Management/Purchasing Contracts
and Consulting Services
Home Health CarePharmacy Services
Hospice Care and Other Pharmacy
Service Agreements
UW Health Department of Pharmacy
1. Receives support from and interacts closely with the CCKM in establishment of evidence-based medication use policy initiatives2. Reports to Brad Ludwig for operational responsibilities; reports to Steve Rough for overall departmental integration
Department Personnel Statistics
• 316 FTEs
• 27 FTE leadership team
– 1 director
– 14 managers, 12 supervisors
• 127 pharmacist FTE
• 148 technicians and support staff
– 52 inpatient
– 29 retail
– 5.5 clinicsp
– 64 inpatient
– 24 retail
– 15 clinic
– 2.5 ED, 2 OR, 2 Nuclear
– 17.5 “other” (drug policy, research, informatics, PBM, hospice, poison)
– 7.7 funded by SOP
– 8 focused on “transitions”
• 3 reimbursement
• 2 indigent drug program
• 2 medication prior authorization
• 1 medication discharge specialist
• 17 residents
10

Pharmacy Residency History1960’s
•Unit dose
•IV admixture
•Unit‐based pharmacists
1970’s
•Clinical pharmacy services
•Computerization
1980’s
•Advanced technician role
•Clinic pharmacists
Residency• 304 past‐residents since 1963
• Since 1963, a single “hospital pharmacy residency” has expanded
•Clinic pharmacists
•Retail growth
1990’s
•Dispensing automation
•Pharmaceutical Research Center (PRC)
•Center for Drug Policy (now the Drug Policy Program)
•PBM (Unity) services
2000’s
•Automation
•Electronic Health Record
•Innovative pharmacist roles and new business ventures
•Entrepreneurial ambulatory growth
2010’s
•Practice model and staff professional development
•Decision support
•Operational efficiency
•Pharmacy primary care role
into 7 distinct programs
• All major milestones in department history have been fueled by resident power!
– Residents are highly integrated into the advancement of the department
Residency‐related statistics
• Inpatient pharmacists n = 77
– PGY1 = 38 (49%)
– PGY1 and 2 = 16 (21%)
– No residency = 23 (30%) – only 2 have < 10 yrs experience
• 17 Residents
– PGY1 hospital (4)
– PGY1 community (1)
– PGY1 and 2 with MS in administration (8)
– PGY2 critical care, transplant, and oncology (3)
– PGY1 and 2 medication use systems and technology (1)
UWHC Residency Program in 2017
• Expand residency program to 25+ residents by 2017
– Increase PGY1 practice, PGY2 specialty
• Scholarly achievements– Meaningful projects and practice research
– Publications
• Emphasize resident accountability– Free up pharmacist time for advancing practice, committee
participation, education, and research
– Less “shadowing,” more “doing”
– On call for patient care overnight
– More integration into the practice model!!!
11

The Johns Hopkins Hospital
• 1,085 licensed patient beds
• 46,775 inpatient admissions
421 933 i
• 5 ‐ affiliate hospitals
• 25 ‐ primary health care sites (Johns Hopkins Community Physicians)
$248 illi i• 421,933 outpatient encounters
• 1,714 full‐time attending physicians
• $994 million hospital redevelopment project
• $248 million in uncompensated care
• $425 million federal research support
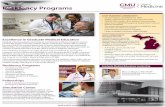
Sr. Director of PharmacyDaniel Ashby 1
Administrative SecretaryJane Odum
Assistant DirectorInvestigational Drug Service
Janet Mighty 2
Assistant DirectorEducation and Training
Cathy Walker
Business ManagerSheila Lind
Director of FinanceRosemary Hines
Division DirectorWeinberg Pharmacy 3
Rowena Schwartz
Medication Safety OfficerRobert Feroli
Associate Director Clinical and Decentralized
Pharmacy ServicesTodd Nesbit
Associate Director Informatics and
Central Pharmacy ServicesCarla Gill
Director Center for Pharmaceutical
Outcomes Kenneth Shermock
Department of PharmacyTable of Organization
Sr. Project AdministratorNew Clinical Building
Edwin Huie
Pharmacy and Therapeutics Committee
Decentralized Service Integration and
Division Directors
Assistant DirectorClinical Informatics
Brian Pinto
Antibiotic Management and Anticoagulation
Program
Assistant Director Purchasing/Contracting
Shirley Geize
Division Director Central Pharmacy Denise Rodriguez
Assistant DirectorMed Use Informatics
Brendan Reichert
Assistant Director QA / Regulatory
Kristen Webb
Medication SafetyResident
Medication Safety Officer (Acute Care)
Elizabeth Fang
Medication Safety Officer (Pediatrics)Nicole MacLaughlin
Director, Pharmaquip Infusion Services 5
Mitra Gavgani
Director, Johns Hopkins Outpatient Pharmacies 5
Nathan Thompson
Division Director Carnegie-6 Pharmacy
John Lewin
Division Director Osler-2 Pharmacy
Virna Almuete
Division DirectorPediatric Pharmacy 4
Michael Veltri
DUE
Formulary
1 Reports to R. Miller and M. Weisfeldt2 Reports to D. Ashby and D. Ford3 Reports to D. Ashby and Oncology Representative4 Reports to D. Ashby an Pediatrics Representative5 Reports to D. Smith and D. Ashby July 2010
Administrative AssistantOdell Carroll
12

Department of Pharmacy
• 5 Decentralized Divisions and 1 Central Pharmacy
• 100 FTEs pharmacists, 115 FTEs technicians, 30 li i l i li t 25
• Acute care services provided 24/7
• Ambulatory services Monday – Friday
clinical specialists, 25 pharmacy residents (13 –PGY1, 12 – PGY2)
• 20 affiliated schools of pharmacy (5 preferred)
• Eclipsys Sunrise Clinical Manager™ interfaced with GE Centricity®
• Robotic unit‐dose‐cart fill
• ADCs for critical or emergency use drugs
Why is this Issue Important?
Todd
20 minutes
The consensus of the Pharmacy Practice Model Summit
• Beliefs and assumptions– A1. There is opportunity to significantly advance the health and well‐being of patients in hospitals and health systems by changing how pharmacists, pharmacy technicians, and technology resources are d l ddeployed.
– A2. In the next 5‐10 years, hospitals and health systems will be under increasing pressure to cut operating costs.
– A3. In the next 5‐10 years, hospital and health‐system executives will require pharmacy department operations to be more efficient.
13

The consensus of the Pharmacy Practice Model Summit
• Beliefs and assumptions– A4. Within the next few years, financial pressures on hospitals and health systems will force them to pursue significant changes in how pharmacy resources are usedused.
– B3. All hospital and health systems will not require the same level of pharmacist‐provided drug therapy management.
– B4. In the next 5‐10 years, there will be increasing demand among new pharmacy graduates for residency training.
The consensus of the Pharmacy Practice Model Summit
• Beliefs and assumptions
– B5. In the next 5‐10 years, an increasing number of pharmacists will pursue clinical specialization.
– B6 The following are barriers to the developmentB6. The following are barriers to the development of optimal pharmacy practice models:
• B6a. Insufficient leadership within the field of hospital and health‐system pharmacy to catalyze change.
• B6b. Resistance to change from current pharmacy staff.
• B6c. Lack of pharmacy staff resources.
The consensus of the Pharmacy Practice Model Summit
• Beliefs and assumptions– C1. In most hospitals and health systems, improvements in technology will be required for pharmacy departments to fully achieve optimal d l t f h i t d hdeployment of pharmacist and pharmacy technician resources.
– D1. Pharmacy technicians who have appropriate education, training, and credentials could be used much more extensively to free pharmacists from drug distribution activities.
14

The consensus of the Pharmacy Practice Model Summit
• Beliefs and assumptions– E4. The following are critical components in the implementation of optimal pharmacy practice models:
• E4a. Department of Pharmacy leadership.
• E4b. Clinical pharmacy leadership.
• E4c. Ensuring competence of staff to provide drug therapy management.
• E4d. Assignment of pharmacists to patient care units.
• E4o. Increased number of residency‐trained pharmacists.
The consensus of the Pharmacy Practice Model Summit
• Drug Therapy Management– Multidisciplinary team process for selecting appropriate drug therapies, educating patients, monitoring patients, and continually assessing outcomes of therapy Pharmacist activities in drugoutcomes of therapy. Pharmacist activities in drug therapy management my include but are not limited to initiating, modifying, and monitoring a patient’s drug therapy; ordering and performing laboratory and related tests; assessing patient response to therapy; counseling and educating a patient about medications; and administering medications.
The consensus of the Pharmacy Practice Model Summit
• Recommendations
– A9. All patients should have a right to the care of a pharmacist.
– B8 Drug therapy management should be providedB8. Drug therapy management should be provided by a pharmacist for each hospital inpatient.
– B9. For hospitals and health systems that provide ambulatory care services, drug therapy management should be available from a pharmacist for each outpatient.
15

The consensus of the Pharmacy Practice Model Summit
• Recommendations
– B23. The following characteristics or activities should be considered essential to pharmacist‐provided drug‐therapy management in optimal p g py g ppharmacy practice models:
• B23p. Pharmacist completion of ASHP accredited residency training or achievement of equivalent experience.
The consensus of the Pharmacy Practice Model Summit
• Recommendations– B24: Every Pharmacy Department should:
• B24a. Identify drug therapy management services that should be provided consistently by its pharmacists.
B24b D l l ll i• B24b. Develop a plan to reallocate its resources to devote significantly more pharmacist time to drug therapy management services.
• B24c. Develop a plan to allocate pharmacy student time to drug therapy management services.
• B24i/j. Manage prospective/retrospective medication‐use evaluation programs to improve prescribing.
The consensus of the Pharmacy Practice Model Summit
• Recommendations– B25: In optimal pharmacy practice models:
• B25c. Individual pharmacists should not be engaged specifically in drug therapy management without an understanding and responsibility for the medicationunderstanding and responsibility for the medication‐use or delivery systems.
• B25d. Individual pharmacists must accept responsibility for both the clinical and the distributive activities of the pharmacy department.
• B25e. Clinical specialist positions are necessary to advance practice, education, and research activities.
16

The consensus of the Pharmacy Practice Model Summit
• Recommendations
– C13: Pharmacy residency programs should provide informatics training to ensure residents’ success in optimal practice models.p p
– C14. Advanced training in pharmacy informatics with residencies and postgraduate education should be expanded.
Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
17

Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
18

Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
19

Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
20

Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
Pharmacy Residency Capacity Stakeholders Conference
• Recommendations– New Models:
• Increasing ratios beyond the current 1:1 preceptor to student ratio
• Introducing the concept of an “attending pharmacist” similar to the medical model that would oversee several residentsto the medical model that would oversee several residents
• Introducing the concept of the resident is a “practitioner learner” as the resident is already a licensed pharmacist advancing themselves, perhaps autonomy occurs sooner in the residency training
• Allowing new administrative oversight to help more programs develop
• Use of distance technology to support remote locations
21

Pharmacy Residency Capacity Stakeholders Conference
• Recommendations
– Existing Models:
• Development of tools to start to expand residencies, targeted by different practice settings
• Develop outreach programs for targeted areas of expansion (300‐500 bed hospitals, colleges of pharmacy not involved in residency training, chain drug stores, managed care organizations, etc.)
Model Business Case Framework for Justifying Residency Program
Growth/Expansion
Steve
40 minutes
What’s the value for UWHC?What’s the value for UWHC?
Spring, 2011
22

External Funding
Cost Reduction & Avoidance
Contribution to mission of UW Health
Benefits of Pharmacy Residency
Provider Satisfaction
Quality, Compliance &
Service
New Business & Service Growth
Pharmacist Recruitment, Development, & Satisfaction
y yPrograms for UW Health
External Funding
Federal Government
• Graduate medical education: “Medicare pass‐through funds” (PTF) available for accredited PGY1 pharmacy residency programs
Other
p g
• State and national pharmacy associations –professional project (research) grants
• Pharmaceutical industry grants
23

Ex: Medicare Pass Through Funds*
Cost Item Calculation ($) Cost ($)
Direct CostsResident
Salary + benefitsTravel
Residency accreditation feeTuition & related expensesTeaching time
Program director
(38,300 + 20% benefits) x10
4 programs9,000 x 4 admin residents
(20% of salary + benefits)
459,6008,6054,725
36,000
41,300Director – administrative timePreceptor – teaching timePreceptor – administrative time
Preceptor travelTotal direct costs
(5% of salary + benefits)(25% of salary + benefits) x10(5% of salary + benefits) x10
10,325312,000
62,4002,125
937,080
Indirect costs (30% of total direct costs) 281,124
Total educational costs 1,218,204
Anticipated Medicare reimbursement
Medicare pt load (35.6%) x total educational costs $433,681
NET COST (1,218,789-433,889) $784,523
*Assumes 10 PGY1 pharmacy residents with a 35.6% UWHC Medicare patient load
Cost Reduction
• All residents are responsible for completing one or more drug cost reduction projects each year*
– On average each project reduces drug costs by– On average, each project reduces drug costs by $40,000
– Total annual cost reduction = $1,280,000
*Administrative residents complete three cost reduction projects per year, all others complete one per year
Cost Avoidance
• Online staffing as clinical pharmacist
– 12 hours/week avoids 0.3 pharmacist FTE
– 0.3 RPh FTE (salary + fringe) = $41,184
– 1 resident FTE (salary + fringe) = $46,800
88% of the cost of a resident is covered by their staffing component alone
Avoids $650,000 in pharmacist FTE per year
24

Cost Avoidance
School of Pharmacy (SOP) lectures SOP lab teaching assistants Monograph preparation Medication use guideline revisions PSN f ll PSN follow‐up Site visit coordination Health Link go‐live and upgrade assistance Audits Drug contract analyses Advertising, training, and relocation fees*
*Average of 2 to 4 UWHC‐trained residents are hired onto staff each year!!
Improved Provider Satisfaction
• Nurse satisfaction– Resource for questions: drug interactions, compatibilities, administration rates, ect.
– Aid in communication with MD/PA/NP
– Assist in assuring patient doses are available to the nurses– Assist in assuring patient doses are available to the nurses at the appropriate time
– Assist in changing the dispensing location of medications for more timely administration of first doses
– Change dosing times to standardized times to reduce time demands on nurses
– Continuing education seminars
Improved Provider Satisfaction
• Physician satisfaction– Dose medications to avoid complications
– Contact prescriber regarding abnormal lab values and cultures found while monitoring patients
– Knowledgeable about UWHC’s drug formulary and therapeutic alternatives
– Drug expert for clinical rounds
– Modification of inappropriate drug orders
– Increase through‐put and efficiency
– Continuing education seminars
25

Improved Quality and Service• Patient care
– Enhance pharmacists’ capacity and effectiveness with patient care rounding, clinical monitoring, medication reconciliation and patient teaching
– Resource to research best way to manage veryResource to research best way to manage very complex patient cases
• Compliance (audits, projects)
– CMS (Centers for Medicare & Medicaid Services)
– TJC (The Joint Commission)
– Third party billing audits
– Detailed follow up on all PSN reports
• Enhanced achievement of external pay for performance quality indicators
– Improved reimbursement for pay‐for‐performance and future accountable care organization measures
Improved Quality and Service
• Increased reimbursement for medication therapy management (MTM) services in UW Health ambulatory pharmacies
– Leads to direct revenue from payers (Navitus, Unity, Group Health, etc…) via patient teaching and care management
Improved Quality and Service
• Recruitment of future (well‐trained) pharmacists
• Community service and professional activitiesactivities
• Enhance capacity of staff
• Formulary review
• Drug policy development
• Opportunity for externally funded projects
26

Expanded Pharmacy Services
Every major new UW pharmacy initiative is powered by a pharmacy resident project
Second year administrative residents complete a rotation with the VP of Professional Services to help advance goals of senior leadership
1990s – 2000s
2000s – 2010s
Electronic
Expanded Pharmacy Services
1960s –1970s
Innovation in core pharmacy services
1970s – 1980s
Advancements in patient care services
1980s – 2000s
New pharmacy business development
Expansion of clinical services into ambulatory and alternate sites
Drug policy and managed care pharmacy program development
Implementation of fully automated medication use process
medical record
Innovative pharmacist roles
New business ventures
Resident Projects
• 1960s – 1970s– 100% unit dose dispensing– Complete IV admixture system– Fully computerized pharmacy order entry/ distribution
system– Pharmacist‐managed drug information center– Pharmacist‐managed medication administration record for g
inpatients• 1970s – 1980s
– Med histories, reconciliation, discharge counseling for all patients
– Pharmacist participation on patient care rounds– Pharmacokinetic dosing services– Decentral pharmacy service in all areas from 0700 to 2300
and around the clock services for critical care areas
27

Resident Projects
• 1980s, 90s, 2000s– Pharmacists participate in >20 ambulatory clinics– Integrated ambulatory pharmacy network throughout Dane
County• 13 pharmacies• Inpatient and in‐home hospice services• Pharmacy management consultative services for hospitals in rural
communitiescommunities
• 1990s – 2000s– Developing, implementing, maintaining, and monitoring policies
related to the use of pharmaceuticals within UWHC– Initiation of several external pharmacy contract services– Manage pharmacy benefit for Unity– Coordination of technology assessment programs– Centralized robot; Automated dispensing cabinets– Barcode medication administration software at point of care– “Smart” IV infusion pump; Medication carousel
Resident Projects
• 2010s (What will we do next?)
– Practice model and professional staff advancement through development and implementation of the pharmacist career ladder
– Decision support expansion to maximize evidence‐based care
– Operational efficiency improvement
– New technologies (IV Robot, etc)
– Integration of pharmacists on primary care teams
Recruitment
• Feeder‐system for new and vacant positions
• More costly to recruit, orient, and train outside candidates
• Attract highly skilled candidates –best RPh’s want to precept residents
Pharmacist Recruitment, Development, and Satisfaction
Development
Satisfaction
• Training of new hires – technicians, interns, and pharmacists
• Promotes workplace energy, practice reflection, innovation, and company dedication to quality improvement
• Resident projects enhance workplace experience
28

Mission – Scholarship
• Faculty‐resident collaboration on scholarly efforts
• Education of other health care professionals
– Residents are required to provide education to doctors, nurses, and pharmacists
– Precept pharmacy students
Mission – Science
Each resident presents posters and many publish results of research projects, quality improvement efforts, and/or patient case reports
Mission – Social Responsibility
Residents volunteer under UW Health name– Drive to Share– Ronald McDonald House– Habitat for Humanity– Transplant games
29

Show me the money...Pharmacy Residency Program Return on Investment (ROI) Analysis
Expense for Current 16 Residents
Expense Item Cost ($)
Salary and Benefits 734,400
Travel 24,585
Tuition 72,000
Accreditation fee 5,175
Recruitment 2,185
Total Expense $838,345
External Funding for Current 16 Residents
Funding Source Funds ($)
Amgen grant 40,000g g
Medicare PTF 442,604
Total Direct Income $482,604
30

Cost Reduction for Current 16 Residents
Resident Type CalculationTotal Cost
Reduction ($)
Administrative 3 projects/yr x $40,000/project x 8 res 960,000
PGY1 1 projects/yr x $40,000/projects x 5 res 200,000
Drug Cost Reduction Project*:
p j /y $ , /p j ,
MSO 1 project/yr x $40,000/project x 1 res 40,000
PGY2 1 project/yr x $40,000/project x 2 res 80,000
Total $1,280,000
*Assumes each drug cost reduction project reduces an average of $40,000
Cost Avoidance for Current 16 residents cont…
Cost Item Calculation Cost ($)
HL go‐live assistance 50 shifts/yr x 4 hr/shift x $66/hr 13,200
Medication audits 8 audits/yr x 15hr/audit x $66/hr 7,920
Med rec assessment 10/res/yr x 0.3 hr/asmt x $66/hr x 16 res 3,168
D l i 5 l / 15h / l i $66/h 4 950Drug contract analysis 5 analyses/yr x 15hr/analysis x $66/hr 4,950
Position advertisement* 2 ads/position x 2 positions/yr x $5000/ad 20,000
New RPh training* 2 RPh FTE/yr x 40hr/wk x 8wks x $66/hr 42,240
New RPh relocation fee* 2 RPh FTE/yr x $4,000/relocation fee 8,000
Staffing ~12hr/wk x 52wk/yr x $66/hr x 16 res 646,272
Subtotal 745,750
*********continued on next slide**********
Cost Item Calculation Cost ($)
UWSOP lectures $300/lecture x 5 lectures 1,500
UWSOP lab TAs 40hr x $66/hr x 5 res 13,200
CE lectures $30/CE credit x 25 RPh/tech attendees x 11 res 8,250
Cost Avoidance for 16 residents
Monograph preparation 10hr/monograph x $66/hr x 10 res 6,600
Med use guideline revision 2hr/revision x $66/hr x 10 res 1,320
PSN follow‐up 1500 PSN/yr x 0.5hr/PSN x $66/hr 49,500
Site visit coordination 12 visits/yr x 10hr/visit x $66/hr 7,920
Subtotal $88,290
Subtotal (previous slide) 745,750
Total Cost Avoidance $834,040
31

financial gain – annual expense
annual expense= ( ) x 100
Return on Investment for Current 16 Residents
Item Cost Benefit
Total Cost $838,345
External Funding $482,604
d $Cost Reduction $1,280,000
Cost Avoidance $834,040
Total ROI $1,758,299
($482,604 + $1,280,000 + $834,040) – $838,345 $838,345ROI = = 210%
ROI Breakdown per Resident Type
Resident Type*Cost per
Resident ($)Financial Value per Resident ($)
Margin ($) ROI
Admin (n=8) 54,937 195,761 140,824 256%
PGY1 (n=5) 49 237 137 998 88 761 180%PGY1 (n=5) 49,237 137,998 88,761 180%
MSO (n=1) 48,637 110,964 62,327 128%
PGY2 (n=2) 48,937 80,382 31,445 64%
* n= # of residents in current FY11 budget
32

Residency Program Expansion
Add a permanent PGY2 oncology resident position Add a fifth administrative resident position for FY12 and FY13
Benefits of Oncology Resident
• Oncology is core UWHC service line• Area of growth and expansion – key pharmacy specialty area
• 25% of UWHC’s $109 million drug budget is oncology drugs
• At forefront of what we can do at ambulatory• At forefront of what we can do at ambulatory clinics
• Hard to find and hire pharmacists with oncology specialty
• MD demand• Services can be expanded while at the same time lowering total costs
33

Oncology PGY‐2 Specialty ResidentOperating Expenses
1.0 FTE oncology resident salary/fringe $47,000
Travel‐related expense $2,025
Lenalidomide drug cost (increase Rx capture from 50% to 65%) $200,739
Total New Operating Expense $249,764
Savings
Reduce 0 2 FTE Clinical pharmacist $29 540Reduce 0.2 FTE Clinical pharmacist $29,540
Tacrolimus drug cost reduction $16,437
Total Savings $45,977
Increased Net Revenue (Reimbursement)
Rituximab (transfer Medicare patient infusion from inpatient to oncology clinic setting)
$88,060
Lenalidomide $220,000
Total Increased Reimbursement $308,060
Total Year‐1 Net Benefit to UWHC $104,273 (42% ROI)
Additional Benefits of PGY‐2 Oncology Resident
• Improved patient access and provider efficiency by improving chemotherapy clinic through‐put
• Develop potential talent pool for difficult to fill specialized clinical pharmacy area and avoid recruiting/relocation costs
• Enhanced clinical pharmacy services in oncology clinic
• Improved compliance with TJC, CMS, NIOSH and accrediting agencies
• Enable future specialty pharmacy script capture
• Contributes to UW Health academic mission
34

Total Cost to UWHC
• Cost of 2 new resident positions
– Salary + Benefits + Travel = $103,873
• In exchange, 0.5* clinical pharmacist FTE will be removedbe removed
– Salary + Benefits = $68,640
• Total Net Investment = $35,233
*0.3 FTE for admin resident (FY12 + FY13 only) and 0.2 FTE for Oncology resident (permanent)
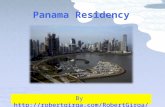
Can we afford more residents?
$2 000 000
$2,500,000
$3,000,000
$500,000
$1,000,000
$1,500,000
$2,000,000
Current Additional Onc Additional Onc & Admin
CostBenefitMargin
Let’s Compare Total ROI
Cost ($) Benefit ($) Margin ($) ROI
Current 838,345 2,596,644 1,758,299 210%
Additional Oncology942 218 2 844 541 1 902 323 202%
& Administrative942,218 2,844,541 1,902,323 202%
Difference $103,873 $247,897 $144,024
Financial return is greater with the addition of oncology and administrative residents
35

Expanding both the number of residency positions and roles of pharmacy residents p p ywill benefit the pharmacy department, the hospital, and most importantly, our patients!
Discussion: What strategies have you found most useful to achieve y
growth in your programs?
15 minutes
Break TimeBreak Time
15 minutes
36

Integrating Residents into Your Practice ModelYour Practice Model
Todd
30 minutes
What strategies are being employed at The Johns Hopkins Hospital consistent
with the ideals of the Pharmacy Practice Model Summit and thePractice Model Summit and the Pharmacy Residency Capacity Stakeholders Conference?
Team Based Pharmacy Services Model with Resident Capacity Expansion
• Assumptions– Demand for residency training opportunities continues to increase
– Pressures to reduce costs will increase over the next several years
– Demand for IPPE and APPE learning experiences will increase over the next several years
– Team based model will accommodate expansion of the PGY1 program and support growth in scope and quality of services
37

Team Based Pharmacy Services Model with Resident Capacity Expansion
• Roles and responsibilities
– Team Leader (Clinical specialist or Point‐of‐Care Pharmacist)
• Manage daily workflow and assignments of teamManage daily workflow and assignments of team members
– Operational
– Clinical programs and services
– Education (students/residents/staff)
• Lead team building and support
• Facilitate effective team communication
Team Based Pharmacy Services Model with Resident Capacity Expansion
• Roles and responsibilities
– Clinical Specialist
• Provide direct patient care
• Provide support and mentorship for other membersProvide support and mentorship for other members
• Serve as preceptor of record for residents/students
• Share in precepting of all residents/students
• Support institutional service (drug policy and formulary management, quality assurance, committee representation)
• Lead research efforts
Team Based Pharmacy Services Model with Resident Capacity Expansion
• Roles and responsibilities– Point‐of‐Care Pharmacist
• Provide direct patient care
• Assume lead responsibility for prospective medication order review and verificationreview and verification
• Direct priorities and activities of pharmacist extender
• Serve as preceptor of record for residents and students
• Share in precepting of all residents and students
• Support team based education and research
• Participate in institutional service
• Provide support and mentorship for other team members
38

Team Based Pharmacy Services Model with Resident Capacity Expansion
• Roles and responsibilities
– PGY1 Resident
• Provide direct patient care– Patient education
– Medication reconciliation
– Discharge follow up phone calls
– Participate in program – oriented services (anticoagulation management, diabetes management, therapeutic drug monitoring, readmission and care transition programs)
• Assume lead responsibility for prospective medication order review and verification
Team Based Pharmacy Services Model with Resident Capacity Expansion
• Roles and responsibilities
– PGY1 Resident
• Direct priorities and activities of pharmacist extender
• Assist in precepting studentsAssist in precepting students
– Resource for questions
– Lead topic discussions
• Support team based education and research
• Participate in institutional service
• Provide support and mentorship for other team members
Team Based Pharmacy Services Model with Resident Capacity Expansion
• Roles and responsibilities
– APPE student(s)
• Provide direct patient care– Medication reconciliation
– Patient education
• Support team based education
• Participate in team research projects – Data collection
– Data analysis
39

Team Based Pharmacy Services Model with Resident Capacity Expansion
• Roles and responsibilities
– Pharmacist Extender (CPHT)
• Collect medication history information
• Support team quality improvement and researchSupport team quality improvement and research projects (data collection)
• Assists in identification of patient’s own meds
• Facilitates missing dose requests
• Monitors continuous infusion replacements
• Verifies selected medication orders– Discontinued orders
Team Based Pharmacy Services Model with Resident Capacity Expansion
• Integrated Practice Rotation Description– A 3 month block experience within one of the pharmacy divisions. – Residents are expected to provide patient‐care services within the
divisional team‐based/integrated model of care. – The resident will be exposed to and expected to perform a variety of
roles and responsibilities expected of a pharmacist practicing in this model This may include but is not limited to:model. This may include, but is not limited to:
• Attending and actively participating in patient care rounds with the multi‐professional team
• Performing order review and verification for assigned patients• Participating in program‐oriented services (such as: anticoagulation,
therapeutic drug monitoring, readmission reduction and transition of care programs, or others)
• Providing drug information and education • Participating in patient safety initiatives, or • Performing any other functions expected of a pharmacist.
Team Based Pharmacy Services Model with Resident Capacity Expansion
• Integrated Practice Rotation – RLS Objectives
– Establish a collaborative, professional relationship with other team members; become an integral member of the health care team and attend patient care rounds, with the entire interdisciplinary team on a daily basis (Goals R2 1entire interdisciplinary team, on a daily basis. (Goals R2.1, R3.1, E4.1, E7.2)
– Perform the role of the Point of Care and/or centralized/coordinator pharmacist in the order review and drug distribution process. (Goals R1.3, R1.4, R1.5, R2.1‐2.4, R2.6‐2.12, R3.1, E7.2, E7.4)
– Prioritize patient care responsibilities appropriately. (Goals R2.2, E7.4)
40

Team Based Pharmacy Services Model with Resident Capacity Expansion
• Integrated Practice Rotation – RLS Objectives
– Assume responsibility for providing and optimizing pharmaceutical care to assigned patients in collaboration with the team by identifying drug‐related problems, identifying goals of therapy, and designing and implementing therapeutic recommendations and monitoring plans. (Goals R2 1‐2 4 R2 6‐2 12 R3 1 E7 2 E7 4)(Goals R2.1 2.4, R2.6 2.12 R3.1, E7.2, E7.4)
– Design an appropriate medication regimen by utilizing patient specific information and identifying specific therapeutic and long term management goals; present this information to other team members. (Goals R2.2, R2.4, R2.7, R2.8, R2.9, R2.10, E4.1, E7.2)
– Identify opportunities to improve the medication use system, including changes in the dispensing process, and communication with the entire multidisciplinary team. (Goals R1.1, R1.2, R1.3, R1.4)
– Provide education to pharmacy staff and/or other health care providers. (Goals R2.1, E7.2)
Discussion: Innovative Resident Roles and Services
20 minutes
Interactive Debate (Breakout Sessions)( )
50 minutes
41

Instructions
• Divide into groups of 6
• Take a pro or con stance on assigned issue
• 3 minute report back to the group on di i ddiscussion and consensus
Pro vs. Con Debate #1
In working to expand your residency program, there is value in converting existing pharmacist or technician positions to pharmacy resident positions…..explain your position
Pro vs. Con Debate #2
In the optimal pharmacy practice model, pharmacy residents should be expected to play a significant role in precepting pharmacy students….if yes, explain the role of the resident versus the preceptor
42

Pro vs. Con Debate #3
In pharmacy residency training models of the future, PGY1 pharmacy residents should spend more time learning within an integrated practice model environment…
Pro vs. Con Debate #4
Resident professional practice experience (e.g.; staffing) should be a minimum of 16 hours per week on average…
Pro vs. Con Debate #5
Residents should be required to take after‐hour (e.g. 3rd shift) on call shifts as part of their training program…
43

Sixteenth Annual ASHP Conference
for Leaders in Health-System Pharmacy REFERENCES Knapp KK, Shah BM, Kim HBK et al. Visions for required postgraduate year 1 residency training by 2020: a comparison of actual versus projected expansion. Pharmacotherapy. 2009;29:1030-38.
Miller DE, Woller TW. Understanding reimbursement for pharmacy residents. Am J Health-Syst Pharm. 1998; 55:1620-3.
Pasek PA, Stephens C. Return on investment of pharmacy residency training program. Am J Health-Syst Pharm. 2010;67:1952-57.
Pharmacy Practice Model for Academic Medical Centers. University Hospital Consortium, Oak Brook, IL. May 2010.
Shane R. Critical requirements for health-system pharmacy practice models that achieve optimal use of medications. Am J Health-Syst Pharm. 2011;68:1101-11.
Smith KM, Sorensen T, Connor KA et al. Value of conducting pharmacy residency training – the organizational perspective. Pharmacotherapy. 2010; 30:490e-510e.
The consensus of the Pharmacy Practice Model Summit. Am J Health-Syst Pharm. 2011;68:1148-52.
http://www.ashp.org/menu/Accreditation/Resources/Residency-Capacity-Conference.aspx. Accessed September 3, 2011.
http://www.ashp.org/DocLibrary/Accreditation/PRC2011/Current-Landscape.aspx. Accessed September 3, 2011.
http://www.ashp.org/DocLibrary/Accreditation/PRC2011/Trends-in-Healthcare.aspx. Accessed September 3, 2011.
http://www.ashp.org/DocLibrary/Accreditation/PRC2011/Perspectives-from-the-Medical-Model.aspx. Accessed September 3, 2011.
46