
WorkReady Online Application Signature...
16
WorkReady Online Application Signature Page Revised 1.18.2018 Instructions: Please read the statements below and acknowledge by signing in the appropriate places. If you are under 18, you must also obtain the signature of a parent or guardian. Print this page and bring it with you to your enrollment appointment. Application Statement I do hereby authorize Philadelphia Youth Network (PYN) and its agents and partners to make inquiries regarding my qualifications for work and my job readiness. I also grant permission to verify income information and, where necessary, to document my eligibility for services. I authorize the release of personal, financial, or academic information to PYN by organizations including, but not limited to: schools, employers, youth-serving organizations and government agencies (including the Department of Public Welfare) for the purpose of determining income and programmatic eligibility and by PYN to its agents and partners in the course of attempting to secure placement for me. I certify that the information provided is true to the best of my knowledge. I am aware that the information I have provided is subject to review and verification (including wage records and employment information) and that I may have to provide documentation to support the information provided. I am also aware that I will be immediately removed from my placement if I am found ineligible after enrollment and may be prosecuted for fraud and/or perjury. I allow release of this information for verification purposes and understand that it will be used to determine eligibility. Equal Employment Opportunity Here is some information about your EQUAL EMPLOYMENT OPPORTUNITY RIGHTS UNDER FEDERAL LAW. The Philadelphia Youth Network is prohibited from discriminating on the grounds of race, color, religion, sex, national origin, age, disability, political affiliation or belief, and, for beneficiaries only, citizenship, or participation in federally funded programs, as amended in admission or access to, opportunity or treatment, in, or employment in the administration of or in connection with any federally funded activity. If you think that you have been subjected to discrimination under a federally funded program or activity, you may file a complaint within 180-days from the date of the alleged violation with the Department of Labor and Industry’s (L&I) Office of Affirmative Action (OAA), or you may file a complaint directly with the Director, Civil Rights Center (CRC), U.S. Department of Labor, 200 Constitution Avenue, N.W., Room N-4123, Washington, DC 20210. If you elect to file your complaint with the Office of Affirmative Action, you must wait until the Office of Affirmative Action issues a decision or until 60-days have passed, whichever is sooner, before filing with the CRC (see above address). If the OAA has not provided you with a written decision within 60- days of filing of the complaint, you need not wait for a decision to be issued, but may file a complaint with CRC within 30-days of the expiration of the 60- day period. If you are dissatisfied with the OAA’s resolution of your complaint, you may file a complaint with CRC. Such a complaint should be filed within 30-days of the date you receive notice of the OAA’s proposed resolution. If you have any questions, regarding YOUR CIVIL RIGHTS, or to file a discrimination complaint, please contact: The Department of Labor and Industry, Office of Equal Opportunity – Room 514, Labor and Industry Building, Seventh and Forster Streets, Harrisburg, Pennsylvania 17120. Or Call (717) 787-1182 • 1-800-622-5422 • TDD 1-800-654-5984. Also, a complaint can be filed by phone or in person at the local office. U.S. Equal Employment Opportunity Commission, 801 Market Street, Suite 1300 , Philadelphia, PA 19107-3127. For general inquiries or to begin the process of filing a complaint of discrimination, call 1-800-669-4000. All complaints will be handled confidentially. Waiver and Release The Philadelphia Youth Network, Inc. (PYN) from time to time creates promotional and educational materials about PYN, its programs and WorkReady Philadelphia. In consideration of the opportunity to participate in the programs offered by the Philadelphia Youth Network, I hereby give permission to PYN, its employees, affiliates, representatives, contractors, agents and members of the media to interview, audiotape, photograph, videotape, film, or capture by any other electronic or other means my image and speech, and, within its absolute discretion, to release, disseminate, or use, in any manner it sees fit including publications and web pages, the resulting images and testimonials and any other information contained therein for the purpose of promoting the objectives of PYN, its programs and WorkReady Philadelphia. I hereby release any and all actions and claims which I, my family members, my child, our heirs, executors or administrators may have against the Philadelphia Youth Network, Inc., its employees, affiliates, representatives, contractors, agents, successors and assigns, arising for any reason whatsoever from the use, publication, distribution, or republication of the words or images gathered for the purpose described above. I intend this to be a legally binding agreement. BUCKLEY AMENDMENT: Consent for Release of Information WorkReady Philadelphia programs are designed to provide participating youth with meaningful learning experiences, including preparation for the workplace and higher education opportunities, and success in school. So that we may ensure that our youth’s needs be fully met, it is helpful to track their performance in school through grades, standardized tests, achievement levels, and other relevant records. Please read the following statement, and sign below to indicate that you agree to allow your/your child’s school to release these records to the Philadelphia Youth Network (PYN) and its partners for use throughout the program. I understand that the Buckley Amendment to the Family Education Rights and Privacy Act of 1974 guarantees that my/my child’s academic record will not be discussed with or disclosed to any third party without my written consent. I hereby authorize officials of the School District of Philadelphia to release my/my child’s educational records (limited to: standardized tests, graduation and promotion information, and copies of report cards) only to PYN and to any corresponding partner agency or agencies with which I/my child will be placed by PYN. This consent will last until I /my child is no longer enrolled in a PYN-sponsored activity or until I rescind this consent in writing. I understand that this information will not be provided to any entity other than those indicated above. I understand that a record will be maintained in my/my child’s educational records, indicating that the information was provided. I understand that I may acquire a copy of this record, as well as of any records provided to PYN, from the Philadelphia School District. Acknowledgement - Instructions: Please read and sign below. Mark (x) the appropriate box below only if you DO NOT accept the statements above. Waiver and Release I DO NOT give permission to PYN, its employees, affiliates, representatives, contractors, agents and members of the media to use my images or speech. Buckley Amendment I DO NOT agree to the terms of this release form. EEO - STATEMENT OF RECEIPT: I hereby Certify that I have received, read and understand my rights under law and acknowledge this with my signature. ________________________________________________________________________________________________________________________________________ Printed Name of Participant Signature of Participant Date signed ________________________________________________________________________________________________________________________________________ Printed Name of Parent/Guardian Signature of Parent/Guardian Date signed
Transcript of WorkReady Online Application Signature...
WorkReady Online Application Signature Page
Revised 1.18.2018
Instructions: Please read the statements below and acknowledge by signing in the appropriate places. If you are under 18, you must also obtain the signature of a parent or guardian. Print this page and bring it with you to your enrollment appointment.
Application Statement I do hereby authorize Philadelphia Youth Network (PYN) and its agents and partners to make inquiries regarding my qualifications for work and my job readiness. I also grant permission to verify income information and, where necessary, to document my eligibility for services. I authorize the release of personal, financial, or academic information to PYN by organizations including, but not limited to: schools, employers, youth-serving organizations and government agencies (including the Department of Public Welfare) for the purpose of determining income and programmatic eligibility and by PYN to its agents and partners in the course of attempting to secure placement for me. I certify that the information provided is true to the best of my knowledge. I am aware that the information I have provided is subject to review and verification (including wage records and employment information) and that I may have to provide documentation to support the information provided. I am also aware that I will be immediately removed from my placement if I am found ineligible after enrollment and may be prosecuted for fraud and/or perjury. I allow release of this information for verification purposes and understand that it will be used to determine eligibility.
Equal Employment Opportunity Here is some information about your EQUAL EMPLOYMENT OPPORTUNITY RIGHTS UNDER FEDERAL LAW. The Philadelphia Youth Network is prohibited from discriminating on the grounds of race, color, religion, sex, national origin, age, disability, political affiliation or belief, and, for beneficiaries only, citizenship, or participation in federally funded programs, as amended in admission or access to, opportunity or treatment, in, or employment in the administration of or in connection with any federally funded activity. If you think that you have been subjected to discrimination under a federally funded program or activity, you may file a complaint within 180-days from the date of the alleged violation with the Department of Labor and Industry’s (L&I) Office of Affirmative Action (OAA), or you may file a complaint directly with the Director, Civil Rights Center (CRC), U.S. Department of Labor, 200 Constitution Avenue, N.W., Room N-4123, Washington, DC 20210. If you elect to file your complaint with the Office of Affirmative Action, you must wait until the Office of Affirmative Action issues a decision or until 60-days have passed, whichever is sooner, before filing with the CRC (see above address). If the OAA has not provided you with a written decision within 60- days of filing of the complaint, you need not wait for a decision to be issued, but may file a complaint with CRC within 30-days of the expiration of the 60- day period. If you are dissatisfied with the OAA’s resolution of your complaint, you may file a complaint with CRC. Such a complaint should be filed within 30-days of the date you receive notice of the OAA’s proposed resolution. If you have any questions, regarding YOUR CIVIL RIGHTS, or to file a discrimination complaint, please contact: The Department of Labor and Industry, Office of Equal Opportunity – Room 514, Labor and Industry Building, Seventh and Forster Streets, Harrisburg, Pennsylvania 17120. Or Call (717) 787-1182 • 1-800-622-5422 • TDD 1-800-654-5984. Also, a complaint can be filed by phone or in person at the local office. U.S. Equal Employment O pport unity Commission, 801 Ma rket Street , Sui t e 1300 , Philadelphia, PA 19107-3127. For general inquiries or to begin the process of filing a complaint of discrimination, call 1-800-669-4000. All complaints will be handled confidentially.
Waiver and Release The Philadelphia Youth Network, Inc. (PYN) from time to time creates promotional and educational materials about PYN, its programs and WorkReady Philadelphia. In consideration of the opportunity to participate in the programs offered by the Philadelphia Youth Network, I hereby give permission to PYN, its employees, affiliates, representatives, contractors, agents and members of the media to interview, audiotape, photograph, videotape, film, or capture by any other electronic or other means my image and speech, and, within its absolute discretion, to release, disseminate, or use, in any manner it sees fit including publications and web pages, the resulting images and testimonials and any other information contained therein for the purpose of promoting the objectives of PYN, its programs and WorkReady Philadelphia. I hereby release any and all actions and claims which I, my family members, my child, our heirs, executors or administrators may have against the Philadelphia Youth Network, Inc., its employees, affiliates, representatives, contractors, agents, successors and assigns, arising for any reason whatsoever from the use, publication, distribution, or republication of the words or images gathered for the purpose described above. I intend this to be a legally binding agreement.
BUCKLEY AMENDMENT: Consent for Release of Information WorkReady Philadelphia programs are designed to provide participating youth with meaningful learning experiences, including preparation for the workplace and higher education opportunities, and success in school. So that we may ensure that our youth’s needs be fully met, it is helpful to track their performance in school through grades, standardized tests, achievement levels, and other relevant records. Please read the following statement, and sign below to indicate that you agree to allow your/your child’s school to release these records to the Philadelphia Youth Network (PYN) and its partners for use throughout the program. I understand that the Buckley Amendment to the Family Education Rights and Privacy Act of 1974 guarantees that my/my child’s academic record will not be discussed with or disclosed to any third party without my written consent. I hereby authorize officials of the School District of Philadelphia to release my/my child’s educational records (limited to: standardized tests, graduation and promotion information, and copies of report cards) only to PYN and to any corresponding partner agency or agencies with which I/my child will be placed by PYN. This consent will last until I /my child is no longer enrolled in a PYN-sponsored activity or until I rescind this consent in writing. I understand that this information will not be provided to any entity other than those indicated above. I understand that a record will be maintained in my/my child’s educational records, indicating that the information was provided. I understand that I may acquire a copy of this record, as well as of any records provided to PYN, from the Philadelphia School District.
Acknowledgement - Instructions: Please read and sign below. Mark (x) the appropriate box below only if you DO NOT accept the statements above.
Waiver and Release I DO NOT give permission to PYN, its employees, affiliates, representatives, contractors, agents and members of the media to use my images or speech.
Buckley Amendment I DO NOT agree to the terms of this release form.
EEO - STATEMENT OF RECEIPT: I hereby Certify that I have received, read and understand my rights under law and acknowledge this with my signature.
________________________________________________________________________________________________________________________________________ Printed Name of Participant Signature of Participant Date signed
________________________________________________________________________________________________________________________________________ Printed Name of Parent/Guardian Signature of Parent/Guardian Date signed
lwilliams
Highlight
lwilliams
Highlight

Form W-4 (2018)Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/FormW4.Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes.Exemption from withholding. You may claim exemption from withholding for 2018 if both of the following apply.• For 2017 you had a right to a refund of all federal income tax withheld because you had no tax liability, and• For 2018 you expect a refund of all federal income tax withheld because you expect to have no tax liability.If you’re exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2018 expires February 15, 2019. See Pub. 505, Tax Withholding and Estimated Tax, to learn more about whether you qualify for exemption from withholding.
General InstructionsIf you aren’t exempt, follow the rest of these instructions to determine the number of withholding allowances you should claim for withholding for 2018 and any additional amount of tax to have withheld. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages.
You can also use the calculator at www.irs.gov/W4App to determine your tax withholding more accurately. Consider
using this calculator if you have a more complicated tax situation, such as if you have a working spouse, more than one job, or a large amount of nonwage income outside of your job. After your Form W-4 takes effect, you can also use this calculator to see how the amount of tax you’re having withheld compares to your projected total tax for 2018. If you use the calculator, you don’t need to complete any of the worksheets for Form W-4.
Note that if you have too much tax withheld, you will receive a refund when you file your tax return. If you have too little tax withheld, you will owe tax when you file your tax return, and you might owe a penalty.Filers with multiple jobs or working spouses. If you have more than one job at a time, or if you’re married and your spouse is also working, read all of the instructions including the instructions for the Two-Earners/Multiple Jobs Worksheet before beginning. Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you might owe additional tax. Or, you can use the Deductions, Adjustments, and Other Income Worksheet on page 3 or the calculator at www.irs.gov/W4App to make sure you have enough tax withheld from your paycheck. If you have pension or annuity income, see Pub. 505 or use the calculator at www.irs.gov/W4App to find out if you should adjust your withholding on Form W-4 or W-4P. Nonresident alien. If you’re a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form.
Specific InstructionsPersonal Allowances WorksheetComplete this worksheet on page 3 first to determine the number of withholding allowances to claim.Line C. Head of household please note: Generally, you can claim head of household filing status on your tax return only if you’re unmarried and pay more than 50% of the costs of keeping up a home for yourself and a qualifying individual. See Pub. 501 for more information about filing status.Line E. Child tax credit. When you file your tax return, you might be eligible to claim a credit for each of your qualifying children. To qualify, the child must be under age 17 as of December 31 and must be your dependent who lives with you for more than half the year. To learn more about this credit, see Pub. 972, Child Tax Credit. To reduce the tax withheld from your pay by taking this credit into account, follow the instructions on line E of the worksheet. On the worksheet you will be asked about your total income. For this purpose, total income includes all of your wages and other income, including income earned by a spouse, during the year.Line F. Credit for other dependents. When you file your tax return, you might be eligible to claim a credit for each of your dependents that don’t qualify for the child tax credit, such as any dependent children age 17 and older. To learn more about this credit, see Pub. 505. To reduce the tax withheld from your pay by taking this credit into account, follow the instructions on line F of the worksheet. On the worksheet, you will be asked about your total income. For this purpose, total income includes all of
Separate here and give Form W-4 to your employer. Keep the worksheet(s) for your records.
Form W-4Department of the Treasury Internal Revenue Service
Employee’s Withholding Allowance Certificate▶ Whether you’re entitled to claim a certain number of allowances or exemption from withholding is
subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
OMB No. 1545-0074
20181 Your first name and middle initial Last name
Home address (number and street or rural route)
City or town, state, and ZIP code
2 Your social security number
3 Single Married Married, but withhold at higher Single rate.
Note: If married filing separately, check “Married, but withhold at higher Single rate.”
4 If your last name differs from that shown on your social security card,
check here. You must call 800-772-1213 for a replacement card. ▶
5 Total number of allowances you’re claiming (from the applicable worksheet on the following pages) . . . 56 Additional amount, if any, you want withheld from each paycheck . . . . . . . . . . . . . . 6 $7 I claim exemption from withholding for 2018, and I certify that I meet both of the following conditions for exemption.
• Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and• This year I expect a refund of all federal income tax withheld because I expect to have no tax liability.If you meet both conditions, write “Exempt” here . . . . . . . . . . . . . . . ▶ 7
Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete.
Employee’s signature (This form is not valid unless you sign it.) ▶ Date ▶
8 Employer’s name and address (Employer: Complete boxes 8 and 10 if sending to IRS and complete boxes 8, 9, and 10 if sending to State Directory of New Hires.)
9 First date of employment
10 Employer identification number (EIN)
For Privacy Act and Paperwork Reduction Act Notice, see page 4. Cat. No. 10220Q Form W-4 (2018)
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight
mhegarty
Highlight

Form W-4 (2018) Page 2
your wages and other income, including income earned by a spouse, during the year.Line G. Other credits. You might be able to reduce the tax withheld from your paycheck if you expect to claim other tax credits, such as the earned income tax credit and tax credits for education and child care expenses. If you do so, your paycheck will be larger but the amount of any refund that you receive when you file your tax return will be smaller. Follow the instructions for Worksheet 1-6 in Pub. 505 if you want to reduce your withholding to take these credits into account.
Deductions, Adjustments, and Additional Income WorksheetComplete this worksheet to determine if you’re able to reduce the tax withheld from your paycheck to account for your itemized deductions and other adjustments to income such as IRA contributions. If you do so, your refund at the end of the year will be smaller, but your paycheck will be larger. You’re not required to complete this worksheet or reduce your withholding if you don’t wish to do so.
You can also use this worksheet to figure out how much to increase the tax withheld from your paycheck if you have a large amount of nonwage income, such as interest or dividends.
Another option is to take these items into account and make your withholding more accurate by using the calculator at www.irs.gov/W4App. If you use the calculator, you don’t need to complete any of the worksheets for Form W-4.
Two-Earners/Multiple Jobs WorksheetComplete this worksheet if you have more
than one job at a time or are married filing jointly and have a working spouse. If you don’t complete this worksheet, you might have too little tax withheld. If so, you will owe tax when you file your tax return and might be subject to a penalty.
Figure the total number of allowances you’re entitled to claim and any additional amount of tax to withhold on all jobs using worksheets from only one Form W-4. Claim all allowances on the W-4 that you or your spouse file for the highest paying job in your family and claim zero allowances on Forms W-4 filed for all other jobs. For example, if you earn $60,000 per year and your spouse earns $20,000, you should complete the worksheets to determine what to enter on lines 5 and 6 of your Form W-4, and your spouse should enter zero (“-0-”) on lines 5 and 6 of his or her Form W-4. See Pub. 505 for details.
Another option is to use the calculator at www.irs.gov/W4App to make your withholding more accurate.Tip: If you have a working spouse and your incomes are similar, you can check the “Married, but withhold at higher Single rate” box instead of using this worksheet. If you choose this option, then each spouse should fill out the Personal Allowances Worksheet and check the “Married, but withhold at higher Single rate” box on Form W-4, but only one spouse should claim any allowances for credits or fill out the Deductions, Adjustments, and Additional Income Worksheet.
Instructions for EmployerEmployees, do not complete box 8, 9, or 10. Your employer will complete these boxes if necessary.New hire reporting. Employers are
required by law to report new employees to a designated State Directory of New Hires. Employers may use Form W-4, boxes 8, 9, and 10 to comply with the new hire reporting requirement for a newly hired employee. A newly hired employee is an employee who hasn’t previously been employed by the employer, or who was previously employed by the employer but has been separated from such prior employment for at least 60 consecutive days. Employers should contact the appropriate State Directory of New Hires to find out how to submit a copy of the completed Form W-4. For information and links to each designated State Directory of New Hires (including for U.S. territories), go to www.acf.hhs.gov/programs/css/employers.
If an employer is sending a copy of Form W-4 to a designated State Directory of New Hires to comply with the new hire reporting requirement for a newly hired employee, complete boxes 8, 9, and 10 as follows. Box 8. Enter the employer’s name and address. If the employer is sending a copy of this form to a State Directory of New Hires, enter the address where child support agencies should send income withholding orders. Box 9. If the employer is sending a copy of this form to a State Directory of New Hires, enter the employee’s first date of employment, which is the date services for payment were first performed by the employee. If the employer rehired the employee after the employee had been separated from the employer’s service for at least 60 days, enter the rehire date.Box 10. Enter the employer’s employer identification number (EIN).
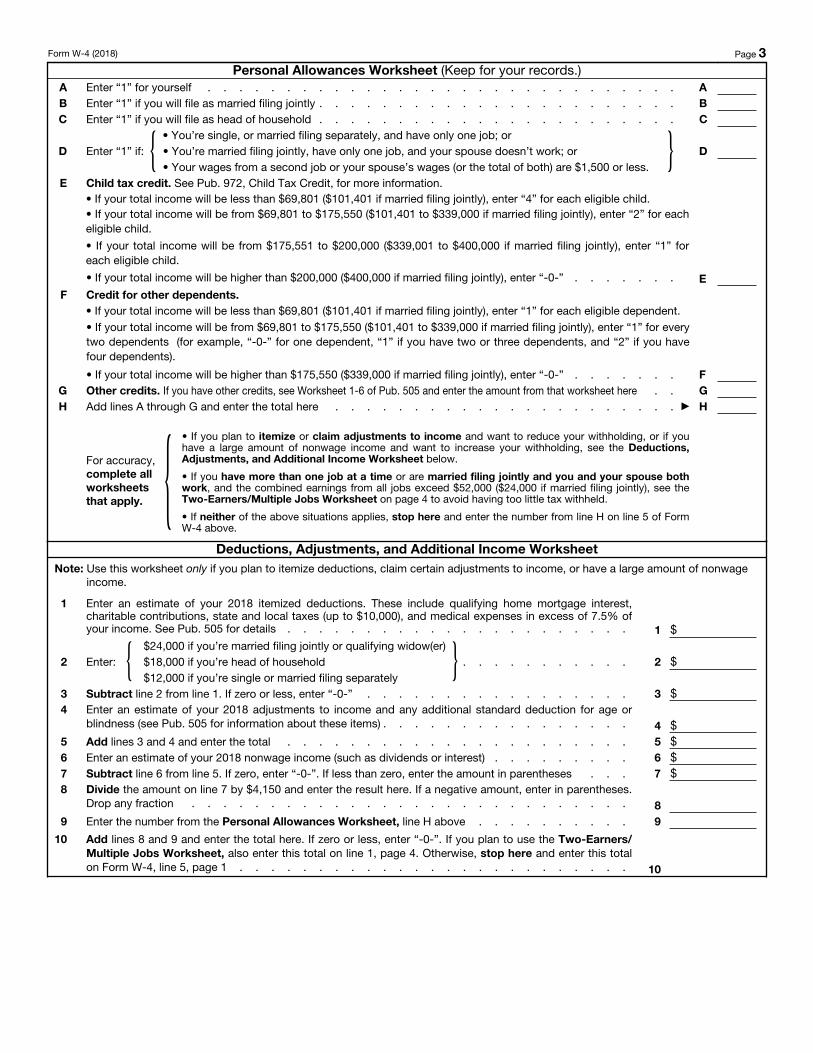
Form W-4 (2018) Page 3Personal Allowances Worksheet (Keep for your records.)
A Enter “1” for yourself . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . AB Enter “1” if you will file as married filing jointly . . . . . . . . . . . . . . . . . . . . . . . BC Enter “1” if you will file as head of household . . . . . . . . . . . . . . . . . . . . . . . C
D Enter “1” if: { • You’re single, or married filing separately, and have only one job; or• You’re married filing jointly, have only one job, and your spouse doesn’t work; or• Your wages from a second job or your spouse’s wages (or the total of both) are $1,500 or less.
} D
E Child tax credit. See Pub. 972, Child Tax Credit, for more information.• If your total income will be less than $69,801 ($101,401 if married filing jointly), enter “4” for each eligible child. • If your total income will be from $69,801 to $175,550 ($101,401 to $339,000 if married filing jointly), enter “2” for each eligible child.
• If your total income will be from $175,551 to $200,000 ($339,001 to $400,000 if married filing jointly), enter “1” for each eligible child.
• If your total income will be higher than $200,000 ($400,000 if married filing jointly), enter “-0-” . . . . . . . EF Credit for other dependents.
• If your total income will be less than $69,801 ($101,401 if married filing jointly), enter “1” for each eligible dependent. • If your total income will be from $69,801 to $175,550 ($101,401 to $339,000 if married filing jointly), enter “1” for every two dependents (for example, “-0-” for one dependent, “1” if you have two or three dependents, and “2” if you have four dependents).
• If your total income will be higher than $175,550 ($339,000 if married filing jointly), enter “-0-” . . . . . . . FG Other credits. If you have other credits, see Worksheet 1-6 of Pub. 505 and enter the amount from that worksheet here . . GH Add lines A through G and enter the total here . . . . . . . . . . . . . . . . . . . . . . ▶ H
For accuracy, complete all worksheets that apply. {
• If you plan to itemize or claim adjustments to income and want to reduce your withholding, or if you have a large amount of nonwage income and want to increase your withholding, see the Deductions, Adjustments, and Additional Income Worksheet below.
• If you have more than one job at a time or are married filing jointly and you and your spouse both work, and the combined earnings from all jobs exceed $52,000 ($24,000 if married filing jointly), see the Two-Earners/Multiple Jobs Worksheet on page 4 to avoid having too little tax withheld.
• If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 above.
Deductions, Adjustments, and Additional Income WorksheetNote: Use this worksheet only if you plan to itemize deductions, claim certain adjustments to income, or have a large amount of nonwage
income.
1
Enter an estimate of your 2018 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes (up to $10,000), and medical expenses in excess of 7.5% of your income. See Pub. 505 for details . . . . . . . . . . . . . . . . . . . . . . 1 $
2 Enter: { $24,000 if you’re married filing jointly or qualifying widow(er)$18,000 if you’re head of household$12,000 if you’re single or married filing separately
} . . . . . . . . . . . 2 $
3 Subtract line 2 from line 1. If zero or less, enter “-0-” . . . . . . . . . . . . . . . . . 3 $4 Enter an estimate of your 2018 adjustments to income and any additional standard deduction for age or
blindness (see Pub. 505 for information about these items) . . . . . . . . . . . . . . . . 4 $5 Add lines 3 and 4 and enter the total . . . . . . . . . . . . . . . . . . . . . . 5 $6 Enter an estimate of your 2018 nonwage income (such as dividends or interest) . . . . . . . . . 6 $7 Subtract line 6 from line 5. If zero, enter “-0-”. If less than zero, enter the amount in parentheses . . . 7 $8 Divide the amount on line 7 by $4,150 and enter the result here. If a negative amount, enter in parentheses.
Drop any fraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89 Enter the number from the Personal Allowances Worksheet, line H above . . . . . . . . . . 9
10
Add lines 8 and 9 and enter the total here. If zero or less, enter “-0-”. If you plan to use the Two-Earners/Multiple Jobs Worksheet, also enter this total on line 1, page 4. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 . . . . . . . . . . . . . . . . . . . . . . . . . 10

Form W-4 (2018) Page 4 Two-Earners/Multiple Jobs Worksheet
Note: Use this worksheet only if the instructions under line H from the Personal Allowances Worksheet direct you here.
1 Enter the number from the Personal Allowances Worksheet, line H, page 3 (or, if you used the Deductions, Adjustments, and Additional Income Worksheet on page 3, the number from line 10 of that worksheet) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you’re married filing jointly and wages from the highest paying job are $75,000 or less and the combined wages for you and your spouse are $107,000 or less, don’t enter more than “3” . . . . . . . . . . . . . 2
3 If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter “-0-”) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet . . . . . . . . . . . . 3
Note: If line 1 is less than line 2, enter “-0-” on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill.
4 Enter the number from line 2 of this worksheet . . . . . . . . . . . 45 Enter the number from line 1 of this worksheet . . . . . . . . . . . 56 Subtract line 5 from line 4 . . . . . . . . . . . . . . . . . . . . . . . . . . 67 Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here . . . . . 7 $8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed . . . 8 $
9
Divide line 8 by the number of pay periods remaining in 2018. For example, divide by 18 if you’re paid every 2 weeks and you complete this form on a date in late April when there are 18 pay periods remaining in 2018. Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 $
Table 1Married Filing Jointly
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $5,000 05,001 - 9,500 19,501 - 19,000 2
19,001 - 26,500 326,501 - 37,000 437,001 - 43,500 543,501 - 55,000 655,001 - 60,000 760,001 - 70,000 870,001 - 75,000 975,001 - 85,000 1085,001 - 95,000 1195,001 - 130,000 12
130,001 - 150,000 13150,001 - 160,000 14160,001 - 170,000 15170,001 - 180,000 16180,001 - 190,000 17190,001 - 200,000 18200,001 and over 19
All Others
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $7,000 07,001 - 12,500 1
12,501 - 24,500 224,501 - 31,500 331,501 - 39,000 439,001 - 55,000 555,001 - 70,000 670,001 - 85,000 785,001 - 90,000 890,001 - 100,000 9
100,001 - 105,000 10105,001 - 115,000 11115,001 - 120,000 12120,001 - 130,000 13130,001 - 145,000 14145,001 - 155,000 15155,001 - 185,000 16185,001 and over 17
Table 2Married Filing Jointly
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $24,375 $42024,376 - 82,725 50082,726 - 170,325 910
170,326 - 320,325 1,000320,326 - 405,325 1,330405,326 - 605,325 1,450605,326 and over 1,540
All Others
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $7,000 $4207,001 - 36,175 500
36,176 - 79,975 91079,976 - 154,975 1,000
154,976 - 197,475 1,330197,476 - 497,475 1,450497,476 and over 1,540
Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and
U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism.
You aren’t required to provide the information requested on a form that’s subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be
retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section 6103.
The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return.
If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.

USCIS Form I-9
OMB No. 1615-0047 Expires 08/31/2019
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Form I-9 07/17/17 N Page 1 of 3
►START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically,during completion of this form. Employers are liable for errors in the completion of this form.
ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no laterthan the first day of employment, but not before accepting a job offer.)Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any)
Address (Street Number and Name) Apt. Number City or Town State ZIP Code
Date of Birth (mm/dd/yyyy) U.S. Social Security Number
- -
Employee's E-mail Address Employee's Telephone Number
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.I attest, under penalty of perjury, that I am (check one of the following boxes):
1. A citizen of the United States
2. A noncitizen national of the United States (See instructions)
3. A lawful permanent resident
4. An alien authorized to work until (See instructions)
(expiration date, if applicable, mm/dd/yyyy):
(Alien Registration Number/USCIS Number):
Some aliens may write "N/A" in the expiration date field.
Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number.
1. Alien Registration Number/USCIS Number:
2. Form I-94 Admission Number:
3. Foreign Passport Number:
Country of Issuance:
OR
OR
QR Code - Section 1 Do Not Write In This Space
Signature of Employee Today's Date (mm/dd/yyyy)
Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1.(Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.)I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct.Signature of Preparer or Translator Today's Date (mm/dd/yyyy)
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code
Employer Completes Next Page
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
mhegarty
Highlight
mhegarty
Highlight
Form I-9 07/17/17 N Page 2 of 3
USCIS Form I-9
OMB No. 1615-0047 Expires 08/31/2019
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.")
Last Name (Family Name) M.I.First Name (Given Name)Employee Info from Section 1
Citizenship/Immigration Status
List AIdentity and Employment Authorization Identity Employment Authorization
OR List B AND List C
Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions)
Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name
Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code
Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.)A. New Name (if applicable)Last Name (Family Name) First Name (Given Name) Middle Initial
B. Date of Rehire (if applicable)Date (mm/dd/yyyy)
Document Title Document Number Expiration Date (if any) (mm/dd/yyyy)
C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below.
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative
400 Market Street Suite 200 Philadelphia PA 19106
Philadelphia Youth Network
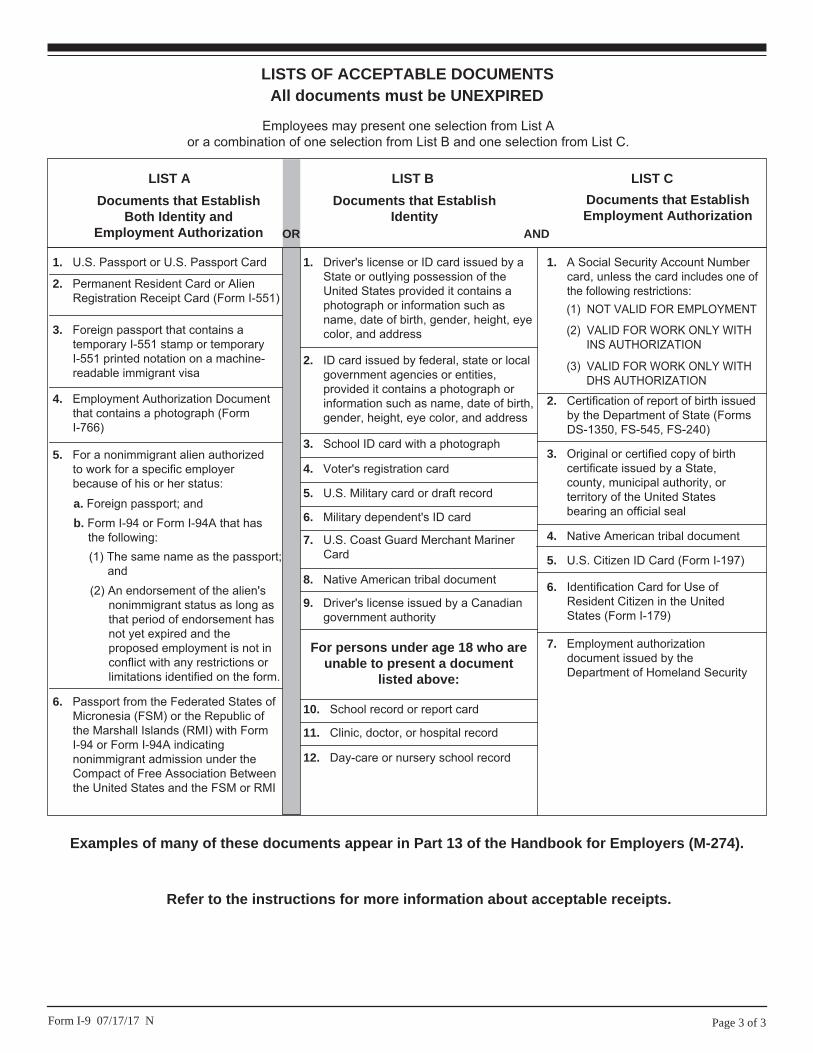
LISTS OF ACCEPTABLE DOCUMENTSAll documents must be UNEXPIRED
Employees may present one selection from List A or a combination of one selection from List B and one selection from List C.
LIST A
2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551)
1. U.S. Passport or U.S. Passport Card
3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machine-readable immigrant visa
4. Employment Authorization Document that contains a photograph (Form I-766)
5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status:
Documents that Establish Both Identity and
Employment Authorization
6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI
b. Form I-94 or Form I-94A that has the following:(1) The same name as the passport;
and(2) An endorsement of the alien's
nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form.
a. Foreign passport; and
For persons under age 18 who are unable to present a document
listed above:
1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
9. Driver's license issued by a Canadian government authority
3. School ID card with a photograph
6. Military dependent's ID card
7. U.S. Coast Guard Merchant Mariner Card
8. Native American tribal document
10. School record or report card
11. Clinic, doctor, or hospital record
12. Day-care or nursery school record
2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
4. Voter's registration card
5. U.S. Military card or draft record
Documents that Establish Identity
LIST B
OR AND
LIST C
7. Employment authorization document issued by the Department of Homeland Security
1. A Social Security Account Number card, unless the card includes one of the following restrictions:
2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240)
3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal
4. Native American tribal document
6. Identification Card for Use of Resident Citizen in the United States (Form I-179)
Documents that Establish Employment Authorization
5. U.S. Citizen ID Card (Form I-197)
(2) VALID FOR WORK ONLY WITH INS AUTHORIZATION
(3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION
(1) NOT VALID FOR EMPLOYMENT
Page 3 of 3Form I-9 07/17/17 N
Examples of many of these documents appear in Part 13 of the Handbook for Employers (M-274).
Refer to the instructions for more information about acceptable receipts.
RESIDENCY CERTIFICATION FORMLocal Earned Income Tax Withholding
EMPLOYEE INFORMATION – RESIDENCE LOCATION
TO EMPLOYERS/TAXPAYERS:
This form is to be used by employers and/or taxpayers to report essential information for the collection and distribution of Local Earned Income Taxes
to the local EIT collector. This form must be utilized by employers when a new employee is hired or when a current employee notifies employer
of a name and/or address change. Use the Address Search Application at www.newPA.com/Act32 to determine PSD codes, EIT rates and
tax collector contact information.
NAME (Last Name, First Name, Middle Initial) SOCIAL SECURITY NUMBER
STREET ADDRESS (No PO Box, RD or RR)
ADDRESS LINE 2
CITY STATE ZIP CODE DAYTIME PHONE NUMBER
CERTIFICATION
SIGNATURE OF EMPLOYEE DATE (MM/DD/YYYY)
PHONE NUMBER EMAIL ADDRESS
MUNICIPALITY (City, Borough or Township)
COUNTY RESIDENT PSD CODE TOTAL RESIDENT EIT RATE
EMPLOYER INFORMATION – EMPLOYMENT LOCATION
EMPLOYER BUSINESS NAME (Use Federal ID Name) EMPLOYER FEIN
STREET ADDRESS WHERE ABOVE EMPLOYEE REPORTS TO WORK (No PO Box, RD or RR)
ADDRESS LINE 2
CITY STATE ZIP CODE PHONE NUMBER
MUNICIPALITY (City, Borough or Township)
COUNTY WORK LOCATION PSD CODE WORK LOCATION NON-RESIDENT EIT RATE
For information on obtaining the appropriate MUNICIPALITY (City, Borough, Township), PSD CODES and EIT (Earned Income Tax) RATES,
please refer to the Pennsylvania Department of Community & Economic Development website:
www.newPA.com/Act32
CLGS-32-6 (6-13)
Under penalties of perjury, I (we) declare that I (we) have examined this information, including all accompanying schedules and statements and to the best of my (our) belief, they are true, correct and complete.
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight

(Must be completed for minors under 16 years of age)*
(This section to be completed by the employer.)
The undersigned parent or legal guardian of , age , (name of minor)
hereby acknowledges and understands that this minor’s employment with
Philadelphia Youth Network , Inc. , commencing , will consist of the following duties and hours:
(name of employer) (date)
(This section to be completed by the employer.)
Duties of minor (e.g., cashier, food service, lifeguard, sales clerk, etc.)
Applicants may be placed in summer work
experiences with duties that could include, but
are not limited to, standard office function and
service projects.
Hours of work:
Sunday .m.- .m.
Monday .m.- .m.
Tuesday .m.- .m.
Wednesday .m.- .m.
Thursday .m.- .m.
Friday .m.- .m.
Saturday .m.- .m.
Other/additional hours (include explanation):
( □ additional sheet(s) attached)
(To be signed by minor’s parent or legal guardian.)
I hereby acknowledge that I understand the above duties and hours to be worked by the above-named minor for this employer and grant permission for this employment. This statement is made subject to the provisions of 18 Pa. C.S. § 4904 (relating to unsworn falsifications to authorities).
□ Parent of (Printed name of parent or legal guardian) □ Legal guardian (Name of minor)
(Signature of parent or legal guardian) (Date) * This form is required to be completed by the parent or legal guardian of a minor employee under 16 years of age pursuant to Section 8(a)(2)(ii) of the Child Labor Act, and the original copy must be kept by the employer at the workplace along with other records of the minor’s employment required by Section 8(d).
LLC-75 01-13
Auxiliary aids and services are available upon request to individuals with disabilities. Equal Opportunity Employer/Program
DEPARTMENT OF LABOR & INDUSTRY BUREAU OF LABOR LAW COMPLIANCE
PARENTAL ACKNOWLEDGEMENT OF MINOR’S DUTIES AND HOURS
OF EMPLOYMENT
STATEMENT OF RECEIPT PARTICIPANT PROCEDURES FORM
I hereby certify that I have received, read and understand the following procedures and policies in the Program Participant Handbook and acknowledge so with my signature.
• Programs Overviews and Guidelines (Participant Handbook pg. 1) • Important Policies and Laws
o Grievance Policy (Participant Handbook pg. 3) o Equal Opportunities and Civil Rights Policy (Participant Handbook pg. 4) o Participant Privacy and Confidentiality Policy (Participant Handbook pg. 4) o Participant’s Release of Information Statement o Using Social Media
• Participant’s Rights and Program Resources o Employee Rights (Participant Handbook pg. 5) o U.S. Department of Labor’s “Youth Rules!” / Occupational Safety and
Health Administration (Participant Handbook pg. 6)
o Disclosure Statement for Employees as Required by the Child Protective Services Law (Participant Handbook pg. 7-8)*
o Workers’ Compensation Policy (Participant Handbook pg.8) o Program and Workplace Conduct (Participant Handbook pg. 9) o Appropriate Attire (Participant Handbook pg. 10) o Getting Paid (Participant Handbook pg. 11)*
o Timesheets and/or Incentive Plans (Participant Handbook pg. 12)
Applicant/Participant Printed Name DOB
Applicant/Participant Signature Date Signed Note: This document must be retained in the Applicant/Participant file.
*Only applicable for youth who are responsible for the welfare of children or have routine interaction and direct contact with children
16

Clearance Consent Form
Philadelphia Youth Network is the managing partner of WorkReady Philadelphia and Project U-Turn.
DISCLOSURE REGARDING EMPLOYMENT / VOLUNTEER BACKGROUND REPORT
PHILADELPHIA YOUTH NETWORK (“COMPANY”) may obtain from Sterling Infosystems, Inc. (“STERLING”), 1
State Street, New York, NY 10004, (877) 424-2457, www.sterlinginfosystems.com, a consumer report and/or
an investigative consumer report (“REPORT”) that contains background information about you in
connection with your employment or volunteer application. If you are accepted, to the extent permitted
by law, COMPANY may obtain from STERLING further reports throughout your employment / volunteer for
purpose without providing further disclosure or obtaining additional consent.
The REPORT may contain information about your character, general reputation, personal characteristics
and mode of living. The REPORT may include, but is not limited to, credit reports and credit history
information; criminal and other public records and history; public court records (e.g., bankruptcies, tax
liens and judgments); motor vehicle and driving records; educational and employment history, including
professional disciplinary actions; drug/alcohol test results; and Social Security verification and address
history, subject to any limitations imposed by applicable federal and state law. This information may be
obtained from public record and private sources, including credit bureaus, government agencies and
judicial records, former employers and educational institutions, and other sources.
If an investigative consumer REPORT is obtained, in addition to the description above, the nature and
scope of any such REPORT will be employment verifications and references, or personal references.
AUTHORIZATION TO OBTAIN EMPLOYMENT / VOLUNTEER BACKGROUND REPORT
I have read the Disclosure Regarding Employment / Volunteer Background Report provided by the
PHILADELPHIA YOUTH NETWORK (“COMPANY”) and this Authorization to Obtain Employment / Volunteer
Background Report. By my signature below, I hereby consent to the preparation by Sterling Infosystems,
Inc. (“STERLING”), a consumer reporting agency located at 1 State Street, New York NY 10004, (877) 424-
2457, www.sterlinginfosystems.com, of background reports regarding me and the release of such reports
to the COMPANY and its designated representatives, to assist the COMPANY in making an employment
or volunteer decision involving me at any time after receipt of this authorization and throughout my
employment or volunteering, to the extent permitted by law. To this end, I hereby authorize, without
reservation, any state or federal law enforcement agency or court, educational institution, motor vehicle
record agency, credit bureau or other information service bureau or data repository, or employer to
furnish any and all information regarding me to STERLING and/or the COMPANY itself, and authorize
STERLING to provide such information to the COMPANY. I agree that a facsimile (“fax”), electronic or
photographic copy of this Authorization shall be as valid as the original.
I allow release of this information for verification purposes and understand that it will be used to determine
eligibility.
____________________________________________________________________________________ Printed Name of Applicant
______________________________________________________________________ ____________ Signature of Applicant Date
As parent/guardian, I grant permission for the collection and release of information as specified above.
___________________________________________________________________________________ Printed Name of Parent/Guardian (if applicant is under 18)
______________________________________________________________________ ___________ Signature of Parent/Guardian (if applicant is under 18) Date
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight

Philadelphia Youth Network is the managing partner of WorkReady Philadelphia, Project U-Turn, and the E3 Centers. For more information, please visit www.pyninc.org.
FOR EMPLOYEES
DISCLOSURE STATEMENT
I swear/affirm that I am seeking a paid position. If being hired on a provisional basis, I have applied for certification through ChildLine, the Pennsylvania State Police, and the Federal Bureau of Investigation and am submitting appropriate information to have my clearances ran OR submitting a copy of clearances to the employer, administrator, supervisor or other person responsible for employment decisions.
I swear/affirm that, if providing certifications that have been obtained within the past (5) five years, I have not been disqualified from employment or service under the Pennsylvania Child Protective Services Law, 23 Pa.C.S. 6344 (c), and have not been convicted of an offense similar in nature to a crime listed in 23 Pa.C.S. 6344 (c) under the laws or former laws of the United States or one of its territories or possessions, another state, the District of Columbia, the Commonwealth of Puerto Rico or a foreign nation, or under a former law of this Commonwealth.
I swear/affirm that I have not been named as a perpetrator of a founded report of child abuse within the past five (5) years as defined by the Child Protective Services Law.
I swear/affirm that I have not been convicted of any of the following crimes under Title 18 of the Pennsylvania consolidated statues or of offenses similar in nature to those crimes under the laws or former laws of the United States or one of its territories or possessions, another state, the District of Columbia, the Commonwealth of Puerto Rico or a foreign nation, or under a former law of this Commonwealth.
Chapter 25 (relating to criminal homicide)
Section 2702 (relating to aggravated assault)
Section 2709 (relating to stalking)
Section 2901 (relating to kidnapping)
Section 2902 (relating to unlawful restraint)
Section 3121 (relating to rape)
Section 3122.1 (relating to statutory sexual assault)
Section 3123 (relating to involuntary deviate sexual intercourse)
Section 3124.1 (relating to sexual assault)
Section 3125 (relating to aggravated indecent assault)
Section 3126 (relating to indecent assault)
Section 3127 (relating to indecent exposure)
Section 4302 (relating to incest)
Section 4303 (relating to concealing death of child)
Section 4304 (relating to endangering welfare of children)
Section 4305 (relating to dealing in infant children)
Section 5902(b) (relating to prostitution and related offenses)
Section 5903(c) (d) (relating to obscene and other sexual material and performances)
Section 6301 (relating to corruption of minors)
Section 6312 (relating to sexual abuse of children), or an equivalent crime under
Federal law or the law of another state.
I swear/affirm that I have not been convicted of a felony offense under Act 64-1972 (relating to the
controlled substance, drug device and cosmetic act) committed within the past five years.
I swear/affirm that I understand that I must be dismissed from employment if I am named as a perpetrator of a
founded report of child abuse within the past five (5) years or have been convicted of any of the crimes listed
above.

Philadelphia Youth Network is the managing partner of WorkReady Philadelphia, Project U-Turn, and the E3 Centers. For more information, please visit www.pyninc.org.
I swear/affirm that I understand that if I am being hired on a provisional basis, I am not permitted to
work alone with children and must work in the immediate vicinity of a permanent employee during
this provisional employment period.
I swear/affirm that I understand that if I am arrested for or convicted of an offense that would constitute
grounds for denying employment or participation in a program, activity or service under the Child
Protective Services Law as listed above, or am named as perpetrator in a founded or indicated report, I must
provide the administrator or designee with written notice not later than 72 hours after the arrest, conviction
or notification that I have been listed as a perpetrator in the Statewide database.
I swear/affirm that I understand that if the person responsible for employment decisions or the
administrator of a program, activity or service has a reasonable belief that I was arrested or convicted for
an offense that would constitute grounds for denying employment or participation in a program, activity or
service under the Child Protective Services Law, or was named as perpetrator in a founded or indicated
report, or I have provided notice as required under this section, the person responsible for employment
decisions or administrator of a program, activity or service shall immediately require me to submit current
certifications obtained through the Department of Human Services, the Pennsylvania State Police, and the
Federal Bureau of Investigation. The cost of certifications shall be borne by the employing entity or
program, activity or service.
I swear/affirm that I understand that if I willfully fail to disclose information required above, I commit a
misdemeanor of the third degree and shall be subject to discipline up to and including termination or denial
of employment.
I swear/affirm that I understand that the person responsible for employment decisions or the
administrator of a program, activity or service is required to maintain a copy of my certifications.
I hereby swear/affirm that the information as set forth above is true and correct. I understand that false
swearing is a misdemeanor pursuant to Section 4903 of the Crimes Code.
Check one that applies:
I am between 14 and 17 years of age and have been a resident of Pennsylvania during the entirety of the
previous ten-year period.
I am between 14 and 17 years of age and I have NOT been a resident of Pennsylvania during the
entirety of the previous ten-year period, have received a FBI Fingerprint Check at any time since
establishing residency in Pennsylvania and have attached a copy of the certification.
I am 18 years of age or older
Name: ___________________________ Signature: _______________________ Date: __________
Witness: __________________________ Signature: _______________________ Date: __________
Parent/Guardian: ________________________ Signature: ___________________ Date: __________
(If you are under the age of 18 a parent signature is required.)
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight
lwilliams
Highlight

CHILDLINE AND ABUSE REGISTRY P.O. BOX 8170
HARRISBURG, PENNSYLVANIA 17105-8170
CONSENT/RELEASE OF INFORMATION AUTHORIZATION FORM FOR THE PENNSYLVANIA CHILD ABUSE HISTORY CERTIFICATION
I, ( _______________________________ ), hereby authorize the PA Department of Human Sevices, ChildLine to Applicant’s Name
release my Pennsylvania Child Abuse History Clearance information directly to ( _______________________________ ). Name of Requesting Agency
I understand that this information is confidential in nature pursuant to §6339 (relating to information in confidential reports)
of the Child Protective Services Law (CPSL) (23 Pa.C.S Chapter 63) and is not otherwise to be released by
( _______________________________ ) without my expressed authorization or pursuant to Section 3490.126 of Name of Requesting Agency
Title 55 of the Pennsylvania Code which states this information is confidential and the requesting agency can be held
criminally liable for a breach of confidentiality related to release of this information. I also understand that the
aforementioned information will not be released directly to me ( _______________________________ ) as stated Applicant’s Name
on the Pennsylvania Child Abuse History Certification application. I understand that I will not receive a copy
of my Pennsylvania Child Abuse History Certification directly from ChildLine; however, I may request a copy of
my Pennsylvania Child Abuse History Certification from ( _______________________________ ) upon written request. Name of Requesting Agency
I have read this Consent/Release of Information Authorization form and fully understand and agree to its content. I further
understand and agree to all information and ramifications of the Pennsylvania Child Abuse History Certification application
as it otherwise relates to this consent. Further I understand that if I am listed in the statewide database for child abuse
that my consent allows the result stating such information to be shared with the agency/organization noted on next page.
Page 1 of 2
CY 999 3/16
lwilliams
Highlight
lwilliams
Highlight

Please send my certification result(s) to:
Agency Name:
Agency Street Address:
Agency City, State, Zip Code:
Date Applicant’s Signature
As the agency/organization representative, I understand that, except for the subject of a report, persons who receive this information are subject to the confidentiality provisions of the CPSL and 55 Pa. Code, Chapter 3490 and are required to ensure the confidentiality and security of the information and are liable for civil and criminal penalties for releasing information to persons who are not permitted access to this information. I agree to receive and maintain this information in accordance with these requirements.
Date Agency’s Representative Signature
NOTE: IF THE PENNSYLVANIA CHILD ABUSE HISTORY CERTIFICATION FORM/APPLICATION (CY 113) IS NOT COMPLETED ACCURATELY OR IF IT IS INCOMPLETE, THE CY 113 WILL BE RETURNED TO THE APPLICANT AND NOT BACK TO A THIRD PARTY.
Revised 12-29-15
Page 2 of 2
CY 999 3/16
lwilliams
Highlight
lwilliams
Highlight


















