Colorectal Screening: Your Best Protection Against Colorectal Cancer

Working with the 70x2020 Colorectal Cancer Screening Initiative to Increase CRC Screening
Rates in the Mississippi Delta
Presenters:Roy J. Duhé, Ph.D., Professor of Pharmacology & Toxicology,
Professor of Radiation Oncology, Associate Director for Cancer Education, University of Mississippi Medical Center, Jackson, MSNancy A. Olson, J.D., Director, Human Research Office, University
of Mississippi Medical Center, Jackson, MS
Wednesday, October 14, 2015 Greenwood Leflore Hospital
1401 River Road, Greenwood, MS 38930

Acknowledgements and DisclosuresAcknowledgments
This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Program Award (EA-1148-UMC).
The 70x2020 Colorectal Cancer Screening Partnership also acknowledges financial support from the University of Mississippi Medical Center Cancer
Institute, C-CHANGE, and an anonymous donor.
DisclosuresRJD is a member of the Advisory Board of the Mississippi Cancer Registry and
the Medical/Research Advisor to the Mississippi Partnership for Comprehensive Cancer Control Executive Board; both positions are uncompensated.
RJD is the recipient of a Patient-Centered Outcomes Research Institute (PCORI) Program Award (EA-1148-UMC).

Learning ObjectivesAfter this activity, participants will be able to:
1) Identify at least three evidence-based interventions to increase stool-based colorectal cancer screens.
2) Explain how community-based research, including comparative effectiveness research and implementation research, can improve colorectal cancer screening rates in Leflore County.
3) Distinguish human subjects research from non-research activities.
4) Describe the protection of human research subjects, including their protected health information (PHI).
5) Describe the process of working with an Institutional Review Board (IRB) to review and approve a human subjects research protocol before initiating any research projects involving human subjects.

You should receive a link to a post-event survey via e-mail within 24 hours. Please complete and submit that survey within one week to receive
Continuing Education credit for this activity.
MNFThe University of Mississippi Medical Center School of Nursing Continuing Education Program is an approved provider of continuing nursing education by the Mississippi Nurses Foundation, Inc. an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.As an approved provider, the University of Mississippi Medical Center School of Nursing awards this activity 1.0 contact hour(s)Participation in and successful completion of this activity will be determined by the participant signing in, attending the sessions for which credit is desired, and completing the evaluation tool. Each participant should claim only those hours of credit that he or she actually spends in the educational activity.
AMAThe University of Mississippi School of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing medical education for physicians.The University of Mississippi School of Medicine designates this evidence-based training for a maximum of 1.0 AMA PRA Category 1 Credit(s)TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
NASWThis organization The University of Mississippi Medical Center provider number SWB 120016 is approved as a provider for continuing education by the Mississippi Board of Examiners and Marriage & Family Therapists; Approval Period: 1/15/2014 through 1/15/2016. Social workers will receive 1.0 continuing education clock hours in participating in this course (Clinical___/Supervision___/Cultural/Competency___/Ethics___/General_X__)

There are several recommended colorectal cancer screening tests
Screening Test DescriptionUnited States Preventive
Services Task Force (USPSTF)
American Cancer Society–U.S.Multi-SocietyTask Force
(ACS-USMSTF)
Fecal occult blood test (FOBT)* and fecal immunochemical test
(FIT)*
Examination of the stool for traces of blood not visible to the naked
eye
Recommends high- sensitivity FOBT and FIT annually for ages
50-75
Recommends high-sensitivity FOBT and FIT annually for
ages ≥ 50
Sigmoidoscopy* Internal examination of the lower part of the large intestine
Recommends every 5 years with high- sensitivity FOBT every 3
years for ages 50-75
Age ≥ 50, every5 years
Double-contrast barium enema* X-ray examination of the colon -- Age ≥ 50, every5 years
Colonoscopy Internal examination of the entire large intestine
Recommends every 10 years for ages 50-75
Age ≥ 50, every10 years
Computed tomography colonography*
Examination of the colon and rectum using pictures obtained using a computed tomography
scanner
-- Age ≥ 50, every5 years
Fecal DNA* Examination of the stool for traces of colorectal cancer DNA -- Age ≥ 50, every 3 years
* Positive findings require follow-up colonoscopy.

Preventive versus early-detection cancer screens
Preventive screens detect pre-cancerous lesions as well as cancers. IF ENTIRELY REMOVED, these pre-cancerous lesions will not develop into
carcinomas.
Early-detection screens detect cancers BEFORE they become symptomatic and/or metastatic, when
treatment is most likely to succeed.


Stool based CRC screens:Comparision of FIT vs. gFOBT
FIT gFOBTBowel Prep? None required None requiredBasis of test Antibody recognition of
human hemoglobinHeme-dependent oxidation of guaiac
Dietary restrictions No dietary restrictions. Aspirin, anticoagulants and other drugs may increase false positive results.
Dietary interferences (e.g., heme from myoglobin in red meat, plant-derived peroxidases, vitamin C or other antioxidants) prohibit certain foods and drugs days before testing.
Fecal manipulation Vendors provide long brushes to make sampling easier
Sensitivity & Specificity Multiple peer-reviewed studies show greatersensitivity & specificity of FIT over gFOBT

Comparison of FIT vs. Multi-target Stool DNA Test
Imperiale, et. al., (2014) NEJM 370:1287-1297
Multi-target Stool DNA Test Fecal Immunohistochemical Test P value
Target(s) Aberrantly methylated BMP3 and NDRG4 promoter regions, mutant KRAS DNA, β-actin DNA (as DNA
quantitation reference) and human hemoglobin
(immunoassay)
Human Hemoglobin (immunoassay)
Sensitivity (+ results in persons with CRC)*
92.3% 73.8% P = 0.002
Specificity (- results in persons w/out CRC)
86.6% 94.9% P < 0.001
Sensitivity for advanced pre-cancerous lesions
42.4% 23.8% P < 0.001
Detection rate of high-grade dysplasia
69.2% 46.2% P = 0.004
Detection rate of serrated sessile polyps (≥ 1 cm)
42.4% 5.1% P < 0.001
Consumer cost range & frequency
~$600 every 3 years ~$25 annual (actual cost varies)
* Critics note FIT sensitivity would be increased by lowering detection threshold from 100 ng hemoglobin / mL

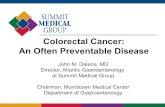
Why does CRC screening matter?Because survival is tremendously improved by early-stage diagnosis
(SEER 2005-2011 Data, All Races, Both Sexes)
Localized (39%) Confined to Primary Site
Regional (36%)Spread to Regional Lymph Nodes
Distant (20%)Cancer Has Metastasized
Unknown (5%)Unstaged
Percent of Cases by Stage
5-Year Relative Survival

http://www.biomedcentral.com/content/pdf/s13104-015-1352-0.pdf

Population-based CRC disparities exist throughout MississippiColorectal cancer characteristic Black
MississipiansWhite Mississippians
Difference (Black –White)
P value
Statistically-significant health disparities
% (Age 50+) reporting NEVER had a sigmoidoscopy or colonoscopy (average: 2006, 2008 & 2010 BRFSS)
53.2% 41.9% 11.3% <0.0001
Age-adjusted colorectal cancer incidence rate (per 100,000; 2006-2010 MCR data)
64.9 50.5 14.4 <0.0001
Age-adjusted colorectal cancer mortality rate (per 100,000; 2006-2010 MCR data)
26.2 17.5 8.8 0.0001
CRC mortality-to-incidence rate 0.40 0.35 0.05 0.0035
No discernible differences between groups
% Advanced stage (regional + distant disease) at initial diagnosis 52.9% 52.3% 0.6% 0.7926
UNPUBLISHED DATA: Statistical analyses performed by Dr. Xu Zhang

Self-reported colonoscopy rates in Mississippi’s Public Health Districts are strongly correlated with CRC incidence rates and mortality rates
UNPUBLISHED DATA: Statistical analyses performed by Dr. Xu Zhang
CRC Incidence and Mortality data source: Mississippi Cancer RegistrySelf-reported CRC screening data source: Mississippi State Department of Health’s Behavioral Risk Factor Surveillance System (BRFSS)

Geographic distribution of facilities offering colonoscopies in Mississippi
Faruque et al. BMC Res Notes (2015) 8:423

Geographic availability of gastroenterologists is a limiting factor in providing high-quality screening colonoscopies throughout Mississippi.
Public Health District Gastroenterologists Residents per gastroenterologist
Gastroenterologistsper Colonoscopy Facility Ratio
1 8 39995 1.33
2 16 22549 1.60
3 3 72236 0.43
4 6 40934 1.20
5 32 20013 1.60
6 6 40485 0.67
7 2 87399 0.33
8 15 20326 1.50
9 16 29181 1.14
Mississippi 104 28586 1.20
Faruque et al. BMC Res Notes (2015) 8:423

Many colonoscopy facilities in MS are understaffed by gastroenterologists79% of the state (38% of the population) is beyond a 30-minute drive to gastroenterologist
52% of the state (17% of the population) is beyond a 30-minute drive to a colonoscopy facility
Faruque et al. BMC Res Notes (2015) 8:423

The regional impact of gastroenterologists on CRC outcomes
Faruque et al. BMC Res Notes (2015) 8:423

So what is our response to this situation?
The goal of the 70x2020 Colorectal Cancer Screening Initiative is
“to ensure that at least 70% of Mississippians are up–to–date with recommended colorectal cancer
screening by the year 2020.”

Who Are We? The 3 Sectors of the 70x2020 Partnership
2015 2017 2018 2019 20202016
Communities
Health Care System
State Leadership
• Increase health literacy
• Create consumer demand
• Close existing gaps in availability and accessibility
• Initiate and follow-up on recommended service delivery
• Establish mandate for institutional responsibility, authority and accountability
• Provide system support

www.umc.edu/70x2020strategicplanThree Strategic Efforts
1) Change Mississippi’s attitudes about colorectal cancer
2) Change Mississippi’s colorectal cancer control tactics
3) Address Mississippi’s geographic and population-based health disparities
Ten Tactics1) 90 percent CRC screening among eligible participants in the State and School Employees’ Health Insurance Plan 2) 90 percent CRC screening among eligible veterans, military service members and their immediate families 3) 90 percent CRC screening among eligible insured employees via workplace participation 4) Increase stool-based CRC screening via primary health care providers, CHCs, FQHCs and RHCs 5) Improved continuity of care linkages between primary and specialty health care providers 6) Community engagement 7) Communication 8) Improved metrics via health data analytics 9) Mission-focused funding strategy 10) 2020 transition

www.umc.edu/70x2020
To join the 70x2020 Partnership, send an e-mail to
[email protected] and write “Please add me to the 70x2020 Partnership” in the subject line.
You will receive our free electronic newsletter.

Eugene Washington PCORI Engagement Award (EA-1148-UMC) a.k.a., “70x2020 Colorectal Cancer Screening Initiative”
OBJECTIVES:1) Engage community residents and primary health care
providers in Mississippi Delta counties by holdingquarterly meetings in three communities: Greenwood(Leflore County), Greenville (Washington County), andCleveland (Bolivar County).
2) Introduce the community to pioneers of successfulbest practices which increased CRC screening incomparable communities.
3) Introduce the community to pioneers of participatorycommunity research on CRC screening interventionsfrom other rural communities.
4) Facilitate the ensuing dialogue at quarterly meetingsto determine the priorities and preferences of thecommunity for participatory comparativeeffectiveness research to increase CRCscreening rates.
STRATEGIC RATIONALE:1) Preparatory activity to establish credibility for PCORI
community-based, comparative effectiveness fundingsupport.

Investigator-Initiated, Hypothesis-Driven Basic Scientific Research
AcceptedTheory

The Lay Community and the Physician-Scientist often have disparate opinions about basic, T1 & T2 translational research:
Edward Jenner“An Inquiry into the Causes and Effects of the Variolae Vaccinae, a Disease discovered in some of the Western Counties of
England, particularly Gloucestershire, and known by the name of the Cow-Pox.” (1798)

Translation of research from bench to bedside and from bedside to communities
• Process of discovery
Basic
• Application to humans
T1 • Application to patients
T2
• Application to practice
T3 • Application to
populations
T4
• Healthy Society
Phase 1 & 2 Clinical Trials
Evidence-Based Systematic
Reviews
Comparative Effectiveness
Research
Public Health Policy
Phase 3 & Post-Market Approval
Clinical Trials

What’s different about community-based participatory research?
What’s different about patient-centered outcomes research?

Which statement best describes the role of your patient in research?
A. The most important thing is to get your patient to sign the informed consent document.
B. The most important thing is to understand what research outcomes are most important to your patient.

Which statement best describes your role in a collaborative research project with the University of
Mississippi Medical Center?
A. The most important thing is to follow the research protocol exactly as described by the Principal UMMC Investigator.
B. The most important thing is to get the Principal UMMC Investigator to understand the health care circumstances in Leflore County.

The Guide to Community Preventive Services: A source for evidence-based interventions
• Community Preventive Services Task Force (2012) “Updated recommendations for client- and provider-oriented interventions to increase breast, cervical, and colorectal cancer screening” Am J Prev Med 43(1):92-96. http://www.ncbi.nlm.nih.gov/pubmed/22704753
• Sabatino, et. al., Community Preventive Services Task Force (2012) “Effectiveness of interventions to increase screening for breast, cervical, and colorectal cancers: nine updated systematic reviews for The Guide to Community Preventive Services” Am J Prev Med 43(1):97-118. http://www.ncbi.nlm.nih.gov/pubmed/22704754

Community Preventive Services Task Force Recommended Evidence-Based Interventions to Increase CRC Screening
Intervention 2008 Review Findings 2012 Review FindingsINCREASING COMMUNITY DEMAND FOR SCREENING
Group education Insufficient evidence Insufficient evidenceOne-on-one education Insufficient evidence Recommended: sufficient evidenceClient reminders Recommended: sufficient evidence Recommended: strong evidenceClient incentives Insufficient evidence Insufficient evidenceMass media Insufficient evidence Insufficient evidence
INCREASING COMMUNITY ACCESS TO SCREENINGReducing structural barriers Recommended: strong evidence Recommended: strong evidenceReducing out-of-pocket costs Insufficient evidence Insufficient evidence
INCREASING PROVIDER DELIVERY OR PROMOTION OF SCREENINGProvider assessment and feedback
Recommended: sufficient evidence Recommended: sufficient evidence
Provider incentives Insufficient evidence Insufficient evidence

What’s next?Community Engagement Meetings
• January 19 & 21, 2016: General “health fair” CEMs in Greenville & Greenwood
• March/April, & May/June 2016: Alternating CE & “health fair” CEMs
• Program year 2: Shifting to mixed audience CEMs which will also include CE activities
• February 1, 2017 through May 31, 2017 (Decisive Community Action Phase)
• April 4 & 5, 2017: Summative Community Engagement Meetings
Examples of visiting Pioneers of Best Practices/Community Engagement
• Michael Preston, PhD, MPH (Director of Cancer Control at the University of Arkansas for Medical Sciences)
• Annette Maxwell, DrPH (Professor, UCLA School of Public Health)
• Durado Brooks, MD, MPH (Director, Cancer Control Intervention, American Cancer Society, Inc.; Steering Committee Member, NCCRT)
• Maria Syl de la Cruz, MD (Assistant Professor, Thomas Jefferson University)
• Michael D. Sarap, MD, FACS (Southeastern Ohio Physicians, Inc.)

Summary• Mississippi’s burden of colorectal cancer is characterized by
significant geographic- and population-based disparities.
• Mississippi can decrease CRC incidence and mortality rates throughdeliberate implementation of best practices throughout the state.
• One-on-one education, client reminders, reducing structural barriers,and provider assessment & feedback are evidence-based interventionswhich increase stool-based colorectal cancer screening rates.
• 70x2020 Partners are seeking collaborators to conduct community-based research, including comparative effectiveness research andimplementation research, to improve colorectal cancer screening ratesin Leflore County and the Mississippi Delta.

A PRIMER ON HUMAN SUBJECTS RESEARCH
Nancy A. Olson, J.D.
Director
Human Research Office/Institutional Review Board
University of Mississippi Medical Center
Jackson, Mississippi

What is an IRB?An Institutional Review Board (IRB) is a federally mandated board charged with overseeing all research projects involving human participants.

SETS OUT THE BASIC ETHICAL PRINCIPLES FOR CONDUCTING RESEARCH INVOLVING HUMAN SUBJECTS
• Respect
• Beneficence
• JusticeThese principles are the basis for subsequent regulations designed to ensure protection of human subjects in research.
The Belmont ReportNational Commission

BELMONT PRINCIPLES
Respect for PersonsInformed consentRespect of privacy of research participantsElements of autonomy
BeneficenceBest possible design to maximize benefits/minimize harmResearchers have appropriate expertiseProhibit research that is w/out favorable risk benefit analysis
JusticeParticipants selected equitablyAvoid exploitation of vulnerable or convenient populations

GOVERNING RULES, REGULATIONS AND GUIDANCE
DHHSFDAOHRP
Declaration of HelsinkiBelmont ReportCommon RuleGood Clinical PracticeInternational Conference on HarmonisationInstitutional policies and procedures

ADDITIONAL PROTECTIONS
• Three subparts under HHS regulations provide additional protections for certain populations
• Subpart B – Fetus, Pregnant Women, and Neonates
• Subpart C - Prisoners
• Subpart D – Children
• Subparts under FDA regulations• Subpart D - Children

WHAT NEEDS IRB REVIEW?
All research involving human subjectsResearch is a systematic investigation designed to
develop or contribute to generalizable knowledge.
Human subject means a living individual about whom an investigator conducting research obtains
(1) Data through intervention or interaction with the individual, or (2) Identifiable private information.


Federal regulations require IRB review of human research before it may begin and give IRBs the authority to:
• Approve, Modify, or Disapprove research• Review and approve proposed changes• Suspend or terminate approval• Observe consent process and research procedures (post-approval
monitoring)• And mandate that IRBs conduct continuing review, not less than once
per year, depending on the risk level of the study

LEVELS OF REVIEW
Convened
Expedited
Exempt
Convened
• Greater than minimal risk study
Expedited & Exempt
• Study must be minimal risk and fall within one or more of the specific categories set out by regulation

HOW IS REVIEW TYPE DETERMINED?
Four Basic Questions:1. Does the proposed project meet the definition
of Research?2. Does the proposed project meet the definition
of Human Subjects?3. What level of Risk is involved in the proposed
project? Minimal vs Greater than 4. If minimal risk, does the proposed project fit
within one or more of the expedited or exempt categories?

IRB MEMBERSHIP
A minimum of 5 members of varying backgrounds
Membership must include at least one non-affiliated member and one nonscientist member
A majority of members must be present (quorum = half plus 1)
Nonscientist must be presentNo nonscientist = no meeting
Meeting stops if number present drops below quorum or nonscientist leaves

IRB MEMBERSHIP
Each member brings unique professional and personal perspectives to the process
Which may include scientific, social, ethical, community, minority, legal, administrative and/or operational perspectives.Each member has an equal voice in meeting
discussions, deliberations and voting.

IRB members must consider:• Research design/methods• Risk/benefit analysis• Informed consent and assent process• Participant selection and recruitment process• Inclusion/Exclusion criteria• Privacy/confidentiality safeguards• Ensure adequate protection of rights/welfare of
participants• Additional safeguards if protected populations involved
(prisoners, pregnant women, children)• Additional safeguards if subjects likely to be vulnerable
to coercion or influence (mentally disabled, economically or educationally disadvantaged)
• Plan for collection, storage, analysis of data and specimen banks
• Qualifications of PI and investigators• Compliance with applicable federal and state
laws/regulations, guidance, and institutional policy

In order to approve research the IRB must find:
• Risks are minimized• Risks are reasonable in relation to benefits• Subject selection is equitable• Informed consent will be sought• Informed consent will be documented• Adequate provision for monitoring data to ensure safety,
when appropriate• Adequate provisions to protect privacy and maintain
confidentiality

DATA PRIVACY
• Anonymous means that no one, not even the researcher, can connect the data to the individual.
• Collection of indirect identifiers (i.e., information regarding other unique individual characteristics) might make it possible to identify an individual from a pool of subjects. Confidential means that a link exists.
• De-identified means that all direct or indirect identifiers or codes linking the data to the individual have been destroyed.
• Coded means that there is a link or key between the data and the individual.
The research team is obligated to protect the data from disclosure outside the research, according to the terms of the research protocol and the informed consent document. Methods to reduce the risk of inadvertent disclosure include:
• Storing the identifiers separately from the research data
• Replacing the indentifiers with a unique code and using the code to refer to the subject data. Note that coding the data does not make it anonymous.
• Storing the code key separately from the identifiers

PATIENT CENTERED OUTCOME RESEARCHAND
COMMUNITY-BASED RESEARCH
Means greater stakeholder involvement in the research process
Presents new challenges for IRBs• Defining the role of the patient – researcher, subject or both
• Depending on role, requirements for oversight will vary
• Recruitment considerations

RESOURCES
• http://www.hhs.gov/ohrp/humansubjects/guidance/belmont.html
• http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html
• http://www.hhs.gov/ohrp/policy/index.html
• http://www.hhs.gov/ohrp/policy/checklists/decisioncharts.html
• http://www.hhs.gov/ocr/privacy/


















