WORKING MATERIAL › Content › end-to-end CIRS … · such as intensity-modulated radiation...
30
1 Rev. February 2019 WORKING MATERIAL IAEA Supported National “End-to-End” Audit Programme for Dose Delivery Using Intensity- Modulated Radiation Therapy through On-Site Visits to Radiation Therapy Institutions Contributors (in alphabetical order) Consultants: Catharine Clark, Eduard Gershkevitsh, Wolfgang Lechner, Jake Van Dyk, Daniel Venencia IAEA staff: Tomislav Bokulic, Pavel Kazantsev, Paulina Wesolowska Joanna Izewska (Scientific Secretary)
Transcript of WORKING MATERIAL › Content › end-to-end CIRS … · such as intensity-modulated radiation...

1 Rev. February 2019
WORKING MATERIAL
IAEA Supported National “End-to-End” Audit
Programme for Dose Delivery Using Intensity-
Modulated Radiation Therapy through On-Site
Visits to Radiation Therapy Institutions
Contributors (in alphabetical order)
Consultants: Catharine Clark, Eduard Gershkevitsh, Wolfgang Lechner,
Jake Van Dyk, Daniel Venencia
IAEA staff: Tomislav Bokulic, Pavel Kazantsev, Paulina Wesolowska
Joanna Izewska (Scientific Secretary)

2 Rev. February 2019
FOREWORD
The technology of radiation oncology has developed significantly over the last decade. New techniques
such as intensity-modulated radiation therapy (IMRT) are becoming common practice in most radiation
therapy institutions. At the same time, it is recognized that a significant number of institutions are not
able to deliver IMRT treatment protocols within defined criteria of acceptability. Quality Assurance (QA)
in all the steps of the radiation treatment process is essential to ensure accurate dose delivery to the
patient and to minimize the possibility of accidental over or under exposure. According to IAEA Safety
Report Series No.17, treatment planning and beam calibration are the main sources of errors in external
beam radiotherapy.
The IAEA has a long history of providing assistance for dosimetry audits in radiotherapy to its Member
States. Together with the World Health Organization (WHO), it has operated postal audit programs using
thermoluminescence dosimeters (TLD) to verify the calibration of radiotherapy beams since 1969.
Detailed follow-up procedures have been implemented for correcting inaccurate beam calibrations. With
time, the number of institutions demonstrating results outside of the criteria of acceptability have
decreased significantly. The IAEA has also supported national dosimetric audits to ensure the optimal
usage of radiotherapy treatment planning systems (TPS) at a time before IMRT became routine clinical
practice.
The objective of this IAEA supported national dosimetric audit programme is to ensure the optimal and
safe usage of newly developed complex IMRT head and neck (H&N) procedures. The expectation is that
any lessons learned from complex H&N procedures have the potential for reducing the probability of dose
delivery problems for other clinical sites as well, thus providing safer radiotherapy.
This publication describes the details of the H&N IMRT audit programme. The methodology was
developed by a group of international experts through a series of consultants’ meetings conducted in
2014-2017. The IAEA officer responsible for this publication was J. Izewska of the Division of Human
Health.

3 Rev. February 2019
Contents
1. INTRODUCTION .................................................................................................................. 4
1.1 Background ................................................................................................................. 4
1.2 Purpose ...................................................................................................................... 4
2. AUDIT STRUCTURE .............................................................................................................. 6
2.1 Request for audit ......................................................................................................... 6
2.2 Guiding principles and procedures of the audit................................................................. 6
2.3 The audit report........................................................................................................... 7
3. AUDIT METHODOLOGY ........................................................................................................ 9
3.1 Head and shoulders phantom and overall audit process .................................................... 9
3.2 Pre-visit activities ........................................................................................................14
3.2.1 Pre-visit MLC tests................................................................................................14
3.2.2 Pre-visit planning process......................................................................................16
3.2.3 On-site visit .........................................................................................................19
3.2.4 CT scanning .........................................................................................................20
3.2.5 Treatment plan ....................................................................................................20
3.2.6 Audit site visit measurements ................................................................................21
3.3 On-site analysis...........................................................................................................23
3.4 Post visit analysis ........................................................................................................23
3.4.1 Filled-in IMRT audit reporting form.........................................................................23
3.4.2 Film analysis procedures .......................................................................................23
3.5 Reporting...................................................................................................................24
3.6 Follow-up ..................................................................................................................26
REFERENCES .........................................................................................................................27

4 Rev. February 2019
1. INTRODUCTION
1.1 Background
The technology of radiation oncology has evolved rapidly during recent years such that many cancer
institutions have advanced, or are about to advance, from 3-dimensional conformal radiation therapy (3-
D CRT) to intensity-modulated radiation therapy (IMRT). The complexity of IMRT treatment planning and
dose delivery is such that there is increased potential for significant patient dose misadministration [1;2].
Thus, detailed quality assurance (QA) procedures need to be implemented to minimize the probability of
such misadministrations.
Audits of dose delivery as well as treatment procedures have been used for many years [3;4] and have
demonstrated great benefit in terms of discovering dose deviations and then allowing the determination
of their cause such that these deviations can be corrected. Both mailed dosimetry programmes and on-
site audit systems exist in parallel. Many on-site review programmes operate at a local or national level
for a limited number of institutions [5-16], whereas mailed systems provide cost effective audits on a
larger scale, involving hundreds or thousands of radiotherapy facilities [4;17;18]. Mailed systems using
phantoms with pseudo-anatomic geometries have also been developed for more complex treatment
technologies such as IMRT [2;19-23]. The experience obtained through the irradiation of the phantoms
by a number of institutions demonstrates that institutions vary significantly in their ability to deliver doses
and dose distributions that agree with their own treatment plans [2;6;16;24-26]. Indeed, on its initial
round of mailed head and neck (H&N) phantoms for assessment of IMRT treatments, the Radiological
Physics Center (RPC) in Houston (now called Imaging and Radiation Oncology Core, IROC – Houston QA
Center) found that 29% of 128 institutions failed the dose/distance criteria of 7%/4mm [2]. Even in 2014,
with further analysis of additional H&N data, of the 1368 irradiations, 233 (17%) failed [26;27]. A recent
report from the IAEA on accuracy considerations and uncertainties in radiation therapy [28] has as its
fourth recommendation, “An independent dosimetry audit should be performed for every new
installation that is about to embark on radiation treatments. In addition, regular (e.g. annual) audits
should be performed using remote services or on-site visits (or equivalent).”
1.2 Purpose
In view of the complexity of IMRT treatments and the knowledge that a significant number of institutions
have not been able to pass anthropomorphic phantom tests for H&N treatments, the IAEA is supporting
the development of a national auditing programme to review H&N IMRT treatments. The programme
provides end-to-end on-site auditing of IMRT treatments using a phantom which is scanned, planned and
treated. The advantage of on-site audit over remote audit is that results can be immediate and discussions
can be held to resolve issues during the visit [16;29]. The emphasis of this program is on the physics
aspects of IMRT treatments. Clinical issues related to these procedures are beyond the scope of the audit.
The methodology simulates the important parts of the external beam IMRT radiotherapy workflow from
patient data acquisition to treatment planning to dose delivery. To be close to a realistic patient
procedure, this audit uses an anthropomorphic phantom combined with a set of contours representing

5 Rev. February 2019
the target volumes and organs at risk. The phantom set-up should be close to real patient set-ups using
the technology normally used in the radiotherapy department such as the use of image-guidance
procedures. The contours are electronically imported and superimposed on the computed tomography
(CT) scans of the phantom. Dose prescriptions and normal tissue constraints are provided such that a
treatment plan can be developed. This treatment plan is transferred to the treatment machine and the
dose is delivered to the phantom. Appropriate dosimeters are used to determine both doses at specific
reference points as well as a 2-D dose distribution in a coronal plane. Comparisons are then made between
the calculated and delivered doses. This comparison is the ultimate result of this audit.
As part of the auditing process, some preparatory (pre-visit) activities will be performed by the institution
being audited several weeks prior to the actual site visit audit date. These preparatory activities are
performed to ensure viability and usefulness for the on-site visit as well as to facilitate an efficient visit by
the national auditing organisation.
The intent of this audit is to review the physics aspects of the overall clinical IMRT performance and to
provide feedback to the institution regarding the quality of a treatment representative of a typical clinical
H&N scenario. If the audit result proves positive, assumptions cannot be automatically made that other
clinical sites as well as other H&N treatments used at the institution being audited are of equal quality,
although it does demonstrate that the physical aspects of the H&N technique were successfully
implemented. While the audit methodology for the anthropomorphic phantom is applicable in general
for other modalities or treatment units, such as TomoTherapy or CyberKnife, the detailed procedures for
such specialized tests have not been addressed in this document.

6 Rev. February 2019
2. AUDIT STRUCTURE
2.1 Request for audit
The IAEA supported national H&N IMRT audit in radiation therapy is voluntary. The local auditing
organisation should conduct a national workshop on IMRT audits to discuss strategies and collect audit
requests from radiotherapy institutions. The institution requesting an audit must have the equipment and
infrastructure to deliver IMRT treatments. This should include high energy teletherapy units, a
computerised treatment planning system (TPS) capable of inverse treatment planning for IMRT
treatments, and access to a CT imaging facility. This needs to include capabilities to register two CT data
sets and transfer the structures between them. The audit is not structured to provide the commissioning
of new IMRT procedures. The institution should have completed full commissioning of IMRT capabilities,
and have the procedures ready for clinical operation or already be using them in clinical practice. All steps
of the IMRT process should have been developed and assessed by the institution well in advance of the
audit.
To participate in this audit, the form in Appendix 1 needs to be completed and submitted to the national
auditing organisation. Appendix 2 will be filled in on site (at the audit location) and will be included in the
“IMRT audit reporting form”.
2.2 Guiding principles and procedures of the audit
The audit procedure is based on the use of a specially designed CIRS IMRT Verification Head and Shoulder
Phantom (SHANE) (Computerized Imaging Reference Systems, Inc., Norfolk, VA, USA). The phantom is
equipped with:
1. Anatomic bone, teeth and air structures typical of human anatomy.
2. Four horizontal (superior-inferior) channels for the insertion of a small volume ion chamber that will
be used for assessing the dose delivery. Currently, the phantom is configured for use with a PTW
31010 Semiflex 0.125 cc ion chamber but can accommodate different ion chambers or other
dosimeters upon request. The channels will be filled with “marked” water-equivalent plastic
materials during the CT scanning process. The “markers” will help define the location of the points of
calculation and the points of measurement.
3. The capability to insert dosimetric film in a coronal plane to provide a 2-D dose distribution of the
planned treatment along with appropriate film reference marks to clearly interpret the film
orientation.
4. Reference marks on the phantom surface to be used in aiding the treatment set-up.
5. A set of five calibrated electron density reference plugs in the shoulder region that enable the
verification of the Hounsfield Units (HU) to relative electron density conversion procedure.
Several weeks prior to the site visit, the institution must provide a set of data, perform some preparatory
tests and submit the results of these tests to the national auditing organisation. These tests must be
completed successfully for the actual site visit to take place. The data include field profiles and output

7 Rev. February 2019
factors that are used by the institution, down to 2 x 2 cm2 field size. In addition, the institution will provide
information on MLC configuration and performance tests. Details of these tests are described in
Appendix 1.
The clinical test case is representative of a typical clinical H&N case to be treated with IMRT. While the
clinical scenario may not be exactly how the institution treats its H&N cases, it does provide a test of the
institution’s capability in both planning and delivering complex H&N treatment. The measurements
performed using the phantom are aimed at confirming that the planned dose and dose distributions
delivered to the phantom agree with those determined by measurement.
For the audit visit, the auditors will bring with them a dedicated dosimetry set including the SHANE
anthropomorphic phantom, a calibrated ionization chamber and electrometer, and film. The overall audit
typically takes 2 days for scanning, planning and delivery, depending on the technology available in the
department. Careful planning by the institution will be needed to avoid unnecessary intervals between
the time of the CT scanner availability, the time of the TPS availability and the time of the radiation
treatment machine availability. On the first day, the CT scanning and test case planning is performed. CT
scanning will require about 45 min of CT scanner time and the test case planning and the transfer of data
to the linac will require several hours. The planning time will depend on the TPS and the number of
iterations for the optimization. This timing is estimated for one clinical scenario and it is recommended
the most common H&N IMRT technique will be assessed. Typically, the planning time does not exceed 4-
5 hours. It should be noted that users are required to plan the phantom with the technique as they would
for their own typical clinical scenarios to generate a clinically acceptable plan. Adding extra detail and time
for optimization may be counter-productive since additional iterations may make the plan much more
difficult to deliver nor does it represent a typical clinical scenario.
During the allotted times, the auditor, along with a local physicist, should have access to the CT scanner,
the TPS workstation with the calculation and planning capabilities as well as to the treatment machine to
deliver the radiation and to perform the measurements. The required linac time will depend on the
treatment technique, e.g. the performance tests and dose delivery verification can last between 3 hours
for VMAT and 5 hours for step-and-shoot techniques.
2.3 The audit report
The preliminary results will be handed over to the audited institution at the end of the on-site audit. Any
discrepancies discovered (dose and/or distance deviations exceeding agreement criteria) will be reviewed
and possible explanations may be found while the auditor is still on site. Follow-up visits could be arranged
if applicable.
The final audit report will be submitted within a few weeks after completion of the on-site visit. The report will be sent only to staff in responsible positions in the radiotherapy department, e.g., the chief medical physicist and other staff members whose roles within the institution are significant to this audit. At all times, the auditing organisation will maintain confidentiality regarding the audit report.

8 Rev. February 2019
The audit results are only valid on the day of the audit. The department takes the full responsibility for
the clinical service following this audit. The resolution of any discrepancies discovered during the IMRT
audit is the responsibility of the audited institution. Upon the completion of H&N IMRT audit, the audit
results cannot be extended to other clinical sites as well as to other H&N treatment techniques at the
institution.
The overall results of the national audit will be reported in an anonymous way to the radiotherapy
community in the country. However, individual institutions will be able to identify its own results and
compare them to the national results. At the same time, the anonymous national results will be
transferred to the IAEA for the IMRT audit international database.

9 Rev. February 2019
3. AUDIT METHODOLOGY
3.1 Head and shoulders phantom and overall audit process
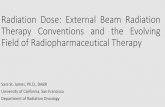
The CIRS SHANE phantom is shown in Figure 1 and represents a typical human H&N patient in proportion,
density and 3-D structure. The phantom has the equivalent of normal tissue, bone, teeth and air cavities
with longitudinal channels to hold interchangeable sleeve and spacer plug inserts to accommodate the
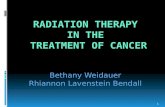
ion chamber and to position it in very well-defined locations. Figure 2 shows a CT scan of the phantom
indicating the location of the ion chamber channels. For each anatomical location, a specific insert (a
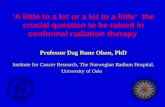
sleeve and a set of plugs) will be used to position the ion chamber. Figure 3 shows the outlines of the
target volumes and the organs at risk (OARs) on two transverse planes using the standardized
nomenclature recommended by Santanam et al [30].
(a)
(b)
Figure 1. Pictures of the anthropomorphic CIRS SHANE phantom used for the on-site audit; (a) assembled
SHANE, (b) SHANE components.

10 Rev. February 2019
(a)
(b)
(c)
(d)
Figure 2. CT study of H&N phantom showing the positions of the ion chamber channels and the
corresponding ion chamber positions, (a) transverse plane, (b) 3-D display, (c) sagittal view, and (d)
coronal view.

11 Rev. February 2019
(a)
(b)
Figure 3. Two transverse planes at different levels in the H&N showing the target volumes and organs at
risk.
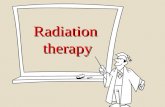
The shoulders accommodate five electron density plugs: cortical bone, trabecular bone, lung inhale, lung
exhale and a vial with water. In addition, anatomical structures such as spinal cord and the phantom body
(soft tissue) can be used for electron density analysis. The location of plugs is shown in Figure 4 and the
composition of plugs is given in Table 1.
Figure 4. CT image of the SHANE shoulder region with electron density plugs: A – water, B – cortical bone,
C – trabecular bone, D – lung exhale, E – lung inhale, F – spinal cord, G – soft tissue.

12 Rev. February 2019
TABLE 1. Electron density data.
Phantom structures Mass density g/cm3
Electron density x 10^23 /cm3
Electron density relative to water
water 1.000 3.340 1.000
cortical bone 1.930 5.956 1.783 trabecular bone 1.200 3.863 1.156
lung exhale 0.500 1.648 0.493 lung inhale 0.205 0.668 0.200 spinal cord 1.070 3.488 1.044
soft tissue 1.055 3.434 1.028 air 0.001 0.003 0.001
The SHANE phantom will be positioned and aligned on the treatment couch. The local set up verification
procedure with on-board imaging (IGRT), for example cone-beam CT [31], portal imaging, ExacTrac, etc.
should be used for the phantom reference position determination.
The steps in the overall H&N end-to-end IMRT QA audit process are summarized in Figure 5.

13 Rev. February 2019
Figure 5. Flowchart of overall audit process.

14 Rev. February 2019
3.2 Pre-visit activities
The purpose of the pre-visit activities is to check the dosimetric data in the TPS, as used for patient IMRT
treatments, related to a radiotherapy treatment unit equipped with an MLC. This will help the auditor to
assess the TPS configuration before the audit.
3.2.1 Pre-visit MLC tests
The participating institution is requested to undertake several activities before the actual audit can take
place. For special technologies such as TomoTherapy and CyberKnife these activities may have to be
adapted.
They include:
Test A. Calculation of MLC shaped small field output factors in the treatment planning system (TPS) Test B. Calculation of MLC in-plane and cross-plane profiles for 2 x 2 cm2 in the TPS Test C. Picket fence/ band test on a linac
Test A. Calculation of output factors for small fields shaped with MLCs
Calculate the number of MUs for 5 MLC-shaped field sizes (10 × 10 cm2, 6 × 6 cm2, 4 × 4 cm2, 3 × 3 cm2 and 2 × 2 cm2) to deliver 10 Gy on axis at 10 cm depth, 100 cm source-to-surface distance in water using the TPS. Input data in the “Small Field OF” form (Appendix 1). Output factors will be automatically calculated.
The auditor will verify the institution’s output factors using published data [32;33]. A tolerance of ±3% for
2 x 2 cm2 and ±2% for larger fields will be applied [34].
1. Small field size output factors for Elekta and Siemens Accelerators: a 30 × 30 × 30 cm3 water phantom will be created in the TPS. The number of monitor units will be calculated to deliver 10 Gy to a point at a depth of 10 cm on the central axis at 100 cm SSD for each MLC-shaped field size set symmetrically about the central axis (10 × 10 cm2, 6 × 6 cm2, 4 × 4 cm2, 3 × 3 cm2 and 2 × 2 cm2).
2. Small field size output factors for Varian Accelerators: a 30 × 30 × 30 cm3 water phantom will be created in the TPS. The number of monitor units will be calculated to deliver 10 Gy to a point at a depth of 10 cm on the central axis, at 100 cm SSD for each MLC-shaped field size set symmetrically about the central axis (10 × 10 cm2, 6 × 6 cm2, 4 × 4 cm2, 3 × 3 cm2 and 2 × 2 cm2) with the secondary jaws kept at a fixed field size of 10 × 10 cm2.

15 Rev. February 2019
Figure 6. Example of a collimator arrangement for small fields on Varian linacs.
Test B. Calculation of MLC-shaped small field profile
1. For the 2 x 2 cm2 MLC-shaped field, use the virtual water phantom and calculate the number of MUs
to deliver 6 Gy to the isocentre at 10 cm depth, 100 cm source-to-axis distance (SAD) using the TPS. The dose distribution will be computed with a calculation grid resolution of 1 mm. The cross-plane (in the direction of MLC movement) and in-plane (perpendicular to the MLC leaf movement) profiles are generated at 10 cm depth and extracted from the TPS either as a line profile, transversal dose plane or dose cube. Please make sure that the length of profile is at least 5 cm in each direction from the central axis.
Figure 7. Example of schematic for generating a field profile for small fields in the direction of MLC movement (cross-plane). The minimum gaps for opposing leaves required for some MLCs are not shown in the figure.

16 Rev. February 2019
The field size and the penumbra width (20%-80%) are calculated from the submitted profiles and
compared to measured baseline data. Differences greater than ±3 mm could be considered for further
follow up.
Test C. Picket fence test/band test on linac
Depending on the dose delivery methods, one of the following tests should be performed:
• picket fence test (leaf openings as used locally or minimum achievable leaf openings, 3 cm gap between strips, 5 strips of all MLC length) [35;36].
• band test (1 cm strip, 2 cm gap between strips, 11 strips of all MLC length) [37;38].
1. Perform picket fence test (for dynamic MLC delivery) or band test (static MLC delivery) on film or EPID. For film measurements, position the film isocentrically on solid slab phantom (SAD = 100 cm) and add at least dmax thickness of build-up material (e.g. 1.5 cm for 6 MV). For EPID image position it as close to the isocentre as possible and provide the source detector distance. Provide set-up information in “MLC test” tab in Appendix 1.
2. Submit the MLC configuration screenshot (guidelines available in “MLC configuration” tab in Appendix 1) and scanned image in a .tif format or DICOM file to the auditing organisation.
(a)
(b)
Figure 8. Examples of MLC performance test results (a) picket fence test, (b) band test.
The results for leaf positions for picket fence test and band fence test within ±0.5 mm and ±1 mm,
respectively, are considered acceptable. Results outside these limits could be followed up.
3.2.2 Pre-visit planning process The clinical test case is designed to simulate a patient IMRT H&N plan with a nasopharyngeal tumour. A
CT scan set of the phantom will be supplied several weeks prior to the audit in DICOM format with

17 Rev. February 2019
structures associated with targets and OARs. Note that each SHANE phantom is slightly different and
comes with a unique identifier and a unique set of contours. These include clinical target volumes (CTV),
planning target volumes and structures relating to the measurement positions of the ion chamber. No
adaptation of these volumes or their names is allowed. However, additional structures may be created by
the institution to guide the planning process.
This exercise is designed without using the usual clinical immobilization devices such as head rests and
masks. Correction factors for attenuation of the base of the face mask holder are not tested in this audit.
Couch attenuation needs to be accounted for as per clinical practice at the institution. The details of how
this is handled in the clinic need to be described in General Information tab of Appendix 1.
This CT scan set has been sent in advance to allow the planning process to be undertaken prior to the site
visit and the preliminary plan must be submitted to the auditor for review. This must be done before the
site visit can be confirmed. The CT images and structure sets sent from the auditing organisation will be
uploaded to the local TPS and processed as a new patient. Volumes of each structure will be checked
against the values established for a particular SHANE phantom (example given in Table 2) to ensure that
no slices are missing, or major adaptation to the structure have taken place, noting that some small
volume differences may be due to the TPS volume calculation. Additional planning structures may be
added to aid the planning process, but the imported structures must not be edited nor renamed.
TABLE 2. Structure sets for a prototype SHANE phantom. Note that volumes for other SHANE phantoms
may differ.
Structure name Description Nominal
volume, cm3
Min volume,
cm3
Max volume,
cm3
PTV_7000 Nasopharynx primary plan target
volume
88.5 87.6 89.4
PTVn1_6000 Involved nodes plan target volume 411.6 397.2 426.0
PTVn2_5400 Elective nodes plan target volume 260.3 244.7 275.9 SpinalCord Spinal cord organ at risk 24.9 22.8 27.0
SpinalCord_03 Spinal cord Plan Risk Volume 3mm 55.1 50.1 60.1
BrainStem Brain stem organ at risk 43.9 42.6 45.2 BrainStem_03 Brian stem Plan Risk Volume 3mm 72.5 71.4 73.6
Parotid_L Contralateral left parotid 19.7 18.9 20.5
Parotid_R Ipsilateral right parotid 23.4 22.5 24.3 IC_PTV_7000 Ion chamber volume in nasopharynx 0.13 0.1 0.2
IC_PTVn1_6000 Ion chamber volume in involved nodes 0.13 0.1 0.2
IC_PTVn2_5400 Ion chamber volume in elective nodes 0.13 0.1 0.2
IC_SpinalCord Ion chamber volume in spinal cord 0.13 0.1 0.2
Channel_1 Channel for IC_PTV_7000 42.0 37.8 46.2
Channel_2 Channel for IC_PTVn1_6000 42.0 37.8 46.2 Channel_3 Channel for IC_PTVn2_5400 42.0 37.8 46.2
Channel_4 Channel for IC_SpinalCord 42.0 37.8 46.2

18 Rev. February 2019
Using the usual local planning technique, a plan is generated aiming to achieve the dose constraints
shown in Table 3 and the resulting plan should be clinically acceptable. For the purpose of this audit, the
ICRU-83 [39] recommendations should be followed, e.g. the reporting of D50 as a prescription dose.
Prescriptions are similar to PARSPORT [40] and RTOG 0022 [41]. The amount of time to prepare the plan
will be consistent with a typical clinical H&N plan in the department.
TABLE 3: Dose-volume constraints for the H&N plan.
Structure Volume Dose Planning priority*
PTV_7000 (primary nasopharynx) 98% >90% (63.0 Gy) 2
95% >95% (66.5 Gy)
50% =100% (70.0Gy)
2% <107% (74.9 Gy)
PTVn1_6000 (involved nodes) 98% >90% (54.0Gy) 3
95% >95% (57.0Gy)
50% 60.0-62.0 Gy
PTVn2_5400 (elective nodes) 98% >90% (48.6Gy) 4
95% >95% (51.3Gy)
50% 54.0-56.0 Gy
SpinalCord 2% <45Gy 1
SpinalCord_03 2% <50Gy
BrainStem 2% <50Gy 1
BrainStem _03 2% <55Gy
Parotid_L Mean <24Gy 5
Parotid_R Mean as low as possible 6
*Planning priority: 1- highest, 6-lowest.
The plan will be generated to deliver 70 Gy in 30 fractions to the PTV_7000.
The priority order of planning aims will be the following:
1. Sparing of spinal cord and brainstem.

19 Rev. February 2019
2. Coverage of PTV_7000
3. Coverage of PTVn1_6000
4. Coverage of PTVn2_5400.
5. Sparing of the Parotid_L (contralateral)
6. Sparing of the Parotid_R (ipsilateral).
If the parotid glands cannot be spared without compromising target coverage then a higher parotid dose
should be accepted. The plan will be calculated using the usual algorithm, heterogeneity corrections and
calculation grid resolution.
A dose volume histogram (DVH) will be calculated for each of the given structures and doses achieved will
be checked against the dose volume constraints. Once the plan is finalised the doses achieved will be filled
into the plan reporting form (Pre-plan results table given in Appendix 1).
To test the deliverability of the plan, prior to submission, the institution will undertake patient -related
QA, as per local routine, to ensure that the plan is both deliverable and gives locally satisfactory QA results.
The QA results should be sent to the auditing organisation.
DICOM files (RT dose, RT plan, RT structure set and CT images) of the pre-audit plan will be sent
electronically to the national auditor, with the “Pre-plan results” given in Appendix 1.
Eventually, the data will be reviewed by the auditor using appropriate metrics. As a minimum, the
homogeneity index for the ion chamber volumes and the total number of monitor units should be
assessed. The treatment plan will be reviewed by comparing the calculated results with the planning
objectives. Homogeneity indices will be calculated using the template given in “Pre-plan results” tab in
Appendix 1. Advanced plan evaluation software tools may also be used by the national auditing
organisations for plan quality comparison between institutions.
The IMRT plan generated in this exercise should be verified following the procedure used routinely in the
clinic. Results are to be reported in “Pre-plan QA” given in Appendix 1.
3.2.3 On-site visit
Preparation of the dosimetry system for audit
The following equipment is required for the audit: CIRS SHANE phantom, calibrated Semiflex ion chamber,
electrometer, box of film (minimum of 4 sheets), cotton gloves, slabs of solid water, including a slab drilled
to take the Semiflex (or similar volume chamber), auditors pack (including Appendix 2).
The Semiflex ion chamber should have been calibrated and characterized prior to the national audit. The
calibration table for kQ against TPR should be taken to all sites for correct application of kQ (as defined in
TRS 398 [42]). The Semiflex cable should be marked with a red and a blue mark to indicate the position of
maximum insertion into the red and blue channels (see Figure 2b). This ensures that the ion chamber
stays fully in position and has not been ejected by air pressure.

20 Rev. February 2019
At all times, the film should be handled whilst wearing gloves. Prior to irradiation the calibration film
should be cut into 10 pieces of 6 x 6 cm2. It is recommended that orientation is marked on the film prior
to cutting.
During the site visit a local CT scan of the phantom will be made using the local standard head and neck
protocol and registered with the pre-visit scan. The structures and the pre-visit plan should then be
transferred to the local CT data set and the plan should be re-calculated, compared to the pre-visit plan
and re-optimised if needed.
3.2.4 CT scanning The phantom is received by the local responsible physicist. The audit process begins with a CT scanning of
the phantom using the typical protocol used by the institution for head and neck IMRT treatments. The
entire phantom will be imaged including the shoulder region which contains electron density inserts. The
phantom will be positioned on the CT couch and will be aligned using the external reference crosses. In
addition, the phantom will be aligned longitudinally using the marks at the chest and shoulder levels. Ion
chamber channels will be filled with the corresponding solid rods with radiopaque markers (BBs, ceramic
spheres of 1.5 mm diameter), see Figure 2 b. The vial supplied for the density calibration will be filled with
water. Upon the completion of this procedure the phantom should be transferred to the treatment room
to acclimatize.
This process requires no more than 45 minutes.
3.2.5 Treatment plan
The local CT images will be transferred to the TPS and the corresponding HU versus electron density curve
will be reviewed. Density values within 20 HU for plastic and 10 HU for water [43] are acceptable. Using a
region of interest (ROI) of 1 cm diameter for the electron density plugs and averaging over two slices,
measurements of the TPS calculated density of the known structures (see Figure 4) will be performed and
the data will be entered in the IMRT audit reporting form (“CTtoRED” tab Appendix 2).
To transfer clinical structures from the reference CT data set to the local clinical CT data set, the local
clinical CT images will be co-registered with the reference CT data and the given structures will be copied
over. Volumetric verification of each of the imported structures will be made and recorded in the “Volume
verification” tab in Appendix 2. To verify the registration, the centre of the individual chamber volumes
will be compared to the location of the BBs and should be within 1 mm. Once verified, density or HU of
ionization chamber structures should be assigned to that of water.
The pre-plan will be recalculated using the planning CT data and the usual calculation grid resolution for
H&N IMRT plans. The recalculated plan will be reviewed by the auditor and compared to the pre-plan
considering the planning constraints. If necessary the plan will be re-optimized. Once the plan is ready the
auditor will record the DVH values for all targets (D98%, D50% and D2%) and OAR in the IMRT audit reporting
form (the “Final plan results” tab, Appendix 2). The mean, minimum and maximum doses from the ion
chamber structures will be recorded for dose measurement comparison. Coronal dose distribution at the

21 Rev. February 2019
film position will be saved in a DICOM RT format. Patient specific IMRT plan QA will be performed using
the local procedure and results should be reported in “Final plan QA” tab in Appendix 2
To confirm the machine calibration, a reference plan on a slab homogeneous phantom with a 10 x 10 cm2
field size at SAD=100 cm and 5 cm depth will be created and MU calculated to give 2 Gy (MUref). The
reference plan will be sent to the R&V system and the plan parameter transfer will be verified. This
arrangement will also be used for film calibration.
This process requires approximately 3 hours or more.
3.2.6 Audit site visit measurements
The on-site measurement programme will include a beam output check with an ionization chamber, MLC
tests and dosimetric verification of the final H&N IMRT plan on SHANE using ion chamber and Gafchromic
film measurements.
The slab phantom and SHANE should be placed in the irradiation room at least 12 hours in advance of the
irradiation to allow temperature stabilization. Before starting the measurements, the electrometer and
ion chamber should be connected and polarized. A dose of approximately 5 Gy should be delivered to
stabilize the measurement system. Ion chamber leakage should be checked.
Using 30 x 30 cm2 slab solid water phantom the following procedures should be performed:
• Ion chamber measurement (Mref) for a 10 x 10 cm2 field size at 10 cm depth and SAD=100 cm and MU
= MUref, as described above. Use IAEA TRS398 [42] or equivalent dosimetry code of practice to
determine the dose. The measurements should be recorded in the “Output check” tab of Appendix 2.
• Film calibration, using a 10 x 10 cm2 field size, 10 cm depth and SAD = 100 cm, for a dose range of 1.0
to 10.0 Gy, in 1.0 Gy steps. The MU used for each film irradiation should be recorded in the “Film
Dosimetry” tab, Appendix 2.
• Film irradiation should be performed with a small field 2 x 2 cm2 at a depth of 10 cm on the central
axis at 100 cm SAD; the film size should be at least 15 x 15 cm2 to measure the leaf transmission (see
Sec. 3.2.1 Test B).
3. Film based MLC positioning test should be performed using a picket fence (dynamic IMRT and VMAT) or a band test (step & shoot IMRT) at SAD = 100 cm. At least dmax thickness of build-up material (e.g. 1.5 cm for 6 MV) should be added. The test should be recorded in “MLC test” tab in Appendix 2.
Prior to the SHANE anthropomorphic phantom irradiation, the treatment plan should be transferred to
the local QA equipment in preparation to carry out the local patient specific IMRT QA as is typically done
for local IMRT H&N cases. This must be done by the local physicist using the local procedures and
equipment.
SHANE will be positioned and aligned on the treatment couch. The local set up verification procedure with
on-board imaging (IGRT) for example CBCT, portal imaging, ExacTrac, etc. should be used for the phantom

22 Rev. February 2019
reference position determination. Any shifts between the laser and IGRT set-ups should be recorded.
Reference images should be obtained from the TPS in DICOM RT Image or .bmp formats for the IMRT plan.
The whole IGRT chain from reference images to localisation/portal images of the anthropomorphic
phantom should be checked by comparing the reference images with the images from the IGRT
measurements. The same set-up procedure will be followed for repositioning the phantom between
measurements. If the difference between the planned and the actual phantom positions is more than 1
mm, positioning adjustments will be necessary.
The SHANE measurements will be performed with a 0.125 cc ionisation chamber. For this, the ion
chamber will be introduced into one of four SHANE measurement channels, to the predefined position,
using the corresponding chamber cavity rod. The ion chamber positions have been described above (see
Figure 2) and are as follows:
• IC_PTV_7000
• IC_PTVn1_6000
• IC_PTVn2_5400
• IC_SpinalCord
To be placed correctly, the ion chamber should be pushed to the end of the cavity rod indicated by the
red and blue marks on its cable. It is advisable to fix the chamber cable (e.g. by taping it to the couch) to
make sure that the chamber does not slide and that it remains in its correct position throughout the
measurement session. Other SHANE channels should be filled with solid plugs. The procedure should be
repeated for the SHANE irradiations for the three remaining channels as given above.
The treatment plan should be delivered through the usual R&V system. The system settings should allow
all 30 fractions can be delivered in a single day in order not to interrupt the measurement sessions. Ion
chamber measurements for all fields should be acquired and repeated twice for reproducibility checking.
If the difference between the two measurements is greater than 0.5%, a third measurement should be
performed. If the results of the three measurements vary by more than 1% further follow up is required.
For evaluation purposes, ion chamber measurements need to be converted to dose using TRS398 [42] or
equivalent code of practice. The dose values have to be recorded in the IMRT audit reporting form
(“IMRT measurements in SHANE” tab, Appendix 2).
Once the ion chamber measurements are done, the film will be irradiated in SHANE. The film will be
positioned into the phantom coronal plane and pressed hard on the pins to generate film registration
marks. With the phantom reassembled, the phantom positioning will be adjusted and verified using the
lowest dose imaging technique available. Three fractions of the total plan will be delivered such that the
film is irradiated to a prescribed dose of approximately 7 Gy.
After irradiation, the film will be stored in an envelope until analysis.
Overall measurement sessions require about 5-7 hours depending on IMRT delivery technique.

23 Rev. February 2019
3.3 On-site analysis
Upon the completion of on-site irradiations and measurements, the auditor will have obtained the
following:
A. Filled in IMRT audit reporting form B. DICOM IMRT plan from TPS (DICOM RT plan, RT structures, RT dose and CT images) C. Irradiated films.
To facilitate the data collection and analysis an Excel file “IMRT audit reporting form” is provided (Appendix 2). The TPS calculated doses and electrometer readings will be typed in and the measured dose will be calculated according to the formalism laid out in IAEA TRS398 [42].
For the evaluation of the measured and TPS calculated values the following equation is used [43]:
Deviation [%] = 100*(Dcal-Dmeas)/Dmeas where Dmeas is the dose value measured at the measurement point.
Additionally, the ratio Dmeas/Dcal will be reported.
The comparison of the ion chamber measured and calculated dose values use the agreement criterion of
5% for PTVs and 7% for the spinal cord.
Further data analysis will be performed post visit.
3.4 Post visit analysis
3.4.1 Filled-in IMRT audit reporting form
The national auditing organisation will review the forms for completeness of information and if necessary
ask for missing/additional information from the audited institution.
3.4.2 Film analysis procedures The films irradiated during the audit including the calibration films, small field irradiated film, the picket
fence/band test film and the coronal plane film from the SHANE anthropomorphic phantom, will be
analysed by the national auditing organisation equipped with specialised hardware and software.
Analysis of MLC tests
The picket fence/band tests will be used to confirm that on the audit date the MLC on the treatment unit
performed as expected. The MLC leaf bias and leaf positioning will be evaluated. Acceptance criteria of
the AAPM and Netherlands working groups [44;45] will be adopted.
The film measured small field profiles will be compared with the TPS generated profiles. The field width
at the 50% dose level and the penumbra width will be evaluated. The agreement between the measured
and calculated data should be within 2 mm and 3 mm, respectively.
Dose distribution analysis
DICOM IMRT plan files from the TPS will be reviewed to assess the general quality of treatment plan.

24 Rev. February 2019
The coronal plane dose distribution will be used to compare the TPS calculated dose distribution with the
film measurements. Gamma analysis will be performed with the following parameters: ROI as defined by
film pin marking, threshold of 20%, normalized to the dose averaged over a small area located in
PTV_7000 in high dose, low gradient region; global gamma, 3%/3 mm. Additional analysis will be
performed for 3% /2 mm and local gamma index analysis. Sample data are shown in Figure 9.
Figure 9. Gamma analysis (right) of the TPS calculated dose distribution (left) with the film
measurements.
3.5 Reporting
A report of the outcome of the audit including all tests will be provided by the auditor using the template
given in Appendix 2. The full audit report should be sent to the local responsible physicist and an
anonymous summary of the audit results will be sent to the IAEA. Ensure all files are named according to
the protocol “Country [XXX]_ Institution [nr]_ audit [nr], e.g. CRO_1_1.
The report should include the following statement clarifying the responsibilities of the auditor and the
local institution:
“This audit was conducted as a ‘spot check’ of specific aspects of physics dosimetry relating to head and
neck IMRT. The responsibility for accuracy of clinical treatment delivery remains with the local institution,
and caution should be used in interpreting these results. It is expected that a full programme of
commissioning and routine quality assurance is performed by the local physics team.”
A brief description of how the audit was carried out will be given, and will include the following:
• Date and the location of the audit

25 Rev. February 2019
• Name, affiliation and contact details of the auditor
• Names, roles and contact details of the local institution staff
• Names of any additional staff who participated in the analysis or checking
• Data on linac, MLC and TPS type and version
• Data on software used for analysis and version number
• Traceability of calibration of ion chambers used
• Summary of the processes undertaken in order to prepare for the audit, e.g. CT scan, plan preparation, set-up of phantom, measurement of dose points, measurements with film.
• Details of treatment plan, e.g. number of fields, delivery technique
• Figure showing the measurement points
• Figure showing the coronal film position
• Specifics of gamma software including criteria and related parameters e.g. point of normalisation, thresholds used, dose difference, distance to agreement, global gamma calculation.
Results
Results from the audit should be given as follows:
A. Calculation of MLC shaped small field output factors on treatment planning system (TPS)
A table will be given of the locally calculated output factors and published output factors for the specific
linac and TPS, with tolerances shown. A comment will be made according to acceptability.
B. MLC profiles for 2 x 2 cm2
The TPS calculated profiles will be analysed against the measured film profiles. A comment will be made
according to acceptability.
C. Picket fence/band test on a linac
A figure will be given of the locally delivered profiles with tolerances shown. A comment will be made
according to acceptability.
D. Output Measurements The results of the output measurements should be tabulated showing the energy used, beam quality, temperature, pressure, field size, distance to the source, depth, MU and dose measured.

26 Rev. February 2019
E. Clinical test case results The results of the ion chamber audit measurements will be tabulated showing the expected values from
the TPS and the dose determined from the ion chamber measurements.
The results from the film analysis will be tabulated showing the percentage pass rate of the analysed
coronal plane for of the gamma criteria given above (Sec. 3.4.2).
Figures of the gamma maps should be shown highlighting the areas of pass and fail. A colour coding will
show regions of varying gamma.
Figure of the dose profiles from the film and the calculated results will be given. The agreement with the
criteria of acceptability will be presented.
Comments
Following the results section in the audit report, additional comments can be made as appropriate.
Recommendations
Recommendations can be given according to the results as to whether investigations and/or adaptations
should be made to the local treatment planning, beam modelling or calibration procedures.
3.6 Follow-up
For results outside of tolerance, further follow-up is required by the local staff, possibly with discussion
with the auditor. The auditor may request and review additional information that may help in identifying
the sources of deviations. If necessary, additional measurements may be needed and a possible follow-
up visit may be scheduled as requested by the institution.
While the auditor may provide advice to help resolve the issues, it is not the responsibility of the auditor
to solve them. It is the responsibility of the audited institution to ensure the quality and accuracy of its
own practice.

27 Rev. February 2019
REFERENCES
[1] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION (ICRP). Preventing Accidental Exposures from New External Beam Radiation Therapy Technologies, ICRP Publication 112, Annals of the ICRP 39 (4). 2009. Oxford, Pergamon Press.
[2] IBBOTT G.S., MOLINEU A., FOLLOWILL D.S. Independent evaluations of IMRT through the use of
an anthropomorphic phantom, Technol.Cancer Res.Treat., 5, (2006) 481-487.
[3] IZEWSKA J., ANDREO P., VATNITSKY S., SHORTT K.R. The IAEA/WHO TLD postal dose quality audits for radiotherapy: a perspective of dosimetry practices at hospitals in developing countries, Radiother.Oncol., 69, (2003) 91-97.
[4] AGUIRRE J.F., TAILOR R., IBBOTT G., STOVALL M., HANSON W. Thermoluminescence dosimetry as a tool for the remote verification of output for radiotherapy beams: 25 years of experience, ( Proceedings of the International Symposium on Standards and Codes of Practice in Medical Radiation Dosimetry, IAEA-CN-96/82, International Atomic Energy Agency (IAEA), Vienna, Austria (2002).
[5] GERSHKEVITSH E., PESZNYAK C., PETROVIC B., GREZDO J., CHELMINSKI K., DO CARMO LOPES M., IZEWSKA J. Results of the IAEA project on TPS audit in radiotherapy in Europe. PD-0336, Radioth.Oncol.(Supplement 1), 103, (2012) S138.
[6] GERSHKEVITSH E., SCHMIDT R., VELEZ G., MILLER D., KORF E., YIP F., WANWILAIRAT S., VATNITSKY S. Dosimetric verification of radiotherapy treatment planning systems: results of IAEA pilot study, Radiother.Oncol, 89, (2008) 338-346.
[7] DIMITRIADIS A., PALMER A.L., THOMAS R.A.S., NISBET A., CLARK C.H. Adaptation and validation of a commercial head phantom for cranial radiosurgery dosimetry end-to-end audit, Br.J Radiol, 90, (2017) 20170053.
[8] PALMER A., MZENDA B., KEARTON J., WILLS R. Analysis of regional radiotherapy dosimetry audit data and recommendations for future audits, Br.J Radiol, 84, (2011) 733-742.
[9] PALMER A.L., DIEZ P., GANDON L., WYNN-JONES A., BOWNES P., LEE C., AIRD E., BIDMEAD M., LOWE G., BRADLEY D., NISBET A. A multicentre 'end to end' dosimetry audit for cervix HDR brachytherapy treatment, Radiother.Oncol, 114, (2015) 264-271.
[10] CLARK C.H., HUSSEIN M., TSANG Y., THOMAS R., WILKINSON D., BASS G., SNAITH J., GOULDSTONE C., BOLTON S., NUTBROWN R., VENABLES K., NISBET A. A multi-institutional dosimetry audit of rotational intensity-modulated radiotherapy, Radiother.Oncol, 113, (2014) 272-278.
[11] HUMBERT-VIDAN L., SANDER T., EATON D.J., CLARK C.H. National Audit of a System for Rectal Contact Brachytherapy, Phys.Imag.Radiat.Oncol., 1, (2017) 1-5.
[12] PASLER M., KAAS J., PERIK T., GEUZE J., DREINDL R., KUNZLER T., WITTKAMPER F., GEORG D. Linking log files with dosimetric accuracy--A multi-institutional study on quality assurance of volumetric modulated arc therapy, Radiother.Oncol, 117, (2015) 407-411.

28 Rev. February 2019
[13] DUNN L., LEHMANN J., LYE J., KENNY J., KRON T., ALVES A., COLE A., ZIFODYA J., WILLIAMS I. National dosimetric audit network finds discrepancies in AAA lung inhomogeneity corrections, Phys Med., 31, (2015) 435-441.
[14] JORNET N., CARRASCO P., BELTRAN M., CALVO J.F., ESCUDE L., HERNANDEZ V., QUERA J., SAEZ J. Multicentre validation of IMRT pre-treatment verification: comparison of in-house and external audit, Radiother.Oncol, 112, (2014) 381-388.
[15] JURADO-BRUGGEMAN D., HERNANDEZ V., SAEZ J., NAVARRO D., PINO F., MARTINEZ T., ALAYRACH M.E., AILLERES N., MELERO A., JORNET N. Multi-centre audit of VMAT planning and pre-treatment verification, Radiother.Oncol, 124, (2017) 302-310.
[16] GERSHKEVITSH E., PESZNYAK C., PETROVIC B., GREZDO J. , CHELMINSKI K., DO CARMO L.M., IZEWSKA J., VAN DYK J. Dosimetric inter-institutional comparison in European radiotherapy centres: Results of IAEA supported treatment planning system audit, Acta Oncol, 53, (2014) 628-636.
[17] IZEWSKA J., SVENSSON H., IBBOTT G. Worldwide Quality Assurance Networks for Radiotherapy Dosimetry, ( Proceedings of the International Symposium on Standards and Codes of Practice in Medical Radiation Dosimetry, IAEA-CN-96/76, International Atomic Energy Agency (IAEA), Vienna, Austria (2002).
[18] IZEWSKA J., THWAITES D. IAEA Supported National Thermoluminescence Dosimetry Audit Networks for Radiotherapy Dosimetry, ( Proceedings of the International Symposium on Standards and Codes of Practice in Medical Radiation Dosimetry, IAEA-CN-96/137, International Atomic Energy Agency (IAEA), Vienna, Austria (2002).
[19] DAVIDSON S.E., POPPLE R.A., IBBOTT G.S., FOLLOWILL D.S. Technical note: Heterogeneity dose calculation accuracy in IMRT: study of five commercial treatment planning systems using an anthropomorphic thorax phantom, Med.Phys., 35, (2008) 5434-5439.
[20] MOLINEU A., FOLLOWILL D.S., BALTER P.A., HANSON W.F., GILLIN M.T., HUQ M.S., EISBRUCH A., IBBOTT G.S. Design and implementation of an anthropomorphic quality assurance phantom for intensity-modulated radiation therapy for the Radiation Therapy Oncology Group, Int.J.Radiat.Oncol.Biol.Phys., 63, (2005) 577-583.
[21] MOLINEU A., HERNANDEZ N., NGUYEN T., IBBOTT G., FOLLOWILL D. Credentialing results from IMRT irradiations of an anthropomorphic head and neck phantom, Med.Phys, 40, (2013) 022101.
[22] TAYLOR P.A., KRY S.F., ALVAREZ P., KEITH T., LUJANO C., HERNANDEZ N., FOLLOWILL D.S. Results From the Imaging and Radiation Oncology Core Houston's Anthropomorphic Phantoms Used for Proton Therapy Clinical Trial Credentialing, Int J Radiat Oncol Biol Phys, 95, (2016) 242-248.
[23] DISTEFANO G., LEE J., JAFARI S., GOULDSTONE C., BAKER C., MAYLES H., CLARK C.H. A national dosimetry audit for stereotactic ablative radiotherapy in lung, Radiother.Oncol, 122, (2017) 406-410.
[24] KERNS J.R., FOLLOWILL D.S., LOWENSTEIN J., MOLINEU A., ALVAREZ P., TAYLOR P.A., KRY S.F. Agreement Between Institutional Measurements and Treatment Planning System Calculations for

29 Rev. February 2019
Basic Dosimetric Parameters as Measured by the Imaging and Radiation Oncology Core-Houston, Int J Radiat Oncol Biol Phys, 95, (2016) 1527-1534.
[25] CARSON M.E., MOLINEU A., TAYLOR P.A., FOLLOWILL D.S., STINGO F.C., KRY S.F. Examining credentialing criteria and poor performance indicators for IROC Houston's anthropomorphic head and neck phantom, Med.Phys, 43, (2016) 6491.
[26] KRY S.F., MOLINEU A., KERNS J.R., FAUGHT A.M., HUANG J.Y., PULLIAM K.B., TONIGAN J., ALVAREZ P., STINGO F., FOLLOWILL D.S. Institutional patient-specific IMRT QA does not predict unacceptable plan delivery, Int J Radiat Oncol Biol Phys, 90, (2014) 1195-1201.
[27] FOLLOWILL D. Level of Accuracy Practically Achievable in Radiation Therapy , Med.Phys. 40 432. 2013.
[28] INTERNATIONAL ATOMIC ENERGY AGENCY (IAEA). Accuracy Requirements and Uncertainty in
Radiation Therapy (In press), International Atomic Energy Agency, Vienna, Austria (2014).
[29] CLARK C.H., AIRD E.G., BOLTON S., MILES E.A., NISBET A., SNAITH J.A., THOMAS R.A., VENABLES K., THWAITES D.I. Radiotherapy dosimetry audit: three decades of improving standards and accuracy in UK clinical practice and trials, Br.J Radiol, 88, (2015) 20150251.
[30] SANTANAM L., HURKMANS C., MUTIC S., VAN VLIET-VROEGINDEWEIJ C., BRAME S., STRAUBE W., GALVIN J., TRIPURANENI P., MICHALSKI J., BOSCH W. Standardizing naming conventions in radiation oncology, Int J Radiat Oncol Biol Phys, 83, (2012) 1344-1349.
[31] WEN N., GUAN H., HAMMOUD R., PRADHAN D., NURUSHEV T., LI S., MOVSAS B. Dose delivered from Varian's CBCT to patients receiving IMRT for prostate cancer, Phys.Med.Biol., 52, (2007) 2267-2276.
[32] FOLLOWILL D.S., KRY S.F., QIN L., LOWENSTEIN J., MOLINEU A., ALVAREZ P., AGUIRRE J.F., IBBOTT G.S. The Radiological Physics Center's standard dataset for small field size output factors, J.Appl.Clin.Med.Phys., 13, (2012) 3962.
[33] FOLLOWILL D.S., KRY S. Response to Thomsen et al.: Comments on "The Radiological Physics Center's standard dataset for small field size output factors", J.Appl.Clin.Med.Phys., 15, (2014) 4841.
[34] AZANGWE G., GROCHOWSKA P., IZEWSKA J. Quality Audits of Small Field Output Factors: A Multi-Centre Pilot Study., Physica Medica 30 (S1) 16. 2014.
[35] LOSASSO T., CHUI C.S., LING C.C. Physical and dosimetric aspects of a multileaf collimation system
used in the dynamic mode for implementing intensity modulated radiotherapy, Med.Phys, 25, (1998) 1919-1927.
[36] BOYER A., BIGGS P.J., GALVIN J., KLEIN E., LOSASSO T., LOW D., MAH K, YU C. AAPM Report No. 72. Basic Applications of Multileaf Collimators. Report of Task Group No. 50, Radiation Therapy Committee (https://www.aapm.org/pubs/reports/RPT_72.pdf Accessed 2017-10-14), Medical Physics Publishing, Madison, WI (2001).

30 Rev. February 2019
[37] BAYOUTH J.E., WENDT D., MORRILL S.M. MLC quality assurance techniques for IMRT applications, Med.Phys, 30, (2003) 743-750.
[38] EZZELL G.A., GALVIN J.M., LOW D., PALTA J.R., ROSEN I., SHARPE M.B., XIA P., XIAO Y., XING L., YU C.X. Guidance document on delivery, treatment planning, and clinical implementation of IMRT: report of the IMRT Subcommittee of the AAPM Radiation Therapy Committee, Med.Phys., 30, (2003) 2089-2115.
[39] INTERNATIONAL COMMISSION ON RADIATION UNITS AND MEASUREMENTS. ICRU Report 83: Prescribing, Recording, and Reporting Photon-Beam Intensity-Modulated Radiation Therapy (IMRT). 2010. Bethesda, Maryland, International Commission On Radiation Units and Measurements.
[40] NUTTING C.M., MORDEN J.P., HARRINGTON K.J., URBANO T.G., BHIDE S.A., CLARK C., MILES E.A.,
MIAH A.B., NEWBOLD K., TANAY M., ADAB F., JEFFERIES S.J., SCRASE C., YAP B.K., A'HERN R.P., SYDENHAM M.A., EMSON M., HALL E. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial, Lancet Oncol, 12, (2011) 127-136.
[41] RADIATION THERAPY ONCOLOGY GROUP (RTOG). Phase I/II Study of Conformal and Intensity Modulated Irradiation for Orophanryngeal Cancer (RTOG 0022). https://www.rtog.org/ClinicalTrials/ProtocolTable/StudyDetails.aspx?study=0022 (Accessed 2017-10-14). 2004. American College of Radiology, Clinical Research Center, Philadelphia, PA, Radiation Therapy Oncology Group (RTOG).
[42] INTERNATIONAL ATOMIC ENERGY AGENCY (IAEA). Absorbed Dose Determination in External
Beam Radiotherapy: An International Code of Practice for Dosimetry Based on Standards of Absorbed Dose to Water. IAEA TRS-398, International Atomic Energy Agency, Vienna (2000).
[43] INTERNATIONAL ATOMIC ENERGY AGENCY (IAEA). Commissioning and Quality Assurance of Computerized Planning Systems for Radiation Treatment of Cancer, IAEA TRS-430, International Atomic Energy Agency, Vienna, Austria (2004).
[44] MANS A., SCHURING D., ARENDS M., VUGTS L., WOLTHAUS J., LOTZ H., ADMIRAAL M., LOUWE R., OILERS M., VAN DE KAMER J. Code of Practice for the Quality Assurance and Control for Volumetric Modulated Arc Therapy. NCS Report 24, Netherlands Commission on Radiation Dosimetry (NCS),2015).
[45] KLEIN E.E., HANLEY J., BAYOUTH J., YIN F.F., SIMON W., DRESSER S., SERAGO C., AGUIRRE F., MA L., ARJOMANDY B., LIU C., SANDIN C., HOLMES T. Task Group 142 report: quality assurance of medical accelerators, Med.Phys., 36, (2009) 4197-4212.