Working draft for consultation DHB non-financial ...€¦ · Web viewWorking draft for...
202
Working draft for consultation DHB non-financial monitoring framework and performance measures 2016/17 2016/17 Working draft for consultation DHB non-financial monitoring framework and performance measures 1
Transcript of Working draft for consultation DHB non-financial ...€¦ · Web viewWorking draft for...
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
2016/17
Working draft for consultation
DHB non-financial monitoring framework and
performance measures
1
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
2016/17 DHB non-financial monitoring framework (working draft)Overview of changes to the measures proposed in the DHB monitoring framework for 2016/17 compared to 2015/16
One measure included in the 2015/16 framework (PP24 Improving Waiting Times – Cancer Multidisciplinary Meetings) is currently proposed for removal in 2016/17. The Ministry’s cancer team are currently confirming with their sector groups.
Both the previous More heart and diabetes checks health target, and the hospital component of the Better help for smokers to quit health target have been incorporated into the accountability measures for 2016/17. The previous’ More heart and diabetes checks’ target has been incorporated into the existing PP20 measure, and a new measure (PP31) has been created for the Hospital component of the ‘Better help for smokers to quit health target’.
Four existing measures have new deliverables included as indicated in the overview table below. (PP20, PP26, PP28, SI2)
Two measures, SI1 Ambulatory sensitive (avoidable) hospital admissions and OS 8 Acute readmissions to hospital, are undergoing a significant review of their definitions with sector input. Updates will be made available as definitions are confirmed.
Several measures are expected to have changes to definitions or deliverables incorporated for 2016/17 that are yet to be confirmed. Updates will be made available as definitions as decisions are finalised.
Overview – DHB heath targets 2016/17 to be confirmed following the Minister’s letter of expectations
Health target Target goalShorter stays in Emergency Departments
TBC
Improved access to elective surgery
TBC
Faster cancer treatment TBCIncreased immunisation TBCBetter help for smokers to quit
TBC
Childhood obesity target TBC
2

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
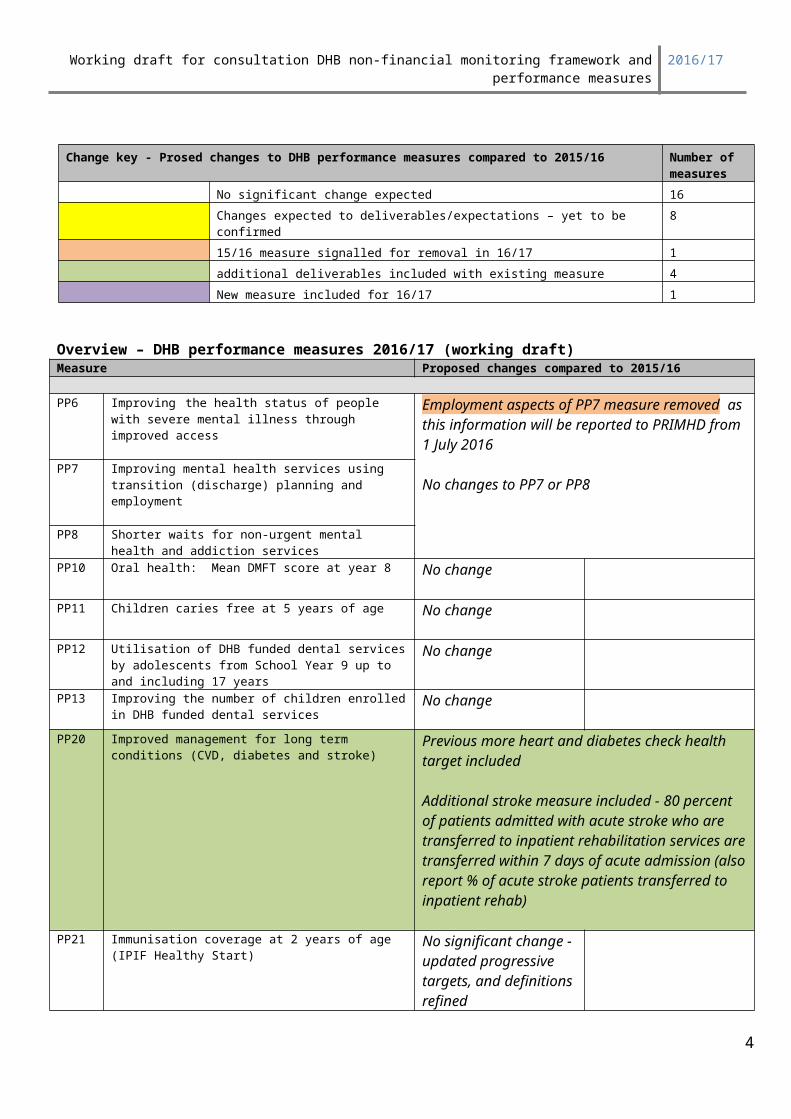
Change key - Prosed changes to DHB performance measures compared to 2015/16 Number of measures
No significant change expected 16Changes expected to deliverables/expectations – yet to be confirmed 815/16 measure signalled for removal in 16/17 1additional deliverables included with existing measure 4New measure included for 16/17 1
Overview – DHB performance measures 2016/17 (working draft)Measure Proposed changes compared to 2015/16
PP6 Improving the health status of people with severe mental illness through improved access
Employment aspects of PP7 measure removed as this information will be reported to PRIMHD from 1 July 2016
No changes to PP7 or PP8
PP7 Improving mental health services using transition (discharge) planning and employment
PP8 Shorter waits for non-urgent mental health and addiction services
PP10 Oral health: Mean DMFT score at year 8 No change
PP11 Children caries free at 5 years of age No change
PP12 Utilisation of DHB funded dental services by adolescents from School Year 9 up to and including 17 years
No change
PP13 Improving the number of children enrolled in DHB funded dental services
No change
PP20 Improved management for long term conditions (CVD, diabetes and stroke)
Previous more heart and diabetes check health target included
Additional stroke measure included - 80 percent of patients admitted with acute stroke who are transferred to inpatient rehabilitation services are transferred within 7 days of acute admission (also report % of acute stroke patients transferred to inpatient rehab)
PP21 Immunisation coverage at 2 years of age (IPIF Healthy Start)
No significant change - updated progressive targets, and definitions refined
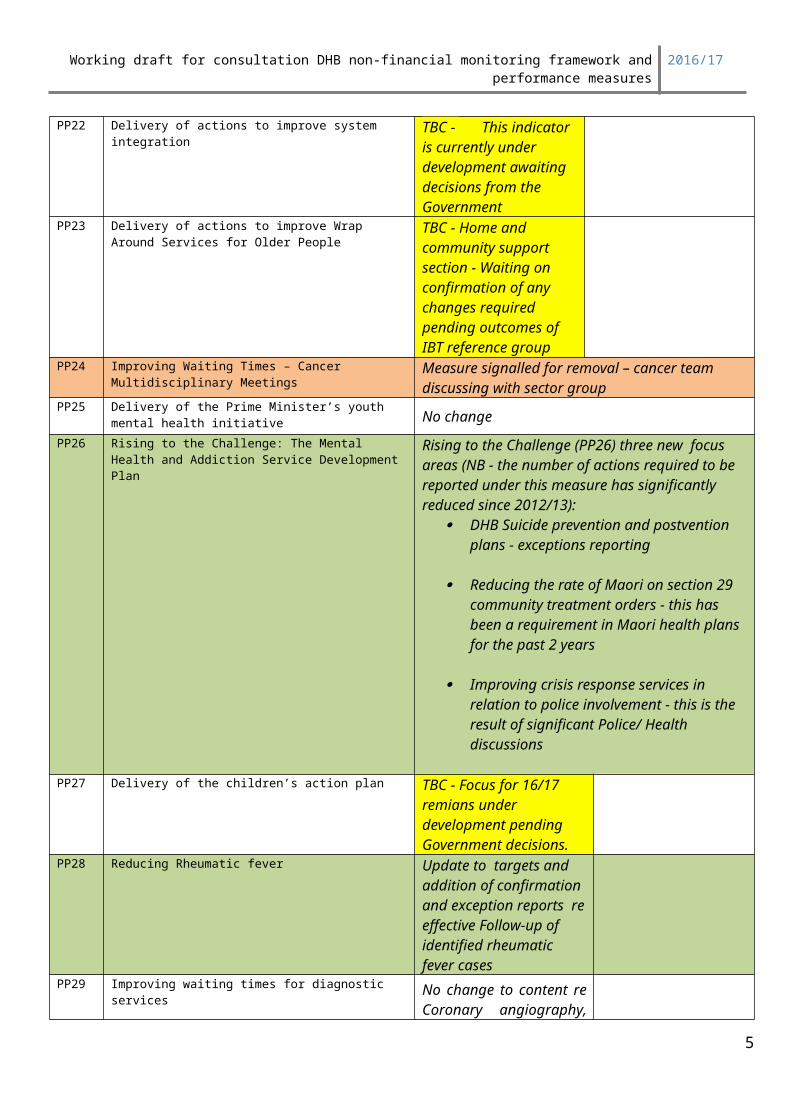
PP22 Delivery of actions to improve system integration
TBC - This indicator is currently under development awaiting decisions from the Government
PP23 Delivery of actions to improve Wrap Around Services for Older People
TBC - Home and community support section - Waiting on confirmation of any
3
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
changes required pending outcomes of IBT reference group
PP24 Improving Waiting Times – Cancer Multidisciplinary Meetings
Measure signalled for removal – cancer team discussing with sector group
PP25 Delivery of the Prime Minister’s youth mental health initiative No change
PP26 Rising to the Challenge: The Mental Health and Addiction Service Development Plan
Rising to the Challenge (PP26) three new focus areas (NB - the number of actions required to be reported under this measure has significantly reduced since 2012/13):
DHB Suicide prevention and postvention plans - exceptions reporting
Reducing the rate of Maori on section 29 community treatment orders - this has been a requirement in Maori health plans for the past 2 years
Improving crisis response services in relation to police involvement - this is the result of significant Police/ Health discussions
PP27 Delivery of the children’s action plan TBC - Focus for 16/17 remians under development pending Government decisions.
PP28 Reducing Rheumatic fever Update to targets and addition of confirmation and exception reports re effective Follow-up of identified rheumatic fever cases
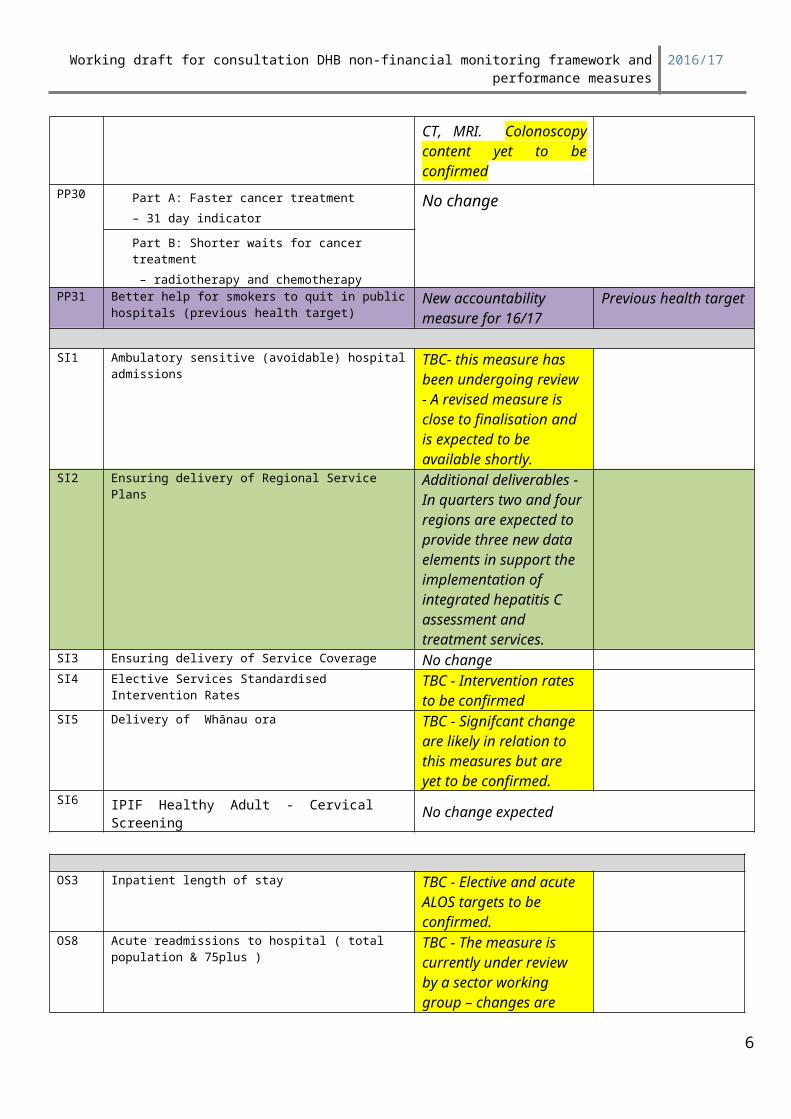
PP29 Improving waiting times for diagnostic services No change to content re Coronary angiography, CT, MRI. Colonoscopy content yet to be confirmed
PP30 Part A: Faster cancer treatment– 31 day indicator
No change
Part B: Shorter waits for cancer treatment – radiotherapy and chemotherapy
PP31 Better help for smokers to quit in public hospitals (previous health target)
New accountability measure for 16/17
Previous health target
SI1 Ambulatory sensitive (avoidable) hospital admissions
TBC- this measure has been undergoing review - A revised measure is close to finalisation and is expected to be available shortly.
SI2 Ensuring delivery of Regional Service Plans Additional deliverables - In 4
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
quarters two and four regions are expected to provide three new data elements in support the implementation of integrated hepatitis C assessment and treatment services.
SI3 Ensuring delivery of Service Coverage No changeSI4 Elective Services Standardised Intervention
RatesTBC - Intervention rates to be confirmed
SI5 Delivery of Whānau ora TBC - Signifcant change are likely in relation to this measures but are yet to be confirmed.
SI6 IPIF Healthy Adult - Cervical Screening No change expected
OS3 Inpatient length of stay TBC - Elective and acute ALOS targets to be confirmed.
OS8 Acute readmissions to hospital ( total population & 75plus )
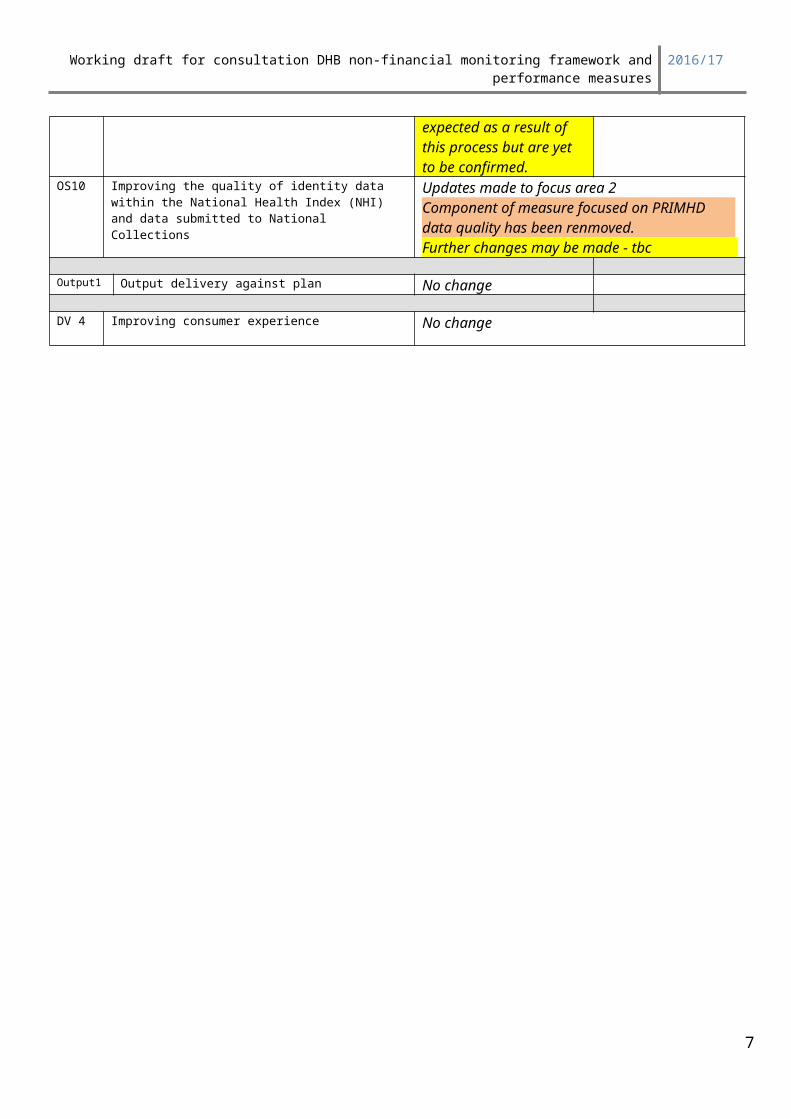
TBC - The measure is currently under review by a sector working group – changes are expected as a result of this process but are yet to be confirmed.
OS10 Improving the quality of identity data within the National Health Index (NHI) and data submitted to National Collections
Updates made to focus area 2Component of measure focused on PRIMHD data quality has been renmoved.Further changes may be made - tbc
Output1 Output delivery against plan No change
DV 4 Improving consumer experience No change
5
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
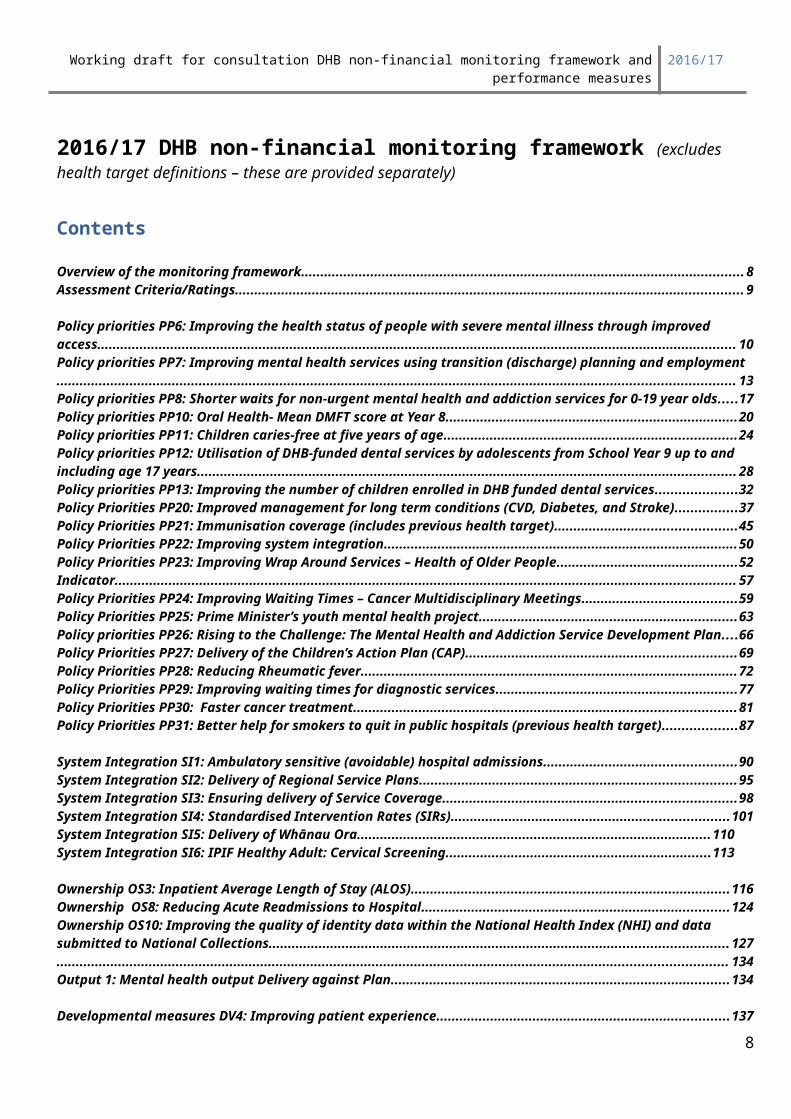
2016/17 DHB non-financial monitoring framework (excludes health target definitions – these are provided separately)
Contents
Overview of the monitoring framework....................................................................................................................... 8Assessment Criteria/Ratings........................................................................................................................................ 9
Policy priorities PP6: Improving the health status of people with severe mental illness through improved access........................................................................................................................................................................... 10Policy priorities PP7: Improving mental health services using transition (discharge) planning and employment....................................................................................................................................................................................... 13Policy priorities PP8: Shorter waits for non-urgent mental health and addiction services for 0-19 year olds....17Policy priorities PP10: Oral Health- Mean DMFT score at Year 8.............................................................................20Policy priorities PP11: Children caries-free at five years of age..............................................................................24Policy priorities PP12: Utilisation of DHB-funded dental services by adolescents from School Year 9 up to and including age 17 years................................................................................................................................................ 28Policy priorities PP13: Improving the number of children enrolled in DHB funded dental services....................32Policy Priorities PP20: Improved management for long term conditions (CVD, Diabetes, and Stroke)..............37Policy Priorities PP21: Immunisation coverage (includes previous health target)................................................45Policy Priorities PP22: Improving system integration..............................................................................................50Policy Priorities PP23: Improving Wrap Around Services – Health of Older People.............................................52Indicator........................................................................................................................................................................ 57Policy Priorities PP24: Improving Waiting Times – Cancer Multidisciplinary Meetings........................................59Policy Priorities PP25: Prime Minister’s youth mental health project.....................................................................63Policy priorities PP26: Rising to the Challenge: The Mental Health and Addiction Service Development Plan. 66Policy Priorities PP27: Delivery of the Children’s Action Plan (CAP).....................................................................69Policy Priorities PP28: Reducing Rheumatic fever...................................................................................................72Policy Priorities PP29: Improving waiting times for diagnostic services...............................................................77Policy Priorities PP30: Faster cancer treatment......................................................................................................81Policy Priorities PP31: Better help for smokers to quit in public hospitals (previous health target)...................87
System Integration SI1: Ambulatory sensitive (avoidable) hospital admissions...................................................90System Integration SI2: Delivery of Regional Service Plans...................................................................................95System Integration SI3: Ensuring delivery of Service Coverage.............................................................................98System Integration SI4: Standardised Intervention Rates (SIRs)..........................................................................101System Integration SI5: Delivery of Whānau Ora...............................................................................................110System Integration SI6: IPIF Healthy Adult: Cervical Screening......................................................................113
Ownership OS3: Inpatient Average Length of Stay (ALOS)...................................................................................116Ownership OS8: Reducing Acute Readmissions to Hospital...............................................................................124Ownership OS10: Improving the quality of identity data within the National Health Index (NHI) and data submitted to National Collections............................................................................................................................ 127..................................................................................................................................................................................... 134Output 1: Mental health output Delivery against Plan............................................................................................134
Developmental measures DV4: Improving patient experience..............................................................................137
6
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Overview of the DHB monitoring framework
ContextThe DHB monitoring framework was developed recognising a DHB funding and operating environment where: • DHBs have responsibility for making decisions on the mix, level and quality of health and disability
services, within the parameters of the NZ Health and Disability Strategies and nationwide minimum service coverage and safety standards.
• The Ministry of Health, as agent of the Minister of Health, defines nationwide service coverage, safety standards and the operating environment. The Minister enters into funding agreements with DHBs, containing DHB specific agreed performance targets, and may exercise reserve powers in the case of repeated performance failures.
DHB non-financial monitoring arrangements operate within wider DHB accountability arrangements including legislative requirements, obligations formalised via Crown Funding Agreements and other contractual requirements, along with formal planning documents agreed with the Minister of Health/Minister of Finance.
The measures included within the DHB non-financial monitoring framework are intended to cover a specific set of markers of DHB performance in key areas, rather than all health services or DHB activity. Views and perspectives about what is most important to monitor, measure, and report for accountability purposes change over time with changing priorities. As a result the monitoring framework is updated periodically, and the measures that populate the framework are updated annually.
The National Health Board (NHB) facilitates DHB planning and monitoring processes within the Ministry. Clinical and subject area experts are involved in all aspects of the monitoring work programme including: indicator design and definition; establishment of baselines; agreement of performance expectations; data supply and performance feedback; performance management and escalation of non-performance; reporting to Ministers and publication of results.
The NHB coordinates an annual review of the measures within the monitoring framework as part of the development of annual DHB planning advice. Working drafts are shared with DHBs for comment and feedback. If new measures are included in the framework, these measures must: incorporate intervention logic and a performance story linking the measure to sector outcomes provide clear and transparent deliverables including clearly defined numerators and denominators for
quantitative measures, with data sources clearly identified identify the actions DHB funders can take to influence performance, and activities DHBs can put in
place that have a proven impact on the measure identify the required detail and frequency of reporting identify clear performance expectations, including what constitutes achievement, partial achievement
and non-achievement of the measure.
The burden of reporting is also an important consideration. New measures need to be strongly justified before they are included in the framework, existing measures are generally required to be removed to make way for new measures and minimise indicator creep over time.
DHBs formally agree to deliver on the performance expectations associated with the measures in the DHB monitoring framework through DHB Annual Plans. The NHB facilitates the Annual Plan review and agreement process across the Ministry. Each individual measure owner reviews and approves performance expectation for their measures.
DHBs provide quarterly reports to the Ministry via a web based reporting tool. The quarterly reporting process is managed by the NHB who are responsible for ensuring all reports are supplied on time, and information flows appropriately. DHB performance against each target or measure is assessed by the
7
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Ministry measure owner/subject expert, and performance assessment and feedback is provided directly to DHBs via the web based reporting tool.
Where DHBs do not meet performance expectations, based on the definitions outlined in this document, the Ministry measure owner/subject expert determines whether the DHB has:
Partially achieved i.e. some or all expected performance expectations/deliverables associated with the measure not met, however there is a an appropriate resolution plan
Not achieved i.e. the deliverable is not met and the DHB does not have an adequate resolution plan.
Where a ‘not achieved’ assessment is made, the NHB facilitates performance escalation coordinated by DHB Relationship Managers and through formal monitoring and intervention processes where required. A monitoring and Intervention Framework is used by the Ministry to monitor and manage DHB performance, and provides for increasingly intensive levels of monitoring and, where necessary, intervention to ensure that issues relating to poor performance are addressed.
Based on the performance assessments undertaken by the Ministry measure owner/subject expert the NHB produces a dashboard style report for each DHB, summarising on one page performance for the quarter against key expectations agreed in accountability documents. The dashboards are used to report DHB performance to the Minister.
Overview of the monitoring frameworkThe current monitoring framework aims to provide the Minister with a rounded view of performance using a range of performance markers. Four dimensions are identified that reflect DHBs functions as owners, funders and providers of health and disability services. The four identified dimensions of DHB performance cover:• achieving Government’s priority goals/objectives and targets or ‘Policy priorities’ • meeting service coverage requirements and Supporting sector and inter-sector connectedness or
‘System Integration’
• providing quality services efficiently or ‘Ownership’
• purchasing the right mix and level of services within acceptable financial performance or ‘Outputs’.
:
Code Dimension
PP Policy Priorities
SI System Integration
OP Outputs
OS Ownership
DV Developmental – Establishment of baseline (no target/performance expectation is set)
8

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Assessment Criteria/RatingsUnless otherwise stated in the definition of the performance measure, the following performance assessment criteria will apply:
Rating Abbrev 0Criteria
Outstanding performer/sector leader
O
1. This rating indicates that the DHB achieved a level of performance considerably better than the agreed DHB and/or sector expectations.
2. For those measures, included in the Maori health plan, this rating is applied when the DHB has met the target agreed in its Annual Plan and has achieved the target level of performance for the Maori population group, and the Pacific population group.
Note: this rating can only be applied in the fourth quarter for measures that are reported quarterly or six-monthly. Measures reported annually can receive an ‘O’ rating, irrespective of when the reporting is due.
Achieved
A
1. Deliverable demonstrates targets / expectations have been met in full.
2. In the case of deliverables with multiple requirements, all requirements are met.
3. For those measures, included in the Maori health plan, this rating is applied when the DHB has met the target agreed in its Annual Plan and has achieved significant progress for the Maori population group, and the Pacific population group.
4. Data, or a report confirming expectations have been met, has been provided through a mechanism outside the Quarterly Reporting process, and the assessor can confirm.
Partial achievement
P
1. Target/expectation not fully met, (including not meeting expectations for Maori and Pacific population groups) but the resolution plan satisfies the assessor that the DHB is on track to compliance.
2. A deliverable has been received, but some clarification is required.
3. In the case of deliverables with multi-requirements, where all requirements have not been met at least 50% of the requirements have been achieved.
Not achieved– escalation required
N 1. The deliverable is not met.2. There is no resolution plan if deliverable indicates non-
compliance.3. A resolution plan is included, but it is significantly deficient.4. A report is provided, but it does not answer the criteria of the
performance indicator.5. There are significant gaps in delivery.6. It cannot be confirmed that data or a report has been provided
9
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
through channels other than the quarterly process.
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP6: Improving the health status of people with severe mental illness through improved accessEach DHB to report confirming access targets are met
Summary informationTarget/performance expectation
Agreed in DHB Annual Plan
Measure type and reporting frequency
Type: Data & exception
Reporting frequency: Six-monthly
Source information for reporting provided by:
Ministry to provide data via NSFL web site http://nsfl.health.govt.nz/accountability/performance-and-monitoringand the DHB quarterly reporting website
Quarterly reporting - standard timeline applies DHB Reports Due 20th of the month following the end of the quarter
Ministry Initial rating & feedback 8-10 working days from receiving reports
DHB Response due 5 working days from receiving initial ratings
Confirmed rating and feedback 4-5 working days from receiving DHB feedback
Link to outcomesDelivery of this measure supports the overarching outcome for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’.
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care*
Improved quality, safety and experience of care(individuals and their family/ focus focus)
10

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child HealthOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Through improving the health status of people with severe mental illness through improved access to a broad range of services, the DHB will contribute to the Ministerial priority of improving value for money by ensuring their mental health services and cost effective, results focused and have regard to the service impacts on people who are severely affected by mental illness. The DHB will provide people with better health and disability services by ensuring that the range of services closes existing service gaps, and making them easier to access.
Better access to a broad range of services improves people’s mental health and wellbeing, and contributes to recovery which impacts on the intermediate outcome to promote and protect good health and independence of New Zealanders who experience mental illness.
The DHB’s range of services will be of high quality, safe, evidence based and provided in the least restrictive environment. This focus is designed to provide better outcomes for people with mental illness and increase people’s confidence and trust in the health and disability system and services.
There are a number of DHBs that have not met minimum access levels particularly for children and youth. Further, improved performance against this measure will support delivery of Rising to the Challenge, The Mental Health and Addiction Service Development Plan 2012-2017, the Prime Minister’s Youth Mental Health project, Vulnerable Children’s work stream and the Drivers of Crime initiatives. One of the Drivers of Crime initiatives is to improve access rates to youth alcohol and drug services and is supported by $2 million funding stream. Rising to the Challenge, The Mental Health and Addiction Service Development Plan 2012-2017 and the Youth Mental Health project have clear expectations that access rates for 12-19 year olds will increase mental health and addiction services while also reducing waiting times.
Actions and activities are that have a proven impact on this measure:Examples of key activities undertaken to support improved access rates are: development of CAMHS services across all regions, packages of care for individuals with high and complex needs, mental health specialists at emergency departments, Kaupapa Maori services, eating disorder services and older people’s needs to manage dementia, are met by setting up psycho geriatric care. Integration of primary and secondary services will result in improving access to a wider range of services and impact on the referrals to specialist mental health services.
Deliverables definitionsNumerator: (Data Source: Ministry of Health)
11
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
The average number of people domiciled in the DHB region, seen per year rolling every three months being reported (the period is lagged by three months) for:
child and youth aged 0-19, specified for each of the three categories Māori, Other, and in total adults aged 20-64, specified for each of the three categories Māori, Other, and in total older people aged 65+, specified for each of the three categories Māori, Other, and in total.
Denominator: (Data Source: Ministry of Health)Projected population of the DHB region by age and ethnicity.
Interpreting Access RatesThere are at least four factors that can impact on making informed decisions regarding access rates both by DHB and nationally. These factors must be taken into consideration by all parties when negotiating targets. They are:
the more recovery-focused a service, the lower the likely demand will be for services. A point will be reached where access will stabilise at a particular rate that is likely to be unique to each DHB
the number and quality of primary ancillary mental health services (e.g. GPs, Private Counsellors, and Relationship Services) will have an impact on access rates to secondary mental health services
that there is a difference between determining serious mental illness epidemiologically, and a clinical assessment of what constitutes a serious mental illness
that only half of older peoples services are funded directly by mental health
Reporting Period Reporting required: Six monthly, as per the table below:
Quarter For the time periodQuarter 2 1 October – 31 December
Quarter 4 1 April – 30 June
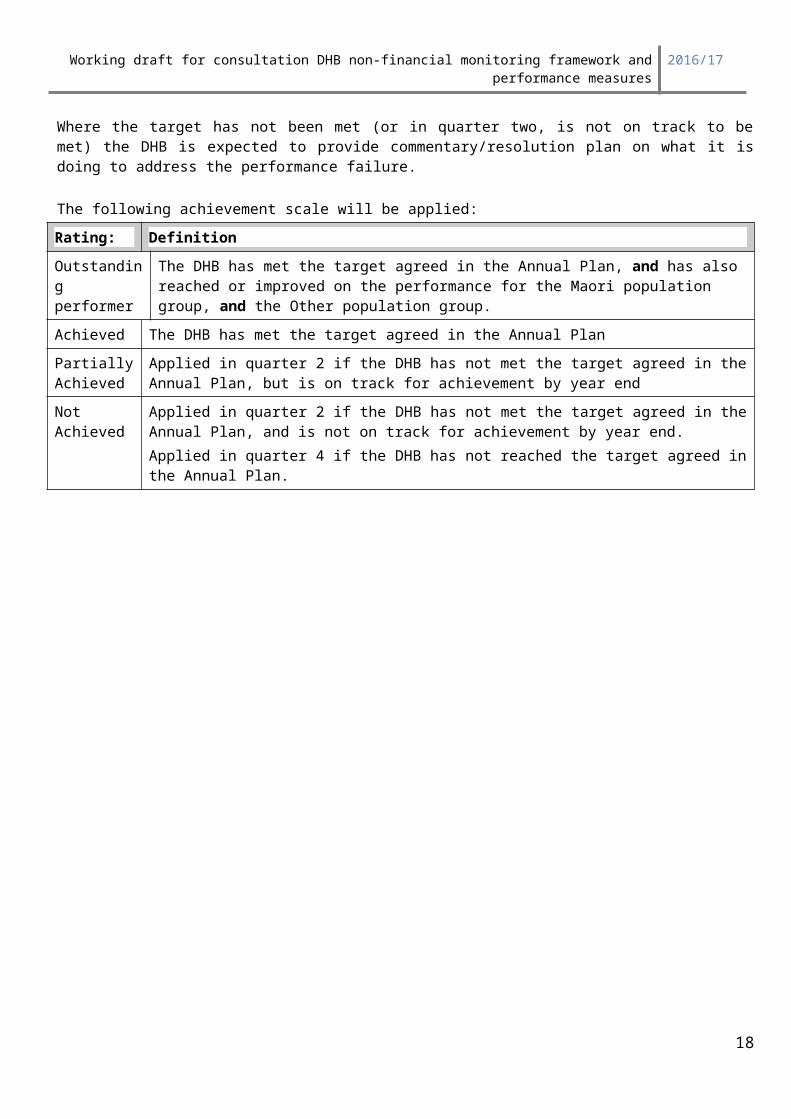
ExpectationsWhere the target has not been met (or in quarter two, is not on track to be met) the DHB is expected to provide commentary/resolution plan on what it is doing to address the performance failure.
The following achievement scale will be applied:
Rating: DefinitionOutstanding performer
The DHB has met the target agreed in the Annual Plan, and has also reached or improved on the performance for the Maori population group, and the Other population group.
Achieved The DHB has met the target agreed in the Annual Plan
Partially Achieved
Applied in quarter 2 if the DHB has not met the target agreed in the Annual Plan, but is on track for achievement by year end
Not Achieved
Applied in quarter 2 if the DHB has not met the target agreed in the Annual Plan, and is not on track for achievement by year end.Applied in quarter 4 if the DHB has not reached the target agreed in the Annual Plan.
12

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
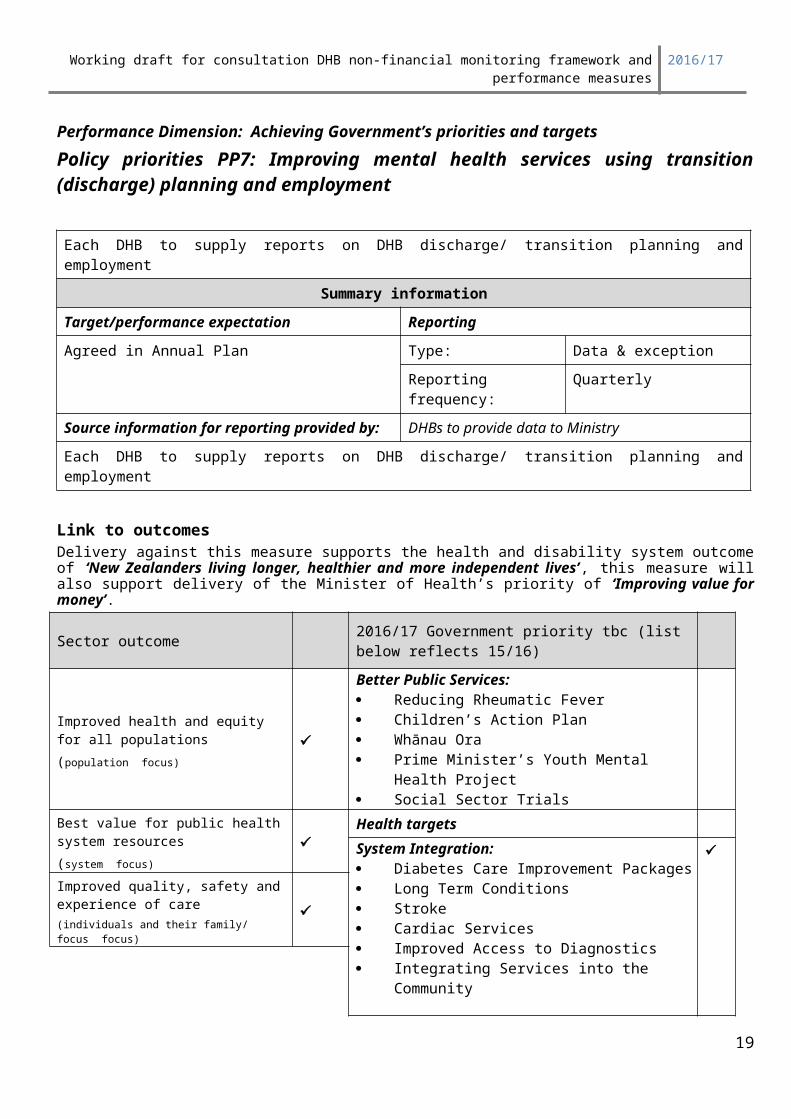
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP7: Improving mental health services using transition (discharge) planning and employment
Each DHB to supply reports on DHB discharge/ transition planning and employment
Summary informationTarget/performance expectation ReportingAgreed in Annual Plan Type: Data & exception
Reporting frequency: Quarterly
Source information for reporting provided by: DHBs to provide data to Ministry
Each DHB to supply reports on DHB discharge/ transition planning and employment
Link to outcomesDelivery against this measure supports the health and disability system outcome of ‘New Zealanders living longer, healthier and more independent lives’, this measure will also support delivery of the Minister of Health’s priority of ‘Improving value for money’.
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
13
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
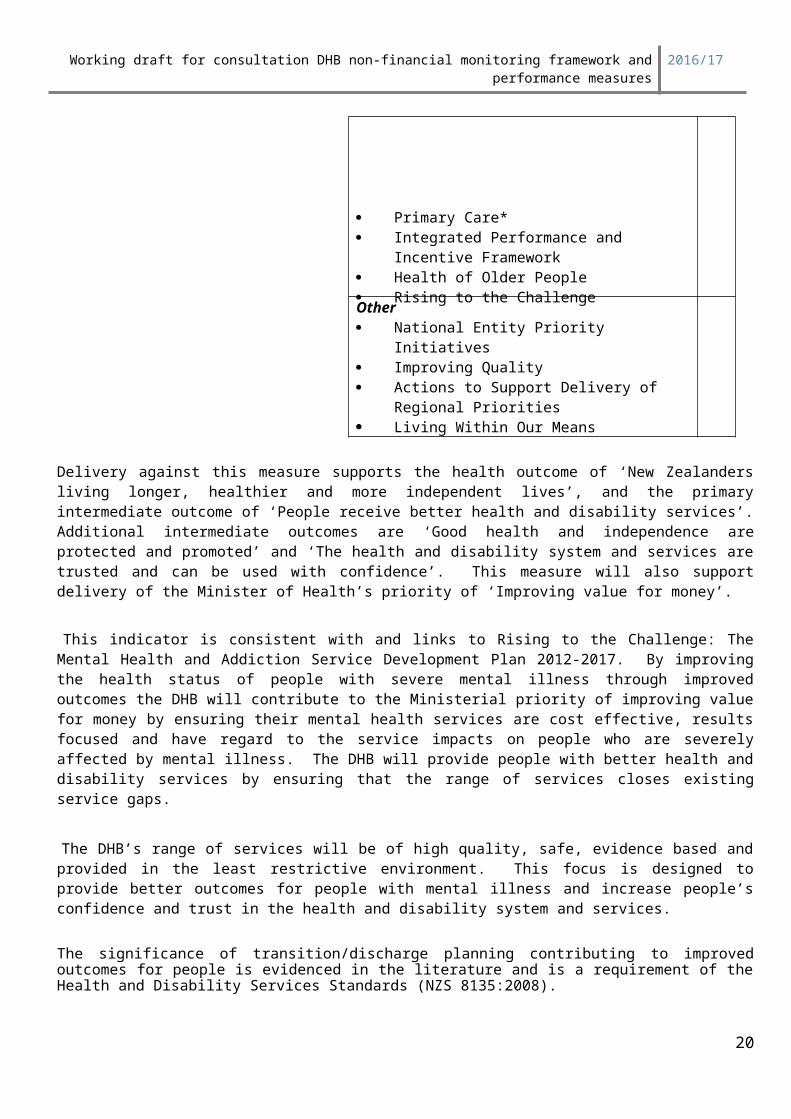
Delivery against this measure supports the health outcome of ‘New Zealanders living longer, healthier and more independent lives’, and the primary intermediate outcome of ‘People receive better health and disability services’. Additional intermediate outcomes are ‘Good health and independence are protected and promoted’ and ‘The health and disability system and services are trusted and can be used with confidence’. This measure will also support delivery of the Minister of Health’s priority of ‘Improving value for money’.
This indicator is consistent with and links to Rising to the Challenge: The Mental Health and Addiction Service Development Plan 2012-2017. By improving the health status of people with severe mental illness through improved outcomes the DHB will contribute to the Ministerial priority of improving value for money by ensuring their mental health services are cost effective, results focused and have regard to the service impacts on people who are severely affected by mental illness. The DHB will provide people with better health and disability services by ensuring that the range of services closes existing service gaps.
The DHB’s range of services will be of high quality, safe, evidence based and provided in the least restrictive environment. This focus is designed to provide better outcomes for people with mental illness and increase people’s confidence and trust in the health and disability system and services.
The significance of transition/discharge planning contributing to improved outcomes for people is evidenced in the literature and is a requirement of the Health and Disability Services Standards (NZS 8135:2008).
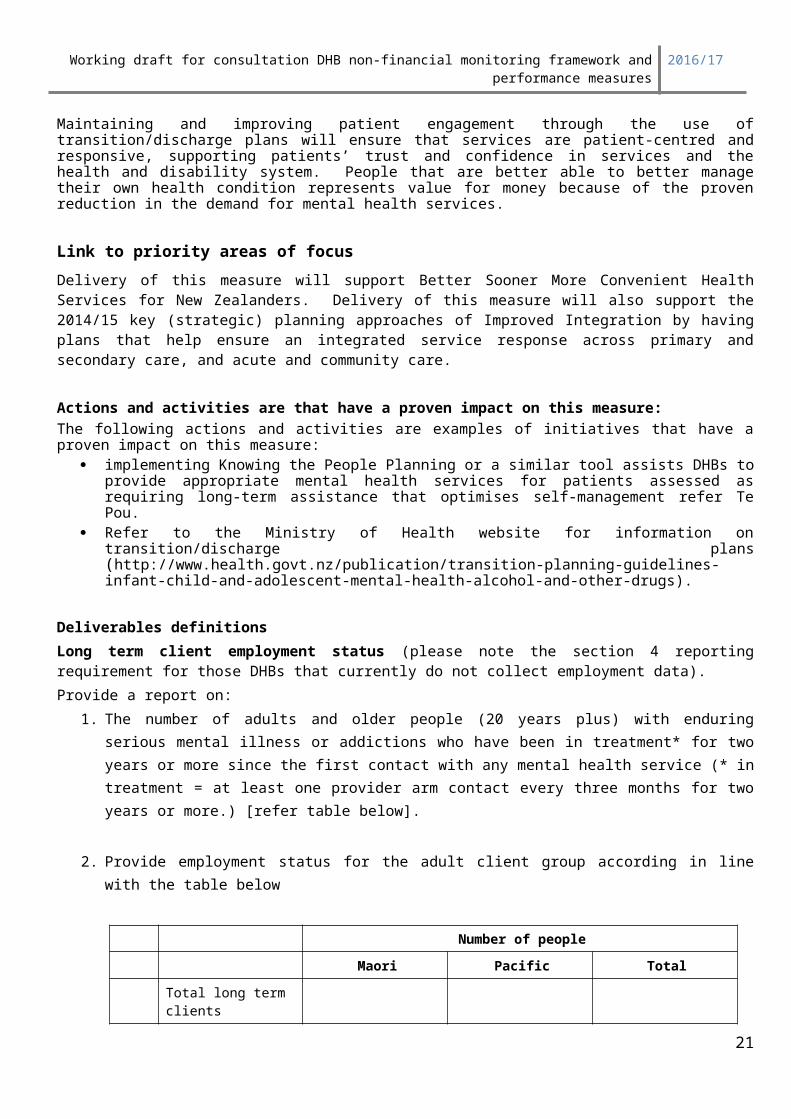
Maintaining and improving patient engagement through the use of transition/discharge plans will ensure that services are patient-centred and responsive, supporting patients’ trust and confidence in services and the health and disability system. People that are better able to better manage their own health condition represents value for money because of the proven reduction in the demand for mental health services.
Link to priority areas of focusDelivery of this measure will support Better Sooner More Convenient Health Services for New Zealanders. Delivery of this measure will also support the 2014/15 key (strategic) planning approaches of Improved Integration by having plans that help ensure an integrated service response across primary and secondary care, and acute and community care.
Actions and activities are that have a proven impact on this measure:The following actions and activities are examples of initiatives that have a proven impact on this measure:
implementing Knowing the People Planning or a similar tool assists DHBs to provide appropriate mental health services for patients assessed as requiring long-term assistance that optimises self-management refer Te Pou.
Refer to the Ministry of Health website for information on transition/discharge plans (http://www.health.govt.nz/publication/transition-planning-guidelines-infant-child-and-adolescent-mental-health-alcohol-and-other-drugs).
Deliverables definitions Long term client employment status (please note the section 4 reporting requirement for those DHBs that currently do not collect employment data).Provide a report on:
1. The number of adults and older people (20 years plus) with enduring serious mental illness or addictions who have been in treatment* for two years or more since the first contact with any mental
14

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
health service (* in treatment = at least one provider arm contact every three months for two years or more.) [refer table below].
2. Provide employment status for the adult client group according in line with the table below
Number of people
Maori Pacific Total
Total long term clients
1 In Paid employment >30 hrs a week
2 In Paid employment 1 - 30 hrs a week
3 Unemployed- less than 1 hour per week
3. Describe the methodology used to ensure adult measure long-term clients employment status. DHBs that have fully implemented KPP across their long-term adult population should state KPP as the methodology.
Reducing Inequalities focus
Deliverables 1 & 2 are to be reported by Māori and non-Māori.For those seven DHBs with high Pacific Island populations the percentage Pacific Island consumers in employment are also required to be reported
4. For those DHBs that do not collect this data please outline what actions are planned to collect this data (please note: the PRIMHD HISO code set contains supplementary indicator codes including employment and the intention is to collect this data in PRIMHD from June 2016).
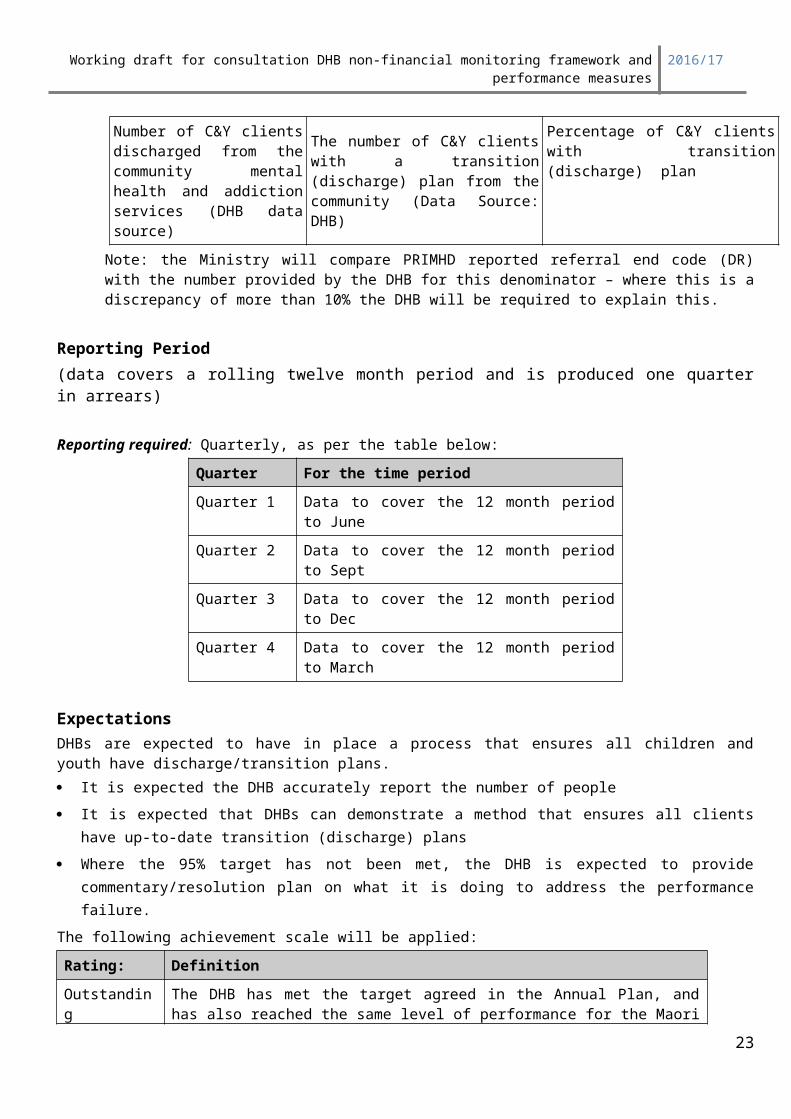
5 Child and Youth with a Transition (discharge) planAt least 95% of clients discharged will have a transition (discharge) plan.
NumeratorThe number of C&Y clients with a discharged from community mental health and addiction services with a transition (discharge plan) (Data Source: DHB)
Denominator: Number of C&Y clients discharged from the community mental health and addiction services (Data Source: DHB)
Number of C&Y clients discharged from the community mental health and addiction services (DHB data source)
The number of C&Y clients with a transition (discharge) plan from the community (Data Source: DHB)
Percentage of C&Y clients with transition (discharge) plan
15

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Note: the Ministry will compare PRIMHD reported referral end code (DR) with the number provided by the DHB for this denominator – where this is a discrepancy of more than 10% the DHB will be required to explain this.
Reporting Period (data covers a rolling twelve month period and is produced one quarter in arrears)
Reporting required: Quarterly, as per the table below:
Quarter For the time periodQuarter 1 Data to cover the 12 month period to June
Quarter 2 Data to cover the 12 month period to Sept
Quarter 3 Data to cover the 12 month period to Dec
Quarter 4 Data to cover the 12 month period to March
ExpectationsDHBs are expected to have in place a process that ensures all children and youth have discharge/transition plans. It is expected the DHB accurately report the number of people It is expected that DHBs can demonstrate a method that ensures all clients have up-to-date transition
(discharge) plans Where the 95% target has not been met, the DHB is expected to provide commentary/resolution plan on
what it is doing to address the performance failure.The following achievement scale will be applied:
Rating: DefinitionOutstanding performer
The DHB has met the target agreed in the Annual Plan, and has also reached the same level of performance for the Maori population group, and the non - Maori population group.
Achieved All agreed rates are met.
Partial Achievement
Some or all agreed rates are not met
Not Achieved All agreed rates are not met
16
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
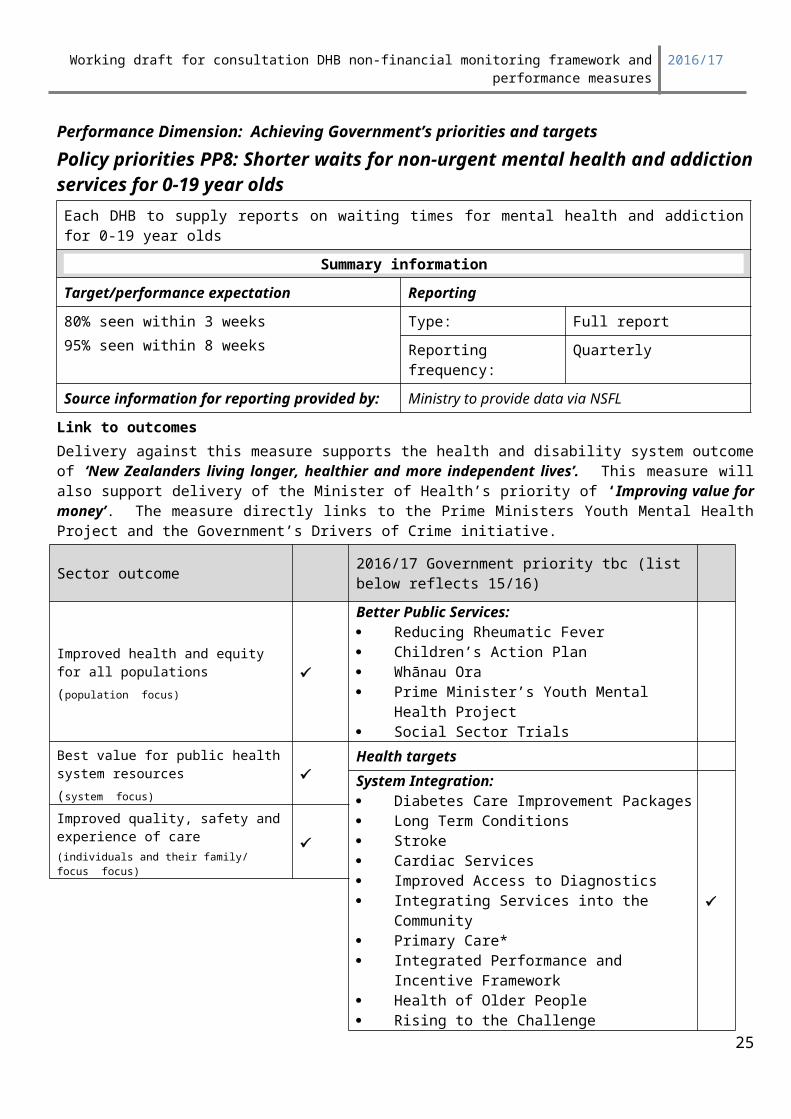
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP8: Shorter waits for non-urgent mental health and addiction services for 0-19 year oldsEach DHB to supply reports on waiting times for mental health and addiction for 0-19 year olds
Summary informationTarget/performance expectation Reporting80% seen within 3 weeks95% seen within 8 weeks
Type: Full report
Reporting frequency: Quarterly
Source information for reporting provided by: Ministry to provide data via NSFL
Link to outcomesDelivery against this measure supports the health and disability system outcome of ‘New Zealanders living longer, healthier and more independent lives’. This measure will also support delivery of the Minister of Health’s priority of ‘Improving value for money’. The measure directly links to the Prime Ministers Youth Mental Health Project and the Government’s Drivers of Crime initiative.
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
17
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Access and shorter waits are very important to patients regardless of the conditions. The waiting time concept is easily understood by the public. Earlier treatment in the progression of illness links to better outcomes as evidenced in international literature. Timeliness is also a key quality indicator in calls for improvement to the health care system. This indicator is consistent with and links to Rising to the Challenge: The Mental Health and Addiction Service Development Plan 2012-2017. This will improve provider performance in relation to the Welfare Working Group’s report and the need to address long term welfare dependency through better access to health services. A reducing waiting time indicator is also supported by the Ministry of Justice and Department of Corrections particularly in relation to access to AOD services. This target is a universal deficiency across the country and requires attention now that we can measure waiting times using PRIMHD data.
Actions and activities are that have a proven impact on this measure:Provider arm and NGO services may need to modify their triage processes to meet this target and possibly look to adopting a single point of entry process. For people who do not attend (DNA) scheduled appointments services generally have in place processes for declining the referral after 3 DNA’s. However, services could put in place processes, if they haven’t already, that improve the likelihood of a person attending their appointment e.g. reminder texts. DHB services will also need to ensure clients accepted into the service have a treatment plan that leads to appropriate timely discharge. Where there is long-term requirement for treatment and care the DHB will need to have in place Knowing the People Planning or something similar to ensure long term clients are in the best possible position to manage their illness and consequently lower demand on services.
Deliverables definitionsAll DHBs are expected to reach 80% of people referred for non-urgent mental health or addiction services are seen within three weeks and 95% of people are seen within 8 weeks this year.
DHBs will be required to meet this target within three years. DHBs will need to set and agree with the Ministry individualised targets (based on data provided by the Ministry).
The wait time will be counted from the time the referral is received for a person who has not been seen for at least a year (or not at all) to the time of the first face to face contact with a mental health or addiction professional. The wait time will also be calculated for provider arm services and AOD NGOs. Where there are two referrals open for the same client the earliest referral will be counted.The wait time will exclude the following:
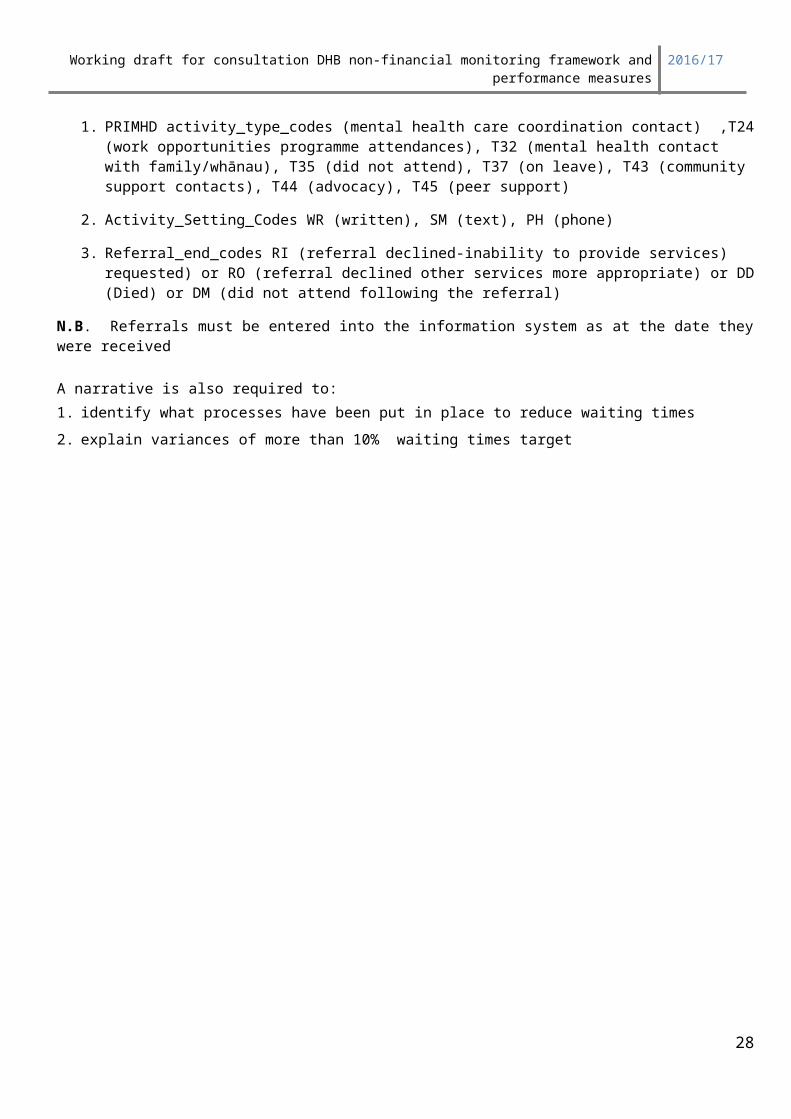
1. PRIMHD activity_type_codes (mental health care coordination contact) ,T24 (work opportunities programme attendances), T32 (mental health contact with family/whānau), T35 (did not attend), T37 (on leave), T43 (community support contacts), T44 (advocacy), T45 (peer support)
2. Activity_Setting_Codes WR (written), SM (text), PH (phone)
3. Referral_end_codes RI (referral declined-inability to provide services) requested) or RO (referral declined other services more appropriate) or DD (Died) or DM (did not attend following the referral)
N.B. Referrals must be entered into the information system as at the date they were received
A narrative is also required to:1. identify what processes have been put in place to reduce waiting times2. explain variances of more than 10% waiting times target
18
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
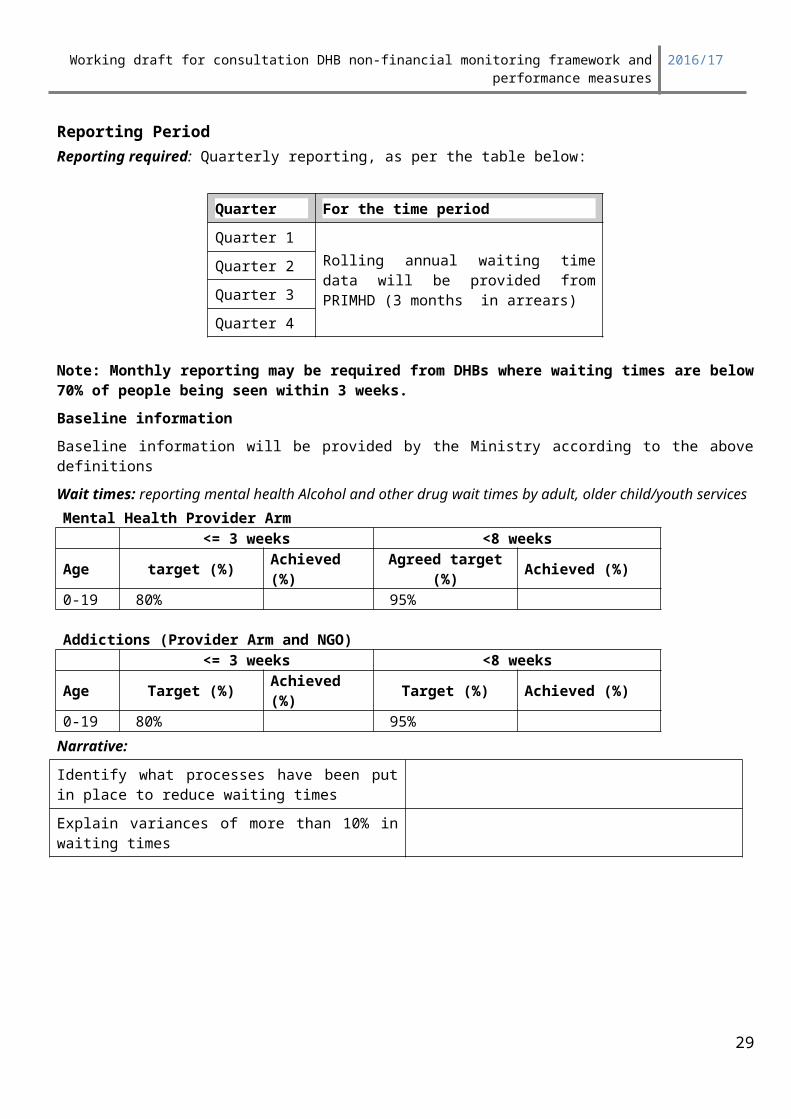
Reporting Period Reporting required: Quarterly reporting, as per the table below:
Quarter For the time periodQuarter 1
Rolling annual waiting time data will be provided from PRIMHD (3 months in arrears)
Quarter 2
Quarter 3
Quarter 4
Note: Monthly reporting may be required from DHBs where waiting times are below 70% of people being seen within 3 weeks.Baseline informationBaseline information will be provided by the Ministry according to the above definitions
Wait times: reporting mental health Alcohol and other drug wait times by adult, older child/youth servicesMental Health Provider Arm
<= 3 weeks <8 weeksAge target (%) Achieved (%) Agreed target (%) Achieved (%)0-19 80% 95%
Addictions (Provider Arm and NGO)<= 3 weeks <8 weeks
Age Target (%) Achieved (%) Target (%) Achieved (%)0-19 80% 95%
Narrative:Identify what processes have been put in place to reduce waiting times
Explain variances of more than 10% in waiting times
19
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP10: Oral Health- Mean DMFT score at Year 8
Summary informationTarget/performance expectation Reporting
Transitional measure not included in performance dashboard reports. It is unlikely that a standardised Electronic Oral Health Record system will be utilised by all DHBs and accessible nationally before 2017/18.
Type: Data and exception report
Reporting frequency: Annually
Source data/template for reporting provided by: Data to be supplied by DHBs, template is on NSFL
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities
20
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Living Within Our Means
Delivery of this measure most strongly supports the following sector outcomes and government priorities: By decreasing the severity of dental decay experienced by children in school Year 8 (12/13-year olds), the DHB will contribute to the outcome of protecting and promoting good health and independence through providing effective publicly funded child oral health programmes (health promotion, prevention and treatments) that reduce the prevalence of oral disease in children of primary school age.This measure also provides information that allows DHBs, and the Ministry, to evaluate how health promotion programmes, and services such as the DHB Community Oral Health Service (COHS) and other child oral health providers, are influencing the oral health status of children. The data breakdowns by ethnicity and fluoridation status enable DHBs to identify and target the populations in their district where children’s oral health status is poorest. It also provides DHBs with information to support the fluoridation of water supplies, which will be important when dealing with territorial local authorities.Through the intermediate outcome, the measure contributes to the high level outcome of New Zealanders living longer, healthier and more independent lives.
Actions and activities are that have a proven impact on this measure:The following actions and activities are examples of initiatives that have a proven impact on this measure: increased enrolment of pre-school children in publicly funded child oral health programmes enables early
engagement and provides opportunities for interventions aimed at prevention of oral disease and oral health promotion, and on an overall basis, reduces the prevalence of dental decay; and
the re-investment programme increases accessibility of regular care through “hub” and mobile clinics that will be open throughout the year and operate longer hours, and as well as increasing service productivity to increase service coverage for a greater number of children during the year.
ContextThis measure indicates the prevalence of oral disease and severity of dental decay experienced in children at the end of their primary schooling (Year 8, 12/13-year olds). This impact indicator measures the oral health status of New Zealand’s child population for demonstrating progress towards the population priority of “improving oral health” in the New Zealand Health Strategy.Publicly funded oral health services are available to children and adolescents from birth to 17 years of age (i.e. until the 18th birthday), through DHBs’ Community Oral Health Services (COHS), DHB-funded contracts with Maori oral health providers to provide child oral health services, and DHB-funded contracts with private dentists and Maori oral health providers to provide adolescent oral health services. In 2008, the Government embarked on a reinvestment programme in child and adolescent oral health services supported by the provision of additional capital and operating funding for renewed physical facilities, increased workforce, increased service coverage and increasing the preventive focus in the service delivery model. The reinvestment programme is expected to be fully implemented by DHBs by December 2015.After school Year 8, the majority of children transfer to publicly-funded oral health services provided for adolescents by private dentists contracted by DHBs, although some DHBs continue to provide some adolescent oral health services in their COHS and hospital dental departments. Improvements in this measure will show the impact made by the reinvestment programme on the effectiveness of publicly funded child oral health services and the COHS in particular. The World Oral Health Organisation (WHO) also regularly collates this measure for inclusion in its global oral health database for cross-country comparisons.
Deliverables definitionsNumerator: (Data source: DHB via COHS and other oral health providers)
21
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Upon the commencement of dental care, at the last dental examination before the child leaves the DHB’s Community Oral Health Service, the total number of:(i) permanent teeth of children in school Year 8 (12/13-year olds) that are –
Decayed (D), Missing (due to caries, M), and Filled (F); and
(ii) children who are caries-free (decay-free).
Denominator: (Data source: DHB via COHS and other oral health providers)The total number of children who have been examined in the Year 8 (12/13-year olds) group, in the year to which the reporting relates.
Other components of this indicator:1. The data reported in the Numerator and Denominator must also be broken down by:
(i) Ethnicity, using “prioritised ethnicity” approach1 into the following (in order of assignment): Māori; Pacific (only for the seven ‘official’ Pacific DHBs); and Other (includes Pacific children in the other DHBs that are not ‘official’ Pacific DHBs); and
(ii) water fluoridation status of the school area the child attends, defined as: fluoridated; and non-fluoridated.
2. The data for this indicator will be generated by DHBs. There is a number of technical interpretation issues associated with oral health, which are centred largely around variances in: processes for data collection amongst DHBs technologies for management of data amongst DHBs.
3. DHBs are encouraged to record data at the unit (individual child) level, using the National Health Index, but data are reported in an aggregated format and should be provided using the Ministry of Health Excel template, available on the quarterly reporting database or from the Ministry of Health’s oral health team.
4. DHBs are required to separately report the number of Decayed, Missing (due to caries), or Filled teeth (DMFT).
Reporting Period Reporting required: Annual, in the third quarter.
Quarter For the time periodQuarter 3 1 January 2016 – 31 December 2016
ExpectationsDHBs are expected to report complete, comprehensive and timely information. It is expected that all DHBs will meet the specific individually agreed targets, for this indicator, as agreed in their Annual Plans. Where the target has not been met, the DHB must provide commentary or a resolution plan that describes the DHB will do to address the performance failure.
1 It is acknowledged that use of the “prioritised ethnicity” approach is not consistent with New Zealand’s Statistical Standard for Ethnicity; but it is considered that this approach is acceptable given that: the historical use of this approach in the long-term data series since 1990 and the standard “total response” approach will not provide an accurate picture of the number of children examined by DHBs’
Community Oral Health Service and other contracted third party providers.22
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
DHBs are expected to set targets for this indicator for each of the two calendar years straddled by the fiscal year that the Annual Plan pertains to.
DHBs will retain the “year 2 targets” from the outgoing fiscal year’s Annual Plan as the “year 1 targets” for the incoming fiscal year’s Annual Plan.
Each DHB’s Annual Plans should focus on the activities that the DHB will put in place to achieve the “year 2 target” – this generally allows DHBs a six-month planning window followed by a 12-month implementation window for DHBs to achieve their “year 2 targets”.
The following achievement scale will be applied:
Rating: DefinitionOutstanding The DHB has met the targets agreed in the Annual Plan, and is more than 5%
over specified targets, and has also has also reached the same level of performance for the Other population group, and the Maori population group, and the Pacific population group (where applicable).
Achieved All targets agreed in the Annual Plan are met, within 95% - 105% of specified targetsanda resolution plan with appropriate actions is provided if the total population target is not met for the Māori population group, and the Pacific population group
Partially Achieved Some or all targets agreed in the Annual Plan are not met, but delivered results are same as, or better than, the results delivered in the prior yearand/orthe DHB has not met the target/performance expectation agreed in its Annual Plan, and a resolution plan with appropriate actions is provided, including actions to deliver improved performance for the Māori population group, and the Pacific population group
Not Achieved Some or all targets agreed in the Annual Plan are not met, and actual results are worse than the results delivered in the prior year
Reporting TemplateThe Ministry of Health Excel reporting template is also located on the nationwide service framework library web site: http://www.nsfl.health.govt.nz/.
23
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP11: Children caries-free at five years of age
Summary informationTarget/performance expectation Reporting
Transitional measure included until national data collection is established (not included in performance dashboard reports)
Type: Data and exception report
Reporting frequency: Annually
Source data/template for reporting provided by: Data to be supplied by DHBs, template is on NSFL
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
24
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Delivery of this measure most strongly supports the following sector outcomes and government priorities: Increasing the proportion of 5-year olds who have never experienced tooth decay will show that the DHB has made an impact on the outcome of protecting and promoting good health and independence through providing effective publicly-funded child oral health programmes (health promotion, prevention and treatments) that reduce the prevalence of oral disease in children of pre-school age.The measure also provides information that allows DHBs and the Ministry to evaluate how health promotion programmes, and services such as Well Child and the Community Oral Health Service (COHS), are influencing the oral health status of children. The data itemised by ethnicity and fluoridation status enable DHBs to identify and target the populations in their district where children’s oral health status is poorest. It also provides DHBs with information to support the fluoridation of water supplies, which will be important when dealing with territorial local authorities.Through the intermediate outcome, the measure contributes to the high level outcome of New Zealanders living longer, healthier and more independent lives.
Actions and activities are that have a proven impact on this measure:The following actions and activities are examples of initiatives that have a proven impact on this measure: increased enrolment of pre-school children in publicly funded child oral health programmes enables early
engagement and provides opportunities for interventions aimed at prevention of oral disease and oral health promotion, and on an overall basis, reduces the prevalence of dental decay; and
the re-investment programme increases accessibility of regular care through “hub” and mobile clinics that will be open throughout the year and operate longer hours, and as well as increasing service productivity to increase service coverage for a greater number of children during the year.
ContextThis measure indicates the prevalence of oral disease and experienced in children of pre-school age. This impact indicator measures the oral health of status of New Zealand’s child population for demonstrating progress towards the population priority of “improving oral health” in the New Zealand Health Strategy.Publicly funded oral health services are available to children and adolescents from birth to 17 years of age, through DHBs’ Community Oral Health Services (COHS), DHB-funded contracts with Maori oral health providers to provide child oral health services, and DHB-funded contracts with private dentists and Maori oral health providers to provide adolescent oral health services. In 2005, the Government embarked on a reinvestment programme in child and adolescent oral health services supported by the provision of additional capital and operating funding for renewed physical facilities, increased workforce, increased service coverage and increasing the preventive focus in the service delivery model. The reinvestment programme is expected to be fully implemented by DHBs around June 2014.Prior to the reinvestment programme, a majority of children enrol in COHS upon entry to primary school between ages 5 and 6. One of the areas of focus for the reinvestment programme is to increase the enrolment of pre-school children in COHS to enable early interventions to be delivered to pre-school children. Improvements in this measure will show the impact made by the reinvestment programme on the effectiveness of publicly-funded child oral health services. The World Oral Health Organisation (WHO) also regularly collates this measure for inclusion in its global oral health database for cross-country comparisons.
Deliverables definitionsNumerator: (Data source: DHB via COHS and other oral health providers)
25
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
At the first examination after the child has turned five years, but before their sixth birthday, the total number of children who are caries-free (decay-free); Denominator: (Data source: DHB via COHS and other oral health providers)The total number of children who have been examined in the 5-year old age group, in the year to which the reporting relates.
Other components of this indicator:1. The data reported in the Numerator and Denominator must also be broken down by:(i) Ethnicity, using “prioritised ethnicity” approach.(ii) 2 into the following (in order of assignment):
Māori; Pacific (only for the seven ‘official’ Pacific DHBs); and Other (includes Pacific children in the other DHBs that are not ‘official’ Pacific DHBs); and
(iii) water fluoridation status of the school area the child attends, defined as: fluoridated; and non-fluoridated.
2. The data for this indicator will be generated by DHBs. There is a number of technical interpretation issues associated with oral health, which are centred largely around variances in: processes for data collection amongst DHBs technologies for management of data amongst DHBs.
3. DHBs are encouraged to record data at the unit (individual child) level, using the National Health Index, but data are reported in an aggregated format and should be provided using the Ministry of Health Excel template, available on the quarterly reporting database or from the Ministry of Health’s oral health team.
4. DHBs are required to separately report the number of decayed, missing (due to caries), or filled teeth (dmft).
Reporting Period Reporting required: Annual, in the third quarter.
Quarter For the time periodQuarter 3 1 January 2016 – 31 December 2016
ExpectationsDHBs are expected to report complete, comprehensive and timely information. It is expected that all DHBs will meet the specific individually agreed targets, for this indicator, as agreed in their Annual Plans. Where the target has not been met, the DHB must provide commentary or a resolution plan that describes the DHB will do to address the performance failure. DHBs are expected to set targets for this indicator for each of the two calendar years straddled by the fiscal year that the Annual Plan pertains to.
DHBs will retain the “year 2 targets” from the outgoing fiscal year’s Annual Plan as the “year 1 targets” for the incoming fiscal year’s Annual Plan.2 It is acknowledged that use of the “prioritised ethnicity” approach is not consistent with New Zealand’s Statistical Standard for Ethnicity; but it is considered that this approach is acceptable given that: the historical use of this approach in the long-term data series since 1990 and the standard “total response” approach will not provide an accurate picture of the number of children examined by DHBs’
Community Oral Health Service and other contracted third party providers.26
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Each DHB’s Annual Plans should focus on the activities that the DHB will put in place to achieve the “year 2 target” – this generally allows DHBs a six-month planning window followed by a 12-month implementation window for DHBs to achieve their “year 2 targets”.
The following achievement scale will be applied:
Rating: DefinitionOutstanding The DHB has met the targets agreed in the Annual Plan, and are more than 5%
over specified targets, and has also has also reached the same level of performance for the Other population group, and the Maori population group, and the Pacific population group (where applicable).
Achieved All targets agreed in the Annual Plan are met, within 95% - 105% of specified targetsanda resolution plan with appropriate actions is provided if the total population target is not met for the Māori population group, and the Pacific population group
Partially Achieved Some or all targets agreed in the Annual Plan are not met, but delivered results are same as, or better than, the results delivered in the prior yearand/orthe DHB has not met the target/performance expectation agreed in its Annual Plan, and a resolution plan with appropriate actions is provided, including actions to deliver improved performance for the Māori population group, and the Pacific population group
Not Achieved Some or all expectations are not met, and actual results are worse than the results delivered in the prior year
Reporting TemplateThe Ministry of Health Excel reporting template is also located on the nationwide service framework library web site: http://www.nsfl.health.govt.nz/.
27
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP12: Utilisation of DHB-funded dental services by adolescents from School Year 9 up to and including age 17 years
Summary informationTarget/performance expectation Reporting
Transitional measure included until national data collection is established (not included in performance dashboard reports)
Type: Data and exception report
Reporting frequency: Annually
Source data/template for reporting provided by: Data to be supplied by DHBs, template is on NSFL
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
28
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Delivery of this measure most strongly supports the following sector outcomes and government priorities: Increasing the proportion of adolescents, in school Year 9 (13/14-year olds) up to and including 17 years of age, who have accessed DHB-funded oral health services will show that the DHB has made an impact on the outcome of protecting and promoting good health and independence by providing accessible and available publicly-funded adolescent oral health programmes. The programmes will help reduce the prevalence and severity of oral disease in adolescents.Through the intermediate outcome, the measure contributes to the high level outcome of New Zealanders living longer, healthier and more independent lives.
Actions and activities are that have a proven impact on this measure:The following actions and activities are examples of initiatives that have a proven impact on this measure: increasing the number of dentists contracted under the Combined Dental Agreement to provide DHB-
funded adolescent oral health services; more effective transfers of children at the end of school Year 8 by the DHB’s Community Oral Health
Service to dentists contracted under the Combined Dental Agreement to provide adolescent oral health services; and
increased promotion and follow-through of enrolments in DHB-funded adolescent oral health services.
ContextThis measure indicates the coverage of publicly funded adolescent oral health services. This output indicator provides a measure that can be used to demonstrate progress towards the population priority of “improving oral health” in the New Zealand Health Strategy.Publicly-funded oral health services are available to children and adolescents from birth to 17 years of age (i.e. until the 18th birthday), through DHBs’ Community Oral Health Services (COHS), DHB-funded contracts with Maori oral health providers to provide child oral health services, and DHB-funded contracts with private dentists and Maori oral health providers to provide adolescent oral health services. In 2005, the Government embarked on a reinvestment programme in child and adolescent oral health services supported by the provision of additional capital and operating funding for renewed physical facilities, increased workforce, increased service coverage and increasing the preventive focus in the service delivery model. The reinvestment programme is expected to be fully implemented by DHBs around June 2012.One of the areas of focus for the reinvestment programme is the reinvestment programme to increase the utilisation of publicly funded oral health services by adolescents. Improvements in this measure will show the impact made by the reinvestment programme on the service coverage of publicly funded adolescent oral health services.
Deliverables definitionsNumerator: (Data source: DHBs, via reporting from Sector Services and other DHB-contracted oral health providers.)In the year to which the reporting relates, the total number of adolescents accessing DHB-funded adolescent oral health services, defined as:(i) the unique count of adolescent patients’ completions and non-completions under the Combined
Dental Agreement; and(ii) the unique count of additional adolescent examinations with other DHB-funded dental services (e.g.
DHB Community Oral Health Services, Māori Oral Health providers and other contracted oral health providers).
29
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
To reduce duplication of effort, at the end of each quarter in the year to which the reporting relates, the Ministry will organise a data extract from Sector Services for all DHBs for claims made by dentists contracted under the Combined Dental Agreement, and provide this data for DHBs’ use in determining part (i) of the Numerator.
Denominator: (Data source: Estimates of DHB population by age, sourced from NZ Census and Statistics New Zealand’s population projections between Census)DHBs do not need to report a denominator. The Ministry will source denominator data, and advise denominator prior to DHBs’ targets being set.The denominator will be calculated as follows:
Half of the cohort aged 13 years All of the cohorts aged 14 – 17 years inclusive.
Other components of this indicator:1. The data reported in the Numerator and Denominator must also be broken down by:(i) Ethnicity, using “prioritised ethnicity” approach3 into the following (in order of assignment):
Māori; Pacific (only for the seven ‘official’ Pacific DHBs); and Other (includes Pacific adolescents in the other DHBs that are not ‘official’ Pacific DHBs); and
The Ministry acknowledges that availability of ethnicity in the Numerator is subject to ethnicity data being available from the source systems concerned.
2. Part of the data for this indicator will be provided by the Ministry (CDA data from the Proclaim payments system) and the balance will be generated by DHBs (non-CDA data on adolescents utilising COHS services and DHB-contracted dental services not paid through Proclaim). There is a number of technical interpretation issues associated with oral health, which are centred largely around variances in: processes for data collection amongst DHBs technologies for management of data amongst DHBs.
3. DHBs are encouraged to record data at the unit (individual child) level, using the National Health Index, but data are reported in an aggregated format and should be provided using the Ministry of Health Excel template, available on the quarterly reporting database or from the Ministry of Health’s oral health team.
Reporting Period Reporting required: Annual, in the fourth quarter.
Quarter For the time periodQuarter 4 1 January 2016 – 31 December 2016
ExpectationsDHBs are expected to report complete, comprehensive and timely information. It is expected that all DHBs will meet the specific individually agreed targets, for this indicator, as agreed in their Annual Plans. Where the target has not been met, the DHB must provide commentary or a resolution plan that describes the DHB will do to address the performance failure. DHBs are expected to set targets for this indicator for each of the two calendar years straddled by the fiscal year that the Annual Plan pertains.
3
30
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
DHBs will retain the “year 2 targets” from the outgoing fiscal year’s Annual Plan as the “year 1 targets” for the incoming fiscal year’s Annual Plan. Each DHB’s Annual Plans should focus on the activities that the DHB will put in place to achieve the “year 2 target” – this generally allows DHBs a six-month planning window followed by a 12-month implementation window for DHBs to achieve their “year 2 targets”.
On a quarterly basis, DHBs are expected to monitor their progress towards achieving the agreed targets in their Annual Plans, and put in place appropriate measures to ensure targets are achieved by the end of the year to which the reporting relates.The following achievement scale will be applied:
Rating: DefinitionOutstanding The DHB has met the targets agreed in the Annual Plan, and are more than
5% over specified targets, and has also has also reached the same level of performance for the Other population group, and the Maori population group, and the Pacific population group (where applicable).
Achieved All targets agreed in the Annual Plan are met, within 95% - 105% of specified targetsanda resolution plan with appropriate actions is provided if the total population target is not met for the Māori population group, and the Pacific population group
Partially Achieved Some or all targets agreed in the Annual Plan are not met, but delivered results are same as, or better than, the results delivered in the prior yearand/orthe DHB has not met the target/performance expectation agreed in its Annual Plan, and a resolution plan with appropriate actions is provided, including actions to deliver improved performance for the Māori population group, and the Pacific population group
Not Achieved Some or all expectations are not met, and actual results are worse than the results delivered in the prior year
Reporting Template
The Ministry of Health Excel reporting template is located on the nationwide service framework library web site NSFL homepage: http://www.nsfl.health.govt.nz/.
31

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP13: Improving the number of children enrolled in DHB funded dental services
Summary informationTarget/performance expectation Reporting
Agreed in Annual Plan Type: Data and exception report
Reporting frequency: Annually
Source data/template for reporting provided by: Data to be supplied by DHBs, template is on NSFL
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
32
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Delivery of this measure most strongly supports the following sector outcomes and government priorities: By increasing the number of pre-school children less than five years of age (0 – 4 year olds, inclusive), who have enrolled for DHB-funded oral health services and reducing the number who are overdue for their scheduled examination, the DHB will show that it has made an impact on the outcome of protecting and promoting good health and independence. The measures indicates the accessibility and availability of publicly-funded oral health programmes, which will in turn reduce the prevalence and severity of early childhood caries, and improve oral health of primary school children.The measures provide information that allows DHBs and the Ministry to evaluate how health promotion programmes, and services such as Well Child and the Community Oral Health Service (COHS), are influencing the oral health status of children and whether oral health service programmes are delivering timely oral health services to children. Through the intermediate outcome, the measure contributes to the high level outcome of New Zealanders living longer, healthier and more independent lives.
Actions and activities are that have a proven impact on this measure:The following actions and activities are examples of initiatives that have a proven impact on this measure: increased enrolment of pre-school children in publicly funded child oral health programmes enables early
engagement and provides opportunities for interventions aimed at prevention of oral disease and oral health promotion, and on an overall basis, reduces the prevalence of dental decay; and
the re-investment programme increases accessibility of regular care through “hub” and mobile clinics that will be open throughout the year and operate longer hours, and as well as increasing service productivity to increase service coverage for a greater number of children during the year.
ContextThis indicates the coverage and timeliness of publicly funded child oral health services delivered by DHBs’ Community Oral Health Services (COHS). The output indicators in this measure can be used to demonstrate progress towards the population priority of “improving oral health” in the New Zealand Health Strategy.Publicly funded oral health services are available to children and adolescents from birth to 17 years of age, through DHBs’ Community Oral Health Services (COHS), DHB-funded contracts with Maori oral health providers to provide child oral health services, and DHB-funded contracts with private dentists and Maori oral health providers to provide adolescent oral health services. In 2005, the Government embarked on a reinvestment programme in child and adolescent oral health services supported by the provision of additional capital and operating funding for renewed physical facilities, increased workforce, increased service coverage and increasing the preventive focus in the service delivery model. The reinvestment programme is expected to be fully implemented by DHBs around June 2014.One of the areas of focus for the reinvestment programme is to increase service coverage and workforce productivity to deliver more and better quality care through DHBs’ COHS. Improvements in these measures show the impact made by the programme on the coverage and timeliness of publicly-funded child oral health services. Ethnicity data in these measures also enable DHBs to identify and target the populations in their district where children’s oral health status is poorest.
Deliverables definitionsMeasure 1: Number of Pre-School Children Enrolled in DHB-funded Oral Health ServicesNumerator: (Data source: DHBs, via their Community Oral Health Services and other oral health providers.)
33
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
In the year to which the reporting relates, the total number of children under five years of age, i.e. aged 0 to 4 years of age inclusive, who are enrolled with DHB-funded oral health services (DHB’s Community Oral Health Service and other DHB-contracted oral health providers such as Māori oral health providers).
Denominator: (Data source: NZ Census sourced estimates of DHB population by age)DHBs do not need to report a denominator. The Ministry will source denominator data, and advise denominator prior to DHBs’ targets being set.In the year to which the reporting relates, the total number of children under five years of age, i.e. ages 0 to 4.
Other components of this measure:1. The data reported in the Numerator and Denominator must also be broken down by:(i) Ethnicity, using “prioritised ethnicity” approach4 into the following (in order of assignment):
Māori; Pacific (only for the seven ‘official’ Pacific DHBs); and Other (includes Pacific children in the other DHBs that are not ‘official’ Pacific DHBs); and
1. The data for this indicator will be generated by DHBs. There is a number of technical interpretation issues associated with oral health. This centres largely around variances in: processes for data collection amongst DHBs technologies for management of data amongst DHBs.
2. DHBs are encouraged to record data at the unit (individual child) level, using the National Health Index, but data are reported in an aggregated format and should be provided using the Ministry of Health Excel template, available on the quarterly reporting database or from the oral health team.
Measure 2: Number of Enrolled Pre-School and Primary School Children Overdue for their Scheduled ExaminationsNumerator: (Data source: DHBs, via their Community Oral Health Services and other oral health providers.)In the year to which the reporting relates:(i) the total number of pre-school children and primary school children in total and for each school
decile who have not been examined according to their planned recall period in DHB-funded dental services (DHB’s Community Oral Health Service and other DHB-contracted oral health providers such as Māori oral health providers); and
(ii) the greatest length of time children has been waiting for their scheduled examination, and the number of children that have been waiting for that period.
Denominator: (Data source: DHBs, via their Community Oral Health Services and other oral health providers.)In the year to which the reporting relates, the total number of children enrolled in DHB-funded dental services (DHB’s Community Oral Health Service and other DHB-contracted oral health providers such as Māori oral health providers), showing separately the number of – pre-school children, and
4 It is acknowledged that use of the “prioritised ethnicity” approach is not consistent with New Zealand’s Statistical Standard for Ethnicity; but it is considered that this approach is acceptable given that: the historical use of this approach in the long-term data series since 1990 and the standard “total response” approach will not provide an accurate picture of the number of children examined by DHBs’
Community Oral Health Service and other contracted third party providers.34

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
primary school children.
Data Definitions
a. Pre-school and primary school children are the children from age 0 (less than 1 year old) to the end of school Year 8 inclusive.
Other components of this measure:1. The data reported in the Numerator and Denominator must also be broken down by:(i) Ethnicity, using “prioritised ethnicity” approach5 into the following (in order of assignment):
Maori; Pacific (only for the seven ‘official’ Pacific DHBs); and Other (includes Pacific children in the other DHBs that are not ‘official’ Pacific DHBs); and
The Ministry acknowledges that availability of ethnicity in the Numerator is subject to ethnicity data being available from the source systems concerned.
2. The data for this indicator will be generated by DHBs. There is a number of technical interpretation issues associated with oral health. This centres largely around variances in: processes for data collection amongst DHBs technologies for management of data amongst DHBs.
3. DHBs are encouraged to record data at the unit (individual child) level, using the National Health Index, but data are reported in an aggregated format and should be provided using the Ministry of Health Excel template, available on the quarterly reporting database or from the oral health team.
Reporting Period Reporting required: Annual, in the third quarter.
Quarter For the time periodQuarter 3 1 January 2016 – 31 December 2016
ExpectationsDHBs are expected to report complete, comprehensive and timely information. It is expected that all DHBs will Annual Plans. It is expected that DHBs will meet the specific individually agreed targets s in their Annual Plans. Where the target has not been met, the DHB must provide commentary or a resolution plan that describes the DHB will do to address the performance failure.
DHBs are expected to set targets for this indicator for each of the two calendar years straddled by the fiscal year that the Annual Plan pertains to.
DHBs will retain the “year 2 targets” from the outgoing fiscal year’s Annual Plan as the “year 1 targets” for the incoming fiscal year’s Annual Plan.
5 It is acknowledged that use of the “prioritised ethnicity” approach is not consistent with New Zealand’s Statistical Standard for Ethnicity; but it is considered that this approach is acceptable given that: the historical use of this approach in the long-term data series since 1990 and the standard “total response” approach will not provide an accurate picture of the number of children examined by DHBs’
Community Oral Health Service and other contracted third party providers.35
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Each DHB’s Annual Plans should focus on the activities that the DHB will put in place to achieve the “year 2 target” – this generally allows DHBs a six-month planning window followed by a 12-month implementation window for DHBs to achieve their “year 2 targets”.
. The following achievement scale will be applied:
Rating: DefinitionOutstanding The DHB has met the targets agreed in the Annual Plan, and are more than
5% over specified targets, and has also has also reached the same level of performance for the Other population group, and the Maori population group, and the Pacific population group (where applicable).
Achieved All targets agreed in the Annual Plan are met, within 95% - 105% of specified targetsanda resolution plan with appropriate actions is provided if the total population target is not met for the Māori population group, and the Pacific population group
Partially Achieved Some or all targets agreed in the Annual Plan are not met, but delivered results are same as, or better than, the results delivered in the prior yearand/orthe DHB has not met the target/performance expectation agreed in its Annual Plan, and a resolution plan with appropriate actions is provided, including actions to deliver improved performance for the Māori population group, and the Pacific population group
Not Achieved Some or all expectations are not met, and actual results are worse than the results delivered in the prior year
Reporting TemplateThe Ministry of Health Excel reporting template is located on the nationwide service framework library web site: http://www.nsfl.health.govt.nz/.
36
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP20: Improved management for long term conditions (CVD, Diabetes, and Stroke)
Summary information
Target/performance expectation:Performance agreed in annual plan
Reporting
Type: Exception reporting
Reporting frequency: Quarterly
Source data/template for reporting provided by: : A reporting template will be provided on NSFL
Linkages: This performance measure is also included in the Maori health plan yes (ACS and CVD)
Linkages: This performance measure is also included in the Integrated performance and incentive framework
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes services Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality
37
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Actions to Support Delivery of Regional Priorities Living Within Our Means
Long Term Conditions (to be updated)Long-term conditions comprise the major health burden for New Zealand now and into the foreseeable future. This group of conditions is the leading cause of morbidity in New Zealand, and disproportionately affects Maori and Pacific peoples. As the population ages and lifestyles change these conditions are likely to increase significantly. Cardiovascular disease, including heart attacks and strokes, are substantially preventable with lifestyle advice and treatment for those at moderate or higher risk. Diabetes is also important as a major and increasing cause of disability and premature death and is a good indicator of the responsiveness of a health service to the people in most need.
Deliverables definitionsThe deliverables will be formally defined in the planning package, including mechanisms for data collection and delivery expectations. Each DHB must provide narrative comment for the indicator on progress on the activities being taken to improve performance, as outlined in their Annual Plan. The narrative is to include specific activities undertaken for Maori and Pacific and where relevant, people from the Indian subcontinent6.
There are five Focus Areas within this policy priority.
FA1 Long Term Conditions, FA2 Diabetes services, FA3 Cardiovascular health, FA4 Acute heart services, FA5 Stroke services.
Focus Area 1 Long Term Conditions
Expectation New Zealanders with Long-term Conditions (LTCs) live longer, healthier and more independent lives, with the assistance of an integrated health system.
Deliverables: Narrative quarterly report on: DHB progress towards meeting its deliverables for Long Term Conditions identified in the
2016/17 annual plans by June 2017, including success stories.Where deliverables are not on track the report must include mitigation strategies and new timeframes for delivery.
Commentary to be provided:
Specific Quarterly Reporting:Quarters 1 and 3: Teleconference-based reporting on progress to date on deliverables for Long Term
Conditions identified in the 2016/17 annual plans. The Minutes from the teleconferences will be taken by the DHBs and provided to support any additional reporting arising from the teleconferences.
Quarters 2 and 4: DHBs to provide a narrative report on progress to date on deliverables for Long Term
Conditions identified in the 2016/17 annual plans, including success stories. The report will include commentary on the Ambulatory Sensitive Hospital admissions (ASH)
rates for Long Term Conditions.Definitions: Actions to support long term conditions include:
Prevention through clearly outlined networks between general practice and community organisations to maximise physical activity, nutrition, quit smoking and reduction in alcohol use.
Identification of populations at risk using risk stratification to inform systematic categorisation of people at risk in order to provide appropriate management. As well, showing evidence of proactive recall and management of at risk populations
Management of people with long term conditions through: development and/or implementation of new models of care to support people with LTCs; provision of multi-disciplinary teams including allied health and kaiawhina supporting service delivery in primary care; primary care access to specialist support where appropriate and provision of
6 The requirement to report about Pacific people applies only to those DHBs with high Pacific populations. These DHBs are: Counties Manukau, Auckland, Waitemata, Waikato, Capital & Coast, Hutt Valley and Canterbury.
38
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
self-management support and education for people with Long Term Conditions. Support regular primary care multidisciplinary teams to undertake collaborative practice review of the 1% of people with a high level of complex problems.
Enablers demonstrating clinical governance for Long Term Conditions services and IT systems to support risk stratification, case management, shared care and or clinical information sharing (focus on collaboration enablers). As well, Show evidence of staff training and education around goal setting, motivational interviewing and shared decision-making concepts and include ongoing workforce development in primary care, and clinical governance with a named clinical lead. IT capability is to be maintained and improved including provision of audit tools and/or a dashboard reporting system.
Linkages with PP22 Delivery of actions to improve system integration, and SI01 Ambulatory sensitive (avoidable) hospital admissions.
Focus Area 2 Diabetes services – DAR indicator to be confirmed (3 or 6 monthly reporting?)
Expectation People living with diabetes are regarded as leading partners in their own care within systems that ensure they can manage their own condition effectively with appropriate support.Improve or, where high, maintain the proportion of patients with good or acceptable glycaemic control. The expectation in 2016/17 is to begin to implement actions in the Diabetes plan “Living Well with Diabetes”.
Commentary to be provided
Quarterly reporting is required on the implementation of actions in the Diabetes plan “Living Well with Diabetes”, and reporting on the HbA1c indicator and Diabetes Annual Reviews.Quarters 1 and 3: Teleconference-based reporting on progress to date on deliverables for Diabetes identified
in the 2016/17 annual plans. The Minutes from the teleconferences will be taken by the DHBs and provided to support any additional reporting arising from the teleconferences.
Quarters 2 and 4: DHBs to provide a narrative report on progress to date on deliverables for Diabetes
identified in the 2016/17 annual plans, including success stories. The report will include data and commentary on the proportion of people with diabetes
above 64mmol/mol, and number of diabetes annual reviews. It will also include an update on progress towards reporting HbA1c above 80 and 100mmol/mol. Numbers of diabetes annual reviews are also to be reported.
Deliverables: HbA1c and DARs
Numerator – Count of enrolled people aged 15-74 in the PHO with diabetes and the most recent HbA1c during the past 12 months of equal to or less than 64 mmol/mol)Denominator - Count of enrolled people in the PHO aged 15-74 with diabetes on the Ministry of Health Virtual Diabetes Register (VDR 2014).
Numerator - Number of Diabetes Annual Reviews undertaken in the quarterDenominator - Count of enrolled people in the PHO aged 15-74 with diabetes on the Ministry of Health Virtual Diabetes Register (VDR 2014).
Data source: MOH will supply VDR, and DHBs/PHOs to provide numerator.Note: Patients coded with diabetes in the General Practice registers can be used instead of VDR once comparisons between the two have been complete, and accuracy of GP registers can be demonstrated.
Additional Commentary
Actions to support delivery of Diabetes services and the Diabetes plan “Living Well with Diabetes” include: Prevention and early intervention, including mental health needs, to reduce the personal and
social burden of disease Reducing disparities in health outcomes between different ethnic, socioeconomic and
geographical groups Providing people centred services including for gamily and whanau when appropriate Being sustainable in the long term with consistent services across the country Achieving effective self-management including responding to people’s demand for
technology-enabled tools Information on evidence and test and evaluation promising interventions to improve our
39
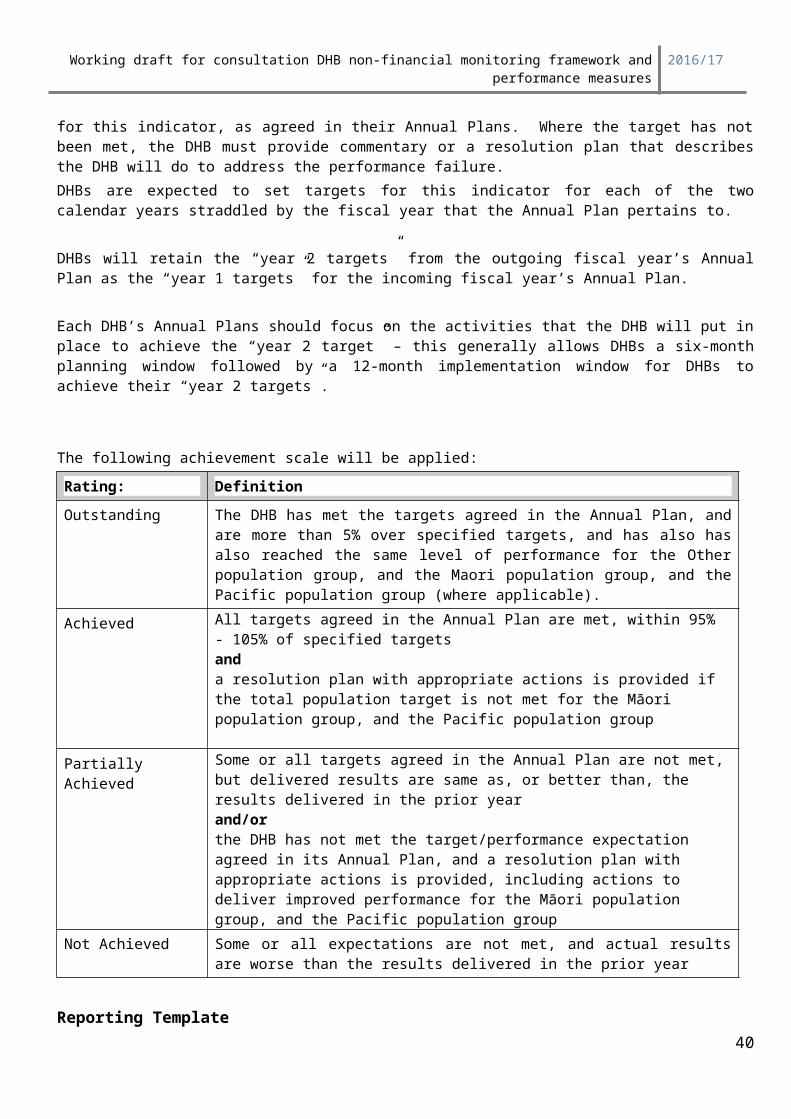
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
knowledge of what works for New Zealanders.
Focus Area 3 Cardiovascular (CVD) health
Expectation The following actions and activities are examples of initiatives that have a proven impact on this measure. Strong collaboration and co-ordination between primary and secondary care Working with primary care to ensure that they have access to good data and can identify
patients who need to be recalled for an appointment or need additional support to manage their health.
Community driven outreach programmes (including for example free CVD risk assessments offered at community events and workplaces, and promotion /education by people the target community identifies with, Nurse-led support of self-management and removal of identified barriers such as cost and time limited consultations.)
Use of Budget 2013 funding to support primary care to deliver services that achieves good heart health
Quality improvement plans in place for managing people at risk. Shared management decisions based on discussions between clinicians and
people at high risk of CVD which account for the benefits of appropriate lifestyle change (principally diet, exercise and smoking), diabetes care and medication therapy.
Commentary to be provided
Specific Quarterly Reporting:Quarters 1 and 3: Teleconference-based reporting on progress to date on deliverables for CVD identified in the
2016/17 annual plans. The Minutes from the teleconferences will be taken by the DHBs and provided to support any additional reporting arising from the teleconferences.
Quarters 2 and 4: DHBs to provide a narrative report on progress to date on deliverables for CVD identified in
the 2016/17 annual plans, including success stories.
Deliverables 90 percent of the eligible population will have had their cardiovascular risk assessed in the last five years.
Numerator: (Data source: IPIF Programme)Count of enrolled people in the PHO within the eligible population who have had a CVD risk recorded within the last five years
Denominator: (Data source: PHO enrolment register)Count of enrolled people in the PHO who are eligible for a CVD risk assessment.The population eligible for CVDRA is as follows: Males of Maori, Pacific, or Indian sub-continent* ethnicity aged 35-74 years at the end of the
reporting period and enrolled with PHO Females of Maori, Pacific, or Indian sub-continent* ethnicity aged 45-74 years at the end of
the reporting period and enrolled with PHO Males of any other ethnicity aged 45-74 years at the end of the reporting period and
enrolled with PHO Females of any other ethnicity aged 55-74 years at the end of the reporting period and
enrolled with PHO
Data source: CVD data provided by the Ministry from the IPIF ProgrammeAdditional Commentary
Each DHB must provide narrative comment for the indicator on the activities being taken to improve performance and achieve the measure agreed through their Annual Plan including the proportion by ethnicity that have high risk (score CVDRA over 20%).
Quarterly report to include progress of actions to improve management of the people that have high risk (by ethnicity) (score CVDRA over 20%).
40

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
The narrative is to include specific activities undertaken for Maori and Pacific7 populations. (The requirement to report about Pacific people applies only to those DHBs with high Pacific populations. These DHBs are: Counties Manukau, Auckland, Waitemata, Waikato, Capital & Coast, Hutt Valley and Canterbury)
*the Indian sub-continent for this report is defined by the person enrolled with the PHO self-identifying as “Indian” ethnicity.
Reporting Period for FA1, FA2 and FA3All deliverables within the measure are to be provided as follows:
Quarter For the time period Indicator to report on1 1 July – 30
SeptemberTeleconference to discuss delivery of services for Long Term Conditions, CVD and Diabetes.
2 1 October – 31 December
Long Term Conditions, CVD and Diabetes. narrative reports and data where required
3 1 January – 31 March
Teleconference to discuss delivery of services for Long Term Conditions, CVD and Diabetes.
4 1 April – 30 June Long Term Conditions, CVD and Diabetes. narrative reports and data where required
Focus Area 4 Acute heart service
Expectation To provide a nationally consistent reporting framework, all regions are required to report measures of Acute Coronary Syndrome (ACS) risk stratification and time to appropriate intervention using ANZACS-QI.
Deliverable: 70 percent of high-risk patients will receive an angiogram within 3 days of admission. (‘Day of Admission’ being ‘Day 0’) by ethnicity
Over 95 percent of patients presenting with ACS who undergo coronary angiography have completion of ANZACS QI ACS and Cath/PCI registry data collection within 30 days
Over 95 percent of patients undergoing cardiac surgery at the five regional cardiac surgery centres will have completion of Cardiac Surgery registry data collection with 30 days of discharge.
Data source: Data provided from ANZACS-QIAdditional Commentary to be provided:
Specific Quarterly Reporting:Quarters 1 and 3: Regional teleconference-based reporting on progress to date on deliverables for ACS
identified in annual plans and actions and progress in quality improvement initiatives to support the improvement of ACS indicators as reported in ANZACS-QI
The minutes from the teleconferences will be recorded and uploaded as the quarterly report.Quarters 2 and 4:DHBs to complete the template provided by the Ministry on progress to date on deliverables for ACS identified in the annual plans, including success stories.
Definitions: A high-risk patient can be defined by the DHBs.
Focus Area 5 Stroke Services
Expectation: All DHBs will provide an organised acute stroke service for their population as recommended in the NZ Clinical Guidelines for Stroke Management.
7 The requirement to report about Pacific people applies only to those DHBs with high Pacific populations. These DHBs are: Counties Manukau, Auckland, Waitemata, Waikato, Capital & Coast, Hutt Valley and Canterbury.
41
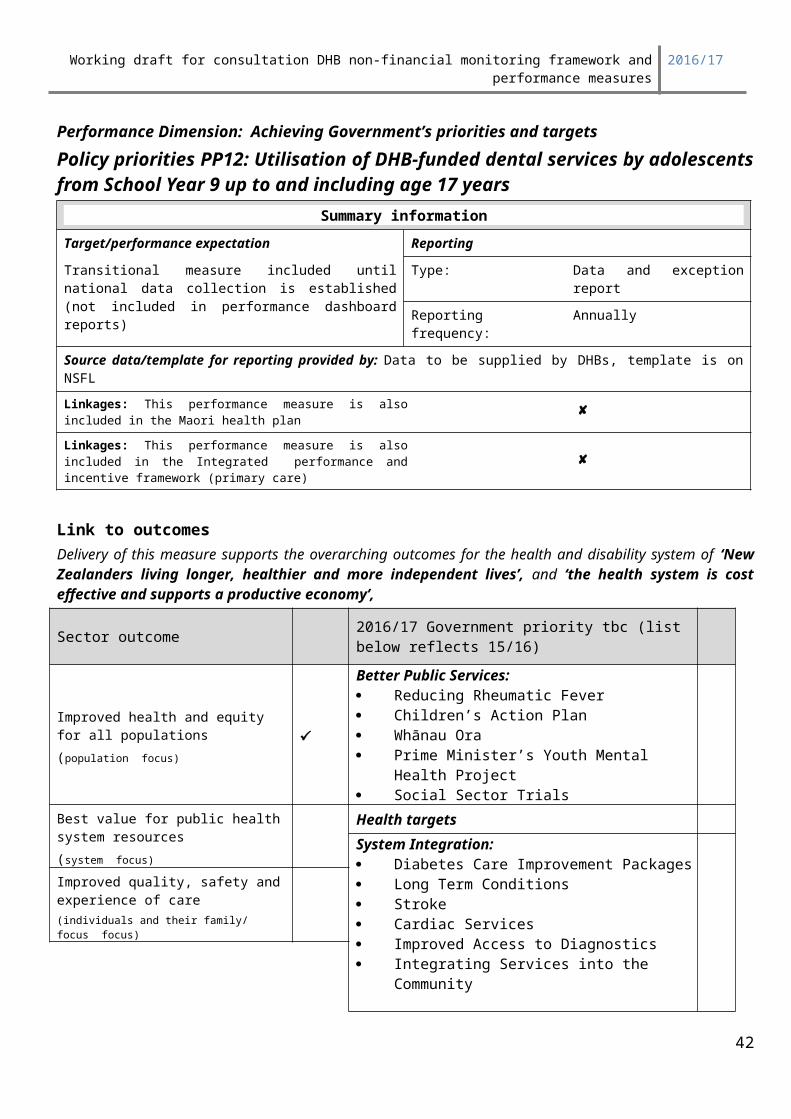
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Deliverable: 6 percent or more of potentially eligible stroke patients thrombolysed 24/7 80 percent of stroke patients admitted to a stroke unit or organised stroke service with
demonstrated stroke pathway 80 percent of patients admitted with acute stroke who are transferred to inpatient
rehabilitation services are transferred within 7 days of acute admission (also report % of acute stroke patients transferred to inpatient rehab)NB: when reporting against above indicators include numerators and denominators in brackets after percent
Data source : DHBs to provideAdditional Commentary to be provided:
Specific Quarterly Reporting:Quarters 1 and 3: Regional teleconference-based reporting on progress to date on deliverables for stroke
identified in the 2015/16 annual plans The minutes from the teleconferences will be recorded and uploaded as the quarterly report.Quarters 2 and 4: DHBs to complete the template provided by the Ministry on progress to date on deliverables
for stroke identified in the 2015/16 annual plans, including success stories.
Definitions: A potentially eligible stroke patient is one who has an ischaemic or undetermined stroke. Other strokes, such as Intracerebral hemorrhage (ICH), transient ischemic attack (TIA), or mimics are excluded.
An acute stroke patient is admitted to hospital with a primary discharge diagnosis of ischaemic, haemorrhagic, or undetermined stroke. TIA patients, stroke mimics, and patients discharged from emergency department without being recorded as a hospital admission are excluded. Care should be taken that patients transferred during their admission are only counted once even if managed at two separate institutions.
ICD10 codes included: I61 Intracerebral Haemorrhage with subcodes for site inclusive, I63 Cerebral Infarction with subcodes 163.0-163.9 inclusive, I64 Stroke, not specified as haemorrhage or infarction)
A stroke unit is defined as a discrete ward, or beds within a ward, with a dedicated specialised multi-disciplinary team (MDT) and could include acute stroke units that discharge patients to a rehabilitation service, or an integrated acute and rehabilitation unit (New Zealand National Acute Stroke Services Audit 2009).
Organised Acute Stroke Services are provided by a coordinated specialised interdisciplinary team (IDT) and consist of early and ongoing comprehensive assessments and treatment which is guided by best practice. This is reflected in the use of stroke specific protocols. The IDT meets regularly to discuss, formulate and implement patient management and optimise rehabilitation and patient function. Ideally care is provided in a geographically discrete unit, but depending on DHB size this may not always be feasible.
Minimum specific organised acute stroke service specifications:
Services provided: Stroke Thrombolysis Rapid TIA Access Acute Stroke Care Early Stroke Rehabilitation
Members of an acute stroke team:Designated to stroke (not necessarily designated to stroke exclusively): A stroke physician* A stroke nurse* Physiotherapist Occupational Therapist
42
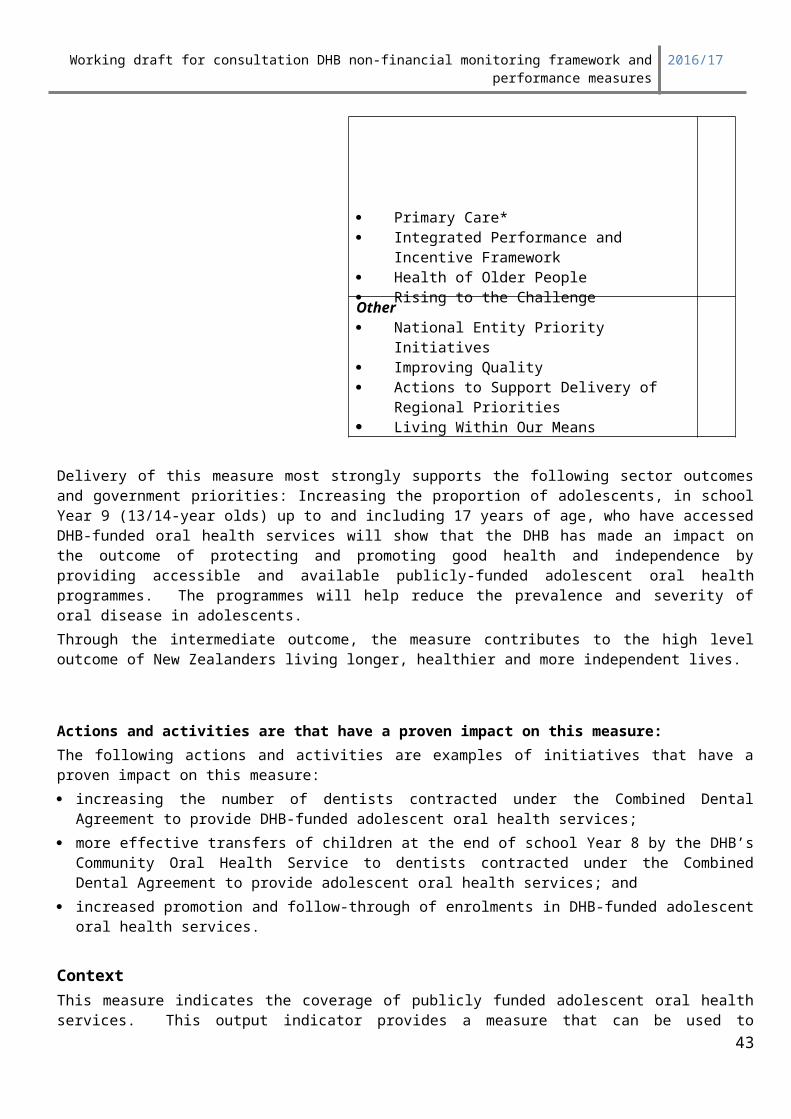
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Speech and Language Therapist Social workerClinicians that add significant value to stroke care, but are not mandatory designated members of the acute stroke team: Dietician Clinical Psychologist Pharmacist
* Each centre should have a designated lead stroke physician and lead stroke nurse. However, for daily clinical activities several clinicians can share patient responsibilities on a rotating basis.
Education: Baseline qualifications yet to be defined. Ongoing education should include a minimum of 8 hours of annual formal stroke education
for each designated acute stroke team member Provision of education to other staff working with stroke
Meetings/collaboration: Minimum IDT meeting once a week to discuss ongoing management, goal setting, and
discharge planningOffering key components of stroke management utilising protocols with specified time frames: Thrombolysis, TIA, stroke care guidelines (medical, nursing, dysphagia, early mobilisation,
functional assessments, education of patients and family)
Links to EMS, ED, radiology, neurosurgery, vascular surgery, rehabilitation
Quality Assurance and audit If providing stroke thrombolysis maintenance of a thrombolysis registry is mandatory.
Additional stroke registry data is desirable although regular stroke relevant audits are an acceptable alternative. All serious adverse events should be fully investigated and discussed as a team.
Research/Advocacy There should be some evidence that the service engages in stroke audits or clinical stroke
research and patient advocacy relating to stroke.
Geographical areaHospitals designated as providing an ‘Organised Acute Stroke Service’ should have a designated geographical area with stroke patients spending the majority of their acute hospital stay in this ‘unit.’ Ideally beds are dedicated to stroke patients, but this is not mandatory. In small hospitals where a dedicated ‘unit’ may not be feasible due to low patient volumes patients may be admitted to a single general medical ward if all other components of an organised stroke service are provided. Alternatively, if organised acute stroke services are not available patients should be transferred to a larger centre using a defined pathway. Formalised remote support from a larger service may in some instances be a further option.
Staffing LevelsExact FTE allocation for interdisciplinary stroke team member staffing levels has not been firmly established at this point in time. However, as a general guide staffing levels should be sufficient to enable care of patients in accordance with NZ Stroke Guidelines. All designated members of the stroke team should have some dedicated time (part – or fulltime depending on patient volumes) specifically allocated to stroke care and maintenance of stroke care competencies.
Stroke Rehabilitation beyond the acute phase Rehabilitation service requirements for sub-acute inpatient and community rehabilitation
beyond the acute phase remain to be defined.These service specifications are undergoing regular review and will be amended as additional relevant information becomes available.
43
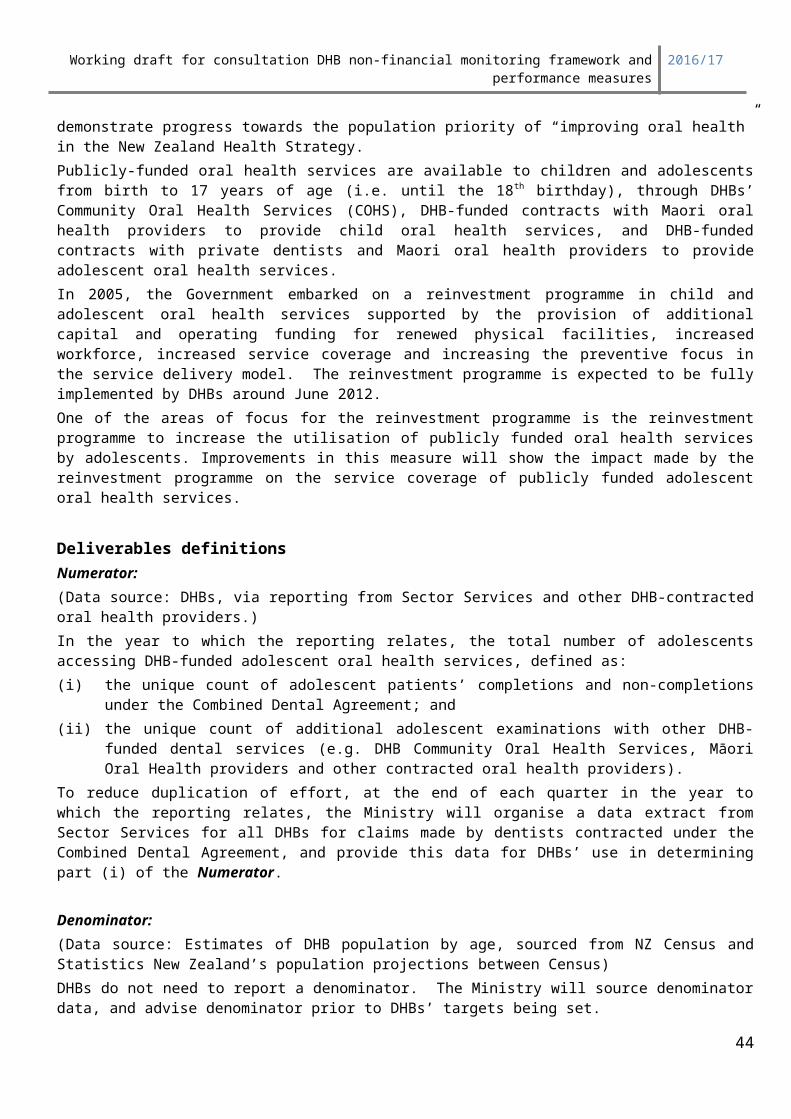
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Reporting Period for FA4 and FA5 All deliverables within the measure are to be provided as follows:
Quarter For the time period
Indicator to report on
1 1 July – 30 September
Regional teleconference to discuss ACS, including discussion on ACS indicatorsRegional teleconference to discuss Stroke, including discussion on stroke indicators
2 1 October – 31 December
DHBs to complete template provided by the Ministry on progress to date on deliverables for ACS identified in the 2016/17 annual plansDHBs to complete template provided by the Ministry on progress to date on deliverables for stroke identified in the 2016/17 annual plans
3 1 January – 31 March
Regional teleconference to discuss ACS, including discussion on ACS indicatorsRegional teleconference to discuss Stroke, including discussion on stroke indicators
4 1 April – 30 June 2017
DHBs to complete template provided by the Ministry on progress to date on deliverables for ACS identified in the 2016/17 annual plansDHBs to complete template provided by the Ministry on progress to date on deliverables for stroke identified in the 2016/17 annual plans
44

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP21: Immunisation coverage (includes previous health target)
Summary informationIndicators At least 95 per cent of two year olds are fully immunised and coverage is maintained At least 95 percent of four year olds are fully immunised by age 5 years as at June 2017 reported
for each three month period quarterly. At least 70 percent of girls are fully immunised for HPV - reported annually in quarter 4. (for
2016/17 it is the 2003 birth cohort measured at 30 June in 2017)Measures Reporting
Target: Targets set in APs Type: Exception
Reporting frequency: Quarterly if coverage is not reachedAnnual for HPV
Source data/template for reporting provided by: Data supplied from Ministry from NIR
Linkages: This performance measure is also included in the Maori health plan or
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care) or
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Supporting vulnerable children (Increase infant
immunisation rates and reduce the incidence of rheumatic fever)
Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targets System Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People
Improved quality, safety and experience of care(individuals and their family/ focus focus)
45
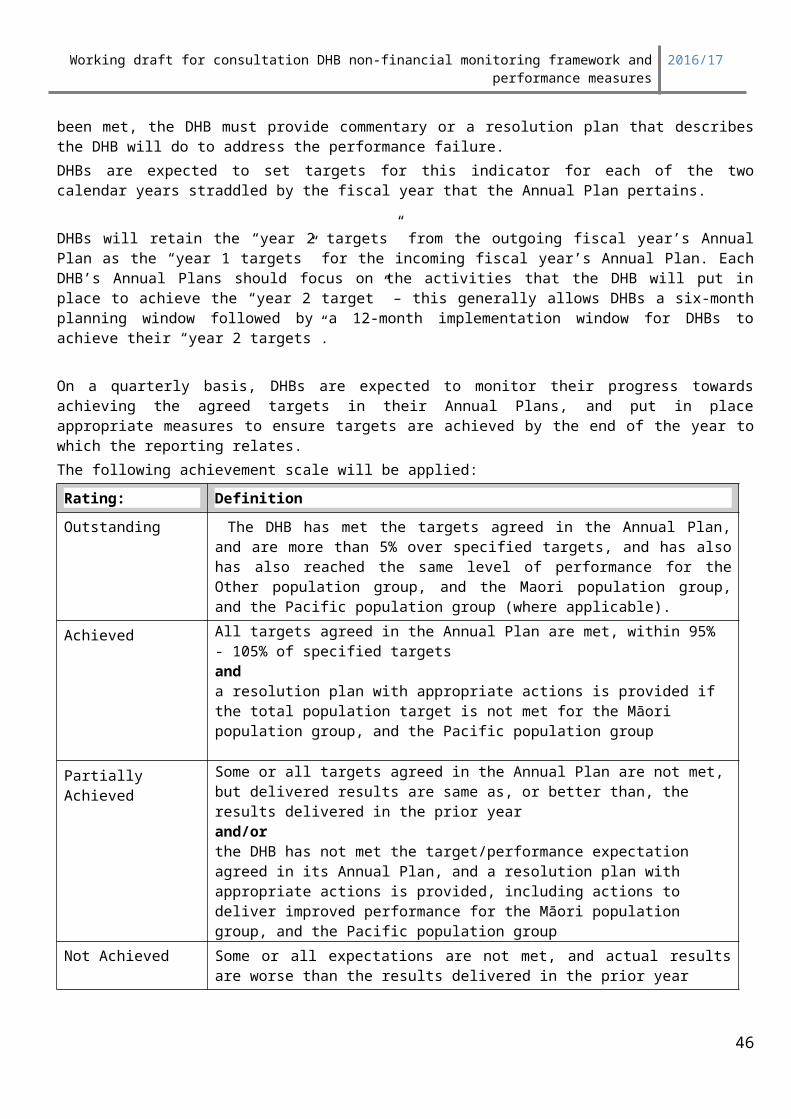
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Rising to the Challenge Maternal and Child Health Cancer ServicesOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Delivery of this measure most strongly supports the following sector outcomes and government priorities: Improved immunisation coverage leads directly to reduce rates of vaccine-preventable disease, and consequently better health and independence for children. This equates to longer and healthier lives. The changes which are required to reach the target immunisation coverage levels will lead to better health services for children, because more children will be enrolled with and visiting their primary care provider on a regular basis. It will also require primary and secondary health services for children to be better co-ordinated. These actions are leading to improved implementation of the Primary Health Care Strategy, and the primary care workforce including maternity is better equipped to address the needs of children and families.
Training in immunisation provision, health education for parents, knowledge about vaccine-preventable diseases and how to identify and provide services to high needs populations will generalise to a range of other child and family service areas.
The Ministry of Health recommends a HPV school-based immunisation programme as the preferred service delivery model for eligible girls attending primary, intermediate and secondary schools. There are successful national and international experiences of school/institution-based mass immunisation programmes, achieving high coverage rates resulting in reduced inequalities (CBG Health Research 2006, Ministry of Health 2004). School-based services may be delivered by public health nursing services on a similar basis to the existing school-based Year 7 immunisation programmes.
DHBs and schools need to work together to determine the most appropriate methods of providing follow up clinics depending upon the needs of the school and the needs of the population.
Training in immunisation provision, health education for parents, knowledge about vaccine preventable diseases and how to identify and provide services to high needs populations will generalise to a range of other child and family service areas.
Deliverables definitions and performance expectations - Focus area 1: 4 months and 5 year old coverage
Percentage of eligible children fully immunised at 24 months of age – total DHB population, Māori and PacificImmunisation coverage for two year olds will be measured quarterly using the National Immunisation Register datamart report. The coverage will be reported for Total, Maori, and Pacific (where relevant).Fully immunised at age 24 months is defined as having received all measured immunisations scheduled for 6 weeks, 3 months, 5 months and 15 months of age. To be measured as fully immunised, the child must have received all age-appropriate doses of diphtheria, tetanus, whooping
46
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
cough, polio, hepatitis B, Haemophilus influenzae type B, pneumococcal, measles, mumps and rubella vaccines. Although rotavirus is included in the National immunisation Schedule, it is not currently included in performance measures or health targets. It is anticipated that rotavirus vaccines will be included in performance measures in the future.
Percentage of eligible children fully immunised at 5 years of age – total DHB population, Māori and PacificImmunisation coverage for five year olds will be measured quarterly using the National Immunisation Register datamart report. The coverage will be reported for Total, Māori, and Pacific (where relevant).Fully immunised at age 5 years is defined as having received all measured immunisations scheduled for 6 weeks, 3 months, 5 months, 15 months and 4 years of age. To be measured as fully immunised, the child must have received all age-appropriate doses of diphtheria, tetanus, whooping cough, polio, hepatitis B, Haemophilus influenzae type B, pneumococcal, measles, mumps and rubella vaccines. Although rotavirus is included in the National immunisation Schedule, it is not currently included in performance measures or health targets. It is anticipated that rotavirus vaccines will be included in performance measures in the future.
Focus area 2: HPV coverage
Percentage of eligible girls fully immunised with HPV vaccine, total DHB population, Māori and Pacific and Other.Immunisation coverage for eligible girls will be measured annually using the National Immunisation Register datamart report. The coverage will be reported for Total, Māori, and Pacific (where relevant) and other.
Assessing DHB Immunisation CoverageFocus area 1: 4 months and 5 year old coverage:Progress towards the 24 months and 5 year old coverage targets will be assessed quarterly.Coverage will be assessed on 3 months data for the previous quarter.
The assessment requirements for each quarter are set out below:
Table 1: Quarters 1, 2 & 3 assessment 24 months and 5 year old coverageRating Explanation
Achieved The DHB has reached the year’s total population immunisation coverage target for children 24 months and children 5 years of age anda resolution plan with appropriate actions is provided if the total population target is not met for the Māori population group, and the Pacific population group..
Partially Achieved The DHB’s immunisation coverage has improved from the coverage at the start of the year
Not Achieved The DHB’s immunisation is has not improved from the coverage at the start of the year
47
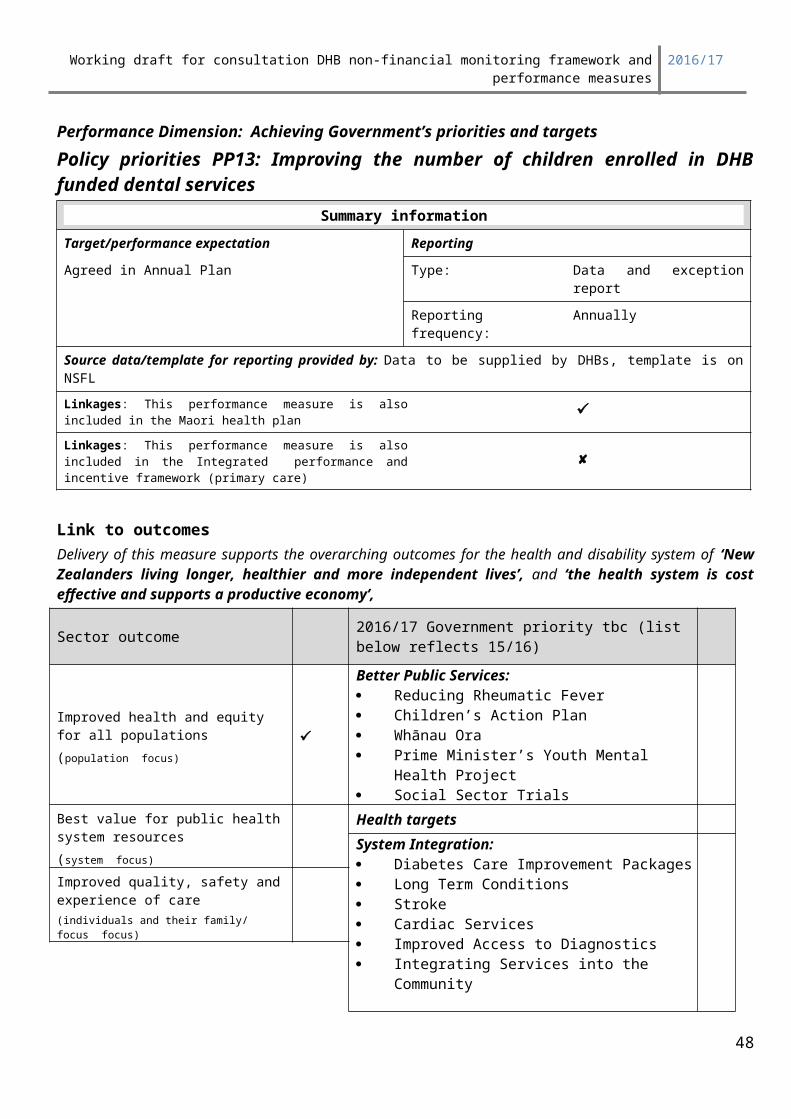
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Table 2: Quarter 4 assessment 24 months and 5 year old coverageRating Explanation
Outstanding Performer
The DHB has substantially exceeded the year’s immunisation coverage target for children 24 months, children 5 years of age and/or
The DHB has reached the year’s immunisation coverage target for children 24 months of age, children 5 years of age for:o the total population, ando the Maori population group, and where applicableo the Pacific population.
Achieved The DHB has reached the year’s total population immunisation coverage target for children 24 months of age, children 5 years of age.
Partially Achieved The DHB’s immunisation coverage has substantially improved from the coverage at the start of the year and target.
Not Achieved The DHB’s immunisation coverage has failed to substantially progress towards the target.
Focus area 2: HPV coverageProgress towards the HPV coverage target will be assessed annually as part of quarterly 3 reports only.
Table 3: Quarter 3 assessmentRating Explanation
Outstanding Performer
The DHB has substantially exceeded HPV coverage target for eligible girls; and/or
The DHB has reached the the HPV target for eligible girls for:o the total population, ando the Maori population group, and where applicableo the Pacific population.
Achieved The DHB has reached the HPV coverage target for eligible girls.
Partially Achieved The DHB’s HPV immunisation coverage has not been achieved but an acceptable resolution plan has been provided.
Not Achieved The DHB’s HPV immunisation coverage has not been achieved and an acceptable resolution plan has not been provided.
48
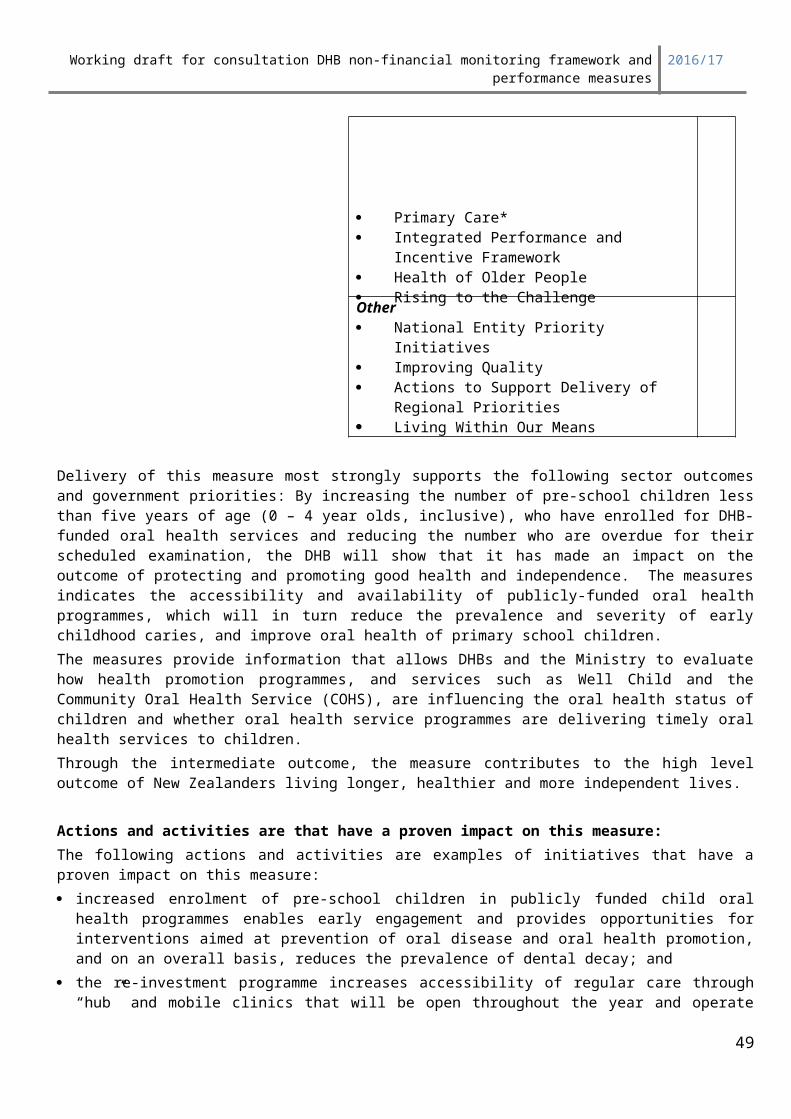
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
How to report on immunisation coverage and progressEach quarter, when DHBs do not reach target coverage they are expected to provide an exception qualitative report advising how they will track towards higher coverage. The Ministry will provide summary data for the quarter on the nationwide service framework library web site NSFL homepage: http://www.nsfl.health.govt.nz/.
DHBs may wish to access information from the NIR Datamart. A User Guide is available on NIR Datamart to assist DHBs with extracting immunisation coverage data from the NIR Datamart.
Reporting periodAll deliverables within the measure are to be provided quarterly if 95% coverage is not reached.
Quarter For the time period1 1 July – 30 September
2 1 October – 31 December
3 1 January – 31 March (coverage for children 24 months and children 5 years of age)Calendar year to 31 December 2015 for HPV coverage
4 1 April – 30 June
NIR Datamart report instructions
Report Name: the NIR Datamart report “NIR BC CI Overview - Milestone Ages DHB.rep’’, three month final dose.
This report includes pneumococcal vaccine. To run this report use last day of the reporting quarter. Both excel and pdf versions of the report as well as summarised report will be available to DHBs
under toolkit section of DHB Quarterly database each quarter. DHBs are expected to use these reports to provide exception qualitative report and/or use this
mechanism to raise issues with the Ministry.
49
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP22: Improving system integrationSummary information
Indicator: Progress on delivery of the actions and milestones to improve integration identified in DHB Annual Plans
Measures Reporting
Target: Actions and milestones agreed in APs Type: Progress update
Reporting frequency: Quarterly
Source data/template for reporting provided by: Checklist of actions supplied on the quarterly reporting website
Linkages: This performance measure is also included in the Maori health plan Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality
50
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Actions to Support Delivery of Regional Priorities Living Within Our Means
Deliverables definitionsThis indicator is currently under development awaiting decisions from the GovernmentDHBs are expected to report on delivery of the actions and milestones to improve integration identified in Annual Plans. Each quarter the Ministry will present checklists that summarise the system integration actions agreed in Annual plans on the quarterly reporting web site as follows:
System integration check listDHBs are required to provide a quarterly update identifying progress made during the quarter against the actions and milestones (deliverables) in each checklist. The progress update must include:
Whether the DHB is on track meeting each deliverable by the end of quarter 4, including comment on specific actions delivered in the quarter
Where deliverables are not on track the report must include mitigation strategies and new timeframes for delivery
Where quantitative measures are reported – Reports must include baseline, target and quarterly performance progress
ExpectationsThe assessment requirements for each quarter are set out below:
Table 1: Quarterly assessmentRating Explanation
Achieved All actions, milestones and measures are on track.
Partially Achieved Some actions, milestones and measures are not on track but adequate mitigation strategies are presented.
Not Achieved Some actions, milestones and measures are not on track and adequate mitigation strategies are not presented or there are any missing deliverable components.
Reporting periodQuarter For the time period1 1 July – 30 September
2 1 October – 31 December
3 1 January – 31 March
4 1 April 13 – 30 June
51
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP23: Improving Wrap Around Services – Health of Older People
Summary informationIndicator: Progress on delivery of the actions and milestones to improve wrap around services for older people identified in DHB Annual Plans
Measures ReportingType: Process Type: Progress update
Target: Actions and milestones agreed in APs
Reporting frequency: Quarterly
Source data/template for reporting provided by: Checklist of actions supplied on the quarterly reporting website
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targets
System Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge
Improved quality, safety and experience of care(individuals and their family/ focus focus)
52
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Maternal and Child Health Cancer ServicesOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
DHBs are expected to report on delivery of the actions and milestones to improve wrap around services for older people identified in 2016/17Annual Plans.
The deliverables for 2016/17 are listed below.
Home and community support services for older people, specifically:Place holder - Pending outcomes resultant of IBT Director General’s Reference Group’s report to the Director General of Health
InterRAI: (Comprehensive Clinical Assessment) in aged residential care and in home setting, specifically:DHBs need to continue to implement the roll out of interRAI Comprehensive Clinical Assessments and individual care plans based on those assessments comprehensively in their districts. They need to check that interRAI assessments are being undertaken within appropriate timeframes in all of the pathways to receiving long-term home and community support and aged residential care services and take corrective action as required. DHBs also need to ensure that regular reassessments are undertaken. DHBs need to be active in initiating and reviewing reporting on volumes and measures. This includes:
Evidence of the number of older people who received long-term support services for home and community support services.
The percentage of people in aged residential care by facility and by DHB who have a subsequent interRAI long term care facility (LTCF) assessment completed within 230 days of the previous assessment.
The percentage of LTCF clients admitted to an aged residential care (ARC) facility who had been assessed using an interRAI-HC (home care) assessment tool in the six months prior to that first long term care facility (LTCF) assessment.
Show time taken for any referral from any source to complete (not triage) an interRAI assessment. i.e. Contact, interRAI-HC, LTFC assessment.
Use interRAI measures to progress and compare performance with other DHBs.
Dementia care pathways, specifically:
Provide specific detail of improvements to support and services available following a dementia diagnosis (e.g. access to education and support programmes for carers or people living with dementia, initiatives to support informal carers).
53
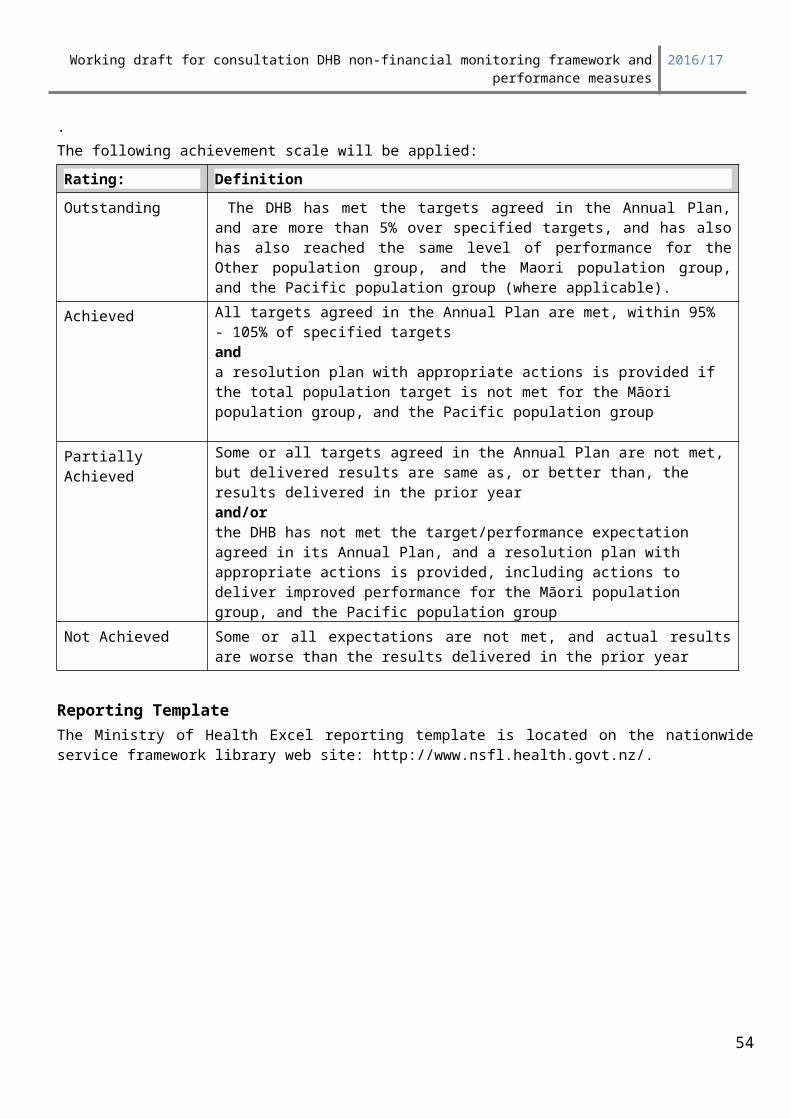
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
HOP specialists: Reporting on this measure is no longer required from 2016/17 but the expectation remains within the service coverage schedule.
Cross Agency: Minimisation Of Harm From Falls And Fracture
Report the number of people who are referred to the fracture liaison service by primary care and by secondary care and following assessment, report the number of people referred to community strength and balance programmes for each group.
Report the number of people who are referred to the fracture liaison service the number referred by primary and by secondary care and after assessment, report the number of people who receive osteoporosis treatment for each group.
Place holder : pending outcomes of cross agency hospital to home project
Actions and activities that have a proven impact on this measure:DHBs are required to provide a quarterly update identifying progress made during the quarter against the actions and milestones (deliverables) as outlined in the guidance. The progress update must include:
whether the DHB is on track to meet each deliverable by June 2017, including comment on specific actions delivered in the quarter
where deliverables are not on track, the report must include mitigation strategies and new timeframes for delivery
where quantitative measures are reported, reports must include baseline, target and quarterly performance progress (where applicable).
Deliverables definitions
As part of the progress report for each expectation, DHBs should:
provide the DHB-specific information and/or data requested
provide any other information that is relevant to the deliverables and measures
provide information on progress against the nationwide expectations and measures if any?
indicate whether or not the DHB is on track to meet its targets and, if not, explain why this is the case, what is being done to address the issue, and any revised timelines
include baseline data (where applicable).
ExpectationsThe assessment requirements for each quarter are set out below:
Table 1: Quarterly assessment
Rating ExplanationAchieved All actions, milestones and measures are on track.
Partially Achieved Some actions, milestones and measures are not on track but adequate mitigation strategies are presented.
Not Achieved Some actions, milestones and measures are not on track and adequate mitigation strategies are not presented.
54

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
55
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Reporting period
Quarter For the time period1 1 July – 30 September
2 1 October – 31 December
3 1 January – 31 March
4 1 April – 30 June
interRAI Assessments For People Receiving Home And Community Support ServicesSummary informationIndicator: The percentage of older people receiving long-term home and community support that have a comprehensive clinical assessment and an individual care plan
Target/performance expectation:Target agreed in annual plan
ReportingType: All DHBs to provide a brief
comment on result (including number and proportion of eligible people receiving assessments).DHBs not meeting expectation are to provide a detailed exception report.
Reporting frequency:
Quarterly
Source data/template for reporting provided by: interRAI data will be supplied by the New Zealand interRAI software host (Health Intelligence Ltd).
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
tbc
Delivery against this measure would result in:
a more unified and improved health and disability system augmented by all health professionals who support older people having a common language of assessment and easily transferred information about the patient’s health conditions
people receiving better health and disability services because service decisions would be based on a robust internationally verified assessment tool
Good health and independence will be protected and promoted through assessment of rehabilitation potential and individual care plans, and the health and disability system and services will be trusted and used with confidence because the assessments are a comprehensive bio-psycho-social assessment that provides the best information for forming care plans. There will also be more confidence in support services because completing the assessments (and reassessments) will enable the quality of services provided to be measured through the quality indicators the tool produces.
56

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Actions and activities that have a proven impact on this measure:DHBs need to implement the roll out of Comprehensive Clinical Assessments and individual care plans based on those assessments comprehensively in their districts. They need to check that assessments are being undertaken in all of the pathways to receiving long-term support services and take corrective action where required. They also need to ensure that regular reassessments are undertaken. System clinicians need to be active in initiating and reviewing reporting on volumes and quality measures.
Deliverables definitionsNumerator: The number of people aged 65 and older who have received long-term home and community support services in the last three months who have had a Comprehensive Clinical Assessment and a completed care plan.
Denominator: The number of people aged 65 and older who have received long-term home and community support services in the last three months.
Interpretation issues Long-term home and community support services are provided for six or more weeks.
This applies to publicly funded home and community support services.
Comprehensive Clinical Assessments include interRAI Contact Assessments, Home Care and Community Health Assessments.
Any previous CCA would be counted, not just those in the last 3 months.
Reporting Period Quarterly. The measure will be calculated based on data that is one quarter in arrears.The numerator is calculated as follows:
• in quarter one, the numerator is based on data recorded for the 3 months to 30 June;
• in quarter two, the numerator is based on all data recorded for the 3 months to 30 September;
• in quarter three, the numerator is based on all data recorded for the 3 months to 31 December;• in quarter four, the numerator is based on all data recorded for the 3 months to 31 March.The denominator is a three month total calculated as follows:
• in quarter one, the denominator is based on data recorded for the three months to 30 June (to calculate those who received services at any time between 1 April and 30 June) adjusted to count only those people who have continued to receive services for at least six weeks. For example if a person begins receiving services on 30 June they must still be receiving services on 11 August to be included in the denominator.
• in quarter two, the numerator is based on data recorded for the three months to 30 September (to calculate those who received services at any time between 1 July and 30 September) adjusted as described above.
• in quarter three, the numerator is based on data recorded for the three months to 31 December (to calculate those who received services at any time between 1 October and 31 December) adjusted as described above.
• in quarter four, the numerator is based on data recorded for the three months to 31 March (to calculate those who received services at any time between 1 January and 31 March) adjusted as described above.
57
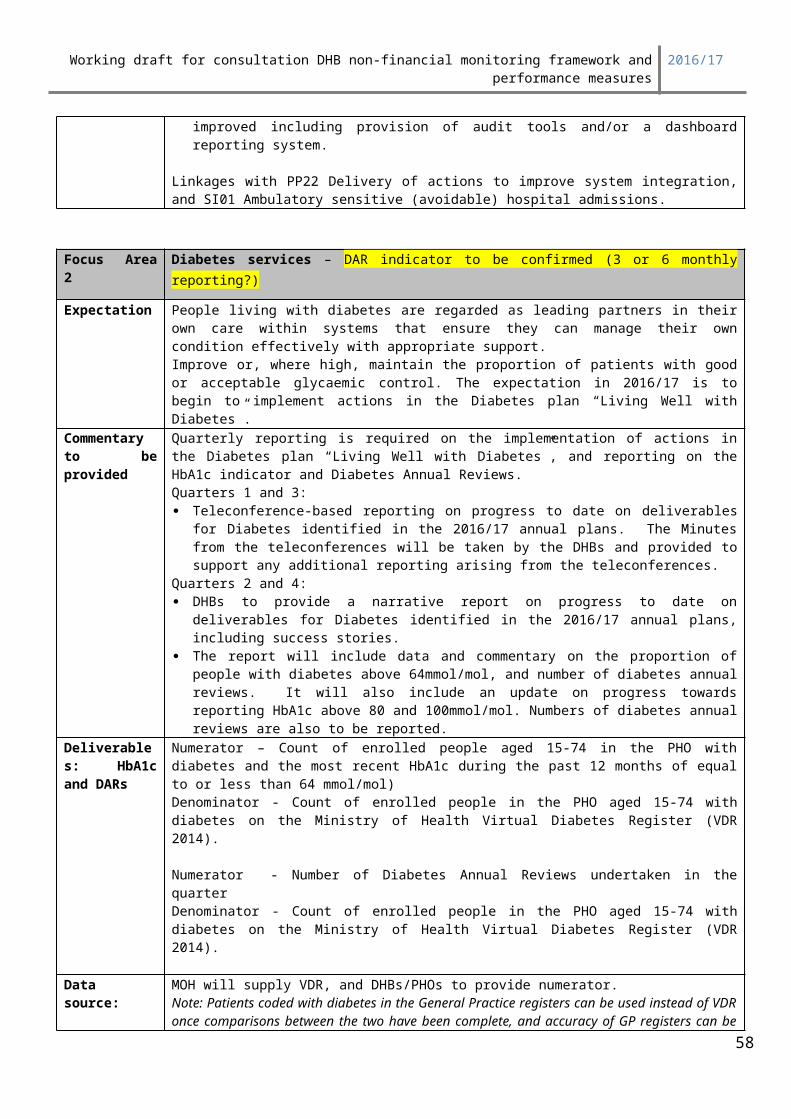
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
InterRAI (LTCF) For People Living In An Aged Residential Care Facility All DHBs need to monitor staff capability/capacity to complete interRAI long term care facility assessments within appropriate timeframes for people living in age residential care. The indicator below has been drafted by Central Technical Advisory Service’s Data Analysis and Reporting service to inform DHBs quarterly of each age residential care facility’s ability to complete assessments as required. The Ministry of Health requires the reported data to be aggregated up by DHB to indicate sector performance against this measure.
Indicator Percentage of people in aged residential care by facility and by DHB who have a subsequent interRAI long term care facility (LTCF) assessment completed within 230 days of the previous assessment.
Rationale This is a key performance measure for DHBs in the 2016/17Planning Priorities for Annual Plans and Regional Service Plans to meet their ministerial expectations.The Ministry of Health requires the interRAI Data Analysis and Reporting Service to provide DHBs with this information. This information will enable DHBs to be aware of each Aged Residential Care (ARC) facility’s progress to complete second assessments as required within the ARC agreements.It will also enable DHBs to identify and support facilities that are having difficulty to complete routine interRAI assessments regularly and to report sector performance back to the Ministry of Health via the Annual Plan quarterly reports.The wording of this indicator has altered slightly from the original outcomes document but is consistent with the intent of the indicator.
ContextFrom July 2015 onwards, an assessor/nurse must complete a short term care plan within 24 hours of admitting a client to an aged residential care facility. It is anticipated that the admission care plan will be informed by the transferred home care assessment. A full interRAI LTCF first assessment and long term care plan should be completed within 21 days of admission. The assessment reference date (ARD) refers to the last date of observation for a particular assessment. A second routine reassessment should be completed within six months of the ARD. Further routine assessments should continue to occur at six month intervals (this indicator of 230 days is more lenient than six months).
PurposeThe purpose of this document is for the interRAI Data Analysis and Reporting team to automate this data to be produced on a quarterly basis to support DHBs in their performance monitoring.
Stakeholders 20 DHB CEOs. DHB GMs Planning and Funding DHB Health of Older People (HOP) Portfolio Managers8
Aged Residential Care (ARC) Providers (note that TAS will send this data only to DHBs not to ARC providers)
Ministry of Health9
TAS Resources Mark Seidelin – BI DeveloperShane Kerr – Senior AnalystJason Theobald – Senior Analyst
Stakeholder Engagement/ Communication
The approach in how to send out this reporting to DHBs still needs to be discussed and agreed by TAS. In the past, we have emailed data directly to DHB Portfolio managers or sent through communication via Susan Noseworthy. However, in the future, we could send through data to DHBs, e.g. via Connex.
8
9 Key contact at the Ministry for this reporting is Penny Hanning, Senior Portfolio Manager, Health of Older People, National Service purchasing National Health Board, Ministry of Health.
58
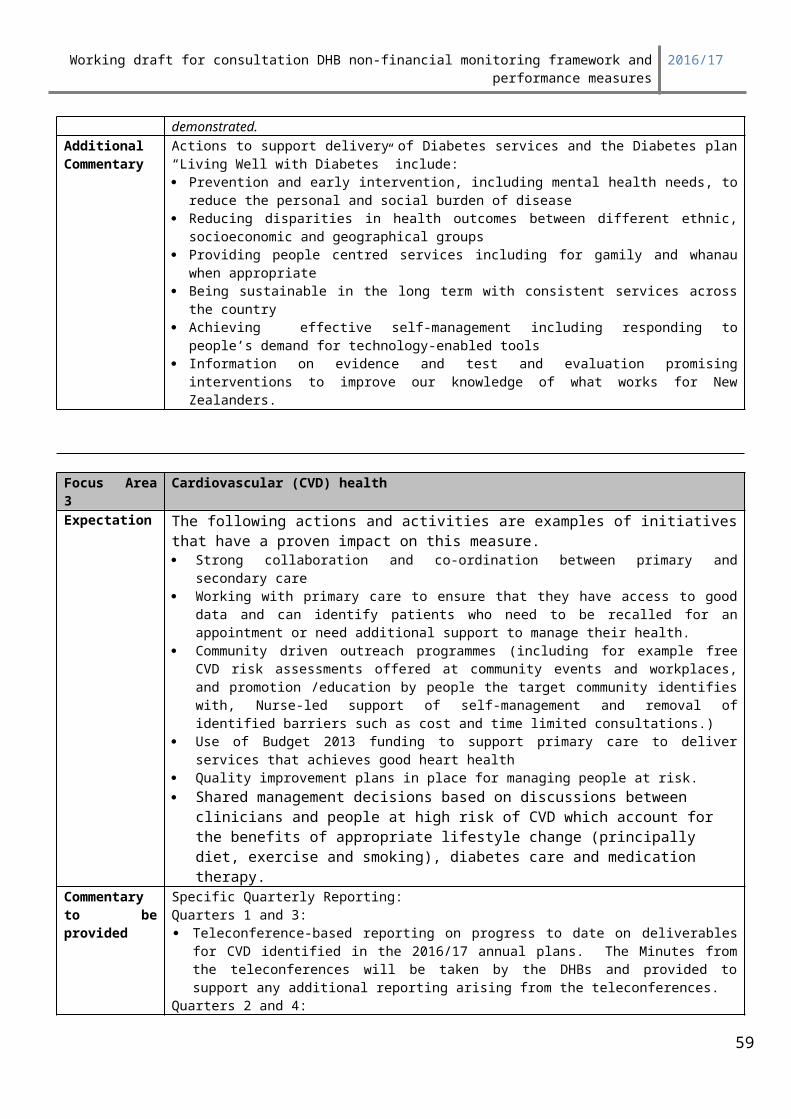
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Indicator Definition
Denominator (note: dates are stated for Q1 2015/16):
Count of assessments whereo Assessment type = LTCFo Assessment date = 13/11/2014 – 12/02/2015 (230 days before the reporting
period of 01/07/2015 – 30/09/2015)o Client has not moved facilities between this assessment and the subsequent
assessment By facility (all facilities are to be included even if no matching assessments have
been recorded during the period), by DHB (linked by facilities mapping table)Numerator:
Using the list of NHIs (with facility, DHB, assessment date) generated in producing the denominator, count the number of NHIs where
o Assessment type = LTCFo Assessment date > previous assessment dateo Assessment date <= previous assessment date + 230 days
Deliverable A table for each DHB showing the indicator: numerator (number of subsequent assessments), denominator (number of previous assessments) and percentage, for every aged residential care facility within the DHB.
Example of how the report should look like for a DHB
Indicator: Percentage of people in aged residential care by facility and by DHB who have a subsequent interRAI long term care facility (LTCF) assessment completed within 230 days of the previous assessment.Period: 2016/17Q1DHB: AucklandFacility Number of previous
assessments (denominator)Number of subsequent assessments (numerator)
Percent
Facility1 XX XX XXFacility2 XX XX XXFacility3 XX XX XXFacility4 XX XX XXTotal: XX XX XX
InterRAI Home Care (HC) Assessments Completed For People Going Into Aged Residential Care
DHBs need to complete interRAI-HC assessments to ensure that each potential subsidised resident admitted to aged residential care (either directly from the community or via in-patient care) has been assessed using the interRAI home care assessment tool within the 6 months before the date on which it is intended. The indicator below has been drafted by Central Technical Advisory Service’s Data Analysis and will be circulated to DHBs quarterly so that they are aware of how aged residential facilities in their district are performing against this measure and can take steps if necessary to remedy needs assessment and service coordination processes.
59

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP24: Improving Waiting Times – Cancer Multidisciplinary Meetings
Summary informationIndicator: Progress delivering improved functionality and coverage of high-quality cancer multidisciplinary meetings (MDMs) based on the actions agreed in the 2014/15 annual plans and the regionally agreed activities using all of the allocated funding.
Measures Reporting
Type: Process Type: Progress update
Target: Funding high-quality MDMs for all main cancer tumour types and increasing the number of cases discussed at MDMs.
Reporting frequency: Six monthly in quarter two and four
Source data/template for reporting provided by:
N/A
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targets
System Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge
Improved quality, safety and experience of care(individuals and their family/ focus focus)
60

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Maternal and Child Health Cancer ServicesOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Improving cancer multidisciplinary meetings provides an opportunity to discuss more patients who are
newly diagnosed with cancer, and those patients whose case requires further review leading to improved
quality, safety and experience of care. International evidence shows that multidisciplinary care is a key part
of providing best-practice treatment and care for patients with cancer.
Some of the benefits of MDMs are that:
treatment planning is improved because health professionals consider the full range of therapeutic
options, which improves outcomes
improved equality of outcomes for patients with cancer
more patients are offered the opportunity to take part in relevant clinical trials
there is greater continuity of care and less duplication of services
services are better coordinated
communication between care providers improves, as clear lines of responsibility are developed
between members of the multidisciplinary meeting
time and resources are used more efficiently.
Actions and activities are that have a proven impact on this measure:The Ministry expects that DHBs will be using the Guidance for implementing high-quality multidisciplinary
meetings (http://www.health.govt.nz/publication/guidance-implementing-high-quality-multidisciplinary-
meetings) to inform their MDM actions. The following actions and activities are examples of initiatives that
have a proven impact on this measure.
1. Reviewing existing MDMs against the Ministry's guidance, identifying areas for improvement, developing action plan and implementing the actions.
2. Reviewing and agreeing formal terms of reference and meeting processes for all MDMs.3. Establishing processes for secondary service DHBs to link into tertiary DHB MDMs, supporting
regional MDMs that are multidisciplinary.10
10 A multidisciplinary meeting is a deliberate, regular meeting either face-to-face or via videoconference at which health professionals with expertise in a range of different specialities discuss the options for patients’ treatment and care prospectively. It is not a multidisciplinary meeting if the meeting only has surgeons present.
61
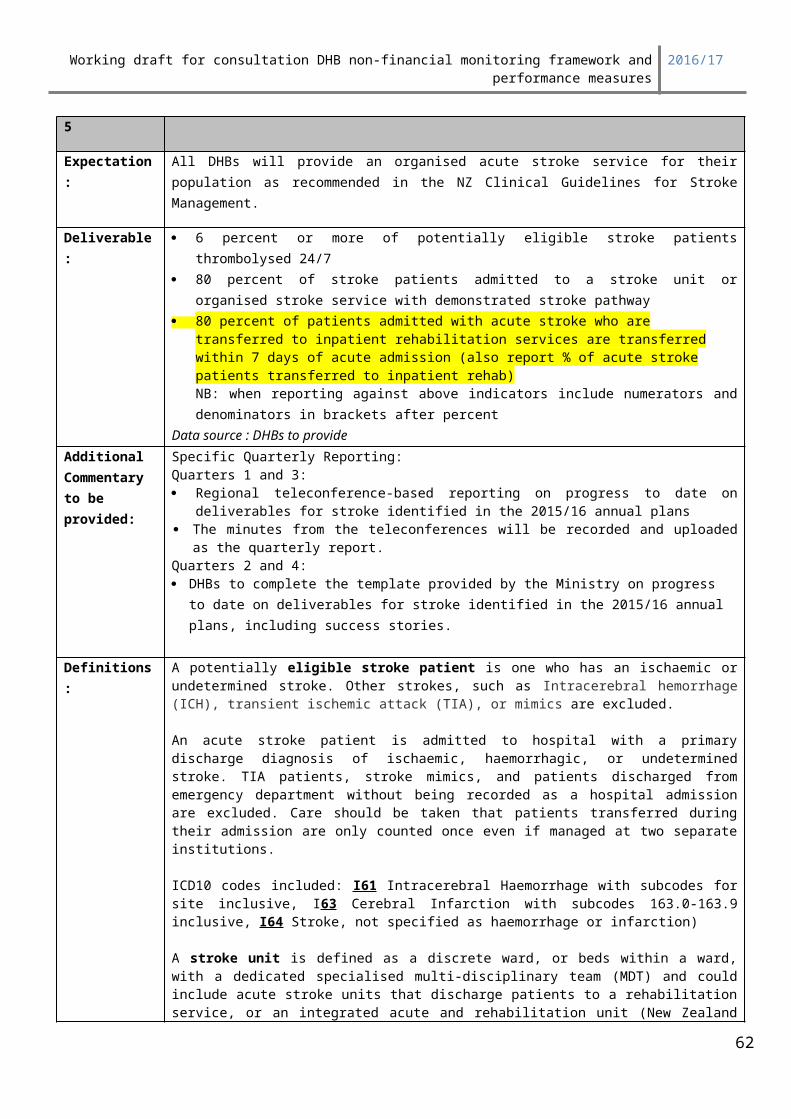
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
4. Implementing tumour specific electronic MDM proformas.5. Purchasing and implementing videoconferencing technology.6. Appointing MDM coordinators.7. Implementing MDM meeting management tools.
The Ministry is developing criteria to help DHBs to prioritise patients to be seen at MDMs, as they continue to work towards improving coverage of MDMs. The National Lung Cancer Working Group has developed the Lung Cancer Multidisciplinary Meeting Toolkit, which includes provisional criteria for lung cancer patients.
Deliverables definitionDHBs are expected to report on their progress delivering improved cancer MDMs using the $2 million in funding directed to increasing MDMs for all main11 cancer tumour types and increasing the number of cases discussed at MDMs. DHBs are also expected to provide a progress update against the actions agreed in the annual plans.
DHBs are expected to provide:1. Information on the activities that the DHB is implementing to improve cancer MDMs; and 2. how the DHB has spent their portion of the funding for MDMs or how the DHB intends to spend the
funding (see table below with information on the funding split for each DHB), and information on any underspend and how it will be managed.
Where the funding is pooled regionally and the MDM actions are undertaken regionally, the Ministry expects each DHB to provide information on the regional actions and the DHB contribution to the delivery of regional actions. The Ministry recommends that you consider a regional approach to most efficiently and effectively fund the additional MDM activity. Regional approaches will allow more patients to benefit from MDMs, particularly those patients from smaller DHBs.Funding allocationsDHB Funding
Auckland $ 184,997.63
Bay of Plenty $ 110,207.51
Canterbury $ 221,345.03
Capital & Coast $ 117,490.52
Counties Manukau $ 218,416.86
Hawkes Bay $ 78,556.61
Hutt $ 63,909.25
Lakes $ 50,301.28
Mid Central $ 82,892.42
Nelson Marlborough $ 67,091.22
Northland $ 86,488.86
South Canterbury $ 29,471.22
Southern $ 137,674.71
Tairawhiti $ 25,592.42
Taranaki $ 54,829.46
11 Main cancer tumour types include bowel, breast, central nervous system (and brain), gynaecological, haematological, head and neck, lung, melanoma, sarcoma, upper gastrointestinal, and urological.
62
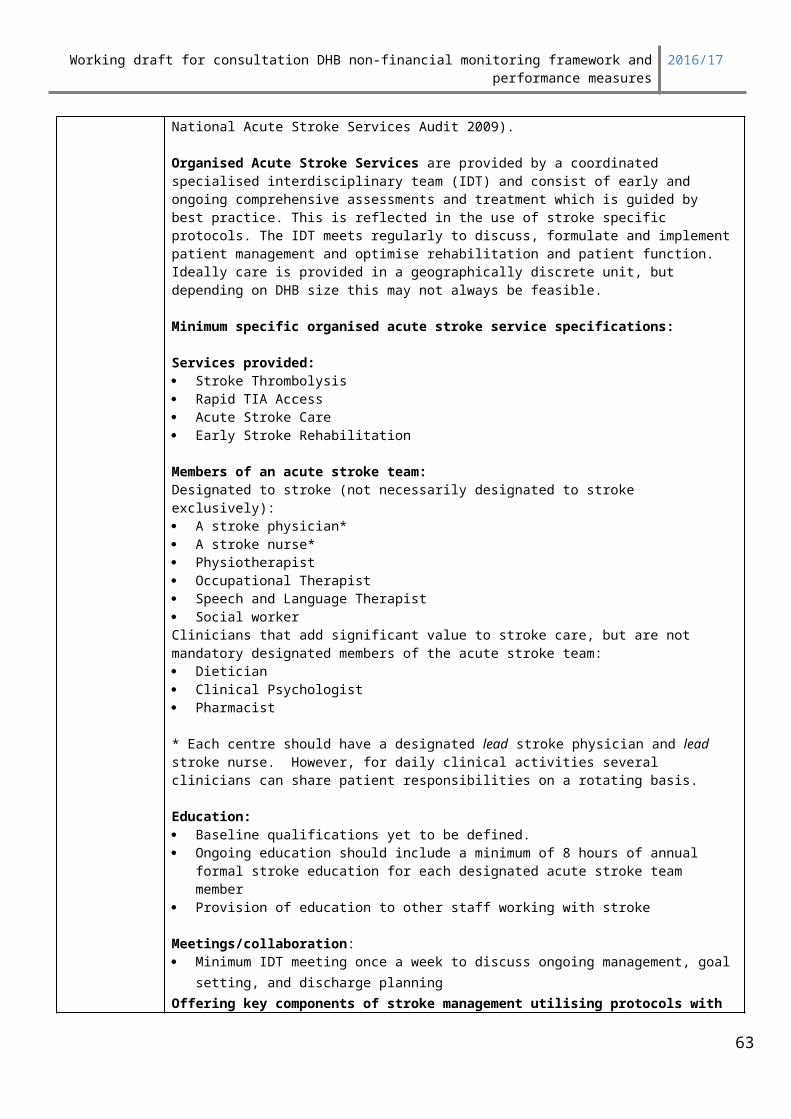
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Waikato $ 173,617.82
Wairarapa $ 21,757.03
Waitemata $ 221,787.14
West Coast $ 18,237.73
Whanganui $ 35,335.28
Total $ 2,000,000.00
ExpectationsThe assessment requirements for each quarter are set out in table 1 below.
Table 1. Quarterly assessmentRating Explanation
Achieved All actions, milestones and measures are on-track. Sufficient information on how the DHB has spent or will spend their portion of the funding is provided.
Partially achieved Some actions, milestones and measures are not on-track but adequate mitigation strategies are presented. Sufficient information on how the DHB has spent or will spend their portion of the funding is provided.
Not achieved Some actions, milestones and measures are not on-track and adequate mitigation strategies are not presented. No or insufficient information on how the DHB will spend their portion of the funding is provided.
Reporting periodQuarter For the time periodone 1 July – 30 Septembertwo 1 October – 31 Decemberthree 1 January – 31 Marchfour 1 April – 30 June
63
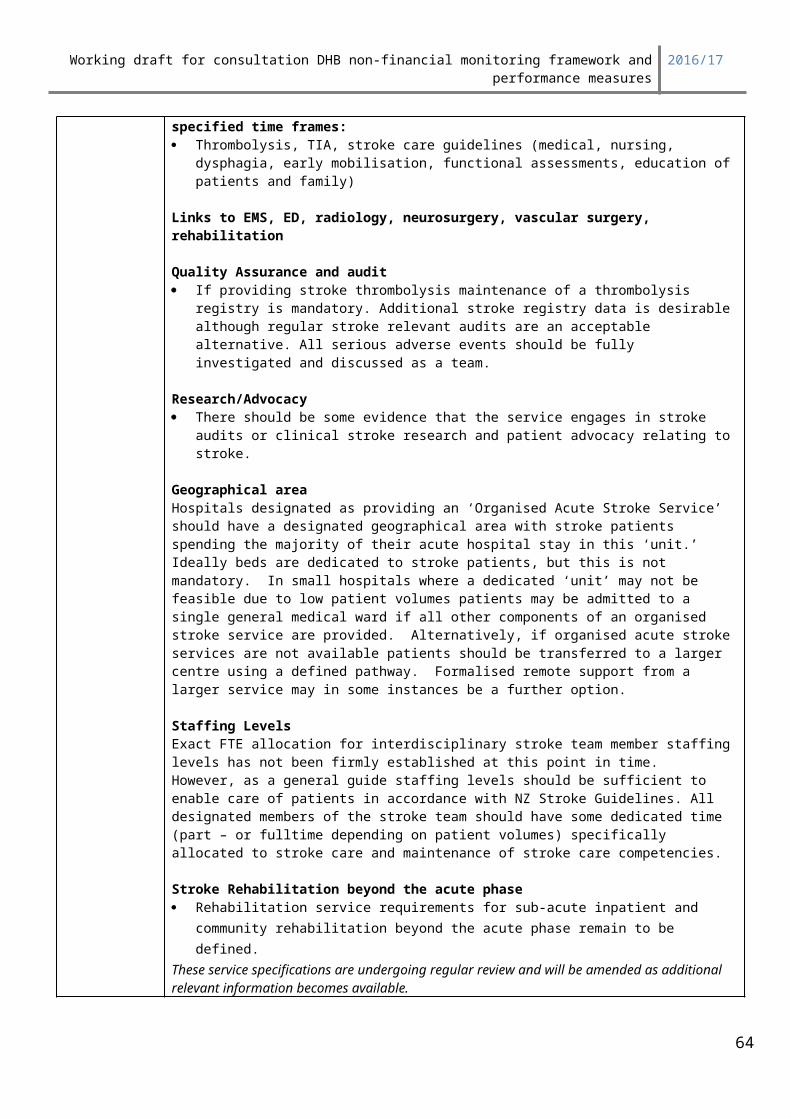
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP25: Prime Minister’s youth mental health project Summary information
Indicator: Progress update reports on actions to implement Initiatives 1, 3 and 5 of the Prime Minister’s Youth Mental Health Project
Measures Reporting
Type: Process Type: Qualitative and quantitative
Target: Provision of complete report Reporting frequency: Quarterly
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other
64
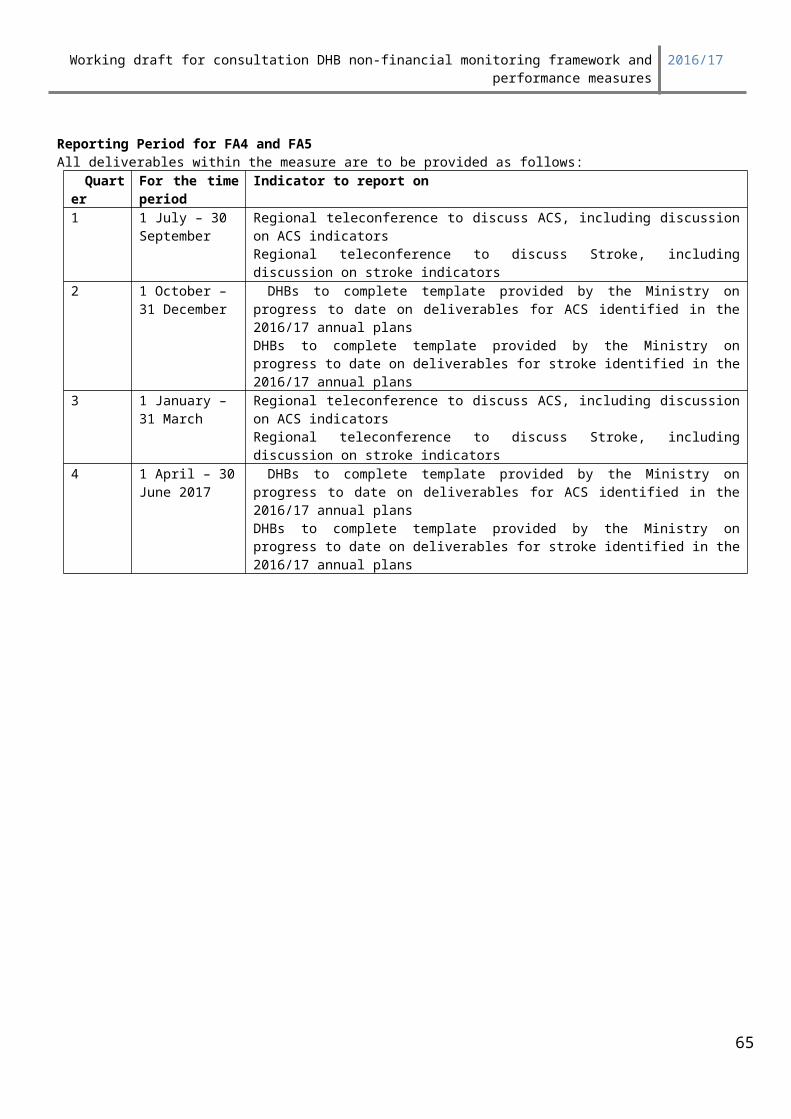
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
PP25 reports on progress towards achieving three initiatives in the Prime Minister’s Youth Mental Health Project:
Initiative 1: School Based Health Services (SBHS) in decile one to three secondary schools, teen parent units and alternative education facilities
Initiative 3: Youth Primary Mental Health ((reported under PP26) Initiative 5: Improve the responsiveness of primary care to youth.
Note: Initiative 6 is reported under PP8, and Initiative 7 is reported under PP7.
Young people are often unable or reluctant to access primary care and mental health services. Often the services in their local area are geared towards treating adults or people with more acute needs. Young people may require a unique mix of social, developmental and health services, and their family GP may not have sufficient expertise to provide the full range of care needed. Young people can also feel uncomfortable discussing their issues with their usual family GP. To improve youth access to appropriate primary care services, young people need a range of sustainable youth-friendly health and social services, including:
youth specific services as appropriate for the locality, which may include youth wellness hubs/networks, School Based Health Services or Youth One Stop Shops (YOSS); and
General practice that is responsive to youth
Responsive primary care, YOSS, Youth Wellness Hubs, and other youth-friendly organisations provide young people with a wide range of services, including mental health services, in a non-judgemental and community-based environment. Youth-friendly services help young people to overcome their reluctance and enable them to open up about their issues. This can lead to significant improvements in their mental health and wellbeing, while assisting with other problems they may be facing.
Changes we would expect to see:
Primary care services are more responsive to the specific needs of young people Improved youth access to appropriate services Improved integration of services for youth Improved sustainability of youth-specific services, such as YOSS
Actions and activities that have a proven impact on this measure:DHBs are expected to use the Alliance Leadership Team and youth Service Level Alliance Teams (SLATs) to jointly develop 2015/16 DHB Annual Plans for the Youth Services component of the Prime Minister’s Youth Mental Health Project. From 2014/15 every District Alliance shall have a youth SLAT to implement an integrated approach to improving the health and wellbeing of young people. Youth SLATs (or equivalent) shall have a mandate to make recommendations to the Alliance Leadership Team on local youth health needs and agreed changes to service provision, while providing oversight on the implementation of actions to improve youth health across the system.
The youth SLATs should include membership from youth specific health services, Social Sector Trials (SST) where they exist, and other relevant stakeholders (including the education and social sectors) as appropriate. Where SST are operating locally, DHBs are expected to work with local SST Leads for the actions identified to improve access to youth mental health and youth AOD services.
65
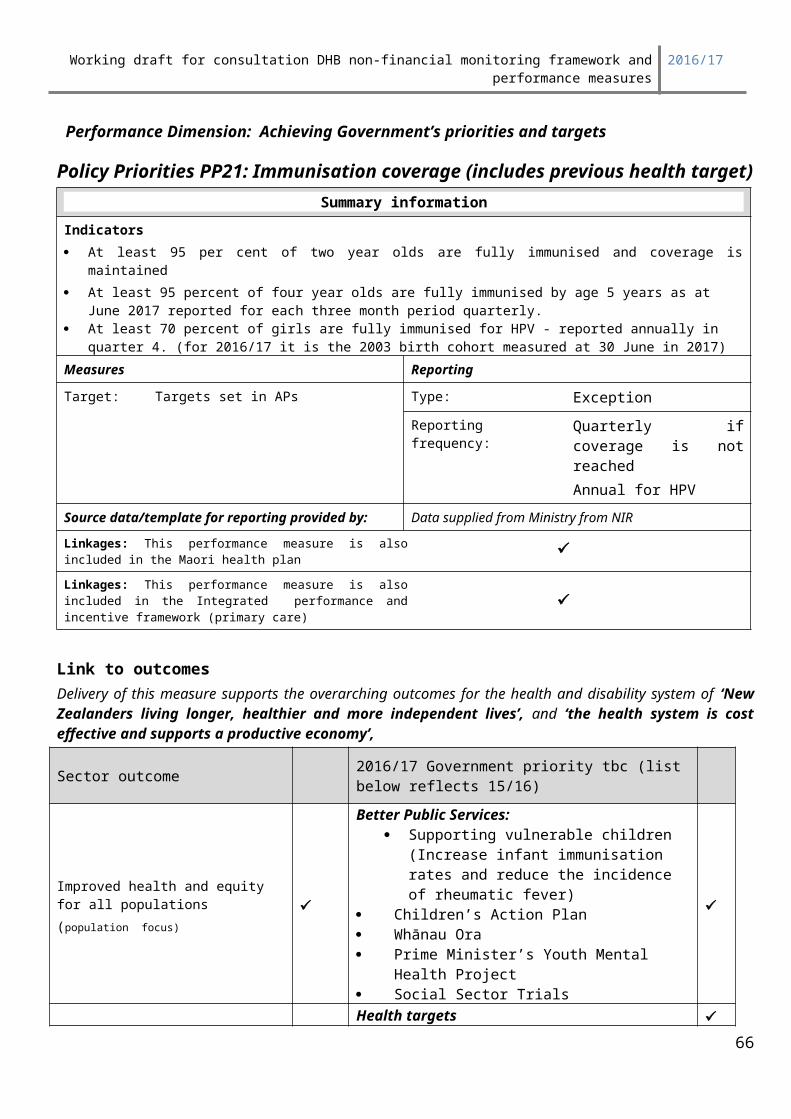
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Deliverables definitionsInitiative 1: School Based Health Services (SBHS) in decile one to three secondary schools, teen parent units and alternative education facilities.
1. Provide quarterly quantitative reports on the implementation of SBHS, as per the template provided. 2. Provide quarterly narrative progress reports on actions undertaken to implement Youth Health Care
in Secondary Schools: A framework for continuous quality improvement in each school (or group of schools) with SBHS.
Initiative 3: Youth Primary Mental Health
1. Provide quarterly narrative progress reports (as part of PP26 Primary Mental Health reporting) with actions undertaken in that quarter to improve and strengthen youth primary mental health (12-19 year olds with mild to moderate mental health and/or addiction issues) to achieve the following outcomes: early identification of mental health and/or addiction issues better access to timely and appropriate treatment and follow up equitable access for Maori, Pacific and low decile youth populations.
2. Provide quantitative reports using the template provided under PP26
Initiative 5: Improve the responsiveness of primary care to youth.
1. Provide quarterly narrative reports with actions undertaken in that quarter to ensure the high performance of the youth SLAT(s) (or equivalent) in your local alliancing arrangements.
2. Provide quarterly narrative reports with actions the youth SLAT has undertaken in that quarter to improve the health of the DHB’s youth population (for the 12-19 year age group at a minimum) by addressing identified gaps in responsiveness, access, service provision, clinical and financial sustainability for primary and community services for the young people, as per your SLAT(s) work programme.
ExpectationsRating Explanation
Achieved All actions, milestones and measures are on track.
Partially Achieved Some actions, milestones and measures are not on track but adequate mitigation strategies are presented.
Not Achieved Some actions, milestones and measures are not on track and adequate mitigation strategies are not presented.
Reporting periodQuarter For the time period1 1 July – 30 September
2 1 October – 31 December
3 1 January – 31 March
4 1 April 13 – 30 June
66
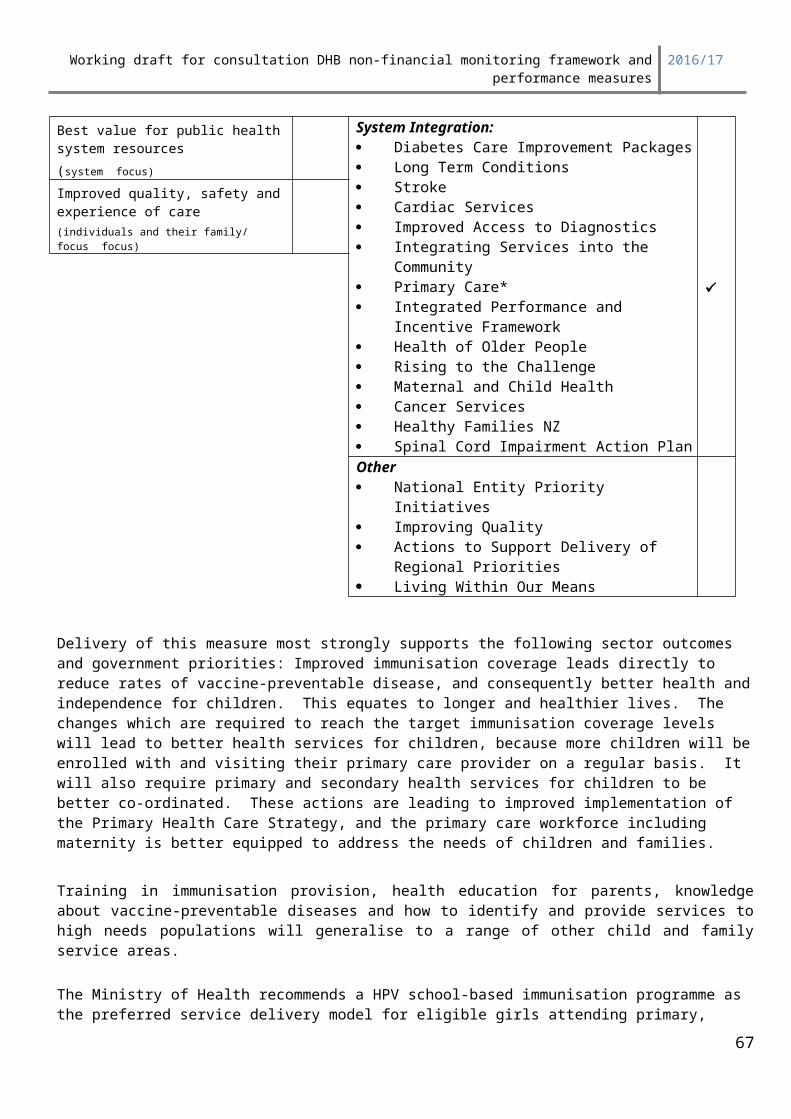
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targetsPolicy priorities PP26: Rising to the Challenge: The Mental Health and Addiction Service Development Plan
Summary informationMeasures Reporting
Type: Input Type: Full report
Target: No target – supply of information Reporting frequency: Quarterly
Source data/template for reporting provided by: Not applicable
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration:
Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge
Maternal and Child Health Cancer Services Healthy Families NZ
Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities
67
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Living Within Our Means
Link to outcomesRising to the Challenge: The Mental Health and Addiction Service Development Plan (Rising to the Challenge) clearly articulates prioritised service developments for the next four years. The Plan aims to ensure that across the spectrum of primary, specialist treatment and support services access and responsiveness will be enhanced; integration will be strengthened while improving value for money and delivering improved outcomes for people using services.
Links with the: Ministry of Health Statement of Intent and the Outcomes Framework
Delivery against this measure supports the health and disability system outcome of ‘New Zealanders living longer, healthier and more independent lives’
Deliverables definitionsFocus area 1: Rising to the Challenge implementation
A minimum of eight actions from the across the four goal areas in Rising to the Challenge identified in the Annual Plan are delivered.
Report on the status of quarterly milestones for a minimum of eight actions to be completed in 2016/17 and for any actions which are in progress/ongoing in 2016/17.
The status definitions for quarterly milestones are defined as: Complete On track Off track with mitigations
For any actions which are off track, provide the mitigation to get this action back on track.
Reporting Period
Reporting required: Each quarter, update the reporting template initially provided to DHBs as part of the in quarter two 2013/14 reporting process (refer to the DHB quarterly reporting web site and toolkit).
Focus area 2: Primary Mental HealthAs part of the implementation of goal six Delivering increased access for adults with high-prevalence conditions while increasing service integration and effectiveness, the Ministry monitors access to evidence-informed psychological therapies for mental health and addictions issues in primary care.
Primary mental health and addiction interventions are for people presenting with mild to moderate mental health and addiction problems. In addition to the general primary care response to the needs of people of any age, access to primary mental health interventions are funded for the following specific population groups:
1. The enrolled adult population focused on Maori, Pacific and/or low income. The expected outcome is increased access to psychological and psychosocial interventions for these at-risk groups.
68
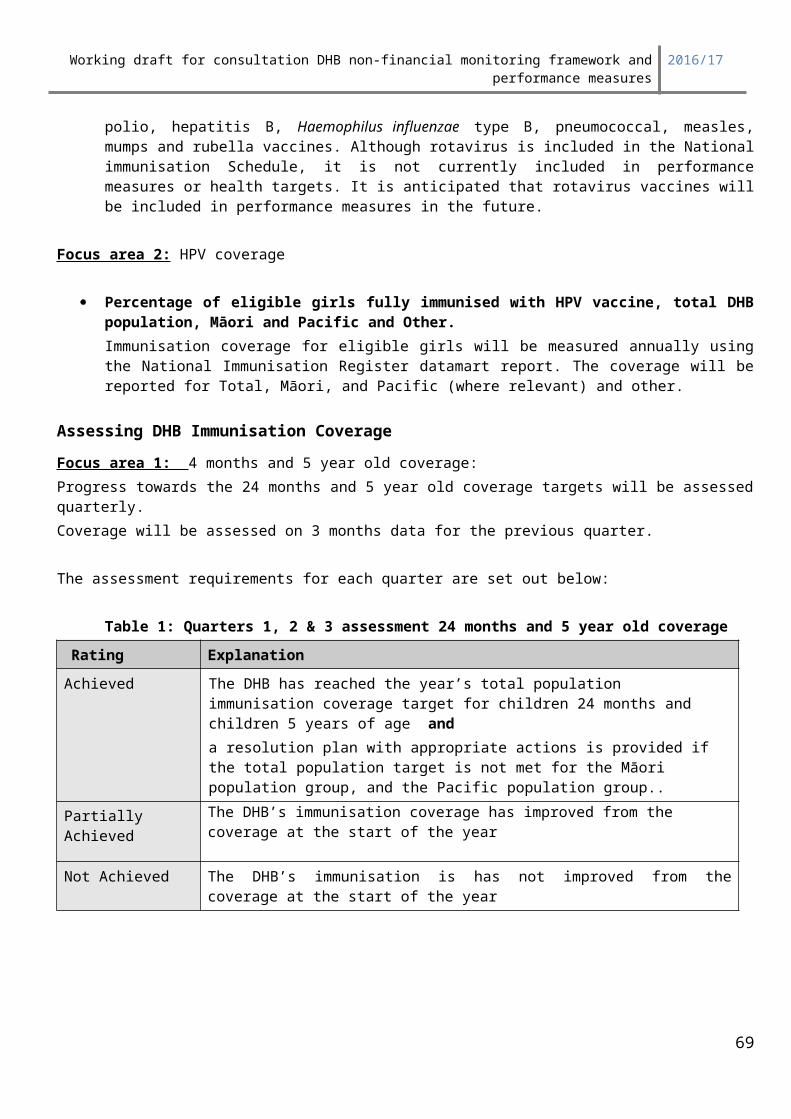
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
2. Youth primary mental health services, available to all youth in the 12 to 19 year age group (regardless of PHO enrolment) who require such a service. The expected outcomes are to enable early identification of developing mental health and/or addiction issues and better access to timely and appropriate treatment and follow up.
Reporting PeriodBy the 20th of January, April, July and October each year using the Ministry quarterly reporting website.
Reporting required: Each quarter, please update the reporting template provided (refer to the DHB quarterly reporting web site and toolkit).
Reporting (also links to PP25 Youth Mental Health Project for youth)1. Provide quarterly reports on the attached template which covers the amount of service delivered
including alcohol brief interventions (numbers of adults and youth (12-19) seen by ethnicity and services accessed). Grey boxes are optional but helpful particularly if outcome data is being captured locally.
2. Narrative report on the following: Overall assessment of the services delivered Any major achievements/successes Major issues that have affected the achievement of the contracted Services Whether services have been externally evaluated / reviewed / audited and status of
recommendations made.
Focus Area 3 District Suicide Prevention and Postvention (TBC)
Suicide prevention and postvention plans were completed and agreed in mid 2015. Please report the following as result of the plan being implemented (note: this is not a comprehensive reporting requirement on every action identified in the plan):
1. Report highlights of the implementation success2. Report expectations where actions are not being progressed and provide reasons3. Report the who has been trained and how many people have been trained
Focus Area 4 Maori Community Treatment Order Rates (TBC)
Reducing the rates of Maori on community treatment orders to be closer to the rate of other ethnicities has been a requirement in Maori Health Plans since 2014/15. Please report:
1. what possible causes have been identified for the high Maori rate of on CTOs2. what processes have been put in place to ensure an appropriate rate of Maori on
CTOs3. what has been the outcome of the actions in point 2 above
Focus Area 5 Improving Crisis response services (TBC)
Reducing the demand on police for crisis support of known clients is an important interagency goal. There is a significant range in the rate of known clients referred by police crisis services. Please outline:
1. what actions have been undertaken to reduce the rate of known clients being referred to by police to crisis teams
69
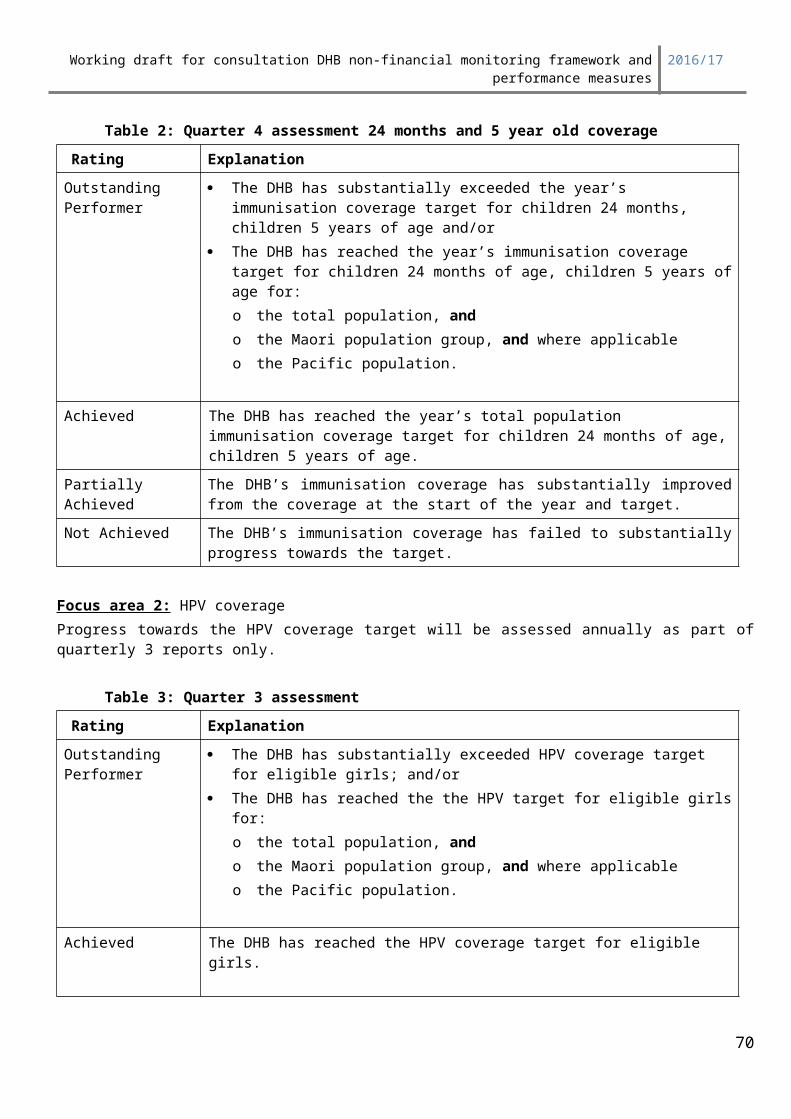
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
2. what difference have the above actions made to police referrals
70

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: ‘Achieving Government’s priorities and targets’
Policy Priorities PP27: Delivery of the Children’s Action Plan (CAP)
Vulnerable Children Act 2014
The measures in the Vulnerable Children Act 2014 (the Act) include standard safety checks for paid staff in the government-funded children’s workforce and new requirements for government agencies and their funded providers to have child protection policies.
Part 2: Child protection policies – where the DHB does not already have a child protection policy, it will adopt one, as soon as is practicable, and review that policy a minimum of three years from the date of its first adoption or most recent review (it must be reviewed thereafter a minimum of every three years). The child protection policy must be written and contain procedures for the identification and reporting of child abuse and neglect in accordance with Section 15 of the Children, Young Persons, and Their Families Act 1989. If a DHB has a pre-existing child protection policy it must also be consistent with the Act’s requirements.
Part 3: children’s worker safety checking – children’s worker safety checking aims to reduce the risk of harm to children by requiring children’s workers to be safety checked. Children’s workers are divided into core and non-core in the Act.
The Act requires that DHBs do not employ any person as a children’s worker without undertaking a safety check of that person and also that DHBs must carry out safety checks on existing workers within the organization. Checks can be made on a staggered basis. The Governor General will appoint the date which worker safety checking comes into force. It is likely that this date will be during July 2015. On this date the DHB is required to begin safety checking new employees that are part of the core workforce. One year after this date DHBs must also be undertaking safety checking for new employees that are within the non-core workforce. Safety checks for all existing core workers must be completed three years after the date worker safety checking comes into force and four years for non-core workers.
Requirements of safety checks are addressed in the Act and will be further specified in regulations prescribed by the Governor General. There are financial penalties for failing to comply with the worker safety checking aspect of the legislation.
Summary informationIndicator: Progress on delivery of the actions and milestones identified in DHB Annual Plans support the implementation of the Children’s Action Plan and reduce child assaults.
Measures Reporting
Type: Process Type: Progress update
Target: Actions and milestones agreed in APs Reporting frequency: Quarterly
Source data/template for reporting provided by: Checklist of actions supplied on the quarterly reporting website
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders are healthier and more independent ’, and ‘the health system is cost effective and supports a productive economy’,
71
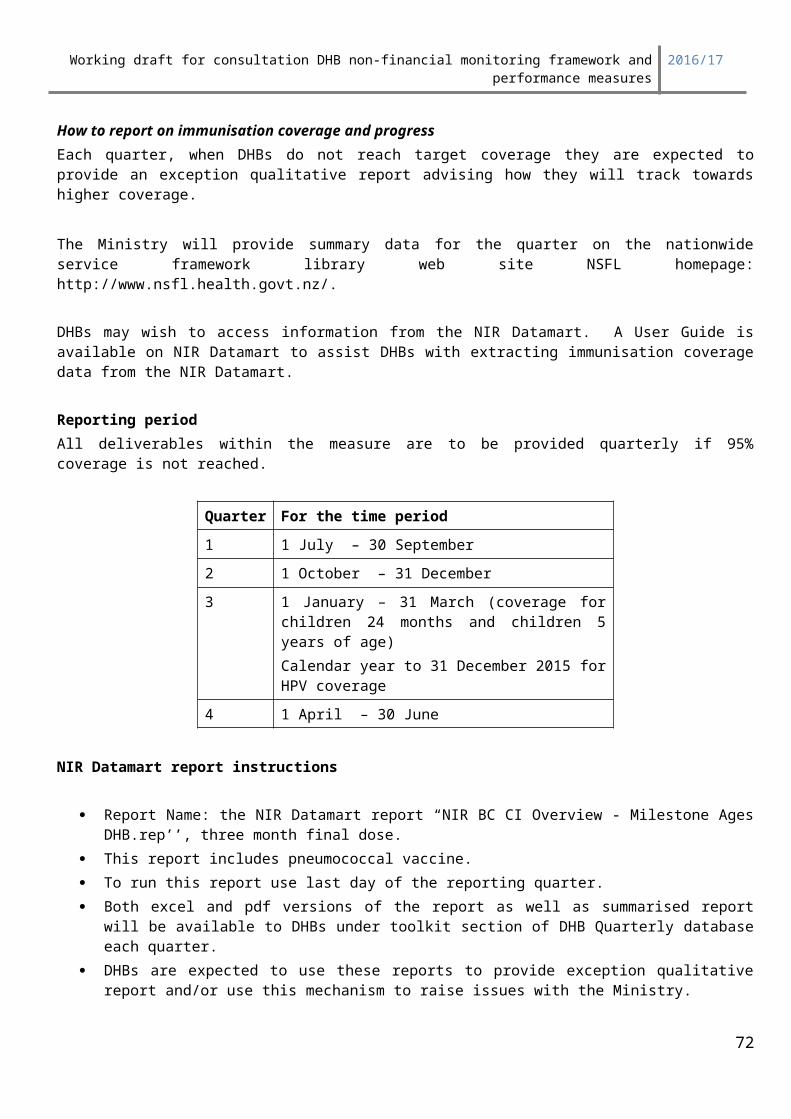
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
The cross-agency Children’s Action Plan (CAP), is a key priority for the Government. The CAP sets out what will be done (over the next five years) to protect vulnerable children who are at greatest risk of maltreatment. The CAP supports the Prime Minister’s Better Public Services Key Result Area for Supporting Vulnerable Children, particularly the result area of reducing child assaults by 5 percent by 2017. DHBs have an important role in supporting the implementation of the CAP and BPS. The Ministry will continue to update guidance as the CAP implementation programme develops and key decisions are taken by Ministers. The White Paper (Volumes 1 & 2) and additional information about CAP can be accessed at www.childrensactionplan.govt.nz
DHBs, through delivering on the CAP, particularly through the support they provide to Children’s Teams, and other health sector initiatives that support the prevention and early identification of child maltreatment (such as VIP programmes, health professional training and implementation of the National Child Protection Alerts System and Shaken Baby Prevention programmes), will contribute to better coordinated services and improved outcomes for vulnerable children and their families/whanau. To support the implementation of the CAP, Cabinet has established: a Ministerial Oversight Group (chaired by the Minister for Social Development and comprising the Ministers of Health, Justice, Education, Police, Ora and Finance); a Vulnerable Children’s Board (chaired by the Chief Executive of the Ministry of Social Development and comprising the Chief Executives from the Ministries of Health, Education, Social Development, Justice,
72
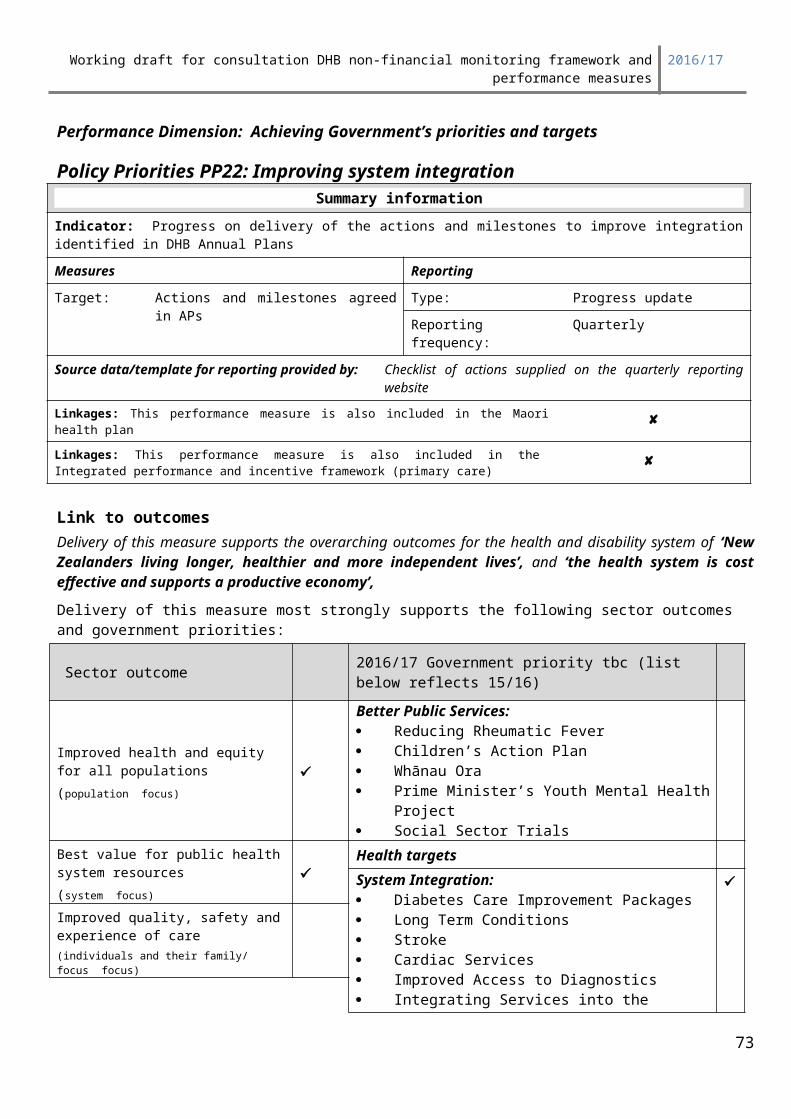
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Business, Innovation and Employment (Housing), and Te Puni Kōkiri), a National Children’s Action Plan Director and Children’s Team Directors . The Vulnerable Children’s Board reports regularly to the Ministerial Oversight Group and is jointly accountable for achieving results for vulnerable children. DHBs will be accountable to the Minister of Health for their contribution to supporting the implementation of the CAP.
Deliverables definitionsEach quarter the Ministry will present checklists aligned with the guidance provided in this toolkit that summarises the actions and milestones that support delivery of the CAP agreed in Annual Plans on the quarterly reporting web site. DHBs are required to provide a quarterly update identifying progress made during the quarter against the actions and milestones (deliverables) in each checklist. The progress update must include:
Whether the DHB is on track meeting each deliverable, including comment on specific actions delivered in the quarter
Where deliverables are not on track the report must include mitigation strategies and new timeframes for delivery
Where quantitative measures are reported – Reports must include baseline, target and quarterly performance progress
ExpectationsThe assessment requirements for each quarter are set out below:
Table 1: Quarterly assessmentRating Explanation
Achieved All actions, milestones and measures are on track.
Partially Achieved Some actions, milestones and measures are not on track but adequate mitigation strategies are presented.
Not Achieved Some actions, milestones and measures are not on track and adequate mitigation strategies are not presented.
Reporting periodQuarter For the time period1 1 July – 30 September
2 1 October – 31 December
3 1 January – 31 March
4 1 April 13 – 30 June
73
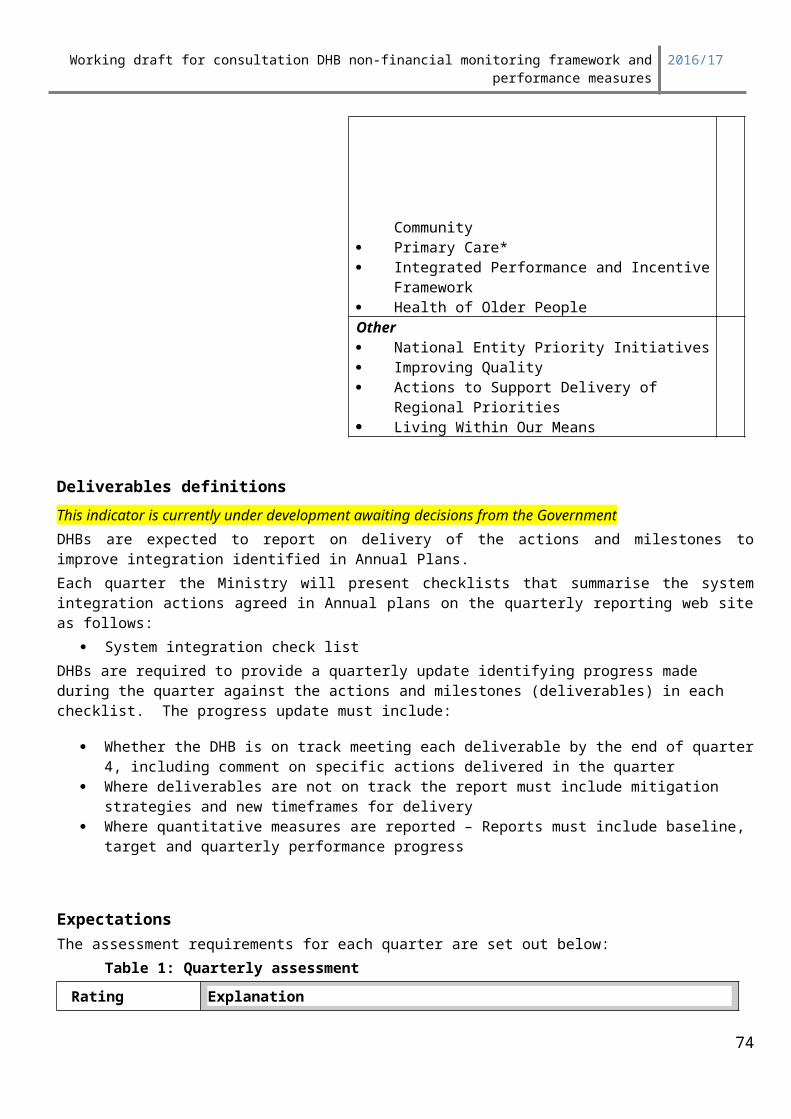
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: ‘Achieving Government’s priorities and targets’
Policy Priorities PP28: Reducing Rheumatic feverSummary information
Progress against the DHBs’ rheumatic fever prevention plan, report on root cause analysis and delivery of agreed acute rheumatic fever hospitalisation rates
Target/performance expectation Reporting
Agreed in Annual Plan Type: progress update and exception report
Reporting frequency: quarterly
Source information for reporting provided by: Ministry sourced from NMDS
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care) x
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
74
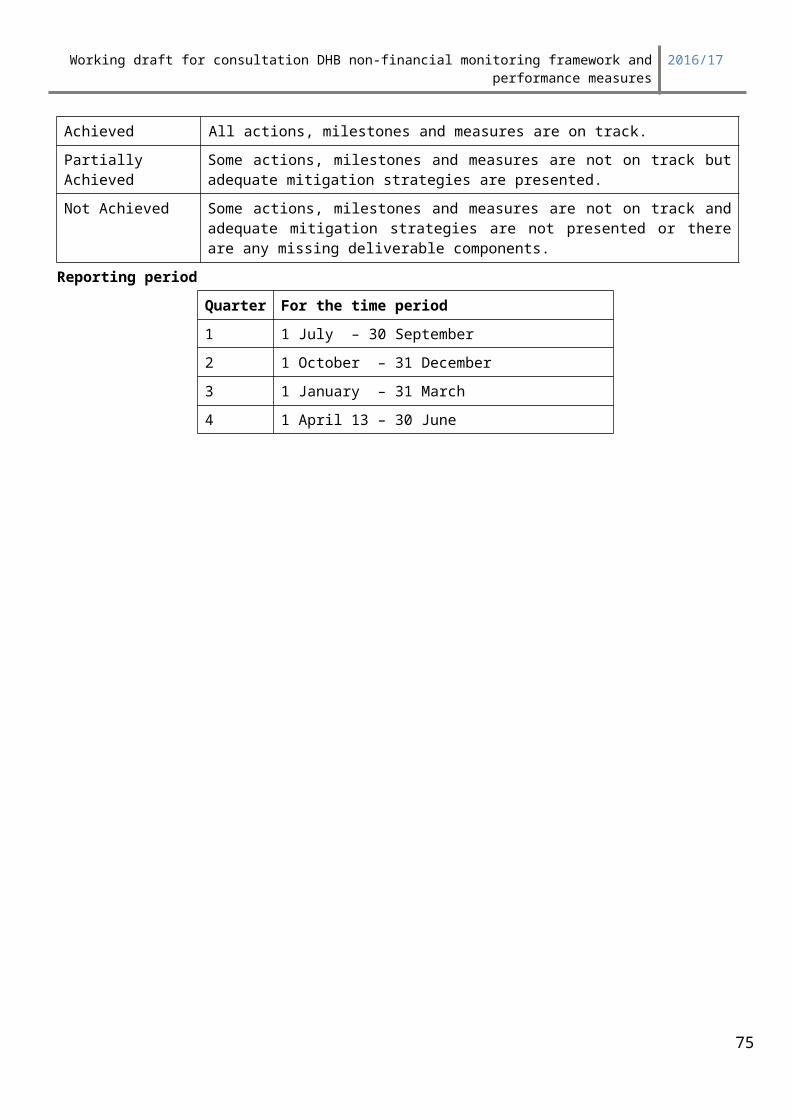
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
In June 2012, Cabinet agreed targets for the Better Public Services (BPS) key result areas. For rheumatic fever, the target is to reduce the incidence of rheumatic fever by two thirds to 1.4 cases per 100,000 people by June 2017. This is considered to be a stretch target that will be challenging to achieve. Rheumatic fever primarily affects school and intermediate-aged children and generally follows a Group A streptococcal throat infection. It is a preventable disease and can have serious consequences, such as the development of rheumatic heart disease. Rheumatic fever is unevenly distributed in New Zealand – it occurs mainly in the North Island, is strongly correlated with poor socio-economic status, and disproportionately affects Māori and Pacific people.
Actions and activities that have a proven impact on this measure:In order to achieve the overall reduction in rheumatic fever, DHB target numbers and rates have been set for each financial year to 2016/17. The target numbers and rates for 2013/14 and 2014/15 are shown in Table 1. The actions DHBs can take to improve performance are included in each DHB’s rheumatic fever prevention plan.The DHB rheumatic fever prevention plans identify the DHB’s approach and commitment to delivering a range of actions which will contribute to achieving their rheumatic fever target. The plans cover the period from 20 October 2013 to 30 June 2017.
Table 1: Acute rheumatic fever initial hospitalisation target rates and numbers per year by District Health Board (per 100,000 total population), 2011/12 and 2015/16
District Health Board
Rates Numbers
2009/10–2011/12
Baseline rate
(3-year average rate)
2013/14
Target:
10% reduction from baseline level
2014/15
Target:
40% reduction from baseline level
2015/16
Target:
55% reduction from baseline level
2009/10–2011/12
Baseline numbers
(3-year average rate)
2013/14
Target:
10% reduction from baseline level
2014/15
Target:
40% reduction from baseline level
2015/16
Target:
55% reduction from baseline level
Northland 10.5 9.5 6.3 4.7 17 15 10 8
Waitemata 2.3 2.0 1.4 1.0 12 11 8 6
Auckland 3.2 2.9 1.9 1.4 15 14 9 7
Counties Manukau 13.2 11.9 7.9 5.9 66 62 42 32
Northern region 6.6 5.9 4.0 3.0 110 102 69 52
Waikato 3.5 3.2 2.1 1.6 13 12 8 6
Lakes 7.8 7.0 4.7 3.5 8 7 5 4
75
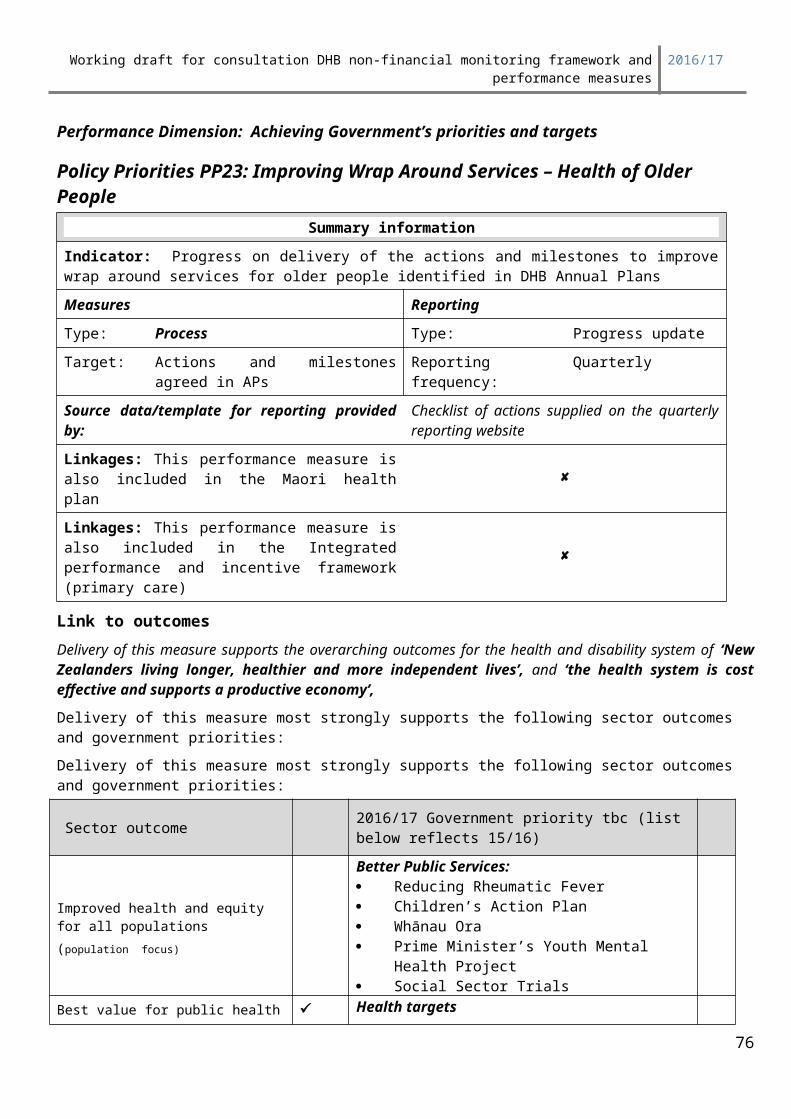
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Bay of Plenty 3.8 3.4 2.3 1.7 8 7 5 4
Tairawhiti 9.3 8.4 5.6 4.2 4 4 3 2
Taranaki 0.9 0.8 0.5 0.4 1 1 1 0
Midland region 4.1 3.7 2.5 1.8 34 31 21 16
Hawkes Bay 4.3 3.9 2.6 1.9 7 6 4 3
MidCentral 1.6 1.4 0.9 1.0 3 2 2 2
Whanganui 3.2 2.9 1.9 1.4 2 2 1 1
Capital and Coast 2.9 2.6 1.8 1.3 9 8 5 4
Hutt 4.9 4.4 2.9 2.2 7 6 4 3
Wairarapa 0.0 0.0 0.0 0.0 0 0 0 0
Central region 3.2 2.9 1.9 1.5 28 25 17 13
Southern region 0.4 0.4 0.3 0.2 5 4 3 2
New Zealand 4.0 3.6 2.4 1.8 177 162 109 83
The 2017 Better Public Service target for each DHB is included in the following table.DHB 2017 Better Public Service
target (rate per 100,000 total population)
Northland 3.5Waitemata 0.7Auckland 1.1Counties Manukau 4.5Waikato 1.2Lakes 2.6Bay of Plenty 1.3Tairawhiti 2.8Taranaki 0.3Hawke’s Bay 1.5MidCentral 0.6Whanganui 1.1Capital &Coast 1.0Hutt Valley 1.6Wairarapa 0.0Southern region 0.2New Zealand 1.4
Deliverables definitions Focus area 1 Reducing the Incidence of First Episode Rheumatic FeverPart 1: 1. Progress against target - 2015/16 target is 55% reduction from baseline (2009/10-2011/12)
2. Progress report for rheumatic fever prevention plan
76
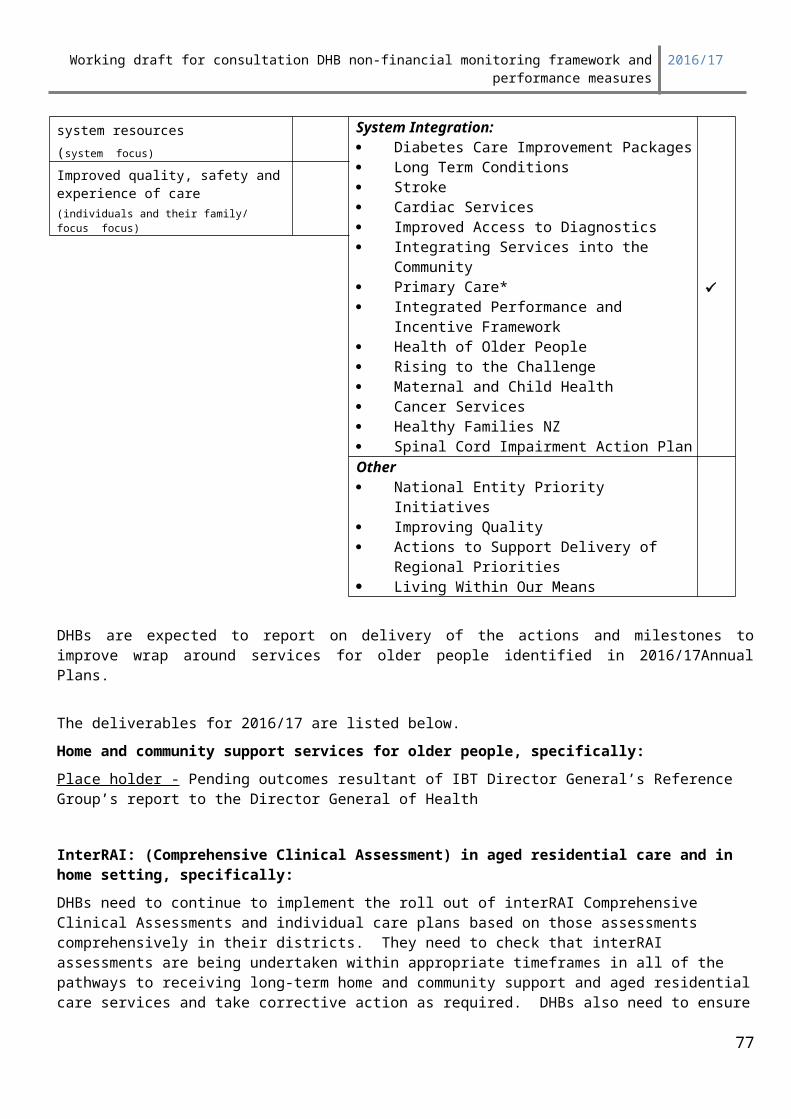
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Each DHB with a high incidence of rheumatic fever (as defined in the guidance document for the rheumatic fever prevention plan issued in July 2013) must provide a progress report against the DHB’s rheumatic fever prevention plan. A template has been supplied by the Ministry in rheumatic fever prevention plan guidance documents.
DHBs with a lower incidence of rheumatic fever are not required to report against their Rheumatic Fever Prevention Plan. The Ministry of Health will monitor the rheumatic fever hospitalisation rates in these DHBs through their general monitoring processes. If a DHB has a significant increase in rheumatic fever numbers or rates, they will be required to submit a more detailed action plan and will be required to report against progress.
3. Provide a report on the lessons learned and actions taken following reviews each quarter. A reporting template has been provided by the Ministry.
Part 2: Exception report
Hospitalisation rates per 100,000 DHB total population for acute rheumatic fever are above the target for the financial year.
Expectation and Deliverable:
Those DHBs with an acute rheumatic fever hospitalisation rate above the agreed target and outside a 95% confidence interval of agreed target are required to provide an exception report outlining the resolution plan the DHB has in place.
Data on acute rheumatic fever hospitalisation rates will be supplied by the Ministry.
Reporting Period Reporting required: Progress reports are required quarterly. Due to the reliance on NMDS data (where the deadline for submission is about one month after the end of the quarter), the data used to derive the hospitalisation measure will be for one quarter in arrears.
ExpectationsThe following achievement scale will be applied:
Rating: DefinitionAchieved Agreed target met or hospitalisation rate below target.
An achieved rating is applied when the DHB has met the target agreed in its Annual Plan and has achieved significant progress for the Māori population group, and the Pacific population group. As 90% of hospitalisation for rheumatic fever are among Māori and Pacific populations, 'significant progress' for Māori and Pacific populations is defined as the DHB meeting the DHB target agreed in its Annual Plan.
Partially Achieved
DHB hospitalisation rate above agreed target (including not making agreed progress for Maori and Pacific population groups), and within a 95% confidence interval of agreed target.As 90% of hospitalisations for rheumatic fever are among Māori and Pacific populations, this rating is applied if the resolution plan supplied by the DHB includes actions specifically focused on improving results for the Maori and Pacific populations.
Not Achieved
DHB hospitalisation rate above agreed target and outside a 95% confidence interval of agreed target
77
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Focus area 2: Facilitating the Effective Follow-up of Identified Rheumatic Fever Cases
Deliverable
DHBs are expected to provide confirmation and exception reports on progress in following -up known risk factors and system failure points in cases of recurrent rheumatic fever.
ExpectationsRating Explanation
Achieved All actions, milestones and measures are on track.
Partially Achieved Some actions, milestones and measures are not on track but adequate mitigation strategies are presented.
Not Achieved Some actions, milestones and measures are not on track and adequate mitigation strategies are not presented.
Reporting periodQuarter For the time period1 1 July – 30 September
2 1 October – 31 December
3 1 January – 31 March
4 1 April 13 – 30 June
.
78
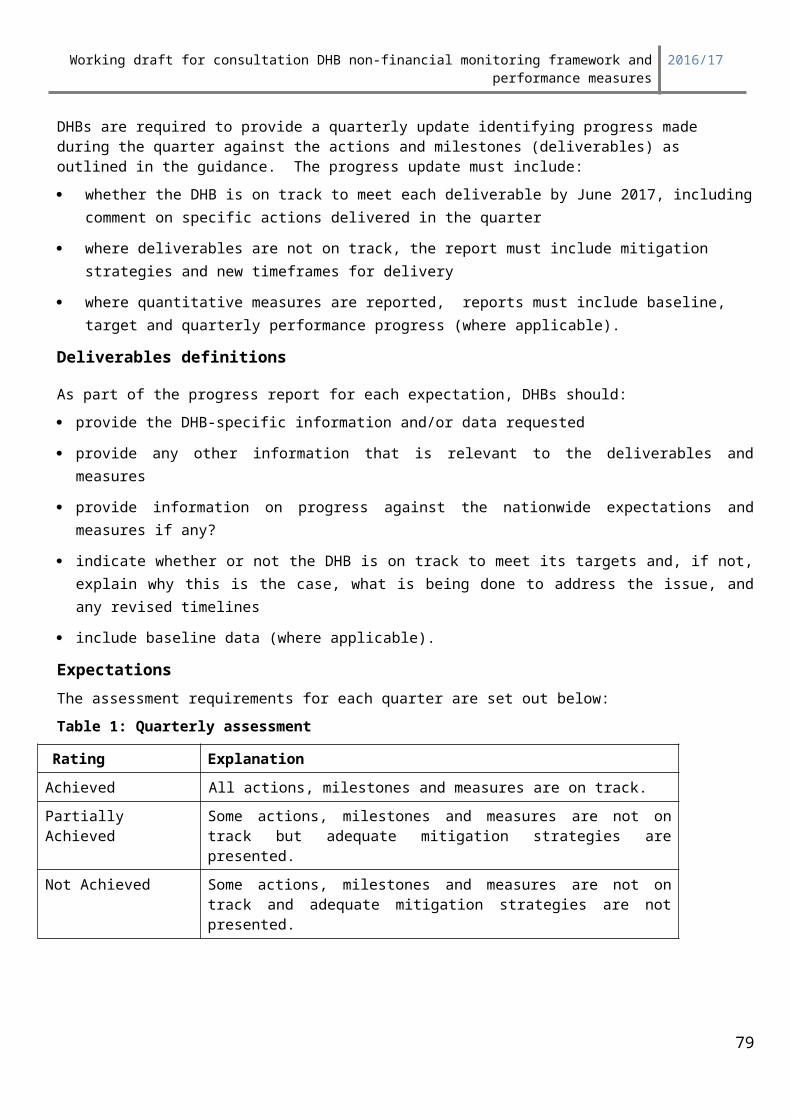
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP29: Improving waiting times for diagnostic servicesSummary information
Measures Reporting
Target: Agreed targetType: Variation from expectation
Reporting frequency: Monthly
Source data/template for reporting provided by:
Coronary Angiography – data to be supplied by DHBs to the National Booking Reporting System (NBRS) in accordance with national collection reporting rules
Colonoscopy – data to be supplied by DHBs either to the NBRS, or via a generic template
Computed Tomography and Magnetic Resonance Imaging - each DHB is to provide monthly data on a generic template. Templates will be due 20 days after the end of the calendar month – a copy of the templates is attached
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomes Delivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework
Improved quality, safety and experience of care(individuals and their family/ focus focus)
79
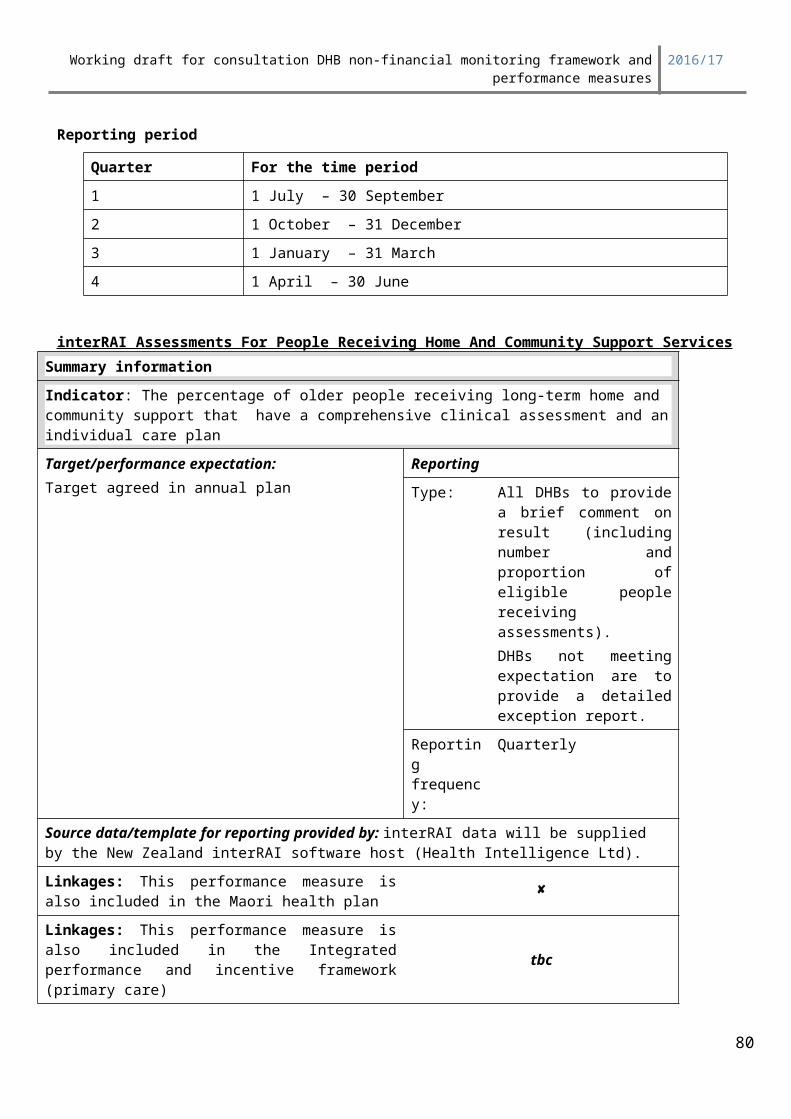
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Health of Older People Rising to the Challenge Maternal and Child HealthOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Diagnostics are a vital step in the pathway to access appropriate treatment. Improving waiting times for diagnostics can reduce delays to a patient’s episode of care and improve DHB demand and capacity management.
Improving access to diagnostics will improve patient outcomes in a range of areas: Cancer pathways will be shortened with better access to a range of diagnostic modalities Emergency Department (ED) waiting times can be improved if patients have more timely access to
diagnostics Access to elective services will improve, both in relation to treatment decision-making, and also
improved use of hospital beds and resources Workforce opportunities can be explored to consider alternative and more efficient ways of providing
diagnostics
These efforts will help to promote and protect good health and independence, and contribute to the high level outcome of New Zealanders living longer, healthier and more independent lives.
A multi-year programme commenced in 2012/13 and involves a staged approach being taken to improving waiting times for diagnostics (from receipt of referral to provision of diagnostic service).
Link to priority areas of focusDelivery of this measure will support Better Sooner More Convenient Health Services for New Zealanders by ensuring people are provided more timely access to diagnostic services. Increasing delivery will improve access and reduce waiting times will increase public confidence that the health system will meet their needs.
Delivery of this measure will also support the 2016/17 key (strategic) planning approaches of regional collaboration and governance, and integration by encouraging DHBs to adopt a regional view of diagnostic service delivery. This requires improved integration across all clinical services, and patient pathways.
Deliverables definitionsDescription:For 2016/17 the programme will involve deliverables in the following four modalities:
Coronary angiography Colonoscopy Magnetic Resonance Imaging (MRI)
80
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Computed Tomography (CT)
These procedures were identified because they are aligned with other health sector priorities, and because national or regional representative groups are established. The Ministry of Health has worked with clinical networks to establish nationally agreed expectations regarding what appropriate timeframes should be for these diagnostic modalities.
Refer to the Improving Waiting Times for Diagnostic Services Indicator Templates for more information on the deliverables, definitions and expectations.
Reporting Period Reporting required: Monthly reporting from as follows:
Elective coronary angiogram to be reported to the National Booking Reporting System (NBRS) in accordance with NBRS data dictionary reporting requirements.
CT, MRI and colonoscopy reporting templates to be submitted to the National Health Board within 20 days of the end of the previous month. The reporting template is emailed out by National Collections.
Performance monitoring against this measure will be undertaken quarterly via the non-financial performance monitoring framework as follows:
Quarter ResultsQuarter 1 September 2015 results
Quarter 2 December 2015 results
Quarter 3 March 2016 results
Quarter 4 June 2016 results
Expectations DHBs are required to collect, measure and monitor how long people are waiting for identified diagnostic procedures. Incremental improvements are required each year. Expectations for 2016/17 are:
1. Coronary angiography – 95% of accepted referrals for elective coronary angiography will receive their procedure within 3 months (90 days)
2. CT and MRI – 95% of accepted referrals for CT scans, and tbc% of accepted referrals for MRI scans will receive their scan within 6 weeks (42 days)
3. Diagnostic colonoscopy – a. 75% of people accepted for an urgent diagnostic colonoscopy will receive their procedure
within two weeks (14 calendar days, inclusive), 100% within 30 daysb. 65% of people accepted for a non urgent diagnostic colonoscopy will receive their procedure
within six weeks (42 days), 100% within 120 daysSurveillance colonoscopy
c. 65% of people waiting for a surveillance colonoscopy will wait no longer than twelve weeks (84 days) beyond the planned date, 100% within 120 days
81
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Ratings for PP29: Improving waiting times for diagnostic servicesSeparate performance rating will be applied for each of the three expectation areas within this performance measure:
1. Coronary angiography (one indicator)2. Radiology (CT & MRI indicators)3. Colonoscopy (three indicators)
The following achievement scale will be applied for each of the three areas
Rating:Achieved The DHB has achieved all the waiting time indicator or indicators for the
respective diagnostic area
Partial Achievement The DHB has either:- achieved some, but not all, of the waiting time indicators for the
respective diagnostic area (for example, achieved the CT indicator but not the MRI indicator), and has provided a report that includes planned actions to lift performance; or
- achieved none of the indicators for the respective diagnostic areas, but shows improvement over the previous quarter, and has provided an adequate work-out plan to reach the target by year-end.
Not Achieved The DHB has not achieved the waiting time indicators for the respective diagnostic area, and has not demonstrated an adequate work-out plan to reach the target by year-end.
82
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targetsPolicy Priorities PP30: Faster cancer treatmentPart A: Faster cancer treatment – 31 day indicator
Link to outcomes Delivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Faster cancer treatment takes a pathway approach to care, to facilitate improved hospital productivity by ensuring resources are used effectively and efficiently. DHBs working towards achievement of Faster cancer treatment supports public trust in the health and disability system; and that these services can be used with confidence. Implementation of Faster cancer treatment requires existing capacity and resources to be maximised, this results in effective and efficient use of resources and supports the key planning consideration of value for money.
83
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Implementing the overall faster cancer treatment programme supports the overarching goal of Better, Sooner, More Convenient Health Services for New Zealanders. Cancer treatment is provided across all DHBs, although not all DHBs provide all services. This requires DHBs to collaborate across boundaries to ensure services are integrated and patients receive a seamless service.
Actions to deliver improved performance in this focus area include: use of the Faster Cancer Treatment Indicators: Business Rules and Data Definitions (version 3.1,
March 2014) and High suspicion of cancer definitions (September 2015) to ensure consistency of reporting
improve the quality of data (volume of patients, number of tumour types, types of first treatment) captured
analysis of the data to identify areas for system and process improve along the patient pathway and any differences in access or timeliness by ethnicity or geography.
review and re-design of the coordination of treatment processes and booking processes to ensure optimal use of capacity.
DeliverablesDHBs will be required to supply data monthly (within 20 days of the end of the month) via secure file transfer protocol on the length of time taken for patients to receive their first cancer treatment (or other management) from date of decision-to-treat.
The Faster cancer treatment 31 day indicator includes all patients who receive a publicly-funded first cancer treatment, irrespective of how they were initially referred.
Detailed information on the definitions, inclusions and process for submitting data to the Ministry of Health is outlined in Faster Cancer Treatment Indicators: Business Rules and Data Definitions (version 3.1, March 2014) available from: http://nsfl.health.govt.nz/accountability/performance-and-monitoring/business-rules-and-templates-reporting/faster-cancer.
The DHB of domicile is responsible for collecting and reporting information on their domiciled population even if it is not the DHB of:
receipt of referral service.
No further quantitative reporting is required as part of the quarterly reporting process.
DHBs are required to submit a quarterly qualitative report through the quarterly reporting database outlining:
the activities being undertaken to ensure data quality and volumes delays identified along the cancer pathway and challenges with implementing Faster cancer
treatment actions taken and planned in response to the delays and challenges identified.
Reporting period
84
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
DHB achievement of the Faster cancer treatment 31 day indicator will be calculated based on six months rolling data as outlined in the table below:
Reporting quarter Achievement based on patients receiving their first cancer treatment between:
Quarter 1 1 April – 30 September
Quarter 2 1 July – 31 December
Quarter 3 1 October - 31 March
Quarter 4 1 January – 30 June
ExpectationsThe following achievement scale, which is aligned to the achievement scale for the Faster cancer treatment health target, will be applied:
Rating:
Achieved will apply where at least 85 percent of patients receive their first cancer treatment (or other management) within 31 days from data of decision-to-treat.
Partially Achieved will apply where less than 85 percent of patients receive their first cancer treatment (or other management) within 31 days from data of decision-to-treat, but the narrative comment satisfies the assessor that the DHB has a plan to improve achievement.
Not Achieved will apply where less than 85 percent of patients receive their first cancer treatment (or other management) within 31 days from data of decision-to-treat and the narrative comment does not satisfy the assessor that the DHB has a plan to improve achievement.
85

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Part B: Shorter waits for cancer treatment – radiotherapy and chemotherapy
Link to outcomes Delivery against this measure supports the health and disability system outcome of ‘New Zealanders living longer, healthier and more independent lives’, and the intermediate outcome of ‘the health and disability system and services are trusted and can be used with confidence’.
Continued performance of the DHB against this measure, ensuring the timely access to cancer treatment for everyone needing it, will support public trust in the health and disability system; and that these services can be used with confidence. Through the intermediate outcomes the measure contributes to the high level outcome of New Zealanders living longer, healthier and more independent lives.
Radiotherapy treatment is provided in the six cancer centre DHBs requiring DHBs to collaborate across boundaries to support continued achievement of this measure for the DHB’s domicile population. Chemotherapy treatment is provided in almost all DHBs and requires collaboration across boundaries to ensure services are integrated and patients receive a seamless service.
Achievement of this measure requires existing capacity and resources to be maximised, this results in effective and efficient use of resources and supports the key planning consideration of value for money.
Actions to deliver improved performance in radiotherapy include: use information systems that provide information on prospective demand management allowing
flexibility in management of workflow and scheduling undertake lean-thinking reviews to identify areas where the workflow can be streamlined from First
Specialist Assessment (FSA) to start of treatment to ensure patients start treatment within four weeks
undertake regular process reviews to identify system bottlenecks and ensure processes can be put in place to minimise the bottlenecks and / or impact of bottlenecks on target achievement
continue to upgrade and replace capital in timely manner to ensure appropriate capacity is maintained
improve training and education opportunities to improve the skill mix of key workforce include radiation therapists, medical physicists and radiation oncologists
implement strategies to support recruitment and retention of key workforce.
Actions to deliver improved performance in chemotherapy include: use information systems that provide information on prospective demand management allowing
flexibility in management of workflow and scheduling undertake lean-thinking reviews to identify areas where the workflow can be streamlined from FSA
to start of treatment to ensure patients start treatment within four weeks undertake regular process reviews to identify system bottlenecks and ensure processes can be put
in place to minimise the bottlenecks and / or impact of bottlenecks on target achievement implement strategies to support recruitment and retention of medical oncology and haematology
workforce.
86
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
87
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
DeliverablesAll patients ready-for-treatment, wait less than four weeks for radiotherapy or chemotherapy from decision to treat.
Radiotherapy – DHB of service (Cancer Centre DHB) reports all patients by DHB of domicileCompleted monthly templates that measure the interval between the decision-to-treat and the patient beginning radiation treatment along with other related measures, are supplied on time and complete from the DHB of service (Cancer Centre DHB) as detailed in the reporting template located on the nationwide service framework library web site NSFL homepage: http://www.nsfl.health.govt.nz/. Patients are identified by DHB of domicile.
Chemotherapy – DHB of service reports all patients by DHB of domicileCompleted monthly templates that measure the interval between the decision-to-treat and the patient beginning chemotherapy treatment along with other related measures, are supplied on time and complete from all DHBs where chemotherapy treatment has commenced (DHB of service) as detailed in the reporting template located on the nationwide service framework library web site NSFL homepage: http://www.nsfl.health.govt.nz/. Patients are identified by DHB of domicile.
All DHBs – confirmation and exception reports Provide a report confirming the DHB has reviewed the monthly wait time templates produced by the DHB of service or its own DHB where treatment commenced at that DHB for the quarter.
Where the monthly wait time data identifies: any patients domiciled in the DHB waiting more than four weeks, due to capacity issues, and/or wait time standards were not met.
DHB of domicile must understand and report the resolution path being taken by the DHB of service where it does not provide radiotherapy or chemotherapy itself.
Interpretation issuesWhere there are clearly identified reasons for delays that meet the defined delay code criteria, other than service capacity issues, the target will be treated as met.
Reporting Period Monthly supply of templates (within two weeks of the end of the month) and quarterly supply of confirmation and exception reports, as per the following table:
Quarter For the time periodQuarter 1 1 July – 30 September
Quarter 2 1 October – 31 December
Quarter 3 1 January – 31 March
Quarter 4 1 April – 30 June
88
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
ExpectationsThe following achievement scale will be applied: Rating:
Achieved will apply, for all of the three months under review, where all patients ready-for-treatment receive treatment within four weeks from decision-to-treat (excluding delays that meet the defined delay code criteria).
Partially Achieved will apply, for two of the three months under review, where all patients ready-for-treatment receive treatment within four weeks from decision-to-treat (excluding delays that meet the defined delay code criteria).
Not Achieved will apply, for one month or more in the period under review, where some patients ready-for-treatment did not receive treatment within four weeks from decision-to-treat (excluding delays that meet the defined delay code criteria).
Note: Calculation of target achievement excludes Category D radiation patients.
89
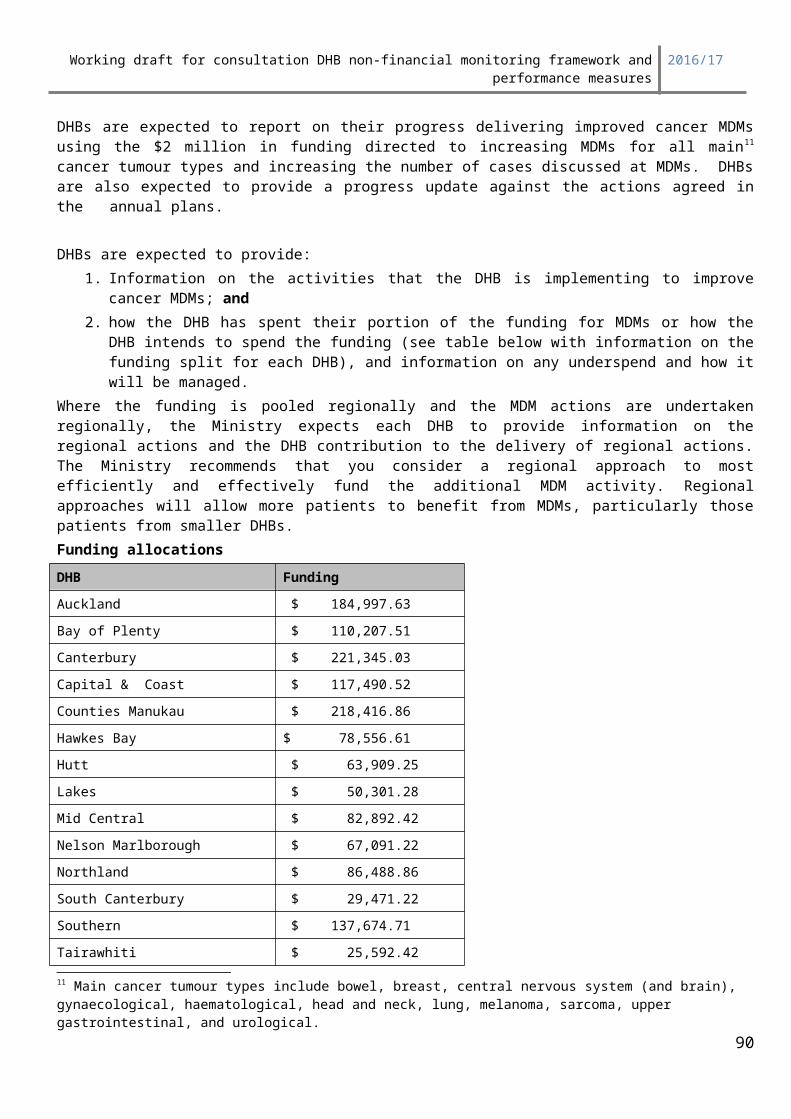
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Achieving Government’s priorities and targets
Policy Priorities PP31: Better help for smokers to quit in public hospitals (previous health target)
Summary information 95 percent of hospital patients who smoke and are seen by a health practitioner in a public hospital
are offered brief advice and support to quit smoking
Measures ReportingTarget: Target agreed in
Annual PlansType: Data & report
Reporting frequency: Quarterly
Source data/template for reporting provided by:
Hospital target data – supplied by DHBsAll reporting templates will be supplied by the Ministry.
Link to outcomes Delivery against this measure supports the health and disability system outcome of ‘New Zealanders living longer, healthier and more independent lives’, as well as the intermediate outcome of ‘a more unified and improved health and disability system’. The measure also supports the Government’s aspirational goal of a Smokefree New Zealand by 2025. Achieving a Smokefree New Zealand will mean that: our children and grandchildren will be free from exposure to tobacco and tobacco use the prevalence of smoking across all populations will be less than 5 percent tobacco will be difficult to sell and supply.
At present, tobacco smoking places a significant burden on the health of New Zealander’s and on the New Zealand health system. Tobacco smoking is related to a number of life-threatening diseases, including cardiovascular disease, chronic obstructive pulmonary disease and lung cancer. It also increases pregnant smokers’ risk of miscarriage, premature birth and low birth weight, as well as their children’s risk of Asthma and Sudden Unexplained Death in Infants (SUDI).
Stopping smoking confers immediate health benefits on all people, and is the only way to reduce smokers’ risk of developing a smoking-related disease. Providing smokers with brief advice to quit increases their chances of making a quit attempt. The chance of that quit attempt being successful is increased if medication and/or cessation support are also provided. Most medications roughly double a smoker’s chance of quitting, but using medication in conjunction with a cessation support service (such as the Quitline or an Aukati KaiPaipa service) can increase a smoker’s chance of quitting by as much as four times.
By ensuring that all health professionals are routinely providing their patients with advice and support to quit, DHBs are helping to ensure that people receive better health and disability services, and live longer and healthier lives.
The following actions and activities are examples of initiatives that have had an impact on this measure: Mechanisms for capturing data are accessible and easy to use. Methods for referring patients to cessation support services are simple and succinct. Services are able to monitor their progress towards the target on a regular basis.
90
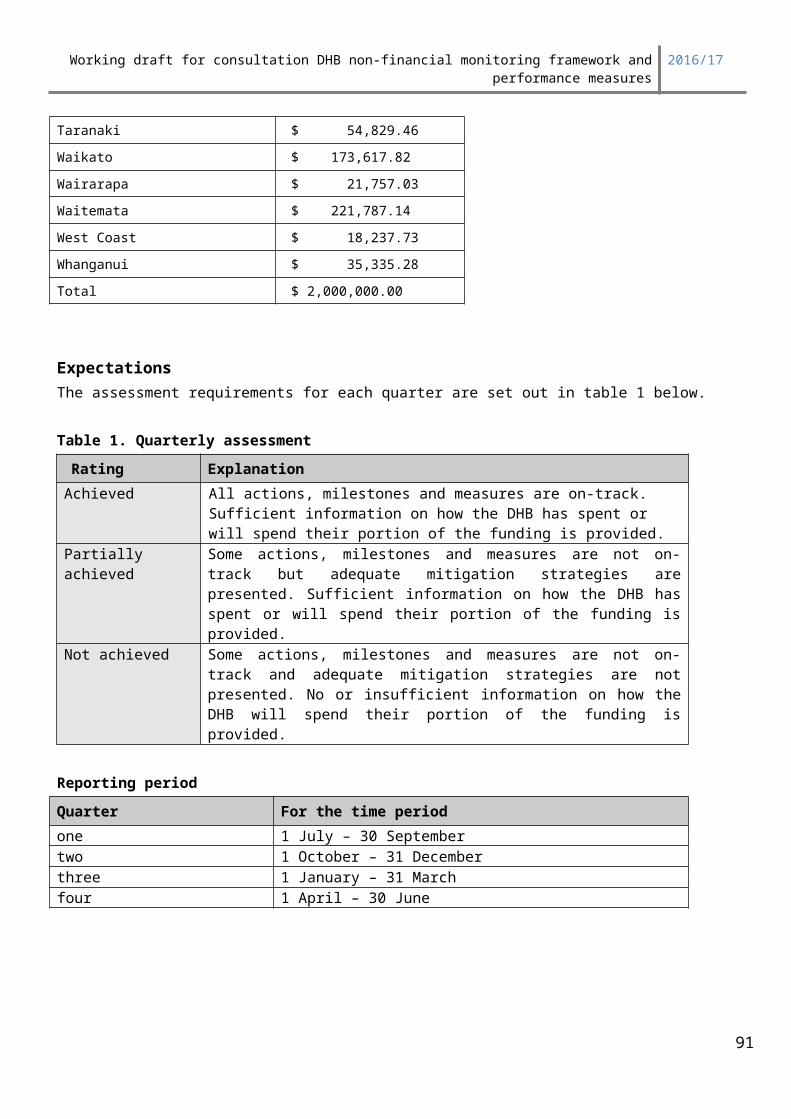
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Smokefree champions are in place within each ward, practice or service to provide motivation, education and support for the target.
DeliverablesEach quarter, DHBs will be required to complete the template supplied by the Ministry (numerical and narrative sections must be completed). Local patient management systems will be used to capture the necessary data using the relevant ICD-10-AM codes (see table 1).
Table 1: Smoking related ICD-10-AM codes
Measurement of Target
ICD Code ICD Definition
Hospitalised smokers
F17.1 Mental and behavioural disorders due to use of tobacco, harmful use is assigned when a clearly documented relationship exists between a particular condition and smoking.
F17.2 Mental and behavioural disorders due to use of tobacco, dependence syndrome is assigned only when a formal diagnosis of ‘tobacco dependence syndrome’ has been made.
Z72.0 Tobacco use, current is assigned if the patient has smoked tobacco within the last month and when there is insufficient documentation available to qualify the assignment of either F17.1 or F17.2.
Advice and support
Z71.6 Counselling for tobacco use disorder is assigned in addition to a tobacco status code when a health care worker has provided either advice to quit smoking and/or cessation therapy while the patient is in hospital.- For completeness if Z71.6 coding exists in the absence of a code for
hospitalised smoker, then apply code Z72.0.
Those DHBs that do not meet the 95 percent target for the quarter must provide the Ministry with an action plan detailing how they will improve their result, and must begin reporting their results to the Ministry monthly.
Eligible populationsAll adults who are: aged 15 years and over admitted to hospital either acutely or for elective procedures admitted as an inpatient; and identified as a current tobacco smoker at the time of admission (a current tobacco smoker is someone
who has smoked within the last four weeks).
Explanation of termsFor the purpose of the hospital target a current smoker is someone who has smoked at all within the last four weeks. A facility is a place which may be a permanent, temporary or mobile structure, which health care users attend or are resident in, for the primary purpose of receiving health care or disability support services. This definition excludes supervised hostels, halfway houses, staff residences and rest homes where the rest home is the patient’s usual place of residence.For the purposes of data collection for the hospital target, private hospitals are excluded. Therefore, the facility type includes, but is not limited to, public hospitals, psychiatric hospitals and drug and alcohol treatment facilities.
91
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Reporting periodQuarterly reports must be submitted to the Ministry by the 20th of the month following the relevant quarter.
Expectations All DHBs are expected to maintain performance of 95 percent for the hospital target. The achievement scale below will be applied to each of the target areas individually every quarter.
achievement Scale
Rating Definition
Achieved* The DHB has met the percentage target for the quarter (ie, 95 percent for the hospital target and 90 percent for the primary care target).
Partial Achievement The DHB has not met the percentage target, but has improved on its result from the previous quarter.
Not Achieved The DHB has not met the percentage target, and its result has dropped since the previous quarter.
*From 2014/15 for all performance measures included in the Maori health plan this rating is applied when the DHB has met the target agreed in its Annual Plan and has achieved significant progress for the Maori population group, and the Pacific population group.
92
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Meeting service coverage requirements and Supporting sector inter-connectedness
System Integration SI1: Ambulatory sensitive (avoidable) hospital admissions
The Ministry is presently undertaking a review of the way in which we define and utilise ASH data to ensure that it is a meaningful measure which can drive improved system performance.
ASH data has been collected and reported in New Zealand since 2001. ASH conditions are a subset of all health conditions that are believed to be relatively amenable to out-of-hospital management, and ASH rates are undoubtedly impacted by the quality of primary care services, but also by high quality population health care, and the interfaces between population health, primary/community care, and secondary/hospital care.
Systems of in-hospital care and hospital coding practices can have significant impact on ASH rates, and whilst there have been minor changes to the way in which the Ministry define ASH over the years, it is timely to review the way in which we define and use ASH. In particular it is important to consider the impact of these system changes on the value of ASH as an indicator of quality, as well as how we might differently use the information to drive improved health system performance.
A revised measure is close to finalisation and is expected to be available shortly.
Summary informationTarget/performance expectation Reporting
Type: Exception report
Target: Target agreed in Annual Plan Reporting frequency: Six monthly
Source data/template for reporting provided by: Data supplied by Ministry (NMDS)
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
or unknown at present
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
93
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Link to outcomesReducing ambulatory sensitive hospital admissions (ASH) will show that the DHB has addressed the Ministerial priorities of, timely patient care closer to home and value for money by ensuring that patients who need services that can be provided in community settings receive them there rather than at hospitals. This will free up hospital staff and resources for more acute and urgent cases while also ensuring the services being funded in the community, including primary care, are being used optimally.
Alliance Leadership Teams, through their “whole of system” approach that focusses on the patient journey, or care pathway, provide a valuable forum for identifying opportunities to reduce local ASH rates.
The Māori and Pacific Health Plans will show how the DHB intends to reduce ASH rates for Māori and Pacific populations to that of the total population.
Link to priority areas of focusDelivery of this measure will support Government priorities, including improved integration and regionalization and will also help to reduce the fragmentation of services. Activities that reduce ASH will
94
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
also contribute to a reduction in the total number of unplanned hospital admissions, a substantial proportion of which are ambulatory sensitive.
Actions and activities that have a proven impact on this measure:These actions are best identified through a “whole of system” approach that engages primary and secondary clinicians, as well as managers from both sectors, within an alliancing framework. There are a range of initiatives that have a proven impact on this measure, they include:
1. Comprehensive disease management programmes which are patient-focused and involve multidisciplinary teams.
2. Education and self-management programmes especially when associated with disease management programmes.
3. Disease prevention programmes especially when linked to risk management for vulnerable groups.4. System level changes such as programmes to increase access to health services for specific
population groups.A Systematic Review that identified the effective interventions for reducing these admissions was published in 2008 by the Health Services Assessment Collaboration.12
Deliverables definitions
Each DHB is expected to provide a commentary on their latest 12 month ASH data which is available on the nationwide service framework library web site (NSFL) homepage: http://www.nsfl.health.govt.nz/. The data on this site is based on the DHB of domicile population, so all ASH admissions will be captured regardless of which hospital people are admitted to.
The DHB commentary may include additional district level data that is not captured in the national data collection and also information about local initiatives that are intended to reduce ASH admissions.
ASH per 100,000The number of ASH admissions per 100,000 population (DHB and national rates) are provided for three different age groups. These are 0 – 74 years, 45 – 64 years and 0 – 4 years.
The key metric against which targets are set, and DHBs monitored, is the ASH rate for the total population – sometimes referred to as “All.”
This age band data is further divided into: Māori Pacific – for the seven DHBs with the highest number of Pacific people. These are: Auckland,
Waitemata, Counties Manukau, Waikato, Capital and Coast, Hutt, and Canterbury Other All
Additional information can be found on the nationwide services framework library web site www.nsfl.govt.nz including five year trend data (DHB and national), which together with the condition level data assists with interpretation at a DHB level. Denominator:
12 Basu, A., & Brinson, D. (2008). The effectiveness of interventions for reducing ambulatory sensitive hospitalisations: A Systematic Review. HSAC Report.
95
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
The DHB population is derived from PHO enrolment data and age standardised using the World Health Organisation (WHO) population age group distribution.
Additional DataAdditional condition level data is available to DHBs through the NSFL website.
Reporting Period Six monthly in the second and fourth quarters, (against results based on most complete previous 12 months’ data).
Expectations Targets will be derived from ASH rates for the total population. The baseline rates for the DHB will be compared with national rates, and targets set according to the table below.
The same targets will apply to the total (“all”) population, as well as to the Maori and Pacific populations.
Expected improvement should fall in the following ranges based on baseline position:Baseline Level - total population Expected Improvement> 35% Above National Rate 15% to 20%25% to 35% Above National Rate 10% to 14.9%15% to 25% Above National Rate 6% to 9.9%5% to 15% Above National Rate 3% to 5.9%5% Below to 5% Above National Rate 1% to 2.9%< 95% of National Rate Remain Below
Worked example:
Fictional DHB
Age Group Baseline DHB rate
Per 100,000
Compared to national rate
Target % Targetrate
0 – 4 years
Total 4759 103% 102% 4712
Māori 4712
Pacific 4712
45 – 64 years
Total 3048 150% 135% 2743
Māori 2743
Pacific 2743
0 – 74 years
Total 2357 126% 113% 2113
Māori 2113
Pacific 2113
Assessment CriteriaThese assessments will be based on analysis of the most complete 12 months rolling data available at the time of the fourth quarter assessment. The following achievement scale will be applied:
96
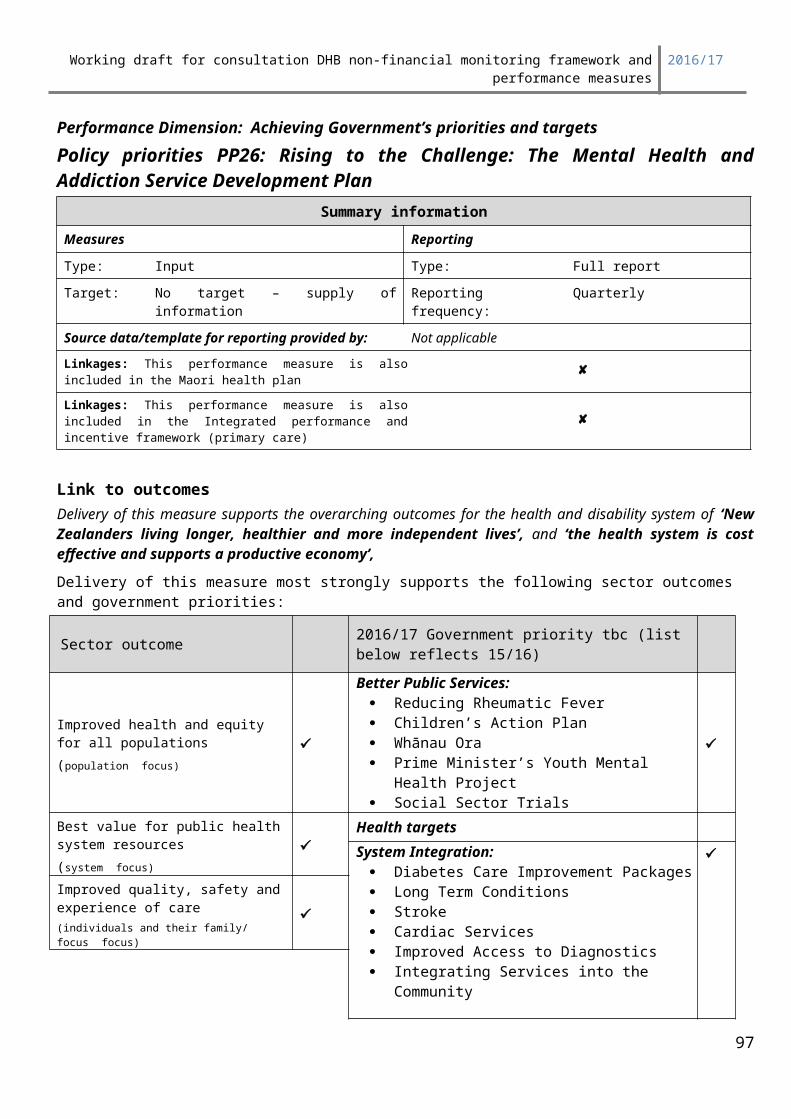
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Rating:Outstanding Performer The DHB has met all targets agreed in the Annual Plan, and has
similar ASH rates across its total population, as well as its Māori and Pacific populations.
Achieved An achieved rating is applied when the DHB has met all the targets agreed in its Annual Plan for its total (all) population across the three age groups.In addition it has reduced ASH rates for its Māori and Pacific populations.An appropriate resolution plan is also provided that will demonstrate how the DHB will further reduce ASH rates for Maori and Pacific so that their rates will move closer to that of the total population.
Partially Achieved The DHB has met all of the targets agreed in its Annual Plan for its total (all) population, but rates for Maori and Pacific have not improved.An appropriate resolution plan is provided that will demonstrate how the DHB will reduce ASH rates for Maori and Pacific.
The DHB has met some of the targets agreed in its Annual Plan for its total (all) population.An appropriate resolution plan is provided that will demonstrate how the DHB will reduce ASH rates for its population(s).
The DHB has met none of the targets agreed in its Annual Plan for its total (all) population, but rates for Maori and Pacific have improved.An appropriate resolution plan is provided that will demonstrate how the DHB will reduce ASH rates for its population(s).
Not Achieved The DHB has met none of the targets agreed in its Annual Plan for its total (all) population.An appropriate resolution plan is provided that will demonstrate how the DHB will reduce ASH rates for its population(s).
97
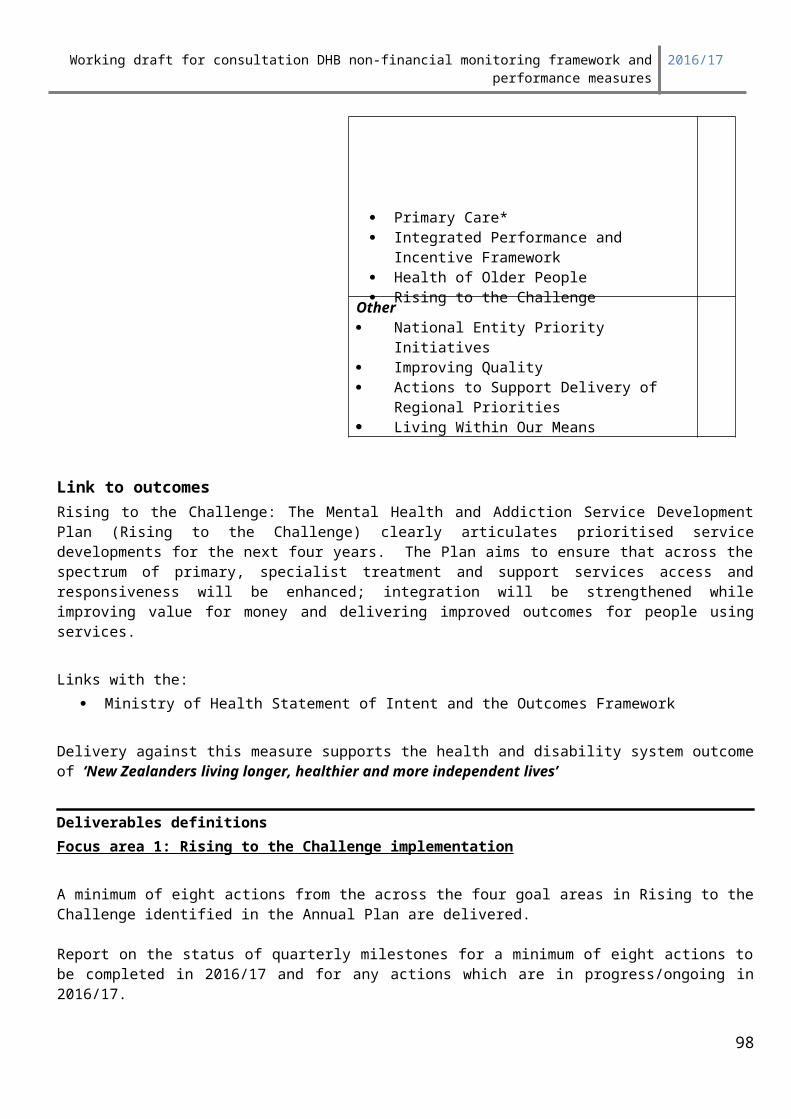
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Meeting service coverage requirements and supporting sector inter-connectedness
System Integration SI2: Delivery of Regional Service PlansSummary information
Target/performance expectation:Agreed in Regional and Annual Plans
Reporting progress report against actions in the regional implementation plan
Type: Qualitative
Reporting frequency: Quarterly
Source data/template for reporting provided by:Report to be provided by Shared service agency on behalf of DHBs.
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targets System Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
98
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
By reporting on the regional performance measure the DHB demonstrates that they are collaborating regionally. This measure enables the formal monitoring of delivery of regional priorities and supports achieving the regional planning purpose. Regional planning objectives are to reduce clinical and financial vulnerability of services and improve service sustainability, reduce costs and improve quality, by coordinated service model development and coordinated planning of workforce and information technology. Delivery of this measure supports achieving improved system integration by linking commitments made in the Regional Service Plans (RSP) and Annual Plan (AP).
RSPs include the regional government priorities and may also include locally agreed regional priorities. The Ministry’s assessment of RSPs and quarterly reports is focussed on the government priorities. Per government priority area the regions are required to specify measures and deliverables as per the RSP guidance.
Deliverables1. A single progress report will be supplied on behalf of the region, agreed by all DHBs within that region.
The report should focus on the actions agreed by each region as detailed in its RSP implementation plan.
For each government priority, and its associated actions, the progress report will identify:
the nominated lead DHB/person/position responsible for ensuring the action is delivered
whether actions and milestones are on track to be met or have been met
performance against agreed measures and targets; and
financial performance against budget associated budget associated with the action where applicable.
If actions/milestones /performance measures/financial performance are not tracking to plan a resolution plan must be in place and agreed. The resolution plan should include actions and regional decision-making processes being undertaken to agree to the resolution plan.
To streamline reporting individual DHBs will not be required to report on local actions to support regional priorities through their local DHB quarterly reports.
2. In quarters two and four regions are expected to provide the following information in support the implementation of integrated hepatitis C assessment and treatment services:
Report six monthly broken down by quarters on the following measures:
Measures Data and source1. Number of people diagnosed with hepatitis C
per annum (by age).Total number of people with a positive HCV PCR test in the DHB region (data from 5 reference labs provided to regional DHBs).
2. Number of HCV patients who have had a Fibroscan in the last year(a) new patients(b) follow up(by age and ethnicity).
Total number of hepatitis C Fibroscans performed annually (data from the delivery of Fibroscans in primary and secondary care).
99
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
3. Number of people receiving PHARMAC funded antiviral treatment per annum (by age and ethnicity).
Total number of people prescribed antiviral treatment who have hepatitis C (data from PHARMAC provided to regional DHBs).
Reporting Period Quarterly
Reporting required: A reporting template will be developed to support consistency of approach across the regions.
Quarter For the time periodQuarter 1 1 July – 30 September
Quarter 2 1 October – 31 December
Quarter 3 1 January – 31 March
Quarter 4 1 April – 30 June
ExpectationsRegional progress in the delivery of each government priority area will be assessed quarterly according to the criteria outlined below:
Definitions of ratings of government prioritiesAchieved All health targets/deliverables/milestones have been tracking to plan;
Partially Achieved
Health targets have been achieved; some indicators/deliverables/milestones are not tracking to plan but an adequate resolution plan is in place; more clarification is required from the region.
Not Achieved One or more health targets indicators/deliverables/milestones have not been achieved; no adequate resolution plan is in place; there are delays in the implementation of the plan.
The overall report for this performance measure will get one rating based on the following criteria:
Definitions of ratings of overall regional reportAchieved All regional government priorities are tracking to plan
Partially Achieved
Some priorities are not tracking to plan but an adequate resolution plan has been provided.
Not Achieved One or more priorities are not tracking to plan and resolution plan is inadequate.
100
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Meeting service coverage requirements and Supporting sector inter-connectedness
System Integration SI3: Ensuring delivery of Service CoverageSummary information
Measures Reporting
Type: Output Type: Confirmation & exception
Target: Exceptions set out in APs Reporting frequency: Six monthly
Source data/template for reporting provided by: Not Applicable
Linkages: This performance measure is also included in the Maori health plan Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities
101
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Living Within Our Means
By ensuring service coverage for its population and addressing service gaps, the DHB will increase the public’s trust and confidence that the health and disability system is able to provide them the services they may need. Providing these essential health services will contribute to the high level outcome of New Zealanders living longer, healthier and more independent lives.
This measure is included as a formal mechanism for ensuring service coverage gaps are transparently managed. The DHB monitoring framework focuses on key marker services. This measure allows performance failures in those service areas that are not routinely monitored to be formally managed within the accountability framework.
Delivery of this measure will support Better Sooner More Convenient Health Services for New Zealanders by ensuring that service risks are managed and Government’s decisions about the national minimum range of services to be made available to the public are delivered.
Delivery of this measure will also support the key (strategic) planning approaches of Improved Integration and Regionalisation by encouraging DHBs to collaborate to find solutions to service coverage issues and risks, especially in relation to vulnerable services and collectively ensure service coverage is delivered.
Actions and activities that have a proven impact on this measure:Actions that support resolution of service coverage gaps and issues may include: development and implementation of a work-out plan, employment of additional staff or equipment, funding additional volumes or making service(s) available through an alternate provider/DHB, or identifying funding, contractual, or other constraints, which must be addressed before the issue can be resolved.
Deliverables definitionsQualitative indicatorDHBs to report providing the following information:Report progress achieved during the quarter towards resolution of exceptions to service coverage identified in the Annual Plan, and not approved as long term exceptions, and any other gaps in service coverage identified by the DHB or Ministry through:• analysis of explanatory indicators• media reporting • risk reporting• formal audit outcomes• complaints mechanisms• sector intelligence.
Reporting Period Reporting required: Six Monthly, in the second and fourth quarters
ExpectationsDHBs are expected to ensure service coverage expectations are met, and to demonstrate resolution of service coverage gaps by reporting complete, comprehensive, and timely information on the deliverable outlined above, demonstrating an appropriate resolution plan is in place for identified issues, and adequate progress is being made against the resolution plan.• A partial achievement rating will be obtained when a DHB has a service coverage gap that has not
been agreed as a formal long term exception for the period of the DAP, and an appropriate resolution
102
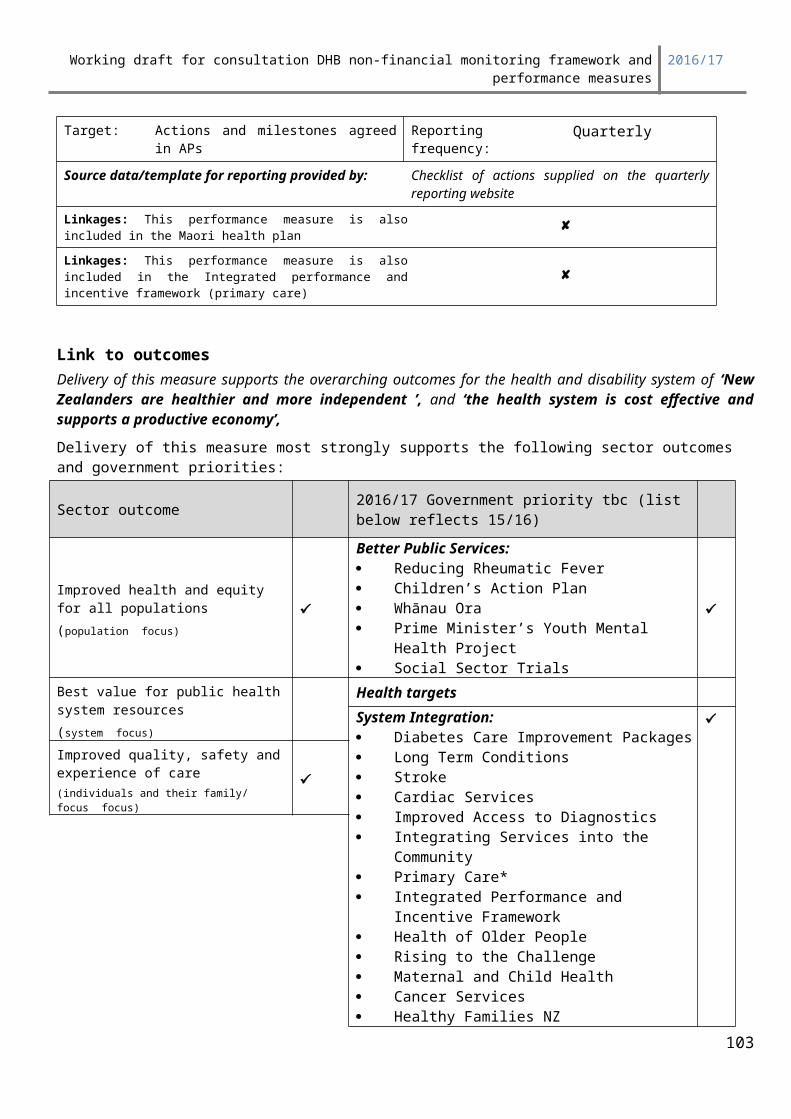
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
plan is supplied that demonstrates the DHB is making progress towards resolution of the service coverage gap.
• An achieved rating will be obtained when all service coverage expectations have been met for the period under review.
• An outstanding performer/sector leader rating does not apply for this risk-based measure.
Exception reporting Exception reports should include progress made towards resolution of service coverage gaps, including milestones for final resolution.
103
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Meeting service coverage requirements and Supporting sector inter-connectedness
System Integration SI4: Standardised Intervention Rates (SIRs)Summary information
Standardised Intervention Rates (SIRs) measure a DHB’s service delivery to their population relative to the service delivery in other DHBs, standardised to take account of variations in the population profiles of different DHBs. The Ministry will be monitoring DHB SIRs for cataracts, major joints, and cardiac services, including cardiac surgery, percutaneous coronary revascularization (angioplasty), and coronary angiography services.
Measures Reporting
Type: Impact Type: Exception
Target: Targets agreed in AP Reporting frequency: Annually cataracts major joints
Quarterly cardiac surgery coronary
angiography coronary angioplasty
Source data/template for reporting provided by: Data supplied by DHBs to the National Minimum Dataset, and report provided by Ministry. Reports will be loaded on Quickr.Note: While DHB reporting on cataracts and major joints is only required on an annual basis, update reports will be made available on Quickr quarterly to allow DHBs to monitor their progress.
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system Health targets
104
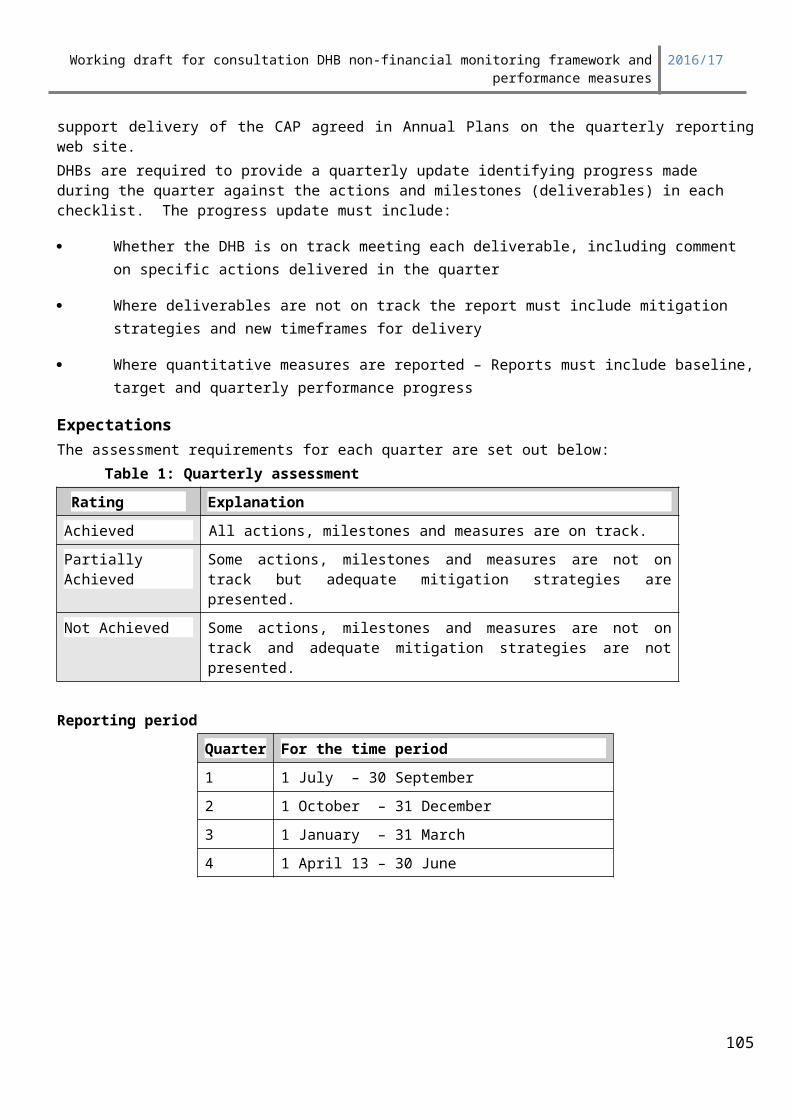
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
resources(system focus)
System Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Link to outcomesDelivery against this measure supports the health and disability system outcome of ‘New Zealanders living longer, healthier and more independent lives’ and the primary intermediate outcome that ‘People receive better health and disability services’. An additional outcome is ‘The health and disability system and services are trusted and can be used with confidence’.
Elective services, including cardiac, are an important part of the health care system for the treatment, diagnosis and management of health problems. Timely access to these services is also considered a measure of the effectiveness of the health system. Elective surgery is important to New Zealanders as these are essential services to reduce pain or discomfort, and improve independence and wellbeing. This is particularly the case for surgery such as cardiac, cataract, and major joint replacement procedures. To provide elective services at appropriate rates for its population, the DHB will need to improve or maintain access to key elective procedures, and ensure people receive better and more timely access to treatment.
Improving relative access to electives will also contribute to delivery of the Government’s pledge to increase elective surgery by an average of 4,000 discharges year on year.
Meeting standardised intervention rates for a variety of types of surgery means that access is fair, and not dependent upon where a person lives. Knowing that access to services is equitable will improve the public’s trust and confidence in the public health system.
This measure will help improve people’s quality of life and help people to live longer, healthier and more independent lives.
Link to priority areas of focus
105
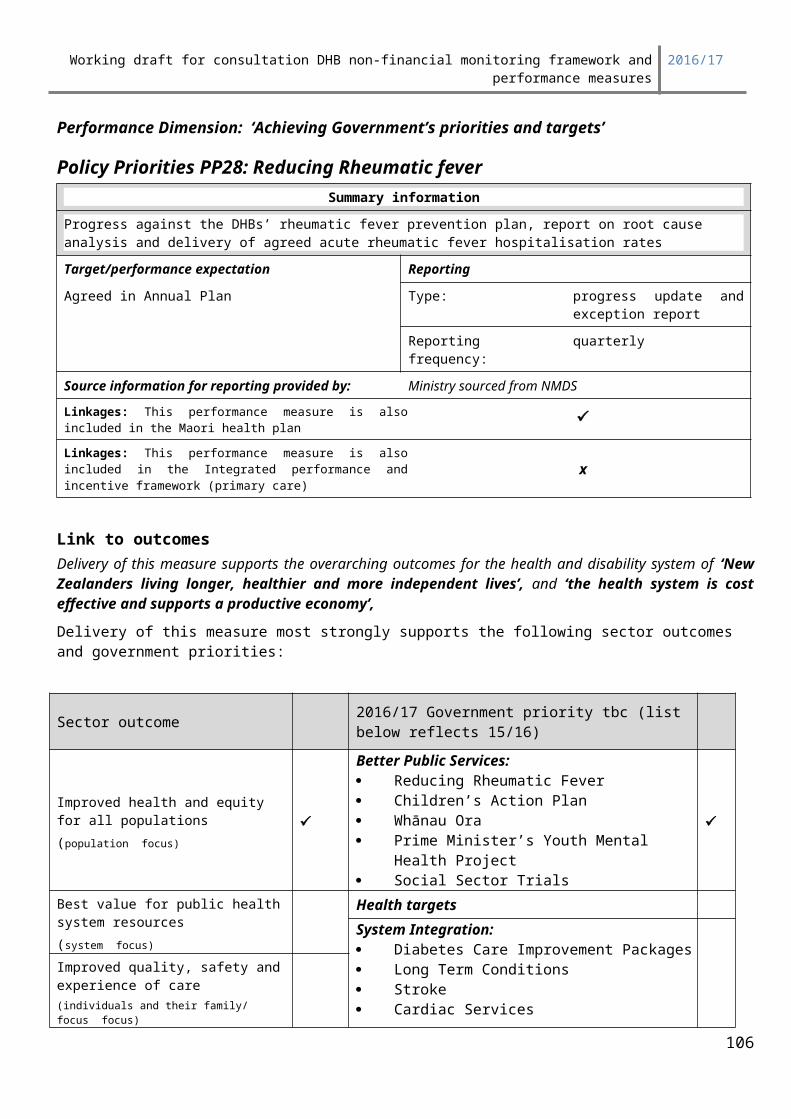
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Delivery of this measure will support Better Sooner More Convenient Health Services for New Zealanders by improving or maintaining access to elective services, and ensuring people receive better and more timely access to health services, regardless of where they live.
Pathways to improve access for these conditions require seamless flow between primary and secondary care, and regional collaboration.
The following actions and activities are examples of initiatives that have a proven impact on this measure. 1. The Orthopaedic, Cataract and Cardiac Initiatives, which provided additional ring fenced funding for
joint, cataract and cardiac surgery – funding continues to be available to DHBs to support improved access to these procedures;
2. The Electives Initiative which has provided funding to improve access to a wide range of elective surgery, including cardiology inpatient treatment or diagnostics;
3. The Ambulatory Initiative which has provided funding to improve access to first specialist assessments, including cardiology, and to community referred diagnostics.
Deliverables definitionsQuantitative Indicator*Expectations
• For major joint replacement procedures, a target intervention rate of tbc per 10,000 of population will be achieved.
• For cataract procedures, a target intervention rate of tbc per 10,000 of population will be achieved.• For cardiac surgery13 a target intervention rate of tbc per 10,000 of population will be achieved.
DHBs with rates of tbc per 10,000 or above in previous years will be required to maintain this rate.• For percutaneous revascularization a target rate of at least tbc per 10,000 of population will be
achieved. • For coronary angiography services a target rate of at least tbc per 10,000 of population will be
achieved.• ICD10 codes for each of the procedure groups are included in the technical specification to this
document.
Qualitative IndicatorFor any procedure where the standardised intervention rate in the preceding 12 month period is significantly below the target level a report demonstrating:1. what analysis the DHB has done to review the appropriateness of its rate
AND2. whether the DHB considers the rate to be appropriate for its population14
OR3. a description of the reasons for its relative under-delivery of that procedure; and
13 Cardiac surgery is defined as coronary artery bypass graft (CABG), and valve replacement or repair (including transcatheter aortic valve implantation, and valve sparing aortic root procedures) for patients aged 15 and over.14 If a DHB deems the rate delivered to be appropriate then this must be supported with the analysis the DHB has done to review the appropriateness of its rate (as per 1 and 2 above). If the analysis is substantial enough to give confidence in the DHBs position, then this would be accepted, and an Achieved rating would be provided. If not, depending on the analysis provided, a Partial rating may be given. It is important to acknowledge that DHBs commit to SIRs in their annual plans. Analysis should be completed at least annually, and this should inform the rate which is agreed between the Ministry and the DHB. If a DHB considers that their SIR should be set lower than the national rate, then this analysis and discussion should be discussed with the NHB as part of the annual planning cycle.
106
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
4. the actions being undertaken in the current year (2016/17) that will ensure the target rate is achieved.
Reporting periodFor cataracts and major joints, annually as follows:
Quarter For the time periodQuarter 1 2015/16 financial year’s results
For cardiac services, reported quarterly as follows:
Quarter For the time period*Quarter 1 2015/16 financial year’s results
Quarter 2 2016/17 quarter 1 results
Quarter 3 2016 calendar year’s results
Quarter 4 2016/17 quarter 3 results
* Due to the reliance on NMDS data (where the deadline for submission is about one month after the end of the quarter), the data used to derive this measure will be for one quarter in arrears.
ExpectationsWhat are the Ministry’s expectations of performance?Quantitative measures Standardised intervention rates not significantly below the expected level.
Qualitative measuresThe analysis report (1 and 2 above) must cover the relationship between the secondary and primary sectors, including evidence of consultation with primary care as to the perceived level of access (does primary care have patients they consider should be able to access this procedure who cannot, or who they are no longer referring because of historic access issues, etc.). The report must also provide confirmation from the relevant service clinical director that the rate being provided is appropriate for the DHB population.
Unless the above information is provided, the Quarter One report (3 and 4 above) needs to outline actions being undertaken in the current year (2016/17) to achieve the required rate. Subsequent quarterly reports for cardiac services need to outline progress being made against these plans.
Baseline informationBaseline information can be found on the Electives restricted access website (Quickr). Current performance reports will be provided by the Ministry via the quarterly reporting database. Full standardised intervention rate information is available via Quickr, the restricted Electives website.
Technical Specifications –
WIES version
107
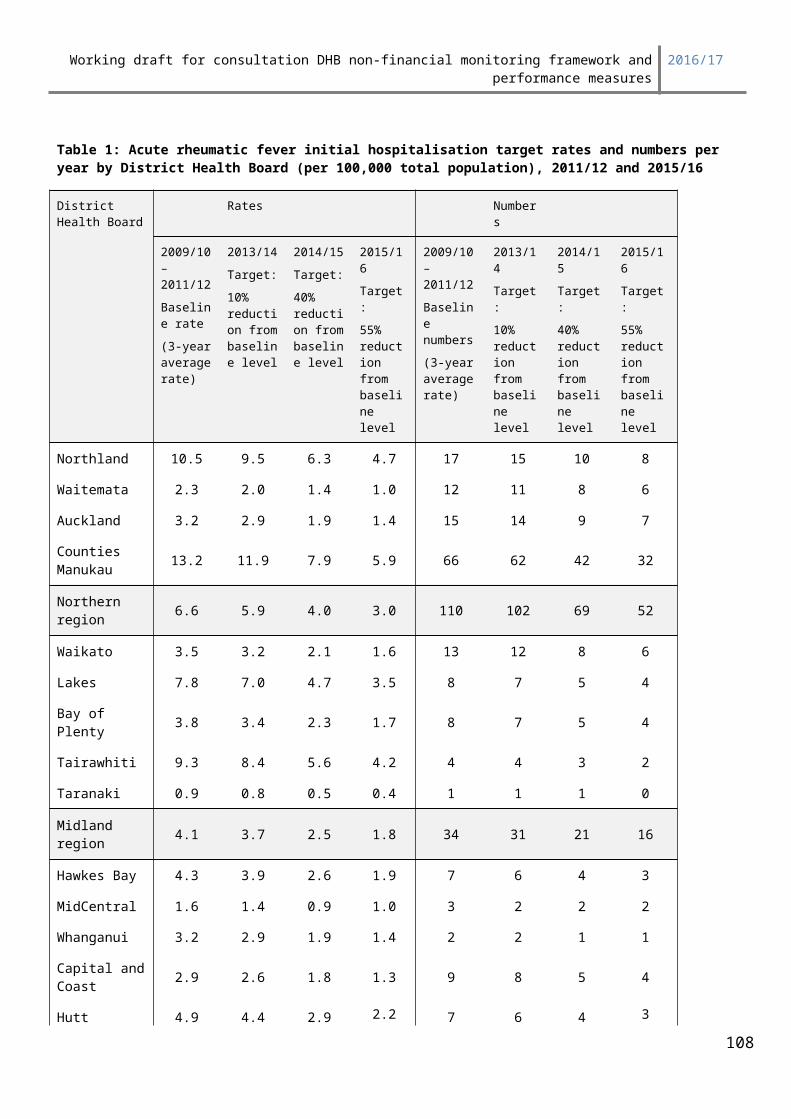
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
The most current version of WIES available at the time baseline data is run. For 2016/17 this is New Zealand WIES version tbc methodology.
Standardisation Methodology
Date is standardised by - Age (5 year age bands)- Gender (Male, Female)- Ethnicity (Maori Pacific, Other)- Deprivation Quintile (NZ Dep 2006 Quintiles)
DHB data is standardised to the total New Zealand population using indirect standardisation methodology.
Direct standardisation methodology relies on there being a number of people in all possible population groups. If these criteria are not met there is a risk of unreliable intervention rates for population groups with very low numbers. The distribution of the standard population should not be markedly different from the study populations being compared.
However many of the possible population groups within some DHBs have few or no people, and the population profiles vary markedly between DHBs. Therefore, the indirect standardisation methodology is used to develop the DHB’s intervention rates, to avoid the risk of distortion.
The national intervention rate for each population group is applied to the same population group in each DHB, for all population groups, and these numbers are summed to give an expected number of procedures.
The observed (actual) number of procedures is divided by the expected number of procedures to give a standardised discharge ratio (SDR). The national intervention rate is multiplied by the SDR to give the standardised intervention rate for the DHB
SIR = total observed discharges x national intervention rate total expected discharges
= ∑ni x R∑piRi
Where:ni = the number of discharges in age, gender, ethnicity and dep group ipi = the population in age, gender, ethnicity and dep study group iRi = the national intervention rate for age, gender, ethnicity and dep group iR = the overall national intervention rate
Admission types:
• AC – Acute• AA – Arranged• AP – Private hospital elective admission• WN – Admitted from waiting list (Elective)
108
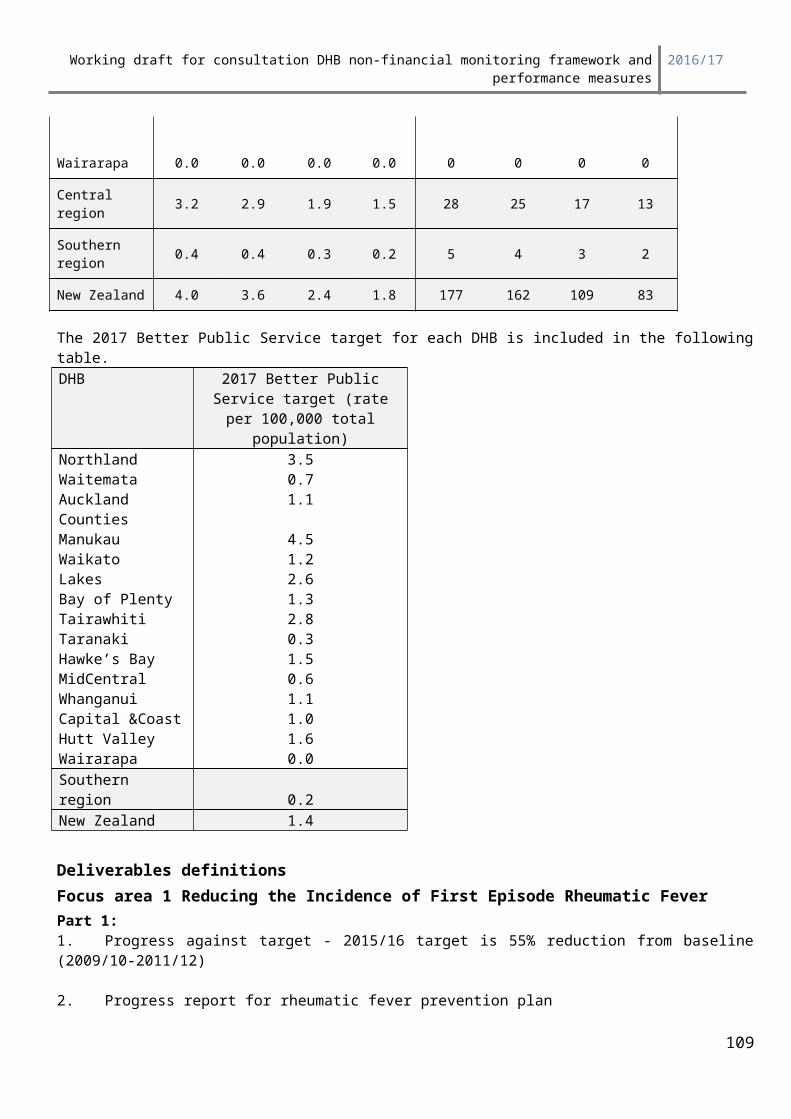
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Principle health purchaser code:
• 13 – DHB base purchase (retired)• 20 – Overseas eligible• 34 – MOH funded purchase• 35 – DHB funded purchase
Purchase units:
All purchase units
ICD10 Codes included in the reports
To ensure no procedures are omitted from a procedure group, all relevant codes from all ICD versions are included in this list.
Type Code DescriptionCardiac Surgery 3849700 Coronary artery bypass, using 1 saphenous vein graftCardiac Surgery 3849701 Coronary artery bypass, using 2 saphenous vein graftsCardiac Surgery 3849702 Coronary artery bypass, using 3 saphenous vein graftsCardiac Surgery 3849703 Coronary artery bypass, using >= 4 saphenous vein graftsCardiac Surgery 3849704 Coronary artery bypass, using 1 other venous graftCardiac Surgery 3849705 Coronary artery bypass, using 2 other venous graftsCardiac Surgery 3849706 Coronary artery bypass, using 3 other venous graftsCardiac Surgery 3849707 Coronary artery bypass, using >= 4 other venous graftsCardiac Surgery 3850000 Coronary artery bypass, using 1 LIMA graftCardiac Surgery 3850300 Coronary artery bypass, using >= 2 LIMA graftsCardiac Surgery 3850001 Coronary artery bypass, using 1 RIMA graftCardiac Surgery 3850301 Coronary artery bypass, using >= 2 RIMA graftsCardiac Surgery 3850002 Coronary artery bypass, using 1 radial artery graftCardiac Surgery 3850302 Coronary artery bypass, using >= 2 radial artery graftsCardiac Surgery 3850003 Coronary artery bypass, using 1 epigastric artery graftCardiac Surgery 3850303 Coronary artery bypass, using >= 2 epigastric artery graftsCardiac Surgery 3850004 Coronary artery bypass, using 1 other arterial graftCardiac Surgery 3850304 Coronary artery bypass, using >= 2 other arterial graftsCardiac Surgery 9020100 Coronary artery bypass, using 1 other material graft, not elsewhere classifiedCardiac Surgery 9020101 Coronary artery bypass, using 2 other material grafts, not elsewhere classifiedCardiac Surgery 9020102 Coronary artery bypass, using 3 other material grafts, not elsewhere classifiedCardiac Surgery 9020103 Coronary artery bypass, using >=4 other material grafts, not elsewhere classifiedCardiac Surgery 3863700 Re-operation for reconstruction of occluded coronary artery graftCardiac Surgery 3845610 Open valvotomy of aortic valveCardiac Surgery 3848000 Repair of aortic valve, 1 leafletCardiac Surgery 3848100 Repair of aortic valve, 2 or more leafletsCardiac Surgery 3848300 Decalcification of aortic valve leafletCardiac Surgery 3848800 Replacement of aortic valve with mechanical prosthesisCardiac Surgery 3848801 Replacement of aortic valve with bioprosthesisCardiac Surgery 3848900 Replacement of aortic valve with homograftCardiac Surgery 3848901 Replacement of aortic valve with unstented heterograftCardiac Surgery 3845615 Other intrathoracic procedures on aortic valve without cardiopulmonary bypassCardiac Surgery 3865304 Other intrathoracic procedures on aortic valve with cardiopulmonary bypassCardiac Surgery 3848700 Open valvotomy of mitral valveCardiac Surgery 3848001 Repair of mitral valve, 1 leaflet
109

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Cardiac Surgery 3848101 Repair of mitral valve, >= 2 leafletsCardiac Surgery 3848501 Decalcification of mitral valveCardiac Surgery 3847500 Mitral valve annuloplastyCardiac Surgery 3847700 Mitral valve annuloplasty with ring insertionCardiac Surgery 3847702 Aortic valve annuloplasty with ring insertionCardiac Surgery 3848802 Replacement of mitral valve with mechanical prosthesisCardiac Surgery 3848803 Replacement of mitral valve with bioprosthesisCardiac Surgery 3848902 Replacement of mitral valve with homograftCardiac Surgery 3848500 Reconstruction of mitral valve annulusCardiac Surgery 3845616 Other intrathoracic procedures on mitral valve without cardiopulmonary bypassCardiac Surgery 3865305 Other intrathoracic procedures on mitral valve with cardiopulmonary bypassCardiac Surgery 3845611 Open valvotomy of tricuspid valveCardiac Surgery 3848002 Repair of tricuspid valve, 1 leafletCardiac Surgery 3848102 Repair of tricuspid valve, >=2 leafletsCardiac Surgery 3847501 Tricuspid valve annuloplastyCardiac Surgery 3847502 Aortic valve annuloplastyCardiac Surgery 3847701 Tricuspid valve annuloplasty with ring insertionCardiac Surgery 3848804 Replacement of tricuspid valve with mechanical prosthesisCardiac Surgery 3848805 Replacement of tricuspid valve with bioprosthesisCardiac Surgery 3848903 Replacement of tricuspid valve with homograftCardiac Surgery 3845617 Other intrathoracic procedures on tricuspid valve without cardiopulmonary bypassCardiac Surgery 3865306 Other intrathoracic procedures on tricuspid valve with cardiopulmonary bypassCardiac Surgery 3845601 Open valvotomy of pulmonary valveCardiac Surgery 3848806 Replacement of pulmonary valve with mechanical prosthesisCardiac Surgery 3848807 Replacement of pulmonary valve with bioprosthesisCardiac Surgery 3848904 Replacement of pulmonary valve with homograftCardiac Surgery 3848905 Replacement of pulmonary valve with unstented heterograft
Cardiac Surgery 3845618Other intrathoracic procedures on pulmonary valve without cardiopulmonary bypass
Cardiac Surgery 3865307 Other intrathoracic procedures on pulmonary valve with cardiopulmonary bypassCardiac Surgery 3849000 Reconstruction and re-implantation of subvalvular structures
Cardiac Surgery 3849300Operative management of acute infective endocarditis during heart valve procedure
Cardiac Surgery 3855000 Repair of ascending thoracic aortaCardiac Surgery 3855001 Replacement of ascending thoracic aortaCardiac Surgery 3855300 Repair of ascending thoracic aorta with aortic valve repairCardiac Surgery 3855301 Repair of ascending thoracic aorta with aortic valve replacement
Cardiac Surgery 3855600Repair of ascending thoracic aorta with aortic valve repair and implantation of coronary arteries
Cardiac Surgery 3855601Repair of ascending thoracic aorta with aortic valve replacement and implantation of coronary arteries
Cardiac Surgery 3855900 Repair of aortic arch and ascending thoracic aortaCardiac Surgery 3855901 Replacement of aortic arch and ascending thoracic aortaCardiac Surgery 3856200 Repair of aortic arch and ascending thoracic aorta with aortic valve repairCardiac Surgery 3856201 Repair of aortic arch and ascending thoracic aorta with aortic valve replacement
Cardiac Surgery 3856500Repair of aortic arch and ascending thoracic aorta with aortic valve repair and implantation of coronary arteries
Cardiac Surgery 3856501Repair of aortic arch and ascending thoracic aorta with aortic valve replacement and implantation of coronary arteries
Cardiac Surgery 3855302 Replacement of ascending thoracic aorta with aortic valve repairCardiac Surgery 3855303 Replacement of ascending thoracic aorta with aortic valve replacement
Cardiac Surgery 3855602Replacement of ascending thoracic aorta with aortic valve repair and implantation of coronary arteries
110
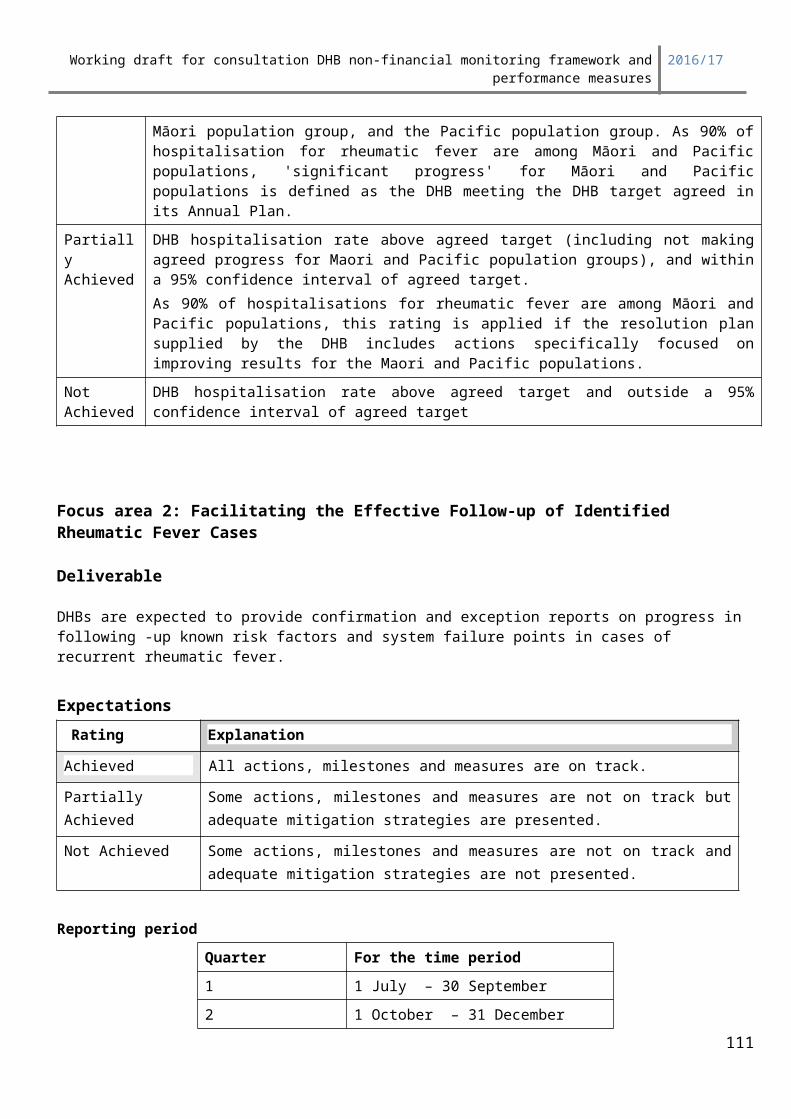
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Cardiac Surgery 3855603Replacement of ascending thoracic aorta with aortic valve replacement and implantation of coronary arteries
Cardiac Surgery 3856202 Replacement of aortic arch and ascending thoracic aorta with aortic valve repair
Cardiac Surgery 3856203Replacement of aortic arch and ascending thoracic aorta with aortic valve replacement
Cardiac Surgery 3856502Replacement of aortic arch and ascending thoracic aorta with aortic valve repair and implantation of coronary arteries
Cardiac Surgery 3856503Replacement of aortic arch and ascending thoracic aorta with aortic valve replacement and implantation of coronary arteries
Cataract 4269800 Intracapsular extraction of crystalline lensCataract 4270200 Intracapsular extraction of crystalline lens with insertion of foldable artificial lensCataract 4270201 Intracapsular extraction of crystalline lens with insertion of other artificial lens
Cataract 4269801Extracapsular extraction of crystalline lens by simple aspiration (and irrigation) technique
Cataract 4270202Extracapsular extraction of crystalline lens by simple aspiration (and irrigation) technique with insertion of foldable artificial lens
Cataract 4270203Extracapsular extraction of crystalline lens by simple aspiration (and irrigation) technique with insertion of other artificial lens
Cataract 4269802Extracapsular extraction of crystalline lens by phacoemulsification and aspiration of cataract
Cataract 4270204Extracapsular extraction of crystalline lens by phacoemulsification and aspiration of cataract with insertion of foldable artificial lens
Cataract 4270205Extracapsular extraction of crystalline lens by phacoemulsification and aspiration of cataract with insertion of other artificial lens
Cataract 4269803Extracapsular extraction of crystalline lens by mechanical phacofragmentation and aspiration of cataract
Cataract 4270206Extracapsular extraction of crystalline lens by mechanical phacofragmentation and aspiration of cataract with insertion of foldable artificial lens
Cataract 4270207Extracapsular extraction of crystalline lens by mechanical phacofragmentation and aspiration of cataract with insertion of other artificial lens
Cataract 4269804 Other extracapsular extraction of crystalline lens
Cataract 4270208Other extracapsular extraction of crystalline lens with insertion of foldable artificial lens
Cataract 4270209Other extracapsular extraction of crystalline lens with insertion of other artificial lens
Cataract 4269805 Other extraction of crystalline lensCataract 4270210 Other extraction of crystalline lens with insertion of foldable artificial lensCataract 4270211 Other extraction of crystalline lens with insertion of other artificial lens
Cataract 4273101Extraction of crystalline lens by posterior chamber sclerotomy with removal of vitreous
Cataract 4271900 Capsulectomy of lensCataract 4271902 Mechanical fragmentation of secondary membraneCataract 4272200 Capsulectomy of lens by posterior chamber sclerotomyCataract 4273100 Capsulectomy of lens by posterior chamber sclerotomy with removal of vitreousCataract 4273400 Capsulotomy of lensCataract 4273700 Needling of posterior capsule of lensCataract 4278800 Capsulotomy of lens by laserCataract 4279102 Corticolysis of lens material by laserCataract 4271600 Removal of juvenile cataractMajor Joints 4931800 Total arthroplasty of hip, unilateralMajor Joints 4931900 Total arthroplasty of hip, bilateralMajor Joints 4932400 Revision of total arthroplasty of hipMajor Joints 4932700 Revision of total arthroplasty of hip with bone graft to acetabulumMajor Joints 4933000 Revision of total arthroplasty of hip with bone graft to femurMajor Joints 4933300 Revision of total arthroplasty of hip with bone graft to acetabulum and femur
111
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Major Joints 4933900 Revision of total arthroplasty of hip with anatomic specific allograft to acetabulumMajor Joints 4934200 Revision of total arthroplasty of hip with anatomic specific allograft to femur
Major Joints 4934500Revision of total arthroplasty of hip with anatomic specific allograft to acetabulum and femur
Major Joints 9060700 Resurfacing of hip, unilateralMajor Joints 9060701 Resurfacing of hip, bilateralMajor Joints 4951700 Hemiarthroplasty of kneeMajor Joints 4951800 Total arthroplasty of knee, unilateralMajor Joints 4951900 Total arthroplasty of knee, bilateralMajor Joints 4952100 Total arthroplasty of knee with bone graft to femur, unilateralMajor Joints 4952101 Total arthroplasty to knee with bone graft to femur, bilateralMajor Joints 4952102 Total arthroplasty to knee with bone graft to tibia, unilateralMajor Joints 4952103 Total arthroplasty to knee with bone graft to tibia, bilateralMajor Joints 4952400 Total arthroplasty of knee with bone graft to femur and tibia, unilateralMajor Joints 4952401 Total arthroplasty of knee with bone graft to femur and tibia, bilateralMajor Joints 4953400 Total replacement arthroplasty of patellofemoral joint of kneeMajor Joints 4953000 Revision of total arthroplasty of knee with bone graft to femurMajor Joints 4953001 Revision of total arthroplasty of knee with bone graft to tibiaMajor Joints 4953300 Revision of total arthroplasty of knee with bone graft to femur and tibiaMajor Joints 4955400 Revision of total arthroplasty of knee with anatomic specific allograftMajor Joints 4953401 Total replacement arthroplasty of patellofemoral joint of kneeMajor Joints 4952700 Revision of total arthroplasty of kneeAngiography 3821500 Coronary angiographyAngiography 3821800 Coronary angiography with left heart catherisationAngiography 3821801 Coronary angiography with right heart catherisationAngiography 3821802 Coronary angiography with left and right heart catherisationAngioplasty 3530400 Percutaneous transluminal balloon angioplasty of 1 coronary arteryAngioplasty 3530500 Percutaneous transluminal balloon angioplasty of >= 2 coronary arteriesAngioplasty 3531000 Percutaneous insertion of 1 transluminal stent into single coronary arteryAngioplasty 3531001 Percutaneous insertion of >= 2 transluminal stents into single coronary arteryAngioplasty 3531002 Percutaneous insertion of >= 2 transluminal stents into multiple coronary arteriesAngioplasty 3830000 Percutaneous transluminal balloon angioplasty of 1 coronary arteryAngioplasty 3830300 Percutaneous transluminal balloon angioplasty of >= 2 coronary arteriesAngioplasty 3830600 Percutaneous insertion of 1 transluminal stent into single coronary arteryAngioplasty 3830601 Percutaneous insertion of >= 2 transluminal stents into single coronary arteryAngioplasty 3830602 Percutaneous insertion of >= 2 transluminal stents into multiple coronary arteriesAngioplasty 3830900 Percutaneous transluminal coronary rotational atherectomy [PTCRA], 1 artery
Angioplasty 3831200Percutaneous transluminal coronary rotational atherectomy [PTCRA], 1 artery with insertion 1 stent
Angioplasty 3831201Percutaneous transluminal coronary rotational atherectomy [PTCRA], 1 artery w insertion >= 2 stents
Angioplasty 3831500Percutaneous transluminal coronary rotational atherectomy [PTCRA], multiple arteries
Angioplasty 3831800Percutaneous transluminal coronary rotational atherectomy [PTCRA], multi arteries w insert 1 stent
Angioplasty 3831801Percutaneous transluminal coronary rotational atherectomy, multi arteries w insert >= 2 stents
112
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Meeting service coverage requirements and Supporting sector inter-connectedness
System Integration SI5: Delivery of Whānau Ora DHBs will support a whānau-centred integrated approach to deliver improved whānau health and other social outcomes, while leveraging on the Te Puni Kōkiri funded Whānau Ora provider collectives and Whānau Ora non-government organisation (NGO) Commissioning Agencies.
Summary informationMeasures Reporting
Target: Progress since last year Reporting frequency:
Annual
Source information for reporting provided by: Not applicable
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ
Improved quality, safety and experience of care(individuals and their family/ focus focus)
113
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Spinal Cord Impairment Action PlanOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Whānau Ora places whānau at the centre of service delivery, requires the health sector to work in a more seamless way with other parts of the social sector and expects improved outcomes and results for New Zealand whānau.
To achieve the objectives of Whānau Ora, Te Puni Kōkiri (with the Ministries of Health, Social Development and Education) has supported a range of providers and provider collectives to transform the way they work (including through capacity building of providers/collectives, support of navigation approaches, and outcomes focused contracting). The Ministry is also leading work to implement a Whānau Ora Information System to support whānau and providers.
In the past year, Whānau Ora Commissioning Agencies have also been established. The three agencies are:
Te Pou Matakana (Whānau-focused North Island Commissioning Agency) Te Pūtahitanga o Te Waipounamu (South Island Commissioning Agency); and Pasifika Futures (Commissioning Agency for Pacific families).
While each agency has its own approach, they have the common aim to commission initiatives that build family/whānau capability in areas like income, employment and healthy lifestyles.
ReportingThe DHB’s provision of a qualitative report will demonstrate their contribution to the strategic change for Whānau Ora in the district, progress on engagement and planned activities with Whānau Ora provider collectives to support and improve service delivery and develop mature providers; and engagement and identification of opportunities with their relevant Whānau Ora NGO Commissioning Agencies to leverage on the investment from Te Puni Kōkiri.
Actions and activities that have a proven impact on this measure:DHBs have a role in continuing their support to Whānau Ora providers and collectives and where appropriate collaborating with Commissioning Agencies to benefit the health of whānau.
As DHBs hold the key relationships with health providers, they are best placed to use the opportunity presented by the Whānau Ora provider collectives’ programmes and the NGO Commissioning Agencies to improve service delivery and build mature providers, while building a whānau-centred approach in their districts.
The DHB actions/activities that demonstrate this include:1. Strengthening the relationship that the DHB has with its local Whānau Ora provider collectives. This
could include:a. outlining how the DHB will involve Whānau Ora providers and collectives in strategic planningb. how the DHB is supporting outcome focused, whānau-centred service delivery through its
contracts with local Whānau Ora providers and collectives, and c. how the DHB is working with Whānau Ora providers and collectives to maximise their capacity
and capacility to improve whānau health outcomes.
114
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
2. Identifying opportunities to collaborate with Whānau Ora Commissioning Agencies. This could include involving local commissioning agencies in planning, working on joint projects/commissioning together or building strong relationships with the Commissiong Agencies for the benefit of families/whānau.
3. Participating in processes led by the Ministry to obtain a broader health sector view on Whānau Ora implementation, including support to providers using the Whānau Ora Information System.
Deliverables definitionsThe DHB provides a qualitative report identifying progress within the year that shows that the DHB has delivered on its planned Whānau Ora activity and what the impact of the activity has been. The report should also demonstrate, more generally, how the DHB is supporting the Whānau Ora approach as it relates to Whānau Ora providers and collectives and the Commissioning Agencies, so that it benefits whānau.
This will include a summary of the following – how the DHB is: contributing to the strategic change for Whānau Ora in the district and demonstrate meaningful
activity moving towards improved service delivery. Supporting, including through investment, Whānau Ora providers and collectives to build capacity
and capability through deliberate activities active engagement with Whānau Ora NGO Commissioning Agencies to identify opportunities for
alignment.
Expectations The following achievement scale will be applied: Achieved Appropriate actions identified in all areas of the measure
deliverable.
Partially Achieved
Some actions identified in most of the measure deliverable.
Not Achieved Limited or no actions identified in two or more of four areas of deliverables.
115
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Meeting service coverage requirements and Supporting sector inter-connectedness
System Integration SI6: IPIF Healthy Adult: Cervical ScreeningSummary information
Indicator: Enrolled women 25 – 69 years who have received a cervical smear in the past three years
Measures Reporting
Target: Actions and milestones agreed in APs Type: Process
Reporting frequency: Quarterly
Source data/template for reporting provided by: Data is sourced from National Cervical Screening Programme Register
Owner: National Cervical Screening Programme
Linkages: This performance measure is also included in the Maori health plan
or
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care) or
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,
Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge
Maternal and Child Health Cancer Services
Improved quality, safety and experience of care(individuals and their family/ focus focus)
116
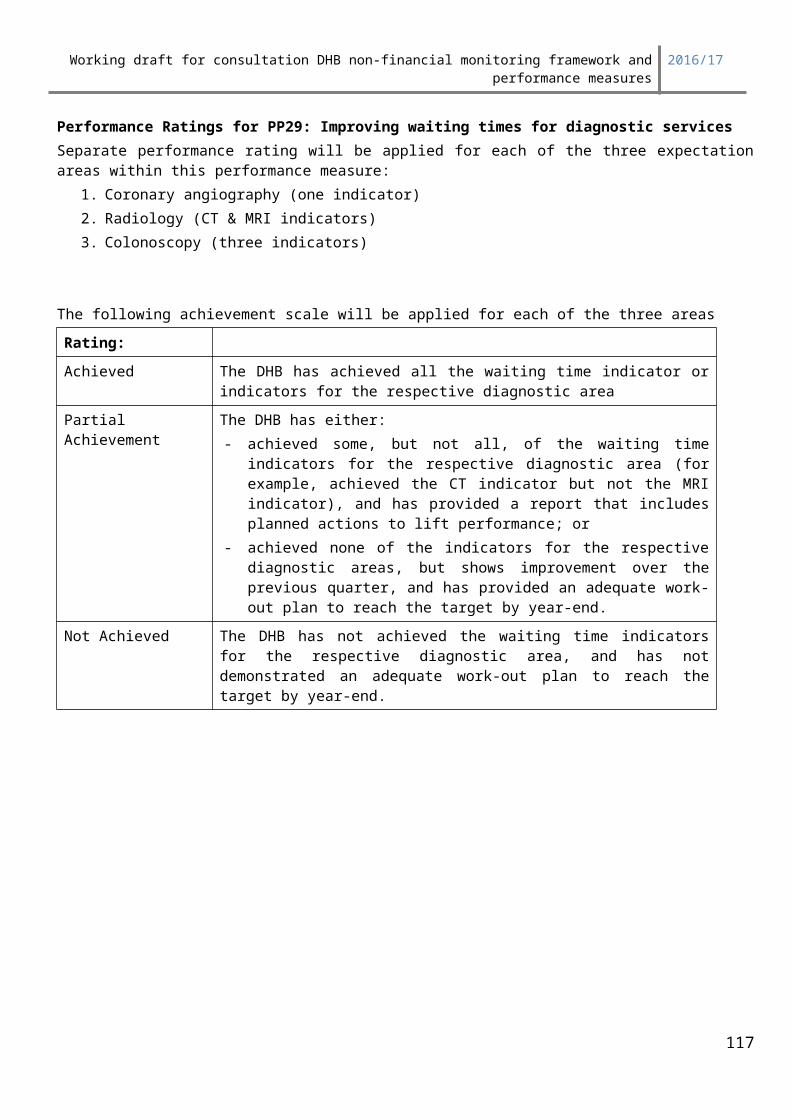
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Healthy Families NZOther
National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Cervical cancer affects about 6 women in every 100,000 (about 160 women each year) and in 2011 the age-standardised mortality rate for cervical cancer was 1.7 per 100,000 population15. Incidence and mortality are less favourable for Māori and Pacific people. Early detection and treatment of cervical cancer and other abnormalities lowers the rate of premature death for women. The available international evidence suggests that women between the ages of 20 and 69 years should have a cervical smear once every three years.
This measure reflects integration, as achievement depends on general practitioners, practice nurses and laboratories working together with colposcopy services to provide a range of activities from health promotion to treatment. The National Cervical Screening Programme (NCSP) has a focus on equity with emphasis on providing services to high priority populations.
Actions and activities that have a proven impact on this measure:DHBs can engage with NCSP activities beyond contracts for colposcopy services, facilitating co-ordination and liaison with key organisations and people, including PHOs, Maori and Pacific Health Providers and GP Practices.
DHBs can use and promote the resources available in the cervical screening section of the National Screening Unit website: https://www.nsu.govt.nz
Deliverables definitions Numerator: Count of enrolled women aged 25 to 69 years at the end of the monitoring period who have received a cervical smear in the past three years
Denominator: Count of women aged 25 to 69 years at the end of the monitoring period based on SNZ population projections (2013 Census base) adjusted for the expected number of women who have had a hysterectomy.
Interpretation issues Nil
Reporting period
Quarter For the time period
1 Three years to 30 September
2 Three years to 31 December
3 Three years to 31 March
15 Ministry of Health. 2014. Cancer: New registrations and deaths 2011. Wellington: Ministry of Health.117
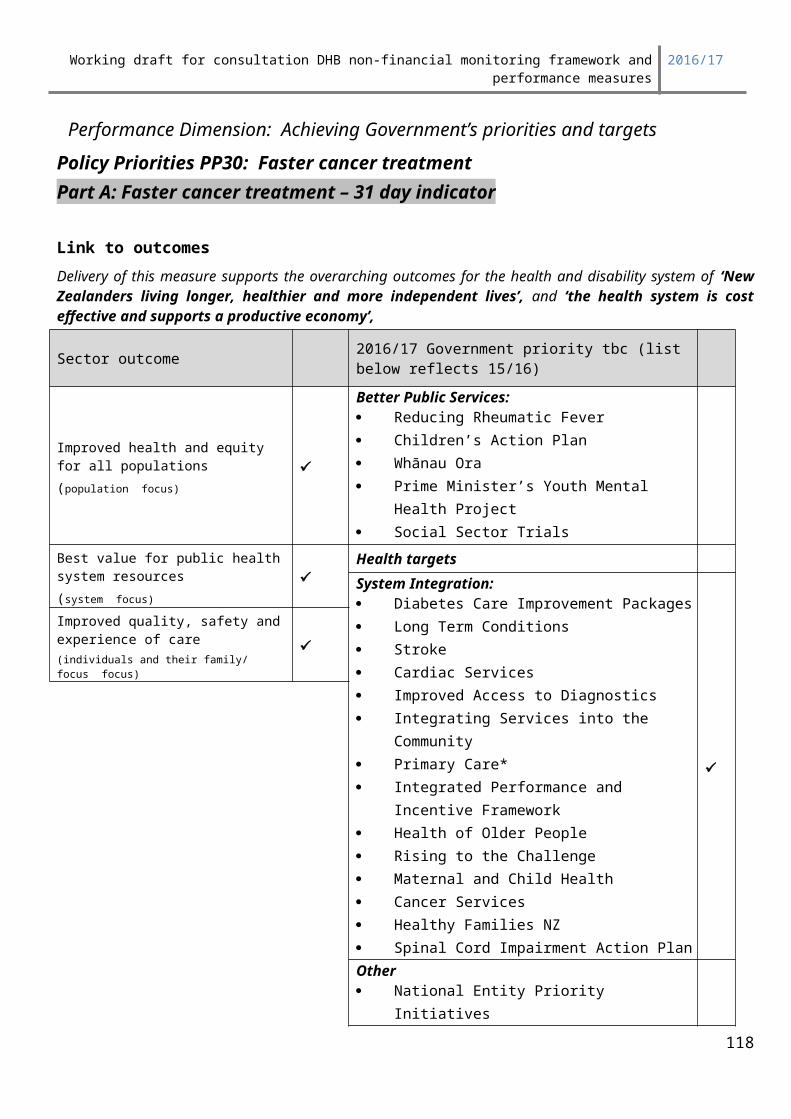
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
4 Three years to 30 June
ExpectationsThe following achievement scale will be applied:
Rating: Definition
Outstanding 90% of eligible women have received cervical screening services within the last 3 years
Achieved 80% of eligible women have received cervical screening services within the last 3 years
Partially Achieved 70 -79% of eligible women have received cervical screening services within the last 3 years
Not Achieved Less than 70% of eligible women have received cervical screening services within the last 3 years
Reporting TemplateNone required.
118
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Providing quality services efficiently
Ownership OS3: Inpatient Average Length of Stay (ALOS)
Summary informationTarget/performance expectation Reporting
Agreed in Annual Plan Type: Comprehensive measurement
Reporting frequency: Quarterly
Source data/template for reporting provided by: Not applicable
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomes Delivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services
Best value for public health system resources(system focus)
Children’s Action Plan
Improved quality, safety and experience of care(individuals and their family/whanau focus focus) PM’s Youth Mental Health Project
Whanua Ora
Health targets
Care closer to home
Living within our Means
Health of Older People
Regional and national collaboration
Other (tbc)
By shortening hospital length of stay, while ensuring patients receive sufficient care to avoid readmission, the DHB will impact on the Ministerial priority of improved hospital productivity. This will be achieved
119
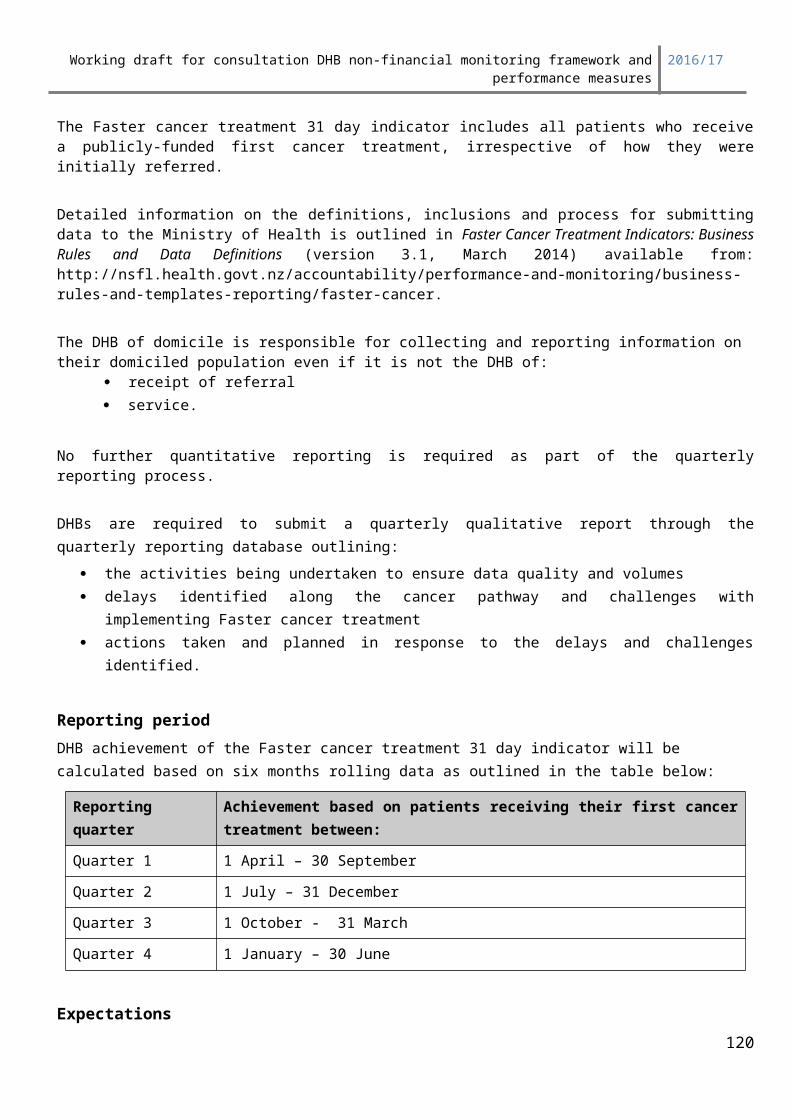
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
through freeing up beds and other resources so the DHB can both provide more elective surgery and reduce length of stay in the emergency department.
There is a need for DHBs to manage within a slower funding growth path and make demonstrable productivity improvements to offset cost pressures and to meet wider Crown expectations (i.e. maintain per capita service coverage, achieve national Health Targets, and eliminate DHB deficits). Shortening hospital length of stay will also help to delay infrastructure expansion and/or make savings that can assist in reducing DHBs’ deficits.
Addressing the factors that influence a patient’s length of stay in hospital will require the DHB to consider its performance on other measures, such as reducing readmissions, and increasing its integration activities that strengthen the ability of primary care to treat people more appropriately in the community. Supporting patients to return home sooner may, in part, be achieved by reducing the rate of patient complications and better use of the time clinical staff spend with patients. Patients will also be less at risk of contracting nosocomial (or hospital-acquired) infections. Through these actions, the DHB will contribute to an improved patient experience.
Actions and activities that have a proven impact on this measure:The following actions and activities are examples of initiatives that have a proven impact on this measure:
Implementing programmes such as The Productive Ward – Releasing Time to Care or Optimising the Patient Journey which focus on improving ward processes and environments to help nurses and therapists spend more time on patient care, thereby improving safety and efficiency
Process mapping and/or service redesign to improve the patient journey, reduce “waste” and improve primary care’s access to services
Improving rates of day of surgery admissions (DOSA) for elective patients Improving pre-admission programmes for elective patients
Deliverables definitionsEach DHB will report against two ALOS measures – Part One: Elective surgical inpatient ALOSPart Two: Acute inpatient ALOS Both Part One and Part Two of the measure are calculated using information held in the National Minimum Data Set (NMDS), and do not require a separate DHB data submission.
Description:The standardised ALOS is the ratio of ‘observed’ (actual) to ‘predicted’ ALOS, multiplied by the nationwide inpatient ALOS.
The length of stay calculation includes day case events, and joins multiple discharge events where The events have the same NHI The events have the same DHB of Service The prior event ends in a transfer There is less than 24 hours between the end of one event and the start of the next event
Where multiple discharge events are joined, the admission type for the stay is the admission type of the first event. In the rest of this document:
An elective discharge is defined as a stay where the first or only event in the stay is elective An acute discharge is defined as a stay where the first or only event in the stay is acute
120
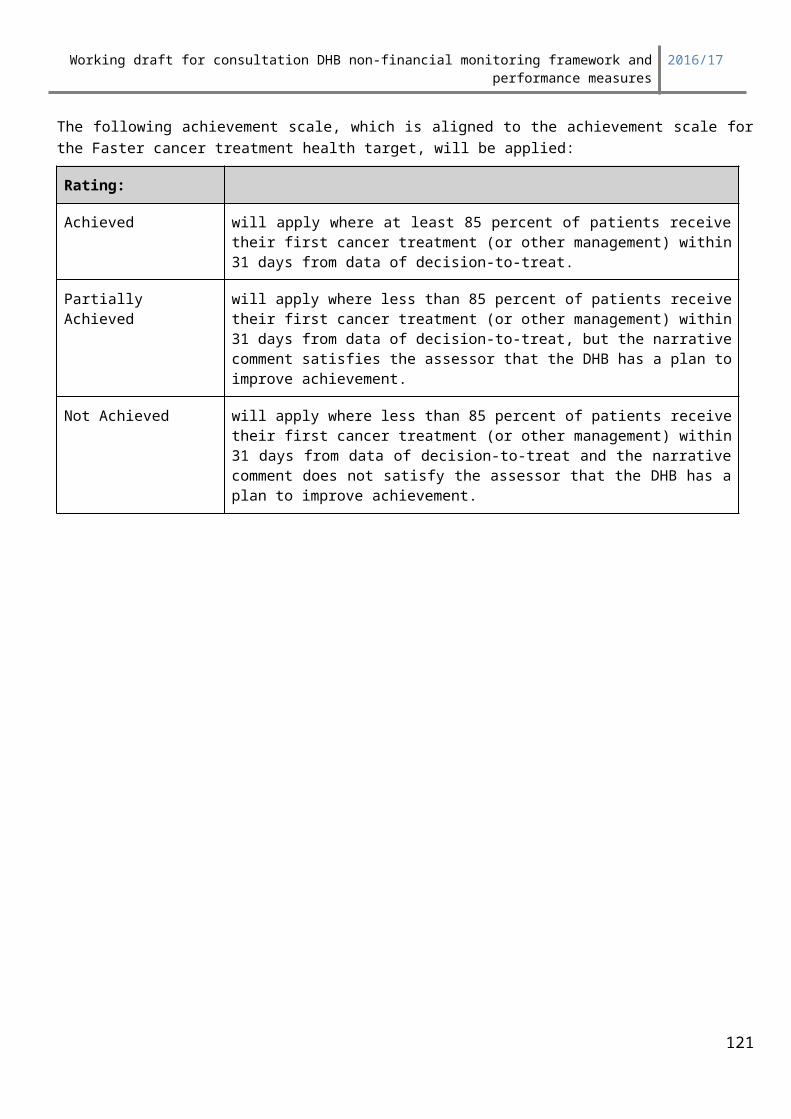
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Other linking criteria are included in the Appendix 1: Technical Specifications1. Elective surgical inpatient average length of stay:
Quantitative Indicator
The standardised ALOS for inpatient discharges in a surgical specialty with an elective admission type, expressed as the ratio of the observed to predicted ALOS, multiplied by the nationwide elective surgical inpatient ALOS.
The DHB observed ALOS, and the nationwide elective surgical inpatient ALOS, are both defined as the total bed days for elective surgical inpatients discharged during the 12 months to the end of the quarter, divided by the total number of discharges for elective surgical inpatients during the 12 months to the end of the quarter.
The predicted ALOS is derived by taking the nation-wide ALOS for each grouping of patient discharges, defined by DRG cluster and complexity group, multiplying this by the proportion of total discharges this group represents, and summing the result across all discharge groups. A contingency table is used to provide the ALOS across all DHBs for each DRG and complexity group. This information is then used to calculate the standardised ALOS for the casemix DRGs within each DHB.
Exclusions:• where the first event in the stay doesn't have a valid DHB of service e.g. is missing• where every event in the stay is non-casemix• where the first event in the stay is not Elective• where the purchaser of the first event in the stay is not in a set list• where the stay is Elective and no event has a surgical purchase unit (ie the purchase unit code does
not start with “S”• where the last event in the stay ended in a transfer
The purchase unit codes for the measure are included in Appendix 1: Technical Specification.
ExpectationsDHBs will be supplied with comparative baseline data for the twelve months to September 2014 showing performance relative to other DHBs.
The suggested target is tbc days, which represents the 75th centile of national performance.
For any DHB that is already achieving an elective surgical inpatient ALOS of tbc days or less in their baseline result (derived from the baseline data), a target that maintains their current performance or represents a modest improvement is suggested.
The Ministry will assume that 25 percent of the improvement towards target can be made each quarter, unless the DHB specifies otherwise.
Where the DHB is not achieving in line with the target, the DHB should provide information about any factors that are thought to be hindering achievement, and any actions being taken to gain improvements.
121
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Reporting PeriodReported quarterly. Due to the reliance on NMDS data (where the deadline for submission is about one month after the end of the quarter), the data used to derive this measure will be for one quarter in arrears.
122
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Rating for Elective ALOS measureA separate performance rating will be applied for each expectation within this performance measure, i.e. the Elective Surgical Inpatient ALOS and the Acute Inpatient ALOS expectations.
The following achievement scale will be applied for the Elective Surgical Inpatient ALOS measure:
Rating:Achieved The DHB has achieved their agreed elective surgical inpatient ALOS target
for the quarter
Partial Achievement The DHB has not achieved the agreed target for the quarter, but has demonstrated an adequate work-out plan to reach the target by year-end.
Not Achieved The agreed ALOS target for the quarter has not been achieved, and the DHB has not demonstrated an adequate work-out plan to reach the target by year-end.
2. Acute inpatient ALOS:
Quantitative Indicator The standardised ALOS for acute discharges in any medical or surgical specialty, expressed as the ratio of the observed (actual) to predicted ALOS, multiplied by the nationwide acute inpatient ALOS.
The DHB observed ALOS, and the nationwide acute inpatient ALOS, are both defined as the total bed days for acute medical or surgical inpatients discharged during the 12 months to the end of the quarter, divided by the total number of discharges for acute inpatients during the 12 months to the end of the quarter.
The predicted ALOS is derived by taking the nation-wide ALOS for each grouping of acute medical or surgical patient discharges, defined by DRG cluster and complexity group, multiplying this by the proportion of total discharges this group represents, and summing the result across all discharge groups.
Exclusions: • where the first event in the stay doesn't have a valid DHB of service e.g. is missing• where every event in the stay is non-casemix • where the first event in the stay is not acute • where the purchaser of the first event in the stay is not in a set list• where the last event in the stay ended in a transfer.
ExpectationsDHBs will be supplied with comparative baseline data showing their performance relative to other DHBs.
The suggested target for 2016/17 is TBC days, which represents the 75th quartile of national performance.
For any DHB that is already achieving an acute inpatient ALOS of TBC days or less in their baseline data, a target that maintains their current performance or represents a modest improvement is suggested.
The Ministry will assume that 25 percent of the improvement towards target can be made each quarter, unless the DHB specifies otherwise.
123
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Where the DHB is not achieving in line with the target, the DHB should provide information about any factors that are thought to be hindering achievement, and any actions being taken to gain improvements.
Reporting PeriodReported quarterly. Due to the reliance on NMDS data (where the deadline for submission is about one month after the end of the quarter), the data used to derive this measure will be for one quarter in arrears.
Performance Rating for ALOS measuresA separate performance rating will be applied for each expectation within this performance measure, i.e. the Elective Surgical Inpatient ALOS and the Acute Inpatient ALOS expectations
The following achievement scale will be applied for the Acute Inpatient ALOS measure:
Rating:Achieved The DHB has achieved their agreed acute inpatient ALOS target for the
quarter
Partial Achievement The DHB has not achieved the agreed target for the quarter, but has demonstrated an adequate work-out plan to reach the target by year-end.
Not Achieved The agreed ALOS target for the quarter has not been achieved, and the DHB has not demonstrated an adequate work-out plan to reach the target by year-end.
124
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Appendix 1: Technical Specifications
WIES version:The most current version of WIES available at the time baseline data is run. For 2015/16 this is NZ WIES version tbc.
DHB of service:Hospital agency codes are used to derive DHB of service.Where the stay has multiple events, the DHB which provides the first event will be considered to be the DHB of Service WIES recognised private facilities are excluded.
Joining Discharge Events into StaysDischarge events are considered to be part of the same stay if:
The events have the same NHI The events have the same DHB of Service The prior event ends in a transfer There is less than 24 hours between the end of one event and the start of the next event
If an event starts before the end of a previous event with the same NHI, its start time is set to the end time of the prior event
If an event ends before the end of a previous event with the same NHI, its end time is set to the end time of the prior event
The quarter before the 12 month time period is also loaded to help detect long stays.
Only stays which end within the 12 month time period are included.
Determining Stay Information Where there is more than one discharge event in a stay, the following criteria are usedDHB of Services = the DHB that provided the first eventStart Date =; the earliest event start dateEnd Date = the latest event end dateAdmission Type = the admission type of the first discharge eventDRG = the DRG of the highest caseweight eventPCCL = the PCCL of the highest caseweight eventCaseweight = the sum of every events' caseweightLength of Stay = the sum of the duration (in hours) of every event in the stay
Calculating Length of Stay
Each discharge event's length is calculated, rounded to the closest half hour, then summed together. No adjustment is made for leave days. Non-casemix events have their length set to zero
125
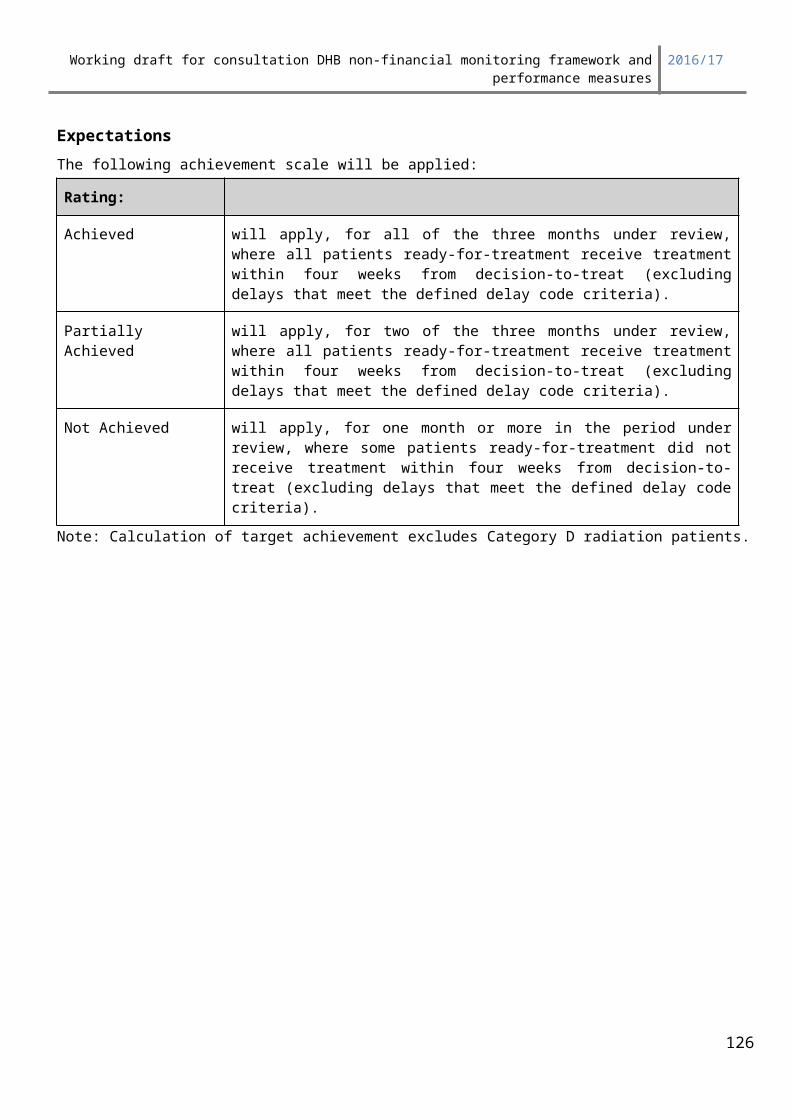
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Admission types: Where multiple discharge events are joined, the admission type for the stay is the admission type of the first event.
Elective surgical inpatient ALOS:
An elective discharge is defined as a stay where the first or only event in the stay has an admission type of:• AP – Private hospital elective admission• WN – Admitted from waiting list (Elective)
Acute inpatient ALOS:
An acute discharge is defined as a stay where the first or only event in the stay has an admission type of:
• AC – Acute• ZC – Acute, discontinued code
All other admission types, including arranged types, are excluded. Views from the sector are that while it is important to manage the length of stay for arranged admissions, inclusion of arranged admission type in either the acute or elective calculation can mask trends, and make the measures less useful. For this reason, arranged admissions are excluded from both calculations.
Principal health purchaser code:
The principal purchaser code for the first or only event in the stay must be in • 20 – Overseas eligible• 34 – MOH funded purchase• 35 – DHB funded purchase
Purchase units
Elective Surgical Inpatient ALOS:
S00001 General Surgery - Inpatient Services (DRGs)S05001 Anaesthesia Services (inpatient)S15001 Cardiothoracic - Inpatient Services (DRGs)S25001 Ear Nose and Throat - Inpatient Services (DRGs)S30001 Gynaecology - Inpatient Services (DRGs)S35001 Neurosurgery - Inpatient Services (DRGs)S40001 Ophthalmology - Inpatient Services (DRGs)S45001 Orthopaedics - Inpatient Services (DRGs)S55001 Paediatric Surgical Services (DRGs)S60001 Plastic & Burns - Inpatient Services (DRGs)S70001 Urology - Inpatient Services (DRGs)S75001 Vascular Surgery - Inpatient Services (DRGs)
Acute Inpatient ALOS:
All medical or surgical purchase units that are casemix included.
126
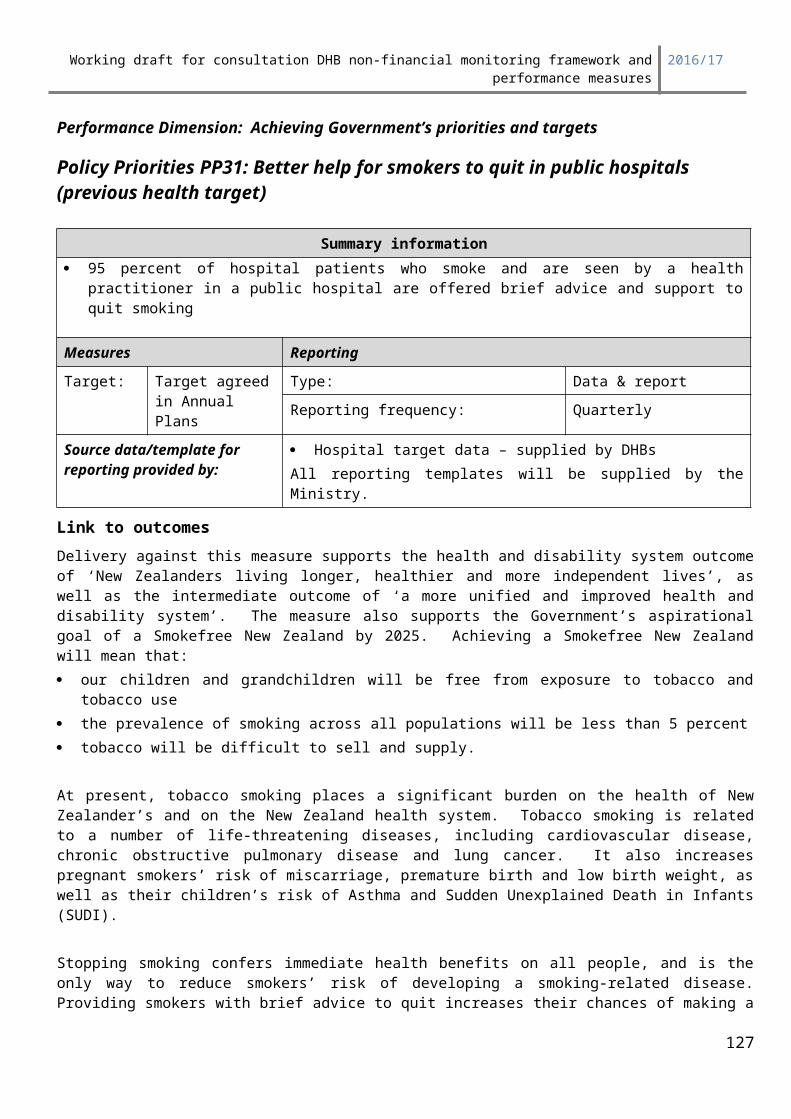
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
How the data is standardisedStandardisation is a process by which health delivery data is adjusted to take account of variations in the characteristics of different population or service delivery groups. This provides a basis for comparison for different populations or providers with different service mixes.
Often data is standardised by age, but data can be standardised by any characteristic that needs to be statistically controlled.
In deciding what variables to use to standardise the data, the effect of various factors such as sex, deprivation, age, ethnicity and rurality on ALOS were tested using regression methods. It was found that the only factors that had a statistically significant effect across all DRGs were admission type (acute or elective), and patient complexity and co-morbidity. Other factors have therefore been omitted from routine consideration.
ALOS is standardised to reflect differences in the type of service provision and is broken down into the following groups:
DRG cluster Patient Complexity and Comorbidity level (pccl)
The DRG cluster is the first three characters of the DRG code. The national ALOS is calculated by these groups using all DHB data for the relevant time period.
The individual DHB data is split by the same DRG cluster and pccl groupings so the record level DHB length of stay can be compared to the national DRG cluster and pccl grouping ALOS.
The data used for the ALOS calculation is:Stays - the number of inpatient stays by DHB meeting the ALOS criteria
Expressed mathematically:standardised ALOS
∑observed length of stayDHB ∑observed length of stayNational
∑ predicted length of stayDHB ∑staysNational
The predicted length of stay is calculated by creating a contingency table of DRG by Complication & Comorbidity Code.
A discharge group is defined by the combination of DRG cluster (first three characters of the DRG) and the pccl group. Standardisation by discharge group is carried out using a contingency table approach16.
The standardised ALOS adjusts for differences between the DHB observed length of stay and the predicted length of stay based on the mix of the services the DHB provides and the ALOS for each DRG cluster. This ratio is applied to the national rate to give a standardised rate.
This method of standardising means that the overall rate is not skewed by the relative proportion of data within each DHB DRG cluster group. All methods of standardisation need to be qualified in that they cannot control for or mitigate data quality or administrative practices.
161 In deciding what variables to use to standardise the data, the effect of various factors such as sex, deprivation, age, ethnicity and rurality on ALOS were tested using regression methods. It was found that the only factors that had a statistically significant effect across all DRGs were admission type (acute or elective), and patient complexity and co-morbidity. Other factors have therefore been omitted from routine consideration. .
127
X
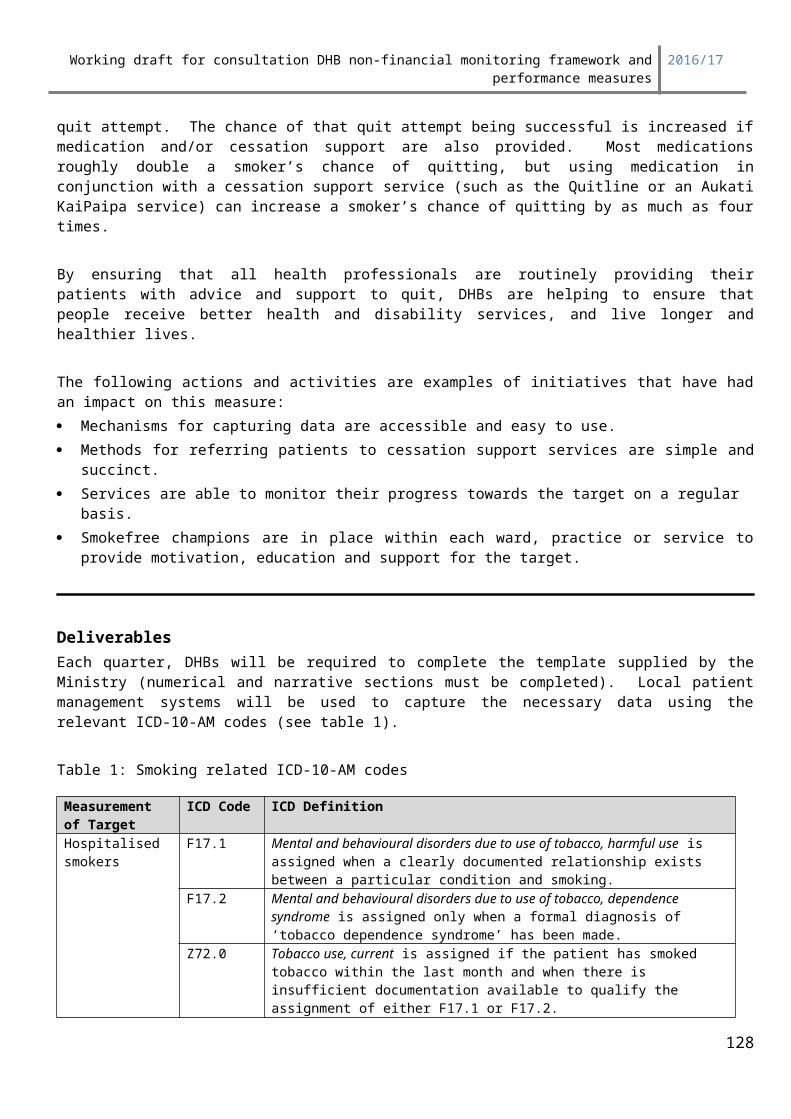
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: Providing quality services efficiently
Ownership OS8: Reducing Acute Readmissions to Hospital
The readmission model currently in use is based on work carried out in 1991, with some technical adjustments made in 1995/96.
A recent assessment suggests there is a need for review and re-development of the model. This work is currently underway with changes to the measure yet to be confirmed.
Summary informationTarget/performance expectation Reporting
Agreed in Annual Plan Type: Comprehensive measurement
Reporting frequency:
Quarterly
Source data/template for reporting provided by: Not applicable – data from NMDS
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care*
Improved quality, safety and experience of care(individuals and their family/ focus focus)
128
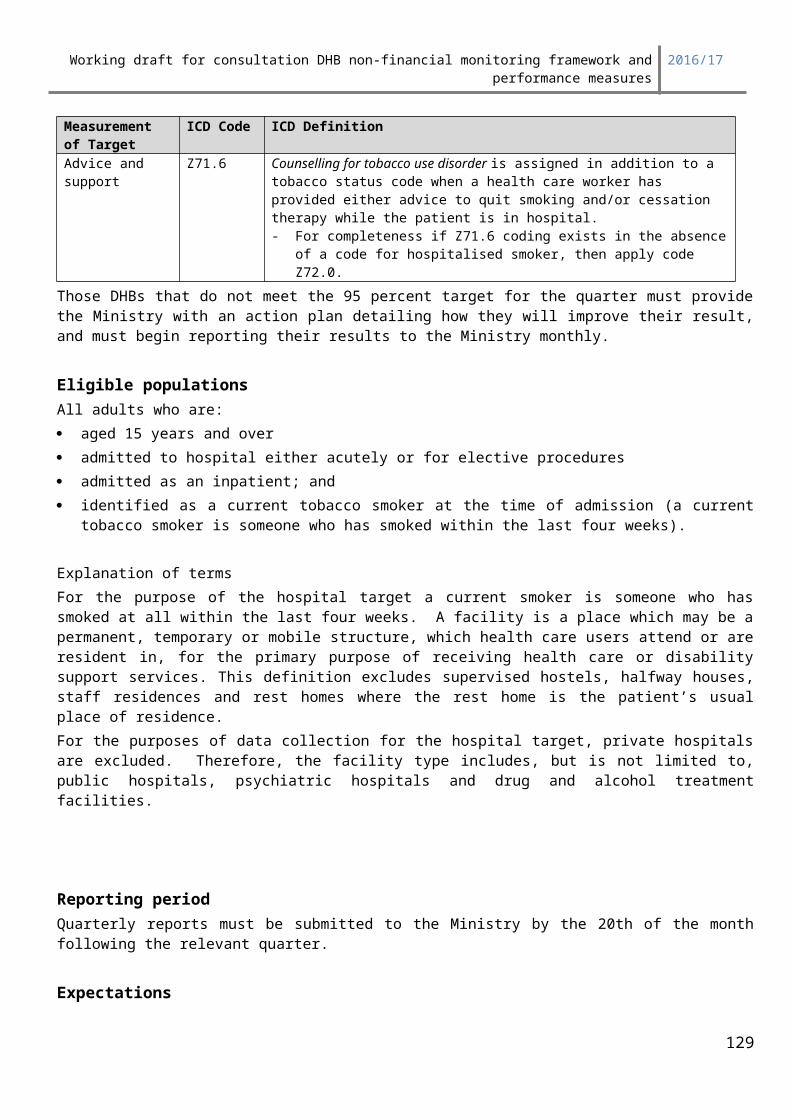
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child HealthOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
An unplanned acute hospital readmission may often (though not always) occur as a result of the care provided to the patient by the health system. Reducing unplanned acute admissions can therefore be interpreted as an indication of improving quality of acute care, in the hospital and/or primary care. , ensuring that people receive better health and disability services. Through the intermediate outcome that people receive better health and disability services, the measure contributes to the high level outcome of New Zealanders living longer, healthier and more independent lives while receiving better care closer to home.
Actions and activities that have a proven impact on this measure:The following actions and activities are examples of initiatives that have a proven impact on this measure: Focus on effective management of long term conditions Process mapping and redesign of patient pathways, particularly to improve primary care access
to services to diagnose and treat people in the community Initiatives to improve hospital discharge processes Appropriate integration between secondary and primary services to ensure continuity of care for
patients.
Deliverables definitions Ownership 8: Acute Readmissions to Hospital is calculated from information held in the National Minimum Data Set (NMDS), and does not require a separate DHB data submission.
The following admissions are excluded: Where the admissions is non-casemix Where the admission is for palliative care Where the DHB of service is unknown
The following readmissions are excluded: Where the readmission is non-acute Where the readmission is more than 28 days from the previous admission Where the readmission is within 24 hours and has a transfer flag Where the readmission matches a list of planned readmissions Where the readmission is a statistical readmission Where any previous admission ended in patient’s death
129
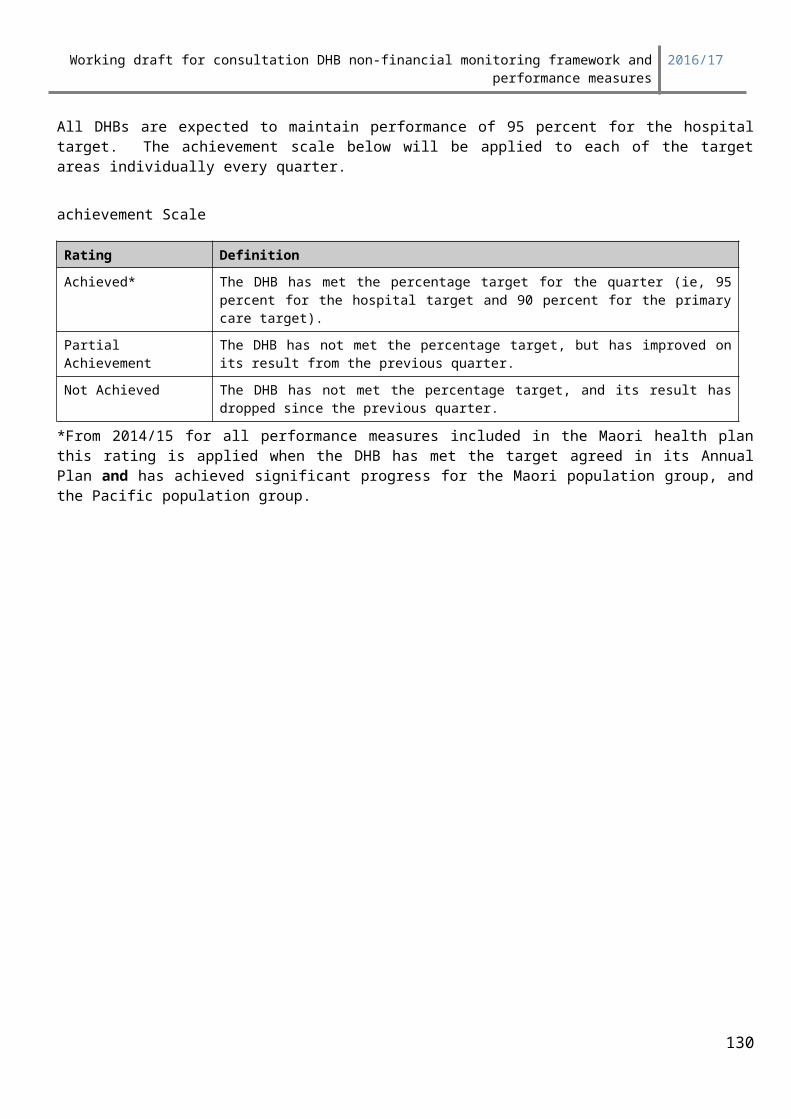
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Readmissions are grouped by the DHB of service. Where the admission and readmission occur in different DHBs, the readmission is counted toward the first DHB.
Ownership 8 provides both standardised and unstandardized acute readmission to hospital rates for each DHB. The standardised rate is calculated using a regression method, and is designed to control for differences in admissions to DHBs, i.e. ethnicity, age, complexity. The formula used to calculate it is:
Reporting PeriodReported quarterly. Due to the reliance on NMDS data (where the deadline for submission is 21 days after the end of the month of discharge), and due to the time lapse required in order to observe 28 day readmissions, this measure will operate using data that is one quarter in arrears.
ExpectationsDHBs will be supplied with comparative data on performance relative to other DHBs and suggested target ranges. There is some flexibility for DHBs to go outside suggested target ranges where DHBs can demonstrate this is in the interests of wider objectives. (As well as measuring DHB performance against target for the standardised measure, the target will be converted to an unstandardised rate to facilitate DHB measurement of performance between quarters.)
Please note: This definition and expectations also apply for over 75 readmissions
DHBs are to state their year-end target. The Ministry will assume that 25 percent of the improvement towards target can be made each quarter, unless the DHB specifies otherwise.
Where the DHB is not achieving in line with target, the DHB should provide information about any factors that are thought to be hindering achievement, and any actions being taken to gain improvements.
The following achievement scale will be applied:
Rating:Achieved The DHB achieves the agreed target for the quarter.
Partial Achievement The DHB has not achieved the agreed target for the quarter, but has demonstrated an adequate work-out plan to reach the target by year-end.
Not Achieved The agreed target for the quarter has not been achieved, and the DHB has not demonstrated an adequate work-out plan to reach the target by year-end.
For the final year-end assessment, a simple achieved/not achieved rating will apply.
130
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Ownership OS10: Improving the quality of identity data within the National Health Index (NHI) and data submitted to National Collections
Summary informationImproving the quality of identity data within the National Health Index (NHI) and event data submitted to the National Collections Systems (NCS).
Measures Reporting
Type: Output Type: Comprehensive measurement
Target: Pre-Set Reporting frequency: Quarterly
Source data/template for reporting provided by:
Data to be supplied by DHBs as required by the Operational Policy Framework (OPF)
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomesDelivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
131
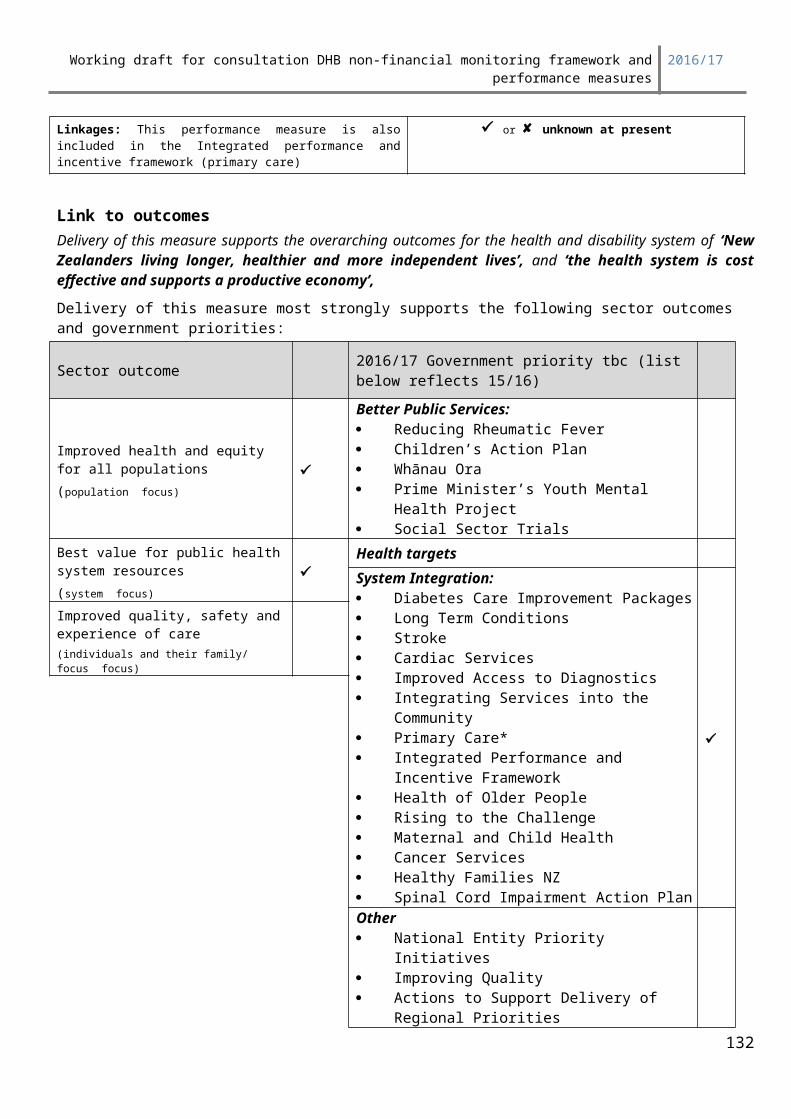
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
By ensuring the quality of the data it provides to the National Collections Systems, the DHB will impact the outcome of unifying and improving the health and disability system. Quality data supports good policy making, decision-making and planning. It also helps identify and address issues and improve services across the whole health and disability system through improving hospital productivity. This happens through DHBs sharing their information, and monitoring and analysis done by the Ministry of Health and health researchers.
DHBs are the primary data stewards of the NHI as the master ‘source of truth’ patient identity system used by all health providers. Ensuring that patient identity is correctly established, confirmed and maintained means that DHBs are able to accurately identify patients, and make sure clinicians can access all relevant health information, previous history and warnings and alerts for them. This means increased patient safety, leading to the health and disability system and services being trusted and used with confidence. It also means reduced duplication and consequent reduction of time and effort spent resolving duplicates to maintain unique identifiers.
Actions and activities that have a proven impact on this measure:Following are the actions and activities that have a proven impact on the indicators within this measure:NHI
New NHI registration in error (causing duplication): Users of the NHI interface must be fully trained in search and evaluation techniques and receive regular refresher training to maintain skills and knowledge. DHBs should provide feedback to individuals involved in instances of duplication detected by monitoring. Business processes should support users in establishment, confirmation and maintenance of identity – eg. use of forms for patients to record details. DHB subscribing Patient Management System (PMS) interfaces to the NHI must be compliant with relevant Standards and technical specifications at all times and present correct and meaningful warning and error messages.
Recording of non-specific ethnicity: Users of the NHI interface must be fully trained in ethnicity collection and recording processes as set out in the Ethnicity Data Protocols for the Health & Disability Sector. DHB’s should provide feedback to individuals involved in instances of recording non-specific values in either new registration or update of records. Business processes should support users in accurate collection and recording eg. use of the Standard ethnicity question, follow-up with a presenting patient to obtain specific ethnicity if a referral was received with no or non-specific ethnicity. DHB subscribing Patient Management System (PMS) interfaces to the NHI must be compliant with relevant Standards and technical specifications at all times.
Address validation quality: Users of the NHI interface must be fully trained in recording patient addresses in a way which validate against the Standard. DHBs should provide feedback to individuals involved in instances of poor quality addresses where validation should have been possible. Business processes should support users in accurate collection, recording and validation
132
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
of addresses. DHB subscribing Patient Management System (PMS) interfaces to the NHI must be compliant with relevant Standards and technical specifications at all times.
Invalid NHI data updates causing potential identity confusion (overlay): Users of the NHI interface must be fully trained in the process of confirming and maintaining patient identity information i.e. selection of the correct person/record and updates to existing data elements of name, DOB, gender or address. DHB’s should provide feedback to individuals involved in instances of updates to these data fields that are subsequently confirmed to be invalid. Business processes should support users in accurate collection and recording of data elements eg. seeking additional confirmation of a change in DOB. DHB subscribing Patient Management System (PMS) interfaces to the NHI must be compliant with relevant Standards and technical specifications at all times and present correct and meaningful warning and error messages.
National collections Standard versus edited diagnosis code descriptors in the NMDS. DHBs are monitoring the standard
versus edited descriptors for the specified range of diagnosis codes. They also encourage Clinical Coders to record more specific descriptors when referring to the clinical record. The Ministry continues to encourage DHBs to update their business processes so that accident and other information are made available to Clinical Coders to record in the diagnosis description fields.
Timeliness of NNPAC data: This is a new measure; however DHBs that are successful on this indicator have a data warehouse which holds data across all of their outpatient services. They will continually monitor data quality and update their records and have regular communication with other DHBs in their region.
NBRS events for exited treated patients match to NNPAC or NMDS events: DHBs that are successful on this indicator have integrated patient management systems for NBRS and outpatient and inpatient data. They use the data from both sources as part of their patient reporting and internal performance monitoring.
National Collections file load success rate: DHBs that are have a high file load success rate for NMDS, NBRS, NNPAC and PRIMHD data are those organisations that have built the business rules into their extracts. They also use the same data to monitor and report within their own organisations as they report to the national collections; thus any systemic data quality issues are identified before the information is provided to the Ministry of Health.
Deliverables definitionsThis measure has three parts as set out below:
Focus area 1: Improving the quality of identity data within the NHI
Focus area 2: Improving the quality of data submitted to National Collections
Focus area 1: Improving the quality of identity data within the NHIIndicator 1: New NHI registration in error (causing duplication)
Numerator: Number of new NHI registrations requiring subsequent linking by MOH per DHB per quarter. It excludes pre-allocated NHI numbers used, newborn NHI registrations and unidentified patient NHI registrations. It is cumulative across the quarter.
133
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Denominator: Total number of new NHI registrations per DHB per quarter (excluding pre-allocated NHI numbers, newborn registrations and unidentified patient NHI registrations).
Indicator 2: Recording of non-specific ethnicity in new NHI registration
Numerator: Total number of new NHI registrations with ethnicity recorded as ‘Not Stated’ (99) or ‘Response Unidentifiable’ (97) per DHB per quarter. It excludes pre-allocated NHI numbers used and unidentified patient NHI registrations. It is cumulative across the quarter.
Denominator: Total number of new NHI registrations per DHB per quarter (excluding pre-allocated NHI numbers, and unidentified patient NHI registrations)
Indicator 3: Update of specific ethnicity value in existing NHI record with a non-specific value
Numerator: Total number of updates to any ethnicity field in an existing NHI record with a non-specific value(‘Not Stated’ [99] or ‘Response Unidentifiable’ [97]) where a specific value existed in that field, per DHB per quarter
Denominator: Total number of NHI ethnicity updates per DHB per quarter
Indicator 4: Invalid NHI data updates
Numerator: Confirmed incorrect updates Denominator: Total number of queried updates
Reporting PeriodTo be reported quarterly.
134

Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
ExpectationsThe table below illustrates the Ministry’s expectations for each measure:
Rating
Not Achieved– Escalation Required
Partial Achievement Achieved
Outstanding Performer/ Sector
Leader
Mea
sure
1 New NHI registration in error (duplication)
SEE NOTE BELOW reA, B and C
A > 6% A>4% and <= 6% A
>2% and <= 4% A
<= 2%
B > 4% B>3% and <= 4% B
>1% and < =3% B
<=1%
C > 12% C>6% and <=12% C
>1.5% and<= 6% C
<= 1.5%
2 Recording of non-specific ethnicity in new NHI registration
Greater than 4%>2% and < or equal to 4%
>05% and < or equal to 2%
< or equal to 0.5%
3. Update of specific ethnicity value in existing NHI record with a non-specific value
Greater than 4%>2% and < or equal to 4%
>05% and < or equal to 2%
< or equal to 0.5%
4. Validated addresses excluding overseas, unknown and dot (.) in line 1
< or equal to 70%>70% and < or equal to 76%
>76% and < or equal to 85% Greater than 85%
5. Invalid NHI data updates
Still to be confirmed
NOTE: this indicator will not be
measured for at least Q1 and Q2
2014-15
Still to be confirmed
Still to be confirmed
Still to be confirmed
135
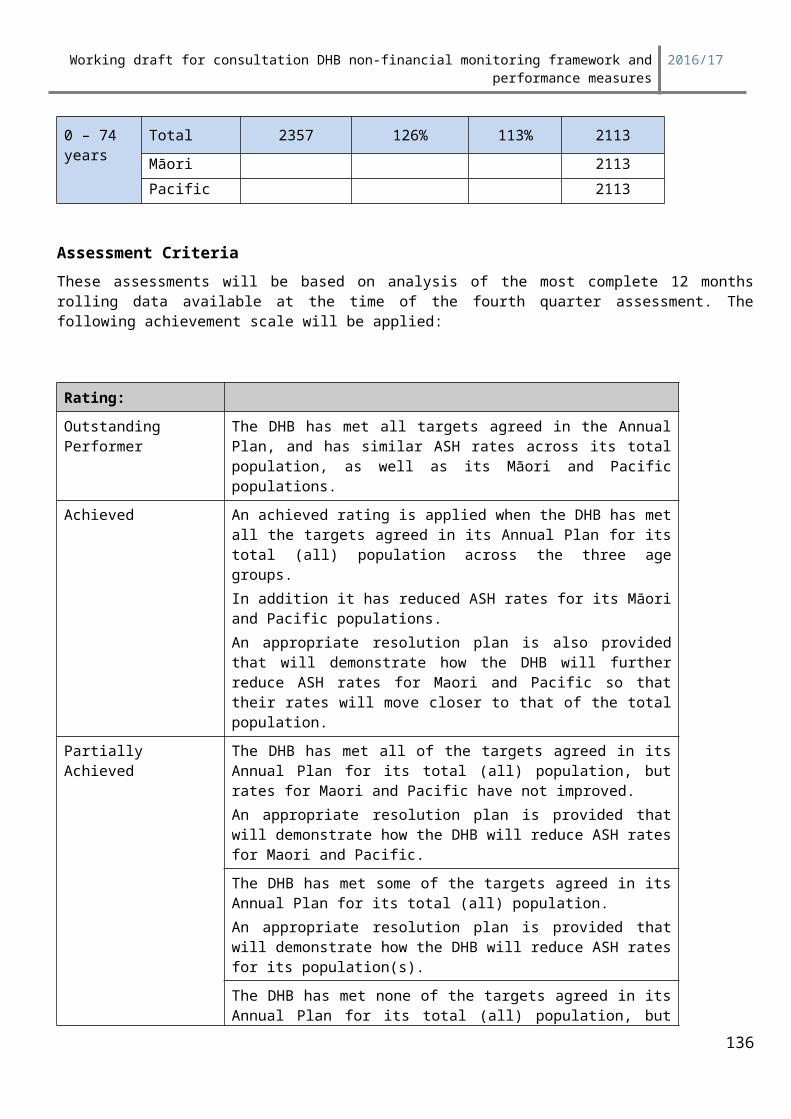
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
DHB’s have been split into 3 groups for measure 1 based on volumes of new registrations (this is to take into account the effect of small numbers on percentages to better reflect actual performance)
GROUP A GROUP B GROUP C
Auckland Bay of Plenty South Canterbury
Canterbury Hawkes Bay TairawhitiCapital and Coast Hutt Valley Wairarapa
Counties Manukau Lakes West Coast
Southern Mid Central Whanganui
Waikato Nelson MarlboroughWaitemata Northland
Taranaki
DHBs must provide explanations if ratings are ‘not achieved’ or ‘partially achieved’ and submit plans for improvement and/or remediation.
Focus area 2: Improving the quality of data Submitted to National Collections DHB results from production data reported to the national collections will be the basis for the initial assessments. All DHBs can provide feedback on their performance. This will inform the Ministry about data quality activities in the DHB and it will also be taken into account when assigning the final ratings. Description:National Collections and Reporting (Information Group, National Health Board) have developed a quarterly toolkit showing results for each DHB by measure.
Indicator 1: NBRS collection has accurate dates and links to NNPAC and NMDS.For all Exited Treated patients in the NBRS there is an event with the same procedure date in NMDS with matching PMS Unique ID or NNPAC with matching Client System Identifier.
Numerator: Total number of records reported as Treated Exited in NBRS where an event with the same procedure date exists in NMDS or NNPAC per DHB per quarter.
Denominator: Total number of records reported as Treated Exited in NBRS per DHB per quarter.
Indicator 2: National Collections File load SuccessNumerator: Number of PRIMHD, NMDS, NNPAC and NBRS records successfully
submitted per DHB per quarter.Denominator: Total number of PRIMHD, NMDS, NNPAC and NBRS records submitted per
DHB per quarter.Note: The rating for this measure will be an average of the rating across all 4 collections. A breakdown of the percentage and rating for each individual collection will be provided.
136
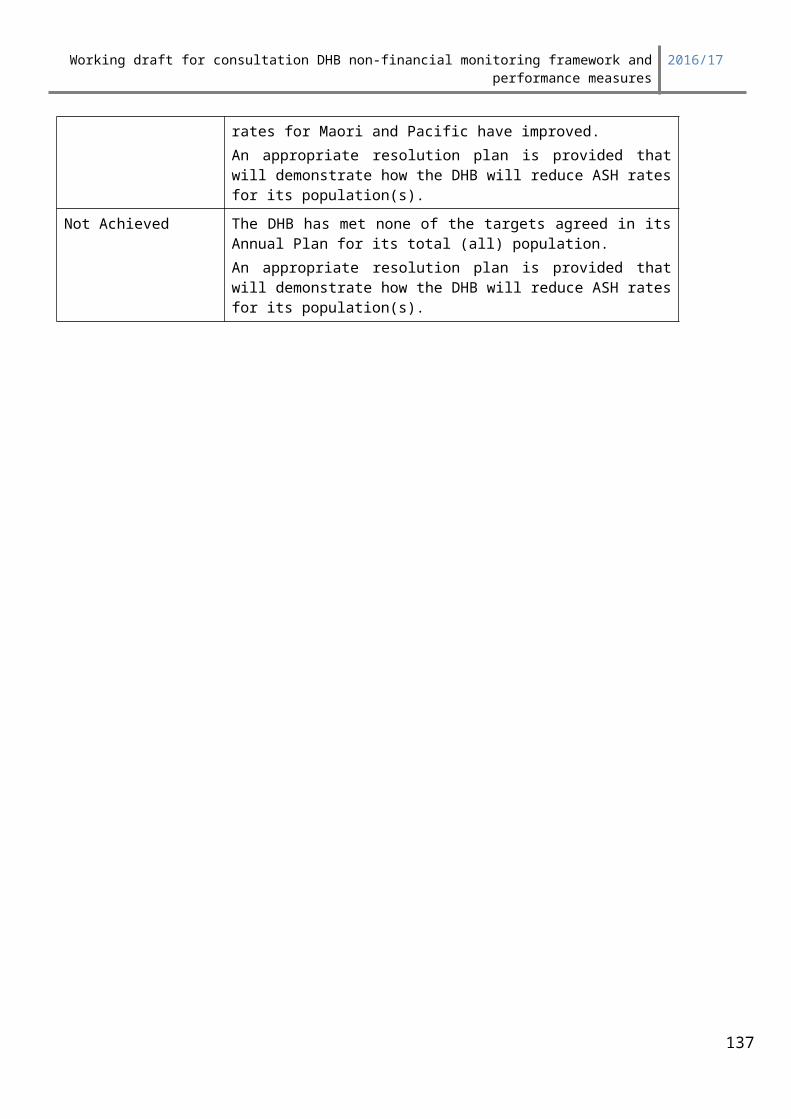
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Indictor 3: Standard versus edited diagnosis code descriptors in the National Minimum Data Set (NMDS)
Numerator: Number of edited text descriptors for specific diagnosis codes (M00 to M99, S00 to T98, U50 to Y98 (excluding U739, Y929, X59)) per DHB per quarter.
Denominator: Total number of specific diagnosis codes (M00 to M99, S00 to T98, U50 to Y98 (excluding U739, Y929, X59)) per DHB per quarter.
Note: Changes to the calculation of Measure 3 are expected after consultation with the sector in December 2015
Indicator 4: Timeliness of National Non-admitted Patient (NNPAC) dataNumerator: Total number of publicly funded NNPAC events loaded into the NNPAC
more than 20 days post month of discharge per DHB per quarter.Denominator: Total number of publicly funded NNPAC events in the NNPAC per DHB per
quarter.
This measure only applies to records reported for mandatory purchase units where the reporting requirements were published in the PUC Data Dictionary at the beginning of the financial yearNote: The date the individual record was loaded into NNPAC will be used to calculate this measure. In the instance that the Ministry is late to load a particular file, late records will be omitted from the figures.
Explanation of termsStandard versus Edited Descriptors: This measure refers to the distinction between the use of
standard text descriptors (as per ICD-10-AM and 3MTM
CodefinderTM) and edited text descriptors for specific diagnosis codes in the NMDS. Standard diagnosis code descriptors limit the usefulness of data, as they lack detail and specificity. DHBs are, therefore, encouraged to edit diagnosis code descriptors by adding detailed text extracted from the clinical record to improve the clarity and context of the information. This measure focuses on musculoskeletal diagnoses, injuries, poisonings and certain other consequences of external cause and external cause i.e. those in the range M00 to M99, S00 to T98 and U50 to Y98 (excluding U739, Y929, X59).
Note: Changes to the calculation of Measure 3 are expected after consultation with the sector in December 2015NBRS links to NNPAC and NMDS NBRS data is used to manage elective booking lists. The links between NBRS and NMDS/NNPAC provides high quality information about the surgeries that is consistent and robust, and also minimises risks of patients being accidentally exited without treatment. This ability to trace a patient’s episode across the national collections is central to developments in this area.
137
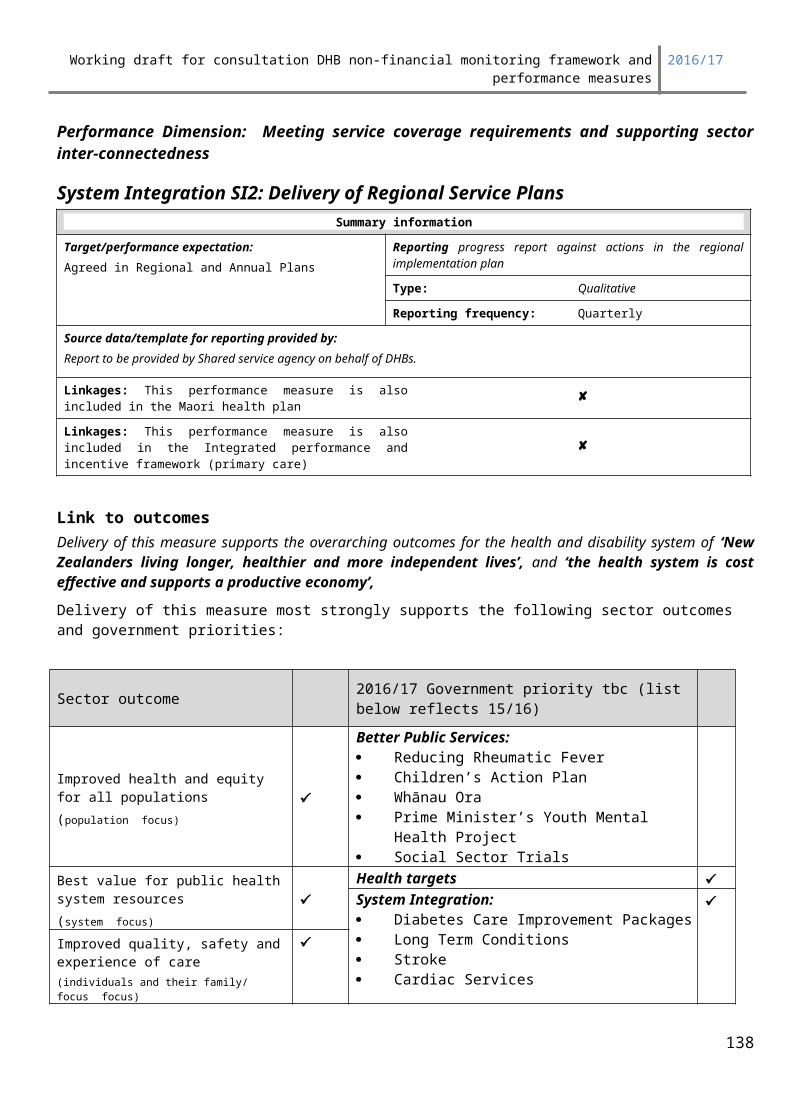
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Timeliness of NNPAC data: Calculated as the difference between the date a record is loaded into NNPAC and the date of service reported in the record. 20 days includes weekends and public holidays. This is the timeliness requirement signed up to in the Operational Policy Framework. Further several DHBs have been deleting their whole years NNPAC data and re-submitting it within days of the end of year wash-up. This measure is to allow users to have a measure of the consistency of the data in this collection.
National Collections File Success Rate This is the success rate of NNPAC, NMDS, NBRS and PRIMHD records submitted by the DHB in the quarter. DHBs are required to reach an high level to achieve compliance and this measure is to ensure that they continue to achieve a rate of 98% or above. Accurate file loading ensures that the national collections data is timely and complete.
DHBs should explain their improvement plans for where their ratings fall into the ‘not achieved’ or ‘partially achieved’ levels. Reporting PeriodTo be reported quarterly, with a toolkit placed on the Quickplace website.ExpectationsThe table below illustrates National Collections and Reporting’s expectations for each measure:
Rating
Not Achieved– Escalation Required
Partial Achievement Achieved
Outstanding Performer/
Sector Leader
Mea
sure
1 NBRS links to NNPAC and NMDS.
Less than95%
Greater than or equal to 95% and
less than 97 %
Greater than or equal to 97% and less than
99.5 %
Greater than or equal to 99.5%
2 National Collections File load Success
Less than95%
Greater than or equal to 95% and
less than 98 %
Greater than or equal to 98% and less than
99.5 %
Greater than or equal to 99.5%
3 Standard vs edited descriptors Less than 60%
Greater than or equal to 60% and
less than 75%
Greater than or equal to 75% and less than
90%
Greater than or equal to 90%
4 NNPACtimeliness Less than
85%
Greater than or equal to 85% and
less than 95 %
Greater than or equal to 95%
and less than 98 %
Greater than or equal to 98%
138
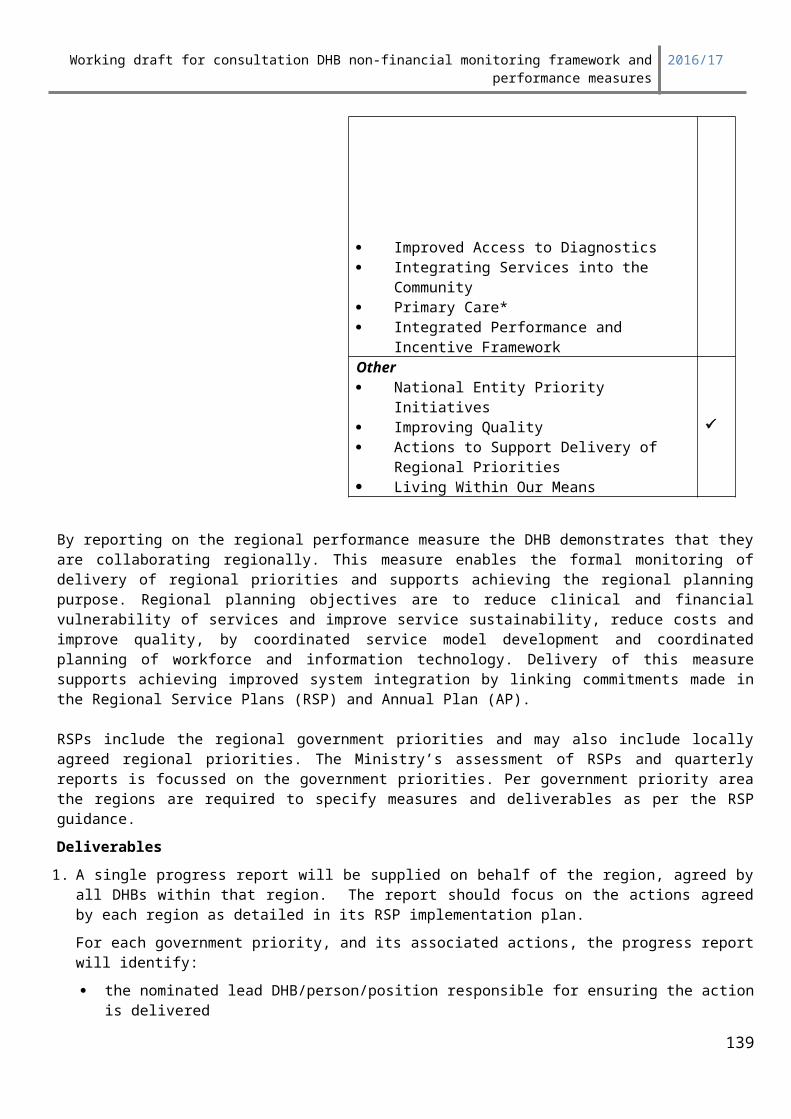
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Performance Dimension: purchasing the right mix and level of services within acceptable financial performance Output 1: Mental health output Delivery against Plan
Summary informationTarget/performance expectation:Agreed in Annual Plan (Production Plan)
Reporting
Type: Comprehensive measurement
Reporting frequency: Quarterly
Source data/template for reporting provided by:Mental Health area (for part B)Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Link to outcomes Delivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the Challenge Maternal and Child Health Cancer Services Healthy Families NZ Spinal Cord Impairment Action Plan
Improved quality, safety and experience of care(individuals and their family/ focus focus)
139
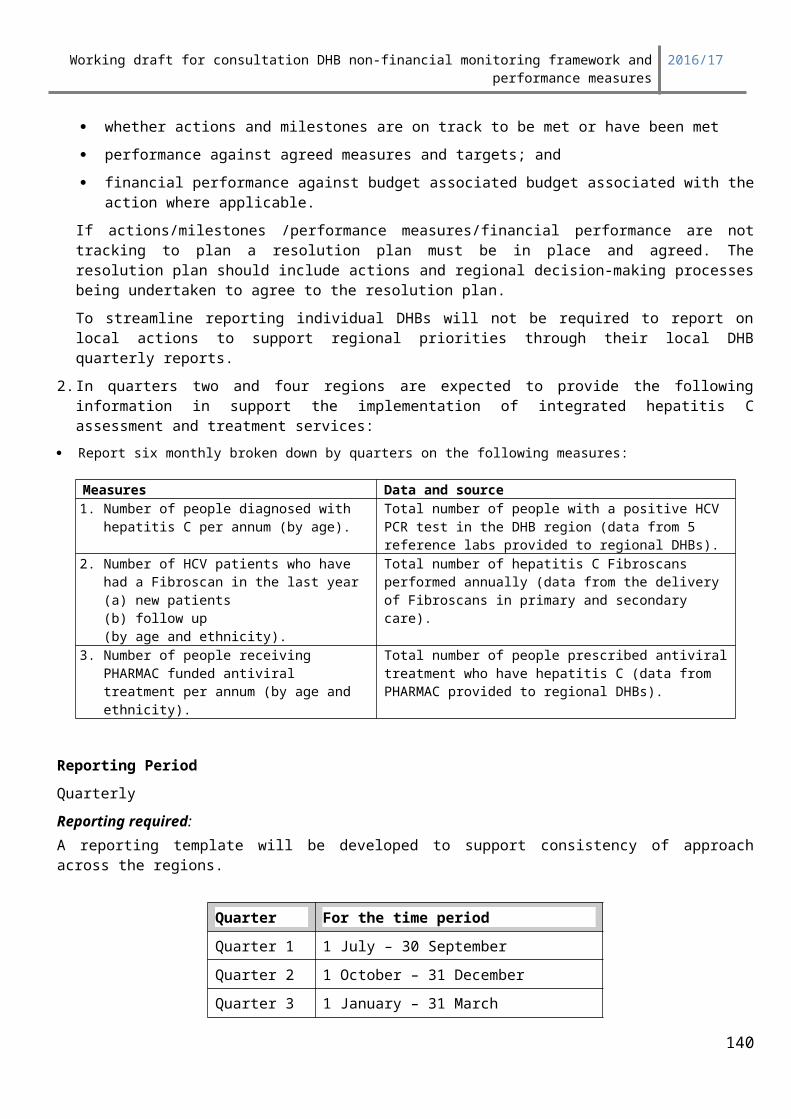
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Other National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Deliverables definitions
DescriptionEach DHB must monitor, evaluate and report on the delivery of Mental Health Services set out in its Annual Plan Production Plan.
For Mental Health Services provided by the DHB’s provider arm, the DHB must complete the Mental Health Volumes Reporting template. This will be provided by the Ministry, and included with the main quarterly reporting template.
Reporting PeriodReported quarterly.
Expectations
The following achievement scale will be applied:
Rating: DefinitionAchieved Volume delivery for specialist Mental Health and Addiction services is within:
a) five percent variance (+/-) of planned volumes for services measured by FTE,b) five percent variance (+/-) of a clinically safe occupancy rate of 85% for inpatient services measured by available bed day, andc) actual expenditure on the delivery of programmes or places is within 5% (+/-) of the year-to-date plan.
Partial Achievement Volume delivery is outside the bounds for an ‘Achieved’ rating and the accompanying exception reporting is satisfactory.
Not Achieved Volume delivery is outside the bounds for an ‘Achieved’ rating and the accompanying exception reporting is not satisfactory.
140
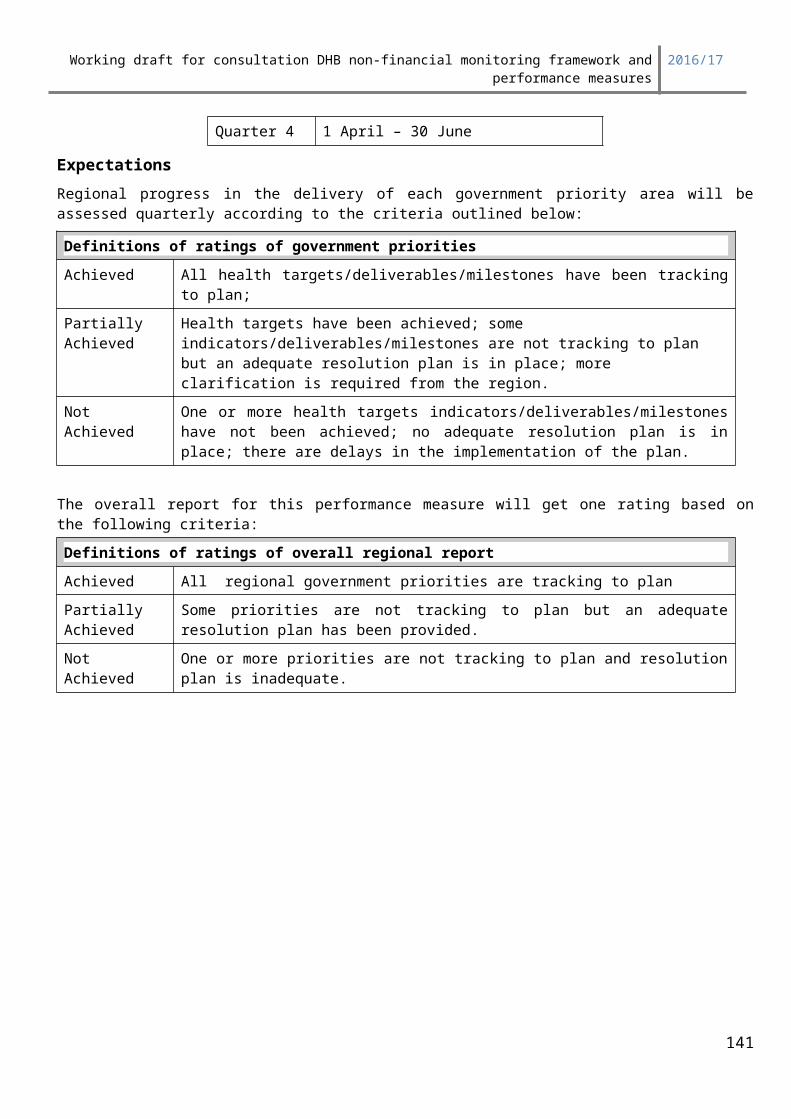
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Developmental measures DV4: Improving patient experienceSummary information
Implementing a national approach to collection, measurement and use of patient experience information.
Measures ReportingTarget: Provide patient experience data
and establish baselines for future target
Reporting frequency:
Quarterly
Source data/template for reporting provided by:
DHBs to supply data by either:- Submitting patient information to the
national survey provider (yet to be appointed) who will conduct the national patient experience survey and reporting on their behalf, or
- Providing completed national patient experience survey data to the national provider for incorporation in national reports.
Linkages: This performance measure is also included in the Maori health plan
Linkages: This performance measure is also included in the Integrated performance and incentive framework (primary care)
Signalled for future development
Link to outcomes Delivery of this measure supports the overarching outcomes for the health and disability system of ‘New Zealanders living longer, healthier and more independent lives’, and ‘the health system is cost effective and supports a productive economy’,Delivery of this measure most strongly supports the following sector outcomes and government priorities:
Sector outcome 2016/17 Government priority tbc (list below reflects 15/16)
Improved health and equity for all populations(population focus)
Better Public Services: Reducing Rheumatic Fever Children’s Action Plan Whānau Ora Prime Minister’s Youth Mental Health Project Social Sector Trials
Best value for public health system resources(system focus)
Health targetsSystem Integration: Diabetes Care Improvement Packages Long Term Conditions Stroke Cardiac Services Improved Access to Diagnostics
Improved quality, safety and experience of care(individuals and their family/ focus focus)
141
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
Integrating Services into the Community Primary Care* Integrated Performance and Incentive Framework Health of Older People Rising to the ChallengeOther National Entity Priority Initiatives Improving Quality Actions to Support Delivery of Regional Priorities Living Within Our Means
Patient experience data is an important performance indicator, and is vital in driving service improvements. However, New Zealand does not have a consistent national approach to collection, measurement and use of patient experience information.
Recent international opinion has shifted from measuring patient satisfaction to measuring the broader concept of patient experience. Furthermore, studies have shown that patient / consumer experience is a good indicator of the quality of health services, with patient experience positively correlated to processes of care for prevention, disease management, and with adherence to medical advice and treatment plans. Better experience, stronger partnerships with consumers, and patient and family-centred care have been linked to improved health, clinical, financial, service and satisfaction outcomes.
The focus on local needs for quality improvement is as important as consistent data for a national perspective. The indicators must be flexible enough to allow DHBs to plan and track local service-level improvements. They must be usable in DHB performance monitoring and accountability processes focused on hospitals, but also have more general application across the system, including in primary care.
Actions to deliver improved performance in this focus area:The information gathered at local and national levels through these measures can be used to benchmark patient experience across the country and to improve services locally. The indicators are collected via surveys completed by patients, carers and family/whānau.
The aim of the national programme is to develop:- a nationally consistent model of patient experience indicators incorporating four key domains
(communication, partnership, coordination, and physical and emotional needs) supported by additional questions
- a set of questions that can be incorporated in existing local patient experience surveys- adopting pre-existing and validated tools, where possible- an approach consistent with international best practice, to allow New Zealand data to be compared
with overseas results.
Deliverables definitions1. DHBs are expected to supply patient experience data according to the detailed information provided
in the requirements document published on the HQSC web site www.hqsc.govt.nz and the nationwide service framework library web site www.nsfl.govt.nz, that includes: the national patient experience survey
142
Working draft for consultation DHB non-financial monitoring framework and performance measures
2016/17
methodological rules (including sample size and timing) patient data extract file specification correspondence examples national reporting rules and timeframes.
2. Each quarter DHBs will supply a report via the DHB quarterly reporting process: confirming patient experience data has been supplied according to the requirements document confirming the DHB has delivered the patient experience actions and milestones identified in its
Annual Plan identifying any local survey management issues providing a resolution plan if it has not delivered to requirements or to plan for any survey
management issues identified.
Reporting Period DHBs will supply patient experience data and confirmation reports in line with the following quarters:
Quarter For the time period1 e.g.1 July – 30 September
2 e.g.1 October – 31 December
3 e.g.1 January – 31 March
4 e.g.1 April – 30 June
Further detail on timing of data supply is specified in the requirements document.
Quarterly survey reports at national and DHB level will be made available by the national survey provider two weeks following the end of the quarter. DHBs will be able to see other DHBs reports.
ExpectationsAll DHBs submit data for a sample group of patients on all the core survey questions. The Ministry of Health and Health Quality and Safety Commission expects that DHBs will make improvements in the quality of the data in each quarter enabling baselines to be set and future performance expectations to be developed.
DHBs are expected to include local patient experience information in their Quality Accounts.
Baseline information
To be established from 2014/15 and 2015/16 data reported.
143