Workbook and Examples of Innovative Services that might ... · 1 Workbook and Examples of...
44
1 Workbook and Examples of Innovative Services that might form part of the Acute Care Pathway January 2016
Transcript of Workbook and Examples of Innovative Services that might ... · 1 Workbook and Examples of...

1
Workbook
and
Examples of Innovative Services that
might form part of the
Acute Care Pathway
January 2016

2
3
1. Increasing the range of options for
people approaching a crisis

4
Host families offer an alternative to hospitalisation for people with mental health challenges who are experiencing a mental health crisis. Initially developed in USA, New Zealand, Australia and in other parts of Europe, Hertfordshire Partnership NHS Trust is pioneering a Host Families Scheme in the UK1 and was awarded the 2012 Health Service Journal Innovation in Mental Health Award for their Host Families Programme2. Host families are recruited within the local community and are trained/supported by mental health professionals.
They offer a short term (up to 3 weeks) supportive home environment to someone with mental health challenges who is in crisis and are paid £600 per week while they are hosting an individual3. Clinical support is provided by clinical staff from the Mental Health Trust Crisis and Home Treatment Team who visit daily and can respond when requested by the family. Host families provide a welcoming and friendly home environment: a less stigmatising, non-institutional alternative to hospital admission that focuses on providing the safety and support a person in crisis needs while maintaining local connections. They can also facilitate early discharge. Early indications from the first 42 people who have stayed with host families show good clinical outcomes and positive feedback from service users4. Host families may be particularly valuable in a more rural situation as they can enable people to remain in their local area as an alternative to admission to a hospital some distance from their home.
1 http://www.communitycare.co.uk/blogs/adult-care-blog/2012/03/adults-in-mental-distress-placed-with-families-to-avoid-
hospital/ 2 http://www.hsj.co.uk/Journals/2012/11/20/r/k/h/HSJAWARDS_121122.pdf 3 http://www.hpft.nhs.uk/_uploads/documents/leaflets/host-families-leaflet-2011.pdf 4 http://www.imroc.org/wp-content/uploads/Seminar-F-Nicodimos-Kamera-Compatibility-Mode.pdf
Increasing the range of
options for people
approaching a crisis
Host families

5
Notes
6
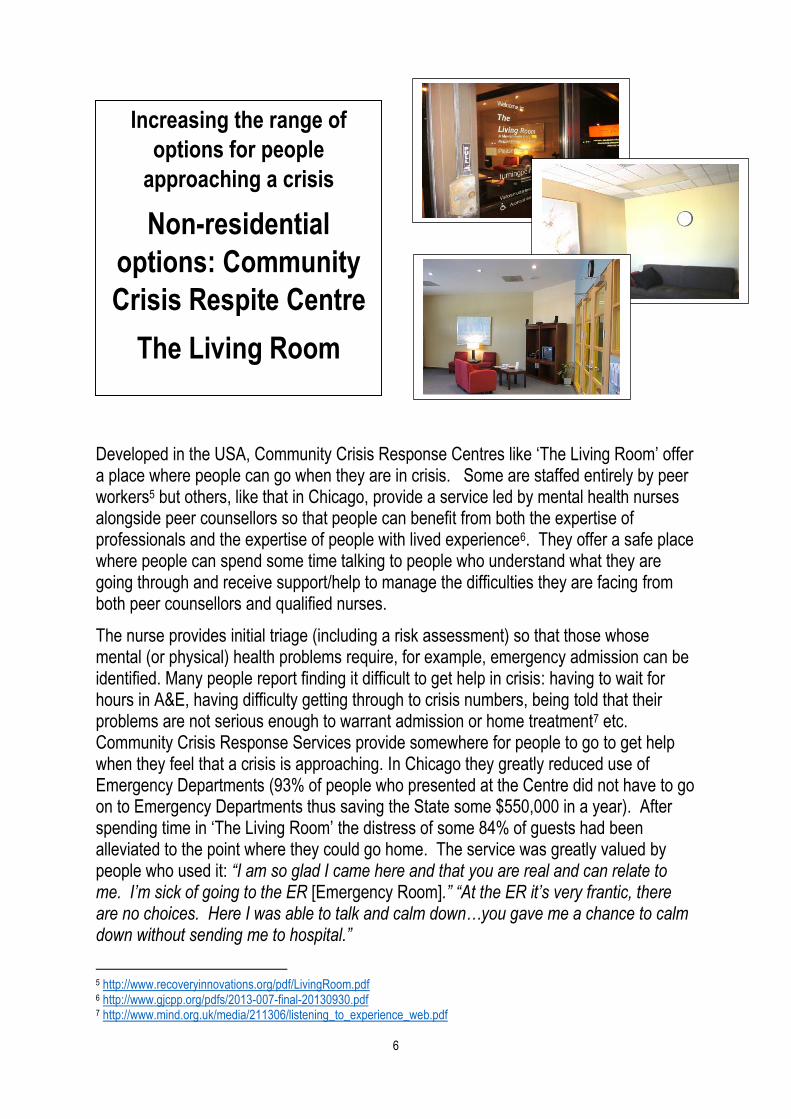
Developed in the USA, Community Crisis Response Centres like ‘The Living Room’ offer a place where people can go when they are in crisis. Some are staffed entirely by peer workers5 but others, like that in Chicago, provide a service led by mental health nurses alongside peer counsellors so that people can benefit from both the expertise of professionals and the expertise of people with lived experience6. They offer a safe place where people can spend some time talking to people who understand what they are going through and receive support/help to manage the difficulties they are facing from both peer counsellors and qualified nurses.
The nurse provides initial triage (including a risk assessment) so that those whose mental (or physical) health problems require, for example, emergency admission can be identified. Many people report finding it difficult to get help in crisis: having to wait for hours in A&E, having difficulty getting through to crisis numbers, being told that their problems are not serious enough to warrant admission or home treatment7 etc. Community Crisis Response Services provide somewhere for people to go to get help when they feel that a crisis is approaching. In Chicago they greatly reduced use of Emergency Departments (93% of people who presented at the Centre did not have to go on to Emergency Departments thus saving the State some $550,000 in a year). After spending time in ‘The Living Room’ the distress of some 84% of guests had been alleviated to the point where they could go home. The service was greatly valued by people who used it: “I am so glad I came here and that you are real and can relate to me. I’m sick of going to the ER [Emergency Room].” “At the ER it’s very frantic, there are no choices. Here I was able to talk and calm down…you gave me a chance to calm down without sending me to hospital.”
5 http://www.recoveryinnovations.org/pdf/LivingRoom.pdf 6 http://www.gjcpp.org/pdfs/2013-007-final-20130930.pdf 7 http://www.mind.org.uk/media/211306/listening_to_experience_web.pdf
Increasing the range of
options for people
approaching a crisis
Non-residential
options: Community
Crisis Respite Centre
The Living Room

7
Notes

8
Staffed by trained counsellors and counsellors in training, Leeds Survivor Led Crisis Service offers an ‘out of hours’ service for people in crisis8. Dial House, open from 6pm to 2am five nights per week (Friday to Monday and Wednesday including Christmas and bank holidays), takes a broad view of crisis: from worsening mental health problems to life crises such as relationship breakdown or losing your job. People call each evening to book themselves in for the evening; if necessary a taxi can be sent to provide transport. The 5 key elements of effective support are listening, treating people with warmth, kindness and respect; people do not feel judged or assessed; being in a different and calm environment and peer support9.
A telephone help-line – ‘Connect’, staffed by trained volunteers, is also available from 6pm to 10.30pm every night of the year. This help-line provides emotional support and information for people in distress: people in crisis, anxious, depressed, lonely … The aim is to provide non-judgemental, empathic support and information about other services if requested. It is also funded to provide emotional support to carers. In addition Dial House @ Touchstone provides a Crisis Service for people from BME groups on two evenings per week.
In 2014 214 people made 1474 visits to Dial House and 4392 people called the telephone help-line. Self-injury was a presenting issue in 46% of visits and suicide in 60%. Abuse (past or present) was a presenting issue in 59% of visits. The service has won a number of awards including the Guardian Public Services Award for Complex Needs and for Customer Service.
8 http://www.lslcs.org.uk/what-do-we-do 9 http://www.imroc.org/wp-content/uploads/Fiona-Venner.pdf
Increasing the range of
options for people
approaching a crisis
Non-residential
options: Leeds
Survivor Led Crisis
Service
When you’re desperate and feel you can’t cope, there is a place where you can talk to someone who’ll listen...

9
Notes

10
In Lambeth, Southwark and Lewisham, Solidarity in Crisis (operated by Certitude)
provides out of hours emotional support over the telephone and in person10. Co-
designed and co-delivered by service users and carers, the service is run by Peer
Supporters who have their own experience of facing and overcoming crises and receive
comprehensive training, supervision and support. Initially open only at weekends, the
service now provides out of hours support 7 days per week: 6pm to midnight Monday to
Friday and midday to midnight on Saturday and Sunday.
The aim of the service is to provide support for people in distress before they reach crisis
point and help guide them towards appropriate professional support as necessary. It
endeavours to reduce isolation out-of-hours by providing support that is respectful and
non-judgemental, using the empathy and knowledge gained through lived experience.
Peer Supporters provide crisis support over the telephone and through meetings in the
community (in mutually agreed public places) to help people move on from the acute
stage of their crisis. By sharing life experiences, Peer Supporters can promote recovery
and enhance feelings of belonging, especially for those who feel isolated. Solidarity in
Crisis receives calls from people who have a variety of different issues, for example,
social isolation/needing someone to talk to, relationship breakdown, bereavement, self-
harming, suicidal thoughts, overdose and support with benefits11. Highly valued by those
who use it, the service has, for some people, reduced admissions and use of Accident
and Emergency Services.
The service has been recognised as an example of good practice in London Mental
Health Crisis Commissioning case studies12.
10 http://www.certitude.org.uk/find-support/mental-health/services-we-offer/support-in-crisis/ 11 http://www.certitude.org.uk/wp-content/uploads/2013/06/SiaC-Report.pdf 12 http://www.crisiscareconcordat.org.uk/wp-content/uploads/2014/11/mh-urgent-commiss-cs-102014.pdf
Increasing the range of
options for people
approaching a crisis
Solidarity in Crisis:
Peer Support in Crisis

11
Notes

12
What options do we want in Dorset:
For people when things start to go
wrong and a crisis might be
looming?
When people are in crisis?

13
2. Personalising support for people in
a crisis

14
A substantial number of people have repeated mental health crises. A Joint Crisis Plan
enables the individual and services to learn from experience and make plans about what
to do in the event of another crisis. It is developed by seeking agreement between the
patient and their mental health team about what to do if they become unwell in the
future. It can include things like an individual the patient would like to have contacted in a
crisis; treatments that have been helpful or unhelpful in the past; treatment preferences
or refusals, and practical arrangements. Research demonstrates that Joint Crisis Plans
can significantly reduce compulsory detention and number of admissions13. They can
also reduce the risk of relapse via early intervention and, when they work well, are both
clinically useful and result in service users reporting improved therapeutic relationships
and more empowerment and control over their illness
However, it does appear to be important that Joint Crisis Plans are developed collaboratively, used effectively and form a core part of the team’s work – if poorly implemented they do not have the desired effect14. In the initial research trials an independent person – a facilitator – helped to balance the power relationship between the service user and their mental health professionals and promote a dialogue that encourages reflection, negotiation, and problem solving. It may not be possible to provide this for everyone using a busy mental health service. However, in South West London, they specifically focused on embedding and sustaining practices and identifying barriers to doing this. They focused on engaging care co-ordinators, making Collaborative Crisis Plans meaningful for them, integrating them with Care Planning, and producing materials to aid conversations between service users and staff: within one year approaching 80% of people on CPA and 50% of those not on CPA had a completed Collaborative Crisis Plan15.
13 Henderson, C. et al (2004) Effect of joint crisis plans on use of compulsory treatment in psychiatry: single blind randomised controlled trial, BMJ, doi:10.1136/bmj.38155.585046.63 (published 7 July 2004) https://www.researchgate.net/publication/8469589_Effect_of_joint_crisis_plans_on_use_of_compulsion_in_psychiatric_treatment_single_blind_RCT Flood, C. et al (2006) Joint crisis plans for people with psychosis: economic evaluation of a randomised controlled trial, BMJ, doi:10.1136/bmj.38929.653704.55 (published 16 August 2006) 14 http://www.imroc.org/wp-content/uploads/Claire-Henderson.pdf 15 http://www.healthcareconferencesuk.co.uk/news/newsfiles/miles-rinaldi_1208.pdf
Personalising support for
people in a crisis
Joint Crisis Plans

15
Notes

16
Evaluations of personal health budgets
(PHBs) clearly demonstrate significant
improvements in quality of life, choice and
control and psychological well-being and that
the greatest gains were achieved for people
with mental health conditions, learning
disabilities and younger people with physical
impairments. They also demonstrated that
Personal Health Budgets were most cost
effective for those with mental health
conditions and continuing healthcare, for
people with high-value personal budgets and
where budgets were used more flexibly16.
While limited progress has been made in the widespread use of personal health budgets in mental health, there are a number of examples where Personal Health Budgets have offered alternatives to hospitalisation or support that enables people to leave hospital much earlier. Some people have found hotels, ‘bed and breakfasts’ or retreats to be useful to alleviate crises. Indeed, use of hotels with support provided by the mental health team was a component of the original Maddison Assertive Community Treatment Team on which UK Assertive Outreach Teams were modelled17. Other people have received support at home during crisis from a Personal Assistant employed using a Personal Budget during a crisis. Typically, a person is allocated a set number of days in a hotel/retreat or a set number of hours of a PA each year which they can call upon when a crisis is looming. For example, one woman using an inner London mental health service had repeated short admissions in crisis. She did not find hospital helpful, but had no alternatives until she received a personal budget that allowed her to purchase up to 12 nights per year in a retreat outside London when she felt a crisis was looming. It is noteworthy that she never used all of her allocated 12 days. The cost of this was a small fraction of the cost of hospital admission and it was effective in preventing the need for hospitalisation for the ensuing two years.
Such alternatives may be supported by a Home Treatment Team who can provide clinical input and could usefully be combined with Joint Crisis Plans18. However, at present, the range of available options is limited (e.g. inpatient admission, home treatment, a crisis house) and early intervention at the first signs of a ‘relapse’ is often difficult: pressure on services means that both of these are usually restricted to those who are already in crisis, rather than as an early
16 https://www.phbe.org.uk/getFile.php?id=report 17 Stein, L.I. & M.A. Test. (1980). Alternative to Mental Hospital Treatment Conceptual Model,
Treatment Program, and Clinical Evaluation. Archives of General Psychiatry, 37, 392-397 18 Henderson, C. et al (2004) Effect of joint crisis plans on use of compulsory treatment in psychiatry:
single blind randomised controlled trial, BMJ, doi:10.1136/bmj.38155.585046.63 (published 7 July 2004)https://www.researchgate.net/publication/8469589_Effect_of_joint_crisis_plans_on_use_of_compulsion_in_psyc
hiatric_treatment_single_blind_RCT
Personalising support for
people in a crisis
Personal Health
Budgets

17
intervention to prevent the build-up of a crisis once warning signs are identified. Personal health budgets, in conjunction with Joint Crisis Plans could offer a genuinely personalised range of supports and the possibility of intervening early to obviate the need for hospital admission. There may also be a role for personal budgets in maintaining community links and facilitating early discharge (e.g. paying for transport so people can visit the local area and re-establish relationships during admission or paying for transport so relatives and friends can visit).
Personal budgets offer the opportunity for more personalised support in crisis that might be particularly targeted on those who make highest use of inpatient services, often on a compulsory basis: a small number of people typically use a disproportionate number of available bed days.
A personal health budget is an amount of money to support your identified health and wellbeing needs,
planned and agreed between you and your local NHS team. The aim is to give people with long-term
conditions and disabilities greater choice and control over the healthcare and support they receive.
Money can be managed in three ways:
A notional budget managed by statutory services
A third party manages the budget : an independent voluntary organisation or an individual (relative, friend ...) manages the money for the person and buys what they need
A direct payment: the money is transferred to the person and they buy goods and services themselves. An independent direct payment support agency (e.g. Independent Living Centre) may help the person to manage their direct payment
For more information see Paths to Personalisation in Mental Health
http://www.ndti.org.uk/uploads/files/New_Paths_to_Personalisatio
n_%28NDTi,_April_2013%29.pdf
Mind Guide to Personal Budgets for Social Care:
http://www.mind.org.uk/information-support/guides-to-support-
and-services/personal-budgets/#.VTEhbpNWvgQ
Choice Control and Recovery, Mental Health Foundation
http://www.mentalhealth.org.uk/content/assets/PDF/publications/c
hoice_control_recovery.pdf?view=Standard

18
Notes
19
How can we personalise crisis
support in Dorset?
20
3. Increasing the range of support in
the community to promote recovery
and prevent crisis

21
Since 1990 the term ‘Care Programme Approach (CPA)’ has been used to describe the
framework that supports and co-ordinates effective mental health care for people with
severe mental health problems in secondary mental health services. Responsibility for
care co-ordination traditionally rests within secondary mental health services and has
been conducted by trained clinicians. CPA Care plans cover not only clinical treatment
and interventions, but also social support that the person may require. However, after 25
years, the results are less than impressive.
“Not only is the evidence about the fundamental effectiveness of case management
equivocal at best, but the CPA is viewed as being excessively bureaucratic and as
effectively turning skilled clinicians into administrators. Perhaps the most damming
critique is that most patients and their families are not even aware what the CPA is.” (Centre for Social Justice Report on Mental Health, 2011)19
It is questionable whether, given the shortage of trained professionals, professional
time is best used in the task of co-ordinating the provision of treatment and therapy
rather than providing it.
The effectiveness of existing mechanisms is also questionable. The 2015 Care
Quality Commission Community Mental Health Survey20 showed that only 42% of
service users knew the plan for their treatment and care and only 55% were as
involved as they wanted to be in decisions about treatment and therapies. Further, a
large proportion said they did not receive the social support they needed:
19 http://www.centreforsocialjustice.org.uk/published-policy/mental-health 20 http://www.cqc.org.uk/sites/default/files/20151020_mh15_statistical_release.pdf
Increasing the range of
support in the community to
promote recovery and prevent
crisis
Clinical and Social
Support:
Care Co-ordinators and
Personal Navigators

22
43% would have liked help with accommodation but did not get it
43% would have liked financial advice or help with benefits but did not get it
47% would have liked help with finding/keeping work but did not get it
42% would have liked support to take part in an activity locally but did not get it
If care co-ordination and care planning are located within secondary, specialist,
mental health services then these are lost when the person is discharged to Primary
Care. There is also an increasing emphasis on the role of Primary Care in the
treatment of people with mental health conditions, both ‘common’ and ‘severe’.
Typically it is expected that people will not spend long periods of time in the care of
secondary mental health services but, as with physical health challenges, when
people are ‘clinically stable’ they are typically discharged to Primary Care. However,
being clinically stable does not mean that people do not have needs for social
support, nor that they are able to navigate life and services, or reconnect if their
condition deteriorates. Support is required after people have left secondary services
if recovery is to be promoted and crises, relapse and readmission are to be
minimised.
Such considerations have led to the development of a range of ‘navigator’ roles in
relation to a range of long term health conditions – including mental health2122. Usually
employed within the voluntary sector, such personal ‘navigators’ build relationships with
people and help them to solve problems and locate resources and opportunities that
promote recovery, inclusion and well-being. They also help people to navigate and
access the range of health care services the person may need. Based in community
settings they can span primary and secondary care and continue to support people who
need ongoing assistance to navigate life, communities and services after discharge from
specialist mental health treatment services. Some specifically focus on providing peer
support by employing people with their own lived experience23.
Examples of ‘personal navigator’ type services:
The Evolve Navigator Service in Waltham Forrest24 provides 12 – 18 months support from a designated navigator to adults with serious mental health challenges in their discharge from secondary to primary care. Provided by a local
21 http://www.londonhp.nhs.uk/wp-content/uploads/2012/10/12-08-21-Navigator-role-in-mental-health-models-of-care-legacy-final.pdf 22 http://www.hsj.co.uk/topics/integration/safer-passage-how-care-navigators-help-improve-mental-health-
services/5041420.fullarticle
http://lambethcollaborative.org.uk/about/our-service-model
http://www.turning-point.co.uk/community-commissioning/connected-care/projects/connected-care-in-hartlepool.aspx
http://bristolmentalhealth.org/media/654252/november-2014-newsletter.pdf 23 http://vancouver-fraser.cmha.bc.ca/how-we-can-help/adults-and-seniors/peer-navigator-program
https://www.tynesidemind.org.uk/.../peer-navigator-role-specification 24 http://www.slcsn.nhs.uk/scn/mental-health/mh-urgent-commiss-cs-102014.pdf http://www.healthwatch.co.uk/sites/healthwatch.co.uk/files/170715_healthwatch_special_inquiry_2015_1.pdf

23
voluntary organisation – CREST – personal navigators adopt a person-centred recovery focus (including encouraging people to develop Wellness Recovery Action Plans) in supporting people to decrease social isolation and access a range of local opportunities/services. They also ensure that people attend appointments with their GP/practice nurses to monitor their physical and mental health and gain additional support in crisis. By building relationships, they are able to identify early signs of mental health crisis and help prevent relapse. If someone does enter a period of crisis they receive increased contact with their navigator who can arrange re-referral, urgent out-patient appointments and development of a recovery plan. Outcomes of the pilot showed an overall reduction in crises where regular contact with the navigator is maintained. There have also been reductions in the duration of crisis episodes and the time spent by individuals in secondary care.
In South Australia, navigators in the form of peer support workers provide support to facilitate early discharge from hospital and prevent re-admission. All of the peer workers have their own experience of hospital admission as well as prior experience (paid or unpaid) of providing support. They meet people prior to discharge and agree an individualised package of support to be provided on discharge from hospital. ‘Hospital avoidance support’ can also be provided for those who are at risk of being admitted. The emotional and practical support offered can include phone calls, information about services and opportunities, home visits, accompanying the person to their GP or other appointments and activities, linking with community supports, help to develop relapse prevention and self-management strategies and information and support for relatives and carers. Research showed that, within 3 months, 49 support packages saved 300 bed days and feedback from all stakeholders (service users, mental health staff, carers, GPs and peer support workers) was overwhelmingly positive25.
More generally, working together with mental health professionals, ‘personal navigator’
roles within the voluntary sector could allow mental health professionals to focus on the
provision of treatment and therapy leaving more co-ordination of treatment and support
to navigators. Navigators could enable people to access these professionals as well as
other services and supports (including personal budgets) they may need and provide the
recovery-focused social support some people need to make the most of their lives. They
could also continue to provide this when people have left services. It should be noted
that, in the original case-management services developed in the USA, care managers
were not qualified professionals but people (some peers) specifically trained to perform
this function26.
25 http://www.tandfonline.com/doi/abs/10.1080/09638230701530242 26 http://www.oxfordbibliographies.com/view/document/obo-9780195389678/obo-9780195389678-0096.xml

24
Notes
Stein, L.I. & M.A. Test. (1980). Alternative to Mental Hospital Treatment Conceptual Model, Treatment Program, and Clinical
Evaluation. Archives of General Psychiatry, 37, 392-397

25
How can we provide individuals with
the clinical and social support they
need AND improve continuity and
communication?

26
Personal budgets can be an important tool in promoting recovery27. A personal budget is
an allocation of social care or NHS resources or an integrated allocation of both that is
controlled by an individual and can be used to meet identified goals: personal budgets
(PBs) in social care and personal health budgets (PHBs) in the NHS can help embed
and enhance recovery-oriented practice. If people have effective support tailored to their
preferences, aspirations and needs, evidence suggests that admissions can be reduced
and thus the cost of care decreased28 (Alakeson and Mycawka, 2014):
27 http://www.centreformentalhealth.org.uk/recovery-personalisation 28 http://www.slideshare.net/incontrolpartnerships/webinar-slides-personal-health-budgets-and-mental-health-getting-ready-
and http://www.neneccg.nhs.uk/resources/uploads/files/Northants%20MH%20report%20July%202014.pdf
Increasing the range of
support in the community to
promote recovery and
prevent crisis
Personal health and
social care budgets

27
Notes

28
There is now a wealth of evidence that peer support can be particularly important in
promoting recovery29. Peer support helps people feel less alone, offers support from
someone who understands what you are going through, allows people to share
experiences and different ways of understanding what has happened, helps people to
work out ways of dealing with problems and, most importantly, offers images of
possibility and helps people find the courage to keep going when times are difficult.
Peer support workers provide a different kind of relationship to that between mental
health professionals and the people they serve: a relationship that is based on mutuality
and a shared journey without claims to ‘special knowledge’ or expertise. “Peer Support
is about being an expert in not being an expert and that takes a lot of expertise”
(Recovery Innovations, 2009)’
In order to create recovery-oriented services we must bring together the expertise of
lived experience and the expertise of professionals on equal terms and enable people
who use services to access both sorts of expertise to assist them in their journey.
Relatives, friends and carers have also gained a great deal from peer support provided
by others who face similar challenges.
There are many ways of providing peer support, including peer support networks outside
services and Peer Support Workers within mental health services (in both statutory and
voluntary sectors). Both would appear to be important.
29http://www.nhsconfed.org/~/media/Confederation/Files/Publications/Documents/ImROC%20Peer%20Support%20Workers
%20Theory%20and%20Practice.pdf http://www.imroc.org/wp-content/uploads/7-Peer-Support-Workers-a-practical-guide-to-implementation.pdf
Increasing the range of
support in the community to
promote recovery and
prevent crisis
Peer Support

29
Within both statutory and non-statutory services, trained Peer Support Workers are
taking on a variety of roles. It would appear that support from a Peer Support Worker
may be particularly important at times of transition like coming into hospital, leaving
hospital and re-establishing life at home and leaving services. There may also be a role
for Peer Support Workers in fostering the development of networks (see Circle of
Friends and Prosper below).
Benefits to people being supported
increased self-esteem and confidence
improved problem solving skills increased sense of empowerment improved access to work and
education more friends, better relationships,
more confidence in social settings greater feelings of being accepted
and understood (and liked) reduced self-stigmatisation greater hopefulness about their
own potential more positive feelings about the
future reduced re-admissions and longer
community tenure
Benefits to the Peer Support Workers
• empowered in their own journey of recovery
• greater confidence and self-esteem • more positive sense of identity • less self-stigmatisation • feel valued, more money, more skills
“I work hard to keep myself well now, I’ve
got a reason to look after myself better...
It’s made a real big difference to me, you
know, contributing something to them.
And hopefully changing their lives for the
better”.
Benefits to the teams in which they work
• Support the development of recovery-focused practice • provide hope and inspiration for both others using services and staff • facilitate better understanding between staff and people using services
“I just stand back and watch him work his magic. Not just with the patients who come in
here so frightened and hopeless, but with staff too. He can help them see things in a
completely different way.”
“Peer workers have significantly changed the recovery focus of our team, they challenge
the way we talk about people from a problem and diagnosis focus to one of strengths
and possibilities” (Politt et al., 2012)

30
Notes

31
Real Lives is a Community Interest Company in Nottingham that was established to provide peer support for people with significant mental health challenges using personal budgets30. Support is provided by Peers and Allies for Living (PALS) who are recruited from among people with lived experience of mental health challenges and trauma: all PALS receive training and supervision and have ‘Wellness and Development Plans’ that identify their aspirations, support needs and detail how they will manage any challenges they themselves face in a work context.
Choice and flexibility lie at the heart of Real Lives. Each client chooses their own PAL from profiles on the web site31. All have a ‘Wellness and Safety Plan’, co-produced with their PAL which starts from their ambitions/goals, the support they want and what they want to get out of that support, and their warning signs and environments/situations in which they feel unsafe. These individual support plans are funded by personal social care budgets.
The accessible heart of the Real Lives service is the Crocus Café – a Vegan/Vegetarian Café that serves not only clients of the service but the whole community. Clients have ranged in age from 18 to 95. Most have serious mental health problems, a range of complex needs and have been hospitalised many times. Some have a forensic history. Evidence from individuals shows that the service is successful in maintaining people in community living, reducing hospital admissions and use of emergency services and helping them to move forward in their lives.
30 http://www.real-lives.co.uk/
Perkins, R. et al (2015) Real Lives: promoting recovery through personalisation and peer support, Mental Health and Social Inclusion, 19(1), 22-29 http://www.emeraldinsight.com/doi/abs/10.1108/MHSI-11-2014-0037
31 www.real-lives.co.uk/choose-your-pal-2/
Increasing the range of support in the community to promote
recovery and prevent crisis
An example of combining the power of personal
budgets and Peer Support: Real Lives in
Nottingham

32
Notes

33
Might personal budgets and Peer
Support Workers have a role to play in
personalising support in Dorset?

34
Social isolation is a major problem for people experiencing mental health challenges32. Too often it is social isolation that traps people in services: other than family, if they have one, many people have no contacts outside the mental health workers who visit them33. When someone is discharged because their symptoms have been controlled, they lose even the limited social contact provided by visits from a mental health worker, thus increasing their isolation. It is often the lack of friends that prevents people engaging in activities in the local community, and being a part of that community - doing things like going bowling or to the gym on your own can be very daunting!
Social isolation and exclusion from community life are extremely bad for mental and physical health34. Lack of social relationships is a major risk factor for physical health. Many research studies show a strong relationship between social isolation and mortality: social isolation is comparable with smoking and is worse than many well-established risk factors such as obesity and inactivity35. There is also some evidence of a relationship between social isolation and admission: lengthy and repeated admissions were associated with smaller social networks36. Researchers at the International Centre for Life-course Studies in Society and Health have demonstrated that social isolation is a key trigger for mental illness and that supportive relationships with friends, family and neighbours have beneficial effects on mental health and well-being37. This showed that small scale funding for community organisations can have a major impact. This means that, as well as thinking about clinical support inputs for people who experience mental health crises, it is also important to think about the role services can play in fostering social relationships and acting as a catalyst to the development of social networks that can be protective against relapse and facilitate recovery.
32 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/320509/building-understanding-main-
report.pdf 33 Ford, R et al (1994) Developing case management for the long term mentally ill. Bulletin of the Royal College of
Psychiatry, 17, 409-411 34 Marmot, M. (2015) The Health Gap, London: Bloomsbury 35 http://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000316 36 Holmes-Eber, P. and Riger, S. (1990) Hospitalisation and the composition of patients social networks. Schizophrenia
Bulletin, 16, 157 37 http://www.esrc.ac.uk/_images/ESRC_Evidence_Briefing_Mental_health_social_rel_tcm8-26243.pdf
Increasing the range of support
in the community to promote
recovery and prevent crisis
The importance of Social
Networks

35
There are a number of examples of ways in which primary and secondary mental health services have attempted to do this, for example:
In Phoenix Arizona, Circle of Friends provides members with a range of
opportunities to get together and engage in activities in the community38. Co-
ordinated by a Peer Support Worker from the local mental health service, it offers
an extensive range of activities such as bowling and baseball matches39. It
therefore provides people with the opportunity to create new friendships, build
support networks, and gain peer support to access a wide range of community
resources/supports to help further their own recovery. Circle of Friends also
provides activities and events designed specifically for young adults.
Although Circle of Friends does not provide transport, other similar initiatives
have made arrangements for helping people to come to events, for example,
setting up arrangements for a peer (someone else who is attending) to travel with
someone who is having difficulties, use of volunteers (who may be peers) to act
as ‘travel buddies’, use of Personal Budgets to provide transport, etc.
In South West London the Trust has provided a small amount of resource to
facilitate the development of Prosper40: a self-directed community of service-
users and service user groups that recognises not only the importance of social
networks, but also the value of peer support in enabling people to support each
other to build their own personal resilience and gain greater control over their
lives. Prosper enables people to do things for each other and increases the
provision of peer-led alternatives and mutual support groups41.
38 http://riinternational.com/our-services/arizona/circle-of-friends/ 39 http://www.recoveryinnovations.org/riaz/documents/COFMARCH2013.pdf 40 http://www.prospernetwork.co.uk/ 41 http://www.emeraldinsight.com/doi/pdfplus/10.1108/MHSI-08-2014-0026

36
In South West Yorkshire the Trust has supported the creation of Creative Minds42. The Trust develops community partnerships with a range of different local community organisations and co-funds creative projects across their localities. 130 creative projects in 95 voluntary, third sector, not-for-profit organisations and other community groups deliver creative, spiritual, sporting and environmentally based activities to more than 3,000 people43. This programme won the 2015 Patient Experience Network National Strengthening the Foundations award and the 2014 Health Service Journal Compassionate Patient Care award44.
City and Hackney Clinical Commissioning Group have developed a primary care
Social Prescription and Community Referral service45. A non-statutory
organisation has been commissioned to provide a social prescription assessment
service in 18 surgeries to which GPs can refer socially isolated people with
mental health problems. This service explores people’s interest, needs and
aspirations and refers them to a range of community activities.
Other initiatives have been more informal, like a service introducing people with similar
interests to each other and assisting groups pf people with similar interests to organise
opportunities to get together. Personal budgets may be of value to support this.
42 http://www.creativemindsproject.org.uk/ 43 http://www.emeraldinsight.com/doi/abs/10.1108/MHSI-12-2014-0041 44 http://www.southwestyorkshire.nhs.uk/quality-innovation/creative-minds/award-winning/ 45 http://www.health.org.uk/programmes/shine-2014/projects/commissioning-pilot-primary-care-social-prescriptioncommunity
37
Notes

38
Most people who experience mental health problems would like to be able to work, yet it remains the case that the vast majority do not have access to the support they need to gain and sustain employment. Around 28% of people with mental health problems are employed, compared to around 70% of the general population, but among those with more serious mental health challenges, only around 8% are in employment46. This is important because appropriate employment appropriate reduces symptoms and the likelihood of relapse and suicide as well as improving well-being and quality of life.
Employment provides meaning and purpose in life, status and identity and social contacts. It also helps lift people out of poverty and links people to their communities, and is good for physical health. Unemployment increases the risk of many physical health problems and premature death47. There is now a wealth of evidence that, with the appropriate help and support – Individual Placement and Support (IPS) evidence based supported employment – around 60% of people with serious mental health problems, can gain and sustain employment48. IPS does not only enable people to gain jobs, but also to sustain them and reduces the need for admission and use of mental health services49. NICE Quality statements for people with a diagnosis of psychosis and schizophrenia and bipolar disorder50 make it clear that people should have access to IPS, yet despite these recommendations and the extensive evidence base, such support is currently available to only a small proportion of those who need it.
46https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/265388/Mental_Health_Dashboard.pdf 47http://www.rcpsych.ac.uk/usefulresources/workandmentalhealth/clinician/workisakeyclinicaloutcome/importanceofemploym
ent.aspx https://www.gov.uk/government/publications/better-employment-support-for-people-with-a-mental-health-condition
48 http://www.centreformentalhealth.org.uk/individual-placement-and-support http://www.centreformentalhealth.org.uk/briefing-37-doing
49 http://www.lancet.com/journals/lancet/article/PIIS0140-6736%2807%2961516-5/abstract http://ajp.psychiatryonline.org/doi/abs/10.1176/appi.ajp.2014.13070857?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed
50 https://www.nice.org.uk/guidance/qs80/chapter/Quality-statement-5-Supported-employment-programmes http://www.nice.org.uk/guidance/qs95/chapter/quality-statement-8-supported-employment-programmes
Increasing the range of support
in the community to promote
recovery and prevent crisis
The importance of work

39
Notes
40
How can we increase the range of
community support available in
Dorset to promote recovery and
prevent crisis?

41
Whatever the range of services offered, it is critical that people can access these easily
and quickly when they need them – not just in full-blown crisis, but when there are signs
that a crisis is looming: early intervention can reduce both service usage and disruption
to people’s lives and wellbeing.
Often pathways into services have been confusing with multiple different teams each
with their own access points taking their own referrals. For this reason, many services
have developed a ‘Single Point of Access’ for all referrals51. These have been
successful and cost-efficient. However, it is important to ensure that there is ‘no-wrong-
door’: whether a person self-refers, or goes to their GP, a voluntary sector or community
organisation, A&E or a local pharmacist they can still get to the single point of access.
Typically services assume linear pathways: assessment –
diagnosis – treatment – discharge. Many mental health
problems fluctuate meaning that people need to be able to
move into and out of services when their problems wax and
wane. Therefore pathways need to be circular and
personalised. People are different - different influences, networks, cultures and beliefs,
risk factors, preferences52 - so personalising access,
especially for people with longer term challenges, may be
important.
Too often people are reluctant to leave services because
they know they cannot easily get back to the person they
trust and who knows them without a tortuous journey of
having to go back to their GP who refers to the single point
of access, where they are assessed before they can be
referred on to the team that knows them. Clinicians may
51See for example
http://www.nhsiq.nhs.uk/media/2635697/ltc_case_study_single_point_of_referral_hertfordshirepartnership.pdf 52 http://www.slideshare.net/AlainvanGool/2015-1126-neuroinformatics-and-personalized-health-care-symposium-nijmegen-
alain-van-gool
Access –
getting help:
A final note
on pathways

42
also be reluctant to discharge people when they are doing well if their experience shows
that in the coming months they will need specialist help again.
Some teams provide such opportunities ‘unofficially’ when people who they have known
well call for help, and it can be very efficient: if a team or clinician knows a person well
then they can often offer advice more quickly. For example, in the 1980s, the Maudsley
Hospital’s ‘District Services Centre’ for local people with long term mental health
challenges kept a register of ‘support patients’: people who had used the service and
who could return if their problems recurred. Often this took the form of a single phone
call or visit to deal with a problem or avert a crisis, but at other times the person required
a period of more intensive support or referral to another service. If, after a number of
years, the person had not re-accessed the service, their position was reviewed.
It may be desirable, therefore, to complement a Single Point of Access for people new to
services (and those who have been out of contact for a long period of time) with the
possibility of someone who has received treatment from a clinical team being able to re-
contact and return to the team and people who they know and who know them if their
problems recur. This could be achieved as part of a discharge plan, agreed with all
parties, that detailed warning signs, or trigger events, and who the person should contact
if these happen. This would allow the possibility of early intervention – before problems
escalated to crisis pitch. If people with ongoing mental health challenges know that they
can easily get help from the clinicians/team who know them then they are likely to be
more willing to leave services when things are on an even keel.

43
Notes

44
How can we improve access to
services in Dorset
For people who are new to the
service?
For people returning to the service?