
WOMEN’S HEALTH IN THE 21 ST CENTURY Jayme Bristow PharmD Candidate UGA College of Pharmacy.
40
WOMEN’S HEALTH IN THE 21 ST CENTURY Jayme Bristow PharmD Candidate UGA College of Pharmacy
-
Upload
calvin-carroll -
Category
Documents
-
view
213 -
download
0
Transcript of WOMEN’S HEALTH IN THE 21 ST CENTURY Jayme Bristow PharmD Candidate UGA College of Pharmacy.

WOMEN’S HEALTH IN THE 21ST CENTURY
Jayme Bristow
PharmD Candidate
UGA College of Pharmacy

LEADING CAUSES OF DEATH

REPORTED HEALTH STATUS

PERCENT OF ADULTS WITH OBESITY

PERCENTAGE OF ADULTS WITH DIABETES
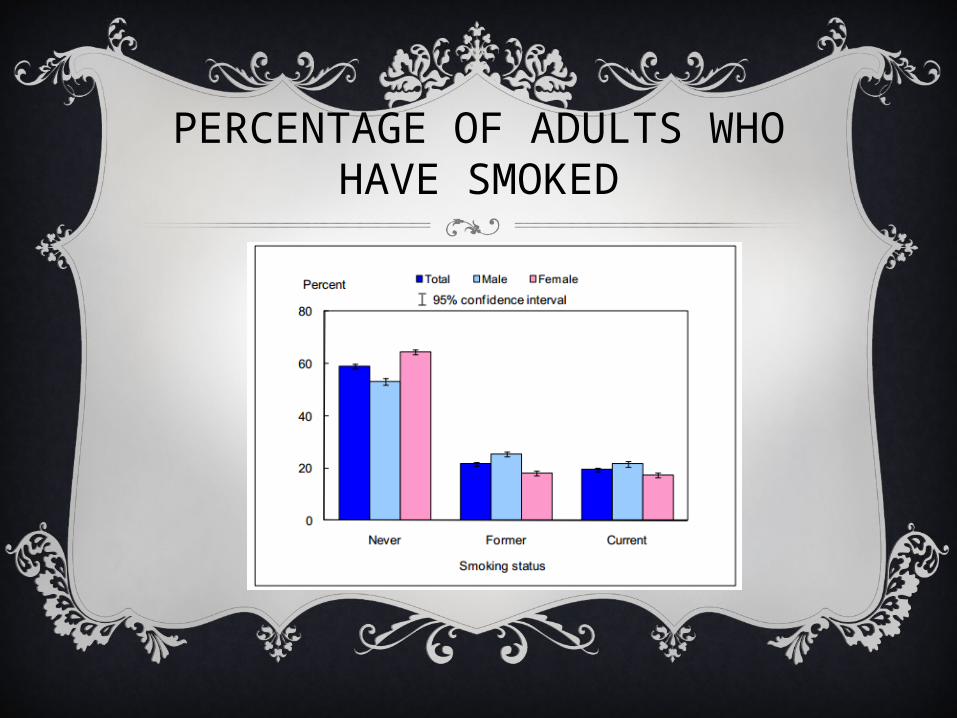
PERCENTAGE OF ADULTS WHO HAVE SMOKED

PERCENTAGE OF ADULTS WHO DRINK*
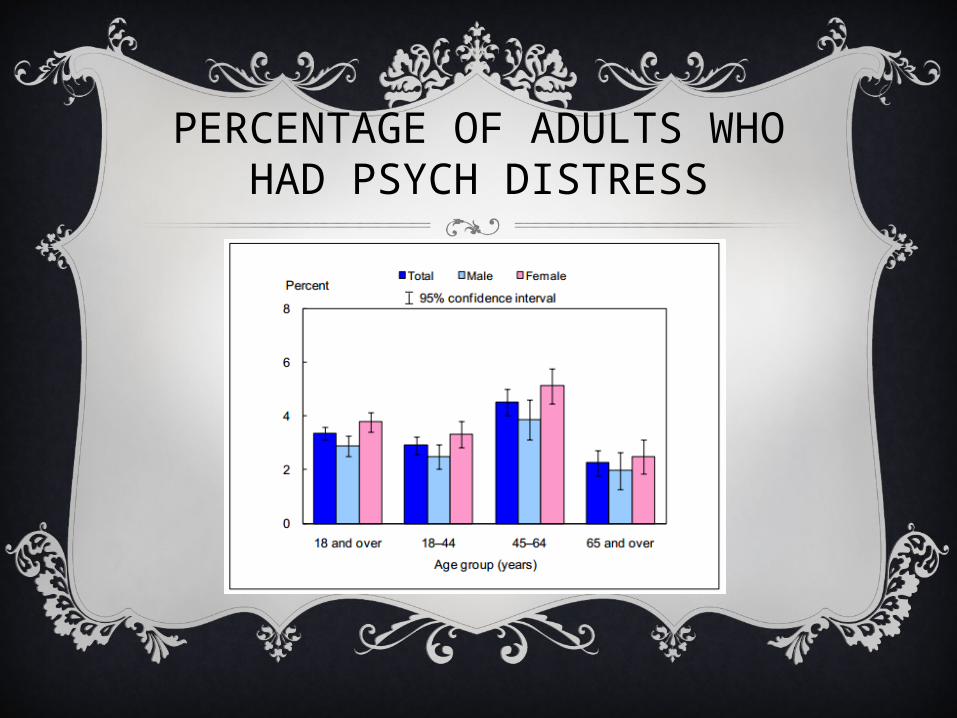
PERCENTAGE OF ADULTS WHO HAD PSYCH DISTRESS
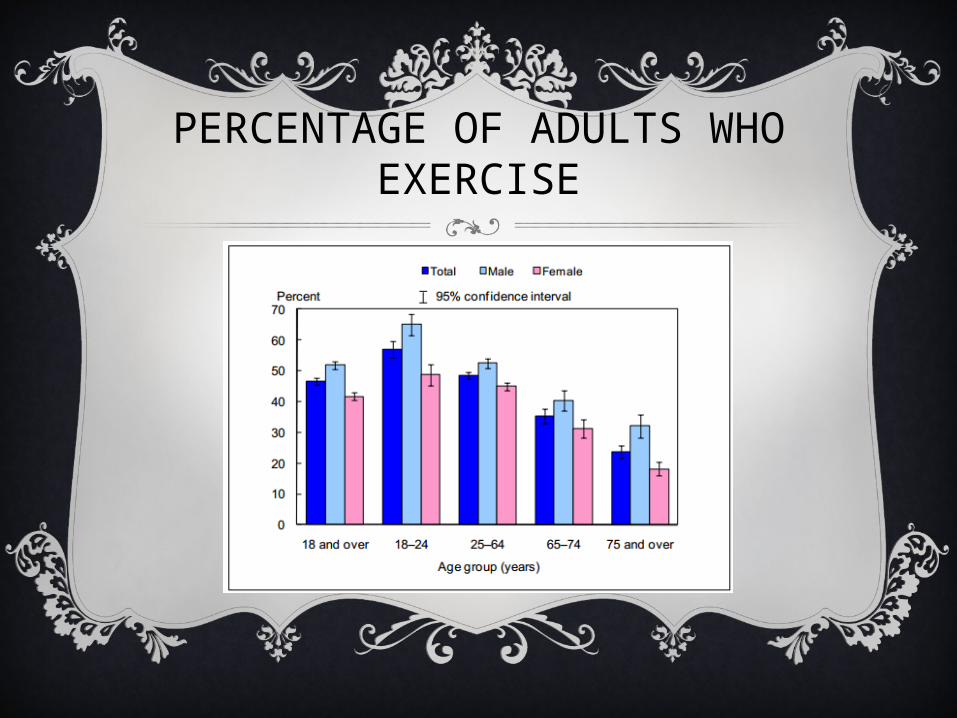
PERCENTAGE OF ADULTS WHO EXERCISE

PERCENTAGE OF ADULTS >65 WHO NEED HELP WITH PERSONAL CARE
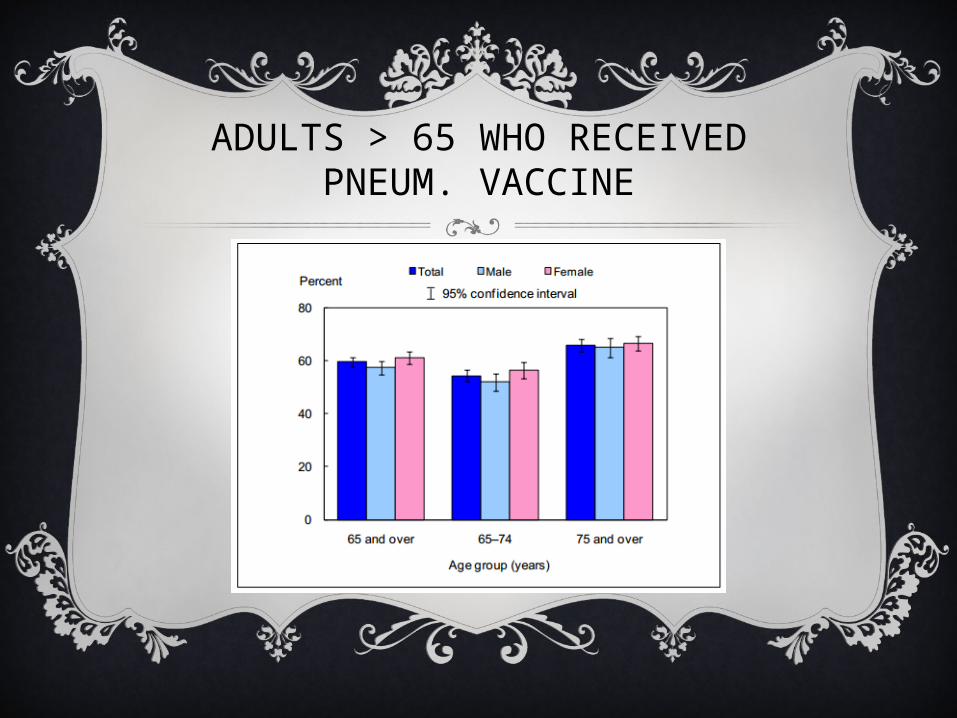
ADULTS > 65 WHO RECEIVED PNEUM. VACCINE

ADULTS WHO RECEIVED FLU VACCINE

CVD RISK - GENERAL
Coronary heart disease (CHD) includes MI, angina pectoris (AP), stroke, CHF, and cardiac arrest
CVD affects 25% of American women and men
CVD is the leading killer in America, but most women think that CVD is a “man’s disease”
Since 1984, more women than men have died of CVD every year
In 2002, CVD killed 493,623 women compared with 433,825 men
Fifty-three percent of CVD deaths occur in women
In 2002, CVD killed nearly 500,000 women compared to approximately 41,500 deaths by breast cancer
In 2002, nearly twice as many American women died of CVD than from all types of cancer combined

MI AND ANGINA
Women typically develop clinically evident CHD up to ten years later than men
According to the Framingham Heart Study (FHS), the lifetime risk of developing CHD after age 40 is 49% and 32% in men and women, respectively
While CHD deaths have decreased in men, studies indicate that CHD deaths in women have remained stable or even have increased
Women are more likely to suffer from MIs at older ages than men
• The average age of first MI is 65.8 and 70.4 in men and women, respectivelyA
fter menopause, the rate of CHD is 2-3 times that of premenopausal women who are the same age
Significantly more women than men (3.3 million vs 3.1 million) suffer from AP, which is chest pain due to myocardial ischemia

STROKE
Each year, approximately 40,000 more women than men suffer from a stroke
• This is related to women’s greater life expectancy and the higher rates of stroke in the oldest age groups
Female stroke patients are more likely than male patients to have atrial fibrillation, the most common form of irregular heartbeat
• One of the most common risk factors for stroke

CHF
According to the FHS, at age 40, the lifetime risk of developing CHF is 1 in 5 in both sexes
At younger ages, men have a higher prevalence of CHF, whereas after age 75, the prevalence is higher in women
Women who present with CHF are more likely to have comorbid diabetes and hypertension than men
CARDIAC ARREST
Cardiac arrest is about 3 times greater in men than in women; however, women have lower recovery and survival rates than men
A recent study showed that between 1989 and 1998, the rate of sudden cardiac death decreased in men across all age groups but increased in women between the ages of 35-44 years
Arrhythmias can occur in healthy people, but they also may indicate serious problems with the heart and lead to cardiac arrest
Women are more likely than men to have certain types of cardiac arrhythmias (irregular heartbeat), drug-induced torsade's de pointes, and long QT syndrome
• The mechanism for these sex differences may be related to the longer QT interval on the electrocardiogram in women
CVD RISK FACTORS AND WOMEN
Women who consume one alcoholic drink per day have a lower risk of CVD than nondrinkers
• Excessive or binge drinking can contribute to obesity and high triglycerides, raise blood pressure, cause heart failure, and lead to stroke
Studies have shown that low levels of HDL convey a higher risk for CVD in women
Women’s total cholesterol is higher than men’s cholesterol beginning at age 45
As women go through menopause, their lipid profiles change and become more atherogenic
High triglycerides may increase the risk of CVD for women more than for men

CVD RISK FACTORS AND WOMEN
AHA currently recommends assessment of CRP as a marker for cardiovascular risk
A recent study demonstrated that women had higher CRP levels than men
• Levels were also higher in African Americans than in Caucasians• Further studies are necessary to determine if these differences in CRP levels
lead to differences in CVD outcomes.B
efore the age of 55, a higher percentage of men than women have hypertension; however, this relationship switches after age 55
• Hypertension affects 74% of women ages 65 to 74• In 2002, 59% of the deaths from hypertension were in women
Several studies, including the FHS, have reported that hypertension and diabetes are greater risk factors for CHF and stroke in women than in men

CVD RISK FACTORS AND WOMEN
Studies have shown that depression may increase the risk of CHD in women
Women with MI suffer more severe and long-term depression than men, and depression may even increase mortality after MI in women
Depression and phobic anxiety have been shown to increase the risk of cardiac arrest and sudden cardiac death in women
• 40% of women who had a cardiac arrest experienced stress such as a divorce or depression beforehand, compared with only 16% of men
• Only 5% of the women reported physical exertion before a cardiac arrest, compared with 40% of men
Studies have shown that women who smoke have a higher risk of developing or dying from heart disease, stroke, and CHF than men
• Smoking was shown to increase the risk of MI in women younger than 55, a population that normally is at relatively low risk

CVD OUTCOMES
Studies have shown that women have worse in-hospital and long-term outcomes than men after MI
Women were twice as likely to experience complications such as infection, bleeding, and irregular heartbeat during and after CABG compared to men
Women also experienced a higher readmission rate within 6 months of their MI and CABG
Results demonstrated that within 6 years of an MI, more women than men will have another heart attack (35% vs 18%), be disabled with CHF (46% vs 22%), and suffer a stroke (11% vs 8%)

CVD OUTCOMES
38% of women who have had an MI will die within one year, compared with 25% of men
• This is partly because women have MIs at older ages than men and are more likely to die from them within a few weeks
• Higher mortality may also be due to women’s worse baseline characteristics and comorbidities
Women were more physically and mentally impaired than men 3 months after their stroke
In 2002, stroke claimed the lives of 100,050 women, which represents 61.5% of the total stroke deaths
MENTAL HEALTH
Depressive disorders afflict almost 10 percent of the United States population, with 2-3 times more females than males affected
Prior to age 13, approximately equal numbers of girls and boys experience depression, but more females than males over age 13 become depressed
The rate of synthesis of serotonin, and level of serotonin in the blood are significantly higher in men than women
• Serotonin is a chemical required in the brain for mood maintenance• These differences may help explain why depression is more
common in women than in men

MENTAL HEALTH
Women who experience depression are more likely than others to develop alcohol problems within a few years of their first depressive episode, whereas there appears to be no such link between depression and alcohol problems in men
Women who suffer from chronic major and double depression are more likely to:
• Be unmarried• Have a younger age at onset• Greater family history of affective disorder• Complain of more marital problems• Sleep changes• Psychomotor retardation• Anxiety/somatization than men
MENTAL HEALTH - AD
Several studies have shown that women are at higher risk for developing AD than men
AD features a distinct type of damage to the white matter of the brain
• Damage to the white matter is more common and more severe in women than in men suffering from AD
Female AD patients show more severe early alterations of cells in a particular part of the brain, the nucleus basalis of Meynert, than do males
• The number of these cellular alterations correlates with the severity of dementia

MENTAL HEALTH - AD
Men with AD have a higher risk of mortality than women with the disease
Death in men with AD tends to be associated with factors related to the disease itself such as the severity of dementia and the occurrence of episodes of delirium
Death among women with AD tends to be associated with measures of disability, such as malnutrition and impairment in performing the activities of daily living
These differences suggest that the underlying mechanism for Alzheimer’s disease may be different in men and women

OBESITY
Between 2005-2006, 33.1% of men and 35.2% of women were obeseBetween 1999-2004, the prevalence of extreme obesity was higher
in women (7% vs 3%)A racial/ethnic divide exists for overall obesity and for sex
differences in obesity• Among black people, 54.3% of females and 36.3% of males were obese
between the years 2003-2006• Among Mexican females and males, the prevalence was 42.6% and
30.4%, respectivelyNormal weight individuals with diabetes, dyslipidemia, or
hypertension had significantly greater medical expenditures than those without these conditions, but obesity significantly exacerbated this effect by at least $7600
Obesity also exacerbated the increase in missed work days and lost productivity seen in patients with these conditions

METABOLIC SYNDROME
Metabolic syndrome is a primary risk factor for developing heart disease and diabetes. It is diagnosed in the presence of at least 3 of the following:
Elevated waist circumference (men ≥ 40 inches; women ≥ 35 inches)
Elevated triglycerides ≥ 150 mg/dL
Reduced HDL (“good”) cholesterol (men ≤ 40 mg/dL; women ≤ 50 mg/dL)
Elevated blood pressure ≥ 130/85 mm Hg
Elevated fasting glucose ≥ 100 mg/dL
METABOLIC SYNDROME
It is estimated that over 50 million Americans have metabolic syndrome, and there is an apparent “female advantage” in premenopausal women compared with age-matched men
Women usually lose the sex protection following menopause
The prevalence of metabolic syndrome has risen particularly in young women, where it is mainly driven by obesity
When premenopausal women develop metabolic syndrome they are at increased risk of cholesterol-related diseases vs. men with the diagnosis

MENOPAUSE
An estimated 6,000 US women reach menopause every day (over 2 million per year)
Nearly 40 million US women are past the average age of natural menopause
All women experience menopause, but each one does so in a unique way
How a woman responds to the physical changes of menopause may be similar to the way her mother responded, although the evidence to support this notion is limited
MENOPAUSE
In one study, 80% of women experiencing menopause reported no decrease in quality of life (QOL)
75% of the women denied experiencing any loss in their attractiveness
Most women (62%) reported positive attitudes toward menopause itself
In another study, most women viewed menopause as inconsequential, and suggested that other events of midlife were more important or stressful
A cohort of well-educated, midlife women described the menopause transition as a normal developmental event
Only about 10% of peri- and postmenopausal women participating in community-based studies reported feelings of despair, irritability, or fatigue during the menopause transition

MENOPAUSE
There are two major health problems are associated with menopause:
• Osteoporosis: losing estrogen around the time of menopause causes women to lose more bone than is replaced and in time, bones can become weak and break easily
• Heart Disease: after menopause, women are more likely to have heart disease• Changes in estrogen levels may be part of the cause• So is getting older: as you age, you may gain weight and
develop other problems, like high blood pressure
MENOPAUSE
Don't smoke
Eat a healthy diet, low in fat, high in fiber, with plenty of fruits, vegetables, and whole-grain foods, as well as all the important vitamins and minerals
Get enough calcium and vitamin D—in your diet or with vitamin/mineral supplements
Learn what healthy weight is, and try to stay there
Do weight-bearing exercise, such as walking, jogging, or dancing, at least 3 days each week for healthy bones
Try to be physically active in other ways for your general health

HORMONES??
During perimenopause, some doctors suggest birth control pills to help with very heavy, frequent, or unpredictable menstrual periods
• These pills might also help with symptoms like hot flashes, as well as prevent pregnancy
Symptoms like hot flashes, night sweats, or vaginal dryness might be treated with estrogen (as well as progesterone, if you still have a uterus)
• This is known as menopausal hormone therapy (MHT)• Taking these hormones will help with menopause symptoms• It also can prevent the bone loss that can happen at menopause

HORMONES??
Research has found that in some women there are serious risks, including an increased chance of heart disease, stroke, blood clots, and breast cancer, when using MHT
There may also be an increased risk of dementia in women when they start MHT after age 65
These concerns are why every woman needs to think a lot before deciding to use menopausal hormone therapy
Some side effects include:
• Breast tenderness, return of period/spotting, cramping, bloating

OSTEOPOROSIS
In the United States, 50% of women over age 50 have osteopenia, or low bone mass
Osteoporosis, which is characterized by loss of bone mass leading to increased risk of fracture, affects 8 million women and 2 million men
By 2010, 9 million and 26 million women over age 50 are expected to have osteoporosis or osteopenia, respectively
One in two women and one in four men over 55 will have an osteoporosis-related fracture in the remainder of their lifetime

OSTEOPOROSIS
A women’s risk of hip fracture is equal to her combined risk of breast, uterine, and ovarian cancer
One half of women who sustain a hip fracture fail to return to their pre-fracture function level
Independent of bone mineral density (BMD), previous fracture is the most important risk factor for future fractures
OSTEOPOROSIS
Risk Factors
• Women: start with less bone mass and lose it more quickly• Type 2 Diabetes: women have higher BMD than healthy
women, and are therefore less likely to suffer from osteoporosis
• Ethnicity: osteoporosis is more common in Caucasian, Asian, and Hispanic women than in African American women
• Alcohol: lower levels of alcohol are associated with higher BMD
• Exercise: increase in exercise increases BMD• Smoking: smoking decreases BMD• Weight: low weight is a predictor of low BMD

QUESTIONS???

REFERENCES
“
Early Release of Selected Estimates Based on Data From the 2010 National Health Interview Survey.” CDC. Accessed 17 March 2012.
http://www.cdc.gov/nchs/nhis/released201106.htm#4
“
Menopause.” NIH: National Institute of Aging. Accessed 17 March 2012. http://www.nia.nih.gov/health/publication/menopause
“
Menopause.” WomensHealth.gov. Accessed 17 March 2012. http://womenshealth.gov/menopause/symptom-relief-treatment/
“
Leading Causes of Death in Females 2007.” CDC. Accessed 17 March 2012. http://www.cdc.gov/women/lcod/index.htm
“
Terms and Statistics.” North American Menopause Society. Accessed 17 March 2012. http://www.menopause.org/edumaterials.aspx
“
Diabetes”. Society for Women’s Health Research. Accessed 16 March 2012. http://www.womenshealthresearch.org/site/PageServer?
pagename=hs_healthfacts_diabetes
“
Musculoskeletal Health.” Society for Women’s Health Research. Accessed 16 March 2012. http://www.womenshealthresearch.org/site/PageServer?
pagename=hs_healthfacts_musculo
“
Cardio/Cerebrovascular Diseases” Society for Women’s Health Research. Accessed 16 March 2012.
http://www.womenshealthresearch.org/site/PageServer?pagename=hs_healthfacts_cardio
“
Mental Health.” Society for Women’s Health Research. Accessed 16 March 2012. http://www.womenshealthresearch.org/site/PageServer?
pagename=hs_healthfacts_mental


















