Window Tech 20040402 - BRMedical Tech 20040402.pdf · • Anatomic plate of dual radius curvature...
16
WINDOW WINDOW ™ ™ Cervical Cervical Dynamic Plate System Dynamic Plate System SURGICAL TECHNIQUE SURGICAL TECHNIQUE T-SFS-002-AE
Transcript of Window Tech 20040402 - BRMedical Tech 20040402.pdf · • Anatomic plate of dual radius curvature...

WINDOWWINDOW™™ Cervical Cervical
Dynamic Plate SystemDynamic Plate System
SURGICAL TECHNIQUESURGICAL TECHNIQUE
T-SFS-002-AE

FOREWORD :FOREWORD :
• In the past years, various anterior spinal fixation plate systems failed in meeting with the surgeon’s approbation because of bulkiness, thickening, high profile, improper radian, technical demanding,
and restriction of inserting angle of the screw.
• With intensive researches and improvement, A-Spine is proud to introduce the most advanced “ WINDOW™ Cervical Dynamic Anterior Locking Plate System ” ( WINDOW Plate ).
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
DESIGN RATIONALES DESIGN RATIONALES ::
• Dynamic design allows for natural vertebral graft subsidence/settlement during graft remodeling;
• Prevents gap formation between graft and vertebral body to create solid fusion;
• Dynamic design also releases stress at screw/plate interface.
• Anatomic plate of dual radius curvature minimizes bone removal & plate bending;
• Anatomic plate accommodates & restores natural lord sis of cervical spine;
• Anatomic plate permits natural screw orientation following ascending vertebrae morphology;
• Flexibility of screw placement & angulations up to 7° optimizes plate/screw implantation;• Flexibility of dynamic or static screw configuration yields surgeon’s options;
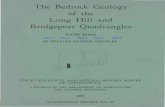
16mm
L
Thickness
2 mm
ADVANTAGE ADVANTAGE ::
• The thickness of plate of 2.0 mm reduces tissue irritation.
• The width (16 mm) of plate is smaller than other plates. (Figure 1)
• Cutouts designed at all edges of plate facilitate temporary fixation using fixation spikes.
• The screws are available in 12-16 mm in length and of cancellous thread blunt tip design, avoiding
possibility of penetrating the vertebral body. ( Figures 2 and 3 )
• Window™ plate is locked on by screw’s thread, therefore, eliminating possibility of dislodging.
• Window™ plate is easy to bend and to contour to match the vertebral body, as the plate is made of
high performance titanium alloy material.
D
L
Fig. 1
Fig. 2 Fig. 3
1
Cutout

INDICATIONS FOR USE INDICATIONS FOR USE ::
• Subluxation of lower cervical spine
• Dislocation of C2-3
• Total or partial Corpectomy
• Multiple segments discectomy
• Vertebral body fracture or deformity
• Fracture at posterior element of C2
• Burst fracture or metastatic lesion
CONTRAINDICATIONSCONTRAINDICATIONS ::
• Severe osteoporosis
• Active infection of the involved vertebral bodies
• Sensitivity to metallic implant materials
COMPONENTS COMPONENTS :: The system is made of Titanium alloy
• Cervical plates
• Locking screws
• Emergency locking screws
Cervical Cervical PlatesPlates ::
Plate Thickness : 2.0 mm ( Figure 4 )
Plate Width : 16 mm
Length: 26 ~ 90 mm
Holes :• Bilateral Elliptical :
to receive locking screws
• Central Elliptical : to receive screws locking bone graft
• Round(small): fixing the fixation screws temporarily
16mm
L
Thickness
2 mm
Elliptical Hole
Fixation
Screw Hole
Fig. 4
2
STERIZATIONSTERIZATION ::
• The system is provided Non-Sterile to hospital.
• A-Spine suggest the device should be sterilized via steam autoclave under 121°C (250°F), 20 PSIG for 30 min to assure SAL(10-6).
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique

Screws Screws ::
1. Locking Screw ::::•Diameter: 4.0 mm
• Length : 12 , 14 , 16 mm
• Specially design:
allows the screw to be inserted within 7 degree range to the plate ( Figures 6 and 7 )
2. Emergency Screw ::::• Diameter: 4.3 mm
• Length : 16 mm
• Specially design:
D
L
Fig. 7Fig. 6
Fig. 5
3
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
15°

Figure Item Description
2001–01 Drill Guide
2002-01 Awl
2003–01 Handle
2004–01 Drill
2005-01 Screwdriver
2006–01 Plate Holder
2007–01 Tap
2008-01 Stabilization Pin
2009-01 Plate Bender
2010-01 Stabilization Pin Driver
2011-01~2013-01 Pleate Template
WINDOWWINDOW™™ CERVICAL DYNAMIC PLATE SYSTEM INSTRUMENTSCERVICAL DYNAMIC PLATE SYSTEM INSTRUMENTS
Fig. 8
4
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique

• CT or MRI is employed to confirm the location of lesion, dimensions of the vertebrae(s) to be fused, to determine the lengths of plate & screws to be implanted.
• Operation is performed under endo-tracheal anesthesia.
A. PreA. Pre--OP PreparationOP Preparation
Surgeon
Image IntensifierIntubation
Assistant
Adhesive tape distally
retracts shoulders
B. Patient Positioning B. Patient Positioning
• The patient is placed in a supine position. ( Figure 9 )
• Patient’s neck is positioned with a rolled-up towel & pad between the scapulae to keep the operated site slightly overextended if desired.
• The head is kept in neutral position and is rotated 15°°°° to 30°°°° to the oppositeside.
• Both shoulders were pulled downward with strips of adhesive tape to obtain clear access of radiographic visualization of lower cervical spine.
••Caution: Care should be taken to avoid overstretching the brachCaution: Care should be taken to avoid overstretching the brachial ial plexus.plexus.
• One iliac crest or leg is placed, padded and prepared for autologous bonegraft harvesting.
Fig. 9
5
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique

Step 1: Step 1: Locate & ExposeLocate & Expose
• A transverse incision parallel to the neck fold is indicated to expose one or two seg-ments, while a longitudinal incision anterior to the sternocleidomastoid muscle is prefered for a broad exposure of several segments of the cervical spine. After incision,the platysma muscule is divided by the direction of its’ fiber and retracted to both sidesfor exposing the superficial cervical fascia. This fascia is divided at the junction of theanterior border of the sternocleidomastoid muscle. If the omohyoid muscle runstransversely across the operative field, can be divided by two ligatures and retractedbilaterally. ( Fig. 10 & 11 ) Note: Protection of the superior laryngeal nerve sh ould be noted to avoid postoperative hoarseness and spee ch disorder .
• The deep prevertebral fascia is divided from the midline and dissected laterally to thelong muscle of the neck, followed by the elevation with rasp on both side on theanterior longitudinal ligament. With a longitudinal resection of ligament, the anteriorsurface of cervical vertebrae is exposed. ( Figure 12 )
1. Sternocleidomastoid muscle withsuperficial cervical fascia
2. Platysma muscle, cut
3. Superficial cervical fascia
4. Anterior jugular vein
5. External jugular vein
6. Punctum nervosum
7. Transverse nerve of the neck
8. Great auricular nerve
9. Superficial ansa cervicalis
10. Superior thyroid artery & vein
11. Lingual artery
12. External carotid artery
13. Common carotid artery
14. Internal jugular vein
15. Facial vein
16. Prevertebral cervical fascia
17. Long muscle of the neck
IV~VI C4~C6 Cervical vertebrae
Fig. 10
Fig. 12
6
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
11
57
4 9 2
3
286
Division of
fascia
10
1112
13 1415
1
3
1314 16
5
17 VI
Fig. 11

Step 2: Step 2: DiscectomyDiscectomy
• The lesioned segment(s) is confirmed with C-arm.
• The longus colli muscle is retracted laterally with a self-retaining retractor whileCasper spreader is applied longitudinally distracting the upper and lower bodies.The anterior longitudinal ligament and anterior portion of the annulus fibrosus areexcised, exposing vertebral body. (Fig. 13)
• The upper and lower end plates of the adjacent vertebrae are removed. Large anterior osteophytes are trimmed, yet the original cortical edge is retained. (Fig.14)
• If the end plates are highly sclerotic and avascular, perforation at individual spotswith a ball-pointed drill is carried out with an prepared bone bed surface averaged
15mm X 15mm.
Fig. 13
Fig. 14
Fig. 15
7
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
• The maximal expansion of the intervertebraspace and exact measurement of graft sizeis conducted with Caspar spreader. (Fig. 15)
• The Fixation Pins of the Casper spreader are inserted into the vertebraes at the midline of the anterior cortex.
Longus colli
Sternocleidomastoid
Sup. thyroid Vessels

Step 3:Step 3: Preparing & Placing Bone GraftPreparing & Placing Bone Graft
• In monosegmental fusionin and bisegmental (one or two) corpectomy, autologousgraft is harvested from the iliac crest. Fibula bone graft is used for polysegmentalcorpectomy (three or more levels).
• With the cortical surface placing vertically, the graft trimmed according to themeasured dimensions is wedged into the expanded intervertebral space in a posterior-open horseshoe fashion. The graft is seated correctly without anterior protrusion. ( Fig. 16 & 17)
Fig. 17Fig. 16
8
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
• In bisegmental fusion, a corticocancellous autologous iliac crest graft is trimmed to the required dimension. Care is taken to ensure anoblique ascent profile of the lower & upper end plates on the cervical spine. (Fig. 18)
• The graft is impacted with cortex forward-facing and spreader in place. (Fig. 19)
Fig. 18 Fig. 19

Step 4:Step 4: Placing the WINDOW platePlacing the WINDOW plate
• Measure the plate length by reading scales shown on Plate Template (2011-01, 2012-01, 2013-01). The both ends of Window Plate should be within the farthest endplates of the fusing vertebraes for the preservation of normal motion activity of the unfused disc. (Fig. 20)
• The spur is removed to create a smooth surface for plate bedding. Identify themidline of spinal column and Window Plate™ of appropriate size is then placed over the anterior surface of vertebral body smoothly. The plate is temporarily fixed with two Stablization Screw(2008-01) using Stablization Pin Driver(2010-01).(Fig. 21)
• The Window™ Plate can be bent with Window Plate Bender (2009-01) following the anatomic lordotic curve when desired. 3 modes of bending curvature selectionare provided on the bender by rotating the center knob. Note the center of bending should be at the plate cutout to facilitate easy bending and maintenance of plate strength. (Fig. 22)
Fig. 22
9
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
Fig. 21Fig. 20

•
Step 5:Step 5: Inserting the locking screwsInserting the locking screws
A. A. Assembling the drill guideAssembling the drill guide
• The tip of drill guide(2001-01) is positioned on the plate‘s elliptical hole. Unique screw slot design permits 7° cephalic/caudal angulation of screw insertion based on surgeons’ preference and clinicial consideration. (Figure 23)
B. DB. Drill and taprill and tap
• Awl (2002-01) is used through the drill guide following by drilling and tapping on thevertebral body ( Figure 24 )
• Repeat the above step with other holes of the plate.
10
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
15°
Fig. 23
Fig. 24

1
2
34
C. Inserting and Tightening C. Inserting and Tightening the screwthe screw• Insert Window™ screw without fastening (one or two thread left ) until all screws
are introduced into bony structure. (Fig. 25)
• The sequence of screw insertion is shown in Fig. 26.
• Remove Stabilization Pin .
• Fasten all screws to bring Window™ Plate in firm contact with body surface. The absence of screw thread at screw head junction prevents screw from looseningand/or backing out. The screw is designed for full seating once the edge of the screw head is almost lined up with plate surface. (Fig. 27 & 28)
Step 5:Step 5: Inserting the locking screws Inserting the locking screws ((continued)continued)
Fig. 25
11
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique
Fig. 26
Fig. 27 Fig. 28

WOUND CLOSUREWOUND CLOSURE1. A drain is introduced, and the wound is closed by suturing the platysma and skin.2. The wound is subsequently closed in the routine manner.
POSTOPERATIVE MANAGEMENTPOSTOPERATIVE MANAGEMENT1. The patient is immediately mobilized.
2. Drain is removed 48 hours post-operatively.
3. Patients should be instructed to wear a soft plastic form cervical collar for six weeksfollowing surgery.
POSTSCRIPTPOSTSCRIPTThe above description serves only as the standard installing procedure of the WINDOW cervical dynamic plate system. Since the physiological condition of every individual patient is different, the surgeon should take thorough examination and careful judgment prior to surgery to ensure the safety and the early recovery of the patient.
12
WINDOWWINDOW™™ Cervical Dynamic Plate System Surgical TechniqueCervical Dynamic Plate System Surgical Technique

INSTRUCTIONS FOR PATIENTINSTRUCTIONS FOR PATIENT1. The patient must be aware of all postoperative restrictions, particularly limitations
related to occupational and sports activities .
2. The patient should be warned that non-compliance with the postoperative instructions
may lead to failure of the implant. Additional surgery may also be required to remove
the device.
AppendixGENERAL WARNINGS, PRECAUTIONS AND POSSIBLE EFFECTS
Precautions to Surgeons:Precautions to Surgeons:1.The WINDOW cervical plate should not be used to span more than three segments at
the C3 ~ C7.
2.The surgeons must be thoroughly knowledgeable of the mechanical and metallurgical
limitations of metallic surgical implants.
3.The patient should be adequately instructed. Postoperatively care and the patient’s
ability and willingness to follow instructions are one of the most important aspects of
successful bone healing. The patient must be made aware of the limitations of the
implant, and that physical activity and full weight bearing have been implicated in
premature failure of metallic internal fixation devices. The patient should be made
aware that a metallic implant is not as strong as normal, healthy bone and will fracture
if excessive demands are placed on it in the absence of complete bone healing. An
over-active, debilitated or demented patient who can’t properly use weight-supporting
devices may be particularly at risk during postoperative rehabilitation.
4.Removal of the implant after healing: Metallic implants can be loosen, fracture,
corrode, migrate, possibly increase the risk of infection, cause pain or stress shield
bone even after healing, particular in young, active patients. The surgeons should
carefully weigh the risks versus benefits when deciding whether to remove the implant.
Implant removal should be followed by adequate postoperative management to avoid
re-fracture. If the patient is older and has a low actively level, the surgeon may choose
not to remove the implant, thus eliminating the risks involved with a 2nd surgery.
5.Until firm bony union (confirmed by clinical and radiographic examination) is
established, the patient should employ adequate external support and restrict
physical activities which would place excessive stresses upon the implant or allow
movement and delay or prevent healing.
13

AppendixGENERAL WARNINGS, PRECAUTIONS AND POSSIBLE EFFECTS
Precautions to Patients:Precautions to Patients:
1. Although the use of internal fixation implants has given the surgeons a mean of bone
fixation and help generally in the management of fracture and reconstructive surgery,
these implants are only intended to be a temporary device to assist normal healing
and are not intended to replace normal body structures. Metallic bone fixation
devices are internal splints which provide a means of bone fixation while normal
bone healing occurs.
2. Postoperative care is extremely important. The patient must be instructed in the
limitations of this implant and must be warned regarding weight-bearing and body
stress on the device prior to firm bone healing. The patient should be warned that
non-compliance with postoperative instructions could lead to failure of the device and
the possible need thereafter for additional surgery to remove the device.
Possible Adverse Effects:Possible Adverse Effects:The following are specific adverse effects which should be understood by the surgeon
and explained to the patient.
These do not include all adverse effects which can occur with surgery in general, but
are important considerations particular to metallic internal fixation devices. General
surgical risks should be explained to the patient prior to surgery.
. Dural leak
. Nerve damage due to surgical trauma
. Infection
. Pain, discomfort or abnormal sensations due to presence of the device.
. Metal sensitivity or allergic reaction to a foreign body.
. Bending or fracture of the implant; loosening of the implant
. Delayed union or nonunion
. Decrease in bone density due to stress shielding
. Bursitis
14

Possible Risks and Complications:Possible Risks and Complications:. Screw improperly positioned. Incorrect fixation of vertebral plate. Failure to tighten nuts fully. Failure to fashion graft to properly fit the resection gap. Failure to properly fill and compress bone graft material into the bony defect. Failure to carefully dissect and retract the collis longus muscle muscle away from the
spinal segments to avoid nerve root damage
Warnings:Warnings:. Correct selection of the implant is extremely important. The potential for satisfactory
fixation is increased by the selection of the proper size, shape and design of the implant.While proper selection can help minimize risks, the size and shape of human bonespresent limitations on the size, shape and strength of implants. Metallic internal fixationdevices cannot withstand activity levels equal to those placed on normal, healthy bone.No implant can be expected to withstand indefinitely the unsupported stress of full weightbearing.
. Implants can break when subjected to the increased loading associated with delayedunion or nonunion. Internal fixation appliances are load sharing devices which are useduntil normal healing occurs. If healing is delayed, or does not occur, the implant mayeventually break due to metal fatigue. The degree or success of union, loads producedby weight bearing and activity levels will dictate the longevity of the implant. Notches,scratches or bending of the implant during the course of surgery may also contribute toearly fatigue. (Patients should be fully informed of risks of implant failure.). Correcthandling of the implant is extremely important. Contouring of metal plates should onlybe done with proper bending equipment. The surgeon should avoid any notching orscratching of the device when contouring it. Alterations will produce defects in surfacefinish and internal stresses, which may become the focal point for eventual breakage ofthe implant. Bending of screws will significantly decrease their ability to hold within thebone and may cause failure.
. Mixing metals can cause corrosion. Dissimilar metals in contact, such as titanium screwsin a stainless steel bone plate, accelerate the corrosion process of stainless steel andrapid attack occurs. The presence of corrosion often accelerates fatigue fracture of theimplant. Internal fixation devices, such as plates and screws which come in contact, must be made from like or compatible metals.
. Surgical implants must never be reused. An explained implant should never be re-implanted.
AppendixGENERAL WARNINGS, PRECAUTIONS AND POSSIBLE EFFECTS
15