Why equity in health and in access to health care are ...
26
Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=rgph20 Download by: [University of Cape Town Libraries] Date: 02 January 2018, At: 23:42 Global Public Health An International Journal for Research, Policy and Practice ISSN: 1744-1692 (Print) 1744-1706 (Online) Journal homepage: http://www.tandfonline.com/loi/rgph20 Why equity in health and in access to health care are elusive: Insights from Canada and South Africa Solomon Benatar, Terrence Sullivan & Adalsteinn Brown To cite this article: Solomon Benatar, Terrence Sullivan & Adalsteinn Brown (2017): Why equity in health and in access to health care are elusive: Insights from Canada and South Africa, Global Public Health, DOI: 10.1080/17441692.2017.1407813 To link to this article: https://doi.org/10.1080/17441692.2017.1407813 Published online: 04 Dec 2017. Submit your article to this journal Article views: 90 View related articles View Crossmark data
Transcript of Why equity in health and in access to health care are ...

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=rgph20
Download by: [University of Cape Town Libraries] Date: 02 January 2018, At: 23:42
Global Public HealthAn International Journal for Research, Policy and Practice
ISSN: 1744-1692 (Print) 1744-1706 (Online) Journal homepage: http://www.tandfonline.com/loi/rgph20
Why equity in health and in access to health careare elusive: Insights from Canada and South Africa
Solomon Benatar, Terrence Sullivan & Adalsteinn Brown
To cite this article: Solomon Benatar, Terrence Sullivan & Adalsteinn Brown (2017): Why equityin health and in access to health care are elusive: Insights from Canada and South Africa, GlobalPublic Health, DOI: 10.1080/17441692.2017.1407813
To link to this article: https://doi.org/10.1080/17441692.2017.1407813
Published online: 04 Dec 2017.
Submit your article to this journal
Article views: 90
View related articles
View Crossmark data

Why equity in health and in access to health care are elusive:Insights from Canada and South AfricaSolomon Benatara,b, Terrence Sullivanc and Adalsteinn Brownc,d,e
aFaculty of Health Sciences, University of Cape Town, Cape Town, South Africa; bDalla Lana School of Public Health,University of Toronto, Toronto, Ontario, Canada; cInstitute for Health Policy, Management and Evaluation, Dalla LanaSchool of Public Health, University of Toronto, Toronto, Ontario, Canada; dLi Ka Shing Knowledge Institute,St. Michael’s Hospital, Toronto, Ontario, Canada; eMassey College, Toronto, Ontario, Canada
ABSTRACTHealth and access to health care vary strikingly across the globe, anddebates about this have been pervasive and controversial. Somecomparative data in Canada and South Africa illustrate the complexity ofachieving greater equity anywhere, even in a wealthy country likeCanada. Potential bi-directional lessons relevant both to local and globalpublic health are identified. Both countries should consider theimplications of lost opportunity costs associated with lack of explicitresource allocation policies. While National Health Insurance is attractivepolitically, Canada’s example cannot be fully emulated in South Africa.Short- and medium-term attempts to improve equity in middle-incomecountries should focus on equitable access to insurance to coverprimary health care and on making more use of nurse practitioners andcommunity health workers. In the longer-term, attention is needed tothe economic and political power structures that influence health andhealth care and that ignore the social and societal determinants ofsustainable good health locally and globally. This long-term vision ofhealth is needed globally to achieve improvements in individual andpopulation health in a century characterised by limits to economicgrowth, widening disparities, continuing conflict and migration on alarge scale and multiple adverse impacts of climate change.
ARTICLE HISTORYReceived 23 September 2017Accepted 17 November 2017
KEYWORDSSouth Africa; Canada; health;health services; funding;National Health Insurance;social innovation; ecology
Introduction
The state of human health varies strikingly across the globe with gaps remaining so wide that long-term human security is threatened on many fronts in an increasingly unstable world (Benatar, 1998,2001, 2015a; Garrett, 1994). Debates about improving equity in access to health care, narrowing gapsin health locally and globally and regarding global health governance in an era of emerging newinfectious diseases, with potentially disastrous consequences, have been long-standing, pervasiveand controversial (Gill & Benatar, 2016; WHO, 2008). Equitable access to health care services iswidely, and with some justification, seen as a high priority for reducing inequitable health statuswithin countries. Universal access to health care (UHC), long advocated by WHO, is again beingdescribed within the Sustainable Development Goals (SDGs) as a major global political goal andethical endeavour (World Bank, 2003; Reis, 2016).1 It is being strongly promoted as a panacea forhealth inequities, and is manifesting in different jurisdictions as voluntary insurance schemes, auton-omous programmes for the poor only, and parallel private insurance or co-payments for servicesbeyond a basic package (Cotlear, Nagpal, Smith, Tandon, & Cortez, 2015), and has been ratified
© 2017 Informa UK Limited, trading as Taylor & Francis Group
CONTACT Solomon Benatar [email protected], [email protected]
GLOBAL PUBLIC HEALTH, 2017https://doi.org/10.1080/17441692.2017.1407813
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18
as one of his priorities by the new Director-General of theWorld Health Organization (WHO). Somesuccess in reaching this goal has been gratifying (for example in making treatment widely availablefor HIV and AIDS in South Africa and elsewhere), but much less impressive than what could havebeen achieved, given available resources, medical advances and our knowledge of the implications ofchanging patterns of disease in ageing populations in the context of local/global/planetary healthchallenges.
Here we contrast and compare some illustrative data about health disparities, health funding andaccess to health care in two very different countries, Canada with 2016 per capita GDP of $42,156and South Africa with per capita GDP of $5273 (World Bank SA Data Portal, 2015) to illustrate thecomplexity of achieving greater equity even in wealthy countries and to reveal potential bi-direc-tional lessons of relevance to local and global public health about health care funding approachesand other potential means of reducing health inequities in the future. The rationale for the choiceof these two countries is based on the facts that (i) they both have heterogeneous populations spreadacross large land masses and face complex challenges, including meeting their respective aspirationsto improve equity in health and health care, although from very different social contexts and econ-omic status, (ii) both have marginalised populations linked to their colonial history and patterns ofsocio-economic development, (iii) all the authors have interests in health care equity and in the con-trasts within and between these two countries and (iv) Canada has contributed indirectly to healthinequity in South Africa through recruitment of physicians and nurses.
Health
Good health is in the first instance, and most importantly, dependent on the social, economic andpolitical environments that support populations effectively, so that individuals are able to flourishfrom conception, through adulthood and into old age (Marmot, Bloomer, & Goldblatt, 2013). In jur-isdictions where, in addition to favourable social/environmental conditions for good health, there isaccess to effective health care ‘from womb to tomb’, spectacular advances in modern medicine haveadded considerably to longevity and healthy lives. Access to health care services, like access to edu-cational services, should ideally be thought of as an essential social function to be available to allpeople as citizens of equal moral worth.
Although often ignored, it is notable that the social conditions conducive to good health andaccess to effective health care modalities are available only to a small minority of the world’s popu-lation (about 20–30%) (Benatar, 1998, 2015b ; Kochhar, 2015), while an increasing number of peopleare being displaced into a precarious state of life (Standing, 2014). Even in affluent countries, such asCanada, poverty and other social conditions marginalise many citizens (both within dense urbanareas and in remote locations), and especially First Nations’ People, from advantages available toothers. While rapidly advancing and expensive modern, technologically based and commercialisedmedical care, together with public health interventions have dramatically improved health andhealth care for some, they have simultaneously contributed to widening local and global disparitiesin access to these benefits and to health and longevity (Birn, 2011).
The scale of disparities across the world is succinctly portrayed by six statistics: (i) maternal mor-tality in 2015 ranged from 7 per 100,000 pregnancies in Canada, to 134 in South Africa, 789 inSouthern Sudan and 1360 in Sierra Leone (range 999–1980) (WHO, 2015a), (ii) the death rateunder 5 years ranges from 5 per 1000 live births in Canada to 137 per 1000 live births in Somalia(World Bank, 2012) where the average fertility rate is 6.6 children per woman and 1 out of every12 women dies due to pregnancy related causes (Child and Maternal Health UNICEF 2012;World Bank, 2012), (iii) life expectancy at birth spans the wide range of 49 years to over 80 years(WHO, 2015b), (iv) per capita income in 2016 ranged from $302 in Malawi to $78,000 in Switzer-land and $102,000 in Luxembourg (World Bank, 2015), (v) annual per capita health care expenditurein 2014 extended from a low of less than $50 in many poor countries to over $9000 in the U.S.A.(WHO, 2015a), (vi) the number of physicians per 100,000 people ranges from 2 in Malawi to 351
2 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

in the U.S.A., 328 in Sweden and 591 in Cuba (Physicians per 100,000 People, by Country, 2017).Within most countries, these patterns of difference also persist with dramatic (although typicallysmaller) differences in life expectancy and other key metrics of health between the highest and lowestsocio-economic groups and across population groups.
Many health disparities are preventable and therefore inequitable, but not inevitable as illustratedwith the success of the Brazilian Bolsa Familia in reducing disparities (Tepperman, 2016). TheWHOcommission on the social determinants of health (SDOH) highlighted multiple examples of evidencefor successful improvements in the health of populations based on employment conditions among arange of other themes (WHO, 2008). We note here that equity is not the same as equality. Equity isan ethical concept, grounded in principles of distributive justice and human rights. Health inequitiesare differences that are unnecessary, avoidable, unfair and socially unjust and that systematically putthe already socially disadvantaged at a further disadvantage with respect to health (Whitehead,1992).
Health care systems/services
Health care systems around the world are diverse mixtures of the public- and privately funded ser-vices with widely differing cost implications for patients and payers and variable impacts on access tocare and on health outcomes. Health care reform over many decades has been shaped by a dialecticbetween the ideals of the welfare state based on solidarity within civil societies that respect a broadrange of human rights, and an increasingly dominant neoliberal market civilisation attuned to free-dom of choice and dominance of civil and political rights.
It should be acknowledged that health care services everywhere are distorted (with the structure ofhealth systems not closely geared to the burden of disease), dysfunctional (because of the intrusive-ness of commercial and bureaucratic considerations) and unsustainable (because of fragmentation,lack of co-ordination of care and failure to set priorities explicitly in the face of demands for healthcare which exceed the ability to supply such care) (Campbell, Morris, & Marsh, 2017; Rosenthal,2017). Distortions are aggravated by funding mechanisms that fail to focus on the value of care(creating and sustaining health and satisfaction with health status, at the lowest possible cost), theways that social factors interfere with access to care (even when free at the point of consumption)and that re-enforce barriers between health and social services. Finally, accountability structuresthat do not promote transparency regarding expenditure and outcomes miss the opportunity tobegin correcting these distortions, dysfunctions and sustainability challenges. Both the Canadianand South African health systems – to the extent that they can be described as systems – are bur-dened by these problems.
Currently evolving global economic challenges have fostered realisation that even in wealthycountries endless economic growth and ongoing escalation of expenditure on health care cannotcontinue unchecked (Benatar, Gill, & Bakker, 2009, 2011; Brill, 2013). In addition, health service pol-icies and priorities tend to be determined more by specific ideological, scientific or medical interestssuch as the driving forces of ambitious individual physicians intent on developing specific services,and such commercial stimuli as the pharmaceutical industry and partnerships with technology com-panies in developing new medical prostheses and diagnostic instruments. These personal, financialand commercial forces have in the past been more influential than deliberate attempts to achieve aneconomically optimal mix of services that could maximise outcomes of biomedical health care.
Attempts to control and standardise health care services and ensure accountability have spawned acomplex bureaucracy that, while advantageous in some ways, also poses significant impediments (Nay-lor et al., 2015). These challenges are faced by all nations attempting to reform their health services andbyinternational organisations seeking to improve global health. The U.K. has set an admirable example inestablishing aNational Institute forHealth andCare Excellence (NICE, 2017) in an attempt to overcomedifferential availability of treatments dependent on theNational Health ServiceHealthAuthority area inwhich the patient happens to live. It has become well known internationally as an exemplary model for
GLOBAL PUBLIC HEALTH 3
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

the development of clinical guidelines, based on the explicit determination of cost–benefit analyses(NICE, 2017).
Some comparative health-relevant data
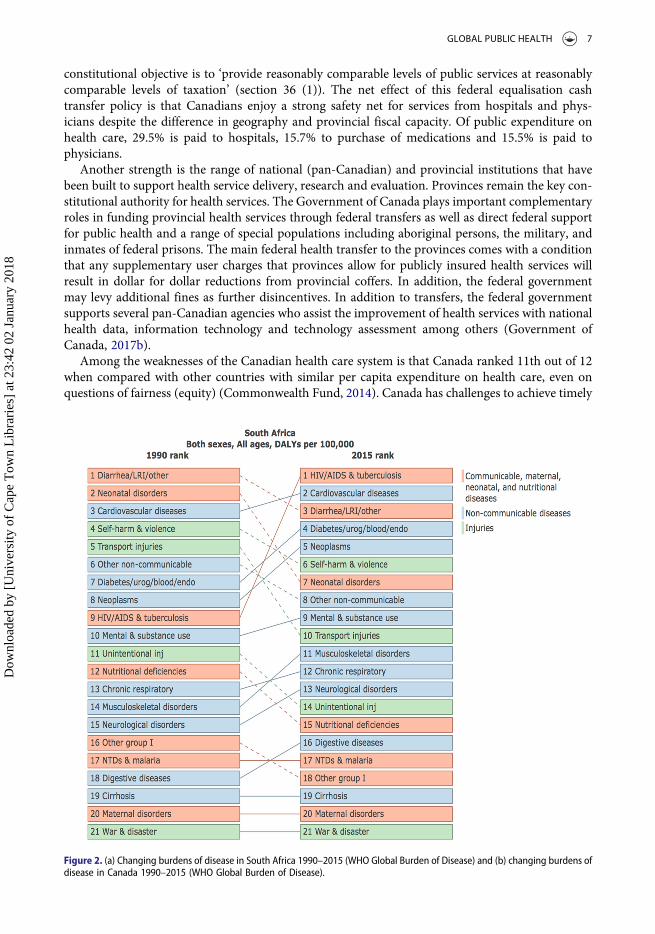
The extent of the many differences in life and health within and between South Africa (Kon & Lac-kan, 2008) and Canada (Cameron, del Pilar Carmargo Plazas, Santos Salas, Bourque Bearskin, &Hungler, 2014) is succinctly illustrated in the shape of the respective population pyramids (Figure 1)(CIA World Factbook, 2014, 2016) and in Table 1. South Africa has a higher ratio of young to oldthan Canada, where middle-aged and older people are preponderant with many implications forhealth care today and into the future. The distribution of diseases contributing to the overall burdenof diseases is also very different (Table 1, Figure 2(a,b)) (WHO, 2016a). For example consider theincidence of tuberculosis (TB) and prevalence of HIV infection, the number of people per millionwho have access to renal dialysis and transplantation and the differences between such access inthe public and private sectors in South Africa (Moosa, Maree, Chirehwa, & Benatar, 2016).
The spectra of diseases, with greater prominence of infectious diseases in South Africa, reflects thedelayed and as yet incomplete epidemiologic transition resulting from failure to achieve morebalanced access to the SDOH during the racially divisive colonial and apartheid periods, the diffi-culty of dealing with TB over many decades, and the devastation associated with the HIV andAIDS epidemic, inclusive of the recrudescence of TB and the emergence of drug-resistant strains(Benatar, 2004).
We have previously described the South African government’s arrogant denial of the link betweenHIV infection and AIDS in the face of overwhelming scientific evidence provided by the global scien-tific community, and its failure to promote an early prevention campaign. Its initial focus on inef-fective treatments contributed to the sustained and pervasive denial of the existence of the HIVpandemic as well as the perpetuation of the stigma associated with HIV and AIDS. It has alsobeen noted that although the president, minister of health and others in the government long pub-licly denied the link between HIV and AIDS and failed to provide high-profile leadership on thisissue, the Ministry of Health had quietly formulated a comprehensive national strategic plan forHIV and AIDS that included such vital components as education, programmes for the modificationof sexual behaviour, and treatment of opportunistic infections. The many obstacles that frustratedthe introduction and maintenance of comprehensive and effective programmes for preventing thetransmission of HIV and for treating infected patients with antiretroviral drugs were eventually over-come and the local production of generic drugs and further substantial reductions in prices becamepossible (Benatar, 2004; Kevany, Benatar, & Fleischer, 2013).
Thus after many years of government denial and minimal funding for HIV and AIDS, local andinternational pressures resulted in the introduction of an ambitious national programme to provideantiretroviral therapy (ART) to all patients with HIV infection in South Africa. Treatment of an ever-expanding number of patients resulted in HIV and AIDS expenditure increasing at an averageannual rate of 48.2% between 1999 and 2005 – consistently higher than in other areas of nationalhealth expenditure, and continued at an annual rate of approximately 25%, with dedicated HIVfunding estimated at $400 million (in U.S. dollars) per annum, of which about 40% comes frominternational donors. More than 2 million of 6 million HIV-positive South Africans receive ART.Life expectancy for them has returned close to that of demographically matched patients who arenot HIV positive (Mayosi & Benatar, 2014). The large number of untreated HIV positive personsaccounts for increasing numbers of disability adjusted life years (Figure 2(a)).
The 2003, 2007 and 2011 national plans for HIV, with funding increasingly skewed toward HIVtreatment for many more patients, had implications for a deteriorating national public health systemcommitted to equitably serving all South Africans (Fleischer, Kevaney, & Benatar, 2005; Kevanyet al., 2013). For those concerned about spending a large proportion of the health budget on patients
4 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

with HIV and AIDS it is noteworthy this expenditure adds many decades of extra life for each patienttreated as compared with expenditure on often futile aggressive treatments in the last years of life.
As also previously described South Africa also has one of the worst TB epidemics in the world. In2007, South Africa, with 0.7% of the world’s population, had 17% of the global burden of HIV infec-tion, with its TB epidemic compounded by rising drug resistance and HIV co-infection (AbdoolKarim, Churchyard, Abdool Karim, & Lawn, 2009). Driven by the spread of HIV infection, the
Figure 1. Population pyramids South Africa 2016 and Canada 2014 (CIA World Factbook).
GLOBAL PUBLIC HEALTH 5
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18
incidence of TB increased from 300 per 100,000 people in the early 1990s to more than 600 per100,000 in the early 2000s, and to more than 950 per 100,000 in 2012. Despite notable progressin improving treatment outcomes for new smear-positive TB cases, the TB burden remains enor-mous. Multidrug-resistant (MDR) TB accounts for 1.8% of all new cases of TB (and 6.7% of retreat-ment cases). A study involving patients with extensively drug-resistant (XDR) TB in rural SouthAfrica made international headlines, and South Africa reported the most XDR TB cases in theworld. Annual notifications increased from 298 in 2005 to 1545 in 2012. Approximately 10% ofMDR TB cases reported in South Africa are XDR TB cases (Mayosi & Benatar, 2014). TB remainsthe leading underlying natural cause of death in 2015 with 460,236 deaths from TB that year(accounting for 7.2% of deaths, with diabetes mellitus in 2nd place (5.4% of deaths) (allAfrica, 2014).
Canadian health care – strengths and weaknesses
One of Canada’s major strengths is that it has what many consider to be a desirable universal healthcoverage system founded on admirable principles, including most notably public administration, thatfor annual expenditure of 10.9% of GDP on health – about $219 billion in 2015 ($6105 per capita)delivers better overall population health than the U.S.A. (Guyatt et al., 2007) where per capita expen-diture on health care is over $8000 (almost 20% of GDP) (Kaiser Family Foundation, 2007). In 2012among countries with comparable accounting systems, Canada was in the top quartile of 30 Organ-isation for Economic Co-operation and Development (OECD) countries with per capita healthexpenditure at U.S.$4602, below that of the U.S.A. (U.S.$8745) and comparable with figures for Den-mark (U.S.$4698) and Luxembourg (U.S.$4578) (National Health Expenditure Canada, 2014).
Insured health care services in the context of the Canada Health Act, means hospital services,physician services and some surgical–dental services provided to insured persons. A Canadian
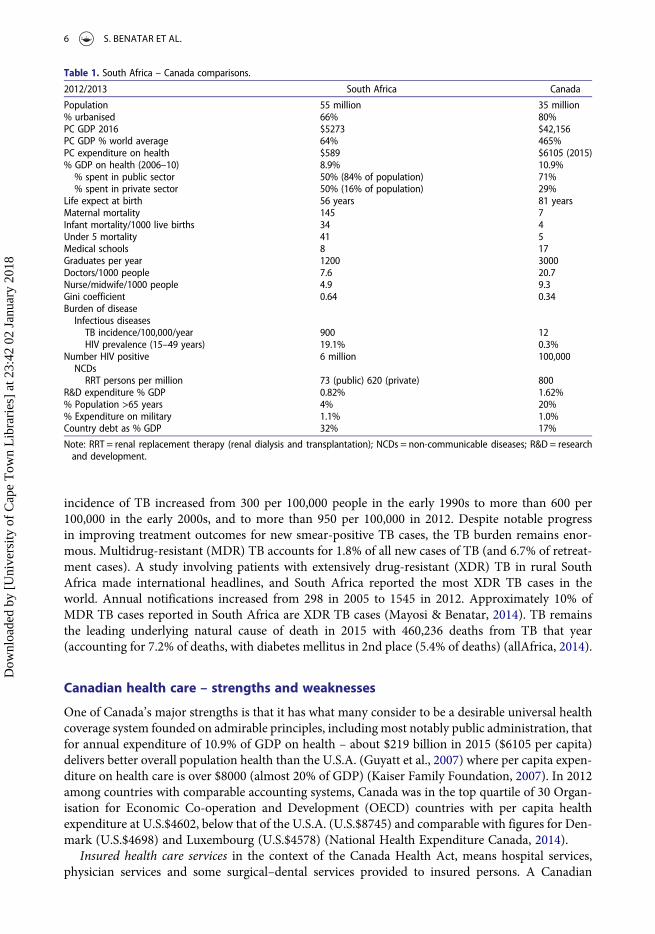
Table 1. South Africa – Canada comparisons.
2012/2013 South Africa Canada
Population 55 million 35 million% urbanised 66% 80%PC GDP 2016 $5273 $42,156PC GDP % world average 64% 465%PC expenditure on health $589 $6105 (2015)% GDP on health (2006–10) 8.9% 10.9%% spent in public sector 50% (84% of population) 71%% spent in private sector 50% (16% of population) 29%
Life expect at birth 56 years 81 yearsMaternal mortality 145 7Infant mortality/1000 live births 34 4Under 5 mortality 41 5Medical schools 8 17Graduates per year 1200 3000Doctors/1000 people 7.6 20.7Nurse/midwife/1000 people 4.9 9.3Gini coefficient 0.64 0.34Burden of diseaseInfectious diseasesTB incidence/100,000/year 900 12HIV prevalence (15–49 years) 19.1% 0.3%
Number HIV positive 6 million 100,000NCDsRRT persons per million 73 (public) 620 (private) 800
R&D expenditure % GDP 0.82% 1.62%% Population >65 years 4% 20%% Expenditure on military 1.1% 1.0%Country debt as % GDP 32% 17%
Note: RRT = renal replacement therapy (renal dialysis and transplantation); NCDs = non-communicable diseases; R&D = researchand development.
6 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18
constitutional objective is to ‘provide reasonably comparable levels of public services at reasonablycomparable levels of taxation’ (section 36 (1)). The net effect of this federal equalisation cashtransfer policy is that Canadians enjoy a strong safety net for services from hospitals and phys-icians despite the difference in geography and provincial fiscal capacity. Of public expenditure onhealth care, 29.5% is paid to hospitals, 15.7% to purchase of medications and 15.5% is paid tophysicians.
Another strength is the range of national (pan-Canadian) and provincial institutions that havebeen built to support health service delivery, research and evaluation. Provinces remain the key con-stitutional authority for health services. The Government of Canada plays important complementaryroles in funding provincial health services through federal transfers as well as direct federal supportfor public health and a range of special populations including aboriginal persons, the military, andinmates of federal prisons. The main federal health transfer to the provinces comes with a conditionthat any supplementary user charges that provinces allow for publicly insured health services willresult in dollar for dollar reductions from provincial coffers. In addition, the federal governmentmay levy additional fines as further disincentives. In addition to transfers, the federal governmentsupports several pan-Canadian agencies who assist the improvement of health services with nationalhealth data, information technology and technology assessment among others (Government ofCanada, 2017b).
Among the weaknesses of the Canadian health care system is that Canada ranked 11th out of 12when compared with other countries with similar per capita expenditure on health care, even onquestions of fairness (equity) (Commonwealth Fund, 2014). Canada has challenges to achieve timely
Figure 2. (a) Changing burdens of disease in South Africa 1990–2015 (WHO Global Burden of Disease) and (b) changing burdens ofdisease in Canada 1990–2015 (WHO Global Burden of Disease).
GLOBAL PUBLIC HEALTH 7
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

access for primary care, specialty care and some elective procedures. Rural areas are most adverselyaffected, with indigenous people throughout Canada being especially vulnerable. Access issues havealso been key considerations in the Chouilli constitutional decision (Flood & Sullivan, 2005), on pri-vate payment if wait times are excessive, in the ongoing case of Brian Day regarding the right to pri-vate surgical billing in British Columbia (Merti, 2016).
Another weakness is that Canadian provinces have a range of limitations on public coverage forpharmaceuticals, dental care and home and community care. These latter areas are particularly chal-lenging given dramatic growth in the ageing population in the country. Reasons for this are apparentfrom the evolution of Canadian Medicare, its key actors and geographic variations (Naylor, 1986;Naylor, Girard, Mintz, Fraser Jenkins, & Power, 2015). Inequities in access relate inter alia to thefact that up to 30% of health care expenditure in Canada is not covered by national insurance.This expenditure is mainly on drugs, rehabilitation and a small range of private services which isborne out of pocket (14%) with the heaviest burden falling on those without supplementary insur-ance typically obtained through employment benefits (Canadian Institute of Health Information,2015). Concern about expenditure on health care exceeding economic growth rates has focusedon many attempts to reduce the costs of health care (Choosing Wisely Canada, 2017; RomanowReport, 2002), rather than on explicit priority setting and allocation of resources that could providebetter health outcomes than can be achieved under conditions of implicit and occult resourceallocation.
Figure 2 Continued
8 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

It would seem that the evolution of access to health care in Canada has largely stalled (Marchil-don, 2013). In the last decade, attention has been focused on access to primary care and acute care,diagnostic imaging, and surgery. With increased funding, there has been some improvement in longwaiting times for elective procedures but minimal progress in access to primary health care (PHC)(Health Council of Canada, 2014). Care of the frail elderly or of patients suffering from multiplechronic diseases is less well managed. Despite regional restructuring within provinces and some con-solidation of primary care groups, there is stagnation of reforms related to reimbursement schemesfor providers, activity-based payment for hospitals and major health system performance improve-ments. Recent attention has focused on increasing public access to home care and to pharmacare,which have less well-specified and less complete levels of public coverage compared to physicianand hospital services.
The 2015Naylor report on health care innovation calls for the creation of a federal Healthcare Inno-vation Agency of Canada with a budget of at least $1-billion annually (Naylor et al., 2015). This wouldrequire a new philosophy that involves Ottawa having ‘ … a different model for federal engagement inhealth care – one that depends on an ethos of partnership, and on a shared commitment to scale exist-ing innovations and make fundamental changes in incentives, culture, accountabilities, and infor-mation systems’. Weighing all these inputs, and consistent with its mandate, five broad areas wereidentified where federal action was important to promote innovation and enhance both the qualityand sustainability of Canadian health care services and policy across the jurisdiction: (i) patient engage-ment and empowerment, (ii) health systems integration with workforce modernisation, (iii) techno-logical transformation via digital health and precision medicine, (iv) better value from procurement,reimbursement and regulation and (v) use of industry as an economic driver and innovation catalyst.
Thus, the Canadian system maintains a system of universal access but is facing significant issuesaround sustainability, to which there are few clear answers while issues of equity and more broadly ofaccess to some types of care (e.g. drugs) persist.
South African health care – strengths and weaknesses
The major weakness of health care in South Africa is its provision within an increasingly disparatetwo-tiered system (Table 1) with overall health expenditure in the country of R311 billion ($31 bil-lion) (8.6% GDP) during the 2013/2014 financial year.2 The evolution and structure of inequitablehealth care services have long been topics of critical debate within the context of the recent history(40 years of apartheid followed by a peaceful transition 23 years ago) (Benatar, 1986, 1997a; VanRensburg, 2012), its geographic location (in an increasingly impoverished subcontinent, longravaged by infectious diseases, exploitation, natural and human disasters) (Schwab, 2001) and withina broader global context shaped by global economic policies, that profoundly influence healthadversely (Benatar et al., 2009; Deloitte, 2015; Gill & Bakker, 2011; Mayosi & Benatar, 2014; Rowden,2009; Terreblanche, 2002).
Despite all the legislative, social and economic achievements in the first decade of the new SouthAfrica, some of which have been previously described (Benatar, 1991, 2004; Habib, 2013; Mayosiet al., 2009), increasing corruption within government and widespread mismanagement of publicenterprises, has aggravated the economic and health divide and many South Africans remain despe-rately deprived. While the two-tiered health care system has long been seen by some as a major weak-ness, it is unlikely that it will be displaced. The challenge is to capitalise on its strengths andweaknesses, and the establishment of National Health Insurance (NHI) is one method in whichmuch hope has been pinned to achieve this (vide infra).
Public sector
Health care in the publicly funded system is provided by 35% of the country’s doctors for 84% of thepopulation through national and provincial departments of health and through medical services in
GLOBAL PUBLIC HEALTH 9
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18
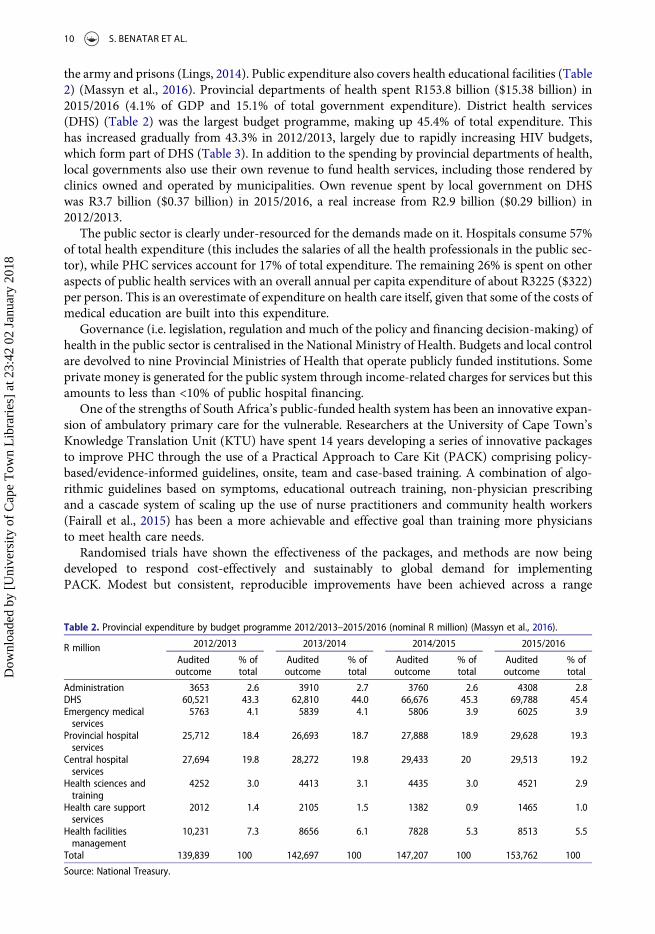
the army and prisons (Lings, 2014). Public expenditure also covers health educational facilities (Table2) (Massyn et al., 2016). Provincial departments of health spent R153.8 billion ($15.38 billion) in2015/2016 (4.1% of GDP and 15.1% of total government expenditure). District health services(DHS) (Table 2) was the largest budget programme, making up 45.4% of total expenditure. Thishas increased gradually from 43.3% in 2012/2013, largely due to rapidly increasing HIV budgets,which form part of DHS (Table 3). In addition to the spending by provincial departments of health,local governments also use their own revenue to fund health services, including those rendered byclinics owned and operated by municipalities. Own revenue spent by local government on DHSwas R3.7 billion ($0.37 billion) in 2015/2016, a real increase from R2.9 billion ($0.29 billion) in2012/2013.
The public sector is clearly under-resourced for the demands made on it. Hospitals consume 57%of total health expenditure (this includes the salaries of all the health professionals in the public sec-tor), while PHC services account for 17% of total expenditure. The remaining 26% is spent on otheraspects of public health services with an overall annual per capita expenditure of about R3225 ($322)per person. This is an overestimate of expenditure on health care itself, given that some of the costs ofmedical education are built into this expenditure.
Governance (i.e. legislation, regulation and much of the policy and financing decision-making) ofhealth in the public sector is centralised in the National Ministry of Health. Budgets and local controlare devolved to nine Provincial Ministries of Health that operate publicly funded institutions. Someprivate money is generated for the public system through income-related charges for services but thisamounts to less than <10% of public hospital financing.
One of the strengths of South Africa’s public-funded health system has been an innovative expan-sion of ambulatory primary care for the vulnerable. Researchers at the University of Cape Town’sKnowledge Translation Unit (KTU) have spent 14 years developing a series of innovative packagesto improve PHC through the use of a Practical Approach to Care Kit (PACK) comprising policy-based/evidence-informed guidelines, onsite, team and case-based training. A combination of algo-rithmic guidelines based on symptoms, educational outreach training, non-physician prescribingand a cascade system of scaling up the use of nurse practitioners and community health workers(Fairall et al., 2015) has been a more achievable and effective goal than training more physiciansto meet health care needs.
Randomised trials have shown the effectiveness of the packages, and methods are now beingdeveloped to respond cost-effectively and sustainably to global demand for implementingPACK. Modest but consistent, reproducible improvements have been achieved across a range
Table 2. Provincial expenditure by budget programme 2012/2013–2015/2016 (nominal R million) (Massyn et al., 2016).
R million 2012/2013 2013/2014 2014/2015 2015/2016
Auditedoutcome
% oftotal
Auditedoutcome
% oftotal
Auditedoutcome
% oftotal
Auditedoutcome
% oftotal
Administration 3653 2.6 3910 2.7 3760 2.6 4308 2.8DHS 60,521 43.3 62,810 44.0 66,676 45.3 69,788 45.4Emergency medicalservices
5763 4.1 5839 4.1 5806 3.9 6025 3.9
Provincial hospitalservices
25,712 18.4 26,693 18.7 27,888 18.9 29,628 19.3
Central hospitalservices
27,694 19.8 28,272 19.8 29,433 20 29,513 19.2
Health sciences andtraining
4252 3.0 4413 3.1 4435 3.0 4521 2.9
Health care supportservices
2012 1.4 2105 1.5 1382 0.9 1465 1.0
Health facilitiesmanagement
10,231 7.3 8656 6.1 7828 5.3 8513 5.5
Total 139,839 100 142,697 100 147,207 100 153,762 100
Source: National Treasury.
10 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

of outcomes, including the care of patients with communicable and non-communicable diseases(Fairall et al., 2005). This is important, as strengthening one part of the health system is oftenaccompanied by weakening another part. Improvements extend beyond the quality of care indi-cators to patient health outcomes (unusual in trials of health systems) and included shifts inhealth care utilisation (reductions in length/duration of hospital admissions). This effective andempowering low-intensity delivery of educational outreach is highly acceptable and popularamong nurses and trainers. Ongoing amplification of such care has a future in South Africaand the hope is that integrated and innovative services could be achieved for low-incomeSouth Africans.
Private sector
The private health care system in South Africa has evolved into an expensive substitute for the publicsystem for the small proportion of the population it serves (16%), that is now inclusive of all ethnicgroups, who can afford health insurance coverage.3 Much of this is provided through enrolment incorporate health insurance plans, although it should be noted that the range of insurance that can bepurchased is very wide – from only in-hospital cover in a limited selection of hospitals, to muchwider cover, all dependent on what individuals with differing incomes can afford. The private sectorwas a much smaller component of health services in the 1960s and 1970s when all sophisticatedmedical care was provided for all who needed this, in teaching hospitals that were a major com-ponent of the state-funded public system. Erosion of the latter was accompanied by the growth ofthe private sector (Benatar, 1986, 2001). Within this moderately well-resourced fee-for-service pri-vate sector, patients have a considerable choice over their physicians who provide generally high-quality treatment. Expenditure in 2013/2014 amounted to R156 billion ($15.6 billion) of which81% came from private, prepaid medical schemes and medical insurance and about 14% fromout-of-pocket payments. Annual per capita health expenditure is R17,730 ($1773) with hospitalsaccounting for about 35.3% of expenditure, medications for 15.8% and payments to physiciansfor 28.5%.
Private health sector governance is fragmented across a wide range of health providers. TheCouncil for Medical Schemes (CMS) provides an overall framework of control, with some limitationsimposed on its functions by the government. The values of the CMS are claimed to stem from thoseunderpinning the Constitution of South Africa, and from the specific vision and mission of the CMSthat subscribes to a rights-based framework – where everyone is equal before the law, the right ofaccess to health care must be protected and enhanced, and access simplified in a transparent manner
Table 3. DHS sub-programme objectives (Massyn et al., 2016).
District management: Planning and administration of services; managing personnel and financial administration; co-ordination andmanagement of the day hospital organisation and community health services rendered by local authorities and non-governmental organisations within the metro; determining work methods and procedures; and exercising district control.
Community health clinics: Rendering a nurse-drivenPHC service at clinic level, including visiting points, mobile clinics and localauthority clinics.
Community health centres: Rendering a primary health service with full-time medical officers in respect of mother and child health,health promotion, geriatrics, occupational therapy, physiotherapy, psychiatry, speech therapy, communicable diseases, mentalhealth, etc.
Community-based services: Rendering a community-based health service at non-health facilities in respect of home-based care,abuse victim care, mental health and chronic care, school health, etc.
Other community services: Rendering environmental and part-time district surgeon services, etc.HIV and AIDS: Rendering aPHC service in respect of HIV and AIDS campaigns and special projects.Nutrition: Rendering a nutrition service aimed at specific target groups and combining direct and indirect nutrition interventions toaddress malnutrition.
Coroner services: Rendering forensic and medico-legal services in order to establish the circumstances and causes surroundingunnatural death.
District hospitals: Rendering of a hospital service at the district level.
Source: National Treasury.
GLOBAL PUBLIC HEALTH 11
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

(Council for Medical Schemes, 2014–2015). All the insurance companies are obliged to take onpatients with common chronic medical conditions and to include cover for their medications.The CMS aims to regulate the medical schemes industry in a fair and transparent manner andadvises the National Minister of Health on appropriate regulatory and policy interventions thatwill help achieve national health policy objectives.
Development of NHI
The many historical milestones in the quest for UHC are recorded in the recent White Paper on NHI(2015). The central aim of the Department of Health’s Draft Charter of the Public and Private HealthSectors was to address the legacy of apartheid regarding access to health care for all South Africans(Reynolds, London, & Sanders, 2005). There has been an ongoing emphasis on equitable access tohealth within a PHC oriented system, with simultaneous support for private medical care forthose who are able to afford more sophisticated health care. Support includes approval of the pro-vision of social services by private organisations and some tax relief for private expenditure on healthcare, which saves the nation from having to provide health care for its privileged classes.
The admirable principles underlying the quest for NHI in South Africa include, the (progressivelyachievable) right to universal access to a comprehensive set of health services with a continuum ofcare from community outreach, health promotion and prevention to other levels of care. Paymentfrom a single payer and a single fund is intended to provide financial risk protection against financialhardship without deterrence from accessing and utilising needed health services. NHI is also viewedas a means to enhancing social solidarity, through health care as an affordable public good providedwithin efficient, effective, appropriate and innovative service delivery models tailored to local needsand delivered at appropriate levels of care.
The aspiration is to create a unified health system by improving equity in financing, reducingfragmentation in funding pools, and by making health care delivery more affordable and accessiblefor the population – in particular at the PHC level – and to eliminate out-of-pocket payments (Whitepaper on NHI, 2015). Movement towards NHI is a priority political goal for the African NationalCongress Government, and its implementation is planned to take place in 3 phases over a 14-yearperiod, with re-engineering of PHC through 4 streams to improve timely access, and to promotehealth and prevent disease: a municipal ward-based PHC outreach team, an integrated school healthprogramme, a district clinical specialist team and contracting of non-specialist health professionals.Major hurdles include geographic disparities and long-standing tensions between publicly and pri-vately provided health care that sustain inequity in access to and provision of health care. Initiativesto improve management and governance of health facilities at the PHC and hospital levels areplanned through strengthening their physical structures, administrative functions, financial manage-ment and accountability.
Antagonism to the private sector has recently been softened, with the Department of Healthreconsidering its approach on the role of the private sector in implementing NHI, thus openingthe way for the industry to play a greater role (Kahn, 2017). It should be noted that this representsacknowledgement that within health reform debates shaped by a dialectic between the opposingideas of health care services as a social good governed by a concept of social-efficiency and the mar-ket efficiency ideas of neoliberal capitalism, the power of the latter, as promoted by the World Devel-opment Report (World Bank, 1993, 2003), helped transform the operation of the state sector into aparticipant in the capitalist market place.
NHI funding is planned through personal taxation and mandatory employer contributions. Costestimates from the White Paper on NHI indicate that the roll-out of NHI will require about R10.4billion ($1.04 billion) every year (total of R145 billion ($14.5 billion) in real terms over the next 14years), over and above current expenditure on public health care (‘Health financing and NationalHealth Insurance in South Africa’, 2012; KPMG, 2017). These additional resources would increaseannual expenditure in the public sector from R149 billion ($14.9 billion) to R159 billion ($15.9
12 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18
billion) (about 7%), a significant boost, in particular as those who contributed these additionalamounts would probably continue using their private health insurance, thus enabling enhancedcare for the poor in the public sector. However, the gap between private and public sector serviceswould only be marginally narrowed (Benatar, 2013). Much more money will be required to signifi-cantly narrow the overall gap, and increased taxation of the small proportion of the population pay-ing personal income tax, is the only possibility of achieving this, unless savings can be achieved fromother public expenditure, for example, military activities (Visser, 2016). Twenty per cent of the popu-lation accrue 83% of the total annual income and the country has a small tax base. Of 51 millionSouth Africans, 13.7 million are registered as tax payers, 3.3 million pay income tax, 8.1% of all tax-payers earn R500,000 ($50,000) or more and they pay the majority of national personal income tax(Gon, 2013; Rolling Alpha, 2017).
In 2014 the government began selecting pilot sites and conducting various projects in selecteddistricts, with significant national and provincial support, as precursors for the roll-out of NHI.Such plans, like so much else in South Africa (as in many lower and middle income countries(LMICs)), are not matched by the ability to put them into effective practice (Kahn, 2016). Giventhe distribution of forces conducive to improved health and access to health care, and taking intoaccount the failure of wealthy countries like Canada to achieve greater equity, it is arguably naivelyoptimistic to highlight NHI in South Africa as the major route to reducing health inequities (Mayosi& Benatar, 2014).
Estimates of the extent of human resource requirements for staffing PHC in South Africa using anadapted, WHOwork load tool, have identified some important resource challenges (Daviaud & Cho-pra, 2008) with eight thematic priorities defined (South African Government, 2011; Street, 2016).These priorities4 are all admirable goals, but the means of implementing them have not been clearlydefined and the skills required remain to be developed. Doubts about the workability of the NHIhave generated an alternative ‘Our Health Plan’ (James, 2016a). Scholarly work on health policyanalysis in LMICs (Gilson & Raphaely, 2008) provides insights into the importance of carefully con-sidering the kaleidoscope of social, economic and cultural contexts that characterise a country likeSouth Africa (Gilson & McIntyre, 2008). These considerations are complicated by the potentialrole of traditional health practitioners (THPS) (Answers Africa, n.d.), and the many complexitiesassociated with regulating 200,000 THPs. Incompetence at many levels within the governmentand in health services also needs attention and rectification (Odhiambo, 2010). Thus, while SouthAfrica pursues universal access it faces even more significant challenges around sustainability thatspan the legitimacy of the system(s) and its capacity to modernise and make good on the promiseof universal access.
Health professional requirements and their mobility in both countries
There are also major challenges in terms of health professional requirements. For example, there is adeficit of 80,000 professional nurses in South Africa (James, 2016b). Recruitment of health pro-fessionals into wealthy countries from poorer countries, with little consideration for health andother costs to citizens of those countries, is one of the many adverse manifestations of globalisation.Of the estimated 60 million health care workers in the world, a third are in the Americas, while onlyabout 3% are in Africa which bears 25% of the global burden of disease and is hardest hit by theadverse effects of globalisation and medical migration (Benatar, 2007, 2015b). In the early 2000s,international medical graduates accounted for between 23% and 28% of physicians in the U.S.A.,the U.K., Canada and Australia (the major recipient countries in the world) (Mullan, 2005). Low-income countries supply 40–75% of these international graduates (Whelan, Arkles, Dewdney, &Zwi, 2004). In Canada’s rural Saskatchewan more than 50% of doctors are immigrants and about20% of doctors working there obtained their first degree in South Africa. In 2002, 7% of Canada’snurses were foreign graduates – 27% of these coming from the Philippines (and almost 25% fromthe U.K.) (Labonté, Packer, & Klassen, 2006).
GLOBAL PUBLIC HEALTH 13
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Retention of health professionals is a problem for South Africa and Canada. Recognition of thehigh-quality training of health professionals in South Africa has resulted in active recruitment oflocal graduates into wealthier countries. In Canada, there is little option but to keep professionalincomes close to American neighbours if only to prevent the outmigration of health professionalsto the U.S.A. because of better pay. This has occurred periodically in the last few years for nursesand doctors largely over issues regarding full-time employment (McGillis Hall et al., 2009), but cur-rent social changes in the U.S.A. may change this.
Solutions to migration have been sought at many levels ranging from ethical arguments, appealsto individuals to be loyal to practising in their home countries and to Governments to improvehealth governance and conditions of service to enable retention of skills in the country at least forsome minimum time after qualification (Brock & Blake, 2015) and, not uncontroversially, allowingsome limited private practice to full-time public physicians. Some have suggested trying to preventwealthy nations from actively recruiting or at least to pay developing countries for the costs of edu-cating the professionals they recruit (Benatar, 2007).
Bi-directional lessons
There are four main bi-directional and global public health lessons to be learned from this briefoverview of health care services in two very different countries. The first is that greater equity inhealth care and in health outcomes could be achieved through explicit priority setting and resourceallocation decision-making. The second is that although an efficient, well-funded, single-payer pub-lic service system may be the ideal, it is unlikely in either country that a private sector is entirelyavoidable. Third, narrowing inequity in health care and in health cannot be achieved through bio-medical means alone, without attention to the SDOH. Finally, within the context of many globaland planetary threats new approaches will be needed to develop sustainable improvements inhealth.
Priority setting/resource allocation
It is notable that despite almost 10 times the per capita GDP and per capita expenditure on healthcare in Canada than in South Africa, glaring disparities in health persist in Canada. The lesson here isthat it is not just more money that is needed but also a reconsideration of how that money should bespent within health care. The challenge is to do better with less and hence the need for explicitresource allocation policies. Much scholarly work on, and clinical application of, well-developedresource allocation policies has shown the value of such an approach (Benatar & Ashcroft, 2017;Ham & Coulter, 2001). As admirable as the Canadian health care system may be, its governanceand architecture are becoming outmoded, notwithstanding radically egalitarian provisions for phys-ician/hospital services and some progress at levelling out the disparity in access to those services.However, given that the focus on the notion of reasonable compensation to physicians has resultedin a fairly stilted set of predictable negotiations with the main professional bargaining bodies forphysicians, there is a less than desirable level of focus on value, quality and performance in suchagreements (Lewis & Sullivan, 2013).
In both South Africa and Canada, the allocation of resources and priority setting are highlylinked to physician preferences and commercial forces as mentioned earlier. Over the past twodecades, there has been significant work and some notable successes in the use of health technol-ogy assessment and, more specifically, cost-effectiveness analysis in Canada to inform coveragedecisions for expensive drugs and to set priorities including an ongoing regulatory reform ofpharmaceutical products at entry (Government of Canada 2017a; Levin et al., 2011; Young, Chat-wood, & Marchildon, 2016).
However, there is a need to go beyond such technical measure and an ethical basis, inclusive ofconcern for the principle of justice in health care must underpin much-needed priority setting
14 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

processes to achieve improved population health outcomes. Given the lack of consensus on substan-tive definitions of justice for setting priorities in health care, successful application of transparent andaccountable priority setting (procedurally fair) processes to some high-cost clinical problems and thetriage of access to expensive facilities such as renal dialysis and transplantation in South Africa(Moosa et al., 2016), and to some health services in Canada (Gibson, Martin, & Singer, 2004,2005) could be more widely applied to resource allocation decisions for increasingly large segmentsof the health care system. To do so it will be necessary to have comprehensive knowledge of the dis-tribution of health care costs across the health care system (hospitals and the cost of different serviceswithin these, and in community services), to identify high-cost areas and re-evaluate these. Hospitalsoperate within global budgets and detailed information is lacking about the distribution of expendi-ture across disciplines and of the quality of care provided or the results achieved.
The need to explicitly and rationally set defensible limits on very expensive and minimally ben-eficial practices, must also be acknowledged, even though this may mean withholding or withdraw-ing treatment from some who could benefit only marginally. This does not imply that patientsshould be abandoned, but rather that supportive palliative care, delivered with compassion andmaximum respect for individual comfort should be encouraged where this is most appropriate(Gawande, 2010).
The recent controversy over continuing treatment under conditions of futility exemplifies theneed for explicit priority setting when public resources, contributed to by all, are being spent(CBC News, 2013; Klitzman, 2017). There are vast lost opportunity costs associated with desperateattempts to keep people alive for a few more months in ICU’s, when hope for longer life is minimal.The Charlie Gard case and the Rasouli case, are good examples (CBC News, 2013; Klitzman, 2017). Itis also important to acknowledge that the lives of some (for example infants and dying elderly adultswith prognoses limited to survival in non-sentient states) seem to be valued more than the lives ofothers (for example patients with HIV and AIDS who can lead active and productive lives for manyadditional years on antiretrovirals).
It has been cogently argued that
an interpretation of the right to health that ignores resource limitations can only be sustained at the expense ofuniversality if only a small proportion of the population is granted the unlimited right to any benefits at anygiven time.
The minority of individuals who are granted this unlimited right via the judiciary are therefore pri-vileged over the rest of the population. In essence, the challenges are to find a balance between therationality of private self-interest and the rationality of public health interest.
One of the lessons that South Africa may take from Canada is the need to engage constantly withthe public in ways that reflect changing social mores in the setting and maintenance of standards forcoverage. In both Canada and South Africa, such considerations do not imply a need to relinquishthe quest for progress or excellent medical attention throughout the life cycle. Indeed, high-costmedicine in itself should not be a deterrent to the provision of sophisticated health care. Judicioususe of expensive and effective medical and surgical treatments provides great benefits for many,including saving the lives of some very young as well as elderly people, and should be strongly sup-ported. A second lesson may be the importance of capacity development – where Canada hasinvested heavily – which can help integrate the use of transparent and rational priority setting pro-cesses into management activities.
A mix of public and private health care and funding
The role of private medicine needs to be reconsidered. Both in Canada and in South Africa this sectorshould neither be ignored, nor over or under played. The pragmatic short-term aim should be tocapitalise on the strengths of both the private and the public sectors and to reduce their weaknessesby constructively altering the balance between them.
GLOBAL PUBLIC HEALTH 15
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Two-tier payment systems can provide a safety net but they cannot adequately control costs in theprivate payer system. Goals regarding total expenditure on health and on public expenditure onhealth, need to be clearly specified. In pursuing such goals, it should be appreciated that whereverthe private system goes, the public pressures will also tend to increase – a reality for both countriesin this comparison. Canada may well be compromised now because the social consensus is obsessedwith avoiding private insurance for publicly insured services. But it should also be noted that manyhealth professional services within the universally accessible care system, covered by national healthinsurance are paid for on a fee-for-service basis (Naylor, 1986). With no alternative, some in themedical profession may seek to re-shape the ethos of organised medicine with consequent adverseeffects on health care reform. The intensity of the antagonism between supporters of private andpublic funding of health care in the Tommy Douglas era is illustrative (Lam, 2011).
Two-tier systems also cannot fully protect against the brain drain between countries althoughhigher overall compensation does seem to have some stability impact when looking at the differencesbetween retaining physicians in South Africa and Canada (Brock & Blake, 2015). In South Africa, therights of full-time public service physicians to limited private practice, and preservation of a privatesector for the practice of tertiary medicine, play a significant role in overcoming the cutbacks in ter-tiary medicine at the teaching hospitals that can drive ambitious physicians out of the country (Bena-tar, 1997a, 2004). Moreover, the lesson to both countries is that two-tier systems are neithernecessary nor sufficient to prevent brain drain. Overall compensation and work life as well as therelative attractiveness of other markets can have as much or greater impact.
Rather than attempting only to extend the private insurance model, focusing on equal access tophysician and hospital services, it may be preferable to limit universal coverage to some services, cov-ering as much as possible for those who need financial assistance, and to allow some element of two-tier service (as in Germany) based on ability and willingness to pay. This would need to be done in aninnovative, comprehensive and integrated way, rather than having some services more equal thanothers within a distorted, dysfunctional and unsustainable system.
Excessive focus on private medicine can create problems where investments that could providethe biggest return in health status are unaffordable in the context of often inappropriate demandfor and use of high-cost technology. With the phased introduction of NHI in South Africa it willbe essential to enhance the ability to efficiently and effectively utilise additional taxation for NHIto improve access to health care in the public sector, within which improved integrated and coop-erative services could be coupled to community participation, and targeted specifically at those areascharacterised by the widest disparities. It will also be necessary to develop partnerships with the pri-vate sector, despite potential disadvantages (Flood & Archibald, 2001). Success would be dependenton acknowledging the importance of achieving positive outcomes with advantage favouring the pub-lic sector and the common good, in recognition of the long-term advantages of this balance. It isessential not to believe that any single health care umbrella can overcome disparities in healththat arise more from lack of access to the SDOH than from inadequate access to care.
It is considered likely that with restructuring how health care is delivered, greater use of commu-nity-based multi-disciplinary teams, explicit priority setting and improved public education, itshould be possible to provide most reasonable health care expectations more equitably within cur-rent budgets (at least in Canada). There are sufficient policy tools (focused on maternal and childhealth, small enterprise development, public health interventions and primary care), but little byway of a well-developed strategic bundle of interventions to simultaneously maximise more equitablepopulation health.
Social determinants of health (SDOH)
The third lesson is that health disparities in Canada, as in South Africa, are significantly related tosocio-economic status, ethnicity, gender, age and geography (Denburg & Daneman, 2010; Younget al., 2016). Yet in both countries, the focus is on improving health through biomedicine, with
16 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

neglect of the SDOH. An assessment of relative contributions to health in Canada is revealing – 50%is accounted for by social and economic determinants, 25% by health care, 15% by biology and gen-etics and 10% by the built and natural environment (The Standing Senate Committee on SocialAffairs, Science & Technology, 2009). Attributable proportions in South Africa would likely showa much larger percentage pertaining to social and economic determinants. The recent UNICEFReport placing the health of Canadian children 26th among 35 of the world’s richest countries (UNI-CEF, 2016) has provoked questions about Canadian values and social policies (Denburg, 2016), and acall for a new Canadian vision for child health (Picard, 2016).
The plight of the First Nations people that has given rise to the Truth and Reconciliation Com-mission in Canada is a welcome acknowledgment of the social impact of colonialism and racialisa-tion on aboriginal health. However, beyond some notable exceptions, there remains little attention toequity, outside of the promise that medically necessary care is free at the point of consumption. Simi-larly, causes of disparities in health and wealth in South Africa go beyond economic differences andinclude ethnic, gender and age discriminatory forces that reflect ongoing long-term effects of apart-heid as well as globally pervasive divisions along all these lines (Alexander, 1996; Van Rensburg &Benatar, 1993).
Both countries also face the prospect of an increasing number of immigrants from war-torn, pooror economically unstable countries. From 2011 to 2015 the number of people displaced globallyincreased from 42.5 million to 65.3 million. It has been estimated that the overall foreign populationin South Africa ranges from 1.6 to 2 million, or 3–4% of the total population, with between 1 and 1.5million legal and illegal Zimbabwean immigrants (Campbell, 2013). Canada admitted over 4 million(mainly legal) immigrants from 2000 to 2016 (Statista, 2017). Providing health care for immigrants,especially those who are illegal, is a major challenge, and one which will only increase with time if con-ditions of life remain grossly inadequate for somany in their own countries. Funding of health care formigrants has very different implications for South Africa and Canada that cannot be pursued here.
Yet these SDOH are largely ignored and access to biomedical care through NHI is seen rathernaively by some as the single most important thrust towards reducing inequities in health. This ismore politically convenient than focusing on improving the efficiency and effectiveness of existinghealth care services in the public sector and addressing the social and societal determinants of health(Birn, 2011). A price is now being paid (Johnson, 2017) for ignoring insights from 20 years agoregarding the requirements to narrow disparities in South Africa and to promote social justiceand better living conditions as a means of avoiding the anger and civil unrest that would only bedisplaced into the future if progress was limited to the transfer of political power (Benatar, 1990,1997b, 1997c; Lalonde, 1981).
For South Africa, we should agree that NHI is a necessary contributor to reducing inequities inhealth in South Africa, but that it is also a form of social compromise, incomplete egalitarianism(even more incomplete than in Canada) and a useful political approach to promoting a measureof social harmony, but that only in part addresses the problem of inequity. The main challengesregarding health equity in South Africa will clearly not be met simply by introducing some formof universal health insurance coverage, as this cannot alone significantly narrow the enormous healthand health service gradient effects of widely disparate material living conditions.
Canada, that was an early beacon of light in supporting attention to the SDOH with theLalonde report of 1981 (Evans, Barer, & Marmor, 1994) and fairly advanced analysis of factorsdriving the health of populations, (Young et al., 2016) also needs to reexamine its health servicesystem with a view to both rebuilding and focusing on setting priorities for health expendituregenerally as well as specifically on marginalised populations. For example, per capita expenditureon health in the North West Territories is double the average for all Canadians with a muchpoorer outcome (Young et al., 2016). How such priorities could be set remains controversial,but Canada has pioneered transparent and accountable processes. More attention should alsobe directed at the SDOH.
GLOBAL PUBLIC HEALTH 17
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Global interdependence
The final long-term problem facing both countries is that the state of local and global populationhealth is only one of many signs of an unstable world in a state of entropy (Benatar, 2015a;McMichael, 2014) in what is now called the Anthropocene era. The idea of global health nowgoes beyond anthropocentric conceptions of health to include the notion of healthy people ona healthy planet on which the health of all life is interdependent. The health and lives of billionsof people are being, and will continue to be affected by environmental degradation and climatechange – through direct long-term effects on water security, food chain integrity, populationmigration and displacement, redistribution and recrudescence of vector-borne diseases, increas-ing anti-microbial resistance and significant short-term health impacts from catastrophicextreme climatic events (Hotez & Murray, 2017). There are also significant environmental healthconcerns globally that are not directly associated with climate change. These include the crueltyof ‘farming’ of animals in mass production facilities and the impact of this on food safety, anti-biotic resistance, the contamination of food and water supplies with cumulative amounts of toxicindustrial agents and climate change (Benatar, 2011; Friel, Butler, & McMichael, 2011).
It is increasingly understood that ‘progress’ along a linear trajectory extending twentieth-centuryadvances and ongoing economic growth is unlikely under conditions of limited renewable naturalresources and other constraints on continued economic growth, wasteful consumption patterns,environmental degradation, extinction of species and the effects of climate change on disease vectorsand patterns of morbidity and mortality in all countries consequent on these processes. The currentglobal political economy deliberately imposes structural forces that widen rather than narrow localand global disparities at enormous opportunity costs, and prevents meaningful reform beyond theexisting paradigm (Benatar 2015b). This may not be widely appreciated by those who enjoy thebest that the modern world has to offer, and who have become complacent about their entitlements.Excess mortality from climate change will predictably be much greater in the global south than in theglobal north, as exemplified by the conservative estimate of 50,000 additional deaths attributable toclimate change in the year 2000 in the world’s poorer and vulnerable populations. These lessons arerelevant for all countries including the wealthy (Friel et al., 2011).
The fact that disparities in wealth and health and the challenges to narrow these in South Africa,exemplify the situation in low- and middle-income countries where the majority of the world’speople live, adds to the relevance of the issues raised here to public health issues globally. Wealthycountries like Canada also need a wake-up call as they cannot ignore such issues because of linkedrisks and interdependencies in a globalised world where the emergence and spread of new infectiousdiseases and many adverse socio-economic and political trends pose major potential threats to globalpublic health (Boushey, Delong, & Steinbaum, 2017). It is notable that there has been a markedincrease in the all-cause mortality of middle-aged white non-Hispanic men and women in theU.S.A. between 1999 and 2013, and that this reversal of decades of progress in mortality, uniqueto the U.S.A., has been attributed in part to adverse social and economic trends. Had mortalityrates in this group continued to decline at the same rate between 1979 and 1998, 500,000 deathswould have been avoided in the period 1999‒2013. This is similar to the number of lives lost inthe U.S. AIDS epidemic through mid-2015 (Case & Deaton, 2015).
Conclusions
We contend that both South Africa and Canada (and indeed many other countries) should be able tolearn from the considerations we have raised here, despite one (Canada) that is much betterresourced offering incomplete universal coverage, and one (South Africa) that is still building uni-versal coverage. Both countries have widely dispersed populations and struggle to maintain theirdesired economic growth, both achieve less equity in health and health care than they are capableof doing, and both could achieve more through commitments to explicit resource allocation and
18 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

priority setting to reduce waste and unnecessary procedures resulting in the over-payment in somesectors at the risk of others. A lesson from Canada is that a presumed equitable NHI can have a dis-torted emphasis on physician and hospital payments at the cost of uneven home/community careand pharmaceutical coverage. While it is clear that material and demographic challenges are hugein many rural and remote parts, there may be solutions at hand in both countries to extend nationalcoverage through increased taxation and spread of delivery system and technology innovationswhich seek to foster human resource solutions, like the nurse practitioner and community clinicsin South Africa (Gumede, 2017). For both countries, the expansion of equity and full coverage ofhealth services remain matters begging for better health policy and stronger local implementationof policy and service execution tied to local solutions.
We have outlined elsewhere how health care reform debates over the past 40 years have beenshaped by a dialectic between the opposing ideas of: (a) health care services as a social good governedby a concept of social-efficiency; and (b) the notion of a ‘market civilization’ governed by neoliberalpolitical and pro-market forces (Benatar, Sanders, & Gill, in press). Sadly, as is becoming increasinglyapparent, the latter route dominates as an unsustainable global model of ‘development’ focused onthe flawed economic theory being widely pursued to the detriment of the poorest in our societies andglobally (Stiglitz, 2002).
The challenges for South Africa are more daunting in the context of recent upheavals (LatestAfrica News, 2017; Powell, 2017). The work noted above on the epidemiological context and tran-sitions is key to focusing on what needs to be introduced and where: Canada needs better home andcommunity services for an ageing population and South Africa needs a stronger material base for thepoorest populations, supported by a broader blanket of primary care and continued work on infec-tious disease reductions alongside the expansion of health care coverage.
Canadians, like so many other privileged people globally, have extraordinarily high expectationsfor health care. The intractable problem of excessively long waiting periods for available effectivetreatment of remediable conditions while expenditure seems almost unrestricted for some ineffec-tive, even futile, treatments is in part due to: (i) unrealistic expectations of entitlements, (ii) an uncri-tical, distorted understanding of what medicine can offer, (iii) expenditure of a large portion of thehealth budget on attempts to extend biological life when cognitive life has ended, or if there is little, ifany, possibility of this being achieved at the beginning of life, (iv) psychological reassurance that ‘allwill be done’ in desperate situations and (v) the ‘hope for miracles’.
Even in the wealthiest societies, resources for health care are not limitless (Reuben, 2010). Provid-ing expensive care with minimal benefits to some either diminishes equitable access to effective treat-ments for others or increases the costs of health care. The result is that most health care ‘systems’ arenot designed to deliver what most thoughtful citizens, cognisant of resource limitations, would likelychoose to ensure the best quality of life and care for themselves over their life spans. Such opportu-nity costs need to be examined and addressed. Throughout the world, including Canada, health sta-tus is worst among those who are most deprived and whose living conditions are less than adequate(WHO, 2008, 2014, 2015a, 2015b, 2016a, 2016b; Cameron et al., 2014).
Against this background and in the face of a still evolving global economic crisis with limited pro-spects for endless economic growth, an important question for Canadians is not whether moremoney is needed to improve their health but rather whether available money could be spent morewisely to provide optimal, balanced, easily accessible and effective care services throughout life(Deber, 2009), and whether political logics would permit such a deliberate redistribution. In theabsence of specific health goals at either the provincial or federal levels, priorities in Canadian healthcare are currently set implicitly and covertly and Canadians do not have the opportunity to choosewhat the shape and spectrum of their health services should be. Yet research in Canada and else-where shows that in democratic societies, explicit, accountable, publicly transparent and negotiablepriority setting is possible (Ham & Coulter, 2001).
Although equity is important everywhere, potential responses to the challenges of achievinggreater equity in access to sustainable, high-quality health care vary greatly from country to country.
GLOBAL PUBLIC HEALTH 19
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

In Canada, where considerable resources are spent on health care, the potential lies predominantly infacilitating choices by Canadians for innovative, integrated and coordinated hospital and home ser-vices desired across their life span, within the limits of what they are willing to pay for these throughtaxation and supplementary insurance or out of pocket payments. In South Africa, the persistence ofwidespread absolute and relative poverty perpetuates a large deficit in access to the SDOH that arethe major causes of health inequities. Here the quest for narrowing very wide inequities across social,economic, ethnic and geographic groups is more complex, given the vast differences in availableresources, much wider disparities in wealth, the country’s long history of lack of commitment totreating all its citizens as equals, and very marked differences between the publicly funded healthcare facilities using moneys accrued through Beveridge style tax financing, and privately providedhealth care services using payroll or entirely private models of funding.
Perhaps a new understanding is needed of what could be considered to be reasonable and sustain-able health care entitlements for all (Benatar, 2009; Bensimon & Benatar, 2006). From the South Afri-can perspective, the current economic wealth of Canadians should enable both better health outcomesand reduced inequity. From the Canadian perspective, South Africans have much to learn about ega-litarian health care. Based on all the many considerations outlined above and limitations on endlesseconomic growth, achieving equity in health or even in access to health care will remain elusive,and the challenge should include efforts to do better with less. Both societies may have to acceptthat perfect equity is not achievable and that the goal of equitable use of resources, minimal wastageand optimal individual and community health benefits to develop sustainability remains a long-termsocial project that should be facedwith humility, courage, wisdom and solidarity in the knowledge thatthe forces influencing health and health care will change significantly over the coming decades.
Notes
1. Richard Horton, Editor of the Lancet has criticized the SDGs as being ‘fairy tales, dressed in bureaucratese ofintergovernmental narcissism, adorned with the robes of multilateral paralysis. The goal “attain healthy lives forall at all ages” is a mixture of business-as-usual (the MDGs rebooted), non-communicable diseases and univer-sal health coverage… and a strange assortment of promises… ’ (The Lancet, 2014, Vol. 383, Issue 2074).
2. The exchange rate of the SAR and for the Canadian and U.S. dollars has fluctuated considerably over severalyears. For the purposes of this article, an exchange rate of SAR 10 = CDN $1 is used. It should be noted that thissimple conversion does not reflect purchasing power values.
3. The number of people with access to medical aid (insurance) increased from about 7 million in 1993 to about 8million in 2008 while the number of those without such access increased from about 31 million in 1993 to justover 40 million in 2008.
4. Leadership, governance and accountability; health workforce information and health workforce planning; re-engineering of the workforce to meet service needs; scaling up and revitalising education, training and research,creating the infrastructure for workforce and service development – academic health complexes and nursingcolleges; strengthening and professionalising the management of HR and prioritise health workforce needs;ensuring professional quality care through oversight, regulation and continuing professional development;and improving access to health professionals and health care in rural and remote areas.
Acknowledgements
Thanks are due to C. David Naylor for a critical reading of an earlier draft of this paper and to anonymous reviewersfor their constructive comments.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
Abdool Karim, S. S., Churchyard, G. J., Abdool Karim, Q., & Lawn, S. D. (2009). HIV infection and tuberculosis inSouth Africa: An urgent need to escalate the public health response. The Lancet, 374(9693), 921–933.
20 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Alexander, T. (1996). Unravelling global apartheid. Cambridge: Polity Press.allAfrica. (2014). South Africa: Tuberculosis leading cause of death in 2015. Retrieved from http://allafrica.com/stories/
201703240667.htmlAnswers Africa. (n.d.). South Africa seeks to regulate traditional healers. Retrieved from https://answersafrica.com/
south-africa-seeks-to-regulate-traditional-healers.htmlBenatar, D. (2011). Animals, the environment and global health. In S. Benatar, & G. Brock (Eds.), Global health &
global health ethics (pp. 210–220). Cambridge: CUP.Benatar, S. R. (1986). Medicine and health care in South Africa. New England Journal of Medicine, 315, 527–532.Benatar, S. R. (1990). A unitary health service for South Africa. South African Medical Journal, 77, 441–447.Benatar, S. R. (1991). Medicine and health care in South Africa: 5 years later. New England Journal of Medicine., 325,
30–36.Benatar, S. R. (1997a). Health care reform in the new South Africa. New England Journal of Medicine, 336, 891–895.Benatar, S. R. (1997b). Towards social justice in the new South Africa.Medicine Conflict and Survival, 13(3), 229–239.Benatar, S. R. (1997c). War, or peace & development: S. Africa’s message for global peace & security.Medicine, Conflict
and Survival, 13(2), 125–134.Benatar, S. R. (1998). Global disparities in health and human rights. A critical commentary. American Journal of Public
Health, 88, 295–300.Benatar, S. R. (2001). The coming catastrophe in international health: An analogy with lung cancer. International
Journal, LV1(4), 611–631.Benatar, S. R. (2004). Health care reform and the crisis of HIV and AIDS in South Africa. New England Journal of
Medicine, 351, 81–92.Benatar, S. R. (2007). An examination of ethical aspects of migration and recruitment of health care professionals.
Clinical Ethics, 2(1), 2–7.Benatar, S. R. (2009). Global health: Where to now? Global Governance, 11(2). Retrieved from http://www.ghgj.org/
benatar2.2wherenow.htmBenatar, S. R. (2013). The challenge of health disparities in South Africa. South African Medical Journal, 103(3), 154–
155.Benatar, S. R. (2015a). Explaining and responding to the Ebola epidemic. Philosophy, Ethics, and Humanities in
Medicine, 10(5). doi:10.1186/s13010-015-0027-8Benatar, S. R. (2015b). Health in low-income countries. In J. D. Wright (Ed.), International encyclopedia of the social &
behavioral sciences (2nd ed., Vol. 10, pp. 633–639). Oxford: Elsevier.Benatar, S. R., & Ashcroft, R. (2017). International perspectives on resource allocation. In S. R. Quah & W. C.
Cockerham (Eds.), The international encyclopedia of public health (2nd ed., Vol. 4, pp. 316–321). Oxford:Academic Press.
Benatar, S. R., Gill, S., & Bakker, I. (2009). Making progress in global health: The need for a new paradigm.International Affairs, 85(2), 347–371.
Benatar, S. R., Gill, S., & Bakker, I. C. (2011). Global health and the global economic crisis. American Journal of PublicHealth, 101, 646–653.
Benatar, S. R., Sanders, D., & Gill, S. (in press). The global politics of health care reform. In The Oxford handbook ofglobal health politics (Chapter 26).
Bensimon, C. A., & Benatar, S. R. (2006). Developing sustainability: A new metaphor for progress. TheoreticalMedicine and Bioethics, 27(1), 59–79.
Birn, A.-E. (2011). Addressing the societal determinants of health: The key global health ethics imperative of our times.In S. Benatar & G. Brock (Eds.), Global health and global health ethics (pp. 37–52). Cambridge: CambridgeUniversity Press.
Boushey, H., Delong, B., & Steinbaum, M. (Eds.). (2017). After Piketty: The agenda for economics and inequality.Cambridge, MA: Harvard University Press.
Brill, S. (2013, April 4). Bitter Pill: Why medical bills are killing us. Time Magazine.Brock, G., & Blake, M. (2015). Debating brain drain: May governments restrict emigration? New York: Oxford
University Press.Cameron, B. L., del Pilar Carmargo Plazas, B., Santos Salas, A., Bourque Bearskin, L., & Hungler, K. (2014).
Understanding inequalities in access to health care services for aboriginal people. A call for nursing action.Advances in Nursing Science, 37(3), E1–E16.
Campbell, J. (2013). How many immigrants does South Africa have? That depends on who you ask. ChristianScience Monitor. Retrieved from http://www.csmonitor.com/World/Africa/Africa-Monitor/2013/0221/How-many-immigrants-does-South-Africa-have-That-depends-who-you-askhttps://www.statista.com/statistics/443063/number-of-immigrants-in-canada/
Campbell, D., Morris, S., & Marsh, S. (2017, January). NHS faces ‘humanitarian crisis’ as demand rises, British RedCross warns. The Guardian. Retrieved from https://www.theguardian.com/society/2017/jan/06/nhs-faces-humanitarian-crisis-rising-demand-british-redcross?utm_source=esp&utm_medium=Email&utm_campaign=GU+Today+main+NEW+H+categories&utm_term=207338&subid=20419384&CMP=EMCNEWEML6619I2
GLOBAL PUBLIC HEALTH 21
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Canadian Institute of Health Information. (2015). National health expenditure trends 1975–2015. Retrieved fromhttps://www.cihi.ca/sites/default/files/document/nhex_trends_narrative_report_2015_en.pdf
Case, A., & Deaton, A. (2015). Rising morbidity and mortality in midlife among white non-hispanic Americans in the21st century. Proceedings of the National Academy of Sciences, 112(49), 15078–15083.
CBC News. (2013, October 18). Hassan Rasouli case: Top court upholds life-support right. The Canadian Press.Retrieved from http://www.cbc.ca/news/canada/toronto/hassan-rasouli-case-top-court-upholds-life-support-right-1.2125140
Child and Maternal Health UNICEF. (2012). Retrieved from https://www.unicef.org/somalia/health.htmlChoosing Wisely Canada. (2017). Retrieved from http://www.choosingwiselycanada.org/CIAWorld Factbook. (2014). Population pyramid Canada 2014. Retrieved from http://www.indexmundi.com/canada/
age_structure.htmlCIA World Factbook. (2016). Population pyramid S Africa 2016. Retrieved from http://www.indexmundi.com/south_
africa/age_structure.htmlCommonwealth Fund. (2014).US health system ranks last among eleven countries on measures of access, equity, quality,
efficiency, and healthy lives. Retrieved from http://www.commonwealthfund.org/publications/press-releases/2014/jun/us-health-system-ranks-last
Cotlear, D., Nagpal, S., Smith, O., Tandon, A., & Cortez, R. (2015). Going universal: How 24 developing countries areimplementing universal health coverage reforms from the bottom up . World Bank group.Washington, DC: WorldBank.
Council for Medical Schemes. (2014–2015). Annual report. Retrieved from https://www.medicalschemes.com/ReadNews.aspx?110
Daviaud, E., & Chopra, M. (2008). Howmuch is not enough? Human resource requirements for primary health care: Acase study from S Africa. Bulletin of the World Health Organization, 86(1), 46–51.
Deber, R. B. (2009, September 3). Handling the high spenders: Implications of the distribution of health expenditures forfinancing health care. Paper presented at the 2009 American Political Science Association Annual Meeting.
Deloitte. (2015). Health care outlook. South Africa. Retrieved from https://www2.deloitte.com/content/dam/Deloitte/global/Documents/Life-Sciences-Health-Care/gx-lshc-2015-health-care-outlook-south-africa.pdf
Denburg, A. (2016). Canadian values, social policy and the health of our kids. Paediatrics and Child Health, 21(5), 242–244.
Denburg, A., & Daneman, D. (2010). The link between social inequality and child health outcomes. HealthcareQuarterly, 14, 21–31.
Evans, R., Barer, M., & Marmor, T. (1994). Why are some people healthy and others not: The determinants of health ofpopulations. New York: Aldine de Gruyter.
Fairall, L. R., Bateman, E., Cornick, R., Faris, G., Timmerman, V., Folb, N.… Smith, R. (2015). Innovating to improveprimary care in less developed countries: Towards a global model. BMJ Innovation, 1, 196–203.
Fairall, L. R., Zwarenstein, M., Bateman, E. D., Bachmann, M., Lombard, C., Majara, B. P. … Chapman, R. D. (2005).Effect of educational outreach to nurses on tuberculosis case detection and primary care of respiratory illness:Pragmatic cluster randomized controlled trial. British Medical Journal, 331, 750–754.
Fleischer, T., Kevaney, S., & Benatar, S. R. (2005). Will escalating spending on HIV treatment displace funding fortreatment of other diseases? South African Medical Journal, March 100(1), 32–34.
Flood, C., & Archibald, T. (2001). The illegality of private health care in Canada. Canadian Medical AsoosciationJournal, 164, 825–830.
Flood, C. M., & Sullivan, T. (2005). Supreme disagreement: The highest court affirms an empty right. CanadianMedical Association Journal, 173(2), 142–143. doi:10.1503/cmaj.050759
Friel, S., Butler, D., & McMichael, A. (2011). Climate change and health: Risks and inequities. In S. Benatar & G. Brock(Eds.), Global health and global health ethics (pp. 198–209). Cambridge: CUP.
Garrett, L. (1994). The coming plague. New York: Farrar Strauss and Giroux.Gawande, A. (2010, August 2). Letting go: What should medicine do when it can’t save your life? The New Yorker.Gibson, J. L., Martin, D. K., & Singer, P. A. (2004). Setting priorities in health care organizations: Criteria, processes,
and parameters of success. BioMed Central Health Services Research, 4, 335.Gibson, J. L., Martin, D. K., & Singer, P. A. (2005). Evidence, economics and ethics: Resource allocation in health ser-
vices organizations. Health Care Quarterly, 8, 50–59.Gill, S., & Bakker, I. C. (2011). The global crisis and global health. In S. Benatar & G. Brock (Eds.), Global health and
global health ethics (pp. 221–238). Cambridge: CUP.Gill, S., & Benatar, S. R. (2016). Global health governance and global power: A critical commentary on the Lancet uni-
versity of Oslo commission report. International Journal of Health Services. doi:10.1177/002073141663173Gilson, L., & McIntyre, D. (2008). The interface between research and policy: Experience from South Africa. Social
Science and Medicine, 67, 748–759.Gilson, L., & Raphaely, N. (2008). The terrain of health policy analysis in low and middle-income countries: A review
of published literature 1994–2007. Health Policy and Planning, 23, 294–307.
22 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Gon, S. (2013). The myth of white privilege. SA Institute of Race Relations. Retrieved from http://irr.org.za/reports-and-publications/articles-authored-by-the-institute/the-myth-of-white-privilege-2013-politicsweb-7-december-2015.
Government of Canada. (2017a). Protecting Canadians from excessive drug prices: Consulting on proposed amendmentsto the patented medicines regulations. Ottawa. Retrieved from https://www.canada.ca/en/health-canada/programs/consultation-regulations-patented-medicine/document.html?=undefined&wbdisable=true
Government of Canada. (2017b). Review of pan-Canadian health organizations. Retrieved from https://www.canada.ca/en/health-canada/programs/external-advisory-body-pan-canadian-health-organizations/terms-of-reference.html
Gumede, M. (2017, May 31). Ailing KwaZulu-Natal health system faces crippling claims: Several departments couldlose accreditation to train specialists. Business Day. Retrieved from http://www.medicalbrief.co.za/archives/collapsing-kzn-health-may-lose-specialisttraining-accreditation-hpcsa
Guyatt, G., Devereaux, P. J., Lexchin, J., Stone, S., Yalnizyan, A., Himmelstein, D.,… Bhatnagar, N. (2007). A systema-tic review of studies comparing health outcomes in Canada & the United States. Open Medicine, 1(1), 27–30.
Habib, A. (2013). South Africa’s suspended revolution: Hopes and prospects. Johannesburg: Wits University Press.Ham, C., & Coulter, A. (2001). Explicit and implicit rationing: Taking responsibility and avoiding blame for health care
choices. Journal of Health Services Research and Policy, 6, 163–169.Health Council of Canada. (2014). Progress timeline 2003–2014: Highlights of health care reform. Retrieved from http://
www.longwoods.com/articles/images/HCC_Progress_Report_Eng.pdfHealth financing and the National Health Insurance in South Africa: An overview. (2012). Retrieved from http://polity.
org.za/article/health-financing-and-the-national-health-insurance-in-south-africa-an-overview-2012-03-27Hotez, P. J., & Murray, K. O. (2017). Dengue, West Nile virus, Chikungunya, Zika and now Mayaro? PLoS Neglected
Tropical Diseases, 11(8), e0005462. doi:10.1371/journal.pntd.0005462James, W. (2016a). Our health plan: The DA’s health plan is the best route to a healthy and fair SA. Retrieved from
https://www.da.org.za/2016/11/health-plan-das-health-plan-best-route-healthy-fair-sa/James, W. (2016b). Shortage of 80,000 professional nurses in South Africa. Retrieved from http://allafrica.com/stories/
201612070909.htmlJohnson, R. W. (2017, May 9). South Africa contemplates the abyss. Thinking the unthinkable. Politicsweb. Retrieved
from http://www.politicsweb.co.za/opinion/south-africa-contemplates-the-abyssKahn, T. (2016, November 24). The public health system is in crisis, and its flagship programme does not offer a better
deal for patients. Business Day. Retrieved from http://www.businesslive.co.za/bd/national/health/2016-11-24-nhi-pilot-projects-fail-to-reach-targets/
Kahn, T. (2017, August 29). Private health care industry to play a greater role in NHI. Business Day. Retrieved fromhttps://www.businesslive.co.za/bd/national/health/2017-08-29-private-healthcare-industry-set-to-play-larger-role-in-nhi
Kaiser Family Foundation. (2007, January). Health care spending in the United States and OECD countries. Retrievedfrom http://www.kff.org/insurance/snapshot/chcm010307oth.cfm
Kevany, S., Benatar, S. R., & Fleischer, T. (2013). Improving resource allocation decisions for health and HIV programsin South Africa: Bioethical, cost-effectiveness and health diplomacy considerations. Global Public Health: AnInternational Journal for Research, Policy and Practice. doi:10.1080/17441692.2013.790461
Klitzman, R. (2017). What Charlie Gard case teaches us about life and death. CNN. Retrieved from http://www.cnn.com/2017/07/05/opinions/gard-bioethical-questions-opinion-klitzman/index.html
Kochhar, R. (2015). A global middle class is more promise than reality: From 2001 to 2011, nearly 700 million step out ofpoverty, but most only barely. Washington, DC: Pew Research Center. Retrieved from http://www.pewglobal.org/2015/07/08/a-global-middle-class-is-more-promise-than-reality
Kon, Z. R., & Lackan, N. (2008). Ethnic disparities in access to care in post-apartheid South Africa. American Journal ofPublic Health, 98(12), 2272–2277. doi:10.2105/AJPH.2007.127829
KPMG. (2017). Funding NHI: A spoonful of sugar? An economic analysis of NHI. Retrieved from https://www.kpmg.com/ZA/en/IssuesAndInsights/ArticlesPublications/General-Industries-Publications/Documents/KPMG%20NHI%20Economic%20Impact%20Research%20brochure.pdf
Labonté, R., Packer, C., & Klassen, N. (2006). Managing health professional migration from sub-Saharan Africa toCanada: A stakeholder inquiry into policy options. Human Resources for Health, 4, 12. doi:10.1186/1478-4491-4-22
Lalonde, M. (1981). A new perspective on the health of Canadians. Retrieved from http://www.phac-aspc.gc.ca/ph-sp/pdf/perspect-eng.pdf
Lam, V. (2011). Tommy Douglas. Toronto: Penguin.Latest Africa News. (2017, January 2). Political turmoil in 2016 can be traced back to the 2008 financial crisis. Retrieved
from https://www.latestafricanews.com/latest-update/2017/01/political-turmoil-in-2016-can-be-traced-back-to-the-2008-financial-crisis
Levin, L., Goeree, R., Levine, M., Krahn Easty, T., Brown, A., & Henry, D. (2011). Coverage with evidence development.The Ontario experience. International Journal of Technology Assessment in Health Care, 27, 159–168. doi:10.1017/S0266462311000018
GLOBAL PUBLIC HEALTH 23
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Lewis, S., & Sullivan, T. (2013, June 3). Deal with doctors. Policy Options. Retrieved from http://policyoptions.irpp.org/magazines/nudge/lewis-sullivan/
Lings, K. (2014). South Africa: National budget. 2013/2014. Retrieved from http://www.stanlib.com/newsatstanlib/Documents/SANationalBudget2013-2014.pdf
Marchildon, G. P. (2013). Canada: Health system review. Health Systems in Transition, 15(1), 1–179.Marmot, M., Bloomer, E., & Goldblatt, P. (2013). The role of the social determinants of health in a context of economic
crisis. Public Health Reviews, 35(1), 213–224.Massyn, N., Pee, N., English, R., Padarath, A., Barron, P., & Day, C. (Eds.). (2016). District health barometer 2015/16.
Durban: Health Systems Trust.Mayosi, B., & Benatar, S. R. (2014). Health and health care in South Africa. New England Journal Medicine, 371, 1344–
1352.Mayosi, B. M., Lawn, S., van Niekerk, J. E., Bradshaw, D., Abdool Karim, S. S., & Coovadia, H. M., for the Lancet South
Africa Team (2009). Health in South Africa: Changes and challenges since. The Lancet, 380, 2029–2043.McGillis Hall, L., Pink, G. H., Jones, C., Leatt, P., Gates, M., Pink, L.,… Seto, L. (2009). Gone south: Why Canadian
nurses migrate to the United States. Healthcare Policy, 4(4), 91–106. doi:10.12927/hcpol.2009.20821McMichael, A. J. (2014). Population health in the anthropocene: Gains, losses and emerging trends. The Anthropocene
Review. doi:10.1177/2053019613514035Merti, S. (2016). Public health care challenged in BC court. Canadian Medical Association Journal, 188(14), E333–
E334.Moosa, M. R., Maree, J. D., Chirehwa, M. T., & Benatar, S. R. (2016). Use of the accountability for reasonableness’
approach to improve fairness in accessing dialysis in a middle-income country. PLoS One, 11(10), e0164201.doi:10.1371/journal.pone.0164201
Mullan, F. (2005). The metrics of the physician brain drain. New England Journal of Medicine, 353, 1810–1818.National Health Expenditure Trends Canada. (2014). Retrieved from https://www.cihi.ca/en/nhex_2014_report_en.
pdfNational Institute for Health and Care Excellence (NICE). (2017). Retrieved from https://www.nice.org.uk/Naylor, C. D. (1986). Private practice, public payment. Canadian medicine and the politics of health insurance.
Montreal: McGill-Queen’s University Press.Naylor, D., Girard, F., Mintz, J., Fraser Jenkins, T., & Power, C. (2015). Report of the advisory panel on healthcare inno-
vation. Retrieved from http://www.healthycanadians.gc.ca/publications/health-system-systeme-sante/report-healthcare-innovation-rapport-soins/index-eng.php
Odhiambo, A. (2010, December). Healthcare is failing women. Mail and Guardian. Retrieved from https://www.hrw.org/news/2011/12/20/healthcare-failing-women
Physicians per 100,000 People, by Country.. (2017). Infoplease. Sandbox Networks, Inc., publishing as Infoplease.Retrieved from https://www.infoplease.com/world/health-and-social-statistics/physicians-100000-people-country/
Picard, A. (2016). Canada needs a vision for child health. Paediatrics and Child Health, 21(5), 237–238.Powell, A. (2017, April 4). South Africa credit downgrade deepens political turmoil. Vox. Retrieved from http://www.
voanews.com/a/south-africa-credit-downgrade-deepens-political-turmoil/3795638.htmlReis, A. A. (2016). Universal health coverage – the critical importance of global solidarity and good governance:
Comment on “ethical perspective: five unacceptable trade-offs on the path to universal health coverage.International Journal of Health Policy and Management, 5. doi:10.15171/ijhpm.2016.61
Reuben, D. B. (2010). Miracles, choices, and justice. JAMA, 304(4), 467–468.Reynolds, L., London, L., & Sanders, D. (2005). The draft charter of the private and public health sectors of the republic
of S Africa: Health for all or profits for few? South African Medical Journal, 85(10), 742–743.Rolling Alpha. (2017). Who pays South Africa’s tax? The 2017 edition. Retrieved from http://www.rollingalpha.com/
2017/10/26/who-pays-south-africas-tax-the-2017-edition/Romanow Report. (2002). Building on values: the future of health care in Canada: Retrieved from http://publications.
gc.ca/site/eng/237274/publication.htmlRosenthal, E. (2017). An American sickness. How medicine became big business and how you can take it back.
New York: Penguin Press.Rowden, R. (2009). The deadly ideas of neoliberalism: How the IMF undermined public health and the fight against
AIDS. London: Zed Books.Schwab, P. (2001). Africa: A continent self-destructs. New York: Macmillan.South African Government. (2011). Human resources for health South Africa: HRH strategy for the health sector: 2012/
13–2016/17. Retrieved from http://www.gov.za/sites/www.gov.za/files/hrh_strategy_0.pdfStanding, G. (2014). A precariat charter. London: Bloomsbury Academic.The Standing Senate Committee on Social Affairs, Science & Technology. (2009). A healthy, productive Canada: A
determinant of health approach (Final report of senate subcommittee on population health). Retrieved fromhttps://sencanada.ca/content/sen/Committee/402/popu/rep/rephealthjun09-e.pdf
Statista: The Stastics Portal. (2017). The number of immigrants to Canada from 2000–2017. Retrieved from https://www.statista.com/statistics/443063/number-of-immigrants-in-canada/
24 S. BENATAR ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18

Stiglitz, J. (2002). Globalization and its discontents. London: Penguin Books.Street, R. A. (2016). Unpacking the new proposed regulations for South African traditional health practitioners. South
African Medical Journal, 106(4), 325–326.Tepperman, J. (2016). Brazil’s antipoverty breakthrough: The surprising success of Bolsa Família. Foreign Affairs, 95,
34–44.Terreblanche, S. (2002). A history of inequality in South Africa 1652_2002. Pietermaritzburg: University of Natal Press.UNICEF. (2016). The state of the world’s chidren reports. Retrieved from https://www.unicef.org/sowc/Van Rensburg, H. (Ed.). (2012). Health care in South Africa (2nd ed.). Pretoria: Van Schaik.Van Rensburg, H. C. J., & Benatar, S. R. (1993). The legacy of apartheid in health and health care. South African Journal
of Sociology, 24, 99–111.Visser, A. (2016, July 1). NHI costs to skyrocket. Business News. Retrieved from http://www.iol.co.za/business/news/
nhi-costs-to-skyrocket-2040660Whelan, A. M., Arkles, R. S., Dewdney, J., & Zwi, A. B. (2004). International movement of health professionals: Ethical
policy challenges for developed nations. Harvard Health Policy Review, 5, 97–111.Whitehead, M. (1992). The concepts and principles of equity in health. International Journal of Health Services, 22,
429–445.White Paper on National Health Insurance (NHI). (2015). Retrieved from http://www.gov.za/documents/national-
health-insurance-10-Idec-2015-0000World Bank. (1993). World development report 1993: Investing in health. New York: Oxford University Press.
Retrieved from https://www.nap.edu/read/5513/chapter/4World Bank. (2003). World development report 2003: Sustainable development in a dynamic world – transforming
institutions, growth, and quality of life. World Bank. Retrieved from https://openknowledge.worldbank.org/handle/10986/5985 License: CC BY 3.0 IGO
World Bank. (2012). Retrieved from http://data.worldbank.org/indicator/SH.DYN.MORTWorld Bank. (2015). Retrieved from http://data.worldbank.org/indicator/NY.GDP.PCAP.CDWorld Bank. SA Data Portal. (2015). Retrieved from http://southafrica.opendataforafrica.org/mhrzolg/gdp-by-
country-statistics-from-the-world-bank-1960-2015?country=WorldWorld Health Organization (WHO). (2008). Commission on the social determinants of health – Final report. Retrieved
from http://www.who.int/social_determinants/thecommission/finalreport/en/World Health Organization (WHO). (2014). Retrieved from http://data.worldbank.org/indicator/SH.XPD.PCAPWorld Health Organization (WHO). (2015a). Retrieved from http://gamapserver.who.int/gho/interactive_charts/
mdg5_mm/atlas.htmlWorld Health Organization (WHO). (2015b). Retrieved from https://en.wikipedia.org/wiki/List_of_countries_by_
life_expectancyWorld Health Organization (WHO). (2016a). Global burden of diseases. Geneva. Retrieved from https://vizhub.
healthdata.org/gbd-compare/World Health Organization (WHO). (2016b). Evidence on social determinants of health. Geneva. Retrieved from
http://www.who.int/social_determinants/themes/en/Young, T. K., Chatwood, S., & Marchildon, G. P. (2016). Health care in Canada’s north: Are we getting value for
money? Healthcare Policy, 12(1), 59–70.
GLOBAL PUBLIC HEALTH 25
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ape
Tow
n L
ibra
ries
] at
23:
42 0
2 Ja
nuar
y 20
18