Why Do We Do the Things We Do

of 20
Transcript of Why Do We Do the Things We Do
-
7/29/2019 Why Do We Do the Things We Do
1/20
-
7/29/2019 Why Do We Do the Things We Do
2/20
-
7/29/2019 Why Do We Do the Things We Do
3/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 19
we hear every day reacts to certain laws, ultra-sound is held to similar laws and constraints.
In audible sound (20-20,000 hertz), we can hear
thesound from voicesor noises reflecting from dis-tant objects. We also know that audible sound hasdifficulty passing or traveling through certain sub-stances and will be attenuated or not heard at all.We know that different ranges or frequencies ofsound affect us differently. The booming bass gen-erated by a neighbors stereo seems to penetrate allthe walls in your house. The high frequencies of thelead sopranos voice is piercing to the front-rowlistener but hardly audible to the rear of the perfor-mance hall. We live every day with sound andaccept what we hear.
In ultrasound, our sound cannot travel throughair; it can only exist and travel in a media, which, inour case, is the tissues and blood of our bodies.
How Do We Produce Ultrasound?
Transducers or crystals produce ultrasound.Electronic stimulation of these crystals causes anexpansion and contraction (Piezoelectric effect) ofthe crystal material, which subsequently producesa mechanical wave of energy we call ultrasound.From this point on, everything you do in your
sonogram relates to controlling how much soundgoes into the body and how we shape, focus, andconfigure the sound that is transmitted and re-ceived. All of this is accomplished through propertransducer selection (type and frequency) and thecorrect utilization of your system controls. Re-member that manufacturers do not put lots ofknobs, buttons, and dials on a system to improve itslooks. They are there for you to control andimprove the acoustic data you are transmitting andreceiving.
This Thing Will Not Explode?
Many, many times over my career as an instruc-tor, I have heard the comments, We never touchthat control, or My boss told me to never flip thatswitch, or, my favorite, We taped that one downso we could not adjust it. You simply cannot hurtan ultrasound system by manipulating its controls;you only improve or worsen the transmitted and re-ceived data. Since there are no one-button ma-
chines and no one-button patients, a control thatis not used potentially limits acoustic data by re-stricting proper manipulation of the sound.
GainThe Most Basic of Controls
There are several types of gain found on the ul-trasound system: power/transmit gain, master/receive gain, depth/time gain compensation, andlateral gain compensation.
All systems have controls regulating how muchpower is sent into the body (transmit gain). Youmust remember that transmit gain regulates howmuch power the patient is being insonated with.The Food and Drug Administration (FDA) regu-
lates this gain by exam and transducer type. Mostmodern systems use icons or presets that will notlet you use more power than is allowed for that typeof exam; however, power levels can be exceededby using incorrect configurations. (Example: usingan adult cardiac probe and preset to perform a fetalexam.) It is the responsibility of the operator to en-sure that proper probe types and power levels areutilized.
Master gain or receive gain simply amplifies thereturning signal or the received data, much liketurning up the volume of your stereo.
Another type of gain is depth/time gain compen-sation (DGC/TGC). This gain lets us configure ourgain for depth by compensating for attenuation orthe loss of power throughout the field of view(FOV). DGC lets us amplify far-field echoes andminimize near- and mid-field echoes so a balanced2D display is received. DGC is like master or re-ceive gain in that it is received data that are beingmanipulated, not transmitted gain. You are onlyadjusting the received sound. For a more thoroughexplanation of system controls, refer to the glos-sary of controls at the end of this article.
Lateral gain compensation (LGC) is similar toDGC/TGC but changes the gain across the field ofview. This allows the sonographer to compensatefor lateral loss of power.
Taming the Beast
Your life will be made infinitely easier by usingthe manufacturers specified icons, presets, andexam-type settings. These automatically select the
-
7/29/2019 Why Do We Do the Things We Do
4/20
FDA recommended power settings for 2D, M-mode, and Doppler and allow you to set up yoursystem quickly and efficiently. This does not meanyou dont have to learn the system controls because
their purpose is to fine-tune the presets. Finally,dont be afraid to ask for help if you dont under-stand all of the controls on your system. Request-ing help lets your coworkers know that you are atrue professional and lets you know how much theydont know either.
ProbesThat Old Black Magic
Probes really are the heart and soul of a system.Most manufacturers use basically the same com-
puters and beam forming technologies to provideus with the beautiful pictures we are used to seeing;however, not everyone uses the same probes. Infact, there are very few transducer manufacturers,
and most systems use crystals made by someoneelse for the production of their probes. Specific in-formation on how transducers are manufactured isproprietary.
So Whats Up With AllThese Different Probe Types?
Cardiac sonographers are used to using phased-array probes for echocardiograms. However, mostsonographers cross over into different specialty
20 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY January/February 2005 VOL. 21, NO. 1
FIG. 3.
FIG. 4.
-
7/29/2019 Why Do We Do the Things We Do
5/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 21
areas, and we are used to seeing linear-array probesas well. In fact, it is becoming quite common forshared service systems to utilize all probe types:
phased, flat linear, curved linear, etc. So why do wehave all of them? A basic fact we must learn is thatan ultrasound exam is a series of trade-offs or com-promises. For every advantage a certain technol-ogy has, there will also be a disadvantage. Thesedifferences directly affect the quality and ease ofacquisition of our ultrasound data. We all knowfrom our years of intense study of ultrasound phys-ics that a high frequency will provide better spatialresolution with decreased penetration, while alower frequency penetrates large patients, but thespatial resolution leaves something to be desired.
This is all based on sound wave intervals and otherconversation-starting words like period, wave-length, and cycles per second.
The modern lab of today requires that we selectprobes not only on frequency but also for band-width, footprint, image quality, and Doppler per-formance.
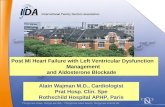
Modern probes also employ broad bandwidths,which means that there are multiple frequenciesavailable for image and Doppler acquisition withineach probe. The listed frequency on the probe is thecenter frequency. As Figure 4 shows, different
transmit and receive frequencies maybe selected tooptimize image quality and penetration and Dopp-ler penetration, sensitivity, and aliasing limits.
Our final types of transducer arrays are linearand curved-linear or switched-array probes. Whilephased and linear probes are both electronic, linearprobes generate their sectors differently fromphased arrays. Linear and curved-linear probes aretypically larger than phased arrays and are ideallysuited for vascular examinations (flat linear) andabdominal, OB/GYN studies (curved linear). Theirlarger probe face, shape, and overall footprint pro-vide much bigger and better near fields than phasedarrays but limit their use in cardiology.
Newer transducers also have bandwidths capa-ble of providing harmonics, which enables en-hanced imaging capabilities. A harmonic image iscreated by sending a frequency into tissue (lets say2 MHz or f 1) and listening to the multiple of thatfrequency (in this case, 4 MHz or f 2). When ultra-soundpropagates through tissue, the inherent resis-tance, along with the time and distance traveled,
produces multiple frequencies in the positive andsubharmonic ranges. Signal-processing techniquesallow the operator to utilize the 2nd harmonic or
the doubled fundamental frequency to our advan-tage. Harmonic imaging allows us to have the ben-efit of low-frequency imaging for penetrationwhile displaying the high-frequency multiple,which provides optimal spatial resolution.
Harmonics are also being used in conjunctionwith ultrasound contrast agents in the positive andsubharmonic frequency ranges to elicit increasedactivity and reflectivity in differing agents.
Okay, now you know a little about sound, its ba-sic controls, frequencies, and probes, so whatsnext?
Christian Doppler: Did He KnowAnything About Blood Flow?
I dont think Mr. Doppler knew anything aboutthe detection of moving blood cells or the potentialrevenue generated by speeding tickets, but his leg-acy is alive and well in both ultrasound labs and po-lice departments. Mr. Doppler was in reality tryingto figure out why stars twinkle (or give off coloredlight shifts, depending on the relative motion be-tween themselves and the stationary observers . . .
us). For fun, look up his original paper On theTheory of Coloured Lights of Stars, written in1842. His genius will amaze you and give you awhole new outlook on the science of Doppler.
His observations stated that if a target is in mo-tion and emitting a light source, then the distancebetween the source and the person or thing observ-ing that motion will increase or decrease. This dif-ference is the frequency shift generated by theshortening or lengthening of the signal intervalsbased on distance. (Say that five times quickly.)
To us as sonographers, it means that if wetransmit a frequency (your choice) from astationary object (the probe) to a moving target(blood cells), the distance between the blood cellsand the probe will either lengthen or shortendepending on the directional movement of theblood. The speed at which this happens is called afrequency shift. The frequency shift is expressed inkilohertz (kHz), converted to velocity (cm/sec) anddisplayed. The equation, which expresses Doppleracquisition, is as follows:
-
7/29/2019 Why Do We Do the Things We Do
6/20
22 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY January/February 2005 VOL. 21, NO. 1
FIG. 5.
FIG. 6.
-
7/29/2019 Why Do We Do the Things We Do
7/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 23
pf= 2foVc
(cos),
wheref= thedetected Doppler frequency shift,fo =fundamental Doppler frequency, V = velocity ofthe moving blood, c = speed of sound in tissue, and = the angle between the ultrasound beam and theflow direction.
Im Not a Mathematician, So DoI Need to Know That Equation?
The answer is YES. You simply cannot be aDopplerist without understanding the Dopplerequation. It relates to and explains everything wedo in Doppler. Let me explain. Delta f is the de-tected frequency shift or the difference betweenwhat was transmitted into the body in MHz andwhat was received in kHz. Lets say, for example,that you used a 6.0-MHz Doppler transmit fre-quency and the received signal was 4.0 kHz in thepositive direction. This means 6 million cycles persecond were transmitted into the bloodstream, andwhat returned was 6 million plus 4.0 kHz. If theblood were moving away from the transducer, thesignal would be read as 6 million minus 4 kHz, andthe display would be in the negative direction.
Now we can see that the frequency shift deltafisalways going to be the product of the equation andwill be affected if we change any of the parametersin that equation. Now lets look at those remainingparameters: 2,fo, V, c, cos.
2This indicates that the sound must travel intothe body and return to the probe. Since thisalways has to happen for Doppler detection,this parameter becomes a constant.
foThe Doppler frequency that you are using.If this changes, the frequency shift willchange.
VVelocity of the blood. This will change, andthechange is reflected in the frequencyshift.
cThe speed of sound in tissue. Again, aconstant.
cosineThe cosine of the angle between the
insonation beam and the blood flow.
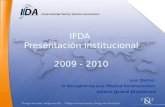
One can now see why you need to understandthe relationship of these parameters. Anychange inthem directly affects the frequency shift. Now youknow why proper Doppler frequency selection andangle are so important. The higher the Dopplerfrequency, the higher the returned frequency shift.The closer to 0 degrees your angle becomes, thehigher the frequency shift becomes. To the novice,this becomes confusing but is easily explained.Doppler is an angles game. The best angle forDoppler is 0 degrees. However, this is difficult(and very painful) to obtain on noncardiac studies.We must therefore rely on varying insonationangles to transmit and receive an adequatefrequency shift. We have all heard that the worstangle for Doppler detection is 90 degrees, andFigure 8 shows why.
FIG. 7.
-
7/29/2019 Why Do We Do the Things We Do
8/20
Okay, I Believe in Anglesbut What Angles Do I Use?
We now have two different sets of rules to liveby. In the vascular and abdominal Doppler world,the Intersocietal Commission for the Accreditationof Vascular Labs (ICAVL) states: Doppler angles
of 60 degrees or less must be maintained. Byproper use of angles within this range, the errors as-sociated in estimating frequencies and velocitiesare minimized. The closer to 90 degrees the anglebecomes, the higher the error rates and associatedspectral broadening artifact. Incorrect angles cancause over/underestimation of signals and intro-duce artifactual spectral noise. Sixty degrees or lesshas been proven to have an acceptable error rangefor vascular and abdominal Doppler. CardiacDoppler is another story, however, and anglecorrection should not be used (0 degrees to the
Doppler cursor).
So Is All of This Just Relatedto the Doppler Cursor Angle?
Yes and no. The insonation angle of the Dopplercursor is but one part of the answer. By using onlythe displayed Doppler cursor, you only know theinsonation angle, and that is all you need for fre-quency detection. However, frequencies are very
difficult to reproduce patient to patient because asour Doppler equation demonstrated, if you changeDoppler probe frequencies or angles, the frequencyshift changes as well. In modern labs with multipleDoppler probes, frequencies, and operators, youcan see how this becomes difficult to work with. Itessentially means that you must have a separate di-
agnostic reference chart for every Doppler fre-quency that you use and for different angles aswell. It can be done, but who needs the grief?
So Whats the Real Deal?
All of the previously mentioned problems existwhen we live in the frequency world. To eliminatethese problems, we simply convert our frequencyshifts to velocities. This is done by inputting theflow angle. The sonographer selects the proper an-gle, that angle (cosine) is then displayed, and con-
version to velocity is accomplished.With proper probe angulation and accurate an-
gle correction, reproducible velocity conversionsare obtained. One can nowutilize multiple Dopplerprobe frequencies at multiple angles, and as long asthe cosine is
-
7/29/2019 Why Do We Do the Things We Do
9/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 25
Pulsed, High PRF and CW Doppler:Gimmicks or Real Tools?
Different types of Doppler exist because not anyone type can provide all of the information onblood flow that we require. Sometimes we need ac-curate range location so we know precisely where aproblem exists. This is when pulsed and high PRFDoppler comes into play. By targeting a specificsite with your sample volume (location) and puls-ing your Doppler frequency at certain speeds(pulse repetition frequency), we can, through timeand distance calculations, accurately assess bloodflow at specific sites. More simply stated, the sys-tem knows the distance from the crystal to the sam-ple volume and how long it will take for the pulsesof Doppler signals to get there. When that elapsedtime has passed, Doppler receivers activate, andthe blood signals at that point in time are collected.How fast we sample that point in time is how wecan accurately assess the speed of the blood. Oursampling time is called pulse repetition frequency
(PRF), or sometimes it is referred to as scale. High-speed flows require high sampling rates (PRF) foraccurate, unaliased detection, and slow-movingblood requires lowPRF for maximum sensitivity toslow flow.
That Sounds Great, but DoesntThere Have to Be a Downside?
Of course there has to be a downside. If thespeed of the blood is faster than one half of thePRF, a pulsed Doppler system will alias, or the sig-nal will wrap around the spectral display. Thisaliasing point is called the Nyquist limit.
One More Time
Example: If our PRF is 6 kHz, the Nyquist oraliasing point is 3 kHz. A detected blood signal >3kHz will be clipped off and seen to be coming fromthe opposite side of the scale. Aliasing is an artifactthat occurs in all aspects of life, and we have all
FIG. 9.
-
7/29/2019 Why Do We Do the Things We Do
10/20
seen examples. The forward-moving stagecoachwheel on TV that appears to be turning backwardsor an airplane propeller that is rotating one direc-tion but appears to be moving slowly in another areexamples of aliasing. Since PRF affects our detec-tion speed, then it would make sense to just in-
crease the PRF to eliminate aliasing. This is whywe select high-PRF Doppler, which, through someelectronic trickery, utilizes multiple sample vol-umes along the Doppler cursor. This allows thesystem to transmit a higher level of PRF to the sam-ple volumes than allowed with single-gate pulsed
26 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY January/February 2005 VOL. 21, NO. 1
FIG. 10.
FIG. 11.
-
7/29/2019 Why Do We Do the Things We Do
11/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 27
Doppler. This works to a point, but even with highPRF selected, some flows, especially cardiacflows, will exceed pulsed Doppler capabilities, andthen we employ another tool, continuous-waveDoppler (CW).
CW Doppler essentially uses a split crystal ortwosets of crystals to continuously transmit and re-ceive Doppler data. Continuous-wave Dopplerdoes not operate with PRF constraints, which pro-vides us the ability to detect and display extremelyhigh velocities without aliasing. The compromise,though (and there always is one), is that wesacrifice range location.
Our sample volume in a CW probe is where thetwo beams intersect and can be quite long depend-ing on probe frequency and configuration. Thislack of a precise sample volume limits accuraterange location. This does not present a large prob-lem in cardiology but can present confusing spec-tral signals in the presence of multiple, closelyspacedarteries andveins,which will allbe detectedsimultaneously in a CW sample volume.
So Which One Do I Use and When?
This is one of those rare moments in life wherethe answer is easyand I have one that works. Accu-rate range location requires the use of pulsed orHPRF Doppler. As long as the PRF is capable ofdisplaying the data you want in an unaliased form,this is the way to go. PW plus HPRF Doppler pro-vides accurate range location and excellent spectralDoppler quality. So to provide velocity informationat a specific location, pulsed Doppler should beused. The downside, Nyquist limits. Continuous-wave Doppler provides limited range location withgood spectral Doppler quality and no Nyquistlimits. Continuous wave should be used when as-sessing peak velocity information. Both are invalu-able tools, and a full-service Doppler laboratoryneeds both.
Color My World
The biggest problem with understanding colorDoppler is eliminating all of the myths that existconcerning color Doppler. The most common are:
FIG. 12.
-
7/29/2019 Why Do We Do the Things We Do
12/20
Color Doppler results are the same from alltypes of systems.
Color Doppler provides quantitative velocitydata.
Color Doppler provides a real-time accurateassessment of blood flow.
Why Are Systems Different?
In reality, color Doppler is not the same from allsystems because not all systems process Dopplerthe same way. Different manufacturers use variousalgorithms to process data, and though the basiccolors of red, blue, and green may look similar sys-tem to system, interpretively, they can be quite dif-ferent. There are no industry standards for whatfrequency shift depicts what shade of blue or red.
Add to this the fact that by changing Doppler trans-mit frequency or color maps and the color schemewill change as well, and you begin to see why dif-ferent systems will provide different-looking data.
I Heard There Was Velocity Data in Color
You are not alone in that belief, but because ofthe way color data are processed, it is impossible toderive accurate velocity data from a color display.Let me explain.
Color Doppler is a pulsed Doppler technology,meaning that to know where to depict the blood, wemust know range location. Just as pulsed spectralDoppler uses a sample volume for range location,color does the same but utilizes many sample vol-umes. In fact, there can be thousands of sample vol-umes being sampled on a color image.
A single sample volume can be corrected for an-gle and the data converted to a velocity. This is thejob that pulsed or CW spectral Doppler does for us.In color, however, since thousands of sample vol-umes are used throughout a large region of interest(ROI), they cannot be angle corrected. Add to thisthe processing method color Doppler uses(autocorrelation), and the problem compounds it-self. Autocorrelation means that all data from allcolor sample volumes being utilized in the color re-
gion of interest are averaged together to produce amean frequency estimate. So, multiple sample vol-umes, uncorrected for angle and averaged together,cannot provide a quantitative velocity. Prettycolors, yes. Quantitation, no.
These facts combined with the slow frame ratesinherent in color Doppler, all of the various systemcontrols that may be used to increase or decreasesensitivity, and different color maps may limit ac-curate, real-time displays of flow.
28 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY January/February 2005 VOL. 21, NO. 1
FIG. 13.
-
7/29/2019 Why Do We Do the Things We Do
13/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 29
So What Is Color Good Forand Why Should I Use It?
Its simple. Now that you know the limitationsof color Doppler, the attributes are easy to see.Color provides qualitative data on three things:
The existence of blood flow: If its there,moving, and you have your system controlsproperly adjusted, you see it.
Direction: If you can detect blood flow, thenyou can tell which direction its going.
Spatial characteristics: Color will show,again all things being properly adjusted, thequality of flow and the spatial characteristics
(i.e., complete filling of vessels, chambers,etc.).
It all adds up to this:
Existence of flow, direction, and spatialcharacteristics of flow = a qualitative
assessment of blood flow.
Color Doppler also provides a rapid assessment offlow abnormalities and general location, so pulsedor CW spectral Doppler can be employed. Spectral
Doppler provides a quantitative assessment offlow.
Im Beginning to Seethe Big Picture Now
Color helps me locate the flow abnormality(qualify), andspectral Doppler then allowsme tomeasure the velocities (quantify).
Youve got it. You can see why spectral Dopplerand color Doppler are complementary technolo-gies. We need them both, and neither one really
stands on its own. I like to look at it as a check andbalance system. Doppler and color show essen-tially the same things but in different-looking dis-plays. This means that if I suspect a problem, bothcolor and Doppler should give positive results. Ifall my data match my suspicions, Ive found theproblem.
Lets Review
Spectral Doppler can be continuous wave orpulsed wave.
CW Doppler detects high frequencieswithout aliasing but has limited rangelocation.
Pulsed Doppler has accurate range locationbut is a pulsing technique (PRF) and will aliasif the speed of the blood exceeds 1/2 of thePRF (Nyquist limit).
Both PW and CW Doppler use the FastFourier Transform (FFT) process to computepeak frequency data from a single samplevolume.
CW and PW Doppler frequency shifts can becorrected for angle and converted tovelocities.
Spectral Doppler data are quantitative data. Color Doppler is a pulsedDoppler technique. Color Doppler must use pulse repetition
frequencies.
Color Doppler uses the autocorrelationprocessing technique.
Autocorrelationaverages the frequency shiftsfrom millions of blood cells moving throughthousands of sample volumes.
A color Doppler display shows averagefrequency data.
Color Doppler data are qualitative data.
FIG. 14.
-
7/29/2019 Why Do We Do the Things We Do
14/20
Doppler Displays
You should now understand that Doppler iscolor andcolor is Doppler. This becomes apparentwhen we look at the similarities in the data pro-vided on our spectral and color Doppler displays.
As Figure 15 demonstrates, all displays show thedifference between positive and negative flows.
The spectral Doppler graph describes flow thatis either moving towards or away from the trans-ducer. A positive spectral shift will be writtenabove the zero baseline. A positive color shift iswritten above thezero color baseline as well. Nega-tive Doppler and color shifts are simply written inthe opposite direction. As the graph shows, thereare different kinds of displays available that all pro-vide the same type of data.
Caution
All Doppler units have spectral and color invertcontrols, which allow positive and negative shiftsto be reversed on their displays. There are timeswhen this is an advantage, such as making arteriesappear red regardless of their direction of flow. Theinvert control can help call attention to venous flow
or reversed flow by encoding it blue. Do not everaccept a color display at face value. Arterial flow isnot always red, and venous or reversed flow is notalways blue. A sound knowledge of anatomy,physiology, and hemodynamics is the best way toavoid mistakes in Doppler diagnosis.
And Finally, Use thePower!!!! (Power Doppler!)
Our final type of blood-detecting technology iscalled power Doppler imaging (PDI).
PDI is essentially the same Doppler signal thatcolor Doppler uses but is processed differently onthe return trip through the system electronics.
Color Doppler is a display of the non-angle-corrected, average, or mean frequency shiftedDoppler data that is returned from the insonated
blood. It is displayed in varying shades of red andblue and is subject to all of the artifacts and limita-tions of pulsed Doppler technology.
Power Doppler displays the power or amplitudeof the returned signal. Now, at this point, the aver-age readers eyes begin to glaze over, but just bearwith me for a moment as it is really rather easy tounderstand. Think about this; every b-mode image
30 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY January/February 2005 VOL. 21, NO. 1
FIG. 15.
-
7/29/2019 Why Do We Do the Things We Do
15/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 31
you produce and look at displays amplitude. Thestrongest amplitudes are displayed as the brightestwhites, and the weakest amplitudes are displayed
as the darkest grays or blacks.Power Doppler simply analyzes the strength oramplitude of the insonated blood cells and displaysthose ranges in shades of gold or yellow or some-thing close to that. The highest concentrations ofblood cells are located in the center of blood ves-sels, so the power display is brightest there. Thereare less blood cells at the edges of the vessels, sothe returned amplitude signals are smaller, thus thedefinition of vessel walls. Those signals are dis-played in shades of darker colors.
Since we are looking at amplitude, not fre-
quency data, PDI is not subject to the commonDoppler artifacts such as aliasing, angle ofinsonation, etc. PDI is not as dependent on anglesas color, so the typical signal dropout at 90-degreeinterfaces is greatly reduced.
And an added bonus is that PDI is more sensitiveto extreme slow flow than color Doppler is!
So, if you need to know the direction of bloodflow, use color Doppler and live with the inherentartifacts.
If you need extreme sensitivity to slow flow orneed to visualize residual lumens better or just hate
Doppler artifacts, use power Doppler. As I saidway back at the beginning of this article, though,everything has a trade-off, and PDI is much moresensitive to motion artifact, so uncooperative pa-tients will present a problem. Also, PDI does notdisplay hemodynamics very well, so color shouldbe used to evaluate the motion of blood.
A Glossary of Doppler/Color DopplerControls, Functions, and Uses
Note: All ultrasound systems use basically thesame controls, but not all of the controls are calledthe same thing on all ultrasound systems. Its notthat manufacturers deliberately try to confuse you,but marketing people need something to do withthe thesaurus they got in college. Patents, trade-marks, and lawyers also figure into this situation.All controls listed here use generic but accuratenames.
PRESETS/ICON
Function
Allows rapid optimization of image, Doppler,and color parameters for all clinical applications.Proper use of system icons saves time, reduces but-ton pushing, and ensures diagnostic results.
Recommendations
Presets/icons do many useful things. Many ul-trasound manufacturers provide presets as a placeto start, but optimizing the presets to lab prefer-ences will be helpful. Their use sets proper gains,powers, PRF, DGCcurves, filters, etc. Most impor-
tant, they provide the FDA-recommended powerlevels for each application. Different clinical situa-tions require that you intervene with system con-trols to optimize parameters. Use the preset/iconsetting as a stepping-off point and adjust controlsaccordingly to clinical needs. Dont worry aboutpower settings as the proper preset/icon selectionwill not let you exceed power levels for thatapplication.
Clinical Situations
Improper use of preset/icons will yield inade-quate results. For example, the leg vein preset/iconsets parameters for low-speed venous flow detec-tion. Trying to perform cardiac studies with the legvein preset/icon will result in sensitivity to slow,phasic flow but no aliasing control for high-speedcardiac flow. Using the renal icon for a carotidstudy would provide the wrong filters and PRF per-formance, so a carotid study would be inadequate.
Let the preset/icons work for you, not againstyou. You will save time, avoid frustration, and ob-tain optimal clinical data.
MASTER OR RECEIVE GAIN:COLOR OR SPECTRAL DOPPLER
Function
Increases or decreases the received signalonly
Does notcontrol insonative energyinto tissue
-
7/29/2019 Why Do We Do the Things We Do
16/20
Recommendation
Dont rely on icon preset adjustments. Alwaysadjustgain for optimal signal display. Sometimes ithelps to increase gain until display becomes noisyand then reduce gain to an acceptable level. Thisensures you have correct gain settings.
Clinical Situations
Not enough Doppler gain = reduced displayof low flow.
Too much image gain can minimize colordisplay.
Too much color gain causes color bleedingonto tissue.
PRF/SCALE
Function
Scale or PRF controls the sample time or looktime that is required to process Dopplerinformation.
Slow flow detection requires low PRFsettings.
High flow detection requires high PRF
settings. PRF also controls aliasing.
Recommendation
Do not rely on preset/icon PRF settings. Scalemust be adjusted for each patient and different clin-ical situations. Use the preset as a starting pointonly. Increase or decrease scale for high or lowflows and to control aliasing.
Clinical Situations
Increased PRF may eliminate display of ex-tremely slow flows. When you suspect total occlu-sion or small areas of reflux, scale must be set atlower levels. Remember, color alone cannot diag-nose total occlusion. Only rare cardiac situationsrequire changing color Doppler PRF.
Scale set too low will cause Doppler aliasing.Remember: aliasing occurs if the speed of the
blood is faster than 1/2 PRF (Nyquist limit). Nor-mal flow can alias.
Scale set too low in color can cause tissue flash
to overlie blood signals or show color outside ofcardiac chambers.
HIGH-PASS FILTERS (HPF)
Function
Blood signals are high frequency, lowamplitude.
Tissue signals are low frequency, highamplitude.
Low-frequency tissue signals can mask lowblood flow signals.
Filters help to eliminate low-frequencysignals from tissue, thereby increasing thedisplay of slow blood flow.
Recommendation
Use filters to display low-flow signals and re-duce tissue flash. Filters should be set independentof PRF if possible.
Caution: Think of filters as electronic erasers.They eliminate all signals from frequency shiftslower than the filter number you select (i.e., a filter
setting of 200 Hz will display no frequencies lowerthan 200 Hz).
Clinical Situations
Filters set too high will erase slow flow inextremely stenotic lumens and valves.
Filters set too high can erase bidirectionalflow in dissected vessel lumens.
Filters set too low will cause tissue flash toobliterate small vessels.
Filters set too high will erase the diastolic
component of the waveform and the colorprofile.
Filters set too high will erase small refluxflows.
Use caution when comparing Doppler resultsfrom different systems. If the filters are notthe same, the diastolic or low-flowcomponent of the waveforms and colors canbe different.
32 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY January/February 2005 VOL. 21, NO. 1
-
7/29/2019 Why Do We Do the Things We Do
17/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 33
DOPPLER ANGLE/STEERING
Function
To provide optimal angle of interrogation anglesfor accurate Doppler signal acquisition. Rememberthat interrogation angles closest to 0 degrees pro-vide highest frequency shifts.
Recommendation
Spectral Doppler requires angles less than 60 de-grees in vascular work and 0 degrees in cardiac foraccurate conversion of frequency shifts to veloci-ties. The closer your angles are to 0 degrees, thebetter the quality of the signal will be, and velocity
conversion will be even more accurate.Color Doppler does not display velocity data;therefore, angle is not as critical. Most color map-pers provide steering angles of 20 degrees left orright of center. This provides directional color (red/blue). Vessels that lie closest to 0 degrees will dis-play the highest shifts and can cause aliasing. Re-member, if you need directional color, steer left orright. Maximum color sensitivity to extremelyslow flow, however, is obtained at the 0-degreeangle.
DOPPLER/COLOR INVERT
Function
A Doppler invert control simply reverses the di-rection of the Doppler display. This helps maintainan antegrade or retrograde display for exam conti-nuity regardless of flow direction.
Recommendation
Tortuous vasculature will have flow that movesin one direction in the vessel but in many directions
to the interrogating Doppler beam. Use the Doppler/color invert control to maintain a unidirectional coloror spectral display.
Clinical Situations
Vascular labs have adopted the practice of dis-playing arteries as red and veins as blue. This canbe easily accomplished as the major arteries and
veins in the neck and extremities are somewhatstraight. Using Doppler/color invert makes it fairlysimple to maintain a red or blue display regardless
of the angle of Doppler interrogation.This is not the case in abdominal or cardiacDoppler. In these studies, red conventionally indi-cates positive flow, and blue indicates negativeflow.
REGION OF INTEREST SIZE
Function
The color region of interest (ROI) is adjustablein theaxial and lateral dimensions to facilitate sam-pling large and small organs, various lengths of
vessels, and small areas such as stenotic heartvalves.
Recommendation
The color ROI should be kept as small as possi-ble to maintain optimal system performance.Opening the ROI in the axial dimension adds hun-dreds and sometimes thousands of sample volumesfor color processing. If these sample volumes are intissue and not the vasculature being sampled, thesystem is made inefficient by having to service
sample sites of no interest.Increasing the ROI in the lateral dimension has a
direct result on system frame rate and thereforetemporal resolution. The wider the ROI is opened,the slower the frame rate becomes. Conversely, thesmaller the ROI, the faster the frame rate. For opti-mal system performance, keep the ROI as small aspossible while sampling the necessary area ofinterest.
Clinical Situations
It can be advantageous to display long segmentsof vessels, entire organs such as the kidneys, orcomplete cardiac chambers. This makes for easyinterpretations, but frame rate and temporal resolu-tion can be severely compromised. When it is nec-essary to increase ROI width, try reducing thecolorquality setting. By reducing the number of timeseach color vector is sampled, frame rate will in-crease. When color quality is set at its lowest set-
-
7/29/2019 Why Do We Do the Things We Do
18/20
ting and the ROI is at its smallest size, the systemwill be at its most efficient performance level.
COLOR QUALITY
Function
Controls the dwell time or sampling time forcolor Doppler. Color quality is also known aspacket size or length and ensemble length. It sim-ply means how many times and for how long doesthe system sample each color vector for our threebasic components of flow, direction, speed andvariance, or turbulence.
Recommendation
Color quality is directly related to how good thecolor display is. The longer the dwell time, the pret-tier and more homogeneous the color display. Ashorter dwell time results in a more pixilated colordisplay with a more accurate display ofhemodynamic changes. The sonographer must de-cide what the quality of the color display will be.
Clinical Situations
Color quality affects frame rates. The longer thedwell time, the prettier the color, but the slower theframe rate becomes. Reduced dwell times providecolor images that may not be as aesthetically pleas-ing but will have faster frame rates and thereforebetter temporal resolution.
B-SCAN/COLOR PRIORITY
Function
Allows color Doppler information to be dis-played when vasculature is too small to be visual-ized in B-scan.
Recommendation
A color mapper is designed to write color whereit sees no gray-scale tissue data. This makes it easyfor the system to write color on black vessels andnot on tissue. There are many blood vessels in thebody, however, that are smaller than the image res-olution capabilities of ultrasound technology.
These vessels contain moving blood that Doppleris detecting, but since they are not seen as black,the system does not write color in them. B-scan/
color priority overcomes this liability by reducingthe priority of gray scale in the decision process ofwriting color data. By reducing the gray-scale pri-ority, color will be written in areas that are detectedby Doppler but not displayed in B-mode imaging.
Clinical Situations
Incorrect B-scan/color priority settings willeliminate flow from tiny vessels that are not visual-ized. When performing color Doppler studies ofthe thyroid, testicles, fingers, tumors, etc., whichtypically have microvasculature, be certain that thepriority is given to colornot B-scan.
COLOR MAPS
Function
To provide different color schemes for the dis-play of various hemodynamic conditions.
Recommendation
Everyone perceives color differently. Select thecolor map that presents the most frequency data(color) to your eyes. Icon or preset maps are usu-ally best suited for their particular applications.
Clinical Situations
Red/blue mapsprovide directional indication. Arainbow map displays more colors than red andblue to match the various frequency shifts present.A rainbow map shows all flow present. The vari-ance map should be used to indicate turbulent flowassociated with luminal stenosis or valvularstenosis.
IMAGE/DOPPLER FREQUENCY CONFIGURE
Function
Provides multiple frequencies for 2D, spectral,and color Doppler imaging. These frequencies mayall be different from the center frequency of theprobe.
34 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY January/February 2005 VOL. 21, NO. 1
-
7/29/2019 Why Do We Do the Things We Do
19/20
WHY WE DO THE THINGS WE DO (IN ULTRASOUND) / Milburn 35
Recommendations
Frequency configure is an extremely importantcontrol as it lets the sonographer optimize theproper frequency to the clinical situation.
When it becomes advantageous to use highertransmit or receive frequencies for increased back-scatter, greater sensitivity, improved spatial resolu-tion, or lower frequencies to increase penetrationand reduce aliasing, frequency configure should beused.
Clinical Situations
When using a 2.25-MHz transducer to image theheart, shifting image and Doppler frequencies can
increase/decrease image resolution and Dopplersensitivity, increase/decrease Doppler backscatter,and improve color resolution. Backscatter can beincreased for signal strength, small signals can bereceived at higher frequency shifts for easier detec-tion, and resolution can be increased in bothimaging and Doppler.
A Few More Interesting ThingsYou Might Want to Know
The following charts list the most commonly
used metric measurements. Since we use the metricsystem in medicine, you must be familiar withthese values and terms.
CUSTOMARY/METRIC CONVERSIONS
Linear Measurements
10 millimeters = 1 centimeter10 centimeters = 1 decimeter10 decimeters = 1 meter10 meters = 1 decameter10 decameters = 1 hectometer10 hectometers = 1 kilometer
Square Measure
100 sq. millimeters = 1 sq. centimeter100 sq. centimeters = 1 sq. decimeter100 sq. decimeters = 1 sq. meter
100 sq. meters = 1 sq. decameter 100 sq. decameters = 1 sq. hectometer100 sq. hectometers = 1 sq. kilometer
Cubic Measure
1000 cu. millimeters = 1 cu. centimeter1000 cu. centimeters = 1 cu. decimeter1000 cu. decimeters = 1 cu. Meter
Linear Measure
English Metric
1 inch 25.4millimeters 0.3937inch 1 centimeter
2.54 centimeters
1 foot 30.48 centimeters 3.937 inches 1 decimeter
3.048 decimeters
0.3048 meter1 yard 0.9144 meter 39.37 inches 1 meter
3.2808 feet
1.0936
1 mile 1609.3 meters 3280.8 feet 1 kilometer
1.6093 kilometers 1093.6 yards
0.6137 mile
0.6138
0.03937 inch 1 millimeter
METRIC SYSTEMS
Powers
of Ten Prefix Symbol Meaning10
9giga G billion
106
mega M million
103
kilo k thousand
102
hecto h hundred
101
deca da ten
101
deci d tenth
102
centi c hundredth
103
milli m thousandth
106
micro millionth
109
nano n billionth
COMPLIMENTARY METRIC UNITS
Numbers Metric Equivalents
billions and billionths giga & nano G & n
millions and millionths mega & micro M &
thousands and thousandths kilo & milli k & m
hundreds and hundredths hecto & centi h & c
tens and tenths deca & deci da & d
-
7/29/2019 Why Do We Do the Things We Do
20/20
JDMS21:3637 January/February2005
JDMS21:3637 January/February2005
SDMS-JDMS CME TEST
Article: An Overview: Why We Do the Things We Do (in
Ultrasound)
Author: Donald T. Milburn, RDCS, RVT
Category: Cardiac Physics and Instrumentation (CPI)
Credit: 2.0
Objectives: After studying the article, An Overview: Why
WeDothe Things WeDo(inUltrasound), youwillbe able to
1. Describe optimal angles for Doppler tracings in cardiac
and in abdominal and vascular examinations.
2. Describe the work of Christian Doppler.
3. Analyze the footprint associated with different types of
transducers.
4. Associate types of gain to tissue and image effects.
5. Describe characteristics of color Doppler and continuous
wave Doppler.
6. Convert metric values.
7. Define Nyquist limits that result in aliasing.
8. Describe the use of filters.
9. Specify synonyms for pulse repetition frequency.
1. In a cardiac sonography examination, the Doppler angle
should be _____ degrees.
a. zero
b. 45
c. 60 or lessd. 90
2. Which of the following probes typically has a small
footprint?
a. linear array
b. curved linear array
c. switched array
d. phased array
3. Theoretical bioeffects ofultrasoundarerelated towhichof
the following?
a. transmit gain
b. master gain
c. depth/time gain compensationd. near field gain
4. Christian Doppler investigated which of the following?
a. velocity of moving blood cells
b. conversion of matter to energy
c. light emitted from stars
d. movements of bats
5. A signal will alias with pulsed Doppler when the speed of
blood is faster than ____ the pulse repetition frequency.
a. .05 times
b. .5 times
c. 1 times
d. 1.5 times
6. Continuous wave spectral Doppler is useful fora. assessing peak velocity without aliasing
b. providing velocity information at a specific location
c. converting the signal to a color display
d. determining the Nyquist limit
7. Filters set too low will
a. erase small reflux flows
b. erase slow flow in stenotic lumens
c. erase bidirectional flow
d. allow tissue flash to obliterate small vessels
8. Which of the following statements about color Doppler is
false? Color Doppler
a. is qualitative datab. is continuous wave Doppler
c. displays average frequency data
d. uses the autocorrelation processing technique
9. Pulse repetition frequency (PRF) is also known as
a. velocity
b. amplitude
c. scale
d. power
10. 254 millimeters is how many decimeters?
a. 0.254
b. 2.54
c. 25.4
d. 254
36 JDMS 21:3637 January/February 2005
http://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asphttp://www.sdms.org/members/JDMS/jdmscme2101.asp