Why Commission Early Detection Services? John Marshall Assistant Director Commissioning ALWPCT.
32
Why Commission Early Detection Services? John Marshall Assistant Director Commissioning ALWPCT
Transcript of Why Commission Early Detection Services? John Marshall Assistant Director Commissioning ALWPCT.
Why Commission Early Detection Services?
John Marshall
Assistant Director Commissioning
ALWPCT

What I want to cover
• Policy Context for commissioning• Policy Context as it relates to mental health• LDP Targets• Evidence• DUP /DUI• Economics• Added Value of Provider• Summary• Personal thought.

Policy Context for Commissioning
• NHS Plan (2000)• Shifting the Balance of Power (2001)• National Health Service Reform and Health Care Professions
Act (2002)• Delivering the NHS Plan (2002)• Plans for Foundation trusts (2002)• NHS Improvement Plan (2004)• Choosing Health (2004)• Our health, our care , our say (2006)• CPLNHS (2006)

Effective commissioning makes the best use of allocated resources to achieve the following
goals:
• improve health and wellbeing and reduce health inequalities and social exclusion;
• focus on prevention and early intervention
• secure access to a comprehensive range of services; • improve the quality, effectiveness and efficiency of services; and
• increase choice for patients and ensure a better experience of
care through greater responsiveness to people’s needs.

Policy Framework Mental Health• ‘New Ways of Working for
Psychiatrists’ – enhancing effective person centred services through new ways of working in multi-disciplinary and multi-agency context;
• Out Health, Our Care, Our Say – a new direction for community services;
• Everybody’s Business: Integrated mental health services for older people – a service development guide;
• Making it Possible: Improving Mental Health Well-being in England – Care Standards Improvement Partnership & NIMHE;
• From Values to Action: The Chief Nursing Officers review of Mental Health Nursing;
• The Neglected Majority – Sainsbury Centre;
• Social Perspectives Network for modern mental health;
• NSF’s, Children/ Adults Older People
• The NSF 5 Years on.• The Journey to recovery• The Future of Mental Health: Out
Vision for 2015 – Sainsbury Centre/LCA/NHS Confederation;
• Services Users and Carers: Our Vision – Rethink;
• Mental Health Act;• PbC, PbC, PbC/PbR, PbR, PbR.


LDP Targets.
• PCT’s are required to commission Early Intervention in Psychosis Services.
• Number of people with newly diagnosed cases of first episode psychosis receiving early intervention in psychosis services
• Local target is for 164 places over 3 years.• Recovery target of 54 places per year.• Our needs assessment indicated that we would
need no more than 90 places.• This was based on ………

• Assumptions of numbers requiring early intervention figures are based upon local needs assessment.
• Population aged 15 – 34 in Wigan = 78,889 (2001 Census)
• Actual number of in-patient admissions to Wigan services for individuals aged 17 – 25 with first episode diagnosis of schizophrenia.
• 1998 = 25, 1999 = 24, 2000 = 22
• Incidence figures from study by Scully suggest an expected
prevalence rate of 2 – 4 individuals per 10,000 of relevant population which equates to an assessed need between 16 – 32 individuals per year.
• Given the actual number of admissions and the expected prevalence we believe that our plans for a service for 30 new case per year, leading to a total case load of 90 over 3 years are adequate.
Number of people receiving early intervention services.

Current performance against target
• 62 people in service over 2 years
• Expected Outturn of 30 this year.
• 3 potential reasons for this.i. The trajectories are not accurate.
ii. The services within Wigan have affected the prevalence rate of psychosis thereby affecting trajectories.
iii. The current EI service is not effectively capturing all new cases of psychosis.

Evidence
• There is a growing body of good evidence to support the development of Early Detection Services.
• However Cochrane review States
“At the moment it is not clear whether treating people presenting with prodromal symptoms of schizophrenia provides any benefits. There is insufficient data on personal and social consequences of providing treatment to people who will not necessarily become unwell. Specialised treatment services for people with prodromal
symptoms are only justified on an experimental basis.” (Marshall et al 2006)

Cochrane also says
“For people in their first episode of psychosis there is little evidence to support the intervention of specialist teams for people in their first episode of psychosis. However, since such people do require treatment in some form, the ethical issues are less intense than
for people with prodromal symptoms.”
However
• Many other mental health services have been developed without solid RCT methodology, initially, and have proved to be successful.
• Case Management, Home Treatment, Assertive Outreach,
• Treatment for Hay fever ………• Early Intervention is a National priority.
And it is not just us.

Canada’s Early Intervention Services
Ontario:•PEPP, London •FEPP, Toronto •Psychotic Disorders U., Hamilton•Ottawa FEPP•KPP&TP, Kingston
Alberta:•EPT&PP, Calgary (930,000)
British Columbia:•EP Initiative of British Columbia•EPIVMHC,Victoria•Vancouver•EPIP, White Rock
Quebec:•Levis•Montreal•Quebec City
Nova Scotia:•NSEPP•Halifax -
Saskatchewan:•EIPP, Saskatoon
Key figures:•Jean Addington•Bob Zipursky•Ashok Malla•Lili Kopala
Newfoundland•N&L EPP

Early Psychosis Programs in the USA
Pittsburg:•EI program (Keshevan)
N. Narolina:•FEP & prodrome studies (Lieberman)
New York:•Prodrome (Cornblatt)
Yale, New Haven:•PRIMHE (T. McGlashan)
Portland, Maine•PIER service (McFarlane)
LA California:•UCLA (Ventura, Neuchterlien etc)
Bethseda, MD: •NIMH research:(Wyatt etc)
Salem, Oregon:•Early Assessment & Support Team (EAST) (pop 600,000) Managed care funded

New Zealand’s Early Intervention Services
• Auckland: EPI Centre, Kari Centre, Taylor Centre, Manaaki CMHT - FEP, St Lukes FEP, Hartford House EPI, Campbell team Lodge EI team
•Wellington: Wellington EI service (400,000)
•Christchurch: Tatara House EIP service (380,000)
•Dunedin: Aspiring House EI service (150,000)
..
...
New Zealand National Early Intervention Group

Early Psychosis Programs in Australia
Victoria:•EPPIC•Dandenong•EP Program, Alfred Hosp.•Central East EP Project
Western Australia:•First Psychosis Liaison Unit, Bentley•EPOES, Fremantle •EEPP, Rockingham/Kwinana
New South Wales:•YPPI service, Gosford•EP program, Marouba•EP program, North Sydney•EPIP-SWAHS, Liverpool•EPIC, Penrith•Western Sydney FEPP
South Australia:•Noarlunga EP Program
Queensland:•Uni of Brisbane studies
ACT:•Canberra EI service .. . ..
.
..
National Early Psychosis Project (based at EPPIC)

South East Asian Early Psychosis Network
Singapore:EPIP
1 team covers 4 M(S. Chong et al)
Tokyo, Osaka
(South Africa)Palau, Miconesia
Hong Kong: EASY - 4 teams cover 7M
(Eric Chen et al)
South Korea

Swiss Early Psychosis Programs
Geneva & Zurich:Swiss Early Psychosis Project SWEPP (Simon, Umbricht & Merlo)
Bern:•Uni Hosp. of Social & Comm. Psych.(Gekle) (Merlo - moved to Geneva)
Basil:•Uni Hosp. Basil: Basil FEPSY screening study (Gschwandtner et al)

German Early Psychosis Programs
Mannheim:•Central Insitute of Mental Health (Hafner, Maurer et al)
Dusseldorf:•RCT of psychological Rx in FEP (Klinberg)
Bonn:•Prodrome Rx (Hambrecht et al)
Cologne:•Cologne early Recognition study (Klosterkotter, Schultze-lutter et al)
Heidelberg: •Heidelberg Early Adolescent & Adult Recognition & Therapy Centre for Psychosis (HEART) EI service since since 1994 (Franz Resch et al)
Vienna, Austria:•Adolescent EI program at University Hosp. of Vienna (Amminger, Edwards)
......

Scandinavian Early Psychosis Services
0
2
4
6
8
10
12
14
16
DUP (median in weeks)
Early detectionStandard
Norwegian Services:•TIPS - Roskilde/Stravanger (Larsen, Johannessen etc)•UNA-projektet, Oslo•EOP, Skien
Swedish Services:•Parachute Project (1.5 M), Stockholm•Sodertalja Psykiatriska Sektor, Sodetalje•TUPP Project, Stockholm (Cleland)
Finland:•Turku: Detection of early Psychosis project(Suomela et al)
Control
DU
P m
edia
n (
wee
ks)

Dutch & Belgian EI Programs
Belgian Projects:•PECC (Janssen-Cilag)
Netherlands:•Academic Medical Centre (Don Linszen)•University of Maastricht: NEMESIS (Van Os, J.) •University Med Centre, Utrecht (Dutch Prediction of Psychosis Study- DUPS)
Other European Projects:•European Prediction of Psychosis (EPOS) study (6 centres: Birmingham, Amsterdam, Cologne, Turku, Santander, Dannstadt)•Dublin: SJOG Hospital (E. O’Callaghan)•Bordeaux: (Helen Verdoux)•Barcelona, Madrid, Santander: 4 prodrome research programs•Lisbon: planning EI service•Eastern European, Russian & Middle East: research programs & plans for services

Summing up RCT’s
“Strictly speaking randomised controlled trials are still needed to confirm the effectiveness of early detection and intervention services. However, the testimony of patients and families, non – randomised evaluations of services such as those provided by EPPIC and obvious validity or common sense supports their wider introduction.” (Lewis and Drake 2001)
“It should be acknowledged that scientific evidence is not the only driver of service reform; socio-political factors, including political pressure and community demand based on perceived gaps and deficiencies are also potent forces.” (Edwards et Al 2005)

• Duration of Untreated Psychosis DUPthe amount of time from onset of symptoms of psychosis to the prescription of antipsychotic medication
• Duration of Untreated Illness DUIthe amount of time from the recognition that things are not going well to the prescription of antipsychotic medication
DUP / DUI
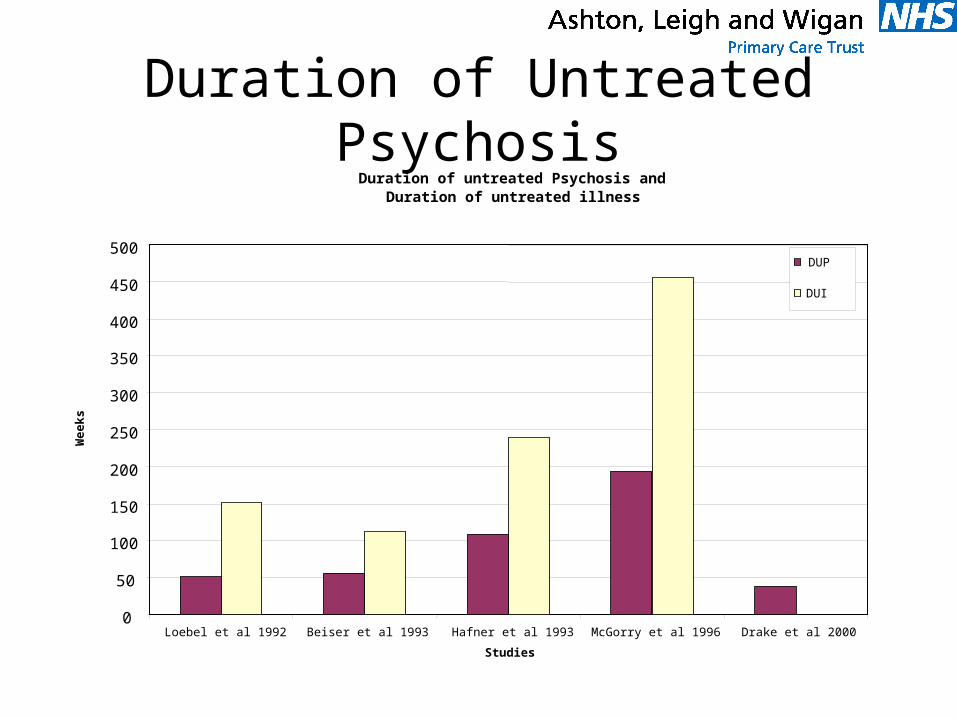
Duration of Untreated PsychosisDuration of untreated Psychosis and
Duration of untreated illness
0
50
100
150
200
250
300
350
400
450
500
Loebel et al 1992 Beiser et al 1993 Hafner et al 1993 McGorry et al 1996 Drake et al 2000
Studies
Wee
ks
DUP
DUI

Reduction of DUP/DUI should be the core business of Early Intervention services
“DUP has been reported to be 1 to 2 years. Case note narratives
and studies of pathways into care suggest that this period is characterised by contacts with criminal justice services, visits to a and e and interruptions to employment. All of these consequences incur costs, and interventions to reduce DUP should reduce these.” (McCrone 2007)
YET “DUP is not a valid measure for establishing the effectiveness of
early intervention services that aim solely to provide evidence – based care in an assertive manner without an early detection arm” (Swaran P. Singh (2007)

Economics• Schizophrenia 2 to 3% of total NHS budget.• Extrapolating PCT total budget of £450m • £9m to £14m of a £30m mental health
budget.• Locally just under 1000 people with psychotic
disorder.• Per person = £9000 to £14000 per patient per
year, NHS costs.

Economics cont’d
• Service sees 60 people per year• Potential costs if 100% Transition• Range £480,000 - £840,000
• Potential cost of 30 – 40% transition• 2% £480,000 30% =£144k 40% = £192K• • 3% £840,00030% = £252k 40% = £336k• • Unknown savings on SS costs• Potential significant saving for those who may have transited
without early intervention.

The provider
• BST are one of the few organisations in the world delivering Early Detection Services.
• BST have the relevant skills to deliver the service.• The service is and will continue to be subject to robust
research and evaluation.• The service will provide additional expertise to our
whole system and bring added value.• The service will complement and enhance our current
early intervention service.• Wigan residents will benefit from a cutting edge service.

In Summary
• NHS policy expects commissioners to be effective commissioners who increasingly focus services upon wellbeing, prevention and early intervention.
• In mental health terms this is about transforming services to focus upon individuals rather than services
• The requirement to deliver Early intervention Services is a recognition of these agendas.
• This service will help the PCT to meet it’s targets around Early Intervention.
• Commissioners need evidence of effectiveness to commission services, however, evidence comes in many shapes and forms and services have not traditionally been developed after successful RCT’s

Summary cont’d
• The evidence for Early Intervention and Detection is developing, but there is growing international evidence that these services are effective. This is supported by the level of both international and national resources being ploughed into this area.
• There is an emerging view that Early Intervention Services will not reduce the duration of untreated psychosis without an Early Detection function associated with the service.
• The economic arguments for preventing or delaying the onset of psychosis are compelling.
• The added value in terms of skills, training,research and evaluation that this service will bring cannot be underestimated

Finally
• A Personal Thought…………..