Whole Health Coaching Participant Manual.Feb19.2021
146
WHOLE HEALTH COACHING Participant Manual Created under contract with TechWerks, LLC
Transcript of Whole Health Coaching Participant Manual.Feb19.2021

WHOLEHEALTHCOACHINGParticipantManual
CreatedundercontractwithTechWerks,LLC

VHA Office of Patient Centered Care and Cultural Transformation
• Assist the Veteran in developing a per-sonalized health plan that is based on what matters most to the Veteran; the plan is based on the Veteran’s own goals, values, preferences, and lifestyle. The agenda is the Veteran’s.
• Partner with the Veteran with proactively taking action toward behavior change that is present- and future-oriented.
• Recognize that health is much broader than the absence of disease. The emphasis is on health enhance-ments/strengths rather than disorders/weaknesses.
• Support the Veteran in achieving their standard of optimal health that takes into account the mental, physical, and social well-being of the Veteran.
TIME COMMITMENT: Pre-Course Orientation - 1 hrSession 1 - 25 hrsBetween session Triad Calls - 6 hrsSession 2 - 24 hrsAsynchronous Learning - 5 hrsSession 3 - 25 hrsPost-Course Triad Calls - 6 hrsAsynchronous Learning - 15 hrs
The virtual Whole Health Coaching course integrates principles of change theory and practice to support Veterans in realizing their health potential.
LEAVE WITH THE SKILLS TO:
VHA WHOLE HEALTH COACHING
COURSE FORMAT:
Virtual learning (Zoom)Class discussionWH coaching practice Skills practiceSmall groups
*Daily tech support will be available
Participants wishing to receive CEUs and a cer-tificate of completion re-quired for their application for NBC-HWC certifica-tion must attend all three weeks of training (75 hrs), all 12 hours of triad prac-tices, and all 20 hours of asynchronous training.
COURSE ACCREDITATION:
NBHWC
Register HEREFor more information, contact: [email protected]
WHY WHOLE HEALTH COACHING?
Whole Health Coaches play an integral role in Veterans’ behavior change and the radical redesign of health care, and the OPCC&CT is committed to providing optimally trained Whole Health Coaches for Veterans.
Health coaches can provide individual and group coaching services not only within the Well-being Program but also within Whole Health Clinical Care.
VHA Office of Patient Centered Care and Cultural Transformation
WHO SHOULD APPLY TO ATTEND?Dedicated Health Coaches, PACT members, social workers, RNs/LPNs, pharmacists, peer support specialists, medical assistants, residents, physical therapists, kinesiolo-gists, dietitians, and individuals associated with behavior change programs, to name a few. Non-clinicians are encouraged to attend, especially those interested in serv-ing in a health coaching role. CME accreditation is available for physicians, non-phy-sicians, pharmacists, dietitians, nurses, psychologists, and social workers.
• VA staff in a Whole Health Coach PD
• VA staff who are connected to the local Whole Health Program and want to support the evolution of Whole Health at their medical center.
FINAL CONSIDERATIONS• To be eligible to apply for the national board exam, participants must complete
an approved training program and submit a log of 50 coaching sessions along with their certificate of completion from the course. Participants may start documenting sessions after meeting all course requirements and receiving their certificate of completion. The recommended time to complete the coach-ing sessions is 6 months.
• This is not an exam preparation course; however, attending this program will better prepare participants for the national board certification exam along with a rigorous independent study plan.
• In order to use the new 2020 American Medical Association Health Coach CPT code, health coaches need to be NBHWC certified. Non-certified coach-es cannot use CPT codes.
For more information about NBHWC, please visit their website: www.nbhwc.org
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|3
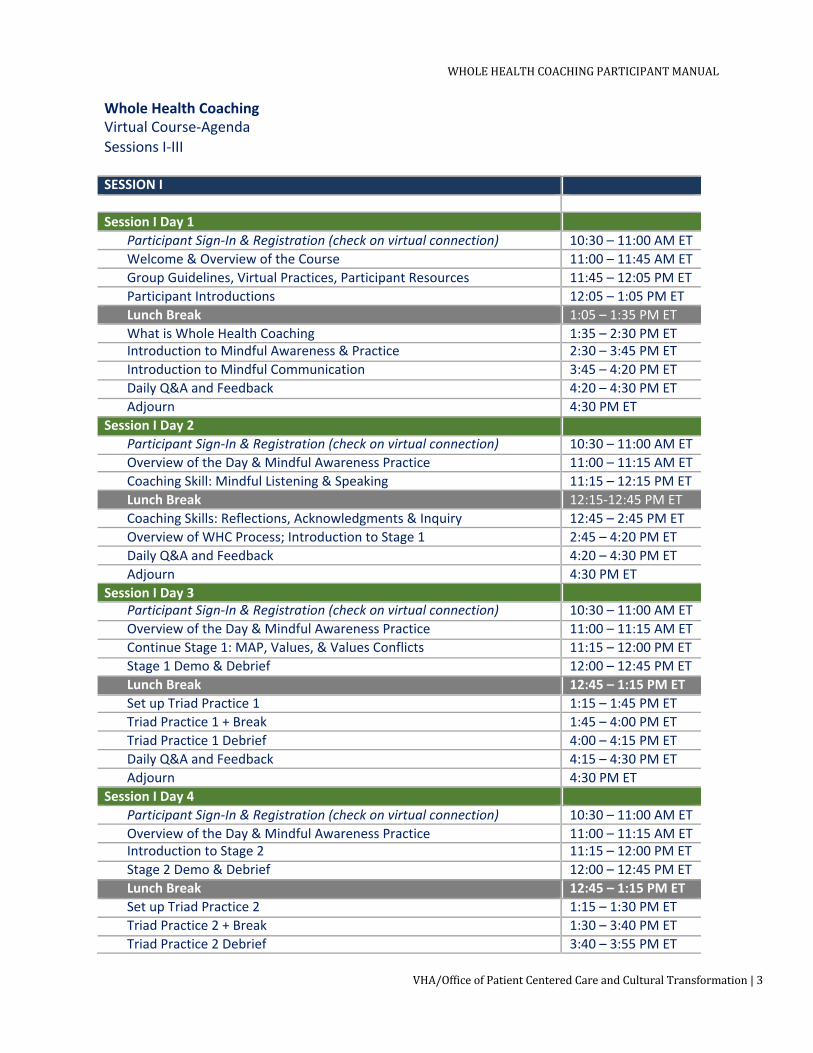
Whole Health Coaching Virtual Course-Agenda Sessions I-III
SESSION I Session I Day 1
Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Welcome & Overview of the Course 11:00 – 11:45 AM ET Group Guidelines, Virtual Practices, Participant Resources 11:45 – 12:05 PM ET Participant Introductions 12:05 – 1:05 PM ET Lunch Break 1:05 – 1:35 PM ET What is Whole Health Coaching 1:35 – 2:30 PM ET Introduction to Mindful Awareness & Practice 2:30 – 3:45 PM ET Introduction to Mindful Communication 3:45 – 4:20 PM ET Daily Q&A and Feedback 4:20 – 4:30 PM ET Adjourn 4:30 PM ET
Session I Day 2 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Coaching Skill: Mindful Listening & Speaking 11:15 – 12:15 PM ET Lunch Break 12:15-12:45 PM ET Coaching Skills: Reflections, Acknowledgments & Inquiry 12:45 – 2:45 PM ET Overview of WHC Process; Introduction to Stage 1 2:45 – 4:20 PM ET Daily Q&A and Feedback 4:20 – 4:30 PM ET Adjourn 4:30 PM ET
Session I Day 3 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Continue Stage 1: MAP, Values, & Values Conflicts 11:15 – 12:00 PM ET Stage 1 Demo & Debrief 12:00 – 12:45 PM ET Lunch Break 12:45 – 1:15 PM ET Set up Triad Practice 1 1:15 – 1:45 PM ET Triad Practice 1 + Break 1:45 – 4:00 PM ET Triad Practice 1 Debrief 4:00 – 4:15 PM ET Daily Q&A and Feedback 4:15 – 4:30 PM ET Adjourn 4:30 PM ET
Session I Day 4 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Introduction to Stage 2 11:15 – 12:00 PM ET Stage 2 Demo & Debrief 12:00 – 12:45 PM ET Lunch Break 12:45 – 1:15 PM ET Set up Triad Practice 2 1:15 – 1:30 PM ET Triad Practice 2 + Break 1:30 – 3:40 PM ET Triad Practice 2 Debrief 3:40 – 3:55 PM ET
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
4|VHA/OfficeofPatientCenteredCareandCulturalTransformation
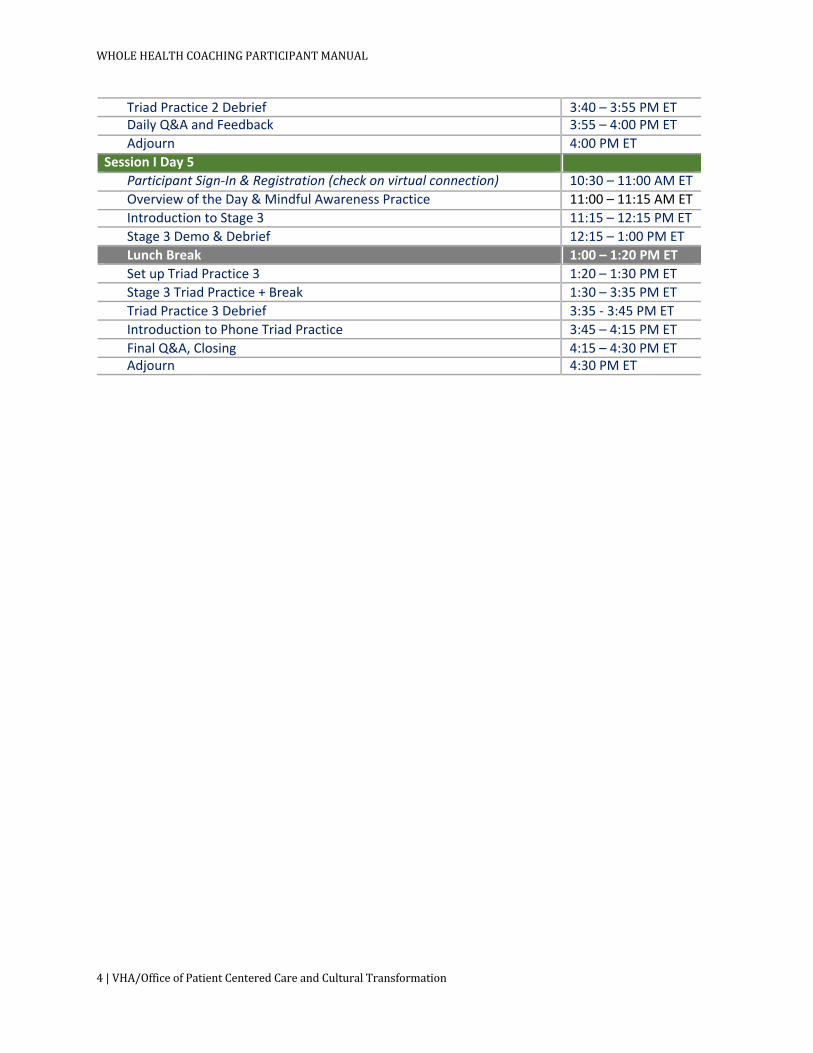
Triad Practice 2 Debrief 3:40 – 3:55 PM ET
Daily Q&A and Feedback 3:55 – 4:00 PM ET
Adjourn 4:00 PM ET
Session I Day 5
Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET
Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET
Introduction to Stage 3 11:15 – 12:15 PM ET
Stage 3 Demo & Debrief 12:15 – 1:00 PM ET
Lunch Break 1:00 – 1:20 PM ET Set up Triad Practice 3 1:20 – 1:30 PM ET Stage 3 Triad Practice + Break 1:30 – 3:35 PM ET
Triad Practice 3 Debrief 3:35 - 3:45 PM ET
Introduction to Phone Triad Practice 3:45 – 4:15 PM ET
Final Q&A, Closing 4:15 – 4:30 PM ET
Adjourn 4:30 PM ET

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|5
SESSION II Session II Day 1
Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Welcome Back, Ice Breaker & Mindful Awareness Practice 11:00 – 11:45 AM ET Review of Between Session Practice, Skills, & Process 11:45 – 12:05 PM ET Introduction to Stage 4 12:05 – 12:35 PM ET Stage 4 Demo & Debrief 12:35 – 1:05 PM ET Lunch Break 1:05 – 1:35 PM ET Set up Triad Practice 4 1:35 – 1:45 PM ET Triad Practice 4 + Break 1:45 – 3:50 PM ET Triad Practice 4 Debrief 3:50 – 3:55 PM ET Daily Q&A and Feedback 3:55 – 4:00 PM ET Adjourn 4:00 PM ET
Session II Day 2 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Introduction to Barriers Strategies: Brainstorming & Values Conflicts 11:15 – 1:15 PM ET Lunch Break 1:15 – 1:45 PM ET Barriers Strategies Continued: EPE & Limiting Beliefs 1:45 – 3:45 PM ET Daily Q&A and Feedback 3:45 – 4:00 PM ET Adjourn 4:00 PM ET
Session II Day 3 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Review of Barriers Strategies 11:15 – 11:35 AM ET Set up Triad Practice 5 11:35 – 11:55 AM ET Triad Practice 5 + Lunch Break 11:55 – 2:25 PM ET Triad Practice 5 Debrief 2:25 – 2:40 PM ET Revisit Course Requirements, NBHWC Certification 2:40 – 2:55 PM ET Break 2:55 – 3:05 PM ET How & When to Refer & Suicide Prevention 3:05 – 3:50 PM ET Daily Q&A and Feedback 3:50 – 4:00 PM ET Adjourn 4:00 PM ET
Session II Day 4 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Introduction to Group Coaching 11:15 – 12:00 PM ET Group Coaching Demo & Debrief 12:00 – 12:35 PM ET Lunch Break 12:35 – 1:05 PM ET Group Coaching Practice 1 1:05 – 3:35 PM ET Group Practice 1 Debrief 3:35 – 3:50 PM ET Daily Q&A and Feedback 3:50 – 4:00 PM ET Adjourn 4:00 PM ET
Session II Day 5 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
6|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET
Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET
Coaching Within Your VHA Role 11:15 – 1:15 PM ET
Lunch Break 1:15 – 1:45 PM ET Group Coaching Practice 2 1:45 – 3:45 PM ET Group Practice 2 Debrief 3:45 – 3:55 PM ET
Final Q&A, Closing 3:55 – 4:00 PM ET
Adjourn 4:00 PM ET

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|7
SESSION III Session III Day 1
Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Welcome Back & Overview of Session III 11:00 – 11:30 AM ET Review Course Requirements, WHC Process Model, Coaching Skills 11:30 – 12:00 PM ET Coaching Presence & Mindful Awareness 12:00 – 1:00 PM ET Lunch Break 1:00 – 1:30 PM ET Advanced Skills: Interrupt/Redirect, Metaphor, Decisional Balance 1:30 – 2:55 PM ET Advanced Skills: Exploring Perspectives 2:55 – 3:50 PM ET Daily Q&A and Feedback 3:50 – 4:00 PM ET Adjourn 4:00 PM ET
Session III Day 2 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Coaching Structure Session 1 – Initial Session 11:15 – 12:00 PM ET Lunch Break 12:00 – 12:30 PM ET Triad Practice #1 – Initial Session + Break 12:30 – 3:45 PM ET Triad Practice 1 Debrief 3:45 – 3:55 PM ET Daily Q&A and Feedback 3:55 – 4:00 PM ET Adjourn 4:00 PM ET
Session III Day 3 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Coaching Structure Session 2 – Routine Ongoing Session 11:15 – 12:00 PM ET Lunch Break 12:00 – 12:30 PM ET Triad Practice 2 – Ongoing Session + Break 12:30 – 3:30 PM ET Triad Practice 2 Debrief 3:30 – 3:35 PM ET Coaching Structure: Final Session 3:35 – 3:55 PM ET Daily Q&A and Feedback 3:55 – 4:00 PM ET Adjourn 4:00 PM ET
Session III Day 4 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Coaching Theories 11:15 – 12:15 PM ET Lunch Break 12:15 – 12:45 PM ET How to Coach Around Stages of Change 12:45 – 1:55 PM ET Ethics & Scope of Practice 1:55 – 3:40 PM ET Certification Exam Prep 3:40 – 3:55 PM ET Daily Q&A and Feedback 3:55 – 4:00 PM ET Adjourn 4:00 PM ET
Session III Day 5 Participant Sign-In & Registration (check on virtual connection) 10:30 – 11:00 AM ET Overview of the Day & Mindful Awareness Practice 11:00 – 11:15 AM ET Group Coaching – Group Design, Structure, Demo & Debrief 11:15 – 12:15 PM ET Lunch Break 12:15 – 12:45 PM ET

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
8|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Lunch Break 12:15 – 12:45 PM ET Group Coaching Practice 12:45 – 2:55 PM Group Practice Debrief 2:55 – 3:00 PM ET Asynchronous Logistics, Phone Triad Setup 3:00 – 3:45 PM ET Final Q&A, Closing 3:45 – 4:00 PM ET Adjourn 4:00 PM ET

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|9
TableofContents
SESSIONI&IICONTENT..................................................................................................................12
WELCOME.................................................................................................................................................................13INTRODUCTION.....................................................................................................................................................15FUTUREOFHEALTHCOACHINGINTHEVHA...........................................................................................17HEALTHCOACHCERTIFICATION...................................................................................................................18CHAPTER1:PRINCIPLESOFHEALTHCOACHING....................................................................20COACHESARENOTTHEONLYEXPERTSINTHEROOM......................................................................20THREEHELPINGSTYLES....................................................................................................................................21SPECIFICVHAHEALTHCOACHINGPRINCIPLES.....................................................................................24CHAPTER2:QUALITIESOFAWHOLEHEALTHCOACH..........................................................26THEDESIREDQUALITIESOFAWHOLEHEALTHCOACH....................................................................26MINDFULAWARENESS.......................................................................................................................................28CHAPTER3:ACTIVECOMMUNICATIONSKILLSFORCOACHING.........................................32LISTENING................................................................................................................................................................32SIMPLE&COMPLEXREFLECTIONS...............................................................................................................32INQUIRY.....................................................................................................................................................................37DIRECTCOMMUNICATION................................................................................................................................39CHAPTER4:THEHEALTHCOACHINGPROCESS.......................................................................40HOWTOUSETHEHCPM.....................................................................................................................................41STAGESANDPHASESOFTHEHCPM.............................................................................................................43WHENUTILIZINGTHEFULLCOACHINGPROCESSISNOTFEASIBLEORPOSSIBLE...............59CHAPTER5:ENHANCINGYOURWHOLEHEALTHCOACHINGSKILLS...............................61UTLIZINGAPEERSUPPORTGROUP..............................................................................................................62SUGGESTIONSFORCREATINGAHEALTHCOACHINGENHANCEMENTPROGRAM................63ESTABLISHINGAHEALTHCOACHINGSUPPORTNETWORKATYOURLOCALSITE...............63WHOLEHEALTHCOACHINGTRAININGIMPLEMENTATIONASSESSMENT...............................64CHAPTERSIX:GROUPCOACHING.................................................................................................67OPPORTUNITIESWITHGROUPCOACHING...............................................................................................67SETTINGUPAGROUP–SOMECONSIDERATIONS..................................................................................69DEALINGWITHDIFFICULTGROUPBEHAVIORORGROUPPROCESSES.......................................74CHAPTER7:PRE-SESSION,FIRSTSESSION,ANDLASTSESSIONCONSIDERATIONS..............................................................................................................................76PRE-SESSION...........................................................................................................................................................76FIRSTSESSION........................................................................................................................................................77LASTSESSION.........................................................................................................................................................77
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
10|VHA/OfficeofPatientCenteredCareandCulturalTransformation
SESSIONIIICONTENT.......................................................................................................................78
CHAPTER8:MINDFULAWARENESSANDCOACHINGPRESENCE........................................79HOWMINDFULAWARENESSSUPPORTSTHECOACHINGPROCESS.............................................79STEPSFORGUIDINGAMINDFULMOMENT...............................................................................................81MINDFULAWARENESSVS.MINDFULNESS–VHARESOURCES.......................................................81MINDFULAWARENESSSCRIPTS....................................................................................................................82CHAPTER9:ADVANCEDCOACHINGSKILLS...............................................................................90METAPHOR..............................................................................................................................................................90INTERRUPT&REDIRECT...................................................................................................................................91DECISIONALBALANCE........................................................................................................................................94PERSPECTIVES.......................................................................................................................................................96CHAPTER10:COACHINGSTRUCTURE......................................................................................100COACHANDVETERANRESPONSIBILITIES/EXPECTATIONS.........................................................108CHAPTER11:OUTCOMEVS.BEHAVIORALGOALS................................................................110CHAPTER12:COACHINGTHEORIES..........................................................................................112TRANSTHEORETICALMODEL:SIXSTAGESOFCHANGE..................................................................112TRAVISILLNESS-WELLNESSCONTINUUM.............................................................................................114SELF-DETERMINATIONTHEORY................................................................................................................115SOCIALCOGNITIVETHEORY.........................................................................................................................115GROWTHMINDSET...........................................................................................................................................116CHAPTER13:THETRANSTHEORETICALMODEL–COACHINGAROUNDSTAGESOFCHANGE.........................................................................................................................117PRECONTEMPLATION......................................................................................................................................117CONTEMPLATION..............................................................................................................................................118PREPARATION.....................................................................................................................................................119ACTION....................................................................................................................................................................120MAINTENANCE....................................................................................................................................................121TERMINATION/ADOPTION(RELAPSE/RECYCLE).............................................................................122CHAPTER14:THEETHICSOFCOACHING.................................................................................124FACTORSCONTRIBUTINGTOCHOOSINGETHICALACTION..........................................................124AREASOFCOACHINGREQUIRINGETHICALCONSIDERATION.....................................................127COMMONETHICALBLINDSPOTS...............................................................................................................129APPROACHINGETHICS:KEYPOINTS........................................................................................................130SOURCESFORINFORMATIONINTHISCHAPTER................................................................................130CHAPTER15:GROUPCOACHINGCONTINUED........................................................................131ESSENTIALELEMENTSOFGROUPCOACHING......................................................................................131BEGINNINGTHEGROUP–INITIALSESSION..........................................................................................134
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|11
ROUTINE-ONGOINGGROUPSESSIONSTRUCTURE............................................................................135THEFINALSESSION..........................................................................................................................................136CHAPTER16:EXAMINATIONPREPARATION.........................................................................138WHYPURSUECERTIFICATION?...................................................................................................................138EXAMPREP............................................................................................................................................................139RESOURCES&REFERENCES..........................................................................................................143WHOLEHEALTHWEBSITE............................................................................................................................143COMMUNITYOFPRACTICECALLS.............................................................................................................144OTHERVARESOURCES....................................................................................................................................144SUGGESTEDWEBSITES....................................................................................................................................145SUGGESTEDREADINGMATERIALS............................................................................................................145

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
12|VHA/OfficeofPatientCenteredCareandCulturalTransformation
SESSIONI&IICONTENT
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|13
WELCOME
WelcometotheWholeHealthCoachingProgram,anApprovedHealthandWellnessCoachTrainingandEducationProgrambytheNationalBoardforHealthandWellnessCoaching(NBHWC).
VeteransHealthAdministration(VHA)establishedtheOfficeofPatientCenteredCareandCulturalTransformation(OPCC&CT)in2011toleadoneofthemostmassivechangesinthephilosophyandprocessforhealthcaredeliveryeverundertakenbyanorganizedhealthcaresystem.TheUndersecretaryforHealthdescribestheidealsystemasoneinwhich“patientsareincontroloftheirhealthcare,andthesystemisdesignedaroundtheneedsofthepatient.”Toaccomplishthisrequiresaparadigmshiftfromproblem-baseddiseasecaretoWholeHealthCare,basedonthewholeperson.
VHAdefinesWholeHealthaspatient-centeredcarethataffirmstheimportanceofapartnershipbetweentheclinicianandpatient.Thefocusisonthewholepersonwhileco-creatingapersonalized,proactive,andpatient-drivenexperience.Thisapproachisinformedbyevidence,andmakesuseofallappropriatetherapeuticapproaches,healthcareprofessionals,anddisciplinestoachieveoptimalhealthandwell-being.
ThehealthcareteambeginswiththeVeteranasanindividualandwhatmatterstotheVeteranintheirlife.TheteamutilizesinformationfromthePersonalHealthInventory,atoolthathelpsVeteransexploretheirvisionoflivinglifefully,theirvalues,andtheirpriorities.APersonalHealthPlaniscreatedbydrawingonthePersonalHealthInventoryandriskassessmenttools,establishingsharedpatientandclinicalgoals,employingevidence-basedtraditionalandnon-traditionalinterventionsandtreatments,andleveragingsupportsystemswithinandoutsideofVHA.Corecompetenciesinteam-basedinter-professionalcollaborationarecritical.
Additionally,newprocessesandnewrolesareneeded,notonlyforthehealthcareteambutfortheVeteran.Thisincludesbuildingskillsandconnectingwithsupportandresourcesforsustainablebehaviorandlifestylechangeandimprovedhealthoutcomes.
Keycomponentsofthisapproachtohealthcareincludethefollowing:
• Personalvisionandmissionforlifeandhealth.• Personalizedhealthplanning.• Integrativemedicineandself-careskillbuildingandknowledgeacquisition.• Lifestyleandbehaviorchangestrategies.• Supporttosucceedwithandfromsignificantothers,healthcareteammembers,and
thecommunity.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
14|VHA/OfficeofPatientCenteredCareandCulturalTransformation
TheWholeHealthCoachingProgramisa15-dayintensivetrainingincommunicationandcoachingskillsdividedintothree,five-day,virtualsessions,withstudyandpracticesessionsrequiredbetweenSessions1and2,andafterthecompletionofthethirdsessionoftraining.
WholeHealthCoachingteachesandtrainsindustrybestpracticesforintegratedhealthcoaching,strategies,andmethods.ItisaprofessionaltrainingprogramthatistailoredtotheVeteranpopulation.WholeHealthCoachingcorecompetenciesincludeunderstandingtheroleofthehealthcoach,coachinginvarioussettings(face-to-face,individual,groups,telecommunicationvenues,etc.),establishingtrustingrelationshipsandeffectivecommunication,creatingawareness,designingactions,planning,settinggoals,managingprogressandaccountability,coachingstructure(initialandroutineongoingsessions),documentmanagement,andinterfacingwiththeclinicalteam.
Itisoursincerehopethatyourexperienceinthistrainingnotonlyenhancestheskillsandcorecompetenciesyoualreadypossess,butalsoprovidesyouwithapersonalizedexperiencethatwillenrichyourlife.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|15
INTRODUCTION
ThismanualisdesignedtosupplementthehealthcoachtrainingdevelopedanddeliveredforVeteransHealthAdministration(VHA)employees,muchlikeatextbook.Itcontainsdescriptionsofthekeytrainingconcepts,skillsandstrategiesthatareofferedinvirtualtrainingandreferencesandresourcesforadditionalinformation.Themanualcontainsthesameinformationasdeliveredinthevirtualtrainingbutisorganizedbytopicsanddoesnotalwayscoverthematerialinthesameorderaspresentedinthetraining.
Throughoutthemanual,thetermVeteranorcoachingpartnerisused,usuallyastherecipientofcoaching.Inothervenues,thetermpartner,client,orpatientmightbeused.TheuseofVeteraninthismanualisnotintendedtobeinclusiveofonlyVeterans,norisitintendedtoexcludeanyoneelse,suchasReservists,ActiveDuty,orfamilymembers.Tobelesscumbersome,thetermVeteranorpartnerisusedtoaddresseveryonereceivingcoaching.Similarly,thetermsWholeHealthCoach,healthcoach,orcoachareinterchangeableandusedthroughoutthisdocument.AllrefertothoseprovidingcoachingtotheVeterans.
WHYHEALTHCOACHTRAINING?
“TheVHAVisionPlanwasreleasedinDecember2020.TheplanestablisheskeystrategiesandconceptscentraltoVA’stransformationintoaHigh-PerformingIntegratedDeliveryNetwork(HPIDN).ItalignstoVA’sconcurrentstrategicplanninginitiatives,suchastheVAStrategic
Plan,VHALong-RangePlan,andVHAModernizationPlan,preparingthewayforimplementationofdiscrete,data-drivenactionplans.ThismarksthenextstepinVA’stransformation,demonstratingtheorganization’scommitmenttosafetyandVeteran
experience.ThisnetworkwillhelpVAattainandsustainapositionasthemostconvenientandaccessiblehealthcaresysteminhistory.”
BenjaminKigler,MD,MPHExecutiveDirectorOPCC&CT
HealthCoachingisanimportantlinktohelpingtheVHAachievetheirStrategicGoalsandObjectivesfor2013-2021.TheseGoalsareto:
1. ProvideVeteranspersonalized,proactive,patient-drivenhealthcare(andsupporttosuccessfullyimplementtheirpersonalhealthplans).
2. Incentivizemeasurableimprovementinhealthoutcomes.3. AlignresourcestodeliversustainedvaluetoVeterans.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
16|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Onfurtherexamination,itcouldbesaidthatthesecondandthirdgoalsarereallyinsupportofthefirstgoal.Giventhis,healthcoachingisbeingdisseminatedandtrainedwithintheVHAto“provideVeteranspersonalized,proactive,patient-drivenhealthcare.”
Furthermore,whenconsideringthedefinitionoftheabovetermsinGoal1,itbecomesclearerhowhealthcoachingsupportsthatgoal.Thedefinitionsofthesetermsare:
PERSONALIZED
Adynamicadaptationorcustomizationofrecommendededucation,preventionandtreatmentthatisspecificallyrelevanttotheindividualuser,basedontheuser’shistory,clinicalpresentation,lifestyle,behavior,andpreferences.
CoachesassisttheVeteranindevelopingaplanthatisbasedonwhatmattersmosttotheVeteran;theplanisbasedontheVeteran’svalues,preferences,andlifestyle.
PROACTIVE
Actinginadvanceofalikelyfuturesituation,ratherthanjustreacting;takinginitiativetomakethingshappenratherthanjustadjustingtoasituationorwaitingforsomethingtohappen.
CoachesassisttheVeteranintakingactionthatispresentandfutureoriented.TheyassisttheVeteraninengaginginlife/healthenhancingendeavorsthatarenotjustreactivebutproactiveintakingresponsibilityforwhattheVeteranwants.
PATIENT-DRIVEN
Anengagementbetweenapatientandahealthcaresystemwherethepatientisthesourceofcontrolsuchthattheirhealthcareisbasedintheirneeds,values,andhowthepatientwantstolive.
CoachesrecognizetheVeteranasthesourceofcontrolforhowtheywanttolive,andinwhatchangestheywanttoengageandwhen.CoachespartnerwiththeVeteranstosupporttheminachievingtheVeteran’sgoals,needsandbehaviorsthatsupporttheirvalues.
HEALTH
Astateofcompletephysical,mental,andsocialwell-being,andnotmerelytheabsenceofdiseaseorinfirmity.(WorldHealthOrganization)
CoachesrecognizethathealthismuchbroaderthantheabsenceofdiseaseandthathealthisimpactedbymanyfacetsofaVeteran’slife,andthathealingcanexistdespitethepresenceofdisease.CoachesseektosupporttheVeteraninachievingoptimalhealth,by
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|17
theVeteran’sstandardthattakesintoaccountthemental,physical,andsocialwell-beingoftheVeteran.
PERSONALHEALTHPLAN
Auniquelypersonalizedplanforhealththatisbuiltuponeachpatient’svalues,conditions,needsandcircumstanceswhichusesthemostappropriateinterventionsandstrategies.Itaddressestheskillsandsupportneededtohelpengagedpatientsmanagetheirdisease,inordertoregainandmaintainoptimalhealthandwellbeingandmanagechronicdiseaseanddisabilitytothegreatestextentpossible.
CoachesassisttheVeteraninplanningfortheirhealth,notsimplyreactingtothemostcurrenthealthconcern.Again,thePersonalHealthPlanisdesignedbytheVeteranwiththesupportoftheCoaches.
FUTUREOFHEALTHCOACHINGINTHEVHA
TheOfficeofPatientCenteredCare&CulturalTransformation(OPCC&CT)recognizesthatWholeHealthCoaching(WHC)buildsonexistingcoachtrainingintheDepartmentofVeteransAffairs(VA)andcontinuestoevolvetobefullyintegratedwiththeotherprograms.Sinceitsinitialcourseofferingin2013,WHChasbecomeasignificantcomponentoftheWholeHealthSystem–itisacoreserviceofboththePathwayandWell-beingProgramsandagrowingcomponentofClinicalCare.AnationallyclassifiedPositionDescriptionwasdevelopedandadoptedin2015.Atthestartof2020,nearly2,300VAWholeHealthCoachesworkwithVeteransnationwidetohelpthemsetgoalsbasedontheirhealthprioritiesandpersonalhealthplans.Coachesalsooffersupport,encouragement,andattentiontohelpVeteransstayontracktomeettheirhealthandwell-beinggoals.
VAhasachievedamilestoneinhealthcaretrackingadvancingthefutureofhealthcoachingasatreatment.In2019,VAsuccessfullyappliedtotheAmericanMedicalAssociation(AMA)tocreatenewCategoryIIICurrentProceduralTerminology(CPT®)trackingcodesforHealthandWell-beingCoaching.Toaccomplishthis,VAteamedwiththeNationalBoardforHealthandWellnessCoaching(NBHWC),thenon-profitorganizationthatcreatedthenationalstandardsforhealthCoaches.VAanticipatesuseofthecodeswillincreaserecognitionofHealthCoachingasavaluableservice,makeitsusagemorecommonthroughouthealthcareandsupportitsbenefitasaserviceinthefuture.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
18|VHA/OfficeofPatientCenteredCareandCulturalTransformation
HEALTHCOACHCERTIFICATION
ThroughtheeffortsoftheNationalBoardforHealth&WellnessCoaching(NBHWC),formerlyInternationalConsortiumforHealthandWellnessCoaching(ICHWC),anationalcertificationprocessisnowinplace.
In2016,theVHAwasapprovedasaTransitionallyAccreditedHealthCoachingProgrambyNBHWC.Tomeetthisrequirement,PracticalSkillsEvaluations(PSA)wereaddedtothementoringprocess.Allcourseparticipantswhometthetransitionalprogramrequirementsofattendingallsessionsofthetrainingandparticipatinginallthreebetweensessiontriadpractices,andwhoreceivedaCertificateofCompletionfollowingthecoursewereeligibletoapplyforthenationalexam.
TheWholeHealthCoaching(WHC)programexpandeditscurriculumtoadheretonationalcredentialingstandards,establishedbyNBHWC.Inadditiontotheexisting2-weekFoundationscourse,OPCC&CToffereda3rdCertification-focusedweek.ParticipantsregisteringfortheWHCCertificationcoursemusthavecompletedtheFoundationscoursetobeeligible.TheSession3CertificationcoursewaspilotedinFY20.
InMarch2020,OPCC&CTappliedtoNBHWCforpermanentphaseprogramapproval.Followinganonlineinterviewandreviewprocess,OPCC&CTreceivednoticeinApril2020thattheVHAWholeHealthCoachingProgramwasapprovedbyNBHWCfortheeducationandtrainingofhealthandwellnesscoaches.InFY21,theseparate2-weekFoundations,and1-weekCertificationofferingwerecombinedtoofferone3-weekcomprehensiveWholeHealthCoachingProgram.
AsanoverviewofWHCprogramofferedinFY21,thefirsttwoweeksofthe3-weekprogramcontinuetoofferacomprehensivecurriculumoffoundationalandessentialcoachingskillsandstrategiesthatbothdedicatedhealthcoachesandVAemployeesmayuseandapplytotheirrespectivejobrolesthroughouttheVHA.RecentadditionstoitsexistingcontenttothefirsttwoweeksinFY20include:
• ExperientialpracticesforbarriersoftenencounteredbyVeterans.• Enhancedinstructionaroundgroupcoaching.• Moretimeforpersonalizedfacultymentorfeedback.
Session3ofthevirtual3-weekWHCtrainingfocusesonadvancedskillsandtheintroductionandpracticeofcoachingstructure(initialandroutineongoingsessions)relevanttodedicatedWholeHealthCoaches.Week3curriculumhighlightsinclude:

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|19
• CoachingSessionStructure(coachingagreements,howtoconductaninitialsession,routineongoingsessions,closingsessions).
• HowtouseMindfulAwarenesstohelpsupportcoachingpresenceandthecoachingrelationship.
• Advancedcoachingskillsandstrategies(includinginterrupt/redirect,perspectives,coachingaroundstagesofchange).
• Coachingethics.• Groupcoachingtips&techniques,includinghandlingchallenginggroupdynamics.
NBHWCCERTIFICATIONEXAMINATION
ToearntheNationalBoardCertification,healthandwellnesscoachesmustmeettheeligibilityrequirementsofthe3-weekWholeHealthCoachingProgram,receiveaCertificateofCompletion,andpasstheNationalBoardCertificationExamination.TheexaminationisbasedupontheNBHWCJobTaskAnalysis/ContentOutline.ThewrittenexaminationisadministeredthroughouttheUnitedStatesandinseveralinternationallocations.
NATIONALCERTIFICATIONREQUIREMENTSANDELIGIBILITY
Itisvitalthatany/allWHCparticipantswishingtoseeknationalboardcertificationtakeadvantageoftheNBHWCwebsiteinseekingoutinformationpertainingtotheeligibilityrequirements,documentationprocess,andanyotherNBHWC-relatedinformationorquestions.WHCfacultystronglyrecommendallcertificationseekingcoachesusethisasthePRIMARYsourceofinformationforallthingscertificationrelated.TherehavebeenanumberofchangesoverthepastseveralyearsregardingthecertificationrequirementsandtheNBWHCwebsiteisthebestpossiblelocationtokeepupdatedandaware.AnyquestionsregardingthenationalcertificationprocessarealsobestansweredbytheveryresponsiveNBHWCfaculty.
RequirementsforcredentialingcanbefoundonlineattheNBHWCwebsite:https://nbhwc.org.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
20|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER1:PRINCIPLESOFHEALTHCOACHING
ThischapterisdevotedtothehealthcoachingprinciplesthathavebeendeemedsignificantforVHAstafftopossessinmovingforwardwithhealthcoachtraining.Thisisnotnecessarilyacompletelist,asotherprogramsmayincludeadditionalideologies;however,theseprovideasolidfoundation.
COACHESARENOTTHEONLYEXPERTSINTHEROOM
Coachesaretrainedtoelicitthe“expertise”fromtheVeterans.ThisprincipleassumesthattheVeteranisthebestpersontodecidewhatisintheirbestinterest,bothintermsoftheagendaforthecoachingsessionsaswellasthetimingandstrategiesofgettingtotheVeteran’sgoalsandactions.TheVeteranmaydecidethattheyneedfurtherinformationoreducation,andthecoachcanassisttheVeteraningettingtheinformationtheyneed.Thecoach’sexpertiseliesinguidingthechangeprocess.Inaddition,coachesmayhaveexpertiseinagivencontentarea.InthewholehealthcoachingtrainingofferedbytheVHA,coacheswillbeprovidedaformatforsharingtheirexpertise,ifappropriate.Thisprocessiscalled,“Elicit,Provide,Elicit.”
THEAGENDAISTHEVETERAN’S
CoachesoperateontheprinciplethattheagendaforthetrainingsessionscomesfromtheVeteran.Althoughthishasbeenstatedabove,itwarrantsaseparateprinciple.CoachesmayhavemanyopinionsaboutwhattheVeteranshouldidentifyastheagendaforcoaching.Coachesmayhaveopinionsaboutwhere,when,andhowmuchefforttheVeteranshouldbeexpendinginacertaincontentarea.However,thisisnotuptothecoachestodecide.TheremaybepressurefromthemedicalteamorotherprovidersastowhatshouldbethefocusoftheVeteran’scoachingsessions.Coachesneedtoartfullyaddressthesepressures.Intheend,itistheVeteranwhowilldecidetheagendaandcourseofaction,orresistancewillbeencounteredandtheeffortto“change”theVeteranwillbethwarted.
HEALTHCOACHINGISPRIMARILYPRESENTANDFUTURE-FOCUSED
TheemphasisinhealthcoachingismovingfromwheretheVeterancurrentlyistowheretheywanttobe.Thisisapresentandfutureorientation.Generallyspeaking,thereislittleemphasisonexploringpasthistoryorpasteventsasameanstounderstandingtheVeteran’scurrentsituation.Attimes,coacheswillwanttoexplorepastsuccessesorbarrierstochangebutwillmoveveryquicklytotheimplicationsforthepresent.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|21
EMPHASISISONHEALTHENHANCEMENT,STRENGTHS,ANDASPIRATIONS
HealthcoachingplacesmoreemphasisonenhancingtheVeteran’swellnessandwholehealthaccordingtotheirvalues,interests,andaspirations,ratherthanfocusingondeficits,deficiencies,ordisorders.TheyalsoseektodrawontheVeteran’sstrengthsratherthanattemptingtoshoreupdeficiencies,unlessthatisthedirectiontheVeteranwantstogoaspartofmovingforward.
THREEHELPINGSTYLES
HEALTHCOACHINGUSESAGUIDINGSTYLE,RATHERTHANDIRECTINGORFOLLOWINGSTYLE
Nurses,physicians,healthcareproviders,nutritionists,psychologists,andcounselorsoftenencourageVeteranstodohealthpromotingbehaviors(i.e.,takeyourprescriptionasprescribed,exercise,stopsmoking,decreasesubstanceuse,makeappointmentsforcare,followadiet).
Mosttimesthisencouragementtakestheformofadirectinghelpingstyleincludingadvice.Veteransmayrespondsilentlyorexplicitlytothiswell-intendedandaccurateadvicewith“Yes,but...”describingreasonsnottochange.
• AdirectinghelpingstyleisverytemptingifthehealthcareproviderassumestheVeterandoesnotknowwhattheyneedtoknowordoesnotcaresufficientlyaboutthehealthrisks.
• Aguidinghelpingstylemightincludemoreofthepatient’sexperienceandyetstillmovetowardahealthgoal.
• Afollowinghelpingstylesimplyfollowswhateverthepartnerchoosestobringup.
WholeHealthCoachingcanbeconsideredaspecializedversionofaguidinghelpingstylethathelpsVeteransaccesstheirownreasonsanddesirestodothehealthpromotingbehavior.
Thefollowingdiagramsservetoillustratethedifferencesbetweenadirectingstyleandaguidingstyleintermsofwhoisdoingthespeaking,aswellashowmuchlisteningasopposedtoinformingisdoneinthesessions.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
22|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Adirectinghelpingstyleisprobablythemostcommonapproachusedinhealthcare.Ifyouwanttoexperimentwithusingacoachingstyle:
Insteadofdoingthis: Trythisandseeifyouliketheresults:
Explainingwhyhe/sheshoulddothehealthpromotingbehavior.
ListenwiththegoalofunderstandingtheVeteran’sdilemmaofdoingthehealthpromotingbehavior.
TeachingtheVeteran,tellingtheVeteranwhattodo,orgivinghim/heradvice.
AskwhattheVeteranknows,providesomeadditionalinformation,andthenaskhowthatfitswithhis/herlife.
Describingspecificbenefitsthatwouldresultfromdoingthehealthpromotingbehavior.
Ask,“Whatmightbethebenefitofdoingthishealthpromotingbehavior?”
Tellinghim/herhowtodothehealthpromotingbehavior.
Ask,“Whatareyoualreadydoingthatwouldmakeitpossibleforyoutodothishealthpromotingbehavior?Howmightyoudothishealthpromotingbehaviorsoitfitsinyourlife?”
EmphasizinghowimportantitisfortheVeterantodothehealthpromotingbehavior.
Ask,“Whatmightbeimportanttoyoutothinkaboutordothishealthpromotingbehavior?
TellingorinspiringtheVeterantodothehealthpromotingbehavior.
Ask,“Whatisimportanttoyouaboutenhancingyourhealth?
OTHERMODELSTHATSHAREPRINCIPLESINCOMMONWITHWHOLEHEALTHCOACHING
Thereareotherinterventionmodelsthatshareprinciplesincommonwithhealthcoaching.Threeexamplesofsuchare:
1. MotivationalInterviewing(MI)2. AppreciativeInquiry(AI)3. PositivePsychology

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|23
MOTIVATIONALINTERVIEWING
TheSpiritofMI,asidentifiedbelow,canalsobefullyappliedtohealthcoaching.(Miller,W.R.andRollnick,S.{2012}.MotivationalInterviewing:HelpingPeopleChange{3rdEd.}.NewYork:Guilford.)ThesefourSpiritsofMIandcoachingare:
1. Collaboration=comingalongside,joiningup,orlookingattheVeteran’slifeorsituationwiththeVeteran;partneringwiththeVeterantoconsideradifficultsituation.
2. AcceptingtheVeteran=empathizingwithandrecognizingthatitistheVeteranwhohastodothehealthpromotingbehavior;supportingthattheVeterancandecidetochangenow,orlater,ornotatall,believingtheVeteraniscapable,competent,andexpertintheirownlife.
3. Curiosity=helpingtheVeteransayoutloudhis/herdesireandreasonsfordoingthehealthpromotingbehavior;acting“asif”youdon’tknowinordertohelpyourselfsolicitandlearnwhattheVeteranknows.
4. Compassion=dedicationtotheVeteran’swelfareandwell-being.
APPRECIATIVEINQUIRY
AppreciativeInquiryisdesignedforenhancingorganizationaldevelopment.However,theprinciplescanbeappliedtoindividualenhancementsaswell.ThefollowingprinciplesarefromRichardSteele’sarticleonAppreciativeInquiry(IntroductiontoAI.(2008,January12).NewParadigmOrganizationConsulting.https://www.new-paradigm.co.uk/introduction_to_ai.ht)
• Discover=Theidentificationoforganizationalprocessesthatworkwell.• Dream=Theenvisioningofprocessesthatwouldworkwellinthefuture.• Design=Planningandprioritizingprocessesthatwouldworkwell.• Destiny(orDeploy)=Theimplementation(execution)oftheproposeddesign.
POSITIVEPSYCHOLOGY
PositivePsychologyisanewerbranchofPsychologythatfocusesonhumanthrivingratherthanmentalillness.ThefollowingquotesarefromthePositivePsychologywebsiteattheUniversityofPennsylvania(http://ppc.sas.upenn.edu/):
1. “PositivePsychologyisthescientificstudyofthestrengthsandvirtuesthatenableindividualsandcommunitiestothrive.Thefieldisfoundedonthebeliefthatpeoplewanttoleadmeaningfulandfulfillinglives,tocultivatewhatisbestwithinthemselves,andtoenhancetheirexperiencesoflove,work,andplay.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
24|VHA/OfficeofPatientCenteredCareandCulturalTransformation
2. “PositivePsychologyhasthreecentralconcerns:positiveemotions,positiveindividualtraits,andpositiveinstitutions.Understandingpositiveemotionsentailsthestudyofcontentmentwiththepast,happinessinthepresent,andhopeforthefuture.Understandingpositiveindividualtraitsinvolvesthestudyofstrengthsandvirtues,suchasthecapacityforloveandwork,courage,compassion,resilience,creativity,curiosity,integrity,self-knowledge,moderation,self-control,andwisdom.Understandingpositiveinstitutionsentailsthestudyofthestrengthsthatfosterbettercommunities,suchasjustice,responsibility,civility,parenting,nurturance,workethic,leadership,teamwork,purpose,andtolerance.”
LikeAI,itiseasytoseetheoverlapbetweentheprinciplesofhealthcoachingandtheprinciplesofPositivePsychology.Bothareconcernedwithidentifyingtheaspirationsofindividualsandassistingtheminworkingtowardthese—notfocusingonthenegativeandthepast,butthepositiveandthefuture.
SPECIFICVHAHEALTHCOACHINGPRINCIPLES
ThereareprinciplesthatmaybemorespecifictotheVHAsettingsincethishealthcoachtrainingisbeingofferedtosupportWholeHealth.Theseprinciplesincludethefollowingconcepts.
CULTURALSENSITIVITY&CULTURALCOMPETENCE
GiventhatallVeteranswhowillbecoachedonceservedinthemilitary;itbehoovescoachestobeasfamiliaraspossiblewiththemilitaryculture.TherearetrainingopportunitieswithintheVHAtogainfurthermilitaryculturalcompetency.Thathavingbeensaid,likeanyhelpingprofessional,itisimportanttoalsobeculturallysensitivetotheindividual(s)withwhomcoachesarecoaching.Thismeansbeingawareof,andsuspending,anyprejudgmentsaboutthepersonbeingcoached,includingsuchfactorsasrace,religion,appearances,communityassociationsandanyotherstatuses.
TEAMCARE:PACTS&PROVIDERS
Coacheswillmostfrequentlyworkwithothercareteamprovidersandmustbefullyawareoftheirfunctionwithintheteamapproach.CoachesmustlearntheroletheyprovideandhowtheycanbeofsupporttooverallteamcareoftheVeteran.
Insummary,thefollowingquotesmayhelptothinkabouttheprinciplesofhealthcoaching:

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|25
• “Peoplearegenerallybetterpersuadedbythereasonswhichtheyhavethemselvesdiscoveredthanbythosewhichhavecomeintothemindofothers.”(Pascal,Blaise,{1623-1662}.Pascal’sPensées.NewYork:E.P.Dutton,1958).
• “Youcan’ttugonacornstalktomakeitgrowfasterortaller,andyoushouldn’tyankamarigoldoutofthegroundtoseeifithasroots.Youcan,however,tillthesoil,pulloutweeds,addwaterduringdryspells,andensurethatyourplantshavethepropernutrients.”EtienneWenger(Wenger,E.&Snyder,W.{2000}Communitiesofpractice:Theorganizationalfrontier.HarvardBusinessReview,78{1},139-145.)
• “Thereishealingmorethantherearehealers.”AndrewWeil,MD.• “Peopledon'tcarehowmuchyouknowuntiltheyknowhowmuchyoucare.”John
Maxwell

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
26|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER2:QUALITIESOFAWHOLEHEALTHCOACH
AWholeHealthCoach(WHC)ideallydemonstratescertainqualitieswhilecoaching.Thesequalitiescanbedevelopedwithpractice.Inadditiontodemonstratingthequalitiesdescribedthatfollow,aWholeHealthCoachutilizeswholehealthcoachingCommunicationSkillsasdescribedinChapterThree;andbecomesfamiliarwithaWholeHealthCoachingProcessasdescribedinChapterFour.
THEDESIREDQUALITIESOFAWHOLEHEALTHCOACH
ALISTENER
PerhapsthisisthemostimportantqualityaWholeHealthCoachcandemonstrate.AneffectiveWHCsetsasidehis/herownagendastofullylistentotheother.Effectiveuseofcommunicationskillsandthecoachingprocesscanonlycomefromeffectivelistening.Effectivelisteningcanbefurtherdevelopedbypracticingmindfulawarenessasdescribedlaterinthischapter.ACoachisnota“teller,”norinclinedtogiveadviceorinstruct/educatetheother.AWHCisfirstandforemostalistenerthatallowstheinnerwisdomofthecoachingpartnertosurface.
RESPECTFUL
AWholeHealthCoachhonorstheuniqueagenda,resourcesand“innerwisdom”ofanother.AWHCmustself-managetokeepinchecktheirownvalues,thoughtsandbeliefsandsupportthevalues,thoughts,andbeliefsofthecoachingpartner.
FULLYPRESENT
BeingfullyavailablefortheotherisanimportantqualityofaneffectiveWHC.Acoachcannotlisteneffectively,norfullyunderstandthecoachingpartner,unlesstheyarefullypresent.Beingfullypresentcanbecultivatedbypracticingmindfulawareness,whichisheavilyemphasizedthroughouttheWHCtraining.Afurtherdescriptionofmindfulawarenessandsuggestionsforpracticeandcultivationareprovidedattheendofthischapter.
EMBODIESTHEATTITUDESOFMINDFULNESS
Inadditiontobeingfullypresent,aWHCcoachwillconsistentlypracticetheNineAttitudesofMindfulnessasarticulatedbyJonKabat-Zinn(Kabat-Zinn,J.{2004edition},Fullcatastropheliving:Howtocopewithstress,painandillnessusingmindfulnessmeditation,London:PiatkusPublishing).(Thiseditionincludesthepreviouslynoted“SevenAttitudes”

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|27
butnottheadditionalTwo,spokenofbyKabat-Zinninamorerecentvideobutnotinwritingasofthisdate).
• Beginner’sMind—Asacoach,beingcuriousandnotassumingthatyoualreadyknowsomething.Askingquestionsandbeingexcitedabouthowyourmindworks,askingquestionslike:Whoisseeing?Whoisthinking?
• Non-judging—Agentlestateofnon-judgment,beingkindtoyourself,andallowingwhatis.Tryingnottocompare,label,orfindfault.
• Patience—Letthingshappenastheyneedtoandintheirowntime.Lettinggooftheideathatyouhaveto“getsomewhere,dosomething,ormakesomethinghappen.”
• Non-striving-Mindfulawarenessisaboutbeing,notdoing,ifitfeelslikeyou’reworkingtoohardyouprobablyare.It’sawayofbeing,beingawaketowhatishappeninginyourliferatherthanwhatishappeninginyourmind.
• Acceptance-Seeingthingsastheyare.Itiswhatitis.Trytobewiththingsastheyare.Letgoofthestoriesthemindcreatesandacceptthepresentmomentforwhatitis.
• Lettinggo—Nothavingasetagendaforwhat“should”happen.Beingopentoallpossibilitiesandoutcomes.
• Trust—Asawarenessgrows,sodoestrustinone’semotionsandintuition;beyourselfineveryway.Havefaithinhowyoumovethroughtheworld.Trustyourselfandwhatyouknow.
• Gratitude–Theabilitytobringgratitudetothepresentmoment,nottakingthings,eventhesmallestofthings,forgranted.
• Generosity–Thepowerofgivingyourselfovertolife,tobringjoytoothers’lives.Givingyourtimeandattentiontolifeandothersenhancesinterconnectednessanddemonstratesthatyoucare.
APARTNER
AWholeHealthCoach“goesalongside,”orpartnerswith,theotherontheirjourney.Coachesarenotexperts,outinfrontleadingfromtheirownvalues,thoughts,andbeliefs.Theyprovideaguidingstyleintermsofleadingaprocess,buttheydonotattempttoinstilltheirvalues,thoughts,andbeliefs,butrather,drawthemfromthecoachingpartner.
ARTICULATE&SUCCINCT
AneffectiveWHCusesaclearandsuccinctcommunicationstyle.Theyuseasfewwordsaspossiblewheninteractingwiththecoachingpartner.InaWHCconversation,themajorityofthewordsshouldcomefromthecoachingpartner.Attimes,beingsuccinctisreferredtointhecourseasbottom-lining.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
28|VHA/OfficeofPatientCenteredCareandCulturalTransformation
WILLINGTOLEARN&BEOPEN
Insomecases,WholeHealthCoachtrainingcanruncountertohowhealthcareproviderswerepreviouslytrained.AneffectiveWHCiswillingandabletoassumeadifferentapproachtobeingwiththeother,thatmaydifferfromtheirprevioustraining.AneffectiveWHCiscognizantofwhentheyareusingacoaching,guidingstylevs.adirectingstyle.Inadditiontobeingopentoadifferentapproach,WHCoachesapproacheachencounter,andeachmomentoftheencounter,with“beginner’smind.”Inordertopracticebeginner’smind,coachesmustcomefromaplaceof“notknowing”andbeingvulnerableandopentothemoment.
EMPATHIC
WholeHealthCoachesseektofullyunderstandandbepresentwiththeexperienceofanother.Thisisattherootofbeingempathic.Attimes,empathyisthoughtofasaquality,“Icanrelate—I’vebeenthere,too.”However,thatapproachcanactuallyhinderacompleteunderstandingoftheother.Toassume“Icanrelate”becauseofasimilarexperiencemaynottakeintoaccounthowtheotherhasinterpretednormadesenseoftheirownexperience.Oftentimesacknowledgingtheemotionsandexperienceofanotherisenoughtoconveyempathywithphraseslike“Thatsoundsrough”or“Thatmusthavebeenapainfulexperience”.
INTERESTINHEALTHENHANCEMENT&EDUCATION
AlthoughWholeHealthCoachesarenotnecessarily“experts”inallareasofhealth,theyvaluehealthenhancementandeducationandseektobecomeasinformedaspossibleinallareasofhealth.Whenbecomingmoreeducated,WHCsholdtheirknowledgewithadegreeofhumility,knowingthatknowledgewithinthefieldcanchangewithfurtherresearchandgreaterawareness.Impartinginformationisnottheprimaryroleofawholehealthcoach.Attimes,havingmoreknowledgecanactuallyimpedeawillingnesstoassistthecoachingpartnerinassessingtheirownknowledgeorseekingoutinformationontheirown.
MINDFULAWARENESS
MindfulawarenessisakeypartoftheComponentsofProactiveHealthandWell-Being(alsoreferredtoastheCircleofHealth)andthefirstlevelaround‘ME’onthecircle.Itispayingattentiononpurposetowhatishappeninginthepresentmomentwithoutjudgment.Itistheintentiontopayattention.Mindfulawarenessisnoticing,awareness,andattention.Mindfulawarenessisnotguidedimagery,relaxation,normeditation.
Whatdoesmindfulawarenesshavetodowithourhealth?Ourbodiesandmindssendusmessagesallthetime,butoftenwe’renotlistening.Researchshowsthatpracticingmindful

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|29
awarenesscanlowerstressandhelpstress-relatedhealthproblems,aswellashelpusimproveourmood,mentalwell-being,andqualityoflife.
Mindfulawarenesshasseveraldistinguishingfeatures.Theseinclude:
• Beingawareinthemoment,withcompassiontowardselfandothers. • Noticingexternalstimuli(sights,sounds). • Bringingattentiontointernalsensations(breath,body)andourresponsestothem. • Bringingattentiontoourmentalphenomena. • Listeningtothepersonal,innerwisdomofourowninterconnectedself-carecircles.
Practicingmindfulawarenessinyourcoachingcomeswithsomeimportantconsiderations:
• Mindfulawarenessmaytriggerthoughts,emotions,andevenphysicaldiscomfortforsomecoachingpartners.Beawareofthementalhealth“warmhandoff”atyoursite.
• Coachingaclientwithrespiratorydifficulties/COPDmightmeanchoosingadifferenttypeofmindfulawarenesspracticeunrelatedtothebreathorbreathingexercise.
• Mindfulawarenessisnotrequiredineverycoachingsession. • Askingpermissiontopracticemindfulawarenessinacoachingsessionisimportant
inestablishingtrustandrapportandencouragingautonomyfortheclient.Checkinginwiththeclientonwhattheynoticedcanbeenlighteningforthecoachandtheclient.
TheOfficeofPatient-CenteredCareandCulturalTransformation(OPCC&CT)makesadistinctionbetweenmindfulawarenessandMindfulness.MindfulnessfacilitationandinstructionrequiresspecializedtrainingandisbeyondthescopeofWholeHealthCoachtraining.ForcoacheswhoareinterestedinfacilitatingMindfulness,thereareresourcesinternalandexternaltotheVAthatwouldbehelpfultoexplore.Inparticular,trainingintrauma-sensitiveMindfulnessisespeciallyimportant,sothatpractitionerscanbehelpfulwithoutcausingharmtotheVeteranswithwhomtheywork.
ItisnotanexpectationthatyoufacilitatemindfulnesswithyourVeterans.MindfulnessfacilitationisbeyondthescopeoftheWHCtraining.Coachesinterestedinpracticing,oroffering,amoreformalmindfulnesspracticecanaccessbothinternalVAandexternalresources.(VACALM,MBSR,etc.)

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
30|VHA/OfficeofPatientCenteredCareandCulturalTransformation
BASICINSTRUCTIONS:MINDFULAWARENESSOFTHEBREATH
• Settleinandfeelthesupportofthechairorfloor. • Ifyoulike,allowyoureyestoclose,orsetasoftgazesomewherearoundtheroom. • Rememberattitudesofnon-striving,non-judging,andpayingattention. • Thisisanopportunitytoletgoofbusinessorlife’sconcerns. • Nowpayattentiontoyourbreathwhereveryouexperienceit.Don’ttrytochangeit,
justpayattentiontoit.Feelthebreathascompletelyaspossible,theinhaling,pausing,andexhalingofthebreath.Itmaybeeasiertofocusonyourabdomenastheexperienceofbreathing.
• Whenyounoticeyourattentionissomewhereelse,congratulateyourselffornoticingandgentlyreturntothebreath.Noticingthatyourmindhaswanderedisthepractice.
• Noticeanystrugglesandgentlyletthemgo. • Ifyounoticeoutside(orinside)distractions,simplynoticethem,andbreathewith
them.Donottrytochangeit.Letgoofanyfightingthedistraction. • Practicethiswayaslongasyouwish. • Allowyourselftorestandlookmoredeeplyasyousettleintothis. • Whenready,youmayendyourmindfulawarenesssessionbysimplyopeningyour
eyes.
FORMALPRACTICE
• SetaSmartGoalforyourself.Forexample,youmaywanttostartwith2-5minutesandeventuallymoveupto20or30minutesforeachsession.
• Youmayexperienceresistancetodoingthepractice;simplynoticethis. • Youdon’thavetolikeyourexperience,butyoudohavetodoitifyouwantto
experiencepresencethatcomesfrommindfulawareness. • Practicedailyor5daysoutof7. • Evenifyouarenotinyourregularroutineorplace,practicemindfulawareness
whereyouare. • Usetapesorguidanceifitishelpful.
INFORMALPRACTICE
• Taketimetonoticeyourbreathingthroughoutyourday. • Thismaytakeeffortandwork. • It’snothidingordisconnectingbutpayingattentiontoyourbreathasawayof
payingattentiontothepresent. • Thinkofpayingattentiontobreathingasafriend,notachore.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|31
• Practiceindifferentsituations.
Youmayfeelcalmer,andyoumaynot.That’sOK.It’samatterofpayingattentiontothemomentandbecomingaware.
AWHCshouldbepreparedtodevelopstrategiesandtrainpartnersinmindfulawareness.Atfirst,theymaysimplywanttouseascriptliketheonesfoundintheresourcesectionatthebackofthismanual.Eventually,manyhealthcoacheswillbecomeproficientinusingmindfulawarenesswithouttheuseofscripts.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
32|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER3:ACTIVECOMMUNICATIONSKILLSFORCOACHING
Mostcoachingisdoneusingtwoprimarycommunicationskills:reflectionsandinquiry(orquestioning).Attimes,coachesmightwanttoshareinformation,providedirection,ormakedisclosures.However,thebulkofeffectivecoachingwillbebuiltonreflectionsandinquiry.AsdescribedinChapter2,QualitiesofaWholeHealthCoach,listeningisthefoundationforthesetwoactivecommunicationskills.
LISTENING
Listeningstartsbybeingfullypresent.(SeeChapter2,QualitiesofaWholeHealthCoach.)Withoutbeingfullypresent,listeningeffectivelyiscompromised.Forthisreason,coachesareencouragedtofullydeveloptheirmindfulawarenessinordertobefullypresentfortheVeteranpartner.
Attimes,coachescanbeeffectivelistenersbysimplylisteningwithoutinterjectingquestionsorreflections.(ParticipantsintheWholeHealthCoachingTrainingwillhaveanopportunitytoexperiencethis.)SimplylisteningwithoutspeakingcanhaveaprofoundimpactontheVeteranpartner.“Holdingthespace”forapartnertohearthemselvesandreflectonwhattheyaresayingisaphrasethatdescribesthisofferingtothepartner.
Listeninginvolvespayingattentiontowhatthepartnerissaying,ornotsaying,bothverballyandnon-verbally.Inadditiontosilentlylistening,coachesalsouseactivelisteningskillsofsimpleandcomplexreflections.
THEPAUSE
Whenutilizinganyofthecommunicationskills,itisimportanttonotonlybeawareoftheskillbeingused,butalsothepaceatwhichtheyareused.Duringthecoachingsession,thetimeandspacewithoutwordscanbeasimportanttothereflectiveprocessasthetimewhenwordsarebeingspoken.Provideamplemomentsofsilenceandpausesthroughoutthecoachingsessionsinordertoallowpartnersadequatetimetoreflect.Itisinthesemomentsofsilencethatsomeofthedeepestinsightsandreflectionsarerealized.Fillingthesepauses/momentsofsilencewithwordsmaydetractfromthepartner’sabilitytogaingreaterinsight.
SIMPLE&COMPLEXREFLECTIONS
Simpleandcomplexreflectionsarethemostfrequentlyusedwholehealthcoachingcommunicationskills.Thinkofofferingtwotothreereflectionsforeveryquestionasked
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|33
whencoaching;astheyarejustaseffectiveindeepeningtheconversation,exploration,andforwardmovementasinquiry.Reflectionsarepowerfultoolsforallowingacoachingpartnertofurtherreflectonwhattheyaresaying.Reflectionsprovidea“mirror”forthecoachingpartner,whichinturn,mightprovidefordeeperreflectionandinsightintovalues,beliefs,andbehavior.
SIMPLEREFLECTIONS
Simplereflectionsmirrorbacktothecoachingpartnerwhattheyhavesaid.Simplereflectionsaddverylittle,ifany,meaningtowhathasbeensaid.Yet,theycanbeverypowerfulastheycapturetheessenceofwhatisbeingsaid.Thereare3typesofsimplereflectionstrainedintheWholeHealthCoachingcourse.Theyare:
• Parroting—usingafewofthepartner’sexactwords. • Paraphrasing—usingdifferentwordswithoutchangingthemeaningofwhatthe
partnerhassaid. • Summary—offeringasummarystatementthatcapturestheessenceofwhatthe
partnerhassaid.
Itshouldbenotedthatacoachdoesnotneedtoreflecteverythingapartnerhassaid.Decidingwhattoreflectisimportantinguidingthecoachingprocess.Forinstance,ifthetopicbeingdiscussedcentersonvalues,thencoacheswillwanttoreflectwhatvaluesthepartnerisidentifying.Reflectingtangentialthoughtsmaytaketheconversationinadirectionthatisnotasusefultothepartner.
COMPLEXREFLECTIONS
Complexreflectionsareeffectiveindeepeningtheconversation,exploration,insight,andforwardmovementoftheVeteran.Theyreflectthemorenuancedlanguage,tone,feelings,emotions,andmeaningofacoachingpartner’swords.Thismightbeinmeaningorperhapsinemphasis.Genuinelyinterestedandcuriouslistening–towhatisandisnotbeingsaid,andwhatismeant–iskeyinofferingreflectionsthatgobeyondthesimpleholdingupofthe“mirror”.
Thereareseveralformsofcomplexreflections.Therearetwocomplexreflectionsfocusedoninthiscourse:
• Double-sidedreflections—Reflectingtwosidestoanissuethepartnerhasraised,oftenfocusedonavaluesconflict.Thesereflectionsareoftenintheformof“ontheonehand…ontheotherhand”.Double-sidedreflectionsshouldendwiththesecondsideofthereflectionendingonthesideofchange(orpositivedirection).

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
34|VHA/OfficeofPatientCenteredCareandCulturalTransformation
• Intuitiveordeepermeaningreflections—Addingahunch(orintuition)orgoingbeyondwhatthepartnerhassaidtostimulatefurtherinsightintowhathasbeensaid.
Thefollowingscenariosoffersomeexamplesofeachofthetypesofreflections.Remember,therearemanypotentialreflections;theintentistoreflectinawaythatwillforwardthecoachingprocessandagendabydeepeningtheconversation,insight,andexploration.
EXAMPLE1
TheVeteransays,“I’msad,lonely,depressed.Ithinknobodylovesme…somedaysitseemsthatnobodycaresaboutme.Iwanttodie.So…becauseI’mfeelingthisway,I’mgonnasay,maybeabottleofvodkawilltakecareofit.So,bam!Imixitin.Mixitinwiththevodka&thenI’mfeelingsogoodI’mdrinking2morebeers.MaybeI’llsmokeajoint.MaybeI’llfeelbetter.Andthen,thenextdayafterallthehappiness&funisgone,darkholeagain.Itsortofcontinues.Itdoesn’tstop.Anditgetsworse.Itmakesittoughtochangemydietandgetmoving…it’ssohardtodoandIdon’tknowifit’sworthitwhenI’mfeelingsobadanyhow.Yet,somedaysI’mnotreadytogiveup…IhavesomethingsIwanttoaccomplishinlife,andIknowIwon’thavetheenergyifIdon’tchangesomethings.”
Somepotentialreflectionsbythecoachmightbe:
• Parroting—“You’renotreadytogiveup.” • Paraphrasing—“Thisisreallyadifficultsituationforyou.” • Summary—“You’redownbecauseofyourlifesituation,butyou’renotreadytogive
upbecauseyouhavethingsyouwanttoaccomplish.” • Double-sided—“Ontheonehandyou’renotsureit’sworththeefforttomake
changes,yetontheotherhandyouhavethingsyouwanttoaccomplishyetinlife.” • DeeperMeaning—“You’reheretodaybecauseyoureallywanttofulfillyour
aspirationsorpurposeinlife.”
EXAMPLE2
TheVeteransays:“IwassoexcitedaboutmydecisiontocutbackthenumberofhoursIwasworking.ButnowI’mreallystrugglingwithmakingendsmeet.It’salmostasstressfulaswhenIwasworkingsomuch.I’mnotsurewhatthebestroutetogoisatthispoint.”
Somepotentialreflectionsare:
• Parroting—“You’renotsurewhatthebestrouteisatthispoint.” • Paraphrasing—“It’sstillastressfulsituationthatyouwouldliketoresolve.” • Summary—“Youwereexcitedaboutyourdecision,butyoustillhavestressandare
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|35
notsurewhattodoatthispoint.” • Double-sided—“Ontheonehand,you’vecreatedsomenewstressors,butonthe
otherhandyouwereabletomakesomechanges.” • Deepermeaning—“Itseemsthatreducingstressisareallyhighvalueforyouand
onethatyou’rewillingtotackle…justnotsurewhichdirectiontogo.”
EXAMPLE3
TheVeteransays:“MydocthinksIneedtocutbackonmyovereatinganddropsomeweight.Shemayberight,butI’mnotconvinced.Sofar,I’vebeenabletomanagewithouttoomanyconsequences…Shedoesn’tseemtounderstandhowmuchpleasureIgetoutofcookingformyfamilyandeatingwiththem.Itmaybeanissuesomeday,butthereasonstochangerightnowdon’toutweighallthereasonstocontinue.”
• Parrot—“Morereasonstocontinuethanchangerightnow.” • Paraphrase—“Inspiteofwhatyourdocissuggesting,youdon’tseeaneedto
changerightnow. • Summary—“Yourdocwouldlikeyoutocutback,butyouenjoycookingandeating
andyou’renotseeingreasonstocutbackrightnow,althoughsomedaytheremaybemorereasonstochange.”
• Double-sided— “On the one hand you enjoy it toomuch and there aren’t enoughreasonstochange,butontheotherhand,you’vebeenprovidedreasonsyoumaywanttocutbackonyoureating.”
• Deepermeaning—“Pleasureisahighervaluetoyouthananyriskstoyourhealthyourovereatingmaybecausing.”
METAPHOR
Metaphoristheuseofanalogies,figuresofspeech,orimages(intheformofareflection)thatfurtherassisttheVeteraninfeelingunderstoodandcanbeusedlikeacomplexreflection.Muchofourlanguageincludestheuseofmetaphor–weoftenuseittoillustrateourthoughts,ourbeliefs,ourperspectives.Acoach’sabilitytolistenformetaphorintheVeteran’slanguage,ortocreatemetaphorfromtheVeteran’swords,canbeimpactfulinlettingtheVeteranknowtheyarebeingheard.Here’sanexample:
Veteran:“Iamsotiredofcarryingtheburdenofcaringformyagingparentswithnohelpfrommybrothersandsisters.”
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
36|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Coach:“You’recarryingtheweightoftheworldonyourshouldersandnooneisofferingafingertolightentheload.”
ACKNOWLEDGMENT
Anacknowledgmentisacoachingskillthatrecognizesandbringsattention(oftenintheformofareflection)totheclient’squalities,strengths,efforts,learnings,progress,andsuccesses.Thereispowerintheprocessofacknowledgingwhatyou,thecoach,hears/seesinyourVeteran’slanguage.
Manyhealthprofessionsteach/offerpraise,cheerleading,andencouragements–oftenofferedtocreateease,optimism,comfort,support,orpositiveregard.Thecoachingmodelofofferingacknowledgmentislessaboutthetemporary“feelgood”moment.ItisabouttappingintotheVeteran’sinternalmotivation.Thelastingimpact,effect,andshiftoccurswhenlessofwhatthecoach“thinks/feels”ispresentinthesession,andmorefocus/lightisshoneonacknowledgingthecoachingclient.
ADDITIONALCOMPLEXREFLECTIONS
AdditionalreflectionsworthnotingarefoundinMotivationalInterviewing(MI).Thoughtheyarenottaught/practicedinthiscoursetheyarenotableandusefulinthecoachingprocess.
• AmplifiedReflection–Reflectingwhatthecoachingpartnerhassaid,inanamplifiedorexaggeratedform.Acoachmightuseanamplifiedreflectionwitharesistant,or“stuck”clienttomovethemforwardtowardspositivechange.Becauseoftheexaggeratedtoneofthisreflection,itmustbedeliveredwithempathyandpatience.Anyhintofsarcasm,irony,impatience,orincredulitycanelicitahostileorresistantreaction.Anexample:
o Veteran:“Idon’tknowwhatmydocisworriedabout.I’vegotahandleonmyeatingandmybloodlevelsdon’tseemthathigh.”
o Coach:“So,yourdoctorisworryingneedlessly.”
• ShiftingFocusReflection–Shiftingfocusattemptstogetarounda“stuck”pointbysimplyside-stepping.Anexample:
o Veteran:“I’mjusttoobusy,Idon’thavetimetogetoutandexercise.”o Coach:“Soundslikeyouareprettybusy.Whatdoyouliketogetoutanddo?”
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|37
INQUIRY
Nexttolisteningandreflections,inquiryisprobablythenextmostusedcommunicationskillbycoaches.Inquiryisused,notsomuchtogaininformationfromthepartner,buttohelpthepartnerreflect,furtherself-explore,andbecomemoreinsightfulandawareoftheirownthoughts/feelings.Genuinelycurious,open-endedinquirycanassistthecoachindeepeningtheconversationandexplorationwiththeVeteran.
Inquiryshouldalwaysbebalancedwithlisteningandreflections.Ifinquiryisoverutilizedthecoachingsessionwilltakeontheformofaninterrogationorintakeassessment.
TherearetwotypesofquestionstaughtanddemonstratedintheWholeHealthCoachingtraining:closed-endedandopen-endedquestions.
CLOSED-ENDEDQUESTIONS
Closed-endedquestionstendtoelicitonewordorshortresponsesandfrequentlydonotleadtohigh-levelinsights.Therearesomeusesforclosed-endedquestions(likeaskingpermissiontooffersomeinformationorbrainstorming)andcoachesshouldbeawareofclosed-endedquestionsinordertomakeconsciouschoicesaboutwhentousethem.
Someexamplesofclosed-endedquestionsare:
• Areyoureadytomoveforward? • Wereyousuccessfulinmeetingyouractionstep/goal? • Areyouencouragedwithyourprogress? • Doyoufindthecoachinghelpful?
Althoughtheabovequestionsmaynotbeashelpfulasopen-endedquestions(alltheabovecouldbeeasilychangedtoopen-endedquestions(byaddingHoworWhat),therearetimeswhenclosed-endedquestionsmaybehelpful.Closed-endedquestionsaregenerallyusefulwhen1)makingtransitionsor2)askingpermission.
Moreexamplesofclosed-endedquestionsare:
• MayIofferyousomeresourcesthatI’mawareof?(FirstpartofElicit-Provide-Elicit) • Areyoureadytomoveon? • WereyouabletocompletetheWorksheets? • Isthereanythingelseyouwanttoaddresstoday?
OPEN-ENDEDQUESTIONS
Byfar,themostfrequentlyusedformofinquiryinWholeHealthCoachingistheuseofopen-endedquestions.Mostoften,thesequestionsbeginwith“What”or“How.”Sometimes

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
38|VHA/OfficeofPatientCenteredCareandCulturalTransformation
“Why”questionscanbeusedeffectivelytoelicitadditionalreflection.However,“Why”questionscansometimesbeperceivedasaskingforjustification,whichmayelicitdefensivenessfromthepartner.Forinstance,asking“WhydoyouwatchsomuchTVatnight?”mayelicitadifferentresponsethan“WhatvaluesareyouhonoringbywatchingTVatnight?”
Rememberthatquestionscomeoutofyourlisteningtoyourcoachingpartnerandguidingtheprocess.Forthesakeofprovidingsomeexamples,herearesomeopen-endedquestionsthatareassociatedwitheachStageoftheHealthCoachingProcessModel,introducedlaterinChapter4:
STAGEONE
• Whatreallymatterstoyouinyourlife?• Whatdoyouwantyourhealthfor?• Whatisyourmission,aspiration,orpurposeinlife?• Whataresomeofyourhighestvalues?• Whenareyourbehaviorsnotalwaysconsistentwithyourhighestvalues?• Whatwilllifebelike3yearsfromnowifyoudon’tmakechanges?• Whatwillitbelikeifyoudo?
STAGETWO
• AsyoucompletedthispartofthePHI,whatstoodoutforyou?• Whichareaswouldyouconsiderstrengths,orareasyou’redoingwellin?• Whatisanareathatyoumightwanttoenhance?• Whatmadethatareaa“2”foryou?• Whatmakesita2andnota1ora0?• Howcouldyouraiseittoa2.5?• Howimportantisittoyoutomakeachangeinthisarea?• Howconfidentareyouthatyoucouldmakeachangeinthearea?
STAGETHREE
• Wherewouldyouliketobe3monthsfromnowwhenyouthinkaboutmakingthischange?
• Whatactionstepsareyouwillingtoconsiderstartingwiththisweek?• Whatbarriersorchallengesdoyouanticipateencounteringasyoutakeonthese
actionsteps?• Whatwillbeyourplanofactionwhenyouencounterthischallenge?Howdoyou
wanttobeaccountable?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|39
STAGEFOUR
• Howdiditgoforyouthislastweek?• Whatdidyoulearnaboutyourself?• Whatchallengesdidyouencounter?• Howwouldyouliketochangeyouractionstepsfornextweek?• Howisthiseffortsupportingwhatyousaidwasimportanttoyou?
DIRECTCOMMUNICATION
Attimes,itmaybenecessarytomakestatements,directtheprocess,orprovideresources/information.Inallofthesecases,coachesareencouragedtousesimpleanddirect“I”Statements.
Someexamplesofdirectcommunication,or“I”Statementsare:
“I’dlikeyoufilloutthisformfornextsession.”
“Iwanttoexploresomepotentialbarriersyouthinkyoumayencounter.”
“Itseemstomeyou’vemadesomerealprogresssincelastsession.”
“Iwanttoprovideyouamomentofsilencetoreflectonthisnextquestion.”
“Iwanttosharewithyousomeofmythoughtsonwhatcoachingisandwhatitisnot.”
Whenusingdirect“I”statements,andwhenprovidinginformationorresources,coachesareencouragedtousethe“Elicit-Provide-Elicit”strategy(describedinChapter4)inordertominimizeresistancetohearinginformation.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
40|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER4:THEHEALTHCOACHINGPROCESS
Thefollowingdiagramshowsthevariousstagesofthehealthcoachingprocessforthistraining:
WerefertothisdiagramastheHealthCoachingProcessModel(HCPM).ItisimportanttonotethatthismodelservesasatrainingtoolandseldomwillaneffectiveandVeteran-centeredcoachingexperiencefollowthismodelexactly.Thoughtheindividualstagesaretaughtinalinearfashioninthetraining,rememberthattheHCPMisacircle–adynamic,circularprocessinwhichstagescanbevisited,andrevisited,duringanycoachingsession.Therearesomefurtherconsiderationsinutilizingthismodel.
EventhoughtheagendaforthecoachingsessionsistheVeteran’s,itisimportanttorememberthatthecoachistheholderoftheprocess.TheVeterandeterminesthedirectionhe/shewishestogo,andthecoachsupportstheminthatdirectionbykeepingthesessionsfocusedandmovinginaproductivedirection.Attimes,theVeteranwillbesharingstoriesofhis/herlifeandthestory’spurposemaynotbeclear.Itisthecoach’sresponsibilitytointerruptanon-productivestory,orflowofthesession,inordertobringtheprocessbacktoaproductivepath.Thisstrategyiscalleddirectand/orredirecttheprocess.CoachesmaythinkthattheyarebeingdisrespectfultotheVeteranincarryingoutthisresponsibility.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|41
However,allowingnon-productive,lengthystoriestocontinueisnotservingtheVeteranandtheircoachingexperience.CoachesshoulddevelopastyleofinterruptingandredirectingthatnotonlyisconsistentwiththeircoachingstylebutisdoneinsuchamannerthattheVeterandoesnotfeeldisrespected.Interruptingcanbedoneinagentleandrespectfulmanner.Onewaytosuccessfullydothatistomakeitpartoftheco-createdgroundrulesforthecoachingsessions.AskingtheVeteranhowtheywouldliketobeinterrupted,shouldtheneedarise,goesalongwayinpreparingthemforthepossibility.
Itisimperativethatcoacheshavetherequisitecompetenciestoconducteffectivecoaching.Initially,coachesmayalsovalueamapordirectiontowheretheyaremovingwiththeVeteran.ThisHCMPservesasthatmap.ThefollowingisabriefoverviewoftheHCPM.Amorecompletedescriptionofelementsofthismodelwillfollowthebriefoverview.
Stage1:DevelopAPersonalMission.Inthisstage,theVeterandevelopsa“personal”mission,aspirations,orpurposestatement(MAP)thatnotonlycontextualizesanyfuturechanges,butalsoguidestheoverallpersonalizedhealthplan.Thismayalsobethoughtofasa“statementofpurpose”oranoverall“healthvision.”Asapartofthisstage,VeteransalsoexplorethevaluesembeddedinthispersonalMAP.ItisalsohelpfultoexplorewhatothervaluesoftheVeteranimpedeorconflictwiththese“ideal”values.
Stage2:Assess&Focus.Inthisstage,theVeteranispreparingforactionby:
• AssessingtheirhealthinavarietyofareasasoutlinedintheCircleofHealth/PHI.• Definingafocus,orwheretheywanttostarttoenactachangeconsistentwiththeirimmediateinterestsandvalues.• Self-assessingandbuildingtheirreadinessforthepotentialchange.
Stage3:PlanforAction. Inthisstage,theVeteransetsgoals,developsactionsteps,identifiesbarriersandbackupplans,establishesaccountability,andidentifiessupport.Withoutthesestepsoftheplan,sustainedactionislikelytofail.
Stage4:ExecutetheAction.Thisstageiswhere“therubbermeetstheroad”andtheVeterancarriesouttheplanbasedontheirpreparationsandpersonalmission.Oncetheactionisattempted,theVeteranevaluateshowtheactionwasorwasnotsuccessful,whatwerethelessonslearned,whatre-planningneedstotakeplace,andwhatfurtheractionswillbeexecuted.
HOWTOUSETHEHCPM
Thereareseveralconsiderationstokeepinmindwhenutilizingthismodel:

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
42|VHA/OfficeofPatientCenteredCareandCulturalTransformation
TheHCPMisamap(ofsorts),notascript.Itisnottoberigidlyfollowed.TheVeteran’sprocessshouldultimatelyindicatewhereacoachneedstobeinthisprocess.However,foratrainingtool,ithelpsthenewcoachthinkabout
wheretheyareintheprocessandwhatmayneedtobeaddressedbeforeproceeding.Forexample,aVeteranwhohasnotcommittedtoaclearfocus,orwhattheywanttotakeonintermsofachange,maybewastingtimedevelopinggoalsandactionsteps.AnotherexamplewouldbeifaVeteranischoosingafocus,orareatowork,buthasnotgivenmuchthoughttohowthischangefitsintowhatreallymatterstothem.Withoutthisarticulationoftheirpurpose/missionorwhatreallymatterstothem,theyarerobbingthemselvesofimportantmotivationtosustainthechange.
Coachesmaywanttorevisitastage.AstheVeteranmovesthroughtheprocess,coachesmayfindithelpfultorevisitastage,especiallyiftheVeteranisencounteringdifficultiesinmakingthechange.Forexample,assumethattheVeteranhashadafewweeksinwhichtheyseemedunabletoenacttheiractionsteps.Itmaybenecessarytorevisitthe“settingactionsteps”phasetoseeiftheactionstepsweretooambitious,orifotheractionstepsmaybemoreimportantatthistime.Inotherwords,thisisnotastaticprocessofvisitingthestageonceandthenneverreturning.It’sadynamic,unfoldingprocessthatmaymeanvisitingaparticularstagemanytimes.
Thetimeframeforthestagesisflexible.CoachesmaywanttokeepinmindthetimeframetheyhavewiththeVeteran.Iftheencounterisonlyfor½hour,coacheswillwanttothinkaboutwhereintheprocesstofocustomaximizetheimpactfortheVeteran,giventhetimeconstraints.Ifcoacheshave8-9sessionswiththeVeteran,theycanbemuchmorethoroughateachstageandthinkaboutreturningtoeachstagemorefrequently.
TheHCPMisatrainingtool.CoachesshouldrememberthatthisisatrainingtooltohelpnewcoachesthinkaboutwheretheymightwanttogonextintheprocessofcoachingwiththeVeteran.Oncecoachesgetfamiliarwiththeprocess,wheretogonextwillbecomemore“secondnature”withafocusonwhataretheimmediateneedsoftheVeteraninthismoment.Likepracticingscalesinlearningmusic,itmaybeusefultohaveastructureinthebeginning.
However,mostmusicianswillsoonleavethescalepracticingtomakemusic...andtheymayreturntopracticingscaleswhentheyseetheutilityindoingso.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|43
STAGESANDPHASESOFTHEHCPM
Inthissection,wewilldescribethestagesandphasesoftheHCPMprocess.Inaddition,wewillprovideastrategy,orstrategies,forhowtoaddressthephaseofeachstage.Wewillstartwiththemission/purposestageandcontinuearoundthewheelinclockwisedirection.
STAGEONE
STAGEONE,PHASE1–CREATEAVISION
CreateaVisionStrategy.Atthisstage,coachesassisttheVeteranindevelopingamission,aspiration,orpurposestatement(MAP),ortheirvisionoftheiroptimallife.(coachesshouldexplorewhichtermbestsuitstheVeteran.)TheVeteranmayhavegivenmuchpreviousthoughttothisquestionorverylittle.Usingtheskillsofreflectionandexploratoryquestions,timeshouldbegiventotheVeterantoexplorethisquestionwithoutrushingtothenextstageorphaseoftheprocess.
ThereareseveralwaystoassisttheVeteraninexploringtheirMAP.Thefirst5questionsofthePHIbegintheprocessofhavingtheVeteranconsidertheirlivesandwhatmatterstothem.
AnsweringthesequestionscanbeapowerfulexperiencefortheVeteran.Itcanalsobeatimeofuneaseordiscomfort,astheVeteranmightbesurprisedbytheirresponses.ItisnotunusualfortheVeterantoexpressdiscomfortwiththinkingaboutthequestionsforthefirsttimeinaverylongtime,orever.
ItcanbehelpfultohavetheVeteranvisualizetheirfuturebyguidingthemthroughvisualization.HavetheVeteranpaintavividpicture,intheirmind’seye,oftheirfutureincludingsuchfactorsashowtheyfeel,howtheylook,theactivitiesinwhichtheyareengagingandenjoying,whoiswiththemandwhathealthbehaviorstheyarepracticing.Havethemwalkthroughatypicaldayintheiridealfuturewhentheyarelivingaccordingtowhatmattersmost.
Askinggenuinelycurious,exploratory,open-endedquestionsallowstheVeterantoarticulatetheirMAPandwhatmattersmosttothem.ItisimportanttohavetheVeteranvocalizewhatmatterstothem.Writingitdownhasimpactandarticulatingthestatementstoanotherperson(inthiscase,thecoach)canhaveanevenmorepowerfulimpact.
ThepurposeofhavingtheVeteranarticulatetheirMAPandwhatmatterstothemistwofold:First,itprovidesamotivationforanysubsequentchangeinitiatives,givingthemareasontoparticipateinthechangeprocessandsustainitwhenthegoinggetsdifficult.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
44|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Second,itallowsthemtofeelmorefullyunderstoodbythecoachandallowsthemtobeknownatadeeperlevelthantheyareprobablyusedtosharingwithahealthcareprovider.
ThisexplorationshouldbeofferedasanopportunityandnotimposedontheVeteran.Whenofferedtheopportunity,mostVeteranswillprobablywanttoparticipate.Imposingthisasanecessarystepincoachingmaytriggerresistance.
Thereisalsothequestionofwhentoofferthisopportunity.SomecoacheshavefoundithelpfulfortheVeterantocompletethePHIquestionsaftertheyhavehadtheopportunitytomeetwiththecoach,establishtheinitialrelationshipandexplorethevalueofcompletingthePHIwiththecoach.Althoughitisusuallycompletedbytheendofthefirstsession,thismaynotalwaysbethecase,dependingontheuniquecircumstancesofeachcoachingencounter.
OthercoacheshavefoundithelpfultooffertheVeterantheopportunitytocompletethefirstfivequestionsofthePHIbeforecomingtotheinitialsession—eitherbysendingacopyviamail,orhavingtheVeterancompleteitonline.Theadvantageofdoingthisallows1)theVeterantotaketimetothinkaboutthequestions,and2)itcanpreparethemfortheinitialcoachingsession.
ThedisadvantageisthattheVeteranmaynotyetknowwhatcoachingis–andthePHIquestionsmightbeoff-putting.TheVeteranmaynotunderstandwhythey’vebeenaskedtocompletethePHI,andpossiblywhythey’vebeensenttoseeacoach.CompletingthePHImaynotbeofinteresttotheVeteranbeforearrivingatthecoachingsession.Theymayquestionwhetherthisiswhatthey“signedupfor”.Theymayhaveanticipateddealingdirectlywiththeirpresentingissue.
ThecoachmightfindithelpfultofirstaddresstheVeteran’spresentingissueasameansoffocusingonwhatisimportanttothematthatmoment.Veteranscometocoachingforavarietyofreasons;theymayhavebeenreferredbyanotherhealthcareproviderforaspecificfocus,suchaslosingweightorstoppingsmoking.TheVeteranmayhaveself-selectedtocometocoachingforaspecificfocus.Or,theymaybecomingforgeneralizedhealthenhancement,notsurewhattheywanttoworkoninitially;theyjustknowtheywouldliketobelivingamorefulfillinglife.Eachofthesepresentationsinfluencehowthecoachingbegins.WhenaVeteranispresentingforaspecificissue,itisbesttostartwiththatissueratherthanimmediatelyhavingthemcompletethePHI.Iftheyarecomingwithoutaspecificfocusoranunclearfocus,itmaydictatethatthecoachmovestothePHIsoonerintheprocess.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|45
Inallcases,completingthisfirstelementofthePHI,developingaMAP,isanimportantstageinthehealthcoachingprocessandshouldbeofferedatsomepointintheinitialsessionsofcoaching.Theexperienced,artfulcoachwillmakeitanaturalpartoftheflowofthecoachingprocess;byofferingitwhentheVeteranhasexpressedinterestinexploringthecontextforthebehavioralchangesheorshemaybeinterestedinmaking.
STAGEONE,PHASE2–DISCOVERINGVALUESANDVALUESCONFLICTS
ExploringValuesandValueConflictsStrategies.OncetheVeteranhasarticulatedtheirMAP,itmaybeusefulforthemtoexplorewhatthatsaysabouttheirvaluesorwhatisimportanttothem.TheVeteranmaywanttoidentifyatleast3valuesthatcomeoutoftheirMAPs.Itisimportantthatthisdiscoveryprocessnotberushed.Itmaybehelpfultoreflectthevaluesheardandgivequiettimetoreflect.Seeminglysimplequestionssuchas“Whatelseisimportanttoyou?”or“Isthereanothervaluebehindthevalueyoujustidentified?”areoftennotsosimple–andcanbethoughtprovokingandprofound.Forinstance,iftheVeteransaysthatonevalueis“havingenoughmoneytonotbeworried”,theremaybeanothervaluebehindthisvalue.Thevalueof“freedomfromworry”or“mentalpeace”maybethevalue.Inthesecases,thesimplequestionsof,“Whatelsematters?Or“Whatothervaluemaybebehindthisvalue?”becomepowerfulquestions.Powerfulquestionsarethosequestionsthatleadtogreaterinsight,orthenext“ah-hah”momentfortheVeteran.
Itisimportant,inthisstage,toexploreValuesConflicts.Valuesconflicts,thosethingsthatareimportanttousthatmightbeinconflictwithotherheldvalues,areameaningfulandusefulareaofexplorationfortheVeteranandthecoach.IdentifyingthattheyhaveothervaluesthatconflictwiththeiridealvaluesisanimportantpartoftheVeteran’sself-discoveryprocess.ItallowstheVeterananopportunitytolookatwhattheygetoutoftheircurrentbehavior,evenwheninconsistentwiththeirhighestvalues.This,inturn,allowsthemtomakeinformedchoicesaboutwhichbehaviorstheywanttocontinueandwhichonestheymaywanttolookatchanging.Itisallbasedontheirself-assessmentofwhattheysayismostimportanttothem.IdentifyingvaluessetsthestageforexploringwhentheVeteran’sbehaviorsarenotalwaysconsistentwithwhattheysayismostimportant.Explorationofvaluesconflictsisimportantintwoways:1)itallowsVeteranstolearnaboutvalueconflictsthatwillbecomeevenmoreimportantastheymovedownthepathofattemptingtochangeabehaviororachieveagoal,and2)itallowsthemtoexplorethediscrepancybetweentheirbehaviorsandtheirvalues.
Examplesofquestionsthatcoachesmaybeutilizingatthisstageinclude:
• WhenyouthinkaboutyourMAP,whatcomestomindaboutwhatreallymatterstoyouinyourlife?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
46|VHA/OfficeofPatientCenteredCareandCulturalTransformation
• Youstatedwhenyoucameinthatyouwantedtoworkon...HowwouldworkingonthissupportyourMAPandwhatisimportanttoyouaboutdoingthat?
• ThinkoftimeswhenyouarenotachievingyourMAP?WhatotherthingsbecomeimportantthatmayhinderyoufromlivingaccordingtoyourMAP?
• Howisyourcurrentbehaviorconsistentorinconsistentwithwhatyousayisimportanttoyou?Isthissomethingyouwanttofurtherexplore?Whatwouldyoubegivingupifyouchangedthisbehavior?(Thiswillgetatconflictingvalues.)
STAGETWO
STAGETWO,PHASE1–CONDUCTASELF-ASSESSMENT
ConductingaSelf-AssessmentStrategy.AftertheVeteranhasexploredtheirvaluesandvaluesconflicts,itmaybeusefultoconductaself-assessmentthatlooksatalltheareasoflifeaffectingtheVeteran’shealthandwell-being.ThiscanbedoneutilizingtoolsfromthePHI,includingtheWhereYouAreandWhereYou’dLiketoBehandout,(Handoutpages6-9),whichrelatestotheCircleofHealth.Again,coachesmayofferthisasanotheropportunitytolookatwhatmatterstothemintermsoftheirhealthandassesswheretheyareandwheretheymaywanttobeinthevariousareasoftheirlifethatimpacttheirhealth.ImposingthisontheVeteranmayengenderresistance.Ideally,itworksbesttoofferthisatatimewhentheVeteranhasindicatedtheyarewillingtolookatissuesotherthanthepresentingissuethatmaybeimpactingtheirlives.
ThepurposeofthisstageistohelptheVeteranfurtherclarifywhatismostimportant,orwhatisofgreatestinterestforthemtobeworkingonatthistime.ItisnotunusualforaVeterantocometocoachingwithapresentingissue,andbythetimetheyhavegivenfullconsiderationtoallareasimpactingtheirlife,decidethattheyarereallymoreinterestedinworkingonanotherissue.Forexample,aVeteranmaycometocoachinghavingdecidedthattheyneedtohavemorephysicalactivityintheirlife.Aftercompletingtheassessment,theVeteranmaydecidethattheyreallyaremoreinterested,atthepresentmoment,inworkingatreducingtheirstress.-Itmaybethattheywanttoworkonacombinationofboth.Ineithercase,itismorelikelythattheVeteranwillachievesuccessiftheyworkontheareathatisofmostinteresttothem.Successbreedssuccess.Aftersomesuccessinonearea,theymaybemoremotivatedtotakeonanotherarea.
TheVeteranwillhavelearnedskillsandstrategiesforbehavioralchangeintheinitialundertakingthattheycannowapplytothenextchallenge.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|47
Attheassessmentphase,thecoachisnotlookingforacommitmenttochange.TheyaresimplyaskingtheVeterantoself-assessthevariousareasoftheirlivesthatimpacttheirwell-being.
ThereareotherformsofassessmentstheVeteranmayhaveavailabletothemandmaywanttoconsideraswell.Forexample,thesecouldbeothermedicalassessments,psychologicalassessments,andstressassessments.
STAGETWO,PHASE2–SELECTINGAFOCUS
SelectingaFocusStrategy.Allthecoach’sinteractionswiththeVeteranhavebeenleadinguptothispoint.ItiscriticaltonotaskaboutanareaoffocusuntilthecoachsensesthattheVeteranisreadytohomeinonanarea.Prematurelyaskingfortheareaoffocusmayevokeresistance.Ontheotherhand,theVeteranmaybeanxioustogetonwiththecoachingintheareaoffocuswithwhichtheyinitiallypresented.TheseinterveningphasesmayhavehelpedconfirmfortheVeteranthatthisiswheretheywanttomakechanges.
ItisimportantforcoachestorealizethatVeteransmaynotnecessarilywanttostartwithanareathattheyscoredthemselvesthelowestinwhencompletingtheWhereYouAreandWhereYou’dLiketoBehandout.TherearemanyfactorsthatgointotheVeteransdecidingwhichareatheywanttoaddressfirst.
Theseconsiderationsinclude:
• Theimportanceoftheareatotheminthemoment.• Theconfidencetheyhavetomakechangesinthatarea.• Theenergyandtimetheyfeeltheyhavetotakeonthatchallenge.• Theimmediatebenefitstheymayperceivewillbeforthcoming.• Thelong-termbenefitsofmakingthechange.• Theexcitementtheyhaveformakingthechange.
Coachesmustself-managetomakesuretheyarenotintentionally,orunintentionally,steeringtheVeteransinthedirectiontheythinkwouldbebestfortheVeteranstoaddress.
STAGETWO,PHASE3–ASSESSINGREADINESS
AssessingReadinessStrategies.BeforeproceedingtothenextstageofPlanningforChange,coacheswillwanttoassessiftheVeteranisadequatelymotivatedtotakeonthechallengeofchange.OnewaytodothatistoassesstheimportanceofthischangetotheVeteranaswellastheconfidencetheVeteranhasthattheycanmakechangesinthisarea.
Typicalquestionsthatcoachesmayfindthemselvesaskingatthisphaseare:
• Whatmakesthemostsenseforyoutothinkaboutchangingatthistime?Howdo

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
48|VHA/OfficeofPatientCenteredCareandCulturalTransformation
youwanttogoaboutprioritizingwhereyouwanttostart?• Whatwouldyoubemostexcitedaboutchangingatthistime?• Whatisitthatyouthinkyoumayhavethetimeandenergyforchangingatthis
time?• Whatwouldbethemostimportantareaforyoutothinkaboutchangingatthis
time?Onascaleof1to10,howimportantistoyou?• Inwhatareadoyouthinkyouhavethemostconfidenceforbeingabletomakea
change?Onascaleof1to10,howconfidentareyouthatyoucanmakeachangeinthisarea?
STAGETHREE
STAGETHREE,PHASE1–SETTINGAGOAL
Goalsettingisusuallycriticalforsuccessfulandsustainedaction.AgoalnotonlyenhancesmotivationforchangebutprovidestheVeteransameasureforhowtheyareprogressing.
However,settinganeffectivegoalisimportantand,ifnotdonewell,canalsohavetheimpactofdemoralizingtheVeteran.Itisimportantthatgoalsettingnotbedonehastily,butthatallelementsofsettinganeffectivegoalarecarefullyconsideredbeforemovingaheadintheprocess.
SettingaSMARTGoalStrategy.Thereisnotaspecifictimeframeforsettingagoal,butgenerally3-6monthshasbeenmostfrequentlyutilized.ThetimeframeshouldtakeintoaccounttheinterestoftheVeteran.Agoalthatistoofaroutinfrontmayseemtoodistanttoberelevant;agoalthatistoocloseintimemaynotallowtheVeteranstoexperiencethenon-linearmovementtowardthegoal,resultinginthegoalnotbeingobtained.Inotherwords,mostVeteranswillexperiencehighsandlowsintheirmovementtowardagoal;itisimportanttoallowenoughtimetomakeitthroughthispartoftheprocess.
CharacteristicsofeffectivegoalsettingfollowtheacronymSMART,whichstandsfor:
Specific—Agoalshouldbeclearandconcise.Itisdifficulttoknowwhenactiontowardagoalhasbeenstartedandwhenithasbeencompletedifitisnotspecific.
Measurable—AgoalshouldbemeasurablesothatVeteranscantracktheirprogress.Veteransneedtohaveclearcriteriaforprogressandcompletionwhentakingactiononagoal.Keepingtabsonprogresscanbeinspiring.
ActionOriented—Agoalshouldincludeaction.AndthatactionshouldbeindirectcontroloftheVeteran.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|49
Realistic—AgoalshouldbelargelywithinthereachoftheVeterans.Itisbesttoworkonsmalllifestylechangesthataredoable.AvoidthepitfallsofhavingVeteransseeonlythebigpictureandnotthesmallsteps.
Timed—Agoalshouldbetiedtoatimetableforcompletingspecific,measurable,andrealisticaction.
ThereareseveralquestionsthatcoachesmaywanttohaveVeteransconsiderwhensettingagoal.Theseare:
• IsthegoalasignificantenoughstretchfortheVeteranthatitcreatesexcitementinachievingtheoutcome?OrisittoogreatastretchthatitbecomestoomuchofareachfortheVeteranandthemotivationisdecreased?
• IsthissomethingtheVeteranreallywants,oristhisimportantenoughthattheVeteraniswillingtoengageinactionstepstowardthegoal?Inotherwords,doesthisgoalreallymattertothem?
• WhatdailypromptsorremindersarehelpfultotheVeteraninkeepingthegoalinmindonaregularbasis?
• DidtheVeterancommittheirgoaltopaper?Goalscaneasilybeforgottenormodifiedinadvertentlyovertimeifnotwrittendown.
• Isthegoalclearlyinlinewith,andinsupportof,theVeteran’smission/purposeandvalues?ItmaybeusefultohavetheVeteranverbalizeandwritedownhowthisgoalwillhelptheminfulfillingtheirmission/purpose.
• DoestheVeteranneedmoreinformationinhelpingthemestablishagoal?Forinstance,whatisareasonableamountofweightonecanexpecttoloseinagiventimeframe?Whatadditionalmealplanningdotheyneediftheirgoalistoeatanutritionallybalancedmeal4outof5meals?
Attimes,Veteranshaveoptionsinhowtheymaywanttomeettheirgoal.ItmaybehelpfultohaveVeteransbrainstormwaysofmeetingthegoal.Forinstance,let’sassumethataVeteranwantstodecreasehisweightby5%overthenext3months.BeforeassistingtheVeteraninestablishingactionsteps,itmaybehelpfultothinkofoptionstheVeteranhasforreducingweight.Inassistingthem,avoiddoingthebrainstormingforthem.Allowthemtimetoreflectanddotheirownbrainstorming.Asmuchaspossible,allowtheideastobetheirown.Thiswillhelpmaximizesuccessincarryingouttheactions.Someexamplesofwhattheymightcomeupwithinclude:
• Eatlessofwhattheycurrentlyeat.• Eatdifferentfoodsthanwhattheyarecurrentlyeating.• Increasetheirlevelofregularphysicalactivity,suchaswalkingupstairsand

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
50|VHA/OfficeofPatientCenteredCareandCulturalTransformation
parkingtheircarfurtherawayinaparkinglotordancingmore.• Increasethekindsofactivitiestheydothatincluderegulartripstoafitnesscenter
orwalkingseveralmiles3timesaweek.• Reducethesugarydrinksintheirdietordrinkmorewater.• Takeweightlosssupplements.• Dealwithstressorsthatleadtoovereating.• Eatmoremindfully.
ThisbrainstormingmayhelptoexpandthelimitednumberofwaystheVeteranwasthinkingtheycouldloseweightandtheymaycomeupwithaplanthatismorelikelytosucceed.
STAGETHREE,PHASE2–ESTABLISHINGACTIONSTEPS
EstablishingActionStepsStrategies.AnotherveryimportantpartofthePlanningStageisestablishingactionsteps.ActionstepsarethoseinitialandongoingbehaviorsthatwillhelptheVeteransachievetheirgoals.Actionstepsarethosebehaviorsthatareestablishedforthenextweek,orashortdurationoftime.Actionstepsarewhere“therubbermeetstheroad.”
ActionStepsshouldbeestablishedaccordingtothesameSMARTCriteriautilizedforsettinggoals.(SeeSMARTcriteriaunderStage3,Phase1GoalSetting)Again,itisimportantnottorushestablishingactionsteps.TheVeteran’smotivationforcontinuingthechangeprocesscanbeenhancedordiminishedbytheirinitialsuccessesinachievingtheiractionsteps.
ItisimportantforcoachestorealizethatinitialactionstepsmaybeobtainingmoreinformationthatwillhelptheVeteranestablishfutureactionsteps.Forinstance,iftheVeteran’sgoalcentersoneatingmore,healthyfoods,theVeteran’sinitialstepmaybeobtainingmoreinformationaboutwhatfoodstheywanttobepurchasing.Or,theymaywanttoexplorewhichrestaurantsservethefoodsthatmeettheirspecificationsfor“healthy.”Or,theymayhavetospendthefirstweeklearningtoreadlabelsingrocerystores.
Anotherexampleofgatheringinformationmightcenteronaddingmoreactivitytotheirlives.Theymayhavetoexplorethefollowingfactorsbasedontheirinterests.Thesefactorsmayincludethefollowing:
• Determiningwhatadditionalgear/clothing/shoestheymayneedtogetstarted.• Determiningasafeplacetowalkifthatispartoftheirplan.• Findinganotherpersonoragroupofpersonstowalkwith.• Findingouttheadvantagesofjoiningafitnessclubvs.havingequipmentathome.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|51
• Becomingfamiliarwithanyrisksassociatedwiththeirpreferredchoiceofmovement.
ItisimportanttorememberthatestablishingactionstepsaccordingtotheSMARTcriteriacanmakeorbreakthesuccessoftheVeterans’endeavors.Plancarefully.
STAGETHREE,PHASE3–IDENTIFYINGANDEXPLORINGPOTENTIALBARRIERS
IdentifyingBarriers/ChallengesandContingencyPlansStrategy.BarrierstosuccessfulactionmayariseinallstagesandphasesofthecoachingprocessthattheVeteranmayneedtoovercome.ThissectionwilllookatthekindofbarriersaVeteranmayidentifyandstrategies,orbackupplans,fordealingwithpotentialorrealizedbarriers.
WeareintroducingbarriersherebecauseitcanbeavaluableexperiencetohaveVeteransanticipatebarriersbasedontheirknowledgeofthemselvesandpreviousexperiences,aswellastheexperiencesofothers.Onceactionstepsareinitiated,andduringeachsubsequentcoachingsession,itmaybeusefultocontinuetoexplorewhatbarrierstosuccessfulactionaroseduringtheweekandmakeplansforovercomingthem.
Therearetwobroadcategoriesofbarriers—internalandexternal.ThisdistinctionislargelybasedontheVeteran’sperceptionsbecausemostperceivedexternalbarriersarereallybarriersbasedontheVeteran’sinternalperspectivesandresponsestothosebarriers.Examplesmayfurtherclarifythis:
AVeteranmayidentifygoingtoabarwherealcoholisservedandbeingaroundpeoplewhoaredrinkingasanexternalbarriertohis/herachievingsobriety.AlthoughthismaybeperceivedbytheVeteranasanexternalbarrier,itmaybeusefulfortheVeterantonoticethatitishis/herresponsetotheexternaldrinkingenvironmentthatalsoplaysintotheirabilitytoresist.Inthiscase,itbecomesmoreofaninternalbarriertoplanfor.
OtherVeteranswhowanttoslowdownandlimittheamountoftimespentatworkmayperceivetheirdebtloadasanexternalbarriertolimitingtheamountoftimeatwork.Onfurtherexploration,itmaybewhattheyaretellingthemselvesabouttheirdebtthatisthebarriertoslowingdown.
Itisimportanttonotethatalthoughthereareplansthatcanbeestablishedtoworkaroundtheperceivedexternalbarriers(i.e.,nothangingoutinbars,choosingcarefullywhoonechoosestohangoutwithindrinkingsituations),therearealsoopportunitiestodevelopplanstodealwiththeinternalbarriers(i.e.,rehearsingrefusalskills,visualizingwhatitwillbelike3hoursfromnowifIdodrink).Mostofthetime,Veteranswillperceivethemselves
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
52|VHA/OfficeofPatientCenteredCareandCulturalTransformation
ashavingmorecontroloverinternalbarriersthanexternalones.Externalbarriersareoftenperceivedas“onesIcannotcontrol”;onesimplyneedstocontroltheirproximitytotheexternalbarrier(person,place,thing,orevent).
IDENTIFYINGANDDEALINGWITHINTERNALBARRIERS
Internalbarriersgobymanynamesanddescriptions.ChoosetheonesthatarerightforyouortheVeteransyouserve.Eachofthesewillhavethesameoutcomesifappliedeffectively.
ItisimportanttonotethatyoudonotneedtoidentifythebarriersbyanylabeltoeffectivelydealwiththeVeterans.CoacheslistenforandsimplynotewhenVeteransarediscussingbarrierswithouthavingtonamethem.Forinstance,aVeteranmaysay“IwishIhadstartedthiswhenIwasyounger.ItwouldbemuchsimplertodoifIwereyounger”.ThecoachmaysimplycallthatstatementtotheVeteran’sattentionandaskthemtoexplorehowthatstatementmaybeservingthem,ornotservingthem,intermsofmovingforwardwithanactionplan.
Eachofthesewaysofperceivingbarrierswillbebrieflyidentifiedinthefollowingsections.
DEVELOPINGPERSPECTIVES
Aperspectiveisonewayofviewingasituation.Veteransmightidentifytheirperspectiveasthe“truth,”ortheonlywayofperceivingthesituation.Manytimes,limitingone’sperspectivelimitsthealternativesfordealingwithaspecificsituation.
ChangingperspectivesissimilartotheworkofAlbertEllisandtheSPCmodelthatflowsfromhiswork.(ThisisalsocalledCognitiveBehavioralTherapy(CBT),inwhichmanymentalhealthprofessionalswithintheVHAhavebeentrained.)ThefollowingbrieflydescribestheSPCmodel:
‘S’standsforSituation—Asituationisdescribedinobjectiveterms—who,what,whenandwhere.ThesituationisthefocusforexploringtheVeterans’perspectivesandresultantbehavior. DoorwayorMirror?
‘P’standsforPerspective—Perspectivesarederivedfromthethoughtsandbeliefsaboutthesituation.Thoughtsaretheinterpretationsoftheeventorwhattheysaytothemselvesaboutthefacts.Thesethoughtsarebasedonthebeliefsthatpertaintothesituation.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|53
‘C’standsforConsequences,eitheremotionalorreactions(behaviors)—EmotionsarewhatVeteransfeelasresultoffilteringtheactivatingeventthroughtheirthoughtsandbeliefs.
Reactionsarewhattheydoinresponse.
PerspectivescanbeproductiveorcounterproductivetotheVeterans’progressinmakingchange.ItisimportanttoassistVeteransinrecognizinghowtheirperspectivesareservingthemornotservingthem.Veteransmaybeunawarethattheremaybeanotherlensthroughwhichtoviewthesituation,andthisdifferentviewcouldinfluencetheirbeliefs,feelings,andactions.
AnothertermthatmaybeusefultotheVeteranissubstitutingtheword“story”for“perspective.”Astoryiswhatsomeonetellsthemselves,orothers,aboutasituation.Again,thestorytellermayseetheirwayoftellingtheirstoryasthe“truth.”
However,frequentlyitistheirinterpretationoftheevent.Veteransmaybeinvitedtothinkabouthowtherecouldbeanotherstoryabouttheeventsandaskedtothinkabouthowtheycouldchangethestoryinawaythatwouldservethemdifferently.
SomeexamplesofperspectivesorbeliefsthatmayhaveimpactonVeteransmovingforwardinthechangeprocessmaybe:
• Myworthisdependentonwhatpeoplethinkofme.• Everyonemustlikemeandmyideas.• IfImakeamistake,peoplewillloseconfidenceinme.• Imustbeasgoodastheothermusiciansperformingpublicly.• I’mafailureifIdon’tsticktothedietplanwedesigned.• There’snotmuchIcandoaboutthestressorsIexperienceinmylife.
ThereisaperspectivesworksheetintheHandoutsectionthatmaybeusefulforcoachestousewithVeteransinhelpingthemidentifyhowtheirperspectiveinfluencestheirchangeprocess.
WORKINGWITHNEGATIVESELF-TALK
We,ashumans,allhaveself-talkandmay,ormaynot,beawareofit.Self-talkisthemessagewesaytoourselvesaboutourselves.Veteransarenotalwaysawareofthesenegativemessagestheysaytothemselves.Likeperspectives,negativeself-talkmaybelimitingandinterferewithsuccessfulaction.Itmaybehelpfulforcoachestobringthisnegativeself-talktotheVeterans’awarenessandhelpthemassesswhattheygainfromit,orhowithindersthem.Someexamplesofnegativeself-talkare:

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
54|VHA/OfficeofPatientCenteredCareandCulturalTransformation
• “I’mnotsmartenough.”• “I’mtoolazy.”• “IalwaysfailwhenItryto...”• “I’mtoooldtostartthis.”• “Idon’tdeservethis...”• “Idon’thaveenough...”
Coacheswillseethatworkingwithnegativeself-talkisalmostidenticaltoworkingwithperspectives.Thesamestrategies,stylesandquestionsapply.Theintenthereistoshowthesimilaritiesandallowcoachestochoosewhichlanguageworksbestforthem.ThesameistrueofWorkingwiththeInnerCritic.
WORKINGWITHTHEINNERCRITIC
Likenegativeself-talk,innercriticworkinvolvesassistingtheVeteraninidentifyinghowtheircriticalthoughtsaboutthemselvesmayservetheminsomewaysbutnotinothers.Effectivecoachinginvolvesidentifyingthesecriticalmessages,assistingtheVeteraninidentifyinghowtheinnercriticdoesordoesnotservethem,andhelpsthemmakechoicesaboutwhichmessagestheywanttogivetheinnercritic,including:
• Payingattentiontotheinnercritic.• Makingpeacewithorbefriendingtheinnercritic.• Ignoringtheinnercritic.Orchoosingnottobelievetheinnercritic.• Givingtheinnercriticlesspower.• Namingtheinnercritic.• Playingwiththeinnercritic.• Askingtheinnercritictoleave.
Anotherwaytoignoretheinnercriticistofocusonpositivemessages.Thiscanbedoneby:
• FocusingontheVeterans’mission/purposeandvalues.• Brainstormingotherperspectiveswiththem.• HaveVeteransidentifyamessagetheymightgiveafriendstrugglingwithaninner
critic.• Elicitingwhatbringsjoy,peace,and“aliveness”.• Recognizingtheirprogressandencouragingactionsteps.• EncouragingVeteranstoparticipateinwhatnourishesthem.
WORKINGWITHCOMPETINGORCONFLICTINGVALUES
Whatmaybeperceivedasabarrierinsomecasesisanothervaluethatiscompetingforthetime,attention,andenergyoftheVeteran.HelpingtheVeteranidentifytheirown

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|55
competingvaluesmaymakeiteasiertothinkaboutstrategiesorplansforconsciouslyselectingwhatvaluetheywanttohonorinthemoment.
ItmaybeimportantforthecoachtorecognizethatvalueconflictsarenotnecessarilyperceivedassuchbytheVeteran.Acoachmighthearwordslike,“Ireallyvaluemyhealth,butI’mjustlazyandwanttohangoutonthecouch.Lyingonthecouchandbeinglazyisnotavalueofmine.”ItmaytakesomereframingofthesituationfortheVeterantorealizetheydogetsomethingoutof“beinglazyandlayingonthecouch”eventhoughtheydon’tviewitasavalue.Ithassomeimportanceinthatparticularmomentthatservestheminsomecapacity.Assistingtheminunderstandingwhattheygetfromthatbehavior,withoutjudgingthemselves,istheartfulchallengeforthecoaches.
ELICIT-PROVIDE-ELICIT
Whencoachesbelieveitmaybevaluabletoprovidesomeinformationorpotentialresourcesforthepartner,theinformation/resourcesmaybemoreeasilyheardwhenusingthefollowingstrategy:
• ElicitwhethertheVeteranisinterestedinlearningsomethingyouthinkmightbehelpfulorrelevant.IftheVeterandeclines,stop.Providinginformationnowisapttomakechangelesslikely.
• IftheVeteranisinterested,providetheinformationorconcernyouhave.Rememberingtokeepitbrief.Thisisnotthecoach’sopportunitytoofferupeverythingtheyknoworoverloadtheVeteranwithtoomuchinformation.
• ElicittheVeteran’sinterpretationofthatinformation,howshethinksitappliestoher,whatsenseshemakesoutofit.EmphasizethattheVeteranistheonetodecidewhattodowiththeinformation.
BRAINSTORMING
Anotherstrategyforworkingwithbarriers/challengesisbrainstorming.Inbrainstorming,coachesaskpartnersiftheywouldliketobrainstormsomeideas(elicitpermission).
• Explainthebrainstormingprocess–abriefexchangeofideas,notmeanttobeponderedordiscussed,but“thrownagainstthewalllikespaghetti”.Itismeaningfulforthecoachtoemphasizethat“anythinggoes”–anyideaisworthofferingup,nomatterhowbig,small,oroutlandish.Theideaistogeneratethinkingwithoutjudgment.
• ThecoachandVeterantaketurnsofferingideaswithnojudgment.FirsttheVeteran,thenthecoach,andsoonuntilanagreeduponnumberofideasareonthetable.
• AttheendofthisexchangethecoachaskstheVeteranwhich,ifany,ideassound

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
56|VHA/OfficeofPatientCenteredCareandCulturalTransformation
doableforthem.Insummary,therearemanywaystoviewbarriersthatmaybehelpfulforboththeVeteransandcoaches.Theimportanttaskforcoachesistolistenforwords,thoughts,andexpressionsthatmaybelimitingthecoachingpartnerinsomeway.HavetheVeteransidentifyhowthatperspectiveisbothservingthemandnotservingthem.Havethemexploretheirattachmenttothatparticularperspectiveandassistthemin“tryingon”anotherperspectivetoseewhatmightbepossiblefromthatnewperspective.
STAGETHREE,PHASE4–ESTABLISHACCOUNTABILITY
EstablishingAccountabilityStrategy.Mostpeoplefindthatbycommittingtoanotherpersontoreportwhattheyaccomplishedordidnotaccomplishfortheweek(oranyothergiventimeperiod)canbeverymotivatinginachievingthedesiredactionstep.Manywillindicatetheirdesiretobeaccountabletothecoachattheirnextmeeting.Othersmaywanttosolicitthehelpofaspouseorfriendtoholdthemaccountable.Sometimes,aVeteranmaywanttobeaccountabletothemselvesbywritingdownorjournalinghowtheydideachdayinachievingtheiractionstep.
NomatterwhatmethodtheVeteransuse,itisanotherimportantpartoftheprocess.ThisisanotherplacewherethisphaseshouldbeofferedasanopportunityandnotjustassumedthattheVeteransarewillingorwantingtoestablishaccountability.
Questionsthecoachesmaywanttoconsideratthisphaseinclude:
• Ifyoufinditusefultoholdyourselfaccountabletosomeone,I’mofferingmyservices.Ifyouwantmetobethepersontowhomyouholdyourselfaccountable,howcanIdoitinthewaythatismostsupportiveofyou?
• Aretherewaysthatyouwanttobeaccountabletoyourself?Ifso,whatmightbesomeofthoseways?
• Isthereanyoneelsewhocouldbethe“right”persontocommittoholdingyouresponsible?
STAGETHREE,PHASE5–PROVIDEAFFIRMATIONS
ThisisnotphaseofStage3,perse,butthroughoutthecoachingsession—andespeciallyafterthepartnerhasinitiatedaction—thecoachwillwanttolookforopportunitiestoprovideaffirmations.Thefollowingarestrategiesforprovidingaffirmations.
Thereareseveralstylesofaffirmationswithwhichcoacheswillwanttobefamiliar:
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|57
• Judgment:“Youhavedonearemarkablejobinstoppingyourcuttingbackonyoursugarintake.”
• Impact:“Iappreciatehowhonestyouarebeingintalkingaboutthesethings.”(AdescriptionofapositiveexperienceinresponsetowhattheVeteranisdoingorhasdone.)
• Observation:“Youweresuccessfulinstoppingthefighting.”(FocusontheVeteranandfactsthatemphasizethepositive.)
Therearealsosomecautionsinutilizingaffirmations.Thefollowingquestionsmayhelpcoachestothinkaboutthesecautions:
• Isyouraffirmationcomingfromadeficitworldview,whereyousoundlikeyoubelieveyourVeteranlacksknowledge,skills,orattitudes?
• IfyousaytheVeteran’sbehavioris“good,”thenadifferentbehaviororchoicewouldhavebeenlabeled“bad”?
• or• IsyouraffirmationcomingfromaviewoftheVeteranascompetent?• IdentifyingvaluesorcharacteristicsoftheVeteranthattheVeteranmightusetofeel
seen,unique,worthy?
STAGEFOUR
STAGEFOUR,PHASE1–ASSESSTHEACTIONTAKEN(ORNOTTAKEN)
AssessingActionTakenStrategy.OncetheVeteranhascommittedtotakinganActionstep(s),thecoachingentersanotherstage.TheVeteranwillhavedoneoneofthesethreepossibilities:
• Fullycompletedorexceededtheproposedactiontobetaken.• Partiallycompletedtheproposedactiontobetaken.• Didnottakeanyactionthatwasproposedandcommittedto.
Inallcases,thereispotentialforlessonslearnedwhichinturnresultsinsustaining,modifying,oreliminatingtheplanandreturningtoanearlierstage.
STAGEFOUR,PHASE2–LESSONSLEARNED
AssessingLessonsLearnedStrategy.Inassessingtheactiontaken,ornot,thefirststepistoexplorewiththeVeteranwhattheylearnedfromtheexperience.
TheVeteranmayhaveencounteredadditionalbarriers,bothinternalandexternal,thattheydidnotanticipate.ItmaybeusefultoexplorewiththeVeteranwhattheyplantodo
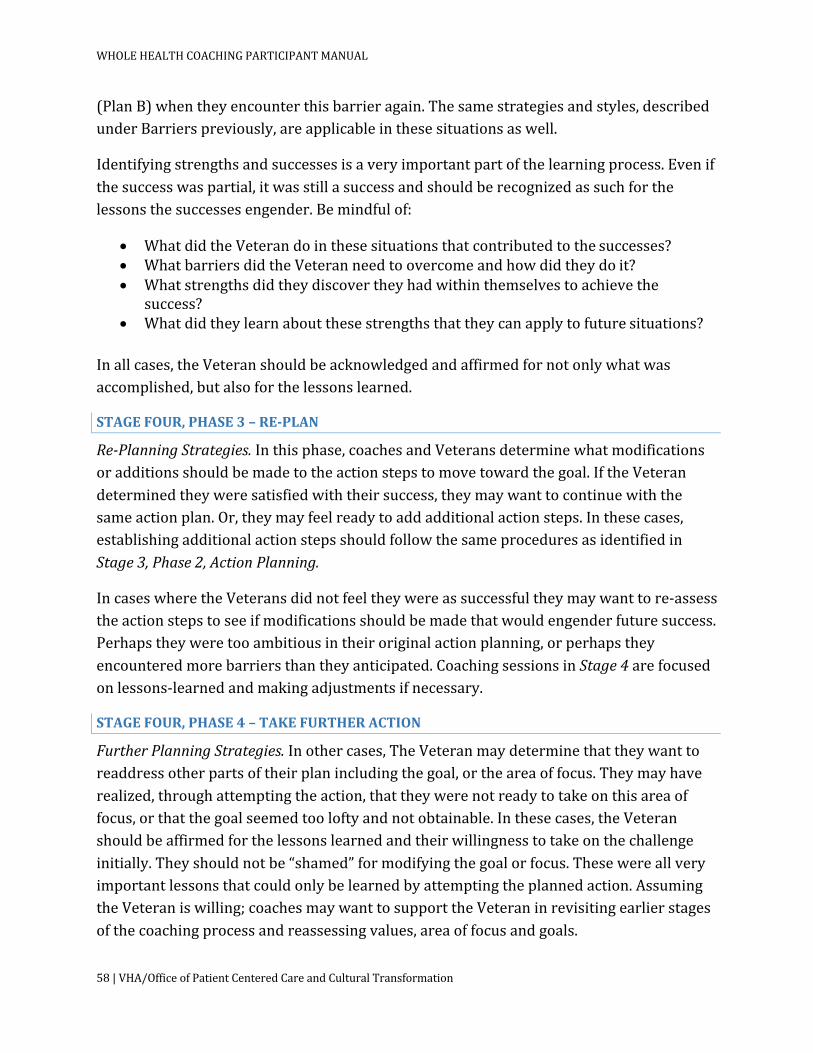
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
58|VHA/OfficeofPatientCenteredCareandCulturalTransformation
(PlanB)whentheyencounterthisbarrieragain.Thesamestrategiesandstyles,describedunderBarrierspreviously,areapplicableinthesesituationsaswell.
Identifyingstrengthsandsuccessesisaveryimportantpartofthelearningprocess.Evenifthesuccesswaspartial,itwasstillasuccessandshouldberecognizedassuchforthelessonsthesuccessesengender.Bemindfulof:
• WhatdidtheVeterandointhesesituationsthatcontributedtothesuccesses?• WhatbarriersdidtheVeteranneedtoovercomeandhowdidtheydoit?• Whatstrengthsdidtheydiscovertheyhadwithinthemselvestoachievethe
success?• Whatdidtheylearnaboutthesestrengthsthattheycanapplytofuturesituations?
Inallcases,theVeteranshouldbeacknowledgedandaffirmedfornotonlywhatwasaccomplished,butalsoforthelessonslearned.
STAGEFOUR,PHASE3–RE-PLAN
Re-PlanningStrategies.Inthisphase,coachesandVeteransdeterminewhatmodificationsoradditionsshouldbemadetotheactionstepstomovetowardthegoal.IftheVeterandeterminedtheyweresatisfiedwiththeirsuccess,theymaywanttocontinuewiththesameactionplan.Or,theymayfeelreadytoaddadditionalactionsteps.Inthesecases,establishingadditionalactionstepsshouldfollowthesameproceduresasidentifiedinStage3,Phase2,ActionPlanning.
IncaseswheretheVeteransdidnotfeeltheywereassuccessfultheymaywanttore-assesstheactionstepstoseeifmodificationsshouldbemadethatwouldengenderfuturesuccess.Perhapstheyweretooambitiousintheiroriginalactionplanning,orperhapstheyencounteredmorebarriersthantheyanticipated.CoachingsessionsinStage4arefocusedonlessons-learnedandmakingadjustmentsifnecessary.
STAGEFOUR,PHASE4–TAKEFURTHERACTION
FurtherPlanningStrategies.Inothercases,TheVeteranmaydeterminethattheywanttoreaddressotherpartsoftheirplanincludingthegoal,ortheareaoffocus.Theymayhaverealized,throughattemptingtheaction,thattheywerenotreadytotakeonthisareaoffocus,orthatthegoalseemedtooloftyandnotobtainable.Inthesecases,theVeteranshouldbeaffirmedforthelessonslearnedandtheirwillingnesstotakeonthechallengeinitially.Theyshouldnotbe“shamed”formodifyingthegoalorfocus.Thesewereallveryimportantlessonsthatcouldonlybelearnedbyattemptingtheplannedaction.AssumingtheVeteraniswilling;coachesmaywanttosupporttheVeteraninrevisitingearlierstagesofthecoachingprocessandreassessingvalues,areaoffocusandgoals.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|59
TheprocessdescribedhereinStage4continuesuntiltheVeteranandcoachagreetoendthecoachingsessions.ThismayoccurwhentheVeteranfeelstheyhaveexperiencedenoughsuccesstocontinueontheirown,ortheydeterminethatwhatevertheyhavelearnedorgainedisenoughatthispoint.
Insomecases,thecoachingendsbecausethecoachingisnotworkingfortheVeteranandprogresshasstopped.Inthesecases,thecoachshouldassisttheVeteranindeterminingwhatotherservicesmaybehelpfultothemorassistthemindeterminingwhentheymightwanttotrycoachingagainandunderwhatcircumstances.
CoachesshouldassistVeteransinframingtheterminationofthecoachingsessionsnotasterminationperse,butasastepintheprocessofmovingtowardwhatmatterstothemandrealizingtheirMAP.Itisallpartofthejourney.
WHENUTILIZINGTHEFULLCOACHINGPROCESSISNOTFEASIBLEORPOSSIBLE
Therearemanytimeswhenutilizingthefullcoachingprocess,asrepresentedinthischapter,isnotfeasible,norpossible.Frequently,participantsintheWholeHealthCoachTrainingarenotintendingtodocoachingexclusivelybutareinterestedinaddingthecoachingskillstowhattheycurrentlydointheirVHAcapacities.Tothatend,trainingtimewillbedevotedtoutilizingcoachingskillsincarryingoutpartsofthecoachingprocessthataremostrelevantgivenlimitedtimeframes.ThefollowingPowerPointslidesofferaglimpseintohowelementsofthecoachingprocessmaybeutilizedinlimitedtimeframes.
• IfaVHAemployeehadanopportunityintheircurrentjobtoaskonequestion,itmaybeonelikethis:
• Iftherewasanopportunitytoexplorefurther,scalingquestionsmightbeutilized:
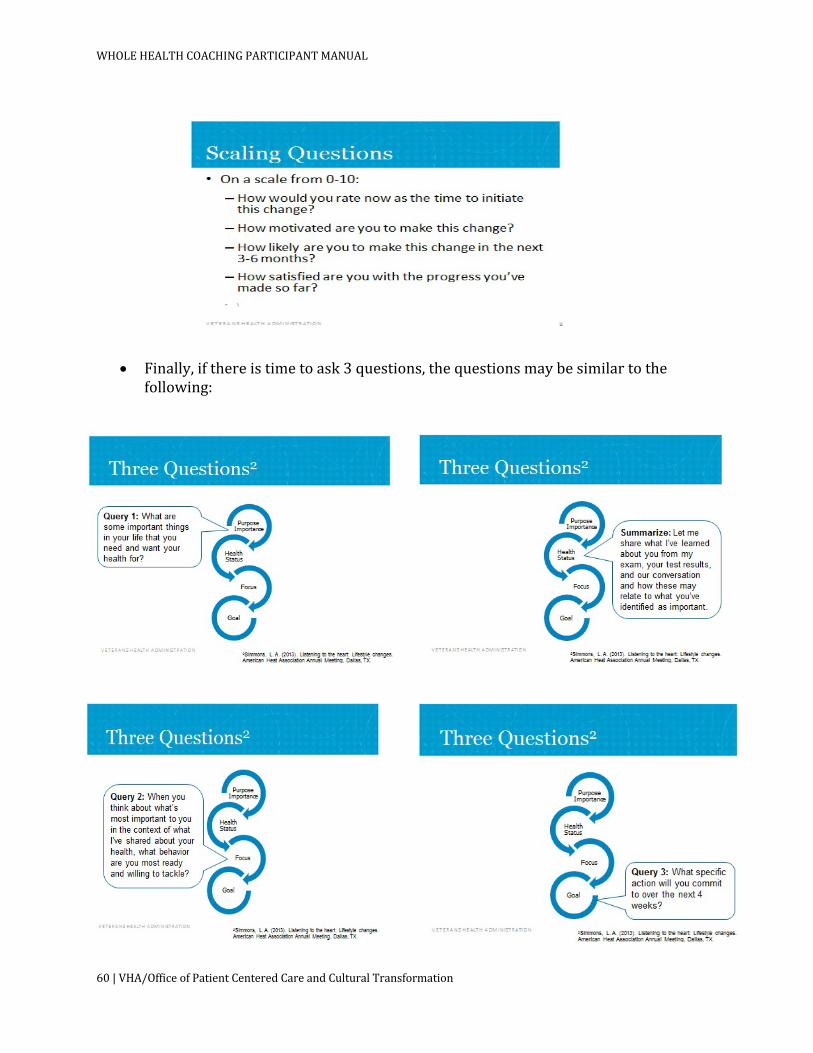
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
60|VHA/OfficeofPatientCenteredCareandCulturalTransformation
• Finally,ifthereistimetoask3questions,thequestionsmaybesimilartothefollowing:
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|61
CHAPTER5:ENHANCINGYOURWHOLEHEALTHCOACHINGSKILLS
Thereareseveralwaystothinkaboutenhancingyourhealthcoachingskills.Onewaytoenhanceyourhealthcoachingskillsistopracticewithpeers.Createcommonsituationswhereyouwouldliketouseyourhealthcoachingskillsand,withthegroup,brainstormpossibleresponses.
Perhapsitwouldbehelpfultoapplysomeratingscaleforhealthcoachingskillsdemonstrated.
Anotheristoseekoutamentororpeerwhoiswillingtoobserveyouandprovideyoufeedback.Somewaysthepeerormentormighthelpyouare:
1. Listento5-10minutesoftheinteractionanddescribewhichofthehelpingstyles(directing,following,orguiding)mightfit.
2. Thehelpermightusemorethanonehelpingstyleduringtheinteractionandyoumightbeabletoconsiderwhyaparticularstylewasusedforsomeparticularcontent.
3. Forthoseinstanceswhereadirectinghelpingstylewasused,itcanbeusefultoconsiderwhatwouldhavetobemodifiedsothatitwouldbemorelikeaguidinghelpingstyle.
4. Listento5-10minutesoftheinteractionandcountthenumberofopenandclosedquestions.
5. Acoachingstyleofteninvolvesmoreopenthanclosedquestions.6. Oneguidelineistohaveatleastasmanyopenquestionsasclosed,and
evenbetteristohavetwiceasmanyopenasclosedquestions.7. Onewaytopracticeistoconsidereachclosedquestionandgeneratea
correspondingopenquestionthatmighthavebeenusedinitsplace.8. Listento5-10minutesoftheinteractionandcountthenumberofsimple
andcomplexreflections.9. Acoachingstyleofteninvolvesmorereflectionsthanquestions.10. Oneguidelineistohaveatleastasmanyreflectionsasquestionsandeven
betteristohavetwiceasmanyreflectionsasquestions.11. Morecomplexreflectionsthansimplereflectionsarealsoconsidered
valuable.12. Onewaytopracticeistoconsidereachquestionandgeneratea
correspondingreflectionthatmighthavebeenusedinitsplace.13. Similarly,considereachsimplereflectionandperhapsgenerateacomplex
reflectionthatcouldhavebeenusedatthatpointintheinteraction.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
62|VHA/OfficeofPatientCenteredCareandCulturalTransformation
14. Listento10ormoreminutesoftheinteractionandcountthenumberofaffirmations.
15. Acoachingstyleofteninvolvesaffirmations.16. Listenformomentswhenyoucouldhavehighlightedwhatthepartnerwas
doingasadmirableorinspiredyou.
UTLIZINGAPEERSUPPORTGROUP
Ifyouwanttouseapeersupportgrouporapeerinterestgroup,youmightconsidertheseguidelines.YoumightconsiderincludingtheHealthBehaviorCoordinator(HBC)orothercolleagueswhohavereceivedthehealthcoachtraining.
1. Scheduleregularmeetingsforthesolepurposeofworkingtogethertostrengthenhealthcoachingskills.
2. Don’tletadministrativedetailsorotheragendafillthetime.
3. Anhourmeetingtwiceamonthwouldbeonepossibility.
4. Inearlymeetings,itmaybehelpfultodiscussspecificreadingsthattheparticipantshavedonebetweenmeetings,ortheirexperienceofaCommunityofPracticeCall.Ajournalclubof20minutesorsomightbeadded.
5. Ratherthansimplylisteningtoeachotherpracticecoaching,makeuseofsomestructuredcodingtools.Someexamplesare:
6. Countingquestionsandreflections.
7. Codingdepthofreflections(simplevs.complex).
8. Countingpartnerchangetalkandnotingwhatprecededit.
9. Trackingpartnerreadinessforchangeduringthesession,andkeymomentsofshift.
10. Thepersonwhodidtheinterviewmightcommentfirstonitsstrengthsandareasforimprovement.
11. Thegroupmayalsowatch“expert”tapes,codinganddiscussingtheskillsbeingdemonstratedinthem.AsktheOPCCiftheseareavailableforyouruse.
12. ThegroupmayalsowatchexamplesfromYouTubewhich,althoughoftendescribedasexamplesofcoaching,providemoreofastimulusforhowonemightimprovetheuseofcoachingskillsthanademonstrationofgoodcoachingskills.
13. The group may focus on practicing and strengthening specific components ofcoachingskills.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|63
SUGGESTIONSFORCREATINGAHEALTHCOACHINGENHANCEMENTPROGRAM
Generallyspeaking,itisnotenoughtosimplyattendahealthcoachingtraininginordertobeaneffectivehealthcoach.Likewise,itisseldomsufficientforanorganizationtosimplyprovideacoachingtraininginordertosustainahealthcoachingprogram.Inorderfortheinitiallylearnedskillstobeenhancedanddeveloped,anongoingsupportsystem,includingeffectivefeedbackandmentoring,needstobeestablished.And,thehealthcoachmustcontinuetopracticeandreceivefeedbackabouttheskillslearnedintheinitialtraining.Ideally,eachsitewillhavealeaderoradministratortoarrangemeetingsandcoordinateongoingactivitiesthatsupportskillenhancementandprogramdevelopment.Meetingonaregularbasistosupporteachotherinenhancinganddevelopingskillsiscritical.Evenifthesitedoesnothaveanexperiencedmentorortrainer,thereismuchthatcanbedonethroughpeersupport.Oneadvantageofnothavingaleadmentororsupervisoristhatthecoacheslearntomorefullyrealizetheirownpotentialtosupporteachotherinmakingimprovements,withlessrelianceonthe“experts.”
Ifyouare“onyourown”asahealthcoach,thereareideaslistedhereinthesecondsectionthatyoucanusetoenhanceyourskillsaswell.
ESTABLISHINGAHEALTHCOACHINGSUPPORTNETWORKATYOURLOCALSITE
Thereareseveralimportantfactorsthatleadtoasuccessfulcoachingprogram.Evidencehasshownthatnomatterhoweffectivetheinitialtrainingexperience,thelearningwillnotbesustainedwithoutotherfactorsbeingconsidered.Infact,itcouldbearguedthattheinitialtrainingexperienceisnotthemostimportantfactor;thereareseveralotherissuestoaddressthatmaybeofequalormoreimportance.Thetablethatimmediatelyfollowsallowsforanassessmentofsomeofthemostimportantfactorsinsettingupahealthcoachingprogram.
Asasummaryoftheassessment,theprimaryfactorstoconsiderare:
• Weretherightpeopleselectedforthetrainingtobehealthcoaches?• Wasthetrainingadequateandgearedtotheleveloftheparticipants?• DoestheHealthCoachingProgramhaveleadershipsupportatalllevels?• DoPerformanceMeasuresadequatelysupporttheworkofHealthCoaches?• Isthereanongoingsupportsysteminplacetoencouragethefurtherenhancement
ofcoachingskills?• Areindividualcoachesprovidedspecificfeedbackandskillenhancementplans?• Isthereanongoingevaluationprocessinplacetoassistindeterminingthe
effectivenessoftheprogram?• DoestheProgramhaveconsultantstheycanutilizetoassistinestablishingtheir
Program?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
64|VHA/OfficeofPatientCenteredCareandCulturalTransformation
WHOLEHEALTHCOACHINGTRAININGIMPLEMENTATIONASSESSMENT
Program/CourseAssessed___________________________ ByWhom____________________________
ForWhom_____________________________________________ Date__________________________________QuestionsforConsideration Ratingor
NumberComments
ExtentofProgram NumberofProgramstobeEstablishedbyWhen?
NumberofVeteranstobeServedbyCoaching?
Other OutcomesDesired Vision,Mission,andStrategicInitiativeshavebeenestablished
12345
Milestoneshavebeenestablished 12345 DesiredOutcomeshavebeenclarified 12345 ValuesofProgramhavebeenPrioritized(reduceddependenceonservices,VeteranSatisfaction,cost-benefit,improvedbiomarkers,goalachievement)
12345
Other ProgramAlignswithNBHWCProjectedAccreditationStandards
Numberofpre-Servicetraininghoursmeetprojectedstandard
12345
Numberofdocumentedpracticehourshasbeenestablished
12345
Numberofmentoredhourshasbeenestablished
12345
Mentors,trainers,andsupervisorsmeetprojectedNBHWCcriteria
12345
Contentofpre-servicetrainingmeetsnationalstandard
12345
Knowledgetesthasbeendeveloped 12345 Performancetesthasbeendeveloped 12345 SelectioncriteriahasbeenestablishedthatmeetsNBHWCrequirements
12345
OngoingCEUswillbeavailableforhealthcoaches
12345
ScreeningWHCApplicants AneffectiveWHCapplicantscreeningtoolandprocessisinplace
12345
Other Pre-ServiceTraining
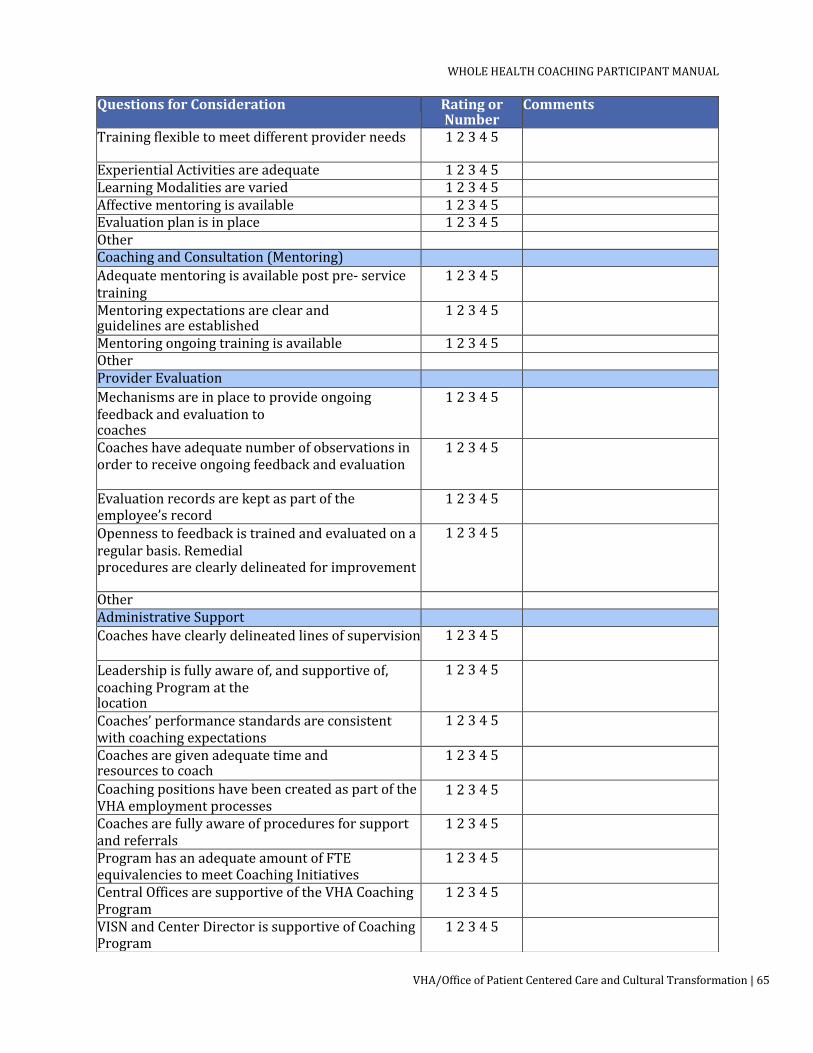
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|65
QuestionsforConsideration RatingorNumber
Comments
Trainingflexibletomeetdifferentproviderneeds 12345
ExperientialActivitiesareadequate 12345 LearningModalitiesarevaried 12345 Affectivementoringisavailable 12345 Evaluationplanisinplace 12345 Other CoachingandConsultation(Mentoring) Adequatementoringisavailablepostpre-servicetraining
12345
Mentoringexpectationsareclearandguidelinesareestablished
12345
Mentoringongoingtrainingisavailable 12345 Other ProviderEvaluation Mechanismsareinplacetoprovideongoingfeedbackandevaluationtocoaches
12345
Coacheshaveadequatenumberofobservationsinordertoreceiveongoingfeedbackandevaluation
12345
Evaluationrecordsarekeptaspartoftheemployee’srecord
12345
Opennesstofeedbackistrainedandevaluatedonaregularbasis.Remedialproceduresareclearlydelineatedforimprovement
12345
Other AdministrativeSupport Coacheshaveclearlydelineatedlinesofsupervision 12345
Leadershipisfullyawareof,andsupportiveof,coachingProgramatthelocation
12345
Coaches’performancestandardsareconsistentwithcoachingexpectations
12345
Coachesaregivenadequatetimeandresourcestocoach
12345
CoachingpositionshavebeencreatedaspartoftheVHAemploymentprocesses
12345
Coachesarefullyawareofproceduresforsupportandreferrals
12345
ProgramhasanadequateamountofFTEequivalenciestomeetCoachingInitiatives
12345
CentralOfficesaresupportiveoftheVHACoachingProgram
12345
VISNandCenterDirectorissupportiveofCoachingProgram
12345

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
66|VHA/OfficeofPatientCenteredCareandCulturalTransformation
GeneralComments:
QuestionsforConsideration RatingorNumber
Comments
Mid-levelManagementandSupervisorsaresupportiveofCoachingProgram
12345
Other ProgramEvaluation AnongoingProgramevaluationprocessandtoolhasbeenclearlydevelopedandisinplace
12345
OngoingResearchandevaluationarepartoftheProgram
12345
Other ContinuumofServices Thereisacontinuumofservicesclearlyestablished 12345
ThecontinuumofservicesisadequatefortheVHAneeds
12345
Cliniciansareawareof,andclearlyinformedof,thecoachingservicesavailable
12345
Veteransareawareof,andclearlyinformedof,thecoachingservicesavailable
12345
Other StaffCoachingandWellness Avarietyofcoachingforstaffwellnessisavailable 12345
Supportisavailableforstafftotakeadvantageofwellnesscoaching
12345
Other MarketingofServices Veteransareadequatelyinformedofcoachingservices
12345
ClinicalStaffisfullyinformedofcoachingservices
12345
Other

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|67
CHAPTERSIX:GROUPCOACHING
TothispointintheManual,thefocushasbeenonindividualcoaching.However,groupcoachingisapotentiallypowerfulmodalitytowhichthecoachingstyles,processesandstrategiescanbeapplied.Groupcoachingoffersavarietyofopportunitiesandchallengescomparedtoindividualcoaching.Inthischapter,weexaminesomeoftheseopportunitiesandchallengesandprovideseveralframeworks,aswellastechniques,forhowgroupcoachingmightbeconducted.Aswiththeindividualcoachingchapters,we
willprovideasetofpotential“maps”forgroupcoaching.However,theactualgroupjourneymaynotunfoldaccordingtoanyparticularmaporframework.Thesesuggestedframeworksareonlyastartingpointforcoachestobeginconceptualizinghowtheymaywanttoinitiateandconductgroupcoaching.
OPPORTUNITIESWITHGROUPCOACHING
Groupcoachingprovidesopportunities,oradvantages,forcoaches,Veterans,andorganizations.Someoftheseadvantages/opportunitiesare:
VETERANS’ADVANTAGES/OPPORTUNITIES
• Learnfromeachother.Veteransareabletohearfromothersabouttheirchangeprocessesandthinkabouthowtoapplywhattheyheartotheirownlearningandchangeprocess.
• Supporteachother.Asgroupmembersdevelopcamaraderie,theyareabletooffersupporttooneanother,bothduringthegroupmeetingsaswellasoutsidethegroupsetting.Veteranshaveasharedsenseofmissionandaregenerallyverysupportiveofoneanother–thiscanbeharnessedtotheirbenefitingroupcoaching.
• Reducedcost.Veteransmightrealizeareducedcostforgroupsessionsincomparisontoindividualsessions.
• Learnwithothersinsimilarsituation.NotonlydoVeteranslearnaboutthechangeprocessbylisteningtoothergroupmembers,buttheyalsomaylearninformation,especiallyiftheyareworkingonasimilarissue(i.e.,diabetes,heartdisease).
COACHES’ADVANTAGES/OPPORTUNITIES
• Workwithseveralindividualsatonetime.CoachesareabletoworkwithseveralVeteransatonetime;thishastheadditionaladvantageofaccomplishingmoreVeterancoachinginagiven timeframe.
Ifyouwanttogoquickly,goalone.Ifyouwanttogofar,go
together.
– Africanproverb
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
68|VHA/OfficeofPatientCenteredCareandCulturalTransformation
• Allowsforcoachingbyexample.Veteransobservethecoachcoachingothergroupmembersand,inmanycases,beabletoapplywhattheyareobservingtotheirown situations.
• Severalsourcesforlearning.GroupVeteranswillnotonlylearnfromthecoachbutwilllearninformationaswellaschangeprocessesfromothergroupmembers.
ORGANIZATIONALADVANTAGES/OPPORTUNITIES
• Abilitytogetmemberscoachedinashorterperiodoftime.Largeorganizations,whowanttoimpactoverallhealthoftheorganization,willbeabletogetthe
• target audience trained/coached in a shorter expanse of time compared to individual coaching.
• Reducedcosts.Groupcoachingmightbelessexpensivetoanorganizationthanindividualcoaching.
• Supportforteameffort.Byworkingingroups,asopposedtoindividualcoaching,membersoftheorganizationwillmorelikelydevelopsupportforeachotheranddevelopa“teameffort”approachwithintheorganization.Thiswillespeciallybethecaseiftheorganizationhaschosentotargetspecifichealthbehaviors.
Groupcoachingalsopresentssomeuniquechallengesthatmaynotbeencounteredasfrequentlyinindividualcoaching.Thesechallengesinclude:
• Balancingequaltimeforgroupmembers.Inmanygroups,someVeteranswilltendtotalkmorethanothers.Attimes,itcanbeachallengeforthecoachtogiveallmembersequalopportunitiestospeak.Respectfulgroupmanagementiskeyinthese
• situations. • Notallgroupmemberswillbesupportiveofeachother.Notallgroupmembers
may“like”eachotherorwanttosupporteachother.Theremaybeconflictsamonggroupmembersthatmustbeaddressedinorderforthegrouptofunctioninaneffectivemanner.
• Groupmaytakeonanegativedynamic.Groupscantakeonmanydynamics,impactingtheeffectivenessofthegroup.Ifsomegroupmembersbecomeunhappywiththeirexperienceitcouldimpactthegroupdynamicsinanegativeway.
• Groupmembersmaybeindifferentplacesinchangeprocess.Morethanlikelygroupmemberswillbeindifferentplacesinthechangeprocess.Whilesomewill stillbedecidingonafocus,othersmaybereadytotakeaction.Thismay
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|69
providesomelearningopportunities,butalsomayprovidechallengesforthecoach.
• Groupmembersmaynotalwaysbepresentforeachsession.Withindividualcoaching,ifaVeteranisunabletomakethesession,itcanfrequentlyberescheduled.Withgroups,itwouldbemuchmoredifficulttorescheduleforthesakeofoneortwogroupmembers.Ifgroupmembersareunabletoattenditwillhaveanimpactongroupdynamicsandthenon-attendingmemberswillbeatadisadvantageinnotexperiencingtheeventsofthesessiontheymissed.
• Maintainingawarenessofbothgroupandindividualdynamics.Asinanygroupprocessthereisanartandchallengetostayingawareofbothgroupdynamicsandindividualmember’sprocesses.Ifcoachesfocustoomuchonindividual
• member’s processes, they may “lose” other group members. If the focus is on group dynamics, members may think that not enough time is being devoted to their individual needs.
• Membersmaybeworkingondifferenthealthissues.NotonlywillVeteransbeindifferent places in the change process, but they may also be working ondifferenthealth
• issues. This may be a challenge if members are not able to extrapolate from another member’s content area and apply it to their own.
• Confidentialitymaybeanissue.Coacheswillnotbeabletocontrolwhatothergroupmembersdowithdisclosuresinthegroup.Althoughconfidentiallyshouldbeaddressed,itdoesnotassurethatallgroupmemberswilladheretotheconfidentialityagreements.
SETTINGUPAGROUP–SOMECONSIDERATIONS
Thereareamultitudeofdecisionscoacheswillneedtomakebeforesettingupgroupcoachingsessions.Asthegroupcontinuesitsprocess,additionaldecisionsmayneedtobemadealongtheway.Thesedecisionpointswillbeoutlinedbelowalongwithideasforconsideration.
GroupSize.Therearemanyfactorstoconsiderwhendetermininghowlargeacoachinggroupshouldbe.Thesefactorsinclude:
• Availability.HowmanyVeteransareavailableatanygiventime?Iftoomuchtimeelapseswhileagroupiswaitingtoform,Veteranswhosignedupinitiallymaybecometiredofwaitingtoget started.
• Amountofindividualtime.Tosomeextent,coachesneedtodecideaheadoftime howmuchapproximatetimetheywanttoprovideforeachgroup
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
70|VHA/OfficeofPatientCenteredCareandCulturalTransformation
member.This willhaveimpactonthenumberofgroupmembers.Ifagroupbecomestoounwieldyintermsofnumbers,individualmayfeel“lost”inthegroup.Ifagroup istoosmall,groupmembersmaynotbenefitasmuchfromlearningfromothers.Tosomeextent,thiswillbedeterminedbythevaluesofthecoaches,andhoweffectivetheybelievetheycanbeinlargerorsmallergroups.
• Costeffectiveness.IftheVHAisconductinggroupcoaching,theymayhaveacertainnumbertheywanttogetcoachedeachtime,giventheunitcost.
OpenorClosedGroup.Inaclosedgroup,allmembersbeginandendatthesametime.Nonewmembersareallowedtojointheclosedgroup.Inanopengroup,sessionsareongoingwithmembersleavingorjoiningatdifferenttimesandfordifferentlengthsoftime.Theadvantageofaclosedgroupistheintimacyandtrustthatgetsestablishedamonggroupmembers.Also,allmembersareawareofwhathasbeensharedhistoricallywitheachmember.Therewillnotbememberscomingandgoing.Anopengrouphassomeadvantagesaswell.Veteransdonothavetowaittojoinandhavefreedomtoenter/leavethegroupaccordingtotheirownwants/needs.
Veteranscancomeandgoaftertheybelievetheyhaveachievedwhattheywanttoachieve.Withnewmemberscomingintoagroup,thegroupdynamicschange;newideasandnewdynamicscanbestimulatingtothegroupprocess.
TelephonicorIn-PersonSessions.Thecoachwillneedtodecidethenumberofsessionsthegroupwillmeetinpersonandthenumberoftelephonicsessionswillbeheld.Grouptelephonicsessionscanpresentnewchallengesbeyondthoseofindividualtelephonicsessions.Itmaybedifficulttoassessgroupmembers’processwithmorethanonepersononthephone.Itrequiresalotmore“checkingin”toseewheregroupmembersare.Groupdynamicsmaybemoredifficulttoassesswithoutthenon-verbalcues.Theadvantagesoftelephonicsessionsarethesameasfortelephonicindividualsessions.Theyrequirelesstraveltime,aneedforspace,andallowforgreaterflexibilityintermsofhavingtobeinacertainlocation.
Ifcoachesusetelephonicsessions,theymaywanttoaddressthefollowing:
• Apersonalcommitmentnottomulti-taskwhengroupmembersareonthephone.
• Groupmembersmayneedtoidentifythemselveswhentheybegintospeak.• Groupmemberscommittolisteningwhenothersarespeaking.• Toreduceoreliminatebackgroundnoisewhenparticipatinginthetelephonic
group.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|71
SingleThemed.Agroupcouldbefocusedonasinglehealthconcernsuchasdiabetesorheartdisease.Asingularlyfocusedgrouphasseveraladvantages:
• Groupmembersmayfeelagreaterbondwhendealingwithsimilarissues.• Groupmemberswillmorethanlikelyfeelasiftheyarewithotherswho
understandwhattheyaregoing through.• Groupmemberswilllearninformationfromeachotherthatpertainstotheir
issue.• Coachescanbemorefocusedonwhatinformationtopresent.• Chancesaregreatertheywillcontinuetosupporteachotherafterthegroup
sessionsareover.LengthofGroupProcess.Thecoach(ortheorganization)needstodecidehowmanysessionsthegroupwillbeandoverwhatperiodoftime.Thismaybeeasiertonegotiatewithanindividual.Inthecaseofagroup,thecoachmayhavetodeclarethelengthofthegroup.Itmaybedifficulttodeterminealengthiflefttoa“democratic”process.
• Lengthoftimeandhowmanysessionswillalsobeinfluencedbythepurposeofthegroup.Somegroupscouldbeopen-endedintermsoflength,especiallyifgroupmemberswantedtoworkonseveralissuesorserialissues(i.e.,oneright
• afteranother).Agroupthathasaspecificissuewithaspecificoutcomecanmoreeasilylimitthenumberofsessionsanddurationofthegroup.
• Timebetweensessionswillalsohavetobedetermined.Coacheswanttogivegroupmembersenoughtimetoprocessand/ortryoutnewactions.However,toomuchtimebetweensessionscouldbedetrimental,especiallyforthosewhoarestrugglingwithexecutingnewactions.Manycoacheswouldfindthatformostgroups,anythinglessthanoneweekbetweensessionsistooshortandanythingover2weekswouldbetoolong.
EducationalComponent.Again,dependingonthepurposeofthegroup,itmaybeadvantageoustohaveaneducationalcomponent.Ifthegrouphasasingularhealthissuetheyaredealingwith,guestspeakerswithexpertiseinthathealthissuemaybebeneficial.Ifthecoachisknowledgeableinthehealtharea,theymaywanttoprovidesomeeducationoreducationalresources.Also,thegroupmemberscouldbetaskedtofindoutinformationonvariousaspectsofthehealthissue.Aswithindividualhealthcoaching,coachesmustbecarefultoavoidgivingmedicaladvice.Likewise,ifthematerialcomesfromgroupmembers,itshouldnotbeconstruedasthesameasexpertmedicaladvice.Coachesshouldsuggesttogroupmembersthatanyinformationtheymayreceiveinthegroupshouldbecheckedoutwiththeirmedicalproviders.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
72|VHA/OfficeofPatientCenteredCareandCulturalTransformation
AmountandTypeofGroupStructure.Somegroupscouldoperatewithverylittlestructureandbesuccessful.Coachescouldbeginsessionswithveryopen-endedquestions,suchas“Whathaveyoulearnedsincelastsession?”andessentiallygofromthere.Theycouldusewhateverarisesinthesessiontomakesalientpoints.Or,coachescouldbeverystructured,planningthequestionsandformatthatwillbeusedforeachsessionandstrictlyfollowingthosequestionsandformat.Theformatandstructurewillbedeterminedbytheoutcomeintentofthegroup.Forinstance,agroupthathasbeenstructuredaroundweightlossmayrequiregreaterstructurethanagroupwhoseintentistoimproveeachmember’soverallhealth.
CoacheswillalsohavetodetermineiftheyaregoingtotakethegroupthroughtheWholeHealthCoachingProcessasagroup,orifeachmemberwillbecoacheddependingonwheretheyareintheprocess.Forinstance,coachescouldstartoutagroupbyhavingeverygroupmembertalkabouttheirvisioninthefirstsession.Thegroupdoesnotmoveontovaluesuntileveryonehashadachancetodefinetheirhealthvision.Likewise,thegroupdoesnotmoveontoGoalSettingandPlanninguntileverygroupmemberhaschosenafocus.Clearly,agroupsetupthiswaywillhaveuniquechallenges.Mainly,groupmemberswillbereadytomoveatdifferenttimesandtheywillhavetowaitontheirfellowgroupmembers.
Bycontrast,agroupcouldbesetupsothateverygroupmembermovesthroughthecoachingprocessattheirownpace.Groupmemberswhoarenotnecessarilyinthesamestagecouldstilllearnfromlisteningtoothergroupmembersatthatstage.Coachesneedtobeadeptatrememberingandaddressingeachindividualwheretheywereintheprocess.Theywouldalsohavetobeskilledatpointingoutthelessonsthatcouldbelearnedfromgroupmemberswhoareindifferentstagesintheprocess.
Itmaybehelpfultothinkofsessionshaving3phases:
1) Beginningofacoachingsession-Thebeginningofthecoachingsessionstartswith
someformofcheck-in,whichisusuallyanopen-endedquestionaddressedtoeveryone.Potentialopeningquestionsare:a) “Whatdidyousucceedwiththisweek?”b) “Whatoneworddescribesyourweek?”c) “Whatthemewouldyouusetodescribeyourweek?”
Somecoachesmightwanttobeginwithamindfulawarenessactivitytoassistgroupmembersinbecomingpresent.
2) Bodyofacoachingsession-Thebodyofthecoachingsessionoftenincludesprocessing

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|73
themembers’experiencessincethelastsession.Morespecifically,theprogresstowardgoalsandovercomingchallengeswillusuallytakethebulkofthetime.Questionsmaybe:a) “Whatsuccessesdidyouexperiencethisweek?”b) “Whatwasachallengeforyouthisweek?”c) “Wheredidyouexperienceexcitement?”
3) Endofacoachingsession-Letmembersknowyouhaveanallottedamountoftime
left.Aswiththecheck-in,itisimportanttohearfromeveryoneduringcheck-out.Questionsmightinclude:a) “Whatareyoutakingawayfromthisgroupthisweek?”b) “Whatnewbehaviorwillyoudothisweek?”c) “Whatwouldyoulikeus/metoholdyouaccountabletoduringournext
session?”
MissedSessions.Coacheswillneedtoaddress,aheadoftime,howmissedsessionswillbehandled.Willtheabsentmemberneedtomakeupthesessionsomehow?Willtheyhavetolistentoatapeofthesession?Willtheyneedtobebroughtuptodateonwhattheymissed?
BlendingGroupandIndividualInterventions.Onechallengeforcoachinggroupsisbalancingtheamountoftimespentonanyoneindividualandgivingtimetotheoverallgroupprocess.Onewaytobalancethisprocessistostaymindfuloftheamountoftimeyouasacoacharedevotingtothefollowing:
• Coachingindividualgroupmembersandbringingtherelevanceforwardtoallgroupmembers.
• Coachingthewholegroup,askingquestionsforthewholegrouptoconsider,andlisteningforcommonthemesaswellasdifferences.Useresponsestoweaveinteachablemomentsforthewholegroup.
• Groupmemberscoachingeachothercanhavearealimpactforthegroup.Thecoachmayhavetoinvitegroupmemberstocoachbyaskingquestionssuchas“Ifyouwerethecoach,whatwouldyousay,orwhatwouldyouasktheVeteranrightnow?”Thistakesthefocusoffthecoachastheonlyonewhoisabletocoachandallowsformoregroupinteractionsasopposedtoeveryinteractiongoingthroughthecoach.Itmightbeimportanttoremindgroupmembersthatthisisnotanopportunitytoofferadvice,asagreeduponinthegroupdesign/groundrules.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
74|VHA/OfficeofPatientCenteredCareandCulturalTransformation
DEALINGWITHDIFFICULTGROUPBEHAVIORORGROUPPROCESSES
Groupscanpresentuniquechallengesthatwillnotlikelybeencounteredinindividualcoaching.Managingthesedifficultiesmayrequireadditionalpracticeandexperiencetobeaneffectivegroupcoach.Someofthesedifficultgroupsituationsmightbe:
Situation:Memberswhomonopolizeorramble
Intervention:“Irespectyourviewpointandamgratefulforyourwillingnesstoshare.Ialsowanttohearfromotherpeopleinthegrouponthistopic.”
Sometimes,groupmembersarenotawareofhowmuchtheyinteractcomparedtoothers.Twowaystoaddressthisare1)Askthewholegrouptobeawareofhowmuchtheyasgroupmembersareinteractingcomparedtoothersor2)Addressitdirectlywiththegroupmember,perhapsonabreakorafterthegroupsession.
Situation:Memberswhotendtocomplainincessantly
Intervention:“Ihearthatthisisupsettingforyou.I’dliketogiveyouanotherminutetoexpressyourviewandthenI’dliketohearfromothers.”
Situation:Memberswhogivefrequentadvicetoothers
Intervention:(Assumingnotgivingadvicehasbeensetupasagroundrule)“Ihearwhatyouareofferingnowasadvice.Howcouldyouchangeyourapproach,andaskaquestionthatwouldallowthepersontoexplorewhatyouareoffering?”
Situation:Sidebarconversations.
Intervention(Assumingthishasbeensetupasagroundrule)Eyecontactwith thesidebarmembers.Ageneralreminderaboutthegroundrulesandsidebarconversations,“Wedidspeakaboutsidebarconversationsinthegroundrules–itishelpfultorememberthem”.Usingproximity(standingnearby)tobringattentiontothespeakers,andthenperhapsaskingparticipantstochangeseatstoseparatethem.Finally,simplyaskingthemtorefrainfromsidebarconversationsforthesakeofthelargergroup.
Someofthesedifficultsituationscanbeavoidedoratleastaddressedbysettingupgroundrulesinthebeginningsession.Memberscouldthenberemindedofthegroundrulesthroughoutthesessions.
SETTINGUPTHEINITIALGROUPSESSION
Thereareseveraltaskscoacheswillwanttobemindfulofastheybeginthefirstsessionofgroupcoaching.Someofthesearesimilartoindividualcoachingfirsttasksbutmaytakeon

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|75
adifferentflavorwhendoingtheminagroupsetting.Thesetasksarepartofdesigningthegroupcoachingalliance:
• Introduceyourselfandyourintentorgoalforthegroup.Youmaywanttoconsiderintroducingyourselfwhenothergroupmembersintroducethemselves,providingthesameinformationtheyprovide.Thiswillcontributetoadifferentgroupdynamicthanifyouintroduceyourselfdifferently,oratanothertimeintheprocess.
• Createguidelinesorgroundrulesforthegroup.Itemssuchasconfidentiality,bottomlining,notgivingadvice,howmemberswillcommunicatewithoneanother,andattendanceareallissuesthatcouldbeaddressedduringthistime.Coachesmaywanttoprovidesomeofthegroundrules,whileothersmaybegeneratedfromthegroup.Generally,memberswilltakemoreresponsibilityandownershipforcarryingoutorenforcinggroup-generatedgroundrules.
• Emphasizethatthegroupwillbeinteractive,focusedondialogueandnotbesimplytheforumforthecoach.
• Providethegroupinformationonthestructureofthegroupandhowyouenvisionthegroupprocesstakingplace.
• Besuretoallowadequatetimeforeachgroupmembertobeheardinthefirstsession.
• Providesomerelatively“safe”open-endedquestionsthatallgroupmemberscanrespondto.
ENDINGTHEGROUPEXPERIENCE–THELASTSESSION
Thereareseveralpointscoacheswillwanttokeepinmindwhenendingthegroupexperience.Theseare:
• Areviewofwheregroupmembershavecomefromovertime,andwhatchangestheyhavemade,isusuallyveryusefulandmotivating.
• Havingmembersstatewhattheyhavelearnedthatcanbeappliedtootherareasoftheirlivescanbehelpfulinhavingthemidentifychangestrategies.
• Sharinglastthoughts,theymaywanttoexchangewithothermembersofthegroup.• Havinggroupmembersnotonlyidentifywhattheyhavelearned,butalsothink
aboutwhatotherareaoftheirlifetheymaywanttoworknext.• Feedbackforthecoachintermsofwhathasbeenhelpfulaboutthegroup,aswellas
howthegroupcouldbeimproved.• Exchangeofcontactinformationifappropriate.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
76|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER7:PRE-SESSION,FIRSTSESSION,ANDLASTSESSIONCONSIDERATIONS
Thischapteraddressessomeuniqueconsiderationsthatcoacheswillwanttoconsiderinbeginningandendingcoaching.
PRE-SESSION
CoachesmaywanttothinkofprovidingVeteransapacketofinformationthatincludesthefollowingbeforethecoachingsessionsstart:
Abriefdescriptionofwhatcoachingis.Veteransmaynotbefamiliarwithwhathealthcoachingis.Abriefbrochureonwhathealthcoachingis,andwhathealthcoachingisnot,mayprovidetheVeteranwithinformationaboutwhattheymaybeencountering.IfVeteransarereferredbyotherhealthcareprovidersortheirPACT,itwouldbeusefultobegivenabrochureorhandoutatthetimeofthereferralalongwithanopportunityfortheVeteranstoaskquestions.
AdescriptionofwhattheVeteran’sresponsibilitiesis,andwhattheCoach’sresponsibilitiesare,intheCoachingsessions.ThismayhelptoclarifywhatcoachingisfortheVeterans.Afewoftheseideasare:
• TheVeteranwillberesponsiblefortheagendaandwhattheywanttoworkon.• ThecoachingwillbeconductedinthecontextofwhatmatterstotheVeteran.• Coacheswillmakeeveryefforttoprovideasafeandsupportiveenvironmentand
willhonortheinterestsoftheVeterantoaddress(ornotaddress)whatevertheVeteranbringsup.
• Coachingisnotonlyaboutlearningandgaininginsight,butabouttakingactionaswell.
• TheVeteranwillbeexpectedtodothework;thecoachistheretoguidetheprocessandsupportthem.
Anyinventoriesorassessmentsthatthecoacheswouldliketohaveavailableforthefirstsession.Forinstance,somecoachesmaywanttheVeteranstocompletethePHIbeforecomingtothefirstsession.Ifthatisthecase,theyshouldprovidethePHIseveralweeksinadvancewithspecificinstructionsinfillingitoutalongwithsomeguidanceabouthowitwillbeused.
Anylogisticsaboutthecoachingsessions.Directionsonwheretogo,howtogetthere,thelengthofsessions,howmanysessions,expectationsforbeingontime,areallpartofthelogisticsthatshouldbeprovidedtotheVeteran.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|77
FIRSTSESSION
Thefirstsessioncanbeveryimportantindevelopingtrustandsettingthetoneforfuturecoachingsessions.Likeanyhelpingprofession,effortsshouldbemadetojoinwiththeVeteran,usingcommoncourtesieswhengreetingandmeetinganotherpersonforthefirsttime.AskingtheVeteranwhattheyneedtobemorecomfortablewouldbeanexample.Alsoaskingaboutwhatinformationtheywouldliketoknowaboutthecoachingsessionsmaybeimportant.
Providinga“healing”spacethatispeaceful,uncluttered,quiet,andnotpronetodistractionsorinterruptionswillbeimportantinpromotingafavorable“firstimpression”.CoachesshouldmakeeveryefforttobefullypresentfortheVeterans,perhapspreparingfortheencounterbypracticingsomemindfulawarenesspriortothesession.
TheVeteransmayhavequestionsaboutconfidentialityandwhoelse(otherproviders)willhaveaccesstoanyinformationtheymayshareintheirsessions.CoachesshouldbehonestwiththeVeteransandsharewhattheirroleisinrelationtoanyotheroftheVeteran’shealthcareproviders.
LASTSESSION
Endingthecoachingrelationshipcanassistinleavingafavorableimpression(andperhapsreferrals)fortheVeterans.Moreimportantly,askingtheappropriatequestionscanassistinpreparingtheVeteranforthefuturewithoutthesupportofcoaching.QuestionsfoundpreviouslyundertheGroupCoachingLastSessionsectionarealsoappropriateforindividualcoaching,thosequestionsare:
• AreviewofwheretheVeteranhascomefromovertime,andwhatchangestheyhavemade,isusuallyveryusefulandmotivating.
• HavingVeteransstatewhattheyhavelearnedthatcanbeappliedtootherareasoftheirlivescanbehelpfulinhavingthemidentifychangestrategies.
• Sharinganylastthoughts,theymaywanttoexchangewiththecoach.• HavingtheVeterannotonlyidentifywhattheyhavelearned,butalsothinkabout
whatotherareaoftheirlifetheymaywanttoworknext.• Feedbackforthecoachintermsofwhathasbeenhelpfulaboutthecoaching,aswell
ashowthecoachingcouldbeenhanced.• Sinceregoodbyes.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
78|VHA/OfficeofPatientCenteredCareandCulturalTransformation
SESSIONIIICONTENT
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|79
CHAPTER8:MINDFULAWARENESSANDCOACHINGPRESENCE
MindfulAwarenessandCoachingPresencearefoundationaltocoaching,andthetermsareoftenusedinterchangeably.Presenceisanessentialqualityandskillofaneffectivecoach.ItisaNBHWCcorecompetency.
“Coachiscalm,present,andemotionallyavailable”(NBHWCContentOutline1.1.1)
“Engage[s] in self-awareness practices, including emotional self-regulation”
(NBHWCContentOutline4.1.3)
Beingpresenttakespractice.Similartomusclememory,presencerequiresintention,awareness,andrepetition.
HOWMINDFULAWARENESSSUPPORTSTHECOACHINGPROCESS
Mindfulawarenessservesthecoachingprocessby:
• Enablingthecoachtotrackthesenseofconnection,energy,andfeelingsforbothselfandclient.
• Providingthecoachwithvaluableinformationtoguidethesessionmosteffectivelyinserviceoftheclient.
• Aidingthecoachinnoticingthoughts,judgments,andopinions. Thereisanemergingbodyofresearchtodocumenttheimpactofmindfulawarenessonsupportiveandtherapeuticpresence.Researchhasshownthatpatientoutcomesimproveevenwhenpatientsorclientshavenoideathattheirpractitionerwaspracticingmindfulawareness.Theclientalsodoesnotneedtoknowanythingaboutmindfulawarenesstoexperiencethisbenefit.Itsimplycomesfromthepractitioner’spresence.Oneexampleofaresearcharticledescribingthedetailsofthiscanbefoundatthislink:
https://www.attach.org/wp-content/uploads/2015/05/Therapeutic-Presence-and-Polyvagal-Theory-2014.pdf
MINDFULAWARENESSPRACTICES:FORMALVERSUSINFORMAL
Adistinctionismadebetweenformalandinformalpracticesofmindfulawareness.Bothtypesarepracticedwithintentionandbotharegenerallyseenascomplementingoneanother.Additionally,bothtypesofpracticesupportone’swell-beingandenhancecoachingeffectiveness.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
80|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Formalmindfulawarenesspracticeisthemeditationpracticeofremainingstill,usuallyinaseatedposition,oftenwitheyesclosed,whilenoticinginternalandexternalsensations.Suchpracticescanbeself-guidedorledbyanotherperson.Examplesincludeawarenessofbreathorsound,bodyscan,mindfulwalking,andmindfuleating.
Informalmindfulawarenesspracticemeansconsciouslybringingyourfullattentiontosomethingyouarealreadydoing,likewashingdishesorpettingthecat.Theideaistobringyourfullattentiontotheunfoldingexperience,andwhenthemindwanders,bringyourattentionback.
WHATMINDFULAWARENESSIS–ANDWHATITISNOT
Mindfulawarenesshasseveraldistinguishingfeatures.Theseinclude:
• Beingawareinthemoment,withcompassiontowardselfandothers.• Noticingexternalstimuli(sights,sounds).• Bringingattentiontointernalsensations(breath,body)andourresponsestothem.• Bringingattentiontoourmentalphenomena.• Listeningtothepersonal,innerwisdomofourowninterconnectedself-care
circles.
Meanwhile,thereareseveralotherusefulpracticesthatmayincorporatesomeoftheabovefeaturesbutarenotconsideredmindfulawareness.Someexamplesare:
• GuidedImageryandVisualization.• ProgressiveMuscleRelaxationandotherrelaxationpractices.
Otherpracticesaremoreformalapplicationsofmindfulawareness.Theseformalpracticesgobeyondsimplynoticingyourpresentmomentexperience,sowedistinguishthesefrommindfulawareness.
• YogaandTaiChi.• Meditation.• Mindfulness-basedStressReduction(MBSR).
Notethattheterms“mindfulawareness”and“Mindfulness”areoftenusedinterchangeablyineverydaylanguage.TheOfficeofPatient-CenteredCareandCulturalTransformation(OPCC&CT)drawsadistinctionwhichisdiscussedinfurtherdetailattheendofthischapter.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|81
STEPSFORGUIDINGAMINDFULMOMENT
Asacoach,itisappropriatetoguideVeteransinamindfulmomentatthebeginningofacoachingsession,sobothcoachandVeteranbecomepresentandgrounded.ThisshortpracticetrainstheVeterantobecomeawareofwhatthebodyandmindaredoing;thisskillmayalsohelptheVeteranlistendeeplytowhatreallymattersduringacoachingsession.Thefollowingaregeneralstepsthatcanbeusedtoguideamindfulmoment.
• Beginbyaskingpermission.• Encouragefindingacomfortableposition.• Inviteclosedeyes,loweredgaze,orsoftvisionfocus.• Bringattentiontothebreath(noticeinhalation,chest/bellyriseandfall,exhalation).• Whenattentionwanders,noticewithoutjudgementwhereitwent.• Gentlybringattentionbacktothebreath.• Allowpauses-thispermitspeopletopractice.• Bringpracticetoaclose.• Checkin(“Whatdidyounotice?”)
MINDFULAWARENESSVS.MINDFULNESS–VHARESOURCES
TheOfficeofPatient-CenteredCareandCulturalTransformation(OPCC&CT)makesadistinctionbetweenmindfulawarenessandMindfulness.MindfulawarenessisinthecenteroftheCircleofHealthandisaboutnoticing,beingfullypresent,andpayingattentiononpurpose.
MindfulnessfacilitationandinstructionrequiresspecializedtrainingandisbeyondthescopeofWholeHealthCoachtraining.ForcoacheswhoareinterestedinfacilitatingMindfulness,thereareresourcesinternalandexternaltotheVAthatwouldbehelpfultoexplore.Inparticular,trainingintrauma-sensitiveMindfulnessisespeciallyimportant,sothatpractitionerscanbehelpfulwithoutcausingharmtotheVeteranswithwhomtheywork.
Forthoseinterestedinlearningmore,thebestplacetobeginisbypursuingtrainingthroughareputableprogramandbeginningtopracticeyourself.Ifthepracticeresonateswithyou,youmaywanttopracticeinformalmindfulawarenesswithVeterans,payingconsciousattentiontotheunfoldingexperienceofyourinteraction.However,intheroleofcoach,andwithoutpropertraining,itisnotappropriatetoteachMindfulnesstoVeterans.Instead,allowyourcoachingpresencetogiveVeteransthesharedexperienceofmindfulawareness.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
82|VHA/OfficeofPatientCenteredCareandCulturalTransformation
MINDFULAWARENESSSCRIPTS
AsstatedpreviouslyintheMindfulAwarenesssectionofChapter2,MindfulAwarenessisnoticing,awareness,andattention.Mindfulawarenessisnotguidedimagery,relaxation,normeditation.Beforebeginningamindfulawarenessmoment,offersetupcommentsincludingaskingpermissiontoofferamindfulmoment.
INCLUDESET-UPCOMMENTS
• “I’dliketoofferamindfulawarenessmoment.Wouldthatbeokwithyou?”• “Thismaynotbeforeveryone”• “Closeyoureyesifyoulike,orleavethemopen”• “Disregardmyvoiceatanytime”• “Stopanytimeyouareexperiencinganydiscomfort”• “Rememberthisisabout‘payingattentiononpurposeandnotnecessarilyabout
relaxation.”
AWARENESSOFBREATHSCRIPT
• Settleinandfeelthesupportofthechairorfloor.• Allowyoureyestocloseorsetasoftgazearoundtheroom.• Remembertomaintainattitudesofnon-striving,non-judging,andpayingattention.• Thisisatimetoletgoofbusinessorlife’sconcerns.• Nowpayattentiontoyourbreathwhereveryouexperienceit.Don’ttrytochangeit,
justpayattentiontoit.Feelthebreathascompletelyaspossible,theinhaling,pausing,andexhalingofthebreath.Itmaybeeasiertofocusonyourbellyduringtheexperienceofbreathing.
• Whenyounoticethatyourattentionissomewhereelse,congratulateyourselfandgentlyreturntothebreath.Youwillprobablyneedtodothismanytimes.
• Noticethesoundofyourbreath,thewarmthofyourexhales,andthecoolnessofyourinhales.
• Ifyounoticeoutside(orinside)distractions,simplynoticethem,andthenpatientlyreturnyourfocusbacktoyourbreathing.
• Noticethelengthanddepthofeachbreath.• Practicethiswayaslongasyouwish.• Allowyourselftorestandlookmoredeeplyasyousettleintothis.• (Aftertimeisup)Whenready,youmayendyourmindfulawarenesssessionby
simplyopeningyoureyes.
PRACTICEOFMUSCLEAWARENESSSCRIPT
First,findacomfortableposition,withyourbackfeelingsupportedbythechairandyourfeetsupportedbytheground.Sometimeswesaysittingwithafirmbackandanopenheart.Takeadeepbreath;letitoutslowly.Whatwe’llbedoingisalternatelytensingandrelaxing

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|83
specificgroupsofmuscles.Aftertension,amusclewillbemorerelaxedthanpriortothetensing.
Concentrateonthefeelofthemuscles,specificallythecontrastbetweentensionandrelaxation.Intime,youwillrecognizetensioninanyspecificmuscleandbeabletoreducethattension.
FocusontensingonlythespecificmusclegroupIcalloutateachstep.Trynottoholdyourbreath,grityourteeth,orsquint.Breatheslowlyandevenlyandthinkonlyaboutthetension-relaxationcontrast.(Notetofacilitator:Eachtensingisfor6seconds;eachrelaxingisfor6seconds.Notethateachstepisreallytwosteps—onecycleoftension-relaxationforeachsetofopposingmuscles.)Aswithothermindfulawarenesspractices,youmaynoticeyourmindwanders.Ifitdoes,justgentlybringitbacktothesensationsinyourbody.Youmaycloseyoureyesorsetasoftgazearoundtheroom.
(Optionalinstruction:Iwillcountslowlytosixwhileyoutenseandrelaxeachmusclegroup.)
1. Hands.Tenseyourhands,makingafist(6secs).Nowrelaxyourhands,fingers
relaxedinyourlap(6secs).
2. Bicepsandtriceps.First,makeamuscle—shakingyourhandstomakesureyouarenottensingthemintoafist(6secs).Nowrelax,droppingyourarmstothechair(6secs).Nowtenseyourtriceps,tryingtopushyourstraightenedarmstowardstheback(6secs).Nowdropthemandrelax(6secs).
3. Shoulders.Pullyourshouldersback(6secs)andthenrelaxthemtoneutral(6secs).Pushtheshouldersforwardasifhunching(6secs).Andthenrelaxthemtoneutral(6secs).
4. Neck(lateral).Withtheshouldersstraightandrelaxed,turnyourheadslowlytotheright,asfarasyoucan(6secs);nowrelaxtothefront(6secs).Turnyourheadtotheleft(6secs);andrelaxtothefront(6secs).
5. Neck(forward).Digyourchinintoyourchest(6secs);nowrelax,bringingtheheadforwardtoneutral(6secs).(Tiltingtheheadbackisnotrecommended).
6. Mouth.Openyourmouthasfaraspossibleandhold(6secs);nowrelaxthemouth(6secs).Bringyourlipstogetherandpursedastightlyaspossible;hold(6secs);nowrelax(6secs).
7. Eyes.Openyoureyesaswideaspossibleandhold(6secs);nowrelax(6secs).Closeyoureyestightly,holdingasquint(6secs);nowrelax(6secs).
8. Back.Withshouldersrestingonthebackofthechair,pushyourbodyforwardso

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
84|VHA/OfficeofPatientCenteredCareandCulturalTransformation
thatyourbackisarched(6secs);nowrelax(6sec).
9. Butt.Tensethebutttightlyandraisepelvisslightlyoffchair(6sec);nowrelax(6secs).
10. Thighs.Raiseyourstraightenedlegsabout6”offthefloororthefootrest–trynottotensethestomachasyoudothisandhold(6secs).Nowrelax(6secs).
11. Stomach.Pullinthestomachasfaraspossibleandhold(6secs);relaxcompletely(6secs).Pushoutthestomachortenseitasifyouweregettingreadyforapunchinthegut(6secs);nowrelax(6secs).
12. Calvesandfeet.Pointthetoes(withoutraisingthelegs)andhold(6secs);relax(6secs).Pointthefeetupward,asifyouwerepullingyourtoestoyourshinsandhold(6secs).Nowrelax(6secs).
13. Toes.Withlegsrelaxed,digyourtoesintothefloor(6secs);relax(6secs). Thatconcludesourbodyscanwithmusclerelaxationexercise.Takeacoupleofdeepbreaths,openyoureyesiftheyareclosed,andlet’scontinuebydiscussingtheexperience.
MINDFULEATINGSCRIPT
FacilitatorInstructions:Thisexercisecanbedonewithoneorseveralfooditems.Itmaybeadvantageoustohaveseveralsmallfooditemsavailable,sotheparticipantcanmindfullynoticethechoiceofanitemtheychose.Youwillhavetoplanaheadtomakesuretohavefooditem(s)available.
1. Startbyfindingacomfortablesittingposition.
2. Takethreeslow,deepbreathsandnoticehowyoufeelphysically.
3. (ifapplicable)Payattentiontothechoiceoftheitemyouchose.Onwhatbasisdidyouchoosethisitem?
4. Placethefooditeminyourhand.Don’teatitquiteyet.Noticehowyouwouldnormallyputtheiteminyourmouthwithouttakingthetimetofullyappreciateit.Nowpretendthisisthefirsttimeyou’veeverseenthefooditem.
5. First,feeltheweightofthefooditeminyourhand.Isitheavierthanyouimagined?
6. Now,takealookatthefooditem.Seeitasifforthefirsttime.Whatdoyounoticethatyoumayhavenotnoticedbefore?
7. Imaginewheretheitemcamefrom.Wasitproducedlocallyorbroughtoverfromaverydifferentplace?Thinkabouthowmanypeoplewereinvolvedinbringingthisitemtoyoutoday.
8. Slowlybringtheitemclosetoyournose.Doesithaveasmell?Doesthatsmell

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|85
remindyouofaneventfromthepast?
9. Continuetonoticeanypositiveandnegativethoughtsyouhaveabouttheitem.Noticewhatyoumightbeexpectingittotastelikeatthispoint.Isyourmouthstartingtomakesalivainanticipationofeatingthefooditem?
10. Eversoslowly,placetheiteminyourmouth,withoutbitingintoit.Useyourtonguetopushtheitemagainsttheroofofyourtongueandthenagainstthebackofyourteeth.
11. Keepthefooditeminyourmouthforatleast10moresecondswithoutchewingandnoticehowittastes.
12. Now,youarefinallyreadytoeatthisitem.Softlybiteintotheitemandcontinuechewingitasmanytimesasyoucan.Trytochewtheitematleast15timesbeforeswallowingit.
13. Onceyouhaveswallowedtheitem,takeamomenttositquietlyandnoticehowyoufeel.Didthisprocessmakeeatingtheitemmoresatisfying?
Youcanrepeatthesestepswithotherfoods.Youcanalsopracticeaquickerversionofthiswithmealsjustbypayingmoreattentiontowhatyouareeatingandlettingallofyoursensesexperienceafoodbeforeyouswallowit.
LOVINGKINDNESSMEDITATIONSCRIPT
We’regoingtobeginwithanewMindfulAwarenesspracticecalledLoving-Kindness.Findacomfortablepositionwithyourbackrestingagainstyourchairandyourfeetsupportedbythefloor.Thispracticecanbeintenseforpeople.Ifyoudecideyoudon’tlikethispracticeatanypoint,justtreatmyvoice-asIguidethepractice-asyouwouldanynoisethatmightdistractyou.Youdon’thavetofightmyvoiceandyoudon’thavetofollowiteither.Justturnyourattentiontoyourbreath.
Allowyoureyestocloseorsetasoftgazearoundtheroom.
Now,takefiveabdominalbreaths,breathinginandoutatyourownpace.Remember,youdon’thavetochangeyourbreathingpattern,justtakedeep,fullbreathsinyourowntime.
Thenwe’llstartthefourphrases.Thereareseveraldifferentwaystodothispractice.Youwillrepeatthephrasesquietlytoyourself.Bringingyourselfintofocus,offerthefollowingphrases:
• MayIbehappy.(pause)• MayIbehealthy.(pause)

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
86|VHA/OfficeofPatientCenteredCareandCulturalTransformation
• MayIbesafe.(pause)• MayIbepeaceful.(pause)
(Repeatthesephrasesonemoretime.)
Now,directingyourattentiontosomeonewhomyoulike—maybeafriend,familymemberorapet,offerthesephrasestothem:
• Mayyoubehappy.(pause)• Mayyoubehealthy.(pause)• Mayyoubesafe.(pause)• Mayyoubepeaceful.(pause)(Repeatthesephrasesonemoretime.)
Nowdirectingloving-kindnesstowardssomeoneorsomethingthatmaybecausingyounegativeemotions.Picturingthatpersonandbringingintofocus,andofferingthefollowingphrases:
• Mayyoubehappy.(pause)• Mayyoubehealthy.(pause)• Mayyoubesafe.(pause)• Mayyoubepeaceful.(pause)(Repeatthesephrasesonemoretime.)
Nowofferingthistothoseintheroomandbringingthegroupintofocus.Andofferingthefollowingphrases:
• Mayyoubehappy.(pause)• Mayyoubehealthy.(pause)• Mayyoubesafe.(pause)• Mayyoubepeaceful.(pause)(Repeatthesephrasesonemoretime.)(Optional,dependingontime.)
Nowofferingthistoeveryoneinourworld:
• Mayyoubehappy.(pause)• Mayyoubehealthy.(pause)• Mayyoubesafe.(pause)• Mayyoubepeaceful.(pause)(Repeatthesephrasesonemoretime.)
Finally,onceagaincomingbacktoyourself:
• MayIbehappy.(pause)

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|87
• MayIbehealthy.(pause)• MayIbesafe.(pause)• MayIbepeaceful.(pause)(Repeatthesephrasesonemoretime.)
Nowfinishingwithfivemoredeepabdominalbreaths.Andopeningyoureyeswhenyou’refinished.
MINDFULWALKINGINSTRUCTIONS
LetParticipantsknowthattodayyouaregoingtointroduce‘Mindfulwalking’.Thisactivityisaboutfocusingattentionontheactualexperienceofwalking—noticinghowyourfeettouchthesurfaceonwhichyouarewalking.
Tobegin,haveparticipantspracticewalkingintheroomforaminuteorsojusttogetthesenseofwhatit’sliketopayattentiontotheirfeetcontactingthefloor.
Givethem5minutestowalkeitherinthebuildingoroutsideifpossible.Havethemwalkinsilence,nottalkingtoothers.
Havethemnoticethefollowing:
• Whatit’slikejusttowalk,continuingtonoticetheirfeetcontactingthesurfaceonwhichtheyarewalking.
• Noticetheirspeedofwalking.• Whatelsetheymaynoticewhentheirmindorattentiongoessomewhereelse:
sights,sounds,orothersensations-thingstheymayneverhavenoticedbefore.• Practicebringingtheirattentionbacktotheirwalkingwhentheirattentionhasgone
elsewhere.Letthemknowthetimewhenyouwantthembackintheroom.
BODYSCANMINDFULAWARENESSPRACTICESCRIPT
Thisisatimetotallysetasideforyou,andtobewithyourself.Atimeforrenewal,rest,andhealing.Atimetonourishyourhealthandwellbeing.Rememberthatmindfulawarenessisaboutbeingwiththingsastheyare,momenttomoment,astheyunfoldinthepresent.Letgoofideasaboutpersonaldevelopment.Letgoofyourtendencyforwantingthingstobedifferentfromhowtheyareandallowthemtobeastheyare.Giveyourselfthespacetobeasyouare.Youdon’tevenneedtotrytorelax.Relaxationmayhappenoritmaynot.Relaxationisn’ttheaimofthebodyscan.Ifanything,theaimistobeawareofyourexperience,whateveritmaybe.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
88|VHA/OfficeofPatientCenteredCareandCulturalTransformation
1. Loosenanytightclothing,especiallyaroundyourwaistorneck.Youmaycloseyoureyesorsetasoftgazearoundtheroom.Youmayliketoremoveyourshoes.(Pause)
2. Beginbyfeelingtheweightofyourbodyinthechair.
3. Noticethepointsofcontactbetweenthatandyourbody.Eachtimeyoubreatheout,allowyourselftosinkalittledeeperintothemat,bed,orchair.(Pause)
4. Becomeawareofthesensationsofyourbreath.
5. Youmayfeelthebreathgoinginandoutofyournostrils,orpassingthroughthebackofyourthroat,orfeelthechestorbellyrisingandfalling.Beawareofyourbreathwhereveritfeelsmostpredominantandcomfortableforyou.(Pause)
6. Whenyou’reready,moveyourawarenessdowntheleftleg,pastthekneeandankleandrightdownintothebigtoeofyourleftfoot.
7. Noticethesensationsinyourbigtoewithasenseofcuriosity.Isitwarmorcold?Nowexpandyourawarenesstoyourlittletoe,thenallthetoesin-between.Whatdotheyfeellike?Ifyoucan’tfeelanysensation,that’sokay.(Pause)
8. Expandyourawarenesstothesoleofyourfoot.
9. Focusontheballandheelofthefoot.Theweightoftheheel.Thesidesandupperpartofthefoot.Theankle.Then,whenyou’reready,letgooftheleftfoot.(Pause)
10. Repeatthisprocessofgentle,kind,andcuriousacceptingawarenesswiththelowerpartoftheleftleg,theknee,andtheupperpartoftheleftleg.(Pause)
11. Noticehowyourleftlegmaynowfeeldifferenttoyourrightleg.(Pause)
12. Gentlyshiftyourawarenessaroundanddowntherightleg,tothetoesinyourrightfoot.(Pause)
13. Becomeawareofyourpelvis,hips,buttocksandallthedelicateorgansaroundhere.(Pause)
14. Moveuptothelowertorso,thebelly,andlowerback.(Pause)
15. Bringyourattentiontoyourchestandupperback.
16. Feelyourribcagerisingandfallingasyoubreatheinandout.Bemindfulofyourheartbeatingifyoucan.(Pause)
17. Gotobotharmstogether,beginningwiththefingertipsandmovinguptotheshoulders.(Pause)
18. Focusonyourneck.
19. Thenmoveyourmindfulattentiontoyourjaw,noticingifit’sclenched.Feelyourlips,insideyourmouth,yourcheeks,yournose,youreyelidsandeyes,yourtemples,

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|89
yourforeheadandcheckingifit’sfrowning,youreyes,thebackofyourhead,andfinallythetopofyourhead.Takeyourtimetobewitheachpartofyourheadinamindfulway.(Pause)
20. Nowletgoofallefforttopracticemindfulness. Getasenseofyourwholebody.Feelyourselfascomplete,justasyouare.Rememberthissenseofbeingisalwaysavailabletoyouwhenyouneedit.Restinthisstillness.
Pauseandtheninviteyourcoachingpartnerorgrouptoreturntheirfocustothepresentmoment.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
90|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER9:ADVANCEDCOACHINGSKILLS
CoachesattendingtheWHCTrainingareexpectedtohaveasoundandfoundationalgraspofthecoachingqualities,skills,andstrategiesspecifictotheProcessModelstages.TheSession3curriculumfocuses,largely,onsomemore“advanced”coachingskillsandprocesses.Thischapterwillintroducethoseadvancedcoachingskills.Theabilitytolearn,understand,andutilizetheseskillswillenhancethecoaches’currentpracticewithVeterans;andincreasetheirknowledgeinanticipationofsuccessonthenationalexam.
METAPHOR
Metaphorisanotheradvancedcoachingskillor“tool”inthecoach’stoolkit.Manypeopleusemetaphorintheirdailyconversationsasawaytoexpresstheirthoughtsandfeelingswithavisualanalogy.Incoaching,metaphorscanbeofferedbythecoachtodeepentheconversation,furtherexplore,andencourageforwardmovement.ThecoachmayalsoheartheVeteranuseametaphor,anditcanbeeffectiveforthecoachtoreflectthisback.
WHYAMETAPHOR?
Ametaphorisafigureofspeechthatdirectlyreferstoonethingbymentioninganother,suchas“stuckbetweenarockandahardplace”or“I’montopoftheworld.”Anotherwaytothinkaboutmetaphorisavisualanalogy;metaphorconveysapicturethatcapturestheessenceofwhatisbeingsaid.Utilizingmetaphorisusefulbecauseitcreatesimagesinthemindthattapintoaclient’screativity,unlockingideasandpotential.
Researchhasshownthatusingmetaphorstodescribeathought,feeling,orcircumstancedoesmorethansimplyhelpingusunderstand.Metaphorsactivatepartsofthebrainassociatedwithtouch,feeling,andmovement,thusmakingametaphoricalstatementmorepowerfulthanitsliteralcounterpart.Theuseofmetaphor,therefore,mayofferthecoachdeeperinsightintotheVeteran’suniqueperceptionoftheirsituation,maycreateenlightenmentfortheVeteran,anditmayshifttheVeteran’sperspectiveinhowtheyseethemselvesortheirsituation.
USINGMETAPHORINTHECOACHINGROLE
MetaphorisapowerfultoolforboththecoachandtheVeteran.Toeffectivelyusemetaphorinthecoachingrole,itisimportanttolistentotheVeteran’suniquelanguageinordertoofferanappropriateandusefulmetaphor.DoingsohelpsbuildrapportwiththeVeteranandletsthemknowtheyareheard.MetaphorsthatincorporatetheVeteran’sownlanguagecanalsohelpdeepentheconversation,solidifyanidea,andincreasetheVeteran’smotivation.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|91
IfaVeteranexpressesathought,feeling,orcircumstanceusingametaphor,useit!Reflectitback,worktoweaveinthemetaphorthroughoutthecoachingsession,andseeifittakestheconversationdeeper.Asacoach,ifyouofferametaphorforwhattheVeteranhassaid,playwithit.Recognizethatthemetaphormaynotlandorlast.IftheVeteranshowsnoenergyinfollowingthepathofmetaphor,letitgo.
EXAMPLESOFCOMMONMETAPHORS
ThefollowinglistofmetaphorsaretakenfromGavin,J.,&Mcbrearty,M.(2019).Lifestylewellnesscoaching.Champaign,IL:HumanKinetics(p.188)
Ifeelbluetoday.Ifeelontopoftheworld.Ifeelflighty.Ifeelinsideout.Ifeelblownaway.
She’scuteasabutton.Shehasaheartofgold.She’sawitch.She’samoneymagnet.She’sanangel.She’sadevil.
Life’sabeach.Life’sabowlofcherries.Life’sarollercoaster.Life’sjustadream.Life’sahardroadtotravel.Life’sagift.
He’scoldasice.He’sarock(asnake,apig,aknightinshiningarmor,adiamondintherough).
Timeismoney.Astitchintimesavesnine.Don’tcryoverspilledmilk.Makehaywhilethesunshines.Abirdinthehandisbetterthantwointhebush.Apennysavedisapennyearned.
INTERRUPT&REDIRECT
HealthcoachingrequiresafinebalancebetweenallowingtheVeteranfullautonomyinasessionwhilealsomaintainingthesessionstructure.Oneofthecoach’sresponsibilitiesistoholdthefocusandstructureofasessionfortheVeteran.TheskillofInterruptandredirectisanadvancedcoachingskillusedtoensurethefocusofacoachingsessionismaintained.
Culturally,weareoftentaughtnottointerrupt.Incoaching,however,interruptingisausefulskillwhenintentionallyandgentlyemployed.Beforefurtherexploringtheskillofinterruptandredirect,itisimportanttodifferentiatebetweenunconsciousinterruptingandconsciousinterrupting.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
92|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CONSCIOUS&UNCONSCIOUSINTERRUPTING
Unconsciousinterruptingoftenhappensinconversationswithoutpeopleevenrealizingtheyareinterrupting.Itisoftenaresultofnottrulylistening,andnotwaitingtoheartheendofastoryorathought.Unconsciousinterruptinginvolvesthetendencytointerjectone’sownopinionmidsentenceornoteffectivelypausing.
Consciousinterruptingisanintentionalredirection;itisdonewiththeintentiontoserveabiggerprocessorreason.Incoaching,consciousinterruptingisutilizedwhenthecoachunderstandsthereisaneedandpurposetoredirecttheVeterantobestservetheirsession.Consciousinterruptingmaybeusedto:
• Focus. • Redirect. • Exploredeeper.
THEPURPOSEOFINTERRUPT&REDIRECTASASKILL
Whenusedappropriatelyandwithintention,interruptandredirectgivesthecoachanothertooltoensureeachcoachingsessionmeetstheneedoftheVeteran.Interruptandredirectcanbeusedinavarietyofinstances,someofwhichinclude:
• Toredirectbacktothecoachingconversation. • Tokeepthecoachingprocessontrack. • TohelptheVeteranstayfocusedonwhatismostimportant. • Topauseandofferappropriateaffirmationoracknowledgment.
Itisimportanttonotethatinterruptandredirectisnotusedasanopportunitytoinsertthecoach’sopinion.Rather,thecoachgentlyinterruptstheVeteranandguidestheconversationbacktothecoachingfocuswithaquestion,reflection,oracknowledgment.
THESKILL
Beinginterruptedoftenleaveaspeakerfeelingembarrassedorself-conscious,sometimestothepointofshuttingdowntheirabilityordesiretocontinuespeaking.Therefore,itisimportantforthecoachtobeawareofhowtointerruptwithagentle,intentional,andrespectfulapproach.
Thecoachistheexpertoftheprocessandstructureofeachsession.TheskillofinterruptandredirectisdirectivebutcanbeusedinawaythatstillallowstheVeteranautonomywithinthesession.First,askingpermissiontointerruptatthebeginofacoachingsessioncanreducemanyofthenegativefeelingsaVeteranmightexperiencewhenbeing
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|93
interrupted.Second,interruptingwiththeintentionofgainingtractionandmaintainingforwardmovementaroundtheVeteran’schosenfocussupportsVeterangoalsandautonomy.
WHENTOINTERRUPT&REDIRECT
DecidingwhentointerruptandredirectrequiresanunderstandingoftheVeteran’sfocus,personalself-awareness,andknowledgeofsessionstructure.Belowaresomeexamplesofsituationswhereinterruptandredirectmaybeusefulandhowitmaysoundduringacoachingsession:
• TheVeteranhassaidalotandthecoachrecognizesaneedtobottomlineorsummarize
o “You’vesaidalot–howcanyoubestsaythatinonesentence?”• TheVeteran’sstoryisaboutfixing,blaming,orfocusingonsomeoneelse
o “Ihearyoufeel bythisperson/situation.Whenyouthinkaboutthis,whatdoyounoticethatyouhavecontrolover?”
• TheVeteranhassharedsomethingimportantthatneedstobeexploredmoredeeply(struggle,valuesconflict,oversights,etc.)
• “I’mgoingtopauseyouforamomenttodivedeeperintowhatyoujustsaid.”• TheVeteranhasgoneoffonatangentunrelatedtothefocusofthesession• “MayIpauseyouforamoment?Saymoreabouthowthisstoryrelatestowhatyou
wantedtodiscusstoday.” Beforeinterrupting,alwayspauseandconsidertheintention.
HOWTOINTERRUPT&REDIRECT
Aspreviouslydiscussed,beinginterruptedcanoftenleavethespeakerembarrassedorself-conscious.Therefore,itisimportanttoestablishguidelinesforinterruptingearlyinthecoachingprocess.InthefirstcoachingsessionwithaVeteran,clearlyexplainoneofthecoach’sresponsibilitiesistomaintainsessionstructureandfocus;explicitlystatethatinterruptingmaybeoneofthewaysacoachkeepsthesessionfocused.LettheVeteranknowwhyinterruptingisimportantanduseopen-endedquestionsandreflectionstoexplorehowtheVeteranfeelsaboutbeinginterrupted.Finally,asktheVeteran“Whatisthebestwayformetopauseandinterruptyouduringoursession?”Honortheirrequestiftheneedforinterruptandredirectarisesinsubsequentsessions,alwaysredirectingwithintentionandrespect.
USEFULEXAMPLES
InterruptandredirectlookandsoundsdifferentineverysessionandwitheveryVeteran.Belowaremoreusefulexamplesofwaystogentlyinterrupt(I)andredirect(R)aVeteran.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
94|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Noticetheprocessofinterruptingisalwaysfollowedwitharedirectionbacktothecoachingconversation.ConsiderrephrasingthesebasedonhowVeteranssharetheywouldliketobeinterrupted.
• “Let’spauseforamoment(I)andnotice(R)…” • “Ihearthisstoryisimportanttoyou(I).Whatdidyoulearn(R)?” • “Youhavealottosay(I)–whatisthemostimportantthingyouwantmeknow
aboutthis(R)?” • “MayIpauseyouforamoment(I)?Iwanttohearwhatismostimportanttoyouin
thisstory(R).” • “Letmepauseyouforamoment(I).Youhavealreadyhadsuccessinthisarea(R).” • “Yousaidyouareinspiredby…(I).Theseareimportantvaluesforyou.Let’sgo
backtohowthesesupportyourhealth(R).”
DECISIONALBALANCE
Veteransworkwithacoachbecausethey’reinterestedinmakingchanges.Decisionalbalanceisatoolthatinvolvesexploring,withnonjudgmentandcuriosity,theprosandconsofmakingachange.
DecisionalbalanceisatooloftenutilizedwhenaVeteranisinContemplation(accordingtotheTranstheoreticalModel/StagesofChange)orexperiencingambivalencearoundaspecificbehaviorchange.Thecoach’sroleistoexploretheprosandconsofchangingandnotchanging,whilemaintaininganattitudeofnonjudgmentandcuriosity.
COACH’SNONJUDGMENT
Maintaininganattitudeofnonjudgmentisakeycoachingqualitythatisespeciallyimportantwhenusingthetoolofdecisionalbalance.NonjudgmentisimportanttofosterasenseofpsychologicalsafetyfortheVeterantoexploreandprocesshonestly.Thecoach’sroleisnottodirecttheVeterantochangeorencourageonesideofchangeovertheother.Instead,thecoachallowstheVeterantofreelyexploreallaspectsofchangingandnotchanging.
CoachingskillsthatsupportanonjudgmentalenvironmentincludeallowingtheVeteranfullautonomy,offeringdouble-sidedreflections,andreflectingchangetalk.Double-sidedreflectionsofferbackbothsidesofthedecisiontheVeteranisconsidering;using“and”insteadof“but”oftenhelpsthereflectionsoundnonjudgmental.Remembertoendthedouble-sidedreflectiononthesideofchange,sincethisisthelastthingtheVeteranhears.ChangetalkisdefinedastheVeteran’sownstatementsthatdescribereasonsformakingchange.WheneveryouheartheVeteransharingreasonsforchange,reflectthechangetalk.
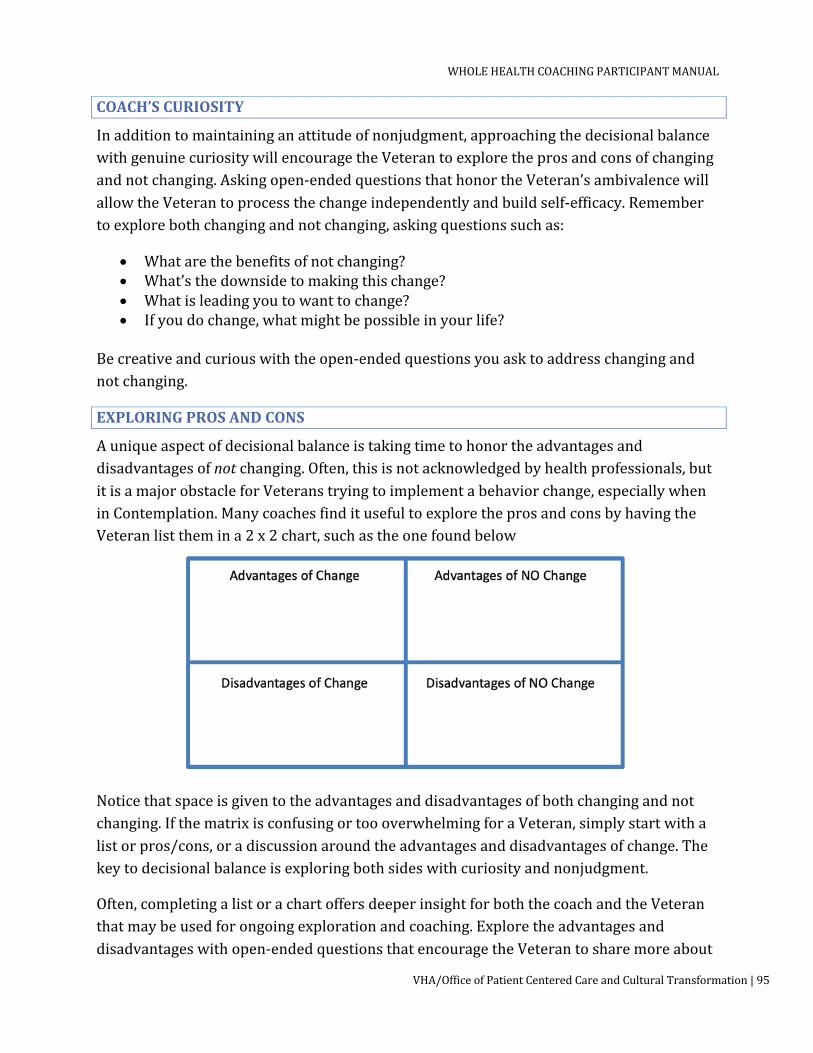
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|95
COACH’SCURIOSITY
Inadditiontomaintaininganattitudeofnonjudgment,approachingthedecisionalbalancewithgenuinecuriositywillencouragetheVeterantoexploretheprosandconsofchangingandnotchanging.Askingopen-endedquestionsthathonortheVeteran’sambivalencewillallowtheVeterantoprocessthechangeindependentlyandbuildself-efficacy.Remembertoexplorebothchangingandnotchanging,askingquestionssuchas:
• Whatarethebenefitsofnotchanging? • What’sthedownsidetomakingthischange? • Whatisleadingyoutowanttochange? • Ifyoudochange,whatmightbepossibleinyourlife?
Becreativeandcuriouswiththeopen-endedquestionsyouasktoaddresschangingandnotchanging.
EXPLORINGPROSANDCONS
Auniqueaspectofdecisionalbalanceistakingtimetohonortheadvantagesanddisadvantagesofnotchanging.Often,thisisnotacknowledgedbyhealthprofessionals,butitisamajorobstacleforVeteranstryingtoimplementabehaviorchange,especiallywheninContemplation.ManycoachesfinditusefultoexploretheprosandconsbyhavingtheVeteranlistthemina2x2chart,suchastheonefoundbelow
Noticethatspaceisgiventotheadvantagesanddisadvantagesofbothchangingandnotchanging.IfthematrixisconfusingortoooverwhelmingforaVeteran,simplystartwithalistorpros/cons,oradiscussionaroundtheadvantagesanddisadvantagesofchange.Thekeytodecisionalbalanceisexploringbothsideswithcuriosityandnonjudgment.
Often,completingalistorachartoffersdeeperinsightforboththecoachandtheVeteranthatmaybeusedforongoingexplorationandcoaching.Exploretheadvantagesanddisadvantageswithopen-endedquestionsthatencouragetheVeterantosharemoreabout
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
96|VHA/OfficeofPatientCenteredCareandCulturalTransformation
theemotion,motivation,andreasonsforchangingornotchanging.Decisionalbalanceisnotaone-timetool;itisanongoingstrategyforprocessingthathonorsthechallengeandambivalencethatmaysurroundbehaviorchange.Theinitialexerciseoftenservesasatemplateforexplorationandinsightthroughouttheentirecoachingrelationship.
PERSPECTIVES
Aperspectiveisaview,outlook,orlensthroughwhichpeopleseethemselves,asituation,ortheirworld.Itisimportanttorecognizethateveryonehasperspectivesabouteverythingtheydoandexperience.Individualsmayormaynotbeconsciousofalltheirperspectives,but,ultimately,perspectivesinform,create,andinfluenceourbeliefsystems.Perspectivesinfluencehowpeopleinteractwithothers,howtheyinteractwiththemselves,andhowtheyinteractwiththeirworld.
Withregardstocoaching,itisimportanttolistenforthelanguageofperspectives,understandhowperspectivesimpactbeliefsystems,andeffectivelyutilizethecoachingtoolofexploringperspectives.
THELANGUAGEOFPERSPECTIVES
Perspectivescanbebothpositiveandnegative;theyaresimplyalensthroughwhichpeopleviewtheworld.Incoaching,itisimportanttolistenforthelanguageofperspectives.Positiveperspectivescanbeempoweringandmotivating,pushingtheVeterantoreachtheirfullestpotential.Negativeperspectives,ontheotherhand,cancreateinternalbarriers,hinderingtheVeteranfromimplementingchange,tryingnewthings,andreachingtheiroptimalhealthvision.
ListenforsomecommonphrasesthatindicateaVeteranissharingtheirperspective:
• “Ithink…” • “Ibelieve…” • “Inmyopinion…” • “Frommypointofview…” • “I’mjust…”
• “ThewayIseeit…” • “I’mtoo…” • “Ican’t…” • “Iwon’t…”
AmplifypositiveperspectivesandbewillingtoexplorehowthisperspectivemaymotivateorsupporttheVeteranintheirbehaviorchange.ReflectnegativeperspectivesandusethisasanopportunitytoassisttheVeteraninexploringhowaperspectiveisaffectingtheirbeliefsystem,theiractions,andtheirself-talk.Thecoach’sroleisnottochangeaVeteran’sperspective,buttoexploreaVeteran’sperspectiveandinvitethemtoconsiderlookingattheirperspectiveindifferentways.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|97
PERSPECTIVESANDBELIEFSYSTEMS
Perspectivesoftencreateandinformbeliefsystems.Aspreviouslystated,positiveperspectivescanmotivateandempoweraVeteran,pushingthemtomoveforward.NegativeperspectivescanfuellimitingbeliefsandleaveaVeteranfeelingstuckorboxedin,becomingabarriertoforwardmovementincoaching.
ListenempatheticallyandnonjudgmentallyasVeteransshareperspectivesandlimitingbeliefs.Aperspectivemayhaveoncefeltsafe,confined,orcomfortable,but,overtime,theperspectivenolongerfits.Exploringanddevelopinganewperspectivetakestime,growth,andawillingnesstostretch.Similartochange,takingonanewperspectivecanbeadauntinganduncomfortabletask,sobewillingtoaffirmtheVeteran’sefforts,strengths,andwillingnesstostretchthemselves.
EXPLORINGPERSPECTIVES
Exploringperspectivesisacoachingtooltobeusedwhenneeded.Belowareexamplesofscenarioswhenexploringperspectivesmaybeuseful:
• Exploringandovercomingfeelingsofbeingstuck. • Exploringandmovingoutofresistance. • Exploringalimitingbelief. • Exploringnewopportunities. • Exploringanewattitudeorapproach.
Exploringperspectivescanbedeepanddifficultworkthatrequiresuncoveringtheemotions,thoughts,andbeliefsbehindabehavior.Asacoach,recognizethebehaviorastheconsequenceofthedeeperemotions,thoughts,andbeliefsaVeteranholds.Emotionsinfluencebehavior,thoughtsempowerordisempoweractionthroughinnerdialogue,andbeliefsaredeeplyingrainedideasinone’ssubconsciousandunconscious.ThetoolofexploringperspectivesgivestheVeterananopportunitytouncovertheemotions,thoughts,andbeliefsbehindabehavior,withtheopportunitytotryonanewperspective
POWERFULQUESTIONS
PerspectivescanservetomoveaVeteranforward,andtheycanlimitaVeteran,keepingthemstuck.Onethoughtful,meaningfulquestionhasthepowertoshiftperspective.Possibilitiesexistfromeveryperspective.ShiftingalimitedperspectiveorbeliefopenstheVeteranuptonewpossibilities,filledwithpositivityandpossibility.
Asacoach,yourjobisnotto“change”theVeteran’sperspective,buttosimplyofferanopportunitytoexploredifferentwaystolookatasituation.WhenaVeteransharesalimiting

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
98|VHA/OfficeofPatientCenteredCareandCulturalTransformation
belieforfeelsstuck,thefollowingquestionsmaybeusefultoencouragethemtoconsideradifferentperspective:
• Howmightsomeoneelseseeit?(the‘other’perspective) • Whatmightyoutellsomeoneelse? • Howmightyourolder/wiserselfseeit? • Whatmightyouryoungerself(orachild)saytoyou? • Whatmightbeacompletelyoppositebelief? • Whatwouldbepossibleifyouheldtheoppositebelief? • Whatbeliefwouldopenuppossibilities?
GentlyexplorethenewperspectiveandgivetheVeterantimeandspacetorespond.ReflectanyshiftinperspectiveandrecognizetheVeteranstillmaynotbereadytoadoptanewperspectiveorturnanewperspectiveintoaction.TheexplorationallowstheVeterantoattempttoviewthesituationdifferently.Remember,alotofworkandprocessinghappensbetweencoachingsessions.
EXPLORINGMULTIPLEPERSPECTIVES
FormanyVeterans,adiagramortoolisusefulinexploringdifferentperspectives.WhenaVeteranhasanareaoffocusoragoalinwhichtheyarelimitedinmovingforward,considerinvitingthemtoparticipateinawrittenexercisesurroundingthefocusorgoal.ThediagrambelowisanexampleofavisualtoolthatallowsaVeterantoexploremanydifferentperspectivesaroundaspecificfocusorgoal:
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|99
WiththeVeteran,firstinvitethemtoidentifytheareainwhichtheyfeelstuckandthebelieforperspectivetheybelieveisholdingthemback.Checkinoninternalbarriers,limitingbeliefs,thoughts,andemotions.Explorethebehavior,consequences,andpossibilitieswhenoperatingfromthatperspective.
Whenthatperspectiveisexhausted,invitetheVeterantochooseanotherperspectivefromthelistbelow,oroneoftheirownchoosing:
• Oppositebelief. • Friend. • Olderself. • Youngerself. • Trustedmentor. • Successfulself. • Whatwouldyoutellafriendinthissituation? • Other?
InvitetheVeterantoconsiderthethoughts,feelings,andemotionswiththisnewperspective.Explorethebehavior,consequences,andpossibilitieswhenoperatingfromthesecondperspective.
IftheVeterandesires,completetheexerciseoneortwomoretimeswithdifferentperspectives.OncetheVeteranhasexploredmultipleperspectives,explorewhattheynoticed,whatstoodout,andwhattheyaretakingawayfromtheexercise.Remindthemthisisatooltheycanutilizeindependentlywithanylimitingperspectiveorareainwhichtheyfeelstuck.
Exploringperspectivescanopenaworldofpossibilities.Thelanguageofshiftedperspectivesinvolvespositiveself-talkandpositivereframing.Asacoach,whenaVeteranshiftsfrom“Ican’t…”to“Ican…,”“Iwon’t…”to“Iwill…,”or“I’mtoo…”to“Iam…,”reflectitback,amplifytheshift,andacknowledgetheeffortittakestoadoptanewperspective.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
100|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER10:COACHINGSTRUCTURE
Healthandwellnesscoachingsessionsaretypicallytime-limitedinterventions,designedtosupportbehaviorchangeoverthecourseofseveralmonths.Akeyresponsibilityofacoachistomaintaintheoverarchingstructureofthehealthcoachingprocess,aswellasthestructureofeachindividualcoachingsession.TheNationalBoardforHealth&WellnessCoaching(NBHWC)suggeststhecoachingprocessbeorganizedintoaparticularsequence,witheachcomponenthavingkeyelementscriticaltothebehaviorchangeprocess:
• Coachpreparation. • Initialsession. • Routineongoingsessions. • Closingsession.
Inthischapter,thesessionsandkeyelementsaredescribedindetail.Althoughthelengthofeachsessionmayvaryaccordingtotimeconstraints,coach’sstyle,andVeterancomplexity,itisimportanttoaddressallthecomponents.ThiswillrequireflexibilityandadaptabilityforbothyouandtheVeteran,asyoudeterminethecomponentsforagivensessionandarriveatnaturalstoppingpoints.Pickupatthestoppingpointatthenextsessionsonocomponentsaremissed.
Notethatcoaching“structure”willdeviatefromthecoaching“stages”(Stages1-4)thatareoriginallytaughtintheWholeHealthCoachingmodel.WhiletheWholeHealthCoachingstagesarehelpfultogroupthemesandpartsofthecoachingconversation,theydonotcorrespondtocoachingsessionorvisits.Assuch,thecoachingstructuredescribedbelowdoesnotdirectlycorrelatewithStages1-4;however,youwillrecognizecomponentsfromStages1-4interweavedthroughout.
PREPARATION
Personalpreparationisessentialpriortoanycoachingsession.Notonlyisthecoachresponsibleforpaperworkandlogistics,butalsoensuringthatafocused,mindful,andsafeatmosphereismaintainedforthedurationofacoachingsession.Priortoanycoachingsession,itisrecommendedthecoachsetaside5to10minutestocompletethefollowing:
• ReceiveandreviewallVeteranmaterials(referrals,PHI,previoussessionnotes,etc.). • Secureadistraction-free,confidentialspace. • Confirmtimeanddurationofcoachingsession. • Personalpreparationtoensurecoachispresentandfocused(mindfulawareness
practice).

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|101
INITIALSESSION
Theinitialcoachingsessionhasseveralkeycomponentsthataretypicallyaddressedtosetthegroundworkforongoingcoachingsessions:
• Explanationofthecoachingrelationship. • Coachingagreement. • ReviewofPersonalHealthInventory(PHI). • AssessVeteran’scurrentstate(CircleofHealth). • Identifyanareaoffocus. • Nextsteps.
Initialsessionsrangeindurationfrom60-90minutes.ItisimportanttonotethatexploringtheVeteran’svalues,vision,mission,andcurrentstatearefoundationaltotheentirecoachingprocess.Ifa90-minuteblockisnotfeasibleforthecoachandtheVeteran,thecomponentsoftheinitialsessionmaybeaddressedovermultiplemeetings.Considerthetimeavailableandtheconversationathandwhendeterminingwheretodividethecomponentsofaninitialsession,ifnecessary.Besuretocoverallcomponentsoftheinitialsessionbeforeaddressinganycomponentsofanongoingcoachingsession.
INTRODUCTION
Atthebeginningofthecoachingprocess,brieflyintroduceyourselfandallowtheVeterananopportunitytointroducethemselves.Usecurious,open-endedquestionsandreflectionstoexplorewhatmotivatedtheVeterantoparticipateincoaching.TheinitialsessionisanimportanttimetolistenandconsideriftheVeteranisanappropriatecandidateforcoaching.Veteransdisplayingsignsofmentalillnessorsubstanceabusewhoarenotalsoworkingdirectlywithamentalhealthprofessionalmaynotbeappropriateforcoaching.
RememberthatthecoachingrelationshipwillbenewtomanyVeterans.Therefore,itisimportanttotaketimetoexplainthecoachingrelationship,thecoachingprocess,andreviewcoachandVeteranresponsibilities(seesectionbelow).Usingopen-endedquestionsandreflections,explorewhattheVeteranhasheardaboutcoaching.Askpermissiontosharehowhealthcoachingisdifferentfromotherhealthcarerelationships:
• CoachingisVeteran-centered(i.e.,Veteransaretheexpertsintheirownlife). • Coachingisnottherapy. • Coachescannotprescribeordiagnose. • Veteransareactiveparticipantsinthecoachingprocess(expectedto“do”mostof
thework). • CoachingisacollaborativepartnershipbetweenthecoachandtheVeteran.
Afterintroducingthecoachingrelationship,itmaybehelpfultopauseandelicitanyquestionsorconcernsfromtheVeteran.Onceallcomponentsoftheintroductionhavebeen

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
102|VHA/OfficeofPatientCenteredCareandCulturalTransformation
addressed,pausetotakeamomentandexplaintheagendafortheremainderoftheinitialsession.
VALUES,VISION,ANDSTRENGTHS
AkeycomponentoftheinitialsessionisunderstandingwhatmakestheVeteran“tick,”ortheirvalues,vision,andstrengths.Usingopen-endedquestionsandreflections,explorethefirstthreequestionsoftheVeteran’sPersonalHealthInventory(PHI).Considerasking:
• Whatmattersmosttoyouinyourlife? • Whataresomeofthestrengthsthatarehelpingyoubesuccessful? • Wheredoyouseeyourselfinthreetofiveyears?
Inaddition,encouragetheVeterantosharewhattheyseeastheirmission,aspiration,andpurpose(MAP)inlife.ExploretheirMAP,howitconnectstotheirvalues,vision,andstrengths.OffermultiplereflectionsandacknowledgmentsoftheVeteran’svaluesandstrengths,rememberingtopausetoallowtheVeterantimeandspacetoexpandordeepentheconversation.
AVeteran’svalues,vision,strengths,andMAParekeymotivatorsforbehaviorchange.Ensureadequatetimeisspentexploringeachofthesecomponents.Asacoach,youwillregularlyrevisittheVeteran’svalues,vision,andstrengthsinongoingcoachingsessionstoincreasetheVeteran’smotivationforchange.NotonlywillaVeteran’svalues,vision,andstrengthsbeimportantforthecoachtoknow,buttheyareimportantforaVeterantorecognizeandverbalize,increasingmotivation,buildingcompetence,andimprovingself-efficacy.
ASSESSCURRENTSTATE
TheCircleofHealthisaself-careassessmenttoolthatallowstheVeterantoexplorewheretheyareandwheretheywanttobeindifferentareasofself-care.WhilesomeVeteransmaywanttodiscussallareasontheCircleofHealth,itisnotalwaysnecessarytodoso.Instead,startbyaskingtheVeterantoidentifyareasinwhichtheygavethemselvesahighernumber,andexplore.Followingthisdiscussion,asktheVeterantoidentifyareasinwhichtheygavethemselvesalowernumber.ForeachareaontheCircleofHealththeVeteranwantstodiscuss,ataminimum,ask:
• Whatnumberdidyourateyourself? • Whatdoesthatnumbermeantoyou? • Wherewouldyouliketoseeyourself? • Whatwouldyourlifelooklikeifyouwereata ?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|103
Aseachsectionisexplored,listenforgapsbetweenwheretheVeteranisandwheretheVeteranwantstobe.Considerexploringdeeperusingpowerfulquestionsinadditiontothequestionsabove(“Whatelse?”).EncouragetheVeterantoconsidertheimpactofmakingachangeinaspecificarea,whatmakesthatareaimportant,andwhatelsewillbepossibleintheirlifewhentheydomakeachange.AllowtheconversationaroundtheCircleofHealthtobeanexploration,notaproblem-solvingsession.Useopen-endedquestionsandreflectionstofullyexploretheVeteran’svisionoftheiroptimalhealth.OncetheCircleofHealthhasbeenfullyexplored,theVeteranhasaclearerpictureofwheretheyareandwheretheywanttobe.
FOCUSANDNEXTSTEPS
AfterexploringtheCircleofHealth,invitetheVeterantoidentifyoneortwoareastheywouldliketofocusoninthenextthreetosixmonths.Usingascalingquestion,assessimportancearoundthisareaoffocus.Iftimeallows,exploreimportanceusingscaling(0-10)andrelatethefocusareabacktotheVeteran’svalues,usingareflection.
Toclosetheinitialsession,brieflyaddressthefollowing:
• Giveanoverviewofthenextsession(settingalong-termgoal) • Setanactionbeforenextvisit(“Beforeournextsession,whatisonethingyou’dliketo
tryinyourareaoffocus?”) • AsktheVeteranforkeytakeaways/learnings • Confirmthetimeforthenextvisit
EventhoughtheVeterandoesnotyethavealong-termgoal,besuretoinvitetheVeterantocommittosometypeofactionbeforethenextvisit.Thecoachingprocessisaboutconsistentforwardmovement,soitisimportanttheVeteranhassomethingtoworkoninbetweeneachcoachingsession.Nexttime,theVeteranwillhavetheopportunitytosharewhattheylearnedwhenattemptingthisaction.ThisisthestandardwaytobegineachRoutineOngoingSession.
ROUTINE-ONGOINGSESSIONS
OngoingcoachingsessionsfollowaspecificstructurethatallowtheVeterantoassesstheirpreviousactionstep,identifyanareaaroundwhichtheywouldlikecoaching,andsetanewactionstep.Mostcoachingsessionswillfollowthestructureoutlinedbelowforongoingcoachingsessions:
• Reviewpreviousactionsteps. • Sessionfocus–wherewouldyouliketogofromhere? • Setnewormodifypreviousactionstep. • Veterantakeaways.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
104|VHA/OfficeofPatientCenteredCareandCulturalTransformation
ASSESSACTION
AfterbrieflycheckinginontheVeteran’scurrentstateandofferinganoverviewoftheupcomingsession,assesstheVeteran’spreviousactionstep.Usingopen-endedquestionsandreflections,explore:
• Whatwentwellwiththeactionstep? • Whatdidnotgoaccordingtoplan? • Whatdidyoulearn?
IntentionallyaskaboutVeteransuccessesfirst,ashumannatureistosharewhateverdidnotgorightfirst.ReflectandaffirmtheVeteran’ssuccess,effort,orawareness,eveniftheactionstepwaspartiallycompletedornotcompletedatall.AstheVeteransharesobstaclesorsetbacks,itcanbehelpfultoacknowledgethedifficultyandthenreframeitasalearningopportunity.BesuretoasktheVeteranwhattheylearnedfromtheexperienceandreflecttheirlearnings.
Amplifyanynewinsightsorperspectiveshiftsinthereflection.
SETALONG-TERMGOAL(FOLLOWINGINITIALSESSION)
Animportantpartofthecoachingprocessoccursinthesessionthatfollowstheinitialsession:settingalong-termgoal.InvitetheVeterantosetalong-termgoalintheirarea(s)offocus.Sincetheareaoffocuswaschosenintheinitialsession,check-infirstwiththeVeterantoseeifithaschangedorwillstaythesame.AsktheVeteranwhattimeframetheywanttosetalong-termgoal,typically3-6months.Thelong-termgoalshouldbeabehavioralgoalinSMARTformat(SeeChapteronOutcomevsBehavioralGoals)
Itisimportanttorealizethisstepoccursonlyinthesessionthatfollowstheinitialsession.Duringfutureongoingsessions,itisappropriatetoaskhowtheVeteransfeelstheyareprogressingtowardtheirlong-termgoal.
FOCUS
Inmostroutineongoingsessions,thesessionfocusisanopportunityfortheVeterantodiscusswheretheywouldliketogonext(intoday’ssession).ThesessionfocusshouldbeelicitedfromtheVeteranwithanopen-endedquestion,suchas:
• Wherewouldyouliketogofromhere? • Whatwouldyouliketofocusontoday? • Whatismostimportantforyoutoreceivecoachingaroundtoday?
OncetheVeteranhasidentifiedtheareaoffocus,useanopen-endedquestiontoelicitwhatisimportantaboutthisareaandhowitrelatestotheiroverallhealthandwell-being.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|105
Duringthefocus,usethecoachingskillsofpowerfulquestions,reflections,acknowledgments,andotherskillstoexplorehowmakingachangeinthisareawillimpacttheVeteran’slife.ExplorehowtheareaoffocusconnectstotheVeteran’svision,MAP,andvalues.IftheVeteranisstuckorneedsfurtherinformation,offerbrainstormingorprovideinformationwithElicit-Provide-Elicit.Thefocusshouldconstitutemuchofthecoachingsessionandmayleadtoaneworrevisedactionstep.
NEXTSTEPSANDCLOSING
Afterthesessionfocus,assesstheVeteran’sreadinesstosetanactionstep.Actionstepsinongoingsessionsmaybenew(relatedtothesessionfocus)ortheymaybecontinuationormodificationsofpreviousactionsteps.Foranynewormodifiedactionstep,ensuretheactionstepisbehavioralandinSMARTformat.UseguidingquestionstohelptheVeterancreateanactionstepthatisSMART:
• Howoftenwillyou…? • Whendoyouplanto…? • Whattimewillyou…? • Whatdoyouseeyourselfdoinginthenextweek? • Howwillyoutrackyouractionstep? • Whoorwhatwillhelpholdyouaccountable?
Veteransaremorelikelytobesuccessfulinimplementingactionstepsiftheplaniswelldeveloped.Useopen-endedquestionstoexploreprevioussuccessesandhowtheVeteranmayapplypersonalstrengthstoimplementthisactionstep.Fullyexploreinterpersonal,environmental,andexternalsupports.EnsuretheVeteranhasaccesstotheresourcesnecessarytoimplementtheiractionstep.Inaddition,useopen-endedquestionstoasktheVeteranwhatbarriersorobstaclesmightgetintheway;allowtheVeterantoidentifythebarriersthatmaycomeupintheirownlife.HelptheVeteransetaspecificcontingencyplanforeachbarriertheyidentify.Whenaddressingsupportsandbarriers,ask“Whatelse?”untiltheVeteranhasnothingelsetoshare.
OncetheVeteranhasaclearplan,useascalingquestion(0-10)toassesshowconfidenttheyaretheywillcompletetheiractionstep.IfaVeteranhasaconfidencelessthana7,askthemwhatwouldincreasetheirconfidencetoa7.
ToensuretheVeteranhasaclearunderstandingofnextsteps,itishelpfultoask,“Inyourownwords,whatisyournextstepbeforewemeetagain?”Finally,asktheVeteranwhattheyaretakingawayfromthesession.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
106|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CLOSINGSESSION
Theclosingsessionisanopportunitytoreflectonthecoachingprocess,celebratetheVeteran’ssuccesses,andestablishamaintenanceplan.Atthebeginningofthecoachingrelationship,thecoachandVeterantypicallyagreetoacertainnumberofsessionsormonthsofcoaching.Duringongoingsessions,itishelpfultoperiodicallyremindtheVeteranhowmanysessionstheyhavepriortotheclosingsessionsotheycanbegintomentallyprepare.
ASSESSGOALS
Likeongoingcoachingsessions,theclosingsessionstillbeginswithareviewofthepreviousweeks’actionsteps(successes,obstacles,learnings).Ratherthanshiftingtothesessionfocus,timeisspentreviewingtheVeteran’sprogresstowardtheirlong-termgoal(s).
Usingopen-endedquestionsandreflections,invitetheVeterantosharewhatprogresstheyhavemadetowardstheirlong-termgoal.Asyoureflect,fillinanygapsandaffirmtheirprogress.
ReflectonchallengesthatarosethroughoutthecoachingprocessandwhattheVeterandidinresponse.
Someofthequestionsbelowmaybeusefulwhenreviewinglong-termgoals:
• Whatprogressdoyoufeelyouhavemadetowardsyourlong-termgoal? • Whatdoyouconsideryourbiggestsuccessinrelationtothisgoal? • Whatwasmostchallenginginworkingtowardsthisgoal? • Howdidyoudealwiththischallenge?
RecognizethatnotallVeteranswillfullymeettheirlong-termgoals.ItisimportanttonormalizethisfortheVeteranaswell.Affirmanysuccessorprogressinanyarea.HighlightandreflectVeteranlearnings,efforts,andstrengthsdisplayedastheyworkedtowardstheirlong-termgoal.
REFLECT,TAKE-AWAYS
AkeycomponentoftheclosingsessionisofferingtheVeterananopportunitytoreflectonthecoachingprocess.Useopen-endedquestionsandreflectionstoexploreVeteranlearnings,newperspectives,andkeytakeawaysfromthecoachingprocess.SolicitfeedbackfromtheVeteranonthesupportyouofferedasacoach.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|107
SomeofthequestionsbelowmaybeusefulastheVeteranreflectsonthecoachingexperience:
• Whatdidyoulearnfromthecoachingprocess? • Whatisyourkeytakeaway? • Howhasyourperspectivearound…changed? • Whatnewinsights/perspectiveshaveyougained? • Asyourcoach,whatdidIdothatbestsupportedyou? • WhatcouldIhavedonedifferentlytosupportyouasyourcoach?
ListenandreflectnonjudgmentallyastheVeteranshares.Thecoachingprocessisallaboutlearningandgatheringnewinsight,sospendsometimewiththeVeteranastheyreflect.
MAINTENANCEPLAN
Atthispoint,theVeteranispreparingtomaintaintheirprogressandinitiatenextstepsindependently.Thecoachingprocessisdesignedtobuildself-efficacyandempowerVeteranstoimplementbehaviorchangeontheirown,butitisimportanttodiscussamaintenanceplanduringtheclosingsession.Keycomponentstoaddressinamaintenanceplaninclude:
• Supportsneededtomaintainprogress. • Accountability. • Potentialchallengestomaintainingprogress. • Contingencyplans.
Inaddition,theVeteranmaybeconsideringimplementingnewchangesinotherareas.InvitetheVeterantosharewhattheyseeastheirnextstepsfortheirhealthandwellness.Useopen-endedquestionsandreflectionstoexplorewhatsupports,resources,andstrengthstheyhaveastheymoveforward.ItisalsoimportanttoaddresswhatmightsignaltheVeterantheyneedtoreturntocoaching.
Someofthequestionsbelowmaybehelpfulwhenestablishingamaintenanceplanintheclosingsession:
• Whatsupportswillhelpyoumaintainyourprogress? • Whatmightgetinthewayoftheprogressyouhavemade? • Howdoyouplantodealwiththischallenge? • Whatareyournextstepsforyourhealthandwellness? • Whatsupports,resources,and/orstrengthswillhelpyoutakethenextstep? • Howwillyouknowyoumightneedtoreturntocoachingforsupport?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
108|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Oncethecomponentsofaclosingsessionhavebeenaddressed,bepreparedtosaygoodbyetothisformoftherelationshipwithaVeteran.AdheretotheguidelinesofyourVHAfacilityanddeterminewhattypeofcontactisappropriatetohavewiththeVeteran.ThismayrangefromtheVeteranusingtheMyHealthyVetSecureMessaging,periodiccheck-insordrop-ins.
COACHANDVETERANRESPONSIBILITIES/EXPECTATIONS
Thecoachingrelationshiptypicallyinvolvesawrittenagreementoutliningmutuallyagreedupontermsfortherelationship,including:
• Lengthofthecoachingrelationship. • Frequencyofsessions. • Adescriptionofthecoachingprocess. • Coachresponsibilities. • Veteranresponsibilities.
Belowisabriefdescriptionofthecoachingrelationshipandresponsibilitiesthatmaybeincorporatedintoaformalhealthcoachingagreement.BothcoachandVeteranshouldhaveaccesstoasignedcopyofthecoachingagreement.
THECOACHINGRELATIONSHIP
Thehealthcoachingrelationshipempowerstheclienttomakechangesthataremotivatingandpersonallymeaningful.AkeytenantofthecoachingrelationshipisthebeliefthattheVeteranistheexpertintheirownlife.CoachingisaboutthepartnershipbetweentheVeteranandthecoach.Thecoach’sroleisNOTthatofanexpertwhodiagnoses,advises,educates,ortellstheVeteranwhattodo.Coachingisnotcounselingortherapy.TheVeteranisanactiveparticipantinthecoachingprocessandisexpectedtodomostofthe‘work’ofcoaching.Thecoach’sexpertiseisintheprocessofsustainablechange,guidingtheVeterantoself-discoverstrategiesthattheVeterancansustainovertime.
VETERANRESPONSIBILITIES
• IwillbeontimeforsessionswithaclearagendaofwhatIwanttofocuson. • Iwillbeauthenticandhonest,especiallyaboutanythingthatdoesnotfeelrightto
me. • Iunderstandthatcoachingisacomprehensiveprocessthatinvolvesallareasofmy
life,andIchoosetodiscloseonlywhatfeelssafeandcomfortable. • Iwillkeepanopenmindtoexplorenewperspectivesandtrynewthings. • Iwillnotexpectthecoachtoprovidesolutionsorsolvemyproblems. • IwillprovideadequatenoticeifIamnotabletoattendacoachingsession. • Imayendthecoachingrelationshipatanytime.IfIchoosetoendthecoaching.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|109
relationship,Iwillgivethecoachadvancenoticeforafinalsessiontosummarizewhatwaslearned.
COACHRESPONSIBILITIES
• Iwillbefullypresentduringcoachingsessions. • Iwillhonorandsupportwhatismostimportanttotheclient. • Iwillberespectful,honest,anddirectinconversation,includingconversations
aboutanythingIfeelmaybeaffectingthecoachingrelationship. • Duringsessions,Iwillcheck-inregularlyonwhattheclientisexperiencing. • Whilekeepingtrackofoutcomes,Iwillfocusoninvitingtheclienttoexplorewhat
theyarelearningaboutthemselvesduringthechangeprocess. • Iwillmakereferralsasnecessary(forthesakeofclientandcoach). • Iwillprotecttheclient’sconfidentialityandPersonalHealthInformation(PHI)in
accordancewithstandardsofdutytoreport.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
110|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER11:OUTCOMEVS.BEHAVIORALGOALS
Goal-settingtheoryidentifiestwodifferenttypesofgoals:
• Outcomegoals–focusedonadesiredresult,oroutcome. • Behavioralgoals–focusedonaspecificactionorbehavioroverwhichyouhave
control. Veteransoftencometocoachingwiththedesiretosetanoutcomegoal;forexample,“Iwanttolose15pounds”or“Iwanttoquitsmoking.”Whilethiscanfeelmotivatingatfirst,focusingonanoutcomeincreasesthelikelihoodaVeteranwillexperiencefeelingsoffrustrationsorfailureiftheyarenotsuccessful.Ultimately,theoutcomeisoutoftheVeteran’sdirectcontrol.WhattheVeterancancontrol,however,aretheactionsorbehaviorsthatleadtothatoutcome.Therefore,incoaching,itisoftenbettertosetbehavioralgoals.
SettingabehavioralgoalinvolvesfocusingspecificallyonstepsandactionsoverwhichtheVeteranshasdirectcontrol.Achievingabehavioralgoalimprovesself-efficacy,developsskills,andenhancesconfidencearoundspecificbehaviorsthattheVeterancanapplytomultiplesareasoftheirlife.ObstaclesthatarisearoundabehavioralgoalareovercomebytappingintotheVeteran’sstrengthsandsupports,againimprovingself-efficacyandempoweringtheVeterantoovercomefuturebarriers.
Toeffectivelysetabehavioralgoal,encouragetheVeterantodiscusswhatstepsorbehaviorsarenecessarytoachievethedesiredoutcome.Forexample,ifaVeteranhopestolose15poundsinthreemonths,askthemwhattheyhopetobedoinginthreemonthsthatwillleadtotheirdesiredoutcome.Perhapstheywanttobeworkingout4timesaweekoreatingthreeservingsoffruitsandvegetableseachday,orwalkingfor25minutesfivetimesaweek,orcookingfourdinnersathomeeachweek.Eachoftheseisanexampleofabehavioralgoal.Itmayormaynotleadtothedesiredoutcomebutworkingtowardthatgoalwillproduceresultsinthedesireddirection,whilebuildingtheVeteran’sconfidencethattheycan,infact,implementchange.
ConsidersomeofthequestionsbelowtohelpguidetheVeterantowardabehavioralgoal:
• Whatcanyoudothatwillhelpyou ? • Whataresomeofthebehaviorsyouhopetoincorporateinyourlife? • Whatwillyoubeabletodowhenyouaccomplish thatyoucannotdo
now?• Whatstepsdoyouseeyourselftakingtoachievethisgoal?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|111
• Howwillyourlifelookdifferentin3-6monthsthanitdoesnowwhenyouaccomplish______________?
Examples:
OutcomeGoal“WhatresultdoIwanttoachieve?”
BehavioralGoal“WhatwillIdotogetthatresult?”
Iwilllose15poundsin3months. In3months,Iwillexercise4timesaweekfor45minutes.
In6months,Iwillsleep7hours5nightsaweek.
In6months,Iwillmeditatefor30minutesbeforebed5nightsaweek.
In3months,Iwillhavelessanxiety. In3months,Iwillparticipateinyogatwiceaweek.
In4months,Iwillbeabletoruna5K. In4months,Iwillrunfor40minutes3timesaweek.
Whensettingbehavioralgoals,itisimportanttofollowSMARTcriteria:
• Specific • Measurable • Actionable • Realistic • Time-bound
Beginbyestablishingalong-termbehavioralSMARTgoal,andthensettingsmaller,incrementalstepseachsessionthatledtheVeterantowardthelong-termgoal.Afteralong-termbehavioralgoalisset,asktheVeteranwhatisoneactionthatwillgetthemclosertothatgoal.Oraskwhatthefirststepistheywouldneedtotake.Forexample,ifalong-termbehavioralgoalistoeatthreeservingsofvegetableseveryday,anactionstepforthenextweekmightbetoeattwoservingsofvegetablesonTuesdayandThursday.Long-termbehavioralSMARTgoalsareeasiertobreakdownintoactionsteps,increasingthelikelihoodofgoalattainmentandlifestylebehaviorchange.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
112|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER12:COACHINGTHEORIES
Behaviorchangeisacomplexprocessthatinvolvesmorethanadecisiontochange.Thecomponentsofbehaviorchangerangefromintrinsicmotivationtoneurologicalchangesthatoccurasanewhabitisformed.Thefieldofhealthandwellnesscoachingemergedfromstudiesinmotivation,behavioralneuroscience,andhealthpsychology.Healthcoachesarebehaviorchangeexpertswhounderstandscientifictheoriesthatunderlysustainablebehaviorchange.
Asahealthcoach,itisimportanttobefamiliarwithandutilizebasicbehaviorchangetheories.Inthischapter,youwillfindabriefoverviewofthefollowingtheories:
• TranstheoreticalModel(StagesofChange). • Travis-IllnessWellnessContinuum. • Self-DeterminationTheory. • SocialCognitiveTheory(includingSocialLearningTheoryandSelf-EfficacyTheory). • GrowthMindset.
TRANSTHEORETICALMODEL:SIXSTAGESOFCHANGE
Changeisnotalinearprocess,butoftenacyclicalone.TheTranstheoreticalModelofBehaviorChangeidentifiessixstagesofchangepeoplecyclethroughwhenimplementingbehaviorchange.RecognizingthestageofchangeaVeteranisinwithregardstoaspecificbehaviorchangewillhelpyourecognizethecoachingskillsthatwillbestsupporttheVeteraninimplementingchange.
Abriefdescriptionofeachstageofchangeisoutlinedbelow.AVeteranmaystartatanystageandmayshiftinoroutofonestageduringtheprocessofchange.Itisimportanttonote,Veteransmayalsobeindifferentstageswithregardstodifferentactions.
PRECONTEMPLATION
AVeteraninprecontemplationisnotreadytochangeandhasnointentionofchanginginthenext6months.Asacoach,youmaynoticeaVeteraninprecontemplationwithdrawingorbeingdefensivewhenchangeisaddressed.Youmayalsoheartalkoffailure,lackofawareness,orevenrationalizationofagivenbehavior.
WhencoachingaVeteraninprecontemplation,itisimportanttoholdthespace,listennon-judgmentally,buildrapport,anddemonstrateatrustingrelationship.UtilizingthePHIasaninitialexplorationmayormaynothelptheVeteranidentifyanunhealthybehavior;

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|113
allowthistobeacceptableand,instead,inviteinputanddiscussionaroundtheexperienceofcompletingthePHI.
CONTEMPLATION
AVeteranincontemplationseesreasonsbothforchangingandfornotchanging.Contemplationisthefirstsignwherechangeistrulybeingconsidered.Asacoach,youwilloftenheartheVeteranofferingreasonsfornotchanging,orfrequent“Yeah,but…”inresponsetoaspecificbehaviorchange.
WhencoachingaVeteranincontemplation,itisimportanttoholdthedecisionalbalanceandelicitchangetalk.Listenforboththereasonstochangeandnottochangeandreflectbothback.EncouragetheVeterantoverbalizetheprosandconsofchanging.UsevisioningquestionsthatencouragetheVeterantoconsidertheshortandlong-termconsequencesofnotchangingandofimplementingachange.Thecoachmayalsoimproveself-efficacybyaskingtheVeterantoidentifystrengthsandsupportsthatmaytipthebalanceinthedirectionofchange.
PREPARATION
AVeteraninpreparationhasmadethedecisiontoimplementchangeandisbeginningtoprepareforchange.Asacoach,youwillheartheVeterandiscussingthechange,supports,resources,andstrategies.Coachesmayalsohearexcitementaroundchangeorworryandfearoffailure.
WhencoachingaVeteraninpreparation,offerasupportiveenvironmentwheretheVeterancanopenlydiscussboththeirsupportsandtheirpotentialobstacles.EncouragetheVeterantocreatearealisticplanwithSMARTgoalsandcontingencyplans.Themorespecifictheplan,themorelikelytheVeteranwillbetoputtheplanintoaction.
ACTION
AVeteranintheactionstagehasimplementedchangewithinthepastmonthandisworkingondevelopingaplantosustainthechange.Asacoach,youwillheartheVeteranexpressingsuccessaroundimplementingactionsteps.
WhencoachingaVeteranintheactionstage,itisimportanttocontinuetoassesssuccesses,obstacles,andlearningsforeachactionstepinthechangeprocess.WorkwiththeVeterantomodifyactionsteps,ifneeded,creatingcontingencyplansasnewobstaclesarise.SupporttheVeteran’sself-efficacyandconfidencebyregularlyreflectingbackstrengthsandvaluesandlinkingthechangetotheVeteran’soverallhealthvision.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
114|VHA/OfficeofPatientCenteredCareandCulturalTransformation
MAINTENANCE
AVeteraninmaintenancehassustainedabehaviorchangeformorethansixmonths.WhencoachingaVeteraninmaintenance,itisimportanttoacknowledgetheeffort,strengths,andsuccessuptothispoint.EncouragetheVeterantoexpandtheirsupportnetworkstoincludeotherswhomaintainasimilarhabit.DiscusspotentialchallengesandthepossibilityofrelapsewiththeVeteran;helpthemidentifystrengths,tools,andcontingencyplanstocopewithfuturechallenges.
TERMINATION/ADOPTION(RELAPSE&RECYCLE)
Onceabehaviorhasbeenmaintainedformorethansixmonths,thecoachhelpstheVeterandeterminebetweenterminationandcontinuedmaintenance.WhencoachingaVeteranatthisstage,youmaysupporttheVeteranastheyworktoimplementnewbehaviors,summarizethebehaviorchangeprocess,andcelebratetheVeteran’saccomplishments.Ultimately,thecoachsupportstheVeterantomovetowardsindependenceinthebehaviorchangeprocess.
Evenafternewbehaviorshavebeenmaintained,thecoachrecognizesthatrelapseisatypicalpartofthechangeprocess.NormalizethisbyremindingtheVeterantheyhavebeenherebefore,sowhatdidtheylearnwhentheywereatthisstage?WhileitcanbedemoralizingfortheVeteran,thecoachremainscuriousandsupportive.AskwhattheVeteranlearnedpreviouslythatcanberecycled.Changeisnotalinearprocess,butoftenacyclicalone.
TRAVISILLNESS-WELLNESSCONTINUUM
TheTravisIllness-WellnessContinuumpresentswellnessindegreesofillnessandwellnessratherthanstatesof“illness”andstatesof“wellness.”Inaddition,theIllness-WellnessContinuumdemonstratestherelationshipofthetreatmentparadigmtothewellnessparadigm.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|115
Thetreatmentparadigm(medication,surgery,therapy,etc.)maybeusedtobringanindividualfromtheillnesssideofthecontinuumuptothe“neutral”point.Similarly,thewellnessparadigmmaybeimplementedatanypointonthecontinuum,helpingindividualsmoveasfartowardswellnessaspossible.
High-levelwellnessisnotdefinedbytheabsenceofillness.Instead,wellnessisdefinedbythechoicesonemakes.Researchhasalsoshownitmatterslesswhereoneisonthecontinuumandmoreinwhichdirectionheorsheisfacing.Asacoach,youcansupportaVeteraninimplementingactionsthatsupporthigh-levelwellness,includingself-care,positiveself-talk,creativity,improvingsurroundings,physicalmovement,activespirituality,positiverelationships,andpsychologicalself-care.UtilizingthePHIandtheCircleofHealthcanhelptheVeteranidentifywherechangeismostneeded.
SELF-DETERMINATIONTHEORY
Self-DeterminationTheoryexploreswhethermotivationisextrinsicorintrinsic,anditidentifieskeyfactorsthatsupportthedevelopmentofintrinsicmotivation.Ingeneral,changeiseithermotivatedextrinsically(byoutsidefactorssuchasmoneyorpraise)orintrinsically(byinternalfactorssuchassatisfactionandfun).Thehigherone’sintrinsicmotivationforchange,themorelikelyitisthebehaviorchangewillbesuccessful.
Self-DeterminationTheorynamesthreeuniversalneedsforpsychologicalhealthandwell-beingthatincreaseintrinsicmotivation:autonomy(notfeelingpersuadedorcontrolled),competence(confidence)andrelatedness(connectednesstoothers).Asacoach,itisimportanttofosterautonomy,competence,andrelatednessineverycoachingsession.
SOCIALCOGNITIVETHEORY
SocialCognitiveTheoryexplorestheimportanceofobservation,imitation,andmodelingonone’sperceivedself-efficacy.ManyVeteransarehesitanttoattemptchangebecausetheydonotbelievetheyarecapableofcreatingandsustaininganewhabit.Inotherwords,theirself-efficacymaynotbehighenoughtobeginthebehaviorchangeprocess.Asacoach,youcanworkwiththeVeterantoimprovetheirself-efficacybyutilizingsociallearningtheoryandself-efficacytheory.
SOCIALLEARNINGTHEORY
Sociallearningtheoryemphasizestheimportanceofobservationandrolemodelsasmotivators.Veteran’swithalowself-efficacymayfirstbenefitfromconsideringrolemodelsorotherswhohaveimplementedasimilarbehaviorchange;seeingthepossibility
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
116|VHA/OfficeofPatientCenteredCareandCulturalTransformation
ofchangeinothersmayencouragetheVeterantotakethatfirststeptowardschange.AschangeisimplementedandtheVeteranbeginstoexperiencesuccess,theirself-efficacywilllikelyincrease.ThemotivationforchangewillshiftfromtherolemodeltotheVeteran.
SELF-EFFICACYTHEORY
Self-efficacyreferstoone’sconfidenceintheirabilitytoachieveagoaloroutcome.Thelowerone’sself-efficacy,thelesslikelyactionwillbeattempted.Self-efficacyoftenincreaseswithsuccess,sothecoachsupportsSMARTactionstepswhileencouragingtheVeterantoconsidersupports,motivators,andpotentialchallenges.Asthisiscompletedoverandoveragain,theVeteranwillbegintotakeownershipoftheprocess.Overtime,theylearntheyhavetheabilitytonavigatetheupsanddownsofbehaviorchangeontheirown.
GROWTHMINDSET
Growthmindsetisthebeliefthatabilitiesarenotfixedbutcanbecontinuouslyimprovedwithexperimentationandpersistentefforts.Researchhasshownanindividual’sbeliefabouttheirowncapabilitieshasasignificantimpactonmotivation,effort,andresilience.Individualswhobelievetheirabilitiesareincontinuousdevelopmentaremorelikelytotakeonchallengesandchange.
CoachescanhelpaVeterandevelopagrowthmindset.Approachingbehaviorchangeasanexperimentwillsetthestageforchangeasanopportunitytolearnratherthansomethingatwhichtobeperfect.Whenassessingactionstaken,coachesshouldcuriouslyaskaboutsetbacks,listeningforstrengths,efforts,andsmallsuccesses;reflectthesemomentsbackandaffirmanyeffort,forethought,attemptorstrengthyouhear.RegularlydiscussinglearningsfromattemptedactionwillimprovetheVeteran’sresiliencyandcontinuetosupportagrowthmindset.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|117
CHAPTER13:THETRANSTHEORETICALMODEL–COACHINGAROUNDSTAGESOFCHANGE
TheTranstheoreticalModeldescribesbehaviorchangeasacyclicalprocesswithsixdifferentofstagesofchange:
• Precontemplation • Contemplation • Preparation • Action • Maintenance • Termination/Adoption(Relapse/Recycle)
AVeteranmaycometocoachingatanystageinthechangeprocessandmaymoveinandoutofdifferentstagesthroughoutcoaching.Asacoach,itishelpfultorecognizethestageofchangeaVeteranisinandutilizedifferentcoachingskillsaccordingly.Inthischapter,youwillbeintroducedtoeachstageofchange,howtorecognizeeachstage,andusefulcoachingskillsandstrategiesforeachstage.
PRECONTEMPLATION
AVeteraninprecontemplationisnotreadytochangeanddoesnotintendtochangeinthenext6months.
WHATTHEVETERANMIGHTSAY
Asacoach,youmaynoticeaVeteraninprecontemplationwithdrawingorbeingdefensivewhenchangeisaddressed.Youmayalsoheartalkoffailure,lackofawareness,orevenrationalizationofagivenbehavior.AVeteranmayfrequentlysay“Ican’t”or“Iwon’t”inresponsetoaspecificbehaviorchange.
AVeteraninprecontemplationmayhavemultipleresponsestochange.Somemaybeclearlyresistanttochangeandseenoimmediateneedforchange.Somemaywanttomakeachange,butdonotintendtomakeachangeinthenextsixmonths.Somemaybetoldtheyshouldorneedtomakeachange,butdonotintendtomakeachangeinthenextsixmonths.ThecoachshouldrecognizethataVeteranwhodoesnotintendtochangeinthenextsixmonthsisinprecontemplation.
THECOACH’SROLE
Asacoach,listenmindfullywithempathyandnonjudgment.ReflectwhattheVeteransharesandhonortheVeteran’sthoughtsandfeelingsaroundchange.Whenreflecting,

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
118|VHA/OfficeofPatientCenteredCareandCulturalTransformation
amplifyanyvaluesconflictsyouhear(“Soyourgrandchildrenyoulovesomucharenowonyourcasetostopsmoking”).Reflectthelackofreadinesstochange,andseedchange(“Youaren’treadytochangeyourdietyet”).Usingopen-endedquestionsandnonjudgmentalreflections,explorethereasonstheVeterandoesnotwanttochange.IftheVeteran’sstateisnotanimmediatehealthrisk,allowtheVeterantoexplorefreelyduringthestateofprecontemplation.
RecognizethatsomeVeteransmaybeinprecontemplationbecauseoflowself-efficacy.Usingopen-endedquestionsandreflections,exploretheprosofchange,theVeteran’sstrengths,andtheVeteran’ssupports.Acknowledgeanythought,effort,orpastsuccesstheVeteransharesinthisarea.
OtherVeteransmaybeinprecontemplationbecausetheyaremisinformedabouttherisksoftheircurrentbehavior.Usingopen-endedquestionsandreflections,exploretheircurrentknowledge.
IfaVeteranismisinformed,useElicit-Provide-Elicittoshareinformation.PersonalizetheinformationbasedontheVeteran’sspecificrisk.
USEFULQUESTIONS
ExploringprecontemplationisaboutunderstandingboththereservationsandthemotivationsoftheVeteran.BelowaresomepotentialquestionsthatmaybeusefulwhencoachingaVeteraninprecontemplation:
• Howwillyouknowthatit’stimetochange? • Whatwouldhavetohappenforthistobeaproblem? • Whatexperiencedoyouhavewithtryingtochangeinthepast? • Whatarethebenefitsofchanging? • Whatwillyourlifelooklikein5yearsifyoudon’t ? • Howdoesyourbehaviorimpactothers?
CONTEMPLATION
AVeteranincontemplationseesreasonsbothforchangingandfornotchanging.Contemplationisthefirststagewherechangeistrulybeingconsidered.
WHATTHEVETERANMIGHTSAY
Asacoach,youwilloftenheartheVeteranexpressingambivalenceordoubtaroundtheirabilityordesiretochange.TheVeteranmayofferreasonsfornotchanging,orfrequentlysay,“Yeah,but…”inresponsetoaspecificbehaviorchange.AVeteranwhoexpressesa
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|119
desiretochangebutstrugglestocommitorfollowthroughonanactionisusuallyincontemplation.
THECOACH’SROLE
WhencoachingaVeteranincontemplation,itisimportanttoholdthedecisionalbalance(seechapteronDecisionalBalance)andelicitchangetalk.HonortheVeteran’sambivalenceandcompetingagendas;listenforboththereasonstochangeandnottochangeandreflectbothback.ElicitmotivationbyallowingtheVeteranspacetoprocesstheprosandconsofbothchangingandnotchanging.
Intentionalopen-endedquestionsarealsousefulwhencoachingaVeteranincontemplation.AskvisioningquestionsthatencouragetheVeterantoconsidertheshortandlong-termconsequencesofnotchangingandofimplementingachange.EncouragetheVeterantosharewhatmakesthechangeworththeeffort.Thecoachmayalsoimproveself-efficacybyaskingtheVeterantoidentifystrengthsandsupportsthatmaytipthebalanceinthedirectionofchange.
USEFULQUESTIONS
Usingdecisionalbalance,coachingaVeteranincontemplationismosteffectivewhenspaceisgivenfortheVeterantoexplorebothreasonsforandreasonsfornotchanging.BelowaresomepotentialquestionsthatmaybeusefulwhencoachingaVeteranincontemplation:
• Defaultself:Ifyoudonothingdifferent,whatwillyourlifelooklikein5years? • Optimalself:Ifyoudomakethischange,whatwillyourlifelooklikein5years? • Evokereasonsfornotchanging:Whatareyourreasonsfornotchanging?Whatare
theconsequencesofchanging? • Evokereasonsforchanging:Whatismotivatingyoutoconsiderthischange?What
arethebenefitsofchanging? • Whatmakesthischangeworththeeffort? • Howdoesmakingthischangehonoryourvalues? • Howwouldyourlifebebetterif…? • Whatwillhelpyoumakethischange?
PREPARATION
AVeteraninpreparationhasmadethedecisiontoimplementchangeandisbeginningtoprepareforchangewithinthenextmonth.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
120|VHA/OfficeofPatientCenteredCareandCulturalTransformation
WHATTHEVETERANMIGHTSAY
Asacoach,youwillheartheVeterandiscussingthechange,supports,resources,andstrategies.TheVeteranmaysay“Iplanto…”or“Iamgoingto…”.Coachesmayalsohearexcitementaroundchangeorworryandfearoffailure.
THECOACH’SROLE
WhencoachingaVeteraninpreparation,shiftthefocusfromelicitingmotivationtobuildingbehavioralskills.OfferasupportiveenvironmentwheretheVeterancanopenlydiscussboththeirsupportsandtheirpotentialobstacles.WorkwiththeVeterantocreatearealisticplanwithSMARTgoalsandcontingencyplansthatfitstheirlifestyle.Themorespecifictheplan,themorelikelytheVeteranwillbetoputtheplanintoaction.AssesstheVeteran’sconfidencearoundimplementingtheplanusingascalingquestion(0-10).IfaVeteranexpressesconfidencelessthan7,useopen-endedquestionstoexplorewhatwouldimprovetheirconfidence.
USEFULQUESTIONS
CoachingaVeteraninpreparationisfocusedongarneringsupportsandskillsthattheVeteranmayusetosuccessfullyimplementabehaviorchange.BelowaresomepotentialquestionsthatmaybeusefulwhencoachingaVeteraninpreparation:
• Howwillyoumakethischange? • Whatisthefirststepyouarewillingtotake? • Whenwillyoudothis? • Whatsupportsdoyouneedtotakethefirststep? • Whatmightgetintheway? • Whatisyourbackupplan?
ACTION
AVeteranintheactionstagehasimplementedchangewithinthepastmonthandisworkingondevelopingaplantosustainthechange.
WHATTHEVETERANMIGHTSAY
Asacoach,youwillheartheVeteransharingsuccessandobstaclesaroundimplementingbehaviorchange.TheVeteranmightsay“Iamdoing…”,“Iattempted…”,or“Thisweek,Itried…”.AVeteranintheactionstageisactivelyworkingtoimplementabehaviorchange.
THECOACH’SROLE
WhencoachingaVeteraninAction,itisimportanttoassesssuccesses,obstacles,andlearningsforeachactionstepinthechangeprocess.Supportsmallsuccesses,acknowledge

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|121
effort,andreframeobstaclesaslearningopportunities.Normalizeobstaclesandsetbacksaspartoftheongoinglearningprocessinvolvedinanybehaviorchange.
Whenmodifyingorcreatinganewactionstep,ensureeachactionstepisintheSMARTformatandclearlyalignswiththeVeteran’slong-termgoaloroverallhealthvision.Assesssupports,accountability,obstacles,contingencyplans,andconfidenceforeachactionstep.EnsuretheVeteranhasaclearplaninplaceaftereachsession.SupporttheVeteran’sself-efficacyandconfidencebyregularlyreflectingbackstrengthsandvaluesandlinkingthechangetotheVeteran’soverallhealthvision.
USEFULQUESTIONS
• Whatwentwellwithimplementingthechange? • Whatobstaclesdidyouencounter? • Whatdidyoulearnwhentryingthisaction? • Whatsmallstepwouldyouliketotakenext? • Whatsupportsdoyouneed? • Whatmightgetintheway? • Whatwillyoudoif ?Whatisyourcontingencyplan? • Howconfidentareyouonascaleof1to10youwillcompleteyournextstep?
MAINTENANCE
AVeteraninmaintenancehassustainedabehaviorchangeformorethansixmonths.
WHATTHEVETERANMIGHTSAY
Asacoach,youwillseeorheartheVeterandescribingabehaviortheyhavesustainedforatleastsixmonths.
THECOACH’SROLE
WhencoachingaVeteraninmaintenance,itisimportanttoacknowledgetheeffort,strengths,andsuccessuptothispoint.Useopen-endedquestionsandreflectionstoexplorehowthebehaviorchangelinkswiththeVeteran’svalues.ReflectthebigpictureofchangeandcelebratetheVeteran’ssuccess.
EncouragetheVeterantoexpandtheirsupportnetworkstoincludeotherswhomaintainasimilarhabit.DiscusspotentialchallengesandthepossibilityofrelapsewiththeVeteran;helpthemidentifystrengths,tools,andcontingencyplanstocopewithfuturechallenges.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
122|VHA/OfficeofPatientCenteredCareandCulturalTransformation
USEFULQUESTIONS
AVeteraninmaintenanceneedstonotonlycelebratetheirsuccess,butalsodevelopaplantomaintaintheirprogressandconfrontfutureobstacles.BelowaresomepotentialquestionsthatmaybeusefulwhencoachingaVeteraninmaintenance:
• Whatishelpingyoutochange? • Whatwillhelpyousustainyourchange? • Whatwouldputyourchangeatrisk? • Ifyoufindyourselffacedwith[thisrisk],howdoyouplantoconfrontit?
TERMINATION/ADOPTION(RELAPSE/RECYCLE)
Onceabehaviorhasbeenmaintainedformorethansixmonths,thecoachhelpstheVeterandeterminebetweenterminationandcontinuedmaintenance.
WHATTHEVETERANMIGHTSAY
Asacoach,youmayhearaVeteranexpressingadesiretoexploreanewbehaviorchangeortoconcludecoachingsessions.AVeteranmightsay“I’mreadyto…”,takingownershipoftheirbehaviorchangeprocess.
THECOACH’SROLE
Atthisstage,aVeteranhassuccessfullymaintainedabehaviorformorethansixmonthsandisreadyforoneoftwopaths:terminationoradoption.TerminationwilllikelyleadtotheconclusionofcoachingwithaVeteran.AdoptionallowstheVeterananopportunitytocontinuecoachingandworktoimplementnewbehaviors.
IfaVeteranchoosestoendthecoachingrelationship,itisimportanttosummarizethebehaviorchangeprocess,celebratetheVeteran’saccomplishments,andexploretheVeteran’slearnings.
Anotherimportantpieceofendingthecoachingrelationshipisplanningforthefuture.Asacoach,itisimportanttoensuretheVeteranunderstandsthatrelapseisatypicalpartofthechangeprocess.NormalizethisandencouragetheVeterantoconsiderwhatstrengths,supports,andlearningstheynowhavethattheycanrecycleinthefuture.BrainstormfutureobstaclesandbackupplanswiththeVeteransotheyarepreparedtomaintainthebehaviorindependently.
EnsuretheVeteranconsiderssignsthatindicatetheyneedfuturecoachingorsupportinthebehaviorchangeprocess.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|123
IfaVeteranchoosestocontinuecoaching,itislikelyyouwillsupporttheVeteranastheyworktoimplementnewbehaviors.Aswithtermination,summarizethebehaviorchangeprocess,celebratetheVeteran’saccomplishments,andexploretheVeteran’slearnings.Remaincuriousandsupportiveaboutanyrelapsethathappenswiththesuccessfulbehaviorchange.ExplorewhatstepstheVeteranwantstotakenextfortheirhealthandwellness.Usecuriousopen-endedquestionsandnonjudgmentalreflectionstoassesswhatstageofchangetheVeteranisinwithregardstothenewchange.AskwhattheVeteranhaslearnedpreviouslythatcanbeadoptedandrecycledastheybegintoimplementanewbehavior.Ultimately,thecoachsupportstheVeterantomovetowardsindependenceinthebehaviorchangeprocess.
USEFULQUESTIONS
Inthefinalstageofthebehaviorchangeprocess,thecoachencouragestheVeterantoexplorelearnings,strengths,supports,andsuccessesthatemergedduringbehaviorchange.BelowaresomepotentialquestionsthatmaybeusefulwhencoachingaVeteraninthetermination/adoption(recycle/relapse)stage:
• Whatareyoutakingawayfromthechangeprocess? • Whatmostsupportedyouinthechangeprocess? • Whatstrengthsdidyouusetoovercomeobstacles? • Whatobstaclesdoyouforeseeinthefuture? • Howdoyouplantoaddressrelapse? • Whatdidyoulearnthatcanberecycledforfuturechange? • Whatareyournextstepsforyourhealthandwellness? • Howwillyouknowyouneedcoachingorsupportinthefuture?
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
124|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER14:THEETHICSOFCOACHING
HealthCoachingisarelativelynewandevolvingfield.Trainingprogramsarerecognizinganimportantnichetheycanfillinaddressingtheneedsofthisnewendeavor.Academicprogramshavebegun.However,thisevolvinginterestandeducationalresponseshavearisenpriortoclearnationalguidelinesforpractice,trainingandethicsbeingestablished.AlthoughthereisaCodeofEthicsdevelopedbytheNationalBoardforHealthandWellnessCoaching(NBHWC)forcoachingingeneral,thereisnotacodeofethicsforHealthCoachesperse.Therearenostateregulationsnormonitoringofhealthcoaches;therefore,self-regulatoryethicsareveryimportant.Asthisfieldprogresses,ethicalstandardswillundoubtedlyproliferate.Untilthen,ethicalstandardsareaworkinprogress.
HealthcoachesworkingwithintheVHAsettingshouldfamiliarizethemselveswithVHAethicalguidelinesforallclinicians.
CoachesshouldbeawarethattheNBHWChasbeenrecognizedasaprimaryorganizationforsettingnationalstandardsforcoachingingeneral.InadditiontoaCodeofEthics,theyhavedeveloped:
• DefinitionofCoaching. • CoreCompetencies/Standards. • ProfessionalCoachCredentialing,includingongoingCEUrequirements. • OversightforEthicalConductReview. • OngoingSelf-RegulatoryOversight
Thepurposeofthischapteristooutlinebroadareasofethicalconcerns;thedetailsinhowtoaddresstheseconcernswillneedtobeimplementedbyindividualcoaches.Usingmature,professionaljudgment,andkeepingtheVeteran’sbestinterestattheforefrontwhenaddressingtheseconcernswillgoalongwayinfosteringanethicalcoachingpractice.
FACTORSCONTRIBUTINGTOCHOOSINGETHICALACTION
Beforeoutliningspecificareasofconcerns,itisusefultorecognizethattherearefactorsthatwillcontributetohowindividualcoacheswillrespondinethicalsituations.Someofthesefactorsareoutlinedanddetailedbelow.
INDIVIDUAL’SPERSONALCHARACTER
Coachesbringahistoryofpersonaldevelopmenttothecoachingsituation.Theattributesthatfollowhavebeendevelopedovertime,butcoachesmustconsciouslycontinueto

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|125
practicebehaviorconsistentwiththeseattributesinthecoachingsetting.Thesepersonalattributesare:
• PrudenceorPracticalWisdom.Carefullythinkingthroughthepotentialramificationsofanybehaviorandavoidingtheappearanceofimproprietyisacharacterskill/traitdevelopedfromyearsofexperience.Prudenceorpracticalwisdomalsoincludesthinkingthroughthelong-termconsequencesofanygivenbehavior.
• Integrity.Coachesactingoutofintegrity,beinghonest,andpromotingthebestinterestofVeteransarelesslikelytoencounterethicalissues.Coacheswithintegritydonotnecessarily“need”acodetoguidetheirethicalbehavior.Itcomesoutofasenseofintegrity.Infact,coacheswhopracticeintegrityandhavemoralreasoningskillsmayactuallypracticebehaviorthatgoesbeyondanywrittencodeofethics.
• Trustworthiness.Trustworthinesshasbeendiscussedingreaterdetailpreviouslyinthis chapter. Coaches who have worked to demonstrate trustworthiness in theirrelationshipswithVeteransarelesslikelytoencounterethicalissues.
• Respectfulness.Respectfulnessinvolvesbeingawareof,aswellashonoringtheVeteran’sbeliefsandvalues.PracticingRespectfulnesswillcertainlyreducetheincidentsofethicalconflicts.
• Compassion.UnderstandingandcaringabouttheVeteran’sfeelingsandlifeexperienceswilllimitanypotentialbehaviorsthatresultincompromisedethics.
MORALREASONING
Coacheswhocanreasonfromamoralperspectiveandtakeintoaccount“whatisinthebestinterestforthegreatergood”andnotjustinthecoaches’bestinterest,willhaveabasisformakingdecisionsthatwillresultinfewercompromisedethicalsituations.
PROFESSIONALETHICALIDENTITY
Professionsthemselvesdevelopbothwrittenandunwrittencodesofethicsovertime.Thesecodesaredevelopedbyboththeleadersandconstituentsoftheprofession.Howmuchethicsareemphasized,bothintermsoftrainingandcodeenforcement,begintodefinetheethicalcultureoftheprofession.Underlyingeachprofessionarephilosophicalprinciplesthatmayormaynotbeevidenttomembersoftheprofession.Theseunderlyingphilosophicalprinciplescanhaveanimpactontheprofession’sspokenandunspokencodeofethics.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
126|VHA/OfficeofPatientCenteredCareandCulturalTransformation
ETHICALTRAINING
Eventhoughethicalreasoninganddecisionmakingareheavilyinfluencedbycoaches’personalcharacter,ethicalchoicescanbeenhancedbytraining.Mostprofessionsprovidecoursesortraininginethicaldevelopment.IntheWHCtraining,weprovideopportunitiestoreasonandthinkwithcolleaguesregardingcoachingsituationsinwhichethicaldecisionsneedtobemade.Althoughtheremaynotbeonegiven,specificcourseofactionincomplexethicalsituations,coachesareprovidedanopportunitytothinkthroughpotentialethicalsituationsbeforetheyactuallyoccur.
COMPETENCE
Ifcoacheshavemasteredthecompetenciesofcoaching,therewillbefarfewerviolationsofprofessionalethics.Imbeddedinthecompetenciesofcoachingareattributesthathelptoavoidcompromisedethicalchoices.Thefollowingcompetencieslistedbelowareonlyafewexamplesofcompetenciesthatfostersoundethicaljudgment:
• PromotingtheVeteran’sagendaandbestinterest.CoacheswhokeeptheVeteran’sagendaandbestinterestinmindwillfindthemselvesinfewercompromisedethicalsituations.TheywillbereasoningfromwhatisinthebestinterestoftheVeteranratherthanfromwhatisinthebestinterestofme,thecoach.
• Co-creatingacoachingpartnership.IfcoachesaretrulyinterestedinpartneringwiththeVeteraninordertoassistinpromotingtheiroptimalhealth,theywillfindthemselvesactinginthepartner’sbestinterestinpotentialethicalsituations.
Inaddition,ascertificationbecomesarealityinthefieldofhealthcoaching,theprofessionitselfwillhaveaninfluenceinself-monitoring,andthosewhoarenotcompetentwillnotbecertifiedtopractice.Thisprofessionalinfluence,inadditiontopersonalcompetency,willimpactthenumberofethicalsituationsthatmayariseinthefield.
Inconcludingthissection,itisimportanttonotethatethicalscenariosarenotalwaysblackandwhite.Thereareseveralquestionsthatmaybehelpfulforcoachestoaskthemselvesinethicalsituations.Considerthesequestionswhenreviewingthe“10EthicalScenarios”intheHandoutsection(coveredduringin-persontraining).Answerstothesequestionswillbeinfluencedanddeterminedbythefactorsidentifiedabove.Thesequestionsare:
• Whataremyowninternalvalueconflicts? • Whobenefitsfromwhichcourseofaction? • Whatcorevalues(bothpersonalandprofessional)arebeingcompromised? • Whatcorevalues(bothpersonalandprofessional)arebeingstrengthened? • HowdoesmyVeteranwinorlose,dependingonthecourseofaction?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|127
• Withwhomwoulditbenefitmetoconsulttoexaminetheconflictsinvolved? Thefollowingquestionsmaybeusefulinnurturingethicalsensitivity:
• Whatisyour“gut”responsetothissituation? • Whatisthefocusofyourattention? • Whoelseisinvolvedinthissituation? • Whatmakesyouthink“Thisdoesnotfeelright”? • Whataretheissuesrelatedtocultureand/ordiversity? • Howdoesmyroleascoach(andprivilege)impactmysensitivityandchoices?
AREASOFCOACHINGREQUIRINGETHICALCONSIDERATION
Therearemanyscenariosincoachingwhereethicaldecisionswillneedtobemade.Thesescenariosaregroupedandoutlinedasfollows.
CONFIDENTIALITYVS.DUTYTOREPORT
Aswithallhealth-relatedprofessions,coachesshouldbecarefultoprotectVeteranconfidentiality.Insomesettingsandstates,theremaybe“dutytoreport”issues,especiallyifthecoachdeterminesthattheVeteranmaydopotentialharmtothemselvesorothers.Coachesshouldbecomefamiliarwiththedutytoreportproceduresintheirworkenvironments.Ifcoachesdeterminethatit’sinthebestinterestoftheVeterantoshareinformationwithanotherprofessional,coachesshouldfirstobtainVeteran’spermissionafterdiscussingthereasonsfortheircourseofactionwiththeVeteran.CoachesshouldhaveplacestokeepnotesandVeteraninformation,preferablysecuredwithlockandkeythatisnotavailabletoothers.
Itshouldbeclearlystatedthatsuicidalideationconstitutesalegaldutytoreportandisnotconsideredanethicaldilemma.
VETERAN-COACHRELATIONSHIP
Thereareseveralpotentialconcernstobeawareofunderthistopic.Theseinclude:
• Setclear,appropriate,andculturallysensitiveboundariesregardingphysicalcontact.
• AvoidanysexualmisconductwithVeterans. • ProvideclearandaccuratecommunicationaboutwhattheVeteranmightexpect
fromcoaching.Avoidover-promising. • AvoidexploitationofVeteranformonetaryorpersonalgain. • DiscussterminatingthecoachingrelationshipwhencoachesorVeteransdetermine
thatVeteranscouldbebetterservedbyanothercoachorprofessional. • Establishclearcommunicationbeforecoachingbeginsregardingthenumberand
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
128|VHA/OfficeofPatientCenteredCareandCulturalTransformation
lengthofsessions,finances,andthenatureofthecoachingrelationshipandconfidentiality.
• HonorandsupporttheVeteran’srighttoterminatethecoachingrelationship. • Avoidprovidinganyinformationthatcouldbeconstruedasmedicaladviceor
directingaVeteraninamedicaldirectionthatrunscountertotheirwishesandvalues.
• ConsiderterminatingthecoachingrelationshipwhenVeterans’andcoaches’valuesconflictsarecurrentlyorwillpotentiallyimpedetheeffectivenessofcoaching.
• KeepclearrecordsofsessionsandVeteran/coachagreements.Thiswillhelpinclearingupanymisunderstandingalongthecourseofcoaching.
• WhensolicitinginformationfromtheVeteran,onlysolicittheinformationthatisusefultothecoachingprocess.Havingadditionalinformationnotonlyhaspotentialethicalimplicationsbutcreatesmorepotentialliabilityforcoaches.
DUALORMULTIPLEROLES
Insomecases,thecoachmayfindthemselvesindualormultipleroleswithaVeteran.Forinstance,ifaVeteranisarelative,orVeteranandcoachworkforthesameinstitution,theremaybereasonstohavetheVeteranseekanothercoach.IftheVeteranisaneighborortheVeteranandcoachbelongtosameorganizationssuchasplacesofworship,theremaybeethicalconsiderationsbeforeenteringintoacoachingrelationship.
Also,ifthecoachhasanotherprofession,suchasbeingapsychologist,thecoachwillhavetobeclarifywiththeVeteranwhatroletheyarefulfillingwiththeVeteranandnotattempttoblendthetwo.IfthecoachandVeterandecidetochangethenatureoftheirprofessionalrelationship,itshouldbeexplicit,andtheVeteranshouldnotfeelpressuredtoassumethenewrole.Ifyouserveinanotherhealthcareprofession,beclearastowhichprofessionalguidelinesprevailinethicalsituations.
USEOFASSESSMENTS
Eventhoughassessments,suchasHealthRiskAssessmentsorPersonalHealthInventory,canbeveryusefulinincreasingself-awarenessandfurtheraction,theymustbehandledethically.
Coachesshouldknowthelimitationsofassessments,aswellastheirlimitsinexpertisetointerprettheresultsofassessments.Insomecases,coachesmaywanttoobtaintheservicesofanexperttoadministerandinterprettheassessment.ThisshouldonlybedonewiththeconsentoftheVeteran.Coachesshouldestablishclearboundariesintheuseofinformationtheyreceivefromanyassessment.Culturalsensitivityandconfidentialityarealsoimportantconsiderationsintheuseofassessments.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|129
LIMITSOFCOACHINGAGREEMENT
Inacoachingagreement,coachesshouldbecarefultoarticulatewhattheyareofferingandnotofferingtheVeteran.Thisshouldbeawrittenagreement,signedbyboththecoachandVeteran.Coachesshouldbecarefulnottoover-promisewhattheVeteranwillreceivefromcoaching.
IfcoachesdeterminethattheVeteranhasissuesthatarebeyondthescopeofthecoaches’expertise,theyshoulddiscussotherprofessionalassistancewiththeVeteran.“Whenindoubt,referout”istheguidingprincipletokeepinmind.
PROFESSIONALEXPECTATIONS
Althoughcoachesmayhaveconflictingvalueswithothercoachesorcoachingorganizations,itisexpectedthatcoacheswillnotdenigrateotherpersonsororganizationswithwhomtheirvalues/beliefsand/orofferingsmaydiffer.Coachesmaywantto“defend”whattheyhavetoofferversusanotherhealth-relatedprofessional;however,theyshouldacknowledgedifferenceswithoutplacingavalue(especiallyanegativevalue)ontheother’sservices.
CoachesshouldfamiliarizethemselveswiththeCodeofConductestablishedbytheNBHWC.Asthisfieldemerges,statesmaytakevaryingpositionsandenactlawsgoverningcoachingpractices.Itisimportantthatcoachesfamiliarizethemselveswithanystatelawthatmaypertaintothecoachingprofession.Thesearesubjecttochangeandcoachesshouldfindsourcestokeepthemselvesabreastofnewand/orchanginglaws.
COMMONETHICALBLINDSPOTS
Asahealthandwellnesscoach,maintainingastandardofethicsthatbestservestheVeteranisoftheutmostimportance.Bemindfulofbothyourpersonalandprofessionalcodeofethics,aswellassomecommonethicalblindspots:
• Sellingproductsand/orservices • Recordprotection • HIPAAviolation(sharingpatientinformation,PHI) • Relationships(dating,acquaintancesoffamily/friends) • Confidentialityboundaries(obligationtoVeteranvs.healthcaresystem) • Dualroles • Dutytoreport(safetyvs.knowledgeofunethicalbehavior)
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
130|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Otherethicalscenariosareaddressedduringthein-persontrainingandarereferencedinthehandoutssectionofthemanual.Remembertotrustyourinstinctand,whenindoubt,referout.
APPROACHINGETHICS:KEYPOINTS
Insummary,whenfacinganethicaldilemma,remembersomeofthekeypointsbelow:
• Useyourintuition. • Watchfor“redflags”,bemindfulofyourgutfeeling,andpayattention. • Rememberthescopeofpracticeforcoachingandanyotherlicensureorcertification
youhold. • Consultwithcolleaguesandreferasappropriate. • Seekandreceivementoring. • Seekconsultationorsupervisionasneeded. • Knowyoursupportingstructureandyourchainofcommunication. • Whenindoubt,referout.
SOURCESFORINFORMATIONINTHISCHAPTER
LawandEthicsinCoaching:HowtoSolveandAvoidDifficultProblemsinYourPractice,PatrickWilliamsandSharonAnderson,JohnWileyandSons,Hoboken,NewJersey,2006
TheNBHWCCodeofEthicsandScopeofPractice,NationalBoardforHealth&WellnessCoaching,website:www.nbhwc.org(*BothprovidedasHandoutsinthisParticipantManual.)

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|131
CHAPTER15:GROUPCOACHINGCONTINUED
Groupcoachingisaguidedgroupprocessledbyaprofessionalcoach.Theintentionofthegroupformatistomaximizetheindividualparticipants’combinedenergy,experience,andwisdomtoachieveindividualgoals(definitionadaptedfromGingerCockerham,MCC,GroupCoaching:AComprehensiveBlueprint;iUniverse,2011).
ESSENTIALELEMENTSOFGROUPCOACHING
Thespecificdetailsofgroupcoachingcanvaryacrossdifferentsituations,buttherearecertaincharacteristicsthatremainconsistentacrossgroups.Allcoachinggroupssharethefollowingqualities:
• Thecoachusesfoundationalcoachingskills. • Thecoachusesgroupcoachingskills. • Thegroupprocessfollowstheestablishedcoachingstructureandprocessmodel. • Participantschoosetojointhegroup. • Participantssetpersonalgoalsandcheckinregularlyforaccountability. • Groupsaretypicallycomprisedof6-12participants.
GROUPDESIGNCONSIDERATIONS
Whencreatingagroup,therearemanyfacetstoconsider.MostofthesearecoveredindetailaboveintheParts1and2Contentsection.
• Coachinggroupsaretypicallymadeupof6-12members.Theidealsizeforanygroupwilltakeintoconsiderationhowtobestoptimizeachievementofgroupgoals,anyuniqueparticipantcharacteristics,andthetimeframeallottedforthegroup.
• Closedgroupsarethoseinwhichallmembersstartthegroupatthesametime.Thistypeofgroupworksmosteasilyforgroupcoachingsinceitisimportantforeveryonetobecommitted,andaccountablefromoneweektothenext.Consistencyandcontinuityareimportantformomentuminreachinggoals.
• Opengroupsarethoseinwhichmemberscanjoinatanytime.Inanopengroup,theleaderwillneedtohaveaprocessfororientingnewmemberswhojoinlater,andformanagingthedepartureofgroupmemberswhofeeltheyhavemettheirgoal(oranyotherreason).Itisimportantthatindividualsdonotdropinandoutintermittently.Groupcoachingshouldnotbesporadicasinother“open”groupssuchasAAorWeightWatchers.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
132|VHA/OfficeofPatientCenteredCareandCulturalTransformation
RECRUITMENTANDSELECTIONCRITERIA
Indesigningagroup,itcanbeimportanttoclarifytheprocessforidentifyingandrecruitingpotentialgroupmembers.Insomecases,theymaybereferredbyaVAproviderorprogram.Word-of-mouthcanbeanotherpowerfulrecruitmenttool,ascanoutreachwithintheVAandtovariousexternalVeteranServiceOrganizations.
Itisoftendesirabletohaveparametersforinclusionorexclusioninthecoachinggroup.Ifso,thesecriteriashouldbespecific,determinedpriortorecruitmentandpublicizedasneeded.
GROUPFORMATCONSIDERATIONS
Whenstartingagroup,itmightbeautomatictothinkofanin-persongroupformatbutthinkingoutsidetheboxatotherformatsisoftentimesveryhelpful.OneexampleofthismightbeTele-healthwhichistypicallyconductedusingacamerawithparticipantsjoiningfromadistance,possiblydialinginfromhome.Avariationofthiswouldbeifthecoachleadsfromadistancewhilethegroupistogetherinoneroom.Therearemanypossiblevariationsintermsofformatandcoaches/groupleadersshouldbeopentoexploringallformats.
Timingandschedulingareotherformattingconsiderations.Thesemightincludedeterminingtheideallengthofeachsession,howmanysessions,willthegroupbeopen-ended,howmuchtimetoallowbetweensessionsandfinallythebesttimeofdaytomeet.Someofthesemightbedeterminedbythecoachandothersmightbedependentonmeetingtheneedsofthemajority.
Anotherconsiderationforgroupformatsiswhetheritwillbesinglethemedoramixedfocus.Anexampleofasinglethemedgroupwouldbeonethatfocusesonalifestyleissuelikeweightmanagementorachronicconditionlikediabetes.AmixedfocusgroupmightbeonethatworkswiththeCircleofHealthaddressingdifferentareaseachsession.Regardlessoftheareaoffocus,allgroupsshouldbeconductedfollowingthesetprocessmodel.
Insomegroups,informationmaybesharedrelevanttoatheme.Wheneveraneducationalcomponentisintroduced,itshouldbeofferedusingthecoachingskillsetofelicit-provide-elicit.
STEPSTOCONSIDERBEFOREBEGINNINGTHEGROUP
Therearestepsthecoachcantakebeforebeginningagrouptocreatethefoundationforasuccessfulgroupexperience.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|133
• PreparationandPresence-Prepareyourmaterialsandpracticewhateverhelpsyoutocomeintothepresentmoment,leavingbehindthepastandthefuturetobefullywithyourgroup.
• Systemization-Determinewhowillbeyoursupport:supervisor,mentor,referral,supportsystem,chainofcommand.Knowwhatthereportingprocessentailsintheeventareferralisrequired.
• Practice-“Practicemakesperfect”-themoreyoupracticegroupcoachingskillsandbecomefamiliarwiththecontentyouwanttodeliver,themoreconfidentyoubecome.
• CreatingaSafeSpace-Whilenocoachcanguaranteesafetytogroupmembers,effortsshouldbemadetosetuptheconditionstosupportasenseofsafetyandpredictabilityforthemembers.Manygroupcoacheshaveapartner–a“co-facilitator”.Thiscannotonlyprovidesafetyinnumbers,butitcanalsoenableonecoachtocontinuethesessionastheotherfocusesonamemberwhomightneedpersonalattention.
GROUPCOACHINGSTRUCTURE
Whenyouarefacilitatingaclosedgrouptherewillbeaninitialsession,ongoingsessions,andalastsession.Allparticipantstypicallystartandendtogetherunlesstheydropoutofthegroup.Eachgroupcoachingsessionconsistsofthreephases:beginning,body,andend.
• Initialgroupcoachingsessionstructure-ConsiderationsforsettingupandconductinganinitialgroupsessionaredescribedintheWHCFoundationsManual.Thebasicstepsareasfollows:
• Introductions-Choosehowtointroduceyourselfbasedonthedynamicyouwanttocreateinthegroup.Youmightintroduceyourselfatthesametimetheparticipantsdoorintroduceyourselfatthebeginningofthegroupbeforetheparticipantsdo.OneexampleishowitisdoneintheWHCcourse:name,role,funthing,etc.
• Intention/goalforthegroup-Settingtheintentionofthegroup,upfront,cancreateclarity,anopeningbookend,andsetsomegroupmembersateasearoundwhytheyaregathered.OnegroupmightbeintendedtoworkitswaythroughthePHI,whileanotherfocusesonweightloss,diabetescare,etc.Thisisoftentakencareofingroupadvertisementmaterialsorrecruitment.
• Describethegroupcoachingprocess-NotallVeteranswillbefamiliarwiththegroupcoachingprocessorstructure.Takingtime,intheinitialsession,toexplaintheprocess,format,andstructureofgroupcoachingcancreateclarityandeasewiththeunknown.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
134|VHA/OfficeofPatientCenteredCareandCulturalTransformation
GROUPGUIDELINES
Groupguidelines,oragreements,areanimportantpieceofanycoachinggroup.Consistencyandclarityindesigningtheguidelinesforyourgroupwillenableyoutospeaktothemiftheneedarisesduringagroupcoachingsession.Thecoachcaneitherelicitguidelinesfromthegrouporofferapre-determinedlistofguidelines.Ifthelatter,groupmembersshouldbeofferedanopportunitytorespondandaddormodifyasappropriate.Oncegroupguidelineshavebeenestablished,solicit/discusswiththegroupwhattodoiftheguidelinesarenotfollowed.
Commongroupguidelineareastoaddress:
• Confidentiality.Onequestiontoaskmightbe“whatdoyouneedtofeelsafeinthisgroup”?
• Howmemberswillrespectfullycommunicatewitheachother. o Bottom-lining.o Refrainingfromgivingadvice.o Refrainingfromcrosstalk.o Beingauthentic.
• Attendance o Beingontime.o Followingproceduresformake-upsand/ormissedinformation.
Thesearesomeexamplesofguidelinesforcommunicating.Otherguidelinesincluderespectforothers,balancingtime,andstayingontopic.
BEGINNINGTHEGROUP–INITIALSESSION
Coachinginagroupsettingmeansusingnotonlyfoundationalcoachingskills,butalsogroupcoaching“meta-skills”describedingroupmanagementskillsslide.Willparticipantsworkthroughthestagestogetherorprogressattheirownrate?
Itisimportanttoask“safe”open-endedquestionsinthegroupcoachingsession–thesearequestionsgroupmembersgenerallyfeelcomfortableanswering.Youmightelicitsomepossibilitiesfromthegroup,movingtoyourownideaswhennoneareoffered.Belowisalistofpossibleopen-endedquestionsthatcreateease,conveygenuineinterestandcuriosity,andfeelsafe.
• Whatbringsyoutothisgroup? • Whatdoyouhopetogetoutofthisgroup? • Whatwouldmakethisgroupagreatexperienceforyou? • Howcanyoumakethisgroupexperienceenjoyableforyourself,orothers?

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|135
• Howcanyouuseyourtimeinthisgroupmosteffectively?
MOVINGTHROUGHTHEGROUPSESSION
Onceintroductionshavebeencompleted,guidelinesdiscussed,andthegrouphasbeenmadecomfortablewithgenerallycuriousandsafequestions,itistimetomoveintothe“body”ofthegroupcoachingsession.Thebodyofthegroupsessionmightlooklikethis:
• Askinganopen-endedquestionthatinvitesgroupmemberstospeaktotheirareaof“focus”andhowitisconnectedtotheirvisionandvalues(Stage1-2).
• EncouragingeachgroupmembertocreateanActionStepthatmovesthemclosertotheirareaoffocusandultimatelytheirlong-termgoalforahealthierself.(Stage3).
• ItmightbehelpfultoincludesomeeducationalcontentontheStagesofChangeand/orSMARTGoals.
CLOSINGTHEINITIALGROUPSESSION
Bringingthegroupcoachingsessiontoanendisthefinalpieceinthecoach’sresponsibilitiesinholdingthegroup.Theabilitytocreatea“bookend”forthesessionbringsaclearandvisibleendtothegroup’stimetogether.Justasthecoachstartedthefirstsessionwithopen-ended,safe,questionstopromptcommunicationandflow;itisthesameinendingtheconversation.
• Askeachgroupmembertosummarize–inonesentence–whattheiractionstepwillbefortheupcomingweek.
• Inquirewhatgroupmembersare“takingaway”fromtheday’ssession.
ROUTINE-ONGOINGGROUPSESSIONSTRUCTURE
Routine–ongoinggroupsessionsarethesessionsthatoccurbetweentheinitialgroupcoachingsessionandthefinalsession.Thenumberofongoinggroupsessionsisoftendecidedpriortothegroup’sconvening.Oftenthesitemakesthedecisioninthenumberofsessionsaspecificgroupwillmeet,sendingthisinformationoutinadvertisementmaterialsandrecruitmentpostings.
Theongoingsessionsarethe“meat”ofthegroupcoachingexperience.Thisiswheremuchofthegroupcoachingworkgetsdone.Theon-going,consistentmeetingofgroupmembersistheformationofthegroup’srelationship,bond,andevenidentity.
Ongoinggroupcoachingsessionsfollowthesamebasicstructureateachmeeting:

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
136|VHA/OfficeofPatientCenteredCareandCulturalTransformation
OPENINGAROUTINEGROUPCOACHINGSESSION
Remindthegroupofpreviouslyagreeduponguidelines.Inviteeverymembertocheckinaccordingtoarequestedformat–usuallyanopen-endedquestion.Forexample:
• “Whatoneworddescribestheprogressyoumadewithyouractionstepinthepastweek?”
• “Whatthemewouldyouusetodescribehowyouractionstepwentthispastweek?”
BODYOFAROUTINEGROUPCOACHINGSESSION
Thecoachusesopen-endedquestionstoguidethediscussion,withafocuson1)processinggroupmembers’experiencessincethelastsessionand2)askinggroupmembersabouttheirprogresstowardgoalsandovercomingchallenges:
• “Whatsuccessesdidyouexperiencethisweek?”• “Whatwasachallengeforyouthisweek?”AND“Whatwasyourworkaround?”• “Whatdidyoulearnaboutyourselfthisweek?”
CLOSINGTHEROUTINEGROUPCOACHINGSESSION
Asthegroupcoachingsessionnearsitsend,thecoachshouldletthemembersknowtheallottedamountoftimeleft.Manygroupmembersfindthisannouncementhelpful;somefindtransparencyabouttheprocesscomforting.Thisisthebeginningofthebookend.
• “Whatareyoutakingawayfromyourtimeinthegroupthisweek?”• “Whatnewbehaviorwillyoutakeonthisweek?”• “Whatwouldyouliketobeheldaccountableforduringournextsession?”• “Whatareyoumostexcitedaboutfortheupcomingweek?
FINALROUTINEGROUPCOACHINGSESSION
Thefinalgroupcoachingsessionisthelasttimethisspecificgroupwillgather.Itistheendtotheirgroupcoachingexperiencetogether.Pointstoaddressinthefinalsessionaremeanttobringthegroupcoachingexperiencearoundfullcircle.
THEFINALSESSION
Reviewingtheprogressthatgroupmembershavemadesincethebeginningofthegroupisanappropriate–andmeaningful–wayto“begintheend”.Manymembersinthegroupwillhavemadenotable,meaningful,andsignificantbehavioralchanges.Somewillhavemadechangesandperhapsstumbled,redirected,orcompletelyquiet.Othergroupmembersmightnothavemadetheprogresstheyexpected.Allofthesememberswillneedan

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|137
opportunitytoputtheirvoiceintothegroup.Thecoach–usingacceptance,empathy,acknowledgment,willmeeteachmemberwheretheyaretobringtheirtimetoaclose.
BODYOFTHEFINALSESSION
Elicitwhatthegroupmembershavelearned(especiallywhatmightbeappliedinother,future,situations).Offertheopportunityforparticipantstoexpressfuturegoalsandpossibilitiesandtoidentifypotentialsupportandresources.
CLOSINGTHEFINALSESSION
The closing group coaching session often includes soliciting feedback about the group experience – both positive and enhancements – as well as a chance to share “last thoughts”. Group members may exchange contact information to stay in touch – this is an appropriate action so long as group members agree.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
138|VHA/OfficeofPatientCenteredCareandCulturalTransformation
CHAPTER16:EXAMINATIONPREPARATION
Untilrecently,therewerenonationalstandardsforhealthandwellnesscoaching.Anyonecouldcallthemselvesahealthcoach,regardlessoftrainingorexperience.Beginningin2010,expertsinthefieldofhealthandwellnesscoaching–leadersinscience-basededucation,practicalskillstraining,andresearchincoaching–volunteeredtheirtimeandeffortstodevelopacomprehensivenationalstandard.Afterworkingtogetherformanyyears,thisgroupofdedicatedvolunteerleaderspartneredwiththeNationalBoardofMedicalExaminers(NBME)toofferthefirstnationalcredentialingexam.In2017,thefirstnationalexamwasadministeredtocoachesacrossthecountry.
WHYPURSUECERTIFICATION?
Pursuingcertificationcanbeapersonaland/orprofessionalchoice.Currently,theVAdoesnotrequireWHCoachestobenationallycertified,thoughsomesitesmaycreatetheirownPositionDescriptions(PD)andmakethisapartoflocalsiterequirementsinthefuture.ManyVAHealthCareSystemsandMedicalCentersareintheprocessofhiringdedicatedWHCoachestotheirfacultyofhealthcareprofessionals.Thisiscurrentlyasite-by-sitedecision;yetpossiblesystemwiderequirementscouldbeonthehorizon.Nationalcertificationwillcertainlybepartofthatconversation.
Pursuingnationalcertificationoffersopportunities,bothpersonallyandprofessionally,toVHAWHCtrainedcoaches.ProfessionalstandardsandnationalcertificationwillempowerandequipcoachestomoveforwardinprovidingVeteranswithcoachingthatmeetsnationallyrecognizedrequirementsandcompetencies.
CERTIFICATIONWITHINTHEVHA
AlthoughtherearecurrentlynorequirementsofnationalcertificationforcoachesworkingintheVHA,thereisexpandingenergyandinteresttocoordinatetheeffortsoftheOPCC&CT,VHAVISNleadership,andthehundredsofVHApersonnelwhohavesuccessfullycompletedtheWholeHealthCoachtraining.OpportunitiestoworkwithinPACTteams,specialtyclinics,andmanyotherareasoftheVHAareopeningfornewhealthcoaches.Anenormousamountofworkhasbeendedicated,inthepast5years,togrowingtheWHCoachingprogramsothatparticipantswhosuccessfullycompletethetrainingarebetterpreparedtositforthenationalexam.
TheOfficeofPatientCenteredCareandCulturalTransformation(OPCC&CT)iscommittedtotheWHCoachingprogram,itstrainedcoaches,andtheprofessionalstandardprovidedbynationalcertification.Theirefforts,support,andresourcesarestronglyinplacetoassist
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|139
trainedhealthcoachesintheirindividualpursuitofnationalcertification.TheOPCC&CTisdedicatedtomodelinghowcoachescanbeintegratedintotheVHA–workingaspioneersinthetransformationofthehealthcaresystem.
InJanuary2020,thefirstWeek3WholeHealthCoaching:CertificationTrainingwasheld.InFY21theWeek3Certificationtrainingwascombinedwiththe2-weekFoundationsTrainingtocreateonecomprehensive3-WeekWHCTraining.Coachescompletingthe3-weekWHCTrainingbenefitbylearningandpracticingbothfoundationalandadvancedcoachingskills,strategies,andcompetencies.
Thiscomprehensive3-WeekWHCTrainingbringswithitanincreasedlevelofexpectation–asynchronousinstruction,additionaltelephoniccoachingsessions,advancedcoachingskills,anddedicatedgroup-coachingexperience.Theseadditionalhoursoftraining,alongwithastrongself-studyregimen,allowWHCCoachestomovetowardstheirgoalofsittingforthenationalcertificationexam.
CPTCODES
CoachingintheVHAisaconstantlygrowingandchangingprocess.Thereisincreasingsupportandimplementationofstandardsbeingcreatedtoaddopportunity,standardization,andregulationtothisnewprofessionalrole.OnJuly1,2019,theAmericanMedicalAssociation(AMA)announcedtheapprovalofthreedistinct“CategoryIII”CPTCodesfor“HealthandWellnessCoaching.”TheseCPTCodeswentintoeffectJanuary2020.
TheabilitytoapplyCPTCodestocoachingsessionswithVeteranswillhaveawideimpactonhealthcoachesacrosstheVHA.CoacheswhohavesuccessfullyreceivedtheirNationalCertificationwiththeNBHWCarequalifiedtoapplycodestotheirVeterancoachinginteractions–givingthemtheabilitytoaddreimbursementtopatientvisits.Anadditional,informationaldocumentregardingCPTCodescanbefoundintheHandoutsectionoftheParticipantManual.
EXAMPREP
Preparingforthenationalexamisessential.ThelearningandtrainingreceivedintheWHCTrainingisalignedwithNBHWCstandardsandcompetencies.TheintensiveandcomprehensivetrainingprovidesWHCcoachesintheVAwiththefundamentalcoachingqualities,skills,andstrategiestheyneedtocoachVeteransaroundtheVAsystem.
AsintensiveandcomprehensiveastheWHCtrainingis,itisnotsufficienttofullyprepareparticipantsforthenationalexam.Preparationfortheexamrequiresamulti-facetedapproach:WHCtraining,dedicatedself-study,andplentyofactualcoachingexperience.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
140|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Thischapterwillbrieflycovertheareasimportanttosuccessfullyprepareforthenationalexam.
RESOURCES
TheNBHWCwebsite(https://nbhwc.org)isthemostimportantresourceinthepursuitofnationalcertification.TheWHCtrainingfacultyconsiderthissitetheprimaryresourceinpreparationfortheexam.Allquestionsregardingthenationalexam,examrequirements,contentoutline,referencematerial,andanexhaustiveamountofhealthcoachingresourcesareavailable.
TheNBHWCalsoprovidesopportunitiesforcoachestostaycurrentandtakeadvantageofmanyhealthcoachingresources,throughsocialmedia,emailupdates,andQ&Awebinars.
Additionalhealthcoachingresourcesarereferencedduringthein-personWHCTraining,andadedicatedLinks&ResourcessectionisincludedintheWHCParticipantManual.
SELF-STUDY
Probablythemostimportantstrategytoprepareforthenationalexaminvolvesself-study.AlthoughtheWHCTrainingprovidesthefoundationalcoachingqualities,skills,andstrategiestocreateskilledandcompetenthealthcoaches,itisnotintendedto“prepare”coachesfortheexam.Thecombinationoftraining,self-study,andcoachingpracticearethefoundationsforexampreparation.
AnadditionalWHCExamPrepGuidehasbeencreatedtoaddtotheever-increasinglistofnationalexamresources.ThisguideisanexpansiveandcomprehensivereviewofallVHAWHCcoursematerialsandadditionalNBHWCContentOutlinetopics.SeparateOPCC&CTLandingPages,createdforWHCandAsynchronousLearning,bothincludelinksandreferencetotheExamPrepGuide.UtilizingtheNBHWCwebsiteforresourcereferencesiscrucial.ThesitecontainsanHWCCertifyingExaminationContentOutlinethatcanbedownloadedandusedasastudytool.ThisContentOutlineoffersanextensivelistofresources;takeadvantageofyourexistingknowledgetofocusonareaswhereyoucoulduseadditionallearningandsupport.OtherareastoreviewincludeNBHWCCodeofEthics,ScopeofPractice,andknowledgeofHealthandWellnessbiomarkers.Thematerialisthoroughandcomprehensive,sospendingeffortsinoneareaatatimemaybehelpful.
TheVHASharePointsitealsooffersawealthofhealthcoachinginformation,resources,andtoolsusefulforself-study.WHCTrainingmaterials(ParticipantManual,PowerPointSlides,andcoachingdemonstrationvideos)areavailabletoallVHAcoaches.Anadditional“SampleNBHWCExamStudyGuide”isofferedasanoptionalstudytool.Itisimportantto

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|141
rememberthatthisisa“sample”studyguide,whileitprovidesasenseofwhatisrequiredtopreparefortheexam,cannotberelieduponastheonlysourceofstudymaterial.
The3-WeekWHCTrainingincludesadditionalindependentlearningintheformofasynchronousonlinemodules.ThisasynchronousinstructionisrequiredtomeetNBHWCtrainingstandardsandbetterpreparestudentsforthenationalexamcontent,particularlyaroundHealth&Wellnessmaterial:chronicdiseasebiomarkers,healthbehaviors,andriskfactors.Participantsshouldconsiderthislearningintegraltotheirdevelopmentasqualifiedcoaches;breezingthroughtothefinishlinesimplyto“meettherequirement”shouldbesecondarytotheactuallearning.YourlearningwillsupportthequalityofcoachingprovidedtoVeteransANDincreasetheprobabilityofsuccessinbeingpreparedfortheexam.
Belowisalistofhelpfultipsforcontinuedself-studysuccess:
• Takeyourtimepreparing–don’trushtotaketheexam. • Createstudygroupswithfellowcoaches. • ExplorewhetheryoursitewillpurchasesomeoftheNBHWCreferencedcoaching
books. • Findanonline“examprep”course. • ListentoCommunityofPractice(COP)callsonSharePointregardingthenational
exam(call#31,32,33,34,and35). • UsetheExamGuideOverviewonSharePointasaresource(linkincludedin
References). • Receiveadditionalmentoring.
SELF-CAREDURINGPREPARATION
Ascoaches,youareawareoftheimportanceofbeingpresentandsupportingothers’self-care.Itisimportant,andvital,thatyoupracticethesesameskillsforyourselfduringyourtimeofpreparationfortheexam.Explorewhatreallymatterstoyouaboutthisopportunity.Understandtheimportanceofthisendeavorforyourselfasacoach;thiswillenableyoutostayfocusedasyoustudy,practice,andprepare.
Allowingampletimeforstudy,research,practice,andevenmorepractice,willmeanpacingyourselfandcreatingastudyschedulethatmaintainsbalanceinyourlife.Applyingwhatweknowaboutself-careforothers–toourselves–isanewskill.Creatingastudyschedulethatfeelsrightforyouwilladdtothatbalanceandpreparedness.Organization,timemanagement,andcommitmentwillbethebackbonetoyoursuccessfulstudyroutine.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
142|VHA/OfficeofPatientCenteredCareandCulturalTransformation
Creatingacentralizedlocation(physicalorelectronic)foryourstudymaterialsandresourceswillkeepyouorganizedandhelpinyoursuccess.
SELF-CAREBEFORETHEEXAM
You’vestudied,you’vepracticed,you’veprepared.Youhaveputinthelong,dedicatedhours.Preparingyourselfonthedayoftheexamisjustasimportantandhelpful.Thenationalexamhasarrived,andyouwanttobeatyourbest.Utilizewhatyouknowaboutrestandrecharge–andsleephygiene–tobeawakeandalert.Gettingagoodnight’ssleep,theweekleadingtotheexamwillincreaseyourabilitytofocusonexamday.
Propernutritionandhydrationarealsowaystoprepareyourself,body,andmind,forthetimeyouwillspendtakingtheexam.Foodsheavyinsugarorfat,orprocessedfoods,cancreateasluggishnessinyourmindandbody.Eatingwell,includingfreshfruitsandvegetables,willsupplyyouwiththeenergyrichnutrientsyouneedtomaintainyourstaminathroughthehour’slongexam.Contactingtheexamproctoringsitetoinquireaboutbringinghealthysnacksandwatermaybeonemoresuccessfulself-careapproach.
Onefinalself-caretoolyoumaychooseinvolvesvisualization.Visualizeyourselfsuccessfullyapproachingtheexam,takingtheexam,andcompletingtheexam.Thiscancreateameaningfulandpowerfulvisiontoholdcloseasyouprepare.Thistypeofvisualizationcanbedoneleadinguptotheexam,justbeforetheexam,andevenduring.Addinginmomentsofawarenessofbreathingmaybeanothermindfulawarenesspracticeyouutilize,bothpreparingforandtakingtheexam.Progressivemusclerelaxation,stretching,orbodyscanarealsohelpfulformanytesttakers.Practicewhatyouknowworksforyou–whateverbringsyouease,clarity,focus,andcalm.

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|143
RESOURCES&REFERENCES
WHOLEHEALTHWEBSITE
PublicWebsite(Internet):https://www.va.gov/wholehealth/
SharePoint(Intranet):https://dvagov.sharepoint.com/sites/VHAOPCC/Education/SitePages/Home.aspx
ExamGuideOverview(onSharePoint):https://dvagov.sharepoint.com/sites/VHAOPCC/Education/SitePages/WH-Coaching-National-Exam-Guide.aspxTheVAOfficeofPatientCenteredCareandCulturalTransformation(OPCC&CT)workswithVAleadershipandhealthcareproviderstotransformVA’shealthsystemfromthetraditionalmedicalmodel,whichfocusesontreatingspecificissues,toapersonalized,proactive,patient-drivenmodelthatpromoteswholehealthforVeteransandtheirfamilies.
• Personalizedcaremeansputtingyourneedsfirstandpartneringwithyoutocreateacustomizedhealthplanbasedonyourgoals,personalhistory,andlifestyle.
• Proactivecaremeansyourcareteamwillactivelyworkwithyoutofindpreventive,ratherthanreactive,optionsthatstrengthenyourindividual,innatecapacityforhealthandhealing—forexample,usingmind-bodyapproachesandnutritionalchangespriortosurgeryorchemotherapy.
• Patient-drivencareputsyouattheheadofyourpersonalhealthcareteam,soclinicianscangiveyoutheskills,resources,andsupporttodriveyourowncare.
TheVAisbuildingaproactiveandpersonalizedhealthcaresystemthathonorsVeterans’serviceandempowersthemtoachievetheirgreatestlevelofhealthandwell-being.AstheVAtransformsthedeliveryofcare,auniquecommunityforVeteransthatembracestheirdistinctiveneedsisbeingforged
ThepatientcenteredcaretransformationisgrowingandrobustinmanyVAfacilitiesacrossthecountry.ThroughLiveWholeHealth,OPCC&CTandVAareprovidingtheresourcestogiveVeterans,healthcareproviders,andstaffthefreedomtocreateacultureinwhichthistransformationcanflourish.Now,VeteransandprovidershavetheopportunitytoworktogethertodefinethefutureofWholeHealthcareatVA.
WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
144|VHA/OfficeofPatientCenteredCareandCulturalTransformation
COMMUNITYOFPRACTICECALLS
WholeHealthCoachingCommunityofPracticecall
• WholeHealthcoachingeducationandskill-development,subjectmatterexperts,bestpractices.
• Monthlycallon4thThursdayat2:00ET. • VANTS:1-800-767-1750,AccessCode43351• AdobeConnectlink:http://va-eerc-ees.adobeconnect.com/whcoachcop/
WholeHealth:ContinuetheConversationCommunityofPracticecall
• WholeHealthlearningandskill-development,subjectmatterexperts,bestpractices. • Monthlycallon1stThursdayat2:00ET. • VANTS:1-800-767-1750,AccessCode43351• AdobeConnectlink:http://va-eerc-ees.adobeconnect.com/wh_cop/
OTHERVARESOURCES
TherearemanyvaluableresourceswithintheVAsystemwhichmayprovideadditionaltrainingopportunitiestosupplementtheskillsandconceptslearnedintheWholeHealthCoachingprogram.Theseareasamplingonlyofwhatisavailable.Forspecificopportunitiesatyourlocation,pleasecontactyourimmediatesupervisor,HealthEducationCoordinator,HealthPromotions/DiseasePreventionProgramManager,HealthBehaviorCoordinator,WholeHealthCoordinator,orPatientCenteredCareCoordinatorforcoursesyouareeligibleandabletoattend.
• MotivationalInterviewing(NCP)• TEACH(NCP)• CREW(NCOD)• ClinicianCoaching(NCP)• TelephoneLifestyleCoaching(NCP)
MaketheConnectionstoriesfromVeterans,Servicemembers,andNationalGuard:https://maketheconnection.net/
TheseSharePointsitescontainmanyresourcesthatsupportWholeHealth:
VHANationalCenterforHealthPromotionandDiseasePrevention:http://vaww.infoshare.va.gov/sites/prevention/default.aspx

WHOLEHEALTHCOACHINGPARTICIPANTMANUAL
VHA/OfficeofPatientCenteredCareandCulturalTransformation|145
VHANationalCenterforOrganizationDevelopmenthttp://vaww.va.gov/NCOD/CREW.asp
TelephoneLifestyleCoachinghttps://dvagov.sharepoint.com/sites/VHAPrevention/TLC/default.aspx
SUGGESTEDWEBSITES
(ThesewebsitesareprovidedsolelyforadditionalinformationandarenotendorsementsbyeitherTechWerksortheVHA/OPCC&CT)
• InternationalCoachingFederation-http://www.coachfederation.org/• NationalBoardforHealth&WellnessCoaching–http://www.nbhwc.org• Health&WellnessCoachCertifyingExamination/ContentOutlinewithResources-
https://www.nbme.org/pdf/hwc/HWCCE_content_outline.pdf
SUGGESTEDREADINGMATERIALS
(ThesematerialsareprovidedsolelyforadditionalinformationandarenotendorsementsbyeitherTechWerksortheVHA/OPCC&CT)
• Britton,J.J.(2010).EffectiveGroupCoaching:TriedandTestedToolsandResourcesforOptimumCoachingResults.Hoboken,NJ:JohnWiley&Sons.
• Dossey,B.M.,Luck,S.,&Schaub,B.G.(2014).NurseCoaching:IntegrativeApproachesforHealthandWellbeing.NY.
• Dossey,B.M.,&Hess,D.(2013).ProfessionalNurseCoaching:AdvancesinNationalandGlobalHealthcareTransformation.GlobalAdvancesinHealthandMedicine,2(4),10-16.doi:10.7453/gahmj.2013.044GlobalAdvancesinHealthandMedicine—May2013Vol2No3 http://www.gahmj.com/toc/gahmj/2/3
• Miller,W.R.,&Rollnick,S.(2012).MotivationalInterviewing,ThirdEdition:HelpingPeopleChange.NewYork,NY:GuilfordPress.
• Rollnick,S.,Mason,P.,&Butler,C.C.(2010).HealthBehaviorChangeE-Book.St.Louis,MO:ElsevierHealthSciences.
• Rollnick,S.,Miller,W.R.,&Butler,C.C.(2012).MotivationalInterviewinginHealthCare:HelpingPatientsChangeBehavior.NewYork,NY:GuilfordPress.
• Whitworth,L.,Kimsey-House,H.,Kimsey-House,K.,&Sandahl,P.(2007).Co-ActiveCoaching:NewSkillsforCoachingPeopleTowardSuccessinWorkandLife.London,UnitedKingdom:NicholasBrealeyPublishing.