WHO | Nigeria Health - WHO | World Health Organization
62
Transcript of WHO | Nigeria Health - WHO | World Health Organization



Table of Contents
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Acronyms and Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Important Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
List of Figures and Tables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Part I: Vision for Health ICT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
PART I. SECTION 1: Strategic Context For Health ICT . . . . . . . . . . . . . . . . 14
PART I. SECTION 2: Vision For Health ICT . . . . . . . . . . . . . . . . . . . . . . . . . . 16
PART I. SECTION 3: Foundations For Change . . . . . . . . . . . . . . . . . . . . . . . 21
Part II: Action Plan for Health ICT . . . . . . . . . . . . . . . . . . . . . . . . 29
PART II. SECTION 1: Health ICT Theory of Change . . . . . . . . . . . . . . . . . . . . 29
PART II. SECTION 2: Health ICT Action Plan . . . . . . . . . . . . . . . . . . . . . . . 30
Part III: Monitoring & Evaluation Plan for Health ICT . . . . . . . . 35
PART III. SECTION 1: Monitoring & Evaluation Plan . . . . . . . . . . . . . . . . . . . 35
Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
APPENDIX 1: List of Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
APPENDIX 2: Health ICT Scenario Illustrating Change and Impact on Stakeholders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
APPENDIX 3: Recommended Nigeria Health ICT Architecture . . . . . . . . 39
APPENDIX 4: Proposed Governance Structure . . . . . . . . . . . . . . . . . . . . . 42
APPENDIX 5: Detailed Health ICT Action Plan . . . . . . . . . . . . . . . . . . . . . . 44
APPENDIX 6: Health ICT M&E Framework . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60

0 2 1 1 01
5
2A IA A FDDA CA F A D F A :C , M CFGD .F C ,. N CC F (
CA I A C GACC I A A A F GGFI 2A IA C F C A A F AM I C C FM I AC 2A IA A D A GIF I F A A F I C
F C DFI F : F F I GIF I 2A IA H CC M A I F 0 FID AF
FDD A AF FCF 0 FI A AP IMA A I C A NA GI GGCA AF F 0 FI C I
CAM I IF F I CC C : A F GGCA AF M F : I CAP F FFI A
C 0 F D A C F FFI A AF A I GF A:C FI GCA AF N F I F I A
FD M I C F FD
A C 0 I A -I D NFI A A F I A FD C -I D NFI A IF D G F AF FI I A GGCA AF F 0 F CG A M AM I C C
FM I F I C F C GIAFIA A A FI NACC A C IDF AP GIFMA MFI :C MAIF D FI
A :C GGCA AF F 0 A C FI
A GC NACC C F A A A IA F C , M CFGD 3 I I 3IAM FI A
GGCA AF F 0 F D 2A IA C F C I A I FI CC F FC I A C 0
F GGFI F I MA AF IF I A FFI A A M D GCF D F 0 : D A 2A IA ) R: C 0 NA C C CG :C C AM I
AM I C C FM I S
. - - 3 3 , F
F F I :C A A I F C - I C G :CA F 2A IA

0 2 1 1 01 A
5
IJR 4FBLSI 5 S BSFHJD 2 BMFVO F4FBLSI S BSFH EODTMFNS IBR CFFN EFUFLOPFE BNE P OETDFE SI OTHI SIF UJRJONB LFBEF RIJP P OUJEFE C SIF 4ONO BCLF JNJRSF OG 4FBLSI BNE 4ONO BCLF JNJRSF OG OMMTNJDBSJON
FDINOLOH IFJ LFBEF RIJP OLFR BNE FDOHNJSJON OG SIF R NF HJFR CFSVFFN IFBLSI BNE SFDINOLOH IBR CFFN P JDFLFRR
FUF BL O HBNJ BSJONR IBUF CFFN JNUOLUFE JN EFUFLOPJNH SIF RS BSFH 5S JR JMPORRJCLF SO NBMF BLL SIBS DONS JCTSFE SO SIJR PJFDF OG VO CTS VF VOTLE LJ F SO BD NOVLFEHF BR MBN BR VF DBN IF JNDLTEF CTS B F NOS LJMJSFE SO 0FPB SMFNSR OG 2FEF BL JNJRS OG 4FBLSI, SIF 2FEF BL JNJRS OG OMMTNJDBSJON
FDINOLOH , SIF BUJNH :NF JLLJON JUFR : ; OH BMMF 0FLJUF NJS, SIF JHF JBN 5NGO MBSJON FDINOLOH 0FUFLOPMFNS -HFND 5 0- , SIF BSJONBL
; JMB 4FBLSI B F 0FUFLOPMFNS -HFND , SIF BSJONBL -HFND GO SIF ONS OL OG -50 , SIF BSJONBL 4FBLSI 5NRT BNDF DIFMF 45 , BSJONBL -HFND GO 2OOE BNE 0 THR -EMJNJRS BSJON BNE ONS OL, SIF BSJONBL 5EFNSJS BNBHFMFNS
OMMJRRJON 5 , SIF 4FBLSI ;LBNNJNH FRFB DI BNE SBSJRSJDR 0FPB SMFNS OG 2FEF BL BPJSBL F JSO -EMJNJRS BSJON 4FBLSI BNE 4TMBN F UJDFR FD FSB JBS, SIF SBSF JNJRS JFR OG 4FBLSI, BNE SIF SBSF JNJRS JFR OG OMMTNJDBSJONR O
DJFNDF BNE FDINOLOH :SIF R B F SIF JHF JBN OMMTNJDBSJONR OMMJRRJON, SIF 0JHJSBL . JEHF 5NRSJSTSF, SIF NJUF RBL F UJDF ; OUJRJON 2TNE, SIF JHF JBN OMMTNJDBSJONR BSFLLJSF
JMJSFE, SIF FNS F GO BNBHFMFNS 0FUFLOPMFNS, BNE BLBW .BD CONF ;LD , SIF 1 ; 4 ;5 , SIF BSJONBL NJUF RJSJFR OMMJRRJON, SIF SBNEB ER
: HBNJ BSJON OG JHF JB, SIF FEJDBL BNE 0FNSBL OTNDJL OG JHF JB, OMPTSF ; OGFRRJONBLR FHJRS BSJON OTNDJL OG JHF JB AF DBNNOS SIBN FNOTHI BNE BD NOVLFEHF SIF JMMFNRF DONS JCTSJON G OM PB SNF R JN NON HOUF NMFNSBL O HBNJ BSJONR BNE SIF P JUBSF RFDSO RTDI BR SIF AO LE 4FBLSI : HBNJ BSJON, OIN NOV 5NDO PO BSFE, LJNSON 4FBLSI -DDFRR 5NJSJBSJUF, 4FBLSI 5NGO MBSJON RSFM ; OH BM 45 ; , 5N S BS LOCBL 4FBLSI
OLTSJONR, FDINOLOH -EUJRF R, -- 5 - 5 , ;BSIGJNEF 5NSF NBSJONBL, SIF 4FBLSI FGO M 2OTNEBSJON OG JHF JB, SIF ; BF FLS 2OTNEBSJON, BSF NBL -DSJON GO OCJLF
-LLJBNDF, OTPF PFDJBLF OCJLF -RRODJBSJON, BNE SIF ; JUBSF FDSO 4FBLSI -LLJBNDF OG JHF JB
BRSL SIJR DOLLBCO BSJUF MTLSJ RSB FIOLEF R BNE MTLSJ RFDSO BL EFUFLOPMFNS P ODFRR VOTLE NOS IBUF CFFN PORRJCLF VJSIOTS SIF GTNEJNH RTPPO S G OM SIF
O VFHJBN -HFND GO 0FUFLOPMFNS BNE OOPF BSJON SI OTHI SIF NJSFE BSJONR 2OTNEBSJON BSJSTEF JR BLRO ETF SO SIF 5 ) : 5N OTNS FBM GO GBDJLJSBSJNH BNE DOO EJNBSJNH SIJR DOLLBCO BSJUF P ODFRR AF VOTLE BLRO LJ F SO BD NOVLFEHF SIF FHFNRS JFG 5NRSJSTSF GO SIF VONEF GTL RTPPO S ON SIF B DIJSFDST F BNE IFBLSI JNGO MBSJON FWDIBNHF 451 PJFDF BNE RFUF BL OSIF R VIO VO FE SJ FLFRRL JN SIF CBD H OTNE ;- 4, JSBLABUF, BNE -RJB F4FBLSI 5NGO MBSJON FSVO SO NBMF B GFV AF RJNDF FL FWP FRR OT IFB SGFLS H BSJSTEF SO BLL VIO IBUF DONS JCTSFE JN ONF VB O BNOSIF SO SIF EFUFLOPMFNS OG SIJR JHF JBN 4FBLSI 5 S BSFHJD 2 BMFVO ( ( (
. , , MNJ 2A 25 .- ;F MBNFNS FD FSB 2FEF BL JNJRS OG 4FBLSI

6!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Acronyms and Abbreviations
AIDS Acquired Immunodeficiency Syndrome
CCT Conditional Cash Transfer
CDC Center for Disease Control and Prevention
CHAI Clinton Health Access Initiative
CMD Center for Management Development
CR Client Registry
CRSV Civil Registration and Vital Statistics
DBI Digital Bridge Institute
DPRS Department for Planning Research and Statistics
EMPI Enterprise Master Patient Index
EMR Electronic Medical Record
FCTA Federal Capital Territory Administration
FMCT Federal Ministry of Communication Technology
FMF Federal Ministry of Finance
FMOH Federal Ministry of Health
FR Facility Registry
GBB Galaxy Backbone
GSMA Groupe Speciale Mobile Association
HDCC Health Data Consultative Committee
HDGC Health Data Governance Committee
HIA Health in Africa
HIE Health Information Exchange
HIS Health Information System
HISP Health Information Systems Program
HIV Human Immunodeficiency Virus
HRH Human Resources for Health
HRIS Human Resource Management Information Systems
HWR Health Worker Registry
ICT Information and Communication Technology
ICT4SOML ICT for Saving One Million Lives

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!7
IFC International Finance Cooperation
IHE Integrating the Health Enterprise
IL Interoperability Layer
ITU International Telecommunications Union
IVR Interactive Voice Response
JSI John Snow International
LGA Local Government Area
LMIS Logistic Management Information System
M&E Monitoring and Evaluation
MAMA Mobile Alliance for Maternal Action
MCCT Mobile Conditional Cash Transfer
MCH Maternal and Child Health
MDCN Medical and Dental Council of Nigeria
MDA Ministries, Departments and Agencies
MDG Millennium Development Goal
MEMS Monitoring and Evaluation Management Services
MSH Management Sciences for Health
NACA National Agency for Control of AIDS
NAFDAC National Agency for Food and Drugs Administration and Control
NASCP National AIDS Control and Prevention Programme
NCC Nigeria Communications Commission
NCH National Council on Health
NCS Nigeria Computer Society
NDST Network Data Services and Technology Ltd.
NHIS National Health Insurance Scheme
NHMIS National Health Management Information System
NIGCOMSAT Nigeria Communications Satellite
NIMC National Identity Management Commission
NIMS National Identity Management System
NIN National Identification Number
NITDA National Information Technology Development Agency
NORAD Norwegian Agency for Development Cooperation
NPHCDA National Primary Health Care Development Agency

8!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
NPSCMP National Product Supply Chain Management Programme
NTBLCP National Tuberculosis and Leprosy Control Programme
NUC National Universities Commission
OPENHIE Open Health Information Exchange
PHC Primary Health Care
POS Point-of-Service
RH Reproductive Health
SCMS Supply Chain Management System
SDG Sustainable Development Goal
SHR Shared Health Record
SMS Short Message Service
SOML Saving One Million Lives
SON School of Nursing
SURE-P Subsidy Reinvestment and Empowerment Program
TS Terminology Service
TWG Technical Working Group
UHC Universal Health Coverage
UN United Nations
USAID United States Agency for International Development
USD United States Dollar
USPF Universal Service Provision Fund
WHO World Health Organization

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!9
Important Definitions
Both Health Information and Communication Technology (Health ICT) and electronic health (eHealth) refer to the use of information and com-munication technology (ICT) in support of health and health-related fields, including health care services; health surveillance; health literature; and health education, knowledge, and research. However, Health ICT is a more accessible term and extends beyond ‘electronic’ to involve concepts and systems (e.g., architecture and information systems) and communication (e.g., phone calls, bi-directional transfer of information) along with the necessary physical and technology infrastructure. Health ICT is more than electronic health records; it is applied across the health system and services to ensure continuity of patient care across time. It includes mobile health (mHealth) services, tele-health, health research, consumer health informatics to support individuals in health decision-making, and eLearning by health workers. In practical terms, Health ICT is a means of ensuring that correct health information is provided in a timely, coordinated and secure manner via electronic means for the purpose of improving the quality and efficiency of delivery of health services and prevention programs. mHealth services, in particular, focus on the application of mobile and other wireless technologies for health systems strengthening.
A Health ICT Strategy can serve as an umbrella for planning and coordinating different national Health ICT efforts while considering fundamental elements in terms of regulatory, governance, standards, human capacity, financing and policy contexts. An effective National Health ICT Strategy presents a set of interventions that the health sector plans to use to facilitate the efficient and effective delivery of services. Without an overarching national level strategy, ICT initiatives are left at the hands of individual organizations without coordi-nation and a guarantee that they are in the best interest of clients. A national level Health ICT Strategy with sector-wide participation and ownership is an effort to fill this gap.
Frameworks serve as guides, rules or well-defined approaches towards ad-dressing a particular matter. A Health ICT framework is specifically concerned with applying ICT in a health system. Different frameworks exist and can range from being general, and providing comprehensive approaches to governing the regulatory environment and guiding implementations within that context, to being specific and focusing on a particular aspect of Health ICT, such as data standards.
A roadmap is similar to a framework but is geared towards action. In a road-map, goals and their corresponding activities are aligned in sequence to achieve an overarching vision. Thus, roadmaps contain action plans, mecha-nisms to monitor progress and resource forecasts (i.e., time, human resources, equipment, budget). Roadmaps are typically developed with stakeholders and reflect consensus. Inputs include a vision, current state of affairs, barriers and recommendations.
A health information system (HIS) is a system that collects, transmits, stores and manages health-related data. The data can be patient-specific (or row-level data) or aggregate. Reports can typically be generated from an HIS. If a system is primarily being used to inform and support health management practices, the system is referred to as a health management information system.

10!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
An architecture is a conceptual framework that is used to inform data collec-tion, transmission, storage and sharing. Architectures show the integration of many components into a whole, as well as the interoperability that enables these components work together. Interoperability is the ability of an applica-tion or platform to establish a data exchange with another application or plat-form. For interoperability to occur, both services must use the same standards [for communication].
Standards serve as rules or guidelines that ensure consistency in the context in which they are applied. Standards can be used to align data, processes and systems. The standards development process is variable (e.g., govern-ment-mandated versus stakeholder-based). As such, it is possible for multiple standards to exist. Accordingly, formal alignment among the different stan-dards is necessary.
These definitions were adapted from “Assessing the Enabling Environment for ICTs for Health in Nigeria: A Review of Policies.” 1

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!11
List of Figures and Tables
Figures
FIGURE 1. Current State of Nigeria’s Enabling Environment for Health ICT
FIGURE 2. Nigeria National Health ICT Vision
FIGURE 3. A National Health Information Architecture Drawing from Existing Initiatives
FIGURE 4. Health ICT Governance Structure
FIGURE 5. Key Findings from Baseline Inventory Assessment on Number of Health ICT Implementations by Program Area
FIGURE 6. Theory of Change for the Nigeria National Health ICT Vision
Tables
TABLE 1. Components of the Health ICT Enabling Environment
TABLE 2. Summary of Recommendations to Improve Health ICT Enabling Environment
TABLE 3. Nigeria National Health ICT Vision Integrated Action Plan 2015 - 2020

12!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Executive Summary
Beginning in late 2014 and in the first half of 2015, the Nigerian Federal Ministry of Health (FMOH) and Federal Ministry of Communication Technology (FMCT) led the multi-sectoral and stakeholder development of the National Health Information and Communication Technology (Health ICT) Strategic Framework. This framework, which incorporates the effort and inputs of over 150 public and private health and technology sector stakeholders, is a three-part document that articulates the collective vision and necessary actions of stakeholders involved in the health system in Nigeria. Borne out of the recognition for the opportunities that ICT present to support health systems strengthening and the achievement of health system goals, the National Health ICT Strategic Framework positions Health ICT within the current con-text of the health system. This means addressing Universal Health Coverage (UHC), one of the main priorities of the Federal Government of Nigeria.
Strategic Context
Nigeria is poised to become a major global powerhouse. Currently, Nigeria is Africa’s largest economy and most populous nation. By 2050, Nigeria is expected to be one of the ten largest economies in the world and is already Africa’s most populous country. Despite these economic gains, close to half of the population lives in poverty and life expectancy is projected to only increase marginally. Accordingly, health needs and priorities, along with demographic trends, must be considered to ensure the appropriate allocation of resources and optimize strategies to address the issues.
The government is developing and implementing policies and programs to strengthen the National Health System to support attainment of UHC. Initial focus is on primary health care, and innovations including the use of Health ICT to improve service delivery, access and coverage have been prioritized. Health ICT must be in alignment with the clear, actionable goals of the health system to help achieve UHC and improve service delivery.
Health ICT Vision
Subsequently, the National Health ICT Vision was established through an iter-ative stakeholder engagement process led by the FMOH and FMCT. With UHC as a national health priority, the vision was articulated through the following powerful statement:
“By 2020, health ICT will help enable and deliver universal health coverage in Nigeria.”
To ensure that the vision can be achieved, the enabling environment com-ponents of the World Health Organization-International Telecommunications Union eHealth Strategy Toolkit were used to structure and craft the Health ICT Framework. The specific prioritized activities within Leadership and Governance; Strategy and Investment; Architecture, Standards and Interoperability; Legislation, Policy and Compliance; Capacity Building;

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!13
Infrastructure and Solutions (Services and Applications) reflect the current state and needs of the Nigerian health system as well as stakeholder recom-mendations on the appropriate Health ICT response.
Action and M&E Plans
Drawing from the recommendations for Health ICT to support the achieve-ment of UHC and other health system goals and activities, an action plan was developed. A Theory of Change included as part of this plan articulates the pathway to change from Health ICT enablers to prioritized ICT-related actions to health system priorities and the achievement of UHC. The action plan forms the basis for the roadmap and orients the implementation of prioritized activities. It informs the steps that those governing and involved with the achievement of the Health ICT vision will need to make. The monitoring and evaluation (M&E) plan and budget build on activities outlined in the action plan. The M&E plan provides a link between the vision, action plan and desired results and the budget estimates the resources needed to attain the vision. The indicators captured in the M&E plan reflect short- and long-term activities as guided by the Theory of Change.
The overall approach is separated into three phases over a five-year time period.
PHASE 1: Set-up (Year 1)
PHASE 2: Deploy, Maintain and Support (Year 2 and Year 3)
PHASE 3: Consolidate and Continuous Review (Year 4 and Year 5)
Over the next five years, the National Council on Health, as owners of the Health ICT vision, will oversee the activities according to the action plan. The council will be guided and supported by the Health ICT Steering Committee, Project Management Office and Technical Working Group. Working collabora-tively, the vision of Health ICT can be achieved.
This Nigerian National Health ICT Strategic Framework provides a vision and guide for alignment of current investments in technology within the health system towards a digitized health system that will help Nigeria achieve UHC by 2020.

14!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Part I: Vision for Health ICT
PART I. SECTION 1: STRATEGIC CONTEXT FOR HEALTH ICTWith a growing population and economy, Nigeria is emerging as a major global powerhouse. To maintain the path to prosperity, improvements in the health system are needed to ensure and optimize the health and wellbeing of the country’s citizens. The Government of Nigeria recognizes that a healthy population is important for socio-economic development.
As Africa’s largest economy and most populous nation, Nigeria is experiencing substantial economic expansion, yet the country’s health system is strained. The country’s economy is growing at an average annual rate of 7% and is expected to be among the ten largest economies by 2050.2,3 Despite the country’s economic gains, the overall health status of the Nigerian population is poor (as defined by the 2013 Nigeria Demographic and Health Survey);4 infectious and non-communicable diseases remain among the leading causes of morbidity and mortality,5,6,7,8 continuing to take their toll on the health and survival of Nigerians; and health coverage and financing remains low.9,10,11
Population and health status
•#Over 46% of the population continues to live in poverty (2010 estimate)2,3
•#Rural-urban divide is projected to increase 2,3
•# Maternal and under-five mortality rates remain high at 576 deaths per 100,000 live births and 201 deaths per 1,000 live births, respectively 4
•# Life expectancy at birth is projected to only increase marginally from 54.2 years to 56.2 years over the next 10 years (2015-2025) 2,3
Burden of infectious and non-communicable diseases
•# Nigeria is second to South Africa in the number of people living with HIV/AIDs worldwide. This represent 9% of Global burden of the disease” and a declining prevalence rate of 4.1 as of 2010. (NDHS 2013, page 224)
•#Malaria is the leading cause of infant and child mortality 7
•# Diseases such as hypertension, diabetes and coronary heart disease also represent an increasing share of Nigerians’ burden of disease 4
Low health coverage and financing
•#As of 2013, fewer than 5% of the population were insured 4
•# Nigeria is among the 23 African nations that spends more than USD44 per capita on health care, however, the government expenditure on health is 6.1% of the gross domestic product — which is below the Abuja Declaration’s target of 15% 7, 9

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!15
Despite the health challenges, Nigeria’s rising telecommunications and infor-mation and communication (ICT) sectors and the global proliferation of ICT for health (Health ICT) are creating new opportunities to strengthen the health sys-tem and improve the overall delivery of health services. Accordingly, Health ICT can be used to generate demand, increase access to and improve the quality of health services. Furthermore, Health ICT addresses the critical need to coor-dinate information and resources across the health system in a timely manner.
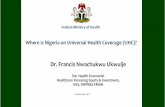
As a result of these opportunities and the Government of Nigeria’s commit-ment to ICT, an assessment of the enabling environment for Health ICT was conducted in 2014. The report, Assessing the Enabling Environment for ICTs for Health in Nigeria, identified the need for a coordinated Health ICT Strategy. In addition, the report concluded that Nigeria is transitioning from ‘experimen-tation and early adoption’ to ‘developing and building up’ (see Figure 1).12
In order to advance the enabling environment and support scale-up of ini-tiatives, a unifying Health ICT Strategic Framework is required. A Health ICT Strategy will enable Nigeria to leverage current and future ICT investments to build an integrated national health information infrastructure and help enable Universal Health Coverage (UHC) by 2020.
FIGURE 1. Current State of Nigeria’s Enabling Environment for Health ICT 13
COMPLETED TRAJECTORYOF NIGERIA ICT
DESIRED TRAJECTORYOF NIGERIA ICT
EMERGING ENABLING
ENVIRONMENTFOR eHEALTH
EMERGING ICT ENVIRONMENT
ESTABLISHED ICT ENVIRONMENT
EARLYADOPTION
SCALE UP
EXPERIMENTATION
DEVELOPING & BUILDING UP
I.
II. III.ESTABLISHED
ENABLING ENVIRONMENTFOR eHEALTH
MAINSTREAMING
CURRENT STATUSOF NIGERIA ICT

16!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Identifying the potentials of Health ICT, the Government of Nigeria has begun to prepare and introduce the necessary building blocks to facilitate the digitization of the health system. The Federal Ministry of Health (FMOH) and the Federal Ministry of Communication Technology (FMCT) have collab-oratively led an inclusive effort to set-up this strategic framework for Health ICT as well as a guiding architecture, health information exchange (HIE) and supportive policies, plans and budgets to improve health and wellbeing for all citizens through technological advancements and innovation. This document, the National Health ICT Strategic Framework, is meant to guide the deliberate and judicious use of ICT within the health system to enable the delivery of quality, affordable and equitable health services to all citizens. This National Health ICT Strategic Framework will facilitate the identification, prioritization and implementation of appropriate technologies that can potentially lead to a strengthened national health system.
PART I. SECTION 2: VISION FOR HEALTH ICTThe FMOH, in collaboration with the FMCT and other Government of Nigeria Ministries, Departments and Agencies (MDAs); donors; and implementing partners, (see Appendix 1) has developed, through an inclusive and iterative process, a collective vision for the use of Health ICTs in Nigeria.
“ By 2020, health ICT will help enable and deliver universal health coverage in Nigeria.”
UHC attainment will ensure that all Nigerians have access to the services they need without incurring financial risks. Specifically, UHC means health insur-ance becomes economical, whereby the cost of care is not a burden. It means equitable access to affordable and quality health services. It also means that the health system must be functional to ensure that supply meets the needs specified by demand. It is because of this last point that the value of Health ICT is so substantial. With its ability to support health systems strengthening, Health ICT can be used to improve the health system and ensure its adequacy for scaling up health insurance and health coverage over the next five years.
The successful use of Health ICTs to achieve UHC in Nigeria will achieve:
•# Improved access to health services through the effective use of tele-medicine and other ICTs for health worker training and support
•# Improved coverage of health services through the effective use of Civil Registration and Vital Statistics (CRVS), National Identity Management System (NIMS), Human Resource Management Information Systems (HRIS), National Health Management Information System (NHMIS) and Logistic Management Information System (LMIS) for tracking demand and supply of health services and commodities
•# Increased uptake of health services through the effective use of mobile messaging and cash transfer incentives for demand creation
•# Improved quality of care through the effective use of ICT for decision support within the continuum of care

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!17
•# Increased financial coverage for health care services through the ef-fective use of ICT for the national health insurance scheme (NHIS) and other health-related financial transactions
•# Increased equity in access to and quality of health services, informa-tion, and financing through the effective use of ICTs for delivering appropriate health services for those who need them
Figure 2 depicts the Nigeria National Health ICT Vision, mapping the goal of UHC with Health ICT outcomes and the long-term ICT output. The National Health ICT Vision embodies the development goals of the Government of Nigeria and provides a concrete target for stepwise, long-term investments into nationally scaled and integrated Health ICT services and applications. This would all be supported by a national Health Information Exchange (HIE), and implemented with appropriate governance, funding, infrastructure & equip-ment, training and policies.
FIGURE 2. Nigeria National Health ICT Vision
By 2020, Health ICT will help deliver and enable universal health coverage — whereby Nigerians will have access to the services they need without incurring financial risk.
NIGERIANATIONAL HEALTH
ICT VISION
Nationally scaled integrated Health ICT services and applications supported byNigerian Health Information Exchange implemented with appropriate funding,
infrastructure & equipment, training & policies.
LONG-TERMICT OUTPUTS
Effective use of telemedicine
and use of ICT for health
worker training and support
Effective use of CRVS, HRIS,
NHMIS & LMIS for tracking demand and
supply of health services and commodities
Effective useof mobile
messaging & cash transfers for demand
creation
Effective use of ICT for decision
support & within the continuum
of care
Effective useof ICT for
health insurance &
other health-related
financial transactions
Effective useof ICTs for delivering
appropriate health services for those who
need themmost based on epidemiology
and abilityto pay
Improvedaccess to
healthservices
Increased coverage of
health services
Increased uptake of
health services
Improvedquality of care
Increased financial
coverage for health care
Increased equity in,
access to, and quality of
health services, information,
and financing.
HEALTH ICT OUTCOMES
UHC OUTCOMES

18!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
In recognition of the significant Health ICT investments already underway in Nigeria, this Health ICT Strategic Framework draws from and seeks to coor-dinate existing projects. As a part of this, an architecture that focuses on the long-term impact of Health ICT will be established. Such a forward-looking architecture will enable the achievement of the vision, while also setting the stage for the sustainable use of Health ICTs across the entire health system. Figure 3 provides an example of what the integration of several key information systems (private and public sectors) in Nigeria could look like within an over-arching architecture. Existing and planned digital point of care tools, such as insurance registration and claims systems, Electronic Medical Records (EMRs), laboratory and hospital information systems, mobile health (mHealth) solutions and Monitoring and Evaluation (M&E) applications could leverage shared health
information services.
Building on both the Vision (with its Health ICT outputs) and architecture, the following scenario illustrates the crosscutting impact that could be possible
FIGURE 3. A National Health Information Architecture Based on Some Existing Initiatives
M&E-DPRS
SECURITY + INTEROPERABILITY Not yet in development
NHIS + NIMC M&E-DPRS NACA +NPHCDA NAFDAC HRH-DPRS
M&EApplications
Mobile Applications
Clinical Record Systems
Hospital Information
Systems
Laboratory Information
Systems
Existing Institutional Initiatives
Existing Shared Health Information Services
Interoperability Layer
Point Of Care Systems
Registry of Health
Facilities
Registry of Clients
National Health
Management Information
System (NHMIS)
Shared Health Records
Terminology Service
Registry of Health
Workers

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!19
with an integrated ICT-enabled health system. It describes a collection of Health ICT advances that are not currently deployed across the three tiers of the Nigerian health system. (See Appendix 2 for the entire scenario and Appendix 3 for information on the Health ICT Architecture.)
While the scenario presented is aspirational, it identifies several capabilities of an ICT-enabled health system, such as the following:
•#Ability to capture and exchange patient-level healthcare information
•#Ability to exchange and report aggregate healthcare information
•#Ability to enroll, pay for health insurance and verify coverage
•# Ability to send appointment and care alerts to patients and health workers
•#Ability for patients to send alerts to health care facilities
•#Availability of electronic training and reference materials
TABLE 1. Components of the Health ICT Enabling Environment
COMPONENT DESCRIPTION
Leadership and Governance Focuses on the oversight and coordination of Health ICT activities at the federal, state and local levels, ensuring alignment with national health goals and priorities
Strategy and Investment Describes the planning for, engagement of and alignment with all stakeholders involved in Health ICT activities and procurement of financing for Health ICT. It also outlines strategies to mobilize ICT in positioning health as an investment with good return to Nigeria economy.
Legislation, Policy and Compliance
Covers national policies and legislation for Health ICT in terms of development, alignment and regular review
Architecture, Standards and Interoperability
Describes the development and use of enterprise architecture and standards for enhanced interoperability, integration and health information exchange
Capacity Building Details the empowerment of the health and ICT workforce to develop, use and maintain Health ICT through education and training programs
Infrastructure Refers to the physical facilities and related assets that forms the foundation for Health ICT implementations
Solutions (Services and Applications)
Reports on devices and tools utilized by end users to collect, transmit, access and maintain health information
Adapted from the 2012 WHO-ITU eHealth Strategy Toolkit,15 Table 4
First printed in the report, “Assessing the Enabling Environment for ICTs for Health in Nigeria: A Review of Policies” 16

20!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
SCENARIO: THE HEALTH ICT VISION IN PRACTICE — IMPACT ON STAKEHOLDERS
A few months ago, Fatima enrolled with the NHIS*. Now, Fatima was expecting and due at any time. When she first learned that she was pregnant, she decided to sign up for weekly SMS* notifications about her pregnancy and to receive appointment reminders and pregnancy-care health information. When Fatima felt contractions, her family members texted the local clinic and called a taxi. Fatima proceeded to the clinic.
Mary arrived at work right on time. She was excited for the day. During shift hand-over, she and her co-worker huddled over one of the clinic’s tablets going through the different cases of clients present at the clinic. They prioritized the cases and she got to work. Shortly thereafter, Mary saw that a woman in labor was making her way to the clinic.
When Fatima arrived, she and her husband realized they had left the NHIS card at home in the hurry. But they were lucky, her NIN* was stored in her husband’s phone contact. With the cross-reference she was triaged. During her assessment of Fatima, Mary observed that the baby was in a breech position. When she had a break, she read up on breech deliveries using the clinic tablet. After reading, Mary decided to review Fatima’s chart again through the EMR* system accessible using the tablet. Mary retrieved Fatima’s shared health record and learned that her first baby had been breech and did not survive. To be safe, Mary requested a brief consult with the obstetrics/gynecology department at the referral hospital. After speaking with the on-call physician, Mary was instructed to contact the physician through phone or videoconference if any complications arose. Mary felt confident going in to the delivery and provided support to Fatima.
After a successful delivery, Mary updated Fatima’s EMR, and updates were automatically sent from the EMR system to the Civil Registration and Vital Statistics database, NHIS database for facility reimbursement, the facility’s LMIS* to account for supplies used during the birth and the NHMIS* for health services planning. The local government M&E* officer was reviewing aggre-gate electronic NHMIS reports and supply requests from each of the LGAs*; he was pleased to see the decline in maternal and neonatal mortality continue.
Meanwhile, mum and baby were doing fine.
* EMR = Electronic Medical Record LGA = Local Government Area LMIS = Logistic Management Information System NHIS = National Health Insurance Scheme NHMIS = National Health Management Information System NIN= National Identification Number M&E = Monitoring and Evaluation SMS = Short Message Service (or text)

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!21
PART I. SECTION 3: FOUNDATIONS FOR CHANGEThe Foundations for Change for the successful application of Health ICT in Nigeria draws from the World Health Organization (WHO) and International Telecommunications Union (ITU) National eHealth Strategy Toolkit. The WHO-ITU components of an enabling environment (see Table 1) are used to provide a strategic and policy-oriented framework to help realize the Nigeria National Health ICT Vision, address critical gaps and track progress.14 The Foundations for Change ensure that investments in Health ICT will help enable and deliver UHC, while setting the stage for the sustainable and effective use of Health ICT across the entire health system.
In this section on Foundations for Change, the current status, critical oppor-tunities and gaps, and recommendations for short- and long-term outputs for each framework component are discussed. Table 2 provides a summary of the recommendations. The recommendations were iteratively developed through an extensive stakeholder engagement process. The Action Plan in Part II builds off of the recommendations and identifies specific inputs and activities required to achieve the desired outcomes.
3.1 Leadership and Governance
Effective leadership and governance of Health ICT activities at all levels is es-sential to ensure coordination, sustainability and alignment with national health priorities. While the National Council on Health (NCH) supports the strategic leadership of the FMOH in collaboration with the FMCT, there is currently no national governance structure in place for Health ICTs and to facilitate coordi-nation across MDAs, with development partners and the private sector.
Therefore, it is essential for Nigeria to establish a National Health ICT Steering Committee and supporting structure. The Steering Committee will be re-sponsible for overseeing Health ICT planning, implementation, coordination, governance and evaluation to the achievement of the Health ICT Vision. Specifically, the National Health ICT Governance Committee will be respon-sible for the following:
•# Oversight of the implementation of the National Health ICT Framework and Strategy
•# Ongoing coordination of Health ICTs across MDAs and with development partners and the private sector
•# Alignment of Health ICT investments and activities with health system priorities
•# Promoting awareness of Health ICT policies, regulations and best practices, and encouraging, incentivizing or mandating adoption of nationally-supported Health ICT services
•# Oversight of Health ICT strategic planning, including integration of Health ICT into new health programs and workflows and evolution of the National Health ICT Architecture
•# Implement National Health ICT Monitoring and Evaluation Plan to ensure delivery of expected outcomes
•# Support and facilitate required change across MDAs

22!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
TABLE 2. Summary of Recommendations to Improve Health ICT Enabling Environment
COMPONENT RECOMMENDATIONS
Leadership and Governance
• Establish a National Health ICT Steering Committee and supporting structure to oversee Health ICT planning, implementation, coordination, governance and evaluation
• Engage in broad stakeholder engagement beyond the Federal Government to involve State governments, private sector and development partners
Strategy and Investment
• Develop and periodically review the National Health ICT Strategy
• Secure sustainable funding to further develop and operationalize the National Health ICT environment, align existing projects and investments and explore incentives and additional sources of both traditional and catalytic funding
• Set up structures and processes to ensure proper investment and management of allocated funds at the National and State levels
• Leverage existing information systems, including the Health Finance Information System
Legislation, Policy and Compliance
• Conduct an extensive review of policies relevant to Health ICT and develop recommendations in collaboration with other ministries to harmonize existing policies and to address current and future policy gaps, including privacy and security of personal health information
• Establish a mechanism for regular review of Health ICT policies, implementation guidance and best practices
• Address key policy and regulatory gaps (i.e., privacy and security or standards and interoperability)
Architecture, Standards and Interoperability
• Define and implement a National Health ICT Architecture that defines high-level nationally-supported health information services, while harvesting from existing projects, supporting long-term meaningful use of ICTs within the health system
• Implement and harmonize digital registries, data collection instruments and reporting indicators that meet the needs of UHC and other prioritized services and applications
• Establish guidelines, minimum functional requirements, and interoperability standards that allow for the consistent and accurate collection and exchange of health information across the health system
Capacity building
• Establish a system for Health ICT workforce monitoring and evaluation, readiness, adoption and practices
• Develop incentive mechanisms to encourage workforce development of Health ICT skills and competencies, leveraging the FMOH Collaborative Center Training Program and other existing mechanisms where possible
• Establish methodology for accreditation and revision of Health ICT training Curriculum
• Establish special Health ICT education, training and career path development programs
• Develop and implement a strategy for the training and recruitment of a cadre of professionals into government positions to design, implement and maintain Health ICT systems
Infrastructure • Reinforce existing strategies for ongoing funding and investment in power provision, acquisition, installation and maintenance at all health facilities throughout the country, including exploring mechanisms (i.e. regulatory) for promoting distribution of alternate power
• Define minimum infrastructure and computing requirements for each type of health facility and health administrative office and link to accreditation and assessment
• Develop and introduce a basic ICT and related equipment package for health facilities based on prioritized services and application needs that encourages local ownership and capacity building
• Strengthen local and regional support programs, such as the Rural Information Technology Centers, to ensure ongoing support for infrastructure development and maintenance
• Install and maintain Internet and/or broadband connectivity for all tertiary and secondary along with prioritized primary health facilities as well as State and LGA level health administrative offices
• Develop incentive mechanism for Health ICT infrastructure improvement
Solutions (Services and Applications)
• Develop and implement services and applications to enable and deliver UHC, including at minimum digital beneficiary enrolment, premium payment, coverage verification, and recording of encounters
• Select additional priority Health ICT services and applications for scale-up based on need, strategic alignment with Health and Health ICT priorities, preparedness and evidence
• Gather and disseminate best practices for the implementation of Health ICT services and applications

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!23
The National Health ICT Steering Committee and supporting structure will direct the application of ICTs to achieve the Health ICT Vision. The Steering Committee will report to the National Council on Health, which will own the Health ICT Vision and approve periodic updates. The Steering Committee will set up a Health ICT Technical Working Group to coordinate technical and operational inputs. A Health ICT Project Management team will be established to carry out the implementation of the Health ICT Vision in support of the Steering Committee and Technical Working Group (TWG). The National Monitoring and Evaluation (M&E) Advisory Group will facilitate M&E and linkages to the NHMIS. The recommended Health ICT governance structure is depicted in Figure 4. Refer to Appendix 4 for a detailed description of each entity in the governance structure.
3.2 Strategy and Investment
The Health ICT Vision requires sufficient funding, sustainable financing mechanisms, incentives and accountability structures to support priority Health ICT activities. The combination of the strategy and investments ensures the development of a responsive plan and approach for improving the Health ICT environment and securing financing for sustained activities. Accordingly, four recommendations were provided that address current gaps in strategy and investment:
•#Develop and periodically review the National Health ICT Strategy
FIGURE 4. Health ICT Governance Structure, State Health ICT Governance
Health ICT Technical Working Group
Provide technical inputs and also responsible for standards and guidelines
Health ICT Project Management
Provide operational management
Health ICT Steering CommitteeHMoH & HMCT
Provide strategic management
Health Sector LeadershipNational Council on Health
Oversee activities and own the vision
State Steering CommitteeHCoH & HCCT
State eHealth Steering Committee
HMoH – Honorable Minister of Health HMCT – Honorable Minister of Communication Technology ICT – Information and Communication Technology M&E – Monitoring and Evaluation NHMIS – National Health Management Information System
HCoH – Honourable Commissioner of Health HCCT – Honourable Commissioner of Communication Technology
Note: in some states, the lead inTechnology is a Special Adviser to the Governor or the Head (DG or ES) of a State Agency for ICT

24!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
•# Secure sustainable funding to further develop and operationalize the National Health ICT environment, align existing projects and invest-ments and explore incentives and additional sources of both traditional and catalytic funding
•# Set up structures and processes to ensure proper investment and man-agement of allocated funds at the National and State levels
•# Leverage existing information systems, including the Health Finance Information System
By drawing from existing health information systems and ongoing and planned activities, such as the Health Finance Information System, NHMIS, Human Resources for Health’s (HRH’s) Health Worker Registry and the National Health Insurance Scheme, the National Health ICT Strategy can leverage current investments in lowering overall costs while maximizing downstream value and providing direction to ensure achievement of the National Health ICT Vision. The National Health ICT Strategy can also capitalize on current funding sources.15 Creative means of funding — catalytic funding, incentives for entrepreneurs and developers — may also be explored for their viability in addition to existing funding sources (e.g., donors and external funders and private sector investments). A recommendation has been made to establish a trust fund for Health ICT to pool government and development partner resources to simplify the management and investment of funds and promote transparency and accountability.
3.3 Legislation, Policy & Compliance
This component of the enabling environment addresses the legal and regula-tory measures, public policy, and observance of rules and regulations related to Health ICT initiatives. There is a special focus on ensuring privacy and secu-rity of personal health information. To maintain and strengthen trust between consumers, the private sector and the health system, use of Heath ICTs must support and improve the safe, effective, efficient, equitable and timely delivery of care. In addition, policy and regulatory guidance must be clear. Three legis-lation, policy and compliance recommendations were suggested:
•# Conduct an extensive review of policies relevant to Health ICT and devel-op recommendations in collaboration with other ministries to harmonize existing policies and to address current and future policy gaps, with a particular focus on privacy and security of personal health information
•# Establish a mechanism for regular review of Health ICT policies, imple-mentation guidance and best practices
•# Develop and put in place systems of accountability and compliance mechanisms for key measures of the Health ICT Framework
There are existing privacy and security policies that are applicable to Health ICT, including Nigeria’s Medical Code of Ethics, Constitution of the Federal Republic of Nigeria and National Health Law 2014. The Code of Ethics contains a special telemedicine provision. The provision covers the safety and mainte-nance of personal health information when that information is stored; sent; or received by fax, computer, e-mail or other electronic means.17 Sections 37, 45 and 46 of the Constitution establish a general right of privacy for Nigerian citizens, which can be applied to health.17 The National Health Law 2014 also provided for authorized access and storage of patient records.18 Awareness

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!25
of these provisions is limited, and education and capacity building in how to apply them to the use of Health ICT is needed.19
3.4 Architecture, Standards and Interoperability
The architecture, standards and interoperability component of the enabling environment addresses the development of a blueprint of nationally sup-ported digital services, such as the NHMIS and Health Worker Registry and their interactions, and the adoption of standards to maximize the meaningful use and sharing of health information. This is of particular importance given the federal structure of Nigeria’s health system and diversity of systems and actors involved in the delivery and administration of health services.
A National Health ICT Architecture, that builds off of existing Health ICT solu-tions in Nigeria and best practices from other countries, was proposed in Part I, Section 2. The architecture defines the high-level structure of systems that the Nigeria FMOH is already supporting. With strategic coordination, the systems could support a broad set of health system use cases, in addition to enabling and delivering UHC by 2020. Proposed nationally-supported architectural components include the NHMIS; a digital facility registry based on the FMOH Department for Planning Research and Statistics (DPRS) registry; a digital health worker registry based on the FMOH HRH Health Worker Registry; a terminology service building off of the National Agency for Food and Drugs Administration and Control (NAFDAC) drug formulary; a registry of clients leveraging NHIS and the National Identity Management Commission (NIMC) and a shared digital patient record building off existing EMR implementa-tions by the National Primary Health Care Development Agency (NPHCDA), National Agency for Control of AIDS (NACA) and others. In a heterogeneous environment with incompatible software projects and limited data and security standards, setting up a standards-based and interoperable National Health ICT Architecture is a prerequisite to a coordinated and connected health system.
Standards define how information is stored in Health ICT systems and how it is transferred between them, enabling interoperability. The absence of man-dated Health ICT standards and interoperability requirements and guidelines has exacerbated fragmentation, limited scale-up and increased market risk. Establishing interoperability, data and software functionality standards and requirements will allow for consistent and accurate collection and exchange of health information across health systems and services.
Recommendations within Architecture, Standards and Interoperability are as follows:
•# Define and implement a National Health ICT Architecture that defines high-level nationally-supported health information services, while align-ing existing projects, supporting long-term meaningful use of ICTs within the health system and helping enable and deliver UHC by 2020
•# Implement and harmonize digital registries, data collection instruments and reporting indicators that meet the needs of UHC and other priori-tized services and applications
•# Establish guidelines, minimum functional requirements and interoper-ability standards that allow for the consistent and accurate collection and exchange of health information across the health system. Outputs may include guidelines for use of Health ICT within public facilities and requirements for electronic reporting of health data and indicators

26!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
3.5 Capacity Building
Skilled and empowered health and ICT workforces are needed to design, develop, maintain, govern and use the services and applications critical to meeting the National Health ICT Vision. Recent estimates put the density of doctors and nurses/midwives in Nigeria at 4 and 16 per 10,000 populations, respectively.20, 21 However, there are significant urban-rural and regional differ-ences in health worker distribution. Health ICT training is limited and there are no career paths available to specialize in Health ICTs in Nigeria. Additionally, no incentive schemes exist for the adoption of ICTs in health service delivery. A recent baseline field assessment of Health ICT implementations across Nigeria’s six geopolitical zones found that 32% of Local Government Area (LGA) M&E Officers interviewed and fewer facility-level health workers had been trained on the use of the widely implemented and adopted NHMIS.22
In response to challenges with managing the health workforce, the FMOH designed and developed an electronic health workforce registry (eRegistry) that has improved the management of a subset of the health workforce and enabled the tracking of capacity building activities and health worker com-petencies. In addition to incorporating Health ICT training into standardized curricula, the eRegistry and other Health ICT services and applications present an opportunity for a nationally scaled health workforce registry and digitally supported health and ICT workforce education and training.
Specific recommendations for the Capacity Building component are as follows:
•# Establish a system for Health ICT workforce monitoring and evaluation, readiness, adoption and use
•# Establish special Health ICT education, training and career path devel-opment programs, leveraging the FMOH Collaborative Center Training Program and other mechanisms where possible
•# Develop incentive mechanisms to encourage workforce development of Health ICT skills and competencies
•# Establish methodology for accreditation and revision of Health ICT training curricula
•# Develop and implement a strategy for the training and recruitment of a cadre of professionals into government positions to design, implement and maintain Health ICT systems
3.6 Infrastructure
Infrastructure refers to the physical facility and related assets that form the foundation for Health ICT implementations, consisting of reliable electricity, cellular and Internet connectivity, and ICT equipment (e.g., computers, servers and data warehouses). Currently, infrastructure is inadequate to scale up Health ICT systems nationally, especially in under-served areas of the country.
Given the magnitude of the gap, infrastructure investments should be co-ordinated to ensure that they are in step with Health ICT and health system priorities (e.g., to enable UHC by 2020). Existing programs, like the Rural Information Technology Centers and the Universal Service Provision Fund’s Community Resource Centers, may be leveraged.
Specific infrastructure recommendations include the following:

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!27
•# Establish a workable strategy for ongoing funding and investment in electrical power provision, acquisition, installation and maintenance at all health facilities throughout the country, including exploring other mechanisms (i.e., regulatory) for promoting distribution of power
•# Define minimum infrastructure and computing requirements for each type of health facility and health administrative office and link to ac-creditation and assessment
•# Develop and introduce a basic equipment package for health facilities based on prioritized services and application needs that encourages local ownership and capacity building
•# Strengthen local and regional support programs, such as the Rural Information Technology Centers, to ensure ongoing support for infra-structure development and maintenance
•# Install and maintain Internet and/or broadband connectivity for all tertiary and secondary along with prioritized primary health facilities as well as State and LGA level health administrative offices
•# Develop incentive mechanism for further Health ICT infrastructure improvements
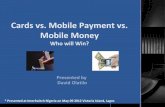
FIGURE 5. Key Findings from Baseline Inventory Assessment on Number of Health ICT Implementations by Program Area (UNF Assessment Report)
Maternal, Newborn& Child Health
63
Nutrition
12Immunizations
20
Malaria
11
EssentialCommodoties
16
eMTCT
22
In 2014, when the baseline assessment was conducted, 84 Health ICT projects were identified and included in the inventory. 28% of those initiatives were pilots and 24% were in the process of scaling up from pilot implementations.

28!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
3.7 Services and Applications
Services and applications provide the tangible means for end users to derive benefits from the application of ICTs to health. They facilitate service delivery and provide access to the information required for health planning and ad-ministration. Examples range from electronic medical records and laboratory information systems to mobile applications for health insurance enrolment, premium payment and verification. The focus of the services and applications component is to facilitate selection of a small number of Health ICT solutions, building off of existing projects where possible, that align with national health system priorities, have sufficient preparedness and evidence for national scale-up and simultaneously drive strategic investments into the National Health ICT Architecture.
Although health services delivery in Nigeria is primarily based on traditional or paper-based approaches, there are numerous Health ICT tools at varying degrees of maturity implemented throughout the country. Prevalent cellular coverage and mobile subscriptions throughout Nigeria has encouraged exper-imentation with mHealth or mobile-supported interventions, especially within maternal and child health. An opportunity remains to integrate mHealth into national health programming, especially in underserved regions. Patient and supply-chain information systems, though at their infancy, are being adopted for health services delivery, as well. NHMIS is the most prevalent Health ICT application in the health system, but routine data is generally still collected manually on paper forms and then entered electronically at the LGAs.23
Specific recommendations for the services and applications component are:
•# Develop and implement services and applications to enable and deliv-ery UHC, including at minimum digital beneficiary enrolment, premium payment, coverage verification, and recording of patient encounters
•# Select additional priority Health ICT services and applications for scale-up based on need, strategic alignment with Health and Health ICT priorities, preparedness and evidence
•# Gather and disseminate best practices for the implementation of Health ICT services and applications

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!29
Part II: Action Plan for Health ICT
PART II. SECTION 1: HEALTH ICT THEORY OF CHANGEICT is well positioned to help achieve the key UHC outcomes of improved equity, access, service and financial coverage, uptake, and quality.25 Each of these aspects of UHC can be supported by ICT services and applications that contribute to its accelerated achievement. The elements required to achieve the vision of Health ICT in the delivery of UHC have been layered on to the National Health ICT Vision, UHC outcomes, Health ICT outcomes and long-term ICT outputs to form the Theory of Change (see Figure 6). The set of intercon-nected elements are presented in a graphical form and illustrate the pathway of change from the Health ICT enablers, short- and long-term ICT-related outputs and Health ICT outcomes as they align with UHC outcomes. The Health ICT enablers, directly and indirectly support activities that make other more direct outputs and outcomes possible, ensuring that there is a career path within the health sector for technology professionals; there is also a requirement that appropriate governance structures are in place to make informed decisions and
By 2020, Health ICT will help deliver and enable universal health coverage — whereby Nigerians will have access to the services they need without incurring financial risk.
Effective use of telemedicine
and use of ICT for health
worker training and support
Effective use of CRVS, HRIS,
NHMIS & LMIS for tracking demand and
supply of health services and commodities
Effective useof mobile
messaging & cash transfers for demand
creation
Effective use of ICT for decision
support & within the continuum
of care
Effective useof ICT for
health insurance &
other health-related
financial transactions
Effective useof ICTs for delivering
appropriate health services for those who
need themmost based on epidemiology
and abilityto pay
Improvedaccess to
healthservices
Increased coverage of
health services
Increased uptake of
health services
Improvedquality of care
Increased financial
coverage for health care
Increased equity in,
access to, and quality of
health services, information,
and financing.
Strategic framework, governance structure &
Health ICT Fund established
Guidance on existing
policies & gaps identified
Review and adoption /
adaptation of prioritized standards
Health ICT assessment, curriculum developed, career path developed
Define minimum package &
plan for connectivity,
power & equipment
Prioritized services &
applications identified &
requirements gathered
SHORT-TERM OUTPUTS
(1 YEAR)
Leadership, governance, strategy & investment
Legislation, policy, and compliance
Standards & Interoperability
Capacity building Infrastructure
Solutions (services &
applications)
HEALTH ICT ENABLERS
Nationally scaled integrated Health ICT services and applications supported byNigerian Health Information Exchange implemented with appropriate funding,
infrastructure & equipment, training & policies.
NIGERIANATIONAL HEALTH
ICT VISION
LONG-TERMICT OUTPUTS
HEALTH ICT OUTCOMES
UHC OUTCOMES
FIGURE 6. Theory of Change for the Nigeria National Health ICT Vision

30!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
investments in technology. The enablers are based on the WHO-ITU eHealth Strategy Toolkit14 and highlight the importance of investing in the enabling envi-ronment in addition to the implementation of ICT services and applications. The Health ICT outcomes include the use of ICT to facilitate and track the coverage and delivery of health services and commodities through digitized CRVS, HRIS, LMIS, health service delivery and timely decision-making (through NHMIS) as well as enrollment, claims and reimbursement software for managing financial transactions within the health system (particularly in relation to insurance).26
The long-term outputs of nationally scaled integrated Health ICT services and applications are the bridge that maps and aligns key Health ICT enablers and short-term outputs with the achievement of UHC. This is supported by a Nigerian Architecture implemented with appropriate funding, infrastructure, equipment, training and policies. Targeted outputs detailed in this National Health ICT Strategic Framework serve as catalysts towards creating the appro-priate combination of governance, strategy, financing, workforce ICT-readiness, infrastructure, policy, standards and prioritized services and applications that will ultimately inform and generate the enabling environment needed for Nigeria to move towards nationally scaled integrated digital health systems that con-tribute to improved health outcomes and greater well-being.
PART II. SECTION 2: HEALTH ICT ACTION PLANA detailed action plan was developed using the Theory of Change along with the stakeholder-generated recommendations from Part I, Section 3. Reflective of the key stakeholders’ inputs and needs, the action plan will be used to direct imple-mentation for the realization of the Health ICT vision (including development of the budget), and the M&E plan will be used to track and assess progress.
The vision recommendations, categorized by the seven components of the enabling Health ICT environment, were converted into an actionable, measur-able form in the detailed action plan (see Appendix 5). Each recommendation has a set of steps that informs how the recommendation will be achieved. The steps have been organized into activities and sub-activities, with dependen-cies noted. The persons or entities responsible for carrying out each of the activities are clearly identified in the plan, as well. The following integrated action plan is a high-level summary of the detailed action plan (see Table 3).
Based on the Theory of Change, the recommendations are connected along a logical pathway of activities with short- and long-term impact. The activities reflect a five-year process, separated into three phases, to support the attain-ment of UHC. The phases are:
PHASE 1: Set-up (Year 1)
PHASE 2: Deploy, Maintain and Support (Year 2 and Year 3)
PHASE 3: Consolidate and Continuous Review (Year 4 and Year 5)
Set-up and preparation will take place in year 1. During years 2 and 3, activities that reflect Deploy, Maintain and Support to help meet the vision will be carried out. The final two years (years 4 and 5) will be focused on Consolidate and Continuous Review activities and reviews of progress. The initial phase will be front-loaded as important foundational structures and activities will need to be established. As time advances, there will be opportunities to assess the status of progress and revisit the action plan.

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!31
Some activities are longitudinal and will span the entire course of the time-frame, while others may be more discrete. All are captured in the action plan, including the timeframe needed to meet or sustain each recommendation. Revisiting the action plan will be important to ensure the continued alignment of the activities with achieving UHC.
The members of the NCH, as owners of the Health ICT vision, will oversee the action plan with guidance and support from the Health ICT Steering Committee, Technical Working Group and Project Management Office.

32!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
TAB
LE 3
. N
iger
ia N
atio
nal H
ealt
h IC
T V
isio
n In
tegr
ated
Act
ion
Plan
20
15 -
20
20
PH
AS
ES
TIM
E/
SE
QU
EN
CE
PH
AS
E 1
– S
ET
UP
PH
AS
E 2
– D
EP
LOY,
MA
INTA
IN A
ND
SU
PP
OR
T (
YE
AR
2 A
ND
YE
AR
3)
PH
AS
E 3
– C
ON
SO
LID
AT
E A
ND
CO
NT
INU
OU
S R
EV
IEW
(Y
EA
R 4
AN
D Y
EA
R 5
)
YEA
R 0
YE
AR
1Y
EA
R 2
YE
AR
3Y
EA
R 4
YE
AR
5
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Lead
ersh
ip &
G
over
nanc
e
Fra
mew
ork
E
ndo
rse-
men
tSt
ate
Eng
agem
ent
/ G
over
nanc
e
Esta
blish
SC
, TW
G &
PM
O
Fra
mew
ork
ad
op
tio
n an
d o
ngo
ing
bro
ad s
take
hold
er e
ngag
emen
t
Link
po
licie
s w
ith
Hea
lth
ICT
Fra
mew
ork
Stra
tegy
&
Inve
stm
ent
Setu
p
Inve
stm
ent
man
agem
ent
stru
ctur
e
Fund
coo
r -di
natio
n m
echa
nism
Exp
lore
so
urce
of
fund
s &
alig
n w
ith
fram
ewo
rkE
stab
lish
cata
lyti
c fu
ndin
gE
stab
lish
ince
ntiv
e m
echa
nism
sR
evie
w a
nd r
e-ex
plo
re s
our
ces
of
Hea
lth
ICT
fun
ds
Est
ablis
h sp
ecia
l pur
po
se H
ealt
h IC
T F
und
Stan
dard
s &
In
tero
pera
bilit
y
Trai
ning
and
ca
pac
ity
bui
ldin
g o
n H
ealt
h IC
T s
tand
ard
s &
inte
rop
erab
ility
Rev
iew
exi
stin
g
nati
ona
l and
inte
rna -
tio
nal s
tand
ard
s
Dev
elop
, ad
apt
or
adop
t hi
gh-
leve
l re
qui
rem
ents
and
d
esig
n fo
r fo
und
atio
nal
Hea
lth IC
T se
rvic
es
Ong
oin
g r
evie
w a
nd u
pd
ate
of
nati
ona
l sta
ndar
ds
and
req
uire
men
ts
Ong
oin
g o
n-th
e-jo
b H
ealt
h IC
T m
ento
ring
Esta
blis
h N
iger
ian
Hea
lth
Info
rmat
ion
Exch
ange
(H
IE)
Sca
le-u
p t
he N
iger
ian
HIE
Ad
voca
cy, c
om
mun
icat
ion
and
ed
ucat
ion
to d
ecis
ion
mak
ers
and
end
use
rs t
o e
nsur
e su
pp
ort
fo
r H
ealt
h IC
T s
tand
ard
s ap
plic
atio
n
Dev
elop
and
app
rove
sta
ndar
ds fo
r se
cure
mes
sagi
ng, h
igh-
prio
rity
heal
th in
form
atio
n, te
rmin
olog
ies
and
data
dic
tiona
ries
Legi
slat
ion,
Po
licy
&
Com
plia
nce
Hea
lth
ICT
PM
O
& T
WG
cap
acit
y st
reng
then
ing
Rev
iew
and
up
dat
e o
f p
olic
ies
Est
ablis
h &
imp
lem
ent
com
plia
nce
mec
hani
sms

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!33
PH
AS
ES
TIM
E/
SE
QU
EN
CE
PH
AS
E 1
– S
ET
UP
PH
AS
E 2
– D
EP
LOY,
MA
INTA
IN A
ND
SU
PP
OR
T (
YE
AR
2 A
ND
YE
AR
3)
PH
AS
E 3
– C
ON
SO
LID
AT
E A
ND
CO
NT
INU
OU
S R
EV
IEW
(Y
EA
R 4
AN
D Y
EA
R 5
)
YEA
R 0
YE
AR
1Y
EA
R 2
YE
AR
3Y
EA
R 4
YE
AR
5
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Cap
acit
y B
uild
ing
Ass
ess
Hea
lth
ICT
rea
din
ess
of
stak
eho
lder
s
Defi
ne p
rofe
ssio
nal
pra
ctic
e st
and
ard
s
Dev
elo
p a
nd R
oll-
out
inve
ntiv
e sc
hem
es f
or
Hea
lth
ICT
ad
op
tio
n
Dev
elo
p s
trat
egy
for
cont
inue
d
Hea
lth
ICT
ski
lls a
nd c
om
pet
ency
ac
qui
siti
on
Des
ign
Hea
lth
ICT
ski
lls a
nd
com
pet
enci
es c
aree
r p
rog
ress
ion
pla
n
Dev
elop
st
anda
rd
Hea
lth IC
T
com
pe-
tenc
y fr
amew
ork
Defi
ne
new
ac
cred
-it
atio
n re
qui
re-
men
ts
Impl
emen
t ne
w a
c-cr
edita
tion
requ
irem
ents
Iden
tify
educ
atio
n an
d tr
aini
ng
cour
se
chan
ges
Rev
iew
FM
oH
co
llab
ora
tive
pro
gra
ms
to
incl
ude
heal
th in
form
atic
s
Imp
lem
ent
educ
atio
n an
d t
rain
ing
co
urse
ch
ang
es
Est
ablis
h sp
ecia
lized
Hea
lth
ICT
qua
lifica
tio
ns
and
cer
tific
atio
n tr
ack
Imp
lem
ent
spec
ializ
ed H
ealt
h IC
T c
our
ses
Mo
nito
r H
ealt
h IC
T a
do
pti
on
Est
ablis
h N
atio
nal H
ealt
h IC
T k
now
led
ge
rep
osi
tory
Dev
elop
H
ealth
ICT
aw
aren
ess
cam
pai
gn
stra
teg
y an
d
roll-
out
Des
ign
M&
E
fram
ewo
rk
for
mea
suri
ng
effec
tive
-ne
ss o
f en
gage
men
t
Mo
nito
r eff
ecti
ve-
ness
of
Hea
lth
ICT
us
e an
d
ado
pti
on
Des
ign
targ
eted
st
akeh
old
er
refe
renc
e an
d
wor
king
gro
up
Eng
age
and
con
sult
with
sta
keho
lder
ref
eren
ce a
nd w
orki
ng g
roup
s
TAB
LE 3
. N
iger
ia N
atio
nal H
ealt
h IC
T V
isio
n In
tegr
ated
Act
ion
Plan
20
15 -
20
20 c
onti
nued

34!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
PH
AS
ES
TIM
E/
SE
QU
EN
CE
PH
AS
E 1
– S
ET
UP
PH
AS
E 2
– D
EP
LOY,
MA
INTA
IN A
ND
SU
PP
OR
T (
YE
AR
2 A
ND
YE
AR
3)
PH
AS
E 3
– C
ON
SO
LID
AT
E A
ND
CO
NT
INU
OU
S R
EV
IEW
(Y
EA
R 4
AN
D Y
EA
R 5
)
YEA
R 0
YE
AR
1Y
EA
R 2
YE
AR
3Y
EA
R 4
YE
AR
5
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Infr
astr
uctu
re
Iden
tify
und
er-
serv
ed
area
s
Dev
elop
dat
a co
nnec
tivity
im
ple
men
tatio
n an
d d
esig
n p
lan
Sele
ct im
ple-
men
tatio
n pa
rtne
rs to
de
velo
p da
ta
conn
ectiv
ity
infra
stru
ctur
e
Dep
loy
dat
a co
nnec
tivity
infr
astr
uctu
re fo
r un
der
serv
ed a
reas
Iden
tify
and
asse
ss
ongo
ing
in
fras
truc
ture
pr
ojec
ts in
un
ders
erve
d
area
s
Loca
l par
tici
pat
ion
of
com
mun
itie
s in
sup
po
rt, m
aint
enan
ce a
nd u
se o
f H
ealt
h IC
T s
ervi
ces
and
ap
plic
atio
ns
Defi
ne m
inim
um
com
put
ing
, pow
er
and
co
nnec
tivi
ty
infr
astr
uctu
re
req
uire
men
ts
for
heal
th
imp
lem
enta
tio
n
Link
hea
lth
orga
niza
tion
prov
ider
s’ H
ealth
IC
T ac
cedi
tatio
n to
m
eet
min
imum
hea
lth
faci
lity
com
putin
g
infr
astr
uctu
re
Ad
voca
te f
or
pri
ori
ty in
fras
truc
ture
Solu
tion
s (S
ervi
ces
&
App
licat
ions
)
Iden
tify
prio
rity
serv
ices
and
/or
app
licat
ions
Dev
elop
/rev
ise
req
uire
men
ts a
nd
des
ign
for
iden
-tifi
ed s
ervi
ces
&
app
licat
ions
Iden
tify
reso
urce
s to
sup
por
t th
e ex
pan
sion
and
d
evel
opm
ent
of
iden
tified
ser
vice
s &
ap
plic
atio
ns
Bui
ld/d
eplo
y/sc
ale
iden
tified
prio
rity
Nat
iona
l Hea
lth IC
T s
ervi
ces
and
/or
app
licat
ions
Op
erat
e, s
upp
ort
and
sus
tain
pri
ori
ty H
ealt
h IC
T s
ervi
ces
and
ap
plic
atio
n
Dev
elo
p/i
mp
lem
ent
colla
bo
rati
on
po
rtal
Fo
ster
co
ntin
uous
up
gra
des
of
imp
lem
ente
d h
igh
pri
ori
ty H
ealt
h IC
T s
olu
tio
ns
Pro
mo
te r
esea
rch
and
dev
elo
pm
ent
of
pri
ori
ty H
ealt
h IC
T s
olu
tio
ns
Ong
oin
g s
cale
-up
of
pri
ori
ty s
ervi
ces
and
ap
plic
atio
n
Iden
tify
bes
t p
ract
ices
in H
ealt
h IC
T a
nd d
isse
min
ate
wid
ely
TAB
LE 3
. N
iger
ia N
atio
nal H
ealt
h IC
T V
isio
n In
tegr
ated
Act
ion
Plan
20
15 -
20
20 c
onti
nued

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!35
Part III: Monitoring & Evaluation Plan for Health ICT
PART III. SECTION 1: MONITORING & EVALUATION PLANThe M&E plan provides a link between the vision, action plan and desired results (see Appendix 6). The M&E plan draws from the Theory of Change to define the relationship between the inputs, activities, outputs, outcomes and impact. Its contents are measurable and presented in the form of indicators. Accordingly, progress towards achievement of the vision can be tracked and evaluated and inform whether the implementation is yielding intended results and outcomes. In line with the adopted result-based management approach27, the M&E plan has three aspects: the indicators for the activities outlined in the action plan, the baseline and target measures and the governance to oversee and support progress.
The indicators developed for and used in the Health ICT M&E framework focus on outcomes and health impact. The outcomes are related to the enabling en-vironment and translate the recommendations and activities from the action plan into a measurable form. The health impact reflects the national focus on UHC and uses national indicators for health services access, delivery, coverage, quality and equity. For each indicator, its scope or reach (e.g., National, State or both) along with the data source, collection method and frequency of data collection are articulated. The baseline measures will be obtained and target measures for 2020 set by the leadership and supporting entities.

36!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Appendices
APPENDIX 1: LIST OF CONTRIBUTING ORGANIZATIONSABT Associates - HS2020
Ajimatics
ANADACH group
Bill and Melinda Gates Foundation
Center for Management Development (CMD)
Centers for Disease Control and Prevention (CDC)
Clinton Health Access Initiative (CHAI)
Computer Professionals (Registration Council of Nigeria)
Digital Bridge Institute (DBI)
eHealth Nigeria
Federal Capital Territory Administration (FCTA)
Federal Civil Service
Federal Ministry of Communication Technology - Department of Planning Research and Statistics (FMCT-DPRS)
Federal Ministry of Health - Budget
Federal Ministry of Health - DPRS
Federal Ministry of Health - Family Health
Federal Ministry of Health - Food and Drugs
Federal Ministry of Health - Hospital Services
Federal Ministry of Health - National AIDS Control and Prevention Programme (FMOH-NASCP)
Federal Ministry of Health - National AIDS Control and Prevention Programme (FMOH-NPSCMP)
Federal Ministry of Health - Public Health
FMCT- eGovernance (FMCT-eGov)
Fortern Global Ltd
Futures Group
Galaxy Backbone (GBB)
Groupe Special Mobile Association (GSMA)
Health Finance and Governance
Health in Africa (HIA)
Health Information Systems Program (HISP) Nigeria
Health Reform Foundation of Nigeria
ICT for Saving One Million Lives (ICT4SOML)
InStrat Global Health Solutions
Intel
International Finance Corporation (IFC)
John Snow Incorporated (JSI)
Medical and Dental Council of Nigeria
Millennium Development Goals (MDGS) Nigeria
Mobile Alliance for Maternal Action (MAMA)
National Agency for Control of AIDS (NACA)
National Agency for Food and Drugs Administration and Control (NAFDAC)
National Health Insurance Scheme (NHIS)
National Identity Management Commission (NIMC)
National Information Technology and Development Agency (NITDA)
National Primary Health Care Development Agency (NPHCDA)
National Tuberculosis and Leprosy Control Programme (NTBLCP)
National Universities Commission (NUC)
Network Data Services and Technology Ltd. (NDST)
Nigeria Communications Commission (NCC)
Nigeria Computer Society (NCS)
Nigeria Telecommunications Satellite (NIGCOMSAT)
Norwegian Agency for Development and Cooperation (Norad)
Nurses and Midwifery Council of Nigeria
Pathfinder International
Praekelt Foundation
Private Sector Health Alliance
Saving One Million Lives (SOML)
Standards organization of Nigeria (SON)
State Ministries of Health - DPRS
State Ministries of Information/ Communication/Science and Technology or Relevant Agencies or designates
Subsidy Reinvestment and Empowerment Program Maternal and Child Health (SURE-P MCH)
United Nations (UN) Foundation
United States Agency for International Development (USAID)
Universal Service Provision Fund (USPF)
USAID Monitoring and Evaluation Management Services (USAID/MEMS)
World Bank
World Health Organization (WHO)

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!37
APPENDIX 2: HEALTH ICT SCENARIO ILLUSTRATING CHANGE AND IMPACT ON STAKEHOLDERS
SCENARIO: THE HEALTH ICT VISION IN PRACTICE
A few months ago, Fatima registered her children in the NHIS* through the Primary School Enrollment Process. At that time, Fatima and her husband were also enrolled in the NHIS and they were issued NHIS Cards that can be used for healthcare services.
Mary woke up early. She checked her phone. It was 6 AM. She had 30 minutes to get ready before going to work. She scrolled through her apps to double check the shift calendar. Earlier on in the week, she had received a request to swap shifts with one of her co-workers who was headed out of town to attend to a family matter. She started getting ready.
Around the same time, Fatima was going about her day. She was expecting and due at any time. She had developed a birth plan with the local midwife. When she first learned that she was preg-nant, she decided to sign up for weekly SMS* notifications about her pregnancy and to receive appointment reminders. She found the messages and pictures informative and even enjoyable, and would often discuss them with her sisters. She was especially proud that she had not missed a single appointment. This was unlike her previous pregnancies. She sighed as she recalled her previous experiences. Back then, she did not know the importance of antenatal visits or setting up a birth plan. Sometimes she would make appointments, but not show up. This time was different…Fatima felt a contraction.
Mary arrived at work right on time. She was excited for the day. During shift hand-off, she and her co-worker huddled over one of the clinic’s tablets going through the different cases of clients present at the clinic. They prioritized the cases and she got to work.
Fatima notified her family members that she needed to be taken to the clinic. She then directed one of her sisters to text the local clinic about the situation. A taxi was called and Fatima proceed-ed to the clinic.
[Alert.] Mary checked the clinic tablet. She read that a 33 year old female, G4P2 (Gravida of 4, Parity of 2)*, in labor was headed to the clinic.
When Fatima arrived, she and her husband realized they had left the NHIS card at home in the hurry. But they were lucky; her NIN* was stored in her husband’s phone contact. With the cross-reference she was triaged and encouraged to relax or walk about until the contractions came closer together.
During her assessment of Fatima, Mary observed that the baby was in a breech position. When she had a break, she decided to read up on breech deliveries. She browsed the resources on the clinic tablet and began reading. After reading, Mary decided to review Fatima’s chart again through the EMR system accessible using the tablet. Fatima had mentioned a history of pregnancy complica-tions, but Mary did not see that in the clinic’s system so she checked the Nigerian Health Exchange to see if the records were there. Mary retrieved Fatima’s shared health record and learned that the first baby had been breech and did not survive. It had been a home delivery in a different village. To be safe, Mary decided to request a brief consult with the obstetrics/gynecology department at the referral hospital. She sent off the request through the hospital tablet. Within a few short minutes, she was on the phone with the on-call physician in that department.

38!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Fatima’s contractions shortened. Mary checked up on her and moved her to the delivery room. Mary had instructions to contact the on-call physician her through phone or videoconference if any complications arose. Mary felt confident going in to the delivery and provided support to Fatima.
Fatima, G4P3, delivered a healthy baby boy weighing 3.4 kgs, 49.3 cm in length at 17h21 on... Mary typed into the clinic computer, updating Fatima’s chart as she smiled. Through the chart update, the baby was registered in the Civil Registration and Vital Statistics database. The data were also automatically transmitted to the NHIS database for facility reimbursement, the facility’s LMIS* to account for supplies used during the birth and the NHMIS* for health services planning. Meanwhile, mum and baby were doing fine in the recovery unit.
One week later, Oye, the local government M&E* officer was reviewing aggregate electronic NHMIS reports from each of the LGAs*. That week, the decline in maternal and neonatal mortality continued. He concluded his day by emailing off performance reports to each of the supervisors in his department and fulfilling supply requests and systems prompts.
* EMR = Electronic Medical Record G = Gravida (number of pregnancies) LGA = Local Government Area LMIS = Logistic Management Information System M&E = Monitoring and Evaluation NHIS = National Health Insurance Scheme NHMIS = National Health Management Information System NIN= National Identification Number P = Parity (number of successful births)

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!39
APPENDIX 3: RECOMMENDED NIGERIA HEALTH ICT ARCHITECTUREIn Health ICT projects, the architecture serves as the conceptual framework that defines the high-level structure and behavior of the system components. The recommended architectural approach is a components-based approach that fosters collaboration and interoperability.
The architecture facilitates interoperability by creating a reusable framework that is service oriented, maximally leverages health information standards, enables flexible implementation and supports the interchangeability of indi-vidual components. Integrating the Health Enterprise (IHE) and other trans-action standards form the basis for the interactions between the architecture components and Point-of-Service (POS) applications. This architecture is designed to build upon and amplify the health benefits of existing Nigerian health and government initiatives.
Many of the components in the proposed architecture are already being developed or can leverage existing projects or information. The following is an overview of each of the proposed architecture components and some examples of Nigerian projects or activities that could be leveraged in the proposed architecture.
•# An enterprise master patient index (EMPI), or Client Registry (CR) manages the unique identity of citizens receiving health services with the country – “For whom”
The work that NIMC and NHIS are doing to link insurance beneficiaries to unique patient identifiers can be leveraged to provide a strong
Health Information Exchange
Interoperability Layer
Point Of Service Applications

40!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
foundation for a client registry portion of a health information exchange (HIE). The National Identification Number (NIN) could be considered as a key, highly “discriminating”, attribute for identifying patients. To take advantage of that, we recommend understanding the relationship be-tween NIMC and NHIS and gaining a better understanding of how the NIN relates to healthcare identification across the entire health system.
•# A Health Worker Registry (HWR) is the central authority for maintaining the unique identities of health providers within the country – “By whom”
HRH has already created an OpenHIE-compatible Health Worker Registry and they are in the process of working towards populating it. To position the registry to be utilized outside of HRH, we recommend that the team continue to expound upon the value that this data can provide across the healthcare system.
•# A Health Facility Registry (FR) serves as a central authority to unique-ly identify all places where health services are administered within the country – “Where?”
Significant work has been done to collect facility registry information, largely led by the FMOH DPRS. This information is valuable and can pro-vide value across the public and private health system. For example, the data can be used in supply chain planning and in verifying the location of a patient’s clinical interaction. The FMOH is well positioned to move this content toward a digital platform that can be more widely used and sup-ported. We recommend further conversations around governance models.
•# A Health Management Information System (HMIS) is a repository containing the normalized version of aggregate-level content created within the community, after being validated against each of the previ-ous registries. It is a collection of indicator-centric records for cohorts with information in the exchange.
The FMOH Department of Planning, Research and Statistics (DPRS) has selected DHIS2 as the HMIS platform and there are currently web and paper data collection processes for reporting of primary health indicators. DHIS2 is compliant with the proposed architecture.
•# A Shared Health Record (SHR) enables the collection and storage of electronic health information about individual patients in a centralized repository which is capable of being shared across different health-care settings.
There are numerous point-of-care systems that are EMRs and captur-ing data about clinical encounters. Depending upon the initial health priority that the team decides to pursue, many of these implementa-tions could provide input on data standards and/or be positioned to contribute to a shared health record.
•# A Terminology Service (TS) serves as a central authority to uniquely identify the clinical activities that occur within the care delivery process by maintaining a terminology set mapped to international standards such as ICD10, LOINC, SNOMED, and others – “What?”
While no terminology service currently exists, some indicator, registry and data definitions do exist. The initial health priority will help focus the team on the terminology standards that need to be defined first.

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!41
•# A Health Interoperability Layer (IL) receives all communications from point of service applications within a health geography, and orches-trates message processing among the point of service application and the hosted infrastructure elements.
Because there currently is not an HIE, this component of the architec-ture does not currently exist in Nigeria.
•# Point of Service (POS), or point of care applications are a diverse group of actors that leverage the health information exchange to im-prove the quality of care by using higher quality and more timely data to support their activities. These systems include mobile messaging tools [SMS/interactive voice response (IVR)], EMRs, laboratory or stock management systems and monitoring and evaluation tools.

42!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
APPENDIX 4: PROPOSED GOVERNANCE STRUCTURE
Federal Level
The following table outlines the proposed Health ICT governance structure. This table complements the governance structure illustration in Part I, section 3.1. The general functions and responsibilities are also included in the table.
ROLE COMPOSITION GENERAL FUNCTIONS AND RESPONSIBILITIES
Health Sector Leadership National Council on Health Provide oversight and own the Health ICT vision
Health ICT Steering Committee
Ministers of Health and Communication Technology in addition to CEOs of Government Departments/ Agencies as may be identified by the two (2) Ministers.
Strategic direction and support
Health ICT Project Management Office
This will be hosted by FMOH Provide operational management through:
• General daily management and operation
• Facilitate design, implementation and mainte-nance of the strategic architecture
• In charge of logistics for meetings of the steering committee
• Generate and coordinate reports and other key documentation for Health ICT
• Stimulate stakeholders and private sector involvement/investment in Health ICT
• Develop and help implement the Health ICT Strategy and administrative funding
• Interface with the Health ICT Steering Committee
Health ICT Technical Working Group
• The Chair member will be appropriate government ministry, department or agency.
• Other members can be drawn from a wide range of stakeholders ranging from the private sectors, to development partners to health ICT subject experts
• There may be several subject matter specific working groups
Coordinate technical consultation on appropri-ate subject matter:
• Produce subject-specific guidelines that will inform the work of the Health ICT Program Management Office
• holding monthly reviews meetings

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!43
State Level
The following table outlines the proposed Health ICT governance structure at the states. This is meant as a guide to help states develop appropriate gover-nance for health ICT. This recognizes that different states have varying priori-ties and varying degree of ICT governance. While some may have ministry of science and technology, other have special advisers and some commissioners embedded in contiguous ministries. The general functions and responsibilities are also included in the table.
ROLE COMPOSITION GENERAL FUNCTIONS AND RESPONSIBILITIES
State Health ICT Committee
Commissioners of Health and Communication Technology / Science and Technology and heads of state government agencies as identified by the two (2) commissioners.
The secretary of this committee shall be the appropriate as identified by SMOH within the state. The State steering com-mittee should also include other agencies of SMOH.
Strategic management and support within the state

44!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
AP
PE
ND
IX 5
: D
ETA
ILE
D H
EA
LTH
IC
T A
CT
ION
PLA
NAp
pend
ix 5: D
etailed He
alth ICT Actio
n Plan
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
n Activ
ity
Activ
ity Descriptio
n Stakeholders
1.0
Leadership and
Governance
1.1
Gove
rnan
ce S
truc
ture
N
atio
nal H
ealth
ICT
gove
rnan
ce
stru
ctur
e es
tabl
ished
Esta
blish
a n
atio
nal H
ealth
ICT
gove
rnan
ce st
ruct
ure
to o
vers
ee
Heal
th IC
T de
cisio
n-‐m
akin
g,
plan
ning
, im
plem
enta
tion
and
mon
itorin
g/ev
alua
tion
Esta
blish
Nat
iona
l Hea
lth IC
T St
eerin
g co
mm
ittee
(SC)
, Nat
iona
l He
alth
ICT
Tech
nica
l Wor
king
Gro
up
(TW
G) a
nd N
atio
nal H
ealth
ICT
Proj
ect M
anag
emen
t Offi
ce (P
MO
)
Gove
rns H
ealth
ICT
plan
ning
, im
plem
enta
tion
and
eval
uatio
n, a
s w
ell a
s int
erop
erab
ility
and
in
tegr
atio
n re
quire
men
ts, f
undi
ng,
clin
ical
doc
umen
tatio
n re
quire
men
ts, a
rchi
tect
ural
gu
idel
ines
, priv
acy,
secu
rity,
and
au
ditin
g re
quire
men
ts
NCH
, FM
OH,
FM
CT p
lus p
artie
s lis
ted
in th
e go
vern
ance
tabl
e
1.2
Stat
e Go
vern
men
t Eng
agem
ent
Stat
e Go
vern
men
t eng
aged
Broa
d st
akeh
olde
r eng
agem
ent
beyo
nd th
e fe
dera
l gov
ernm
ent t
o in
volv
e th
e st
ate
gove
rnm
ents
for
max
imum
supp
ort a
nd p
artic
ipat
ion
Form
alize
gov
erna
nce
inte
ract
ions
be
twee
n Fe
dera
l and
Sta
tes a
s wel
l as
bet
wee
n St
ates
and
LGA
s
Dedi
cate
d He
alth
ICT
gove
rnan
ce
func
tions
will
nee
d to
coe
xist
with
ex
istin
g go
vern
ance
func
tions
op
erat
ing
at F
eder
al, a
nd S
tate
le
vels
Ther
e w
ill b
e a
need
to id
entif
y an
d fo
rmal
ize th
e re
latio
nshi
ps w
ith
thes
e go
vern
ance
func
tions
and
cl
early
def
ine
how
they
will
inte
ract
in
rela
tion
to H
ealth
ICT
stra
tegy
, in
vest
men
t and
coo
rdin
atio
n
FMO
H, F
MCT
, Sta
te H
ealth
and
Te
chno
logy
min
istrie
s, S
tate
PHC
bo
ards
and
age
ncie
s
1.3
Broa
d St
akeh
olde
r Eng
agem
ent
Broa
d st
akeh
olde
r eng
agem
ent
achi
eved
Esta
blish
mec
hani
sms f
or o
ngoi
ng
broa
d st
akeh
olde
r eng
agem
ent
beyo
nd g
over
nmen
t to
invo
lve
the
priv
ate
sect
or, d
evel
opm
ent
part
ners
, civ
il so
ciet
y an
d ci
tizen
s
Broa
d st
akeh
olde
r eng
agem
ent
Beyo
nd g
over
nmen
t MDA
s, in
volv
e th
e pr
ivat
e se
ctor
, dev
elop
men
t pa
rtne
rs, c
ivil
soci
ety
and
citiz
ens
TWG,
PM
O, C
ivil
soci
ety
orga
niza
tions
, Pat
ient
hea
lth
asso
ciat
ions
, priv
ate
prov
ider
s as
soci
atio
n, IC
T pr
ovid
ers
asso
ciat
ion,
dev
elop
men
t par
tner
s an
d pr
ofes
siona
l soc
ietie
s
1.4
Link
ed a
nd In
tegr
ated
Pol
icie
s
Nat
iona
l Hea
lth IC
T Fr
amew
ork
inte
grat
ed a
nd li
nked
with
Nat
iona
l he
alth
Act
, NHP
, Nat
iona
l ICT
pol
icy
and
NSH
DP
Link
Nat
iona
l Hea
lth IC
T Fr
amew
ork
with
the
maj
or e
mer
ging
Nat
iona
l po
licie
s (e.
g., t
he N
atio
nal H
ealth
Ac
t, N
atio
nal S
trat
egic
Hea
lth
Deve
lopm
ent p
lan
(NSH
DP),
Nat
iona
l Hea
lth P
olic
y an
d N
atio
nal
ICT
polic
y)
Ensu
re in
clus
ion
of H
ealth
ICT
durin
g re
view
s of N
HA, N
HP, N
atio
nal I
CT
Polic
y an
d N
HSDP
.
Advo
cate
for a
subs
ectio
n on
Hea
lth
ICT
with
in N
SHDP
, NHP
, and
oth
er
rele
vant
and
em
ergi
ng in
stitu
tiona
l m
echa
nism
s.
FMO
H, F
MCT
, Nat
iona
l Hea
lth A
ct
sub
com
mitt
ees,
Nat
iona
l M&
E te
chni
cal w
orki
ng g
roup
, and
oth
er
rele
vant
pla
tfor
ms.
1.5
Fram
ewor
k Ad
optio
n N
atio
nal H
ealth
ICT
Fram
ewor
k de
velo
ped,
end
orse
d an
d pe
riodi
cally
re
view
ed
Ensu
re th
e en
dors
emen
t, ad
optio
n an
d pe
riodi
c re
view
(at m
ost e
very
5
year
s) o
f dev
elop
ed N
atio
nal H
ealth
IC
T Fr
amew
ork
as a
par
t of a
larg
er
Nat
iona
l Hea
lth S
trat
egy
Ensu
re e
ndor
sem
ent,
perio
dic
revi
ew a
nd a
dopt
ion
of N
atio
nal
Heal
th IC
T Fr
amew
ork
Fram
ewor
k co
ntrib
utes
to
esta
blish
ing
a N
atio
nal H
ealth
ICT
stra
tegi
c fr
amew
ork,
but
mul
ti-‐se
ctor
al a
dopt
ion
is cr
itica
l, as
is a
sy
stem
of 5
-‐yea
rly re
view
and
ev
alua
tion
Stee
ring
Com
mitt
ee, T
WG
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
2.0
Strategy and
Investment
2.1
Fund
ing
for H
ealth
ICT
Fund
ing
for H
ealth
ICT
oper
atio
ns
secu
red
Secu
re su
stai
nabl
e fu
ndin
g fo
r the
de
velo
pmen
t and
ope
ratio
n of
the
natio
nal H
ealth
ICT
envi
ronm
ent,
mak
ing
sure
to e
xplo
re th
e vi
abili
ty
of e
xist
ing
fund
s, c
atal
ytic
fund
ing
and
ince
ntiv
es
A. E
xplo
re so
urce
s of H
ealth
ICT
fund
s and
alig
n w
ith F
ram
ewor
k
Expl
ore
sour
ces o
f Hea
lth IC
T fu
nds:
re
venu
e (N
atio
nal a
nd S
tate
s),
deve
lopm
ent p
artn
ers a
nd e
xter
nal
fund
ers,
incl
udin
g pr
ivat
e-‐se
ctor
in
vest
men
ts
FMO
H-‐DP
RS, H
ealth
Fin
anci
ng, F
MF,
FM
CT, P
rivat
e se
ctor
stak
ehol
ders
B.Es
tabl
ish c
atal
ytic
fund
ing
Esta
blish
seed
cat
alyt
ic fu
ndin
g to
su
ppor
t inn
ovat
ion
FMO
H, F
MCT
, PSH
AN, U
SPF,
WB/
IFC
and
deve
lopm
ent p
artn
ers
C.Es
tabl
ish sp
ecia
l pur
pose
fund
for
Heal
th IC
T
A sp
ecia
l pur
pose
fund
for H
ealth
IC
T w
ill e
nsur
e ad
equa
te fu
ndin
g fo
r He
alth
ICT
inno
vatio
n an
d im
plem
enta
tions
NHI
S, N
ITDA
, CBN
, FM
F, N
CC-‐U
SPF,
de
velo
pmen
t par
tner
s
2.2
Mot
ivat
ion
Mot
ivat
ion
mec
hani
sm e
stab
lishe
d Es
tabl
ish m
otiv
atio
n m
echa
nism
for
Set u
p m
otiv
atio
n m
echa
nism
Es
tabl
ish m
otiv
atio
n m
echa
nism
for
FMO
H, F
MCT
, PSH
AN, W
B/IF
C,
Append
ix 5: D
etailed He
alth ICT Actio
n Plan
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
n Activ
ity
Activ
ity Descriptio
n Stakeholders
1.0
Leadership and
Governance
1.1
Gove
rnan
ce S
truc
ture
N
atio
nal H
ealth
ICT
gove
rnan
ce
stru
ctur
e es
tabl
ished
Esta
blish
a n
atio
nal H
ealth
ICT
gove
rnan
ce st
ruct
ure
to o
vers
ee
Heal
th IC
T de
cisio
n-‐m
akin
g,
plan
ning
, im
plem
enta
tion
and
mon
itorin
g/ev
alua
tion
Esta
blish
Nat
iona
l Hea
lth IC
T St
eerin
g co
mm
ittee
(SC)
, Nat
iona
l He
alth
ICT
Tech
nica
l Wor
king
Gro
up
(TW
G) a
nd N
atio
nal H
ealth
ICT
Proj
ect M
anag
emen
t Offi
ce (P
MO
)
Gove
rns H
ealth
ICT
plan
ning
, im
plem
enta
tion
and
eval
uatio
n, a
s w
ell a
s int
erop
erab
ility
and
in
tegr
atio
n re
quire
men
ts, f
undi
ng,
clin
ical
doc
umen
tatio
n re
quire
men
ts, a
rchi
tect
ural
gu
idel
ines
, priv
acy,
secu
rity,
and
au
ditin
g re
quire
men
ts
NCH
, FM
OH,
FM
CT p
lus p
artie
s lis
ted
in th
e go
vern
ance
tabl
e
1.2
Stat
e Go
vern
men
t Eng
agem
ent
Stat
e Go
vern
men
t eng
aged
Broa
d st
akeh
olde
r eng
agem
ent
beyo
nd th
e fe
dera
l gov
ernm
ent t
o in
volv
e th
e st
ate
gove
rnm
ents
for
max
imum
supp
ort a
nd p
artic
ipat
ion
Form
alize
gov
erna
nce
inte
ract
ions
be
twee
n Fe
dera
l and
Sta
tes a
s wel
l as
bet
wee
n St
ates
and
LGA
s
Dedi
cate
d He
alth
ICT
gove
rnan
ce
func
tions
will
nee
d to
coe
xist
with
ex
istin
g go
vern
ance
func
tions
op
erat
ing
at F
eder
al, a
nd S
tate
le
vels
Ther
e w
ill b
e a
need
to id
entif
y an
d fo
rmal
ize th
e re
latio
nshi
ps w
ith
thes
e go
vern
ance
func
tions
and
cl
early
def
ine
how
they
will
inte
ract
in
rela
tion
to H
ealth
ICT
stra
tegy
, in
vest
men
t and
coo
rdin
atio
n
FMO
H, F
MCT
, Sta
te H
ealth
and
Te
chno
logy
min
istrie
s, S
tate
PHC
bo
ards
and
age
ncie
s
1.3
Broa
d St
akeh
olde
r Eng
agem
ent
Broa
d st
akeh
olde
r eng
agem
ent
achi
eved
Esta
blish
mec
hani
sms f
or o
ngoi
ng
broa
d st
akeh
olde
r eng
agem
ent
beyo
nd g
over
nmen
t to
invo
lve
the
priv
ate
sect
or, d
evel
opm
ent
part
ners
, civ
il so
ciet
y an
d ci
tizen
s
Broa
d st
akeh
olde
r eng
agem
ent
Beyo
nd g
over
nmen
t MDA
s, in
volv
e th
e pr
ivat
e se
ctor
, dev
elop
men
t pa
rtne
rs, c
ivil
soci
ety
and
citiz
ens
TWG,
PM
O, C
ivil
soci
ety
orga
niza
tions
, Pat
ient
hea
lth
asso
ciat
ions
, priv
ate
prov
ider
s as
soci
atio
n, IC
T pr
ovid
ers
asso
ciat
ion,
dev
elop
men
t par
tner
s an
d pr
ofes
siona
l soc
ietie
s
1.4
Link
ed a
nd In
tegr
ated
Pol
icie
s
Nat
iona
l Hea
lth IC
T Fr
amew
ork
inte
grat
ed a
nd li
nked
with
Nat
iona
l he
alth
Act
, NHP
, Nat
iona
l ICT
pol
icy
and
NSH
DP
Link
Nat
iona
l Hea
lth IC
T Fr
amew
ork
with
the
maj
or e
mer
ging
Nat
iona
l po
licie
s (e.
g., t
he N
atio
nal H
ealth
Ac
t, N
atio
nal S
trat
egic
Hea
lth
Deve
lopm
ent p
lan
(NSH
DP),
Nat
iona
l Hea
lth P
olic
y an
d N
atio
nal
ICT
polic
y)
Ensu
re in
clus
ion
of H
ealth
ICT
durin
g re
view
s of N
HA, N
HP, N
atio
nal I
CT
Polic
y an
d N
HSDP
.
Advo
cate
for a
subs
ectio
n on
Hea
lth
ICT
with
in N
SHDP
, NHP
, and
oth
er
rele
vant
and
em
ergi
ng in
stitu
tiona
l m
echa
nism
s.
FMO
H, F
MCT
, Nat
iona
l Hea
lth A
ct
sub
com
mitt
ees,
Nat
iona
l M&
E te
chni
cal w
orki
ng g
roup
, and
oth
er
rele
vant
pla
tfor
ms.
1.5
Fram
ewor
k Ad
optio
n N
atio
nal H
ealth
ICT
Fram
ewor
k de
velo
ped,
end
orse
d an
d pe
riodi
cally
re
view
ed
Ensu
re th
e en
dors
emen
t, ad
optio
n an
d pe
riodi
c re
view
(at m
ost e
very
5
year
s) o
f dev
elop
ed N
atio
nal H
ealth
IC
T Fr
amew
ork
as a
par
t of a
larg
er
Nat
iona
l Hea
lth S
trat
egy
Ensu
re e
ndor
sem
ent,
perio
dic
revi
ew a
nd a
dopt
ion
of N
atio
nal
Heal
th IC
T Fr
amew
ork
Fram
ewor
k co
ntrib
utes
to
esta
blish
ing
a N
atio
nal H
ealth
ICT
stra
tegi
c fr
amew
ork,
but
mul
ti-‐se
ctor
al a
dopt
ion
is cr
itica
l, as
is a
sy
stem
of 5
-‐yea
rly re
view
and
ev
alua
tion
Stee
ring
Com
mitt
ee, T
WG
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
2.0
Strategy and
Investment
2.1
Fund
ing
for H
ealth
ICT
Fund
ing
for H
ealth
ICT
oper
atio
ns
secu
red
Secu
re su
stai
nabl
e fu
ndin
g fo
r the
de
velo
pmen
t and
ope
ratio
n of
the
natio
nal H
ealth
ICT
envi
ronm
ent,
mak
ing
sure
to e
xplo
re th
e vi
abili
ty
of e
xist
ing
fund
s, c
atal
ytic
fund
ing
and
ince
ntiv
es
A. E
xplo
re so
urce
s of H
ealth
ICT
fund
s and
alig
n w
ith F
ram
ewor
k
Expl
ore
sour
ces o
f Hea
lth IC
T fu
nds:
re
venu
e (N
atio
nal a
nd S
tate
s),
deve
lopm
ent p
artn
ers a
nd e
xter
nal
fund
ers,
incl
udin
g pr
ivat
e-‐se
ctor
in
vest
men
ts
FMO
H-‐DP
RS, H
ealth
Fin
anci
ng, F
MF,
FM
CT, P
rivat
e se
ctor
stak
ehol
ders
B.Es
tabl
ish c
atal
ytic
fund
ing
Esta
blish
seed
cat
alyt
ic fu
ndin
g to
su
ppor
t inn
ovat
ion
FMO
H, F
MCT
, PSH
AN, U
SPF,
WB/
IFC
and
deve
lopm
ent p
artn
ers
C.Es
tabl
ish sp
ecia
l pur
pose
fund
for
Heal
th IC
T
A sp
ecia
l pur
pose
fund
for H
ealth
IC
T w
ill e
nsur
e ad
equa
te fu
ndin
g fo
r He
alth
ICT
inno
vatio
n an
d im
plem
enta
tions
NHI
S, N
ITDA
, CBN
, FM
F, N
CC-‐U
SPF,
de
velo
pmen
t par
tner
s
2.2
Mot
ivat
ion
Mot
ivat
ion
mec
hani
sm e
stab
lishe
d Es
tabl
ish m
otiv
atio
n m
echa
nism
for
Set u
p m
otiv
atio
n m
echa
nism
Es
tabl
ish m
otiv
atio
n m
echa
nism
for
FMO
H, F
MCT
, PSH
AN, W
B/IF
C,
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Supp
ort s
etup
of s
tate
leve
l go
vern
ance
stru
ctur
e as
app
ropr
iate

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!45
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers

46!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
5.0
Change and
Ado
ption (Capacity
uilding)
5.1
Syst
em fo
r Hea
lth IC
T Ad
optio
n 5.
1. E
stab
lish
a sy
stem
for H
ealth
ICT
Read
ines
s, M
&E
and
best
pra
ctic
es
adop
tion
Esta
blish
a sy
stem
for s
truc
ture
d as
sess
men
t for
Hea
lth IC
T re
adin
ess
amon
g st
akeh
olde
rs. T
he sy
stem
w
ill su
ppor
t mon
itorin
g an
d ev
alua
tion
of H
ealth
ICT
adop
tion.
A.As
sess
Hea
lth IC
T re
adin
ess o
fst
akeh
olde
rs
Reco
gnize
prio
rity
stak
ehol
der
segm
ents
(con
sum
er, c
are
prov
ider
an
d he
alth
-‐car
e m
anag
er) t
hat s
houl
d be
targ
eted
for H
ealth
ICT
adop
tion,
as
sess
thei
r rea
dine
ss to
ado
pt
spec
ific
Heal
th IC
T so
lutio
ns a
nd
iden
tify
oppo
rtun
ities
to b
uild
m
omen
tum
for s
cale
TWG,
FM
OH
B.Es
tabl
ish n
atio
nal H
ealth
ICT
know
ledg
e re
posit
ory
Crea
te a
nat
iona
l, w
eb-‐b
ased
kn
owle
dge
repo
sitor
y th
at c
aptu
res
Heal
th IC
T pr
ojec
t suc
cess
es a
nd
enab
les k
now
ledg
e sh
arin
g
TWG,
FM
OH,
FM
CT, i
mpl
emen
ting
part
ners
, SM
OH
3.4
Com
mun
icat
ion
Heal
th IC
T st
anda
rds c
omm
unic
ated
an
d ad
voca
ted
Ensu
re th
at c
omm
unic
atio
ns a
nd
info
rmat
ion
diss
emin
ated
abo
ut
Heal
th IC
T st
anda
rds a
re
appr
opria
te to
enc
oura
ge th
e ad
optio
n an
d ap
plic
atio
n of
Hea
lth
ICT
stan
dard
s
A. C
once
rted
and
focu
sed
advo
cacy
, co
mm
unic
atio
n an
d ed
ucat
ion
to
deci
sion
mak
ers a
nd e
nd u
sers
to
ensu
re a
supp
ort f
or th
e ap
plic
atio
n of
stan
dard
s
High
light
ben
efits
of t
he a
dopt
ion
of
Heal
th IC
T st
anda
rds w
hile
em
phas
izing
the
cost
s of n
on-‐
adop
tion
to a
ll re
leva
nt st
akeh
olde
rs
FMO
H, T
WG
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
.0
Legislation Policy and Compliance
4.1
Regu
lato
ry F
ram
ewor
k Es
tabl
ished
Empo
wer
Nat
iona
l Hea
lth IC
T PM
O to
su
ppor
t leg
islat
ion,
pol
icy
and
com
plia
nce
Deve
lop
or id
entif
y a
rele
vant
re
gula
tory
fram
ewor
k (le
gisla
tion,
po
licy
and
com
plia
nce
proc
esse
s) to
en
cour
age
and
ince
ntiv
ize H
ealth
IC
T in
itiat
ives
A.Em
pow
er th
e He
alth
ICT
gove
rnin
g bo
dy w
ith th
e ca
paci
ty to
ov
erse
e, re
view
and
har
mon
ize
polic
y, le
gisla
tion,
regu
latio
n (in
clud
ing
com
plia
nce)
and
im
plem
enta
tion
of H
ealth
ICT
initi
ativ
es
The
Heal
th IC
T go
vern
ing
body
de
scrib
ed u
nder
Lea
ders
hip
and
Gove
rnan
ce sh
ould
be
empo
wer
ed
to g
uide
, inf
luen
ce a
nd m
id-‐w
ife a
re
gula
tory
fram
ewor
k fo
r Hea
lth IC
T ac
tiviti
es
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
Con
sulta
nts a
nd
Part
ners
B.Ag
ree
and
adop
t a n
atio
nally
co
nsist
ent r
egul
ator
y fr
amew
ork
for
heal
th in
form
atio
n
Ensu
ring
priv
ate
and
conf
iden
tial
info
rmat
ion
exch
ange
requ
ires a
na
tiona
lly c
onsis
tent
regu
lato
ry
fram
ewor
k fo
r hea
lth in
form
atio
n pr
otec
tion
This
is of
ten
a re
quire
men
t whe
re
data
pro
tect
ion
legi
slatio
n an
d fr
amew
orks
diff
er, o
r con
flict
, at a
na
tiona
l, st
ate
and
loca
l lev
el
Deve
lopi
ng a
nd a
dopt
ing
such
a
fram
ewor
k en
sure
s tha
t dat
a pr
otec
tion,
priv
acy,
acc
ess a
nd
cons
ent i
s app
roac
hed
and
man
aged
co
nsist
ently
at a
Nat
iona
l, St
ate
and
Loca
l lev
el
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
Con
sulta
nts a
nd
Part
ners
C.Re
view
and
upd
ate
polic
ies
D. E
nsur
e co
mpl
ianc
e of
pro
vide
rs,
serv
ices
and
app
licat
ions
with
re
gula
tory
fram
ewor
k de
fined
in th
e ac
tion
line
abov
e
Focu
sing
on c
ompl
ianc
e w
ith
esta
blish
ed re
gula
tions
(leg
islat
ion
and
polic
y), t
he P
MO
or T
WG
will
pr
omot
e, e
ncou
rage
and
ens
ure
com
plia
nce
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
uni
ts
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Co
mpo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
5.0
Change and
Ado
ption (Capacity
uilding)
5.1
Syst
em fo
r Hea
lth IC
T Ad
optio
n 5.
1. E
stab
lish
a sy
stem
for H
ealth
ICT
Read
ines
s, M
&E
and
best
pra
ctic
es
adop
tion
Esta
blish
a sy
stem
for s
truc
ture
d as
sess
men
t for
Hea
lth IC
T re
adin
ess
amon
g st
akeh
olde
rs. T
he sy
stem
w
ill su
ppor
t mon
itorin
g an
d ev
alua
tion
of H
ealth
ICT
adop
tion.
A.As
sess
Hea
lth IC
T re
adin
ess o
fst
akeh
olde
rs
Reco
gnize
prio
rity
stak
ehol
der
segm
ents
(con
sum
er, c
are
prov
ider
an
d he
alth
-‐car
e m
anag
er) t
hat s
houl
d be
targ
eted
for H
ealth
ICT
adop
tion,
as
sess
thei
r rea
dine
ss to
ado
pt
spec
ific
Heal
th IC
T so
lutio
ns a
nd
iden
tify
oppo
rtun
ities
to b
uild
m
omen
tum
for s
cale
TWG,
FM
OH
B.Es
tabl
ish n
atio
nal H
ealth
ICT
know
ledg
e re
posit
ory
Crea
te a
nat
iona
l, w
eb-‐b
ased
kn
owle
dge
repo
sitor
y th
at c
aptu
res
Heal
th IC
T pr
ojec
t suc
cess
es a
nd
enab
les k
now
ledg
e sh
arin
g
TWG,
FM
OH,
FM
CT, i
mpl
emen
ting
part
ners
, SM
OH
3.4
Com
mun
icat
ion
Heal
th IC
T st
anda
rds c
omm
unic
ated
an
d ad
voca
ted
Ensu
re th
at c
omm
unic
atio
ns a
nd
info
rmat
ion
diss
emin
ated
abo
ut
Heal
th IC
T st
anda
rds a
re
appr
opria
te to
enc
oura
ge th
e ad
optio
n an
d ap
plic
atio
n of
Hea
lth
ICT
stan
dard
s
A. C
once
rted
and
focu
sed
advo
cacy
, co
mm
unic
atio
n an
d ed
ucat
ion
to
deci
sion
mak
ers a
nd e
nd u
sers
to
ensu
re a
supp
ort f
or th
e ap
plic
atio
n of
stan
dard
s
High
light
ben
efits
of t
he a
dopt
ion
of
Heal
th IC
T st
anda
rds w
hile
em
phas
izing
the
cost
s of n
on-‐
adop
tion
to a
ll re
leva
nt st
akeh
olde
rs
FMO
H, T
WG
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
.0
Legislation Policy and Compliance
4.1
Regu
lato
ry F
ram
ewor
k Es
tabl
ished
Empo
wer
Nat
iona
l Hea
lth IC
T PM
O to
su
ppor
t leg
islat
ion,
pol
icy
and
com
plia
nce
Deve
lop
or id
entif
y a
rele
vant
re
gula
tory
fram
ewor
k (le
gisla
tion,
po
licy
and
com
plia
nce
proc
esse
s) to
en
cour
age
and
ince
ntiv
ize H
ealth
IC
T in
itiat
ives
A.Em
pow
er th
e He
alth
ICT
gove
rnin
g bo
dy w
ith th
e ca
paci
ty to
ov
erse
e, re
view
and
har
mon
ize
polic
y, le
gisla
tion,
regu
latio
n (in
clud
ing
com
plia
nce)
and
im
plem
enta
tion
of H
ealth
ICT
initi
ativ
es
The
Heal
th IC
T go
vern
ing
body
de
scrib
ed u
nder
Lea
ders
hip
and
Gove
rnan
ce sh
ould
be
empo
wer
ed
to g
uide
, inf
luen
ce a
nd m
id-‐w
ife a
re
gula
tory
fram
ewor
k fo
r Hea
lth IC
T ac
tiviti
es
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
Con
sulta
nts a
nd
Part
ners
B.Ag
ree
and
adop
t a n
atio
nally
co
nsist
ent r
egul
ator
y fr
amew
ork
for
heal
th in
form
atio
n
Ensu
ring
priv
ate
and
conf
iden
tial
info
rmat
ion
exch
ange
requ
ires a
na
tiona
lly c
onsis
tent
regu
lato
ry
fram
ewor
k fo
r hea
lth in
form
atio
n pr
otec
tion
This
is of
ten
a re
quire
men
t whe
re
data
pro
tect
ion
legi
slatio
n an
d fr
amew
orks
diff
er, o
r con
flict
, at a
na
tiona
l, st
ate
and
loca
l lev
el
Deve
lopi
ng a
nd a
dopt
ing
such
a
fram
ewor
k en
sure
s tha
t dat
a pr
otec
tion,
priv
acy,
acc
ess a
nd
cons
ent i
s app
roac
hed
and
man
aged
co
nsist
ently
at a
Nat
iona
l, St
ate
and
Loca
l lev
el
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
Con
sulta
nts a
nd
Part
ners
C.Re
view
and
upd
ate
polic
ies
D. E
nsur
e co
mpl
ianc
e of
pro
vide
rs,
serv
ices
and
app
licat
ions
with
re
gula
tory
fram
ewor
k de
fined
in th
e ac
tion
line
abov
e
Focu
sing
on c
ompl
ianc
e w
ith
esta
blish
ed re
gula
tions
(leg
islat
ion
and
polic
y), t
he P
MO
or T
WG
will
pr
omot
e, e
ncou
rage
and
ens
ure
com
plia
nce
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
uni
ts
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
5.0
Change and
Ado
ption (Capacity
uilding)
5.1
Syst
em fo
r Hea
lth IC
T Ad
optio
n 5.
1. E
stab
lish
a sy
stem
for H
ealth
ICT
Read
ines
s, M
&E
and
best
pra
ctic
es
adop
tion
Esta
blish
a sy
stem
for s
truc
ture
d as
sess
men
t for
Hea
lth IC
T re
adin
ess
amon
g st
akeh
olde
rs. T
he sy
stem
w
ill su
ppor
t mon
itorin
g an
d ev
alua
tion
of H
ealth
ICT
adop
tion.
A.As
sess
Hea
lth IC
T re
adin
ess o
fst
akeh
olde
rs
Reco
gnize
prio
rity
stak
ehol
der
segm
ents
(con
sum
er, c
are
prov
ider
an
d he
alth
-‐car
e m
anag
er) t
hat s
houl
d be
targ
eted
for H
ealth
ICT
adop
tion,
as
sess
thei
r rea
dine
ss to
ado
pt
spec
ific
Heal
th IC
T so
lutio
ns a
nd
iden
tify
oppo
rtun
ities
to b
uild
m
omen
tum
for s
cale
TWG,
FM
OH
B.Es
tabl
ish n
atio
nal H
ealth
ICT
know
ledg
e re
posit
ory
Crea
te a
nat
iona
l, w
eb-‐b
ased
kn
owle
dge
repo
sitor
y th
at c
aptu
res
Heal
th IC
T pr
ojec
t suc
cess
es a
nd
enab
les k
now
ledg
e sh
arin
g
TWG,
FM
OH,
FM
CT, i
mpl
emen
ting
part
ners
, SM
OH
3.4
Com
mun
icat
ion
Heal
th IC
T st
anda
rds c
omm
unic
ated
an
d ad
voca
ted
Ensu
re th
at c
omm
unic
atio
ns a
nd
info
rmat
ion
diss
emin
ated
abo
ut
Heal
th IC
T st
anda
rds a
re
appr
opria
te to
enc
oura
ge th
e ad
optio
n an
d ap
plic
atio
n of
Hea
lth
ICT
stan
dard
s
A. C
once
rted
and
focu
sed
advo
cacy
, co
mm
unic
atio
n an
d ed
ucat
ion
to
deci
sion
mak
ers a
nd e
nd u
sers
to
ensu
re a
supp
ort f
or th
e ap
plic
atio
n of
stan
dard
s
High
light
ben
efits
of t
he a
dopt
ion
of
Heal
th IC
T st
anda
rds w
hile
em
phas
izing
the
cost
s of n
on-‐
adop
tion
to a
ll re
leva
nt st
akeh
olde
rs
FMO
H, T
WG
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
.0
Legislation Policy and Compliance
4.1
Regu
lato
ry F
ram
ewor
k Es
tabl
ished
Empo
wer
Nat
iona
l Hea
lth IC
T PM
O to
su
ppor
t leg
islat
ion,
pol
icy
and
com
plia
nce
Deve
lop
or id
entif
y a
rele
vant
re
gula
tory
fram
ewor
k (le
gisla
tion,
po
licy
and
com
plia
nce
proc
esse
s) to
en
cour
age
and
ince
ntiv
ize H
ealth
IC
T in
itiat
ives
A.Em
pow
er th
e He
alth
ICT
gove
rnin
g bo
dy w
ith th
e ca
paci
ty to
ov
erse
e, re
view
and
har
mon
ize
polic
y, le
gisla
tion,
regu
latio
n (in
clud
ing
com
plia
nce)
and
im
plem
enta
tion
of H
ealth
ICT
initi
ativ
es
The
Heal
th IC
T go
vern
ing
body
de
scrib
ed u
nder
Lea
ders
hip
and
Gove
rnan
ce sh
ould
be
empo
wer
ed
to g
uide
, inf
luen
ce a
nd m
id-‐w
ife a
re
gula
tory
fram
ewor
k fo
r Hea
lth IC
T ac
tiviti
es
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
Con
sulta
nts a
nd
Part
ners
B.Ag
ree
and
adop
t a n
atio
nally
co
nsist
ent r
egul
ator
y fr
amew
ork
for
heal
th in
form
atio
n
Ensu
ring
priv
ate
and
conf
iden
tial
info
rmat
ion
exch
ange
requ
ires a
na
tiona
lly c
onsis
tent
regu
lato
ry
fram
ewor
k fo
r hea
lth in
form
atio
n pr
otec
tion
This
is of
ten
a re
quire
men
t whe
re
data
pro
tect
ion
legi
slatio
n an
d fr
amew
orks
diff
er, o
r con
flict
, at a
na
tiona
l, st
ate
and
loca
l lev
el
Deve
lopi
ng a
nd a
dopt
ing
such
a
fram
ewor
k en
sure
s tha
t dat
a pr
otec
tion,
priv
acy,
acc
ess a
nd
cons
ent i
s app
roac
hed
and
man
aged
co
nsist
ently
at a
Nat
iona
l, St
ate
and
Loca
l lev
el
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
Con
sulta
nts a
nd
Part
ners
C.Re
view
and
upd
ate
polic
ies
D. E
nsur
e co
mpl
ianc
e of
pro
vide
rs,
serv
ices
and
app
licat
ions
with
re
gula
tory
fram
ewor
k de
fined
in th
e ac
tion
line
abov
e
Focu
sing
on c
ompl
ianc
e w
ith
esta
blish
ed re
gula
tions
(leg
islat
ion
and
polic
y), t
he P
MO
or T
WG
will
pr
omot
e, e
ncou
rage
and
ens
ure
com
plia
nce
FMO
H, N
ITDA
, FM
CT, H
ERFO
N,
NAS
S, L
egal
uni
ts

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!47
C.De
fine
prof
essio
nal p
ract
ice
stan
dard
s
Wor
k w
ith c
ross
-‐sec
tora
l st
akeh
olde
rs to
gui
de th
e de
velo
pmen
t of a
pro
fess
iona
l pr
actic
e st
anda
rds a
nd g
uide
lines
for
heal
thca
re p
rovi
ders
Def
ine
the
expe
ctat
ions
and
ob
ligat
ions
of t
hese
pro
vide
rs to
co
llect
, sto
re a
nd sh
are
high
-‐qua
lity
elec
tron
ic h
ealth
-‐car
e in
form
atio
n in
a
timel
y, a
ppro
pria
te a
nd se
cure
m
anne
r
TWG,
FM
OH,
NIT
DA
D.M
onito
r Hea
lth IC
T ad
optio
nM
onito
r and
revi
ew a
dopt
ion
of
Heal
th IC
T so
lutio
ns ro
utin
ely
amon
g st
akeh
olde
rs
TWG,
FM
OH
5.2
Ince
ntiv
ize sk
ills u
ptak
e 5.
2. D
evel
op a
nd a
dopt
Ince
ntiv
e m
echa
nism
s to
enco
urag
e up
take
of
Heal
th IC
T sk
ills a
nd c
ompe
tenc
ies
Desig
n an
d ad
opt s
truc
ture
d in
cent
ive
sche
me
(bot
h fin
anci
al
and
non-‐
finan
cial
) to
enco
urag
e up
take
and
rete
ntio
n of
Hea
lth IC
T sk
ills a
nd c
ompe
tenc
ies.
A.De
velo
p an
d Ro
ll-‐ou
t in
cent
ive
sche
mes
for H
ealth
ICT
adop
tion
Desig
n in
cent
ive
prog
ram
s to
enco
urag
e th
e ad
optio
n an
d us
e of
He
alth
ICT
serv
ices
and
app
licat
ions
. Th
is sh
ould
incl
ude
cond
ition
s of
fund
ing,
elig
ibili
ty c
riter
ia, a
pplic
atio
n an
d ap
prov
al p
roce
sses
, fun
ding
ad
min
istra
tion,
and
ass
ocia
ted
role
s an
d re
spon
sibili
ties
NCH
, SM
OH,
TW
G, F
MO
H
B.Di
ssem
inat
e in
cent
ive
prog
ram
Deve
lop
com
mun
icat
ion
stra
tegy
and
m
ater
ials
to p
ublic
ize in
cent
ives
and
pu
t in
plac
e ne
cess
ary
mec
hani
sms t
o su
ppor
t thi
s, in
clud
ing
fund
ing
guid
elin
es, i
nfor
mat
ion
and
appl
icat
ion
form
s
C. D
evel
op st
rate
gy fo
r con
tinue
dHe
alth
ICT
skill
s and
com
pete
ncy
acqu
isitio
n
Deve
lop
a st
rate
gy fo
r on
the
job
Heal
th IC
T sk
ills i
mpr
ovem
ent,
trai
ning
and
retr
aini
ng fo
r rel
evan
t ca
dre
of h
ealth
wor
kfor
ce
Com
mun
ity a
nd H
ealth
Pra
ctiti
oner
Re
gist
ratio
n Bo
ard
of N
iger
ia
(CHP
RBN
)Hea
lth R
ecor
ds O
ffice
rs
Regu
lato
ry B
oard
of N
iger
ia
(HRO
RBN
) M
edic
al a
nd D
enta
l Co
unci
l of N
iger
ia (M
DCN
) M
edic
al
Scie
nce
Coun
cil o
f Nig
eria
Nur
sing
and
Mid
wife
ry c
ounc
il of
Nig
eria
(N
MCN
) Ph
arm
acist
s Cou
ncil
of
Nig
eria
(PCN
) En
viro
nmen
tal
Heal
th R
egist
ratio
n Bo
ard
of
Nig
eria
.and
rele
vant
pro
fess
iona
ls
D.De
sign
Heal
th IC
T sk
ills a
ndco
mpe
tenc
es c
aree
r pro
gres
sion
plan
Desig
n an
d in
stitu
tiona
lize
Heal
th IC
T sk
ills a
nd c
ompe
tenc
ies p
rogr
essio
n pl
an th
roug
h th
e fe
dera
l civ
il se
rvic
e an
d ot
her r
elat
ed sc
hem
es o
f ser
vice
CHPR
B H
RORB
N M
DCN
N
MCN
PCN
Env
ironm
enta
l Hea
lth
regi
stra
tion
Boar
d of
Nig
eria
5.3
Skill
s acc
redi
tatio
n an
d cu
rric
ulum
re
view
5.3.
Est
ablis
h m
etho
dolo
gy fo
r ac
cred
itatio
n an
d re
visio
n of
Hea
lth
ICT
Curr
icul
um
Deve
lop/
revi
ew H
ealth
ICT
curr
icul
um i
n he
alth
, tec
hnol
ogy
and
rele
vant
inst
itutio
ns A
lso
supp
ort n
ew a
ccre
dita
tion
regi
mes
fo
r reg
ulat
ory
orga
niza
tions
A.Id
entif
y ed
ucat
ion
and
trai
ning
co
urse
cha
nges
Dete
rmin
e ch
ange
s tha
t are
requ
ired
to e
xist
ing
educ
atio
n an
d tr
aini
ng
cour
ses t
o en
sure
the
deve
lopm
ent
of H
ealth
ICT
wor
kfor
ce c
apab
ilitie
s Sc
hool
of M
edic
ine
Sch
ool o
f He
alth
tech
nolo
gy N
ursin
g an
d ot
hers
Hea
lth In
form
atic
s deg
ree
awar
ding
Uni
vers
ities
NU
C, N
BTE,
N
ITDA
B.
Defin
e ne
w a
ccre
dita
tion
requ
irem
ents
Iden
tify
and
defin
e ch
ange
s to
exist
ing
prof
essio
nal a
ccre
dita
tion
prog
ram
s for
hea
lthca
re in
stitu
tions
an
d in
divi
dual
hea
lthca
re p
rovi
ders
to
incl
ude
Heal
th IC
T
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers

48!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
C.De
velo
p st
anda
rd H
ealth
ICT
com
pete
ncy
fram
ewor
k
Deve
lop
a st
anda
rd H
ealth
ICT
com
pete
ncy
fram
ewor
k fo
r hea
lth
wor
kers
and
Hea
lth IC
T pr
actit
ione
rs
Fram
ewor
k sh
ould
pro
vide
an
unde
rsta
ndin
g of
requ
ired
Heal
th IC
T kn
owle
dge,
skill
s and
att
ribut
es fo
r th
ese
vario
us p
rofe
ssio
nal g
roup
s
FMO
H, T
WG,
NIT
DA
D. E
stab
lish
spec
ializ
ed H
ealth
ICT
qual
ifica
tions
and
cer
tific
atio
n tr
ack
Iden
tify
and
esta
blish
nat
iona
lly
reco
gnize
d te
rtia
ry q
ualif
icat
ions
in
Heal
th IC
T (e
.g. h
ealth
info
rmat
ics
exch
ange
) and
impl
emen
ting
form
alize
d tr
aini
ng/e
duca
tion
prog
ram
s des
igne
d to
reco
gnize
and
pr
omot
e th
e sp
read
of H
ealth
ICT
skill
s and
exp
ertis
e
FMO
H, T
WG,
NU
C, N
BTE
E.Im
plem
ent n
ew a
ccre
dita
tion
requ
irem
ents
Liai
se w
ith th
e ap
prop
riate
pr
ofes
siona
l bod
ies a
nd w
orki
ng
grou
ps to
agr
ee to
cha
nges
to
accr
edita
tion
requ
irem
ents
and
im
plem
ent t
hese
cha
nges
thro
ugho
ut
segm
ents
of t
he h
ealth
sect
or, a
nd
broa
der h
ealth
sect
or
Scho
ol o
f Med
icin
e S
choo
l of
Heal
th T
echn
olog
y H
ealth
In
form
atic
s deg
ree-‐
awar
ding
un
iver
sitie
s N
UC,
FM
OH
5.4
Awar
enes
s and
stak
ehol
der
enga
gem
ent
5.4.
Est
ablis
h a
plan
for H
ealth
ICT
awar
enes
s and
stak
ehol
der
enga
gem
ent
Esta
blish
mec
hani
sm fo
r Hea
lth IC
T ac
tiviti
es a
war
enes
s and
targ
eted
He
alth
ICT
stak
ehol
der
enga
gem
ent.
A.De
velo
p He
alth
ICT
awar
enes
sca
mpa
ign
stra
tegy
Deve
lop
awar
enes
s cam
paig
ns th
at
utili
ze a
ppro
pria
te c
omm
unic
atio
n m
echa
nism
s and
foru
ms t
o pr
omot
e aw
aren
ess o
f Hea
lth IC
T, sp
ecifi
c se
rvic
es a
nd a
pplic
atio
ns, a
nd th
eir
bene
fits
Roll-‐
out a
war
enes
s cam
paig
ns to
hi
gh-‐p
riorit
y ch
ange
and
ado
ptio
n ta
rget
s, a
nd o
ver t
ime
exte
nd to
br
oade
r hea
lth se
ctor
and
pub
lic
TWG,
FM
OH,
Impl
emen
ting
part
ners
B.Ro
llout
Hea
lth IC
T aw
aren
ess
cam
paig
ns
C. D
esig
n M
&E
fram
ewor
k fo
r m
easu
ring
effe
ctiv
enes
s of
enga
gem
ent
Defin
e cl
ear c
riter
ia a
nd ta
rget
s for
He
alth
ICT
awar
enes
s and
pro
gres
s,
and
perio
dica
lly m
easu
re a
ctua
l aw
aren
ess a
nd p
rogr
ams a
gain
st
thes
e, to
ass
ess t
he e
ffect
iven
ess o
f He
alth
ICT
chan
ge a
nd a
dopt
ion
activ
ities
acr
oss s
take
hold
ers
Nig
eria
Med
ical
Ass
ocia
tion
(NM
A)
DPRS
-‐FM
OH
SM
OH
D. D
esig
n ta
rget
ed st
akeh
olde
r re
fere
nce
and
wor
king
gro
ups
Desig
n a
set o
f tar
gete
d st
akeh
olde
r en
gage
men
t for
ums t
hat h
ave
clea
r go
als,
obj
ectiv
es a
nd d
eliv
erab
les
TWG,
FM
OH
E.En
gage
and
con
sult
with
stak
ehol
der r
efer
ence
and
wor
king
gr
oups
Enga
ge/I
nvol
ve st
akeh
olde
r re
fere
nce
grou
ps th
roug
hout
the
deve
lopm
ent o
f the
Hea
lth IC
T en
viro
nmen
t
Grou
ps w
ill b
e in
volv
ed in
exp
lorin
g pa
rtic
ular
issu
es a
nd ri
sks r
elat
ed to
th
e de
velo
pmen
t of t
he c
ount
rys
Heal
th IC
T en
viro
nmen
t, an
d th
e id
entif
icat
ion
of a
ccep
tabl
e so
lutio
ns
to th
ese
TWG,
FM
OH
5.5
Heal
th IC
T Ed
ucat
ion
and
Trai
ning
5.
5. E
stab
lish
Heal
th IC
T ed
ucat
ion
and
trai
ning
pro
gram
s
Crea
te n
ew H
ealth
ICT
educ
atio
n an
d tr
aini
ng p
rogr
ams t
o su
ppor
t im
prov
ed H
ealth
ICT
skill
s and
co
mpe
tenc
ies a
mon
g pr
iorit
y st
akeh
olde
rs (c
onsu
mer
s, h
ealth
pr
ovid
ers,
hea
lth c
are
man
ager
s,
A.Im
plem
ent e
duca
tion
and
trai
ning
co
urse
cha
nges
Wor
k w
ith e
duca
tion
inst
itutio
ns (e
.g.
univ
ersit
ies,
voc
atio
nal t
rain
ing
inst
itutio
ns, p
rofe
ssio
nal b
odie
s) to
in
sert
Hea
lth IC
T in
to th
eir c
urric
ula
wer
e ne
cess
ary.
Scho
ol o
f Med
icin
e S
choo
l of
Heal
th te
chno
logy
Hea
lth
Info
rmat
ics d
egre
e aw
ardi
ng
Uni
vers
ities
NU
C, T
WG
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!49
C.De
velo
p st
anda
rd H
ealth
ICT
com
pete
ncy
fram
ewor
k
Deve
lop
a st
anda
rd H
ealth
ICT
com
pete
ncy
fram
ewor
k fo
r hea
lth
wor
kers
and
Hea
lth IC
T pr
actit
ione
rs
Fram
ewor
k sh
ould
pro
vide
an
unde
rsta
ndin
g of
requ
ired
Heal
th IC
T kn
owle
dge,
skill
s and
att
ribut
es fo
r th
ese
vario
us p
rofe
ssio
nal g
roup
s
FMO
H, T
WG,
NIT
DA
D. E
stab
lish
spec
ializ
ed H
ealth
ICT
qual
ifica
tions
and
cer
tific
atio
n tr
ack
Iden
tify
and
esta
blish
nat
iona
lly
reco
gnize
d te
rtia
ry q
ualif
icat
ions
in
Heal
th IC
T (e
.g. h
ealth
info
rmat
ics
exch
ange
) and
impl
emen
ting
form
alize
d tr
aini
ng/e
duca
tion
prog
ram
s des
igne
d to
reco
gnize
and
pr
omot
e th
e sp
read
of H
ealth
ICT
skill
s and
exp
ertis
e
FMO
H, T
WG,
NU
C, N
BTE
E.Im
plem
ent n
ew a
ccre
dita
tion
requ
irem
ents
Liai
se w
ith th
e ap
prop
riate
pr
ofes
siona
l bod
ies a
nd w
orki
ng
grou
ps to
agr
ee to
cha
nges
to
accr
edita
tion
requ
irem
ents
and
im
plem
ent t
hese
cha
nges
thro
ugho
ut
segm
ents
of t
he h
ealth
sect
or, a
nd
broa
der h
ealth
sect
or
Scho
ol o
f Med
icin
e S
choo
l of
Heal
th T
echn
olog
y H
ealth
In
form
atic
s deg
ree-‐
awar
ding
un
iver
sitie
s N
UC,
FM
OH
5.4
Awar
enes
s and
stak
ehol
der
enga
gem
ent
5.4.
Est
ablis
h a
plan
for H
ealth
ICT
awar
enes
s and
stak
ehol
der
enga
gem
ent
Esta
blish
mec
hani
sm fo
r Hea
lth IC
T ac
tiviti
es a
war
enes
s and
targ
eted
He
alth
ICT
stak
ehol
der
enga
gem
ent.
A.De
velo
p He
alth
ICT
awar
enes
sca
mpa
ign
stra
tegy
Deve
lop
awar
enes
s cam
paig
ns th
at
utili
ze a
ppro
pria
te c
omm
unic
atio
n m
echa
nism
s and
foru
ms t
o pr
omot
e aw
aren
ess o
f Hea
lth IC
T, sp
ecifi
c se
rvic
es a
nd a
pplic
atio
ns, a
nd th
eir
bene
fits
Roll-‐
out a
war
enes
s cam
paig
ns to
hi
gh-‐p
riorit
y ch
ange
and
ado
ptio
n ta
rget
s, a
nd o
ver t
ime
exte
nd to
br
oade
r hea
lth se
ctor
and
pub
lic
TWG,
FM
OH,
Impl
emen
ting
part
ners
B.Ro
llout
Hea
lth IC
T aw
aren
ess
cam
paig
ns
C. D
esig
n M
&E
fram
ewor
k fo
r m
easu
ring
effe
ctiv
enes
s of
enga
gem
ent
Defin
e cl
ear c
riter
ia a
nd ta
rget
s for
He
alth
ICT
awar
enes
s and
pro
gres
s,
and
perio
dica
lly m
easu
re a
ctua
l aw
aren
ess a
nd p
rogr
ams a
gain
st
thes
e, to
ass
ess t
he e
ffect
iven
ess o
f He
alth
ICT
chan
ge a
nd a
dopt
ion
activ
ities
acr
oss s
take
hold
ers
Nig
eria
Med
ical
Ass
ocia
tion
(NM
A)
DPRS
-‐FM
OH
SM
OH
D. D
esig
n ta
rget
ed st
akeh
olde
r re
fere
nce
and
wor
king
gro
ups
Desig
n a
set o
f tar
gete
d st
akeh
olde
r en
gage
men
t for
ums t
hat h
ave
clea
r go
als,
obj
ectiv
es a
nd d
eliv
erab
les
TWG,
FM
OH
E.En
gage
and
con
sult
with
stak
ehol
der r
efer
ence
and
wor
king
gr
oups
Enga
ge/I
nvol
ve st
akeh
olde
r re
fere
nce
grou
ps th
roug
hout
the
deve
lopm
ent o
f the
Hea
lth IC
T en
viro
nmen
t
Grou
ps w
ill b
e in
volv
ed in
exp
lorin
g pa
rtic
ular
issu
es a
nd ri
sks r
elat
ed to
th
e de
velo
pmen
t of t
he c
ount
rys
Heal
th IC
T en
viro
nmen
t, an
d th
e id
entif
icat
ion
of a
ccep
tabl
e so
lutio
ns
to th
ese
TWG,
FM
OH
5.5
Heal
th IC
T Ed
ucat
ion
and
Trai
ning
5.
5. E
stab
lish
Heal
th IC
T ed
ucat
ion
and
trai
ning
pro
gram
s
Crea
te n
ew H
ealth
ICT
educ
atio
n an
d tr
aini
ng p
rogr
ams t
o su
ppor
t im
prov
ed H
ealth
ICT
skill
s and
co
mpe
tenc
ies a
mon
g pr
iorit
y st
akeh
olde
rs (c
onsu
mer
s, h
ealth
pr
ovid
ers,
hea
lth c
are
man
ager
s,
A.Im
plem
ent e
duca
tion
and
trai
ning
co
urse
cha
nges
Wor
k w
ith e
duca
tion
inst
itutio
ns (e
.g.
univ
ersit
ies,
voc
atio
nal t
rain
ing
inst
itutio
ns, p
rofe
ssio
nal b
odie
s) to
in
sert
Hea
lth IC
T in
to th
eir c
urric
ula
wer
e ne
cess
ary.
Scho
ol o
f Med
icin
e S
choo
l of
Heal
th te
chno
logy
Hea
lth
Info
rmat
ics d
egre
e aw
ardi
ng
Uni
vers
ities
NU
C, T
WG
and
heal
th a
dmin
istra
tors
)
B.Im
plem
ent s
peci
alize
d He
alth
ICT
cour
ses
Iden
tify
and
esta
blish
inte
rnat
iona
lly
reco
gnize
d te
rtia
ry q
ualif
icat
ions
in
Heal
th IC
T (e
.g. h
ealth
info
rmat
ics)
an
d im
plem
ent f
orm
alize
d tr
aini
ng/e
duca
tion
prog
ram
s de
signe
d to
reco
gnize
and
pro
mot
e th
e sp
read
of H
ealth
ICT
skill
s and
ex
pert
ise
Scho
ol o
f Med
icin
e S
choo
l of
Heal
th te
chno
logy
Hea
lth
Info
rmat
ics d
egre
e aw
ardi
ng
Uni
vers
ities
NU
C, N
BTE,
TW
G
C. R
evie
w F
MO
H co
llabo
rativ
e pr
ogra
ms t
o in
clud
e he
alth
in
form
atic
s
Desig
n an
d in
sert
rele
vant
Hea
lth IC
T an
d in
form
atic
s com
pete
ncy
skill
s re
quire
d to
adv
ance
rele
vant
skill
s an
d co
mpe
tenc
ies a
mon
gst m
anag
ers
in th
e FM
OH
colla
bora
tive
cent
er
prog
ram
FMO
H, R
elev
ant U
nive
rsiti
es, T
WG
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
.0
Inrastructure
.1 E
xpan
ded
Cove
rage
Co
nnec
tivity
cov
erag
e ex
pand
ed a
nd
enha
nced
Focu
sing
and
prio
ritizi
ng
inte
rven
tions
bas
ed o
n po
pula
tion
dens
ity, d
iseas
e pr
eval
ence
, and
pr
ovid
ing
adeq
uate
con
nect
ivity
an
d su
ppor
ting
them
with
rele
vant
po
licie
s and
ena
blin
g en
viro
nmen
ts
A.Id
entif
y un
ders
erve
d ar
eas
Heal
th F
acili
ties a
nd c
omm
uniti
es.
Serv
ices
cov
erag
e w
ill c
over
pow
er,
conn
ectiv
ity a
nd c
ompu
ting
infr
astr
uctu
re c
over
age
USP
F, T
WG,
GBB
, MGO
s
B. L
ocal
par
ticip
atio
n of
com
mun
ities
in
supp
ort,
mai
nten
ance
and
use
of
infr
astr
uctu
re H
ealth
ICT
serv
ices
and
appl
icat
ion
Ensu
re lo
cal p
artic
ipat
ion
and
owne
rshi
p of
Hea
lth IC
T pr
ojec
ts a
nd
equi
pmen
t
FMO
H, F
MCT
(eGo
vt),
Gala
xy
Back
bone
(GBB
), LG
A an
d co
mm
unity
lead
ers,
Mob
ile
Telc
oms,
NCC
, NGO
s, U
SPF,
NHI
S
C.As
sess
infr
astr
uctu
re a
vaila
bilit
y of
heal
th fa
cilit
ies a
nd p
rogr
ams
Data
con
nect
ivity
is a
key
foun
datio
n fo
r sha
ring
elec
tron
ic in
form
atio
n be
twee
n ca
re p
rovi
ders
, and
for t
he p
rovi
sion
of h
ealth
-‐car
e se
rvic
es th
roug
h el
ectr
onic
ch
anne
ls (e
.g. t
eleH
ealth
ICT)
This
activ
ity n
eeds
to id
entif
y th
e pr
iorit
y he
alth
-‐car
e pr
ovid
er se
gmen
ts a
nd c
omm
uniti
es
that
requ
ire in
vest
men
t in
fit fo
r pu
rpos
e
data
con
nect
ivity
In o
rder
to a
id e
ffici
ency
and
opt
imize
lim
ited
fund
s, h
ealth
car
e fa
cilit
ies
with
the
high
est r
each
in
com
mun
ities
shou
ld b
e id
entif
ied
and
enha
nced
, tec
hnol
ogy-‐
wise
FMO
H, F
MCT
(eGo
vt),
Gala
xy
Back
bone
(GBB
), LG
A an
d co
mm
unity
lead
ers,
Mob
ile
Telc
oms,
NCC
, NGO
s, U
SPF
D.Se
lect
impl
emen
tatio
n pa
rtne
rs to
deve
lop
data
con
nect
ivity
in
fras
truc
ture
The
coun
try
will
nee
d to
sele
ct d
ata
conn
ectiv
ity in
fras
truc
ture
pro
vide
rs
and
oper
ator
s to
assis
t in
deve
lopi
ng
the
requ
ired
data
con
nect
ivity
in
fras
truc
ture
Thes
e co
uld
be p
rivat
e an
d/or
pub
lic
orga
niza
tions
FMCT
, NCC
, USP
F, M
obile
Tel
com
s,
GBB,
NGO
s
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
and
heal
th a
dmin
istra
tors
)
B.Im
plem
ent s
peci
alize
d He
alth
ICT
cour
ses
Iden
tify
and
esta
blish
inte
rnat
iona
lly
reco
gnize
d te
rtia
ry q
ualif
icat
ions
in
Heal
th IC
T (e
.g. h
ealth
info
rmat
ics)
an
d im
plem
ent f
orm
alize
d tr
aini
ng/e
duca
tion
prog
ram
s de
signe
d to
reco
gnize
and
pro
mot
e th
e sp
read
of H
ealth
ICT
skill
s and
ex
pert
ise
Scho
ol o
f Med
icin
e S
choo
l of
Heal
th te
chno
logy
Hea
lth
Info
rmat
ics d
egre
e aw
ardi
ng
Uni
vers
ities
NU
C, N
BTE,
TW
G
C. R
evie
w F
MO
H co
llabo
rativ
e pr
ogra
ms t
o in
clud
e he
alth
in
form
atic
s
Desig
n an
d in
sert
rele
vant
Hea
lth IC
T an
d in
form
atic
s com
pete
ncy
skill
s re
quire
d to
adv
ance
rele
vant
skill
s an
d co
mpe
tenc
ies a
mon
gst m
anag
ers
in th
e FM
OH
colla
bora
tive
cent
er
prog
ram
FMO
H, R
elev
ant U
nive
rsiti
es, T
WG
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
.0
Inrastructure
.1 E
xpan
ded
Cove
rage
Co
nnec
tivity
cov
erag
e ex
pand
ed a
nd
enha
nced
Focu
sing
and
prio
ritizi
ng
inte
rven
tions
bas
ed o
n po
pula
tion
dens
ity, d
iseas
e pr
eval
ence
, and
pr
ovid
ing
adeq
uate
con
nect
ivity
an
d su
ppor
ting
them
with
rele
vant
po
licie
s and
ena
blin
g en
viro
nmen
ts
A.Id
entif
y un
ders
erve
d ar
eas
Heal
th F
acili
ties a
nd c
omm
uniti
es.
Serv
ices
cov
erag
e w
ill c
over
pow
er,
conn
ectiv
ity a
nd c
ompu
ting
infr
astr
uctu
re c
over
age
USP
F, T
WG,
GBB
, MGO
s
B. L
ocal
par
ticip
atio
n of
com
mun
ities
in
supp
ort,
mai
nten
ance
and
use
of
infr
astr
uctu
re H
ealth
ICT
serv
ices
and
appl
icat
ion
Ensu
re lo
cal p
artic
ipat
ion
and
owne
rshi
p of
Hea
lth IC
T pr
ojec
ts a
nd
equi
pmen
t
FMO
H, F
MCT
(eGo
vt),
Gala
xy
Back
bone
(GBB
), LG
A an
d co
mm
unity
lead
ers,
Mob
ile
Telc
oms,
NCC
, NGO
s, U
SPF,
NHI
S
C.As
sess
infr
astr
uctu
re a
vaila
bilit
y of
heal
th fa
cilit
ies a
nd p
rogr
ams
Data
con
nect
ivity
is a
key
foun
datio
n fo
r sha
ring
elec
tron
ic in
form
atio
n be
twee
n ca
re p
rovi
ders
, and
for t
he p
rovi
sion
of h
ealth
-‐car
e se
rvic
es th
roug
h el
ectr
onic
ch
anne
ls (e
.g. t
eleH
ealth
ICT)
This
activ
ity n
eeds
to id
entif
y th
e pr
iorit
y he
alth
-‐car
e pr
ovid
er se
gmen
ts a
nd c
omm
uniti
es
that
requ
ire in
vest
men
t in
fit fo
r pu
rpos
e
data
con
nect
ivity
In o
rder
to a
id e
ffici
ency
and
opt
imize
lim
ited
fund
s, h
ealth
car
e fa
cilit
ies
with
the
high
est r
each
in
com
mun
ities
shou
ld b
e id
entif
ied
and
enha
nced
, tec
hnol
ogy-‐
wise
FMO
H, F
MCT
(eGo
vt),
Gala
xy
Back
bone
(GBB
), LG
A an
d co
mm
unity
lead
ers,
Mob
ile
Telc
oms,
NCC
, NGO
s, U
SPF
D.Se
lect
impl
emen
tatio
n pa
rtne
rs to
deve
lop
data
con
nect
ivity
in
fras
truc
ture
The
coun
try
will
nee
d to
sele
ct d
ata
conn
ectiv
ity in
fras
truc
ture
pro
vide
rs
and
oper
ator
s to
assis
t in
deve
lopi
ng
the
requ
ired
data
con
nect
ivity
in
fras
truc
ture
Thes
e co
uld
be p
rivat
e an
d/or
pub
lic
orga
niza
tions
FMCT
, NCC
, USP
F, M
obile
Tel
com
s,
GBB,
NGO
s

50!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
E. D
evel
op d
ata
conn
ectiv
ity
impl
emen
tatio
n de
sign
and
plan
Inve
stin
g in
dat
a co
nnec
tivity
in
fras
truc
ture
will
be
guid
ed a
hig
h-‐le
vel d
esig
n fo
r how
impr
ovin
g or
pr
ovid
ing
data
con
nect
ivity
to p
riorit
y ca
re p
rovi
ders
and
com
mun
ities
can
be
ach
ieve
d, a
nd h
ow th
is w
ill b
e ex
tend
ed to
the
broa
der h
ealth
se
ctor
and
pop
ulat
ion
Whi
le so
me
gove
rnm
ent a
genc
ies
have
alre
ady
begu
n se
vera
l in
itiat
ives
, the
re st
ill re
mai
ns a
pla
n to
effe
ctiv
ely
link
them
to H
ealth
ICT
FMCT
, NCC
, GBB
F.De
ploy
dat
a co
nnec
tivity
in
fras
truc
ture
for u
nder
serv
ed a
reas
Depl
oym
ent w
ould
exp
lore
wire
d,
fixed
wire
less
and
mob
ile
conn
ectiv
ity in
fras
truc
ture
Som
e go
vern
men
t age
ncie
s hav
e al
read
y be
gun
wor
k on
put
ting
IT
infr
astr
uctu
re in
pla
ce. T
hese
can
be
leve
rage
d fo
r Hea
lth IC
T pu
rpos
es
FMO
H, S
MO
H, U
SDF,
FM
CT, N
CC,
GBB,
Tel
ecom
s
.2 Id
entif
y an
d as
sess
exi
stin
g in
fras
truc
ture
Ex
istin
g In
fras
truc
ture
for H
ealth
ICT
iden
tifie
d an
d as
sess
ed
Exist
ing
infr
astr
uctu
re c
an b
e le
vera
ged
to su
ppor
t Hea
lth IC
T in
itiat
ives
alte
rnat
ive
sour
ces o
f po
wer
cou
ld a
lso b
e ex
plor
ed
NIP
OST
kio
sks a
re a
n ex
ampl
e of
an
orga
niza
tion
infr
astr
uctu
re O
ther
s ar
e Po
wer
, Con
nect
ivity
and
Eq
uipm
ent
Iden
tify
and
asse
ss o
ngoi
ng
infr
astr
uctu
ral p
roje
cts i
n un
ders
erve
d ar
eas
This
activ
ity w
ill e
xplo
re th
e po
ssib
ility
of l
ever
agin
g He
alth
ICT
initi
ativ
es o
n ex
istin
g in
fras
truc
ture
su
ch a
s RIT
Cs, c
omm
unity
co
nnec
tivity
pro
ject
s and
com
mun
ity
base
d po
wer
(sol
ar/ w
ind
etc.
) in
itiat
ives
FMO
H, F
MCT
(eGo
vt),
USP
F, G
BB,
com
mun
ity le
ader
s, p
rivat
e or
gani
zatio
ns (e
spec
ially
tele
com
s)
Alte
rnat
ive
pow
er c
ompa
nies
(sol
ar
gene
ratio
n, h
ydro
, win
d fa
rms,
in
vert
ers,
etc
.)
.3 D
efin
e M
inim
um In
fras
truc
tura
l Re
quire
men
ts
Min
imum
infr
astr
uctu
ral r
equi
rem
ents
fo
r e-‐h
ealth
impl
emen
tatio
n de
fined
By th
inki
ng th
roug
h an
d ag
reei
ng
upon
wha
t diff
eren
t hea
lth fa
cilit
ies
at a
ll le
vels
will
nee
d, th
e FM
OH
can
defin
e th
e ba
sic/ m
inim
um
requ
irem
ents
for H
ealth
ICT
adop
tion.
Onc
e th
ese
requ
irem
ents
are
de
fined
, hea
lth fa
cilit
ies w
ill si
mpl
y no
t ini
tiate
Hea
lth IC
T im
plem
enta
tions
with
out m
eetin
g th
ese
requ
irem
ents
.
This
will
giv
e th
e ge
nera
l pub
lic
som
e co
mfo
rt th
at th
e he
alth
care
fa
cilit
ies t
hey
atte
nd h
as m
et
cert
ain
Heal
th IC
T st
anda
rds/
co
nditi
ons/
requ
irem
ents
.
Defin
e m
inim
um c
ompu
ting,
pow
er
and
conn
ectiv
ity In
fras
truc
ture
re
quire
men
ts fo
r e-‐h
ealth
im
plem
enta
tion
Thes
e ar
e th
e m
inim
um
infr
astr
uctu
ral r
equi
rem
ents
for
heal
th fa
cilit
ies t
o op
timal
ly d
eplo
y an
d im
plem
ent H
ealth
ICT
initi
ativ
es
FMO
H, F
MCT
(eGo
vt),
GBB,
USP
F,
NIT
DA
Link
hea
lthca
re o
rgan
izatio
n an
d pr
ovid
er e
-‐hea
lth a
ccre
dita
tion
to
mee
ting
min
imum
com
putin
g In
fras
truc
ture
One
pot
entia
l met
hod
to d
rive
inve
stm
ents
in H
ealth
ICT
is to
link
th
eir H
ealth
ICT
accr
edita
tion
to th
eir
mee
ting
of d
efin
ed in
fras
truc
tura
l re
quire
men
ts
Alth
ough
it is
typi
cally
a lo
ng-‐t
erm
as
pira
tion,
such
an
activ
ity c
an b
e us
ed to
enc
oura
ge in
itial
inve
stm
ent
in H
ealth
ICT
rela
ted
infr
astr
uctu
re.
Onc
e st
anda
rds h
ave
been
es
tabl
ished
, it b
ecom
es e
asie
r to
mon
itor a
nd e
nfor
ce, a
nd re
war
d co
mpl
ianc
e ac
ross
org
aniza
tions
FMO
H, S
MO
H, N
ITDA
, NHI
S
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
.0
Solutio
ns (Services a
nd
Applications)
.1 P
riorit
ize S
ervi
ces a
nd
Appl
icat
ions
Core
set o
f app
ropr
iate
Hea
lth IC
T se
rvic
es a
nd A
pplic
atio
ns p
riorit
ized
and
depl
oyed
Iden
tify
and
prio
ritize
serv
ices
and
ap
plic
atio
ns th
at h
ave
scal
ed, o
r are
sc
alab
le
A. Id
entif
y se
rvic
es a
nd/o
r ap
plic
atio
ns fo
r prio
ritiza
tion
This
wou
ld in
clud
e id
entif
ying
: -‐ E
xist
ing
scal
able
serv
ices
and
ap
plic
atio
ns
-‐ Nec
essa
ry se
rvic
es a
nd a
pplic
atio
ns
for p
riorit
izatio
n -‐S
ervi
ces a
nd a
pplic
atio
n th
at h
ave
evid
ence
for h
igh
impa
ct
-‐Sol
utio
ns w
ith p
oten
tial f
or e
ase
of
scal
e an
d ar
e co
st e
ffect
ive
-‐Rel
iabl
e so
lutio
ns
FMO
H, N
OTA
P, N
ITDA
, im
plem
entin
g pa
rtne
rs in
priv
ate
sect
or
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers
infr
astr
uctu
re d
evel
opm
ent,
entr
epre
neur
s and
dev
elop
ers,
in
clud
ing
prov
idin
g en
ablin
g en
viro
nmen
t for
pot
entia
l exp
ort
and
reve
nues
from
Hea
lth IC
T
Deve
lopm
ent p
artn
ers a
nd th
e pr
ivat
e se
ctor
2.3
Inve
stm
ent
Inve
stm
ent m
anag
emen
t pla
n es
tabl
ished
Inve
stm
ent m
anag
emen
t to
enab
le
prop
er a
lloca
tion
of H
ealth
ICT
inve
stm
ent f
undi
ng to
prio
rity
proj
ects
A.In
vest
men
t man
agem
ent
stru
ctur
e
Intr
oduc
e a
stru
ctur
e fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets
to im
prov
e pr
iorit
izatio
n, a
lloca
tion
and
rele
ase
FMO
H, F
MCT
and
TW
G m
ajor
fu
nder
s d
evel
opm
ent p
artn
ers a
nd
priv
ate
sect
or
B.Fu
nd c
oord
inat
ion
mec
hani
sm
Esta
blish
fund
coo
rdin
atio
n m
echa
nism
s to
miti
gate
risk
s fro
m
frag
men
ted
fund
ing
stru
ctur
e
FMO
H an
d TW
G, m
ajor
fund
ers,
pr
ivat
e se
ctor
and
dev
elop
men
t pa
rtne
rs
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
3.1
Esta
blish
ed S
tand
ards
St
anda
rds f
or H
ealth
ICT
and
heal
th
info
rmat
ion
exch
ange
def
ined
and
es
tabl
ished
Defin
e an
d pr
iorit
ize H
ealth
ICT
and
rela
ted
data
stan
dard
s, a
s wel
l as
esta
blish
pro
cess
es a
nd
infr
astr
uctu
re to
faci
litat
e sa
fe a
nd
secu
re e
xcha
nge
of h
ealth
in
form
atio
n
A. R
evie
w e
xist
ing
natio
nal a
nd
inte
rnat
iona
l sta
ndar
ds a
nd D
efin
e He
alth
ICT
stan
dard
s
Proc
ess f
or d
evel
opin
g, re
view
ing,
ap
prov
ing
and
publ
ishin
g na
tiona
l He
alth
ICT
stan
dard
s, a
nd w
hich
is
supp
orte
d by
the
heal
th se
ctor
and
th
e He
alth
ICT
indu
stry
will
nee
d to
be
est
ablis
hed
Re
view
exi
stin
g na
tiona
l and
in
tern
atio
nal H
ealth
ICT
and
othe
r st
anda
rds t
o de
term
ine
wha
t can
be
adop
ted
FMO
H, N
ITDA
, FM
CT, T
WG
.0
Standards a
nd Interopera
ility
B. E
stab
lish
a N
iger
ian
Heal
thIn
form
atio
n Ex
chan
ge (H
IE)
A HI
E sy
stem
will
faci
litat
e th
e ex
chan
ge o
f hea
lth in
form
atio
n am
ong
stak
ehol
ders
acr
oss
geog
raph
ical
and
hea
lth-‐s
ecto
r bo
unda
ries b
ased
on
defin
ed
stan
dard
s
FMO
H, F
MCT
, NHI
S, U
SPF,
NIM
C,
NIT
DA, G
alax
y Ba
ckbo
ne, N
BS
3.2
Stan
dard
s cap
acity
bui
ldin
g Ca
paci
ty b
uilt
for e
nsur
ing
stan
dard
s an
d in
tero
pera
bilit
y
Capa
city
of s
take
hold
ers b
uilt
as
appr
opria
te, t
o un
ders
tand
, def
ine,
re
view
, app
ly a
nd m
anag
e st
anda
rds
in H
ealth
ICT
initi
ativ
es
A.Pa
rtne
rs p
rovi
de tr
aini
ng a
ndca
paci
ty b
uild
ing
in H
ealth
ICT
Trai
ning
and
Cap
acity
Bui
ldin
g pr
ovid
ed b
y co
mpe
tent
par
tner
s
FMO
H, N
ITDA
, FM
CT
B. R
egul
ar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
and
ensu
re it
s app
licat
ion
Regu
lar m
ento
ring
and
on th
e jo
b tr
aini
ng to
sust
ain
know
ledg
e ga
ined
an
d en
sure
its a
pplic
atio
n
3.3
Data
Col
lect
ion
and
Regi
strie
s St
anda
rdize
d re
gist
ries,
inst
rum
ents
(d
ata
colle
ctio
n fo
rms,
repo
rts e
tc.)
and
indi
cato
rs
Build
ing
on e
xist
ing
stan
dard
s and
re
quire
men
ts fo
r som
e fo
unda
tiona
l He
alth
ICT
serv
ices
A. D
evel
op, a
dapt
or a
dopt
hig
h-‐le
vel r
equi
rem
ents
and
des
ign
for
foun
datio
nal H
ealth
ICT
serv
ices
Impl
emen
tatio
n of
foun
datio
n He
alth
ICT
serv
ices
(e.g
., na
tiona
l he
alth
iden
tifie
rs, n
atio
nal
auth
entic
atio
n, e
lect
roni
c he
alth
re
cord
s, e
tc.),
beg
ins w
ith
unde
rsta
ndin
g th
e hi
gh-‐le
vel
requ
irem
ents
for t
he se
rvic
e an
d de
finin
g a
high
-‐leve
l des
ign
for h
ow
the
serv
ice
wou
ld b
e de
liver
ed fo
r th
e co
untr
y
FMO
H, F
MCT
, NIM
C, N
ITDA
, NHI
S,
NPC
, TW
G, P
rofe
ssio
nal a
nd
regu
lato
ry o
rgan
izatio
ns e
.g. M
DCN
, N
MCN
FM
OH,
NIM
C, N
ITDA
, NHI
S,
NPC
, im
plem
ente
rs, e
nd-‐u
sers
Build
on
exist
ing
inst
rum
ents
to
supp
ort k
ey re
gist
ries (
heal
th
faci
lity,
pat
ient
, hea
lth w
orke
rs,
citiz
en e
tc.)
foun
datio
nal t
o he
alth
in
form
atio
n ex
chan
ge
B. D
evel
op a
nd a
ppro
ve st
anda
rds
for s
ecur
e m
essa
ging
, hig
h-‐pr
iorit
y he
alth
info
rmat
ion,
term
inol
ogie
s an
d da
ta d
ictio
narie
s
Ensu
res t
hat h
ealth
info
rmat
ion
exch
ange
d be
twee
n he
alth
care
or
gani
zatio
ns a
nd p
rovi
ders
thro
ugh
a na
tiona
l Hea
lth IC
T en
viro
nmen
t ar
e ap
prop
riate
ly d
efin
ed a
nd th
e m
essa
ges u
tilize
stan
dard
te
rmin
olog
ies a
nd re
mai
n pr
ivat
e an
d co
nfid
entia
l.
All m
ust b
e pr
oper
ly a
uthe
ntic
ated
an
d de
liver
ed to
inte
nded
reci
pien
t
FMO
H, N
IMC,
NIT
DA, N
HIS,
NPC
, im
plem
ente
rs, e
nd-‐u
sers

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!51
B. D
evel
op/r
evise
hig
h le
vel
requ
irem
ents
and
des
ign
for
iden
tifie
d na
tiona
l Hea
lth IC
T se
rvic
e an
d/or
app
licat
ion
This
invo
lves
the
deve
lopm
ent o
f re
quire
men
ts fo
r prio
rity
serv
ices
and
ap
plic
atio
ns to
mee
t ide
ntifi
ed
busin
ess p
roce
ss n
eeds
of t
he
Nig
eria
n He
alth
ICT
eco-‐
spac
e
C. Id
entif
y re
sour
ces t
o su
ppor
t the
ex
pans
ion
and
deve
lopm
ent o
f id
entif
ied
serv
ices
and
app
licat
ions
This
invo
lves
iden
tifyi
ng, e
valu
atin
g an
d se
lect
ion
of re
sour
ces (
with
in
publ
ic a
nd p
rivat
e se
ctor
s) to
un
dert
ake
the
deta
iled
desig
n an
d im
plem
enta
tion
or e
xpan
sion
of
natio
nal H
ealth
ICT
serv
ices
or
appl
icat
ions
that
adh
ere
to th
e hi
gh-‐
leve
l req
uire
men
ts a
nd d
esig
n D.
Build
and
Dep
loy
iden
tifie
d pr
iorit
y na
tiona
l Hea
lth IC
T se
rvic
es a
nd/o
r ap
plic
atio
ns
This
invo
lves
wor
king
with
sele
cted
im
plem
enta
tion
part
ners
to e
xecu
te,
need
ed p
rogr
ams a
t sca
le
E.O
pera
te, s
uppo
rt a
nd su
stai
nde
velo
ped
prio
rity
Heal
th IC
T se
rvic
es
and
appl
icat
ion
F.O
ngoi
ng sc
ale-‐
up o
f prio
ritize
dse
rvic
es a
nd a
pplic
atio
n Th
is w
ill fo
cus o
n su
ppor
ting
iden
tifie
d pr
iorit
y se
rvic
es a
nd
appl
icat
ion.
(e.g
., DH
IS2)
G. F
oste
r con
tinuo
us u
pgra
des o
f im
plem
ente
d hi
gh p
riorit
y He
alth
ICT
solu
tions
Tech
nolo
gy is
dyn
amic
, the
refo
re
syst
em re
view
s and
upd
ates
are
m
anda
tory
for l
ong-‐
term
im
plem
enta
tions
H.
Prom
ote
rese
arch
and
deve
lopm
ent o
f prio
rity
Heal
th IC
T so
lutio
ns
.2 S
hare
Bes
t Pra
ctic
es
Best
pra
ctic
es in
dev
elop
men
t and
use
of
Hea
lth IC
T do
cum
ente
d an
d di
ssem
inat
ed
Asse
ss a
nd d
ocum
ent H
ealth
ICT
serv
ices
and
app
licat
ions
in th
e re
posit
ory
(cha
nge
and
adop
tion)
.
Iden
tify
best
pra
ctic
es in
Hea
lth IC
T an
d di
ssem
inat
e w
idel
y A
dyna
mic
por
tal f
or te
xt, d
ocum
ents
an
d au
diov
isual
s res
ourc
e m
ater
ials
FMO
H, N
ITDA
, im
plem
entin
g pa
rtne
rs in
priv
ate
sect
or, M
DCN
, N
UC,
var
ious
med
ical
bod
ies
E. D
evel
op d
ata
conn
ectiv
ity
impl
emen
tatio
n de
sign
and
plan
Inve
stin
g in
dat
a co
nnec
tivity
in
fras
truc
ture
will
be
guid
ed a
hig
h-‐le
vel d
esig
n fo
r how
impr
ovin
g or
pr
ovid
ing
data
con
nect
ivity
to p
riorit
y ca
re p
rovi
ders
and
com
mun
ities
can
be
ach
ieve
d, a
nd h
ow th
is w
ill b
e ex
tend
ed to
the
broa
der h
ealth
se
ctor
and
pop
ulat
ion
Whi
le so
me
gove
rnm
ent a
genc
ies
have
alre
ady
begu
n se
vera
l in
itiat
ives
, the
re st
ill re
mai
ns a
pla
n to
effe
ctiv
ely
link
them
to H
ealth
ICT
FMCT
, NCC
, GBB
F.De
ploy
dat
a co
nnec
tivity
in
fras
truc
ture
for u
nder
serv
ed a
reas
Depl
oym
ent w
ould
exp
lore
wire
d,
fixed
wire
less
and
mob
ile
conn
ectiv
ity in
fras
truc
ture
Som
e go
vern
men
t age
ncie
s hav
e al
read
y be
gun
wor
k on
put
ting
IT
infr
astr
uctu
re in
pla
ce. T
hese
can
be
leve
rage
d fo
r Hea
lth IC
T pu
rpos
es
FMO
H, S
MO
H, U
SDF,
FM
CT, N
CC,
GBB,
Tel
ecom
s
.2 Id
entif
y an
d as
sess
exi
stin
g in
fras
truc
ture
Ex
istin
g In
fras
truc
ture
for H
ealth
ICT
iden
tifie
d an
d as
sess
ed
Exist
ing
infr
astr
uctu
re c
an b
e le
vera
ged
to su
ppor
t Hea
lth IC
T in
itiat
ives
alte
rnat
ive
sour
ces o
f po
wer
cou
ld a
lso b
e ex
plor
ed
NIP
OST
kio
sks a
re a
n ex
ampl
e of
an
orga
niza
tion
infr
astr
uctu
re O
ther
s ar
e Po
wer
, Con
nect
ivity
and
Eq
uipm
ent
Iden
tify
and
asse
ss o
ngoi
ng
infr
astr
uctu
ral p
roje
cts i
n un
ders
erve
d ar
eas
This
activ
ity w
ill e
xplo
re th
e po
ssib
ility
of l
ever
agin
g He
alth
ICT
initi
ativ
es o
n ex
istin
g in
fras
truc
ture
su
ch a
s RIT
Cs, c
omm
unity
co
nnec
tivity
pro
ject
s and
com
mun
ity
base
d po
wer
(sol
ar/ w
ind
etc.
) in
itiat
ives
FMO
H, F
MCT
(eGo
vt),
USP
F, G
BB,
com
mun
ity le
ader
s, p
rivat
e or
gani
zatio
ns (e
spec
ially
tele
com
s)
Alte
rnat
ive
pow
er c
ompa
nies
(sol
ar
gene
ratio
n, h
ydro
, win
d fa
rms,
in
vert
ers,
etc
.)
.3 D
efin
e M
inim
um In
fras
truc
tura
l Re
quire
men
ts
Min
imum
infr
astr
uctu
ral r
equi
rem
ents
fo
r e-‐h
ealth
impl
emen
tatio
n de
fined
By th
inki
ng th
roug
h an
d ag
reei
ng
upon
wha
t diff
eren
t hea
lth fa
cilit
ies
at a
ll le
vels
will
nee
d, th
e FM
OH
can
defin
e th
e ba
sic/ m
inim
um
requ
irem
ents
for H
ealth
ICT
adop
tion.
Onc
e th
ese
requ
irem
ents
are
de
fined
, hea
lth fa
cilit
ies w
ill si
mpl
y no
t ini
tiate
Hea
lth IC
T im
plem
enta
tions
with
out m
eetin
g th
ese
requ
irem
ents
.
This
will
giv
e th
e ge
nera
l pub
lic
som
e co
mfo
rt th
at th
e he
alth
care
fa
cilit
ies t
hey
atte
nd h
as m
et
cert
ain
Heal
th IC
T st
anda
rds/
co
nditi
ons/
requ
irem
ents
.
Defin
e m
inim
um c
ompu
ting,
pow
er
and
conn
ectiv
ity In
fras
truc
ture
re
quire
men
ts fo
r e-‐h
ealth
im
plem
enta
tion
Thes
e ar
e th
e m
inim
um
infr
astr
uctu
ral r
equi
rem
ents
for
heal
th fa
cilit
ies t
o op
timal
ly d
eplo
y an
d im
plem
ent H
ealth
ICT
initi
ativ
es
FMO
H, F
MCT
(eGo
vt),
GBB,
USP
F,
NIT
DA
Link
hea
lthca
re o
rgan
izatio
n an
d pr
ovid
er e
-‐hea
lth a
ccre
dita
tion
to
mee
ting
min
imum
com
putin
g In
fras
truc
ture
One
pot
entia
l met
hod
to d
rive
inve
stm
ents
in H
ealth
ICT
is to
link
th
eir H
ealth
ICT
accr
edita
tion
to th
eir
mee
ting
of d
efin
ed in
fras
truc
tura
l re
quire
men
ts
Alth
ough
it is
typi
cally
a lo
ng-‐t
erm
as
pira
tion,
such
an
activ
ity c
an b
e us
ed to
enc
oura
ge in
itial
inve
stm
ent
in H
ealth
ICT
rela
ted
infr
astr
uctu
re.
Onc
e st
anda
rds h
ave
been
es
tabl
ished
, it b
ecom
es e
asie
r to
mon
itor a
nd e
nfor
ce, a
nd re
war
d co
mpl
ianc
e ac
ross
org
aniza
tions
FMO
H, S
MO
H, N
ITDA
, NHI
S
Compo
nent
Outpu
t Title
Outpu
t (Re
commendatio
n)Outpu
t Descriptio
nActiv
ityActiv
ity Descriptio
nStakeholders
.0
Solutio
ns (Services a
nd
Applications)
.1 P
riorit
ize S
ervi
ces a
nd
Appl
icat
ions
Core
set o
f app
ropr
iate
Hea
lth IC
T se
rvic
es a
nd A
pplic
atio
ns p
riorit
ized
and
depl
oyed
Iden
tify
and
prio
ritize
serv
ices
and
ap
plic
atio
ns th
at h
ave
scal
ed, o
r are
sc
alab
le
A. Id
entif
y se
rvic
es a
nd/o
r ap
plic
atio
ns fo
r prio
ritiza
tion
This
wou
ld in
clud
e id
entif
ying
: -‐ E
xist
ing
scal
able
serv
ices
and
ap
plic
atio
ns
-‐ Nec
essa
ry se
rvic
es a
nd a
pplic
atio
ns
for p
riorit
izatio
n -‐S
ervi
ces a
nd a
pplic
atio
n th
at h
ave
evid
ence
for h
igh
impa
ct
-‐Sol
utio
ns w
ith p
oten
tial f
or e
ase
of
scal
e an
d ar
e co
st e
ffect
ive
-‐Rel
iabl
e so
lutio
ns
FMO
H, N
OTA
P, N
ITDA
, im
plem
entin
g pa
rtne
rs in
priv
ate
sect
or

52!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Append
ix : H
ealth
ICT
rame
ork
Health ICT
nalers
Interm
ediate
Outcome
Proximal
OutcomeOutpu
t
Indicator
Indicator D
einition
Da
ta
Sources
Data
Collection
etho
d
reuency
o Data
Respon
siility
Scop
e 2015
ase
line
2020
Targ et
umerator
Deno
minator
Enab
ling
and
sust
aina
ble
envi
ronm
ent f
or
impl
emen
tatio
n an
d sc
ale -‐
up o
f He
alth
ICT
in
Nig
eria
1.0 stalished
sustaina
le governance
structure
Num
ber (
No.
) of H
ealth
ICT
initi
ativ
es le
d by
key
st
akeh
olde
rs in
gov
ernm
ent -‐
N
atio
nal a
nd S
tate
Tec
hnic
al
Wor
king
Gro
ups (
TWG
s)
N/A
TB
D TB
D
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
es
/No
(/N
)
N/A
PM
O
Repo
rts o
f m
eetin
gs
Bi-‐A
nnua
l TW
Gs -‐
N
atio
nal
and
Stat
e,
FMO
H
Nat
ion
al,
Stat
e
TBD
TBD
1.1 ational H
ealth
ICT governance
structure esta
lished
Nat
iona
l Hea
lth IC
T St
eerin
g Co
mm
ittee
(/N
) N
/A
PMO
FM
OH,
PM
O
Nat
ion
al
TBD
TBD
Nat
iona
l Hea
lth IC
T TW
G/c
omm
ittee
(/N
) N
/A
PMO
TB
D TB
D
Nat
iona
l Hea
lth IC
T pr
ojec
t m
anag
emen
t offi
ce (P
MO
) (
/N)
N/A
PM
O
TBD
TBD
Perc
enta
ge (
) of
mee
tings
he
ld b
y th
e N
atio
nal T
WG
in
a ye
ar (w
ith o
utpu
ts a
nd
reso
lutio
ns)
No.
of m
eetin
gs h
eld
with
in th
e re
port
ing
perio
d
No.
of p
lann
ed
mee
ting
for w
ithin
re
port
ing
perio
d
PMO
TB
D TB
D
1.2 State
Governm
ent
engaged
Stat
e He
alth
ICT
TWG
s es
tabl
ished
(/N
) N
/A
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
TBD
TBD
of s
tate
s in
Nig
eria
with
fu
nctio
nal s
tate
leve
l TW
Gs
(func
tiona
l -‐de
fined
a
mee
ting
per q
uart
er)
No.
of s
tate
s with
fu
nctio
nal T
WG
s 3
Sta
tes o
f Nig
eria
St
ate
PMO
St
ate
TBD
TBD
of s
tate
s in
Nig
eria
with
st
ate
stra
tegy
, pla
n an
d bu
dget
No.
of s
tate
s with
st
ate
stra
tegi
es,
plan
s and
bud
gets
3 S
tate
s of N
iger
ia
Stat
e PM
O
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
Stat
e TB
D TB
D
1.road
stakeholder
engagement
achieved
of i
dent
ified
key
st
akeh
olde
r gro
ups e
ngag
ed
No.
of s
take
hold
er
grou
ps re
pres
ente
d at
mee
tings
Iden
tifie
d st
akeh
olde
r gr
oups
N
atio
nal/S
tat
e PM
O
uart
erly
PM
O
Nat
ion
al/S
tat
e
TBD
TBD
1. ational H
ealth
ICT
rame
ork
integrated and
linked
ith ational
Health Act and
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in th
e pr
eced
ing
year
with
su
bsec
tions
for H
ealth
ICT
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
with
subs
ectio
ns fo
r
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
Polic
y do
cum
ents
re
leas
ed/r
evi
ewed
Polic
y do
cum
ent
revi
ew
early
PM
O
Nat
ion
al
TBD
TBD
AP
PE
ND
IX 6
: H
EA
LTH
IC
T M
&E
FR
AM
EW
OR
K

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!53
Append
ix : H
ealth
ICT
rame
ork
Health ICT
nalers
Interm
ediate
Outcome
Proximal
OutcomeOutpu
t
Indicator
Indicator D
einition
Da
ta
Sources
Data
Collection
etho
d
reuency
o Data
Respon
siility
Scop
e 2015
ase
line
2020
Targ et
umerator
Deno
minator
Enab
ling
and
sust
aina
ble
envi
ronm
ent f
or
impl
emen
tatio
n an
d sc
ale-‐
up o
f He
alth
ICT
in
Nig
eria
1.0 stalished
sustaina
le governance
structure
Num
ber (
No.
) of H
ealth
ICT
initi
ativ
es le
d by
key
st
akeh
olde
rs in
gov
ernm
ent -‐
N
atio
nal a
nd S
tate
Tec
hnic
al
Wor
king
Gro
ups (
TWG
s)
N/A
TB
D TB
D
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
es
/No
(/N
)
N/A
PM
O
Repo
rts o
f m
eetin
gs
Bi-‐A
nnua
l TW
Gs -‐
N
atio
nal
and
Stat
e,
FMO
H
Nat
ion
al,
Stat
e
TBD
TBD
1.1 ational H
ealth
ICT governance
structure esta
lished
Nat
iona
l Hea
lth IC
T St
eerin
g Co
mm
ittee
(/N
) N
/A
PMO
FM
OH,
PM
O
Nat
ion
al
TBD
TBD
Nat
iona
l Hea
lth IC
T TW
G/c
omm
ittee
(/N
) N
/A
PMO
TB
D TB
D
Nat
iona
l Hea
lth IC
T pr
ojec
t m
anag
emen
t offi
ce (P
MO
) (
/N)
N/A
PM
O
TBD
TBD
Perc
enta
ge (
) of
mee
tings
he
ld b
y th
e N
atio
nal T
WG
in
a ye
ar (w
ith o
utpu
ts a
nd
reso
lutio
ns)
No.
of m
eetin
gs h
eld
with
in th
e re
port
ing
perio
d
No.
of p
lann
ed
mee
ting
for w
ithin
re
port
ing
perio
d
PMO
TB
D TB
D
1.2 State
Governm
ent
engaged
Stat
e He
alth
ICT
TWG
s es
tabl
ished
(/N
) N
/A
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
TBD
TBD
of s
tate
s in
Nig
eria
with
fu
nctio
nal s
tate
leve
l TW
Gs
(func
tiona
l -‐de
fined
a
mee
ting
per q
uart
er)
No.
of s
tate
s with
fu
nctio
nal T
WG
s 3
Sta
tes o
f Nig
eria
St
ate
PMO
St
ate
TBD
TBD
of s
tate
s in
Nig
eria
with
st
ate
stra
tegy
, pla
n an
d bu
dget
No.
of s
tate
s with
st
ate
stra
tegi
es,
plan
s and
bud
gets
3 S
tate
s of N
iger
ia
Stat
e PM
O
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
Stat
e TB
D TB
D
1.road
stakeholder
engagement
achieved
of i
dent
ified
key
st
akeh
olde
r gro
ups e
ngag
ed
No.
of s
take
hold
er
grou
ps re
pres
ente
d at
mee
tings
Iden
tifie
d st
akeh
olde
r gr
oups
N
atio
nal/S
tat
e PM
O
uart
erly
PM
O
Nat
ion
al/S
tat
e
TBD
TBD
1. ational H
ealth
ICT
rame
ork
integrated and
linked
ith ational
Health Act and
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in th
e pr
eced
ing
year
with
su
bsec
tions
for H
ealth
ICT
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
with
subs
ectio
ns fo
r
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
Polic
y do
cum
ents
re
leas
ed/r
evi
ewed
Polic
y do
cum
ent
revi
ew
early
PM
O
Nat
ion
al
TBD
TBD
SHDP
and
others
Heal
th IC
T
1.5
ational H
ealth
ICT
rame
ork
developed end
orsed
and perio
dically
revie
ed
Nat
iona
l Hea
lth IC
T fr
amew
ork
endo
rsed
(/N
) A
FMO
Hs
annu
al
repo
rt
Repo
rt o
f re
view
O
ne-‐o
ff FM
OH
DPRS
N
atio
nal
TB
D TB
D
Nat
iona
l Hea
lth IC
T fr
amew
ork
revi
ewed
aft
er 5
ye
ars (
/N)
A PM
O
Repo
rt o
f re
view
5
year
ly
FMO
H N
atio
nal
TB
D TB
D
2.0 Increased
unding o
r He
alth ICT
Reso
urce
s com
mitt
ed to
He
alth
ICT
impl
emen
tatio
n an
d sc
ale-‐
up fr
om p
artn
ers,
do
nors
and
oth
er st
ake-‐
hold
ers (
finan
cial
and
in-‐k
ind
cont
ribut
ions
)
TBD
TBD
2.1 un
ding o
r He
alth ICT
operations se
cured
Tota
l NG
N se
cure
d N
/A
Budg
et
docu
men
t TB
D FM
OH
TBD
TBD
Hea
lth IC
T bu
dget
secu
red
Amou
nt se
cure
d fo
r He
alth
ICT
Annu
al H
ealth
ICT
budg
et
TBD
FMO
H TB
D TB
D
Tota
l am
ount
of s
eed
fund
di
sbur
sed
to H
ealth
ICT
initi
ativ
es
Amou
nt d
isbur
sed
for H
ealth
ICT
Amou
nt o
f see
d fu
nd
allo
cate
d fo
r Hea
lth
ICT
Audi
t re
port
Au
dit r
epor
t TB
D FM
OH
Nat
ion
al
TBD
TBD
of s
tatu
tory
hea
lth b
udge
t al
loca
ted
for H
ealth
ICT
Stat
utor
y he
alth
bu
dget
allo
cate
d fo
r He
alth
ICT
Stat
utor
y he
alth
bu
dget
Fu
nd ra
ised
TBD
FMO
H N
atio
nal
TB
D TB
D
of s
tatu
tory
hea
lth b
udge
t re
leas
ed fo
r Hea
lth IC
T St
atut
ory
heal
th
budg
et re
leas
ed fo
r He
alth
ICT
Stat
utor
y he
alth
bu
dget
Se
ed fu
nds
repo
rts
Seed
fund
s re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
2.2 Incentives
mechanism
esta
lished
No
of in
cent
ive
prog
ram
s/st
ruct
ures
and
m
echa
nism
est
ablis
hed
N/A
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
No
of
com
pani
es/o
rgan
izatio
ns
utili
zing
ince
ntiv
e m
echa
nism
s/sc
hem
e
N/A
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
2.Investment
managem
ent p
lan
esta
lished
Fram
ewor
k fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets d
evel
oped
(/N
)
N/A
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
Nat
iona
l fun
d co
ordi
natin
g m
echa
nism
est
ablis
hed
(/N
) N
/A
TWG
/PM
O
repo
rts
TWG
/PM
O
repo
rts
TBD
FMO
H N
atio
nal
TB
D TB
D
of s
tate
s with
est
ablis
hed
stat
e fu
nd c
oord
inat
ing
mec
hani
sms
No. o
f sta
tes w
ith
esta
blish
ed st
ate
fund
coo
rdin
atin
g m
echa
nism
s
Tota
l no.
of s
tate
s in
Nig
eria
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
.0 Stand
ards and
Interopera
ility
No.
of I
nter
oper
able
Hea
lth
ICT
appl
icat
ions
ava
ilabl
e in
N
iger
ian
Heal
th IC
T sp
ace
N/A
TB
D TB
D TB
D
.1 Stand
ards o
r He
alth ICT and
Stan
dard
s for
Hea
lth IC
T an
d he
alth
info
rmat
ion
exch
ange
N
/A
TWG
/PM
O
repo
rts
TBD
TBD
PMO
N
atio
nal
TB
D TB
D

54!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
health in
ormation
exchange deined
and esta
lished
defin
ed (
/N)
Stan
dard
s for
Hea
lth IC
T an
d he
alth
info
rmat
ion
exch
ange
di
ssem
inat
ed (
/N)
N/A
TW
G/P
MO
re
port
s TB
D TB
D PM
O
Nat
ion
al
TBD
TBD
of d
efin
ed H
ealth
ICT
and
HIE
diss
emin
ated
To
tal d
issem
inat
ed
Tota
l no.
of d
efin
ed
Heal
th IC
T st
anda
rds
and
HIE
TWG
/PM
O
repo
rts
TBD
TBD
PMO
N
atio
nal
TB
D TB
D
.2 Capacity
uilt
or ensuring
standards a
nd
interopera
ility
of i
ndiv
idua
ls tr
aine
d to
pr
ovid
e su
ppor
t for
Hea
lth
ICT
stan
dard
izatio
n an
d in
tero
pera
bilit
y to
oth
er k
ey
stak
ehol
ders
No.
of i
ndiv
idua
ls tr
aine
d to
pro
vide
su
ppor
t for
Hea
lth
ICT
stan
dard
izatio
n an
d in
tero
pera
bilit
y to
oth
er k
ey
stak
ehol
ders
Tota
l No.
of t
arge
ted
indi
vidu
als t
o be
tr
aine
d
TWG
/PM
O
repo
rts
Trai
ning
re
gist
ers
Re
gist
ered
ta
rget
s
uart
erly
PM
O
Nat
ion
al,
Stat
e
TBD
TBD
of o
rgan
izatio
ns tr
aine
d to
pr
ovid
e su
ppor
t for
Hea
lth
ICT
stan
dard
izatio
n an
d in
tero
pera
bilit
y to
oth
er k
ey
stak
ehol
ders
No.
of o
rgan
izatio
ns
trai
ned
to p
rovi
de
supp
ort f
or H
ealth
IC
T st
anda
rdiza
tion
and
inte
rope
rabi
lity
to o
ther
key
st
akeh
olde
rs
Tota
l no.
of t
arge
ted
orga
niza
tions
to b
e tr
aine
d
TWG
/PM
O
repo
rts
Trai
ning
re
gist
ers
Re
gist
ered
ta
rget
s
uart
erly
PM
O
Nat
ion
al,
Stat
e
TBD
TBD
.Re
gistrie
s
instruments (d
ata
collection
orms
repo
rts e
tc.) and
indicators
standardied
of r
egist
ries,
inst
rum
ents
an
d in
dica
tors
stan
dard
ized
in li
ne w
ith th
e ag
reed
Hea
lth
ICT
fram
ewor
k
No.
of r
egist
ries,
in
stru
men
ts a
nd
indi
cato
rs
stan
dard
ized
in li
ne
with
the
appr
oved
He
alth
ICT
fram
ewor
k
Tota
l no.
of r
egist
ries,
in
stru
men
ts a
nd
indi
cato
rs in
use
by
heal
th p
rogr
ams l
ine
with
the
appr
oved
He
alth
ICT
fram
ewor
k
TWG
/PM
O
repo
rts
Regi
strie
s of
inst
rum
ents
an
d st
anda
rdize
d in
stru
men
ts
Bi-‐A
nnua
l FM
OH/
PM
O
Nat
ion
al
TBD
TBD
. Health
ICT
Standards
advocated
or
Heal
th IC
T St
anda
rds
advo
cate
d fo
r (/N
) N
/A
TWG
/PM
O
repo
rts
Mon
thly
Re
port
s M
onth
ly
FMO
H N
atio
nal
, St
ate
TBD
TBD
.0 Legislatio
n Policy and
Compliance
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
(/N
) N
/A
TWG
/PM
O
repo
rts
TBD
TBD
.1 Legislatio
n
policy and
compliance
supp
orted
y
ational H
ealth
ICT
PO
Legi
slatio
n, p
olic
y an
d co
mpl
ianc
e su
ppor
ted
by
Nat
iona
l Hea
lth IC
T PM
O
(/N
)
N/A
TW
G/P
MO
re
port
s Pe
riodi
c Re
view
Bi
-‐Ann
ual
PMO
N
atio
nal
, St
ate
TBD
TBD
5.0 Change and Ad
optio
n (Capacity
uilding)
1.
of c
onsu
mer
s, c
are
prov
ider
s and
hea
lth-‐c
are
man
ager
s usin
g He
alth
ICT
solu
tions
/inno
vatio
ns
2.
of c
onsu
mer
s, c
are
prov
ider
and
hea
lth-‐c
are
man
ager
s sa
tisfie
d w
ith
usin
g He
alth
ICT
solu
tions
/inno
vatio
ns
1. N
o. o
f con
sum
ers,
care
pro
vide
rs a
nd
heal
th-‐c
are
man
ager
s usin
g He
alth
ICT
solu
tions
/inno
vatio
ns
2. N
o. o
f con
sum
ers,
ca
re p
rovi
der a
nd
heal
th-‐c
are
man
ager
s sa
tisfie
d w
ith u
sing
Heal
th IC
T
1. N
o. o
f con
sum
ers,
care
pro
vide
rs a
nd
heal
th-‐c
are
man
ager
s re
ache
d w
ith H
ealth
IC
T so
lutio
n/in
nova
tion
inte
rven
tions
2. N
o. o
f con
sum
ers,
care
pro
vide
rs a
nd
heal
th-‐c
are
man
ager
s re
ache
d w
ith H
ealth
IC
T
TBD
TBD
SHDP
and
others
Heal
th IC
T
1.5
ational H
ealth
ICT
rame
ork
developed end
orsed
and perio
dically
revie
ed
Nat
iona
l Hea
lth IC
T fr
amew
ork
endo
rsed
(/N
) A
FMO
Hs
annu
al
repo
rt
Repo
rt o
f re
view
O
ne-‐o
ff FM
OH
DPRS
N
atio
nal
TB
D TB
D
Nat
iona
l Hea
lth IC
T fr
amew
ork
revi
ewed
aft
er 5
ye
ars (
/N)
A PM
O
Repo
rt o
f re
view
5
year
ly
FMO
H N
atio
nal
TB
D TB
D
2.0 Increased
unding o
r He
alth ICT
Reso
urce
s com
mitt
ed to
He
alth
ICT
impl
emen
tatio
n an
d sc
ale-‐
up fr
om p
artn
ers,
do
nors
and
oth
er st
ake-‐
hold
ers (
finan
cial
and
in-‐k
ind
cont
ribut
ions
)
TBD
TBD
2.1 un
ding o
r He
alth ICT
operations se
cured
Tota
l NG
N se
cure
d N
/A
Budg
et
docu
men
t TB
D FM
OH
TBD
TBD
Hea
lth IC
T bu
dget
secu
red
Amou
nt se
cure
d fo
r He
alth
ICT
Annu
al H
ealth
ICT
budg
et
TBD
FMO
H TB
D TB
D
Tota
l am
ount
of s
eed
fund
di
sbur
sed
to H
ealth
ICT
initi
ativ
es
Amou
nt d
isbur
sed
for H
ealth
ICT
Amou
nt o
f see
d fu
nd
allo
cate
d fo
r Hea
lth
ICT
Audi
t re
port
Au
dit r
epor
t TB
D FM
OH
Nat
ion
al
TBD
TBD
of s
tatu
tory
hea
lth b
udge
t al
loca
ted
for H
ealth
ICT
Stat
utor
y he
alth
bu
dget
allo
cate
d fo
r He
alth
ICT
Stat
utor
y he
alth
bu
dget
Fu
nd ra
ised
TBD
FMO
H N
atio
nal
TB
D TB
D
of s
tatu
tory
hea
lth b
udge
t re
leas
ed fo
r Hea
lth IC
T St
atut
ory
heal
th
budg
et re
leas
ed fo
r He
alth
ICT
Stat
utor
y he
alth
bu
dget
Se
ed fu
nds
repo
rts
Seed
fund
s re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
2.2 Incentives
mechanism
esta
lished
No
of in
cent
ive
prog
ram
s/st
ruct
ures
and
m
echa
nism
est
ablis
hed
N/A
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
No
of
com
pani
es/o
rgan
izatio
ns
utili
zing
ince
ntiv
e m
echa
nism
s/sc
hem
e
N/A
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
2.Investment
managem
ent p
lan
esta
lished
Fram
ewor
k fo
r pla
nnin
g an
d co
ordi
natin
g He
alth
ICT
budg
ets d
evel
oped
(/N
)
N/A
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
Nat
iona
l fun
d co
ordi
natin
g m
echa
nism
est
ablis
hed
(/N
) N
/A
TWG
/PM
O
repo
rts
TWG
/PM
O
repo
rts
TBD
FMO
H N
atio
nal
TB
D TB
D
of s
tate
s with
est
ablis
hed
stat
e fu
nd c
oord
inat
ing
mec
hani
sms
No. o
f sta
tes w
ith
esta
blish
ed st
ate
fund
coo
rdin
atin
g m
echa
nism
s
Tota
l no.
of s
tate
s in
Nig
eria
TW
G/P
MO
re
port
s TW
G/P
MO
re
port
s TB
D FM
OH
Nat
ion
al
TBD
TBD
.0 Stand
ards and
Interopera
ility
No.
of I
nter
oper
able
Hea
lth
ICT
appl
icat
ions
ava
ilabl
e in
N
iger
ian
Heal
th IC
T sp
ace
N/A
TB
D TB
D TB
D
.1 Stand
ards o
r He
alth ICT and
Stan
dard
s for
Hea
lth IC
T an
d he
alth
info
rmat
ion
exch
ange
N
/A
TWG
/PM
O
repo
rts
TBD
TBD
PMO
N
atio
nal
TB
D TB
D
Append
ix : H
ealth
ICT
rame
ork
Health ICT
nalers
Interm
ediate
Outcome
Proximal
OutcomeOutpu
t
Indicator
Indicator D
einition
Da
ta
Sources
Data
Collection
etho
d
reuency
o Data
Respon
siility
Scop
e 2015
ase
line
2020
Targ et
umerator
Deno
minator
Enab
ling
and
sust
aina
ble
envi
ronm
ent f
or
impl
emen
tatio
n an
d sc
ale-‐
up o
f He
alth
ICT
in
Nig
eria
1.0 stalished
sustaina
le governance
structure
Num
ber (
No.
) of H
ealth
ICT
initi
ativ
es le
d by
key
st
akeh
olde
rs in
gov
ernm
ent -‐
N
atio
nal a
nd S
tate
Tec
hnic
al
Wor
king
Gro
ups (
TWG
s)
N/A
TB
D TB
D
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
es
/No
(/N
)
N/A
PM
O
Repo
rts o
f m
eetin
gs
Bi-‐A
nnua
l TW
Gs -‐
N
atio
nal
and
Stat
e,
FMO
H
Nat
ion
al,
Stat
e
TBD
TBD
1.1 ational H
ealth
ICT governance
structure esta
lished
Nat
iona
l Hea
lth IC
T St
eerin
g Co
mm
ittee
(/N
) N
/A
PMO
FM
OH,
PM
O
Nat
ion
al
TBD
TBD
Nat
iona
l Hea
lth IC
T TW
G/c
omm
ittee
(/N
) N
/A
PMO
TB
D TB
D
Nat
iona
l Hea
lth IC
T pr
ojec
t m
anag
emen
t offi
ce (P
MO
) (
/N)
N/A
PM
O
TBD
TBD
Perc
enta
ge (
) of
mee
tings
he
ld b
y th
e N
atio
nal T
WG
in
a ye
ar (w
ith o
utpu
ts a
nd
reso
lutio
ns)
No.
of m
eetin
gs h
eld
with
in th
e re
port
ing
perio
d
No.
of p
lann
ed
mee
ting
for w
ithin
re
port
ing
perio
d
PMO
TB
D TB
D
1.2 State
Governm
ent
engaged
Stat
e He
alth
ICT
TWG
s es
tabl
ished
(/N
) N
/A
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
TBD
TBD
of s
tate
s in
Nig
eria
with
fu
nctio
nal s
tate
leve
l TW
Gs
(func
tiona
l -‐de
fined
a
mee
ting
per q
uart
er)
No.
of s
tate
s with
fu
nctio
nal T
WG
s 3
Sta
tes o
f Nig
eria
St
ate
PMO
St
ate
TBD
TBD
of s
tate
s in
Nig
eria
with
st
ate
stra
tegy
, pla
n an
d bu
dget
No.
of s
tate
s with
st
ate
stra
tegi
es,
plan
s and
bud
gets
3 S
tate
s of N
iger
ia
Stat
e PM
O
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
Stat
e TB
D TB
D
1.road
stakeholder
engagement
achieved
of i
dent
ified
key
st
akeh
olde
r gro
ups e
ngag
ed
No.
of s
take
hold
er
grou
ps re
pres
ente
d at
mee
tings
Iden
tifie
d st
akeh
olde
r gr
oups
N
atio
nal/S
tat
e PM
O
uart
erly
PM
O
Nat
ion
al/S
tat
e
TBD
TBD
1. ational H
ealth
ICT
rame
ork
integrated and
linked
ith ational
Health Act and
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in th
e pr
eced
ing
year
with
su
bsec
tions
for H
ealth
ICT
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
with
subs
ectio
ns fo
r
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
Polic
y do
cum
ents
re
leas
ed/r
evi
ewed
Polic
y do
cum
ent
revi
ew
early
PM
O
Nat
ion
al
TBD
TBD

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!55
health in
ormation
exchange deined
and esta
lished
defin
ed (
/N)
Stan
dard
s for
Hea
lth IC
T an
d he
alth
info
rmat
ion
exch
ange
di
ssem
inat
ed (
/N)
N/A
TW
G/P
MO
re
port
s TB
D TB
D PM
O
Nat
ion
al
TBD
TBD
of d
efin
ed H
ealth
ICT
and
HIE
diss
emin
ated
To
tal d
issem
inat
ed
Tota
l no.
of d
efin
ed
Heal
th IC
T st
anda
rds
and
HIE
TWG
/PM
O
repo
rts
TBD
TBD
PMO
N
atio
nal
TB
D TB
D
.2 Capacity
uilt
or ensuring
standards a
nd
interopera
ility
of i
ndiv
idua
ls tr
aine
d to
pr
ovid
e su
ppor
t for
Hea
lth
ICT
stan
dard
izatio
n an
d in
tero
pera
bilit
y to
oth
er k
ey
stak
ehol
ders
No.
of i
ndiv
idua
ls tr
aine
d to
pro
vide
su
ppor
t for
Hea
lth
ICT
stan
dard
izatio
n an
d in
tero
pera
bilit
y to
oth
er k
ey
stak
ehol
ders
Tota
l No.
of t
arge
ted
indi
vidu
als t
o be
tr
aine
d
TWG
/PM
O
repo
rts
Trai
ning
re
gist
ers
Re
gist
ered
ta
rget
s
uart
erly
PM
O
Nat
ion
al,
Stat
e
TBD
TBD
of o
rgan
izatio
ns tr
aine
d to
pr
ovid
e su
ppor
t for
Hea
lth
ICT
stan
dard
izatio
n an
d in
tero
pera
bilit
y to
oth
er k
ey
stak
ehol
ders
No.
of o
rgan
izatio
ns
trai
ned
to p
rovi
de
supp
ort f
or H
ealth
IC
T st
anda
rdiza
tion
and
inte
rope
rabi
lity
to o
ther
key
st
akeh
olde
rs
Tota
l no.
of t
arge
ted
orga
niza
tions
to b
e tr
aine
d
TWG
/PM
O
repo
rts
Trai
ning
re
gist
ers
Re
gist
ered
ta
rget
s
uart
erly
PM
O
Nat
ion
al,
Stat
e
TBD
TBD
.Re
gistrie
s
instruments (d
ata
collection
orms
repo
rts e
tc.) and
indicators
standardied
of r
egist
ries,
inst
rum
ents
an
d in
dica
tors
stan
dard
ized
in li
ne w
ith th
e ag
reed
Hea
lth
ICT
fram
ewor
k
No.
of r
egist
ries,
in
stru
men
ts a
nd
indi
cato
rs
stan
dard
ized
in li
ne
with
the
appr
oved
He
alth
ICT
fram
ewor
k
Tota
l no.
of r
egist
ries,
in
stru
men
ts a
nd
indi
cato
rs in
use
by
heal
th p
rogr
ams l
ine
with
the
appr
oved
He
alth
ICT
fram
ewor
k
TWG
/PM
O
repo
rts
Regi
strie
s of
inst
rum
ents
an
d st
anda
rdize
d in
stru
men
ts
Bi-‐A
nnua
l FM
OH/
PM
O
Nat
ion
al
TBD
TBD
. Health
ICT
Standards
advocated
or
Heal
th IC
T St
anda
rds
advo
cate
d fo
r (/N
) N
/A
TWG
/PM
O
repo
rts
Mon
thly
Re
port
s M
onth
ly
FMO
H N
atio
nal
, St
ate
TBD
TBD
.0 Legislatio
n Policy and
Compliance
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
(/N
) N
/A
TWG
/PM
O
repo
rts
TBD
TBD
.1 Legislatio
n
policy and
compliance
supp
orted
y
ational H
ealth
ICT
PO
Legi
slatio
n, p
olic
y an
d co
mpl
ianc
e su
ppor
ted
by
Nat
iona
l Hea
lth IC
T PM
O
(/N
)
N/A
TW
G/P
MO
re
port
s Pe
riodi
c Re
view
Bi
-‐Ann
ual
PMO
N
atio
nal
, St
ate
TBD
TBD
5.0 Change and Ad
optio
n (Capacity
uilding)
1.
of c
onsu
mer
s, c
are
prov
ider
s and
hea
lth-‐c
are
man
ager
s usin
g He
alth
ICT
solu
tions
/inno
vatio
ns
2.
of c
onsu
mer
s, c
are
prov
ider
and
hea
lth-‐c
are
man
ager
s sa
tisfie
d w
ith
usin
g He
alth
ICT
solu
tions
/inno
vatio
ns
1. N
o. o
f con
sum
ers,
care
pro
vide
rs a
nd
heal
th-‐c
are
man
ager
s usin
g He
alth
ICT
solu
tions
/inno
vatio
ns
2. N
o. o
f con
sum
ers,
ca
re p
rovi
der a
nd
heal
th-‐c
are
man
ager
s sa
tisfie
d w
ith u
sing
Heal
th IC
T
1. N
o. o
f con
sum
ers,
care
pro
vide
rs a
nd
heal
th-‐c
are
man
ager
s re
ache
d w
ith H
ealth
IC
T so
lutio
n/in
nova
tion
inte
rven
tions
2. N
o. o
f con
sum
ers,
care
pro
vide
rs a
nd
heal
th-‐c
are
man
ager
s re
ache
d w
ith H
ealth
IC
T
TBD
TBD
solu
tions
/inno
vatio
ns
solu
tion/
inno
vatio
n
inte
rven
tions
5.1 System o
r He
alth ICT readiness
and
ado
ption
o est p
ractices
esta
lished
1. H
ealth
ICT
read
ines
sas
sess
men
t com
plet
ed (
/N)
2. H
ealth
ICT
read
ines
s sy
stem
est
ablis
hed
(/N
)
N/A
W
orkf
orce
TW
G
Perio
dic
Revi
ew
Annu
ally
PM
O
Nat
ion
al
TBD
TBD
5.2 Incentive
mechanism
s to
encourage up
take o
He
alth ICT skills a
nd
competencies
esta
lished
1. N
o of
ince
ntiv
em
echa
nism
s dev
elop
ed
2.
of i
ncen
tive
mec
hani
sms
adop
ted
No
of in
cent
ive
mec
hani
sms
adop
ted
No
of in
cent
ive
mec
hani
sms
deve
lope
d
Wor
kfor
ce
TWG
Pe
riodi
c Re
view
Bi
-‐Ann
ual
PMO
N
atio
nal
, St
ate
TBD
TBD
5.
etho
dology
or accreditatio
n and
revision
o Health
ICT training
curriculum
esta
lished
Met
hodo
logy
for
accr
edita
tion
and
revi
sion
of
Heal
th IC
T tr
aini
ng
curr
icul
um e
stab
lishe
d (
/N)
N/A
W
orkf
orce
TW
G
Perio
dic
Revi
ew
Annu
ally
PM
O
Nat
ion
al
TBD
TBD
5. Plan
or Health
ICT a
areness a
nd
stakeholder
engagement
esta
lished
Plan
for H
ealth
ICT
awar
enes
s an
d st
akeh
olde
r eng
agem
ent
esta
blish
ed(
/N)
N/A
W
orkf
orce
TW
G
Perio
dic
Revi
ew
Bi-‐A
nnua
l PM
O
Nat
ion
al
TBD
TBD
5.5 Health
ICT
education and
training program
s esta
lished
No
of H
ealth
ICT
educ
atio
n pr
ogra
ms e
stab
lishe
d N
/A
Wor
kfor
ce
TWG
Pe
riodi
c Re
view
ua
rter
ly
PMO
N
atio
nal
TB
D TB
D
.0 In
rastructure
of h
ealth
pro
vide
rs w
ith
incr
ease
d ac
cess
to
elec
tron
ic h
ealth
info
rmat
ion
No
of h
ealth
pr
ovid
ers w
ith
acce
ss to
ele
ctro
nic
heal
th in
form
atio
n
No
of h
ealth
pr
ovid
ers r
each
with
el
ectr
onic
hea
lth
info
rmat
ion
inte
rven
tions
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
of h
ealth
care
con
sulta
tions
m
ade
thro
ugh
tele
med
icin
e N
o of
hea
lthca
re
cons
ulta
tions
mad
e th
roug
h te
lem
edic
ine
No
of h
ealth
pr
ovid
ers r
each
with
te
lem
edic
ine
in
terv
entio
ns
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.1Co
nnectiv
ity
coverage expanded
and enhanced
1.
of c
omm
uniti
es/ h
ealth
faci
litie
s sup
plie
d w
ith
conn
ectiv
ity h
ardw
are
infr
astr
uctu
re
No
of c
omm
uniti
es/
heal
th fa
cilit
ies
supp
lied
with
co
nnec
tivity
ha
rdw
are
infr
astr
uctu
re
tota
l no.
of
com
mun
ities
/ hea
lth
faci
litie
s tar
gete
d to
be
supp
lied
with
co
nnec
tivity
ha
rdw
are
infr
astr
uctu
re
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
of c
omm
uniti
es/h
ealth
fa
cilit
ies c
onne
cted
to a
n IS
P N
o of
co
mm
uniti
es/h
ealth
fa
cilit
ies c
onne
cted
to
a IS
P
tota
l no.
of
com
mun
ities
/hea
lth
faci
litie
s tar
gete
d to
be
con
nect
ed to
a IS
P
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
Append
ix : H
ealth
ICT
rame
ork
Health ICT
nalers
Interm
ediate
Outcome
Proximal
OutcomeOutpu
t
Indicator
Indicator D
einition
Da
ta
Sources
Data
Collection
etho
d
reuency
o Data
Respon
siility
Scop
e 2015
ase
line
2020
Targ et
umerator
Deno
minator
Enab
ling
and
sust
aina
ble
envi
ronm
ent f
or
impl
emen
tatio
n an
d sc
ale-‐
up o
f He
alth
ICT
in
Nig
eria
1.0 stalished
sustaina
le governance
structure
Num
ber (
No.
) of H
ealth
ICT
initi
ativ
es le
d by
key
st
akeh
olde
rs in
gov
ernm
ent -‐
N
atio
nal a
nd S
tate
Tec
hnic
al
Wor
king
Gro
ups (
TWG
s)
N/A
TB
D TB
D
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
es
/No
(/N
)
N/A
PM
O
Repo
rts o
f m
eetin
gs
Bi-‐A
nnua
l TW
Gs -‐
N
atio
nal
and
Stat
e,
FMO
H
Nat
ion
al,
Stat
e
TBD
TBD
1.1 ational H
ealth
ICT governance
structure esta
lished
Nat
iona
l Hea
lth IC
T St
eerin
g Co
mm
ittee
(/N
) N
/A
PMO
FM
OH,
PM
O
Nat
ion
al
TBD
TBD
Nat
iona
l Hea
lth IC
T TW
G/c
omm
ittee
(/N
) N
/A
PMO
TB
D TB
D
Nat
iona
l Hea
lth IC
T pr
ojec
t m
anag
emen
t offi
ce (P
MO
) (
/N)
N/A
PM
O
TBD
TBD
Perc
enta
ge (
) of
mee
tings
he
ld b
y th
e N
atio
nal T
WG
in
a ye
ar (w
ith o
utpu
ts a
nd
reso
lutio
ns)
No.
of m
eetin
gs h
eld
with
in th
e re
port
ing
perio
d
No.
of p
lann
ed
mee
ting
for w
ithin
re
port
ing
perio
d
PMO
TB
D TB
D
1.2 State
Governm
ent
engaged
Stat
e He
alth
ICT
TWG
s es
tabl
ished
(/N
) N
/A
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
TBD
TBD
of s
tate
s in
Nig
eria
with
fu
nctio
nal s
tate
leve
l TW
Gs
(func
tiona
l -‐de
fined
a
mee
ting
per q
uart
er)
No.
of s
tate
s with
fu
nctio
nal T
WG
s 3
Sta
tes o
f Nig
eria
St
ate
PMO
St
ate
TBD
TBD
of s
tate
s in
Nig
eria
with
st
ate
stra
tegy
, pla
n an
d bu
dget
No.
of s
tate
s with
st
ate
stra
tegi
es,
plan
s and
bud
gets
3 S
tate
s of N
iger
ia
Stat
e PM
O
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
Stat
e TB
D TB
D
1.road
stakeholder
engagement
achieved
of i
dent
ified
key
st
akeh
olde
r gro
ups e
ngag
ed
No.
of s
take
hold
er
grou
ps re
pres
ente
d at
mee
tings
Iden
tifie
d st
akeh
olde
r gr
oups
N
atio
nal/S
tat
e PM
O
uart
erly
PM
O
Nat
ion
al/S
tat
e
TBD
TBD
1. ational H
ealth
ICT
rame
ork
integrated and
linked
ith ational
Health Act and
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in th
e pr
eced
ing
year
with
su
bsec
tions
for H
ealth
ICT
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
with
subs
ectio
ns fo
r
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
Polic
y do
cum
ents
re
leas
ed/r
evi
ewed
Polic
y do
cum
ent
revi
ew
early
PM
O
Nat
ion
al
TBD
TBD

56!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
.2 xisting
Inrastructure or
Health ICT identiied
and assessed
of h
ealth
faci
litie
s with
ne
eds a
sses
smen
t com
plet
ed
no o
f hea
lth fa
cilit
ies
with
nee
ds
asse
ssm
ent
com
plet
ed
no o
f hea
lth fa
cilit
ies
targ
eted
for
asse
ssm
ent
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.
inimum
in
rastructural
reuirements o
r He
alth ICT
inrastructure
deined
Min
imum
infr
astr
uctu
ral
requ
irem
ents
for H
ealth
ICT
infr
astr
uctu
re d
efin
ed (
/N)
N/A
FM
CT
Annu
al
Surv
eys/
TBD
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.0Solutio
ns (Services
and Ap
plications)
TBD
TBD
.1 Core set o
approp
riate Health
ICT services and
Ap
plications
prioritied and
deployed
of i
nnov
ativ
e He
alth
ICT
solu
tion
depl
oyed
N
o of
inno
vativ
e He
alth
ICT
solu
tion
depl
oyed
Tota
l no
inno
vativ
e He
alth
ICT
solu
tion
deve
lope
d/av
aila
ble
TBD
TBD
TBD
FMCT
/FM
OH
Nat
ion
al
/sta
te
TBD
TBD
with
app
ropr
iate
Hea
lth
ICT
solu
tion
amon
gst t
arge
t po
pula
tion
no w
ith a
ppro
pria
te
Heal
th IC
T so
lutio
n am
ongs
t tar
get
popu
latio
n
targ
et p
opul
atio
n TB
D TB
D TB
D FM
CT/F
MO
H N
atio
nal
/s
tate
TBD
TBD
.2 est p
ractices in
developm
ent a
nd
use o Health
ICT
documented and
dissem
inated.
Best
pra
ctic
es in
de
velo
pmen
t and
use
of
Heal
th IC
T do
cum
ente
d an
d di
ssem
inat
ed. (
/N)
N/A
TB
D TB
D TB
D FM
CT/F
MO
H N
atio
nal
/s
tate
TBD
TBD
Health ICT Outcomes
i
Health Im
pact
Proximal
OutcomeOutpu
t Indicator
Indicator d
einition
Da
ta
sources
Data
collection
metho
d
reuency
o Data
Respon
siility
Scop
e 2015 ase
line
2020
Targ et
umerator
Deno
minator
By 2
2, H
ealth
IC
T w
ill h
elp
enab
le a
nd d
eliv
er
univ
ersa
l hea
lth
cove
rage
1.0 Im
proved access to
health se
rvices
Nationa
l ind
icator fo
r access
to hea
lth se
rvices
1.1
ectiv
e use o
telemedicine
of h
ealth
faci
litie
s pro
vidi
ng
tele
med
icin
e se
rvic
es
No.
of h
ealth
fa
cilit
ies d
eliv
erin
g te
lem
edic
ine
serv
ices
No.
or h
ealth
fa
cilit
ies i
dent
ified
as
pote
ntia
l te
lem
edic
ine
cent
ers
NHM
IS-‐
faci
lity
regi
stry
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
O
Nat
ion
al/
Stat
e
TBD
TBD
of h
ealth
enc
ount
ers
reso
lved
or s
uppo
rted
thro
ugh
tele
med
icin
e
No.
of h
ealth
en
coun
ters
reso
lved
or
supp
orte
d th
roug
h te
lem
edic
ine
No.
of h
ealth
en
coun
ters
Te
lem
edic
ine
pl
atfo
rms/
N
HMIS
TBD
TBD
1.2
ectiv
e use o
ICT or health
orker
of h
ealth
wor
kers
trai
ned
usin
g IC
T N
o. o
f hea
lth w
orke
rs
trai
ned
usin
g IC
T N
o. o
f hea
lth w
orke
rs
by c
adre
HR
IS
uart
erly
N
atio
nal/
Stat
e N
atio
nal
/ TB
D TB
D
i Whe
re p
ossib
le a
nd a
ppro
pria
te im
pact
eva
luat
ions
to a
sses
s the
effe
ctiv
enes
s, e
ffica
cy, a
nd c
ost-‐u
tility
of H
ealth
ICT
impl
emen
tatio
ns w
ill b
e co
nduc
ted.
solu
tions
/inno
vatio
ns
solu
tion/
inno
vatio
n
inte
rven
tions
5.1 System o
r He
alth ICT readiness
and
ado
ption
o est p
ractices
esta
lished
1. H
ealth
ICT
read
ines
sas
sess
men
t com
plet
ed (
/N)
2. H
ealth
ICT
read
ines
s sy
stem
est
ablis
hed
(/N
)
N/A
W
orkf
orce
TW
G
Perio
dic
Revi
ew
Annu
ally
PM
O
Nat
ion
al
TBD
TBD
5.2 Incentive
mechanism
s to
encourage up
take o
He
alth ICT skills a
nd
competencies
esta
lished
1. N
o of
ince
ntiv
em
echa
nism
s dev
elop
ed
2.
of i
ncen
tive
mec
hani
sms
adop
ted
No
of in
cent
ive
mec
hani
sms
adop
ted
No
of in
cent
ive
mec
hani
sms
deve
lope
d
Wor
kfor
ce
TWG
Pe
riodi
c Re
view
Bi
-‐Ann
ual
PMO
N
atio
nal
, St
ate
TBD
TBD
5.
etho
dology
or accreditatio
n and
revision
o Health
ICT training
curriculum
esta
lished
Met
hodo
logy
for
accr
edita
tion
and
revi
sion
of
Heal
th IC
T tr
aini
ng
curr
icul
um e
stab
lishe
d (
/N)
N/A
W
orkf
orce
TW
G
Perio
dic
Revi
ew
Annu
ally
PM
O
Nat
ion
al
TBD
TBD
5. Plan
or Health
ICT a
areness a
nd
stakeholder
engagement
esta
lished
Plan
for H
ealth
ICT
awar
enes
s an
d st
akeh
olde
r eng
agem
ent
esta
blish
ed(
/N)
N/A
W
orkf
orce
TW
G
Perio
dic
Revi
ew
Bi-‐A
nnua
l PM
O
Nat
ion
al
TBD
TBD
5.5 Health
ICT
education and
training program
s esta
lished
No
of H
ealth
ICT
educ
atio
n pr
ogra
ms e
stab
lishe
d N
/A
Wor
kfor
ce
TWG
Pe
riodi
c Re
view
ua
rter
ly
PMO
N
atio
nal
TB
D TB
D
.0 In
rastructure
of h
ealth
pro
vide
rs w
ith
incr
ease
d ac
cess
to
elec
tron
ic h
ealth
info
rmat
ion
No
of h
ealth
pr
ovid
ers w
ith
acce
ss to
ele
ctro
nic
heal
th in
form
atio
n
No
of h
ealth
pr
ovid
ers r
each
with
el
ectr
onic
hea
lth
info
rmat
ion
inte
rven
tions
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
of h
ealth
care
con
sulta
tions
m
ade
thro
ugh
tele
med
icin
e N
o of
hea
lthca
re
cons
ulta
tions
mad
e th
roug
h te
lem
edic
ine
No
of h
ealth
pr
ovid
ers r
each
with
te
lem
edic
ine
in
terv
entio
ns
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.1Co
nnectiv
ity
coverage expanded
and enhanced
1.
of c
omm
uniti
es/ h
ealth
faci
litie
s sup
plie
d w
ith
conn
ectiv
ity h
ardw
are
infr
astr
uctu
re
No
of c
omm
uniti
es/
heal
th fa
cilit
ies
supp
lied
with
co
nnec
tivity
ha
rdw
are
infr
astr
uctu
re
tota
l no.
of
com
mun
ities
/ hea
lth
faci
litie
s tar
gete
d to
be
supp
lied
with
co
nnec
tivity
ha
rdw
are
infr
astr
uctu
re
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
of c
omm
uniti
es/h
ealth
fa
cilit
ies c
onne
cted
to a
n IS
P N
o of
co
mm
uniti
es/h
ealth
fa
cilit
ies c
onne
cted
to
a IS
P
tota
l no.
of
com
mun
ities
/hea
lth
faci
litie
s tar
gete
d to
be
con
nect
ed to
a IS
P
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
Append
ix : H
ealth
ICT
rame
ork
Health ICT
nalers
Interm
ediate
Outcome
Proximal
OutcomeOutpu
t
Indicator
Indicator D
einition
Da
ta
Sources
Data
Collection
etho
d
reuency
o Data
Respon
siility
Scop
e 2015
ase
line
2020
Targ et
umerator
Deno
minator
Enab
ling
and
sust
aina
ble
envi
ronm
ent f
or
impl
emen
tatio
n an
d sc
ale-‐
up o
f He
alth
ICT
in
Nig
eria
1.0 stalished
sustaina
le governance
structure
Num
ber (
No.
) of H
ealth
ICT
initi
ativ
es le
d by
key
st
akeh
olde
rs in
gov
ernm
ent -‐
N
atio
nal a
nd S
tate
Tec
hnic
al
Wor
king
Gro
ups (
TWG
s)
N/A
TB
D TB
D
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
es
/No
(/N
)
N/A
PM
O
Repo
rts o
f m
eetin
gs
Bi-‐A
nnua
l TW
Gs -‐
N
atio
nal
and
Stat
e,
FMO
H
Nat
ion
al,
Stat
e
TBD
TBD
1.1 ational H
ealth
ICT governance
structure esta
lished
Nat
iona
l Hea
lth IC
T St
eerin
g Co
mm
ittee
(/N
) N
/A
PMO
FM
OH,
PM
O
Nat
ion
al
TBD
TBD
Nat
iona
l Hea
lth IC
T TW
G/c
omm
ittee
(/N
) N
/A
PMO
TB
D TB
D
Nat
iona
l Hea
lth IC
T pr
ojec
t m
anag
emen
t offi
ce (P
MO
) (
/N)
N/A
PM
O
TBD
TBD
Perc
enta
ge (
) of
mee
tings
he
ld b
y th
e N
atio
nal T
WG
in
a ye
ar (w
ith o
utpu
ts a
nd
reso
lutio
ns)
No.
of m
eetin
gs h
eld
with
in th
e re
port
ing
perio
d
No.
of p
lann
ed
mee
ting
for w
ithin
re
port
ing
perio
d
PMO
TB
D TB
D
1.2 State
Governm
ent
engaged
Stat
e He
alth
ICT
TWG
s es
tabl
ished
(/N
) N
/A
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
TBD
TBD
of s
tate
s in
Nig
eria
with
fu
nctio
nal s
tate
leve
l TW
Gs
(func
tiona
l -‐de
fined
a
mee
ting
per q
uart
er)
No.
of s
tate
s with
fu
nctio
nal T
WG
s 3
Sta
tes o
f Nig
eria
St
ate
PMO
St
ate
TBD
TBD
of s
tate
s in
Nig
eria
with
st
ate
stra
tegy
, pla
n an
d bu
dget
No.
of s
tate
s with
st
ate
stra
tegi
es,
plan
s and
bud
gets
3 S
tate
s of N
iger
ia
Stat
e PM
O
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
Stat
e TB
D TB
D
1.road
stakeholder
engagement
achieved
of i
dent
ified
key
st
akeh
olde
r gro
ups e
ngag
ed
No.
of s
take
hold
er
grou
ps re
pres
ente
d at
mee
tings
Iden
tifie
d st
akeh
olde
r gr
oups
N
atio
nal/S
tat
e PM
O
uart
erly
PM
O
Nat
ion
al/S
tat
e
TBD
TBD
1. ational H
ealth
ICT
rame
ork
integrated and
linked
ith ational
Health Act and
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in th
e pr
eced
ing
year
with
su
bsec
tions
for H
ealth
ICT
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
with
subs
ectio
ns fo
r
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
Polic
y do
cum
ents
re
leas
ed/r
evi
ewed
Polic
y do
cum
ent
revi
ew
early
PM
O
Nat
ion
al
TBD
TBD

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!57
.2 xisting
Inrastructure or
Health ICT identiied
and assessed
of h
ealth
faci
litie
s with
ne
eds a
sses
smen
t com
plet
ed
no o
f hea
lth fa
cilit
ies
with
nee
ds
asse
ssm
ent
com
plet
ed
no o
f hea
lth fa
cilit
ies
targ
eted
for
asse
ssm
ent
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.
inimum
in
rastructural
reuirements o
r He
alth ICT
inrastructure
deined
Min
imum
infr
astr
uctu
ral
requ
irem
ents
for H
ealth
ICT
infr
astr
uctu
re d
efin
ed (
/N)
N/A
FM
CT
Annu
al
Surv
eys/
TBD
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.0Solutio
ns (Services
and Ap
plications)
TBD
TBD
.1 Core set o
approp
riate Health
ICT services and
Ap
plications
prioritied and
deployed
of i
nnov
ativ
e He
alth
ICT
solu
tion
depl
oyed
N
o of
inno
vativ
e He
alth
ICT
solu
tion
depl
oyed
Tota
l no
inno
vativ
e He
alth
ICT
solu
tion
deve
lope
d/av
aila
ble
TBD
TBD
TBD
FMCT
/FM
OH
Nat
ion
al
/sta
te
TBD
TBD
with
app
ropr
iate
Hea
lth
ICT
solu
tion
amon
gst t
arge
t po
pula
tion
no w
ith a
ppro
pria
te
Heal
th IC
T so
lutio
n am
ongs
t tar
get
popu
latio
n
targ
et p
opul
atio
n TB
D TB
D TB
D FM
CT/F
MO
H N
atio
nal
/s
tate
TBD
TBD
.2 est p
ractices in
developm
ent a
nd
use o Health
ICT
documented and
dissem
inated.
Best
pra
ctic
es in
de
velo
pmen
t and
use
of
Heal
th IC
T do
cum
ente
d an
d di
ssem
inat
ed. (
/N)
N/A
TB
D TB
D TB
D FM
CT/F
MO
H N
atio
nal
/s
tate
TBD
TBD
Health ICT Outcomes
i
Health Im
pact
Proximal
OutcomeOutpu
t Indicator
Indicator d
einition
Da
ta
sources
Data
collection
metho
d
reuency
o Data
Respon
siility
Scop
e 2015 ase
line
2020
Targ et
umerator
Deno
minator
By 2
2, H
ealth
IC
T w
ill h
elp
enab
le a
nd d
eliv
er
univ
ersa
l hea
lth
cove
rage
1.0 Im
proved access to
health se
rvices
Nationa
l ind
icator fo
r access
to hea
lth se
rvices
1.1
ectiv
e use o
telemedicine
of h
ealth
faci
litie
s pro
vidi
ng
tele
med
icin
e se
rvic
es
No.
of h
ealth
fa
cilit
ies d
eliv
erin
g te
lem
edic
ine
serv
ices
No.
or h
ealth
fa
cilit
ies i
dent
ified
as
pote
ntia
l te
lem
edic
ine
cent
ers
NHM
IS-‐
faci
lity
regi
stry
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
O
Nat
ion
al/
Stat
e
TBD
TBD
of h
ealth
enc
ount
ers
reso
lved
or s
uppo
rted
thro
ugh
tele
med
icin
e
No.
of h
ealth
en
coun
ters
reso
lved
or
supp
orte
d th
roug
h te
lem
edic
ine
No.
of h
ealth
en
coun
ters
Te
lem
edic
ine
pl
atfo
rms/
N
HMIS
TBD
TBD
1.2
ectiv
e use o
ICT or health
orker
of h
ealth
wor
kers
trai
ned
usin
g IC
T N
o. o
f hea
lth w
orke
rs
trai
ned
usin
g IC
T N
o. o
f hea
lth w
orke
rs
by c
adre
HR
IS
uart
erly
N
atio
nal/
Stat
e N
atio
nal
/ TB
D TB
D
i Whe
re p
ossib
le a
nd a
ppro
pria
te im
pact
eva
luat
ions
to a
sses
s the
effe
ctiv
enes
s, e
ffica
cy, a
nd c
ost-‐u
tility
of H
ealth
ICT
impl
emen
tatio
ns w
ill b
e co
nduc
ted.
.2 xisting
Inrastructure or
Health ICT identiied
and assessed
of h
ealth
faci
litie
s with
ne
eds a
sses
smen
t com
plet
ed
no o
f hea
lth fa
cilit
ies
with
nee
ds
asse
ssm
ent
com
plet
ed
no o
f hea
lth fa
cilit
ies
targ
eted
for
asse
ssm
ent
FMCT
An
nual
Su
rvey
s/TB
D
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.
inimum
in
rastructural
reuirements o
r He
alth ICT
inrastructure
deined
Min
imum
infr
astr
uctu
ral
requ
irem
ents
for H
ealth
ICT
infr
astr
uctu
re d
efin
ed (
/N)
N/A
FM
CT
Annu
al
Surv
eys/
TBD
TBD
TBD
FMCT
N
atio
nal
TB
D TB
D
.0Solutio
ns (Services
and Ap
plications)
TBD
TBD
.1 Core set o
approp
riate Health
ICT services and
Ap
plications
prioritied and
deployed
of i
nnov
ativ
e He
alth
ICT
solu
tion
depl
oyed
N
o of
inno
vativ
e He
alth
ICT
solu
tion
depl
oyed
Tota
l no
inno
vativ
e He
alth
ICT
solu
tion
deve
lope
d/av
aila
ble
TBD
TBD
TBD
FMCT
/FM
OH
Nat
ion
al
/sta
te
TBD
TBD
with
app
ropr
iate
Hea
lth
ICT
solu
tion
amon
gst t
arge
t po
pula
tion
no w
ith a
ppro
pria
te
Heal
th IC
T so
lutio
n am
ongs
t tar
get
popu
latio
n
targ
et p
opul
atio
n TB
D TB
D TB
D FM
CT/F
MO
H N
atio
nal
/s
tate
TBD
TBD
.2 est p
ractices in
developm
ent a
nd
use o Health
ICT
documented and
dissem
inated.
Best
pra
ctic
es in
de
velo
pmen
t and
use
of
Heal
th IC
T do
cum
ente
d an
d di
ssem
inat
ed. (
/N)
N/A
TB
D TB
D TB
D FM
CT/F
MO
H N
atio
nal
/s
tate
TBD
TBD
Health ICT Outcomes
i
Health Im
pact
Proximal
OutcomeOutpu
t Indicator
Indicator d
einition
Da
ta
sources
Data
collection
metho
d
reuency
o Data
Respon
siility
Scop
e 2015 ase
line
2020
Targ et
umerator
Deno
minator
By 2
2, H
ealth
IC
T w
ill h
elp
enab
le a
nd d
eliv
er
univ
ersa
l hea
lth
cove
rage
1.0 Im
proved access to
health se
rvices
Nationa
l ind
icator fo
r access
to hea
lth se
rvices
1.1
ectiv
e use o
telemedicine
of h
ealth
faci
litie
s pro
vidi
ng
tele
med
icin
e se
rvic
es
No.
of h
ealth
fa
cilit
ies d
eliv
erin
g te
lem
edic
ine
serv
ices
No.
or h
ealth
fa
cilit
ies i
dent
ified
as
pote
ntia
l te
lem
edic
ine
cent
ers
NHM
IS-‐
faci
lity
regi
stry
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
O
Nat
ion
al/
Stat
e
TBD
TBD
of h
ealth
enc
ount
ers
reso
lved
or s
uppo
rted
thro
ugh
tele
med
icin
e
No.
of h
ealth
en
coun
ters
reso
lved
or
supp
orte
d th
roug
h te
lem
edic
ine
No.
of h
ealth
en
coun
ters
Te
lem
edic
ine
pl
atfo
rms/
N
HMIS
TBD
TBD
1.2
ectiv
e use o
ICT or health
orker
of h
ealth
wor
kers
trai
ned
usin
g IC
T N
o. o
f hea
lth w
orke
rs
trai
ned
usin
g IC
T N
o. o
f hea
lth w
orke
rs
by c
adre
HR
IS
uart
erly
N
atio
nal/
Stat
e N
atio
nal
/ TB
D TB
D
i Whe
re p
ossib
le a
nd a
ppro
pria
te im
pact
eva
luat
ions
to a
sses
s the
effe
ctiv
enes
s, e
ffica
cy, a
nd c
ost-‐u
tility
of H
ealth
ICT
impl
emen
tatio
ns w
ill b
e co
nduc
ted.
training
PMO
St
ate
1.ectiv
e use o
ICT or health
orker
supervision and
supp
ort
of h
ealth
wor
kers
bei
ng
supe
rvise
d us
ing
ICT
tool
s N
o. o
f hea
lth
wor
kers
supe
rvise
d us
ing
ICT
tool
s by
cadr
e
No.
of h
ealth
wor
kers
by
cad
re
HRIS
ua
rter
ly
Nat
iona
l/ St
ate
PMO
Nat
ion
al/
Stat
e
TBD
TBD
2.0 Im
proved coverage o
health se
rvices
Nationa
l ind
icator fo
r covera
e of hea
lth se
rvices
TB
D TB
D
2.1
ectiv
e use o
CRS or child health
c
hild
ren
born
regi
ster
ed in
bi
rth
regi
stry
syst
em
No.
of c
hild
ren
regi
ster
ed in
birt
h re
gist
ry
No.
of c
hild
ren
born
(e
stim
ated
thro
ugh
DHS
or C
ensu
s)
Birt
h re
gist
ry/
othe
r so
urce
s TB
D
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal
Popu
latio
n Co
mm
issi
on
Nat
ion
al/
Stat
e
TBD
TBD
2.2
ectiv
e use o
pregnancy registry
or maternal health
pre
gnan
t wom
en re
gist
ered
in
pre
gnan
cy re
gist
ry
No.
of p
regn
ant
wom
en re
gist
ered
in
preg
nanc
y re
gist
ry
No.
of p
regn
ant
wom
en (e
stim
ated
th
roug
h DH
S or
Ce
nsus
)
Preg
nanc
y re
gist
ry/
othe
r so
urce
s TB
D
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
2.ectiv
e use o
human re
source
inormation system
(HRIS) o
r distri
ution o
health orkers
hea
lth w
orke
rs b
y ca
dre
regi
ster
ed in
HRI
S N
o. o
f hea
lth w
orke
rs
regi
ster
ed in
HRI
S N
o. o
f hea
lth w
orke
rs
by c
adre
(as
estim
ated
by
key
sour
ces)
Heal
th
wor
kers
by
cadr
e ba
selin
e
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH
HRH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
ectiv
e use o
HIS o
r health
system
plann
ing
of h
ealth
faci
litie
s rep
ortin
g in
to N
HMIS
(pub
lic a
nd
priv
ate)
No.
of h
ealth
fa
cilit
ies r
epor
ting
into
NHM
IS (p
ublic
an
d pr
ivat
e)
No.
of h
ealth
faci
litie
s (p
ublic
and
priv
ate)
DH
IS2
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
ectiv
e use o L
IS
or tracking su
pply
and demand
or
commod
ities
of f
acili
ties w
ith e
LMIS
re
port
ing
no st
ock
outs
N
o. o
f fac
ilitie
s with
eL
MIS
repo
rtin
g no
st
ock
outs
No.
of f
acili
ties w
ith
eLM
IS
eLM
IS
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
.0 Increased up
take o
health se
rvices
Nationa
l ervice eliver
nd
icators
.1
ectiv
e use o
mo
ile messaging
or dem
and creatio
n or R
CH
of p
regn
ant w
omen
and
ne
w m
othe
rs re
ceiv
ing
mob
ile
mes
sage
s acc
essin
g he
alth
se
rvic
es
No.
of p
regn
ant
wom
en a
nd n
ew
mot
hers
rece
ivin
g m
obile
mes
sage
s ac
cess
ing
heal
th
serv
ices
Estim
ated
no.
of
preg
nant
wom
en a
nd
new
mot
hers
ta
rget
ed fo
r mob
ile
mes
sagi
ng
MAM
A/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
O
& M
AMA
Nat
ion
al/
Stat
e
TBD
TBD
.2
ectiv
e use o
mo
ile con
ditio
nal
cash transer o
r demand creatio
n
of c
itize
ns a
cces
sing
heal
th
serv
ices
thro
ugh
mob
ile
cond
ition
al c
ash
tran
sfer
pr
ogra
ms
No.
of c
itize
ns
acce
ssin
g he
alth
se
rvic
es th
roug
h m
obile
con
ditio
nal
cash
tran
sfer
pr
ogra
ms
Estim
ated
no.
of
citiz
ens t
o be
co
vere
d/ su
ppor
ted
thro
ugh
mob
ile
cond
ition
al c
ash
tran
sfer
pro
gram
s
mCC
T/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal
, St
ate
TBD
TBD
.0 Im
proved uality o
care
Nationa
l alit
of care
indicators

58!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
ectiv
e use o ICT
or decision supp
ort
of h
ealth
wor
kers
usin
g de
cisio
n su
ppor
t too
ls to
im
prov
e qu
ality
of c
are
No.
of h
ealth
wor
kers
us
ing
deci
sion
supp
ort t
ools
to
impr
ove
qual
ity o
f ca
re
Estim
ated
no.
of
heal
th w
orke
rs
targ
eted
for d
ecisi
on
supp
ort t
ools
Deci
sion
supp
ort
tool
da
shbo
ards
/ TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
Os
and
impl
eme
nter
s
Nat
ion
al ,
Stat
e
TBD
TBD
ectiv
e use o ICT
ithin th
e continuu
m o
care
(incl. reerrals)
of f
acili
ties i
mpl
emen
ting
ICT
to su
ppor
t the
con
tinuu
m
of c
are
No.
of f
acili
ties
impl
emen
ting
ICT
to
supp
ort t
he
cont
inuu
m o
f car
e
No.
of f
acili
ties
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
Os
and
impl
eme
nter
s
Nat
ion
al ,
Stat
e
TBD
TBD
5.0 Increased
inancial
coverage o
r health
care
Nationa
l finan
cial covera
e for h
ealth
care indicators
5.1
ectiv
e use o
ICT or HIS
of c
itize
ns e
nrol
led
in N
HIS
syst
em
No.
of c
itize
ns
enro
lled
in N
HIS
syst
em
No.
of c
itize
ns
targ
eted
for
enro
llmen
t in
NHI
S
NHI
S/ T
BD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
HIS
Nat
ion
al/
Stat
e
TBD
TBD
of c
laim
s and
re
imbu
rsem
ents
pro
cess
ed
thro
ugh
NHI
S pl
atfo
rm
No.
of c
laim
s and
re
imbu
rsem
ents
pr
oces
sed
No.
of c
laim
s and
re
imbu
rsem
ents
su
bmitt
ed fo
r pr
oces
sing
NHI
S/ T
BD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
HIS
Nat
ion
al/
Stat
e
TBD
TBD
5.2
ectiv
e use o
ICT or non
Insurancerelated
inancial
transactions
TBD-‐
this
may
incl
ude
the
use
of m
obile
mon
ey o
r ele
ctro
nic
paym
ents
for h
ealth
wor
kers
, et
c.
TBD
TBD
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
PM
O/
TBD
Nat
ion
al/
Stat
e
TBD
TBD
.0 Increased euity in
access to
and
uality o
health se
rvices
in
ormation and
inancing
Nationa
l hea
lth e
it
indicators
.1
ectiv
e use o
ICT or delivering
approp
riate health
services o
r tho
se
ho need them
most
ased on
epidem
iology
of d
istrib
utio
n of
serv
ices
an
d hu
man
reso
urce
pla
ns a
nd
fund
allo
catio
ns m
ade
thro
ugh
the
use
of e
pide
mio
logi
cal
data
acc
esse
d th
roug
h IC
T se
rvic
es
No.
of d
istrib
utio
n of
se
rvic
es a
nd h
uman
re
sour
ce p
lans
and
fu
nd a
lloca
tions
m
ade
thro
ugh
the
use
of
epid
emio
logi
cal d
ata
acce
ssed
thro
ugh
ICT
serv
ices
No.
of d
istrib
utio
n of
se
rvic
es a
nd h
uman
re
sour
ce p
lans
and
fu
nd a
lloca
tions
mad
e
NHM
IS/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
PM
O/T
BD
Nat
ion
al/
Stat
e
TBD
TBD
.2
ectiv
e use o
ICT or delivering
approp
riate health
services o
r tho
se
ho need them
most
ased on
inancial need
of p
lans
and
fund
allo
catio
ns
mad
e th
at ta
rget
NHI
S se
rvic
es
to th
e po
or a
nd m
ost i
n fin
anci
al n
eed
No.
of p
lans
and
fu
nd a
lloca
tions
m
ade
that
targ
et
NHI
S se
rvic
es to
the
poor
and
mos
t in
finan
cial
nee
d
No.
of p
lans
and
fund
al
loca
tions
mad
e to
de
liver
NHI
S se
rvic
es
NHI
S/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
PM
O/
TBD
Nat
ion
al /
Stat
e
TBD
TBD
training
PMO
St
ate
1.ectiv
e use o
ICT or health
orker
supervision and
supp
ort
of h
ealth
wor
kers
bei
ng
supe
rvise
d us
ing
ICT
tool
s N
o. o
f hea
lth
wor
kers
supe
rvise
d us
ing
ICT
tool
s by
cadr
e
No.
of h
ealth
wor
kers
by
cad
re
HRIS
ua
rter
ly
Nat
iona
l/ St
ate
PMO
Nat
ion
al/
Stat
e
TBD
TBD
2.0 Im
proved coverage o
health se
rvices
Nationa
l ind
icator fo
r covera
e of hea
lth se
rvices
TB
D TB
D
2.1
ectiv
e use o
CRS or child health
c
hild
ren
born
regi
ster
ed in
bi
rth
regi
stry
syst
em
No.
of c
hild
ren
regi
ster
ed in
birt
h re
gist
ry
No.
of c
hild
ren
born
(e
stim
ated
thro
ugh
DHS
or C
ensu
s)
Birt
h re
gist
ry/
othe
r so
urce
s TB
D
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal
Popu
latio
n Co
mm
issi
on
Nat
ion
al/
Stat
e
TBD
TBD
2.2
ectiv
e use o
pregnancy registry
or maternal health
pre
gnan
t wom
en re
gist
ered
in
pre
gnan
cy re
gist
ry
No.
of p
regn
ant
wom
en re
gist
ered
in
preg
nanc
y re
gist
ry
No.
of p
regn
ant
wom
en (e
stim
ated
th
roug
h DH
S or
Ce
nsus
)
Preg
nanc
y re
gist
ry/
othe
r so
urce
s TB
D
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
2.ectiv
e use o
human re
source
inormation system
(HRIS) o
r distri
ution o
health orkers
hea
lth w
orke
rs b
y ca
dre
regi
ster
ed in
HRI
S N
o. o
f hea
lth w
orke
rs
regi
ster
ed in
HRI
S N
o. o
f hea
lth w
orke
rs
by c
adre
(as
estim
ated
by
key
sour
ces)
Heal
th
wor
kers
by
cadr
e ba
selin
e
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH
HRH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
ectiv
e use o
HIS o
r health
system
plann
ing
of h
ealth
faci
litie
s rep
ortin
g in
to N
HMIS
(pub
lic a
nd
priv
ate)
No.
of h
ealth
fa
cilit
ies r
epor
ting
into
NHM
IS (p
ublic
an
d pr
ivat
e)
No.
of h
ealth
faci
litie
s (p
ublic
and
priv
ate)
DH
IS2
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
ectiv
e use o L
IS
or tracking su
pply
and demand
or
commod
ities
of f
acili
ties w
ith e
LMIS
re
port
ing
no st
ock
outs
N
o. o
f fac
ilitie
s with
eL
MIS
repo
rtin
g no
st
ock
outs
No.
of f
acili
ties w
ith
eLM
IS
eLM
IS
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
FM
OH/
SM
OH
Nat
ion
al/
Stat
e
TBD
TBD
.0 Increased up
take o
health se
rvices
Nationa
l ervice eliver
nd
icators
.1
ectiv
e use o
mo
ile messaging
or dem
and creatio
n or R
CH
of p
regn
ant w
omen
and
ne
w m
othe
rs re
ceiv
ing
mob
ile
mes
sage
s acc
essin
g he
alth
se
rvic
es
No.
of p
regn
ant
wom
en a
nd n
ew
mot
hers
rece
ivin
g m
obile
mes
sage
s ac
cess
ing
heal
th
serv
ices
Estim
ated
no.
of
preg
nant
wom
en a
nd
new
mot
hers
ta
rget
ed fo
r mob
ile
mes
sagi
ng
MAM
A/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
O
& M
AMA
Nat
ion
al/
Stat
e
TBD
TBD
.2
ectiv
e use o
mo
ile con
ditio
nal
cash transer o
r demand creatio
n
of c
itize
ns a
cces
sing
heal
th
serv
ices
thro
ugh
mob
ile
cond
ition
al c
ash
tran
sfer
pr
ogra
ms
No.
of c
itize
ns
acce
ssin
g he
alth
se
rvic
es th
roug
h m
obile
con
ditio
nal
cash
tran
sfer
pr
ogra
ms
Estim
ated
no.
of
citiz
ens t
o be
co
vere
d/ su
ppor
ted
thro
ugh
mob
ile
cond
ition
al c
ash
tran
sfer
pro
gram
s
mCC
T/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal
, St
ate
TBD
TBD
.0 Im
proved uality o
care
Nationa
l alit
of care
indicators
Append
ix : H
ealth
ICT
rame
ork
Health ICT
nalers
Interm
ediate
Outcome
Proximal
OutcomeOutpu
t
Indicator
Indicator D
einition
Da
ta
Sources
Data
Collection
etho
d
reuency
o Data
Respon
siility
Scop
e 2015
ase
line
2020
Targ et
umerator
Deno
minator
Enab
ling
and
sust
aina
ble
envi
ronm
ent f
or
impl
emen
tatio
n an
d sc
ale-‐
up o
f He
alth
ICT
in
Nig
eria
1.0 stalished
sustaina
le governance
structure
Num
ber (
No.
) of H
ealth
ICT
initi
ativ
es le
d by
key
st
akeh
olde
rs in
gov
ernm
ent -‐
N
atio
nal a
nd S
tate
Tec
hnic
al
Wor
king
Gro
ups (
TWG
s)
N/A
TB
D TB
D
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
es
/No
(/N
)
N/A
PM
O
Repo
rts o
f m
eetin
gs
Bi-‐A
nnua
l TW
Gs -‐
N
atio
nal
and
Stat
e,
FMO
H
Nat
ion
al,
Stat
e
TBD
TBD
1.1 ational H
ealth
ICT governance
structure esta
lished
Nat
iona
l Hea
lth IC
T St
eerin
g Co
mm
ittee
(/N
) N
/A
PMO
FM
OH,
PM
O
Nat
ion
al
TBD
TBD
Nat
iona
l Hea
lth IC
T TW
G/c
omm
ittee
(/N
) N
/A
PMO
TB
D TB
D
Nat
iona
l Hea
lth IC
T pr
ojec
t m
anag
emen
t offi
ce (P
MO
) (
/N)
N/A
PM
O
TBD
TBD
Perc
enta
ge (
) of
mee
tings
he
ld b
y th
e N
atio
nal T
WG
in
a ye
ar (w
ith o
utpu
ts a
nd
reso
lutio
ns)
No.
of m
eetin
gs h
eld
with
in th
e re
port
ing
perio
d
No.
of p
lann
ed
mee
ting
for w
ithin
re
port
ing
perio
d
PMO
TB
D TB
D
1.2 State
Governm
ent
engaged
Stat
e He
alth
ICT
TWG
s es
tabl
ished
(/N
) N
/A
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
TBD
TBD
of s
tate
s in
Nig
eria
with
fu
nctio
nal s
tate
leve
l TW
Gs
(func
tiona
l -‐de
fined
a
mee
ting
per q
uart
er)
No.
of s
tate
s with
fu
nctio
nal T
WG
s 3
Sta
tes o
f Nig
eria
St
ate
PMO
St
ate
TBD
TBD
of s
tate
s in
Nig
eria
with
st
ate
stra
tegy
, pla
n an
d bu
dget
No.
of s
tate
s with
st
ate
stra
tegi
es,
plan
s and
bud
gets
3 S
tate
s of N
iger
ia
Stat
e PM
O
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
Stat
e TB
D TB
D
1.road
stakeholder
engagement
achieved
of i
dent
ified
key
st
akeh
olde
r gro
ups e
ngag
ed
No.
of s
take
hold
er
grou
ps re
pres
ente
d at
mee
tings
Iden
tifie
d st
akeh
olde
r gr
oups
N
atio
nal/S
tat
e PM
O
uart
erly
PM
O
Nat
ion
al/S
tat
e
TBD
TBD
1. ational H
ealth
ICT
rame
ork
integrated and
linked
ith ational
Health Act and
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in th
e pr
eced
ing
year
with
su
bsec
tions
for H
ealth
ICT
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
with
subs
ectio
ns fo
r
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
Polic
y do
cum
ents
re
leas
ed/r
evi
ewed
Polic
y do
cum
ent
revi
ew
early
PM
O
Nat
ion
al
TBD
TBD

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!59
ectiv
e use o ICT
or decision supp
ort
of h
ealth
wor
kers
usin
g de
cisio
n su
ppor
t too
ls to
im
prov
e qu
ality
of c
are
No.
of h
ealth
wor
kers
us
ing
deci
sion
supp
ort t
ools
to
impr
ove
qual
ity o
f ca
re
Estim
ated
no.
of
heal
th w
orke
rs
targ
eted
for d
ecisi
on
supp
ort t
ools
Deci
sion
supp
ort
tool
da
shbo
ards
/ TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
Os
and
impl
eme
nter
s
Nat
ion
al ,
Stat
e
TBD
TBD
ectiv
e use o ICT
ithin th
e continuu
m o
care
(incl. reerrals)
of f
acili
ties i
mpl
emen
ting
ICT
to su
ppor
t the
con
tinuu
m
of c
are
No.
of f
acili
ties
impl
emen
ting
ICT
to
supp
ort t
he
cont
inuu
m o
f car
e
No.
of f
acili
ties
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
atio
nal/
Stat
e PM
Os
and
impl
eme
nter
s
Nat
ion
al ,
Stat
e
TBD
TBD
5.0 Increased
inancial
coverage o
r health
care
Nationa
l finan
cial covera
e for h
ealth
care indicators
5.1
ectiv
e use o
ICT or HIS
of c
itize
ns e
nrol
led
in N
HIS
syst
em
No.
of c
itize
ns
enro
lled
in N
HIS
syst
em
No.
of c
itize
ns
targ
eted
for
enro
llmen
t in
NHI
S
NHI
S/ T
BD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
HIS
Nat
ion
al/
Stat
e
TBD
TBD
of c
laim
s and
re
imbu
rsem
ents
pro
cess
ed
thro
ugh
NHI
S pl
atfo
rm
No.
of c
laim
s and
re
imbu
rsem
ents
pr
oces
sed
No.
of c
laim
s and
re
imbu
rsem
ents
su
bmitt
ed fo
r pr
oces
sing
NHI
S/ T
BD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
N
HIS
Nat
ion
al/
Stat
e
TBD
TBD
5.2
ectiv
e use o
ICT or non
Insurancerelated
inancial
transactions
TBD-‐
this
may
incl
ude
the
use
of m
obile
mon
ey o
r ele
ctro
nic
paym
ents
for h
ealth
wor
kers
, et
c.
TBD
TBD
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
PM
O/
TBD
Nat
ion
al/
Stat
e
TBD
TBD
.0 Increased euity in
access to
and
uality o
health se
rvices
in
ormation and
inancing
Nationa
l hea
lth e
it
indicators
.1
ectiv
e use o
ICT or delivering
approp
riate health
services o
r tho
se
ho need them
most
ased on
epidem
iology
of d
istrib
utio
n of
serv
ices
an
d hu
man
reso
urce
pla
ns a
nd
fund
allo
catio
ns m
ade
thro
ugh
the
use
of e
pide
mio
logi
cal
data
acc
esse
d th
roug
h IC
T se
rvic
es
No.
of d
istrib
utio
n of
se
rvic
es a
nd h
uman
re
sour
ce p
lans
and
fu
nd a
lloca
tions
m
ade
thro
ugh
the
use
of
epid
emio
logi
cal d
ata
acce
ssed
thro
ugh
ICT
serv
ices
No.
of d
istrib
utio
n of
se
rvic
es a
nd h
uman
re
sour
ce p
lans
and
fu
nd a
lloca
tions
mad
e
NHM
IS/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
PM
O/T
BD
Nat
ion
al/
Stat
e
TBD
TBD
.2
ectiv
e use o
ICT or delivering
approp
riate health
services o
r tho
se
ho need them
most
ased on
inancial need
of p
lans
and
fund
allo
catio
ns
mad
e th
at ta
rget
NHI
S se
rvic
es
to th
e po
or a
nd m
ost i
n fin
anci
al n
eed
No.
of p
lans
and
fu
nd a
lloca
tions
m
ade
that
targ
et
NHI
S se
rvic
es to
the
poor
and
mos
t in
finan
cial
nee
d
No.
of p
lans
and
fund
al
loca
tions
mad
e to
de
liver
NHI
S se
rvic
es
NHI
S/
Oth
er
sour
ces
TBD
Exist
ing/
new
el
ectr
onic
sy
stem
s
uart
erly
PM
O/
TBD
Nat
ion
al /
Stat
e
TBD
TBD
Append
ix : H
ealth
ICT
rame
ork
Health ICT
nalers
Interm
ediate
Outcome
Proximal
OutcomeOutpu
t
Indicator
Indicator D
einition
Da
ta
Sources
Data
Collection
etho
d
reuency
o Data
Respon
siility
Scop
e 2015
ase
line
2020
Targ et
umerator
Deno
minator
Enab
ling
and
sust
aina
ble
envi
ronm
ent f
or
impl
emen
tatio
n an
d sc
ale-‐
up o
f He
alth
ICT
in
Nig
eria
1.0 stalished
sustaina
le governance
structure
Num
ber (
No.
) of H
ealth
ICT
initi
ativ
es le
d by
key
st
akeh
olde
rs in
gov
ernm
ent -‐
N
atio
nal a
nd S
tate
Tec
hnic
al
Wor
king
Gro
ups (
TWG
s)
N/A
TB
D TB
D
Heal
th IC
T po
licy
chan
ges
adop
ted
and
enac
ted
es
/No
(/N
)
N/A
PM
O
Repo
rts o
f m
eetin
gs
Bi-‐A
nnua
l TW
Gs -‐
N
atio
nal
and
Stat
e,
FMO
H
Nat
ion
al,
Stat
e
TBD
TBD
1.1 ational H
ealth
ICT governance
structure esta
lished
Nat
iona
l Hea
lth IC
T St
eerin
g Co
mm
ittee
(/N
) N
/A
PMO
FM
OH,
PM
O
Nat
ion
al
TBD
TBD
Nat
iona
l Hea
lth IC
T TW
G/c
omm
ittee
(/N
) N
/A
PMO
TB
D TB
D
Nat
iona
l Hea
lth IC
T pr
ojec
t m
anag
emen
t offi
ce (P
MO
) (
/N)
N/A
PM
O
TBD
TBD
Perc
enta
ge (
) of
mee
tings
he
ld b
y th
e N
atio
nal T
WG
in
a ye
ar (w
ith o
utpu
ts a
nd
reso
lutio
ns)
No.
of m
eetin
gs h
eld
with
in th
e re
port
ing
perio
d
No.
of p
lann
ed
mee
ting
for w
ithin
re
port
ing
perio
d
PMO
TB
D TB
D
1.2 State
Governm
ent
engaged
Stat
e He
alth
ICT
TWG
s es
tabl
ished
(/N
) N
/A
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
TBD
TBD
of s
tate
s in
Nig
eria
with
fu
nctio
nal s
tate
leve
l TW
Gs
(func
tiona
l -‐de
fined
a
mee
ting
per q
uart
er)
No.
of s
tate
s with
fu
nctio
nal T
WG
s 3
Sta
tes o
f Nig
eria
St
ate
PMO
St
ate
TBD
TBD
of s
tate
s in
Nig
eria
with
st
ate
stra
tegy
, pla
n an
d bu
dget
No.
of s
tate
s with
st
ate
stra
tegi
es,
plan
s and
bud
gets
3 S
tate
s of N
iger
ia
Stat
e PM
O
uart
erly
St
ate
PMO
, SM
OH,
FM
OH
Stat
e TB
D TB
D
1.road
stakeholder
engagement
achieved
of i
dent
ified
key
st
akeh
olde
r gro
ups e
ngag
ed
No.
of s
take
hold
er
grou
ps re
pres
ente
d at
mee
tings
Iden
tifie
d st
akeh
olde
r gr
oups
N
atio
nal/S
tat
e PM
O
uart
erly
PM
O
Nat
ion
al/S
tat
e
TBD
TBD
1. ational H
ealth
ICT
rame
ork
integrated and
linked
ith ational
Health Act and
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in th
e pr
eced
ing
year
with
su
bsec
tions
for H
ealth
ICT
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
with
subs
ectio
ns fo
r
No.
of n
atio
nal p
olic
y do
cum
ents
re
leas
ed/r
evie
wed
in
the
prec
edin
g ye
ar
Polic
y do
cum
ents
re
leas
ed/r
evi
ewed
Polic
y do
cum
ent
revi
ew
early
PM
O
Nat
ion
al
TBD
TBD

60!|!NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020
Endnotes
1.# UN Foundation in support of ICT4SOML. “Assessing the Enabling Environment for ICTs for Health in Nigeria: A Review of Policies.” Abuja, Nigeria; 2014. Available at: http://www.health.gov.ng/doc/nigeria-Health-ICT-policy-report.pdf
2.# The World Bank. “Nigeria Country Data.” 2015. Available at: http://data.worldbank.org/country/nigeria. Accessed May 27, 2015.
3.# The World Bank. “World Bank Data.” 2015. Available at: http://databank.worldbank.org/Data/Views/VariableSelection/SelectVariables.aspx?source=Health Nutrition and Population Statistics: Population estimates and projections. Accessed May 28, 2015.
4.# National Populations Commission. “Nigeria Demographic and Health Survey 2013.” 1st ed. (USAID, UKAID, UNFPA, eds.). Abuja; 2014. Available at: http://www.population.gov.ng/images/ndhs_data/ndhs_2013/2013_ndhs_final_report.pdf.
5.# The World Bank. “World Bank Data.” 2015. Available at: http://databank.worldbank.org/Data/Views/VariableSelection/SelectVariables.aspx?source=Health Nutrition and Population Statistics: Population estimates and projections. Accessed May 28, 2015.
6.# National Populations Commission. “Nigeria Demographic and Health Survey 2013.” 1st ed. (USAID, UKAID, UNFPA, eds.). Abuja; 2014. Available at: http://www.population.gov.ng/images/ndhs_data/ndhs_2013/2013_ndhs_final_report.pdf.
7.# Center for Disease Control and Prevention. “Impact of Malaria.” 2014: CDC. Available at: http://www.cdc.gov/malaria/malaria_worldwide/impact.html. Accessed May 27, 2015.
8.# WHO. “Nigeria Country Profile.” 2014. Available at: http://www.who.int/nmh/countries/nga_en.pdf.
9.# WHO. “State of Health Financing in the African Region.” 2013. Available at: http://www.afro.who.int/pt/downloads/doc_download/8698-state-of-health-financing-in-the-african-region.html.
10.# NHIS. “Low Enrolment Level Unacceptable – NHIS Boss.” Available at: http://www.nhis.gov.ng/index.php?option=com_content&view=article&id=221:low-enrolment-level-unacceptable--nhis-boss&catid=46:newsletter. Accessed May 27, 2015.
11.# Jenna D, Eric T, Isaac L. “Ghana’s National Health Insurance Scheme: a national level investigation of members’ perceptions of service provision.” BMC Int Health Hum Rights. 2013;13(1):35. doi:10.1186/1472-698X-13-35.
12.# UN Foundation in support of ICT4SOML. “Assessing the Enabling Environment for ICTs for Health in Nigeria: A Review of Policies.” Abuja, Nigeria; 2014. Available at: http://www.health.gov.ng/doc/nigeria-Health-ICT-policy-report.pdf
13.# UN Foundation in support of ICT4SOML. “Assessing the Enabling

NATIONAL HEALTH ICT STRATEGIC FRAMEWORK 2015–2020!|!61
Environment for ICTs for Health in Nigeria: A Review of Policies.” Abuja, Nigeria; 2014. Available at: http://www.health.gov.ng/doc/nigeria-Health-ICT-policy-report.pdf.
14.# UN Foundation in support of ICT4SOML. “Assessing the Enabling Environment for ICTs for Health in Nigeria: A Review of Policies.” Abuja, Nigeria; 2014. Available at: http://www.health.gov.ng/doc/nigeria-Health-ICT-policy-report.pdf.
15.# WHO, ITU. WHO-ITU. “National eHealth Strategy Toolkit.” 2012. Available at: https://www.itu.int/pub/D-STR-E_HEALTH.05-2012.
16.# UN Foundation in support of ICT4SOML. “Assessing the Enabling Environment for ICTs for Health in Nigeria: A Review of Policies.” Abuja, Nigeria; 2014. Available at: http://www.health.gov.ng/doc/nigeria-Health-ICT-policy-report.pdf.
17.# Trust Law, mHealth Alliance, Baker&McKenzie, MSD Bewell. “Patient Privacy in a Mobile World: A Framework to Address Privacy Law Issues in Mobile Health.” 2013. Available at: http://www.trust.org/contentAsset/raw-data/03172beb-0f11-438e-94be-e02978de3036/file.
18.# Federal Government of Nigeria. “National Health Act.” 2014.
19.# Trust Law, mHealth Alliance, Baker&McKenzie, MSD Bewell. “Patient Privacy in a Mobile World: A Framework to Address Privacy Law Issues in Mobile Health.” 2013. Available at: http://www.trust.org/contentAsset/raw-data/03172beb-0f11-438e-94be-e02978de3036/file.
20.# Global Health Workforce. “Human Resources for Health Country Profile Nigeria.” 2008. Available at: http://www.unfpa.org/sowmy/resources/docs/library/R050_AHWO_2008_Nigeria_HRHProfile.pdf.
21.# WHO. “WHO Country Brief: Nigeria” Global Health Workforce Alliance. Available at: http://www.who.int/workforcealliance/countries/nga/en/.
22.# UN Foundation in support of ICT4SOML. “Nigeria Health ICT Phase 2 Field Assessment.” Abuja, Nigeria; 2015. Available at: http://www.health.gov.ng/doc/FieldAssessment.pdf.
23.# UN Foundation in support of ICT4SOML. “Nigeria Health ICT Phase 2 Field Assessment.” Abuja, Nigeria; 2015. Available at: http://www.health.gov.ng/doc/FieldAssessment.pdf.
24.# UN Foundation in support of ICT4SOML. Assessing the Enabling Environment for ICTs for Health in Nigeria: A Landscape and Inventory. Abuja, Nigeria; 2014. Available at: http://www.health.gov.ng/doc/nigeria-Health-ICT-landscape-report.pdf.
25.# Mehl G, Labrique A. “Prioritizing integrated mHealth strategies for universal health coverage.” Science (80- ). 2014;345(no. 6202):1284-1287. doi:10.1126/science.1258926.
26.# Mehl G, Labrique A. “Prioritizing integrated mHealth strategies for universal health coverage.” Science (80- ). 2014;345(no. 6202):1284-1287. doi:10.1126/science.1258926.
27.# UN Development Group. “Results-Based Management Handbook.” 2010. Available at: http://www.un.cv/files/UNDG RBM Handbook.pdf.