WHO Drug Informationapps.who.int/medicinedocs/documents/s21014en/s21014en.pdf · Analyzen...
111
211 WHO Drug Information Vol. 27, No. 3, 2013 WHO Drug Information Quality and Safety of Medicines Falsified lamivudine/zidovudine/ nevirapine tablets: rapid identification using X-ray fluorescence technique 213 Safety and Efficacy Issues Rituximab: hepatitis B reactivation 218 Oral fluoroquinolones and retinal detachment 218 Hydroxyethyl starch solutions: kidney failure 219 Ketoconazole: fatal liver injury 219 Olmesartan medoxomil: enteropathy 220 Ado-trastuzumab emtansine: name confusion 220 Anticholinergics and cognitive impairment 221 Diclofenac : new safety advice 221 New recommendations for intravenous iron-containing medicines 222 Vemurafenib: DRESS syndrome 222 Mefloquine: risk of eye disorders 223 Mefloquine: risk of neurological and psychiatric effects 223 Calcitonin: changes to availability 223 Metoclopramide: changes to use 224 Glucagon-like-peptide-1 therapies: no immediate concern 224 Ergot derivatives: restricted use 225 Flupirtine-containing medicines: restricted use 225 Interim guidelines on bedaquiline for tuberculosis 226 Regulatory Action and News Operation Pangea VI: combating sale of unapproved medicines 227 SARA: System for Australian Recall Actions 227 Oral ketoconazole: suspension of marketing authorization 228 Advanced therapy approved for metastatic prostate cancer 228 Dabrafenib approved for metastatic melanoma 229 Calcitonin nasal spray: market withdrawal 229 Afatinib and companion test approved for late-stage lung cancer 229 Recent Publications, Information and Events Priority medicines for Europe and the world 231 HIV treatment recommendations 231 18th Model List of Essential Medicines and Model List for Children 232 International summit on medicines shortages 232 USAID Deliver Project: supply chain management 233 Consultation Documents The International Pharmacopoeia Aciclovir 234 Aciclovir for injection 240 Aciclovir tablets 244 Radiopharmaceuticals. General monograph 247 Radiopharmaceuticals. Safety considerations 258 Radiopharmaceuticals. Testing: additional guidance 259 Radiopharmaceuticals. Methods of analysis: R3, biological methods 259 Radiopharmaceuticals: specific monograph. Sodiumiodide ( 131 i) solution 262 Radiopharmaceuticals: specific monograph. Technetium ( 99M tc) exametazime complex injection 266 Radiopharmaceuticals: specific monograph.Thallous ( 201 tl) chloride injection 271 International Nonproprietary Names Recommended List No. 70 275 Contents
Transcript of WHO Drug Informationapps.who.int/medicinedocs/documents/s21014en/s21014en.pdf · Analyzen...

211
WHO Drug Information Vol. 27, No. 3, 2013
WHO Drug Information
Quality and Safety of MedicinesFalsified lamivudine/zidovudine/ nevirapine tablets: rapid identification using X-ray fluorescence technique 213
Safety and Efficacy IssuesRituximab: hepatitis B reactivation 218Oral fluoroquinolones and retinal detachment 218Hydroxyethyl starch solutions: kidney failure 219Ketoconazole: fatal liver injury 219Olmesartan medoxomil: enteropathy 220Ado-trastuzumab emtansine: name confusion 220Anticholinergics and cognitive impairment 221Diclofenac : new safety advice 221New recommendations for intravenous iron-containing medicines 222Vemurafenib: DRESS syndrome 222Mefloquine: risk of eye disorders 223Mefloquine: risk of neurological and psychiatric effects 223Calcitonin: changes to availability 223Metoclopramide: changes to use 224Glucagon-like-peptide-1 therapies: no immediate concern 224Ergot derivatives: restricted use 225Flupirtine-containing medicines: restricted use 225Interim guidelines on bedaquiline for tuberculosis 226
Regulatory Action and NewsOperation Pangea VI: combating sale of unapproved medicines 227SARA: System for Australian Recall Actions 227Oral ketoconazole: suspension of marketing authorization 228Advanced therapy approved for metastatic prostate cancer 228Dabrafenib approved for metastatic melanoma 229
Calcitonin nasal spray: market withdrawal 229Afatinib and companion test approved for late-stage lung cancer 229
Recent Publications, Information and EventsPriority medicines for Europe and the world 231HIV treatment recommendations 23118th Model List of Essential Medicines and Model List for Children 232International summit on medicines shortages 232USAID Deliver Project: supply chain management 233
Consultation DocumentsThe International PharmacopoeiaAciclovir 234Aciclovir for injection 240Aciclovir tablets 244Radiopharmaceuticals. General monograph 247Radiopharmaceuticals. Safety considerations 258Radiopharmaceuticals. Testing: additional guidance 259Radiopharmaceuticals. Methods of analysis: R3, biological methods 259Radiopharmaceuticals: specific monograph. Sodiumiodide (131i) solution 262Radiopharmaceuticals: specific monograph. Technetium (99Mtc) exametazime complex injection 266Radiopharmaceuticals: specific monograph.Thallous (201tl) chloride injection 271
International Nonproprietary NamesRecommended List No. 70 275
Contents

212
WHO Drug Information Vol. 27, No. 3, 2013
International Conference of Drug Regulatory Authorities (ICDRA)
The 16th ICDRA will be hosted by the Brazilian National Health Surveillance Agency (ANVISA)
Rio de Janeiro, Brazil 24 — 29 August 2014
http://www.anvisa.gov.br

213
WHO Drug Information Vol. 27, No. 3, 2013
Quality and Safety of MedicinesFalsified lamivudine/zidovudine/nevirapine tablets: rapid identification using X-ray fluorescence technique
On 22 September 2011, the World Health Organization (WHO) announced the discovery of falsified Zidolam-N® tablets in Kenya. These were labelled as manu-factured and supplied by Hetero, India (batch No. E100766). Later, medicines labelled as Hetero batches A9351, A9366 and E110467 were also confirmed to be falsified. Hetero further declared that batches E100766 and E110467 were never supplied to Kenya and that the quantities declared as batches A9351, A9357 and A9366 exceeded those actually manfactured. Falsified medicines labelled as batches A9366 and E100766 were sent to the Kenya National Drug Quality Control Laboratory and to Hetero for examination.
The test results were not conclusive in tracking the source of the falsification. Given this situation, WHO requested the China National Institutes for Food and Drug Control (NIFDC) to develop a rapid detection method to differentiate the authentic from the falsified medicines. The following is a description of testing methods and results.
Instrument usedThermo Scientific Model Nition XL3t XRF Analyzer®. Manufacturer: Thermo NITION Analyzen LLC.Model:XL3t970.Serial:82321.
Testing MethodInstrument settingPlastic mode, 50 kV excitation voltage, main filter measurement time set to 60s, error of measurement display set to ±1σ standard deviation (68.3% confidence).
Tablet testingSix tablets were randomly taken from each sample batch. For each test, two tablets were used and three tests were performed for one batch and tests were repeated the next day.
YIN Li-hui1 LI Jun-qing2 CHEN Jin-quan2 WANG Jun2 ZHANG Xue-bo1 YANG Mei1 ZHU Li1 ZHAO Yu1 XIAO Xin-yue1 JIN Shao-hong11National Institutes for Food and Drug Control, Beijing, China. 2Dongying Institute for Drug Control, Dongying, Shandong Province, China.
The X-ray fluorescence (XRF) technique was used to determine bromine (Br)concentration in lamivudine/zidovudine/nevirapine (Zidolam-N®) tablets from four-teen batches drawn from different sources. Results showed that Br concentration in falsified drugs was significantly higher than that in the authentic drugs. It was also found that Br concentration in the paper liner of the bottle caps containing the falsified drugs was elevated when compared to the liner from the container holding the authentic drug. In conclusion, falsified (Zidolam-N®) can be rapidly identified using the handheld, portable XRF instrument.

214
WHO Drug Information Vol. 27, No. 3, 2013
Packaging material
The bottle bottoms, bottle caps and the paper cap liner were determined.
Optimization of testing conditions
Testing conditions for bromine in tablets (See tables 1 and 2)
Condition aInstrument setting: Plastic mode, thickness correction enabled, main filter set to 60s measurement time, error of measurement set to display ±1σ standard deviation.
Condition bInstrument setting: Plastic mode, thickness correction disabled, main filter set to 60s measurement time, error of measurement set to display ±2σ standard deviation (95.5% confidence).
Condition cInstrument setting: Plastic mode, thickness correction disabled, main filter set to 90s measurement time, error of measurement set to display ±1σ standard deviation.
Results
Results of the packaging materials of samples tested are shown in Table 3.
Quality and Safety of Medicines
Sample source Batch No. Sample No.
Kenya, transfered to WHO A9366 A(Original package with E100766 B bottle) E110467 C
Kenya A9366 D(Nude tablets E100766 E without bottle) E110467 F
Hetero, India A9366 G (Nude tablets E100766 H without bottle) E110467 I
Hetero, IndiaControl sample not for sale A9351 J(Original package with bottle) A9357 K
WHO (originated Kenya) A9366 L(Original package E100766 M with bottle) E110467 N
Sample Information

215
WHO Drug Information Vol. 27, No. 3, 2013 Quality and Safety of Medicines
Sample Measured concentration of Br (mg/kg)
No. Condition a Condition b Condition c
A 13±1 15±1 16±1 B 20±1 23±1 25±1 C 34±1 43±2 42±1 D 16±1 19±1 19±1 E 14±1 18±1 18±1 F 8±1 10±1 10±1 G <3 <3 <3 H <3 <3 <3 I <3 <3 <3 J <3 <3 <3 K <3 <3 <3 L 12±1 17±1 15±1 M 71±1 89±2 90±1 N 44±1 54±2 51±1
Table 1. Results of tablet samples tested
Table 2. Results of tablet samples tested on different days
Sample Br (mg/kg) No. Day 1 Day 2
A 17±1 16±1 B 24±1 24±1 C 43±1 42±1 D 19±1 20±1 E 17±1 16±1 F 9±1 9±1 G <3 <3 H <3 <3 I <3 <3 J <3 <3 K <3 <3 L 17±1 17±1 M 89±1 88±1 N 57±1 57±1

216
WHO Drug Information Vol. 27, No. 3, 2013
Discussion
As seen from the data reported, Br concentrations detected in samples A, B, C, D, E, F, L, M and N are much higher than those in samples G, H, I, J and K which are below the instrument detection limit.
Note: When the instrument is set in plastic mode and the total testing time on the main filter is 30s, the detection limit for Br is 3 ppm.
Instrument repeatability was good.
Relative average deviations of the test results on the two consecutive days are all smaller than 6%.
Br was not detected in inner packages of samples D, E, F, G, H and I.
Br was not detected in the bottom, cap, and side wall of the plastic bottles containing samples A, B, C, J, K, L, M and N.
Br was not detected in the paper liner of the bottle cap of control samples J and K. However, the levels of Br detected in the paper liner of the bottle cap of suspected counterfeit samples A, B, C, L, M and N is relatively high.
Conclusion
An XRF technique was succssfuly used for rapid and non-destructive measurement of Br concentration in samples of tablets of medicines. A handheld XRF instrument employed in this study is simple to use and offers good repeatability and sensitivity for Br in medicinal drugs. It is suitable for rapid, positive authentication of lamivudine/zidovudine/nevirapine (Zidolam-N®) tablets using Br measurement as an indicator.
Quality and Safety of Medicines
Sample No. Bottle bottoms Bottle caps Paper cap liner
A <3 <3 56±2
B <3 <3 82+2
C <3 <3 94±2
J <3 <3 <3
K <3 <3 <3
L <3 <3 42±1
M <3 <3 56±2
N <3 <3 87±2
Table 3. Results of packaging material samples tested

217
WHO Drug Information Vol. 27, No. 3, 2013
References
1. Chou J, Clement G, Bursavich B et al. Rapid detection of toxic metals in non-crushed oyster shells by portable X-ray fluorescence spectrometry. Environmental pollution 2010; 158(6):2230.
2. Gupta S, Deep K, Jain L et al. X-ray fluorescence (XRF) set-up with a low power X-ray tube. Appl Radiat Isot 2010; 68(10):1922.
3. Smolek S, Streli C, Zoeger N et al. Improved micro x-ray fluorescence spectro-meter for light element analysis. Rev Sci Instrum 2010;81(5):053707.
4. Anderson DL. Analysis of beverages for Hg, As, Pb, and Cd with a field portable X-ray fluorescence analyzer. J AOAC Int 2010;93(2):683.
5. Luo Li-qiang Zhan Xiu-chu, Li Guo-hui. X-ray fluorescence spectrometer. Beijing, Chemical Industry Press 2008;5.
6. Tsuyumoto I, Maruyama Y. X-ray fluorescence analysis of hexavalent chromium using Kβ satellite peak observed as counterpart of X-ray absorption nearedge structure pre-edge peak. Anal Chem 2011; 83(19):7566.
7. Aranda PR, Moyano S, Martinez LD, De Vito IE. Determination of trace chromium(VI) in drinking water using X-ray fluorescence spectrometry after solid-phase extraction. Anal Bioanal Chem 2010;398(2):1043.
8. Yin Li-hui,Li Jun-qing,et al.Rapid screening of Cr in vacant capsule by X-ray fluorescence elemental analysis technology. Chin J Pharm Anal 2012;32(6):920.
9. Yin Li-hui,Li Jun-qing,et al.Rapid detection on Cr in gelatin by X-ray fluorescence elemental analysis technology. Chin J Pharm Anal 2012;32(7):1124.
10. Li Jun-qing, Yin Li-hui, et al.Preliminary discusion on X-ray fluorescence elemental analysis technology the rapid determination of Pb and As elements in cosmetics. Chin J Pharm Anal 2012;32(7):1129.
Quality and Safety of Medicines
218
WHO Drug Information Vol. 27, No. 3, 2013
Safety and Efficacy IssuesRituximab: hepatitis B reactivationCanada — Health Canada has informed healthcare professionals of updates to the recommendations for screening and management of hepatitis B virus reactivation in patients treated with rituximab (Rituxan®).
Rituximab is an anti-CD20 monoclonal antibody indicated in the treatment of non-Hodgkin lymphoma, chronic lymphocytic leukemia, rheumatoid arthritis, granulomatosis with polyangiitis (also known as Wegener granulomatosis) and microscopic polyangiitis.
Use of rituximab has been shown to be associated with reactivation of hepatitis B virus in seropositive patients. It is advised that all patients be screened for hepatitis B virus (HBV) before initiation of treatment. Rituximab is not to be used in patients with active hepatitis B viral disease.
Prior to starting treatment in HBV seropositive patients, consultation with a liver disease expert is recommended to determine ongoing monitoring of HBV reactivation and its management.
The use of rituximab has been associated with HBV reactivation in patients with positive HBV surface antigen (HBsAg+ve) and in those with negative HBV surface antigen plus positive anti-HB core antibody (HBsAg-ve/HBcAb+ve), particularly when administered in combination with corticosteroids or chemotherapy.
Reference: Health Canada. Medeffect Safety Alert, 29 July 2013 at http://www.hc-sc.gc.ca/dhp-mps/medeff/advisories-avis/index-eng
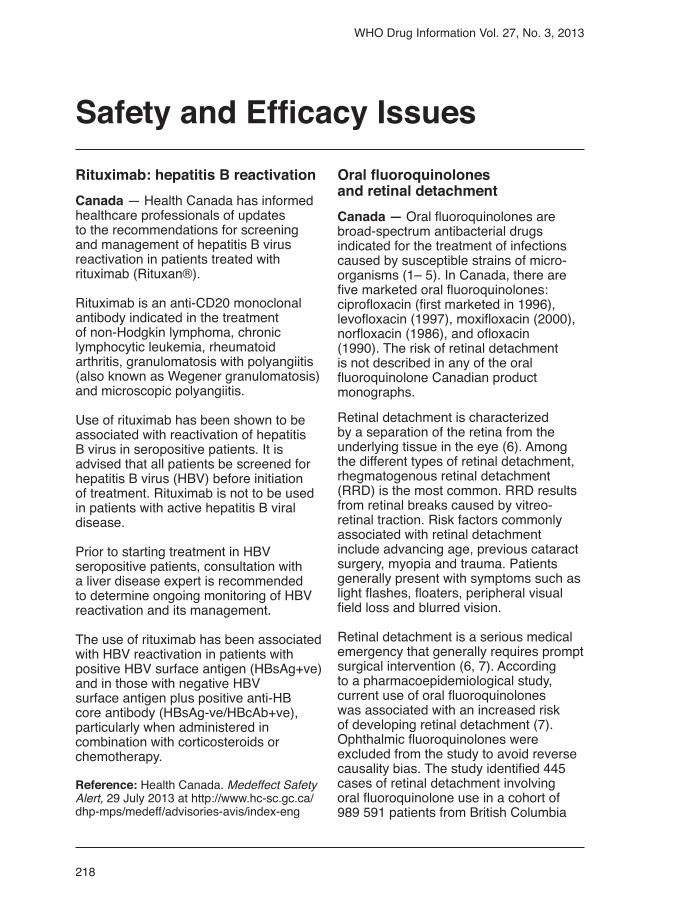
Oral fluoroquinolones and retinal detachmentCanada — Oral fluoroquinolones are broad-spectrum antibacterial drugs indicated for the treatment of infections caused by susceptible strains of micro-organisms (1– 5). In Canada, there are five marketed oral fluoroquinolones: ciprofloxacin (first marketed in 1996), levofloxacin (1997), moxifloxacin (2000), norfloxacin (1986), and ofloxacin (1990). The risk of retinal detachment is not described in any of the oral fluoroquinolone Canadian product monographs.
Retinal detachment is characterized by a separation of the retina from the underlying tissue in the eye (6). Among the different types of retinal detachment, rhegmatogenous retinal detachment (RRD) is the most common. RRD results from retinal breaks caused by vitreo-retinal traction. Risk factors commonly associated with retinal detachment include advancing age, previous cataract surgery, myopia and trauma. Patients generally present with symptoms such as light flashes, floaters, peripheral visual field loss and blurred vision.
Retinal detachment is a serious medical emergency that generally requires prompt surgical intervention (6, 7). According to a pharmacoepidemiological study, current use of oral fluoroquinolones was associated with an increased risk of developing retinal detachment (7). Ophthalmic fluoroquinolones were excluded from the study to avoid reverse causality bias. The study identified 445 cases of retinal detachment involving oral fluoroquinolone use in a cohort of 989 591 patients from British Columbia

219
WHO Drug Information Vol. 27, No. 3, 2013
who visited an ophthalmologist between January 2000 and December 2007. Further research is needed to confirm whether there is a potential association between retinal detachment and fluoro-quinolones as well as to clarify the mechanism of action.
As of 31 December 2012, Health Canada received one report of retinal detachment suspected of being associated with the use of an oral fluoroquinolone. The report described a 52-year-old woman who experienced retinal detachment after a course of ciprofloxacin prescribed to treat a bladder infection. Limited evidence linking retinal detachment to oral fluoroquinolones may explain the low level of reporting to Health Canada.
Extracted from the Canadian Adverse Drug Reactions Newsletter, Volume 23, number 3, 2013.
References
1. Cipro (ciprofloxacin) [product monograph]. Toronto (ON): Bayer Inc.; 2012.
2, Levaquin (levofloxacin) [product monograph]. Toronto (ON): Janssen Inc.; 2012.
3. Avelox (moxifloxacin) [product monograph]. Toronto (ON): Bayer Inc.; 2012.
4. CO Norfloxacin (norfloxacin) [product monograph]. Mississauga (ON): Cobalt Pharmaceuticals Company; 2010.
5. Ofloxacin (ofloxacin) [product monograph]. Toronto (ON): AA Pharma Inc.; 2010.
6. Gariano RF, Kim CH. Evaluation and management of suspected retinal detachment. Am Fam Physician 2004;69(7):1691-8. [PubMed]
7. Etminan M, Forooghian F, Brophy JM et al. Oral fluoroquinolones and the risk of retinal detachment. JAMA 2012;307(13):1414-9.
http://www.hc-sc.gc.ca/dhp-mps/medeff/advisories-avis/index-eng.php?cat=5
Hydroxyethyl starch solutions: kidney failureCanada — Health Canada has informed healthcare professionals of updated information concerning blood volume expanders containing hydroxyethyl starch (HES) solutions recommending that these products no longer be used in critically ill patients with certain health conditions.
HES solutions are used to replace lost blood in patients who are critically ill and experience a sudden drop in blood pressure.
Specifically, HES solutions should not be used:
• In patients with sepsis.
• In patients with severe liver disease.
• In certain types of patients with impaired kidney function.
Some recent studies have compared HES with other blood volume expanders in critically ill patients with sepsis. These studies suggest that patients treated with HES are at a higher risk of kidney failure or death.
Reference: Health Canada. Information Update, 24 June 2013 at http://www.healthy canadians.gc.ca/recall-alert-rappel-avis/hc-sc/2013/34299a-eng.php
Ketoconazole: fatal liver injuryUnited States of America — The Food and Drug Administration (FDA) is taking several actions related to ketoconazole (Nizoral®) oral tablets. These include limiting use, warning of severe liver injuries and adrenal gland problems and advising that it can lead to harmful drug interactions with other medications.
The FDA has approved label changes and added a new medication guide to address these safety issues. As a result, ketoconazole oral tablets should not be considered as first-line treatment for any
Safety and Efficacy Issues

220
WHO Drug Information Vol. 27, No. 3, 2013
patients taking olmesartan develop these symptoms and no other cause is found, the drug should be discontinued, and therapy with another antihypertensive started.
Olmesartan medoxomil is an angiotensin II receptor blocker (ARB) approved for the treatment of high blood pressure, alone or with other antihypertensive agents, and is one of eight marketed ARB drugs. Sprue-like enteropathy has not been detected with ARB drugs other than olmesartan.
Reference: FDA Drug Safety Communication, 3 July 2013 at http://www.fda.gov/Drugs/DrugSafety/ucm359477.htm
Ado-trastuzumab emtansine: name confusionUnited States of America — The Food and Drug Administration (FDA) is alerting healthcare professionals that the use of the incorrect nonproprietary name for the breast cancer drug ado-trastuzumab emtansine (Kadcyla®) in some medication-related electronic systems poses a risk of mix-up with trastuzumab (Herceptin®) and may result in medication errors. The dosing and treatment schedules for ado-trastuzumab emtansine and trastuzumab, another breast cancer drug, are quite different, so confusion between these products could lead to dosing errors and potential harm to patients.
The FDA-approved nonproprietary name ado-trastuzumab emtansine should be used. However, some third-party publications, compendia references, health information systems (e.g., electronic health record systems and systems used for pharmacy prescription processing, wholesaler ordering, pharmacy ordering, etc.) and sites on the Internet are incorrectly using the United States Adopted Name (USAN), which is “trastuzumab emtansine,” and omitting the “ado” prefix and hyphen. Use of this truncated version may cause confusion.
fungal infection. Ketoconazole should be used for the treatment of certain fungal infections, known as endemic mycoses, only when alternative antifungal therapies are not available or tolerated.
Topical formulations of ketoconazole have not been associated with liver damage, adrenal problems, or drug interactions.
Ketoconazole tablets can cause liver injury, which may potentially result in liver transplantation or death. Serious liver damage has occurred in patients receiving high doses of ketoconazole for short periods of time as well as those receiving low doses for long periods. Some of these patients had no obvious risk factors for liver disease.
Ketoconazole tablets may cause adrenal insufficiency and healthcare professionals should monitor adrenal function in patients who have existing adrenal problems or in patients who are under prolonged periods of stress such as those who have had a recent major surgery or who are under intensive care in the hospital. Ketoconazole tablets may interact with other drugs and result in serious and potentially life-threatening outcomes.
Reference: FDA Drug Safety Communication, 26 July 2013 at http://www.fda.gov/Drugs/DrugSafety/ucm362415.htm
Olmesartan medoxomil: enteropathyUnited States of America — The Food and Drug Administration (FDA) is warning that the blood pressure drug olmesartan medoxomil (Benicar®, Benicar HCT®, Azor®, Tribenzor®, and generics) can cause sprue-like enteropathy.
Symptoms include severe, chronic diarrhoea with substantial weight loss. The enteropathy may develop months to years after starting olmesartan, and sometimes requires hospitalization. If
Safety and Efficacy Issues

221
WHO Drug Information Vol. 27, No. 3, 2013
It is important for drug information content publishers to identify drug products by the FDA-approved proprietary (brand) and nonproprietary names that are used in FDA-approved drug labels.
Reference: FDA Drug Safety Communication, 6 May 2013 at http://www.fda.gov/Drugs/DrugSafety/ucm350733.htm Anticholinergics and cognitive impairmentAustralia — Anticholinergics are a class of drug that blocks muscarinic actions of acetylcholine with a wide range of effects. Drugs with definite anticholinergic properties include antiemetics (prometha-zine®), anti-Parkinson agents (benztro-pine), gastrointestinal spasmolytics (propantheline), bladder spasmolytics (oxybutinin, tolterodine) and anti-depressants (imipramine) (1).
Precautions for anticholinergics include using with caution in elderly patients who are more sensitive to adverse events associated with these drugs. In particular, confusion can be precipitated or worsened. When used in elderly patients, anticholinergics should be initiated at a low dose and increased slowly to the lowest effective dose.
Two recent long-term studies examined cognitive impairment in older patients.
One of those studies followed 13 004 patients aged 65 and older for two years (2). The other study followed 1652 African American subjects over 70 years of age, for six years (3). These patients experienced a 1.43 times increased risk of developing cognitive impairment compared to patients not taking a drug with definite anticholinergic properties. Also, the risk increased with the number of anticholinergics being used.
Consideration should be given to routine measurement of cognitive function in older patients taking drugs
with anticholinergic properties for any indication, including non-nervous system indications. It may be possible to lower the anticholinergic burden by replacing such drugs with alternatives that do not have anticholinergic properties.
Extracted from Medicines Safety Update, Volume 4, Number 3, June 2013 at http://www.tga.gov.au/hp/msu-2013-03.htm
References
1. Boustani M, Campbell N, Munger S, Maidment I, Fox C. Impact of anticholinergics on the aging brain: a review and practical application. Aging Health 2008;4:311–20.
2. Fox C, Richardson K, Maidment ID, Savva GM, Matthews FE, Smithard D, et al. Anticholinergic medication use and cognitive impairment in the older population: the medical research council cognitive function and ageing study. J Am Geriatr Soc 2011;59:1477–83.
3. Campbell NL, Boustani MA, Lane KA, Gao S, Hendrie H, Khan BA, et al. Use of anticholinergics and the risk of cognitive impairment in an African American population. Neurology 2010;75:152–9.
Diclofenac : new safety adviceEuropean Union — The Coordination Group for Mutual Recognition and Decentralized Procedures – Human (CMDh) has endorsed new safety advice for diclofenac-containing medicines in the form of capsules, tablets, suppositories or injections. The new advice aims to minimize cardiovascular risk.
This follows a recent review by the European Medicines Agency’s Pharmaco-vigilance Risk Assessment Committee (PRAC), which found that the effects of systemic diclofenac are similar to those of selective COX-2 inhibitors particularly when diclofenac is used at a high dose and for long-term treatment. The PRAC therefore recommended that the same precautions already in place should be applied to diclofenac.
Safety and Efficacy Issues

222
WHO Drug Information Vol. 27, No. 3, 2013
these medicines are greater than their risks, provided that adequate measures are taken to minimize the risk of allergic reactions.
All intravenous iron medicines have a small risk of causing allergic reactions which can be life-threatening if not treated promptly. The Committee therefore concluded that Iron preparations should only be given in an environment where resuscitation facilities are available. In addition, a test dose is no longer recommended but instead caution is warranted with every dose of intravenous iron that is given, even if previous administrations have been well tolerated.
The CHMP also considered that intravenous iron medicines should not be used during pregnancy unless clearly necessary. Treatment should be confined to the second or third trimester, provided the benefits of treatment clearly outweigh the risks to the unborn baby.
The review of intravenous iron medicines was triggered by the French medicines agency, the National Agency for the Safety of Medicine and Health Products (ANSM)
Reference: European Medicines Agency. Press Release, 28 June 2013 at http://www.ema.europa.eu ema
Vemurafenib: DRESS syndromeSingapore — Healthcare professionals have been informed of the risk of RAS-mutant malignancy progression and DRESS syndrome associated with vemurafenib (Zelboraf®). The risk of RAS-mutant malignancy progression is based on a single report from a literature article about a 76 year-old male patient with stage IV melanoma in whom accelerated growth of a pre-existing NRAS-mutated chronic myelomonocytic leukemia (CMML) was observed shortly after initiation of treatment with
Clinical-trial and epidemiological data consistently point towards an increased risk of arterial thrombotic events associated with the use of diclofenac, particularly at high dose (150 mg daily) and in long-term treatment.
Use of diclofenac is contraindicated in patients with established congestive heart failure, ischaemic heart disease, peripheral arterial disease or cerebrovascular disease.
Patients with significant risk factors for cardiovascular events (e.g., hypertension, hyperlipidaemia, diabetes mellitus, smoking) should only be treated with diclofenac after careful consideration.
References
1. Krum H, Swergold G, Gammaitoni A, Peloso PM, Smugar SS, Curtis SP, Brater DC, Wang H, Kaur A, Laine L, Weir MR, Cannon CP. Blood pressure and cardiovascular outcomes in patients taking non-steroidal anti-inflammatory drugs. Cardiovasc Ther. 2012;30(6): 342–350.
2. Coxib and Traditional NSAID Trialists’ Collaboration. Vascular and upper gastro-intestinal effects of non-steroidal anti-inflam-matory drugs: meta-analyses of individual participant data from randomised trials. Lancet, Early Online Publication, 30 May 2013 doi:10.1016/S0140-6736(13)60900-9.
3. European Medicines Agency. Press Release, 28 June 2013 at http://www.ema.europa.eu ema
New recommendations for intravenous iron-containing medicines European Union — The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has completed its review of intravenous iron-containing medicines used to treat iron deficiency and anaemia associated with low iron levels. The CHMP concluded that the benefits of
Safety and Efficacy Issues

223
WHO Drug Information Vol. 27, No. 3, 2013
Mefloquine: risk of neurological and psychiatric effectsUnited States of America — The Food and Drug Administration (FDA) is advising the public about strengthened and updated warnings regarding neurologic and psychiatric side effects associated with the antimalarial drug mefloquine hydrochloride.
Neurological side effects can include dizziness, loss of balance, or ringing in the ears. The psychiatric side effects can include feeling anxious, mistrustful, depressed, or having hallucinations.
Neurological side effects can occur at any time during drug use and can last for months to years after the drug is stopped, or can be permanent.
Reference: FDA Safety Announcement, 29 July 2013 at http://www.fda.gov/Drugs/DrugSafety/ucm362227.htm
Calcitonin: changes to availabilityCanada — Health Canada has advised of important changes to the availability and recommended conditions of use of drugs containing calcitonin. Calcitonin is used as a nasal spray to treat osteoporosis in postmenopausal women, and as an injection to treat Paget disease and hypercalcaemia.
A safety review conducted by Health Canada has concluded that there is a slightly increased risk of cancer associated with prolonged use. A review of the benefits and risks of the nasal spray products found that there was not enough evidence of benefit to continue using calcitonin nasal sprays in treating osteoporosis.
As a result of these reviews, calcitonin nasal spray products will no longer be authorized for sale in Canada as of 1 October 2013.
vemurafenib. Based on its mechanism of action, vemurafenib may cause progression of cancers associated with RAS mutations. Vemurafenib should be used with caution in patients with prior or concurrent cancers associated with RAS mutations.
In addition, cases of DRESS syndrome have been reported with the use of vemurafenib with onset ranging from 7 to 25 days. Treatment should be permanently discontinued if a patient develops DRESS syndrome. The package insert for Zelboraf® will be updated to reflect the new safety information.
Reference: Health Sciences Authority, HSA Safety Update. Information/Communication from Roche. Risk of RAS-Mutant Malignancy Progression and Drug Rash with Eosinophilia and Systemic Symptoms (DRESS Syndrome) associated with Zelboraf® (vemurafenib), 31 July 2013 at http://www.hsa.sg and http://www.hpp.moh.gov.sg/.
Mefloquine: risk of eye disorders Singapore — Healthcare professionals have been informed of an increased risk of eye disorders including cataract, retinal disorders and optic neuropathy during or after treatment with mefloquine (Lariam®). These eye disorders can present with visual impairment and blurred vision. Increased risk of eye disorders is based on outcomes of a review of available evidence from non-clinical studies, the Roche global drug safety database and published literature.
Adverse events may occur or persist up to several weeks after discontinuation of Lariam® due to the long half-life of the drug. The package insert will be updated to reflect the new safety information.
Reference: Health Sciences Authority, HSA Safety Update. Information/Communication from Roche, 25 July 2013 at http://www.hsa.sg and http://www.hpp.moh.gov.sg/.
Safety and Efficacy Issues

224
WHO Drug Information Vol. 27, No. 3, 2013
Calcitonin injectable products will continue to be authorized for sale in Canada. The benefits of these products are considered to outweigh the risks when the product is used as directed. However, the labels for calcitonin injectable products are being updated to include a new warning and to recommend that treatment with calcitonin solution for injection be limited to the shortest possible time, using the minimum effective dose. Treatment of symptomatic Paget disease with calcitonin medicine should be limited to patients who are unable to use other treatments.
Reference: Health Canada. Medeffect Safety Alert, 31 July 2013 at http://www.hc-sc.gc.ca/dhp-mps/medeff/advisories-avis/index-eng and http://healthycanadians.gc.ca/recall-alert-rappel-avis/hc-sc/2013/34781a-eng.php
Metoclopramide: changes to use European Union —The European Medicines Agency’s Committee on Medicinal Products for Human Use (CHMP) has recommended changes to the use of metoclopramide-containing medicines, including restricting the dose and duration of use to minimize the known risks of potentially serious neurological side effects.
Metoclopramide-containing medicines have been authorized separately in individual Member States with differing licensed indications such as nausea and vomiting or gastrointestinal motility disorders.
The review of metoclopramide was carried out at the request of the French medicines regulatory agency (ANSM), following continued safety concerns over side effects and concerns over efficacy. The review confirmed the known risks of neurological effects such as short-term extrapyramidal disorders. The risk of acute neurological effects is higher in children, although tardive dyskinesia is reported more often in the elderly, and the risk is increased at high doses or
with long-term treatment. The evidence indicated that these risks outweighed the benefits of metoclopramide in conditions requiring long-term treatment. There have also been very rare cases of serious effects on the heart or circulation, particularly after injection.
The Committee recommended that metoclopramide should only be prescribed for use up to five days, that it should not be used in children below one year of age and that in children over one year of age, it should only be used as a second-choice treatment for the prevention of delayed nausea and vomiting after chemotherapy and for the treatment of post-operative nausea and vomiting.
In adults, it may be used for the prevention and treatment of nausea and vomiting such as that associated with chemotherapy, radiotherapy, surgery and in the management of migraine. In addition, the maximum recommended doses in adults and children should be restricted, and higher strength formulations removed from the market.
Reference: European Medicines Agency. Press Release, 28 June 2013 at http://www.ema.europa.eu ema
Glucagon-like-peptide-1 therapies: no immediate concernEuropean Union — The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has finalized a review of GLP-1-based diabetes therapies. The Committee concluded that presently available data do not confirm recent concerns over an increased risk of pancreatic adverse events with these medicines.
The rise of type-2 diabetes is a major public-health challenge. GLP-1-based therapies are effective treatments for type-2 diabetes and add to the available medication options. The term
Safety and Efficacy Issues

225
WHO Drug Information Vol. 27, No. 3, 2013
problems with memory and sensation, or to prevent migraine headaches, since the risks are greater than the benefits in these indications. A review of data showed an increased risk of fibrosis and ergotism.
Ergot derivatives indicated for these conditions will have their marketing authorizations suspended. In some EU Member States, ergot derivatives are also authorized for other indications: dementia, including Alzheimer disease, and treatment of acute migraine headache. They will remain authorized for use in those indications.
The review was initiated due to concerns identified by the French National Agency for the Safety of Medicine and Health Products (ANSM) in a national pharmacovigilance review in 2011.
Fibrosis can be a serious, sometimes fatal disease. The CHMP noted that there is a plausible mechanism by which ergot derivatives could cause fibrosis and ergotism. Given that the evidence for benefit in these indications was very limited, the CHMP concluded that the benefits in the concerned indications did not outweigh the risk of fibrosis and ergotism.
Reference: European Medicines Agency. Press Release, 28 June 2013 at http://www.ema.europa.eu
Flupirtine-containing medicines: restricted useEuropean Union — The Coordination Group for Mutual Recognition and Decentralized Procedures – Human (CMDh) has endorsed new recommendations to restrict the use of oral flupirtine medicines and suppositories. These medicines should now only be used for treating acute pain in adults who cannot use other painkillers, such as non-steroidal anti-inflammatory drugs (NSAIDs) and weak opioids and
‘GLP-1-based therapies’ comprises two classes of medicines: glucagon-like-peptide-1 (GLP-1) agonists and dipeptidylpeptidase-4 (DPP-4) inhibitors.
A review was initiated following publication of a study that suggested an increased risk of pancreatitis and pancreatic-duct metaplasia in patients with type-2 diabetes treated with GLP-1-based therapies. Following the review of the publication and consultation of a panel of experts, the CHMP considered that the study itself had a number of methodological limitations which preclude a meaningful interpretation of the results.
These medicines already carry warnings in their product information but the CHMP considered that there would be value in harmonizing the wording to provide consistent advice.
Two large independent studies funded by the European Commission have been under way since 2011 to study the risk profile of diabetes treatments in general. First results of these studies are expected in 2014.
References
1. Butler AE, Campbell-Thompson M, Gurlo T et al. Marked expansion of exocrine and endocrine pancreas with incretin therapy in humans with increased exocrine pancreas dysplasia and the potential for glucagon-producing neuroendocrine tumors. Diabetes 2013;62(7): 2595–2604.
2. European Medicines Agency. Press Release, 26 July 2013 at http://www.ema.europa.eu
Ergot derivatives: restricted useEuropean Union — The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended restricting the use of medicines containing ergot derivatives. These medicines should no longer be used to treat several conditions involving blood circulation problems or
Safety and Efficacy Issues

226
WHO Drug Information Vol. 27, No. 3, 2013
treatment should not last longer than two weeks.
Patient liver function should be checked after each full week of treatment and treatment should be stopped if the patient has any signs of liver problems. Flupirtine must also not be used in patients with pre-existing liver disease or alcohol abuse problems or in patients taking other medicines known to cause liver problems.
The recommendations follow a review by the European Medicines Agency’s Pharmacovigilance Risk Assessment Committee (PRAC). In addition to oral medicines and suppositories, the review also covered injectable flupirtine medicines which were being given as a single injection for pain following surgery. The PRAC concluded that the benefits of injectable flupirtine continue to outweigh their risks when used in this way.
Flupirtine is a non-opioid used to treat pain, such as that associated with muscle tension, cancer, menstrual and pain following orthopaedic surgery or injuries.It was first introduced as an alternative painkiller to opioids and NSAIDs. Subsequently, multiple other actions such as muscle relaxation were identified. Flupirtine works as a selective neuronal-potassium-channel opener.
Reference: European Medicines Agency. Press Release, 28 June 2013 at http://www.ema.europa.eu
Interim guidelines on bedaquiline for tuberculosisThe World Health Organization has issued interim guidance on the use of the anti-TB medicine, bedaquiline, which received accelerated approval by the US Food and Drug Administration on 31 December 2012. In view of the urgent need to combat multidrug-resistant TB (MDR-TB) with improved drugs, WHO has provided recommendations based on clinical trial data.
The MDR-TB epidemic registered 310 000 new cases in 2011. However, only 19% of people thought to be infected are receiving some kind of treatment. It is hoped that bedaquiline — which has been shown in trials to be potentially effective against Mycobacterium tuber-culosis — could become a powerful tool in much-needed treatment regimens that will be significantly shorter, more effective and less toxic than the current regimen which involves a two-year course of up to 20 pills per day and eight months of daily injections.
Reference: World Health Organization. Inte-rim guidance on the use of bedaquiline to treat MDR-TB. http://www.who.int/tb/challenges/mdr/bedaquiline/en/index.html
Spontaneous monitoring systems are useful in detecting signals of relatively rare, serious or unexpected adverse drug reactions. A signal is defined as “reported information on a possible causal relationship between an adverse event and a drug, the relationship being unknown or incompletely documented pre-viously. Usually, more than a single report is required to generate a signal, depending upon the seriousness of the event and the quality of the information”. All signals must be vaidated before any regulatory decision can be made.
Safety and Efficacy Issues

227
WHO Drug Information Vol. 27, No. 3, 2013
Regulatory Action and NewsOperation Pangea VI: combating sale of unapproved medicines
United States of America — The Food and Drug Administration and international regulatory and law enforcement agencies have taken action against more than 9600 web sites that illegally sell potentially dangerous, unapproved prescription medicines to consumers. This action includes issuance of regulatory warnings and seizure of offending web sites and over 41 million US dollars’ worth of illegal medicines worldwide. The action occurred as part of the 6th annual International Internet Week of Action (IIWA), a global cooperative effort to combat the online sale and distribution of potentially counterfeit and illegal medical products. The goal of Pangea VI — which involves law enforcement, customs, and regulatory authorities from 99 countries — was to identify the makers and distributors of illegal drug products and medical devices and remove these products from the supply chain.
As part of this international effort, the FDA Office of Criminal Investigations, in coordination with the United States Attorney’s Office for the District of Colorado, seized and shut down 1677 illegal pharmacy web sites. The effort ran from 18–25 June 2013.
Many of these web sites appeared to be operating as a part of an organized criminal network that falsely purported to be “Canadian Pharmacies.” These web sites displayed fake licences and certifications to convince U.S. consumers to purchase drugs they advertised as “brand name” and “FDA approved.” The drugs collected as part of Operation Pangea were not from Canada, and were neither brand name nor FDA approved.
These web sites also used certain major U.S. pharmacy retailer names to trick consumers into believing an affiliation existed. Reference: FDA News Release, 27 June 2013 at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm358794.htm
SARA: System for Australian Recall ActionsAustralia — The Therapeutic Goods Administration (TGA) recently launched the System for Australian Recall Actions (SARA) — an online, searchable data base of recall actions for therapeutic goods undertaken in Australia.
Health professionals are encouraged to use SARA, along with other resources on the TGA website, such as the Database of Adverse Event Notifications and the alerts web page, to access valuable information on medicines safety.
A recall action is a regulatory action taken for a therapeutic good supplied in Australia to resolve issues or deficiencies relating to safety, quality, efficacy or performance. Recall actions can be recalls, recalls for product correction or hazard alerts. Not all recall actions result in a product being removed from the market, for example hazard alerts may be issued in cases involving implantable devices, and corrections may be undertaken for products that have software issues.
SARA includes recall actions for a range of therapeutic goods including prescription medicines, over-the-counter medicines, complementary medicines, medical devices including

228
WHO Drug Information Vol. 27, No. 3, 2013Regulatory Action and News
Committee also concluded that the clinical benefit of oral ketoconazole is uncertain as data on its effectiveness are limited and do not meet current standards, and alternative treatments are available.
Topical formulations of ketoconazole can continue to be used as the amount of ketoconazole absorbed throughout the body is very low with these formulations.
References
1. García Rodríguez LA, Duque A, Castellsague J, Pérez-Gutthann S, Stricker BHC. A cohort study on the risk of acute liver injury among users of ketoconazole and other antifungal drugs. Br J Clin Pharmacol 1999; 48(6): 847-852.
2. European Medicines Agency. Press Release, 26 July 2013 at http://www.ema.europa.eu ema/index.jsp?curl=pages/news_and_events/news/2013/07/news_detail_001855.
Advanced therapy approved for metastatic prostate cancer European Union — The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended granting a marketing authorization for a new advanced-therapy medicinal product (ATMP). Provenge® is recommended for the treatment of asymptomatic or minimally symptomatic metastatic castrate-resistant prostate cancer in male adults in whom chemotherapy is not yet clinically indicated.
ATMPs are innovative medicines that are derived from gene therapy, cell therapy or tissue engineering. The CHMP recommendation follows the draft opinion of the Committee for Advanced Therapies (CAT), the Agency’s expert committee for ATMPs.
Provenge® is a cellular immunotherapy designed to induce an immune response
in vitro diagnostic medical devices, and biologicals.
The data base holds information on all recall actions that have been undertaken in Australia since 1 July 2012.
SARA has been launched as part of the TGA’s commitment to improve transparency, as well as trust and confidence in the safety and quality of therapeutic goods and regulatory processes.
Reference: Medicines Safety Update, Volume 4, Number 3, June 2013 at http://www.tga.gov.au/hp/msu-2013-03.htm
Oral ketoconazole: suspension of marketing authorizationEuropean Union —The European Medicines Agency’s Committee on Medicinal Products for Human Use (CHMP) has recommended that the marketing authorizations of oral ketoconazole-containing medicines should be suspended throughout the European Union (EU). The CHMP concluded that the risk of liver injury is greater than the benefits in treating fungal infections.
Patients currently taking oral ketocon-azole for fungal infections should make a non-urgent appointment with their doctor to discuss suitable alternative treatments. Doctors should no longer prescribe oral ketoconazole and should review treatment options.
The EU-wide review of oral ketoconazole was triggered by the suspension of the medicine in France. Having assessed the available data, the CHMP concluded that liver injury with oral ketoconazole was higher than with other antifungals. The CHMP was concerned that reports of liver injury occurred early after starting treatment with recommended doses and it was not possible to identify measures to adequately reduce this risk. The

229
WHO Drug Information Vol. 27, No. 3, 2013 Regulatory Action and News
against prostate cancer cells. It uses immune cells that are extracted from and treated outside the patient’s body so that when they are infused back into the patient they trigger an immune response directed against an antigen found in metastasized cancer cells. Provenge® has been shown to improve the overall survival by 4.1 months over placebo in clinical trials.
Reference: European Medicines Agency. Press Release, 28 June 2013 at http://www.ema.europa.eu ema http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2013/06/news_detail_001835.jsp&mid=WC0b01ac058004d5c128/06/2013
Dabrafenib approved for metastatic melanomaEuropean Union —The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended marketing authorization for dabrafenib (Tafinlar®) for the treatment of adult patients with advanced unresectable or metastatic melanoma expressing a BRAF V600 gene mutation.
The therapeutic landscape for the treatment of metastatic melanoma in the European Union has changed significantly in recent years with the granting of marketing authorizations for new targeted active agents: one of them, the monoclonal antibody ipilimumab, targets a molecule found on the surface of T cells and is thought to inhibit immune responses; another agent, vemurafenib, is a first-in-class protein kinase inhibitor, inhibiting the BRAF serine-threonine kinase with a genetic mutation at position 600 (BRAF V600E).
Mutations of the protein kinase BRAF have been identified in about half of patients with metastatic melanoma, with the BRAF V600E mutation found in about 80 to 90% of these. These mutations cause the cell to make an abnormal
protein that promotes cancer growth. By blocking the action of this abnormal protein, BRAF inhibitors help slow down the growth and spread of tumours bearing the BRAF V600 mutation.
Reference: European Medicines Agency. Press Release, 28 June 2013 at http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2013/06/news
Calcitonin nasal spray: market withdrawal Canada — Health Canada has advised of the market withdrawal of all synthetic calcitonin nasal spray products (Mia-calcin®, Sandoz Calcitonin® and Apo-calcitonin®) with effect 1 October 2013. All three products are authorized in Canada for the treatment of post-menopausal osteoporosis in females five years post menopause with low bone mass relative to healthy pre-menopausal females.
Health Canada has concluded, in light of a newly identified risk of cancer, that the benefit-risk profile for the treatment of postmenopausal osteoporosis is no longer considered favourable. As of 3 July 2013, manufacturers have ceased the sale of synthetic calcitonin nasal spray products.
Reference: Health Canada Advisory, 31 July 2013 at http://healthycanadians.gc.ca/recall-alert-rappel-avis/hc-sc/2013/34781a-eng.php
Afatinib and companion test approved for late-stage lung cancer
United States of America — The Food and Drug Administration (FDA) has approved afatinib (Gilotrif®) for patients with late stage (metastatic) non-small cell lung cancer (NSCLC) whose tumours express specific types of epidermal growth factor receptor (EGFR) gene mutations, as detected by an FDA-approved test.

230
WHO Drug Information Vol. 27, No. 3, 2013Regulatory Action and News
In May 2013, the FDA approved erlotinib (Tarceva®) for first-line treatment of patients with NSCLC and a new indication was approved concurrently with the cobas EGFR Mutation Test® to identify patients with tumours expressing the EGFR gene mutations.
Common side effects of Gilotrif® include diarrhoea, skin breakouts that resemble acne, dry skin, pruritus, inflammation of the mouth, paronychia, decreased appetite, decreased weight, cystitis, nose bleed, runny nose, fever, eye inflammation and hypokalemia. Serious side effects include diarrhoea that can result in kidney failure and severe dehydration, severe rash, lung inflammation and liver toxicity. Reference: FDA News Release, 12 July 2013 at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm360499.htm
Lung cancer is the leading cause of cancer-related death among men and women. About 85 percent of lung cancers are NSCLC, making it the most common type of lung cancer. EGFR gene mutations are present in about 10 percent of NSCLC, with the majority of these gene mutations expressing EGFR exon 19 deletions or exon 21 L858R substitution. Afatinib is a tyrosine kinase inhibitor blocking proteins that promote the development of cancerous cells. It is intended for patients whose tumours express the EGFR exon 19 deletions or exon 21 L858R substitution gene mutations. Afatinib is being approved concurrently with the therascreen EGFR RGQ PCR Kit®, a companion diagnostic that helps determine if a patient’s lung cancer cells express the EGFR mutations.

231
WHO Drug Information Vol. 27, No. 3, 2013
Priority medicines for Europe and the worldWorld Health Organization — For the first time, EU countries have more people over 65 years of age than under 15 years of age. Echoing the trend seen in Europe, much of the rest of the world is moving in a similar direction. Priority medicines for Europe and the world 2013 update calls for pharmaceutical researchers to adjust their research and development efforts to account for this shifting demography.
The report focuses on pharmaceutical gaps, where treatment for a disease or condition may soon become ineffective, are not appropriate for the target patient group, does not exist, or are not suffi-ciently effective. This report is an update to the 2004 version and is a collabora-tive product of experts from WHO, EU Member States, industry, academia and other interested stakeholders including patients.
Reference: WHO Press Release, 16 July 2013 at http://www.who.int/mediacentre/news/releases/2013/ageing_priority_medi-cines_20130716/en/index.html
HIV treatment recommendationsWorld Health Organization — The new WHO HIV treatment guidelines recom-mend offering antiretroviral therapy (ART) earlier. Recent evidence indicates that earlier ART will help people with HIV to live longer, healthier lives, and substanti-ally reduce the risk of transmitting HIV to others.
Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection encourage all
countries to initiate treatment in adults living with HIV when their CD4 cell count falls to 500 cells/mm³ or less. WHO has based its recommendation on evidence that treating people with HIV earlier, with safe, affordable, and easier-to-manage medicines can both keep them healthy and lower the amount of virus in the blood, which reduces the risk of transmis-sion.
The new recommendations also propose providing antiretroviral therapy to all HIV positive children under five years of age, pregnant and breastfeeding women with HIV, and all HIV-positive partners where one partner in the relationship is uninfec-ted. WHO continues to recommend that all people with HIV with active tubercu-losis or with hepatitis B disease receive antiretroviral therapy.
Another new recommendation is to offer all adults starting to take ART the same daily single fixed-dose combination pill. The recommended treatment is now a combination of three antiretroviral drugs: tenofovir and lamivudine (or emtricita-bine) and efavirenz, as a single pill, given once daily.
If countries can integrate these changes within their national HIV policies, and back them up with the necessary re-sources, they will see significant health benefits at the public health and individual level. WHO is also encouraging countries to enhance the ways they deliver HIV ser-vices, for example by linking them more closely with other health sectors.
Reference: WHO News Release, 30 June 2013. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. http://www.who.int/
Recent Publications, Information and Events

232
WHO Drug Information Vol. 27, No. 3, 2013
18th Model List of Essential Medi-cines and Model List for Children World Health Organization — The 19th Expert Committee on Selection and Use of Essential Medicines met in April 2013 to review and update the WHO Model List of Essential Medicines and the List of WHO Essential Medicines for Children. The committee considered 52 applica-tions and made 15 reviews.
The 18th WHO Model List of Essential Medicines and the 4th list of WHO Essen-tial Medicines for Children was finalized by the Committee at the end of their deliberations.
• Executive Summary at http://www.who.int/entity/selection_medicines/commit-tees/expert/19/EC19_Executive_sum-mary_Final_web_8Jul2013.pdf.
• WHO Model List of Essential Medicines at http://www.who.int/entity/medicines/publications/essentialmedicines/18th_EML_Final_web_8Jul13.pdf and
• WHO Model List Of Essential Medi-cines For Children at http://www.who.int/entity/medicines/publications/essentialmedicines/4th_EMLc_FINAL_web _8Jul13.pdf
Reference: WHO Notice, 8 July 2013 at http://www.who.int/entity/medicines/EMP_Website_notice_EML_July2013.pdf
International summit on medicines shortagesThe International Pharmaceutical Federa-tion (FIP) — a world federation of phar-macists and pharmaceutical scientists, recently convened an International sum-mit on medicines shortages in Toronto, Canada.
While there has been considerable atten-tion on the issue of medicines shortages in North America and in some European countries, there has been less attention
given to the global reach of this ongoing crisis and to possible global responses.
The Summit was attended by 50 experts representing governments and regulatory authorities, the generic and innovative pharmaceutical industries, wholesalers, group purchasing organizations, phar-macists, various medical specialities, dentists and patient organizations. Input was also provided by the World Health Organization.
The Summit recommends that the fol-lowing approaches should be investiga-ted.
• In order to advance transparency and increase communication between all stakeholders on existing shortages, each country should establish a publi-cly accessible means of providing information. The mid to long term aim should be to aggregate this informa-tion at international level.
• A global process to determine a list of critical or vulnerable products should be developed. This would be most easily done by a multilateral organi-zation. The list will require continuous revision and will inform regulatory responses, procurement practices and risk mitigation strategies. Each country could adapt the list to local conditions.
• All procurers of medicines are urged to move towards active procurement processes that assure the continuity of supply of quality medicines.
• All countries are encouraged to remove unnecessary variability of regulatory practices within and between countries.
• All regulatory authorities need to advance responsible transparency in relation to all regulatory processes.
• All countries should investigate the potential to establish a national body
Recent Publications, Information and Events

233
WHO Drug Information Vol. 27, No. 3, 2013
practical guidance for managing the supply chain, with an emphasis on health commodities. It is intended to help pro-gramme managers who design, manage, and assess logistics systems for health programs. In addition, policymakers, system stakeholders, and anyone work-ing in logistics will also find it helpful as a system overview and overall approach. Available at http://j.mp/1bGeeMh
New assessment guide and tool for HR capacity development in the public health supply chain. Effective public health supply chains require motivated and skilled staff with competency in various essential logistics functions. In an effort to help public health supply chain mana-gers in developing countries assess and improve the management of their human resources, a new toolkit is available at http://j.mp/13n5mre
In highlighting HIV and AIDS preven-tion and treatment efforts, The project’s updated CD toolkit, Resources for Managing the HIV & AIDS and Laboratory Supply Chains, is now available. The CD contains a selection of tools, reports, and briefs for supply chain and programme managers and advisors involved in desi-gning, implementing, and managing in-country supply chains for HIV and AIDS and laboratory commodities available at http://j.mp/16MeTeo
The Number 2, 2013 issue of the Supply Chain Management (SCM) Newsletter is available at http://j.mp/1cRZlnN
Reference: USAID Deliver Project at http://deliver.jsi.com/
charged with gathering and sharing information about demand for and supply of medicines within their juris-diction.
• All countries are encouraged to deve-lop evidence-based risk mitigation strategies which might include stra-tegic buffer stocks and stock piles, contingency planning, pandemic planning and capacity redundancy appropriate to their national needs.
Reference: International Pharmaceutical Federation. News Release at http://www.fip.org
USAID Deliver Project: supply chain management The USAID Deliver Project has published the following new material:
Alternative Public Health Supply Chains: Reconsidering the Role of the Central Medical Store and Getting Products to People Without a Traditional Central Medical Store. The report and policy brief identify a set of approaches that either de-emphasize the Central Medical Store (CMS), or enacts a radical shift in management. These approaches poten-tially offer a superior solution to improv-ing supply chain performance benefits compared to approaches that continue to emphasize the CMS. Available at http://j.mp/13HDMkG.
French and Spanish translations of the updated Logistics Handbook: A Practical Guide for the Supply Chain Management of Health Commodities. The Logistics Handbook, updated in 2011, offers
Recent Publications, Information and Events

234
WHO Drug Information Vol. 27, No. 3, 2013
O
O
OH
N
NN
HN
H2N
AciclovirumAciclovir
This is a draft proposal for The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Molecular formula. C8H11N5O3
Relative molecular mass. 225.20
Chemical name. 2-Amino-9-[(2-hydroxyethoxy)methyl]-1,9-dihydro-6H-purin-6-one. CAS Reg. No. 59277-89-3.
Description. White or almost white, crystalline powder.
Solubility. Slightly soluble in water; freely soluble in dimethyl sulfoxide; very slightly soluble in ethanol (96%). It dissolves in dilute solutions of mineral acids and alkali hydroxides.
Category. Antiviral (purine nucleoside analogue).
Storage. Preserve in well-closed containers. Protect from light and moisture.
Additional information. Aciclovir may exhibit polymorphism.
RequiRements
Definition. Aciclovir contains not less than 98.5% and not more than 101.0% of C8H11N5O3 calculated with reference to the dried substance.
Identity tests
Either test A alone, or test B and D or test C and D may be applied.
Consultation DocumentsThe International Pharmacopoeia

235
WHO Drug Information Vol. 27, No. 3, 2013
A. Carry out the test as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the spectrum obtained from aciclovir RS or with the reference spectrum of aciclovir.
B. Carry out the test as described under 1.14.1 Thin-layer chromatography, using the conditions given under Guanine and related substances test A1. The principal spot in the chromatogram obtained with solution (B) corresponds in position, appearance and intensity to the spot due to aciclovir in the chromatogram obtained with solution (C).
C. Carry out the test as described under 1.14.4 High-performance liquid chromatography, using the conditions given under Guanine and related substances test B. The retention time of the principal peak in the chromatogram obtained with solution (1) corresponds to the retention time of the aciclovir peak in the chromatogram obtained with solution (4).
D. Dissolve about 10 mg of the test substance in 5.0 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100.0 ml with water R. Dilute 5.0 ml of this solution to 50.0 ml with water R. The absorption spectrum (1.6) of the resulting solution, when observed between 230 nm and 350 nm, exhibits a maximum at about 255 nm and the absorption at 255 nm is about 0.5.
Clarity and colour of solution. A solution, containing 0.25 g of the test substance in 25 ml of sodium hydroxide (0.1 mol/l) TS, is clear and not more intensely coloured than standard colour solution Yw1 when compared as described under 1.11 Colour of liquids.
Sulfated ash (2.3). Not more than 1.0 mg/g.
Loss on drying. Dry to constant mass at 105 °C; it loses not more than 60 mg/g.
Guanine and related substances Either test A or test B may be applied.
A. Carry out test A.1 and A.2.
A.1 Guanine. Carry out the test as described under 1.14.1 Thin-layer chromato-graphy, using cellulose R1 as the coating substance (Merck cellulose F plate has been found suitable) and a mixture of 10 volumes of propan-1-ol, 30 volumes of ammonia (260 g/l) TS and 60 volumes of ammonium sulfate (50 g/l) TS as the mobile phase. Apply separately to the plate 10 µl of each of the following four, freshly prepared solutions in sodium hydroxide (0.1 mol/l) TS. For solution (A) use 5 mg of the test substance per ml. For solution (B) dilute 1 volume of solution (A) to 10 volumes. For solution (C) use a solution of 0.5 mg of aciclovir RS and 0.5 mg of guanine R per ml. For solution (D) use 35 µg of guanine R per ml. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air and examine the chromatogram under ultraviolet light (254 nm). In the chromatogram obtained with solution (C) guanine is eluted with a Rf value of 0.5 and aciclovir with a Rf value of 0.7. The test is not valid unless this chromatogram shows two clearly separated spots. Any secondary spot corresponding to guanine in the chromatogram obtained with solution (A) is not more intense than the principal spot in the chromatogram obtained with solution (D) (0.7%).
The International Pharmacopoeia

236
WHO Drug Information Vol. 27, No. 3, 2013The International Pharmacopoeia
A.2 Related substances. Carry out the test as described under 1.14.1 Thin-layer chromatography, using silica gel R4 as the coating substance and a mixture of 2 volumes of ammonia (260 g/l) TS, 20 volumes of methanol R and 80 volumes of dichloromethane R as the mobile phase. Apply separately to the plate 2 µl of each of the following three, freshly prepared solutions in dimethyl sulfoxide R. For solution (A) use 25 mg of the test substance per ml. For solution (B) dilute 1 volume of solution (A) to 200 volumes. For solution (C) use a mixture of 0.5 mg of aciclovir RS and 0.5 mg of aciclovir impurity A RS per ml. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air and examine the chromatogram under ultraviolet light (254 nm). The test is not valid unless the chromatogram obtained with solution (C) shows two clearly separated spots. Any spot with an Rf value greater than that of the principal spot in the chromatogram obtained with solution (A) is not more intense than the principal spot in the chromatogram obtained with solution (B) (0.5%).
B. Carry out the test as described under 1.14.4 High-performance liquid chromatography, using a stainless steel column (25 cm × 4.6 mm) packed with particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl group (5 µm). (Dionex C18 column and Shiseido MG C18 column have been found suitable.)
Use the following conditions for gradient elution:
Mobile phase A: 1 volume of acetonitrile R and 99 volumes of phosphate buffer, pH 3.1, TS.
Mobile phase B: 50 volumes of acetonitrile R and 50 volumes of phosphate buffer, pH 2.5, TS.
Time Mobile phase A Mobile phase B Comments(min) (%v/v) (%v/v)
0–5 100 0 Isocratic5–27 100 to 80 0 to 20 Linear gradient27–40 80 20 Isocratic40–42 80 to100 20 to 0 Return to initial composition42–52 100 0 Re-equilibration
Operate with a flow rate of 1.0 ml per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 254 nm. Maintain the column at 30 °C.
Prepare the following solutions. For solution (1) dissolve 25 mg of the test substance in 5.0 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 25.0 ml with water R. For solution (2) dilute 1.0 ml of solution (1) to 100.0 ml with water R. Dilute 1.0 ml of this solution to 10.0 ml with water R. For solution (3) dissolve 10 mg of guanine R in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100.0 ml with water. Dilute 5.0 ml of this solution to 50.0 ml with water R. For solution (4) dissolve 5 mg of aciclovir RS, 5 mg of guanine R and 10 mg of aciclovir impurity C RS in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100 ml with water R.
Inject separately 20 μl each of solutions (1), (2), (3) and (4). Record the chromatograms for about 45 minutes.
237
WHO Drug Information Vol. 27, No. 3, 2013
O
O
OON
NN
HN
H2N CH3
O
NH
NN
HN
H2N
In the chromatogram obtained with solution (4) the peak of aciclovir impurity C is eluted with a relative retention time of 0.94 with reference to the peak of aciclovir. The test is not valid unless the resolution factor between the peak due to aciclovir impurity C and the peak due to aciclovir is at least 1.5.
In the chromatogram obtained with solution (1):
• The area of any peak corresponding to guanine is not greater than 0.7 times the area of the principal peak in the chromatogram obtained with solution (3) (0.7 %).
• The area of any other peak, other than the principal peak and the peak due to guanine, is not greater than 5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.5%).
• The sum of all other areas, other than the principal peak and the peak due to guanine, is not greater than 8 times the area of the principal peak obtained with solution (2) (0.8%).
Disregard any peak with an area less than 0.5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.05%).
Assay
Dissolve about 0.150 g, accurately weighed, in 60 ml of anhydrous acetic acid R. Titrate with perchloric acid (0.1mol/l) VS, determining the end-point potentiometrically as described under 2.6 Non-aqueous titrations. Carry out a blank titration. Each ml of perchloric acid (0.1 mol/l) VS is equivalent to 22.52 mg of acyclovir (C18H11N5O3).
Impurities
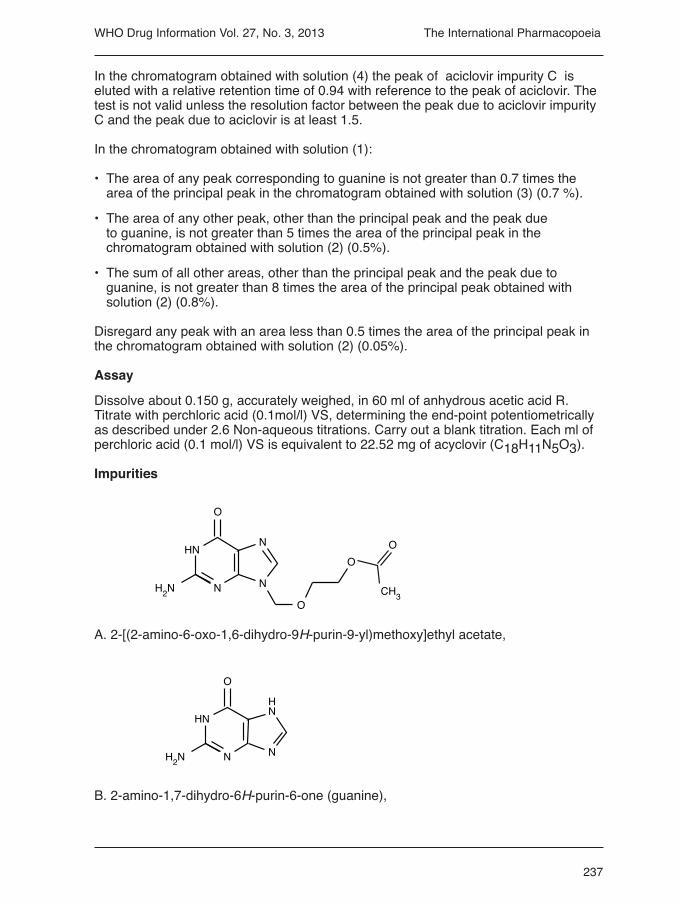
A. 2-[(2-amino-6-oxo-1,6-dihydro-9H-purin-9-yl)methoxy]ethyl acetate,
B. 2-amino-1,7-dihydro-6H-purin-6-one (guanine),
The International Pharmacopoeia

238
WHO Drug Information Vol. 27, No. 3, 2013
HN
O
OH
O
N
NN NH
O
H3C
O
CH3
HN
O
O
O
N
NN NH
O
H3C
NH
O
ON
NN
HN
H2N
NH2
O
O
N
N N
O OHO
N
NN
HN
H2N
NH
O
NH2O O
N
N N
O
N
NN
HN
H2N
C. 2-amino-7-[(2-hydroxyethoxy)methyl]-1,7-dihydro-6H-purin-6-one,
F. N-[9-[(2-hydroxyethoxy)methyl]-6-oxo-6,9-dihydro-1H-purin-2-yl]acetamide,
G. 2-[[2-(acetylamino)-6-oxo-1,6-dihydro-9H-purin-9-yl]methoxy]ethyl acetate,
I. 2-amino-7-[[2-[(2-amino-6-oxo-1,6-dihydro-9H-purin-9-yl)methoxy]ethoxy]methyl]-1,7-dihydro-6H-purin-6-one,
J. 9,9′-[ethylenebis(oxymethylene)]bis(2-amino-1,9-dihydro-6H-purin-6-one),
The International Pharmacopoeia

239
WHO Drug Information Vol. 27, No. 3, 2013
NH HN
O
NH
NHO
OH N
N N
N
NN
O
O
OH
CH3HN
O OO
N
NN NH
O
H3C
O
O
N
NN
HN
OHH2N
O
HN N
NN NH
O
H3CCH3
O
K. 2,2′-[methylenediimino]bis[9-[(2-hydroxyethoxy)methyl]1,9-dihydro-6H-purin-6-one],
L. N-(9-acetyl-6-oxo-6,9-dihydro-1H-purin-2-yl)acetamide (N2,9-diacetylguanine),
M. 2-[[2-(acetylamino)-6-oxo-1,6-dihydro-7H-purin-7-yl]methoxy]ethyl acetate,
N. unknown structure
O. unknown structure
P. 2-amino-9-(2-hydroxyethyl)1,9-dihydro-6H-purin-6-one.
The International Pharmacopoeia
240
WHO Drug Information Vol. 27, No. 3, 2013
New reference substances
Aciclovir RSAciclovir impurity A RSAciclovir impurity C RS
New reagents
Guanine R
C5H5N5O, 2-Amino-1,7-dihydro-6H-purin-6-one.
Amorphous white or almost white powder, practically insoluble in water, slightly soluble in ethanol (96 per cent). It dissolves in ammonia and in dilute solutions of alkali hydroxides.
Test Solutions to be added
Ammonium sulfate (50 g/l) TSTransfer 50 g ammonium sulfate R in a 1000 ml volumetric flask and make up to volume with water R.
Phosphate buffer, pH 2.5, TSDissolve 3.48 g of dipotassium hydrogen phosphate R in 1000 ml of water R and adjust to pH 2.5 with phosphoric acid R.
Phosphate buffer, pH 3.1, TSDissolve 3.48 g of dipotassium hydrogen phosphate R in 1000 ml of water R and adjust to pH 3.1 with phosphoric acid R.
Acicloviri ad injectionem Aciclovir for injection
This is a draft proposal for The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Description. A white powder or loose lumps; odourless or almost odourless.
Category. Antiviral (Purine nucleoside analogue).
Storage. Preserve in well-closed containers. Protect from light and moisture.
Labelling. The label should state that the active ingredient is Aciclovir.
Additional information. Strength in the current WHO Model List of Essential Medicines: 250 mg in vial. Strength in the current WHO Model List of Essential Medicines for Children: 250 mg in vial.
The International Pharmacopoeia
241
WHO Drug Information Vol. 27, No. 3, 2013
RequiRements
The powder for injections and the reconstituted solution for injection comply with the monograph on Parenteral preparations.
Definition. Aciclovir for injection is a sterile powder prepared from Aciclovir with the aid of a suitable alkali. The container of Aciclovir for injection contains not less than 95.0% and not more than 105.0% of the labeled amount of aciclovir (C8H11N5O3).
Identity tests
Either test A alone or test B and D, or test C and D may be applied.
A. To a quantity of the test substance, containing the equivalent of about 100 mg of aciclovir, add 10 ml water R, adjust to pH 4–7 with hydrochloric acid (0.1 mol/l) TS and allow to stand for 30 minutes. Filter, use 20 ml water R to wash the precipitate and dry it at 105 ℃ for 3 hours. Carry out the test with the precipitate as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the spectrum obtained from aciclovir RS or with the reference spectrum of aciclovir. If the spectra thus obtained are not concordant repeat the test by separately adding 10 ml of water R to the test substance and aciclovir RS and preceding as described. The infrared absorption spectrum is concordant with the spectrum obtained from aciclovir RS.
B. Carry out the test as described under 1.14.1 Thin-layer chromatography, using the conditions given under Guanine and related substances test A1. The principal spot in the chromatogram obtained with solution (B) corresponds in position, appearance and intensity to the spot due to aciclovir in the chromatogram obtained with solution (C).
C. Carry out the test as described under 1.14.4 High-performance liquid chromato-graphy, using the conditions given under Assay test A. The retention time of the principal peak in the chromatogram obtained with solution (1) corresponds to the retention time of the aciclovir peak in the chromatogram obtained with solution (2).
D. The absorption spectrum (1.6) of the solution, prepared as described under Assay test B, when observed between 230 nm and 350 nm, exhibits a maximum at 255 nm.
Clarity and colour of solution. A solution, containing the equivalent to 0.10 g of aciclovir in 10 ml of water R, is clear and not more intensely coloured than standard colour solution Yw1 when compared as described under 1.11 Colour of liquids.
Water. Determine as described under 2.8 Determination of water by the Karl Fischer method, Method A. Use 0.5 g of the test substance. The water content is not more than 55 mg/g.
pH value. pH of a solution containing the equivalent to 25 mg of aciclovir per ml of water R, 10.7–11.7.
Guanine and related substances
Either test A or test B may be applied.
A. Carry out test A.1 and A.2.
The International Pharmacopoeia

242
WHO Drug Information Vol. 27, No. 3, 2013The International Pharmacopoeia
A.1 Guanine. Carry out the test as described under 1.14.1 Thin-layer chromato-graphy, using cellulose R1 as the coating substance (Merck cellulose F plate has been found suitable.) and a mixture of 10 volumes of propan-1-ol, 30 volumes of ammonia (260 g/l) TS and 60 volumes of ammonium sulfate (50 g/l) TS as the mobile phase. Apply separately to the plate 10 µl of each of the following four, freshly prepared solutions in sodium hydroxide (0.1 mol/l) TS. For solution (A) dissolve a quantity of the powder to obtain a solution containing 5 mg of Aciclovir per ml. For solution (B) dilute 1 volume of solution (A) to 10 volumes. For solution (C) use a solution of 0.5 mg of aciclovir RS and 0.5 mg of guanine R per ml. For solution (D) use 35 µg of guanine R per ml. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air and examine the chromatogram under ultraviolet light (254 nm). In the chromatogram obtained with solution (C) guanine is eluted with a Rf value of 0.5 and aciclovir with a Rf value of 0.7. The test is not valid unless this chromatogram shows two clearly separated spots. Any secondary spot corresponding to guanine in the chromatogram obtained with solution (A) is not more intense than the principal spot in the chromatogram obtained with solution (D) (0.7%).
A.2 Related substances. Carry out the test as described under 1.14.1 Thin-layer chromatography, using silica gel R4 as the coating substance and a mixture of 2 volumes of ammonia (260 g/l) TS, 20 volumes of methanol R and 80 volumes of dichloromethane R as a mobile phase. Apply separately to the plate 2 µl of each of the following three, freshly prepared solutions in dimethyl sulfoxide R. For solution (A) dissolve a quantity of the powder for injection to obtain a solution containing 25 mg of aciclovir per ml. For solution (B) dilute 1 volume of solution (A) to 200 volumes. For solution (C) use a mixture of 0.5 mg of aciclovir RS and 0.5 mg of aciclovir impurity A RS per ml. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air and examine the chromatogram under ultraviolet light (254 nm). The test is not valid unless the chromatogram obtained with solution (C) shows two clearly separated spots. Any spot with an Rf value greater than that of the principal spot in the chromatogram obtained with solution (A) is not more intense than the principal spot in the chromatogram obtained with solution (B) (0.5%).
B. Carry out the test as described under 1.14.4 High-performance liquid chromato-graphy, using a stainless steel column (25 cm x 4.6 mm), packed with particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl group (5 µm). (DionexC18 and Shiseido MG C18 column have been found suitable.)
Use the following conditions for gradient elution:
Mobile phase A: 1 volume of acetonitrile R and 99 volumes of phosphate buffer, pH 3.1, TS.Mobile phase B: 50 volumes of acetonitrile R and 50 volumes of phosphate buffer, pH 2.5, TS.
Time Mobile phase A Mobile phase B Comments (min) (%v/v) (%v/v)
0–5 100 0 Isocratic 5–27 100 to 80 0 to 20 Linear gradient 27–40 80 20 Isocratic 40–42 80 to100 20 to 0 Return to initial composition 42–52 100 0 Re-equilibration

243
WHO Drug Information Vol. 27, No. 3, 2013
Operate with a flow rate of 1.0 ml per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 254 nm. Maintain the column at 30 °C.
Prepare the following solutions. For solution (1) dissolve a quantity of the powder for injection, equivalent to 25 mg of aciclovir in 5.0 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 25.0 ml with water R. For solution (2) dilute 1.0 ml of solution (1) to 100.0 ml with water. Dilute 1.0 ml of this solution to 10.0 ml with water. For solution (3) dissolve 10 mg of guanine R in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100.0 ml with water R. Dilute 5.0 ml of this solution to 50.0 ml with water R. For solution (4) dissolve 5 mg of aciclovir RS, 5 mg of guanine R and 10 mg of aciclovir impurity C RS in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100 ml with water R. Inject separately 20 μl each of solutions (1), (2), (3) and (4). Record the chromato-grams for about 45 minutes.
In the chromatogram obtained with solution (4) the peak of aciclovir impurity C is eluted with a relative retention time of 0.94 with reference to the peak of aciclovir. The test is not valid unless the resolution factor between the peak due to aciclovir impurity C and the peak due to aciclovir is at least 1.5.
In the chromatogram obtained with solution (1):
• The area of any peak corresponding to guanine is not greater than 0.7 times the area of the principal peak in the chromatogram obtained with solution (3) (0.7 %).
• The area of any other peak, other than the principal peak and the peak due to guanine, is not greater than 5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.5%).
• The sum of all other areas, other than the principal peak and the peak due to guanine, is not greater than 8 times the area of the principal peak obtained with solution (2) (0.8%).
Disregard any peak with an area less than 0.5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.05%).
Assay
Either test A or test B may be applied.
A. Carry out the test as described under 1.14.4 High-performance liquid chromatography, using a stainless steel column (25 cm x 4.6 mm), packed with particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl group (5 µm). (Dionex C18 column and Shiseido MG C18 column have been found suitable.)
As the mobile phase, use a mixture of 90 volumes of Mobile phase A, as described under Guanine and related substances test B, and 10 volumes of acetonitrile R.
Operate with a flow rate of 1.0 ml per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 254 nm. Maintain the column at 30 °C.
The International Pharmacopoeia

244
WHO Drug Information Vol. 27, No. 3, 2013
Prepare the following solutions. For solution (1) dissolve a quantity of the powder for injection, equivalent to about 20 mg of aciclovir, accurately weighed, in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100 ml with water. Dilute 5.0 ml of this solution to 50 ml with water. For solution (2) dissolve 20 mg of aciclovir RS in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100 ml with water. Dilute 5.0 ml of this solution to 50 ml with water.
Inject separately 20 µl each of solution (1) and (2). Record the chromatograms for about 20 min.
Measure the areas of the peak responses obtained in the chromatograms of solutions (1) and (2) and calculate the percentage content of aciclovir ((C8H11N5O3)) per sealed container, using the declared content of (C8H11N5O3) in aciclovir RS.
B. Mix the contents of 5 containers. Transfer a quantity of the powder for injection, equivalent to 150 mg of Aciclovir, accurately weighed, to a 100 ml volumetric flask and dilute to volume with hydrochloric acid (0.1 mol/l) TS, mix and filter. Dilute 1.0 ml of the resulting solution to 100.0 ml with hydrochloric acid (0.1 mol/l) TS. Measure the absorbance of this solution in a 1 cm layer at 255 nm, using hydrochloric acid (0.1 mol/l) TS as the blank. Calculate the percentage content of aciclovir (C8H11N5O3) per sealed container, using an absorptivity value of 56.0. i.e.,
Bacterial endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins. Contains not more than 0.17 IU of endotoxin per mg of aciclovir.
Acicloviri compressiAciclovir tablets
This is a draft proposal for The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Category. Antiviral (purine nucleoside analogue).
Storage. Preserve in well-closed containers. Protect from light and moisture.
Additional information. Strength in the current WHO Model List of Essential Medicines: 200 mg. Strengths in the current WHO Model List of Essential Medicines for Children: 200 mg.
RequiRements
Complies with the monograph on Tablets.
Definition. Aciclovir tablets contain not less than 90.0% and not more than 110.0% of the labelled amount of aciclovir (C8H11N5O3).
A = 5601%–––1cm
The International Pharmacopoeia

245
WHO Drug Information Vol. 27, No. 3, 2013
Identity tests
Either test A and C or test B and C may be applied.
A. Carry out the test as described under 1.14.1 Thin-layer chromatography, using the conditions given under Guanine and related test A1. The principal spot in the chromatogram obtained with solution (B) corresponds in position, appearance and intensity to the spot due to aciclovir in the chromatogram obtained with solution (C).
B. Carry out the test as described under 1.14.4 High-performance liquid chromatography, using the conditions given under Assay test A. The retention time of the principal peak in the chromatogram obtained with solution (1) corresponds to the retention time of the aciclovir peak in the chromatogram obtained with the solution (2).
C. The absorption spectrum (1.6) of the solution, prepared as described under Assay test B, when observed between 230 nm and 350 nm, exhibits a maximum at 255 nm.
Dissolution. Carry out the test as described under 5.5 Dissolution test for solid oral dosage forms, using as the dissolution medium, 900 ml of Hydrochloric acid (~4 g/l) TS and rotating the paddle at 75 revolutions per minute. At 30 minutes withdraw a sample of 10 ml of the medium through an in-line filter. Measure the absorbance (1.6) of the filtered sample, suitably diluted if necessary, at a wavelength of 255 nm. At the same time measure the absorbance of a suitable solution of aciclovir RS in hydrochloric acid (~4 g/l) TS, using the same buffer as the blank.
For each of the six tablets tested calculate the total amount of aciclovir (C8H11N5O3) in the medium from the absorbances obtained, using the declared content of C8H11N5O3 in aciclovir RS. Use the requirements as described under 5.5 Dissolution test for solid oral dosage forms, Acceptance criteria to evaluate the results: the amount in solution is not less than 75% (Q) of the amount declared on the label.
Guanine
Either test A or test B may be applied.
A. Carry out the test as described under 1.14.1 Thin-layer chromatography, using cellulose R1 as the coating substance (Merck cellulose F plate has been found suitable) and a mixure of 10 volumes of propan-1-ol, 30 volumes of ammonia (260 g/l) and 60 volumes of ammonium sulfate (50 g/l). Apply separately to the plate 10 µL of each of the following four, freshly prepared solutions in sodium hydroxide (0.1 mol/l) TS. For solution (A) shake a quantity of the powdered tablets, containing about 25 mg of aciclovir, with 5 ml of sodium hydroxide (0.1 mol/l) TS, filter and use the filtrate. For solution (B) dilute 1 volume of (A) to 10 volumes. For solution (C) use a solution of 0.5 mg of aciclovir RS and 0.5 mg of guanine RS per ml. For solution (D) use 50 µg of guanine R per ml. After removing of the plate from the chromatographic chamber allow it to dry exhaustively in air and examine the chromatogram under ultraviolet light (254 nm). In the chromatogram obtained with solution (C) guanine is eluted with a Rf value of 0.5 and aciclovir with a Rf value of 0.7. The test is not valid unless this chromatogram shows two clearly separated spots. Any secondary spot corresponding to guanine in the chromatogram obtained with solution (A) is not more intense than the principal spot in the chromatogram obtained with solution (D) (1.0%).
B. Carry out the test as described under 1.14.4 High performance liquid chromato-graphy, using the conditions given under Assay test A.
The International Pharmacopoeia

246
WHO Drug Information Vol. 27, No. 3, 2013
Prepare the following solutions. For solution (1) shake a quantity of the powdered tablets, containing 25 mg of aciclovir, with 5.0 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 25.0 ml with water, filter and use the filtrate. For solution (2) dissolve 10 mg of guanine R in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100.0 ml with water R. Then dilute 5.0 ml of this solution to 50.0 ml with water. For solution (3) dissolve 5 mg of aciclovir RS, 5 mg of guanine R in 10 ml of sodium hydroxide (0.1 mol/l) TS and dilute to 100 ml with water R.
Inject 20 μl of solution (3). The test is not valid unless the resolution between the peak due to aciclovir and the peak due to guanine is at least 3.0.
Inject separately 20 μl each of solutions (1) and (2). In the chromatogram obtained with solution (1) the area of any peak corresponding to guanine is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (1.0%).
Assay
Either test A or test B may be applied.
A. Carry out the test as described under1.14.4 High-performance liquid chromatography, using a stainless steel column (25 cm x 4.6 mm), packed with particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl group (5 µm). (Dionex C18 column and Shiseido MG C18 column have been found suitable.)
As the mobile phase, use a mixture of 90 volumes of phosphate buffer, pH 3.1, TS and 10 volumes of acetonitrile R.
Operate with a flow rate of 1.0 ml per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 254 nm. Maintain the column at 30 °C.
Prepare the following solutions. For solution (1) shake a quantity of the powdered tablets, equivalent to about 20 mg of aciclovir, accurately weighed, with 10 ml of sodium hydroxide (0.1 mol/l) and dilute to 100 ml with water. Dilute 5.0 ml of this solution to 50 ml with water. For solution (2) dissolve 20 mg of aciclovir RS in 10 ml of sodium hydroxide (0.1 mol/l) and dilute to 100 ml with water. Dilute 5.0 ml of this solution to 50 ml with water.
Inject separately 20 µl each of the solutions (1) and (2). Record the chromatograms for about 20 min.
Measure the areas of the peak responses obtained in the chromatograms of solutions (1) and (2) and calculate the percentage content of aciclovir (C8H11N5O3) in the tablets, using the declared content of C8H11N5O3 in aciclovir RS.
B. Weigh and powder 20 tablets. Transfer a quantity of the powder, equivalent to about 0.1 g of Aciclovir, accurately weighed, to a 100 ml volumetric flask, add 60 ml of sodium hydroxide (0.1 mol/l), sonicate for about 15 minutes, allow to cool to room temperature and make up to volume with the same solvent, shake and filter. Transfer 15.0 ml of the filtrate to a 100 ml volumetric flask, add 50 ml of water and 5.8 ml of hydrochloric acid (70g/l) TS and dilute to volume with water R. Dilute 5.0 ml of the solution to 50.0 ml with hydrochloric acid (0.1 mol/l) TS. Measure the absorbance of
The International Pharmacopoeia

247
WHO Drug Information Vol. 27, No. 3, 2013
the resulting solution in a 1 cm layer at 255 nm, using hydrochloric acid (0.1 mol/l) TS as the blank. Calculate the percentage content of aciclovir (C8H11N5O3) in the tablets, using an absorptivity value of using an absorptivity value of 56.0, i.e.,
Radiopharmaceuticals: general monograph
This is a draft general monograph revision for The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Additional or amended text.
This general monograph is intended to be read in conjunction with the individual monographs on radiopharmaceutical preparations. A radiopharmaceutical preparation that is the subject of an individual monograph in The International Pharmacopoeia complies with the general requirements stated below and with the general monograph for the relevant dosage form (most commonly that for parenteral preparations) as modified by any of the requirements given below and by any specific instruction included in the individual monograph.
RequiRementsDefinition
Radiopharmaceutical preparation or radiopharmaceutical. A radiopharmaceutical preparation or radiopharmaceutical is a medicinal product in a ready-to-use form suitable for human use that contains a radionuclide. The radionuclide is integral to the medicinal application of the preparation, making it appropriate for one or more diag-nostic or therapeutic applications.
For the purpose of this general monograph radiopharmaceuticals also cover:
Radionuclide generator. A system in which a daughter radionuclide (short half-life) is separated by elution or by other means from a parent radionuclide (long half-life) and later used for production of a radiopharmaceutical preparation.
Radionuclide precursor. A “radionuclide precursor” means any radionuclide not being a radiopharmaceutical or generator or radionuclide kit which is produced for the radiolabelling of another substance for administration.
Kit for radiopharmaceutical preparation. In general a vial containing the non-radionuclide components of a radiopharmaceutical preparation , usually in the form of a sterilized, validated product to which the appropriate radionuclide is added or in which the appropriate radionuclide is diluted before medical use. In most cases the kit is a multidose vial and production of the radiopharmaceutical preparation may require additional steps such as boiling, heating, filtration and buffering.
Chemical precursor. Non-radioactive substances in combination with radionuclide.
A = 5601%–––1cm
The International Pharmacopoeia

248
WHO Drug Information Vol. 27, No. 3, 2013
Manufacture
The manufacturing process for radiopharmaceutical preparations should meet the requirements of good manufacturing practice (GMP).
The manufacturer is responsible for ensuring the quality of his products and especially for examining preparations of short-lived radionuclides for long-lived impurities after a suitable period of decay. In this way, the manufacturer ensures that the manufacturing processes employed are producing materials of appropriate quality. In particular, the radionuclide composition of certain preparations is determined by the chemical and isotopic composition of the target material (see ”Target materials” ) and pilot preparations are advisable when new batches of target material are employed.
When the size of a batch of a radiopharmaceutical preparation is limited to one or few units (for example, certain therapeutic preparations or very short-lived preparations) release of the product must rely on the process control rather than product quality control tests. Therefore validation and revalidation of manufacture process must be fully implemented as well as the product quality control tests.
Radiation Protection. The relevant premises and equipment must be designed, built and maintained so that they do not bear any negative impact on or represent any hazard to the product, personnel or immediate surroundings. The corresponding supporting materials are provided by various IAEA publications.
See Supplementary information chapter: Radiopharmaceuticals and Radiation Protection and Safety of Radiation Sources International Basic Safety Standards. Interim Edition. General Safety Requirements (IAEA, Vienna, 2011); and Radiological Protection for Medical Exposure to Ionizing Radiation Safety Guide (IAEA, Vienna, 2002) Safety Standard Series No. RS-G-1.5, Safety Standard Series No. RS-G-1.5.Consult the IAEA website for the current Safety Standards and publications (http://www-ns.iaea.org/standards/). For more supporting material refer to the list of IAEA publications in Monographs: Radiopharmaceuticals: Supplementary information: Safety considerations.
See also Regulations for the Safe Transport of Radioactive Materials. Safety Requirements. No TS-R-1 (IAEA, Vienna, 2009).for further details. Consult the IAEA web site (http://www-ns.iaea.org/standards/) for current guidance.
Radionuclide production. In general ways of manufacturing radionuclides for use in radiopharmaceutical preparations are:
Nuclear fission. Nuclides with high atomic number are fissionable and a common reaction is the fission of uranium-235 by neutrons in a nuclear reactor. For example, iodine-131, molybdenum-99 and xenon-133 can be produced in this way. Radio-nuclides from such a process must be carefully controlled in order to minimize the radionuclidic impurities.
Charged particle bombardment. Radionuclides may be produced by bombarding target materials with charged particles in particle accelerators such as cyclotrons. The isotopic composition and purity of the target material will influence the radionuclidic purity of irradiated target.
Neutron bombardment. Radionuclides may be produced by bombarding target materials with neutrons in nuclear reactors. The rate of the nuclear reaction
The International Pharmacopoeia

249
WHO Drug Information Vol. 27, No. 3, 2013
depends on the energy of the incident particle, neutron flux and nuclear cross-section. The isotopic composition and purity of the target material will influence the radionuclidic purity of irradiated target.
Radionuclide generator systems. Radionuclides of short half-life may be produced by means of a radionuclide generator system involving separation of the daughter radionuclide from a long-lived parent by chemical or physical separation. Care must be taken to avoid contamination of daughter radionuclide with parent radionuclide and decay products.
Starting materials (including chemical precursors and excipients). In the manufacture of radiopharmaceutical preparations, measures shall be taken to ensure that all ingredients are of appropriate quality, including those starting materials, such as chemical precursors for synthesis, that are produced on a small scale and supplied by specialized producers or laboratories for use in the radiopharmaceutical industry. The actual quantity of radioactive material compared with quantities of excipients is normally very small therefore excipients can greatly influence the quality of the radiopharmaceutical preparation.
Target materials. The composition and purity of the target material and the nature and energy of the incident particle will determine the relative percentages of the principal radionuclide and other potential radionuclides (radionuclidic impurities) and thus ultimately the radionuclidic purity. Strict control of irradiation parameters such as beam energy, intensity and duration is also essential. For very short lived radionuclides including the ones present in most positron emission tomography (PET) tracers the determination of radiochemical and radionuclidic purity of radiopharmaceutical preparation before patient use is difficult. Therefore before clinical use of these radionuclides, strict operational conditions and extensive validations are essential. Any subsequent change in operational conditions should be revalidated.
Where applicable (e.g., cyclotron irradiation of solid targets) each new batch of target material must be tested and validated in special production runs before its use in routine radionuclide production and manufacture of radiopharmaceutical preparation. This will ensure that under specified conditions, the target yields a radionuclide in the desired quantity and quality.
Carriers. A carrier, in the form of inactive material, either isotopic with the radionuclide, or non-isotopic, but chemically similar to the radionuclide, may be added during radionuclide production and radiopharmaceutical preparation. In some situations it may be added to enhance chemical, physical or biological properties of the radiopharmaceutical preparation. The amount of carrier added must be controlled and sufficiently small for it not to cause undesirable physiological effects.
Carrier-free preparation. It is a preparation free from stable isotope of the same element as the radionuclide concerned present in the preparation in the stated chemical form or at the position of the radionuclide in the molecule concerned. When appropriate, specific radioactivity must be measured in the radiopharmaceutical preparation.
No-carrier added preparation. It is a preparation to which no stable isotopes of the same element as the radionuclide concerned are intentionally added in the stated
The International Pharmacopoeia

250
WHO Drug Information Vol. 27, No. 3, 2013
chemical form or at the position of the radionuclide in the molecule concerned. When appropriate specific radioactivity must be measured in the radiopharmaceutical preparation.
Production of radiopharmaceutical preparation. Radiopharmaceutical preparations may contain the types of excipients permitted by the general monograph for the relevant dosage form.
Sterilization. Radiopharmaceutical preparations intended for parenteral administration are sterilized by a suitable method (see 5.8 Methods of sterilization). Whenever possible, steam sterilization is recommended.
All sterilization processes must be validated.
Addition of antimicrobial preservatives. Radiopharmaceutical injections are commonly supplied in multidose containers. The nature of the antimicrobial preservative, if present, is stated on the label or, where applicable, that no antimicrobial preservative is present.
Radiopharmaceutical injections for which the shelf-life is greater than one day and that do not contain an antimicrobial preservative should preferably be supplied in single-dose containers. If, however, such a preparation is supplied in a multidose container requirements of the general monograph for Parenteral Preparations should apply.
Radiopharmaceutical injections for which the shelf-life is greater than one day and that do contain an antimicrobial preservative may be supplied in multidose containers. After aseptic withdrawal of the first dose, the container should be stored at a temperature between 2° and 8° C and the contents used within 7 days unless otherwise specified.
Radiation protection
See Supplementary information chapter on Radiopharmaceuticals and Radiation Protection and Safety of Radiation Sources International Basic Safety Standards. Interim Edition. General Safety Requirements (IAEA, Vienna, 2011) and Radiological Protection for Medical Exposure to Ionizing Radiation Safety Guide (IAEA, Vienna, 2002) Safety Standard Series No. RS-G-1.5.
Identity tests
Tests for identity of the radionuclide are included in the individual monographs for radiopharmaceutical preparations. The radionuclide is generally identified by its half-life or by the nature and energy of its radiation or by both as stated in the monograph.
Other tests
Half-life measurement. The half-life is a characteristic of the radionuclide that may be used for its identification. The half-life is calculated by measuring the variation of radioactivity of a sample to be tested as a function of time. Perform the measurements in the linearity range of a calibrated instrument. Measurements should comply with the R 1.1 Detection and measurement of radioactivity. Approximate half-life can be determined over a relatively short period of time to allow release for use of radiopharmaceutical preparations. The calculated approximate half-life is within the range of the values stated in the individual monograph.
The International Pharmacopoeia

251
WHO Drug Information Vol. 27, No. 3, 2013
Radionuclidic purityRadionuclidic impurities may arise during the production and decay of a radionuclide. Potential radionuclidic impurities may be mentioned in the monographs and their characteristics are described in the general monograph: Annexes: Table of physical characteristics. In most cases, to establish the radionuclidic purity of a radiopharmaceutical preparation, the identity of every radionuclide present and its radioactivity must be known.
Technical details of radionuclide identification and radionuclidic purity determination are described in R1.2 Radiation spectrometry and R1.3 Determination of radionuclidic purity. Because the level of radionuclidic impurities, expressed as a percentage of each impurity, may increase or decrease with time, the measured radioactivity of each impurity must be recalculated to the activity during the period of validity of the preparation.
The individual monographs prescribe the radionuclidic purity required and may set limits for specific radionuclidic impurities (for example, molybdenum-99 in technetium-99m). While these requirements are necessary, they are not in themselves sufficient to ensure that the radionuclidic purity of a preparation is sufficient for its clinical use. The manufacturer must examine the product in detail and especially must examine preparations of radionuclides with a short half-life for impurities with a long half-life after a suitable period of decay. In this way, information on the suitability of the manufacturing processes and the adequacy of the testing procedures is obtained. In cases where two or more positron-emitting radionuclides need to be identified and/or differentiated, for example the presence of 18F-impurities in 13N-preparations, half-life determinations need to be carried out in addition to gamma-ray spectrometry.
Radiochemical purityA radioactive preparation may contain the radionuclide in different chemical forms other than the intended one. Therefore it is necessary to separate the different substances containing the radionuclide and determine the percentage of radioactivity due to the radionuclide concerned associated with the stated chemical form and the contribution to the total radioactivity due to the radionuclide concerned coming from other substances. For this purpose instruments for the detection and measurement of radioactivity are used in combination with a physic-chemical separation technique.Radiochemical purity is assessed by a variety of analytical techniques such as 1.14.4 High-performance liquid chromatography, 1.14.2 Paper Chromatography, 1.14.1 Thin-layer Chromatography and 1.15 Electrophoresis combined with suitable radioactivity measurement described in R1.1 Detection and measurement of radioactivity.
In all cases the radioactivity of each analyte is measured after the separation has been achieved using the stated method.
The radiochemical purity section of an individual monograph may include limits for specified radiochemical impurities, including isomers.
In some cases, it is necessary to determine the physiological distribution of the radiopharmaceutical in a suitable test animal.
Specific radioactivity. Specific radioactivity is defined as radioactivity of a radionuclide per unit mass of the element or of the chemical form concerned. Specific radioactivity is usually calculated taking into account the radioactivity concentration
The International Pharmacopoeia

252
WHO Drug Information Vol. 27, No. 3, 2013
and the concentration of the chemical substance being studied. Specific radioactivity changes with time. The statement of the specific radioactivity therefore includes reference to a date and, if necessary, time.
Specific radioactivity must be measured in carrier added preparations. For some non-carrier added radiopharmaceutical preparations (for example, receptor ligands) it is important to state specific radioactivity. Individual monographs might state the range of specific radioactivity.
Chemical purityChemical purity refers to the proportion of the preparation that is in the specified chemical form regardless of the presence of radioactivity; it may be determined by accepted methods of analysis.
In general, limits should be set for chemical impurities in preparations of radiopharmaceuticals if they are toxic or if they modify the labelling process or alter physiological uptakes that are under study or if they result in undesirable interactions (e.g. aluminium can induce flocculation of Tc-99m sulphur colloid). Special attention is necessary for impurities with a pharmacologically active or pharmacodynamic effect even for very low amounts (for example, receptor ligands). Where appropriate, the stereo-isomeric purity has to be verified. In general, the type of limit for inorganic impurities such as arsenic and heavy metals that are specified in monographs for pharmaceutical substances are also valid for radiopharmaceuticals.
Characterize impurities as much as possible. Generic limits can be set for unidentified impurities. The limits has to be chosen carefully considering amounts and toxicity based upon toxicities of starting materials, precursors, possible degradation products and the final product.
pH When required, measure the pH of non-radioactive solutions as described under 1.13 Determination of pH. For radioactive solutions the pH may be measured using a pH indicator strip R.
[Note from Secretariat: Add pH indicator strip R to the section on Reagents using the following:
pH indicator strip. R. Plastic or paper strip containing multiple segments of different dye-impregnated papers allowing visual determination of pH in the prescribed range by comparison with a master chart.]
SterilityA number of monographs for radiopharmaceuticals contain the requirement that the preparation is sterile. Such preparations comply with 3.2 Test for sterility. The special difficulty arises with the radiopharmaceuticals because of the short half-life of the radionuclide, the small size of batches and the radiation hazards. In the case that the monograph states that the preparation can be released for use before completion of the test for sterility, the sterility test must be started as soon as practically possible in relation to the radiation. If not started immediately, samples are stored under conditions that are shown to be appropriate in order to prevent false negative result.
The International Pharmacopoeia

253
WHO Drug Information Vol. 27, No. 3, 2013
When the size of the batch of a radiopharmaceutical is limited to one or few samples (e.g., therapeutic or very short-lived radiopharmaceutical preparations), sampling the batch may not be possible. In this case, reliance is on process control rather than the final product control.
Bacterial endotoxins/pyrogensWhere appropriate, an individual monograph for a radiopharmaceutical preparation requires compliance with 3.4 Test for bacterial endotoxins. Validation of the test is necessary to exclude any interference or artefact due to the nature of the radiopharmaceutical. The pH of some radiopharmaceutical preparations will require to be adjusted to pH 6.5–7.5 to achieve optimal results.
Where it is not possible to eliminate interference with the test for bacterial endotoxins due to the nature of the radiopharmaceutical, compliance with 3.5 Test for pyrogens may be specified.
LabellingEvery radiopharmaceutical preparation must comply with the labelling requirements established under GMP.
[Note from Secretariat: Check that the text is consistent with current GMP text needs to be undertaken in final version.]
The label on the primary container should include:
• A statement that the product is radioactive or the international symbol for radioactivity;
• Name of the radiopharmaceutical preparation;
• Where appropriate, that the preparation is for diagnostic or for therapeutic use;
• Route of administration;
• Total radioactivity present at a stated date and, where necessary, time; for solutions, a statement of the radioactivity in a suitable volume (for example, in MBq per ml of the solution) may be given instead;
• Expiry date and, where necessary, time;
• Batch (lot) number assigned by the manufacturer; • For solutions, the total volume.
The label on the outer package should include:
• Statement that the product is radioactive or the international symbol for radioactivity;
• Name of the radiopharmaceutical preparation;
• Where appropriate, that the preparation is for diagnostic or for therapeutic use;
• Route of administration;
The International Pharmacopoeia

254
WHO Drug Information Vol. 27, No. 3, 2013
• Total radioactivity present at a stated date and, where necessary, time; for solutions, a statement of the radioactivity in a suitable volume (for example, in MBq per ml of the solution) may be given instead;
• Expiry date and, where necessary, time;
• Batch (lot) number assigned by the manufacturer;
• For solutions, the total volume;
• Any special storage requirements with respect to temperature and light;
• Where applicable, the name and concentration of any added microbial preservatives or, where necessary, that no antimicrobial preservative has been added.
Note: The shipment of radioactive substances is subject to special national and international regulations as regards to their packaging and outer labelling. (Regulations for the Safe Transport of Radioactive Materials. Safety Requirements. No.TS-R-1 (IAEA, Vienna, 2009). For further details and the current guidance consult the IAEA web site at http://www-ns.iaea.org/standards/)
StorageRadiopharmaceuticals should be kept in well-closed containers and stored in an area assigned for the purpose. Storage conditions should be such that the maximum radiation dose rate to which persons may be exposed is reduced to an acceptable level.
Care should be taken to comply with national regulations for protection against ionizing radiation.
Radiopharmaceutical preparations that are intended for parenteral use should be kept in a glass vial, ampoule or syringe that is sufficiently transparent to permit the visual inspection of the contents. Glass containers may darken under the effect of radiation.
Annexes: TerminologyBiological half-lifeThe biological half-life (T½b) of a radiopharmaceutical is the time taken for the concentration of the pharmaceutical to be reduced 50% of its maximum concentration in a given tissue, organ or whole body, not considering radioactive decay.
Critical organThe critical organ is the organ or tissue which is the most vulnerable to radiation damage This may not be the target tissue or the tissue that receives the highest dose and therefore the dose to the critical organ will determine the maximum safe dose which can be administered.
Effective half-lifeThe effective half-life (T½e) is the actual half-life of a radiopharmaceutical in a given tissue, organ or whole body and is determined by a relationship including both the physical half-life and biological half-lives. The effective half-life is important in calculation of the optimal dose of radiopharmaceutical to be administered and in monitoring the amount of radiation exposure. It can be calculated from the formula:
T½e = –––––––T½p x T½bT½p + T½b
The International Pharmacopoeia

255
WHO Drug Information Vol. 27, No. 3, 2013
Where T½p and T½b are the physical and biological half-lives respectively.
Half-life The time in which the radioactivity decreases to one-half its original value.
Explanatory note. The rate of radioactive decay is constant and characteristic for each individual radionuclide. The exponential decay curve is described mathematically by the equation: N = Noe -λt
where N is the number of atoms at elapsed time t, No is the number of atoms when t = 0, and λ is the disintegration constant characteristic of each individual radionuclide. The half-life period is related to the disintegration constant by the equation:
Radioactive decay corrections are calculated from the exponential equation, or from decay tables, or are obtained from a decay curve plotted for the particular radionuclide involved (see Figure 1).
Figure 1. Master decay chart
T = ––––––0.69321
2
0 0.5 1 1.5 2 2.5 3 3.5Half lives
100
90
80
70
60
50
40
30
20
10
Radio
activity %
The International Pharmacopoeia

256
WHO Drug Information Vol. 27, No. 3, 2013
IsotopesAtoms of the same element with different atomic mass numbers are called isotopes.
NuclideNuclide is defined as species of atom as characterized by the number of protons, the number of neutrons, and the energy state of the nucleus.
Radioactive concentrationThe radioactive concentration of a solution refers to the amount radioactivity per unit volume of the solution. As with all statements involving radioactivity, it is necessary to include a reference date and time of standardization. For radionuclides with a half-life of less than one day, a more precise statement of the reference time is required. Units for radioactive concentration are megaBecquerels per millilitre (MBq/ml).
Since the radioactive concentration will change with time due to decrease in the nuclide radioactivity it is always necessary to provide a reference time. For short-lived radionuclides the reference time will be more precise including time of day in addition to date.
Radioactive decayThe property of unstable nuclides during which they undergo a spontaneous transformation within the nucleus. This change results in the emission of energetic particles or electromagnetic energy from the atoms and the production of an altered nucleus.
Explanatory note. The term “disintegration” is widely used as an alternative to the term “transformation”. Transformation is preferred as it includes, without semantic difficulties, those processes in which no particles are emitted from the nucleus.
RadioactivityGenerally the term “radioactivity” is used both to describe the phenomenon of radioactive decay and to express the physical quantity of this phenomenon. The radioactivity of a preparation is the number of nuclear disintegrations or transformations per unit time. In the International System (SI), the term “activity” is used, which corresponds to radioactivity in the context of this general monograph.
It is expressed in becquerel (Bq), which is 1 nuclear transformation per second.
Explanatory note. The term “disintegration” is widely used as an alternative to the term “transformation”. Transformation is preferred as it includes, without semantic difficulties, those processes in which no particles are emitted from the nucleus.
Radiochemical purityThe ratio expressed as a percentage of radioactivity of radionuclide concerned which is present in the radiopharmaceutical preparation in the stated chemical form, to the total radioactivity of that radionuclide present in the radiopharmaceutical preparation. Relevant potential radiochemical impurities are listed with their limits in the individual monographs. (Note: Source of information: European Pharmacopoeia.)
As radiochemical purity may change with time, mainly because of radiolysis or chemical decomposition, the result of the radiochemical purity test should be started at given date and if necessary hour indicating when the test was carried out. The radiochemical purity limit should be valid during the whole shelf-life.
The International Pharmacopoeia
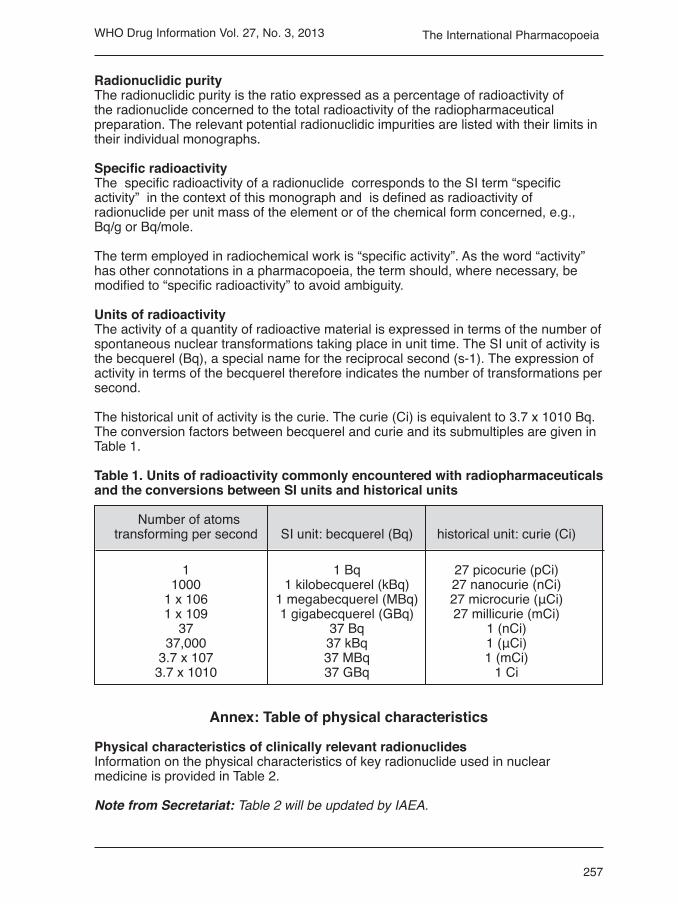
257
WHO Drug Information Vol. 27, No. 3, 2013
Radionuclidic purityThe radionuclidic purity is the ratio expressed as a percentage of radioactivity of the radionuclide concerned to the total radioactivity of the radiopharmaceutical preparation. The relevant potential radionuclidic impurities are listed with their limits in their individual monographs.
Specific radioactivity The specific radioactivity of a radionuclide corresponds to the SI term “specific activity” in the context of this monograph and is defined as radioactivity of radionuclide per unit mass of the element or of the chemical form concerned, e.g., Bq/g or Bq/mole.
The term employed in radiochemical work is “specific activity”. As the word “activity” has other connotations in a pharmacopoeia, the term should, where necessary, be modified to “specific radioactivity” to avoid ambiguity.
Units of radioactivityThe activity of a quantity of radioactive material is expressed in terms of the number of spontaneous nuclear transformations taking place in unit time. The SI unit of activity is the becquerel (Bq), a special name for the reciprocal second (s-1). The expression of activity in terms of the becquerel therefore indicates the number of transformations per second.
The historical unit of activity is the curie. The curie (Ci) is equivalent to 3.7 x 1010 Bq. The conversion factors between becquerel and curie and its submultiples are given in Table 1.
Table 1. Units of radioactivity commonly encountered with radiopharmaceuticals and the conversions between SI units and historical units
Number of atoms transforming per second SI unit: becquerel (Bq) historical unit: curie (Ci)
1 1 Bq 27 picocurie (pCi) 1000 1 kilobecquerel (kBq) 27 nanocurie (nCi) 1 x 106 1 megabecquerel (MBq) 27 microcurie (μCi) 1 x 109 1 gigabecquerel (GBq) 27 millicurie (mCi) 37 37 Bq 1 (nCi) 37,000 37 kBq 1 (μCi) 3.7 x 107 37 MBq 1 (mCi) 3.7 x 1010 37 GBq 1 Ci
Annex: Table of physical characteristics
Physical characteristics of clinically relevant radionuclidesInformation on the physical characteristics of key radionuclide used in nuclear medicine is provided in Table 2.
Note from Secretariat: Table 2 will be updated by IAEA.
The International Pharmacopoeia

258
WHO Drug Information Vol. 27, No. 3, 2013
Radiopharmaceuticals Safety considerations
This is a draft proposed text for the Supplementary Information section of The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Safety considerationsRadiopharmaceuticals are radioactive and can pose a risk to the personnel involved in handling them during inter alia manufacture, storage, transport, compounding, testing, dispensing and administration, to the patients to whom they are administered and to the environment.
All personnel involved in any part of the above operations are required to have appropriate specific additional training. All personnel with access to the areas where these operations are carried out, for example, maintenance and support staff such as cleaners should receive specific instruction and appropriate supervision whilst in the operational areas. Risk to patients should be minimized. It is essential to ensure that reproducible and clinically reliable results will be obtained. All operations should be carried out or supervised by personnel who have received expert training in handling radioactive materials.
Specialized techniques are required to minimize the risks to personnel. All procedures in which radiopharmaceuticals are handled must be designed and carried out in compliance with the ALARA principle, that is to ensure that exposure to radiation is as low as reasonably applicable. Three key components of the ALARA principle are time (reduce time of exposure), distance (the greater the distance, the lower the risk) and shielding (appropriate shielding is essential at all stages of handling).
Airborne radioactive contamination is a risk factor. Protection of staff requires a negative pressure environment which is conflicting with the general GMP requirement to protect the product in a positive pressure environment. These issues should be balanced according to risk-based approach and rationalized.
Radiation shielding. Adequate shielding must be used to protect all personnel from ionizing radiation. Additionally, when testing radiopharmaceuticals instruments must be suitably shielded from background radiation.
References
List of IAEA publications (safety, facility design, etc.)
Note from the Secretariat: IAEA will provide a list of publications.
The International Pharmacopoeia

259
WHO Drug Information Vol. 27, No. 3, 2013
RadiopharmaceuticalsTesting: additional guidance
This is a draft proposed text for the Supplementary Information section of The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Note from the Secretariat: It is suggested that the section on “end-user testing/rapid quality control tests” be replaced with the text below.
End-user testing
An end-user test is meant to be the simplified quality control test provided by the respective kit manufacturer in the package leaflet.
The end-user test may be used provided that it can be demonstrated that the preparation is fully traceable to a batch certified to comply with all the other requirements of the related monograph.
End-user testing is an important step in the quality management of radio-pharmaceutical preparation and for the safety of patients, especially for those radiopharmaceutical preparations that are dispensed or compounded in the end-user facility (for example, nuclear medicine clinics). Application of the test is specified in the relevant monograph may not be possible at this stage either because of the short half-life of the radioisotope or due to other analytical limitations. The use of alternative, simple tests that adequately identify this radiopharmaceutical preparation is therefore advisable.
For further information refer to the IAEA publications: Operational Guidance on Hospital Radiopharmacy. A safe and Effective Approach. http://www-pub.iaea.org/MTCD/ Publications/PDF/Pub1342/Pub1342_web.pdf and the Nulcear Medicine Resources Manual. http://www-pub.iaea.org/mtcd/publications/pdf/pub1198_web.pdf
Radiopharmaceuticals
Methods of analysis: R3, biological methods
This is a draft proposed text for the Supplementary Information section of The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Note from the Secretariat: In principle, the Secretariat will aim to avoid conclusion of this test in order to avoid tests on animals. The following text is nevertheless proposed to replace the previous version as a general method of analysis.
The International Pharmacopoeia

260
WHO Drug Information Vol. 27, No. 3, 2013
R3.1 BiodistributionA physiological distribution test is prescribed for certain radiopharmaceutical preparations. Specific requirements are set out in individual monographs. The distribution pattern of radioactivity observed in specified organs, tissues or other body compartments of an appropriate animal species (usually small animals such as rats or mice) can be a reliable indication of the expected distribution in humans and thus of the suitability of the intended purpose. The individual monograph prescribes the details concerning the performance of the test and the physiological distribution requirements, which must be met for the radiopharmaceutical preparation. A physiological distribution conforming to the requirements will assure appropriate distribution of the radioactive compounds to the intended biological target in humans and limits its distribution to non-target areas. Determination of the biodistribution pattern is usually done in the development phase of a kit, radiopharmaceutical or revalidation of known compound.
Selection of animalsUsually healthy animals are used, except for certain special circumstances such as cancer models, which are drawn from a uniform stock that have not previously been treated with any material which will interfere with the test. If relevant, the species, sex, strain and weight and/or age of the animals are specified in the monograph. Unless otherwise stated, mice weigh not less than 20 g and not more than 30 g; rats weigh not less than 150 g and not more than 250 g; and guinea pigs (especially for cardiac radiopharmaceuticals) weigh not less than 250 g.
MethodPrepare the test radiopharmaceutical, draw required radioactivity in a small volume (e.g. 0.2 mL) into a 1 mL syringe. Inject the specified radioactivity (x) of the radio-pharmaceutical preparation into the tail vein of animals (usually three animals). Weight of the animals is measured in advance. Measure the radioactivity in the syringe before (y) and after the injection (z). Swab the injection site with cotton wool and retain the cotton wool and the residual dose in the syringe after injecting for counting (y) and (z), respectively.
Actual injected dose (a) = x-(y+z).
Immediately after injection, place each animal in a separate cage that is designed to allow collection of excreta and to prevent contamination of the body surface of the animal. After the time period specified in the monograph (uptake time), euthanize the animals. Collect a sample of blood by cardiac puncture and record the weight of the sample. Harvest the required organs, e.g., gall bladder, liver, stomach, intestines, bones and kidneys, and place in separate labelled counting tubes. Remove the tail above the injection site and place in a labelled counting tube. Determine the injected dose by an appropriate method depending on the activity.
Standard solutions of the radiopharmaceuticals are prepared. Draw 0.2 mL of the radiopharmaceutical solution in a syringe and estimate its weight by weighing the empty syringe and the syringe with solution and calculating the difference. Dispense this radiopharmaceutical solution into a clean 100 mL glass beaker and add 20 mL of distilled water. This solution is taken as the standard for estimation of the total activity that is injected into the animals. Corrections for different sample geometries are applied when necessary. Decay correction needs to be applied and times of
The International Pharmacopoeia

261
WHO Drug Information Vol. 27, No. 3, 2013
measurement are recorded. Measurements are done for three times and averaged. Background counts should be subtracted for each measurement.
The activity in the organs, tail and carcass is measured either in an isotope dose calibrator or in a NaI(Tl) crystal scintillation counter which is regularly calibrated.
Biodistribution can be calculated by the following methods.
Method A
The percentage activity in the organ is calculated as follows:
If using an isotope dose calibrator, the activity retained in the organs is calculated as:
If using a NaI(Tl) scintillation counter, the activity retained in the organs is calculated as:
The percentage of radioactivity in blood is determined according to the formula:
[100x(C/Ws) x 0.07 x (Wr) / a]
where C = Radioactivity in specimen of blood; Ws = weight in grams of blood specimen; Wr = weight in grams of animal. (Normally, blood is approx. 7% of total body weight.)
Method B
(ID/g) injected dose per gram of tissue
Where Ct = tissue concentration = activity / volume Vt = tissue volume Wt = tissue weight Dinj = dose injected
SpecificationThe preparation meets the requirements of the test if the distribution of radioactivity in at least two of the three animals complies with the criteria specified in the monograph. Disregard the results from any animal showing evidence of extravasation of the injection (observed at the time of injection or revealed by subsequent assay of tissue radioactivity).
Biodistribution studies by organ counting can be supplemented by the gamma camera imaging.
% injected activity in the organactivity obtained in the organ x 100–––––––––––––––––––––––––––––
total activity injected
% ID/g = Ct 100 Vt • 1 • ––– ––Wt Dinj ( % g )
The International Pharmacopoeia
% injected activity in the organ x 100 counts in organ –––––––––––––––––––––––––counts in standard ( Wi/Ws)x10] [
where Wi is the weight of injection and Ws is the weight of the standard.

262
WHO Drug Information Vol. 27, No. 3, 2013
In the development of new radiopharmaceuticals, repeat studies should be done for different time points of organ harvesting (e.g., 1-hour, 3-hour, 6-hour or 24 hour post injection) with a similar number of animals for same cohort group.
Radiopharmaceuticals: specific monograph
Natriiodidi (131i) solutioSodiumiodide (131i) solution
This is a draft revised proposal for The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Additional or amended text.
Monograph. Radiopharmaceuticals: Specific monographs: Natriiiodidi (131I) solutio - Sodium iodide (131I) solution
Latin. Natrii iodidi (131I) solutio.
English.Sodium iodide (131I) solution.
Structural formula. Na+ I-
Relative molecular mass. 153.895.
Empirical formula. Na 131I
Chemical name. Sodium (131I) iodide
Other names. Natrii radioiodidum, IodotopeSodium iodide I 131
Description. Sodium iodide (131I) solution is a clear colourless solution.Iodine-131 has a half-life of 8.08 days.
Category. Diagnostic or therapeutic.
Storage. Stored at room temperature. Preserve in single-dose or multiple-dose containers that previously have been treated to prevent adsorption.
Labelling.State the date and the time of calibration; the amount of 131I as iodide expressed as total MBq and the concentration expressed as MBq/ml, the expiration date, the name of any excipient, the name and quantity of any added preservative or stabilizer. The label states a statement of the intended use, whether oral or intravenous; a statement of whether the contents are intended for diagnostic or therapeutic use and the statement “Caution-Radioactive material”. The labelling indicates that in making dosage calculations, correction has to be made for radioactive decay, also indicates that the radioactive half-life of 131I is 8.08 days.
The International Pharmacopoeia

263
WHO Drug Information Vol. 27, No. 3, 2013
ManufactureIodine-131 may be obtained by neutron bombardment of tellurium or by extraction from uranium fission products. No carrier iodide is added.
Sodium iodide (131I) solution may contain sodium thiosulfate, sodium hydrogen carbonate or other suitable reducing agents and may contain a suitable buffer. Sodium iodide (131I) solution may be sterilized by «Heating in an autoclave» (see 5.8 Methods of sterilization).
Additional information.Wherever V is used within the tests of this monograph, V is the maximum recommended dose, in millilitres.
RequiRements
Complies with the monograph for “Liquid preparations for oral use”, “Parenteral Preparations” and with that for “Radiopharmaceuticals” as appropriate.
Definition. Sodium iodide solution is an aqueous solution containing of radioactive (131I) processed in the form of sodium iodide, suitable for either oral or intravenous administration. The solution contains not less than 90% and not more than 110% of the declared radioactivity due to iodine-131 stated on the label at the reference date and time. Not less than 99.9% of the total radioactivity is due to iodine-131. Not less than 95% of the total iodine-131 radioactivity is present as iodide. It contains minute amounts of naturally occurring iodine 127. The specific radioactivity is not less than 185 MBq (5 mCi) per microgram of iodine at the reference date and time stated on the label. The iodide content should not more than 20 µg in maximum recommended dose.
Identity tests
Either tests A and C or tests B and C may be applied.
A. Record the gamma-ray and X-ray spectrum using a suitable instrument with a sample of iodine-131, suitably diluted if needed. The spectrum is concordant with the reference spectrum of a specimen ofiodine-131 in that it exhibits a major peak of 364 keV. Standardized iodine-131 solutions are available from laboratories recognized by the relevant national or regional authority.
B. The half-life determined using a suitable detector system is between 184 and 203 hours.
C. Examine the radiochromatogram obtained in the test for radiochemical purity. The principal peak in the chromatogram obtained with the test solution (a) is similar in retention time to the principal peak in the chromatogram obtained with the reference solution (a).
pH value. Carry out the test as described under 1.13 Determination of pH or R1.5under the monograph for “Radiopharmaceuticals”. pH between 7.5 and 9.0 of the solutions intended for parenteral administration and between 7.5 and 10.0 of the solutions intended for oral administration.
Sterility. The solution complies with 3.2.1 Test for sterility of non-injectable preparations, modified as described in the monograph for “Radiopharmaceuticals”.
The International Pharmacopoeia

264
WHO Drug Information Vol. 27, No. 3, 2013
If intended for intravenous administration it complies with 3.2 Test for sterility for injectable preparation, modified as described in the monograph for “Radio-pharmaceuticals”. Test for sterility will be initiated on the day of manufacture. The solution may be released for use before completion of the test.
Bacterial endotoxinsCarry out the test as described under 3.4 Test for bacterial endotoxins, for solution intended for intravenous usemodified as described in the monograph for “Radiopharmaceuticals”. The injection contains not more than 175/V (I.U of endotoxins per millilitre).
Radionuclidic purity. Record the gamma-ray and X-ray spectrum using a suitable instrument and measure the half-life using a suitable method. Determine the relative amounts of iodine-131, iodine-133, iodine-135 and other radionuclidic impurities that may be present. Iodine-133 has a half-life of 20.8 hours and exhibits major peaks of 530 keV and 875 keV. Iodine-135 has a half-life of 6.55 hours and exhibits major peaks of 527 keV, 1132 keV and 1260 keV. Not less than 99.9% of the total radioactivity is due to iodine-131.
Chemical purityIodide. Carry out the test as descried under 1.14.4 High-performance liquid chromatography Prepare the test solution (a) which is the preparation to be examined. Prepare the test solution (b) by diluting test solution (a) using 0.05 M sodium hydroxideuntil the radioactivity is equivalent to about 74 MBq/ml and add an equal volume of a solution containing 1 g/L of potassium iodide R, 2 g/L of potassium iodate R and 10 g/L of sodiumhydrogen carbonate R and mix. The reference solution (a) is prepared by diluting 1 ml of a 26.2 mg/L solution of potassium iodide R to V with water R, (V being the maximum recommended dose in millilitres). Prepare the reference solution (b) by dilution 1 ml of a 24.5 mg/L solution of potassium iodate R to V with water R, (V being the maximum recommended dose in millilitres). Mix equal volumes of this solution and of reference solution (a).Prepare a solution containing 2 mg/ml of each of the components stated on the label, apart from iodide, used as blank solution. Use the column with (l = 0.25 m, Ø = 4.0 mm). The stationary phase is spherical base-deactivated end-capped octadecylsilyl silica gel for chromatography R (5 µm), maintain the temperature constant between 20 °C and 30 °C. Use stainless steel tubing.
Dissolve 5.844 g of sodium chloride R in 1000 mL of water R, add 650 µL of octylamine R and adjust to pH 7.0 with phosphoric acid R; add 50 mL of acetonitrile R and mix. Use the mixture as the mobile phase. The flow rate is 1.5 ml/min, the detector is spectrophotometer at 220 nm and radioactivity detector connected in series. Inject 25 µl of test solution (a), the blank solution and reference solutions (a) and (b). The run time is 12 minutes.
The relative retention with reference to iodide is 5 and to iodate is 0.2 to 0.3.
System suitability
Regarding the chromatogram due to the blank solution, none of the obtained peaks shows a retention time similar to that of the peak due to iodide. The resolution is a minimum of 2 between the peaks due to iodide and iodate in the chromatogram
The International Pharmacopoeia

265
WHO Drug Information Vol. 27, No. 3, 2013
obtained with reference solution (b) recorded with the spectrophotometer. The limit of iodide is detected by studying the chromatogram obtained with the spectrophotometer and comparing the peak due to iodide with the chromatogram due to reference solution (a).
The area of the peak due to iodide is not more than the area of the corresponding peak in the chromatogram obtained with reference solution (a).
Radiochemical purity
Either test A, B, or C may be applied:
A. Carry out the test as described under 1.14.2 Paper chromatography and ascending conditions, using paper for chromatography R (25- × 300-mm). Place a measured volume of a solution containing 100 mg of potassium iodide, 200 mg of potassium iodate, and 1 g of sodium bicarbonate and 25 mm from one end of the chromatographic paper. Allow the paper to dry. To the same area of the paper add an equal volume of appropriately diluted solution such that it provides a count rate of about 20,000 counts per minute and allow to dry. Develop the chromatogram over a period of about 4 hours by ascending chromatography, using dilute methanol (7.0 in 10). Allow the paper to dry in air, and determine the radioactivity distribution by scanning with a suitable radiation detector: the radioactivity of the iodide 131I band is not less than 95% of the total radioactivity, and its RF value falls within ±5% of the value found for sodium iodide when determined under parallel conditions.
Confirmation of the identity of the iodide band is made by the addition to the suspected iodide band of 6 drops of acidified hydrogen peroxide solution (prepared by adding 6 drops of 1 N hydrochloric acid to 10 mL of hydrogen peroxide solution) followed by the dropwise addition of starch TS; the development of a blue color indicates presence of iodide.
B. Carry out the test 1.14.4 High-performance liquid chromatography as described in the test for iodide with the following modification:
• Inject test solution (b)
• Detect Iodide limit by examination of the radioactivity detector, not less than 95 per cent of the total radioactivity is due to [131I] iodide.
C. Carry out the test as described under 1.15 Electrophoresis, Paper-electrophoresis Prepare paper strips, type Whatman No.3 MM for electrophoresis with dimensions of 65 × 3 cm.
Apply 10–20 μl samples in a distance of 10-13 cm from the end of the stripes. Use borate buffer with a concentration of 9 g/l and pH 9 ± 0.1.Carry out the electrophoresis on a potential of 900 V and time is 50 minutes.
The RF value for iodide is between 0.7 and 0.9, RF for iodate is 0.4, periodate from 0 to 0.1. Product can be accepted if the 131I anion content is higher than 95% even on the expiration date.
The International Pharmacopoeia

266
WHO Drug Information Vol. 27, No. 3, 2013
99m
H3C
H3C
H3C
CH3
CH3
CH3
H
H
H
N
NN
NO
OO
TC
Radioactivity. Measure the radioactivity as described under R.1.1 Detection and measurement of radioactivity in suitable calibrated counting equipment by comparison with a standardized iodine-131 solution or by measurement in an instrument calibrated with the aid of such a solution.
Standardized iodine-131 solutions are available from laboratories recognized by the relevant national or regional authority.
Impurities
[131I ] iodate ion.
Radiopharmaceuticals: specific monograph
Technetii (99Mtc) exametazimi multiplex injectioTechnetium (99Mtc) exametazime complex injection
This is a draft revised proposal for The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Additional or amended text.
Monograph. Radiopharmaceuticals: Specific monographs: Technetii (99mTc) exametazimi multiplex injectio – Technetium (99mTc) exametazime complex injection
Latin. Technetii (99mTc) exametazimi multiplex injection.
English. Technetium (99mTc) exametazime complex injection.
Structural formula
Empirical formula. C13H25N4O3.99mTc
Relative molecular mass. 384.269
The International Pharmacopoeia

267
WHO Drug Information Vol. 27, No. 3, 2013
Chemical name. Racemic mixture of (3RS,9RS)-4,8-diaza-3,6,6,9-tetramethylundecane-2,10-dione bisoxime complex with (99mTc) technetium.
Other names. (99mTc)-D,L-Hexamethylpropyleneamine oxime complex injection; (99mTc)-D,L-HMPAO injection.
Description. Technetium (99mTc) exametazime complex injection is a clear, colourless aqueous solution.
Technetium-99m has a half-life of 6.02 hours.
Category. Diagnostic.
Storage. Technetium (99mTc) exametazime complex injection should be kept at a temperature between 2°C to 8°C.
Technetium (99mTc) exametazime complex injection should be used within 30 minutes of reconstitution of the unlabelled kit with Technetium-99m, unless the preparation has been stabilized with either cobalt chloride solution or methylene blue solution.
Labelling. State the date and the time of calibration; the amount of 99mTc as labelled exametazime expressed as total MBq and the concentration expressed as MBq/ml; the expiration date; and the statement “Caution — Radioactive material”. The labelling indicates that in making dosage calculations, correction is to be made for radioactive decay, and indicates that the half- life of 99mTc is 6.02 hours. The label states that upon constitution with Sodium Pertechnetate 99mTc injection, beyond use time is 30 minutes for the unstabilized injection, and between 4 hours and 6 hours for the stabilized injections.
Manufacture. Technetium-99m is a radioactive nuclide formed by the radioactive decay of molybdenum-99. Molybdenum-99 is a radioactive isotope of molybdenum and may be produced by neutron irradiation of natural molybdenum or of molybdenum enriched in molybdenum-98 or it may be produced by uranium fission.
Technetium (99mTc) exametazime injection is prepared aseptically from sterile starting materials such as a sterile kit containing a mixture of (3RS, 9RS)-4, 8-diaza-3,6,6,9-tetramethylundecane-2,10-dione bisoxime and stannous salt with sodium pertechnetate (99mTc) injection (fission or non-fission). The injection may have the pH adjusted and may contain stabilizing agents. The injection may also be prepared under aseptic processing combined with sterilization by Filtration (see 5.8 Methods of sterilization).
Additional information. Wherever V is used within the tests of this monograph, V is the maximum recommended dose in millilitre.
RequiRements
Complies with the monograph for “Parenteral Preparations” and with that for “Radiopharmaceuticals”.
Definition. Technetium (99mTc) exametazime injection is a racemic mixture of (3RS, 9RS)-4, 8-diaza-3,6,6,9-tetramethylundecane-2,10-dione bisoxime (exametazime)
The International Pharmacopoeia

268
WHO Drug Information Vol. 27, No. 3, 2013
complexes with sodium pertechnetate (99mTc) injection (fission or non-fission) in presence of stannous salt. The injection is suitable for intravenous administration and contains sufficient sodium chloride to make the solution isotonic with blood. The content of technetium-99m is not less than 90% and not more than 110% of the content of technetium-99m. Not less than 80% of the total technetium-99m radioactivity is present as lipophilic (99mTc) exametazime complex.
Identity tests
Either tests A and C or tests B and C may be applied.
A. Record the gamma-ray spectrum using a suitable instrument with a sample of technetium-99m, suitably diluted if needed. The spectrum is concordant with the reference spectrum of a specimen of technetium-99m in that it exhibits a major peak of 140 keV.
Standardized technetium-99m solutions are available from competent laboratories recognized by the relevant national or regional authority.
B. The half-life determined using a suitable detector system is between 5.72 and 6.32 hours.
C. Examine the chromatograms obtained in the test Impurity A under Radiochemical purity. The principal peak in the chromatogram obtained with the test solution is similar in retention time to the peak due to lipophilic technetium-99m exametazime in the chromatogram obtained with the reference solution.
pH value. Carry out the test as described under 1.13 Determination of pH or R1.5 under the monograph for “Radiopharmaceuticals”. pH of the injection, between 5.0 to 10.0.
Sterility. The injection complies with 3.2 Test for sterility, modified as described in the monograph for “Radiopharmaceuticals”. Test for sterility will be initiated on the day of manufacture. The injection may be released for use before completion of the test.
Bacterial endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins, modified as described in the monograph for “Radiopharmaceuticals”. The injection contains not more than 175/V I.U of endotoxins per millilitre. The injection may be released for use before completion of the test.
Radionuclidic purity. Record the gamma-ray spectrum using a suitable instrument and measure the half-life using a suitable method. Determine the relative amounts of technetium-99m and radionuclidic impurities that may be present.
Radiochemical purity
Either test A or tests B and C may be applied.
A. Carry out three separate tests as described under 1.14.2 Paper chromatography and ascending conditions. Use suitable cellulose paper strips and methyl ethyl ketone R (system A) or sodium chloride (9 g/l) TS (system B) as the mobile phases.
The International Pharmacopoeia

269
WHO Drug Information Vol. 27, No. 3, 2013
Use suitable silica gel impregnated glass fiber paper strips and a mixture of equal volumes of acetonitrile R and water R as the mobile phase (system C). Apply to the paper about 5 μl of the injection to be examined, suitably diluted to give an optimum count rate and develop for a distance of about 15 cm. Allow the paper to dry in air and determine the radioactivity distribution by a suitable method. In system (A), the secondary exametazime complex and reduced hydrolysed technetium-99m have RF value of 0, and the lipophilic exametazime complex and the pertechnetate ion have RF value of 0.8 to 1.0. In system (B), reduced hydrolysed technetium-99m has RF value of 0, and the lipophilic exametazime complex, the secondary exametazime complex and the pertechnetate ion have an RF value of 0.8 to 1.0. In system (C), the pertechnetate ion has an RF value of 0.8 to 1.0, and the lipophilic exametazime complex, the secondary exametazime complex and reduced hydrolysed technetium-99m have RF value of 0. The sum of the percentages of radioactivity corresponding to the pertechnetate ion in system (C) and reduced hydrolysed technetium-99m in system (B) is less than 10%. Not less than 80% of the total technetium-99m radioactivity is present as lipophilic exametazime complex.
B. Impurity C. Carry out the test described under 1.14.1 Thin-layer chromatography for impurity C use TLC silica gel plate R, a glass fiber plate and 9 g/L solution of sodium chloride as a mobile phase. Apply to the plate about 5 μl of the injection to be examined, and develop immediately for a distance over 2/3 of the plate. Allow the plate to dry in air and determine the radioactivity distribution using a suitable detector. Impurity C has RF value of 0.8 to 1.0; lipophilic technetium-99m exametazime and impurities A, B, D and E do not migrate. The maximum limit of impurity C is 10 per cent of the total radioactivity.
C. Total of lipophilic technetium-99m exametazime and impurity A. Carry out the test under 1.14.1 Thin-layer chromatography. Use TLC silica gel plate R, a glass fiber plate and methyl ethyl ketone as a mobile phase. Apply to the plate about 5 μl of the injection to be examined, and develop immediately for a distance over 2/3 of the plate. Allow the plate to dry in air and determine the radioactivity distribution using a suitable detector. The lipophilic technetium-99m exametazime, impurities A and C have RF value of 0.8 to 1.0; for impurities B, D and E do not migrate.
Calculate the percentage of radioactivity due to impurities B, D and E from test C and the percentage of the radioactivity due to impurity C from test B. Calculate the total percentage of lipophilic technetium-99m exametazime and impurity A from the expression: 100-A-B.
Not less than 80% of the total technetium-99m radioactivity is present as lipophilic technetium 99m exametazime and impurity A.
Impurity A. Carry out the test as descried under 1.14.4 High-performance liquid chromatography Prepare the reference solution by dissolving the contents of a vial of meso-rich exametazime CRS in 0.5 ml of a 9 g/L solution of sodium chloride and transfer to lead-shielded nitrogen-filled vial. Add 6 µL of a freshly prepared 1 g/L solution of stannous chloride R in 0.05 M hydrochloric acid and 2.5 mL of sodium pertechnetate (99mTc) injection (fission or non-fission) containing 370-740 MBq. Mix carefully and use within 30 min of preparation. The size of the column used is (l = 0.25 m, Ø = 4.6 mm). The stationary phase is spherical base-deactivated end-capped octadecylsilyl silica gel for chromatography R (5 µm) with a pore size of 13 nm
The International Pharmacopoeia

270
WHO Drug Information Vol. 27, No. 3, 2013
99m
H3C
H3C
H3C
CH3
CH3
CH3
H
H
H
N
N N
NO
OO
TC
and a carbon loading of 11 per cent. Mix 33 volumes of acetonitrile R and 67 volumes of 0.1 M phosphate buffer solution R pH 3.0 to use as mobile phase. The flow rate is 1.5 mL/min, the detector is radioactivity detector with loop injector the run time is 20 min. The relative retention with reference to lipophilic technetium-99m exametazime to impurity A is about 1.2.
System suitability: reference solutionThe produced chromatogram is similar to the chromatogram provided with meso-rich exametazime CRS. The resolution is a minimum of 2 between the peaks due to lipophilic technetium-99m exametazime and to impurity A. Impurity A should not more than 5 per cent of the radioactivity due to lipophilic technetium-99m exametazime and impurity A.
Chemical purity
Tin. Carry out the test as described under R2.1.4 Tin estimation by UV absorption, using 1.0 ml of a test solution prepared by diluting 1.5 ml of the injection to be examined to 25.0 ml with hydrochloric acid (1 mol/l) VS and mixing thoroughly. Prepare the reference solution by dissolving 0.115 g of stannous chloride R in hydrochloric acid (1 mol/l) VS, diluting to 1000 ml with the same solvent and mixing thoroughly. The absorbance of the test solution is not greater than that of the reference solution; not more than 0.6 µg of Sn per ml.
Radioactivity. Measure the radioactivity as described under R.1.1 Detection and measurement of radioactivity in a suitable calibrated counting equipment by comparison with a standardized technetium-99m solution or by measurement in an instrument calibrated with the aid of such a solution (a good approximation may be obtained using an ionization chamber and employing a standardized solution of cobalt-57 provided that correction for the differences in the radiations emitted are made).
Standardized technetium-99m and cobalt-57 solutions are available from laboratories recognized by the relevant national or regional authority.
Impurities
The International Pharmacopoeia

271
WHO Drug Information Vol. 27, No. 3, 2013
A. Meso isomer of lipophilic technetium-99m exametazime, B. Technetium-99m in colloidal form, C. [99mTc] pertechnetate ion,D. Non lipophilic technetium-99m exametazime complex,E. Meso isomer of non-lipophilic technetium-99m exametazime complex.
Biodistribution. Carry out the test as described under R3.1 Biological distribution using a set of three mice. At 5 to10 minutes post injection not less than 1.5% of the injected radioactivity should be found in the brain and not more than 20% of the injected radioactivity should be found in the intestine. Not more than 15% of the injected radioactivity should be found in the liver.
Radiopharmaceuticals: specific monograph
thallosi (201tl) chloridi Injectiothallous (201tl) chloride injection
This is a draft revised proposal for The International Pharmacopoeia (June 2013). Please address any comments to Quality Assurance and Safety: Medicines, World Health Organization, 1211 Geneva 27, Switzerland. Fax: +41 22 791 4730 or e-mail to [email protected]. Working documents are available for comment on-line at http://www.who.int/medicines.
Additional or amended text.
Monograph. Radiopharmaceuticals: Specific monographs: Thallosi (201Tl) chloridi injectio – Thallous (201Tl) chloride injection
Latin. Thallosi (201Tl) chloridi injectio
English. Thallous (201Tl) chloride injection
Structural formula. Tl+ Cl-
Empirical formula. 201TlCl
Relative molecular mass. 236.423
Chemical name. Thallium (201Tl) chloride
Other names. Thallous (201Tl) chloride
Description. Thallous (201Tl) chloride injection is a clear colourless, aqueous solution.
Thallium-201 has a half-life of 73.1 hours.
Category. Diagnostic.
The International Pharmacopoeia

272
WHO Drug Information Vol. 27, No. 3, 2013
Storage. After aseptic withdrawal of the first dose from a multidose container, the container should be stored at a temperature between 2°C to 8°C and the contents used within 7 days.
Labelling. State the date of withdrawal of the first dose for multidose containers. State the time and date of calibration; the amount of 201Tl as labeled thallous chloride expressed as total MBq and concentration as expressed as MBq/ml at the time of calibration; the expiration date ; and the statement “Caution—Radioactive Material.” The labeling indicates that in making dosage calculations, correction is to be made for radioactive decay, and also indicates that the radioactive half-life of 201Tl is 73.1 hours.
ManufactureNo-carrier-added thallium-201 radioisotope is produced by proton bombardment of enriched thallium 203 target followed by chemical separation of lead 201 radioactive isotopes. The separated lead isotope decay in optimum 32 hours into thallium 201 by electron capture or positron emission Separation of thallium-201 may be done using anion-exchange resin chromatography or solvent– extraction.
Thallous (201Tl) chloride injection may be sterilized by «Heating in an autoclave» (see 5.8 Methods of Sterilization).
Additional informationWherever V is used within the tests of this monograph, V is the maximum recommended dose in millilitres.
RequiRements
Complies with the monograph for “Parenteral Preparations” and with that for “Radiopharmaceuticals”.
Definition. Thallous (201Tl) chloride injection is a sterile, isotonic, aqueous solution of thallium-201 as thallous chloride, suitable for intravenous administration. It contains sufficient sodium chloride to make the solution isotonic with blood and may contain suitable antimicrobial preservatives such as benzyl alcohol or stabilizing agents.
The injection contains not less than 90% and not more than 110% of the content of thallium-201 at the reference date and time stated on the label. Not less than 97% of the total radioactivity is due to thallium-201. Not more than 2% of the total radioactivity is due to thallium-202. The specific radioactivity is not less than 3.7 GBq (100 mCi) of thallium-201 per milligram of thallium at the reference date and time stated on the label.
Identity tests
Either tests A and C or tests B and C may be applied.
A. Record the gamma-ray using a suitable instrument with a sample of thallium-201, suitably diluted if needed. The spectrum is concordant with the reference spectrum of a specimen of thallium-201 in that it exhibits major peaks of 135, 166, and 167keV and X-rays of 69 and 83keV.
Standardized thallium-201 solutions are available from laboratories recognized by the relevant national or regional authority.
The International Pharmacopoeia

273
WHO Drug Information Vol. 27, No. 3, 2013
B. The half-life determined using a suitable detector system is between 70 and 75 hours.
C. Examine the electropherogram obtained in the test for radiochemical purity. The distribution of the radioactivity contributes to the identification of the preparation.pH value. Carry out the test as described under 1.13 Determination of pH or R1.5 under the monograph for “Radiopharmaceuticals”. pH of the injection, 4.0 to 7.0.
Sterility. The injection complies with 3.2 Test for sterility, modified as described in the monograph for “Radiopharmaceuticals”. Test for sterility will be initiated on the day of manufacture. The injection may be released for use before completion of the test.Bacterial endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins, modified as described in the monograph for “Radiopharmaceuticals”. The injection contains not more than 175/V (I.U. of endotoxins per millilitre). The injection may be released for use before completion of the test.
Radionuclidic purity. Record the gamma-ray and X-ray spectrum using a suitable instrument and measure the half-life using a suitable method. Determine the relative amounts of thallium-200, thallium-201, thallium-202, lead-201, lead 203 and other radionuclidic impurities that may be present. Thallium-202 has a half-life of 12.2 days and exhibits a main peak of 440 keV. Thallium-200 has a half-life of 1.09 days and exhibits main peaks of 368, 579, 828 and 1206 keV. Lead-201 has a half-life of 9.4 hours and exhibits a main peak of 331 keV. Lead-203 has a half-life of 2.17 days and exhibits a main peak of 270 keV. Not less than 97% of the total radioactivity is due to thallium-201. Not more than 2% of the total radioactivity is due to thallium-202.
Standardized solutions of thallium-201 and thallium-202, are available from laboratories recognized by the relevant national or regional authority.
Radiochemical purity. Carry out the test as described under 1.15 Electrophoresis, zone-electrophoresis Prepare a suitable cellulose polyacetate strip as the supporting medium and soak the strip in a solution of disodium edetate R (18.6 g/L) as the electrolyte solution. Soak the strip in the electrolyte solution for 45-60 min. Remove the strip with forceps taking care to handle the outer edges only. Place the strip between 2 absorbent pads and blot to remove excess solution. Apply not less than 5 µl of a mixture of equal volumes of the preparation to be examined and the electrolyte solution to the centre of the blotted strip and mark the point of application. Attach the strip to the support bridge of an electrophoresis chamber containing equal volumes of disodium edetate R in each side of the chamber. Ensure that each end of the strip is in contact with the disodium edetate R. Apply an electric field of 250 volts for at 30 minutes. Allow the strip to dry in air. Determine the distribution of radioactivity using suitable detector.
Not less than 95% of the radioactivity on the strip migrates towards the cathode as a single peak.
Chemical purity
Thallium. Transfer 1.0 ml of the injection and 1.0 ml of thallium standard (2 µg/ml Tl) TS to separate screw-cap test tubes. To each tube, add the following five solutions (A, B, C, D and E) and mix after each addition: 2 drops of a solution prepared by
The International Pharmacopoeia

274
WHO Drug Information Vol. 27, No. 3, 2013
carefully mixing 18 ml of nitric acid (~1000 g/l) TS and 82 ml of hydrochloric acid (~250 g/l) TS (solution A); 1.0 ml of sulfosalicylic acid (0.1 mol/l) VS (solution B); 2 drops of hydrochloric acid (~250 g/l) TS (solution C); 4 drops of a solution prepared by dissolving 50 mg of rhodamine B R in hydrochloric acid (~250 g/l) TS and diluting to 100.0 ml (solution D); 1.0 ml of diisopropyl ether R (solution E). Screw the caps on tightly, shake the tubes by hand for exactly 1 minute, releasing any pressure build-up by loosening the caps slightly. Recap the tubes and allow the phases to separate.
Transfer 0.5 ml of the ether layer from each tube to clean tubes. The color of the ether layer obtained from the injection is not darker than that from the thallium standard (2 µg/ml Tl) TS.
Iron. Into separate cavities of a spot plate, place 0.1 ml of the injection and 0.1 ml of iron standard TS diluted with water R to a concentration of 5 µg/ml. Add to each cavity 0.1 ml of a solution of hydroxylamine hydrochloride R (1 in 10), 1 ml of a solution of sodium acetate R (1 in 4), and 0.1 ml of a 0.5% dipyridyl solution prepared by dissolving 0.5 g of 2,2’-dipyridyl R in 100 ml of water R containing 0.15 ml of hydrochloric acid (~250 g/l) TS, and mix. After 5 minutes, the colour obtained from the injection is not darker than that of the iron standard solution.
Copper. Into separate cavities of a spot plate, place 0.2 ml of the injection and 0.2 ml of copper standard (5 µg/ml Cu) TS. Add to each cavity the following 3 solutions (A, B and C) and mix after each addition: 0.2 ml of water R (solution A) and 0.1 ml of a solution of iron thiocyanate prepared by dissolving 1.5 g of ferric chloride R and 2 g of potassium thiocyanate R in water R and diluting to 100.0 ml with the same solvent (solution B); 0.1 ml of a solution of sodium thiosulphate R (1 in 100) (solution C). The time required for the injection to decolorize is equal to or longer than that observed for the copper standard solution.
Radioactivity. Measure the radioactivity as described under R.1.1 Detection and measurement of radioactivity in suitable calibrated counting equipment by comparison with a standardized thallium-201 solution or by measurement in an instrument calibrated with the aid of such a solution.
Standardized thallium-201 solutions are available from laboratories recognized by the relevant national or regional authority.
Impurities
A. Lead-201
B. Lead-203
C. Thallium-200
D. Thallium-202
E. [201Tl] Thallic (III) ion.
Biodistribution. Carry out the test as described under R3.1 Biological distribution using a set of three guinea pigs. At 1 hour post injection not less than 4% of the injected radioactivity should be found in the heart.
The International Pharmacopoeia

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
275
International Nonproprietary Names for Pharmaceutical Substances (INN)
RECOMMENDED International Nonproprietary Names: List 70 Notice is hereby given that, in accordance with paragraph 7 of the Procedure for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances [Off. Rec. Wld Health Org., 1955, 60, 3 (Resolution EB15.R7); 1969, 173, 10 (Resolution EB43.R9); Resolution EB115.R4 (EB115/2005/REC/1)], the following names are selected as Recommended International Nonproprietary Names. The inclusion of a name in the lists of Recommended International Nonproprietary Names does not imply any recommendation of the use of the substance in medicine or pharmacy. Lists of Proposed (1–105) and Recommended (1–66) International Nonproprietary Names can be found in Cumulative List No. 14, 2011 (available in CD-ROM only).
Dénominations communes internationales des Substances pharmaceutiques (DCI)
Dénominations communes internationales RECOMMANDÉES: Liste 70 Il est notifié que, conformément aux dispositions du paragraphe 7 de la Procédure à suivre en vue du choix de Dénominations communes internationales recommandées pour les Substances pharmaceutiques [Actes off. Org. mond. Santé, 1955, 60, 3 (résolution EB15.R7); 1969, 173, 10 (résolution EB43.R9); résolution EB115.R4 (EB115/2005/REC/1)] les dénominations ci-dessous sont choisies par l’Organisation mondiale de la Santé en tant que dénominations communes internationales recommandées. L’inclusion d’une dénomination dans les listes de DCI recommandées n’implique aucune recommandation en vue de l’utilisation de la substance correspondante en médecine ou en pharmacie. On trouvera d’autres listes de Dénominations communes internationales proposées (1–105) et recommandées (1–66) dans la Liste récapitulative No. 14, 2011 (disponible sur CD-ROM seulement).
Denominaciones Comunes Internacionales para las Sustancias Farmacéuticas (DCI) Denominaciones Comunes Internacionales RECOMENDADAS: Lista 70 De conformidad con lo que dispone el párrafo 7 del Procedimiento de Selección de Denominaciones Comunes Internacionales Recomendadas para las Sustancias Farmacéuticas [Act. Of. Mund. Salud, 1955, 60, 3 (Resolución EB15.R7); 1969, 173, 10 (Resolución EB43.R9); Résolution EB115.R4 (EB115/2005/REC/1) EB115.R4 (EB115/2005/REC/1)], se comunica por el presente anuncio que las denominaciones que a continuación se expresan han sido seleccionadas como Denominaciones Comunes Internacionales Recomendadas. La inclusión de una denominación en las listas de las Denominaciones Comunes Recomendadas no supone recomendación alguna en favor del empleo de la sustancia respectiva en medicina o en farmacia. Las listas de Denominaciones Comunes Internacionales Propuestas (1–105) y Recomendadas (1–66) se encuentran reunidas en Cumulative List No. 14, 2011 (disponible sólo en CD-ROM).

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
276
Latin, English, French, Spanish: Recommended INN DCI Recommandée DCI Recomendada
Chemical name or description; Molecular formula; Graphic formula Nom chimique ou description; Formule brute; Formule développée Nombre químico o descripción; Fórmula molecular; Fórmula desarrollada
abiciparum pegolum # abicipar pegol pegylated composite protein for clinical applications (CPCA), with
alternative scaffold domain to antigen receptors based on ankyrin repeats, anti-[Homo sapiens VEGFA (vascular endothelial growth factor A, VEGF-A, VEGF)]; glycyl-seryl-ankyrin repeats (3-35, 36-68, 69-101, 102-123)-lysyl-dialanyl-bis(triglycyl-seryl) linker (127-134)-cysteinyl (1-135), conjugated via a maleimide group linker (thioether bond to C135) to a single linear methoxy polyethylene glycol 20 (mPEG20)
abicipar pégol protéine composite pour applications cliniques (CPCA) pégylée, avec une charpente de domaine alternative aux récepteurs d'antigènes basée sur des répétitions ankyrine, anti-[Homo sapiens VEGFA (vascular endothelial growth factor A, VEGF-A, VEGF)]; glycyl-séryl-domaine à répétitions ankyrine (3-35, 36-68, 69-101, 102-123)-lysyl-dialanyl-linker bis(triglycyl-séryl) (127-134)-cystéinyl (1-135), conjugué via un linker du groupe maléimide (liaison thioéther à C135) à une molécule linéaire unique de méthoxy polyéthylène glycol 20 (mPEG20)
abicipar pegol proteína compuesta para aplicaciones clínicas (CPCA) pegilada, con una estructura de dominio alternativa a los receptores de antígenos basada en repeticiones de la ankirina, anti-[Homo sapiens VEGFA (factor A de crecimiento endotelial vascular, VEGF-A, VEGF)]; glicil-seril-dominio de repeticiones de ankirina (3-35, 36-68, 69-101, 102-123)-lisil-dialanil-conector bis(triglicil-seril) (127-134)-cisteinil (1-135), conjugado mediante un conector maleimida (enlace tioéter en C135) en una molécula lineal única de metoxi polietilenglicol 20 (mPEG20)
C617H969N173O199S2 (protein component)
GSDLDKKLLE AARAGQDDEV RILMANGADV NARDSTGWTP LHLAAPWGHP 50EIVEVLLKNG ADVNAADFQG WTPLHLAAAV GHLEIVEVLL KYGADVNAQD 100KFGKTAFDIS IDNGNEDLAE ILQKAAGGGS GGGSC 135
afoxolanerum afoxolaner 4-{5-[3-chloro-5-(trifluoromethyl)phenyl]-5-(trifluoromethyl)-
4,5-dihydro-1,2-oxazol-3-yl}-N-{2-oxo-2-[(2,2,2-trifluoroethyl)amino]ethyl}naphthalene-1-carboxamide
afoxolaner 4-{5-[3-chloro-5-(trifluorométhyl)phényl]-5-(trifluorométhyl)- 4,5-dihydro-1,2-oxazol-3-yl}-N-{2-oxo-2-[(2,2,2-trifluoroéthyl)amino]éthyl}naphtalène-1-carboxamide
afoxolaner 4-{5-[3-cloro-5-(trifluorometil)fenil]-5-(trifluorometil)-4,5-dihidro- 1,2-oxazol-3-il}-N-{2-oxo-2-[(2,2,2-trifluoroetil)amino]etil}naftaleno- 1-carboxamida

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
277
C26H17ClF9N3O3
HN
NH
CF3
O
O
NOF3C
Cl
F3Cand enantiomeret énantiomèrey enantiómero
afuresertibum afuresertib N-[(2S)-1-amino-3-(3-fluorophenyl)propan-2-yl]-5-chloro-4-(4-chloro-
1-methyl-1H-pyrazol-5-yl)thiophene-2-carboxamide
afurésertib N-[(2S)-1-amino-3-(3-fluorophényl)propan-2-yl]-5-chloro-4-(4-chloro-1-méthyl-1H-pyrazol-5-yl)thiophène-2-carboxamide
afuresertib N-[(2S)-1-amino-3-(3-fluorofenil)propan-2-il]-5-cloro-4-(4-cloro- 1-metil-1H-pirazol-5-il)tiofeno-2-carboxamida
C18H17Cl2FN4OS
O
HN
H
F
NH2
S
Cl
N N
CH3
Cl
albutrepenonacogum alfa # albutrepenonacog alfa human coagulation factor IX (EC 3.4.21.22, Christmas factor, plasma
thromboplastin component) 148-threonine variant fusion protein with prolyl(human coagulation factor IX 148-threonine variant-(137-153)-peptide) fusion protein with human serum albumin, produced in CHO cells (alfa glycoform)
albutrépénonacog alfa variant 148-thréonine du facteur IX humain de la coagulation (EC 3.4.21.22, facteur Christmas, facteur antihémophilique B) protéine de fusion avec le prolyl(variant 148-thréonine du facteur IX humain de la coagulation-(137-153)-peptide), protéine de fusion avec l'albumine sérique humaine, produit par culture de cellules CHO (glycoforme alfa)
albutrepenonacog alfa variante 148-treonina del factor IX humano de coagulación (EC 3.4.21.22, factor Christmas, factor antihemofílico B) proteína de fusión con prolil(variante 148-treonina del factor IX humano de la coagulación-(137-153)-péptido), proteína de fusión con albumina sérica humana, producida por cultivo de células CHO (glicoforma alfa)

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
278
C5077H7846N1367O1588PS67 (peptide)
HO2C CO2H
NH2HHO2C
CO2H
NH2HO
SHO
O O
HO2CCO2H
NH2H
OH
OCO2H
NH2H
PO
HO OH
E7-8-15-17-20-21-26
27-30-33-36-404-carboxyGlu
Y155
O-sulfoTyr
D64
3-hydroxyAsp
S158
O-phosphonoSer
Sequence / Séquence / SecuenciaYNSGKLEEFV QGNLERECME EKCSFEEARE VFENTERTTE FWKQYVDGDQ 50CESNPCLNGG SCKDDINSYE CWCPFGFEGK NCELDVTCNI KNGRCEQFCK 100NSADNKVVCS CTEGYRLAEN QKSCEPAVPF PCGRVSVSQT SKLTRAETVF 150PDVDYVNSTE AETILDNITQ STQSFNDFTR VVGGEDAKPG QFPWQVVLNG 200KVDAFCGGSI VNEKWIVTAA HCVETGVKIT VVAGEHNIEE TEHTEQKRNV 250IRIIPHHNYN AAINKYNHDI ALLELDEPLV LNSYVTPICI ADKEYTNIFL 300KFGSGYVSGW GRVFHKGRSA LVLQYLRVPL VDRATCLRST KFTIYNNMFC 350AGFHEGGRDS CQGDSGGPHV TEVEGTSFLT GIISWGEECA MKGKYGIYTK 400VSRYVNWIKE KTKLTPVSQT SKLTRAETVF PDVDAHKSEV AHRFKDLGEE 450NFKALVLIAF AQYLQQCPFE DHVKLVNEVT EFAKTCVADE SAENCDKSLH 500TLFGDKLCTV ATLRETYGEM ADCCAKQEPE RNECFLQHKD DNPNLPRLVR 550PEVDVMCTAF HDNEETFLKK YLYEIARRHP YFYAPELLFF AKRYKAAFTE 600CCQAADKAAC LLPKLDELRD EGKASSAKQR LKCASLQKFG ERAFKAWAVA 650RLSQRFPKAE FAEVSKLVTD LTKVHTECCH GDLLECADDR ADLAKYICEN 700QDSISSKLKE CCEKPLLEKS HCIAEVENDE MPADLPSLAA DFVESKDVCK 750NYAEAKDVFL GMFLYEYARR HPDYSVVLLL RLAKTYETTL EKCCAAADPH 800ECYAKVFDEF KPLVEEPQNL IKQNCELFEQ LGEYKFQNAL LVRYTKKVPQ 850VSTPTLVEVS RNLGKVGSKC CKHPEAKRMP CAEDYLSVVL NQLCVLHEKT 900PVSDRVTKCC TESLVNRRPC FSALEVDETY VPKEFNAETF TFHADICTLS 950EKERQIKKQT ALVELVKHKP KATKEQLKAV MDDFAAFVEK CCKADDKETC 1000FAEEGKKLVA ASQAALGL 1018
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro18-23 51-62 56-71 73-82 88-99 95-109 111-124132-289 206-222 336-350 361-389 486-495 508-524 523-534557-602 601-610 633-679 678-686 698-712 711-722 749-794793-802 825-871 870-881 894-910 909-920 947-992 991-1000
Modified residues / Résidus modifiés / Restos modificados
Glycosylation sites (N,S,T) / Sites de glycosylation (N,S,T) / Posiciones de glicosilación (N,S,T)Ser-53* Ser-61* Asn-157 Thr-159* Asn-167 Thr-169* Thr-172* Thr-179** potential sites / sites potentiels / posiciones posibles
aldoxorubicinum aldoxorubicin N'-[(1E)-1-{(2S,4S)-4-[(3-amino-2,3,6-trideoxy-α-L-lyxo-
hexopyranosyl)oxy]-2,5,12-trihydroxy-7-methoxy-6,11-dioxo-1,2,3,4,6,11-hexahydrotetracen-2-yl}-2-hydroxyethylidene]- 6-(2,5-dioxo-2,5-dihydro-1H-pyrrol-1-yl)hexanohydrazide
aldoxorubicine N'-[(1E)-1-{(2S,4S)-4-[(3-amino-2,3,6-tridéoxy-α-L-lyxo-hexopyranosyl)oxy]-2,5,12-trihydroxy-7-méthoxy-6,11-dioxo-1,2,3,4,6,11-hexahydrotétracén-2-yl}-2-hydroxyéthylidène]- 6-(2,5-dioxo-2,5-dihydro-1H-pyrrol-1-yl)hexanohydrazide
aldoxorubicina N'-[(1E)-1-{(2S,4S)-4-[(3-amino-2,3,6-tridesoxi-α-L-lyxo-hexopiranosil)oxi]-2,5,12-trihidroxi-7-metoxi-6,11-dioxo- 1,2,3,4,6,11-hexahidrotetracen-2-il}-2-hidroxietilideno]- 6-(2,5-dioxo-2,5-dihidro-1H-pirrol-1-il)hexanohidrazida

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
279
C37H42N4O13
OHO
O OH
OH
N
H O
O
OH
NH2
CH3
OCH3
OH
NH
ON
O
O
alectinibum alectinib 9-ethyl-6,6-dimethyl-8-[4-(morpholin-4-yl)piperidin-1-yl]-11-oxo-
6,11-dihydro-5H-benzo[b]carbazole-3-carbonitrile
alectinib 9-éthyl-6,6-diméthyl-8-[4-(morpholin-4-yl)pipéridin-1-yl]-11-oxo- 6,11-dihydro-5H-benzo[b]carbazole-3-carbonitrile
alectinib 9-etil-6,6-dimetil-8-[4-(morfolin-4-il)piperidin-1-il]-11-oxo-6,11-dihidro-5H-benzo[b]carbazol-3-carbonitrilo
C30H34N4O2
NH
CN
N
N
O
O
H3C
H3C CH3
apitolisibum apitolisib (2S)-1-(4-{[2-(2-aminopyrimidin-5-yl)-7-methyl-4-(morpholin-
4-yl)thieno[3,2-d]pyrimidin-6-yl]methyl}piperazin-1-yl)- 2-hydroxypropan-1-one
apitolisib (2S)-1-(4-{[2-(2-aminopyrimidin-5-yl)-7-méthyl-4-(morpholin- 4-yl)thiéno[3,2-d]pyrimidin-6-yl]méthyl}pipérazin-1-yl)- 2-hydroxypropan-1-one
apitolisib (2S)-1-(4-{[2-(2-aminopirimidin-5-il)-7-metil-4-(morfolin-4-il)tieno[3,2-d]pirimidin-6-il]metil}piperazin-1-il)-2-hidroxipropan-1-ona
C23H30N8O3S
N
NCH3
O
S
N
N
H3C
N
O
N
N
H2N
H OH

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
280
belnacasanum belnacasan 1-[(2S)-2-(4-amino-3-chlorobenzamido)-3,3-dimethylbutanoyl]-
N-[(2R,3S)-2-ethoxy-5-oxooxolan-3-yl]-L-prolinamide
belnacasan 1-[(2S)-2-(4-amino-3-chlorobenzamido)-3,3-diméthylbutanoyl]- N-[(2R,3S)-2-éthoxy-5-oxooxolan-3-yl]-L-prolinamide
belcanasán 1-[(2S)-2-(4-amino-3-clorobenzamido)-3,3-dimetilbutanoil]- N-[(2R,3S)-2-etoxi-5-oxooxolan-3-il]-L-prolinamida
C24H33ClN4O6
O
H
NH
OH
N
HN
H O
OO
CH3
H3C
H3C
O
H2N
ClH
CH3
bimagrumabum # bimagrumab immunoglobulin G1-lambda2, anti-[Homo sapiens ACVR2B (activin
A receptor type IIB, ActR-IIB, ActRIIB) and ACVR2A (activin A receptor type IIA, ActR-II, ActRIIA)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-445) [Homo sapiens VH (IGHV1-2*02 (91.80%) -(IGHD)-IGHJ5*01 [8.8.8] (1-115) -IGHG1*03 (CH1 (116-213), hinge (214-228), CH2 L1.3>A (232), L1.2>A (233) (229-338), CH3 (339-443), CHS (444-445)) (116-445)], (218-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV2-23*02 (90.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimer (224-224'':227-227'')-bisdisulfide
bimagrumab immunoglobuline G1-lambda2, anti-[Homo sapiens ACVR2B (récepteur type IIB de l'activine A, ActR-IIB, ActRIIB) et ACVR2A (recepteur type IIA de l’activine A, ActR-II, ActRIIA)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-445) [Homo sapiens VH (IGHV1-2*02 (91.80%) -(IGHD)-IGHJ5*01 [8.8.8] (1-115) -IGHG1*03 (CH1 (116-213), charnière (214-228), CH2 L1.3>A (232), L1.2>A (233) (229-338), CH3 (339-443), CHS (444-445)) (116-445)], (218-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV2-23*02 (90.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimère (224-224'':227-227'')-bisdisulfure
bimagrumab inmunoglobulina G1-lambda2, anti-[Homo sapiens ACVR2B (receptor tipo IIB de la activina A, ActR-IIB, ActRIIB) y ACVR2A (receptor tipo IIA de la activina A, ActR-II, ActRIIA)], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma1 (1-445) [Homo sapiens VH (IGHV1-2*02 (91.80%) -(IGHD)-IGHJ5*01 [8.8.8] (1-115) -IGHG1*03 (CH1 (116-213), bisagra (214-228), CH2 L1.3>A (232), L1.2>A (233) (229-338), CH3 (339-443), CHS (444-445)) (116-445)], (218-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV2-23*02 (90.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dímero (224-224'':227-227'')-bisdisulfuro

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
281
Heavy chain / Chaîne lourde / Cadena pesada
QVQLVQSGAE VKKPGASVKV SCKASGYTFT SSYINWVRQA PGQGLEWMGT 50INPVSGSTSY AQKFQGRVTM TRDTSISTAY MELSRLRSDD TAVYYCARGG 100WFDYWGQGTL VTVSSASTKG PSVFPLAPSS KSTSGGTAAL GCLVKDYFPE 150PVTVSWNSGA LTSGVHTFPA VLQSSGLYSL SSVVTVPSSS LGTQTYICNV 200NHKPSNTKVD KRVEPKSCDK THTCPPCPAP EAAGGPSVFL FPPKPKDTLM 250ISRTPEVTCV VVDVSHEDPE VKFNWYVDGV EVHNAKTKPR EEQYNSTYRV 300VSVLTVLHQD WLNGKEYKCK VSNKALPAPI EKTISKAKGQ PREPQVYTLP 350PSREEMTKNQ VSLTCLVKGF YPSDIAVEWE SNGQPENNYK TTPPVLDSDG 400SFFLYSKLTV DKSRWQQGNV FSCSVMHEAL HNHYTQKSLS LSPGK 445
Light chain / Chaîne légère / Cadena ligeraQSALTQPASV SGSPGQSITI SCTGTSSDVG SYNYVNWYQQ HPGKAPKLMI 50YGVSKRPSGV SNRFSGSKSG NTASLTISGL QAEDEADYYC GTFAGGSYYG 100VFGGGTKLTV LGQPKAAPSV TLFPPSSEEL QANKATLVCL ISDFYPGAVT 150VAWKADSSPV KAGVETTTPS KQSNNKYAAS SYLSLTPEQW KSHRSYSCQV 200THEGSTVEKT VAPTECS 217
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 142-198 259-319 365-423 22''-96'' 142''-198'' 259''-319'' 365''-423''Intra-L 22'-90' 139'-198' 22'''-90''' 139'''-198''' Inter-H-L 218-216' 218''-216''' Inter-H-H 224-224'' 227-227''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:295, 295''
brilacidinum brilacidin N4,N6-bis[3-{[5-(carbamimidamido)pentanoyl]amino}-
2-{[(3R)-pyrrolidin-3-yl]oxy}-5-(trifluoromethyl)phenyl]pyrimidine- 4,6-dicarboxamide
brilacidine N4,N6-bis[3-{[5-(carbamimidamido)pentanoyl]amino}- 2-{[(3R)-pyrrolidin-3-yl]oxy}-5-(trifluorométhyl)phényl]pyrimidine- 4,6-dicarboxamide
brilacidina N4,N6-bis[3-{[5-(carbamimidamido)pentanoil]amino}- 2-{[(3R)-pirrolidin-3-il]oxi}-5-(trifluorometil)fenil]pirimidina- 4,6-dicarboxamida
C40H50F6N14O6
N NHN
HN
O O
OO
F3CCF3
HN O
HNO
NHHN
NH
NH2
NH
H2N
H
NH
H
HN

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
282
concizumabum # concizumab immunoglobulin G4-kappa, anti-[Homo sapiens TFPI (tissue factor
pathway inhibitor, lipoprotein-associated coagulation inhibitor)], humanized monoclonal antibody; gamma4 heavy chain (1-448) [humanized VH (Homo sapiens IGHV3-21*01 (85.70%) -(IGHD)-IGHJ3*01 M11>T (116)) [8.8.14] (1-121) -Homo sapiens IGHG4*01 (CH1 (122-219), hinge S10>P (229) (220-231), CH2 (232-341), CH3 (342-446), CHS (447-448)) (122-448)], (135-219')-disulfide with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV2-29*02 (90.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimer (227-227":230-230")-bisdisulfide
concizumab immunoglobuline G4-kappa, anti-[Homo sapiens TFPI (inhibiteur de la voie du facteur tissulaire, inhibiteur de la coagulation associé aux lipoprotéines)], anticorps monoclonal humanisé; chaîne lourde gamma4 (1-448) [VH humanisé (Homo sapiens IGHV3-21*01 (85.70%) -(IGHD)- IGHJ3*01 M11>T (116)) [8.8.14] (1-121) -Homo sapiens IGHG4*01 (CH1 (122-219), charnière S10>P (229) (220-231), CH2 (232-341), CH3 (342-446), CHS (447-448)) (122-448)], (135-219')-disulfure avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV2-29*02 (90.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimère (227-227":230-230")-bisdisulfure
concizumab inmunoglobulina G4-kappa, anti-[Homo sapiens TFPI (inhibidor de la vía del factor tisular, inhibidor de la coagulación asociado a lipoproteínas)], anticuerpo monoclonal humanizado; cadena pesada gamma4 (1-448) [VH humanizado (Homo sapiens IGHV3-21*01 (85.70%) -(IGHD)- IGHJ3*01 M11>T (116)) [8.8.14] (1-121) -Homo sapiens IGHG4*01 (CH1 (122-219), bisagra S10>P (229) (220-231), CH2 (232-341), CH3 (342-446), CHS (447-448)) (122-448)], (135-219')-disulfuro con la cadena ligera kappa (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV2-29*02 (90.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dímero (227-227":230-230")-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVKPGGSLRL SCAASGFTFS NYAMSWVRQT PEKRLEWVAT 50ISRSGSYSYF PDSVQGRFTI SRDNAKNSLY LQMNSLRAED TAVYYCARLG 100GYDEGDAMDS WGQGTTVTVS SASTKGPSVF PLAPCSRSTS ESTAALGCLV 150KDYFPEPVTV SWNSGALTSG VHTFPAVLQS SGLYSLSSVV TVPSSSLGTK 200TYTCNVDHKP SNTKVDKRVE SKYGPPCPPC PAPEFLGGPS VFLFPPKPKD 250TLMISRTPEV TCVVVDVSQE DPEVQFNWYV DGVEVHNAKT KPREEQFNST 300YRVVSVLTVL HQDWLNGKEY KCKVSNKGLP SSIEKTISKA KGQPREPQVY 350TLPPSQEEMT KNQVSLTCLV KGFYPSDIAV EWESNGQPEN NYKTTPPVLD 400SDGSFFLYSR LTVDKSRWQE GNVFSCSVMH EALHNHYTQK SLSLSLGK 448
Light chain / Chaîne légère / Cadena ligeraDIVMTQTPLS LSVTPGQPAS ISCKSSQSLL ESDGKTYLNW YLQKPGQSPQ 50LLIYLVSILD SGVPDRFSGS GSGTDFTLKI SRVEAEDVGV YYCLQATHFP 100QTFGGGTKVE IKRTVAAPSV FIFPPSDEQL KSGTASVVCL LNNFYPREAK 150VQWKVDNALQ SGNSQESVTE QDSKDSTYSL SSTLTLSKAD YEKHKVYACE 200VTHQGLSSPV TKSFNRGEC 219
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 148-204 262-322 368-426 22''-96'' 148''-204'' 262''-322'' 368''-426''Intra-L 23'-93' 139'-199' 23'''-93''' 139'''-199''' Inter-H-L 135-219' 135''-219''' Inter-H-H 227-227'' 230-230''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:298, 298''

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
283
copanlisibum copanlisib 2-amino-N-{7-methoxy-8-[3-(morpholin-4-yl)propoxy]-
2,3-dihydroimidazo[1,2-c]quinazolin-5-yl}pyrimidine-5-carboxamide
copanlisib 2-amino-N-{7-méthoxy-8-[3-(morpholin-4-yl)propoxy]- 2,3-dihydroimidazo[1,2-c]quinazolin-5-yl}pyrimidine-5-carboxamide
copanlisib 2-amino-N-{7-metoxi-8-[3-(morfolin-4-il)propoxi]- 2,3-dihidroimidazo[1,2-c]quinazolin-5-il}pirimidina-5-carboxamida
C23H28N8O4
N
N
N
OCH3
ON NH
O
N
N
ONH2
deferitazolum deferitazole (4S)-2-(2-hydroxy-3-{[(methoxyethoxy)ethoxy]ethoxy}phenyl)-
4-methyl-4,5-dihydro-1,3-thiazol-4-carboxylic acid
déféritazole acide (4S)-2-{2-hydroxy-3-{[(méthoxyéthoxy)éthoxy]éthoxy}phenyl)-4-méthyl-4,5-dihydro-1,3-thiazole-4-carboxylique
deferitazol ácido (4S)-2-(2-hidroxi-4-metil -3-{[(metoxietoxi)etoxi]etoxi}fenil)- 4,5-dihidro-1,3-tiazol-4-carboxílico
C18H25NO7S
OH
OO
OO
H3C
S
N
CH3
CO2H
deleobuvirum deleobuvir (2E)-3-(2-{1-[2-(5-bromopyrimidin-2-yl)-3-cyclopentyl-1-methyl-
1H-indole-6-carboxamido]cyclobutyl}-1-methyl-1H-benzimidazol- 6-yl)prop-2-enoic acid
déléobuvir acide (2E)-3-(2-{1-[2-(5-bromopyrimidin-2-yl)-3-cyclopentyl-1-méthyl-1H-indole-6-carboxamido]cyclobutyl}-1-méthyl-1H-benzimidazol- 6-yl)prop-2-énoïque
deleobuvir ácido (2E)-3-(2-{1-[2-(5-bromopirimidin-2-il)-3-ciclopentil-1-metil- 1H-indol-6-carboxamido]ciclobutil}-1-metil-1H-benzimidazol- 6-il)prop-2-enoico
C34H33BrN6O3
O
HN
N
N
CH3
CO2HN
H3C
N
N
Br

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
284
delparantagum delparantag N2-{5-[(5-{5-{L-lysylamino}-2-methoxybenzoyl-L-lysylamino}-
2-methoxybenzoyl-L-lysyl)amino]-2-methoxybenzoyl}-N-(3-carbamoyl-4-methoxyphenyl)-L-lysinamide
delparantag N2-{5-[(5-{5-{L-lysylamino}-2-méthoxybenzoyl-L-lysylamino}- 2-méthoxybenzoyl-L-lysyl)amino]-2-méthoxybenzoyl}- N-(3-carbamoyl-4-méthoxyphényl)-L-lysinamide
delparantag N2-{5-[(5-{5-{L-lisilamino}-2-metoxibenzoil-L-lisilamino}- 2-metoxibenzoil-L-lisil)amino]-2-metoxibenzoil}-N-(3-carbamoil- 4-metoxfenil)-L-lisinamida
C56H79N13O12
H2NO
HN
OCH3
NH
HH O
NH2
4
dupilumabum # dupilumab immunoglobulin G4-kappa, anti-[Homo sapiens IL4R (interleukin 4
receptor, IL4RA, IL-4RA, CD124)], Homo sapiens monoclonal antibody; gamma4 heavy chain (1-451) [Homo sapiens VH (IGHV3-23*04 (92.90%) -(IGHD)-IGHJ6*01) [8.8.18] (1-125) -IGHG4*01 (CH1 (126-223), hinge S10>P (233) (224-235), CH2 (236-345), CH3 (346-450), CHS K130>del (451)) (126-451)], (139-219')-disulfide with kappa light chain (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (96.00%) -IGKJ2*01) [11.3.9] (1'-112') -IGKC*01 (113'-219')]; dimer (231-231'':234-234'')-bisdisulfide
dupilumab immunoglobuline G4-kappa, anti-[Homo sapiens IL4R (récepteur de l'interleukine 4, IL4RA, IL-4RA, CD124)], Homo sapiens anticorps monoclonal; chaîne lourde gamma4 (1-451) [Homo sapiens VH (IGHV3-23*04 (92.90%) -(IGHD)-IGHJ6*01) [8.8.18] (1-125) -IGHG4*01 (CH1 (126-223), charnière S10>P (233) (224-235), CH2 (236-345), CH3 (346-450), CHS K130>del (451)) (126-451)], (139-219')-disulfure avec la chaîne légère kappa (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (96.00%) -IGKJ2*01) [11.3.9] (1'-112') -IGKC*01 (113'-219')]; dimère (231-231'':234-234'')-bisdisulfure
dupilumab inmunoglobulina G4-kappa, anti-[Homo sapiens IL4R (receptor de la interleukina 4, IL4RA, IL-4RA, CD124)], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma4 (1-451) [Homo sapiens VH (IGHV3-23*04 (92.90%) -(IGHD)-IGHJ6*01) [8.8.18] (1-125) -IGHG4*01 (CH1 (126-223),bisagra S10>P (233) (224-235), CH2 (236-345), CH3 (346-450), CHS K130>del (451)) (126-451)], (139-219')-disulfuro con la cadena ligera kappa (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (96.00%) -IGKJ2*01) [11.3.9] (1'-112') -IGKC*01 (113'-219')]; dímero (231-231'':234-234'')-bisdisulfuro

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
285
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LEQPGGSLRL SCAGSGFTFR DYAMTWVRQA PGKGLEWVSS 50ISGSGGNTYY ADSVKGRFTI SRDNSKNTLY LQMNSLRAED TAVYYCAKDR 100LSITIRPRYY GLDVWGQGTT VTVSSASTKG PSVFPLAPCS RSTSESTAAL 150GCLVKDYFPE PVTVSWNSGA LTSGVHTFPA VLQSSGLYSL SSVVTVPSSS 200LGTKTYTCNV DHKPSNTKVD KRVESKYGPP CPPCPAPEFL GGPSVFLFPP 250KPKDTLMISR TPEVTCVVVD VSQEDPEVQF NWYVDGVEVH NAKTKPREEQ 300FNSTYRVVSV LTVLHQDWLN GKEYKCKVSN KGLPSSIEKT ISKAKGQPRE 350PQVYTLPPSQ EEMTKNQVSL TCLVKGFYPS DIAVEWESNG QPENNYKTTP 400PVLDSDGSFF LYSRLTVDKS RWQEGNVFSC SVMHEALHNH YTQKSLSLSL 450G 451
Light chain / Chaîne légère / Cadena ligeraDIVMTQSPLS LPVTPGEPAS ISCRSSQSLL YSIGYNYLDW YLQKSGQSPQ 50LLIYLGSNRA SGVPDRFSGS GSGTDFTLKI SRVEAEDVGF YYCMQALQTP 100YTFGQGTKLE IKRTVAAPSV FIFPPSDEQL KSGTASVVCL LNNFYPREAK 150VQWKVDNALQ SGNSQESVTE QDSKDSTYSL SSTLTLSKAD YEKHKVYACE 200VTHQGLSSPV TKSFNRGEC 219
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 152-208 266-326 372-430 22''-96'' 152''-208'' 266''-326'' 372''-430''Intra-L 23'-93' 139'-199' 23'''-93''' 139'''-199''' Inter-H-L 139-219' 139''-219''' Inter-H-H 231-231'' 234-234''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:302, 302''
dusigitumabum # dusigitumab immunoglobulin G2-lambda2, anti-[Homo sapiens IGF1 (insulin-like
growth factor 1, somatomedin C) and IGF2 (insulin-like growth factor 2, somatomedin A)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-446) [Homo sapiens VH (IGHV1-8*01 (100.00%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -IGHG2*01 (CH1 (121-218), hinge (219-230), CH2 (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV1-51*01 (95.90%) -IGLJ2*01) [8.3.12] (1'-111') -IGLC2*01 (112'-217')]; dimer (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfide
dusigitumab immunoglobuline G2-lambda2, anti-[Homo sapiens IGF1 (facteur de croissance 1 analogue à l'insuline, somatomédine C) et IGF2 (facteur de croissance 2 analogue à l'insuline, somatomédine A)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-446) [Homo sapiens VH (IGHV1-8*01 (100.00%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -IGHG2*01 (CH1 (121-218), charnière (219-230), CH2 (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV1-51*01 (95.90%) -IGLJ2*01) [8.3.12] (1'-111') -IGLC2*01 (112'-217')]; dimère (222-222'':223-223'':226-226'':229-229'')-tétrakisdisulfure
dusigitumab inmunoglobulina G2-lambda2, anti-[Homo sapiens IGF1 (factor de crecimiento análogo a la insulina tipo 1, somatomedina C) y IGF2 (factor de crecimiento análogo a la insulina tipo 2, somatomedina A)], anticuerpo monoclonal de Homo sapiens ; cadena pesada gamma2 (1-446) [Homo sapiens VH (IGHV1-8*01 (100.00%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -IGHG2*01 (CH1 (121-218), bisagra (219-230), CH2 (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV1-51*01 (95.90%) -IGLJ2*01) [8.3.12] (1'-111') -IGLC2*01 (112'-217')]; dímero (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfuro

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
286
Heavy chain / Chaîne lourde / Cadena pesada
QVQLVQSGAE VKKPGASVKV SCKASGYTFT SYDINWVRQA TGQGLEWMGW 50MNPNSGNTGY AQKFQGRVTM TRNTSISTAY MELSSLRSED TAVYYCARDP 100YYYYYGMDVW GQGTTVTVSS ASTKGPSVFP LAPCSRSTSE STAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSNFGTQT 200YTCNVDHKPS NTKVDKTVER KCCVECPPCP APPVAGPSVF LFPPKPKDTL 250MISRTPEVTC VVVDVSHEDP EVQFNWYVDG VEVHNAKTKP REEQFNSTFR 300VVSVLTVVHQ DWLNGKEYKC KVSNKGLPAP IEKTISKTKG QPREPQVYTL 350PPSREEMTKN QVSLTCLVKG FYPSDIAVEW ESNGQPENNY KTTPPMLDSD 400GSFFLYSKLT VDKSRWQQGN VFSCSVMHEA LHNHYTQKSL SLSPGK 446
Light chain / Chaîne légère / Cadena ligeraQSVLTQPPSV SAAPGQKVTI SCSGSSSNIE NNHVSWYQQL PGTAPKLLIY 50DNNKRPSGIP DRFSGSKSGT SATLGITGLQ TGDEADYYCE TWDTSLSAGR 100VFGGGTKLTV LGQPKAAPSV TLFPPSSEEL QANKATLVCL ISDFYPGAVT 150VAWKADSSPV KAGVETTTPS KQSNNKYAAS SYLSLTPEQW KSHRSYSCQV 200THEGSTVEKT VAPTECS 217
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 147-203 260-320 366-424 22''-96'' 147''-203'' 260''-320'' 366''-424''Intra-L 22'-89' 139'-198' 22'''-89''' 139'''-198''' Inter-H-L 134-216' 134''-216''' Inter-H-H 222-222'' 223-223'' 226-226'' 229-229''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH VH N81:73, 73'' H CH2 N84.4:296, 296''
elosulfasum alfa # elosulfase alfa human N-acetylgalactosamine-6-sulfatase (chondroitinsulfatase,
galactose-6-sulfate sulfatase, EC=3.1.6.4) dimer (139-139')-disulfide glycosylated (produced by CHO cells)
élosulfase alfa N-acétylgalactosamine-6-sulfatase humaine (chondroïtinesulfatase, 6-sulfate de galactose sulfatase, EC=3.1.6.4) (139-139')-disulfure du dimère glycosylée (produite par des cellules CHO)
elosulfasa alfa N-acetilgalactosamina-6-sulfatasa humana (condroitinsulfatasa, 6-sulfato de galactosa sulfatasa, EC=3.1.6.4) (139-139')-disulfuro del dímero glicosilado (producido por células CHO)
C5020H7574N1364O1418S34
OCO2H
NH2H
Monomer / Monomère / MonómeroAPQPPNILLL LMDDMGWGDL GVYGEPSRET PNLDRMAAEG LLFPNFYSAN 50PLCSPSRAAL LTGRLPIRNG FYTTNAHARN AYTPQEIVGG IPDSEQLLPE 100LLKKAGYVSK IVGKWHLGHR PQFHPLKHGF DEWFGSPNCH FGPYDNKARP 150NIPVYRDWEM VGRYYEEFPI NLKTGEANLT QIYLQEALDF IKRQARHHPF 200FLYWAVDATH APVYASKPFL GTSQRGRYGD AVREIDDSIG KILELLQDLH 250VADNTFVFFT SDNGAALISA PEQGGSNGPF LCGKQTTFEG GMREPALAWW 300PGHVTAGQVS HQLGSIMDLF TTSLALAGLT PPSDRAIDGL NLLPTLLQGR 350LMDRPIFYYR GDTLMAATLG QHKAHFWTWT NSWENFRQGI DFCPGQNVSG 400VTTHNLEDHT KLPLIFHLGR DPGERFPLSF ASAEYQEALS RITSVVQQHQ 450EALVPAQPQL NVCNWAVMNW APPGCEKLGK CLTPPESIPK KCLWSH 496
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro139-139' 282-393 282'-393' 463-492 463'-492' 475-481 475'-481'
Modified residues / Résidus modifiés / Restos modificados
C53 , 53'
3-oxoAla
Glycosylation sites (N) / Sites de glycosylation (N) / Posiciones de glicosilación (N)Asn-178 Asn-178' Asn-397 Asn-397'
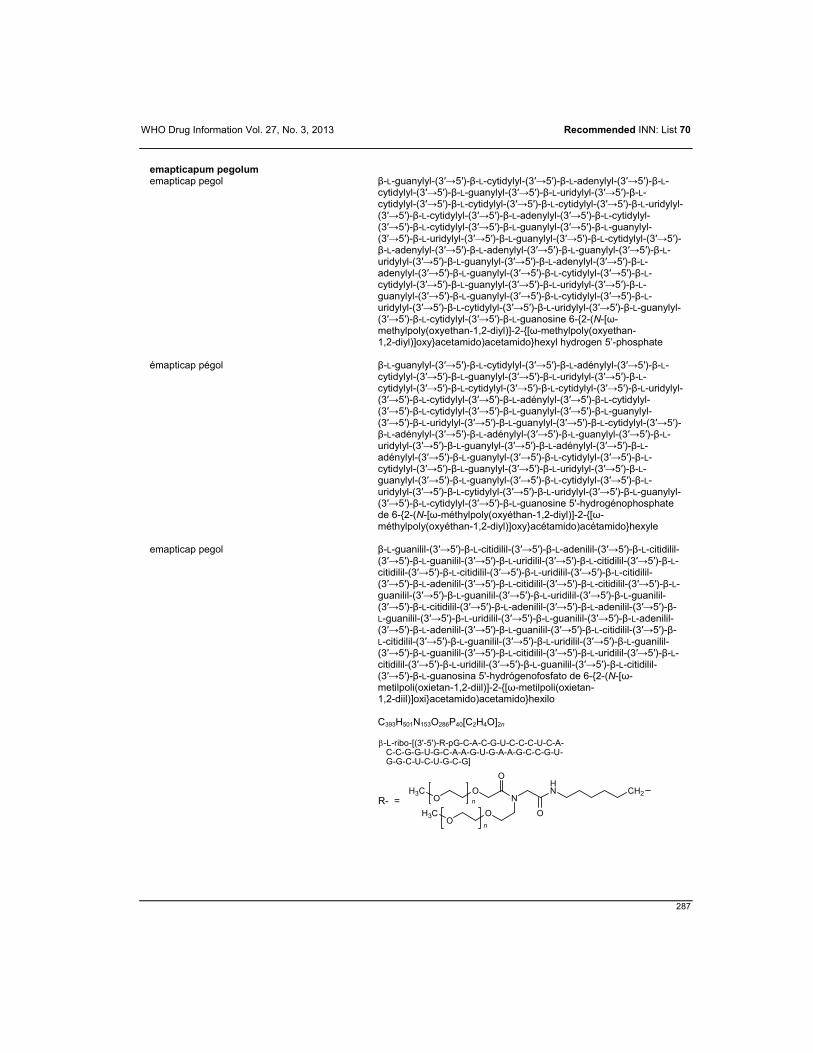
WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
287
emapticapum pegolum emapticap pegol β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-
cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanosine 6-{2-(N-[ω-methylpoly(oxyethan-1,2-diyl)]-2-{[ω-methylpoly(oxyethan- 1,2-diyl)]oxy}acetamido)acetamido}hexyl hydrogen 5’-phosphate
émapticap pégol β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanosine 5'-hydrogénophosphate de 6-{2-(N-[ω-méthylpoly(oxyéthan-1,2-diyl)]-2-{[ω-méthylpoly(oxyéthan-1,2-diyl)]oxy}acétamido)acétamido}hexyle
emapticap pegol β-L-guanilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-guanosina 5'-hydrógenofosfato de 6-{2-(N-[ω-metilpoli(oxietan-1,2-diil)]-2-{[ω-metilpoli(oxietan- 1,2-diil)]oxi}acetamido)acetamido}hexilo
C393H501N153O286P40[C2H4O]2n
R- =
HN
O
NCH2
O
O
O
OH3C
OH3C
n
n
-L-ribo-[(3'-5')-R-pG-C-A-C-G-U-C-C-C-U-C-A- C-C-G-G-U-G-C-A-A-G-U-G-A-A-G-C-C-G-U- G-G-C-U-C-U-G-C-G]
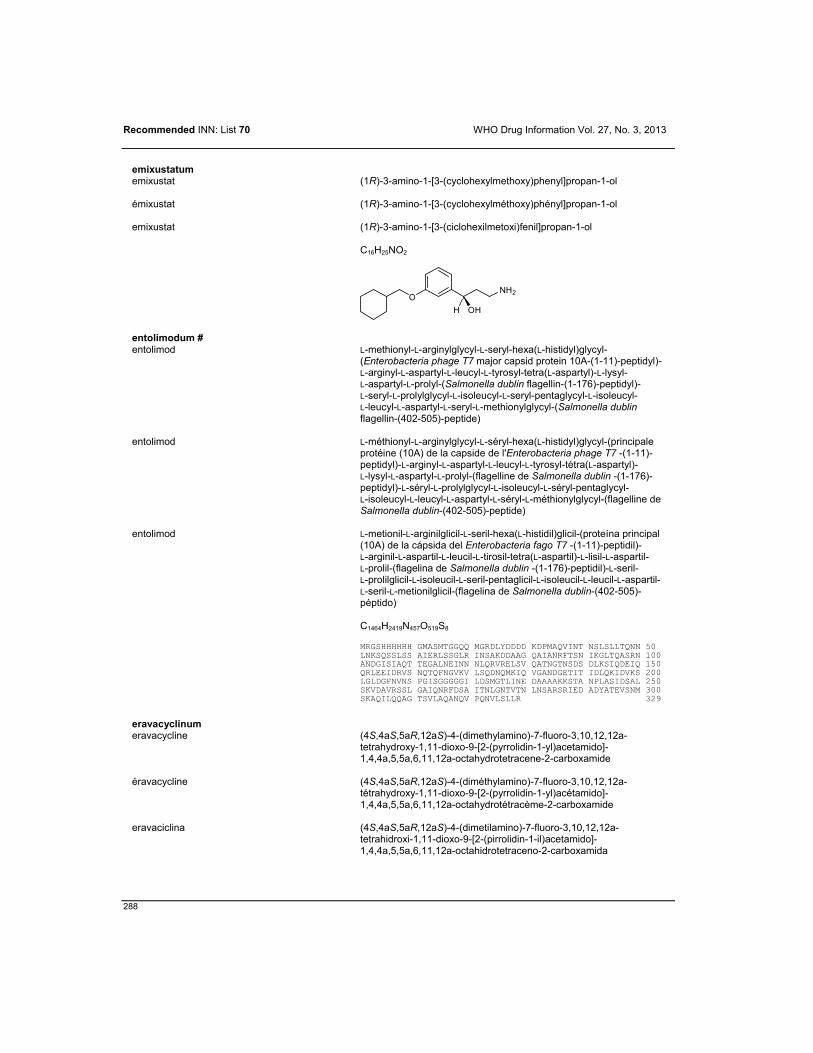
Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
288
emixustatum emixustat (1R)-3-amino-1-[3-(cyclohexylmethoxy)phenyl]propan-1-ol
émixustat (1R)-3-amino-1-[3-(cyclohexylméthoxy)phényl]propan-1-ol
emixustat (1R)-3-amino-1-[3-(ciclohexilmetoxi)fenil]propan-1-ol
C16H25NO2
ONH2
H OH
entolimodum # entolimod L-methionyl-L-arginylglycyl-L-seryl-hexa(L-histidyl)glycyl-
(Enterobacteria phage T7 major capsid protein 10A-(1-11)-peptidyl)-L-arginyl-L-aspartyl-L-leucyl-L-tyrosyl-tetra(L-aspartyl)-L-lysyl- L-aspartyl-L-prolyl-(Salmonella dublin flagellin-(1-176)-peptidyl)- L-seryl-L-prolylglycyl-L-isoleucyl-L-seryl-pentaglycyl-L-isoleucyl- L-leucyl-L-aspartyl-L-seryl-L-methionylglycyl-(Salmonella dublin flagellin-(402-505)-peptide)
entolimod L-méthionyl-L-arginylglycyl-L-séryl-hexa(L-histidyl)glycyl-(principale protéine (10A) de la capside de l'Enterobacteria phage T7 -(1-11)-peptidyl)-L-arginyl-L-aspartyl-L-leucyl-L-tyrosyl-tétra(L-aspartyl)- L-lysyl-L-aspartyl-L-prolyl-(flagelline de Salmonella dublin -(1-176)-peptidyl)-L-séryl-L-prolylglycyl-L-isoleucyl-L-séryl-pentaglycyl- L-isoleucyl-L-leucyl-L-aspartyl-L-séryl-L-méthionylglycyl-(flagelline de Salmonella dublin-(402-505)-peptide)
entolimod L-metionil-L-arginilglicil-L-seril-hexa(L-histidil)glicil-(proteína principal (10A) de la cápsida del Enterobacteria fago T7 -(1-11)-peptidil)- L-arginil-L-aspartil-L-leucil-L-tirosil-tetra(L-aspartil)-L-lisil-L-aspartil- L-prolil-(flagelina de Salmonella dublin -(1-176)-peptidil)-L-seril- L-prolilglicil-L-isoleucil-L-seril-pentaglicil-L-isoleucil-L-leucil-L-aspartil-L-seril-L-metionilglicil-(flagelina de Salmonella dublin-(402-505)-péptido)
C1464H2419N457O519S8
MRGSHHHHHH GMASMTGGQQ MGRDLYDDDD KDPMAQVINT NSLSLLTQNN 50
LNKSQSSLSS AIERLSSGLR INSAKDDAAG QAIANRFTSN IKGLTQASRN 100ANDGISIAQT TEGALNEINN NLQRVRELSV QATNGTNSDS DLKSIQDEIQ 150QRLEEIDRVS NQTQFNGVKV LSQDNQMKIQ VGANDGETIT IDLQKIDVKS 200LGLDGFNVNS PGISGGGGGI LDSMGTLINE DAAAAKKSTA NPLASIDSAL 250SKVDAVRSSL GAIQNRFDSA ITNLGNTVTN LNSARSRIED ADYATEVSNM 300SKAQILQQAG TSVLAQANQV PQNVLSLLR 329
eravacyclinum eravacycline (4S,4aS,5aR,12aS)-4-(dimethylamino)-7-fluoro-3,10,12,12a-
tetrahydroxy-1,11-dioxo-9-[2-(pyrrolidin-1-yl)acetamido]-1,4,4a,5,5a,6,11,12a-octahydrotetracene-2-carboxamide
éravacycline (4S,4aS,5aR,12aS)-4-(diméthylamino)-7-fluoro-3,10,12,12a-tétrahydroxy-1,11-dioxo-9-[2-(pyrrolidin-1-yl)acétamido]-1,4,4a,5,5a,6,11,12a-octahydrotétracème-2-carboxamide
eravaciclina (4S,4aS,5aR,12aS)-4-(dimetilamino)-7-fluoro-3,10,12,12a-tetrahidroxi-1,11-dioxo-9-[2-(pirrolidin-1-il)acetamido]-1,4,4a,5,5a,6,11,12a-octahidrotetraceno-2-carboxamida

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
289
C27H31FN4O8
OOH OH
NH2
H N
H3C
CH3
OOH
HH
O
OH
F
HN
N
O
evodenosonum evodenoson methyl 4-{3-[6-amino-9-(N-cyclopropyl-β-D-ribofuranosyluronamide)-
9H-purin-2-yl]prop-2-yn-1-yl}piperidine-1-carboxylate
évodénoson 4-{3-[6-amino-9-(N-cyclopropyl-β-D-ribofuranosyluronamide)- 9H-purin-2-yl]prop-2-yn-1-yl}pipéridine-1-carboxylate de méthyle
evodenosón 4-{3-[6-amino-9-(N-ciclopropil-β-D-ribofuranosiluronamida)-9H-purin-2-il]prop-2-in-1-il}piperidina-1-carboxilato de metilo
C23H29N7O6
N
N
NH2
N
N
NO
O
H3C
O
ONH
OH
OH
evolocumabum # evolocumab immunoglobulin G2-lambda, anti-[Homo sapiens PCSK9 (proprotein
convertase subtilisin/kexin type 9)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-441) [Homo sapiens VH (IGHV1-18*01 (93.90%) -(IGHD)-IGHJ6*01)) [8.8.8] (1-115) -IGHG2*01 (CH1 (116-213), hinge (214-225), CH2 (226-334), CH3 (335-439), CHS (440-441)) (116-441)], (129-214')-disulfide with lambda light chain (1'-215') [Homo sapiens V-LAMBDA (IGLV2-14*01 (95.90%) -IGLJ2*01) [9.3.9] (1'-109') -IGLC2*01 (110'-215')]; dimer (217-217'':218-218'':221-221'':224-224'')-tetrakisdisulfide
évolocumab immunoglobuline G2-lambda, anti-[Homo sapiens PCSK9 (proprotéine convertase subtilisine/kexine type 9)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-441) [Homo sapiens VH (IGHV1-18*01 (93.90%) -(IGHD)-IGHJ6*01) [8.8.8] (1-115) - IGHG2*01 (CH1 (116-213), charnière (214-225), CH2 (226-334), CH3 (335-439), CHS (440-441)) (116-441)], (129-214')-disulfure avec la chaîne légère lambda (1'-215') [Homo sapiens V-LAMBDA (IGLV2-14*01 (95.90%) -IGLJ2*01) [9.3.9] (1'-109') -IGLC2*01 (110'-215')]; dimère (217-217'':218-218'':221-221'':224-224'')-tétrakisdisulfure

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
290
evolocumab inmunoglobulina G2-lambda, anti-[Homo sapiens PCSK9 (proproteína convertasa subtilisina/kexina tipo 9)], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma2 (1-441) [Homo sapiens VH (IGHV1-18*01 (93.90%) -(IGHD)-IGHJ6*01) [8.8.8] (1-115) - IGHG2*01 (CH1 (116-213), bisagra(214-225), CH2 (226-334), CH3 (335-439), CHS (440-441)) (116-441)], (129-214')-disulfuro con la cadena ligera lambda (1'-215') [Homo sapiens V-LAMBDA (IGLV2-14*01 (95.90%) -IGLJ2*01) [9.3.9] (1'-109') -IGLC2*01 (110'-215')]; dímero (217-217'':218-218'':221-221'':224-224'')-tetrakisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVQSGAE VKKPGASVKV SCKASGYTLT SYGISWVRQA PGQGLEWMGW 50VSFYNGNTNY AQKLQGRGTM TTDPSTSTAY MELRSLRSDD TAVYYCARGY 100GMDVWGQGTT VTVSSASTKG PSVFPLAPCS RSTSESTAAL GCLVKDYFPE 150PVTVSWNSGA LTSGVHTFPA VLQSSGLYSL SSVVTVPSSN FGTQTYTCNV 200DHKPSNTKVD KTVERKCCVE CPPCPAPPVA GPSVFLFPPK PKDTLMISRT 250PEVTCVVVDV SHEDPEVQFN WYVDGVEVHN AKTKPREEQF NSTFRVVSVL 300TVVHQDWLNG KEYKCKVSNK GLPAPIEKTI SKTKGQPREP QVYTLPPSRE 350EMTKNQVSLT CLVKGFYPSD IAVEWESNGQ PENNYKTTPP MLDSDGSFFL 400YSKLTVDKSR WQQGNVFSCS VMHEALHNHY TQKSLSLSPG K 441
Light chain / Chaîne légère / Cadena ligeraESALTQPASV SGSPGQSITI SCTGTSSDVG GYNSVSWYQQ HPGKAPKLMI 50YEVSNRPSGV SNRFSGSKSG NTASLTISGL QAEDEADYYC NSYTSTSMVF 100GGGTKLTVLG QPKAAPSVTL FPPSSEELQA NKATLVCLIS DFYPGAVTVA 150WKADSSPVKA GVETTTPSKQ SNNKYAASSY LSLTPEQWKS HRSYSCQVTH 200EGSTVEKTVA PTECS 215
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 142-198 255-315 361-419 22''-96'' 142''-198'' 255''-315'' 361''-419''Intra-L 22'-90' 137'-196' 22'''-90''' 137'''-196''' Inter-H-L 129-214' 129''-214''' Inter-H-H 217-217'' 218-218'' 221-221'' 224-224''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:291, 291''
fedratinibum fedratinib N-tert-butyl-3-[(5-methyl-2-{4-[2-(pyrrolidin-
1-yl)ethoxy]anilino}pyrimidin-4-yl)amino]benzenesulfonamide
fédratinib N-tert-butyl-3-[(5-méthyl-2-{4-[2-(pyrrolidin- 1-yl)éthoxy]anilino}pyrimidin-4-yl)amino]benzènesulfonamide
fedratinib N-terc-butil-3-[(5-metil-2-{4-[2-(pirrolidin-1-il)etoxi]anilino}pirimidin- 4-il)amino]bencenosulfonamida
C27H36N6O3S
SNH
HN
O O
NN
NH
ON
CH3 CH3
CH3
CH3

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
291
filgotinibum filgotinib N-(5-{4-[(1,1-oxo-λ6-thiomorpholin-
4-yl)methyl]phenyl}[1,2,4]triazolo[1,5-a]pyridin- 2-yl)cyclopropanecarboxamide
filgotinib N-(5-{4-[(1,1-oxo-λ6-thiomorpholin- 4-yl)méthyl]phényl}[1,2,4]triazolo[1,5-a]pyridin- 2-yl)cyclopropanecarboxamide
filgotinib N-(5-{4-[(1,1-oxo-λ6-tiomorfolin-4-il)metil]fenil}[1,2,4]triazolo[1,5-a]piridin-2-il)ciclopropanocarboxamida
C21H23N5O3S
N
S N
N
N
HN
O
O
O
filorexantum filorexant [(2R,5R)-5-{[(5-fluoropyridin-2-yl)oxy]methyl}-2-methylpiperidin-
1-yl][5-methyl-2-(pyrimidin-2-yl)phenyl]methanone
filorexant [(2R,5R)-5-{[(5-fluoropyridin-2-yl)oxy]méthyl}-2-méthylpipéridin- 1-yl][5-méthyl-2-(pyrimidin-2-yl)phényl]méthanone
filorexant [(2R,5R)-5-{[(5-fluoropiridin-2-il)oxi]metil}-2-metilpiperidin-1-il][5-metil-2-(pirimidin-2-il)fenil]metanona
C24H25FN4O2
N
O
O
N
CH3
H
CH3
NNF
H
finerenonum finerenone (4S)-4-(4-cyano-2-methoxyphenyl)-5-ethoxy-2,8-dimethyl-
1,4-dihydro-1,6-naphthyridine-3-carboxamide
finérénone (4S)-4-(4-cyano-2-méthoxyphényl)-5-éthoxy-2,8-diméthyl- 1,4-dihydro-1,6-naphtyridine-3-carboxamide
finerenona (4S)-4-(4-ciano-2-metoxifenil)-5-etoxi-2,8-dimetil-1,4-dihidro- 1,6-naftiridina-3-carboxamida
C21H22N4O3
HN
N
CH3
O
NH2
OH3COCH3
CN
H
CH3

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
292
firtecanum peglumerum firtecan peglumer α-{3-[(α-N-acetylpoly-L-glutamyl)amino]propyl}-
ω-methoxypoly(oxyethan-1,2-diyl) where the free γ-carboxyl groups are partially esterified by (4S)-4,11-diethyl-4-hydroxy-3,14-dioxo-3,4,12,14-tetrahydro-1H-pyrano[3',4':6,7]indolizino[1,2-b]quinolin- 9-yl, partially converted to an amide with (propan-2-yl)[(propan- 2-yl)carbamoyl]amino and partially unchanged
firtécan péglumère α-{3-[(α-N-acétylpoly-L-glutamyl)amino]propyl}- ω-méthoxypoly(oxyéthylène) dont certains acides γ-carboxyliques sont estérifiés par le (4S)-4,11-diéthyl-4-hydroxy-3,14-dioxo-3,4,12,14-tétrahydro-1H-pyrano[3',4':6,7]indolizino[1,2-b]quinoléin- 9-yle et d'autres amidifiés par le (propan-2-yl)[(1-propan- 2-yl)carbamoyl]amino
firtecán peglúmero α-{3-[(α-N-acetilpoli-L-glutamil)amino]propil}-ω-metoxipoli(oxietileno) cuyos algunos ácidos γ-carboxílicos estan esterificados por el (4S)-4,11-dietil-4-hidroxi-3,14-dioxo-3,4,12,14-tetrahidro- 1H-pirano[3',4':6,7]indolizino[1,2-b]quinolein-9-ilo y otros amidificados por el (propan-2-il)[(propan-2-il)carbamoil]amino
C6H13NO2 [C5H6NO2]a [C2H4O]n (C22H19N2O5)x (C7H15N2O)y (HO)z a = x + y + z
ON
N
O
O
O
CH3
HO CH3
=
orouo
N
CH3
H3C
O
NH
R
orouo
OH
H3C
CH3
H3CNH
O
HN
HO
R
O
a
n
OO
CH3
flortanidazolum (18F) flortanidazole (18F) (2RS)-3-[18F]fluoro-2-{4-[(2-nitro-1H-imidazol-1-yl)methyl]-
1H-1,2,3-triazol-1-yl}propan-1-ol
flortanidazole (18F) (2RS)-3-[18F]fluoro-2-{4-[(2-nitro-1H-imidazol-1-yl)méthyl]- 1H-1,2,3-triazol-1-yl}propan-1-ol
flortanidazol (18F) (2RS)-3-[18F]fluoro-2-{4-[(2-nitro-1H-imidazol-1-il)metil]- 1H-1,2,3-triazol-1-il}propan-1-ol

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
293
C9H1118FN6O3
NN
O2N
NN
N
H[18F]
OHand enantiomeret énantiomèrey enantiómero
flotegatidum (18F) flotegatide (18F) cyclo{L-arginylglycyl-L-α-aspartyl-D-phenylalanyl-N6-[2,6-anhydro-
7-deoxy-7-({2-[4-(3-[18F]fluoropropyl)-1H-1,2,3-triazol- 1-yl]acetyl}amino)-L-glycero-L-galacto-heptonoyl]-L-lysyl}
flotégatide (18F) cyclo{L-arginylglycyl-L-α-aspartyl-D-phénylalanyl-N6-[2,6-anhydro- 7-déoxy-7-({2-[4-(3-[18F]fluoropropyl)-1H-1,2,3-triazol- 1-yl]acétyl}amino)-L-glycéro-L-galacto-heptonoyl]-L-lysyl}
flotegatida (18F) ciclo{L-arginilglicil-L-α-aspartil-D-fenilalanil-N6-[2,6-anhidro- 7-desoxi-7-({2-[4-(3-[18F]fluoropropil)-1H-1,2,3-triazol- 1-il]acetil}amino)-L-glicero-L-galacto-heptonoil]-L-lisil}
C41H6018FN13O13
HN
NH
HN
HN
HN
O
NH
O
H2N
NH
O
CO2H
O
O
H
H
H
H
NH
OO
H
OHHO
HO
NH
N
O
N
N
[18F]
fluorfenidinum (18F) fluorfenidine (18F) 3-{2-chloro-5-[(2-[18F]fluoroethyl)sulfanyl]phenyl}-1-methyl-
1-[3-(methylsulfanyl)phenyl]guanidine
fluorfénidine (18F) 3-{2-chloro-5-[(2-[18F]fluoroéthyl)sulfanyl]phényl}-1-méthyl- 1-[3-(méthylsulfanyl)phényl]guanidine
fluorfenidina (18F) 3-{2-cloro-5-[(2-[18F]fluoroetil)sulfanil]fenil}-1-metil- 1-[3-(metilsulfanil)fenil]guanidine
C17H19Cl18FN3S2
HN N
CH3
NH
SCH3
Cl
S[18F]
flutriciclamidum (18F) flutriciclamide (18F) (4S)-N,N-diethyl-9-(2-[18F]fluoroethyl)-5-methoxy-2,3,4,9-tetrahydro-
1H-carbazole-4-carboxamide
flutriciclamide (18F) (4S)-N,N-diéthyl-9-(2-[18F]fluoroéthyl)-5-méthoxy-2,3,4,9-tétrahydro-1H-carbazole-4-carboxamide

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
294
flutriciclamida (18F) (4S)-N,N-dietil-9-(2-[18F]fluoroetil)-5-metoxi-2,3,4,9-tetrahidro- 1H-carbazol-4-carboxamida
C20H2718FN2O2
N[18F]
N CH3
CH3
OO
CH3
H
gandotinibum gandotinib 3-[(4-chloro-2-fluorophenyl)methyl]-2-methyl-N-(5-methyl-
1H-pyrazol-3-yl)-8-[(morpholin-4-yl)methyl]imidazo[1,2-b]pyridazin- 6-amine
gandotinib 3-[(4-chloro-2-fluorophényl)méthyl]-2-méthyl-N-(5-méthyl- 1H-pyrazol-3-yl)-8-[(morpholin-4-yl)méthyl]imidazo[1,2-b]pyridazin- 6-amine
gandotinib 3-[(4-cloro-2-fluorofenil)metil]-2-metil-N-(5-metil-1H-pirazol-3-il)- 8-[(morfolin-4-il)metil]imidazo[1,2-b]piridazin-6-amina
C23H25ClFN7O
N
N
N
CH3
N
NH
O
NHN
H3C
F
Cl
hemoglobinum crosfumarilum (bovinum) # hemoglobin crosfumaril (bovine) S3.β92,S3.β'92-bis(2-amino-2-oxoethyl)-N6.α99,N6.α'99-(but-
2-enedioyl)bovine hemoglobulin (α2β2 tetramer)
hémoglobine crosfumaril (bovine) S3.β92,S3.β'92-bis(2-amino-2-oxoéthyl)-N6.α99,N6.α'99-(but- 2-ènedioyl)hémoglobuline bovine (α2β2 tétramère)
hemoglobina crosfumarilo (bovina) S3.β92,S3.β'92-bis(2-amino-2-oxoetil)-N6.α99,N6.α'99-(but- 2-enodioil)hemoglobulina bovina (α2β2 tetrámero)
C2826H4406N762O802S10
H2N CO2H
H
CO2HH2N
HNH
O
HN
O
H2N CO2H
H S
O
NH2
Alpha chain / Chaîne alpha / Cadena alfaVLSAADKGNV KAAWGKVGGH AAEYGAEALE RMFLSFPTTK TYFPHFDLSH 50GSAQVKGHGA KVAAALTKAV EHLDDLPGAL SELSDLHAHK LRVDPVNFKL 100LSHSLLVTLA SHLPSDFTPA VHASLDKFLA NVSTVLTSKY R 141
Beta chain / Chaîne bêta / Cadena betaMLTAEEKAAV TAFWGKVKVD EVGGEALGRL LVVYPWTQRF FESFGDLSTA 50DAVMNNPKVK AHGKKVLDSF SNGMKHLDDL KGTFAALSEL HCDKLHVDPE 100NFKLLGNVLV VVLARNFGKE FTPVLQADFQ KVVAGVANAL AHRYH 145
Modified residues / Résidus modifiés / Restos modificadosK
99-Lys-crosfumaril-'99-LysC
92 , '92

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
295
ilorasertibum ilorasertib N-(4-{4-amino-7-[1-(2-hydroxyethyl)-1H-pyrazol-4-yl]thieno[3,2-
c]pyridin-3-yl}phenyl)-N'-(3-fluorophenyl)urea
ilorasertib N-(4-{4-amino-7-[1-(2-hydroxyéthyl)-1H-pyrazol-4-yl]thiéno[3,2-c]pyridin-3-yl}phényl)-N'-(3-fluorophényl)urée
ilorasertib N-(4-{4-amino-7-[1-(2-hidroxietil)-1H-pirazol-4-il]tieno[3,2-c]piridin- 3-il}fenil)-N'-(3-fluorofenil)urea
C25H21FN6O2S
NH
NH
O
S
NNH2
NN
HOF
ipatasertibum ipatasertib (2S)-2-(4-chlorophenyl)-1-{4-[(5R,7R)-7-hydroxy-5-methyl-
6,7-dihydro-5H-cyclopenta[d]pyrimidin-4-yl]piperazin-1-yl}- 3-[(propan-2-yl)amino]propan-1-one
ipatasertib (2S)-2-(4-chlorophényl)-1-{4-[(5R,7R)-7-hydroxy-5-méthyl- 6,7-dihydro-5H-cyclopenta[d]pyrimidin-4-yl]pipérazin-1-yl}- 3-[(propan-2-yl)amino]propan-1-one
ipatasertib (2S)-2-(4-clorofenil)-1-{4-[(5R,7R)-7-hidroxi-5-metil-6,7-dihidro- 5H-ciclopenta[d]pirimidin-4-il]piperazin-1-il}-3-[(propan- 2-il)amino]propan-1-ona
C24H32ClN5O2
H3C NH
N
O
N
N N
CH3
H
Cl
H3CH
OH
H
lexaptepidum pegolum lexaptepid pegol β-L-guanylyl-(3'→5')-β-L-cytidylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-
cytidylyl-(3'→5')-β-L-cytidylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-adenylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-cytidylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-cytidine 6-{2-(N-[ω-methylpoly(oxyethan-1,2-diyl)]-2-{[ω-methylpoly(oxyethan-1,2-diyl)]oxy}acetamido)acetamido}hexyl hydrogen 5'-phosphate

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
296
lexaptépid pégol β-L-guanylyl-(3'→5')-β-L-cytidylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-
cytidylyl-(3'→5')-β-L-cytidylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-uridylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-adénylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-cytidylyl-(3'→5')-β-L-guanylyl-(3'→5')-β-L-cytidine 5'-hydrogenophosphate de 6-{2-(N-[ω-méthylpoly(oxyéthan- 1,2-diyl)]-2-{[ω-méthylpoly(oxyéthan- 1,2-diyl)]oxy}acétamido)acétamido}hexyle
lexaptepid pegol β-L-guanilil-(3'→5')-β-L-citidilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-citidilil-(3'→5')-β-L-citidilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-uridilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-adenilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-citidilil-(3'→5')-β-L-guanilil-(3'→5')-β-L-citidina 5'-hidrógenofosfato de 6-{2-(N-[ω-metilpoli(oxietan-1,2-diil)]-2-{[ω-metilpoli(oxietan- 1,2-diil)]oxi}acetamido)acetamido}hexilo
C441H548N188O309P44[C2H4O]2n
R- =
HN
O
NCH2
O
O
O
OH3C
OH3C
n
n
-L-ribo-[(3'-5')-R-pG-C-G-C-C-G-U-A-U-G-G-G- A-U-U-A-A-G-U-A-A-A-U-G-A-G-G-A-G-U-U-G- G-A-G-G-A-A-G-G-G-C-G-C]
lodelcizumabum # lodelcizumab immunoglobulin G1-kappa, anti-[Homo sapiens PCSK9 (proprotein
convertase subtilisin/kexin type 9)], humanized monoclonal antibody; gamma1 heavy chain (1-448) [humanized VH (Homo sapiens IGHV1-2*05 (88.80%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03 (CH1 (119-216), hinge (217-231), CH2 L1.3>A (235), L1.2>A (236) (232-341), CH3 (342-446), CHS (447-448) (119-448)], (221-213')-disulfide with kappa light chain (1'-213') [humanized V-KAPPA (Homo sapiens IGKV3-20*02 (87.60%) -IGKJ2*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01 (107'-213')]; dimer (227-227":230-230")-bisdisulfide

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
297
lodelcizumab immunoglobuline G1-kappa, anti-[Homo sapiens PCSK9 (proprotéine convertase subtilisine/kexine type 9)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-448) [VH humanisé (Homo sapiens IGHV1-2*05 (88.80%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) - Homo sapiens IGHG1*03 (CH1 (119-216), charnière (217-231), CH2 L1.3>A (235), L1.2>A (236) (232-341), CH3 (342-446), CHS (447-448) (119-448)], (221-213')-disulfure avec la chaîne légère kappa (1'-213') [V-KAPPA humanisé (Homo sapiens IGKV3-20*02 (87.60%) -IGKJ2*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01 (107'-213')]; dimère (227-227":230-230")-bisdisulfure
lodelcizumab inmunoglobulina G1-kappa, anti-[Homo sapiens PCSK9 (proproteína convertasa subtilisina/kexina tipo 9)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-448) [VH humanizado (Homo sapiens IGHV1-2*05 (88.80%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) - Homo sapiens IGHG1*03 (CH1 (119-216), bisagra (217-231), CH2 L1.3>A (235), L1.2>A (236) (232-341), CH3 (342-446), CHS (447-448) (119-448)], (221-213')-disulfuro con la cadena ligera kappa (1'-213') [V-KAPPA humanizada (Homo sapiens IGKV3-20*02 (87.60%) -IGKJ2*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01 (107'-213')]; dímero (227-227":230-230")-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QVQLVQSGAE VKKPGASVKV SCKASGYTFS TMYMSWVRQA PGQGLEWMGR 50IDPANEHTNY AQKFQGRVTM TRDTSISTAY MELSRLTSDD TAVYYCARSY 100YYYNMDYWGQ GTLVTVSSAS TKGPSVFPLA PSSKSTSGGT AALGCLVKDY 150FPEPVTVSWN SGALTSGVHT FPAVLQSSGL YSLSSVVTVP SSSLGTQTYI 200CNVNHKPSNT KVDKRVEPKS CDKTHTCPPC PAPEAAGGPS VFLFPPKPKD 250TLMISRTPEV TCVVVDVSHE DPEVKFNWYV DGVEVHNAKT KPREEQYNST 300YRVVSVLTVL HQDWLNGKEY KCKVSNKALP APIEKTISKA KGQPREPQVY 350TLPPSREEMT KNQVSLTCLV KGFYPSDIAV EWESNGQPEN NYKTTPPVLD 400SDGSFFLYSK LTVDKSRWQQ GNVFSCSVMH EALHNHYTQK SLSLSPGK 448
Light chain / Chaîne légère / Cadena ligeraQIVLTQSPAT LSVSPGERAT LSCRASQSVS YMHWYQQKPG QAPRLLIYGV 50FRRATGIPDR FSGSGSGTDF TLTIGRLEPE DFAVYYCLQW SSDPPTFGQG 100TKLEIKRTVA APSVFIFPPS DEQLKSGTAS VVCLLNNFYP REAKVQWKVD 150NALQSGNSQE SVTEQDSKDS TYSLSSTLTL SKADYEKHKV YACEVTHQGL 200SSPVTKSFNR GEC 213
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 145-201 262-322 368-426 22''-96'' 145''-201'' 262''-322'' 368''-426''Intra-L 23'-87' 133'-193' 23'''-87''' 133'''-193''' Inter-H-L 221-213' 221''-213''' Inter-H-H 227-227'' 230-230''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:298, 298''
luminespibum luminespib 5-[2,4-dihydroxy-5-(propan-2-yl)phenyl]-N-ethyl-4-{4-[(morpholin-
4-yl)methyl]phenyl}-1,2-oxazole-3-carboxamide
luminespib 5-[2,4-dihydroxy-5-(propan-2-yl)phényl]-N-éthyl-4-{4-[(morpholin- 4-yl)méthyl]phényl}-1,2-oxazole-3-carboxamide
luminespib 5-[2,4-dihidroxi-5-(propan-2-il)fenil]-N-etil-4-{4-[(morfolin- 4-il)metil]fenil}-1,2-oxazol-3-carboxamida

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
298
C26H31N3O5
OHHO
H3C
CH3
ON
NO
NHO
CH3
molidustatum molidustat 2-[6-(morpholin-4-yl)pyrimidin-4-yl]-4-(1H-1,2,3-triazol-1-yl)-
1,2-dihydro-3H-pyrazol-3-one
molidustat 2-[6-(morpholin-4-yl)pyrimidin-4-yl]-4-(1H-1,2,3-triazol-1-yl)- 1,2-dihydro-3H-pyrazol-3-one
molidustat 2-[6-(morfolin-4-il)pirimidin-4-il]-4-(1H-1,2,3-triazol-1-il)-1,2-dihidro-3H-pirazol-3-ona
C13H14N8O2
N N
N
NHN
N NN
O
O
nesvacumabum # nesvacumab immunoglobulin G1-kappa, anti-[Homo sapiens ANGPT2
(angiopoietin 2, Ang2)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-452) [Homo sapiens VH (IGHV3-13*01 (97.90%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -IGHG1*01 (CH1 (123-220), hinge 221-235), CH2 (236-345), CH3 (346-450), CHS (451-452)) (123-452)], (225-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV3-20*01 (95.80%) -IGKJ1*01) [7.3.8] (1'-107') -IGKC*01 (108'-214')]; dimer (231-231'':234-234'')-bisdisulfide
nesvacumab immunoglobuline G1-kappa, anti-[Homo sapiens ANGPT2 (angiopoïétine 2, Ang2)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-452) [Homo sapiens VH (IGHV3-13*01 (97.90%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -IGHG1*01 (CH1 (123-220), charnière (221-235), CH2 (236-345), CH3 (346-450), CHS (451-452)) (123-452)], (225-214')-disulfure avec la chaîne légère kappa (1'-214') [Homo sapiens V- KAPPA (IGKV3-20*01 (95.80%) -IGKJ1*01) [7.3.8] (1'-107') -IGKC*01 (108'-214')]; dimère (231-231'':234-234'')-bisdisulfure
nesvacumab inmunoglobulina G1-kappa, anti-[Homo sapiens ANGPT2 (angiopoyetina 2, Ang2)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-452) [Homo sapiens VH (IGHV3-13*01 (97.90%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -IGHG1*01 (CH1 (123-220),bisagra (221-235), CH2 (236-345), CH3 (346-450), CHS (451-452)) (123-452)], (225-214')-disulfuro con la cadena ligera kappa (1'-214') [Homo sapiens V- KAPPA (IGKV3-20*01 (95.80%) -IGKJ1*01) [7.3.8] (1'-107') -IGKC*01 (108'-214')]; dímero (231-231'':234-234'')-bisdisulfuro

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
299
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGFTFS SYDIHWVRQA TGKGLEWVSA 50IGPAGDTYYP GSVKGRFTIS RENAKNSLYL QMNSLRAGDT AVYYCARGLI 100TFGGLIAPFD YWGQGTLVTV SSASTKGPSV FPLAPSSKST SGGTAALGCL 150VKDYFPEPVT VSWNSGALTS GVHTFPAVLQ SSGLYSLSSV VTVPSSSLGT 200QTYICNVNHK PSNTKVDKKV EPKSCDKTHT CPPCPAPELL GGPSVFLFPP 250KPKDTLMISR TPEVTCVVVD VSHEDPEVKF NWYVDGVEVH NAKTKPREEQ 300YNSTYRVVSV LTVLHQDWLN GKEYKCKVSN KALPAPIEKT ISKAKGQPRE 350PQVYTLPPSR DELTKNQVSL TCLVKGFYPS DIAVEWESNG QPENNYKTTP 400PVLDSDGSFF LYSKLTVDKS RWQQGNVFSC SVMHEALHNH YTQKSLSLSP 450GK 452
Light chain / Chaîne légère / Cadena ligeraEIVLTQSPGT LSLSPGERAT LSCRASQSVS STYLAWYQQK PGQAPRLLIY 50GASSRATGIP DRFSGSGSGT DFTLTISRLE PEDFAVYYCQ HYDNSQTFGQ 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-95 149-205 266-326 372-430 22''-95'' 149''-205'' 266''-326'' 372''-430''Intra-L 23'-89' 134'-194' 23'''-89''' 134'''-194''' Inter-H-L 225-214' 225''-214''' Inter-H-H 231-231'' 234-234''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:302, 302''
nonacogum gamma # nonacog gamma variant_011773 (148-T>A) of human coagulation factor IX (EC
3.4.21.22, Christmas factor, plasma thromboplastin component), glycosylated (γ-glycoform)
nonacog gamma variant_011773 (148-T>A) du facteur IX humain de coagulation (EC 3.4.21.22, facteur Christmas, facteur antihémophile B) glycosylé (glycoforme γ)
nonacog gamma variante_011773 (148-T>A) del factor IX humano de coagulación (EC 3.4.21.22, factor Christmas, factor antihemofílico B) glicosilado (glicoforma γ)
C2053H3116N558O675P2S26 (peptide)
HO2C CO2H
NH2HHO2C
CO2H
NH2HO
SHO
O O
HO2CCO2H
NH2H
OH
OCO2H
NH2H
PO
HO OH
E7-8-15-17-20-21-26
27-30-33-36-404-carboxyGlu
D64
3-hydroxyAsp
Y155
O-sulfoTyr
S158
O-phosphonoSer
Glycosylation sites / Sites de glycosylation / Posiciones de glicosilación (N, S*, T* )Ser-53* Ser-61* Asn-157 Thr-159* Asn-167 Thr-169* Thr-172* Thr-179** potential sites / sites potentiels / posiciones posibles
Sequence / Séquence / SecuenciaYNSGKLEEFV QGNLERECME EKCSFEEARE VFENTERTTE FWKQYVDGDQ 50CESNPCLNGG SCKDDINSYE CWCPFGFEGK NCELDVTCNI KNGRCEQFCK 100NSADNKVVCS CTEGYRLAEN QKSCEPAVPF PCGRVSVSQT SKLTRAEAVF 150PDVDYVNSTE AETILDNITQ STQSFNDFTR VVGGEDAKPG QFPWQVVLNG 200KVDAFCGGSI VNEKWIVTAA HCVETGVKIT VVAGEHNIEE TEHTEQKRNV 250IRIIPHHNYN AAINKYNHDI ALLELDEPLV LNSYVTPICI ADKEYTNIFL 300KFGSGYVSGW GRVFHKGRSA LVLQYLRVPL VDRATCLRST KFTIYNNMFC 350AGFHEGGRDS CQGDSGGPHV TEVEGTSFLT GIISWGEECA MKGKYGIYTK 400VSRYVNWIKE KTKLT 415
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro18-23 51-62 56-71 73-82 88-99 95-109111-124 132-289 206-222 336-350 361-389
Modified residues / Résidus modifiés / Restos modificados

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
300
olaptesedum pegolum olaptesed pegol β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-
uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adenylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidine 6-{2-(N-[ω-methylpoly(oxyethan-1,2-diyl)]-2-{[ω-methylpoly(oxyethan- 1,2-diyl)]oxy}acetamido)acetamido}hexyl hydrogen 5′-phosphate
olaptésed pégol β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-uridylyl-(3′→5′)-β-L-adénylyl-(3′→5′)-β-L-cytidylyl-(3′→5′)-β-L-guanylyl-(3′→5′)-β-L-cytidine 5'-hydrogénophosphate de 6-{2-(N-[ω-méthylpoly(oxyéthan- 1,2-diyl)]-2-{[ω-méthylpoly(oxyéthan- 1,2-diyl)]oxy}acétamido)acétamido}hexyle
olaptesed pegol β-L-guanilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-uridilil-(3′→5′)-β-L-adenilil-(3′→5′)-β-L-citidilil-(3′→5′)-β-L-guanilil-(3′→5′)-β-L-citidina 5'-hidrógenofosfato de 6-{2-(N-[ω-metilpoli(oxietan-1,2-diil)]-2-{[ω-metilpoli(oxietan- 1,2-diil)]oxi}acetamido)acetamido}hexilo
C442H554N169O326P45[C2H4O]2n
R- =
HN
O
NCH2
O
O
O
OH3C
OH3C
n
n
-L-ribo-[(3'-5')-R-pG-C-G-U-G-G-U-G-U-G-A-U-C-U-A-G-A-U-G-U-A-U-U-G-G-C-U-G-A-U-C-C-U-A-G-U-C-A-G-G-U-A-C-G-C]
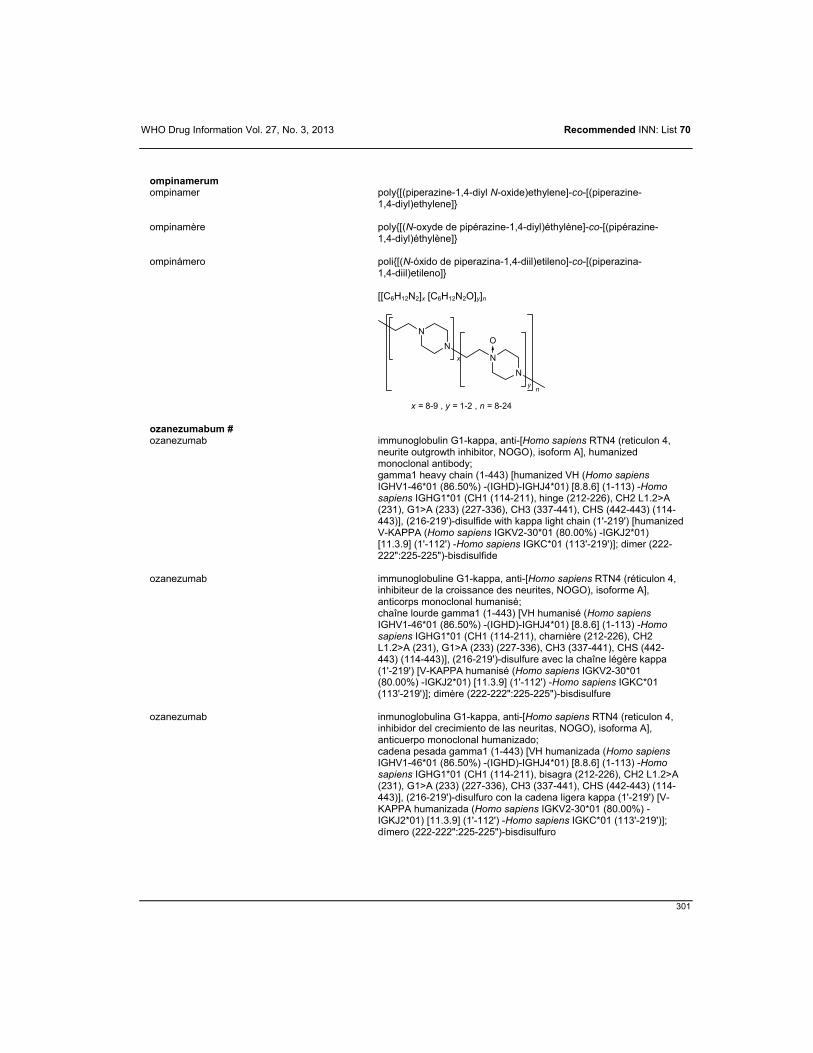
WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
301
ompinamerum ompinamer poly{[(piperazine-1,4-diyl N-oxide)ethylene]-co-[(piperazine-
1,4-diyl)ethylene]}
ompinamère poly{[(N-oxyde de pipérazine-1,4-diyl)éthylène]-co-[(pipérazine- 1,4-diyl)éthylène]}
ompinámero poli{[(N-óxido de piperazina-1,4-diil)etileno]-co-[(piperazina- 1,4-diil)etileno]}
[[C6H12N2]x [C6H12N2O]y]n
N
NN
N
O
x
yn
x = 8-9 , y = 1-2 , n = 8-24
ozanezumabum # ozanezumab immunoglobulin G1-kappa, anti-[Homo sapiens RTN4 (reticulon 4,
neurite outgrowth inhibitor, NOGO), isoform A], humanized monoclonal antibody; gamma1 heavy chain (1-443) [humanized VH (Homo sapiens IGHV1-46*01 (86.50%) -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*01 (CH1 (114-211), hinge (212-226), CH2 L1.2>A (231), G1>A (233) (227-336), CH3 (337-441), CHS (442-443) (114-443)], (216-219')-disulfide with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV2-30*01 (80.00%) -IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimer (222-222":225-225")-bisdisulfide
ozanezumab immunoglobuline G1-kappa, anti-[Homo sapiens RTN4 (réticulon 4, inhibiteur de la croissance des neurites, NOGO), isoforme A], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-443) [VH humanisé (Homo sapiens IGHV1-46*01 (86.50%) -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*01 (CH1 (114-211), charnière (212-226), CH2 L1.2>A (231), G1>A (233) (227-336), CH3 (337-441), CHS (442-443) (114-443)], (216-219')-disulfure avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV2-30*01 (80.00%) -IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimère (222-222":225-225")-bisdisulfure
ozanezumab inmunoglobulina G1-kappa, anti-[Homo sapiens RTN4 (reticulon 4, inhibidor del crecimiento de las neuritas, NOGO), isoforma A], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-443) [VH humanizada (Homo sapiens IGHV1-46*01 (86.50%) -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*01 (CH1 (114-211), bisagra (212-226), CH2 L1.2>A (231), G1>A (233) (227-336), CH3 (337-441), CHS (442-443) (114-443)], (216-219')-disulfuro con la cadena ligera kappa (1'-219') [V-KAPPA humanizada (Homo sapiens IGKV2-30*01 (80.00%) -IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dímero (222-222":225-225")-bisdisulfuro

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
302
Heavy chain / Chaîne lourde / Cadena pesadaQVQLVQSGAE VKKPGASVKV SCKASGYTFT SYWMHWVRQA PGQGLEWIGN 50INPSNGGTNY NEKFKSKATM TRDTSTSTAY MELSSLRSED TAVYYCELMQ 100GYWGQGTLVT VSSASTKGPS VFPLAPSSKS TSGGTAALGC LVKDYFPEPV 150TVSWNSGALT SGVHTFPAVL QSSGLYSLSS VVTVPSSSLG TQTYICNVNH 200KPSNTKVDKK VEPKSCDKTH TCPPCPAPEL AGAPSVFLFP PKPKDTLMIS 250RTPEVTCVVV DVSHEDPEVK FNWYVDGVEV HNAKTKPREE QYNSTYRVVS 300VLTVLHQDWL NGKEYKCKVS NKALPAPIEK TISKAKGQPR EPQVYTLPPS 350RDELTKNQVS LTCLVKGFYP SDIAVEWESN GQPENNYKTT PPVLDSDGSF 400FLYSKLTVDK SRWQQGNVFS CSVMHEALHN HYTQKSLSLS PGK 443
Light chain / Chaîne légère / Cadena ligeraDIVMTQSPLS NPVTLGQPVS ISCRSSKSLL YKDGKTYLNW FLQRPGQSPQ 50LLIYLMSTRA SGVPDRFSGG GSGTDFTLKI SRVEAEDVGV YYCQQLVEYP 100LTFGQGTKLE IKRTVAAPSV FIFPPSDEQL KSGTASVVCL LNNFYPREAK 150VQWKVDNALQ SGNSQESVTE QDSKDSTYSL SSTLTLSKAD YEKHKVYACE 200VTHQGLSSPV TKSFNRGEC 219
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 140-196 257-317 363-421 22''-96'' 140''-196'' 257''-317'' 363''-421''Intra-L 23'-93' 139'-199' 23'''-93''' 139'''-199''' Inter-H-L 216-219' 216''-219''' Inter-H-H 222-222'' 225-225''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:293, 293'
peginterferonum beta-1a # peginterferon beta-1a N2.1-{(2RS)-2-methyl-3-[ω-methoxypoly(oxyethylene)]propyl}human
interferon beta (fibroblast interferon, IFN-beta) glycosylated expressed in mammalian cells
péginterféron bêta-1a N2.1-{(2RS)-2-méthyl-3-[ω-méthoxypoly(oxyéthylène)]propyl}interféron bêta humain (interféron fibroblastoïde, IFN-bêta) glycosylé produit par les cellules de mammifères
peginterferón beta-1a N2.1-{(2RS)-2-metil-3-[ω-metoxipoli(oxietileno)]propil}interferón beta humano (interferón fibroblastoide, IFN-beta) glicosilado producido por las células de mamífero
C913H1417N246O256PS7 [C2H4O]n
H3CO
O NH
CO2H
H
S
CH3
nH CH3
*
and epimer at C*et l'épimère en C*y el epímero al C*
H2N CO2H
H
O P
O
OHOH
Sequence / Séquence / SecuenciaMSYNLLGFLQ RSSNFQCQKL LWQLNGRLEY CLKDRMNFDI PEEIKQLQQF 50QKEDAALTIY EMLQNIFAIF RQDSSSTGWN ETIVENLLAN VYHQINHLKT 100VLEEKLEKED FTRGKLMSSL HLKRYYGRIL HYLKAKEYSH CAWTIVRVEI 150LRNFYFINRL TGYLRN 166
Disulfide bridge location / Position du pont disulfure / Posicion del puente disulfuro31-141
Modified residues / Résidus modifiés / Restos modificados
M1
N-pegMet
S119
O-phosphonoSer
Glycosylation site (N) / Site de glycosylation (N) / Posicion de glicosilación (N)Asn-80

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
303
pexastimogenum devacirepvecum # pexastimogene devacirepvec recombinant vaccinia virus vector (Wyeth strain) with its thymidine
kinase gene de-activated by insertion of a GM-CSF (Granulocytes-macrophages colony stimulating factor) gene under the control of a synthetic early/late promoter and a beta-galactosidase gene under the control of the p7.5 early/late promoter
pexastimogène dévacirépvec vecteur viral recombinant répliquant de la vaccine avec son gène de la thymidine kinase désactivé par l'insertion du gène GM-CSF(facteur de stimulation des colonies de granulocytes et de macrophages) sous le contrôle d'un promoteur synthétique précoce tardif et d'un gène de bêta-galactosidase sous le contrôle du promoteur p7.5 précoce tardif
pexastimogén devacirepvec vector virus vaccinia recombinante replicante con el gen de la timidina kinasa desactivado por inserción del gen GM-CSF(factor de estimulación de colonias de granulocitos y macrófagos) bajo control de un promotor sintético precoz tardío y de un gen de beta-galactosidasa bajo control del promotor p7.5 precoz tardío
pidilizumabum # pidilizumab immunoglobulin G1-kappa, anti-[Homo sapiens PDCD1
(programmed cell death 1, PD-1, PD1, CD279)], humanized monoclonal antibody; gamma1 heavy chain (1-447) [humanized VH (Homo sapiens IGHV7-4-1*03 (83.50%) -(IGHD)-IGHJ3*01 M11>L (112)) [8.8.10] (1-117) -Homo sapiens IGHG1*03 (CH1 (118-215), hinge 216-230, CH2 (231-340), CH3 (341-445), CHS (446-447)], (220-213')-disulfide with kappa light chain (1'-213') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (75.80%) -IGKJ4*01 V9 >L (103)) [5.3.9] (1'-106') -Homo sapiens IGKC*01 (107'-213')]; dimer (226-226":229-229")-bisdisulfide
pidilizumab immunoglobuline G1-kappa, anti-[Homo sapiens PDCD1 (protéine 1 de mort cellulaire programmée, PD-1, PD1, CD279)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-447) [VH humanisé (Homo sapiens IGHV7-4-1*03 (83.50%) -(IGHD)-IGHJ3*01 M11>L (112)) [8.8.10] (1-117) -Homo sapiens IGHG1*03 (CH1 (118-215), charnière 216-230, CH2 (231-340), CH3 (341-445), CHS (446-447)], (220-213')-disulfure avec la chaîne légère kappa (1'-213') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (75.80%) -IGKJ4*01 V9 >L (103)) [5.3.9] (1'-106') -Homo sapiens IGKC*01 (107'-213')]; dimère (226-226":229-229")-bisdisulfure
pidilizumab inmunoglobulina G1-kappa, anti-[Homo sapiens PDCD1 (proteína 1 de muerte celular programada, PD-1, PD1, CD279)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-447) [VH humanizado (Homo sapiens IGHV7-4-1*03 (83.50%) -(IGHD)-IGHJ3*01 M11>L (112)) [8.8.10] (1-117) -Homo sapiens IGHG1*03 (CH1 (118-215),bisagra 216-230, CH2 (231-340), CH3 (341-445), CHS (446-447)], (220-213')-disulfuro con la cadena ligera kappa (1'-213') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (75.80%) -IGKJ4*01 V9 >L (103)) [5.3.9] (1'-106') -Homo sapiens IGKC*01 (107'-213')]; dímero (226-226":229-229")-bisdisulfuro

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
304
Heavy chain / Chaîne lourde / Cadena pesadaQVQLVQSGSE LKKPGASVKI SCKASGYTFT NYGMNWVRQA PGQGLQWMGW 50INTDSGESTY AEEFKGRFVF SLDTSVNTAY LQITSLTAED TGMYFCVRVG 100YDALDYWGQG TLVTVSSAST KGPSVFPLAP SSKSTSGGTA ALGCLVKDYF 150PEPVTVSWNS GALTSGVHTF PAVLQSSGLY SLSSVVTVPS SSLGTQTYIC 200NVNHKPSNTK VDKRVEPKSC DKTHTCPPCP APELLGGPSV FLFPPKPKDT 250LMISRTPEVT CVVVDVSHED PEVKFNWYVD GVEVHNAKTK PREEQYNSTY 300RVVSVLTVLH QDWLNGKEYK CKVSNKALPA PIEKTISKAK GQPREPQVYT 350LPPSREEMTK NQVSLTCLVK GFYPSDIAVE WESNGQPENN YKTTPPVLDS 400DGSFFLYSKL TVDKSRWQQG NVFSCSVMHE ALHNHYTQKS LSLSPGK 447
Light chain / Chaîne légère / Cadena ligeraEIVLTQSPSS LSASVGDRVT ITCSARSSVS YMHWFQQKPG KAPKLWIYRT 50SNLASGVPSR FSGSGSGTSY CLTINSLQPE DFATYYCQQR SSFPLTFGGG 100TKLEIKRTVA APSVFIFPPS DEQLKSGTAS VVCLLNNFYP REAKVQWKVD 150NALQSGNSQE SVTEQDSKDS TYSLSSTLTL SKADYEKHKV YACEVTHQGL 200SSPVTKSFNR GEC 213
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 144-200 261-321 367-425 22''-96'' 144''-200'' 261''-321'' 367''-425''Intra-L 23'-87' 133'-193' 23'''-87''' 133'''-193''' Inter-H-L 220-213' 220''-213''' Inter-H-H 226-226'' 229-229''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:297, 297''
pilaralisibum pilaralisib 2-amino-N-(3-{[3-(2-chloro-5-methoxyanilino)quinoxalin-
2-yl]sulfamoyl}phenyl)-2-methylpropanamide
pilaralisib 2-amino-N-(3-{[3-(2-chloro-5-méthoxyanilino)quinoxalin- 2-yl]sulfamoyl}phényl)-2-méthylpropanamide
pilaralisib 2-amino-N-(3-{[3-(2-cloro-5-metoxianilino)quinoxalin- 2-il]sulfamoil}fenil)-2-metilpropanamida
C25H25ClN6O4S
HN
H2NS
NH
O
CH3H3C OO
N
NHN
Cl
OCH3
pinatuzumabum vedotinum # pinatuzumab vedotin immunoglobulin G1-kappa auristatin E conjugate, anti-[Homo sapiens
CD22 (sialic acid binding Ig-like lectin 2, SIGLEC2, SIGLEC-2, B-lymphocyte cell adhesion molecule, BL-CAM, Leu-14)], humanized monoclonal antibody conjugated to auristatin E; gamma1 heavy chain (1-450) [humanized VH (Homo sapiens IGHV3-66*01 (79.60%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03 (CH1 R120>K (217) (121-218), hinge (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-219')-disulfide (if not conjugated) with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (80.00%) -IGKJ1*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimer (229-229":232-232")-bisdisulfide; conjugated, on an average of 3 to 4 cysteinyl, to monomethylauristatin E (MMAE), via a cleavable maleimidecaproyl-valyl-citrullinyl-p-aminobenzylcarbamate (mc-val-cit-PABC) linker For the vedotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
305
pinatuzumab védotine immunoglobuline G1-kappa conjuguée à l'auristatine E, anti-[Homo sapiens CD22 (Ig-like lectine 2 liant l'acide sialique, SIGLEC2, SIGLEC-2, molécule d'adhésion cellulaire du lymphocyte B, BL-CAM, Leu-14)], anticorps monoclonal humanisé conjugué à l'auristatine E; chaîne lourde gamma1 (1-450) [VH humanisé (Homo sapiens IGHV3-66*01 (79.60%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03 (CH1 R120>K (217) (121-218), charnière (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-219')-disulfure (si non conjugué) avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (80.00%) -IGKJ1*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimère (229-229":232-232")-bisdisulfure; conjugué, sur 3 à 4 cystéinyl en moyenne, au monométhylauristatine E (MMAE), via un linker clivable maléimidecaproyl-valyl-citrullinyl-p-aminobenzylcarbamate (mc-val-cit-PABC) Pour la partie védotine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
pinatuzumab vedotina inmunoglobulina G1-kappa conjugada con auristatina E, anti-[Homo sapiens CD22 (Ig-like lectine 2 que liga ácido siálico, SIGLEC2, SIGLEC-2, molécula d'adhesión celular del linfocito B, BL-CAM, Leu-14)], anticuerpo monoclonal humanizado conjugado con auristatina E; cadena pesada gamma1 (1-450) [VH humanizado (Homo sapiens IGHV3-66*01 (79.60%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03 (CH1 R120>K (217) (121-218), bisagra (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-219')-disulfuro (si no conjugado ) con la cadena ligera kappa (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (80.00%) -IGKJ1*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dímero (229-229":232-232")-bisdisulfuro; conjugado, en 3 - 4 restos cistenil por término medio, con monometilauristatina E (MMAE), mediante un vínculo escindible maleimidacaproil-valil-citrulinil-p-aminobencilcarbamato (mc-val-cit-PABC) Para la fracción vedotina , se pueden dirigir al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGYEFS RSWMNWVRQA PGKGLEWVGR 50IYPGDGDTNY SGKFKGRFTI SADTSKNTAY LQMNSLRAED TAVYYCARDG 100SSWDWYFDVW GQGTLVTVSS ASTKGPSVFP LAPSSKSTSG GTAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSSLGTQT 200YICNVNHKPS NTKVDKKVEP KSCDKTHTCP PCPAPELLGG PSVFLFPPKP 250KDTLMISRTP EVTCVVVDVS HEDPEVKFNW YVDGVEVHNA KTKPREEQYN 300STYRVVSVLT VLHQDWLNGK EYKCKVSNKA LPAPIEKTIS KAKGQPREPQ 350VYTLPPSREE MTKNQVSLTC LVKGFYPSDI AVEWESNGQP ENNYKTTPPV 400LDSDGSFFLY SKLTVDKSRW QQGNVFSCSV MHEALHNHYT QKSLSLSPGK 450
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVT ITCRSSQSIV HSVGNTFLEW YQQKPGKAPK 50LLIYKVSNRF SGVPSRFSGS GSGTDFTLTI SSLQPEDFAT YYCFQGSQFP 100YTFGQGTKVE IKRTVAAPSV FIFPPSDEQL KSGTASVVCL LNNFYPREAK 150VQWKVDNALQ SGNSQESVTE QDSKDSTYSL SSTLTLSKAD YEKHKVYACE 200VTHQGLSSPV TKSFNRGEC 219
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 147-203 264-324 370-428 22''-96'' 147''-203'' 264''-324'' 370''-428''Intra-L 23'-93' 139'-199' 23'''-93''' 139'''-199''' Inter-H-L* 223-219' 223''-219''' Inter-H-H* 229-229'' 232-232'' *Two or three of the inter-chain disulfide bridges are not present, the antibody being conjugated to an average of 3 to 4 drug linkers each via a thioether bond. * Deux ou trois des ponts disulfure inter-chaines ne sont pas présents, l'anticorps étant conjugué à une moyenne de 3 à 4 linker-principe actif chacun via une liaison thioéther.* Faltan dos o tres puentes disulfuro inter-catenarios por estar el anticuerpo conjugado, con sendos enlaces tioéter, a una media de 3 a 4 conectores de principio activo.
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:300, 300'' but lacking carbohydrate/hydrate de carbone manquant/ falta hidrato de carbono
Other post-translational modificationsAutres modifications post-traductionnellesOtras modificaciones post-traduccionalesLacking H chain C-terminal lysine (CHS K2>del)

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
306
piromelatinum piromelatine N-[2-(5-methoxy-1H-indol-3-yl)ethyl]-4-oxo-4H-pyran-2-carboxamide
piromélatine N-[2-(5-méthoxy-1H-indol-3-yl)éthyl]-4-oxo-4H-pyran-2-carboxamide
piromelatina N-[2-(5-metoxi-1H-indol-3-il)etil]-4-oxo-4H-piran-2-carboxamida
C17H16N2O4
O
NH
OHN
H3CO
O
polatuzumabum vedotinum # polatuzumab vedotin immunoglobulin G1-kappa auristatin E conjugate, anti-[Homo
sapiens CD79B (immunoglobulin-associated CD79 beta)], humanized monoclonal antibody conjugated to auristatin E; gamma1 heavy chain (1-447) [humanized VH (Homo sapiens IGHV3-66*01 (79.60%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03 (CH1 R120>K (214) (121-218), hinge (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (220-218')-disulfide (if not conjugated) with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (80.00%) -IGKJ1*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-218')]; dimer (226-226":229-229")-bisdisulfide; conjugated, on an average of 3 to 4 cysteinyl, to monomethylauristatin E (MMAE), via a cleavable maleimidecaproyl-valyl-citrullinyl-p-aminobenzylcarbamate (mc-val-cit-PABC) linker For the vedotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
polatuzumab védotine immunoglobuline G1-kappa conjuguée à l'auristatine E, anti-[Homo sapiens CD79B (CD79 bêta associé à l'immunoglobuline)], anticorps monoclonal humanisé conjugué à l'auristatine E; chaîne lourde gamma1 (1-447) [VH humanisé (Homo sapiens IGHV3-66*01 (79.60%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03 (CH1 R120>K (214) (121-218), charnière (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (220-218')-disulfure (si non conjugué) avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (80.00%) -IGKJ1*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-218')]; dimère (226-226":229-229")-bisdisulfure; conjugué, sur 3 à 4 cystéinyl en moyenne, au monométhylauristatine E (MMAE), via un linker clivable maléimidecaproyl-valyl-citrullinyl-p-aminobenzylcarbamate (mc-val-cit-PABC) Pour la partie védotine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
307
polatuzumab vedotina inmunoglobulina G1-kappa conjugada con auristatina E, anti-[Homo sapiens CD79B (CD79 beta asociado a la inmunoglobulina)], anticuerpo monoclonal humanizado conjugado con auristatina E; cadena pesada gamma1 (1-447) [VH humanizado (Homo sapiens IGHV3-66*01 (79.60%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03 (CH1 R120>K (214) (121-218), bisagra (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (220-218')-disulfuro (si no está conjugado ) con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (80.00%) -IGKJ1*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-218')]; dímero (226-226":229-229")-bisdisulfuro; conjugado, en 3 - 4 restos cisteinil por término medio, con monometilauristatina E (MMAE), mediante un vínculo escindible maleimidacaproil-valil-citrulinil-p-aminobencilcarbamato (mc-val-cit-PABC) Para la fracción vedotina se pueden referir al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGYTFS SYWIEWVRQA PGKGLEWIGE 50ILPGGGDTNY NEIFKGRATF SADTSKNTAY LQMNSLRAED TAVYYCTRRV 100PIRLDYWGQG TLVTVSSAST KGPSVFPLAP SSKSTSGGTA ALGCLVKDYF 150PEPVTVSWNS GALTSGVHTF PAVLQSSGLY SLSSVVTVPS SSLGTQTYIC 200NVNHKPSNTK VDKKVEPKSC DKTHTCPPCP APELLGGPSV FLFPPKPKDT 250LMISRTPEVT CVVVDVSHED PEVKFNWYVD GVEVHNAKTK PREEQYNSTY 300RVVSVLTVLH QDWLNGKEYK CKVSNKALPA PIEKTISKAK GQPREPQVYT 350LPPSREEMTK NQVSLTCLVK GFYPSDIAVE WESNGQPENN YKTTPPVLDS 400DGSFFLYSKL TVDKSRWQQG NVFSCSVMHE ALHNHYTQKS LSLSPGK 447
Light chain / Chaîne légère / Cadena ligeraDIQLTQSPSS LSASVGDRVT ITCKASQSVD YEGDSFLNWY QQKPGKAPKL 50LIYAASNLES GVPSRFSGSG SGTDFTLTIS SLQPEDFATY YCQQSNEDPL 100TFGQGTKVEI KRTVAAPSVF IFPPSDEQLK SGTASVVCLL NNFYPREAKV 150QWKVDNALQS GNSQESVTEQ DSKDSTYSLS STLTLSKADY EKHKVYACEV 200THQGLSSPVT KSFNRGEC 218
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 144-200 261-321 367-425 22''-96'' 147''-203'' 261''-321'' 367''-425''Intra-L 23'-92' 138'-198' 23'''-92''' 138'''-198''' Inter-H-L* 220-218' 220''-218''' Inter-H-H* 226-226'' 229-229'' *Two or three of the inter-chain disulfide bridges are not present, the antibody being conjugated to an average of 3 to 4 drug linkers each via a thioether bond. * Deux ou trois des ponts disulfure inter-chaines ne sont pas présents, l'anticorps étant conjugué à une moyenne de 3 à 4 linker-principe actif chacun via une liaison thioéther.* Faltan dos o tres puentes disulfuro inter-catenarios por estar el anticuerpo conjugado, con sendos enlaces tioéter, a una media de 3 a 4 conectores de principio activo.
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:297, 297'' but lacking carbohydrate/hydrate de carbone manquant/ falta hidrato de carbono
Other post-translational modificationsAutres modifications post-traductionnellesOtras modificaciones post-traduccionalesLacking H chain C-terminal lysine (CHS K2>del)
poziotinibum poziotinib 1-(4-{[4-(3,4-dichloro-2-fluoroanilino)-7-methoxyquinazolin-
6-yl]oxy}piperidin-1-yl)prop-2-en-1-one
poziotinib 1-(4-{[4-(3,4-dichloro-2-fluoroanilino)-7-méthoxyquinazolin- 6-yl]oxy}pipéridin-1-yl)prop-2-èn-1-one
poziotinib 1-(4-{[4-(3,4-dicloro-2-fluoroanilino)-7-metoxiquinazolin- 6-il]oxi}piperidin-1-il)prop-2-en-1-ona

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
308
C23H21Cl2FN4O3
N
N
HN
F
O
Cl
Cl
O
CH3
NH2C
O
pritoxaximabum # pritoxaximab immunoglobulin G1-kappa, anti-[shiga toxin-producing Escherichia
coli (STEC) shiga toxin type 1 (stx1), B subunit)], chimeric monoclonal antibody; gamma1 heavy chain (1-454) [Mus musculus VH (IGHV1-12*01 -(IGHD)-IGHJ2*01) [8.8.15] (1-122) -linker (123-124) -Homo sapiens IGHG1*01 (CH1 (125-222), hinge (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (227-214')-disulfide with kappa light chain (1'-214') [Mus musculus V-KAPPA (IGKV6-23*01 -IGKJ5*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimer (233-233'':236-236'')-bisdisulfide
pritoxaximab immunoglobuline G1-kappa, anti-[sous-unité B de la toxine type 1 shiga (stx1) d'Escherichia coli produisant des shiga-toxines (STEC)], anticorps monoclonal chimérique; chaîne lourde gamma1 (1-454) [Mus musculus VH (IGHV1-12*01 -(IGHD)-IGHJ2*01) [8.8.15] (1-122) -linker (123-124) -Homo sapiens IGHG1*01 (CH1 (125-222), charnière (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (227-214')-disulfure avec la chaîne légère kappa (1'-214') [Mus musculus V-KAPPA (IGKV6-23*01 -IGKJ5*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimère (233-233'':236-236'')-bisdisulfure
pritoxaximab inmunoglobulina G1-kappa, anti-[subunidad B de la toxina tipo 1 shiga (stx1) de Escherichia coli productor de toxinas shiga (STEC)], anticuerpo monoclonal quimérico; cadena pesada gamma1 (1-454) [Mus musculus VH (IGHV1-12*01 -(IGHD)-IGHJ2*01) [8.8.15] (1-122) -vínculo (123-124) -Homo sapiens IGHG1*01 (CH1 (125-222), bisagra (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (227-214')-disulfuro con la cadena ligera kappa (1'-214') [Mus musculus V-KAPPA (IGKV6-23*01 -IGKJ5*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dímero (233-233'':236-236'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesadaQVQLQESGAE LVRSGASVRM SCKASGYTFT SYNMHWVKQT PGQGLEWIGY 50IYPGNGGTNY IQKFKGKAIL TADTSSSTAY MQISSLTSED SAVYFCTRSP 100SHYSSDPYFD YWGQGTTLTV SSEFASTKGP SVFPLAPSSK STSGGTAALG 150CLVKDYFPEP VTVSWNSGAL TSGVHTFPAV LQSSGLYSLS SVVTVPSSSL 200GTQTYICNVN HKPSNTKVDK KVEPKSCDKT HTCPPCPAPE LLGGPSVFLF 250PPKPKDTLMI SRTPEVTCVV VDVSHEDPEV KFNWYVDGVE VHNAKTKPRE 300EQYNSTYRVV SVLTVLHQDW LNGKEYKCKV SNKALPAPIE KTISKAKGQP 350REPQVYTLPP SRDELTKNQV SLTCLVKGFY PSDIAVEWES NGQPENNYKT 400TPPVLDSDGS FFLYSKLTVD KSRWQQGNVF SCSVMHEALH NHYTQKSLSL 450SPGK 454
Light chain / Chaîne légère / Cadena ligeraDIVMSQSHKF MSTSVGDRVS ITCKASQDVG TAVAWYQQNP GQSPKFLIYW 50ASTRHTGVPD RFTGSGSGTD FTLTITNVQS EDLADYFCQQ YSSYPLTFGA 100GTSLELKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 151-207 268-328 374-432 22''-96'' 151''-207'' 268''-328'' 374''-432''Intra-L 23'-88' 134'-194' 23'''-88''' 134'''-194''' Inter-H-L 227-214' 227''-214''' Inter-H-H 233-233'' 236-236''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:304, 304''

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
309
ramaterceptum # ramatercept fusion protein for immune applications (FPIA) comprising Homo
sapiens ACVR2B (activin A receptor type IIB, ActR-IIB) fragment, fused with Homo sapiens immunoglobulin G1 Fc fragment; Homo sapiens ACVR2B precursor fragment 20-134 (1-115) -triglycyl (116-118) -Homo sapiens IGHG1*03 H-CH2-CH3 fragment (hinge 8-15 (119-126), CH2 A115>V (226) (127-236), CH3 (237-341), CHS (342-343)) (119-343); dimer (122-122':125-125')-bisdisulfide
ramatercept protéine de fusion pour applications immunitaires (FPIA) comprenant un fragment d'Homo sapiens ACVR2B (récepteur de type IIB de l'activine A, ActR-IIB), fusionné au fragment Fc de l'Homo sapiens immunoglobuline G1; Homo sapiens ACVR2B fragment 20-134 du précurseur (1-115) -triglycyl (116-118) -Homo sapiens IGHG1*03 fragment H-CH2-CH3 (charnière 8-15 (119-126), CH2 A115>V (226) (127-236), CH3 (237-341), CHS (342-343)) (119-343)]; dimère (122-122':125-125')-bisdisulfure
ramatercept proteína de fusión para aplicaciones inmunitarias (FPIA) que comprende un fragmento de Homo sapiens ACVR2B (receptor de tipo IIB de la activina A, ActR-IIB), fusionado con el fragmento Fc de la Homo sapiens inmunoglobulina G1; Homo sapiens ACVR2B fragmento 20-134 del precursor (1-115) -triglicil (116-118) -Homo sapiens IGHG1*03 fragmento H-CH2-CH3 (bisagra 8-15 (119-126), CH2 A115>V (226) (127-236), CH3 (237-341), CHS (342-343)) (119-343)]; dímero (122-122':125-125')-bisdisulfuro
Fused chain / Chaîne fusionnée / Cadena fusionada
GRGEAETREC IYYNANWELE RTNQSGLERC EGEQDKRLHC YASWRNSSGT 50IELVKKGCWL DDFNCYDRQE CVATEENPQV YFCCCEGNFC NERFTHLPEA 100GGPEVTYEPP PTAPTGGGTH TCPPCPAPEL LGGPSVFLFP PKPKDTLMIS 150RTPEVTCVVV DVSHEDPEVK FNWYVDGVEV HNAKTKPREE QYNSTYRVVS 200VLTVLHQDWL NGKEYKCKVS NKALPVPIEK TISKAKGQPR EPQVYTLPPS 250REEMTKNQVS LTCLVKGFYP SDIAVEWESN GQPENNYKTT PPVLDSDGSF 300FLYSKLTVDK SRWQQGNVFS CSVMHEALHN HYTQKSLSLS PGK 343
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-chain 10-40 30-58 65-84 71-83 85-90 157-217 263-321 10'-40' 30'-58' 65'-84' 71'-83' 85'-90' 157'-217' 263'-321'Inter-chains 122-122' 125-125'
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilación23, 46, 193 (CH2 N84.4)23', 46', 193' (CH2 N84.4)
rebastinibum rebastinib 4-[4-({[3-tert-butyl-1-(quinolin-6-yl)-1H-pyrazol-
5-yl]carbamoyl}amino)-3-fluorophenoxy]-N-methylpyridin- 2-carboxamide
rébastinib 4-(4-{[3-tert-butyl-1-(quinoléin-6-yl)-1H-pyrazol- 5-yl]carbamoyl}amino)-3-fluorophénoxy)-N-méthylpyridin- 2-carboxamide
rebastinib 4-[4-({[3-terc-butil-1-(quinolin-6-il)-1H-pirazol-5-il]carbamoil}amino)- 3-fluorofenoxi]-N-metilpiridin-2-carboxamida

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
310
C30H28FN7O3
N
OHN
CH3
O
HN
HN
OF
NN
N
H3CCH3
CH3
recilisibum recilisib 4-[(1E)-2-{[(4-chlorophenyl)methyl]sulfonyl}ethenyl]benzoic acid
récilisib acide 4-[(1E)-2-{[(4-chlorophényl)méthyl]sulfonyl}éthényl]benzoïque
recilisib ácido 4-[(1E)-2-{[(4-clorofenil)metil]sulfonil}etenil]benzoico
C16H13ClO4S
S
CO2H
O OCl
revexepridum revexepride 4-amino-5-chloro-N-{[(3S,4S)-3-hydroxy-
1-(3-methoxypropyl)piperidin-4-yl]methyl}-2,2-dimethyl-2,3-dihydro-1-benzofuran-7-carboxamide
révexépride 4-amino-5-chloro-N-{[(3S,4S)-3-hydroxy- 1-(3-méthoxypropyl)pipéridin-4-yl]méthyl}-2,2-diméthyl-2,3-dihydro-1-benzofurane-7-carboxamide
revexeprida 4-amino-5-cloro-N-{[(3S,4S)-3-hidroxi-1-(3-metoxipropil)piperidin- 4-il]metil}-2,2-dimetil-2,3-dihidro-1-benzofuran-7-carboxamida
C21H32ClN3O4
O
O
NH
H2N
Cl
CH3H3C
N
HOH O CH3
H
roxadustatum roxadustat N-[(4-hydroxy-1-methyl-7-phenoxyisoquinolin-3-yl)carbonyl]glycine
roxadustat N-[(4-hydroxy-1-méthyl-7-phénoxyisoquinoléin-3-yl)carbonyl]glycine
roxadustat N-[(4-hidroxi-1-metil-7-fenoxiisoquinolin-3-il)carbonil]glicina

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
311
C19H16N2O5
NO
CH3
OH
HN CO2H
O
saroglitazarum saroglitazar (2S)-2-ethoxy-3-[4-(2-{2-methyl-5-[4-(methylsulfanyl)phenyl]-
1H-pyrrol-1-yl}ethoxy)phenyl]propanoic acid
saroglitazar acide (2S)-2-éthoxy-3-[4-(2-{2-méthyl-5-[4-(méthylsulfanyl)phényl]-1H-pyrrol-1-yl}éthoxy)phényl]propanoïque
saroglitazar ácido (2S)-2-etoxi-3-[4-(2-{2-metil-5-[4-(metilsulfanil)fenil]-1H-pirrol-1-il}etoxi)fenil]propanoico
C25H29NO4S
CO2H
ON OH
CH3
CH3
H3CS
seribantumabum # seribantumab immunoglobulin G2-lambda7, anti-[Homo sapiens ERBB3 (receptor
tyrosine-protein kinase erbB-3, HER3)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-445) [Homo sapiens VH (IGHV3-23*01 (90.80%) -(IGHD)-IGHJ4*01) [8.8.12] (1-119) -IGHG2*01 (CH1 (120-217), hinge (218-229), CH2 (230-338), CH3 (339-443), CHS (444-445)) (120-445)], (133-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV2-23*02 (94.90%) -IGLJ2*01 L9>V (108) [9.3.11] (1'-111') -IGLC7*01 (100.00%) (112'-217')]; dimer (221-221'':222-222'':225-225'':228-228'')-tetrakisdisulfide
séribantumab immunoglobuline G2-lambda7, anti-[Homo sapiens ERBB3 (récepteur tyrosine-protéine kinase erbB3, HER3)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-445) [Homo sapiens VH (IGHV3-23*01 (90.80%) -(IGHD)-IGHJ4*01) [8.8.12] (1-119) -IGHG2*01 (CH1 (120-217), charnière (218-229), CH2 (230-338), CH3 (339-443), CHS (444-445)) (120-445)], (133-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V- LAMBDA (IGLV2-23*02 (94.90%) -IGLJ2*01 L9>V (108) [9.3.11] (1'-111') -IGLC7*01 (100.00%) (112'-217')]; dimère (221-221'':222-222'':225-225'':228-228'')-tétrakisdisulfure

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
312
seribantumab inmunoglobulina G2-lambda7, anti-[Homo sapiens ERBB3 (receptor tirosina-proteína kinasa erbB3, HER3)], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma2 (1-445) [Homo sapiens VH (IGHV3-23*01 (90.80%) -(IGHD)-IGHJ4*01) [8.8.12] (1-119) -IGHG2*01 (CH1 (120-217), bisagra(218-229), CH2 (230-338), CH3 (339-443), CHS (444-445)) (120-445)], (133-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens V- LAMBDA (IGLV2-23*02 (94.90%) -IGLJ2*01 L9>V (108) [9.3.11] (1'-111') -IGLC7*01 (100.00%) (112'-217')]; dímero (221-221'':222-222'':225-225'':228-228'')-tetrakisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
EVQLLESGGG LVQPGGSLRL SCAASGFTFS HYVMAWVRQA PGKGLEWVSS 50ISSSGGWTLY ADSVKGRFTI SRDNSKNTLY LQMNSLRAED TAVYYCTRGL 100KMATIFDYWG QGTLVTVSSA STKGPSVFPL APCSRSTSES TAALGCLVKD 150YFPEPVTVSW NSGALTSGVH TFPAVLQSSG LYSLSSVVTV PSSNFGTQTY 200TCNVDHKPSN TKVDKTVERK CCVECPPCPA PPVAGPSVFL FPPKPKDTLM 250ISRTPEVTCV VVDVSHEDPE VQFNWYVDGV EVHNAKTKPR EEQFNSTFRV 300VSVLTVVHQD WLNGKEYKCK VSNKGLPAPI EKTISKTKGQ PREPQVYTLP 350PSREEMTKNQ VSLTCLVKGF YPSDIAVEWE SNGQPENNYK TTPPMLDSDG 400SFFLYSKLTV DKSRWQQGNV FSCSVMHEAL HNHYTQKSLS LSPGK 445
Light chain / Chaîne légère / Cadena ligeraQSALTQPASV SGSPGQSITI SCTGTSSDVG SYNVVSWYQQ HPGKAPKLII 50YEVSQRPSGV SNRFSGSKSG NTASLTISGL QTEDEADYYC CSYAGSSIFV 100IFGGGTKVTV LGQPKAAPSV TLFPPSSEEL QANKATLVCL VSDFYPGAVT 150VAWKADGSPV KVGVETTKPS KQSNNKYAAS SYLSLTPEQW KSHRSYSCRV 200THEGSTVEKT VAPAECS 217
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 146-202 259-319 365-423 22''-96'' 146''-202'' 259''-319'' 365''-423''Intra-L 22'-90' 139'-198' 22'''-90''' 139'''-198''' Inter-H-L 133-216' 133''-216''' Inter-H-H 221-221'' 222-222'' 225-225'' 228-228''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:295, 295''
setoxaximabum # setoxaximab immunoglobulin G1-kappa, anti-[shiga toxin-producing Escherichia
coli (STEC) shiga toxin type 2 (stx2), A subunit)], chimeric monoclonal antibody; gamma1 heavy chain (1-451) [Mus musculus VH (IGHV1-39*01 -(IGHD)-IGHJ1*01) [8.8.12] (1-119) -linker (120-121) -Homo sapiens IGHG1*01 (CH1 (122-219), hinge (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451) (122-451)], (224-220')-disulfide with kappa light chain (1'-220') [Mus musculus V-KAPPA (IGKV8-30*01 -IGKJ5*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01 (114'-220')]; dimer (230-230'':233-233'')-bisdisulfide
sétoxaximab immunoglobuline G1-kappa, anti-[sous-unité A de la toxine type 2 shiga (stx2) d'Escherichia coli produisant des shiga-toxines (STEC)], anticorps monoclonal chimérique; chaîne lourde gamma1 (1-451) [Mus musculus VH (IGHV1-39*01 -(IGHD)-IGHJ1*01) [8.8.12] (1-119) -linker (120-121) -Homo sapiens IGHG1*01 (CH1 (122-219), charnière (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451)) (122-451)], (224-220')-disulfure avec la chaîne légère kappa (1'-220') [Mus musculus V-KAPPA (IGKV8-30*01 -IGKJ5*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01 (114'-220')]; (230-230'':233-233'')-bisdisulfure

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
313
setoxaximab inmunoglobulina G1-kappa, anti-[subunidad A de la toxina tipo 2 shiga (stx2) de Escherichia coli productor de toxinas shiga (STEC)], anticuerpo monoclonal quimérico; cadena pesada gamma1 (1-451) [Mus musculus VH (IGHV1-39*01 -(IGHD)-IGHJ1*01) [8.8.12] (1-119) -vínculo(120-121) -Homo sapiens IGHG1*01 (CH1 (122-219), bisagra (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451)) (122-451)], (224-220')-disulfuro con la cadena ligera kappa (1'-220') [Mus musculus V-KAPPA (IGKV8-30*01 -IGKJ5*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01 (114'-220')]; (230-230'':233-233'')-bisdisulfura
Heavy chain / Chaîne lourde / Cadena pesada
EVQLQQPGPE LEKPGASVKL SCKASGYSFT DYNMNWVKQN NGESLEWIGK 50IDPYYGGPSY NQKFKDKATL TVDKSSSTAY MQLKSLTSED SAVYYCTRGG 100NRDWYFDVWG AGTTLTVSAE FASTKGPSVF PLAPSSKSTS GGTAALGCLV 150KDYFPEPVTV SWNSGALTSG VHTFPAVLQS SGLYSLSSVV TVPSSSLGTQ 200TYICNVNHKP SNTKVDKKVE PKSCDKTHTC PPCPAPELLG GPSVFLFPPK 250PKDTLMISRT PEVTCVVVDV SHEDPEVKFN WYVDGVEVHN AKTKPREEQY 300NSTYRVVSVL TVLHQDWLNG KEYKCKVSNK ALPAPIEKTI SKAKGQPREP 350QVYTLPPSRD ELTKNQVSLT CLVKGFYPSD IAVEWESNGQ PENNYKTTPP 400VLDSDGSFFL YSKLTVDKSR WQQGNVFSCS VMHEALHNHY TQKSLSLSPG 450K 451
Light chain / Chaîne légère / Cadena ligeraDIVLSQSPSS LVVSVGEKVT MSCKSSQSLL YSRNQKNYLA WYQQKPGQSP 50KVLIYWASTR ESGVPDRLTG SGSGTDFTLT ISSVKAEDLA VYYCQQYYSY 100PLTFGAGTKL ELKRTVAAPS VFIFPPSDEQ LKSGTASVVC LLNNFYPREA 150KVQWKVDNAL QSGNSQESVT EQDSKDSTYS LSSTLTLSKA DYEKHKVYAC 200EVTHQGLSSP VTKSFNRGEC 220
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 148-204 265-325 371-429 22''-96'' 148''-204'' 265''-325'' 371''-429''Intra-L 23'-94' 140'-200' 23'''-94''' 140'''-200''' Inter-H-L 224-220' 224''-220''' Inter-H-H 230-230'' 233-233''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:301, 301''
sofosbuvirum sofosbuvir propan-2-yl N-[(S)-{[(2R,3R,4R,5R)-5-(2,4-dioxo-
3,4-dihydropyrimidin-1(2H)-yl)-4-fluoro-3-hydroxy-4-methyloxolan- 2-yl]methoxy}phenoxyphosphoryl]-L-alaninate
sofosbuvir N-[(S)-{[(2R,3R,4R,5R)-5-(2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl)-4-fluoro-3-hydroxy-4-méthyloxolan- 2-yl]méthoxy}phénoxyphosphoryl]-L-alaninate de propan-2-yle
sofosbuvir N-[(S)-{[(2R,3R,4R,5R)-5-(2,4-dioxo-3,4-dihidropirimidin-1(2H)-il)- 4-fluoro-3-hidroxi-4-metiloxolan-2-il]metoxi}fenoxifosforil]-L-alaninato de propan-2-ilo
C22H29FN3O9P
N N
N
NHN
N NN
O
O

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
314
tecemotidum tecemotide human mucin-1 (carcinoma-associated mucin, episialin, CD227)-
(107-131)-peptide (sequence 40 times repeated) fusion protein with 6-N-hexadecanoyl-L-lysylglycine
técémotide mucine-1 humaine (mucine associée au carcinome, épisialine, CD227)-(107-131)-peptide (fragment présent 40 fois) protéine de fusion avec la 6-N-hexadécanoyl-L-lysylglycine
tecemotida mucina-1 humana (mucina asociada al carcinoma, episialina, CD227)-(107-131)-péptido (fragmento presente 40 veces) proteína de fusión con la 6-N-hexadecanoil-L-lisilglicina
C124H203N33O38
CO2H
NH2H
NH
H3C
O
14
Sequence / Séquence / SecuenciaSTAPPAHGVT SAPDTRPAPG STAPPKG 27
Modified residue / Résidu modifié / Resto modificado
K26
palmityl-Lys
telmapitantum telmapitant (5R,8S)-8-({(1R)-1-[3,5-bis(trifluoromethyl)phenyl]ethoxy}methyl)-
8-phenyl-1,3,7-triazaspiro[4.5]decane-2,4-dione
telmapitant (5R,8S)-8-({(1R)-1-[3,5-bis(trifluorométhyl)phényl]éthoxy}méthyl)- 8-phényl-1,3,7-triazaspiro[4.5]décane-2,4-dione
telmapitant (5R,8S)-8-({(1R)-1-[3,5-bis(trifluorometil)fenil]etoxi}metil)-8-fenil-1,3,7-triazaspiro[4.5]decano-2,4-diona
C24H23F6N3O3
O
H CH3
CF3
CF3
NH
NH
HN
O
O
tildrakizumabum # tildrakizumab immunoglobulin G1-kappa, anti-[Homo sapiens IL23A (interleukin 23
alpha subunit (p19), IL-23A)], humanized monoclonal antibody; gamma1 heavy chain (1-446) [humanized VH (Homo sapiens IGHV1-18*01 (81.60%) -(IGHD)-IGHJ4*01)) [8.8.9] (1-116) -Homo sapiens IGHG1*01 (CH1 (117-214, hinge (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimer (225-225":228-228")-bisdisulfide

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
315
tildrakizumab immunoglobuline G1-kappa, anti-[Homo sapiens IL23A (sous-unité alpha (p19) de l'interleukine 23, IL-23A)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-446) [VH humanisé (Homo sapiens IGHV1-18*01 (81.60%) -(IGHD)-IGHJ4*01)) [8.8.9] (1-116) -Homo sapiens IGHG1*01 (CH1 (117-214, charnière (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimère (225-225":228-228")-bisdisulfure
tildrakizumab inmunoglobulina G1-kappa, anti-[Homo sapiens IL23A (subunidad alfa (p19) de la interleukina 23, IL-23A)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-446) [VH humanizado (Homo sapiens IGHV1-18*01 (81.60%) -(IGHD)-IGHJ4*01)) [8.8.9] (1-116) -Homo sapiens IGHG1*01 (CH1 (117-214, bisagra (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dímero (225-225":228-228")-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QVQLVQSGAE VKKPGASVKV SCKASGYIFI TYWMTWVRQA PGQGLEWMGQ 50IFPASGSADY NEKFEGRVTM TTDTSTSTAY MELRSLRSDD TAVYYCARGG 100GGFAYWGQGT LVTVSSASTK GPSVFPLAPS SKSTSGGTAA LGCLVKDYFP 150EPVTVSWNSG ALTSGVHTFP AVLQSSGLYS LSSVVTVPSS SLGTQTYICN 200VNHKPSNTKV DKKVEPKSCD KTHTCPPCPA PELLGGPSVF LFPPKPKDTL 250MISRTPEVTC VVVDVSHEDP EVKFNWYVDG VEVHNAKTKP REEQYNSTYR 300VVSVLTVLHQ DWLNGKEYKC KVSNKALPAP IEKTISKAKG QPREPQVYTL 350PPSRDELTKN QVSLTCLVKG FYPSDIAVEW ESNGQPENNY KTTPPVLDSD 400GSFFLYSKLT VDKSRWQQGN VFSCSVMHEA LHNHYTQKSL SLSPGK 446
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVT ITCRTSENIY SYLAWYQQKP GKAPKLLIYN 50AKTLAEGVPS RFSGSGSGTD FTLTISSLQP EDFATYYCQH HYGIPFTFGQ 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H 22-96 143-199 260-320 366-424 22''-96'' 143''-199'' 260''-320'' 366''-424''Intra-L 23'-88' 134'-194' 23'''-88''' 134'''-194''' Inter-H-L 219-214' 219''-214''' Inter-H-H 225-225'' 228-228''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:296, 296''
tomicoratum tomicorat 4-{5-[(5-fluoro-2-methylphenoxy)methyl]-2,2,4-trimethyl-
1,2-dihydroquinolin-6-yl}-3-methoxyphenyl furan-2-carboxylate
tomicorat furane-2-carboxylate de 4-{5-[(5-fluoro-2-méthylphénoxy)méthyl]-2,2,4-triméthyl-1,2-dihydroquinoléin-6-yl}-3-méthoxyphényle

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
316
tomicorat furan-2-carboxilato de 4-{5-[(5-fluoro-2-metilfenoxi)metil]-
2,2,4-trimetil-1,2-dihidroquinolin-6-il}-3-metoxifenilo
C32H30FNO5
HN
H3C
H3CCH3
O
O
O
O
H3C
F
H3CO
turoctocogum alfa pegolum # turoctocog alfa pegol human coagulation factor VIII-(1-750)-(1638-1648)-peptide
compound with human coagulation factor VIIIa light chain, glycosylated and pegylated; O3.750-[α-methylpoly(oxyethylene) 5-(acetylamino)-2,5-dideoxy- D-glycero-β-D-galacto-non-2-ulopyranosylonate-(2→4)-α-D-galactopyranosyl-(1→4)-2-(acetylamino)-2-deoxy-α-D-galactopyranosyl]-des-(751-1637)-human coagulation factor VIII-(1-1648)-peptide containing 92 kDa factor VIIIa heavy chain compound with human coagulation factor VIIIa light chain glycosylated (glycoform alfa produced in CHO cells)
turoctocog alfa pégol facteur VIII de coagulation humain-(1-750)-(1638-1648)-peptide associé à la chaîne légère du facteur VIIIa de coagulation humain glycosylés et pégylés O3.750-[5-(acétylamino)-2,5-didéoxy-D-glycéro-β-D-galacto-non- 2-ulopyranosylonate de α-méthylpoly(oxyéthylène)-(2→4)-α-D-galactopyranosyl-(1→4)-2-(acétylamino)-2-déoxy-α-D-galactopyranosyl]-dès-(751-1637)-facteur VIII de coagulation humain-(1-1648)-peptide contenant la chaîne lourde de 92 kDa du factor VIIIa associé à la chaîne légère du facteur VIIIa de coagulation humain glycosylés (glycoforme alfa produit par des cellules CHO)
turoctocog alfa pegol factor VIII de coagulación humano-(1-750)-(1638-1648)-péptido asociado a la cadena ligera del factor VIIIa de coagulación humano glicosilados y pegilados; O3.750-[5-(acetilamino)-2,5-didesoxi-D-glicero-β-d-galacto-non- 2-ulopiranosilonato de α-metilpoli(oxietileno)-(2→4)-α-D-galactopiranosil-(1→4)-2-(acetlamino)-2-desoxi-α-D-galactopiranosil]-des-(751-1637)-factor VIII de coagulación humano-(1-1648)-péptido que contiene la cadena pesada de 92 kDa del factor VIIIa asociado a la cadena ligera del factor VIIIa de coagulación humano glicosilados (glicoforma alfa producido por células CHO)

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
317
O
OHNH
O
OHH2N CO2H
H
O
OHHO
O
OH
O
OH
H
OH
HO
NH
CH3
O
OH
O
OO
OCH3
n
H3C
O
Heavy chain / Chaîne lourde / Cadena pesadaATRRYYLGAV ELSWDYMQSD LGELPVDARF PPRVPKSFPF NTSVVYKKTL 50FVEFTDHLFN IAKPRPPWMG LLGPTIQAEV YDTVVITLKN MASHPVSLHA 100VGVSYWKASE GAEYDDQTSQ REKEDDKVFP GGSHTYVWQV LKENGPMASD 150PLCLTYSYLS HVDLVKDLNS GLIGALLVCR EGSLAKEKTQ TLHKFILLFA 200VFDEGKSWHS ETKNSLMQDR DAASARAWPK MHTVNGYVNR SLPGLIGCHR 250KSVYWHVIGM GTTPEVHSIF LEGHTFLVRN HRQASLEISP ITFLTAQTLL 300MDLGQFLLFC HISSHQHDGM EAYVKVDSCP EEPQLRMKNN EEAEDYDDDL 350TDSEMDVVRF DDDNSPSFIQ IRSVAKKHPK TWVHYIAAEE EDWDYAPLVL 400APDDRSYKSQ YLNNGPQRIG RKYKKVRFMA YTDETFKTRE AIQHESGILG 450PLLYGEVGDT LLIIFKNQAS RPYNIYPHGI TDVRPLYSRR LPKGVKHLKD 500FPILPGEIFK YKWTVTVEDG PTKSDPRCLT RYYSSFVNME RDLASGLIGP 550LLICYKESVD QRGNQIMSDK RNVILFSVFD ENRSWYLTEN IQRFLPNPAG 600VQLEDPEFQA SNIMHSINGY VFDSLQLSVC LHEVAYWYIL SIGAQTDFLS 650VFFSGYTFKH KMVYEDTLTL FPFSGETVFM SMENPGLWIL GCHNSDFRNR 700GMTALLKVSS CDKNTGDYYE DSYEDISAYL LSKNNAIEPR SFSQNSRHPS 750QNPPVLKRHQ R 761
Light chain / Chaîne légère / Cadena ligera EI 1650TRTTLQSDQE EIDYDDTISV EMKKEDFDIY DEDENQSPRS FQKKTRHYFI 1700AAVERLWDYG MSSSPHVLRN RAQSGSVPQF KKVVFQEFTD GSFTQPLYRG 1750ELNEHLGLLG PYIRAEVEDN IMVTFRNQAS RPYSFYSSLI SYEEDQRQGA 1800EPRKNFVKPN ETKTYFWKVQ HHMAPTKDEF DCKAWAYFSD VDLEKDVHSG 1850LIGPLLVCHT NTLNPAHGRQ VTVQEFALFF TIFDETKSWY FTENMERNCR 1900APCNIQMEDP TFKENYRFHA INGYIMDTLP GLVMAQDQRI RWYLLSMGSN 1950ENIHSIHFSG HVFTVRKKEE YKMALYNLYP GVFETVEMLP SKAGIWRVEC 2000LIGEHLHAGM STLFLVYSNK CQTPLGMASG HIRDFQITAS GQYGQWAPKL 2050ARLHYSGSIN AWSTKEPFSW IKVDLLAPMI IHGIKTQGAR QKFSSLYISQ 2100FIIMYSLDGK KWQTYRGNST GTLMVFFGNV DSSGIKHNIF NPPIIARYIR 2150LHPTHYSIRS TLRMELMGCD LNSCSMPLGM ESKAISDAQI TASSYFTNMF 2200ATWSPSKARL HLQGRSNAWR PQVNNPKEWL QVDFQKTMKV TGVTTQGVKS 2250LLTSMYVKEF LISSSQDGHQ WTLFFQNGKV KVFQGNQDSF TPVVNSLDPP 2300LLTRYLRIHP QSWVHQIALR MEVLGCEAQD LY 2332
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro153-179 248-329 528-554 630-711 1832-1858 1899-1903 2021-2169 2174-2326
Sulfated residues (Y) / Résidus sulfatés (Y) / Restos sulfatados (Y)Tyr-346 Tyr-718 Tyr-719 Tyr-723 Tyr-1664 Tyr-1680
Modified residue / Résidu modifié / Resto modificado
S750
O-(PEG-Glyc)Ser
Glycosylation sites (N) / Sites de glycosylation (N) / Posiciones de glicosilación (N)Asn-41 Asn-239 Asn-1810 Asn-2118
ulodesinum ulodesine 7-{[(3R,4R)-3-hydroxy-4-(hydroxymethyl)pyrrolidin-1-yl]methyl}-
1,5-dihydro-4H-pyrrolo[3,2-d]pyrimidin-4-one
ulodésine 7-{[(3R,4R)-3-hydroxy-4-(hydroxyméthyl)pyrrolidin-1-yl]méthyl}- 1,5-dihydro-4H-pyrrolo[3,2-d]pyrimidin-4-one
ulodesina 7-{[(3R,4R)-3-hidroxi-4-(hidroximetil)pirrolidin-1-il]metil}-1,5-dihidro-4H-pirrolo[3,2-d]pirimidin-4-ona

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
318
C12H16N4O3
N
NH
HN
O
N
OH
OH
vibegronum vibegron (6S)-N-[4-({(2S,5R)-5-[(R)-hydroxy(phenyl)methyl]pyrrolidin-
2-yl}methyl)phenyl]-4-oxo-4,6,7,8-tetrahydropyrrolo[1,2-a]pyrimidine-6-carboxamide
vibégron (6S)-N-[4-({(2S,5R)-5-[(R)-hydroxyphénylméthyl]pyrrolidin- 2-yl}méthyl)phényl]-4-oxo-4,6,7,8-tétrahydropyrrolo[1,2-a]pyrimidine-6-carboxamide
vibegrón (6S)-N-[4-({(2S,5R)-5-[(R)-hidroxi(fenil)metil]pirrolidin-2-il}metil)fenil]-4-oxo-4,6,7,8-tetrahidropirrolo[1,2-a]pirimidina-6-carboxamida
C26H28N4O3
H
N
HH
NH H N
N
OHH
O
O
voxtalisibum voxtalisib 2-amino-8-ethyl-4-methyl-6-(1H-pyrazol-3-yl)pyrido[2,3-d]pyrimidin-
7(8H)-one
voxtalisib 2-amino-8-éthyl-4-méthyl-6-(1H-pyrazol-3-yl)pyrido[2,3-d]pyrimidin-7(8H)-one
voxtalisib 2-amino-8-etil-4-metil-6-(1H-pirazol-3-il)pirido[2,3-d]pirimidin- 7(8H)-ona
C13H14N6O
N
N
NH2N
CH3
O
H3C
NNH
zamicastatum zamicastat 5-(2-(benzylamino)ethyl)-1-[(3R)-6,8-difluoro-3,4-dihydro-
2H-1-benzopyran-3-yl)-1,3-dihydro-2H-imidazole-2-thione
zamicastat 5-[2-(benzylamino)éthyl]-1-[(3R)-6,8-difluoro-3,4-dihydro- 2H-1-benzopyran-3-yl]-1,3-dihydro-2H-imidazole-2-thione
zamicastat 5-(2-(bencilamino)etil)-1-[(3R)-6,8-difluoro-3,4-dihidro- 2H-1-benzopiran-3-il)-1,3-dihidro-2H-imidazol-2-tiona

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
319
C21H21F2N3OS
O
NNH
SF
FH
NH
# Electronic structure available on Mednet: http://mednet.who.int/ # Structure électronique disponible sur Mednet: http://mednet.who.int/ # Estructura electrónica disponible en Mednet: http://mednet.who.int/ * http://www.who.int/entity/medicines/services/inn/Radical_Book_2012.pdf

Recommended INN: List 70 WHO Drug Information Vol. 27, No. 3, 2013
320
AMENDMENTS TO PREVIOUS LISTS MODIFICATIONS APPORTÉES AUX LISTES ANTÉRIEURES
MODIFICACIONES A LAS LISTAS ANTERIORES Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 36 (Información Farmacéutica OMS, Vol. 10, No. 3, 1996) p. 147 suprimáse insertese fasidotril fasidotrilo Recommended International Nonproprietary Names (Rec. INN): List 58 Dénominations communes internationales recommandées (DCI Rec.): Liste 58 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 58 (WHO Drug Information, Vol. 21, No. 3, 2007) p. 255 methylnaltrexonii bromidum methylnaltrexone bromide replace the chemical name by the following one
(17RS)-17-(cyclopropylmethyl)-4,5-epoxy-3,14-dihydroxy-17-methyl-6-oxo- 14-morphinanium bromide
Recommended International Nonproprietary Names (Rec. INN): List 62 Dénominations communes internationales recommendées (DCI Rec.): Liste 62 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 62 (WHO Drug Information, Vol. 23, No. 3, 2009) p. 248 fidaxomicinum fidaxomicin replace the chemical name by the following one
fidaxomicina sustitúyase el nombre químico por el siguiente
(3E,5E,8S,9E,11S,12R,13E,15E,18S)-3-{[(6-deoxy-4-O-(3,5-dichloro-2-ethyl-4,6-dihydroxybenzoyl)-2-O-methyl-β-D-mannopyranosyl)oxy]methyl}-12-{[6-deoxy-5-C-methyl-4-O-(2-methylpropanoyl)-β-D-lyxo-hexopyranosyl]oxy}-11-ethyl-8-hydroxy-18-[(1R)-1-hydroxyethyl]-9,13,15-trimethyloxacyclooctadeca-3,5,9,13,15-pentaen-2-one
(3E,5E,8S,9E,11S,12R,13E,15E,18S)-3-{[(6-desoxi-4-O-(3,5-dicloro-2-etil-4,6-dihidroxibenzoil)-2-O-metil-β-D-manopiranosil)oxi]metil}-12-{[6-desoxi-5-C-metil-4-O-(2-metilpropanoil)-β-D-lixo-hexopiranosil]oxi}-11-etil-8-hidroxi-18-[(1R)-1-hidroxietil]-9,13,15-trimetiloxaciclooctadeca-3,5,9,13,15-pentaen-2-ona

WHO Drug Information Vol. 27, No. 3, 2013 Recommended INN: List 70
321
Procedure and Guiding Principles / Procédure et Directives / Procedimientos y principios generales
The text of the Procedures for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances and General Principles for Guidance in Devising International Nonproprietary Names for Pharmaceutical Substances will be reproduced in proposed INN lists only.
Les textes de la Procédure à suivre en vue du choix de dénominations communes internationales recommandées pour les substances pharmaceutiques et des Directives générales pour la formation de dénominations communes internationales applicables aux substances pharmaceutiques seront publiés seulement dans les listes des DCI proposées.
El texto de los Procedimientos de selección de denominaciones comunes internacionales recomendadas para las sustancias farmacéuticas y de los Principios generales de orientación para formar denominaciones comunes internacionales para sustancias farmacéuticas aparece solamente en las listas de DCI propuestas.