Which symptoms can distinguish between subjective cognitive impairment (SCI) and mild cognitive...
5
Which symptoms can distinguish between subjective cognitive impairment (SCI) and mild cognitive impairment (MCI)? Bora Yoon a , Yong S. Shim b , Yun-Jeong Hong c , Yong-Duk Kim a , Kee Ook Lee a , Sang-Jun Na a , Dong-Won Yang c, * a Department of Neurology, Konyang University College of Medicine, 685 Gasuwon-dong, Seo-gu, Daejeon 302-718, Republic of Korea b Department of Neurology, College of Medicine, The Catholic University of Korea, Bucheon St. Mary’s Hospital, 2 Sosa-dong, Wonmi-gu, Bucheon 420-717, Republic of Korea c Department of Neurology, College of Medicine, The Catholic University of Korea, Seoul St. Mary’s Hospital, 505 Banpo-dong, Seocho-gu, Seoul 137-040, Republic of Korea 1. Introduction It is known that MCI is a prodromal state of dementia, which needs continuous proper management. The annual conversion rate to probable AD from MCI is around 10–15% per year compared with 1–2% per year in the general population (Petersen et al., 1999). In addition to MCI, SCI recently has been considered as a potential pre-MCI stage or a risk factor for dementia. SCI is fairly common in elderly people; however, its clinical significance is still undetermined. Some studies suggest that SCI is associated with depression (Bolla et al., 1991), anxiety (Clarnette et al., 2001), certain personality traits (Pearman and Storandt, 2004), or stress (Kim et al., 2003; Zandi, 2004). In contrast, other recent studies have found that SCI is indeed predictive of an unfavorable cognitive outcome and is a risk factor for dementia (Gerrlings et al., 1999; Jorm et al., 2001; Treves et al., 2005; Jessen et al., 2010). Jonker et al. (2000) have confirmed that memory complaints in elderly people are not innocent age-related phenomena or depression, but should be taken seriously as a possible early sign of dementia. In addition, a study that has observed outcomes over 7 years in healthy adults with and without SCI has revealed increased decline and accelerated failure time in SCI (Reisberg et al., 2010). Based on imaging studies in SCI, patients with SCI tend to show smaller hippocampal volume (Van der Flier et al., 2004), more cerebral white matter lesions (De Groot et al., 2001), and significantly increased Pittsburgh compound B (PIB) retention in the cortical areas on 11C-PIB positron emission tomography (Rodda et al., 2010). This suggests that SCI reflects cognitive decline due to structural and molecular brain changes. Research on biomarkers has demonstrated that AD profile cerebrospinal fluid findings are more common in SCI patients than in healthy controls, suggesting that patients with SCI might be in the earliest stages of AD (Visser et al., 2009). Given these findings, it would be useful to select patients with SCI who have characteristics that predict MCI, as such identifica- tion would allow for more economical and effective early treatment. In clinical situations, informant questionnaires are widely used. Both SCI and MCI represent very early stages of cognitive decline; therefore, informants’ questionnaires have greater discriminatory power than simple screening tests, such Archives of Gerontology and Geriatrics 54 (2012) 325–329 ARTICLE INFO Article history: Received 15 November 2010 Received in revised form 5 April 2011 Accepted 21 April 2011 Available online 21 June 2011 Keywords: Subjective cognitive impairment Subjective memory impairment Mild cognitive impairment Instrumental activities of daily living ABSTRACT The SCI, the MCI, and the Alzheimer’s disease (AD) are on a spectrum of disease progression; therefore, identification of the earliest signs of cognitive deterioration is becoming a crucial issue. The goal of this study was to examine symptom characteristics and distinguish predictive symptoms in patients with MCI compared with SCI, using caregiver questionnaires. We assessed the Korean Dementia Screening Questionnaire (KDSQ) and Seoul Instrumental activities of Daily Living (S-IADL) of 344 subjects with SCI and 697 with MCI. Multivariate logistic regression analyses were conducted after adjusting for age, sex, and educational status. Common and rare symptoms were similar between the SCI and MCI groups. The most distinguishing features of KDSQ were ‘Finds it hard to go somewhere on his/her own using public transportation’ (odds ratio = OR = 4.56, p < 0.0001), ‘Has difficulty in operating appliances’ (OR = 2.47, p = 0.001), and ‘Keeps repeating the same question’ (OR = 2.03, p < 0.0001). In S-IADL, the most outstanding features were ‘using household appliances’ (OR = 3.99, p < 0.0001), ‘taking medication’ (OR = 2.38, p = 0.01), and ‘using public transportation’ (OR = 1.94, p = 0.04). The dysfunction in ‘using household appliance’ and ‘using public transportation’ reflect the possibility of MCI rather than SCI. Therefore, it is suggested that these symptoms also have a discriminative and predictive power in identifying SCI. ß 2011 Elsevier Ireland Ltd. All rights reserved. * Corresponding author. Tel.: +82 2 2258 6077; fax: +82 2 599 9686. E-mail address: [email protected] (D.-W. Yang). Contents lists available at ScienceDirect Archives of Gerontology and Geriatrics journal homepage: www.elsevier.com/locate/archger 0167-4943/$ – see front matter ß 2011 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.archger.2011.04.027
Transcript of Which symptoms can distinguish between subjective cognitive impairment (SCI) and mild cognitive...

Archives of Gerontology and Geriatrics 54 (2012) 325–329
Contents lists available at ScienceDirect
Archives of Gerontology and Geriatrics
journa l homepage: www.e lsev ier .com/ locate /archger
Which symptoms can distinguish between subjective cognitive impairment (SCI)and mild cognitive impairment (MCI)?
Bora Yoon a, Yong S. Shim b, Yun-Jeong Hong c, Yong-Duk Kim a, Kee Ook Lee a, Sang-Jun Na a,Dong-Won Yang c,*a Department of Neurology, Konyang University College of Medicine, 685 Gasuwon-dong, Seo-gu, Daejeon 302-718, Republic of Koreab Department of Neurology, College of Medicine, The Catholic University of Korea, Bucheon St. Mary’s Hospital, 2 Sosa-dong, Wonmi-gu, Bucheon 420-717, Republic of Koreac Department of Neurology, College of Medicine, The Catholic University of Korea, Seoul St. Mary’s Hospital, 505 Banpo-dong, Seocho-gu, Seoul 137-040, Republic of Korea
A R T I C L E I N F O
Article history:
Received 15 November 2010
Received in revised form 5 April 2011
Accepted 21 April 2011
Available online 21 June 2011
Keywords:
Subjective cognitive impairment
Subjective memory impairment
Mild cognitive impairment
Instrumental activities of daily living
A B S T R A C T
The SCI, the MCI, and the Alzheimer’s disease (AD) are on a spectrum of disease progression; therefore,
identification of the earliest signs of cognitive deterioration is becoming a crucial issue. The goal of this
study was to examine symptom characteristics and distinguish predictive symptoms in patients with
MCI compared with SCI, using caregiver questionnaires. We assessed the Korean Dementia Screening
Questionnaire (KDSQ) and Seoul Instrumental activities of Daily Living (S-IADL) of 344 subjects with SCI
and 697 with MCI. Multivariate logistic regression analyses were conducted after adjusting for age, sex,
and educational status. Common and rare symptoms were similar between the SCI and MCI groups. The
most distinguishing features of KDSQ were ‘Finds it hard to go somewhere on his/her own using public
transportation’ (odds ratio = OR = 4.56, p < 0.0001), ‘Has difficulty in operating appliances’ (OR = 2.47,
p = 0.001), and ‘Keeps repeating the same question’ (OR = 2.03, p < 0.0001). In S-IADL, the most
outstanding features were ‘using household appliances’ (OR = 3.99, p < 0.0001), ‘taking medication’
(OR = 2.38, p = 0.01), and ‘using public transportation’ (OR = 1.94, p = 0.04). The dysfunction in ‘using
household appliance’ and ‘using public transportation’ reflect the possibility of MCI rather than SCI.
Therefore, it is suggested that these symptoms also have a discriminative and predictive power in
identifying SCI.
� 2011 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
It is known that MCI is a prodromal state of dementia, whichneeds continuous proper management. The annual conversion rateto probable AD from MCI is around 10–15% per year compared with1–2% per year in the general population (Petersen et al., 1999). Inaddition to MCI, SCI recently has been considered as a potentialpre-MCI stage or a risk factor for dementia.
SCI is fairly common in elderly people; however, its clinicalsignificance is still undetermined. Some studies suggest that SCI isassociated with depression (Bolla et al., 1991), anxiety (Clarnetteet al., 2001), certain personality traits (Pearman and Storandt,2004), or stress (Kim et al., 2003; Zandi, 2004). In contrast, otherrecent studies have found that SCI is indeed predictive of anunfavorable cognitive outcome and is a risk factor for dementia(Gerrlings et al., 1999; Jorm et al., 2001; Treves et al., 2005; Jessenet al., 2010). Jonker et al. (2000) have confirmed that memorycomplaints in elderly people are not innocent age-related
* Corresponding author. Tel.: +82 2 2258 6077; fax: +82 2 599 9686.
E-mail address: [email protected] (D.-W. Yang).
0167-4943/$ – see front matter � 2011 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.archger.2011.04.027
phenomena or depression, but should be taken seriously as apossible early sign of dementia. In addition, a study that hasobserved outcomes over 7 years in healthy adults with and withoutSCI has revealed increased decline and accelerated failure time inSCI (Reisberg et al., 2010). Based on imaging studies in SCI, patientswith SCI tend to show smaller hippocampal volume (Van der Flieret al., 2004), more cerebral white matter lesions (De Groot et al.,2001), and significantly increased Pittsburgh compound B (PIB)retention in the cortical areas on 11C-PIB positron emissiontomography (Rodda et al., 2010). This suggests that SCI reflectscognitive decline due to structural and molecular brain changes.Research on biomarkers has demonstrated that AD profilecerebrospinal fluid findings are more common in SCI patientsthan in healthy controls, suggesting that patients with SCI might bein the earliest stages of AD (Visser et al., 2009).
Given these findings, it would be useful to select patients withSCI who have characteristics that predict MCI, as such identifica-tion would allow for more economical and effective earlytreatment. In clinical situations, informant questionnaires arewidely used. Both SCI and MCI represent very early stages ofcognitive decline; therefore, informants’ questionnaires havegreater discriminatory power than simple screening tests, such

B. Yoon et al. / Archives of Gerontology and Geriatrics 54 (2012) 325–329326
as the mini-mental state examination (MMSE), or than expensivestructural imaging techniques.
Therefore, we sought to identify discriminative and predictivecognitive performances or activities of daily living that distinguishbetween SCI and MCI. The purpose of the present study was toexamine these by using informant-based questionnaires, includingthe KDSQ (Yang et al., 2002), the S-IADL (Ku et al., 2004), andBarthel Activities of Daily Living (BADL) (Mahoney and Barthel,1965).
2. Subjects and methods
Three hundred forty-four SCI and 697 MCI patients wererecruited from 43 dementia clinics of university-affiliated hospi-tals in Korea from November 2005 to March 2009. The study wasperformed as part of the nationwide multicenter study fordementia: the Clinical Research Center for Dementia of SouthKorea (CREDOS) study. This study was approved by the local ethicscommittee, and informed consent was obtained from all subjects.The inclusion criteria for SCI were as follows: (1) sustainedsubjective memory complaints; (2) normal general cognition(within �1 S.D. of age- and education-adjusted norms on theKorean version of the MMSE (K-MMSE) (Kang et al., 1997) and ascore higher than 26); (3) intact activities of daily living (ADL); and(4) no abnormality (within �1 S.D. of age- and education-adjustednorms) on a comprehensive neuropsychological battery. Wegenerally adhered to the diagnostic criteria for MCI defined byPetersen et al. (2001) and Winblad et al. (2004). The inclusioncriteria for MCI were as follows: (1) patients with memorycomplaints; (2) patients presenting with a total K-MMSE scorewithin 1.0 S.D. below age- and education-adjusted norms on the K-MMSE; (3) normal functional activities (informant’s report ofintact ADL); (4) cognitive impairment (at least 1.5 S.D. below age-and education-adjusted norms) in �1 domain (executive function,memory, language, or visuospatial) on standard neuropsychologi-cal tests; (5) clinical dementia rating (CDR) (Morris, 1993) of 0.5;and (6) not demented according to DSM-IV-TR criteria. Allparticipants were subjected to conventional brain magneticresonance imaging (MRI) to detect organic brain lesions thataffected cognitive impairment.
2.1. Cognitive and functional performance assessments
The questionnaires were filled in by informants after theyreceived appropriate instructions, while patients were undergoingneuropsychological assessment. The informant-based KDSQ wasadministered to verify deterioration of cognitive ability from apreviously higher level of functioning (Table 2). Basic ADL taskswere assessed with the BADL, and IADL tasks were assessed byusing the S-IADL (Table 3).
The KDSQ consists of 15 items that reflect various aspects ofcognitive decline. Five items of the KDSQ were designed to assessglobal memory function (does not know the date or day; cannotfind things he or she previously put down; keeps repeating thesame questions; forgets appointments; comes back without thingshe or she had intended to pick up). Five other items were designedto assess other cognitive functions and behavior. These included:mumbles because names of people or things slip the mind; keepsasking questions because he/she does not get to the point; gets lostor goes astray; has difficulty with financial affairs (e.g., paying billsor calculating change), his/her personality has changed. Anotherfive items were designed to assess IADL. These included hasdifficulty in operating appliances (e.g., washing machine, electriccooker, or cultivator, etc.); cannot keep rooms or a house clean anylonger; does not wear outfits that fit the time, place, and occasion;finds it hard to go somewhere on his/her own using public
transportation (except for the case of physical disability such asarthritis); refuses to change dirty underwear or clothes. All of theitems on KDSQ are scored on a 3-point scale, ranging from 0 to 2,with higher scores indicating poorer function and more frequentevents. S-IADL is a caregiver-administered instrument designed tomeasure IADL. The S-IADL consists of 15 items: using thetelephone; shopping; preparing food/cooking; household chores;using public transportation; going out (short distance); takingmedication; managing finances; grooming; using householdappliances; managing belongings; securing a door; keepingappointments; talking about recurrent events; and leisure/hobbies. All of the items in S-IADL are scored on a 4-point scale,ranging from 0 to 3, with 0 indicating normal, and higher scoresindicating poorer performance on IADL. All KDSQ and S-IADL itemswere carefully reviewed by experts in consensus meetings, werevalidated for the general Korean population, and are widely used inKorea.
Cognitive functioning was assessed by neuropsychologistsusing an extensive cognitive battery (Seoul NeuropsychologicalScreening Battery = SNSB) (Kang, 1998), which includes fivespecific cognitive domains. It tests attention by digit span andletter cancellation; visuospatial function by the copy score of theRey–Osterrieth Complex Figure (ROCF) test (Chey, 2007); languagefunction by the Korean version of the Boston Naming Test (Kim andNa, 1997); verbal memory by the Seoul Verbal Learning Test (SVLT;three free recall trials of 12 words, and a 20-min delayed recall trialof the same 12 items, and a recognition test) (Kang, 1998);visuospatial memory by delayed recall of the ROCF; and frontallobe function by contrasting program, go-no go, fist-edge-palm,Luria loop, Controlled Oral Word Association Test (Lee et al., 2000),and Stroop letter/color reading test. The Korean version of theGeriatric Depression Scale (GDS) was also administered for theevaluation of concomitant depressive symptoms (Cho et al., 1999).
2.2. Statistical analysis
The chi-square and independent t-tests were used to comparedemographic characteristics between SCI and MCI patients. Thefrequencies of items on the KDSQ, S-IADL, and BADL werecompared between SCI and MCI patients using the chi-squaretest. We estimated adjusted OR and the corresponding 95%confidence interval (95% CI) for a 1-point increase in the score(from absence to presence of dysfunction) for each item in theKDSQ, S-IADL, and BADL for SCI and MCI patients. We usedmultivariate logistic regression analysis (conversion to MCI asdependent variable) to adjust for age (continuous variable), sex,and educational status (years of education as a continuousvariable). We quantified the magnitude of the association betweenMCI and a specific symptom, as well as observed the independentpredictive ability of the KDSQ, S-IADL, and BADL variables, bycalculating the adjusted OR and corresponding 95% CI. Groupstatistical analysis was performed using SPSS for Windows ver.12.0 (SPSS, Chicago, IL, USA). The significance level was set atp < 0.05.
3. Results
3.1. Baseline characteristics of participants
Table 1 shows the baseline characteristics of the studypopulation. The SCI group included more women and had longermean disease duration compared with the MCI group. However,age, education level, and family history of dementia or stroke didnot differ between the two groups. The risk factors forcerebrovascular disease, including diabetes mellitus, hyperten-sion, and heart disease, were significantly more frequent in the MCI
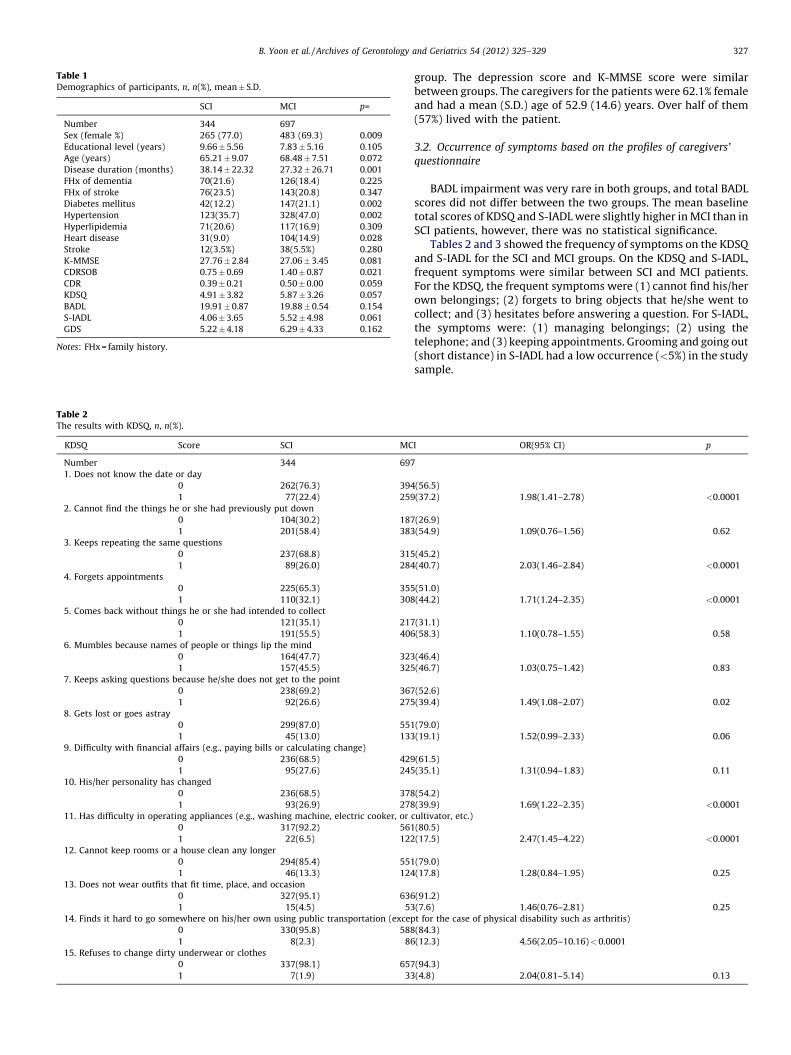
Table 1Demographics of participants, n, n(%), mean� S.D.
SCI MCI p=
Number 344 697
Sex (female %) 265 (77.0) 483 (69.3) 0.009
Educational level (years) 9.66�5.56 7.83�5.16 0.105
Age (years) 65.21�9.07 68.48�7.51 0.072
Disease duration (months) 38.14�22.32 27.32�26.71 0.001
FHx of dementia 70(21.6) 126(18.4) 0.225
FHx of stroke 76(23.5) 143(20.8) 0.347
Diabetes mellitus 42(12.2) 147(21.1) 0.002
Hypertension 123(35.7) 328(47.0) 0.002
Hyperlipidemia 71(20.6) 117(16.9) 0.309
Heart disease 31(9.0) 104(14.9) 0.028
Stroke 12(3.5%) 38(5.5%) 0.280
K-MMSE 27.76�2.84 27.06�3.45 0.081
CDRSOB 0.75� 0.69 1.40� 0.87 0.021
CDR 0.39� 0.21 0.50� 0.00 0.059
KDSQ 4.91�3.82 5.87�3.26 0.057
BADL 19.91�0.87 19.88�0.54 0.154
S-IADL 4.06�3.65 5.52�4.98 0.061
GDS 5.22�4.18 6.29�4.33 0.162
Notes: FHx = family history.
Table 2The results with KDSQ, n, n(%).
KDSQ Score SCI MC
Number 344 697
1. Does not know the date or day
0 262(76.3) 394
1 77(22.4) 259
2. Cannot find the things he or she had previously put down
0 104(30.2) 187
1 201(58.4) 383
3. Keeps repeating the same questions
0 237(68.8) 315
1 89(26.0) 284
4. Forgets appointments
0 225(65.3) 355
1 110(32.1) 308
5. Comes back without things he or she had intended to collect
0 121(35.1) 217
1 191(55.5) 406
6. Mumbles because names of people or things lip the mind
0 164(47.7) 323
1 157(45.5) 325
7. Keeps asking questions because he/she does not get to the point
0 238(69.2) 367
1 92(26.6) 275
8. Gets lost or goes astray
0 299(87.0) 551
1 45(13.0) 133
9. Difficulty with financial affairs (e.g., paying bills or calculating change)
0 236(68.5) 429
1 95(27.6) 245
10. His/her personality has changed
0 236(68.5) 378
1 93(26.9) 278
11. Has difficulty in operating appliances (e.g., washing machine, electric cooker, or
0 317(92.2) 561
1 22(6.5) 122
12. Cannot keep rooms or a house clean any longer
0 294(85.4) 551
1 46(13.3) 124
13. Does not wear outfits that fit time, place, and occasion
0 327(95.1) 636
1 15(4.5) 53
14. Finds it hard to go somewhere on his/her own using public transportation (excep
0 330(95.8) 588
1 8(2.3) 86
15. Refuses to change dirty underwear or clothes
0 337(98.1) 657
1 7(1.9) 33
B. Yoon et al. / Archives of Gerontology and Geriatrics 54 (2012) 325–329 327
group. The depression score and K-MMSE score were similarbetween groups. The caregivers for the patients were 62.1% femaleand had a mean (S.D.) age of 52.9 (14.6) years. Over half of them(57%) lived with the patient.
3.2. Occurrence of symptoms based on the profiles of caregivers’
questionnaire
BADL impairment was very rare in both groups, and total BADLscores did not differ between the two groups. The mean baselinetotal scores of KDSQ and S-IADL were slightly higher in MCI than inSCI patients, however, there was no statistical significance.
Tables 2 and 3 showed the frequency of symptoms on the KDSQand S-IADL for the SCI and MCI groups. On the KDSQ and S-IADL,frequent symptoms were similar between SCI and MCI patients.For the KDSQ, the frequent symptoms were (1) cannot find his/herown belongings; (2) forgets to bring objects that he/she went tocollect; and (3) hesitates before answering a question. For S-IADL,the symptoms were: (1) managing belongings; (2) using thetelephone; and (3) keeping appointments. Grooming and going out(short distance) in S-IADL had a low occurrence (<5%) in the studysample.
I OR(95% CI) p
(56.5)
(37.2) 1.98(1.41–2.78) <0.0001
(26.9)
(54.9) 1.09(0.76–1.56) 0.62
(45.2)
(40.7) 2.03(1.46–2.84) <0.0001
(51.0)
(44.2) 1.71(1.24–2.35) <0.0001
(31.1)
(58.3) 1.10(0.78–1.55) 0.58
(46.4)
(46.7) 1.03(0.75–1.42) 0.83
(52.6)
(39.4) 1.49(1.08–2.07) 0.02
(79.0)
(19.1) 1.52(0.99–2.33) 0.06
(61.5)
(35.1) 1.31(0.94–1.83) 0.11
(54.2)
(39.9) 1.69(1.22–2.35) <0.0001
cultivator, etc.)
(80.5)
(17.5) 2.47(1.45–4.22) <0.0001
(79.0)
(17.8) 1.28(0.84–1.95) 0.25
(91.2)
(7.6) 1.46(0.76–2.81) 0.25
t for the case of physical disability such as arthritis)
(84.3)
(12.3) 4.56(2.05–10.16)<0.0001
(94.3)
(4.8) 2.04(0.81–5.14) 0.13

Table 3S-IADL results, n, n(%).
KDSQ Score SCI MCI OR(95% CI) p
Number 344 697
1. Using the telephone
0 271(78.7) 440(63.1)
1 73(21.3) 247(35.5) 1.52(1.04–22.23) 0.03
2. Shopping
0 334(97.1) 636(91.2)
1 8(2.2) 38(5.4) 1.71(0.70–4.20) 0.24
3. Preparing food/cooking
0 263(76.5) 457(65.5)
1 36(10.5) 77(11.0) 1.19(0.71–2.00) 0.51
4. Household chores
0 292(84.8) 524(75.2)
1 32(9.4) 93(13.4) 1.39(0.80–2.40) 0.24
5. Using public transportation
0 317(92.1) 565(81.1)
1 20(5.8) 88(12.6) 1.94(1.03–3.66) 0.04
6. Going out (short distance)
0 333(96.8) 648(93.0)
1 8(2.2) 29(4.1) 1.04(0.41–2.64) 0.94
7. Taking medication
0 317(92.1) 564(80.9)
1 16(4.7) 85(12.2) 2.38(1.26–4.52) 0.01
8. Managing finances
0 298(86.6) 512(73.4)
1 30(8.7) 114(16.3) 1.65(1.00–2.74) 0.05
9. Grooming
0 344(100) 682(97.9)
1 0(0.0) 13(1.8) Not calculated
10. Using household appliances
0 333(96.8) 606(86.9)
1 9(2.5) 77(11.0) 3.99(1.69–9.46) <0.0001
11. Managing belongings
0 217(63.2) 367(52.6)
1 106(30.7) 249(35.7) 1.35(0.96–1.90) 0.09
12. Securing a door
0 332(96.4) 642(92.1)
1 9(2.5) 36(5.1) 1.53(0.65–3.58) 0.33
13. Keeping appointments
0 269(78.3) 420(60.2)
1 65(18.8) 227(32.5) 1.91(1.32–2.76) <0.0001
14. Talking about recent events
0 261(75.8) 399(57.3)
1 61(17.7) 208(29.8) 1.90(1.30–2.78) <0.0001
15. Leisure/hobbies
0 237(69.0) 384(55.1)
1 53(15.5) 151(21.6) 1.71(1.11–2.64) 0.02
B. Yoon et al. / Archives of Gerontology and Geriatrics 54 (2012) 325–329328
3.3. Likelihood of MCI patients exhibiting cognitive symptoms
compared with SCI
Multivariate logistic regression analyses were conducted tocompare the odds of items of KDSQ and S-IADL in MCI comparedwith SCI patients. Owing to the low prevalence of grooming andgoing out (short distance), we were unable to estimate accuratelythe OR for these two symptoms; thus, we focused the analysis onthe symptoms with higher occurrence.
On the KDSQ, MCI patients, compared with SCI patients, had anincreased incidence of the following: (1) finds it hard to gosomewhere on his/her own using public transportation (OR = 4.56,95% CI = 2.05–10.16, p < 0.0001); (2) has difficulty in operatingappliances (e.g., washing machine, electric cooker, or cultivator)(OR = 2.47, 95% CI = 1.45–4.22, p < 0.0001); and (3) keeps repeat-ing the same question (OR = 2.03, 95% CI = 1.46–2.33, p < 0.0001).
On the S-IADL, MCI patients, compared with SCI patients,showed a higher OR of exhibiting difficulties with (1) usinghousehold appliances (OR = 3.99, 95% CI = 1.69–9.46, p < 0.0001);(2) taking medication (OR = 2.38, 95% CI = 1.26–4.52, p = 0.01); and(3) using public transportation (OR = 1.94, 95% CI = 1.03–3.66,p = 0.04). The results of all logistic regression analyses were
generally similar in the crude and adjusted analyses. There were norelevant differences in any other symptoms in BADL.
4. Discussion
We reported differences in cognitive symptoms and functionalimpairment of IADL in 344 subjects with SCI and 697 with MCI,based on caregivers’ questionnaires. We identified that relativelyfrequent symptoms were consistent in SCI and MCI patients. Afteradjusting for age, sex, and educational level, the most distinguish-ing features between MCI and SCI patients were ‘using householdappliances’, ‘taking medication’ and ‘using public transportation’on the S-IADL, and ‘using public transportation’, ‘appliances’ and‘repeating the same questions’ on the KDSQ. S-IADL resultscorresponded well with those of earlier studies. Perneczky et al.(2006) concluded that ADL tasks that require memory and complexreasoning are most affected in individuals with MCI. In otherstudies, the four specific items (i.e., telephone, transport, medica-tion, and finances) were not only most highly associated withcognitive performance, but were also suggested as strongpredictors of progression to dementia in MCI patients, with theconversion rate being almost four times higher when a restriction

B. Yoon et al. / Archives of Gerontology and Geriatrics 54 (2012) 325–329 329
in completing IADL tasks was reported (Barberger-Gateau et al., 1993,1999; Kim et al., 2009). One recent study identified ‘using householdappliances’ instead of ‘responsibility for own medication’ but theother three items were the same as those in previous studies (Kimet al., 2009). These results imply that the IADL restrictions inthemselves have an additional prognostic value for subsequentdementia, possibly by capturing early deficits experienced in real life,particularly in the executive domain. They could also contribute to anoperational definition of MCI as a predictor of dementia (Peres et al.,2006). We focused on comparing SCI and MCI; therefore, it isinappropriate to compare our results directly with those of previousstudies. However, in view of a spectrum of disease progression, twoitems that are in common to KDSQ and S-IADL, namely, ‘using publictransportation’ and ‘operating appliances’ might be considered aspredictors of progression to MCI in SCI. In other words, although thetotal scores on KDSQ and S-IADL in themselves are not a powerfuldiscriminator of SCI and MCI, each item could be used as an additionaland supportive measure prior to detailed comprehensive neuropsy-chological tests. If subjects who complain of memory impairmenthave additional impairment in the areas of operating appliances andusing public transportation, it is likely that they have MCI rather thanSCI. Nevertheless, we need to be careful not to jump to hastyconclusions, as no longitudinal study has examined this matter.
There are several limitations to the present study. First, it was across-sectional study. Second, our study was performed withoutdividing MCI into subtypes. However, the proportion of non-amnestic MCI is quite small, and this study included a largenumber of participants. Future studies that divide participantsaccording to MCI subtypes, as well as further research to confirmthe predictive values in follow-up are needed. Despite theselimitations, this is believed to be the first study to offer a moredetailed and quantified investigation based on widely usedquestionnaires to characterize differences between SCI and MCI.
Taken together, we suggest that the two variables frominformant reports (operating appliances and using public trans-portation) might have a discriminative and predictive power in SCI,as well as acting as points of differentiation between SCI and MCI. Aprospective follow-up of our patients will clarify whether thosewith SCI who show impairment in these two areas are at greaterrisk of developing MCI and AD.
Conflict of interest statement
None.
Acknowledgements
This study was supported by a grant of the Korea HealthcareTechnology R&D Project, Ministry for Health, Welfare & FamilyAffairs, Republic of Korea (A050079).
References
Barberger-Gateau, P., Dartigues, J.F., Letenneur, L., 1993. Four instrumental activi-ties of daily living score as a predictor of one-year incident dementia. AgeAgeing 22, 457–463.
Barberger-Gateau, P., Fabrigoule, C., Helmer, C., Rouch, I., Dartigues, J.F., 1999.Functional impairment in instrumental activities of daily living: an earlyclinical sign of dementia. J. Am. Geriatr. Soc. 47, 456–462.
Bolla, K.I., Lindgren, K.N., Bonaccorsy, C., Bleecker, M.L., 1991. Memory complaintsin older adults. Fact or fiction? Arch. Neurol. 48, 61–64.
Chey, J., 2007. Elderly Memory Disorder Scale. Hakjisa, Seoul.Cho, M., Bae, J.N., Suh, G.H., Hahm, B.J., Kim, J.K., Lee, D.W., Kang, M.H., 1999.
Validation of geriatric depression scale, Korean version (GDS) in the assessmentof DSM-III-R major depression. J. Korean Neuropsychiatr. Assoc. 38, 48–63.
Clarnette, R.M., Almeida, O.P., Forstl, H., Paton, A., Martins, R.N., 2001. Clinicalcharacteristics of individuals with subjective memory loss in WesternAustralia: results from a cross-sectional survey. Int. J. Geriatr. Psychiatry 16,168–174.
De Groot, J.C., De Leeuw, F.E., Oudkerk, M., Hofman, A., Jolles, J., Breteler, M.M., 2001.Cerebral white matter lesions and subjective cognitive dysfunction: the Rot-terdam Scan Study. Neurology 56, 1539–1545.
Gerrlings, M.I., Honker, C., Bouter, L.M., Ader, H.J., Schmand, B., 1999. Associationbetween memory complaints and incident Alzheimer’s disease in elderlypeople with normal baseline cognition. Am. J. Psychiatry 156, 531–537.
Jessen, F., Wiese, B., Bachmann, C., Eifflaender-Gorfer, S., Haller, F., Kolsch, H., Luck,T., Mosch, E., van den Bussche, H., Wagner, M., Wollny, A., Zimmermann, T.,Pentzet, M., Riedel-Heller, S.G., Romberg, H.P., Weyerer, S., Kaduszkiewicz, H.,Maier, W., Bickel, H., 2010. German Study on Aging Cognition and Dementia inPrimary Care Patients Study Group Prediction of dementia by subjectivememory impairment: effects of severity and temporal association with cogni-tive impairment. Arch. Gen. Psychiatry 67, 414–422.
Jonker, C., Geerlings, M.I., Schmand, B., 2000. Are memory complaints predictive fordementia? A review of clinical and population-based studies. Int. J. Geriatr.Psychiatry 15, 983–991.
Jorm, A.F., Christensen, H., Korten, A.E., Jacomb, P.A., Henderson, A.S., 2001. Memorycomplaints as a precursor of memory impairment in older people: a longitudi-nal analysis over 7–8 years. Psychol. Med. 31, 441–449.
Kang, Y., 1998. Samsung Neuropsychological Screening Battery. Korean DementiaAssociation, Seoul.
Kang, Y.W., Na, D.L., Hahn, S.H., 1997. A validity study on the Korean Mini-MentalState Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 15,300–307.
Kim, H., Na, D.L., 1997. Korean-Boston Naming Test. Hakjisa, Seoul.Kim, J.M., Stewart, R., Shin, I.S., Choi, S.K., Yoon, J.S., 2003. Subjective memory
impairment, cognitive function and depression—a community study in olderKoreans. Dement. Geriatr. Cogn. Disord. 15, 218–225.
Kim, K.R., Lee, K.S., Cheong, H.K., Eom, J.S., Oh, B.H., Hong, C.H., 2009. Characteristicprofiles of instrumental activities of daily living in different subtypes of mildcognitive impairment. Dement. Geriatr. Cogn. Disord. 27, 278–285.
Ku, H.M., Kim, J.H., Kwon, E.J., Kim, S.H., Lee, H.S., Ko, H.J., Jo, S.M., Kim, D.K., 2004. Astudy on the reliability and validity of Seoul Instrumental Activities of DailyLiving (S-IADL). J. Korean Neuropsychiatr. Assoc. 43, 189–199.
Lee, J.H., Kang, Y., Jin, J.H., Na, D.L., Park, J.S., 2000. A normative study of the Koreanversion of Controlled Oral Word Association Test (COWAT) in the elderly.Korean J. Clin. Psychol. 19, 385–392.
Mahoney, F.I., Barthel, D.W., 1965. Functional evaluation: the Barthel index. MDState Med. J. 14, 61–65.
Morris, J.C., 1993. The Clinical Dementia Rating (CDR): current version and scoringrules. Neurology 43, 2412–2414.
Pearman, A., Storandt, M., 2004. Predictors of subjective memory in older adults. J.Gerontol. B: Psychol. Sci. Soc. Sci. 59, P4–P6.
Peres, K., Chrysostome, V., Fabrigoule, C., Orgogozo, J.M., Dartigues, J.F., Barberger-Gateau, P., 2006. Restriction in complex activities of daily living in MCI: impacton outcome. Neurology 67, 461–466.
Perneczky, R., Pohl, C., Sorg, C., Hartmann, J., Tosic, N., Grimmer, T., Heitele, S., Kurz,A., 2006. Impairment of activities of daily living requiring memory or complexreasoning as part of the MCI syndrome. Int. J. Geriatr. Psychiatry 21, 158–162.
Petersen, R.C., Smith, G.E., Waring, S.C., Ivnik, R.J., Tangalos, E.G., Kokmen, E., 1999.Mild cognitive impairment: clinical characterization and outcome. Arch. Neu-rol. 56, 303–308.
Petersen, R.C., Stevens, J.C., Ganguli, M., Tangalos, E.G., Cummings, J.L., DeKosky, S.T.,2001. Practice parameter: early detection of dementia: mild cognitive im-pairment (an evidence-based review). Report of the Quality Standards Sub-committee of the American Academy of Neurology. Neurology 56, 1133–1142.
Reisberg, B., Shulman, M.B., Torossian, C., Leng, L., Zhu, W., 2010. Outcome overseven years of healthy adults with and without subjective cognitive im-pairment. Alzheimers Dement. 6, 11–24.
Rodda, J., Okello, A., Edison, P., Dannhauser, T., Brooks, D.J., Walker, Z., 2010. 11C-PIBPET in subjective cognitive impairment. Eur. Psychiatry 25, 123–125.
Treves, T.A., Verchovsky, R., Klimovitzky, S., Korczyn, A.D., 2005. Incidence ofdementia in patients with subjective memory complaints. Int. Psychogeriatr.17, 265–273.
Van der Flier, W.M., Van Buchem, M.A., Weverling-Rijnsburger, A.W., Mutsaers, E.R.,Bollen, E.L., Admiraal-Behloul, F., Westendorp, R.G., Middelkoop, H.A., 2004.Memory complaints in patients with normal cognitive are associated withsmaller hippocampal volumes. J. Neurol. 251, 671–675.
Visser, P.J., Verhey, F., Knol, D.L., Scheltens, P., Wahlund, L.O., Freund-Levi, Y.,Tsolaki, M., Minthon, L., Wallin, A.K., Hampel, H., Burger, K., Pirttila, T., Soininen,H., Rikkert, M.O., Verbeek, M.M., Spiru, L., Blennow, K., 2009. Prevalence andprognostic value of CSF markers of Alzheimer’s disease pathology in patientswith subjective cognitive impairment or mild cognitive impairment in theDESCRIPA study: a prospective cohort study. Lancet Neurol. 8, 619–627.
Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund, L.O., Nordberg,A., Backman, L., Albert, M., Almkvist, O., Arai, H., Basun, H., Blennow, K., De Leon,M., DeCarli, C., Erkinjuntti, T., Giacobini, E., Graff, C., Hardy, J., Jack, C., Jorm, A.,Ritchie, K., Van Duijn, C., Visser, P., Petersen, R.C., 2004. Mild cognitive im-pairment–beyond controversies, towards a consensus: report of the Internation-al Working Group on Mild Cognitive Impairment. J. Intern. Med. 256, 240–246.
Yang, D.W., Cho, B., Chey, J.Y., Kim, S.Y., Kim, B.S., 2002. Development and validationof Korean Dementia Screening Questionnaire (KDSQ). J. Korean Neurol. Assoc.20, 135–141.
Zandi, T., 2004. Relationship between subjective memory complaints, objectivememory performance, and depression among older adults. Am. J. Alzheimer’sDis. Other Demen. 19, 353–360.