![Psoriasis and Atopic Dermatitis - Home - Springer · psoriasis should, therefore, incorporate a strategy to address both physical and non-physical comorbidities [24]. Burden of Psoriasis](https://static.fdocuments.us/doc/165x107/5d41538588c9936e348b4fce/psoriasis-and-atopic-dermatitis-home-springer-psoriasis-should-therefore.jpg)
What’s new in Psoriasis treatment - The Australian ... · Comorbidities in Psoriasis •A...
45
Comorbidities Peter Foley MBBS, BMedSc, MD, FACD Associate Professor of Dermatology, The University of Melbourne, Department of Medicine (Dermatology), St Vincent’s Hospital Melbourne Dermatology Investigation, Biological Therapies and Photobiology Clinics, St Vincent’s Hospital Melbourne Phototherapy and Biological Clinics, Skin and Cancer Foundation Inc (Victoria) Copyright
Transcript of What’s new in Psoriasis treatment - The Australian ... · Comorbidities in Psoriasis •A...

Comorbidities
Peter Foley MBBS, BMedSc, MD, FACD Associate Professor of Dermatology, The University of Melbourne, Department of Medicine (Dermatology), St Vincent’s Hospital Melbourne Dermatology Investigation, Biological Therapies and Photobiology Clinics, St Vincent’s Hospital Melbourne Phototherapy and Biological Clinics, Skin and Cancer Foundation Inc (Victoria)
Copyri
ght

Disclosures / Conflicts of Interest
• CSL – A, SP
• Galderma/PhotoCure – A, C, I, SP, T
• 3M/iNova/Valeant – A, I, SP
• LEO/Peplin – A, C, I, SP, T
• Roche – C, SP, T
• Ascent – C, SP, T
• Clinuvel – A, C, I
• GSK/Stiefel – A, I, SP
– A = advisory board
– C = consultant
– I = investigator (clinical trials)
– SP = speaker’s bureaux
– T = travel grants
• Abbott – A, SP
• BiogenIdec – A, I, SP
• Janssen-Cilag – A, C, SP
• Merck Serono - A, I, SP
• Schering-Plough/MSD – A, I, SP
• Wyeth/Pfizer – A, C, I, SP
• Amgen – A, I
• Novartis – A, I, SP, T
• Eli Lilly - I
• Celgene - I
• Australian Ultraviolet Services - C
• Aspen - SP
• BMS - I
Copyri
ght

Psoriasis morbus fortiorium
“Psoriasis: the disease of people in good health”
Copyri
ght

Comorbidities in Psoriasis
• A distinct number of concomitant disease entities have more frequently been observed than expected
• Such associations referred to as ‘comorbidities’ • May represent effect of shared risk factors
– Genetic predisposition – Environmental exposure – Factors related to long course of psoriasis – Factors related to treatment of psoriasis
• May represent an artifact because of increased surveillance of patients with psoriasis
Copyri
ght

Comorbidities in Psoriasis
• Metabolic syndrome – Hypertension – Diabetes mellitus Type II – Dyslipidaemia
• Obesity • Cardiovascular disease and death • Psoriatic arthritis • Inflammatory Bowel Disease • Anxiety and Depression • Smoking and Alcohol • Lymphoma
Copyri
ght

Co-morbidities In Psoriasis Patients
Hypertension Anxiety
Psoriatic arthritis
Depression
Diabetes Substance / Alcohol
abuse
All other forms of arthritis
Total (n=1000)
Moderate (n=398)
Severe (n=204)
Very Severe (n=397)
27%
23%
22%
17%
16%
16%
11%
10%
8%
2%
8%
31%
37%
28%
39%
23%
19%
22%
16%
15%
11%
3%
11%
15%
35%
23%
24%
25%
21%
16%
14%
13%
12%
2%
11%
23%
17%
20%
14%
10%
11%
12%
6%
7%
4%
1%
6%
44%
Obesity
Hypercholesterolaemia
Skin Cancer
Other
None
EU CHART study report 2004
Copyri
ght

Psoriasis Co-morbidities in Australia
Co-morbidity n %
Obesity 328 48.7
Hypertension 178 26.4
Hyperlipidaemia 139 20.6
Depression 105 15.6
Diabetes 91 13.5
Non-melanoma skin cancer 61 9.1
Liver disease 60 8.9
Ischaemic heart disease 36 5.3
Other psychiatric illness 30 4.5
Other cancer 25 3.7
Melanoma skin cancer 18 2.7
Alcoholism 18 2.7
Copyri
ght
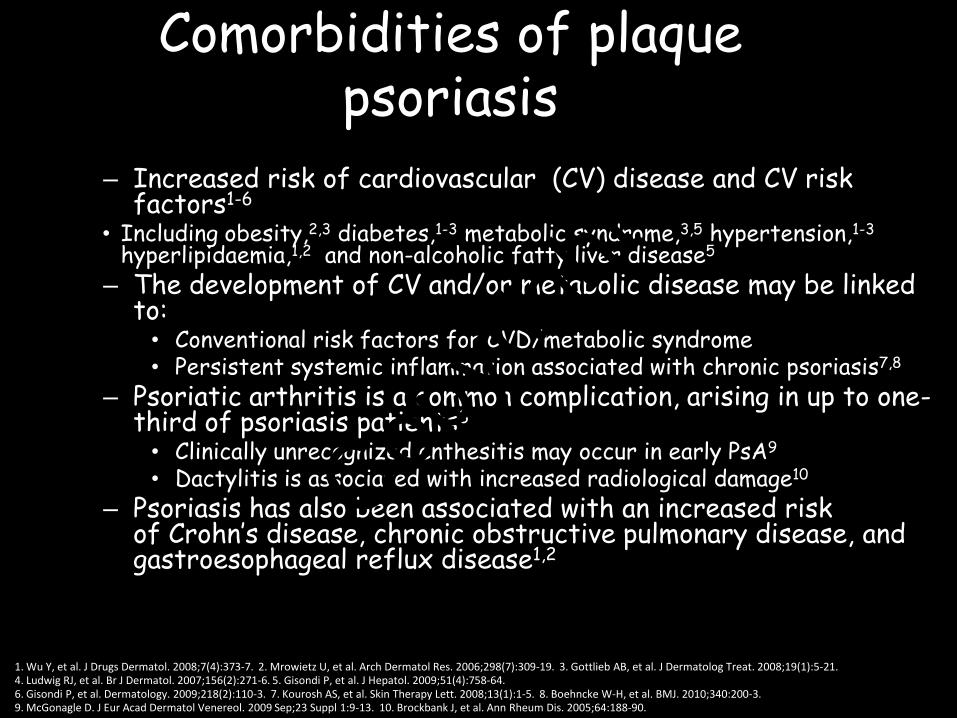
Comorbidities of plaque psoriasis
– Increased risk of cardiovascular (CV) disease and CV risk factors1-6
• Including obesity,2,3 diabetes,1-3 metabolic syndrome,3,5 hypertension,1-3 hyperlipidaemia,1,2 and non-alcoholic fatty liver disease5
– The development of CV and/or metabolic disease may be linked to:
• Conventional risk factors for CVD/metabolic syndrome • Persistent systemic inflammation associated with chronic psoriasis7,8
– Psoriatic arthritis is a common complication, arising in up to one-third of psoriasis patients3
• Clinically unrecognized enthesitis may occur in early PsA9
• Dactylitis is associated with increased radiological damage10
– Psoriasis has also been associated with an increased risk of Crohn’s disease, chronic obstructive pulmonary disease, and gastroesophageal reflux disease1,2
1. Wu Y, et al. J Drugs Dermatol. 2008;7(4):373-7. 2. Mrowietz U, et al. Arch Dermatol Res. 2006;298(7):309-19. 3. Gottlieb AB, et al. J Dermatolog Treat. 2008;19(1):5-21. 4. Ludwig RJ, et al. Br J Dermatol. 2007;156(2):271-6. 5. Gisondi P, et al. J Hepatol. 2009;51(4):758-64. 6. Gisondi P, et al. Dermatology. 2009;218(2):110-3. 7. Kourosh AS, et al. Skin Therapy Lett. 2008;13(1):1-5. 8. Boehncke W-H, et al. BMJ. 2010;340:200-3. 9. McGonagle D. J Eur Acad Dermatol Venereol. 2009 Sep;23 Suppl 1:9-13. 10. Brockbank J, et al. Ann Rheum Dis. 2005;64:188-90.
Copyri
ght
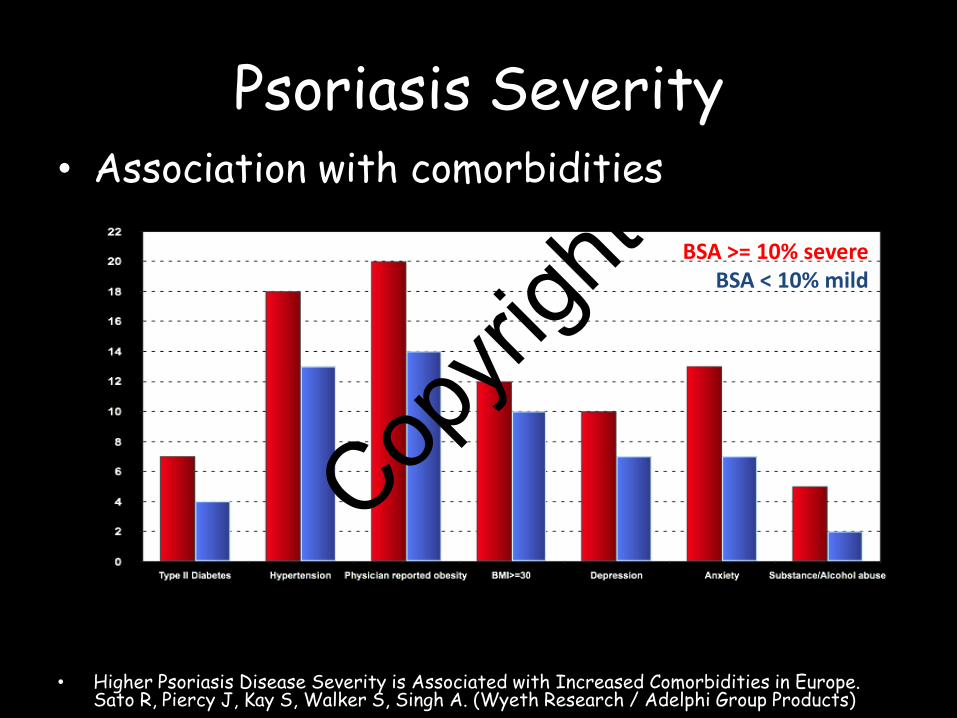
• Association with comorbidities
• Higher Psoriasis Disease Severity is Associated with Increased Comorbidities in Europe. Sato R, Piercy J, Kay S, Walker S, Singh A. (Wyeth Research / Adelphi Group Products)
BSA >= 10% severe BSA < 10% mild
Psoriasis Severity
Copyri
ght

Inflammatory dysfunction is likely to contribute to the development of comorbidities in psoriasis
• Immune dysregulation and inflammation play an important role in the development and progression of psoriasis1,2
• As psoriasis progresses, persistent inflammatory dysfunction may drive the development of comorbid conditions such as cardiovascular disease1,2
1. Kourosh AS, et al. Skin Ther Lett. 2008;13(1):1-5. 2. Boehncke W-H, et al. BMJ. 2010;340:200-3.
The psoriatic march2
Cardiovascular disease
Atherosclerosis
Obesity
Endothelial dysfunction
Insulin resistance
Systemic inflammation
Psoriasis Smoking/alcohol
= association
Copyri
ght

The psoriatic march and the development of comorbidities
Gisondi P, Girolomoni G. Actas Dermosifiliogr. 2009;100 Suppl 2:14-21.
Diabetes
Psoriasis
Psoriatic arthritis
NAFLD
Hypertension
Dyslipidaemia
Smoking
Cardiovascular diseases
Metabolic syndrome
Obesity
Genes Environmental
triggers
Copyri
ght

Metabolic Syndrome
• For metabolic syndrome to be diagnosed, at least three of the following apply: – Waist circumference > 102 cm (men); 88 cm
(women) – Serum triglycerides >= 1.69 mmol/L – HDL cholesterol < 1.04 mmol/L (men); 1.29
mmol/L (women) – Blood pressure >= 130/85 mm Hg – Serum glucose >= 6.1 mmol/L
– NIH ATP III (Adult Treatment Panel), www.nhlbi.nih.gov/guidelines/cholesterol
Copyri
ght

Metabolic Syndrome
• Psoriasis patients: – Have risk of developing metabolic
syndrome
– More severe psoriasis: risk
• Not known whether link is causative or a result of patient habits eg sedentary life, smoking, alcohol Cop
yrigh
t

Psoriasis is associated with an increased risk of the metabolic
syndrome
Type of rate OR and 95% CI OR 95% CI
Unadjusted 2.16 1.16-4.03
Multivariate† 1.96 1.02-3.77
0 3 2 1
Odds ratios (OR) for the metabolic syndrome* in a psoriasis population vs a control population
National Health and Nutrition Examination Survey, 2003-2006. (US; n = 71 cases, n = 2385 controls) Love TJ, et al. Arch Dermatol. 2011;147(4):419-24.
4
*Revised NCEP ATP III Definition †Adjusted for for age, sex, race/ethnicity, smoking status, and C-reactive protein (CRP) levels
Copyri
ght

Hypertension, Diabetes, Dyslipidaemia
• All are more common in pts with psoriasis • Obesity, hypertension, heart failure and diabetes were as much
as two-fold more prevalent in 2,941 psoriatic inpatients compared to age-matched non-psoriatic patients (Henseler T and Christophers E, Disease concomitance in psoriasis. J Am Acad Dermatol 1995; 32: 982-6).
• Hypertension – rate due to obesity or use of cyclosporin – Smoking
• Diabetes Type II – Insulin resistance / metabolic syndrome – Associated with obesity
• Dyslipidaemia – Secondary to medication eg retinoids – Associated with obesity – Alcohol
Copyri
ght
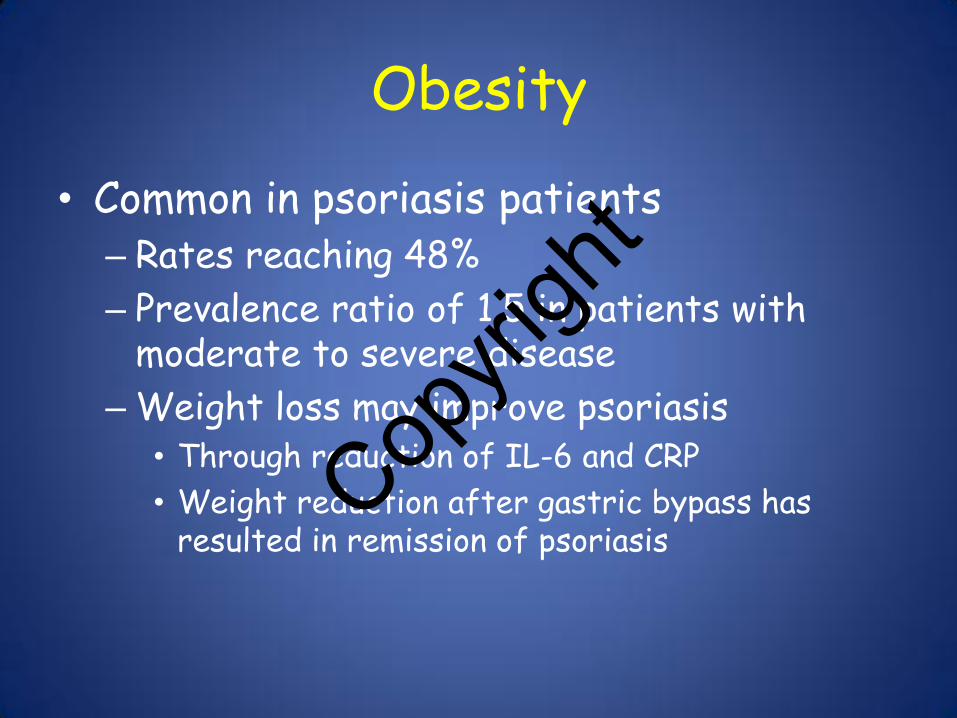
Obesity
• Common in psoriasis patients – Rates reaching 48%
– Prevalence ratio of 1.5 in patients with moderate to severe disease
– Weight loss may improve psoriasis • Through reduction of IL-6 and CRP
• Weight reduction after gastric bypass has resulted in remission of psoriasis
Copyri
ght

Cardiovascular Disease and Death
• Psoriasis is an independent risk factor for atherosclerosis
• Severity of psoriasis is independent risk factor for MI regardless of presence of the metabolic syndrome
• Pts with PASI 10-20 and pts with PASI >20: – Similar 10-yr risk of coronary heart disease and stroke
• Compared with general population, 10-yr risk was: • 28% greater for coronary heart disease (P<0.001) • 11.8% greater for stroke (P=0.02)
Kimball et al (Am J Med 2010;123(4):350-357)
• Peripheral vascular disease increased in psoriasis patients
Prodanovich et al (Arch Derm 2009;145(6):700-3)
Copyri
ght

Cardiovascular Disease and Death
• Young patients with severe psoriasis have MI / cardiovascular mortality – Psoriasis patients treated at least once as an inpatient had a 50%
increased risk for cardiovascular mortality compared to the general population
– Risk was clearly associated with: • severity of psoriasis • number of hospital admissions • admission at a young age
(Mallbris L, Akre O, Granath F, et al., Eur J Epidemiol 2004; 19:225-230)
• In UK: – Lifespan of patients with severe psoriasis decreased by 5% – Patients with onset < 25 yo: Lifespan shortened by 20 years
• Psoriasis most likely predisposes to increased risk of
cardiovascular disease by causing increase in TH-1 cytokines (TNF-α, IL2, IFNγ) – Cause upregulation of adhesion molecules and endothelins – Cause premature vascular damage and atherogenesis
Copyri
ght

Adjusted relative risk of MI in patients with psoriasis based on patient age
1.29
3.10
1.08
1.36
Psoriasis may confer an independent risk of MI. The RR was greatest in young patients with severe psoriasis.
Gelfand JM, et al. Risk of myocardial infarction in patients with psoriasis. JAMA 2006; 296:1735-41.
Copyri
ght

Severe psoriasis is associated with an increased risk of all-cause mortality
Gelfand JM, et al. Arch Dermatol. 2007; 143:1493-9.
Hazard
ratio
of m
orta
lity
vs
con
trols
(95
% c
onfi
denc
e int
erv
als)
Mild psoriasis (n=133,568) Severe psoriasis (n=3951)
3.0
0.5
0 95
Age (years)
85 75 65 55 45 35 All ages
1.0
1.5
2.0
2.5
3.5
Hazard ratio (95% confidence interval) for all-cause mortality vs controls
4.0
Retrospective, population-based cohort study (UK; n=137,519 cases, n=575,433 controls)
Copyri
ght

Risk of obesity is significantly increased in patients with psoriasis
Prey S, et al. J Eur Acad Dermatol Venereol. 2010;24 Suppl 2:23-30.
Risk of obesity in psoriatic patients (odds ratio with 95% confidence interval)
Study*
*See slide notes for citations in full.
Herron 2005
Naldi 2005
Neimann 2006
Gisondi 2007
Kaye 2008
Cohen 2008
Naldi 2008
Driessen 2008
2.39
1.9
1.84
1.29
1.19
1.18
1.7
1.7
5.49
2 4 6 8 10
Matching
Not matching
Mild and moderate
Severe
Populations
Type of psoriasis
General population (databases)
Dermatological patients
Control
Cross sectional studies about risk
of obesity in psoriatic patients
(odds ratio with 95% confidence
interval).
Copyri
ght

Obesity is a relevant risk factor for psoriasis and precedes development
of psoriasis
– Body mass index is a risk factor independently associated with onset of psoriasis1
– Increased adiposity and weight gain are strong risk factors for incident psoriasis in women2
– Obesity in early adulthood has also been shown to be a risk factor for psoriatic arthritis3
1. Naldi L et al. J Invest Dermatol 2005;125:61-7 2. Setty AR et al. Arch Intern Med 2007;167:1670-5 3. Soltani-Arabshahi R et al. Arch Dermatol 2010;147:721-6
Copyri
ght

0
0.5
1.5
RR
fo
r d
eve
lop
ing
PsA
Increased BMI is associated with increased risk of psoriatic arthritis
Love JT, et al. Ann Rheum Dis. 2012;71(8):1273-7.
BMI <25 25-29.9 30-34.9 ≥35.0
1.0
Copyri
ght

Psoriasis and obesity: a vicious cycle of systemic inflammation
Skin inflammation – psoriasis
Adapted from: Davidovici BB, et al. J Invest Dermatol. 2010;130(7):1785-96.
TNF; IL-1, IL-6, IL-8 IL-15, IL-18, IL-19, IL-20 IL-12, IL-23, IFN-γ, IL-l7 S100 proteins IL-10 (IL-4, IL-13)
TNF MCP-1, M-CSF Leptin, IL-6, IL-5, iNoS Adiponectin, PAI-1, renin-angiotensin (angiotensinogen) SHBG
Adipose tissue – obesity
Auto-inflammatory loop
Cytokines Leukocytes
Copyri
ght

Weight gain may occur in patients receiving anti-TNF-a treatment
Mean weight (kg) change from baseline to Week 48
Adapted from: Saraceno R, et al. Pharmacol Res. 2008;57(4):290-5.
5
Me
an w
eig
ht
chan
ge (
kg)
1
0
3
4
2
Patients in group showing weight gain
48% 44% 40%
Infliximab n=50
1.53
p=0.0001
Etanercept n=50
2.18
p=0.007
Adalimumab n=30
2.57
p=0.0014
Copyri
ght

1. Gisondi P, et al. J Eur Acad Dermatol Venereol. 2008;22(3):341-4. 2. Di Renzo L, et al. Dermatol Ther. 2011;24(4):446-51. 3. Prignano F, et al. Curr Med Res Opin. 2009;25(9):2311-6.
Weight gain may occur in patients receiving anti-TNF treatment
Mean body weight increased significantly from baseline in patients receiving etanercept (1.5±2.7 kg) (n=58) or infliximab (2.5±3.3 kg) (n=40) (p=0.004)1
A relative increase in bodyweight of 2.6±3.2% was observed in a mixed group of patients receiving either etanercept (n=28) or infliximab (n=12)2
– Blockade of TNF activity was associated with fat and lean mass gain in psoriasis and psoriatic arthritis patients
Increased bodyweight was recorded in the majority of patients receiving etanercept (54%) (n=62) or infliximab (53%) (n=36)3
In three studies in which patients with plaque psoriasis received anti-TNFs with follow up at 24 weeks:
Copyri
ght

Psoriasis is associated with an increased risk of diabetes
Type of rate OR and 95% CI OR 95% CI P
Crude data 1.83 1.71-1.96 <0.00001
Age-adjusted 1.33 1.26-1.41 <0.00001
Age- and gender-adjusted
1.33 1.25-1.40 <0.00001
0 3 2 1
Odds ratios (OR) for diabetes in a psoriasis population vs a control population
Clalit Health Services database (Israel; n=15,757 cases, n=49,358 controls) Cohen AD, et al. J Eur Acad Dermatol Venereol. 2008;22(5):585-9.
Copyri
ght

Cardiovascular Comorbidities
RA IBD Psoriasis
Hypertension
Dyslipidemia
Atherosclerosis
Metabolic syndrome
Thromboembolism ̶ ̶ Biomarkers of CV risk sICAM-1
homocysteine CRP IL-6
sICAM-1 homocysteine*
CRP IL-6
sICAM-1 homocysteine
IL-6 MCP-1
Increased mortality 2-3x 1.5x 3-4x
Reduced life expectancy
10-20 years unknown 3-20 years
*no association with increased CV risk
Copyri
ght

Psoriatic Arthritis • Chronic inflammatory arthritis
– Causes progressive joint damage, reduced function – Uveitis frequently associated
• Prevalence 6-25% – Lack of consistency between studies concerning diagnostic criteria for PsA
• HLADR4 +ve: severe destructive form
• Usually develops after onset of psoriasis – Typically 10 years later
• Increased mortality in psoriatic arthritis – Previously active and severe disease, manifested by:
• Prior use of medications; and • Radiologic changes; and • Elevated ESR at presentation (Gladman et al, Arthritis Rheum 1998;41:1103-10).
• TNF-α – Plays central role in pathogenesis – Triggers osteoclastogenesis and bone resorption
• By stimulating both receptor activation of NF KappaB and its ligand • Expressed in bone marrow osteoclast precursors and stomal cells respectively
Copyri
ght

1. Ibrahim G, et al. Clin Exp Rheumatol 2009;27(3):469-74. 2. Husni ME, et al. J Am Acad Dermatol 2007;57(4):581-7. 3. Gladman D, et al. Ann Rheum Dis 2008;68(4):497-501. 4. Tinazzi I, et al. Rheumatology (Oxford). 2012 Aug 9. [Epub ahead of print]
• Psoriasis Epidemiology Screening Tool (PEST)1
– 5-item questionnaire
– Sensitivity 92%; specificity 78%
• Psoriatic Arthritis Screening and Evaluation Tool (PASE)2
– 15-item questionnaire
– Sensitivity 82%; specificity 73%
• Toronto Psoriatic Arthritis Screen (ToPAS)3
– 12-item questionnaire
– Sensitivity 87%; specificity 93%
– Designed to detect PsA in any population, including non-psoriasis populations
• Early Arthritis for Psoriatic Patients (EARP)4
– 10-item questionnaire
– Sensitivity 85%; specificity 92%
Screening tools for psoriatic arthritis
PEST. Courtesy of Professor P Helliwell.1
Copyri
ght

Depression and Anxiety • Prevalence of depression 10-62% amongst psoriasis patients
– Range due to inpatient (high) vs outpatient (low)
– Higher rates of suicidal ideation in severely affected psoriasis inpatients c/w pts with atopic dermatitis, acne
• PASI not a reliable predictor of depression risk
• Pruritus associated with depression in psoriasis patients ? poor sleep
• Impact that psoriasis has on quality of life is a stronger indicator of psychiatric morbidity than clinical severity
• Patients with PsA and skin psoriasis report significantly worse quality of life; joint pain associated with depression
• Perception of stigmatisation amongst psoriasis sufferers the most important predictor of depression
• Those who developed psoriasis young:
– Harbour stronger feelings of stigmatisation
– Lack of support correlated with depression
• Depression is:
– An independent risk factor for heart disease
– Associated with excess mortality, particularly from cardiovascular disease
• Anxiety found in up to 43% of psoriasis patients Hayes & Koo 2010
Copyri
ght
Inflammatory Bowel Disease (Crohn’s Disease, Ulcerative Colitis)
• Crohn’s disease patients – 7x higher risk of developing psoriasis
• Psoriasis patients – 3x higher risk of Crohn’s disease
• Ulcerative colitis – Statistically significant association with psoriasis but
not as high as Crohn’s disease • Crohn’s disease, ulcerative colitis and psoriasis
share the same susceptibility loci (6P21), IL-23 receptor and IL-12B genes – IL-23 receptor encodes for a subunit of IL-23, pro-
inflammatory cytokine • Crohn’s disease and psoriasis primarily mediated by
Th-1 lymphocyte producing cytokines such as TNF-α and IFNg
Copyri
ght

What is non-alcoholic fatty liver disease (NAFLD)?
Characterised by insulin resistance and strongly associated with type 2 diabetes and obesity1-3
Defined by fatty changes in the liver in the absence of a history of excessive alcohol consumption1
The spectrum of the disease ranges from simple steatosis to steatosis with evidence of hepatocellular inflammation (non-alcoholic steatohepatitis, or NASH), advanced fibrosis, and cirrhosis1,2
NAFLD may be primary (associated with the metabolic syndrome) or secondary (associated with nutrition, drugs, toxins, or metabolic or other diseases)1,2
1. Adams LA, et al. CMAJ. 2005;172(7):899-905. 2. Angulo P. N Engl J Med. 2002;346(16):1221-31. 3. Bhatia LS, et al. Eur Heart J. 2012;33(10):1190-200.
Copyri
ght

Prevalence of NAFLD in psoriasis patients vs controls
0
20
40
100
80
Psoriasis patients (n=130)
NA
FLD
pre
vale
nce
(%
)
* 60
Control (n=260)
*p<0.0001
Prevalence of NAFLD in psoriasis patients by disease severity
0
20
40
100
80
PASI <10 (n=59)
NA
FLD
pre
vale
nce
(%
)
* 60
PASI ≥10 (n=71)
*p<0.01
Psoriasis is associated with non-alcoholic fatty liver disease (NAFLD)
Gisondi P, et al. J Hepatol. 2009;51(4):758-64.
Copyri
ght

Bhatia LS, et al. Eur Heart J. 2012;33(10):1190-200.
NAFLD is a CV disease risk factor
IR: insulin resistance
Excess caloric intake Sedentary lifestyle
Genetic susceptibility
Deranged adipokine profile
Ectopic fat in other organs e.g. heart
Hyperinsulinaemia Plasma FFA
Visceral and subcutaneous
fat and/or adiposopathy
Adipose tissue IR
Skeletal muscle lipids
Ectopic fat
Skeletal muscle IR
Adipose tissue IR
NASH
Hepatic IR
Hepatic steatosis
CV risk (↑ endothelial dysfunction, ↑ dyslipidaemia,
hypercoaguability, ↑ inflammation, ↑ atherosclerosis, CV lipotoxicity)
Copyri
ght

Smoking and Alcohol
• Smoking – Positive correlation between smoking and psoriasis
• >20 cigarettes per day assoc. with 2.2x in more severe forms of psoriasis
• Female smokers: 3.3x risk of psoriasis
• Palmoplantar pustulosis has strongest association
– Pathophysiology of smoking: • Psoriasis involves a neutrophil – predominantly inflammatory infiltrate
• Smoking thought to alter the morphology and function of neutrophils
• Also causes damage via oxidation – Anti-oxidant levels are low in psoriasis patients, making them more susceptible to
oxidative damage
• Alcohol – Psoriasis patients have higher prevalence of excess alcohol intake
– Disease severity positively correlated with alcohol intake
– Excess alcohol intake shown to precipitate psoriasis
– Excess alcohol consumption a known association with anxiety and depression
Copyri
ght

Traditional systemic treatments for psoriasis may impact CV risk factors
Methotrexate1-3
– Few studies are available in the psoriasis population and data are not conclusive
– One study suggested no significant impact on risk of MI, with a trend towards reduced risk in younger patients1
– Another study indicated that moderate doses may reduce the risk of vascular disease versus non-treated psoriasis patients2
– May induce hyperhomocysteinaemia, a risk factor for thrombosis3
– May favour steatohepatitis4
Ciclosporin3
– May increase blood pressure (induce or worsen hypertension)
– May alter glucose tolerance
– May promote hyperlipidaemia
Retinoids3
– May promote hyperlipidaemia
1. Abuabara K, et al. Br J Dermatol. 2011;165(5):1066-73. 2. Prodanovich S, et al. J Am Acad Dermatol. 2005;52(2):262-7. 3. Gisondi P, Girolomoni G. Actas Dermosifiliogr. 2009;100 Suppl 2:14-21. 4. Adams LA, et al. CMAJ. 2005;172(7):899-905.
Copyri
ght

Therapeutic Potential for Biologics in Managing Comorbidities
• Metabolic Syndrome – Insulin resistance
• Biologics inhibit pro-inflammatory cytokines, potentially improving insulin sensitivity • Isolated cases of psoriasis and rheumatoid arthritis pts with diabetes developing
unpredictable hypo- or hyperglycaemia after commencing anti-TNF-α treatment
– Body Mass Index and weight • Reports of anti-TNF-α medications associated with significant weight gain and
increases in BMI (Gisondi et al, J Eur Acad Dermatol Venereol 22:341-344, 2008)
• Weight gain may aggravate preexisting metabolic syndrome • Biologics with a fixed-dose regimen may have a compromised efficacy in heavier
individuals (Clark et al. J Am Acad Dermatol 2008; 58:443-6)
• Fully human monoclonal anti-p40 antibody not associated with weight gain
– Blood lipids • Biologics’ effects on blood lipids: mixed and unclear results
• Cardiovascular Disease – Biologics inhibit pro-inflammatory cytokines
• Potentially decreasing cardiovascular risk and mortality – TNF-α antagonist contraindicated in pts with moderate-severe forms of
congestive heart failure
Copyri
ght

Therapeutic Potential for Biologics in Managing Comorbidities
• Psoriatic Arthritis – Clinical trials have shown that TNF-α
antagonists: • Markedly inhibit inflammation • Reduce structural joint damage
– Radiographic evidence of inhibition of progressive joint disease
• Inflammatory Bowel Disease – Crohn’s disease and ulcerative colitis
• Anti-TNF-α antibodies have proven beneficial effect • Etanercept: Lack of efficacy
– Report of development of Crohn’s disease in treated pts
Copyri
ght

Biologic treatments for psoriasis: impact on CV risk factors
Data gathered from rheumatoid arthritis populations receiving anti-TNFs indicate potential for:1
– Reduced insulin resistance
– Control of inflammation (CRP, IL-6)
– Increased HDL-cholesterol
– Decreased risk of arteriosclerotic plaque formation
In a retrospective study of patients with psoriasis or psoriatic arthritis (n=8845), those treated with TNF inhibitors (n=1673) showed:2
– Significant reduction in MI risk vs topical agents
– Significantly lower MI incident rate vs topical agents
1. Kaplan MJ. Vasc Health Risk Manag. 2008;4(6):1229-35. 2. Wu JJ, et al. Arch Dermatol. Epub 20 Aug 2012.
Copyri
ght

Management of Comorbidities
• Look closely for comorbidities – eg signs of insulin resistance
• Be aware of the risk profile – e.g. early onset, severe psoriasis
increase risk
• For all psoriasis patients: – Take complete history
• DLQI, Smoking, Alcohol
– Physical examination • incl. blood pressure
– Laboratory screening • incl. fasting glucose and lipids
– CXR, ? ECG
– Regular monitoring of risk factors • Disease associated
• Medication associated
Copyri
ght

Management of Comorbidities
• Encourage lifestyle changes (diet, exercise, stop smoking) • High body mass index is associated with a reduced short-term
clinical response to all systemic treatments (Naldi et al. Dermatology 2008; 217:365-73)
• Weight loss improves the response of obese patients with
moderate-to-severe chronic plaque psoriasis to low-dose ciclosporin therapy
(Gisondi et al. Am J Clin Nutr 2008; 88:1242-7)
• Early referral, eg: – Metabolic syndrome: refer to endocrinologist / cardiologist – Diabetes: refer to diabetic educator / endocrinologist – Anxiety / Depression: Psychologist / psychiatrist – Liaise closely with GPs eg hypertension control, lipid-lowering meds
Copyri
ght

Psoriasis: Beyond the Skin
• Need to recognise psoriasis as a chronic inflammatory disorder
• Choices for therapy should take into account adverse effects of drugs on co-morbidities and dangerous drug interactions
• Therapy of psoriasis is influenced by and may affect other organ systems and co-morbid diseases; – High index of suspicion of side effects associated
with systemic treatments
• Therapy of psoriasis may benefit from treating associated metabolic disorders
Copyri
ght

Psoriasis: Beyond the Skin
• Inflammation associated with moderate-to-severe psoriasis confers a higher cardiovascular morbidity and mortality risk; therefore long-term disease control with systemic therapy may reduce cardiovascular morbidity and mortality in psoriasis patients.
• Patients with psoriasis need a global approach, taking into account their cardiovascular risk profile.
• Assessment of psoriasis severity should take a broader view than just a PASI assessment; address comorbidities such as: – Cardiovascular risk factors – Psoriatic arthritis – Psoriasis symptoms (pruritus, cutaneous pain, burning, bleeding,
desquamation) – Quality of life
• Broader assessment may indicate earlier treatment than when
using PASI alone to assess psoriasis severity
Copyri
ght

QUESTIONS?
Copyri
ght