What to Do When a Patient with Community Acquired Pneumonia Fails to improve?
32
-
Upload
gamal-agmy -
Category
Health & Medicine
-
view
892 -
download
1
Transcript of What to Do When a Patient with Community Acquired Pneumonia Fails to improve?


What to Do When a Patient with Community
Acquired Pneumonia Fails to improve?
Gamal Rabie Agmy, MD,FCCP Professor of Chest Diseases, Assiut university

Introduction
Treatment failure is a matter of
particular concern in the
management of CAP.
Treatment failure is associated with
high morbidity and mortality rates.
Its detection and management
require careful clinical assessment.

Definition
Lack of response or worsening of
clinical status (i.e., hemodynamic
instability, incidence of respiratory
failure, need for mechanical
ventilation, radiographic progression
, or appearance of new metastatic
infectious foci)
Definition
Failure to respond to
antimicrobial treatment was
classified as nonresponding or
progressive pneumonia.

Definition
◙Nonresponding pneumonia was defined as
persistent fever > 38°C and/or clinical
symptoms (malaise, cough, expectoration,
dyspnea) after at least 72 hours of
antimicrobial treatment.
◙Progressive pneumonia was defined as
clinical deterioration in terms of the
development of either or both septic shock
and acute respiratory failure requiring
ventilator support after at least 72 hours of
treatment.
Types
1-Early Failure: within 72 hours
2-Late failure: after 72 hours

Incidence
2.4 to 31% for early failure and
from 3.9 to 11% for late failure.
Factors associated with treatment failure
◙ High-risk pneumonia
◙ Liver disease ,neurological, neoplasia and
aspiration
◙ Multilobar infiltrates
◙ Legionella pneumonia
◙ Gram-negative pneumonia
◙ Pleural effusion
◙ Cavitation
◙ Leucopenia, and
◙ Discordant antimicrobial therapy.

Lower risk of failure
◙ Influenza vaccination
◙Initial treatment with
fluoroquinolones, and
◙ Chronic obstructive pulmonary
disease

Microbiology of Treatment Failure
◙ Gram negative bacteria
◙ MRSA
◙ Streptococcus pneumoniae
◙ L. pneumophila
Treatment of community-acquired pneumonia in adults who require
hospitalization. File et al, Jan 2016, Up to Date
Laboratory markers for treatment failure
1-Procalcitonin
2-CRP
3- IL6, IL8
4- IL1
5-Pleural effusion
6-Multilobar affection
7-CURB 65>3
Predicting treatment failure in patients with community acquired pneumonia: a
case-control study. Loeches et al, Respiratory Research2014 ,15:75

Evaluating a patient who is not responding to therapy
◙Repeating the history (including travel and pet
exposures to look for unusual pathogens), chest
radiograph, and sputum cultures, blood cultures, and urine antigen testing for Streptococcal
pneumoniae and Legionella if not previously done .
◙If this is unrevealing, then further diagnostic
procedures,, such as chest computed
tomography [CT], bronchoscopy, and lung biopsy
can be performed.

Chest sonography
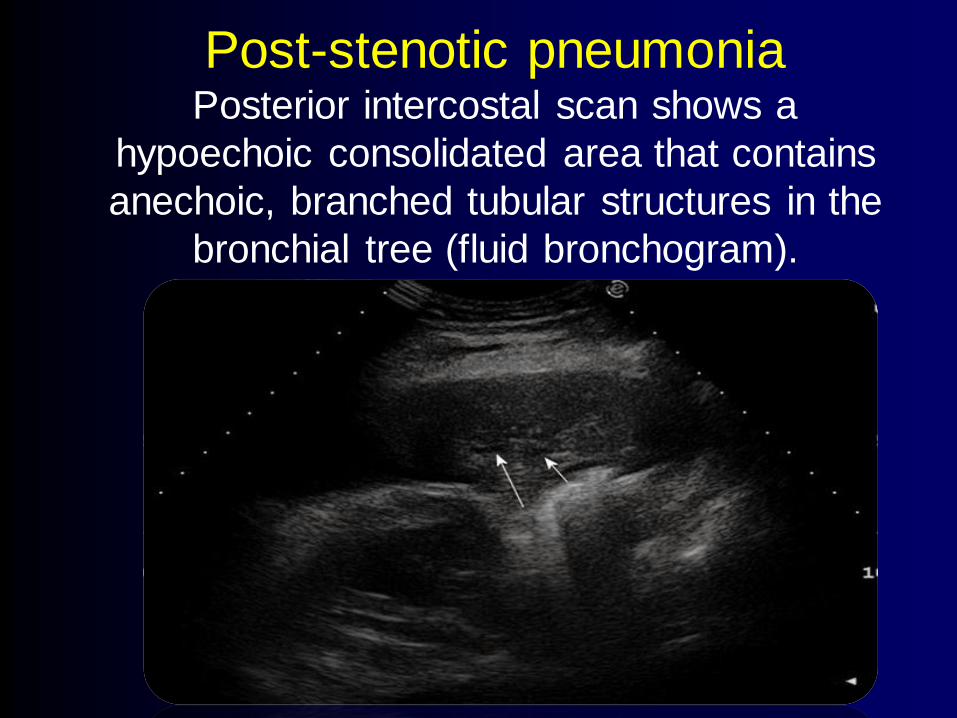
Post-stenotic pneumonia Posterior intercostal scan shows a
hypoechoic consolidated area that contains
anechoic, branched tubular structures in the
bronchial tree (fluid bronchogram).

Chest sonography

Chest sonography

Chest CT
Chest CT can detect pleural effusion, lung
abscess, or central airway obstruction, all of
which can cause treatment failure.
It may also detect noninfectious causes such as
bronchiolitis obliterans organizing pneumonia .
Since empyema and parapneumonic effusion can
contribute to nonresponse, thoracentesis should
be performed in all nonresponding patients with
significant pleural fluid accumulation.

Chest CT
Bronchoscopy
Bronchoscopy can evaluate the airway for
obstruction due to a foreign body or
malignancy, which can cause a
postobstructive pneumonia.
Protected brushings and bronchoalveolar
lavage (BAL) may be obtained for
microbiologic and cytologic studies; in
some cases, transbronchial biopsy may be
helpful.

Bronchoscopy
In addition, BAL may reveal evidence of
noninfectious disorders or, if there is a
lymphocytic rather than neutrophilic
alveolitis, viral or Chlamydia infection

Thoracoscopic lung biopsy
Thoracoscopic or open lung biopsy may be
performed if all of these procedures are
nondiagnostic and the patient continues to
be ill. The advent of thoracoscopic
procedures has significantly reduced the
need for open lung biopsy and its
associated morbidity.

Considerations*
Scenario
Resistant microorganism or uncovered
pathogen
Parapneumonic effusion or empyema
Nosocomial superinfection
Noninfectious condition, such as pulmonary embolism, drug fever, bronchiolitis obliterans,
organizing pneumonia, congestive heart
failure, vasculitis
Delayed response to
therapy with no
improvement after 72
hours
Severity of illness at presentation
Metastatic infection, such as empyema,
endocarditis, meningitis, arthritis
Inaccurate diagnosis, such as acute respiratory
distress syndrome, aspiration Exacerbation of comorbid illness or coexisting
noninfectious disease, such as renal failure,
acute myocardial infarction, pulmonary
embolism
Clinical deterioration
or continued
progression of illness





Nov. 2011

Nov. 2011