Lumbar Spine. Normal X-ray Views of Lumbar Spine AP viewLateral viewL5-S1 Spot View.
Upload
spineplusCategory
view
103download
0
What to do if the spine x-‐ray shows a …
Dr Paul Licina Dr Greg Cowderoy Spine surgeon Radiologist

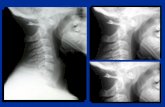
MVA with Flexion Injury Report : Alignment is satisfactory. Small fracture at the anterior corner C3. Disc degeneration and narrowing C3 –C6.

Flexion Teardrop Fracture Posterior ligament disruption and anterior compression fracture of the
vertebral body which results from a severe flexion injury.
Best seen on lateral view
Signs: Prevertebral swelling associated with anterior longitudinal ligament tear.
Teardrop fragment from anterior vertebral body avulsion fracture. Posterior vertebral body subluxation into the spinal canal.
Spinal cord compression from vertebral body displacement.
Fracture of the spinous process.

45 yr M
Axial injury onto head off mountain bike
C/O neck pain at coffee after the ride
Otherwise well


Bilateral Facet Dislocation
Anterior dislocation of the vertebral body resulting from extreme hyperflexion injury. It is associated with a very high risk of cord damage.
Best seen on lateral view
Signs: Anterior dislocation of affected vertebral body by half or more of
the vertebral body AP diameter.
Disruption of the posterior ligament complex and the anterior longitudinal ligament.
"Bow tie" or " bat wing" appearance of the locked facets.




Unilateral Facet Dislocation Facet joint dislocation and rupture of the apophyseal joint
ligaments resulting from rotatory injury of the cervical vertebrae.
Best seen on lateral or oblique views
Signs: Anterior dislocation of affected vertebral body by less than half
of the vertebral body AP diameter.
Discordant rotation above and below involved level.
Facet within intervertebral foramen on oblique view.
Widening of the disk space.
"Bow tie" or "bat wing" appearance of the overriding locked facets.


30 yr M
Persisting pain 3 weeks after MVA.
Neck stiffness
No Neurology
X-ray – Mild acute angle kyphosis at C5/6 with widening of the interspinous distance. No fracture is seen.

IMG_2085.JPG

Hyperflexion Injury
Disruption of the posterior ligamentous complex resulting from hyperflexion.
Signs:
Loss of normal cervical lordosis.
Anterior displacement of the vertebral body. Fanning of the interspinous distance.


C/O Neck Pain following preseason rugby camp.


Clay Shoveler’s Fracture
Fracture of a spinous process C6-T1
Best seen on lateral view
Signs:
Spinous process fracture on lateral view.
Ghost sign on AP view (i.e. double spinous process of C6 or C7 resulting from displaced fractured spinous process).

40 yr male
• Lumbar back pain following mountain bike accident
• No radiculopathy
• Tender mid lumbar spine

Report: Mildly displaced fractures of the left transverse processes of L2 and L3. No other fracture identified.

Crush Fractures And yet another fall in the making!
• Mechanism
• Low Energy- Osteoporotic
Elderly
• High Energy- All ages.
Need to exclude more significant injury
– Burst fracture
-- Chance fracture

Crush Fractures



file:///.file/id=6571367.7469579


Burst Fracture
Fracture that results from axial compression.
Burst fracture is a type of compression fracture which results in disruption of the posterior vertebral body cortex with retropulsion into the spinal canal. When involves the thoracolumbar level, it tends to occur between T9 and L5 levels . Burst fractures may be stable or unstable.
CT and MR is required for all patients to evaluate extent of injury.

Flexion Injury on holidays
Severe thoracolumbar back pain and tenderness
No radiculopathy
Haematuria



Chance Fracture


PERCUTANEOUS VERTEBROPLASTY INDICATIONS
Painful crush fracture Osteoporosis Few weeks
Malignant crush fracture Biopsy + vertebroplasty
Haemangioma Galibert 1987

PERCUTANEOUS VERTEBROPLASTY PATIENT SELECTION is the key to success
Back pain Sudden onset May radiate anteriorly NOT sciatica Mechanical Restricted activity Poor sleep
Local tenderness

PREPROCEDURE IMAGING
Purposes of pre-procedure imaging: Confirm presence of crush fracture Confirm that crush fracture is acute/ununited Diagnose other acute levels Integrity of spinal canal Accurately localise level

MRI PRE-VERTEBROPLASTY
Sagittal plane
T1 for anatomy
T2 fat saturation or STIR Marrow black
Oedema white

MRI
2
3
2
3


NEEDLE PLACEMENT LUMBAR

CEMENT INJECTION

PERCUTANEOUS VERTEBROPLASTY LITERATURE
Amar Neurosurg 2001;49:1105
97 pat., 258 levels
‘better life’ 74% Narcotic/analgesic use Mobility
Better sleep
Evans Radiology 2003;226:366 488 pat, 245 follow-up Pain scale 8.9 → 3.4 Impaired ambulation: 72% pre → 28% post
N Engl J Med. 2009 Aug 6;361(6):557-68.
A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures.
No benefit of vertebroplasty compared with a placebo procedure

PERCUTANEOUS VERTEBROPLASTY LOCAL RESULTS
Sept 2001 – June 2004
131 procedures
112 patients F 78, M 34 Ages 58-94, average 76
186 levels
‘Complete’ response 73.3%
Moderate response 17.6%
No response 9.2%

Scoliosis Classification:
Idiopathic: 80% Infantile <3; Juvenile 4-10; Adolescent: 10-18
Or: Early onset <5; Late onset >5
Congenital: Osteogenic: hemivertebra, fused vertebra
Neurogenic: tethered cord, syringomyelia, Chiari
Developmental: Achondroplasia
NF OI
Neuromuscular: Cerebral palsy
Tumour: Osteoid osteoma
BPNST