What is the Preferable Treatment Option for T1/T2 Low Rectal Cancer? Christopher H. Crane, M.D....
20
What is the Preferable Treatment Option for T1/T2 Low Rectal Cancer? Christopher H. Crane, M.D. Program Director, GI Section Program Director, GI Section Department of Radiation Oncology Department of Radiation Oncology
-
Upload
chad-booker -
Category
Documents
-
view
215 -
download
1
Transcript of What is the Preferable Treatment Option for T1/T2 Low Rectal Cancer? Christopher H. Crane, M.D....

What is the Preferable Treatment Option for T1/T2
Low Rectal Cancer?
What is the Preferable Treatment Option for T1/T2
Low Rectal Cancer?
Christopher H. Crane, M.D.Program Director, GI SectionProgram Director, GI Section
Department of Radiation OncologyDepartment of Radiation Oncology
Christopher H. Crane, M.D.Program Director, GI SectionProgram Director, GI Section
Department of Radiation OncologyDepartment of Radiation Oncology

No Disclosures

Complications of Radical Rectal Surgery
• Permanently altered bowel function– Often colostomy
• Urinary dysfunction from 7-68%• Impotence 15-100%• Retrograde ejaculation 3-35%

*RESPONDING PATIENTS
Chemoradiation Followed by Local Excision*

NCDB LE Special Study (1994-96)Local Recurrence – T2
5- Year
LE RR
T2 22% 15%
T2: p=0.01
You et al. Ann Surg 245(5):726-33, 2007
N=164
N=866

German Trial (CAO / ARO / AIO)Pre-operative vs Postoperative CXRT
• Significantly lower acute toxicity rate – 27% vs 40%, p=0.001
• LR improved with preoperative CXRT– 5 yr: 6% vs 13%, p=0.001
• SP higher in preoperative CXRT– 39% vs 19%, p=0.006– Subjective need for APR, not whole group
• Significantly lower late toxicity– 14% vs 24%, p=0.01
• anastamotic stricture (12% vs 4%)• Diarrhea, SBO (9% vs 15%)
Sauer, R NEJM, 351, 2004

Can Radical Surgery Be Avoided in Selected Rectal Cancer
Patients?

CXRT / Mesorectal resection- cT3 N0 ptsypN+ according to ypT stage
Crane, pESTRO 2004
ypT0 in T3 NX (including clinically node +) = 4/45 = 9%
Bedrosian, J Gastroint Surg, 2004
Pathologic T Stage
Institution 1 Institution 2 Institution 3 Total
ypT0 0/27 (0%) 0/14 (0%) 1/43 (2%) 1/84(1%) ypT1 2/29 (7%) 0/12 (0%) 4/17 (24%) 6/58 (10%) ypT2 15/95 (16%) 12/97 (12%) 4/60 (7%) 31/252 (12%) ypT3 54/166 (33%) 62/164 (38%) 15/68 (22%) 131/398 (33%) ypT4 0 5/5 (100%) 2/2 (100%) 7/7 (100%)
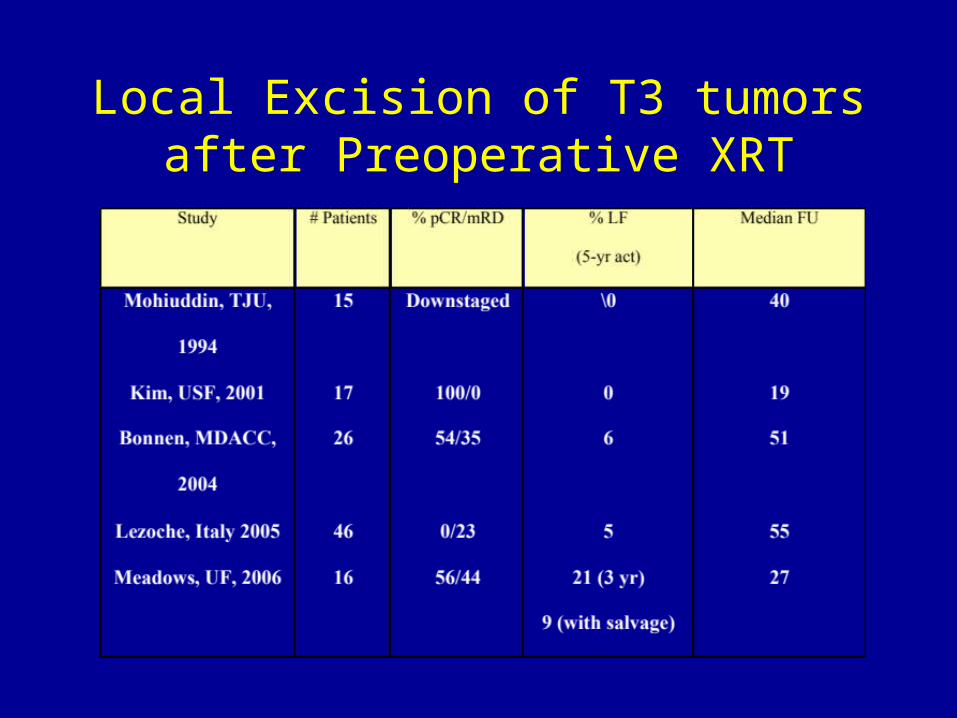
Local Excision of T3 tumors after Preoperative XRT
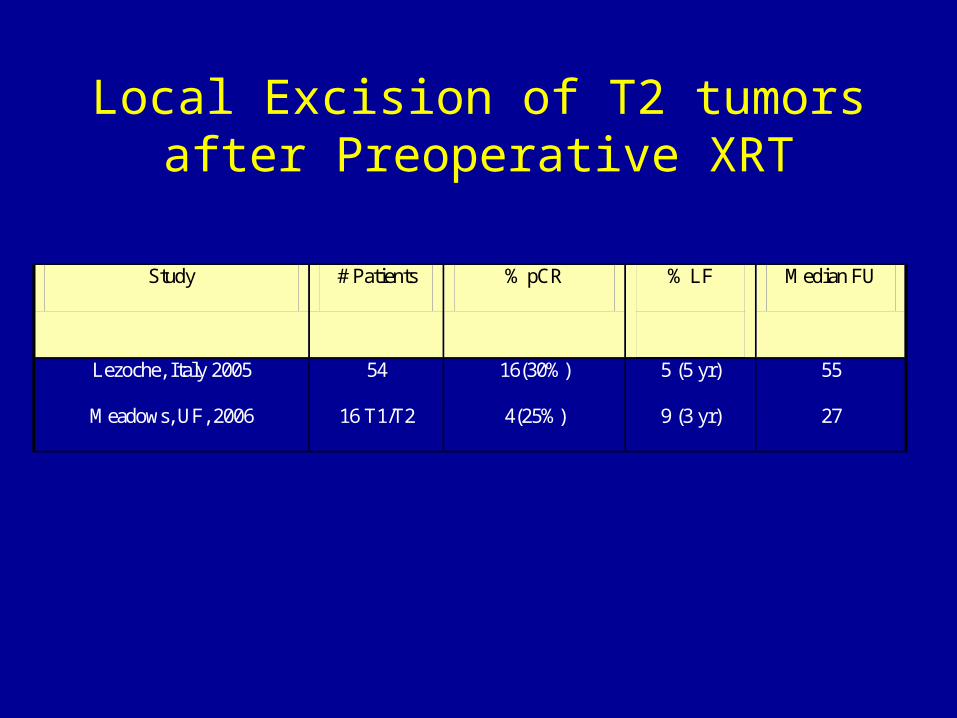
Local Excision of T2 tumors after Preoperative XRT
Study # Patients % pCR % LF
Median FU
Lezoche, Italy 2005 54 16(30%) 5 (5 yr) 55
Meadows, UF, 2006 16 T1/T2 4(25%) 9 (3 yr) 27

ypT stage
All patients -seven studies
LR
T0 0/53 (0%)
T1 1/45 (2%)
T2 6/85 (7%)
T3 7/33 (21%)
Total 17/237 (7%)
Cumulative recurrence rates based on ypT StageCXRT/LE (cT2/cT3)
Modified from Table 5, Borschitz, et al Ann Surg Onc, 2008

Randomized Trial - T2 Rectal Cancer CXRT then TAE vs Laparoscopic Resection
• 40 pts
• 50.4 Gy + PVI 5-FU (200 mg/m2)– 20 TAE– 20 LAP Resection
• One recurrence in each group (5%)
• Median FU 56 mo
Lezoche, et al Surgical Oncology, 2005
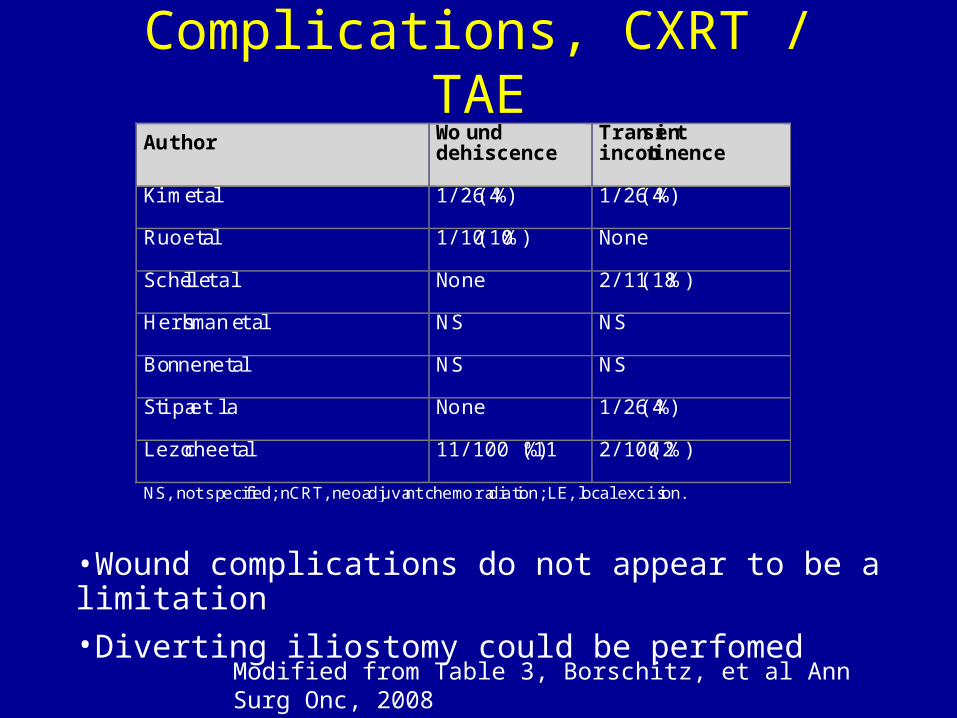
Author Wound dehiscence
Transient incontinence
Kim et al 1/26 (4%) 1/26 (4%)
Ruo et al 1/10 (10%) None
Schell et al None 2/11 (18%)
Hershman et al NS NS
Bonnen et al NS NS
Stipa et al None 1/26 (4%)
Lezoche et al 11/100 (11%) 2/100 (2%)
NS, not specified; nCRT, neoadjuvant chemoradiation; LE, local excision.
Complications, CXRT / TAE
Modified from Table 3, Borschitz, et al Ann Surg Onc, 2008
•Wound complications do not appear to be a limitation
•Diverting iliostomy could be perfomed
Non-operative Management in Complete Responders?
• University of São Paulo, Brazil• Pre-op Chemoradiation (50.4 Gy + FU/LV)• 265 pts
– Clinical CR = observation (n=71, 26%)• 2 endorectal failures, 5y OS 100%
– Incomplete CR / radical surgery, pCR (n=22%, 8.3%)• 2 DOD, 5y OS 88%
• Median follow-up 57.3 months
Habr-Gama, Ann Surg. 240(4):711-718, 2004

ACOSOG Z6041 Study Design
uT2 rectal cancer(EUS-MRI)
CXRTCape (850mg/m2 bid)oxali (50 mg/m2/wk)54 Gy
Local excision
T0-T2 R0: Observation
T3 or R+: radical resection
Follow
<8 cm fromanal verge<4 cm size
Primary Obj: 3 yr DFS in uT2N0
Chan, ASTRO 2010

ACOSOG Z6041 Study Design
uT2 rectal cancer(EUS-MRI)
CXRTCape (650mg/m2 bid)oxali (50 mg/m2/wk)50.4Gy
Local excision
T0-T2 R0: Observation
T3 or R+: radical resection
Follow
<8 cm fromanal verge<4 cm size
Primary Obj: 3 yr DFS in uT2N0
Chan, ASTRO 2010

ConclusionsNeoadjuvant CRT with CAPOX
• 44% pCR
• Only 5% of patients needed radical surgery
• Long term follow-up is needed for LC endpoint
• High GI toxicity rates
Chan, ASTRO 2010
Organ Preservation ModelLocally Advanced Rectal Ca
• Clinical selection will affect success– Tumor size, nodal status, tumor grade, others
• Neoadjuvant CXRT– Endoscopic CR
• Full thickness local excision = excisional biopsy of tumor bed– ypT0, no further surgery
• Radical surgery only for non-responders: – Gross residual disease or ypT3
• What about microscopic residual disease?
Crane, Annals of Surg Onc, (3) p288-90, 2006

Response of Primary Tumor to CXRT
• Observing response of primary key to organ preserving strategy
• Predicts Control of Microscopic Mesorectal Disease
• Could predicting response help?– Only if it leads to personalized therapy– Increase the pool of responders
• Pair agents to patients– Proteomics, genomics
• Change agents during therapy (PET)?

The Message RegardingPre-op/LE
• Promising strategy, especially in responding patients
• Better long term GI and sexual function
• Salvage rates of LR 50-70%– Close FU is critical
• Multidisciplinary team has to be on the same page