
What is the best way to treat the axilla? Jayant S Vaidya MBBS MS DNB FRCSGlag PhD FRCS(Gen Surg) 19...
67
What is the best way to treat the axilla? Jayant S Vaidya MBBS MS DNB FRCSGlag PhD FRCS(Gen Surg) 19 th century 21 st century
-
Upload
jose-mcdonough -
Category
Documents
-
view
217 -
download
1
Transcript of What is the best way to treat the axilla? Jayant S Vaidya MBBS MS DNB FRCSGlag PhD FRCS(Gen Surg) 19...
What is the best way to treat the axilla?
Jayant S VaidyaMBBS MS DNB FRCSGlag PhD FRCS(Gen Surg)
19th century19th century 21st century21st century

ForAxillary Sampling …with a choice of
flavours… Clearance
4-node SampleBlue dye guided Sample
Sentinel Node biopsy
for…A CHOICE
of axillary sampling procedures

Tata Memorial Cancer Centre
Axillary Clearance
Once upon a time…..
Middlesex Hospital, University College LondonMiddlesex Hospital, University College London
Sentinel Node Biopsy
Axillary Clearance
Ninewells Hospital, University of Dundee
Axillary Clearance
Sunshine in Oct
Snowshine in Feb
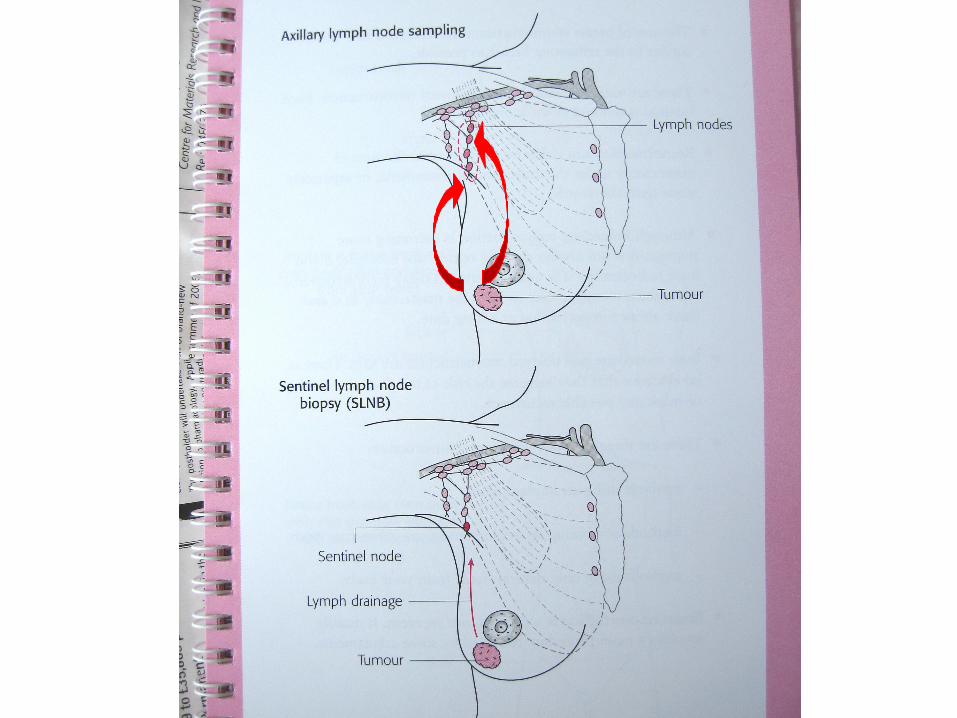
Axillary Sample –
Sentinel Node Biopsy
best of both worlds
False negative rateThe chance of missing a
positive axillaCould cause harm by
Axillary relapse
Missed opportunity to institute systemic adjuvant therapy

How Much?

MathematicalModel
MathematicalModel

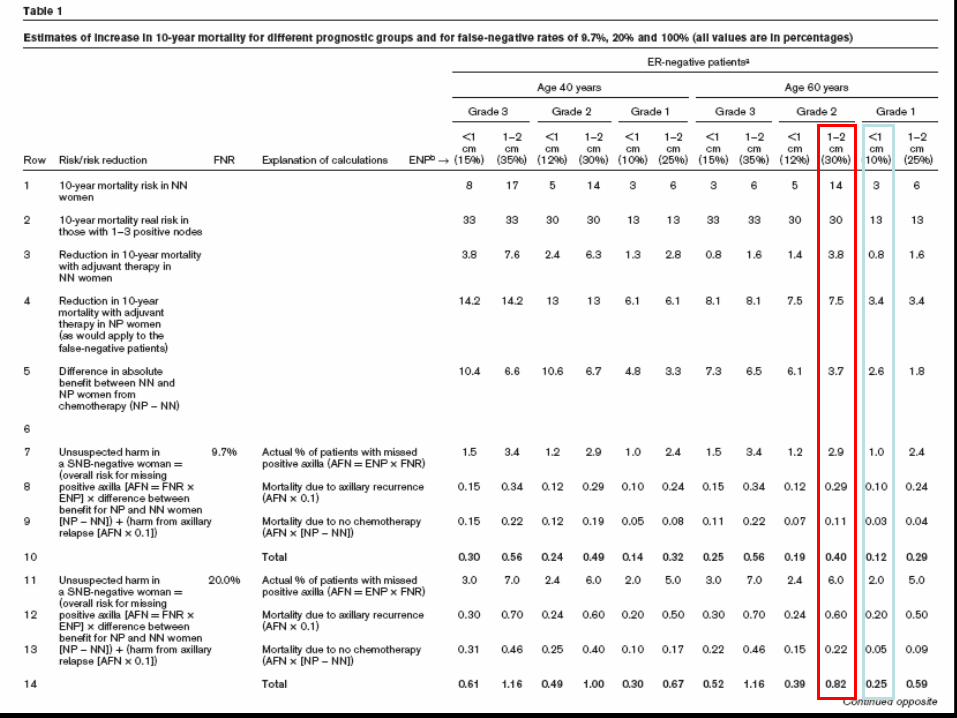
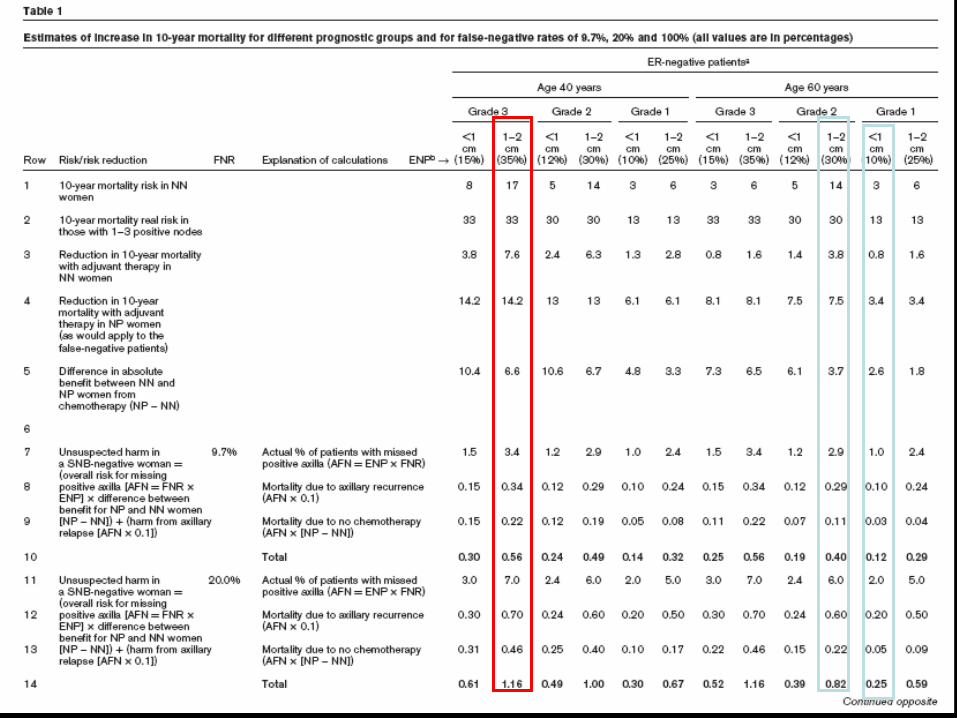
The mathematical model- the known facts
(NSABP B-32) trial False negative rate (FNR)
SEER dataset Estimated node positivity (ENP)
www.adjuvantonline.com Benefit from chemotherapy in ER negative womenThis would be similar to additional benefit of chemotherapy in ER positive women on top of hormone therapy
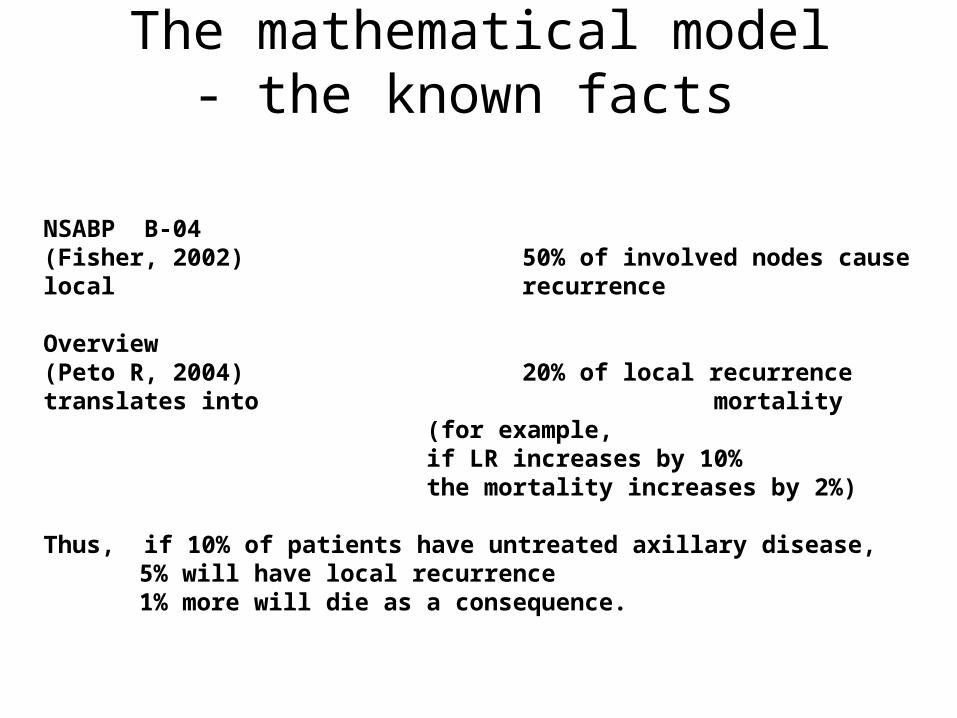
The mathematical model- the known facts
NSABP B-04(Fisher, 2002) 50% of involved nodes cause local
recurrence
Overview(Peto R, 2004) 20% of local recurrence translates into
mortality (for example, if LR increases by 10% the mortality increases by 2%)
Thus, if 10% of patients have untreated axillary disease,5% will have local recurrence1% more will die as a consequence.
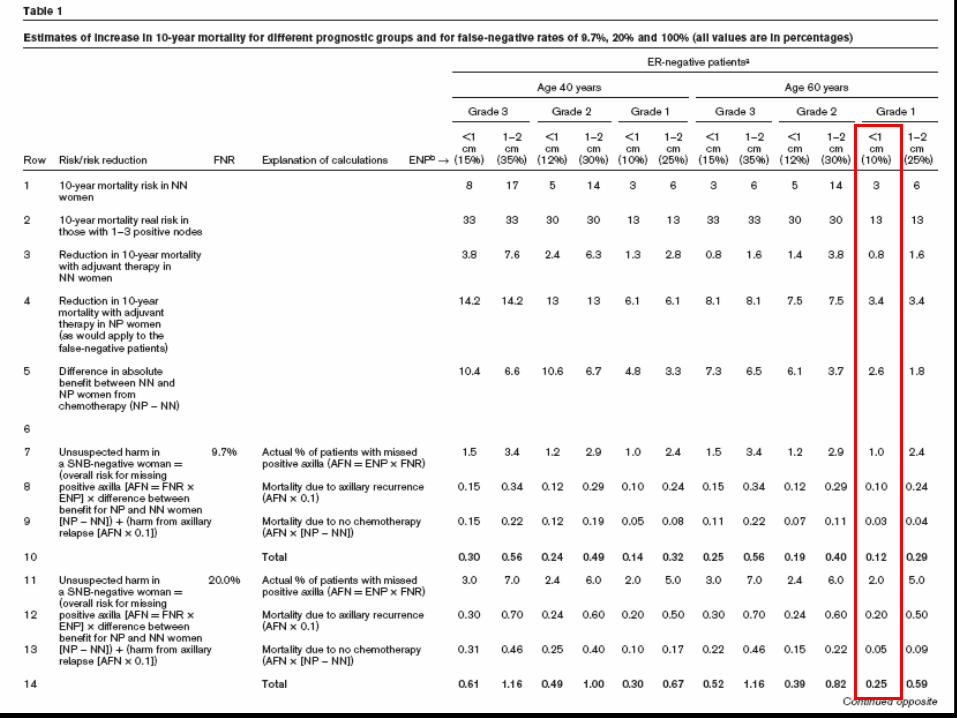
Mathematical Model
•Age 60 years•Grade 1•0.5cm•ER negative•Estimated Node Positivity (ENP) = 10%
The 10-Year mortality risk
Node negative women3%
1 to 3 - Node positive women13%
The Benefit from adjuvant chemotherapy
(reduction in 10 year mortality)
If Node negative(adjuvantonline.com)
0.8%
If (1 to 3) Node positive(adjuvantonline.com)
3.4%
Difference in benefit “if NN” vs. “if NP”
is
3.4% minus 0.8% = 2.6%

Let us assume the False Negative Rate of SNB is
9.7%

Mathematical Model
Actual (chance of )False Negative axilla in this patient undergoing
SNB is =
AFN = FNR x ENP
e.g., if FNR =9.7% and ENP is 10%
AFN= 1%

Mathematical Model
Actual chance of missing a positive axilla in this patient is (AFN=ENP x
FNR)1%
Increased mortality due to axillary recurrence
1/10th of 1% = 0.1%

Mathematical Model
Actual chance of missing a positive axilla in this patient is (AFN=ENP x FNR)
1%
Increased mortality due to “no chemotherapy”
= 2.4% times D (diff. in benefit in NN and NP)
= 1% x 2.6%= 0.02%

Unsuspected harm in this SNB-negative woman (60yrs, 1.5cm, Grade
I, ER-ve) because of omitting chemotherapy on
assumption that she is node negative
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”
0.1% + 0.02% = 0.12%

Tweak…Increase False Negative Rate to
20%
100%

Unsuspected harm in this SNB-negative woman (60yrs, 0.5cm,
Grade i, ER-ve) because of omitting chemotherapy on
assumption that she is node negative(FNR=20%)
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”0.2% + 0.05%
= 0.25%
Unsuspected harm in this SNB-negative woman (60yrs, 0.5cm,
Grade i, ER-ve) because of omitting chemotherapy on
assumption that she is node negative(FNR=100%)
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”1% + 0.26%
= 1.26%

False negative rate does not
matter…

But…
More Tweaks…
Increase tumour size and grade
Grade 2
Size 2cm
Unsuspected harm in this SNB-negative woman (60yrs, 2 cm, Grade
ii, ER-ve) because of omitting chemotherapy on
assumption that she is node negative(FNR=9.7%)
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”0.29% + 0.11%
= 0.4%
Unsuspected harm in this SNB-negative woman (60yrs, 2 cm, Grade
ii, ER-ve) because of omitting chemotherapy on
assumption that she is node negative(FNR=20%)
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”0.6% + 0.22%
= 0.82%
Tweaks…Increase tumour size, grade and reduce age
Grade 3
Size 2cm
Age 40
Unsuspected harm in this SNB-negative woman (40yrs, 2 cm, Grade
iii, ER-ve) because of omitting chemotherapy on
assumption that she is node negative(FNR=9.7%)
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”0.34% + 0.22%
= 0.56%
Unsuspected harm in this SNB-negative woman (40yrs, 2 cm, Grade
iii, ER-ve) because of omitting chemotherapy on
assumption that she is node negative(FNR=9.7%)
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”0.34%0.34% + 0.22%
= 0.56%

Unsuspected harm in this SNB-negative woman (40yrs, 2 cm, Grade
iii, ER-ve) because of omitting chemotherapy on
assumption that she is node negative(FNR=20%)
Increased Mortality due to axillary recurrence
+Increased mortality due to “no
chemotherapy”0.70.7 + 0.46%
= 1.16%

We need to inform our patients and take a shared decision about using Sentinel Node Biopsy?

NSABP B-32 Smoothed False Negative Rates
p = 0.30
Surgeon Case Number
0
20
Per
cen
tag
e F
alse
Neg
ativ
e
0 50 100 150
40
60
NSABP B-32 Smoothed Technical Failure Rates
p < 0.0001
0 50 100 150
0
5
10
15P
erc
en
tag
e T
ech
nic
al F
ailu
re
Surgeon Case Number
We need to accept that this 10% false negative rate is not a correctable technical error
It is an indicator of the biological behaviour of breast cancer

“barking dogs do not bite”
but
the dog doesn’t know that
SNB is appealing because it is precise
and logical But
breast cancer doesn’t know the rules!

In 10% of cases tumour skips the sentinel lymph node
Is there an alternative?
There isan alternative

Replace “dogma” with
“informed choice”

Edinburgh Studies
Prof Bob Steele, Mr Udi Chetty, Sir Patrick Forrest and colleagues
Mastectomy (417)Breast conservation (466)
RANDOMISATION
4- node sample
Axillary clearance
Outcome- local relapse, survival and morbidity
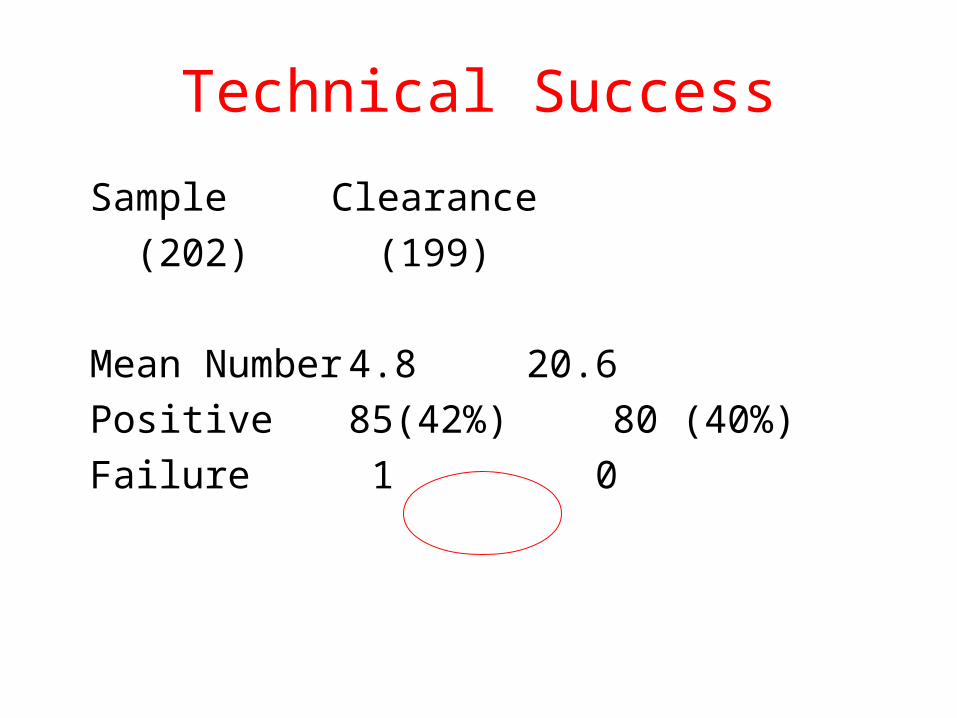
Technical Success
Sample Clearance
(202) (199)
Mean Number 4.8 20.6
Positive 85(42%) 80 (40%)
Failure 1 0

In 135 patients, randomisation was done after sampling
N Positive Additional Positive
Sample only 68 26 (38%) -
Sample+Clearance 67 26 (39%) 0
False negative rate
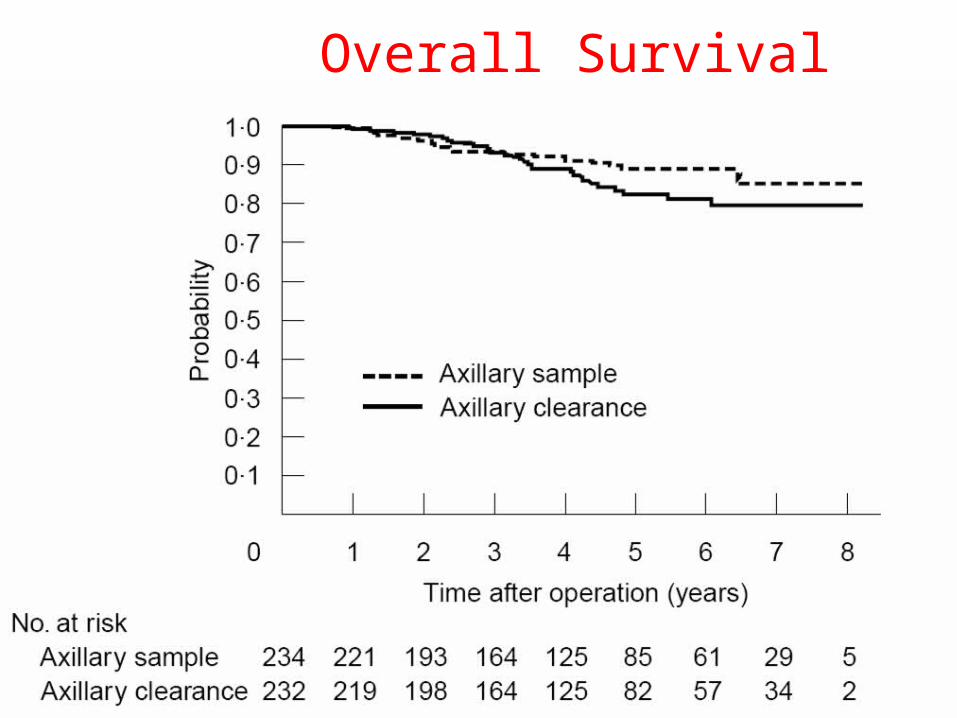
Overall Survival

Axillary Recurrence

Arm Oedema

4-node samplethe Edinburgh technique
Near 100% detection rate
Near 0% false negative rate
Low morbidity
Survival and local relapse equivalent
4-node sample - Other benefits
• No need of costly equipment
• No need of Nuclear medicine and ARSAC
• No need of radiation protection
• Needs proper surgical training

Study of biology of Biological tissues are NOT contaminated
with radiation
So can be stored in tissue bank for further study – e.g., gene microarray analysis.
RADIATION HAZARD
Applying the Mathematical model to 4 node sampl e
• FNR = 0%
• Effect of mortality = 0
• Effect of local recurrence = 0

Node positivity in trials of SNB
26%
On average,
1 in 4 patients have a second operation

Patient Choice
A. ¾ chance of an unnecessary axillary procedure, but the full treatment is completed in one operation (AC)
B. ¼ chance of 2nd operation + 1/10 chance of a missed positive node (SNB)
C. ¼ chance of a 2nd procedure + 0 chance of a missed positive node (AS)

What is the right way?
INFORMED CHOICE AND PATIENT SELECTION
• Those with high risk of nodal metastasis= Axillary clearance
• Those with medium risk of nodal metastasis = Axillary sample
• Those with low risk of nodal metastasis =Sentinel node biopsy (don’t bother about FNR)

REMEMBER WHEN YOU VOTE
• If you Vote for the action then you are
voting for a choice – surgeon choice and patient choice- in different ways of sampling the axilla – Clearance-Sample-SNB
• If you Vote against the action then you are voting against such an informed and wise choice – and NOT for Sentinel node biopsy.
Remember
VOTING AGAINST this action is NOT the same as to VOTING
FOR SNB
So if you believe that SNB is
A right way then you should vote FOR the
action

Vote for choice
If you believe that Surgeons and
Patients should be allowed to
make an informed choice
Vote for the action
If you wish to just replace the
dogma of Axillary
clearance to the dogma of Sentinel node
biopsy
Vote against the action
























