
What is Cancer? Disorder of cell growth and behavior Proliferate in the absence of normal growth...
42
What is Cancer? • Disorder of cell growth and behavior • Proliferate in the absence of normal growth regulatory signals • Malignancies arise in populations of immature or undifferentiated cells – Loss of tumor suppressor gene products (p53, Rb) – Activation of proto-oncogenesis (ras, c-myc) – Somatic mutations • DNA translocations • Gene amplification • Cells can multiply at a rate of about 2 divisions each day. • Single cell can give rise to a detectable mass of 1g (10 9 cells) in just 15days. • Tumors are “altered self” cells that maintain similarities to “normal cells” making it difficult to target cancer cells specifically
-
Upload
gregory-watson -
Category
Documents
-
view
214 -
download
1
Transcript of What is Cancer? Disorder of cell growth and behavior Proliferate in the absence of normal growth...

What is Cancer?
• Disorder of cell growth and behavior• Proliferate in the absence of normal growth regulatory
signals
• Malignancies arise in populations of immature or undifferentiated cells
– Loss of tumor suppressor gene products (p53, Rb)– Activation of proto-oncogenesis (ras, c-myc)– Somatic mutations
• DNA translocations• Gene amplification
• Cells can multiply at a rate of about 2 divisions each day. • Single cell can give rise to a detectable mass of 1g (109
cells) in just 15days.
• Tumors are “altered self” cells that maintain similarities to “normal cells” making it difficult to target cancer cells specifically

2007 Estimated US Cancer Cases*
*Source: American Cancer Society, 2007.
Children 0-14years, 15-100,000 cases, 2.5-100,000 deaths
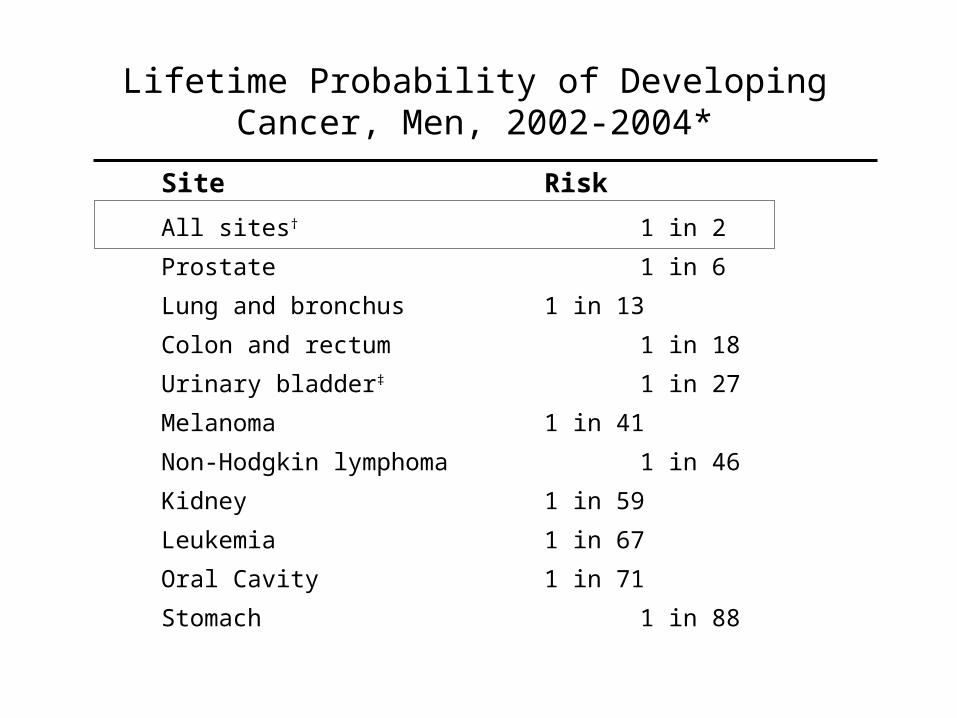
Lifetime Probability of Developing Cancer, Men, 2002-2004*
Site Risk
All sites† 1 in 2
Prostate 1 in 6
Lung and bronchus 1 in 13
Colon and rectum 1 in 18
Urinary bladder‡ 1 in 27
Melanoma 1 in 41
Non-Hodgkin lymphoma 1 in 46
Kidney 1 in 59
Leukemia 1 in 67
Oral Cavity 1 in 71
Stomach 1 in 88

Lifetime Probability of Developing Cancer, Women, US, 2002-2004*Site Risk
All sites† 1 in 3
Breast 1 in 8
Lung & bronchus 1 in 16
Colon & rectum 1 in 19
Uterine corpus 1 in 41
Non-Hodgkin lymphoma 1 in 53
Melanoma 1 in 61
Ovary 1 in 71
Pancreas 1 in 76
Urinary bladder‡ 1 in 85
Uterine cervix 1 in 142

Trends in Five-year Relative Survival (%)* Rates, US, 1975-2003
Site 1975-1977 1984-1986 1996-2003
• All sites 50 54 66
• Breast (female) 75 79 89
• Colon 51 59 65
• Leukemia 35 42 50
• Lung and bronchus 13 13 16
• Melanoma 82 87 92
• Non-Hodgkin lymphoma 48 53 64
• Ovary 37 40 45
• Pancreas 2 3 5
• Prostate 69 76 99
• Rectum 49 57 66
• Urinary bladder 74 78 81
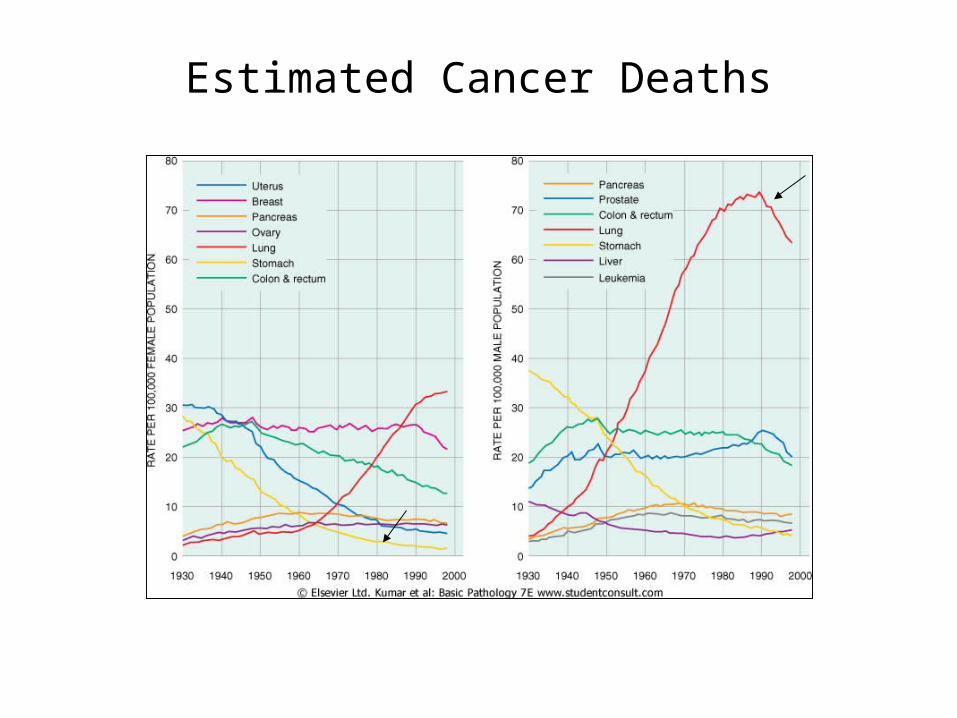
Estimated Cancer Deaths
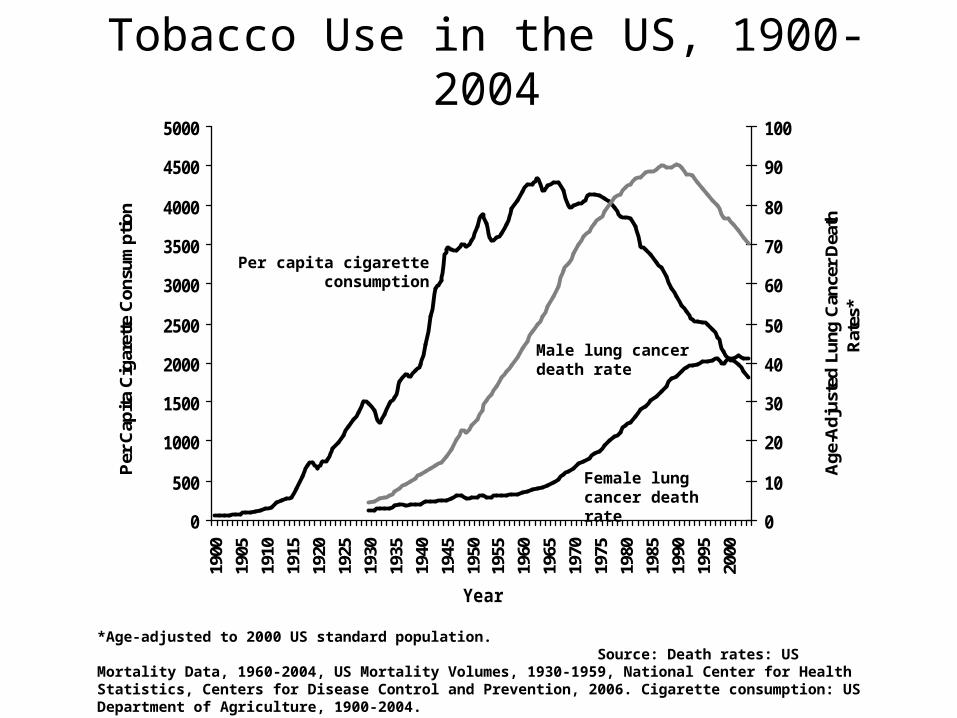
Tobacco Use in the US, 1900-2004
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
1900
1905
1910
1915
1920
1925
1930
1935
1940
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
Year
Per
Cap
ita C
igar
ette
Con
sum
ptio
n
0
10
20
30
40
50
60
70
80
90
100
Age
-Adj
uste
d Lu
ng C
ance
r D
eath
R
ates
*
*Age-adjusted to 2000 US standard population. Source: Death rates: US Mortality Data, 1960-2004, US Mortality Volumes, 1930-1959, National Center for Health Statistics, Centers for Disease Control and Prevention, 2006. Cigarette consumption: US Department of Agriculture, 1900-2004.
Per capita cigarette consumption
Male lung cancer death rate
Female lung cancer death rate
Basic terminology/nomenclature
• Cancer– Disorder of cell growth and dysregulation
• Neoplasia– “New growth”– Depends on the host for nutrition and blood supply– Aka “tumor”
• Benign• Malignant
Cancer Therapy• Surgery
– Most effective form of treatment for cancer– Most aggressive.– Confined to particular anatomical site (if identifiable)– Can be used in together with other treatments
• Radiation– Used for local treatment– Can be used as sole treatment or in conjunction with another form of treatment– Mechanism:
• High energy radiation kills cells by damaging the DNA of the cancer cells and blocking their ability to divide and proliferate.
• Chemotherapy– Typically used together with surgery
• Post-surgery = to eliminate undetectable disease– Called adjuvant therapy
• Pre-surgery – Called neoadjuvant
– Requires multiple cycles of treatment

R
Cell decides whether to continue

Categories of Chemotherapeutic Agents
1. antimetabolites
a. non-base analogs: methotrexate, hydroxyureab. pyrimidine analogs: 5-flurouracil, cytarabinc. purine analogs: 6-mercaptopurine (6-MP), 6-thioguanine
2. topoisomerase Inhibitors: etoposide, teniposide
3. microtubule inhibitors: vincristine, vinblastine, paclitaxel
4. antitumor antibiotics: doxorubicin, bleomycin, dactinomycin
5. alkylating agents: mechlorethamine, cyclophosphamide, cisplatin
6. hormones: prednisone, tamoxifen
7. other: procarbazine, endostatin, angiostatin, Campath®

Antimetabolites
• false substrates, structurally related to normal cellular components
• S phase specific, DNA synthesis
• many are nucleic acid base analogs and can get incorporated into DNA or RNA
• others inhibit enzymes involved in nucleotide biosynthesis & metabolism
Types of Antimetabolites:a. Folic acid analogues: methotrexate, hydroxyureab. Pyrimidine analogues: 5-flurouracil, cytarabinc. Purine analogues: 6-mercaptopurine, 6-thioguanine

Folic Acid Analogues
1. Methotrexate (MTX)
FH2 ----------------->FH4
methotrexate folic acid
• In clinical use to treat cancer since 1948.• An antagonist of Dihydrofolate reductase (DHFR) –similar in structure to folic acid• Inhibits DHFR to cease production of tetrahydrofolate (FH4) – an active cofactor
required for thymidylate synthetase and purine synthesis• large doses of MTX are toxic to normal cells – deprives the cells of the various
folate coenzymes• normal cells can be rescued by administering relatively low levels of folinic acid
which is converted to FH4 independent of DHFR• Due to interference with folic acid, also used in treatment of types of arthritis.• S-phase specific drug
DHFR

Pyrimidine Analogues
1. 5’ Flurouracil (5‑FU)
dUMP ------------------------------->dTMP (2’-deoxythymidylate) ---------->DNA Synthesis
• Inhibits DNA synthesis• Principally used as a thymidylate (dTMP) synthase inhibitor.• Interrupts action of an enzyme which is critical in synthesis of pyrimidine
(thymine) which is important in DNA replication.• It is a S-phase specific drug• 5‑FdUMP can also get incorporated into DNA and lead to strand breakage• primarily used in treatment of slowly growing, solid tumors (breast, ovarian,
pancreatic)
2. Cytarabine (Ara-C)
• incorporated into DNA and causes chain termination• It is a S-phase specific drug• clinical use in acute nonlymphocytic (myelogenous) leukemia

Purine Analogues
6-MP --------------------------- 6-MPRP (6-mercaptopurine ribose phosphate, thiol analog Hypoxanthine-guanine of hypoxanthine) Phosphoribosyl Transferase
• unnatural nucleotide inhibits purine ring biosynthesis • dysfunctional RNA and DNA result from incorporation of guanylate
analogs• 6-MP is metabolized by xanthine oxidase, the dose of 6-MP must be
reduced when allopurinol is given• When used with allopurinol:
• Allopurinol inhibits xanthine oxidase which prevents oxidation of 6-MP• Inhibits inactivation of 6-MP
• Toxicity of 6-MP are potentiated!
• 6-MP is used in the maintenance of remission in acute lymphoblastic leukemia (ALL)
1. 6-mercaptopurine (6-MP)
(aka Purinethol)

Topoisomerase Inhibitors
• Topoisomerase – Enzyme involved in replication and segregation of bacterial DNA.– Topoisomerase enzymes (I and II) control changes in DNA structure
• Topoisomerase Inhibitors:– Interferes with action of topoisomerase enzymes (topoisomerase I and
II) • Blocks ligation step of cell cycle• Therefore interferes with transcription and replication of DNA
• Examples of Topoisomerase Inhibitors:– Etoposide– Teniposide
Etoposide and Teniposide
• Etoposide Phosphate– Brand name: Eposin, Etophphos, VP-16– Inhibits topoisomerase II– Typically given to patients diagnosed with lung cancer, testicular cancer,
leukemia– Administered: orally, intravenously– Often given in combination with drugs that damage DNA directly (bleomycin or
cisplatin)
• Teniposide– Brand name Vumon ,VM-26– Typically given to treat childhood acute lymphocytic leukemia– Slows growth of cancer cells in body– Administered through injection– Major side effect:
• Lowers WBC• Lowers platelet count• Bone marrow suppression
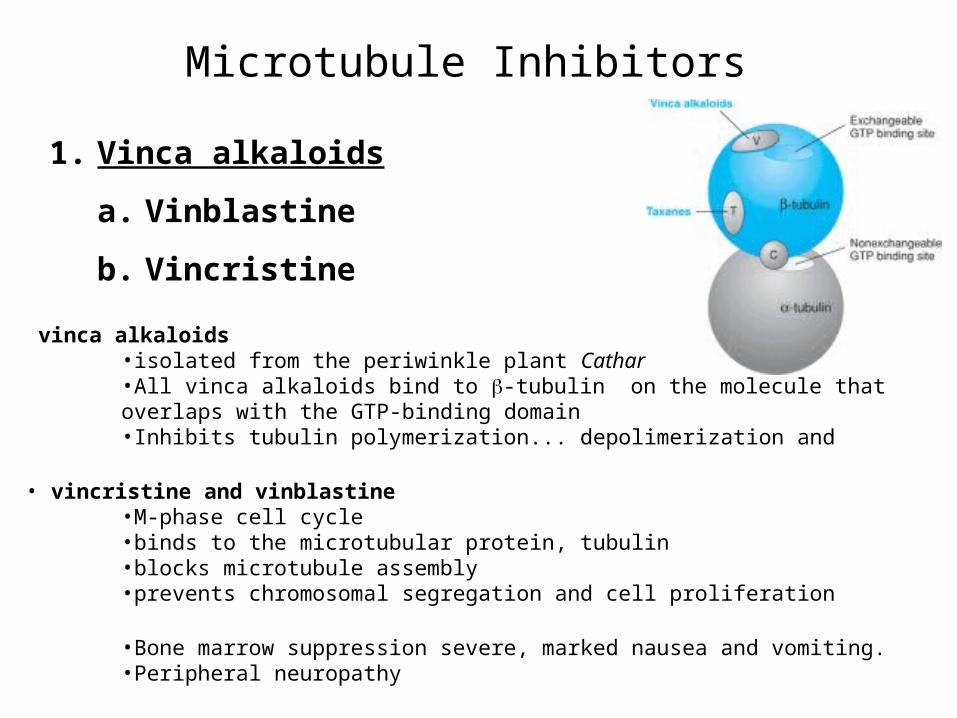
Microtubule Inhibitors
1. Vinca alkaloids
a. Vinblastine
b. Vincristine
vinca alkaloids •isolated from the periwinkle plant Catharantus roseus•All vinca alkaloids bind to -tubulin on the molecule that overlaps with the GTP-binding domain•Inhibits tubulin polymerization... depolimerization and
• vincristine and vinblastine•M-phase cell cycle •binds to the microtubular protein, tubulin•blocks microtubule assembly•prevents chromosomal segregation and cell proliferation
•Bone marrow suppression severe, marked nausea and vomiting.•Peripheral neuropathy

• Taxanes
a. Paclitaxel (taxol)
• isolated from the bark of the western yew tree
• Taxanes
•binds to -tubulin subunit inside the microtubules at distinct site from vinca alkaloids
•Promotes microtubule polymerization and inhibit depolymerization
•Irreversibly stabilizes cells in Mitosis leading to apoptosis.
•Paclitaxel
•Interferes with normal microtubule growth by hyperstabilizing microtubule function--overly stable microtubules are dyfunctional
•Binds to tubulin and promotes polymerization and stabilization of the polymer rather than disassembly
•Irreversibly stabilizes cells in mitosis leading to apoptosis.
Antitumor Antibiotics
• first isolated as red substances from microorganisms in 1939
• members of the Anthracycline antitumor antibiotic family
•G2 phase specific
•despite their severe cardiotoxicity, these drugs have been widely used as chemotherapeutic agents for the treatment of cancers such as leukemia since their discovery in the early 1960's
• the cytotoxicity arises from an intercalation of the drug between the base pairs of the DNA using non-covalent interactions and interfering with DNA replication
• also, hydroxyl radicals (OH·) can be generated, which can damage proteins, membranes and DNA and stop cell growth
1. Daunorubicin and Doxorubicin

Cartoon diagram of two doxorubicin molecules intercalating DNA
From protein data bank
The planar aromatic chromophore portion of the molecule intercalates between two base pairs of the DNA, while the six-membered daunosamine sugar sits in the minor groove and interacts with flanking base pairs immediately adjacent to the intercalation site, as evidenced by several crystal structures.
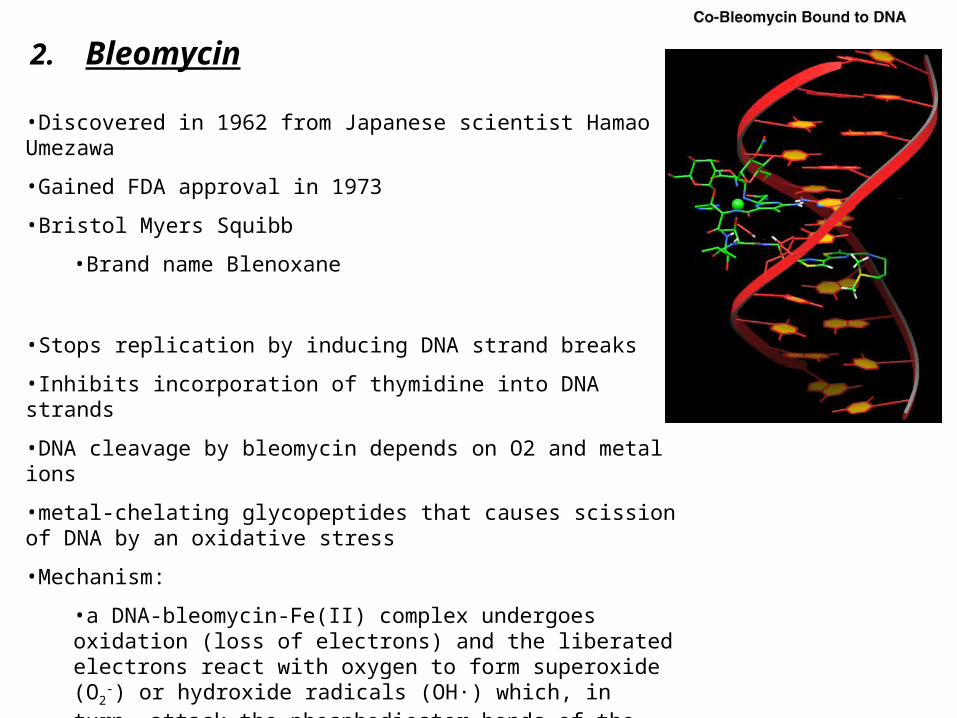
•Discovered in 1962 from Japanese scientist Hamao Umezawa
•Gained FDA approval in 1973
•Bristol Myers Squibb
•Brand name Blenoxane
•Stops replication by inducing DNA strand breaks
•Inhibits incorporation of thymidine into DNA strands
•DNA cleavage by bleomycin depends on O2 and metal ions
•metal-chelating glycopeptides that causes scission of DNA by an oxidative stress
•Mechanism:
•a DNA-bleomycin-Fe(II) complex undergoes oxidation (loss of electrons) and the liberated electrons react with oxygen to form superoxide (O2
-) or hydroxide radicals (OH·) which, in turn, attack the phosphodiester bonds of the DNA, resulting in strand breakage and chromosomal damage
Side-EffectsCan cause pulmonary toxicity
2. Bleomycin

Alkylating Agents
•most important step is the formation of a carbonium ion (a carbon atom with only six electrons in its outer shell) which reacts instantaneously with an electron donor such as amine, hydroxyl or sulfhydryl groups
• most alkylating agents are bi-functional, i.e. they have two alkylating groups capable of reacting with two groups on the DNA and causing intra- or interchain cross-linking
• cross-linking DNA strands and interferes with transcription and DNA replication•leads to excision of the guanine base and pairing of the alkylated guanine with thymine instead of cytosine
•Cells cannot separate and divide
•Nonspecific cell cycle phase
• although alkylating agents may be used for most types of cancer, they are generally of greatest value in treating slow-growing cancers
• these chemotherapy drugs not only affect the cancer cells but also disrupt normal cell growth in progress--in the lining of the gastrointestinal tract, blood cells, hair, nails and are closely linked to the development of secondary cancers
1. Cyclophosphamide• Generic name = Cytoxan, Neosar• Is classified as a nitrogen mustard alkylating agent• Used to treat lymphomas and some solid tumors• Slows/stops cell growth• Also, works by decreasing the immune system’s response to various
diseases
• Mechanism:– first needs to be activated by biotransformation with P450 mixed function oxidase
to hydroxylated intermediates which, in turn, undergoes breakdown to form the active compounds, phosphoramide mustard and acrolein
– inserts foreign molecules into the genetic material of dividing cancer cells which kills cells by disrupting their normal function and by preventing their further growth and multiplication

2. Mechlorethamine (aka nitrogen mustard)
• Mustard gas derived from chemical warfare in 1943– Exposed civilians and soldiers had decreased WBC suggesting
possibility as a chemotherapy – Used in treatment of Hodgkin’s disease or non-Hodgkin’s lymphoma– Stops cell growth by facilitating DNA strand breaks
• Mechanism:– Drug loses a chloride ion and forms a reactive intermediate that alkylates the N7
nitrogen of a guanine residue in one or both strands of a DNA molecule– alkylation leads to cross-linkages between guanine residues and/or depurination
that facilitates DNA strand breakage

• 3. Cisplatin (diaminedichloroplatinum (DDP))
• first synthesized by M.Peyrone in 1844 and called Peyrone’s chloride• in 1960’s, B.Rosenberg at the Michigan State University designed and
experiment to measure the effects of electrical current on cell growth yielding E.coli that were 300 times the normal length
• the effect was found to be due to a chemical agent formed in the reaction between the supposedly inert Pt electrode and components of the solution
• Prevents cell division without retarding cell growth, leading to elongation• Kills cancer cells by binding to basic site of DNA and interfering with its
repair mechanism• DNA repair enzymes are recruited to the site and become irreversibly
bound, preventing repair

Hormones
• Tamoxifen
• tamoxifen blocks the action of estrogen in breast tissue by binding to the estrogen receptors of breast cells, thereby preventing estrogen molecules from binding to these receptors
• unlike estrogen, binding of tamoxifen to the receptor does not cause the receptor molecule to acquire the changed shape needed for binding to coactivators and cell proliferation cannot be activated
• unlike normal breast cells, cancer cells arising in the breast do not always have receptors for estrogen
• the growth of estrogen receptor-negative cancer cells is not governed by estrogen and cannot be treated with tamoxifen

Tamoxifen
while tamoxifen acts as an antiestrogen that blocks the effects of estrogen on breast cells, it mimics the actions of estrogen in other tissues such as the uterus
its estrogen-like effects on the uterus stimulate proliferation of the uterine endometrium and increases the risk of uterine cancer

Cell Cycle specificity of antineoplastic drug classes
• some agents are "cell cycle" active i.e. predominantly cytotoxic to actively cycling cells
1. Antimetabolites: S phase
2. Microtubule Inhibitors: M phase
• others can be cytotoxic at any phase of cell cycle
1. prednisone 2. alkylating agents
Combination Chemotherapy
• Multi-therapy regimen:– Reduces toxicity to the host– Reduces resistance to drug– To enhance activity (efficacy) of drug therapy against infection– To treat multiple simultaneous infections (aka polymicrobial infections)
– Introduces potential for multiple adverse effects and drug interactions
• Goal– To efficiently remove offending pathogen or tumor without incurring
unacceptable toxicity in host.
Synergy, Additivity, Antagonism
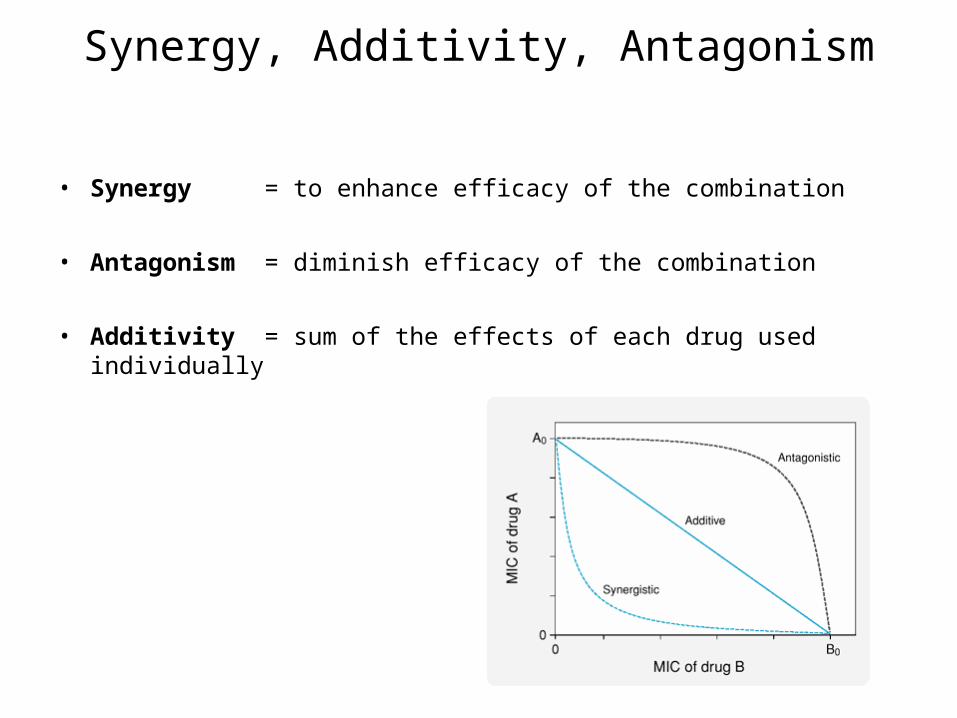
• Synergy = to enhance efficacy of the combination
• Antagonism = diminish efficacy of the combination
• Additivity = sum of the effects of each drug used individually
Examples of antineoplastic combination chemotherapy pp730
• Stage of disease determines treatment
• Hodgkin’s Disease– Prior to 1960s, single drug chemotherapy resulted in median survival of 1 year– MOPP (mechlorethamine, vincristine, procarbazine, prednisone)
• From this combination, 50% of these patients were cured• Significant toxicity
– ABVP (doxorubicin, bleomycin,vinblastine, dacarbazine)• Just as effective as MOPP• Less toxic
• Testicular Cancer:– PVB (cisplatin, vinblastine and bleomycin)

More examples of Combination therapy
• Leucovotin (5-FU/folinic acid)– 5-FU (Fluorouracil)
• Pyrimidine analog
• Inhibits thymidylate synthesis
– Folinic acid (leukovorin)• Enhances effect if 5-FU on inhibiting thymidylate synthase by
increasing MTHF.
– First line of treatment for colon cancer

Promising new approach in treating breast cancer
• PARP (Poly [ADP-ribose] polymerase) – Enzyme involved in repairing DNA damage and programmed cell death– Assists in repairing single-stranded DNA nicks
• PARP inhibitors– Potential in effectively killing tumor cells in women with variation in BRCA1 and BRCA2 genes.– Less toxic to healthy cells– How does this work:
• New class of drugs, PARP inhibitors are designed to exploit specific genetic make-up of some tumor cells
• Repairs damaged DNA
• Studies:– PARP1 deficient mice– -human cells in culture are treated with PARP1 inhibitors
• Normal human cells undergo/capable of normal cell division• human cells deficient in BRCA1 or BRCA2 are killed in response to PARP1 inhibitors.

Human aspartyl (asparaginyl) beta-hydroxylase (HAAH)
• HAAH is a cancer molecular marker that has been detected by immunohistochemical staining in a broad range of cancers; this marker was originally discovered at the Rhode Island Hospital / Brown University
• HAAH gene is up-regulated in human malignancies such as breast, colon, liver, and bile duct tumor.
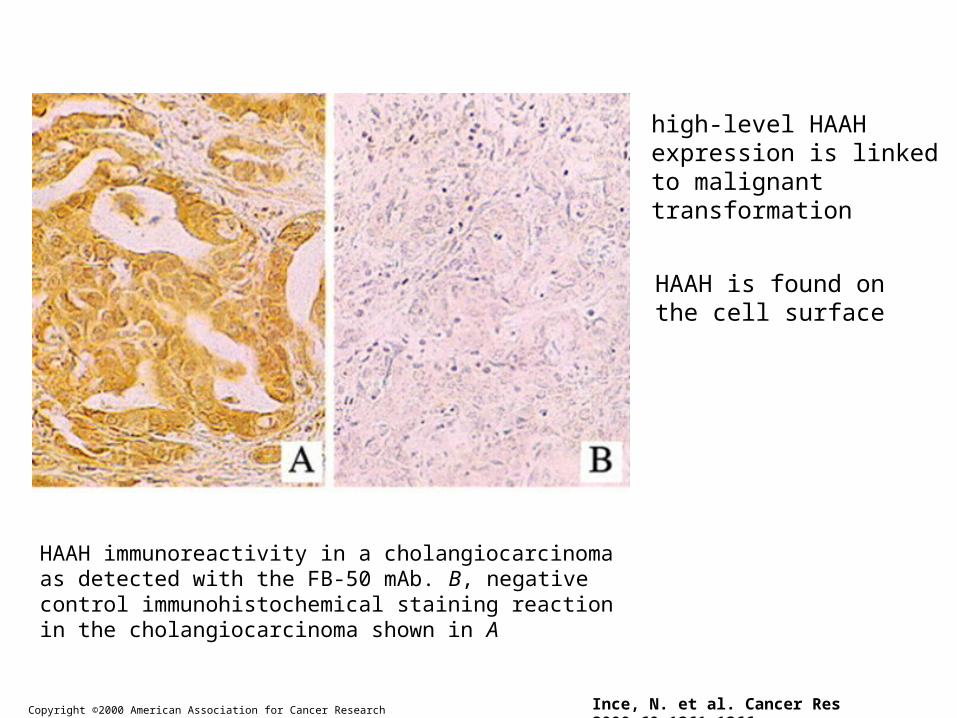
Copyright ©2000 American Association for Cancer Research Ince, N. et al. Cancer Res 2000;60:1261-1266
HAAH immunoreactivity in a cholangiocarcinoma as detected with the FB-50 mAb. B, negative control immunohistochemical staining reaction in the cholangiocarcinoma shown in A
high-level HAAH expression is linked to malignant transformation
HAAH is found on the cell surface

HAAH antibody staining in lung cancer

Tumor formation in nude mice that received injections of transfected clones overexpressing murine AAH
Ince, N. et al. Cancer Res 2000;60:1261-1266Copyright ©2000 American Association for Cancer Research
high-level HAAH expression is linked to the malignant progression and invasiveness of multiple cancers.

Three weekly IP injections of anti-HAAH antibody decrease tumor growth in a xenograft model of primary human liver cancer

Panacea Pharmaceutics
• PAN-622, is an all-human sequence anti-HAAH monoclonal antibody being developed as a cancer therapeutic antibody drug and the start of Phase 1 clinical trials are anticipated in early 2009
• PAN-622 inhibited tumor growth in 90 percent of animals, with 40 percent showing no visible tumor. Tumors did not re-grow beyond the period of drug administration.
• Prevents tumor growth.– Chronic treatment– Linkage to toxin

Summary
• Tumors are “altered self” cells that maintain similarities to “normal cells” making it difficult to target cancer cells specifically
• Cancer therapies include:– Surgery
– Radiation
– Chemotherapy
• Multi therapies
• Multi-drug regimen


















