Unit Six Success preparation Listening-centered Activities Reading-centered Activities.

Journal of Pediatric Nursing (2014) xx, xxx–xxx
What Impact Do Hospital and Unit-Based RulesHave Upon Patient and Family-Centered Care inthe Pediatric Intensive Care Unit?
Jennifer Baird, PhD, MSW, RNa,⁎, Betty Davies, PhD, RN, FAANb,Pamela S. Hinds, PhD, RN, FAANc, Christina Baggott, PhD, RN, PNP-BCd,Roberta S. Rehm, PhD, RN, FAANaaUniversity of California, San Francisco School of Nursing, San Francisco, CAbUniversity of Victoria School of Nursing, Victoria, BC, CanadacChildren's National Medical Center, Washington, DCdStanford University Pediatric Oncology, Palo Alto, CA
Received 1 June 2014; revised 29 September 2014; accepted 3 October 2014
h0
Key words:Patient and family-centered care;
Pediatric intensivecare unit;
Children with complexchronic conditions
Patient and family-centered care (PFCC) is the foundation for pediatric healthcare. The existence of hospitalrules can, however, impact the extent to which PFCC is delivered. This qualitative, grounded theory studyidentified the existence of explicit and implicit rules in a pediatric intensive care unit, all of which negativelyaffected the family's ability to receive care that was attentive to their needs. The rules also placed the registerednurse in the challenging position of serving as rule enforcer and facilitator of PFCC. Further work is needed toexplore how to adapt the hospital environment to better meet families' needs.© 2014 Elsevier Inc. All rights reserved.
Background
AS THE NUMBER of children in the United States withcomplex chronic conditions (CCC) grows, so too does ourunderstanding of their unique care needs and the dailychallenges faced by family members as they provide thiscare. An extensive body of literature now exists that definesand describes this group of children (Feudtner, DiGiuseppe,& Neff, 2003; Gordon et al., 2007; Harrigan, Ratliffe,Patrinos, & Tse, 2002; Srivastava, Stone, & Murphy, 2005)and that identifies the unique challenges they and theirfamilies face in navigating the healthcare system and
⁎ Corresponding author: Jennifer Baird, PhD, MSW, RN.E-mail address: [email protected].
ttp://dx.doi.org/10.1016/j.pedn.2014.10.001882-5963/© 2014 Elsevier Inc. All rights reserved.
engaging in life in the “normal” world (Kirk, Glendinning,& Callery, 2005; Ray, 2002; Reeves, Timmons, & Dampier,2006; Rehm & Bradley, 2005a, 2005b). The literature thathas accumulated over the past 25 years has contributed toimprovements in care for these children and their families,but it has also raised questions about current care deliverysystems and identified gaps in our knowledge base. Amongthe most significant of those gaps is how to help HCPsdevelop the skills necessary to build strong workingrelationships with families, thereby promoting optimal carefor some of our most vulnerable children.
Patient and family-centered care (PFCC), a model thatrecognizes the family as expert in the care of their child andthat seeks to establish and maintain a partnership betweenfamily and provider, is the gold standard in pediatrics and iswidely accepted as the philosophy of care upon whichoptimal pediatric healthcare practice is built. Professionalorganizations and government agencies have endorsed

2 J. Baird et al.
PFCC, and it has become an established part of thecurriculum in programs that train future pediatric providers(American Academy of Pediatrics, 2012; American NursesAssociation, 2008). The following components are generallyconsidered to be key elements of the PFCC model: respectfor family preferences; flexibility and customization of care;honest information sharing to promote participatory deci-sion-making; collaboration across all levels of the healthcaredelivery system; and a strengths-based approach to workingwith patients and families (American Academy of Pediatrics,2012; Institute for Patient and Family-Centered Care, 2010;Jolley & Shields, 2009; Malusky, 2004; Mikkelsen &Frederiksen, 2011; Shields et al., 2012). Despite widespreadacceptance of the concepts of PFCC, implementation hasremained a challenge in pediatric healthcare settings, withfamilies reporting widely disparate experiences in the qualityand family-centeredness of the care they receive (Balling &McCubbin, 2001; Davies, Baird, & Gudmundsdottir, 2013;Graham, Pemstein, & Curley, 2009). The inpatient, acutecare setting has historically not provided optimal PFCC andhas particularly struggled with the PFCC concepts of respectfor family preferences and flexibility and customization ofcare. Traditional practices such as visitation restrictions andfamily exclusion from care planning and the roundingprocess have limited the extent to which PFCC was achieved(Meert, Clark, & Eggly, 2013; Uhl, Fisher, Docherty, &Brandon, 2013). Children with CCC and their families arethe ones most in need of this type of care, and a failure toengage the family in a partnership and to recognize theexpertise that they have regarding the care of their child canhave detrimental effects upon the family and can result inunnecessary, wasteful, and potentially harmful care.
Yet, some families do experience care that acknowledgesand respects the expertise they bring; there are healthcareproviders who embrace the concept of PFCC and consis-tently incorporate it into their practice (Davies et al., 2013).Efforts to improve the quality of care for children,particularly for those with CCC, must focus on theseproviders, understanding how they engage with familiesand how they operate within the busy and complex context ofthe modern healthcare environment. The pediatric intensivecare unit is a natural setting in which to explore interactionswith such providers because it is a high-stress, high-stakesenvironment with rapidly-evolving care situations necessi-tating frequent and, at times, complex communication withfamilies. Further, a large percentage of the patients whoreceive care in the PICU are children with CCC (Edwardset al., 2012; Namachivayam et al., 2012).
The data presented in this paper are one component of theanalysis from a qualitative, grounded theory study, theoverall goal of which was to identify best practices in parent/nurse interactions in the pediatric intensive care unit (PICU)setting for the parents of children with CCC. Some of thestrongest themes from the data centered around the existenceand enforcement of rules in the PICU and the implicit rules,or social norms (Bicchieri, 2006), that guided practice in that
environment. Emerging from these themes was an under-standing of the ways in which the model of PFCC, ascurrently conceptualized, fails to adequately account for thecontext in which parent/nurse interactions are occurring andthe ways in which existing social norms may run counter tothe goal of delivering optimal PFCC. This paper adds to theexisting literature by exploring these two important contex-tual factors that challenge the delivery of PFCC in theinpatient setting. Although context is implicit in the existingmodel of PFCC, the model may need to more fully explicatethese factors in order to for PFCC to be fully actualized inpediatric healthcare settings.
Methods
This grounded theory study had, as its foundation, thesociological theory of symbolic interactionism, which positsthat meaning is central to understanding human behavior andthat it is a social product, derived from a person's interactionswith others. Social interaction is therefore central to thecreation of meaning, and social researchers are thus chargedwith studying and understanding how and why interactionsoccur and the meanings individuals derive from thoseinteractions (Blumer, 1969; Hall, 1987; Strauss, 1993).Grounded theory and symbolic interactionism have beendescribed as a “theory/methods package” (Clarke, 2005, p. 4)because of grounded theory's emphasis on understandinginteraction, social processes, and interpretation of meaning.Accordingly, this study sought to understand interactions,processes, and the creation of meaning for the parents ofchildren with CCC and nurses in the PICU.
A single PICU in a large, urban teaching hospital in thewestern United States served as the data collection site, and thefirst author was the sole data collector. Approval from the localinstitutional review board was obtained prior to the start of datacollection, and guidelines for the ethical conduct of researchwere followed throughout the study process. Eligibility criteriafor parents included: age greater than 18 years, English-speaking, and being the parent of a child with a CCC whowas currently admitted to the PICU and who had an expectedlength of stay in the PICU of at least 7 days. Parents who agreedto participate allowed the investigator to observe theirinteractions with healthcare providers from the child's room inthe PICU at various times over the course of a week. Near theend of that week, parent participants also engaged in a single, in-depth interview that asked questions about their experienceswith healthcare providers while in the PICU. Conducting theinterview while the child was still hospitalized in the PICUprovided parents with an opportunity to report and to reflect in“real time” on their experiences and may have helped tohighlight some of the day-to-day concerns thatwould be lost in amore traditional retrospective interview. Parents were invited tobegin the discussion by describing their child, including a briefsummary of their child's illness and their past experiences in thehealthcare system. During the course of the observations and

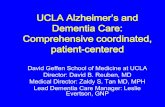
Rule enforcement
PF
CC
+
+
--
Unpredictable, infrequent rule enforcement
Families do what they want, rules unnecessary
Rules in place, but families create them
Families must complywith all hospital/unit rules, no exceptions
Rules are co-created and both nurses and families participate in
enforcement
igure 1 Rules positional map. Example of a positional mapcreated during data analysis.
3Impact of Hospital and Unit-Based Rules on Care in PICU
interviews, parents also helped identify their key healthcareproviders, and these providers were invited to participate in aseparate in-depth interview. All formal interviews were audio-recorded and transcribed verbatim by a professional transcrip-tion service, and the first author verified each interview aftertranscription. Field notes were taken during each observationsession and during additional general observation sessions onthe unit, during which time the investigator sat at the nurses'stations in the unit to observe movement about the unit,workflow, and the type and frequency of exchanges that happenoutside of patients' rooms. Additional data collection came inthe form of participation in unit staff meetings and review ofrelevant texts, including policies, guidelines, and materialsdistributed to families during their stay in the PICU.
There were a total of 19 participants in the study, 7 parents(5 mothers and 2 fathers, all the parents of different children)and 12 nurses (all female). Relevant demographics for theseparticipants are displayed in Appendices A and B.Interestingly, 10 of the 12 nurse participants (83.3%)identified as Caucasian, whereas 35% of the registerednurses in the county where this study was conducted areCaucasian (California Health Care Foundation, 2010). Fiveof the seven parent participants (71.4%) identified as Latino,also higher than the county demographic of 48.2% (UnitedStates Census Bureau, 2014).
This studywas conducted using a constructivist, postmodernconceptualization of grounded theory that focuses on “theoriz-ing” rather than theory production and questions the usefulnessof focus on a single core category, suggesting that it may lead tooversimplification of complex social processes (Charmaz, 2006;Clarke, 2005). Consistent with Clarke's conceptualization ofpostmodern grounded theory, situational analysis, whichfocuses on the contextual nature of data, positionality, andawareness of and illumination of discourses, provided a guidingframework for the analytical work.
The first step in data analysis was open coding of theinterviews, field notes, and policy documents. Frequentlyoccurring initial codes relevant to this analysis included“rules,” “enforcement,” and “expectations.” These initialcodes were later clustered into groups in the process of axialcoding, or the linking of open codes together into categoriesfor further exploration and analysis (Charmaz, 2006). Thisanalysis occurred in memos about many of the identifiedcategories, including the set of rules that families areexpected to follow, the differences between the explicitand implicit rules, and the ways in which families learn theserules. Writing memos on these topics allowed deeperexploration of these themes and recognition of the need formore information. In subsequent data collection, informationthat specifically solicited content about rules and ruleenforcement on the part of the nurse was sought. Consistentwith grounded theory methods, constant comparativeanalysis, in which new cases are compared to existing onesto identify similarities and differences that advance theanalysis (Corbin & Strauss, 2008), occurred throughout theanalytical process. As a component of the analysis, the raw
data, codes, and themes were compared and contrasted,which allowed for similarities and differences in the data tobe highlighted and further examined. This ongoing compar-ison was particularly helpful in understanding the competingpriorities that nurses face related to rule enforcement and thedifferences in perceptions of these rules between nurses andfamily members. The construction of situational andpositional maps, key components of the situational analysistoolbox (Clarke, 2005), helped to provide additional insightinto these competing priorities and varying standpoints. Thesituational maps, which attempt to capture the full scope ofthe situation by listing all relevant elements and actors(Clarke, 2005), helped to highlight the complex and, at times,chaotic context within which care for children in the PICU isoccurring. This in turn helped to shed light on healthcareproviders' need for rules that help to bring structure andcontrol to an otherwise out-of-control environment. Posi-tional maps helped to identify positions within the data, someof which may be hidden, implicit, or otherwise difficult todescribe, and none of which are assumed to be better thananother for the purposes of analysis (Clarke, 2005). Anexample of a positional map about rule enforcement is shownin Figure 1. This map helped to illustrate the dominantpositions in the data, as well as those that were under-represented or not represented at all. Rigor in the analyticalprocess was ensured through frequent discussion of findingswith members of the research team, and these discussionshelped to highlight areas of potential bias and conceptualweakness and the possibility of alternative explanations(Whittemore, Chase, & Mandle, 2001).
Findings
Although not a topic of inquiry on the initial interview guidefor parents or nurses, rules quickly became an important area offocus for both parents and nurses. Consistent with the co-
F

4 J. Baird et al.
occurring processes of data collection and analysis in groundedtheory, the interview guide was subsequently revised to inquireexplicitly about formal rules and to seek information about arelated emerging theme, implicit rules.
Explicit Rules
Parent Perceptions
Family members and visitors of patients in the PICU wereintroduced early in the hospital admission to the basic rules ofthe unit. This process of “learning the rules,” one of the codesgenerated from both parent and observation data, occurred mostoften through verbal explanation from the admitting nurse. Therules were also documented in the unit welcome packet that wasoffered to each family at the time of admission. The rulesdiscussed in the welcome packet covered awide range of topics,from access to the unit and alarmmanagement to isolation statusand visitor personal care needs. The rules pertaining to personalcare needs were mentioned most frequently by parentparticipants. These rules were the ones that had the most impactupon their day-to-day life in the PICU and that often became aburden as the length of the hospitalization increased. From thesedata, the code “struggling with the rules” was generated. Thiscode referred to the challenges that parents faced when theyencountered rules that made it difficult to either be with theirchild when they wanted to or to live for an extended period oftime in the PICU. The two rules that parents considered mostproblematic were the need to leave the unit in order to use therestroom and a ban on family members or visitors eating at thebedside. Although there were three restrooms located within thePICU, all three were designated exclusively for staff memberuse. This necessitated that parents exit to use visitor restroomslocated just outside of the unit, and they then had to call for re-entry to the unit after using the restroom. The need to exit andreenter was a particular frustration during the night time hours,when reduced staffing often meant delays in responding to theparent's request to reenter the unit. One parent stated:
There's not a bathroom inside, so you can't really…that,to me, really bugs me that you have to every time goout…call, come back. [Participant M600]
The ban on eating at the bedside was also problematic forseveral of the parents. Parents and other visitors in the PICUwerepermitted to have drinks in the patient rooms, but solid foodswereprohibited in most cases. Some of the parents complied despiteobjecting, and others found ways to bypass the rule.
I mean, I sneak food in. I do eat, but I don't eat messystuff. I try not to make crumbs… [Participant M700]
Those parents who complied with the ban expressedconcern about leaving their child's bedside for extendedperiods, worrying that the child would awaken and befrightened that the parent was not there or that there would be
a deterioration in the child's condition during his or herabsence. Two parents indicated that they had delayed leavingthe unit to eat, resulting in extended periods of time duringwhich they had not eaten; this behavior was at least in partdue to their inability to have meals or other snacks in theirchild's room. Observation periods yielded numerous exam-ples of parents eating on the unit, some having only lightsnacks and others eating entire meals in their child's room.This variability in compliance was not confined to the ruleabout eating, as parents were noted to be “breaking” a varietyof rules, including adherence to the use of personal protectiveequipment (PPE) in the rooms of children on isolation,silencing of alarms within the patient rooms, entry into theunit without prior approval of the RN, and having more thanone visitor sleeping overnight in the patient room.
Nurse Perceptions
“Enforcing the rules” quickly became a significant area ofdiscussion in interviews with nurse participants and afrequently occurring code, despite the fact that it was notan explicit topic in early iterations of the interview guide.When asked to describe how she learned to communicatewith families, one nurse responded,
I feel like some people just have good communicationskills and some people would feel more comfortable thanothers. Just little things like, ‘Sorry, you can't eat inhere.’ There'll be nurses that will let [parents] eat in herebecause they don't want to tell them, ‘Don't eat in here.’[Participant RN203]
This response and subsequent discussion later in theinterview suggested that the nurse equated communicationwith rule enforcement, and she viewed her willingness toengage in such enforcement as evidence of her ability tocommunicate well with families. Other nurses expressedvarying degrees of difficulty with the concept of ruleenforcement, leading to the occurrence of “not consistentlyenforcing the rules” as a frequent code. These nurses notedthat enforcement became more difficult when the rules wereinconsistently applied. Once the family had “gotten away”with something like eating in the room or not having to wearPPE in the room of a child on isolation status, it was thendifficult for some nurses to step in and reestablish the rules.
A lot of families refuse to wear the precautions. If youare the one to tell them that they need to wearprecautions, or, ‘You can't bring food or drinks in,’they shut you out…if you try to enforce the rules aboutcontact [isolation] and bringing food in the ICU, theyjust put you by the wayside after that, like you're not…[Participant RN201]
Only one nurse expressed a concern about the impact thatenforcement of certain rules could have upon the family'sefforts to be together and to support one another during theirchild's hospitalization. This nurse stated that she does

5Impact of Hospital and Unit-Based Rules on Care in PICU
sometimes purposefully choose not to enforce rules, notbecause enforcement in difficult but because of her beliefsabout the family situation. She expressed a belief thatallowing a father to eat at his child's bedside or permittingboth parents to sleep at the bedside overnight was moreimportant than adherence to a prescribed set of rules that donot take into account the individual family's needs.
Rule enforcement was a topic of concern not only for thenurse participants in this study, but also for the nursing staffas a whole. Rules were a regular topic of discussion atobserved unit staff meetings and a frequent subject of whole-staff emails. Those nurses who most closely identified withthe role of rule-enforcer often initiated discussion of the topicat the meetings, but the discussion always generatedsignificant interest, with several nurses speaking up tooffer examples of families who failed to comply with therules and many other nurses offering both verbal and non-verbal affirmations of the frustration expressed by the nurseswho spoke. As stories about problems with family rulecompliance were shared in these meetings, many nurses werenoted to nod their head in agreement or to offer sidecomments about similar experiences to those sitting nearby.The level of agreement about the need for rule enforcementnoted at these meetings was, however, at odds with the extentto which compliance with rules was noted during observa-tions in the unit. With such significant agreement, one wouldexpect to see a high level of compliance with the stated rules.The discordance between these two observations suggeststhat nurses were perhaps not as confident about the need forsuch strict rule enforcement or about their role as enforcer asthey had let on to their peers.
Intersection of Parent and Nurse Perceptions
The intersection between parent and nurse perceptions ofexplicit rules occurred in the enforcement of such rules. Theextent to which nurses were willing and able to enforce therules largely dictated the level of parent compliance with therules. Although many parents were noted to be out ofcompliance with the rules, an equal number were observed tocomply, often without complaint or expressed concern. Thiscreated an additional area of concern for the nursing staff:some parents were expected to comply with the rules, whileothers were allowed to forego compliance and insteadengage in whatever behavior best suited their needs. Uponfacing a family that was out of compliance with the rules, thenurse was therefore faced with a dilemma: choosing toenforce the rules and risking the ire of the family, oroverlooking the lack of compliance and possibly being heldaccountable for failing to enforce the rules. The inconsis-tency of rule enforcement on the part of the nursing staff wasconfusing for the parents and led to questions about thenecessity of the rules, which in turn led to rules being eithermodified or broken by the parents. A cycle of non-compliance was thus created, contributing to frustration on
the part of the nursing staff and undermining optimalrelationship development between parents and nurses.
Implicit Rules
Of equal impact upon the patient and family experiencewere the implicit, or unspoken, rules of the PICU, which canalso be thought of as the social norms of the hospital setting.These implicit rules/norms were never clearly discussed withfamilies and as a result, parents did not speak directly in theinterviews about them. The data to support this findingtherefore came from interviews with nurses and observationsof interactions between nurses and parents. Because of theirimplicit nature, families were dependent upon social cuesand an understanding of and/or familiarity with thehealthcare system in order to successfully navigate theserules. The code “knowing the hospital routine” reflected thefact that parents were expected to know that the hospital hada set schedule that was dependent upon a variety of factors,including the work hours of the nursing staff, the educationalneeds of the physicians-in-training, and schedules fordelivery of supplies and medications. Parent requests tovary or interrupt this schedule were not welcome and mayhave been perceived as demanding by the nurses, who havelearned to structure their work day to accommodate thehospital routine.
I've had families where they want…everything is specificand their needs are written out on paper. [A mom]wanted the meds given at 0800 on the dot, and withchange of shift and doing your safety [checks]—itdoesn't happen. She would scold you for not having itdone at 0800. It was a lot of pressure and stressful. It wasuncomfortable. [Participant RN201]
Another code, “understanding care priorities,” capturedthe idea that parents were expected to understand that thenurse's focus was on care of the child, and that tasks that thenurse perceived as interfering with or delaying the child'scare were given low priority. These tasks included things asbasic as retrieving drinks for family and visitors or ascomplex as engaging in discussion with the family aboutchanges in the child's condition or the plan of care for theday. Some of the nurses interviewed seemed to have anexpectation that parents would be able to read the situation,understand how busy the nurse was, and adapt theirquestioning or demands upon the nurse accordingly. Onenurse stated,
I think that we sometimes…we let people forget what aserious area that we work in. And that this is an ICU andthese people that are here are sick and that's what we'redoing here. This isn't like a social gathering in any way…we don't want to make light of the fact your kid is sickenough to be in the ICU, and that is what we're herefor—to care for them. And that's our primary concern.Yeah, we want [parents] to have coffee and want

6 J. Baird et al.
[parents] to feel like [they're] getting free information…we want to recognize that [parents] need information, wewant to give it to [them]. But [parents] really shouldn'tinterrupt us when we're giving report. [They] really needto understand that what we're doing with [their child's]medications is more important than [their] coffee.[Participant RN903]
Parents were additionally expected to recognize theexpertise that the nurse brought to the bedside; this wascaptured in the code, “respecting the nurse as professional.”The nurses expressed frustration with parents who offereddetailed suggestions on how best to care for their child orwho did not respect the nurse's authority or role as aprofessional. Some of the nurses' comments were territorialin nature; they wanted parents to recognize that the PICUwas the nurse's domain and that the nurse—not the parent—was the expert in that domain. One nurse said,
…And [parents] are kind-of infringing upon my job, andtelling me what to do, it's like that little loss of respect iskind of hard to work with. [Participant RN901]
Above all, parents were expected to be compliant, easy-going, and emotionally stable and to realize that they wereguests in the PICU, regardless of the length of time that theirchild had been hospitalized in the unit. Parents who failed tomeet these standards were labeled as “difficult,” a label thatgot passed from nurse to nurse during shift report and thatcould then follow the parents throughout the hospitalization,potentially coloring the interactions that subsequent nurseshad with the patient and family.
…We had a lot of difficult families in the unit. We'll getreport and the nurse already has her opinion. It's givenlike, ‘Oh, this family is so difficult…it's going to be theworst day. The family is so difficult and terrible.’[Participant RN203]
In rare cases, the labeling of parent behavior was soextreme as to make it challenging to find nurses who werewilling to care for a patient and their family:
With [patient], nobody wanted to take care of herbecause her mom was so difficult. I had to literally makea stink about making a continuity list for her and pickingout, looking at the calendar, and picking out people, thisis who's going to take care of her because otherwise thisis going to be a nightmare. [Participant RN900]
Several of the nurses interviewed expressed frustrationwith this labeling behavior, preferring not to draw prematureconclusions and instead to approach each family with a“blank slate.” These nurses didn't necessarily have differentexpectations for parent behavior, but they wanted theopportunity to judge the behavior for themselves or tofurther investigate the cause of the problematic behavior.Other nurses, however, did make allowances for parents,
recognizing that their emotional stress or their lack offamiliarity with the PICU environment might lead tobehavior considered outside the norm for the hospital setting.One nurse summed up her approach to working with familiesin this way:
So [I] just remember if they are asking a lot of questionsor if they are, if there are difficult times with them, thatthey really, really love their child, and you really, reallycare about your patient—so if nothing else, you reallyhave that in common. [Participant RN404]
Discussion
The complexity of the modern healthcare environmentnecessitates the creation of an ever-growing list of rules towhich patients, families, and visitors to the hospital areexpected to adhere. Many of these rules are designed topromote the safety of everyone in the hospital environment.Few would argue, for example, about the necessity of a set ofrules regarding use of PPE to prevent transmission ofcommunicable diseases. These safety-related rules makesense to most visitors, and staff members are easily able tooffer rationale for their existence and the necessity ofenforcement. These rules are also largely explicit, and theyare typically the rules about which families and visitors areinformed early on in their visit to the unit. There are,however, many other explicit and implicit rules that do notfall as clearly into the safety category, and they appear toexist either to maintain order in the environment or for theconvenience of hospital staff. The explicit rules from thesetwo categories were the ones about which parents expressedthe most frustration, and the implicit rules from the samecategories were the most problematic for nurses.
This frustration on the part of both parents and nurses overthe rules not directly related to safety may be due to thecompeting perceptions and goals of both groups. Nurses arerapidly socialized into the healthcare environment as a part oftheir training, both during their formal educational programand upon entry into the workplace (Dinmohammadi,Peyrovi, & Mehrdad, 2013; Price, 2008). They quicklylearn institutional norms, the hospital routine, and their rolewithin it, including their responsibility for performing thetasks necessary to ensure safe patient care. They also learnthe stumbling blocks to efficient care and have devisedmechanisms to avoid such stumbling blocks, often in theform of policies and rules, many of which have a directimpact upon families and visitors. Parents, on the other hand,come to the hospital environment with the goal of ensuringthe highest quality care for their child, and they have varyinglevels of familiarity with the healthcare system and thestructures and routines contained therein. Depending upontheir past history, parents may not have yet been socialized tothe norms of the healthcare environment and to their rolewithin that environment. Further, they are encouraged by

7Impact of Hospital and Unit-Based Rules on Care in PICU
other healthcare providers, by family and friends, and by thelay healthcare literature to be an active participant in theirchild's care. Parents are repeatedly told to ask lots ofquestions, advocate for their child, question decisions that donot make sense, and pursue individualized care that matchesthe routine and the customs of the family (Family Voices,2013). These very behaviors, though, are the ones that nursesidentified as challenging, problematic, and undesired, and thatmay, paradoxically, subject the family to a lower quality of careby reducing nursing staff engagement with the family.
Why do some nurses find these key tenets of parentparticipation so problematic? The answer may lie, in part, in anoutdated understanding of the parental role within the hospitalsetting. The norms upon which nurses are basing theirexpectations of parent behavior are a holdover from a time inwhich parentswere viewed as visitors or guests (Harrison, 2010;Jolley & Shields, 2009) and not as integral members of thechild's care team. The field of pediatrics has endorsed theconcept of PFCC for decades, but the extent to which the modelhas become actualized within the acute care setting remains inquestion (Jolley & Shields, 2009). Parents repeatedly encounterbarriers to full and active participation in their child's care,whether in the form of limited accommodation of their personalneeds during the child's stay at the hospital or of dismissal oftheir concerns about the child's care on the part of the nursingstaff. Both of these types of barriers undermine the parent's roleas a member of the care team and serve to maintain the statusquo, in which the focus on hospital routine and work efficiencyis given priority over the needs of patients and families. Thesebarriers also help to foster the territorialism expressed in severalof the nurses' comments and to promote a hierarchy inwhich thenurse as professional has power over the parent.
Further, the nurses responsible for simultaneously providingPFCC and for serving as the front-line face of the healthcaresystem and the de facto rule-enforcer may be experiencing rolestrain, or the felt stress that occurs in the attempt to meet theexpectations of a role with competing demands (Ward, 1986).The emotion with which several of the nurse participantsexpressed concern and frustration about parental violation ofunit rules and norms lends credibility to this assertion; discussionabout the rules, in particular the implicit rules/norms, was oftenone of the most animated sections of the interview. The conflictthat exists between the historical role of the parent-as-visitor andthe modern conceptualization of the parent-as-team-member isactualized in the day-to-day interactions of parents and nurses,such that the nurse is unsure which role to assume and of theexpectations associated with that role. The emergence of thepay-for-performance movement and the accompanying empha-sis on ensuring patient and family satisfaction with the hospitalexperience (Wolosin, Ayala, & Fulton, 2012) has focusedattention on the extent to which the hospital environment ispatient and family-centered. Unfortunately, nurses have beengiven little guidance about how to successfully navigate thedualities of their role: the need tomaintain safety and orderwhilesimultaneously providing an excellent care experience for eachpatient and family. The end result is a sense of frustration on the
part of both the nursing staff and the families that runs contraryto the goal of establishing PFCC.
This analysis thus complicates the PFCC model, suggest-ing that its challenges to full implementation may lie, in part,in its failure to fully and explicitly contend with contextualfactors, of which this discussion of rules and norms is but oneexample. Nurses are working under a mandate to provideoptimal PFCC, but they are being asked to do so in a contextthat runs contrary to and often demands something other thanthis type of care. Healthcare institutions create rules and haveestablished norms, and RNs are socialized to work withinthese contexts such that they embrace and adopt the rules andnorms, which in turn makes it difficult for them to take theidealized concepts of PFCC and put them into action.Further, RNs may lack sufficient support to effectivelyintegrate competing demands. Thus, the adherence to rulesand norms takes precedence, and the discrepancy betweenwhat parents are seeking and what RNs provide occurs. Thecurrent model of PFCC fails to sufficiently account for thiscontextual factor and may begin to offer an explanation forthe discrepancy between PFCC as a concept that nearlyeveryone endorses and its adoption in practice, whichexisting literature and this study suggest may not be optimal.It may be necessary, therefore, to further extend the PFCCmodel by emphasizing that true partnership between parents andproviders can only occur when the importance of context isgiven adequate attention. This attention to context must includea thorough, ongoing, and self-reflective analysis of the ways inwhich families experience a particular healthcare setting, takinginto account both the explicit and implicit messages that theyreceive and the impact that socialization to norms and roles hashad upon providers working within that setting.
Study Limitations
This was a single-site study and as such, only reflects thepolicies, practices, and viewpoints of parents and nursesfrom that site. The specific set of rules to which parents andvisitors are expected to adhere varies from hospital tohospital, such that the challenges identified in this paper maynot be of concern in other locations. In addition, the nurseparticipants in this study were a relatively homogenousgroup; all of the nurses were female, and all but one wereCaucasian. While reflective of the demographics of thenursing staff within this unit, it is not representative of thepopulation of nurses in the county in which this study wasconducted, and it is likely that the views of male and non-Caucasian nurses are not adequately reflected in the data.The ethnicities of the parent participants are also not fullyreflective of those of the county in which these data werecollected, and the impact of this discrepancy upon thebehaviors and opinions captured here is not known.
The first author was employed part-time as a clinicalnurse in the unit in which this study was conducted and assuch, had an “insider” status in this environment. Her

8 J. Baird et al.
position as an insider afforded her entrée into the researchsetting and full access to the workings of the unit. This accessfacilitated data collection and gave her credibility with thenurse participants, enabling her to gain candid, openfeedback about their experiences caring for patients andfamilies in the PICU. This insider status may also, however,have impacted the type and amount of data collected, sincethis was not an environment that she was experiencing forthe first time. Her familiarity with the setting may havepredisposed her to see processes, behaviors, and interactionsin a particular way. Similarly, data analysis may have beenimpacted by this insider status, contributing to bias in theanalytical process or early attributions based on previousexperiences in this known environment. The research teamhelped to mitigate this by reviewing observation field notes andinterview transcripts, looking for ways in which this insiderstatus may have impacted data collection. The team alsoremained attentive to this status throughout the analyticalprocess by reviewing its impact upon the emerging findings.
Implications for Practice and Research
The findings from this portion of the study indicate thatparents encounter significant barriers to full participation intheir ill child's care in the PICU, such that true PFCC is notyet a reality. These barriers arise in the form of both codifiedrules and in an outdated understanding of the parental role inthe hospital setting. Efforts to achieve optimal PFCC may,therefore, require a reevaluation of the existing rules to whichfamilies are subject. Is it possible, for example, to design oradapt the environment to accommodate parents' basic needs?Can existing policies about such things as eating andovernight visitation be modified to maximize the time thatfamilies are together? Changes to these rules are certain tohave an impact upon staff, and the implications of thesechanges would need to be evaluated and addressed.Allowing families to eat in the rooms, for example, wouldnecessitate setting guidelines for food storage and mayrequire more frequent rounds by housekeeping staff, in orderto remove uneaten food that could attract pests. Permittingmore than one family member to stay overnight with thechild would similarly require adjustments on the part of thenight shift nursing staff, who have become accustomed toproviding care with a minimal number of visitors present.
In tandem with a reevaluation of these explicit rules, aneducational initiative that explores the value of PFCC and thechallenges associated with its provision is needed. Thiseducational effort should go beyond the basics that mostnurses receive in their pre-licensure academic programs andinstead delve into and begin to challenge the assumptionsthat practicing nurses bring with them to interactions withpatients and families. It would include an identification of theimplicit rules to which families are expected to adhere, aswell as an evaluation of the extent to which these rulespreserve the status quo and undermine parent and family
participation in care. This information should be presented inthe context of the current healthcare environment and theACA mandates that are driving organizations to focussignificant attention on the extent to which patients andfamilies are satisfied with their healthcare experience(Wolosin et al., 2012). Interventions to improve patient andfamily satisfaction are necessarily largely focused on nursingcare, and nurses must therefore possess both an understand-ing of the drivers of patient and family satisfaction and awillingness to adapt their care to better meet patient andfamily needs. Equipped with this knowledge, nurses couldidentify changes to their own practice and modifications tothe unit culture that would foster PFCC. At the same time,nurses need a forum to discuss the difficulties that they facein carrying out the dualities of their role, serving as bothfacilitator of PFCC and rule enforcer. A need exists for bothone-on-one and group coaching, where these nurses canreport on challenging family scenarios and receive feedbackon how best to handle the situation and support for theirefforts to provide optimal PFCC. Working with families incrisis and the parents of children with CCC is a complexendeavor, and it requires a skill set that nurses will notacquire without advanced training and ongoing support. It istime that we acknowledge this fact and afford learning tointeract with families the same attention and resources thatwe give to technical skill acquisition.
Finally, there is a need for further research in this area. Theconcept of PFCC has garnered significant interest in thepediatric literature, but relatively few studies have investigatedthe extent to which acute care environments are patient andfamily-centered or the barriers to achieving this goal. Thisstudy identifies some significant barriers within the context ofa single PICU environment, but there is a need to expand uponthis work, assessing the extent to which these barrierstranscend this particular setting. Are these challengesconsistent with those encountered in other PICUs, and towhat extent are these problems encountered across thepediatric acute care trajectory? If these problems exist inother settings, what interventions are successful in challengingthe status quo and improving the patient and familyexperience? There may also be an opportunity to learn fromthe significant PFCC work that has been done in neonatalintensive care units (Cooper et al., 2007; Gooding et al., 2011),given some of the similarities between these two environ-ments. Patient and family-centered care is widely accepted asthe ideal in pediatric healthcare, but it is time to generate theknowledge that will help transform this ideal into reality.
Acknowledgments
The research described in this article was funded by anindividual National Research Service Award from theNational Institute for Nursing Research, grant numberNIH-5F31NR012093.

9Impact of Hospital and Unit-Based Rules on Care in PICU
Appendix A. Parent demographics.
Parent Demographics (n = 7)
Age Mean 29.9,range 22–53
Age of child Mean 5.2,Range 7 months–15 years
RaceWhite 5 Child's genderUnidentified 2 Male 4Female 3
Ethnicity Child's primary conditionHispanic Gastrointestinal 3Not Hispanic Genetic disorder 2
Income Seizure disorder 1N$100,000 1 Heart disease 1$75,000–99,999 1$50,000–74,999 1$25,000–49,999 2b$24,999 1Unidentified 1
EducationBachelor's degree 1Some college 3High school 3
Appendix B. Registered nurse demographics.
Registered nurse Demographics (n = 12)
Age Mean 35.4, range 24–62RaceWhite 10Black 1More than one race 1
Highest level of nursing educationMaster 1Bachelor 9Associate 2
Years of experienceLess than 2 42–5 36–10 211–20 0Greater than 20 3
References
American Academy of Pediatrics Committee on Hospital Care, & Institutefor Patient and Family-Centered Care (2012). Patient- and family-centered care and the pediatrician's role. Pediatrics, 129, 394–404,http://dx.doi.org/10.1542/peds.2011-3084.
American Nurses Association (2008). Pediatric nursing scope andstandards of practice. Silver Spring, MD: American Nurses Association.
Balling, K., & McCubbin, M. (2001). Hospitalized children with chronic illness:Parental caregiving needs and valuing parental expertise. Journal of PediatricNursing, 16, 110–119, http://dx.doi.org/10.1053/jpdn.2001.23157.
Bicchieri, C. (2006). The grammar of society: The nature and dynamics ofsocial norms. New York, NY: Cambridge University Press.
Blumer, H. (1969). Symbolic interactionism: Perspective and method.Berkeley, CA: University of California Press.
California Health Care Foundation (2010). California Health CareAlmanac. Oakland, CA: Author.
Charmaz, K. (2006). Constructing grounded theory: A practical guidethrough qualitative analysis. Thousand Oaks, CA: Sage Publications.
Clarke, A. E. (2005). Situational analysis: Grounded theory after thepostmodern turn. Thousand Oaks, CA: Sage Publications.
Cooper, L. G., Gooding, J. S., Gallagher, J., Sternesky, L., Ledsky, R., &Berns, S. D. (2007). Impact of a family-centered care initiative on NICUcare, staff, and families. Journal of Perinatology, 27, S32–S37, http://dx.doi.org/10.1038/sj.jp.7211840.
Corbin, J., & Strauss, A. (2008). Basics of qualitative research: Techniquesand procedures for developing grounded theory (3rd ed.). ThousandOaks, CA: Sage Publications.
Davies, B., Baird, J., & Gudmundsdottir, M. (2013). Moving family-centered care forward: Bereaved fathers' perspectives. Journal ofHospice and Palliative Nursing, 15, 163–170.
Dinmohammadi, M., Peyrovi, H., & Mehrdad, N. (2013). Concept analysisof professional socialization in nursing. Nursing Forum, 48, 26–34,http://dx.doi.org/10.1111/nuf.12006.
Edwards, J. D., Houtrow,A. J., Vasilevskik, E. E., Rehm,R. S.,Markovitz, B. P.,Graham, R. J., et al. (2012). Chronic conditions among children admitted toU.S. pediatric intensive care units: Their prevalence and impact on risk formortality and prolonged length of stay. Critical Care Medicine, 40,2196–2203, http://dx.doi.org/10.1097/CCM.0b013e31824e68cf.
Family Voices (2013). Quality health care for children with specialhealthcare needs. Retrieved from. http://www.familyvoices.org/admin/work_caring/files/QualityHealthCare.pdf

10 J. Baird et al.
Feudtner, C., DiGiuseppe, D. L., & Neff, J. M. (2003). Hospital care forchildren and young adults in the last year of life: A population-basedstudy. BMC Medicine, 1, 3, http://dx.doi.org/10.1186/1741-7015-1-3.
Gooding, J. S., Cooper, L. G., Blaine, A. I., Franck, L. S., Howse, J. L., &Berns,S. D. (2011). Family support and family-centered care in the neonatalintensive care unit: Origins, advances, impact. Seminars in Perinatology, 35,20–28, http://dx.doi.org/10.1053/j.semperi.2010.10.004.
Gordon, J. B., Colby, H. H., Bartelt, T., Jablonski, D., Krauthoefer, M. L., &Havens, P. (2007). A tertiary care-primary care partnership model formedically complex and fragile children and youth with special healthcare needs. Archives of Pediatric and Adolescent Medicine, 161,937–944, http://dx.doi.org/10.1001/archpedi.161.10.937.
Graham, R. J., Pemstein, D. M., & Curley, M. A. Q. (2009). Experiencingthe pediatric intensive care unit: Perspective from parents of childrenwith severe antecedent disabilities. Critical Care Medicine, 37,2064–2070, http://dx.doi.org/10.1097/CCM.0b013e3181a00578.
Hall, P. M. (1987). Interactionism and the study of social organization. TheSociological Quarterly, 28, 1–22.
Harrigan, R. C., Ratliffe, C., Patrinos, M. E., & Tse, A. (2002). Medically fragilechildren: An integrative review of the literature and recommendations forfuture research. Issues in Comprehensive Pediatric Nursing, 25, 1–20.
Harrison, T. M. (2010). Family-centered pediatric nursing care: State of thescience. Journal of Pediatric Nursing, 25, 335–343, http://dx.doi.org/10.1016/j.pedn.2009.01.006.
Institute for Patient and Family-Centered Care (2010). What are the coreconcepts of patient and family-centered care? Retrieved from. http://www.ipfcc.org/faq.html
Jolley, J., & Shields, L. (2009). The evolution of family-centered care.Journal of Pediatric Nursing, 24, 164–170, http://dx.doi.org/10.1016/j.pedn.2008.03.010.
Kirk, S., Glendinning, C., & Callery, P. (2005). Parent or nurse? Theexperience of being the parent of a technology-dependent child. Journalof Advanced Nursing, 51, 456–464.
Malusky, S. K. (2004). A concept analysis of family-centered care in theNICU. Neonatal Network, 24, 25–32, http://dx.doi.org/10.1891/0730-0832.24.6.25.
Meert, K. L., Clark, J., & Eggly, S. (2013). Family-centered care in thepediatric intensive care unit. Pediatric Clinics of North America, 60,761–772, http://dx.doi.org/10.1016/j.pcl.2013.02.011.
Mikkelsen, G., & Frederiksen, K. (2011). Family-centered care of childrenin hospital—A concept analysis. Journal of Advanced Nursing, 67,1152–1162, http://dx.doi.org/10.1111/j.1365- 2648.2010.05574.x.
Namachivayam, P., Taylor, A., Montague, T., Moran, K., Barrie, J.,Delzoppo, C., et al. (2012). Long-stay children in intensive care: Long-term functional outcome and quality of life from a 20-yr institutional
study. Pediatric Critical Care Medicine, 13, 520–528, http://dx.doi.org/10.1097/PCC.0b013e31824fb989.
Price, S. L. (2008). Becoming a nurse: A meta-study of early professionalsocialization and career choice in nursing. Journal of Advanced Nursing,65, 11–19, http://dx.doi.org/10.1111/j.1365- 2648.2008.04839.x.
Ray, L. D. (2002). Parenting and childhood chronicity: Making visible theinvisible work. Journal of Pediatric Nursing, 17, 424–438, http://dx.doi.org/10.1053/jpdn.2002.127172.
Reeves, E., Timmons, S., & Dampier, S. (2006). Parents' experiences ofnegotiating care for their technology-dependent child. Journal ofChild Health Care, 10, 228–239, http://dx.doi.org/10.1177/1367493506066483.
Rehm, R. S., & Bradley, J. F. (2005a). Normalization in families raising achild who is medically fragile/technology dependent and developmen-tally delayed. Qualitative Health Research, 15, 807–820, http://dx.doi.org/10.1177/1049732305276754.
Rehm, R. S., & Bradley, J. F. (2005b). The search for social safety andcomfort in families raising children with complex chronic conditions.Journal of Family Nursing, 11, 59–78, http://dx.doi.org/10.1177/1074840704272956.
Shields, L., Zhou, H., Pratt, J., Taylor, M., Hunter, J., & Pascoe, E. (2012).Family-centered care for hospitalised children aged 0–12 years.Cochrane Database of Systematic Reviews, http://dx.doi.org/10.1002/14651858.CD004811.pub3 (Art. No.: CD004811).
Srivastava, R., Stone, B., & Murphy, N. (2005). Hospitalist care of themedically complex child. Pediatric Clinics of North America, 52,1165–1187, http://dx.doi.org/10.1016/j.pcl.2005.03.007.
Strauss, A. L. (1993). Continual permutations of action. New Brunswick,NJ: Aldine Transactions.
Uhl, T., Fisher, K., Docherty, S. L., & Brandon, D. H. (2013). Insights intopatient and family-centered care through the hospital experiences ofparents. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 42,121–131, http://dx.doi.org/10.1111/1552-6909.12001.
United States Census Bureau (2014). State and county quick facts: LosAngeles County, CA. [Data file]. Retrieved from. http://quickfacts.census.gov/qfd/states/06/06037.html
Ward, C. R. (1986). The meaning of role strain. Advances in NursingScience, 8, 39–49.
Whittemore, R., Chase, S. K., & Mandle, C. L. (2001). Validity inqualitative research. Qualitative Health Research, 11, 522–537, http://dx.doi.org/10.1177/104973201129119299.
Wolosin, R., Ayala, L., & Fulton, B. R. (2012). Nursing care, inpatientsatisfaction, and value-based purchasing: Vital connections. Journal ofNursing Administration, 42, 321–325, http://dx.doi.org/10.1097/NNA.0b013e318257392b.