Welcome to Pakistan Research Repository:...
222
Study of Multifactorial Eye Disorders in Pakistan By Humaira Ayub CIIT/SP09-PBS-002/ISB PhD Thesis In Biosciences COMSATS Institute of Information Technology Islamabad, Pakistan Spring, 2015
Transcript of Welcome to Pakistan Research Repository:...

Study of Multifactorial Eye Disorders in
Pakistan
By
Humaira Ayub
CIIT/SP09-PBS-002/ISB
PhD Thesis
In
Biosciences
COMSATS Institute of Information Technology
Islamabad, Pakistan Spring, 2015

ii
COMSATS Institute of Information Technology
Study of Multifactorial Eye Disorders in Pakistan
A Thesis Presented to
COMSATS Institute of Information Technology, Islamabad
In partial fulfillment
Of the requirement for the degree of
PhD
(Biosciences)
By
Humaira Ayub
CIIT/SP09-PBS-002/ISB
Spring, 2015

iii
Study of Multifactorial Eye Disorders in Pakistan
A Doctoral Thesis submitted to the Department of Biosciences as partial
fulfillment of the requirement for the award of Degree of PhD (Biosciences).
Name Registration Number
Humaira Ayub CIIT/SP09-PBS-002/ISB
Supervisor
Prof. Dr. Raheel Qamar (T.I.)
Tenured Professor of Biochemistry & Molecular Biology
Dean of Research, Innovation & Commercialization
COMSATS Institute of Information Technology,
Islamabad, Pakistan
Co-Supervisor
Prof. Dr. Anneke I den Hollander
Professor in Molecular Ophthalmology
Departments of Ophthalmology and Human Genetics, Radboud
University Medical Center,
Nijmegen, The Netherlands
COMSATS Institute of Information Technology,
June, 2015

iv
Final Approval
This PhD thesis titled
Study of Multifactorial Eye Disorders in Pakistan
By
Humaira Ayub
CIIT/SP09-PBS-002/ISB
Has been approved
For COMSATS Institute of Information Technology, Islamabad
External Examiner: __________________________________________
Dr. Bushra Mirza
Professor & Chairperson
Department of Biochemistry
Quaid-e-Azam University Islamabad
External Examiner: __________________________________________
Dr. Atika Mansoor
Chief Scientific Officer
Institute of Biomedical & Genetic Engineering
KRL Hospital, Islamabad
Supervisor: ________________________________________________
Prof. Dr. Raheel Qamar (T.I.)
Tenured Professor of Biochemistry & Molecular Biology
Dean of Research, Innovation & Commercialization, Islamabad
HoD: __________________________________________________
Prof. Dr. Raheel Qamar (T.I.)
Tenured Professor of Biochemistry & Molecular Biology
Department of Biosciences, CIIT, Islamabad
Chairman:_________________________________________________
Prof. Dr. Mahmood A Kayani
Department of Biosciences, CIIT, Islamabad
Dean, Faculty of Science: __________________________________________
Prof. Dr. Arshad Saleem Bhatti (T.I.)
CIIT, Islamabad

v
Declaration
I, Humaira Ayub, CIIT/SP09-PBS-002/ISB hereby declare that I have produced the
work presented in this thesis, during the scheduled period of study. I also declare that I
have not taken any material from any source except referred to wherever due, that
amount of similarity with other sources is within the acceptable range. If a violation of
Higher Education Commission of Pakistan (HEC) rules of research has occurred in this
thesis, I shall be liable to punishable action under the plagiarism rules of the HEC.
Date:__________________
______________________
Humaira Ayub
(CIIT/SP09-PBS-002/ISB)

vi
Certificate
It is certified that Ms. Humaira Ayub, CIIT/SP09-PBS-002 has carried out all the
work related to this thesis under my supervision at the Department of Biosciences, CIIT,
Islamabad and the work fulfills the requirement for the award of PhD Degree.
Date:_______________
Supervisor:
_______________________
Prof. Dr. Raheel Qamar, T.I.
Tenured Professor of Biochemistry & Molecular Biology
Dean of Research, Innovation & Commercialization, Islamabad
Head of Department:
________________________
Prof. Dr. Raheel Qamar (T.I.)
Head
Department of Biosciences
CIIT, Islamabad.

vii
DEDICATION
My Parents – who mean the world to me!

viii
ACKNOWLEDGEMENTS
Acknowledgements may not be of substance to any research work but it’s a unique
opportunity for a writer to express gratitude to all people who have made valuable
contributions in the completion of the task. First of all, the Higher Education
Commission (HEC), Pakistan, made this endeavor possible, without whose financial
support none of the work could have been conducted.
Special thanks to my supervisor Prof. Dr. Raheel Qamar for his patience, who endured
and refined my raw work and groomed me gradually as a researcher. He is a thorough
gentleman. My co-supervisor Prof. Dr. Anneke I den Hollander helped, encouraged
and made Radboud University a wonderful learning experience, thanks to her. I am
also grateful to Mrs. Frederieke Schoenmaker-Koller, Dr. Eiko de Jong and Bjorn
Bakker in The Netherlands, who provided invaluable assistance in my work.
Dr. Maleeha Azam, Dr. Muhammad Ajmal, Dr. Syeda Hafiza Benish Ali, Dr.
Muhammad Imran, Mr. Moeen Riaz, Mr. Raja Khurram, Mr. Shakeel Ahmad, Mr.
Muhammad Shakil Khan, Mr. Liaqat Ali, Ms. Maleeha Maria, Ms. Saba Saleem and
my dear friends Sobia Shafique and Zehra Agha shared their valuable experiences
with me. Moreover their active participation and interest in my research work has
always been healthy. They were the sole outlet that I had for sharing light moments of
my time spent at CIIT. I have no enough words to thank my hostel mates and beloved
friends Ruqia, Rabia, Zarqa and Javeria who were always there to enlighten my days
far from family. I am grateful to the clinicians Dr. Farah Akhtar and Dr. Muhammad
Asim Khan and my sister-in-law Mrs. Zahida Adil for their invaluable clinical input
and help in sampling the patients.
My PhD studies also provided me an opportunity to admire the cultural diversity in
different European countries including Spain, Italy, Belgium, Germany, The
Netherlands & Portugal, which was a lifetime experience.
I would especially like to thank my family for their encouragement and support, without
which I would not have been able to achieve my goals in life and I am also grateful for

ix
their love and their constant source of admiration and for always being there whenever
I needed them. My most special thanks to my dear father Dr. Muhammad Ayub and
mother Mrs. Asma Ayub (late) who have been an inspiration and motivation
throughout my life.
In the end my sincere gratitude to all the families who donated their blood samples for
this study.
Humaira Ayub
CIIT/SP09-PBS-002/ISB

x
ABSTRACT
Study of Multifactorial Eye Disorders in Pakistan The aim of the current study was to investigate the underlying genetic cause in the
Pakistani population of common multifactorial eye disorders including glaucoma and
age-related macular degeneration. For this purpose linkage analysis of the families
suffering from these diseases as well as case-control association analysis of sporadic
cases of reported single nucleotide polymorphisms (SNPs) was performed. The
genotyping was done by Sanger sequencing, SNP microarray analysis, exome
sequencing and Taqman/KASPar SNP genotyping assays. The preliminary analysis of
glaucoma families was carried out by sequencing candidate genes MYOC, OPTN,
WDR36 and CYP1B1, which resulted in the identification of a disease-causing mutation
(c.868dup; p.Arg290Profs*37) in CYP1B1 in a large family with primary congenital
glaucoma (PCG). 250K microarray analysis of families with PCG and juvenile-onset
open angle glaucoma (JOAG) resulted in the identification of a possible novel locus on
chromosome 7 in one family. Exome sequencing revealed possible trigenic inheritance
(variants in three genes MYO18A; c.2071G>A; p.Arg691Cys, ENOX1; c.171C>T;
p.Met57Ile and COL9A2; c.1061C>T; p.Pro354Leu) in a family with JOAG, and
another variant (c.724C>T; p.Val242Met) in NCOA7 segregating with the disease in
the same family among individuals with late onset of the disease. Moreover in another
family a possible disease-causing variant was found in the PHKG1 gene (c.125 C>T;
p.Thr42Met). In the AMD families, sequencing of the complement factor H (CFH) gene
revealed no mutations.
Association analysis was performed of polymorphisms previously reported to be
associated with glaucoma and AMD, in 1000 samples with glaucoma comprising of
500 samples of primary open angle glaucoma (POAG), 200 samples of primary angle
closure glaucoma (PACG) and 300 pseudoexfoliation glaucoma (PEXG) samples, as
well as 300 unaffected controls. In addition, 300 samples of AMD patients and 250
unaffected age and gender-matched controls were screened. Of the 11 polymorphisms
screened in the glaucoma cohort, significant association of HSP70 (rs1043618) and
NOS3 (27bp VNTR in intron 4) polymorphisms with all three types of glaucoma were
found, whereas association of BIRC6 (rs2754511) and P450 (c.-2805T>C)
polymorphisms were found only for PEXG. 16 polymorphisms in genes of the
apoptotic, oxidative stress, complement and inflammatory pathways were screened in

xi
the AMD cohort. Significant association was found for polymorphisms in MMP2
(rs243866) and CX3CR1 (rs3732378 and rs3732379) with dry AMD, for NOS3 (27bp
VNTR in intron 4), and ARMS2 (rs10490924) with wet AMD and for ILβ (rs16944)
both with wet and dry AMD.
In conclusion, in the present study possible novel genetic causes of familial glaucoma
were identified, which included a possible novel locus in a PCG family, a possible
trigenic pattern of inheritance in a JOAG family involving three genes (MYO18A,
ENOX1, COL9A2), and in the same family a variant in the NCOA7 gene possibly
responsible for late-onset glaucoma in a separate loop. Furthermore, in another family
with JOAG, a variant in the PHKG1 gene was found to segregate with the disease.
Moreover, SNPs in oxidative stress and apoptosis components were found to be to be
associated with sporadic glaucoma. In addition, AMD-associated genes were for the
first time screened in the Pakistani population, which resulted in the identification of
variants in the complement and inflammatory pathway to be associated with AMD in
the Pakistani population.

xii
TABLE OF CONTENTS
1 Introduction………………………………………………………………
1
1.1 Multifactorial Diseases…………………………………………………. 2
1.2 Anatomy of Eye with Reference to Glaucoma and AMD……………… 2
1.2.1 Outer Segment…………………………………………………... 2
1.2.2 Interior Segment………………………………………………… 2
1.2.3 Posterior Segment………………………………………………. 4
1.2.4 Optic Nerve Head………………………………………………. 8
1.3 Glaucoma……………………………………………………………….. 8
1.3.1 Types of Glaucoma……………………………...……...………. 8
1.3.1.1 Primary Open Angle Glaucoma………………………. 9
1.3.1.2 Primary Angle Closure Glaucoma……………………. 9
1.3.1.3 Pseudoexfoliative Glaucoma……………………...….. 10
1.3.1.4 Syndromic Forms of Glaucoma…….………………… 11
1.3.2 Prevalence………………………………………………………. 11
1.3.3 Pathophysiology of Glaucoma…………………….……………. 11
1.3.4 Signs, Symptoms and Diagnosis………………………………... 13
1.3.5 Risk Factors of Glaucoma………………………………………. 14
1.3.5.1 Raised Intraocular Pressure…………………………… 14
1.3.5.2 Age……………………………………………………. 14
1.3.5.3 Ethnicity………………………………………………. 14
1.3.5.4 Miscellaneous Factors……………………………..…. 14
1.3.6 Treatment of Glaucoma…………………………………………. 14
1.4 Age-Related Macular Degeneration……………………………………. 15
1.4.1 Prevalence of AMD……………………………………………... 16
1.4.2 Clinical Classification of AMD………………………………… 16
1.4.2.1 Dry AMD……………………………………………... 16
1.4.2.2 Wet AMD……………………………………………... 17
1.4.3 Pathophysiology of AMD…………..…………………………... 17
1.4.2.1 Formation of Drusen………………………………….. 17
1.4.2.2 Formation of Lipofuscin……………………………… 20
1.4.2.3 Choroidal Neovascularization and Inflammation…….. 20
1.4.4 Risk Factors……………………………………………………... 21
1.4.4.1 Age……………………………………………………. 21
1.4.4.2 Smoking………………………………………………. 21
1.4.4.3 Diet……………………………………………………. 21
1.4.4.4 Exposure to Sunlight………………………………….. 21
1.4.5 Treatment of AMD……………………………………………… 22
1.5 Molecular Pathology of Glaucoma and AMD…….……………………. 23
1.5.1 Role of Oxidative Stress in Glaucoma and AMD………………. 23
1.5.2 Role of Immune system in Glaucoma and AMD……………….. 27
1.6 Genetic Etiology of Glaucoma and AMD……...………………………. 28
1.6.1 Molecular Genetics of Glaucoma……………………………… 29
1.6.2 Molecular Genetics of AMD…………………………………... 33
1.7 Study Overview………………………………………………………… 34

xiii
2 Materials & Methods………………………………………………………….. 36
2.1 Ethics Statement…………………………………………………………. 37
2.2 Participants of the Study…………………………………………………. 37
2.2.1 Families with Glaucoma and AMD……………………………… 37
2.2.2 Sporadic Cases and Controls…………………………………….. 37
2.3 Clinical Diagnostic Criteria……………………………………………… 39
2.3.1 Diagnosis of Sporadic Cases…………………………………….. 39
2.3.2 Diagnosis of Families……………………………………………. 39
2.4 Collection of Blood Samples and Genomic DNA Extraction……………. 40
2.4.1 DNA Extraction and Dilution……………………………………. 40
2.5 Screening Glaucoma and AMD Families………………………………... 41
2.5.1 Exclusion of Known Genes…..………………………………….. 41
2.5.1.1 Primer Design and Polymerase Chain Reaction……….. 41
2.5.1.2 Sanger Sequencing and InSilico Analysis of Variants... 41
2.5.1.3 Segregation Analysis of Variants in OPTN, MYOC and
WDR36…………………………………………………
42
2.5.1.4 Mutation and Segregation Analysis of Variants in
CYP1B1………………………………………………...
42
2.5.2 Homozygosity Mapping Using Microarray Analysis……………. 43
2.5.2.1 Brief 250K Microarray Protocol………………………. 43
2.5.3 In Silico Analysis of 250K Microarray Data…………………….. 43
2.5.4 CA-repeat Marker Analysis……………………………………… 43
2.5.5 Plausible Candidate Gene Analysis and Mutation Screening…… 44
2.6 Exome Sequencing……………………………………………………….. 45
2.6.1 Exome Variant Filtering….……………………………………… 49
2.6.1.1 Variant Filtering in Recessive Families……………….. 49
2.6.1.2 Variant Filtering in Dominant Families……………….. 49
2.6.2 Variant Screening and Validation………………………………... 50
2.7 Screening of Sporadic Cases……………………………………………... 50
2.7.1 SNPs Genotyped by Taqman® / KASPar Assay…….................. 51
2.7. 2 PCR Restriction Fragment Length Polymorphism Analysis…… 51
2.7.3 Variable Number of Tandem Repeat (VNTR) Genotyping….…. 59
2.7.4 Variation Analysis by Sanger Sequencing…………….………... 59
2.8 Statistical Analysis……………………………………………………….. 61
3 Results………………………………………………………………………….. 62
3.1 Results of Glaucoma Families………………………………………….. 63
3.2 Exclusion of Known Genes…………………………………………….. 63
3.2.1 MYOC, OPTN, WDR36 and CYP1B1 Screening……………….. 63
3.2.1.1 MYOC, OPTN and WDR36 Analysis………………… 63
3.2.1.2 Identification of a Homozygous CYP1B1 Mutation in
PCG Family GLC 16………………………………….
65
3.3 SNP Microarray Analysis Results…………………………..………….. 69
3.3.1 Identification of a Possible Novel Locus of Primary Congenital
Glaucoma……...
69
3.3.2 Identification of Homozygous Region in JOAG Family
GLC4……...……………………………………………………
73

xiv
3.3.3 Identification of Homozygous Region in Juvenile Open Angle
Glaucoma Family GLC 8…………………...………………….
76
3.4 Next Generation Sequencing Analysis ………………………………… 79
3.4.1 Identification of Three Variants MYO18A, ENOX1 and
COL9A2 in JOAG Family GLC 1……………………………..
79
3.4.2 Identification of a Variant in PHKG1 in JOAG Family GLC 5.. 82
3.5 Case-Control Association Studies ……………………………………... 85
3.5.1 Case-Control Studies of Glaucoma……………………………. 85
3.5.1.1 Screening BIRC6 and PDIA5 Polymorphisms in
Glaucoma Cohort …………………………………….
85
3.5.1.2 Screening OPTN and MYOC Polymorphisms in
Glaucoma Cohort……………………………………..
88
3.5.1.3 Screening Oxidative Stress and Apoptotic Pathway
Gene Polymorphisms in Glaucoma Cohort…………..
88
3.5.1.4 Screening PLEKHA7, COL11A1, PCMTD1
Polymorphisms in PACG Cohort…………………….
94
3.6 Results of AMD Families...…………………………………………….. 94
3.7 Case-Control Studies of AMD………………………………………….. 97
3.7.1 Screening Polymorphisms Known AMD Genes…………..…... 98
3.7.1.1 CFH and ARMS2…………………………………….. 98
3.7.1.2 C2/CFB……………………………………………..... 98
3.7.1.3 C3…………………………………………………….. 101
3.7.2 Screening Polymorphisms in Lipid pMetabolism Associated
Gene…………………………………………………………….
101
3.7.2.1 APOE………………………………………………… 101
3.7.3 Screening Polymorphisms in Immune System Pathway Gene.. 104
3.7.3.1 CX3CR1……………………………………………… 104
3.7.4 Screening Vascular System Related Gene Polymorphisms…… 106
3.7.4.1 VEGF………………………………………………… 106
3.7.4.2 Intron 4, 27bp VNTR in NOS3………………………. 108
3.7.5 Screening Polymorphisms in Genes Implicated in Oxidative
Stress……………………………………………………………
108
3.7.5.1 MMPs………………………………………………… 108
3.7.5.2 TIMP3………………………………………………... 111
3.7.5.3 TNF and ILβ………………………………………….. 111
3.8 Summary……………………………………………………………….. 114
4 Discussion……………………………………………………………………… 121
4.1 Glaucoma Families…………………………………………………….. 122
4.2 Case-Control Association Analysis: Glaucoma………………………... 128
4.3 Familial Screening and Case-Control Association Analysis: Age-
Related Macular Degeneration………………………………………….
138
4.4 Conclusion……………………………………………………………… 145
4.5 Future Perspective……………………………………………………… 145
5 References……………………………………………………………………… 147

xv
Fig 1.1
Cross sectional view of the eye……………………………………………..
3
Fig 1.2 A schematic diagram of the retina…………………………………………. 7
Fig 1.3 Differences between an RPE cell of a 3-year old child and an 80-year old
person……………………………………………………………………….
18
Fig 1.4 Pathological mechanisms involved in glaucoma…………………………... 24
Fig 1.5 Pathological mechanisms involved in AMD……………………………….. 25
Fig 3.1 Segregation analysis and sequencing chromatogram of identified variants
in OPTN in POAG families………………………………………………...
66
Fig 3.2 Sequence chromatogram of rs11258194; c.293T>C; p.Met98Lys in OPTN. 67
Fig 3.3 Pedigree of a large consanguineous Pakistani family with PCG (GLC 16).. 68
Fig 3.4 Clinical analyses of the two affected members in the PCG family GLC 2.... 70
Fig 3.5 Homozygosity mapper plot of the PCG family (GLC 2)............................... 71
Fig 3.6 Homozygous region linked to PCG in two affected individuals II: 3 and II:
4 of family GLC 2..........................................................................................
72
Fig 3.7 Homozygosity mapper plot of homozygous regions in a juvenile open
angle glaucoma family GLC 8.......................................................................
74
Fig 3.8 Pedigree of a recessive consanguineous Pakistani family with juvenile
open angle glaucoma (GLC 4)................…………………………………...
75
Fig 3.9 Pedigree of a consanguineous Pakistani family with juvenile open angle
glaucoma (GLC 8)…………………………………………………………..
77
Fig 3.10 Homozygosity Mapper plot of homozygous regions in juvenile open angle
glaucoma family GLC 8………………………………...…………………..
78
Fig 3.11 Pedigree of a consanguineous Pakistani family with JOAG (GLC 1a & 1b) 80
Fig 3.12 Retinal Nerve Fiber Layer thickness for patient IV:10 of JOAG family 1a 81
Fig 3.13 Pedigree of a consanguineous Pakistani family with late-onset glaucoma
(GLC 1b)……………………………………………………………………
83
Fig 3.14 Pedigree of a consanguineous Pakistani family with JOAG GLC 5……….. 84
Fig 3.15 Pedigree of non-consanguineous Pakistani families with AMD…………… 96
Fig 3.16 Forest plot of the SNPs screened for POAG……………………………….. 115
Fig 3.17 Forest plot of the SNPs screened for PACG……………………………….. 116
Fig 3.18 Forest plot of the SNPs screened for PEXG……………………………….. 117
Fig 3.19 Forest plot of the SNPs screened for wet AMD……………………………. 118
Fig 3.20 Forest plot of the SNPs screened for dry AMD……………………………. 119
Fig 4.1 Summary of the SNPs genotyped in glaucoma…………………………...... 129
Fig 4.2 Summary of the SNPs genotyped in AMD.................................................... 140
LIST OF FIGURES

xvi
Table 1.1 Loci associated with glaucoma…………………………………………. 30
Table 1.2 Genes and polymorphisms associated with POAG and PACG……….... 32
Table 2.1 Overview of collected glaucoma and AMD families ….………………. 38
Table 2.2 Primer sequences of CA repeat markers used for the chromosome 3
locus in PCG family GLC 2………………………..……………………
46
Table 2.3 Primer sequences of CA repeat markers used for the chromosome 7
locus in PCG family GLC 2…………………………
47
Table 2.4 Primer sequences of CA repeat markers used for the chromosome 15
locus in PCG family GLC 2……………………………………………..
48
Table 2.5 Exome variants and their primer sequences screened in JOAG family
GLC 5…………………………………………………………………...
52
Table 2.6 Variants detected by exome sequencing and analysed for segregation in
JOAG family GLC 1………………….………………………..………..
55
Table 2.7 Homozygous variants detected by exome sequencing and analysed for
segregation analysis in PCG family GLC 2……………………………
58
Table 2.8 Primer sequences and restriction enzymes used for RFLP analysis…..... 60
Table 3.1 Recurrent SNPs and de novo variations in glaucoma and AMD
associated genes identified by sequencing........…………………………
64
Table 3.2 Demographic and clinical features of the control, POAG, PACG and
PEXG cohorts…………………………………………………………...
86
Table 3.3 Results of logistic regression analysis for genotype and allele
frequencies of SNPs rs11720822 in PDIA5 and rs2754511 in BIRC6 in
POAG, PCAG and PEXG patients and control individuals…………….
87
Table 3.4 Logistic regression analysis for rs11258194, rs10906308 in OPTN and
rs2234926 in MYOC in Pakistani glaucoma cohorts and controls………
89
Table 3.5 Haplotype analysis of OPTN polymorphisms rs11258194 and
rs10906308 in Pakistani POAG cohorts………………………………...
90
Table 3.6 Logistic regression analysis of allele frequency distribution of P21
(rs1801270), P450 (rs2567206), P53 (rs1042522), HSP70 (rs1043618)
and NOS3 (27bp intron 4) polymorphisms in Pakistani glaucoma
cohorts and controls……………………………………………………..
92
Table 3.7 Allele frequency distribution of P21 (rs1801270), P450 (rs2567206),
P53 (rs1042522), HSP70 (rs1043618), and NOS3 (27bp intron 4)
polymorphisms in Pakistani glaucoma cohorts and controls…………...
93
Table 3.8 Logistic regression analysis of genotype and allele frequency
distribution of COL11A1 (rs3753841), PCMTD1 (rs1015213), and
PLEKHA7 (rs11024102) polymorphisms in Pakistani PACG cohorts
and controls……………………………………………………………...
95
Table 3.9 Logistic regression analysis of genotype and allele frequency
distribution of polymorphisms rs1061170 in CFH and rs10490924 in
ARMS2 in AMD patients and controls…………………………………..
99
Table 3.10 Logistic regression analysis of genotype and allele frequency
distribution of rs429608 polymorphism near C2/CFB in AMD patients
and controls……………………………………………………………...
100
Table 3.11 Logistic regression analysis of genotype and allele frequency
distribution of rs2230199 polymorphism near C3 in AMD patients and
controls…………………………………………………………………..
102
LIST OF TABLES

xvii
Table 3.12 Logistic regression analysis of genotype and allele frequency
distribution of rs4420638 polymorphism near APOE in AMD patients
and controls……………………………………………………………...
103
Table 3.13 Logistic regression analysis of genotype and allele frequency
distribution of rs3732378 and rs3732379 polymorphism in CX3CR1 in
AMD patients and controls……………………………………………...
105
Table 3.14 Logistic regression analysis of genotype and allele frequency
distribution of VEGF polymorphisms in AMD patients and controls…..
107
Table 3.15 Logistic regression analysis of genotype and allele frequency
distribution of 27bp VNTR polymorphism in NOS3 in AMD patients
and controls……………………………………………………………...
109
Table 3.16 Logistic regression analysis of genotype and allele frequency
distribution of MMP9 (rs17576) and MMP2 (rs243866) polymorphism
in AMD patients and controls…………………………………………...
110
Table 3.17 Logistic regression analysis of genotype and allele frequency
distribution of rs5749482 polymorphism near TIMP3 in AMD patients
and controls……………………………………………………………...
112
Table 3.18 Logistic regression analysis of genotype and allele frequency
distribution of polymorphisms rs1800629 in TNF and rs16944 in ILβ in
AMD patients and controls……………………………………………...
113

xviii
Annexure 1 Product size and primer sequences used to amplify the exons
and intron-exon junctions of MYOC and OPTN ………………
187
Annexure 2 Product size and primer sequences used to amplify exons and
intron-exon junctions of WRD36 and CYP1B1…………………
189
Annexure 3 Standard PCR reagent concentrations…………………………. 191
Annexure 4 Product size and primer sequence and PCR products for
candidate genes in the homozygous regions of families GLC 2,
GLC 4 and GLC 8………………………………………………
192
Annexure 5 Product size and primer sequences for the gene SH3PXD2B…. 194
Annexure 6 Homozygous regions obtained in the affected members of
families GLC 2, GLC 4 and GLC 8.............................................
195
Annexure 7 Unsolved glaucoma families........................................................ 196
Annexures

xix
LIST OF ABBREVIATIONS
Alpha
Beta
g Microgram
l Microliter
m Micrometer
A2E N-retinylidene-N-retinylethanolamine
AMD Age-Related Macular Degeneration
Apo-B Apolipoprotein B
ARM Age-Related Maculopathy
ARMS2 Age-Related Maculopathy Susceptibility 2
BAM Binary Sequence Alignment/Map format
BM Bruch’s Membrane
C3 Complement Component 3
CDR Cup-to-Disc Ratio
CETP Cholesteryl Ester Transfer Protein
CFH Complement Factor H
CNV Choroidal Neovascularization
CYP1B1 Cytochrome P450
ECM Extracellular Matrix
ET-1 Endothelin 1
GAGs Glycosaminoglycans
GWAS Genome-Wide Association Study
HDL High Density Lipoprotein
HSPs Heat Shock Proteins
HTG High Tension Glaucoma
HTRA1 High temperature requirement A1
IL Interleukin Beta
IOP Intraocular Pressure
LIPC Hepatic Lipase
LPL Lipoprotein Lipase
MYOC Myocillin
NO Nitric Oxide
NTG Normal Tension Glaucoma
ONH Optic Nerve Head
OPTN Optineurin
PACG Primary Angle Closure Glaucoma
PCG Primary Congenital Glaucoma
PEDF Pigment Epithelium Derived Factor
PEXG Pseudoexfoliative Glaucoma
POAG Primary Open Angle Glaucoma
PUFAs Poly Unsaturated Fatty Acids
RFLP Restriction Fragment Length Polymorphism
RNFL Retinal Nerve Fiber Layer
ROS Reactive Oxygen Species
RPE Retinal Pigment Epithelium
SCRs Short Consensus Repeats
SIG Steroid Induced Glaucoma
TM Trabecular Meshwork
TNF Tumor Necrosis Factor Alpha

xx
VEGF Vascular Endothelial Growth Factor
WDR36 WD repeat domain 36
NOS3 Endothelial Nitric Oxide Synthase
HSP70 Heat Shock Protein 70

Chapter 1
Introduction

2
1 Introduction
1.1 Multifactorial Diseases
Diseases involving multiple causative factors are known as multifactorial diseases. These
factors can be environmental, metabolic, functional or genetic, with strong interactions
between them. Several organs of the human body might be affected because of the complex
interactions of these factors.
There are many diseases of the eye that are multifactorial in nature e.g. myopia, diabetic
retinopathy, dry eye disease, age-related macular degeneration (AMD), glaucoma, etc.
According to the global data on visual impairment, 16 million people around the globe are
visually impaired, while 37 million are blind due to the presence of different eye diseases,
and, in addition, 137 million people have low vision. Of the visually impaired, glaucoma
and age-related macular degeneration are the major cause after cataract (Resnikoff et al.,
2004). The main focus of the current study was to explore the genetics of the multifactorial
eye diseases glaucoma and AMD.
1.2 Anatomy of the Eye with Reference to Glaucoma and AMD
Vision is one of the five most widely used senses that enable human beings to see their
surroundings. The eye is the organ that is involved in the vision process, which can be
divided into three segments namely outer, interior and posterior segments and it also
consists of the optic nerve head (ONH).
1.2.1 Outer Segment
The outer segment of the eye includes the eye lid, orbit and sclera; these parts protect the
eye from external hazards.
1.2.2 Interior Segment
The interior segment consists of the cornea, iris, aqueous humor, lens, ciliary body, stroma
and pupil, which are mostly involved in focusing the light coming from an object and
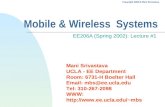
maintaining the pressure in the eye (Fig.1.1). The cornea is the transparent portion of the

3
Figure 1.1 Cross sectional view of Eye (Patel and Lundy 2002)

4
eye with no blood supply and allows the light rays to enter the eye through it. Corneal
transparency is lost at the ends where it merges into the sclera; this point of merging is
called the limbus. There is a fluid filled chamber between the lens and the cornea, which
is known as the aqueous chamber. The fluid in the aqueous chamber is secreted by the
ciliary body and is known as aqueous humor (Riordan-Eva and Whitcher 2007). This fluid
provides nutrients to the cornea and the lens, and provides the path to the light rays entering
the eye. Aqueous humor is also involved in maintaining the pressure inside the eye
(Agarwal et al., 2003; Morrison and Pollack 2011). Once the nutrients from the fluid are
extracted, it is secreted from the chamber via the drainage system i.e the trabecular
meshwork (TM) that lies behind the limbus. The fluid passes through the angle between
the cornea and anterior iris which is known as angle of the anterior chamber or iridocorneal
angle. Almost 80% of the fluid is secreted through this passage and empties into the
episcleral venous pathway; the remaining 20% of the fluid is secreted via the Schlemm’s
canal through the uveoscleral pathway (Distelhorst and Hughes 2003). The fluid outflow
is hindered to maintain the intraocular pressure (IOP) between 15-21 mmHg, which thus
maintains the proper shape of the eye and keeps all tissues in their proper position
(Morrison et al., 2005). The iris is the colored portion of the eye and can be viewed from
the cornea. This structure controls the amount of light entering the eye via a small opening;
the pupil (Michael 2005).
1.2.3 Posterior Segment
The posterior segment of the eye consists of the vitreous and retina. The vitreous is a clear
gel like fluid, which fills the posterior segment of the eye and also provides protection to
it. At the anterior side, the vitreous is in contact with the ciliary body and the lens, whereas
on the posterior side it comes in contact with the retina (Corina 1999).
The retina is a thin, almost transparent tissue, which is specialized in capturing the light
photons and initiates the process of image formation by the brain. It is composed of ten
layers of neurons interconnected by synapses and supporting cells. The deepest layer of the
retina is composed of the retinal pigment epithelium (RPE). The RPE is a single layer of
pigmented cells and is crucial for normal metabolic and supportive functions of the retina
(De Jong 2006). It serves as an obstruction in flow of ions, nutrients, metabolic products,

5
and water between the retina and the choriocapillaries. It is also responsible for the
restoration of the visual cycle (conversion of excited trans-retinal to 11-cis retinal and
recycling it back to the photoreceptors). The photoreceptors shed their tips, which are
degraded by the lysosomes through the phagocytic activity of the RPE. The regeneration
of the rod cells occurs at the base by the addition of the membrane of the outer segment,
whereas in the case of the cone cells replacement of lipids, proteins and membranes occurs
all over the individual cell rather than just at the base. This regeneration function of the
RPE is performed by the secretion of growth factors that maintain the photoreceptors,
endothelium and the choriocapillaries (Ehrlich et al., 2008). Moreover,
immunosuppressive factors are also secreted by the RPE that help to maintain the immune
functions of the eye (Strauss 2005).
The rest of the nine layers of the retina are involved in the conversion of light into
electrochemical signals and subsequently transmission of these signals to the brain via the
optic nerve for image formation. The macula lutea is the central yellow portion of the retina
with a diameter of about 6mm and is responsible for central vision. Central to the macula
is a depression known as the fovea, which has the highest concentration of cone
photoreceptor cells and thus is responsible for sharp image formation and color vision. The
yellowish appearance of the macula is caused by the presence of different pigments
consisting of antioxidants (xynthophill, carotenoids, lutein, zeaxanthin). Although only
0.5% of the retina is occupied by the fovea, 50% of the nerve fibers carry the information
from the fovea due to its dense concentration of the photoreceptor cells.
The rod and cone photoreceptors convert light into an electrical impulse. Their distribution
throughout the retina varies. The concentration of cones is highest in the fovea (199,000
cones/mm2) and decreases towards the periphery, whereas the concentration of the rods is
highest in the area at 20o from the fovea (160,000 rods/mm2). The photoreceptor density
also decreases towards the periphery. The cones contain a visual pigment known as opsin,
which is sensitive to a wide range of wavelengths, depending on the structure of the opsin
molecule. ‘L’ cones are sensitive to light with long wavelengths (red light, 564 nm), ‘M’
cones are sensitive to light with medium wavelengths (green light, 533 nm) and ‘S’ cones
to light with short wavelengths (blue light, 437 nm). The rods contain visual pigment called

6
rhodopsin, and are sensitive to blue-green light (500 nm). Rods enable vision in dim light,
are sensitive enough to even detect a single photon of light and are able to detect contrast,
motion and brightness (Provencio et al., 2000).
The Bruch’s membrane (BM) is a three-layer connective tissue sandwiched between two
basement membranes: the RPE basement membrane and choriocapillary basement
membrane (Figure 1.2). The three layers of BM are the inner collagenous layer adjacent to
the RPE known as the RPE basement membrane, an elastic central layer, and the outer
collagenous layer adjacent to the choriocapillaries basal lamina (Sivaprasad et al., 2005;
De Jong 2006). BM plays two important functions in the eye; structural support and
transport facilitation. It covers more than half of the eye and whenever extra pressure is
exerted due to raised IOP or increasing blood volume in the choroid, BM adjusts with it,
stretching along with the corneoscleral envelope, and when the pressure is lowered the
membrane reverts back to its original position (Beers and Heijde 1994; Charman 2008).
The choriocapillaries lie just behind the BM and provide the choroidal vasculature for the
transport of nutrients and waste products to and from the photoreceptors via the RPE and
BM (Nowak 2006). The transport of nutrients takes place from the choriocapillaries to the
RPE, and waste product removal occurs in the opposite direction via the BM. Certain
factors necessary for the proper functioning of the photoreceptors such as signalling
molecules and vitamins are carried to the RPE in the form of lipoproteins passing through
the BM. The fluid in the eye is moved from the RPE to the BM, which then passes to the
capillary bed and is subsequently taken away to the main blood stream. With advancing
age, significant changes occur in the BM that hinder its transport function, resulting in
accumulation of the waste material in the BM (Curcio and Johnson 2013). The retina
requires more oxygen as compared to any other tissue (Nowak 2006). In dark conditions
the photoreceptors are anoxic and thus are dependent upon the choriocapillaries for the
provision of oxygen, which provides 90% of it. Any harm to the capillaries can prove to
be fatal to the photoreceptors (Jong 2006). To fulfill the energy requirements of the retina,
it is enriched by two systems of the vasculature, the retinal vessels and the choriocapillary
bed. The retinal vessels provide nutrients to the inner retina, whereas the choroid provides

7
Figure 1.2 A schematic diagram of the retina is shown in the figure. The inset shows the choroid and layers of the retina, including the
retinal pigment epithelium (RPE) Bruch’s membrane (BM) choroid, rod cells & cone cells and basement membranes [modified; Zhang
et al., 2012]

8
nutrients to the outer retina, which is completely devoid of vessels (Campochiaro 2004;
Das and Mcguire 2003).
1.2.4 Optic Nerve Head
The optic nerve head (ONH) is a central convergence point for all retinal ganglion cells,
comprised of 1.2 million ganglion cell axons (Morrison and Pollack 2011). The nerve fibers
of these ganglion cells leave the eye at the optic disc where it forms a depression called the
cup, whereas the outer rim of this region is known as the disc (Quigley 2011). The optic
disc is 1.5 mm in diameter and the cup is 0.3 mm, with the ratio between the two in a
normal eye around 1:3 (Morrison and Pollack 2011; Karen 2006). The optic disc consists
of nerve fiber layers only and thus is not involved in any excitatory visual process; therefore
it is also referred to as the blind spot of the eye. Some ganglion cells have a pigment known
as melanopsin, which is not involved in image formation but is involved in the rapid
adjustment of the pupil size (Provencio et al., 2000).
Damage to the ONH or macula due to the interplay of multiple factors results in glaucoma
and AMD, respectively.
1.3 Glaucoma
Glaucoma is a group of nurodegenerative eye disorders, generally characterized by optic
nerve damage in one or both eyes, subsequently resulting in gradual narrowing of the visual
field. The damage is a result of the death of the retinal ganglion cells and axons in the optic
nerve (Quigley 2011). It is the second major cause of blindness worldwide (Resnikoff et
al., 2004), affecting mostly Asians (Stein et al., 2011) and Africans (Ntim-Amponsah et
al., 2004). More than 67 million people are estimated to suffer from glaucoma at present
(Quigley 1996), and the number is expected to rise to 80 million by the year 2020 (Varma
et al., 2011).
1.3.1 Types of Glaucoma
Glaucoma can be divided into primary glaucoma and secondary glaucoma. In primary
glaucoma the etiology of the disease is unknown. This form of glaucoma can be divided
into three subclasses: primary open angle glaucoma (POAG), primary angle closure

9
glaucoma (PACG) and primary congenital glaucoma (PCG). In secondary glaucoma the
etiology is usually known, and most often this category is named after the causative factor.
Secondary glaucoma consists of pseudoexfoliative glaucoma (PEXG), steroid induced
glaucoma (SIG), neovascular glaucoma, and pigmentary glaucoma.
1.3.1.1 Primary Open Angle Glaucoma
The most common type of glaucoma is POAG; a progressive chronic neuropathy of the
eye, in which many factors play a role in initiation, progression and damage to the optic
nerve with irreversible vision loss (Center 2007). POAG is a complex disease and its
classification is based on the age of onset (0-3 years primary congenital glaucoma; 10-35
years, juvenile-onset glaucoma, JOAG; 36 years and above adult glaucoma) (Gemenetzi et
al., 2012). POAG is not always associated with raised IOP and hence can also be classified
into NTG and high tension glaucoma (HTG), which classification is based upon the
pressure in the eye. In NTG the pressure remains in the normal range (less than 21mmHg),
but lowering the pressure further protects the ONH from further damage (Valk et al., 2005).
The patient becomes aware of the problem only when considerable damage has occurred
(Hewitt et al., 2006; Mukesh et al., 2002). Although the IOP is not raised in NTG, the loss
to the ONH and loss of vision is at the same level as in HTG. The reason for the occurrence
of POAG even at low pressure is still unclear, but genetic and environmental factors are
postulated to play a combined role in POAG (Fan et al., 2006).
The risk factors associated with POAG other than raised IOP (Tielsch et al., 1994), are
family history of the disease, hypertension and cigarette smoking (Wilson et al., 1987).
1.3.1.2 Primary Angle Closure Glaucoma
PACG anatomically is characterized by closure of the angle of drainage between the
trabecular meshwork (TM) and the iris (Tarongoy et al., 2009; Kim and Jung 1997). The
American Academy of Ophthalmology classifies the primary group of angle closure into
primary angle closure suspect, primary angle closure without damage and the final stage
of PACG (Tarongoy et al., 2009). PACG is more aggressive as compared to POAG, and
patients suffer from an acute and sudden attack resulting in loss of vision, but this condition
is preventable. The blockage in PACG occurs via two mechanisms; papillary block

10
mechanism and angle crowding, both of which result in abrupt elevation of IOP leading to
glaucomatic changes in the eye. The aqueous humor flows from its site of production into
the posterior chamber and then to the anterior chamber, flowing from underneath the iris,
above the lens, passing through the pupil and finally flows out from the TM. There is a
pressure difference of 0.23 mmHg in the posterior chamber and the anterior chamber (Heys
et al., 2001). In pupillary blockage, this pressure increases to 10-15 mmHg, which results
in the increased convexity of the iris, resulting in iris bombe´ that blocks the TM and thus
the drainage route of the aqueous humor. The eye anatomy is the strongest risk factor for
the development of PACG. The shape and the size of iris, placement of the lens and
anatomy of the ciliary body are the usual factors for the pupillary block. The other mode
of development of PACG is the mechanism of angle crowding, in which the iris is
sandwiched between the TM and the ciliary body forming a raised iris arrangement called
plateau iris, which then blocks the drainage of the aqueous humor and results in the raised
IOP (Wand et al., 1977; Tarongoy et al., 2009). Patients suffering from PACG also
experience pain in the eyes, vision blurring, headache, eye redness, vomiting, nausea and
circles of rainbow color around a light source. The pain radiates to the head and sinuses
and might cause corneal edema as well (Morrison and Pollack 2011). Family history, age,
and female gender are risk factors of PACG (Coleman 1999; Karen 2006)
1.3.1.3 Pseudoexfoliative Glaucoma
PEXG is a secondary form of glaucoma, occurring in the eye(s) mostly with an age-related
systemic disorder known as exfoliation syndrome (Viso et al., 2010). The syndrome is
present in almost 25% patients of open angle glaucoma (OAG) worldwide (Ritch and
Schlotzer-Schrehardt 2001). PEXG is characterized by the deposition of fibrillar
exfoliative material on the aqueous bathed surfaces of the eye including the lens, the non-
pigmented iris epithelium and trabecular and corneal endothelium (Naumann et al., 1998;
Ritch and Schlotzer-Schrehardt 2001). The disease usually manifests when the normal
passage of aqueous humor is blocked in the TM due to the accumulation of fibrillar
material, which leads to raised IOP causing OAG (Johnson et al., 2008), which is
considered to be the primary cause of the development of glaucoma in PEX syndrome.

11
1.3.1.4 Syndromic Forms of Glaucoma
There are various systemic disorders that involve ocular abnormalities. Several with
abnormalities of the anterior segment result in glaucomatic changes in the ONH and are
known as glaucoma syndromes (Wiggs 2007). These syndromes include for example Nail
patella syndrome, Alfred Reiger’s syndrome, aniridia pigment dispersion syndrome, an
Marfan’s syndrome.
1.3.2 Prevalence
Being the second most prevalent disease responsible for causing bilateral blindness,
glaucoma affects 16 million people worldwide, ¾ of whom suffer from POAG. Females
are mostly affected, comprising 55% of POAG patients, 70 % of PACG and 59% of other
types of glaucoma. Among various ethnic groups of the world, Asians are more prone to
develop glaucoma after Africans, who have the highest chance of developing glaucoma.
Among Asians, Chinese have a higher incidence of PACG patients, whereas the Japanese
have higher number of normal tension glaucoma (NTG) patients. The prevalence of POAG
is similar among various populations of the world, with the exception of Africans, where
it is the highest (Cook and Foster 2012).
1.3.3 Pathophysiology of Glaucoma
The pathophysiological features of glaucoma revolve around the TM, outflow of the
aqueous humor, the retinal ganglion cells and the optic nerve.
The TM is the vital drainage pathway for the normal outflow of the aqueous humor (Tamm
2009). Pressure is built up inside the anterior chamber of the eye in response to any
resistance in the outflow of aqueous humor from the TM (Gabelt and Kaufman 2005). A
normal pressure is necessary to maintain the normal shape of the eye and keep various
tissues in their respective positions. At stable IOP, the production rate of aqueous humor
in the ciliary body and its outflow is balanced due to a basal resistance, which helps
maintain the pressure around 20-21 mmHg. With advancing age, various physiological
changes occur in the TM. As a result, the resistance increases hindering the normal outflow
of the aqueous humor and raising the IOP (Gabelt and Kaufman 2005). The TM outflow is

12
responsible for 80% of the aqueous humor drainage, while the rest of it is done by the
uveoscleral pathway (Alm and Nilsson 2009)
A raised IOP results in disturbances in the microcirculation of nutrients to the ganglion
cells. In addition, a raised IOP can also directly damage these cells by triggering apoptosis
(Osborne et al., 2001). Moreover the TM cells have the capability of producing
extracellular matrix (ECM) components and when these components attach to the ECM, it
starts generating various cellular signals thus acting as a signaling molecule (Zhou et al.,
2000). These cells also act as phagocytes and thus have the ability to detach from the site
of formation and move around. With advancement in age these cells become committed to
phagocytosis more than any other function; once they detach from their place of origin they
may be lost via Schlemm’s canal. The TM cells are lost at a rate of 12,000 cells/ year as a
result of their movement (Gabelt et al., 2003). This decrease in the TM cells resultantly
hinders the catabolic organization of the cellular matrix (Grierson et al., 1982). Besides,
accumulation of debris in the TM blocks the drainage of the TM, and thus the nutrients
present in the aqueous humor do not reach the TM cells. In addition this also blocks the
toxic metabolites that are needed to be removed (Kaufman., 1995). Another mechanism
for the loss of retinal nerve fibers in glaucoma is accumulation of plaques that covers the
fine fibrils, which connect the ciliary epithelium and matrix of the TM thus thickening it
(Gottanka et al., 1997). The exact relationship of loss of the retinal nerve fibers with the
accumulation of the sheath particles is not known but it is postulated that the factors that
affect the formation of the sheath are the same that result in the death of the retinal fibers,
moreover, they may act in combination with IOP or by themselves may be enough to cause
the damage (Gabelt and Kaufman 2005). This accumulation results in disruption of the
cellular arrangement and death of astrocytes (neurosupportive cells; a type of glial cells
present in abundance in retina) leading to optic cupping. The death of the cells in the ONH
results in its progressive thinning till the ratio between optic rim (disc) and optic cup
decreases to 1 (Hernandez 2000). The primary damage to the optic nerve is also thought to
be due to compliance, a phenomenon in which the ONH is pushed back due to the raised
IOP, reverting to its original position when the pressure is reduced (Burgoyne et al., 1995),
this phenomenon results in disorganization of the ONH structure. If the pressure remains
high for a longer period of time, it results in reduced compliance, which then causes the

13
initial insult to the axons, besides resulting in the accumulation of the ECM material
(Johnson et al., 2000). The raised IOP also interferes with the transfer of nutrients
(neurotrophins) to the axons of the ganglion cells, and results in neuronal cell death
(Quigley 1999). Moreover, cellular apoptosis of the retinal ganglion cells is also one of the
mechanisms that can lead to pathophysiological changes of glaucoma (Quigley et al.,
1995).
1.3.4 Signs, Symptoms and Diagnosis
Raised IOP is considered to be the most important sign of glaucoma but this is not always
the case. Lower elevation in IOP indicates suspicion of glaucoma and higher eye pressure
clearly indicates the development of the disease (Coleman 1999). Rapid elevation to
extreme levels (which is mostly the case in PACG) results in sudden and chronic insult to
the ONH and rapid loss of vision. In the case of POAG, the IOP remains between 20-30
mmHg, thus causing progressive damage over a number of years (Karen 2006). A
tonometer is used to measure the IOP, to assess the individuals at risk of developing
glaucoma.
Cupping of the ONH is another symptom of glaucoma, which refers to the disturbance of
the cup-to-disc ratio. With the maximum number of axons dying, the ratio falls to 1:1,
resulting is maximum damage of the ONH (Coleman 1999; Adatia and Damji 2005).
Vision tunneling is an obvious sign of glaucoma and occurs due to the loss of ganglion
cells in the ONH (Arthur and Jan 2005). The progressive loss of the peripheral vision leads
to tunneling of the vision, and the patient remains unaware of the damage until only the
central vision is left (Buckingham et al., 2008). The visual field damage starts appearing
when 50 percent of the axons of the ganglion cells are dead (Cook 2009). Visual field
testing is done to measure the entire field of vision in both eyes individually in order to
estimate the damage to the field of vision as a result of glaucoma.
In addition, ophthalmic tests are conducted to differentiate between open angle and angle
closure glaucoma. A gonioscope is used to measure the angle of the anterior chamber of
the eye (Fraser and Manvikar 2005). Gonioscopy also helps to differentiate between
primary and secondary glaucoma (Morrison and Pollack 2011).

14
1.3.5 Risk Factors for Glaucoma
1.3.5.1 Raised Intraocular Pressure
Elevated IOP is the most important risk factor for glaucoma, and damage caused as a result
of elevated IOP is associated with disease progression. However, the role of IOP in
glaucoma is controversial in the case of NTG, as the pressure is normal. The disease
remains unnoticed until substantial damage has occurred (Rao 2014).
1.3.5.2 Age
Age is also a potential risk factor for glaucoma, although the disease can affect all age
groups (Drance 2008; Fraser and Manvikar 2005). The usual age range is from 10 years to
70 years for POAG, with the majority being affected after the age of 40 years (Alward et
al., 1998).
1.3.5.3 Ethnicity
The risk of development of glaucoma is higher among the Afro-Caribbean’s as compared
to white people. Africans are the most POAG susceptible ethnic group followed by Asians
(Quigley and Broman 2006)
1.3.5.4 Miscellaneous Factors
Gender is also a risk factor; females have been found to be more susceptible than males
(Quigley and Broman 2006). Vascular abnormalities, vasospasm, migraine, and diabetes
are also associated with glaucoma (Leske 2007; Fraser and Manvikar 2005). Family history
of glaucoma increases the risk many fold (Adatia and Damji 2005; Taylor and Keeffe
2001).
1.3.6 Treatment of Glaucoma
Glaucoma treatment involves only the management of IOP as it is the only treatable factor
known till date (Wilensky 1999). Once glaucoma is confirmed, controlling IOP can help
stop/slow down the progression of the disease (Lichter 2002). In the past, leeching

15
procedures were used to lower the IOP, but now medications are used to lower it. These
medications can be administered orally or in the form of ophthalmic drops.
These drops given to the patient are of different types. Miotics facilitate the flow of aqueous
humor out of the drainage system by opening it wider. Beta-blockers decrease the rate of
flow of the aqueous humor into the anterior chamber (Zimmerman and Kaufman 1977).
Lantoprost increases the flow of the aqueous humor out of the eye (Alm 2014).
Apraclonidine is used during surgeries and otherwise, to stop the sudden increase in IOP.
Sometimes when the IOP cannot be controlled with eye drops alone, a combination with
oral medication is prescribed, which targets the production of the aqueous humor.
Surgery for the treatment of glaucoma involves trabeculectomy, a procedure in which a
portion of the TM is removed surgically to facilitate the outflow of aqueous humor.
Although this procedure relieves the patient from pain and glaucoma medication, cataract
develops as an after effect of surgery mostly within 5 years. Laser surgery is becoming
more and more popular because of its fewer post-operative complications and also as it is
a painless procedure. In this procedure a laser beam is used to shrink the TM muscles,
resulting in widening of the path for the aqueous humor outflow.
1.4 Age-Related Macular Degeneration
Initial cases of age-related macular degeneration (AMD) were seen in 1875 by two
clinicians, Hutchinson and Tay, who explained the condition in aged patients due to
different changes in the fundus. Ten years later, in 1885, this condition was clinically
recognized and was known as “senile macular degeneration” by Otto Haab. Today it is
alternatively called AMD or age-related maculopathy (ARM) (Mcconnell and Silvestri
2005).
It is mainly a disease of the RPE layer of the retina that leads to various age-related changes,
causing deterioration of the photoreceptors primarily in the macular region resulting in loss
of central vision (Chen et al., 2010b). This loss of central vision adversely affects normal
daily chores of a person, such as reading, driving and facial recognition (Ehrlich et al.,
2008).

16
1.4.1 Prevalence of AMD
The usual age of onset of AMD is 50 years. Above the age of 65 years the disease
occurrence increases to 35%, and being prevalent mostly in people of 80 years of age.
Therefore, for AMD-based epidemiological studies, 50 years is chosen as the minimum
patient inclusion criterion (Bird et al., 1995). AMD is more prevalent in Caucasians as
compared to other populations (Chen et al., 2010b). AMD is common in the female gender
above the age of 75 years, and the prevalence of wet AMD is twice as high in females as
compared to males (Smith et al., 1997). Epidemiological studies in the U.S. have shown
that there are 8 million people suffering from intermediate AMD, whereas 2 million have
the advanced stages of the disease (Owen et al., 2003).
1.4.2 Clinical Classification of AMD
Changes in the macula are used to clinically diagnose AMD (Jong 2006), which can be
grouped into two classes: dry and wet AMD.
1.4.2.1 Dry AMD
Dry AMD can be classified as early, intermediate and late dry AMD. Characteristic
features of early AMD are the accumulation of small drusen without any significant loss
of vision. In intermediate AMD, accumulation of drusen occurs (both basal laminar and
basal linear deposits). Moreover, lipofuscin accumulation, thickening and disturbance in
the architecture of the BM and hyper- or hypo-pigmentation in the macular region also
takes place. The first sign of late dry AMD is the appearance of the geographic atrophy of
the RPE cells, and thus it is also known as geographic AMD or non-exudative AMD. This
results in the degeneration of the photoreceptor cells and thinning of the retinal layer, and
consequently, deterioration of vision. The retinal atrophy also moves to the other layers of
the retina, thus worsening the condition. Hyperpigmentation of the peripheral regions of
the patchy areas occurs in response to apoptosis of the RPE cells (Ding et al., 2009). Dry
AMD is responsible for loss of vision in 20% of the AMD patients (Ferris et al., 1984).

17
1.4.2.2 Wet AMD
A characteristic feature of wet AMD is the formation of new vessels in the sub-retinal
space, and therefore it is also known as neovascular AMD or exudative AMD. The classical
pattern of growth of these vessels is across the BM and into the sub-retinal space (Ding et
al., 2009). Vision is severely compromised, primarily due to hemorrhage and exudate
formation, and secondly due to the cellular apoptosis. The CNV can cause detachment of
the RPE or the retina. As the CNV progresses to the macular region, the elastic layer of the
BM becomes thin in the foveal region. This results in reduction of the foveal region to
55nm, also increasing the porosity of the foveal region to up to 35% (Ambati et al., 2003).
The end stage of wet AMD is disciform scar formation, vascularised by the choroid and
sometimes by the retinal blood supply as well. The bigger the scar is, the greater the loss
of the RPE and photoreceptors (Green and Enger 2005). People with wet AMD may also
develop blind spots.
1.4.3 Pathophysiology of AMD
The outer surface of the retina, which is a combination of RPE, photoreceptor cells (rods
and cones) and Bruch’s membrane (BM), faces the choroid and hence is dependent on the
choriocapillaries for nutrition, while the internal surface faces the vitreous chamber. All
these parts together are called Ruysch’s complex and are responsible for retinal function
(Jong 2006). With advancing age, degenerative changes in RPE, BM and choriocapillaries
(in the case of wet AMD) are the characteristic features of AMD (Coleman et al., 2008).
The pathological features of AMD involve changes in the RPE cells, Bruch's membrane
and photoreceptor cells (Fig. 1.3) and the mechanisms leading to AMD are formation of
the drusen, formation of lipofuscin, choroidal neovascularisation and inflammation.
1.4.3.1 Formation of Drusen
The clinical hallmark of AMD is the formation of deposits or drusen, which can vary in
color (white to yellow) and size (De Jong 2006; Nowak 2006). The particles of drusen
lump together as a result of the aging process, which in turn is due to many factors including
physiological changes, oxidative stress, inflammation and the activity of the immune
system, which all play a central role in the formation of drusen (Anderson et al., 2010).

18
Figure 1.3 Differences between an RPE cell of a 3-year old child and an 80-year old person.
The outer segments of the rods and cones are embedded in the interphotoreceptor matrix
(blue-gray areas) and partially surrounded by apical pseudopodial RPE processes). The
figure shows the shed disks (right-hand panel); digested by the RPE. The right-hand panel
shows enlarged lipofuscin granules, the thickened Bruch's membrane, and attenuation of
the choriocapillaries. The central elastic lamina in Bruch's membrane becomes more
porous in old age (De Jong 2006)

19
Drusen are generally composed of glycoproteins (central part), surrounded by
apolipoproteins (A & E), chaperone proteins, inflammatory proteins, fibronectin,
vitronectin and RPE debris (Jong 2006). The major components of drusen are lipids, which
originate from the membrane debris of the shed photoreceptor discs (Malek et al., 2003).
The RPE transports the membrane bound particles (secretary proteins, lipids, and
cytoplasm), and malfunctioning of the RPE is thus thought to be involved in the formation
of drusen in the BM. Moreover, ECM remodelling is also suggestive of drusen formation
due to its presence in different regions in the BM (Hageman and Mullins 1999; Luibl et
al., 2006). Moreover, drusen formation is probably an active and discriminatory process
rather than just a slow build-up of lipid and protein debris in the BM, and thus not only age
but also genetic components and environmental stress factors coalesce to cause the disease,
which explains why not all elderly people have AMD (Ehrlich et al., 2008; Sivaprasad et
al., 2005; Jong 2006).
Drusen, on the basis of their aggregation site in the BM and composition are classified into
two categories: basal laminar drusen and basal linear drusen. Basal laminar drusen are
located between the RPE and basement membrane of RPE (Russell et al., 2000), whereas
basal linear drusen are located between the RPE basement membrane and the inner
collagenous layer of BM (Curcio and Millican 1999). Basal laminar drusen are considered
as a histological finding of AMD, consisting mostly of collagen, fibronectin, laminin, and
lipids, which are formed during advanced stages of the disease (Yamada et al., 2006; Reale
et al., 2009). Basal linear drusen consist of lipoprotein particles and lipid aggregates that
stack together forming a lipid wall (Curcio and Millican 1999).
Based on the appearance of the boundary of drusen, they can be classified into ‘soft’ or
‘hard’, drusen. Soft drusen are known to accumulate in the macular region, increasing the
risk of AMD many-fold (Davis et al., 2005; Klein et al., 2007). Soft and basal linear drusen
are fragile, oily and not easily isolatable particles, and the lipids present in the soft drusen
are membranous debris (Rudolf et al., 2008). Hard drusen mostly accumulate in the
peripheral region and are easily isolated. The major components of hard drusen are
apolipoproteins and lipoproteins (Ryan et al., 2012)

20
1.4.3.2 Formation of Lipofuscin
Yellowish brown cellular debris, known as age pigment or lipofuscin, accumulates over
time in the RPE (Terman and Brunk 1998). It is composed of bisretinoids, lipids (~50%)
and proteins (~44%) (Julien and Schraermeyer 2012) and shed membranes of the outer
segments of photoreceptor cells (Saprunova et al., 2010). The accumulation of lipofuscin
causes the death of RPE cells and result in dark patchy areas (geographic atrophy) that
gives rise to dry AMD (Holz et al., 2007). Lipofuscin amassing in the RPE results in
adverse effects on the RPE. Its component N-retinylidene-N-retinylethanolamine (A2E)
seems to eliminate the acidic environment of the lysosome and thus hinders the degradation
activity of the lysosome, in turn hindering the phagocytic property of the RPE cells (Godley
et al., 2005). Moreover, A2E activates the complement system, which then results in
activation of the immune system (Radu et al., 2011). It also has the ability to stimulate the
production of reactive oxygen species (ROS) in response to light (Saprunova et al., 2010).
1.4.3.3 Choroidal Neovascularization (CNV) and Inflammation
Normally, endothelial cells control angiogenic signals, and thus a balance is maintained
between the pro-angiogenic factors (VEGF) and anti-angiogenic factors (pigment
epithelium derived factor, PEDF) (Das and Mcguire 2003). If this balance is disturbed as
a result of ischemia or hypoxia, it results in upregulation of angiogenic growth factors
(Campochiaro 2004). In the choriodal vasculature, besides ischemia and insult, also local
inflammation and activation of the immune system are thought to play a significant role in
the initiation and progression of CNV (Das and Mcguire 2003; Anderson et al., 2002). The
immune cells, like mast cells and neutrophils, have the ability to disrupt the balance of pro-
and anti-growth factors by releasing pro-angiogenic factors (Kijlstra et al., 2005). VEGF
and PEDF have been postulated to play a very important role in the formation of CNV, and
thus therapeutic strategies have been and are being developed to maintain the balance
between VEGF and PEDF (Nowak 2006). The new vessels (neovascularisation) thus
formed either remains under the RPE or they may break through the RPE cells and enter
the sub-retinal tissue. The blood from these vessels may also seep out into the sub-retinal
area giving it a grayish color (Ambati et al., 2003).

21
1.4.4 Risk Factors
1.4.4.1 Age
Age is a major risk factor for AMD. In the age group of 65-74 years, it is prevalent among
approximately 20% of people, and in the 75-84 year age group it occurs in almost 35% of
people (Bonnel et al., 2003). Major changes occurring with age are the accumulation of
lipids and lipofuscin formation in the BM, which when exposed to daylight generate ROS
that are potent in damaging the membranes (protein and lipid). A2E creates phototoxic
environment (via blue light), disrupting the membrane integrity, and apoptotic death of the
RPE cells. Similarly, lumping of drusen associated with AMD occurs with increasing age
(Sparrow et al., 2000; Schutt et al., 2000).
1.4.4.2 Smoking
Smoking is a single, strong, modifiable risk factor of AMD that increases the risk of
development of disease 2 to 4 times, and persists as a risk factor for even 20 years after
cessation of smoking (Morris et al., 2007). There is a linear relationship in the number of
cigarettes smoked and the progression of AMD (Coleman et al., 2008). Depletion of
antioxidants and the resultant oxidative stress might be the result of smoking, but the exact
mode of action of involvement of smoking in causing AMD is not known (Dhubhghaill et
al., 2010; Cano et al., 2010).
1.4.4.3 Diet
A diet rich in fats and cholesterol has been associated with increased risk of developing
AMD. A mineral- and antioxidant-rich diet decreases the risk of disease progression by
25% (2001). Carotenoids are also found to have a protective role in AMD (Seddon et al.,
1994).
1.4.4.4 Exposure to Sunlight
Exposure to sunlight has been shown to be associated with increased risk of development
of AMD but not its progression. Use of sunglasses or a hat have been seen to be protective
against the development of AMD (Tomany et al., 2004a). The possible mechanism of

22
sunlight-induced damage is the creation of oxidative stress in the macular region (Taylor
et al., 1992).
1.4.5 Treatment of AMD
There is no standard treatment of AMD that can revert the loss of vision. Therefore,
prevention is the best mode of defense against the disease. Taking care of modifiable risk
factors, such as smoking and diet, can help reduce the chances of developing the disease
(Tomany et al., 2004b).
Currently, there is no medication available for the cure of dry AMD or its prevention from
advancing to the late stage. Usually, dietary supplements are used to reduce the chances of
the disease entering into advanced stages. The Age Related Eye Disease Study (AREDS)
found that a combination of antioxidant minerals and vitamins act as preventive agents, but
this study could not establish a regimen for the cure of the disease, since the combination
supplement could not prevent the disease from entering the advanced stages (Age-Related
Eye Disease Study Research Group., 2001). In the next study trial, lutein and zeaxanthin
were added to the supplementation, which further decreased the chances of development
of advanced stages of the disease. It was found to be 20% more beneficial as compared to
the previous supplement (Age-Related Eye Disease Study 2 Research Group., 2013). Beta-
carotene has been reported to be associated with lung cancer in smokers, and hence was
removed from the final formulation of the supplement. The current supplement that is given
to patients with dry AMD comprises of vitamin C (500 mg), vitamin E (400 IU), zinc (as
zinc oxide 80 mg), copper (as cupric oxide 2mg), lutein (10mg)/zeaxanthin (2 mg), omega-
3 long-chain polyunsaturated fatty acids, docosahexaenoic acid (DHA-350 mg) and its
precursor, eicosapentaenoic acid (EPA-650 mg) (Ratnapriya and Chew 2013).
The most effective therapy for wet AMD is anti-VEGF therapy, which involves intravitreal
injections of humanized monoclonal antibodies, Avastin (bevacizumab) and Lucentis
(ranibizumab). The mode of action of this drug is neutralization of all active forms of
VEGF and thus its angiogenic capacity. A new therapic compound, Aflibercept, is also
given to the patients via intravitreal injections, and it acts as a soluble receptor that traps
the VEGF family of proteins (Ratnapriya and Chew 2013).

23
1.5 Molecular Pathology of Glaucoma and AMD
Many aspects of glaucoma and AMD are not fully understood, and the treatment options
are thus very limited. Therefore, there is a need to study the molecular mechanism of the
disease to gain a better understanding of the disease processes, and thus create the
possibility of developing better treatments. Interactions of various molecular mechanisms
involved in glaucoma and AMD are depicted in the flowchart in Figures 1.4 & 1.5.
1.5.1 Role of Oxidative Stress in Glaucoma and AMD
Oxidative stress can be described as the physiological production of ROS, and failure of
scavenging enzymes to eliminate them thus creates an environment of stress. With
advancement in age, the concentration of free radicals increases and results in oxidative
stress and damage to various tissues of the body, especially post-mitotic tissues such as
brain, heart, liver, and the retina. (Shigenaga et al., 1994). ROS include radical OH-,
peroxyl radical ROO-, super anion of oxygen O2-, hydrogen per oxide H2O2, hydroxyl and
singlet oxygen 1O2 (Ferreira et al., 2004). Free radicals are involved in lipid per-oxidation
of cell membrane components thus disrupting it, increasing the vulnerability of DNA,
proteins and mitochondrial DNA. This mechanism is believed to play a general role in most
degenerative diseases (Sacca et al., 2007). Under the influence of age, smoking, pollution,
and inflammation, free radicals keep on leaking from the active sites of the enzymes
(Borish et al., 1987). Oxidative stress has been reported in different ocular complications
including glaucoma (Ferreira et al., 2004) and macular degeneration (Yildirim et al., 2004).
Its role in glaucoma was postulated thirty years ago (Alvarado et al., 1981; Alvarado et al.,
1984). Subsequently, in vivo and in vitro experiments were conducted to determine the role
of oxidative stress in glaucoma (Izzotti et al., 2006). In the in vitro studies, TM cells were
treated with H2O2, which demonstrated that these cells lose their integrity and cell-to-cell
adhesion capacity decreases in the presence of H2O2 (Zhou et al., 1999). In vivo studies on
calf showed that perfusion with H2O2 resulted in a change in the drainage of aqueous humor
from the interior chamber to the posterior chamber (Kahn et al., 1983). Moreover,
treatment with anti-oxidants has been shown to provide protection to retinal ganglion cells
in rats (Ko et al., 2000). Superoxide dismutase, glutathione oxidase and catalase act as
antioxidant enzymes in eye tissues, in particular in the TM and aqueous humor, and provide

24
Figure: 1.4 Pathological mechanisms involved in glaucoma [modified (Vohra et al., 2013), (Sacca et al., 2007)]. IOP; Intra Ocular
Pressure, NO; Nitric Oxide, ET1; Endothelin1, TBM; Trabecular Meshwork, RGC; Retinal Ganglion Cells.

25
Figure: 1.5 Pathological mechanisms involved in AMD [modified (Anderson et al., 2010; Nowak 2006; Kopitz et al., 2004)].
RPE; Retinal Pigment Epithelium, NO; Nitric Oxide, CFH; Complement factor H, C3; complement 3, C2; Complement 2.

26
a defense mechanism against free radicals by scavenging them (Behndig et al., 1998).
Carotenoids such as lutein and zeaxanthin are present in the macular region (macular
pigments), where they provide the first line of defense to neurons, particularly from singlet
oxygen (Frank 1996). It has been found that the level of glutathione is lower in glaucomatic
eyes, suggesting that its protective role is compromised. Moreover, polymorphisms in
Glutathione S Transferase Mu 1 (GSTM1; that catalyse reaction of glutathione with variety
of organic compounds and is involved in detoxification process) have been associated with
glaucoma (Izzotti et al., 2003). Although the enzyme is not directly involved in IOP
management, it may protect aqueous-bathed surfaces from the possible damaging effects
of H2O2 (Kahn et al., 1983). Most damaging changes due to H2O2 occur in the inner layers
of the TM due to oxidative stress, which together with other factors can induce TM cell
loss, the thickening of the fibrils in TM, which result in compromising the integrity of the
TM (Sacca et al., 2007). The structural units of TM, glycosaminoglycans (GAGs) and
hyaluronic acid, play an important role in the outflow of aqueous humor, and their integrity
is disturbed in the presence of reduced quantities of ascorbate (Sacca et al., 2007).
Moreover, due to elevated free radicals, nitric oxide (NO) has the capacity to generate toxic
substances that can damage the TM and alter its properties (Lipton 1999). Endothelin levels
have been seen to be elevated in glaucomatous eyes, which reduce the blood flow in the
ONH and/or hinder the axonal transport and cause glaucomatic damage (Yorio et al.,
2002).
The retina has the highest consumption of oxygen compared to all other tissues, and
therefore accumulatess a high concentration of free radicals. The RPE contains many
photosensitizers, such as in the outer segments of the photoreceptor cells that contain
polyunsaturated fatty acids (PUFAs), which are continuously being shed and phagocytosed
by the RPE cells (Beatty et al., 2000). The burden of phagocytosis by the RPE increases as
a consequence of the above mentioned changes, which results in peroxidation of lipids that
damages the RPE itself thus triggering apoptosis of the RPE. As a consequence, the
apoptotic RPE cells and the undigested phagocytosed material pile up in BM and trigger
drusen formation (Ishibashi et al., 1986; Cai et al., 2000). Lipofuscin present in the RPE
cells acts as a photosensitizer, generating ROS and damaging the RPE. Moreover, the A2E
compound of lipofuscin hinders the function of the RPE, reducing its capacity of

27
phagocytosis (Gaillard et al., 1995; Holz et al., 1999). Lipofuscin can also induce
generation of ROS under the influence of light (Beatty et al., 2000).
1.5.2 Role of Immune System in Glaucoma and AMD
An inflammatory response is elicited in the eye in response to ischemia, vascular
dysregulation, oxidative stress, hypoxia, and raised IOP (Ergorul et al., 2010). The immune
system maintains the tissue architecture by helping the cells to overcome these stresses and
thus maintain the tissue architecture, which otherwise would result into neurodegenerative
changes (Schwartz and Ziv 2008). With advancing age and chronic increase in stress
factors, the potential of the immune system to overcome the stress decreases. Initially
providing a protective mechanism, the immune system overactivates the immune
regulatory protection of the tissues and thus results in an autoimmune-triggered
neurodegenerative process (Tezel 2009).
The complement cascade, auto-antibodies and T-cell cytotoxicity have been found to be
involved in the degeneration of RGC and axons in glaucoma (Wax et al., 2008). Heat shock
proteins (HSPs) have an antigenic character, and their upregulation is taken as a signal for
the removal of harmful and stressed cells thereby activating the immune response (Tezel
et al., 2000). The vascular dysregulation, as a result of raised IOP and other stressors is
also seen to play a role in activation of the immune response and ischemic injury to the
ONH (Vohra et al., 2013). In response to these changes (raised IOP, ischemia, stressors),
nitric oxide (NO) and endothelin 1 (ET-1) levels rise in the vasculature, resulting in
lowering of the IOP. However ET-1 also lowers the blood flow to the ONH, with potential
damaging consequences (Sugiyama et al., 1995). Ubiquitin-dependent proteosomal
degradation system is also disrupted by the ET-1, which decreases the ubiquitination in the
ONH and activates caspase-3, resulting in apoptosis (Dibas et al., 2008). As a result of
this disruption in the ocular blood flow, other inflammatory compounds are also
upregulated, which include tumor necrosis factor (TNF), C reactive protein (CRP),
vascular endothelial growth factor (VEGF), and interleukins (ILs) (Vohra et al., 2013). The
overexpression of VEGF activates the major histocompatability complex (MHC-I and
MHC-II), thus eliciting an immune response (Chintala et al., 2002). VEGF interaction with

28
ET-1 and involvement in VEGF has been previously reported in POAG and NTG (Iwabe
et al., 2010).
The most significant pathogenic mechanism of the immune system involved in AMD is
the complement pathway (Parmeggiani et al., 2012). Macrophages and lymphocytes have
also been reported to be present in the Ruysch's complex (Penfold et al., 1985; Dunaief et
al., 2002), moreover the oxidative stress produced in the photoreceptors also influences the
activation of the complement system, resulting in apoptosis of retinal cells in the Ruysch's
complex and accumulation of drusen (Hollyfield et al., 2010). It has been reported that the
retina and RPE can manufacture as well as transport lipoproteins, besides extracting them
from the blood (Zheng et al., 2012). Apolipoprotein B (Apo-B) mediated transport of
cholesterol has been observed to be the most important mechanism involved in the
pathogenesis of AMD (Curcio et al., 2010). The particles (Apo-B) pile up in the BM,
resulting in activation of drusenogenesis with advancing age (Curcio et al., 2009). Various
genes in these pathways have been identified as pathogenic factors for AMD in genome-
wide association studies (GWAS), which include high density lipoprotein (HDL) related
genes such as ATP binding cassette transporter 1 (ABCA1), hepatic lipase (LIPC),
cholesteryl ester transfer protein (CETP), and lipoprotein lipase (LPL) (Neale et al., 2010).
The accumulation of drusen in the BM and RPE is capable of triggering inflammation by
triggering the complement system and cytotoxicity (Pauleikhoff et al., 1990).
1.6 Genetic Etiology of Glaucoma and AMD
Various DNA sequence variations with pathogenic consequences have been reported to be
associated with the development of genetic disorders (Lai 2001). Advancement in
statistical and bioinformatics tools as well as evolution of techniques such as GWAS,
microarrays and advancement in sequencing techniques has enabled researchers in better
understanding complex diseases such as glaucoma and AMD (Feero et al., 2008). These
advancements have made the genetic analysis of these diseases somewhat easier (Fuse
2010). As glaucoma and AMD are both mutlifactorial complex disorders, multiple genes
can be involved in the pathogenicity of these diseases (Donoso et al., 2006). The current
etiology of these disease mechanisms is not clearly understood due to the complex nature
and involvement of a combination of factors in their manifestation. The interactions of

29
these multiple factors result in deviation from the Mendelian mode of inheritance of
multifactorial diseases such as glaucoma and AMD (Fan et al., 2004; Libby et al., 2005).
In addition, in the case of multifactorial diseases, more than one gene might interact with
each other in disease manifestation (Faucher et al., 2002; Baird et al., 2003). Monogenic
forms of glaucoma and AMD also exist such as PCG (Lopez-Garrido et al., 2013) and
juvenile macular degeneration (Stargardt disease) (Tuo et al., 2004).
1.6.1 Molecular Genetics of Glaucoma
To date 20 loci (Table 1.1) (GLC1A to GLC1N, GLC3A to GLC3D) have been reported
to be associated with familial glaucoma and three genes, myocillin (MYOC), optineurin
(OPTN), and WD repeat domain 36 (WDR36), have been reported to be the causative
factor in these loci (Fuse 2010). Cytochrome P450 (CYP1B1) has been found to be
associated with PCG. These loci have been found by candidate gene analysis in which a
plausible gene is screened in the family on the basis of its function (Fuse 2010). In total
more than 20 genes (Table 1.2) have been reported to be associated with POAG (Fuse
2010) and 9 genes associated with PACG were identified by GWAS (Vithana et al., 2012)
and case-control association studies in different cohorts (Shastry 2013).
Worldwide more than 70 point mutations in MYOC have been found to be associated with
POAG (predominantly with JOAG), with a 3-5% overall association with POAG (Challa
2011). MYOC encodes a 570 kDa protein, spans a 17 kb genome region and has 3 exons.
The MYOC protein has a C-terminal alfactomedin-like domain and an N-terminal myosin-
like domain (Suzuki et al., 1997). In the eye it has been reported to be present in the TM,
aqueous humor (Suzuki et al., 1997) and in the sheath of the optic nerve fibers (Tamm et
al., 1999). Different mutations in MYOC have been reported to interfere with aqueous
humor outflow and thus increase the IOP. However, the mechanism of the rise in IOP has
not been clearly defined yet (Mackey et al., 2003; Wilkinson et al., 2003).
In vivo studies of MYOC have shown that it does not seem to play a role in the pathogenesis
of glaucoma, which could be a coincidental finding, or the gene might be acting in tandem
with another gene. For examples, the. Gly399Val mutation in the the MYOC gene has been
reported to cause late-onset POAG (mean age of 51 years), however, when it occurs in

30
Table: 1.1 Loci associated with glaucoma
Locus name Gene Name Chromosomal
location
Characteristic
Features
Mode of inheritance Population
studied
References
GLC1A Myocilin 1q23 JOAG; high IOP Autosomal dominant Sheffield et al., 1993
GLC1B - 2cen-q13 Late onset, moderate IOP Stoilova et al., 1996
GLC1C - 3q21-24 Late onset Autosomal dominant Wirtz et al., 1997
GLC1D - 8q23 Adult onset Medium IOP Autosomal dominant Trifan et al., 1998
GLC1E Optineurin 10p13 Adult onset NTG Variable pattern British Sarfarazi et al., 1998
GLC1F ASB10 7q36 Late onset, low and high
IOP
Autosomal dominant U.S Wirtz et al., 1999
GLC1G WDR36 5q22.1 POAG, NTG Monemi et al., 2005
GLC1H - 2p16-p15 Late onset, moderate to
high IOP
Variable segregation
pattern
British Suriyapperuma et al.,
2007
GLC1I - 15q11-q13 Adult onset Complex segregation Caucasian Allingham et al., 2005
GLC1J - 9q22 JOAG Autosomal dominant Wiggs et al., 2004
GLC1K - 20p12 JOAG Wiggs et al., 2004
GLC1L - 3p22-p21? Late onset, autosomal dominant British Baird et al., 2005
GLC1M - 5q22.1-q32 JOAG Autosomal dominant Filipino Pang et al., 2006
GLC1N - 15q22-q24 JOAG Autosomal Dominant Chinese Wang et al., 2006a
GLC1O NTF4 19q13.3 POAG, NTG European Pasutto et al., 2009
GLC1P TBK1* 12q14 NTG, early onset Autosomal dominant African-
American
Fingert et al., 2011
GLC3A CYP1B1 2p21 PCG, very high IOP Autosomal recessive Sarfarazi et al., 1995
GLC3B 1p36.2-p36.1 PCG, very high IOP Autosomal recessive Akarsu et al., 1996
GLC3C 14q24.3-31.1 PCG, very high IOP Autosomal recessive Stoilov and Sarfarazi.,
2002
GLC3D LTBP2 14q24 PCG, very high IOP Autosomal recessive Pakistani Firasat et al., 2008
*300kb duplication in TBK1 gene

31
combination with the Arg368His mutation in CYP1B1, the age of onset of the disease
decreases to a mean age of 27 years (Challa 2011). In vivo analysis of MYOC mutations in
double mutant mice revealed that the gene is not associated with IOP maintenance, since
no TM abnormalities were seen in transgenic mice after the introduction of these mutations
(Liu and Neufeld 2003).
The optineurin gene has been reported to be associated with a late age of disease onset, but
it has been found to account for only about 1% of glaucoma mutations. Polymorphisms in
the gene are associated with NTG, and the Glu50Lys variant has been reported in POAG
cases (Leung et al., 2003). The Met98Lys variant is also associated with NTG (Craig et
al., 2006). The gene encodes a 577-kDa protein expressed in the TM, ciliary muscle, and
retina, and has been shown to have a protective role in the eye, being expressed in response
to stress (Vittotow and Borras 2002).
Mutations in WDR36 account for pathogenicity in less than 1% of glaucoma cases.
Although initially associated with glaucoma, later studies have shown no involvement of
the gene in glaucoma (Gemenetzi et al., 2012).
PCG is a developmental disorder of infants, usually occurring in sporadic cases, but
familial cases of the disease have also been reported. The disease is inherited as an
autosomal recessive trait (Sarfarazi et al., 2003; Bejjani et al., 2000). Although to date four
loci have been linked to the condition, GLC3A, GLC3B, GLC3C and GLC3D, only two
genes have been found in these loci to be causative of the disease i.e. GLC3A (CYP1B1)
and GLC3D (Latent transforming growth factor beta binding protein; LTBP2)
(Mozaffarieh et al., 2008; Coleman 1999). Around 60 different mutations in CYP1B1 have
been reported to be associated with PCG (Ressiniotis et al., 2005). To date, a single
mutation in LTBP2 has been identified to cause PCG in a Pakistani family (Ali et al., 1999),
which was also found homozygously later as a founder mutation in 12 Gypsy PCG
probands (Azmanov et al., 2011). Besides the mutations, there is just one report of a single
basepair deletion in the gene resulting in PCG (Narooie-Nejad et al., 2009).

32
Table: 1.2 Genes and polymorphisms associated with POAG and PACG
Gene Disease type Population Original study
AGTR2 POAG Japanese Hashizume et al., 2005
ANP POAG Australian Tunny et al., 1996
APOE POAG -- Copin et al., 2002
CDH-1 POAG Chinese Lin et al., 2006
EDNRA POAG Japanese Ishikawa et al., 2005
GPDS1 POAG Japanese Nakamura et al., 2009
GST POAG Estonian Juronen et al., 2000
HSPA1A POAG Japanese Tosaka et al., 2007
IGF2 POAG Chinese Tsai et al., 2003
Ilβ POAG Chinese Lin et al., 2003b
MFN1 POAG German Wolf et al., 2009
MFN2 POAG Dutch Wolfs et al., 1998
MTHFR POAG -- Junemann et al., 2005
NCK2 POAG Japanese Akiyama et al., 2008
NOS3 POAG Australian Tunny et al., 1998
NTF4 POAG German Pasutto et al., 2009
OCLM POAG -- Fujiwara et al., 2003
OLFM2 POAG Japanese Funayama et al., 2006
OPA1 POAG European Aung et al., 2002
PARL POAG German Wolf et al., 2009
PON1 POAG Japanese Inagaki et al., 2006
TAP1 POAG -- Lin et al., 2004
TLR4 POAG Japanese Shibuya et al., 2008
TNF POAG Chinese Lin et al., 2003a
TP53 POAG Chinese Lin et al., 2002
PLEKHA7 PACG Asian Vithana et al., 2012
COL11A1 PACG Asian Vithana et al., 2012
PCMTD1 PACG Asian Vithana et al., 2012
MMP9 PACG Chinese
Taiwanese
Caucasian
Qui 1990
Wang et al., 2006b
Awadalla et al., 2011a
MFRP PACG Chinese Aung et al., 2008
MTHFR PACG Pakistani Michael et al., 2008
NOS3 PACG Pakistani Ayub et al., 2010
HSP70 PACG Pakistani Ayub et al., 2010
HGF PACG Nepalese Awadalla et al., 2011b

33
1.6.2 Molecular Genetics of AMD
The role of genetics in the pathogenesis of AMD has lately been reported in a number of
genetic studies, which have been conducted to explore the underlying cause of the disease
and its mechanisms (Edwards et al., 2005). Twin studies, combined linkage analysis and
GWAS have contributed considerably in the understanding of the genetics of AMD
(Spencer et al., 2011). Studies on smaller families has resulted in the identification of
susceptible loci at 1q25-31, 9p13, 9p24, 10q26, 15q21 and 17q25 (Mancebo 1992; Klein
et al., 1998; Weeks et al., 2004; Abecasis et al., 2004) and GWAS identified loci in the
vicinity of genes such as COL8A1/FILIP1L, IER3/DDR1, SLC16A8, TGFBR1, RAD51B,
ADAMTS9, and B3GALTL (Fritsche et al., 2013). GWAS and candidate gene studies have
highlighted the role of genes including complement factor H (CFH) (Zareparsi et al.,
2005), complement component 3 (C3) (Maller et al., 2007), complement component 2,
complement factor B (C2-CFB) (Gold et al., 2006), complement factor I (CFI) (Fagerness
et al., 2009), HTRA1/LOC387715/ARMS2 (Rivera et al., 2005; Kanda et al., 2007), CETP,
TIMP3 (Chen et al., 2010a), hepatic lipase gene (LIPC) (Neale et al., 2010), VEGF-A,
COL10A1 (Yu et al., 2011), TNFRSF10A (Arakawa et al., 2011) and APOE (Mckay et al.,
2011).
Rare variant studies and GWAS have shown upregulation of the alternative pathway of the
complement system in AMD (Fritsche et al., 2013). Variants at two loci have been
recurrently shown to be associated with AMD in several studies in the world. These two
loci contain the genes complement factor H (CFH) and age-related maculopathy
susceptibility 2/High temperature requirement A1 (ARMS2/HTRA1) (Sobrin et al., 2011).
The C3 convertase enzyme and other components of the immune system are activated as a
result of complement system activation, which can occur through any of the three pathways
i.e. classical, lectin or alternative pathway, all of which act as a component of the
membrane attack complex and cell lyses. CFH has been shown to be involved in controlling
the alternative pathway of complement activation by inhibiting the activation of C3 to C3a
and C3b (Klein et al., 2005). CFH is composed of 20 repeating units of 60 amino acids
called short consensus repeats (SCRs) (Edwards et al., 2005). In SCR7 a change in the
amino acid tyrosine to histidine at position 402 has mostly been found to be associated with

34
AMD (Klein et al., 2005). This polymorphism lies in the region of the protein critical for
binding of CFH to heparin and C-reactive protein (CRP) ( Cordoba et al., 2004).
Involvement of CFH in the incidence as well as progression to the end stages of AMD has
been well established (Cao et al., 2013).
Polymorphisms in ARMS2/HTRA-1 have also been reported to be associated with increased
risk of AMD (Sundaresan et al., 2012). ARMS2 lies in the mitochondrial membrane and
is hypothesized to cause AMD by interfering with energy metabolism of the photoreceptors
as well as by activating apoptosis and reactive oxygen species (Kanda et al., 2007). The
HTRA1 protein is located in the vascular endothelium and the polymorphisms in the gene
are postulated to cause AMD by degrading the ECM by increasing the expression of the
matrix metalloproteinases (Ding et al., 2009). The variant rs10490924 in HTRA1 is
reported to be significantly associated with AMD (Sobrin et al., 2011).
1.7 Study Overview
The current study was based on investigating the underlying genetic causes of
multifactorial eye diseases, glaucoma and AMD. Both diseases are complex inherited
disorders and determination of their genetic basis is very difficult. Therefore, in order to
better understand the genetic etiology in Pakistani glaucoma and AMD patients, we
conducted genetic linkage analysis and case-control association studies. AMD familial
cases are rare, therefore mostly sporadic cases were included for genetic investigation. The
genetic analyses were conducted using high-throughput techniques, such as microarray
analysis that led to the identification of a possible novel locus for PCG, and next generation
sequencing analysis that revealed possible genetic causes in two glaucoma families with
juvenile onset of the disease.
In addition, polymorphisms in different genes were screened in sporadic cases of glaucoma
and AMD, which had been previously reported to be significantly associated with the
respective diseases in various populations. Restriction fragment length polymorphism
(RFLP), Taqman® allelic discrimination assay, KASPar assays and Sanger sequencing
were employed to explore the genetic causes of glaucoma and AMD, which led to the
identification of a number of genes involved in the pathogenesis of glaucoma and AMD in

35
the Pakistani population. However, there were also contradictory results for some of the
previously reported associated variants.

Chapter 2
Materials and Methods

37
2 Materials and Methods
2.1 Ethics Statement
The current study was approved by COMSATS Institute of Information Technology,
Islamabad, Department of Biosciences, Ethics Review Board and conforms to all of the
norms of the Helsinki Declaration. Informed written consent was obtained from all the
participants recruited for the analysis prior to sampling.
2.2 Participants of the Study
In the current study, families with glaucoma and AMD, as well as sporadic cases of
glaucoma and AMD were included.
2.2.1 Families with Glaucoma and AMD
Twenty families diagnosed with glaucoma and two families diagnosed with AMD,
collected mainly from the Punjab province and the Khyber Pakhtunkhwa (KPK) province
of Pakistan and were included in the current study. The probands were identified by
clinicians of different hospitals and were approached for a brief interview about their
family history, age of onset, and severity of their disease. After drawing the pedigree,
venous blood was drawn from all family members, and information on their medication,
diet, occupation, smoking status, and any other disease was documented.
After a detailed clinical examination the families were classified into different subtypes of
glaucoma, including POAG, PACG and PCG (Table 2.1). Complete interview and
ophthalmic examination of the POAG families allowed further classification into JOAG
and late-onset glaucoma. The potential mode of inheritance was also noted (Table 2.1).
2.2.2 Sporadic Cases and Controls
Approximately 500 POAG patients, 200 PACG patients, 300 PEXG patients and 300 AMD
cases were recruited from different ophthalmological centers in Pakistan, including the Al-
Shifa Eye Trust Hospital in Rawalpindi, the Myo Hospital in Lahore and the Ayub
Teaching Hospital in Abbottabad. In addition, 300 age- and gender-matched controls with
no signs of glaucoma or AMD were also sampled from the same centers, as well as from

38
Table 2.1 Overview of collected glaucoma and AMD families
Family Potential mode
of inheritance
Age of
onset
Number of sampled individuals
(Affected/Unaffected)
Disease
GLC 1 Dominant Juvenile 10/9 JOAG
GLC 2 Recessive Congenital 2/5 PCG
GLC 3 Recessive Juvenile 4/5 JOAG
GLC 4 Recessive Juvenile 8/11 JOAG
GLC 5 Dominant Juvenile 7/2 JOAG
GLC 6 Dominant Late 9/6 POAG
GLC 7 Dominant Late 8/6 POAG
GLC 8 Recessive Juvenile 6/8 JOAG
GLC 9 Dominant Late 11/4 POAG
GLC 10 Recessive Late 2/3 PACG
GLC 11 Dominant Late 3/5 POAG
GLC 12 Dominant Late 10/4 POAG
GLC 13 Dominant Juvenile 8/9 PACG
GLC 14 Dominant Juvenile 4/4 PACG
GLC 15 Dominant Juvenile 5/6 JOAG
GLC 16 Dominant Congenital 8/16 PCG
GLC 17 Recessive Congenital 8/12 PCG
GLC 18 Dominant Late 3/1 POAG
GLC 19 Dominant Late 10/6 POAG
GLC 20 Dominant Late 5/7 POAG
AMD 1 Recessive NA 3/2 AMD
AMD 2 Recessive NA 2/6 AMD
NA; Not applicable

39
the general population.
2.3 Clinical Diagnostic Criteria
2.3.1 Diagnosis of Sporadic Cases
The sporadic cases of POAG, PACG and PEXG were selected on the basis of their clinical
history, cup–to-disc ratio (CDR), evaluation of the optic disc, visual field determination
and elevated IOP. They were categorized into open angle (POAG) and closed angle
(PACG) groups based on gonioscopic findings. In order to determine the presence of
exfoliative deposits on the pupillary border and the iris of the patients with PEXG, slit lamp
biomicroscopy was initially performed without dilation of the pupil. Subsequently, after
pupil dilation, patients were re-examined to detect the presence of white deposits on the
anterior lens surface. Angles were measured with a gonioscope to differentiate between
narrow and open angles among PEXG patients. Age-matched controls were recruited in
the study after complete clinical examination of the fundus. In addition, to rule out any
ocular anomalies, the controls also underwent applanation tonometery, slit lamp
examination to exclude exfoliative deposits, CDR measurement and visual field
assessment. All controls had normal visual fields, IOPs (≤ 20 mmHg) and CDRs (≤0.2).
AMD patients were recruited on the basis of a diagnosis of severe macular degeneration.
They were aged ≥ 50 years and recruited on the basis of presence of at least 15 intermediate
(64-125μm) or at least one large drusen (>125μm). Fundus photography was done as a
confirmatory test for the presence of drusen and progression of the geographic atrophy (dry
AMD), whereas fundus fluorescein angiography (FFA) and optical coherence tomography
(OCT) were performed to distinguish between patients with dry AMD and choroidal
neovascularisation (wet AMD). Control subjects were aged ≥60 years of age and did not
have AMD. Fundus examination of the eye was done for all controls before sampling to
rule out the presence of drusen.
2.3.2 Diagnosis of Families
All glaucoma family members underwent complete ophthalmic examination. Tests
included fundoscopy to observe the optic discs, tonometery to measure the IOP and

40
gonioscopy to distinguish the angle (closed or open). Moreover, FFA was done for all the
individuals of the family for examination of the retinal nerve fiber layer (RNFL) and to
determine the thickness of the nerve fiber layer. The diagnosis of PCG was made on the
basis of an age of onset of less than 3 years; megalocornea or buphthalmos (horizontal
corneal diameter >13 mm); corneal haze; breaks in Descemet membrane; raised intraocular
pressure (>21 mmHg); CDR >0.6; and the presence of additional symptoms such as
blepharospasm and photophobia.
JOAG was diagnosed on the basis of juvenile appearance of glaucoma symptoms in the
second decade of life in affected family members. On the other hand, individuals of
families with a disease onset in the fourth decade of life were diagnosed as late onset
glaucoma.
The AMD families went through similar ophthalmic examination as the sporadic cases
described in 2.3.1.
2.4 Collection of Blood Samples and Genomic DNA Extraction
Venous blood was drawn from affected and unaffected family members, sporadic cases
and controls, and stored at 4oC in acid citrate dextrose (ACD)-containing vacutainers till
further processing.
2.4.1 DNA Extraction and Dilution
The blood samples were first treated with erythrocyte lysis buffer (ELB) to lyse the red
blood cells and further treatment overnight with reagents (Pronase E, Sodium Dodecyl
Sulphate, Tris Sodium/Nitrium Chloride EDTA) to digest the proteins, remove cellular
debris and expose the nucleus. The DNA was then precipitated by the salting-out method
using 6M NaCl and 99% ethanol. The DNA was then washed in 70% ethanol. The isolated
and dried DNA was resuspended in 1X TE buffer (pH 8.0) and stored at -20˚C. The
extracted DNA was separated on 1% agarose gels containing ethidium bromide along with
a λ-HinD-III DNA ladder for quantification. After electrophoresis, DNA was visualized
using the Gel Documentation System and Bio Cap MW software V11.01 (Vilber Lourmat,
Marne-La-Vallee, Cedex1, France).

41
2.5 Screening Glaucoma and AMD Families
Twenty families with glaucoma were pre-screened for mutations in known glaucoma
genes. Two families with AMD were analysed for mutations in known AMD genes.
2.5.1 Exclusion of Known Genes
The probands of the 20 glaucoma families were first screened for mutations in MYOC,
OPTN and WDR36 followed by pathogenicity assessment of the variants and segregation
analysis in the family. Similarly, two families with AMD were screened for mutations in
CFH.
2.5.1.1 Primer Design and Polymerase Chain Reaction
Screening of the genes was done by designing primers for all coding exons and exon-intron
boundaries (enlisted in Annex 1 and 2) using the Exon Primer tool of the UCSC Genome
browser (http://genome.ucsc.edu/). Specificity of the primers as well as the primer
conditions were confirmed by using the online tool Primer 3 version 0.4.0
(http://frodo.wi.mit.edu/primer3/). The coding regions of all genes were amplified in a 25µl
reaction volume using a thermal cycler (GeneAMP, PCR System 9700, Applied
Biosystems) using 1X PCR buffer (100 mM Tris-HCl, (pH 8.3), 500 mM KCl), 0.25mM
dNTPs, 2.5mM Mg+2, 0.5μM of each primer, 2.5U Taq polymerase (Fermentas Life
Sciences, Ontario, Canada) and 50ng gDNA. The thermal cycling consisted of initial
denaturation at 95˚C for 5 min followed by 30 cycles of amplification at 95˚C for 1 min,
58˚C for 30 sec and 72˚C for 45 sec. A final extension was carried out at 72˚C for 5 min.
After amplification the samples were separated on 2% agarose gels, visualized under UV
transillumination and documented using the Gel Documentation System (Vilber Lourmat,
Marne-La-Vallee, Cedex1, France).
2.5.1.2 Sanger Sequencing and in Silico Analysis of Variants
The amplified PCR products of candidate genes were purified using the GeneJET TM PCR
purification kit (Fermentas, Life Sciences, Ontario, Canada) and sequenced bidirectionally
with forward and reverse primers using dye-termination chemistry (BigDye Terminator,
version 3 on a 3730 or 2100 DNA analyzer; Applied Biosystems) at the sequencing facility

42
of the Department of Human Genetics, Radboud University Medical Centre, Nijmegen,
The Netherlands. Sequence data were analyzed using Vector NTI Advance 11 software
(Invitrogen, Life Technologies, Carlsbad, CA). Identified variants were analyzed for their
pathogenicity by in silico analysis using online Alamut Biointeractive software
(http://www.interactive-biosoftware.com). Conservation scores of the variants
(http://genetics.bwh.harvard.edu/pph2), defined by the phyloP score and the Grantham
score (http://www.interactive-biosoftware.com), were calculated for each identified
variant. Moreover, the damaging effect of the variants was determined online by SIFT
(sorting intolerant from tolerant) (http://sift.jcvi.org) and Polyphen (polymorphism
phenotyping v2) (http://genetics.bwh.harvard.edu/pph2/). The Exome Variant Server
(EVS) (http://evs.gs.washington.edu/EVS/) was used to investigate the population
frequency of identified variants.
2.5.1.3 Segregation Analysis of Variants in OPTN, MYOC, WDR36
Variants in OPTN, MYOC and WDR36 with high pathogenicity scores were analysed in
the respective families for segregation using Sanger sequencing.
2.5.1.4 Mutation and Segregation Analysis of Variants in CYP1B1
Three PCG families were screened for mutations in CYP1B1. Primer designing for the two
coding exons of CYP1B1 was done as explained in section 2.5.1.1. DNA samples of the
probands of the three families were first screened for mutations. Segregation analysis was
performed in all members of PCG family GLC16 by Sanger sequencing.
2.5.2 Homozygosity Mapping Using Microarray Analysis
Three families (GLC 2, GLC 4 and GLC 8) with juvenile-onset disease were selected for
genotyping using 250K SNP arrays (Affymetrix, Santa Clara, CA) to determine
homozygous regions shared among the affected individuals of the family.
2.5.2.1 Brief 250K Microarray Protocol
Briefly, the array analysis consisted of digestion of 250 ng of genomic DNA with
restriction enzyme NspI. The digested fragments were incubated for 3 hours at 16oC to

43
ligate adaptors, followed by incubation at 70oC for 20 minutes. The ligated DNA fragments
were then amplified using PCR master mix containing Titanium Taq PCR Buffer, 2.5 mM
dNTPs, GC-Melt 5M (1µl), 100µM PCR primers and Titanium Taq DNA polymerase. The
initial denaturation of the thermal cycle was at 94ºC for 3 minutes (1 cycle) followed by
30 cycles of denaturation at 94 ºC for 30 sec and annealing at 60ºC for 45 sec followed
by extension at 68 ºC for 15 sec. Final extension was done at 78 ºC for 7 min. The amplified
product was then treated with DNase I and the 3' ends were labeled at 37 ºC for 4 hours.
The fragmented samples were then hybridized with the probes on the Affymetrix 250K
array platform, after which the array was scanned using a GeneChip scanner 3000 7G
(Affymetrix).
2.5.3 In Silico Analysis of 250K Microarray Data
The 250K SNP microarray data were initially analyzed using Homozygosity Mapper, an
online tool (http://www.homozygositymapper.org/), which provides common homozygous
regions shared between the affected individuals. Homozygous regions larger than 1 Mb
were further analyzed by CA-repeat marker analysis, and exons of candidate genes in the
selected regions were sequenced to determine the presence of mutations. All data were
analysed using the Human Genome Build (hg19) release Feb. 2009.
2.5.4 CA-repeat Marker Analysis
Homozygosity mapping with 250K SNP arrays identified three homozygous regions in
family GLC 2 on chromosomes 3, 7 and 15, three homozygous regions in family GLC 4
on chromosomes 1, 2 and 10, and four homozygous regions in family GLC 8 on
chromosomes 3, 4, 6, and 11. CA-repeat marker analysis was performed for family GLC 2
to determine which of the regions segregated with the disease in the family. CA markers
were chosen on chromosomes 3, 7 and 15, with heterozygosity greater than 70%. Primer
sequences to amplify the polymorphic markers, as well as their cytogenetic locations, were
obtained from the UCSC genome browser (STS marker; https://genome.ucsc.edu), the
Marshfield Medical Center database (www.marshmed.org.gov/genetics/) and the Human
Genome Database (www.gdb.org). M13-tailed primers were designed by addition to the
forward and reverse CA markers the forward M13 sequence 5'-

44
TGTAAAACGACGGCCAGT-3' and a reverse M13 sequence (M13 tail) 5'-
CAGGAAACAGCTATGACC- 3' respectively. A list of the CA markers used is provided
in Tables 2.2 to 2.4.
A two-step PCR was used, in which the first PCR was a standard PCR amplifying the CA
markers under standard PCR conditions (Annex 3). In a second PCR, 1 ul of the first PCR
product was amplified using M13 forward primers fluorescently labeled with FAM (blue),
NED (yellow) or VIC (green) and an M13 reverse primer. For the second PCR, 2 mM
MgCl2, 10 mM dNTPs, 20 µM fluorescently labeled M13 forward primer (FAM, VIC or
NED), 20 µM unlabelled M13 reverse primer, and 1 U Taq polymerase were used in a
reaction volume of 10µl. The thermal cycling for the second PCR consisted of an initial
denaturation step of 3 min at 94oC, then 10 cycles of denaturation at 94oC for 30 sec,
annealing at 55oC for 30 sec and elongation at 72oC for 30 sec, followed by a final extension
step of 6 min at 72 oC. The products were then visualized on 2% agarose gels to confirm
amplification. Subsequently, 2µl of the PCR products were mixed with 0.5µl LIZ (internal
lane standard) and 7.5µl formamide in a final reaction volume of 10µl. The samples were
then submitted to the Genescan facility of the Department of Human Genetics, Radboud
University Medical Centre, Nijmegen, The Netherlands, where the fragments were size-
separated using capillary electrophoresis on 3730(XL) DNA analyzer. The results obtained
were analyzed using Applied Biosystem software Gene Mapper v4.0. The difference in the
allele sizes of the selected polymorphic markers enabled the construction of haplotypes in
affected and unaffected family members. The ultimate goal was to use this information to
determine whether the haplotypes segregated with the disease in the family, and to
determine the critical linkage interval of the disease locus.
2.5.5 Plausible Candidate Gene Analysis and Mutation Screening
Several potential candidate genes resided in the homozygous regions of two families
(TMCO1 for GLC 4; TMEM74, PITX2, FOXC1 for GLC 8) and were thus screened for
mutations in the probands of the respective families by Sanger sequencing (sequencing
primers and product sizes are provided in Annexure 4), followed by segregation analysis
in all affected and unaffected family members.

45
2.6 Exome Sequencing
Two unsolved families with JOAG (GLC 1 and GLC 5) and one unsolved family with PCG
(GLC 2) were sequenced for all exons in the genome by exome sequencing. This technique
enables the identification of novel disease genes. In exome sequencing, enrichment of all
genes of the human genome is performed followed by next-generation sequencing. Three
affected members of GLC 1, two affected members of GLC 2, and four affected members
of GLC 5 were selected for exome sequencing.
The procedure was performed on a 5500xl Genetic Analyzer platform from Life
Technologies (Carlsbad, CA). The Sure Select XT Human All Exon v.2 Kit (50Mb) from
Agilent Technologies, Inc. (Santa Clara, CA) was used to capture all coding regions of
~21,000 genes in the selected family members. This procedure is known as target
enrichment. Genomic DNA is digested into smaller fragments of 150-200 bps, blunt ends
were created followed by phosphorylation of the 5’ end and adenine overhangs were
produced via Klenow fragments, followed by ligation to the indexing-specific adaptors and
subsequent PCR amplification. The PCR products were hybridized to the enrichment probe
library containing biotinylated ribonucleic acid (RNA) probes. Streptavidin-coated
magnetic beads were used to extract the hybridized fragments and the RNA probes were
digested, yielding enriched DNA for further use.
A SOLiD TM sequencer (Life Technologies) was used for next-generation sequencing,
which uses five universal sequencing primers and a ligation-mediated di-base detection
system. Initially, the universal primers were annealed to the adapter sequences, followed
by annealing and ligation of 8 nucleotide probes that was composed of two color-coded
bases and a fluorescent label at the 3’end. The 3 bases at the 3’ end of the 8 nucleotide
probes along with the fluorescent label were then cleaved off. All five universal primers
were then offset by a base followed by probe annealing, ligation, fluorescence detection
and finally by cleavage of the fluorescent label for the detection of the inserted bases. The
template DNA sequence was retrieved by decoding the sequences of the colors. The hg19
reference genome assembly was used to align the variants, using Life Scope software v2.1
(Life Technologies). Small insertion-deletion changes in the sequences were detected using
the Small Indel Tool, and variations in single nucleotides were detected using the DiBayes

46
Table 2.2 Primer sequences of CA repeat markers used for the chromosome 3 locus in PCG
family GLC 2. The Marshfield location (cM), the primer sequence and with product length
are provided.
Marker Location
(cM)
Primer Sequence 5’ to 3’ Product
size (bp)
D3S3678 67.73 F-ACCTGTAGAGTCCAGGGATGC
R-GGGCTCATTCTCATGCAAAG
219-265
D3S3647 67.73 F-GGCTCAGAGCAGGCATAC
R-CCTAACTAATAAAATGTGTTCCCAG
190-228
D3S3597 68.38 F-CACACCCATTAGGATGGAA
R-GCAAATAGTAGGTGCTCAATAAACA
261-269
D3S3624 68.77 F-GGCTCAGAGCAGGCATAC
R-CCTAACTAATAAAATGTGTTCCCAG
190-228
D3S2409 70.61 F-GGTGACAGAGACTCTTGTCTCA
R-CATTCTGGTTGGGGAACATA
115-127
D3S3629 70.81 F-CAAGCAGATGTTGCTGCC
R-GGAATTACCTGGATTGCCC
236-25
D3S3667 70.89 F-TTTAAGAAGCCTTTGTCAGAA
R-CTATTGATGTTTCATGGTGC
167-183
D3S1568 70.89 F-CCATGAACAGAACCTCCCTA
R-CCGCTGTCCTGCTGTAAG
276-296
D3S1621 70.89 F-TTTGAGAAATGCCCCC
R-GAGCCAAGCCCTGGTT
97-139
D3S1573 70.89 F-TTCATTTTTGCTTATTAAGATATGC
R-CCAGTAAATNACAGGGCTAT
136-154
D3S3561 71.22 F-TCCTGGGGACTGTGATG
R-TCCTGGGGACTGTGATG
185-229
D3S1581 71.41 F-CAGAACTGCCAAACCA
R-GGGTAACAGGAGCGAG
78-102
D3S1578 70.61 F-GCCAACACACATTAATCACATA
R-GGGGCCAAAATCTGCT
140-166
D3S1582 72.21 F-CAGCAGGTACTATGAAAGCCTGT
R-GGAACAGCCCTATGGTTCAC
154-178
D3S3660 74.65 F-GCATTTTAAGACTCACAGAATGTT
R-TGGCAGGAAGTTCTTCATT
192-202
D3S1613 75.18 F-TGTGATAAGGACCAAGGC
R-GAGCAAATTGCAGAATGAG
225-253
D3S3721 77.26 F-GAAACCTCCTGACCATCC
R-CCAGTCTTGCTCTGTCAATC
203-219
F, Forward; R, reverse

47
Table 2.3 Primer sequences of CA repeat markers used for the chromosome 7 locus in PCG
family GLC 2. The Marshfield location (cM), the primer sequence and with product length
are provided.
Marker Location
(cM)
Primer Sequence 5’ to 3’ Product
size (bp)
D7S509 142.55 F-ACTGAACCTGGGGTGG
R-GTTGCTGGCCCTGTAGTA
203-225
D7S495 145.33 F-TGGCATTCATTTACAATAGCC
R-AGCACCTGGTCCAATTTTCT
150-168
D7S2560 145.34
F-AATGACTATTGCAGACTCAAAC
R-TAATTTCTTAGGATTCTTCAGAGG
149-195
D7S684 147.22
F-GCTTGCAGTGAGCCGAC
R-GATGTTGATGTAAGACTTTCCAGCC
169-187
D7S2202 148.73 F-TCTCTTACCCTTTGGGACCT
R-CTTGCAGATGGCCTAATTGT
149-169
D7S2513 150.22 F-GCAGCATTATCCTCAACAGC
R-CACAAATGGCAGCCTTTC
157-181
D7S661 151.16 F-TTGGCTGGCCCAGAAC
R-TGGAGCATGACCTTGGAA
252-282
D7S676 152.14 F-TGANTCTAAGCAGCCACCT
R-GCAACATGATCCAGAAAACA
148-166
D7S2511 154.43 F-CAGAGCAATACCATCAAAAC
R-GTACCATAAACTGGGTGGC
225-265
D7S794 155.1 F-GCCAATTCTCCTAACAAATCC
R-TATGCCCATGTGTTAGGGTT
168-208
D7S2442 159.53
F-TGAGCCAAGATCACAGCACT
R-TGAGCCAAGATCACAGCACT
226-236
D7S688 159.53
F-TGCAGAAATGCCTCCCTAAATATAA
R-ACAGGAAACGATTGCCATCCTT
147-161
D7S2426 160.09
F-GGTGGCTTGCCCAGAG
R-CCAGTGCATCTGTTTCCC
105-127
F, Forward; R, reverse

48
Table 2.4 Primer sequences of CA repeat markers used for the chromosome 15 locus in
PCG family GLC 2. The Marshfield location (cM), the primer sequence and with product
length are provided.
Marker Location
(cM)
Primer Sequence 5’ to 3’ Product
size (bp)
D15S155 52.33 F-TGGAGTTTCCTGCACCTATC
R-TGCACCCAGCCTGCTAT
229-249
D15S117 56.46 F-GCACCAACAACTTATCCCAA
R-CCCTAAGGGGTCTCTGAAGA
132-150
D15S1026 72.37
F-TGAATTGAACACCTGCCC
R-AGTCAAGTTGGTTTCCCTGG
181-215
D15S1005 75.27
F-GGCTAGAAACAGGATGTCCTC
R-GCCCAGCCTTAACTGCTT
102-122
D15S114 80.3 F-AGAATGAGCAGCACTGTTTG
R-TTGTCACTGCTTTTCTCTGC
177-187
F, Forward; R, reverse

49
algorithm, with high-stringency calling. The data generated were then filtered to identify
the potential disease-causing mutation.
2.6.1 Exome Variant Filtering
Filtering of the genetic variants in the exome data was performed, as initially thousands of
variants were obtained in each individual. For each family, variants were selected that were
present in all affected individuals that were analyzed by exome sequencing. The variants
that were detected in less than 10 reads were removed. Exclusion of synonymous and non-
coding variants resulted in a few hundred remaining variants. Different filtering protocols
were used for recessive and dominant families.
2.6.1.1 Variant Filtering in Recessive Families
In recessive families variants with a population frequency of less than or equal to 0.5% in
the dbSNP database were retained. Moreover, filtering for homozygous variants was
conducted by retaining variants that were present in more than 80% of variant calls. For
filtering of the compound heterozygous variants, 20-80% variant calls were also taken into
account and only considered 2 (or more) variants that were present in the same gene. To
confirm the number of the variant calls, validation was done by checking the Binary
Sequence Alignment/Map format (BAM file) to minimize the chances of automatic
generation of the number of reads in the output file. Moreover, the variants with a
Grantham score higher than 80 or a phyloP score of more than 2.0 were retained. All these
filtering steps enabled to narrow the number of variants from hundreds to just a few
variants.
2.6.1.2 Variant Filtering in Dominant Families
In dominant families, all filtering steps were the same as for recessive families, except that
variants that were present on 20% - 80% of variant calls were retained, which potentially
represent heterozygous changes. Moreover, sequences with more than 2 reads were also
considered.

50
2.6.2 Variant Screening and Validation
Variant filtering in PCG family GLC 2 resulted in the identification of a single
heterozygous 18-bp deletion in SH3PXD2B (previously implicated in Frank-Ter Haar
syndrome, an autosomal recessive disorder involving glaucoma (Iqbal et al., 2010)) and 9
homozygous variants. These variants were screened for segregation in all family members
by Sanger sequencing. To determine whether a second heterozygous variant in SH3PXD2B
was missed by exome sequencing, all coding exons of SH3PXD2B were screened in family
GLC 2 by Sanger sequencing (primer sequences are given in Appendix 5). The exome
data for the dominant families GLC 1 and 5 were filtered using the above mentioned
criteria. First, variants in genes in the known glaucoma loci were filtered, and sequenced
to evaluate their segregation in the families (Table 2.5). Next, heterozygous variants and
compound heterozygous variants with high phyloP or Grantham scores were then analysed
for segregation (Table 2.5). Finally, variants in genes related to pathways of known
glaucoma genes were screened for segregation in family GLC 5 (Table 2.5).
After variant filtering, less than 40 potentially pathogenic variants remained for families
GLC 1 and GLC 5, which were all validated and analysed for segregation in the families
by Sanger sequencing. The sequencing primers for the variants were designed by the online
software Primer3 (http://frodo.wi.mit.edu/). The primer sequences and product sizes that
were used to amplify all analysed variants in GLC 1, GLC 2 and GLC 5 are provided in
Tables 2.5-2.7. The amplified PCR products were sequenced as described above in section
2.5.1.2.
2.7 Screening of Sporadic Cases
Approximately 500 cases with POAG, 200 cases with PACG, 300 cases with PEXG
patients, 300 AMD patients and 300 age- and gender-matched controls were genotyped for
various glaucoma and AMD associated SNPs. The SNPs were selected on the basis of their
previously reported associations with the disease. In addition, for the glaucoma cohorts two
variants (p.Thr377Arg in MYOC and p.Met98Lys in OPTN) were selected that were
recurrently detected in affected individuals of glaucoma families by exome sequencing and
were predicted to be potentially pathogenic by different pathogenicity predicting softwares.

51
Moreover, the Exome Variant Server (EVS) (http://evs.gs.washington.edu/EVS/) and 1000
Genomes were used to determine the frequency of the variants. Selected SNPs were
genotyped in the respective cohorts using various techniques as described in the following
sections (2.7.1 to 2.7.4).
2.7.1 SNPs Genotyped by Taqman® / Kaspar’s (KASP) Assay
Three intronic SNPs, rs11720822 in PDIA5, rs2754511 in BIRC6, rs10906308 in OPTN,
and the exonic variant rs2234926 in MYOC were screened in sporadic glaucoma cases and
matched controls, whereas rs1061170 in CFH, rs10490924 in ARMS2, rs429608 near CFB,
rs2230199 near C3, rs5749482 near TIMP3 and rs442063 near APOE were genotyped in
AMD samples and matched controls using the Taqman®/KASP allelic discrimination
assays performed by Real-time PCR (Applied Biosystems 7900HT Fast System and
Sequence Detection Systems Software v2.3, Foster City, CA). PCR amplification was
performed according to the protocol of the manufacturer using 10ng of DNA in a reaction
mixture of 4l, using fluorescently labeled primers containing VIC and FAM. After an
initial denaturation step of 12 min at 95oC, 50 cycles of amplification were performed for
15 sec at 92oC and termination for 90 sec at 60oC. The results of the Taqman® and KASPar
allelic discrimination assays were then analyzed with the software SDS1.4/SDS2.0.6 on
the 7500 Fast Real-time PCR system or SDS2.3/SDS2.4 on the 7900HT Fast Real-time
PCR system.
2.7. 2 PCR-Restriction Fragment Length Polymorphism (RFLP) Analysis
Glaucoma and matched control samples were genotyped by PCR-RFLP, for the following
SNPs: exonic SNPs rs11258194 in OPTN, rs1801270 in p21, rs2567206 in CYP1B1,
rs1042522 in p53, rs1043618 in HSP70, rs11024102 in PLEKHA7, rs3753841 in
COL11A1, and rs1015213 in PCMTD1. The AMD samples and matched controls were
genotyped by PCR-RFLP for the following SNPs: rs3732379 and rs3732378 in CCRX1,
rs243866 in MMP2, rs17576 in MMP9, rs1800629 in TNF and rs16944 in IL1B. PCR
primers used for amplifying the genomic intervals containing these SNPs, the product
length of the PCR product, and the annealing temperature for the PCR are provided in

52
Table 2.5 Exome variants and their primer sequences screened in JOAG family GLC 5
F, Forward; R, reverse
Gene
name
Variant PhyloP Grantham SNP/ Novel
variant
Primer Sequence 5’ to 3’ Product
size bp)
SH3RF2 1105G>C; p.Ala369Pro
3.22 0.00 rs145544864
F-CCACAAACCACAGAGAGGAC 356
R-TGTCTCTGGATGGGATGTTT
ERAP1 1939C>T;
p.Val647Ile
5.71 29 rs111363347 F-ATGATCGGGCGAGTCTCATT 246
R-TCCTTCCTTCAAGTGCCTTAGT
GPR151 694G>A;
p.Arg232*
0.05 1000 Novel F-GAGACAGTGCCAAATGTTCC 376
R-TGGTTTAACATGGCCAGAAT
TSSK1B 28G>A; p.Arg10*
1.01 1000 Novel F-CAGCCAGCAACACTTCCTTG 230
R-GGAGATGAGCATGTGGAGGA
ITGA8 405C>G;
p.Trp135Cys
6.089 215 Novel F-TTTGGAGGAGTTTGACAAGG 288
R-GCTTGAAAACATTCCAGTGC
ICMT 211A>T;
p.Cys71Arg
2.82 112 Novel F-TCAGCAAATCGGCTCTATCT 292
R-GATGAGACAGGGATGAGGAA
CASD 1046G>A;
p.Ser349Asn
2.48 81 Novel F-TGAGCTAAGACCCCCACAG 388
R-CCACAGAGAGACCGAGAGAA
MYCBP2 7295A>C;
p.Ile2432Thr
142 99 Novel F-TAGGATTGCCAGGAGGTATG 447
R-AGTCATGAGGGCTACAGTGC
SLC7A7 1103A>G;
p.Met368Thr
3.5 81 Novel F-AAACCAGAAGAGGACCAGGA 326
R-ACAACTCCAGCTGTTTCAGG
HEATR5A 911T>C; p.Glu304Gly
4.92 94 rs191067821 F-CGCAGAGTATCTTTGGAGGA 290
R-AATGTTTTGGCCTTACCATTTA
DLGAP4 733G>A;
p.Ala245Thr
5.30 58 rs146757517 F-AGTCCAGCGGCTTTTCTT 439
R-AATGTTTTGGCCTTACCATTTA
DNAH17 11588G>T;
p.Ser3863Phe
5.75 144 Novel F-GCTGAAGAAAGTCCACCAAA 364
R-TGAAGTGGTGTCTCATGTGC

53
Table 2.5 cont.
F, Forward; R, reverse
Gene
name
Variant PhyloP Grantham SNP/ Novel
variant
Primer Sequence 5’ to 3’ Product
size bp)
UQCRB 200A>T; p.Leu67Pro 4.65 113 rs139283183 F-AGGGTTAATGCGAGATGATACA 204
R-TGAGCAACACTGTCAGGTAGA
OPLAH 1750C>A; p.Gly584Ser 2.31 159 rs10107332 F-AGAAGCAGAACAGGTGTCCT 246
R-AGTCAGGAAGCCACGTACC
RMI1 980del;
p.Gln327_Thr333delinsPro
4.11 1000 rs146219782 F-CAGAACGATGTTTCACCACA 389
R-AACAGATGGACAACCAAATGA
GPR148 266C>T; p.Pro89Leu 1.48 98 Novel F-CAGCCAGCAACACTTCCTTG 230
R-GGAGATGAGCATGTGGAGGA
GPR148 205C>G; p.Leu69Leu 2.39 32 Novel F-CAGCCAGCAACACTTCCTTG 230
R-GGAGATGAGCATGTGGAGGA
MASTL 928A>G; p.Ile310Val 1.69 29 Novel F-GGAATGCCTGTGAAGTGTCT 157
R-TCCCTCAAACCTGGCAATCT
MASTL 2128C>T; p.Thr710Ala 5.33 74 Novel F-ACGCCTAGTAGCCTATGAGC 228
R-TCAGGTGCAAGGTAGTCTGG
NUP210 4063C>A; p.Ala1355Thr 1.78 99 Novel F-TTTTGTTTTCCAAAGGGATG 292
R-CGTTCACCTTCCAGCTAAGA
EBLN1 644T>C; p.Glu215Gly 0.46 98 Novel F-CGATATGCACCAACAGCCTC 247
R-ATCATCTGTGCTTTGCTGGC
MMP14 1016G>A; p.Arg339His 2.91 29 rs140740223 F-GACAACAGTGTGAGACTCCATC 351
R-GAGTGCCTGGTTACCTTTGA
IFT80 1229G>A; p.Pro410Leu 2.8 98 rs148396265 F-TTTTCCCAAGGATAAACTATTCTG 397
R-TTTGAAAACAAAATAGAAAGCTCA
GBA2 587C>T; p.Arg196Gln 4.53 43 Novel F-TGATGGTGCAGTGGTAACAG 322
R-AAGATGGGTGTGATCTGACG

54
Table 2.5 cont.
Gene
name
Variant PhyloP Grantham SNP/ Novel
variant
Primer Sequence 5’ to 3’ Product
size bp)
APLO3 104C>A 0.84 109 rs148885226 F-CTGGGAAGCATCCTGTTTT 176
R-AACAGCTGGATCTTGCTCAC
SKIV2L2 1A>T; p.Met1? 3.11 11 Novel F-ATCGTGGGTAGGAGGGAGAT 182
R-TCCTTACCCTGCCTTGTCTG
EYS 6982C>T;
p.Gly2328Arg
0.30 125 Novel F-GCCATATTCCTGCAAATGTT 300
R-GACTTGTCATTTTCGTCTCTCA
SPHK1 957G>C;
p.Pro319Pro
2.23 22 Novel F-TGAGAAGTATCGGCGTCTGG 236
R-CTAGCACAAAGTCCTCGTCG
MYCBP2 7295A>C;
p.Ile2432Thr
3.30 142 Novel F-CCAGTGAGAATATGCTGATCCG 210
R-GTCTAGTGCAAGTTAATGGGCA
BDKRB1 844C>G;
p.Arg282*
0.17 125 rs145322761 F- CGCAAGGATAGCAAGACCAC 194
R- AGGGAGCTGTTAGTGAAGGC
ATM 2932T>C;
p.Ser978Pro
3.98 74 rs139552233 F-GAAGAGTACCCCTTGCCAAT 374
R-CTTGCATTCGTATCCACAGA
DCBLD1 568G>A;
p.Val190Ile
2.36 29 Novel F- CCCCTTGCCAATGGAAGATG 249
R- GTCCATATTGCTTTGACCTAGGT
COL22A1 3754C>T;
p.Gly1252Ser
2.73 56 Novel F-TGAAACTGCCTTCGTCTTTC 288
R-TGGGGACAGCAGTGTTTACT
F, Forward; R, reverse

55
Table 2.6 Variants detected by exome sequencing and analysed for segregation analysis in JOAG family GLC 1
Gene
name
Variant PhyloP Grantham SNP/ Novel
Variant
Primer Sequence 5’ to 3’ Product size
(bp)
VPS13D
3272G>A;
p.Cys1091Tyr
6
194 Novel F-TTTGATATTCCAACGGGAAG 380
R-CCTTGTTCTCTGAAGCTTCTTT
AASS
2152G>A;
p.His718Tyr
5.86
83 Novel F-GTGTGCCTTCTCAATGTTCC 399
R-CTGTCCCCAACTCCTAATGA
KIF19
664G>A; p.Ala222Thr
5.82
58 rs34016821 F-TTTCCCAACTGCTCAGACAT 469
R-TCCAACTCCTACGAAGCTGA
GCDH
886G>A;
p.Gly296Ser
5.57
56 Novel F-TGTGATGTGAACCACAACCT 299
R-AGAGAGTGAAACCCAAGCTG
ENOX1
171C>T;
p.Met57Ile
5.41
10 Novel F-AACAAACACCCTTGCCTATG 294
R-AAAGACTGTGTCCAACACTCG
PLIN2
269A>G; p.Ile90Thr
4.58
89 Novel F-AGCCCATTATTGCCATTTTT 224
R-CCAGGTTGGGAAAACAAGTA
COL9A2
1061G>A;
p.Pro354Leu
4.48
98 Novel F-AATCAGGAGCCAAGAGGATT 146
R-AGGAGAAAGAGCTTCCCTGA
MYO18A
2071G>A; p.Arg691Cys
4.42
180 Novel F-TCCTTTAGGACCTGCTCATTC 491
R-CAGAGCATCTGTTCACTCCA
NFIB
274G>A; p.Phe92Leu
4.34
74 rs140030018 F-CATTCATCGAGGCACTTCTT 285
R-CGGGATTGGATAAGACACAG
TMPRSS7
311T>G; p.Leu104Ser
3.79
61 Novel F-ATTGGCCTTACCTTGAATCC 382
R-TCCCACATTGTAATGCTTCA
R3HDM1
2492T>C;
p.Val831Ala
3.76
64 Novel F-GGCTTCAACCTGGTTTTCTT 369
R-CGGGATTTCAAATTCAAGC
CNTRL
1136A>G;
p.Asp379Gly
3.49
94 Novel F-TCCAAACTTTCACTCTTCTGTG 388
R-GTTGTTCATCTGGCTCCATC
F, Forward; R, reverse

56
Table 2.6 continued
Gene name Variant PhyloP Grantham SNP/ Novel
variant
Primer Sequence 5’ to 3’ Product size
(bp)
SUSD4
190C>T;
p.Glu64Lys
3.11
56 Novel F-TAAAATGTCCTTGGCTTTGG 362
R-TTCCGTGGAGAAGTAAGCAC
ADPRH
977C>A;
p.Ser326Phe
3.07
144 Novel F-TCTTTCGGTGTGAAGGAGAG 397
R-AATCCATCAGAAGTGAACATCA
C4orf21
163C>T 2.62
21 rs148197910 F-CGCCTAGCTCTAATATGTGTTGT 273
R-TCGGCCAGAGGATATAAATG
CNGB3
1208C>T;
p.Arg403Gln
2.39
43 rs147876778 F-CCTCCTTGGGCTTGTTTCAT 390
R-GTTTGTGGTTCTGGAAGGCC
ARHGAP44
2371C>T;
p.Arg791Cys
2.21
180 Novel F-ATCGACTGTGCAACACAATG 298
R-AGAACACTTGGCAAGCTCAT
C9orf128
133A>C 0.89
99 rs151344607 F-TGAAGCCTGTACCCTGTTCT 370
R-ATAGGTAGGGGTCTCTGAAGGA
WBSCR28
373G>A;
p.Ala125Thr
0.71
58 Novel F-TGCTCCTCAAGATCAACCTC 146
R-AAGCAGTGGGACTTCTGACA
BDKRB1
721G>A; p.Gly241Arg
0.62
125 rs45528332 F-TCCCAGATCTGAACATCACC 497
R-GCTTGCACCTGGAATAAGAA
DKK3
1018C>A;
p.Ala340Thr
0.53
99 Novel F-GATGTTGACGGGAAGTGAAG 491
R-GGGGAAACTTACTGGGAAGA
WBSCR28
550C>T;
p.Arg184Cys
0.009
180 Novel F-TGTCAGAAGTCCCACTGCTT 295
R-TCTGGGAGTTTCTTGCTCTG
CGN
725A>G;
p.Asp242Gly
0.79
94 Novel F-TCACTCATCAACAAGTTTGACAG 270
R-CAAAACTCTGAAGGACCCAGT
NCOA7
724C>T;
p.Val242Met
0.26
83 Novel F-ACCTGGCTTCAGAAAAGGAT 298
R-CAAATGCAGAAGAAGTGTCG
F, Forward; R, reverse

57
Table 2.6 continued
Gene name Variant PhyloP Grantham SNP/ Novel
variant
Primer Sequence 5’ to 3’ Product size
(bp)
ZP4
1226G>A;
p.Pro409Leu
0.62
98 Novel F-CCATCCTGGTAAAGGGGTAA 390
R-TTGTAAGTTGGGGAGGTTCA
ASB10
545G>A;
p.Lys182Arg
2.39
64 rs151344607 F-CTGTGTTCATGTGCTGCTGG 154
R-GCCTCTTTGCTTCCCTTCAG
NEBL
1108G>T;
p.Gln370*
3.16
53 rs146198369 F-ATATGCTTTTCTTTTTCCAATGA 296
R-TAGACAAGATCCCAGGCAGT
F, Forward; R, reverse

58
Table 2.7 Homozygous variants detected by exome sequencing and analysed for segregation analysis in PCG family GLC 2
Gene name
Variant PhyloP Grantham SNP/ Novel
Variant Primer Sequence 5’ to 3’
Product
size(bp)
SH3PXD2B
2629del;
p.Phe876Lysfs*16
4.35
1000
Novel
F-CTCTTTGTATGTGGCCGTGG
202 R-TCTAGGCAGAAAGGGAGTCG
CACNA1D
2474T>C;
p.Ile825Thr
4.27
89
rs147933585
F-TTCAGCCTTCTTCTCACCTG
452 R-GTGACACATTCTGCCTGTGA
CILP
217G>A;
p.Arg73Trp
3.80
101
Novel
F-AGGGAAAGGAGAACTGGAGC
162 R-ACGGTCCCCATAGTAGAAGC
ANKDD1A
1096C>T;
p.Arg366Cys
2.5
180
rs144426862
F-ACCTTTCTGCTCTCAGCGTA
349 R-ATCACCTGCTTGGAGACTGA
LRRC8E
580G>C;
p.Gly194Arg
2.33
125
Novel
F-TCGTGGTCATTCACACACTC
492 R-CCACCAGGAAACTGATCTTC
CSPG4
4813G>A;
p.Leu1605Phe
2.22
24
Novel
F-GTGCTGATCATGGGCATT
505 R-TTCTGGGAACATGAACTTGC
CLRN3
532C>T;
p.Gly178Arg
1.89
125
Novel
F-CATGCCATGCATGAAACTC
300 R-ATAAAATTCCGTCCCTTGGA
ALS2CL
2843T>G;
p.His948Arg
0.46
77
Novel
F-CTATTGAGCCCTAGATCCTGTG
299 R-AGCATCTTCCTGTGCAAAAC
TRAIP
898C>T;
p.Glu300Lys
2.83
56
rs143310707
F-AGGTCATCTCTGCCTTCAGC
112 R-GGGGGAGTATCCACATCAAA
F, Forward; R, reverse; del, deletion

59
Table 2.8. After PCR amplification, PCR products were subjected to RFLP analysis for all
above mentioned SNPs. The amplified products were digested overnight at 37°C with
respective restriction enzymes (Fermentas, Waltham, MA) (Table 2.8). The digested
products were then electrophoretically separated on agarose gels ranging from 2-4%,
resulting in the separation of the homozygous ancestral allele from heterozygous and
homozygous variant alleles.
2.7.3 Variable Number of Tandem Repeat (VNTR) Genotyping
A 27-bp insertional VNTR in intron 4 of NOS3 was genotyped by PCR amplification in
the glaucoma and AMD cohorts, and matched controls. The VNTR region was amplified
using the Gene amp® PCR system 2700 (ABI, Foster City, CA). Briefly, the protocol
consisted of 35 cycles of DNA denaturation at 95°C for 1 min, primer annealing at 60°C
for 45 sec and extension at 72°C for 1 min, followed by a final extension step at 72°C for
5 min. The constituents of the reaction consisted of: 1.2 pM of each primer, 10 mM dNTPs,
2 mM MgCl2, 1 U Taq polymerase and 1× PCR buffer, along with 40–50 ng of DNA. The
PCR products were electrophoretically separated on 4% agarose gels and visualized under
ultraviolet light. Two alleles were obtained when this region was amplified: “NOS34a,”
which was 393 bp long and consisted of four 27-bp repeat units, and “NOS34b,” which
was 420 bp long and consisted of five 27-bp repeat units.
2.7.4 Variant Analysis by Sanger Sequencing
150 AMD samples and 150 matched controls were sequenced for eight SNPs in the
promoter region of VEGF using a single primer set with forward primer 5’-
GCAGCGTCTTCGAGAGTGAG-3’ and reverse primer 5’-
CCGCTACCAGCCGACTTT-3’. The promoter region variants were selected because
these variants may be important for regulating the gene expression. The SNPs that were
analyzed in this 0.5kb region were rs833061 (-460C>T); rs833062 (-417T>C); rs13207351
(-152G>A); rs59260042 (-1210C>A); rs79469752 (-1203C>T); (-160C>T); rs28357093 (-
141A>C); and rs1570360 (-116G>A). The sequences were analyzed using Vector NTI
Advance 11 software (Invitrogen Life Technologies, Carlsbad, CA).

60
Table 2.8 Primers sequences and restriction enzymes used for RFLP analysis
Gene Variant Primer Sequence 5’ to 3’ Annealing
Temp.
Enzyme
OPTN rs11258194 F-TCCACTTTCCTGGTGTGTGA
R-TTTTCCAAGCTCTTCCTTCAA
58oC Stu1
P21 rs1801270 F-GTCAGAACCGGCTGGGGATG
R-CTCCTCCCAACTCATCCCGG
57oC Esp1
CYP1B1 rs2567206 F-GGTTGTGAGCGTGGTTC
R-TCTCACAACTGGAGTCGCAG
55oC Taq1
P53 rs1042522 F-TTGCCGTCCCAAGCAATGGATGA
R-TCTGGGAAGGGACAGAAGATGAC
60oC Bsh12361
HSP70 rs1043618 F- CGCCATGGAGACCAACACCC
R- GCGGTTCCCTGCTCTCTGTC
60oC Brsb1
PLEKHA7 rs11024102 F-GTAGCACCTACTATATGATCT
R-TTCGCCTAGCTGGCTTCT
58 oC AseI
COL11A1 rs3753841 F-TCATTCTAGGGTCCTGTTGGT
R-TCCTGCATTTGCAATTACTTT
58oC NlaIV
PCMTD1 rs1015213 F-CTGATGCTGAGGCTGTACCTC
R-GAGGCTGACCTACCTCTGGTG
58oC HpyCH4III
TNF rs1800629 F-AGGCAATAGGTTTTGAGGGCCAT
R- GTAGTGGGCCCTGCACCTTCT
60oC NcoI
IL1B rs16944 F- TGGCATTGATCTGGTTCATC
R- GTTTAGGAATCTTCCCACTT
60oC Ava1
CX3CR1 rs3732379 F-CTCCCCAGCAAATGCATAG
R- GAATGCCTTGGTGACTACCC
60 oC AcI1
CX3CR1 rs3732378 F-GCAATGCATCTCCATCACTC
R-AACCACAAGAAAGCCAAAGC
60 oC HpyCH4III
MMP2 rs243866 F-ACTGACTCTGGAAAGTCAGAGCA
R-GGCACAGGGTGAGGGATGG
63oC Tsp45I
MMP9 rs17576 F-GAGAGATGGGATGAACTG
R-GTGGTGGAAATGTGGTGT
63oC MspI
F, Forward; R, reverse; Temp, temperature

61
2.8 Statistical Analysis
Allele frequencies between the unaffected controls and the patient groups were compared
with the Pearson χ2 test using online software (http://statpages.org/ctab2x2.html). The
genotype frequencies were calculated by logistic regression analysis keeping age and
gender as covariates. The data were statistically analyzed using R software (R Core Team
(2012). (R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0,
URL http://www.R-project.org/). In addition, Bonferoni correction was applied to the
individual p-values generated from logistic regression analysis.

Chapter 3
Results

63
3 Results
In the current study, twenty families with glaucoma and 2 families with AMD were
analysed. In addition, in the glaucoma association studies 350 healthy controls, 500 POAG,
200 PACG and 300 PEXG patients were analyzed for different SNPs, while for the AMD
association studies 300 healthy controls and 300 AMD patients were analysed for different
SNPs.
3.1 Results of Glaucoma Families
Initial screening of glaucoma families for mutations in known glaucoma associated genes,
resulted in linking one family with PCG to CYP1B1. In the rest of the families, two affected
members of the GLC 2 family (PCG), one member of GLC 4 (JOAG) and four affected
members of GLC 8 (JOAG) were selected for 250K SNP array analysis.
Of the unsolved glaucoma families, two affected members of GLC 1 with early onset of
symptoms of the disease, two affected members of GLC 2, and four affected members of
GLC 5 were selected for exome sequencing.
3.2 Exclusion of known genes
3.2.1 MYOC, OPTN, WDR36 and CYP1B1 Screening
Probands of the 20 families with glaucoma were screened for mutations in known
glaucoma-associated genes: MYOC, OPTN, WDR36 and CYP1B1.
3.2.1.1 MYOC, OPTN and WDR36 analysis
Several known and novel variants in MYOC, OPTN and WDR36 were found in the
probands of the 20 families, but these variants did not segregate with the disease in these
families (Table 3.1). However, a non-synonymous SNP in MYOC (rs2234926 c.227G>A,
p.(Arg76Lys)) was found in 50% of the probands, and an intronic SNP (rs2032555,
c.730+35G>A) was found in 13 % of the probands. In OPTN three variants were identified
in the families. Of these, the synonymous SNP rs2234968 (c.102G>A, p.(=)), c.293T>A,

64
Table 3.1 Recurrent SNPs and de novo variations in glaucoma and AMD associated genes identified by sequencing
NC; Not checked because the SNPS were not pathogenic
Gene Families
Screened
Coding
Exons
Recurrent
Variants (SNPs)
Segregation of
SNPs in Family Novel
Variants
Segregation of Novel
Variants in Family
MYOC 20 Glaucoma
families 3
rs2234926 NC c.648G>A Not Segregating
rs2032555 NC c.1438A>C
OPTN 20 Glaucoma
families 16
rs2234968 NC p.Glu95Gln Not segregating
rs11258194 Not Segregating
WDR36 20 Glaucoma
families 23 -- -- c.1628G>A Not Segregating
CYP1B1
20 Glaucoma
families 1 -- -- c.1169G>A Segregating
PXDN GLC 2 23 rs17841813 NC p.Thr237Asn Not segregating
rs1863135 NC p.Val1284Leu Heterozygous
TMEM74 GLC 8 2 -- --
CFH 2 AMD
families 23
rs800292 NC
p.Glu850Lys Not Segregating rs1061147 Not Segregating
rs368670743 NC

65
p.(Met98Lys) Fig. 3.1) was identified in 6.3% probands. In addition a novel variant (M2:
c.283G>C, p.(Glu95Gln)) in exon 5 of OPTN was found in one proband, however, none of
these variants segregated with the disease in the families (segregation is shown in Fig. 3.1
A,B,C & D, chromatograms are shown in Fig. 3.2 A & B).
Analysis of the variants Arg76Lys in MYOC and Met98Lys in OPTN were further extended
by screening the association of these variants with unrelated sporadic cases of POAG,
PACG and PEXG and compared with unaffected controls. The MYOC variant was not
associated with any subtype of glaucoma, but the OPTN variant was associated with
increased risk of POAG (section 3.5.1.2).
In WDR36 a novel variant, c.1628G>A (p.Arg543Lys), was identified in exon 14 of a
single proband, but further segregation analysis in the family revealed that the variant did
not segregate with the disease in the family.
3.2.1.2 Identification of a Homozygous CYP1B1 Mutation in a PCG family
Affected individuals of a family (GLC 16) were diagnosed with PCG, with the symptoms
appearing in the first decade of life. The affected individuals shared the same phenotype
and had raised IOP (>40 mmHg) and visual field damage. They had large bulging eyes
(buphthalmus) with varying opacity in the affected individuals. Due to the corneal
opacification, the optic nerve could not be examined. The elder affected members of the
family in their third and fourth decade, were completely blind. All symptoms were absent
in normal individuals of the family. The proband V:1 had bilateral juvenile open angle
glaucoma, 360o iris processors and increased CDR (right eye=0.6, left eye=0.9).
Pachymetry revealed thin corneas (right=0.44, left=0.43). Bilateral trabeculectomy had
been done and in the left eye, and a glaucoma Ahmed valve was inserted to control the
IOP.
Sequence analysis of the coding exons of CYP1B1 revealed a homozygous missense
mutation (c.868dup; p.Arg290Profs*37) segregating with the disease in PCG family
GLC16 (Fig.3.3). The variant was not found in 140 unaffected control individuals.

66
Figure 3.1 Segregation analysis and sequencing chromatogram of identified variants in
OPTN in POAG families A, B & C. Pedigrees with segregation analysis of rs11258194
(M1: c.293T>A, p.[Met98Lys]) and of a novel variant (M2: c.283G>C p.[Glu95Gln] D).
Generation numbers in the pedigrees are indicated by roman numerals. Filled squares and
circles are affected males and females, respectively, while the unfilled symbols are
unaffected individuals. Probands are indicated by an arrow, and all individuals that
underwent molecular genetic analysis are indicated by their mutation pattern, ‘+’ indicatest
the ancestral allele, ‘M’ indicates the derived allele. Individuals indicated with +|+ carry
the homozygous ancestral genotype, those indicated by +|M are heterozygotes carrying one
ancestral and the derived allele, and individuals with M|M carry the derived allele
homozygously.

67
Figure 3.2 A) Sequence chromatogram of rs11258194 c.293T>A p.Met98Lys in OPTN
showing the homozygous ancestral genotype (upper panel), the heterozygous genotype
(middle panel), and the derived homozygous genotype (lower panel). B) Sequence
chromatogram of c.283G>C showing the ancestral homozygous genotype (upper panel),
the heterozygous genotype (middle panel), and the derived homozygous genotype (lower
panel).
A B

68
Figure 3.3 Pedigree of a large consanguineous Pakistani family with PCG (GLC 16). The c.868dup; p.Arg290Profs*37 mutation in
CYP1B1 is indicated with an M, and the ancestral allele with a +. All affected individuals carry the mutation homozygously, while the
unaffected individuals are heterozygous or do not carry the mutation. The mutation segregates with the disease in the family through a
recessive mode of inheritance.
GLC16 (c.868dup; p.Arg290Profs*37)

69
3.3 SNP Microarray Analysis Results
3.3.1 Identification of a Possible Novel Locus of Primary Congenital Glaucoma
A recessive PCG family (GLC 2) was sampled from a village in Multan located in southern
Punjab, consisting of two affected and five unaffected individuals. Both affected
individuals suffered from raised IOP and nystagmus bilaterally. They had completely
opaque and bulging avascularised corneas, which were highly sensitive to touch and hence
normal ophthalmic tests were not possible for the affected individuals (Fig. 3.4). The IOP
measurement was conducted carefully with air puff tonometery and the IOP was found to
be >40 mmHg in both individuals. The patients’ fundus and the optic nerve could not be
visualized due to the opacity of the cornea. The patients also had Haab’s striae, which are
horizontal breaks in the Descemet's membrane. The signs of the disease started appearing
in the first year of their life, which was progressive and resulted in complete blindness.
Trabeculectomy had also been done for one individual to lower the IOP and pain in the
eyes. All the other unaffected siblings had no signs of glaucoma.
Affymetrix 250K SNP microarray analysis was conducted for both affected members of
the family, followed by analysis of the data by Homozygosity Mapper. This revealed five
homozygous regions: one on chromosome 3, one on chromosome 7 and three regions on
chromosome 15 (Fig. 3.5). Microsatellite marker analysis confirmed the homozygous
region on chromosome 7 and excluded the regions on chromosome 3 and 15 (Fig. 3.6). The
region was further refined by using microsatellite markers and a 2 Mb region was marked
as a common homozygous region in the affected individuals, while it was not homozygous
among any of the unaffected individuals, thus suggesting a possible novel locus for PCG.
No plausible candidate gene was present in the locus, and therefore the family was further
analyzed by exome sequencing. No potentially pathogenic variants were found within this
homozygous region on chromosome 7. In addition, all filtered homozygous variants with
high pathogenicity scores observed in the exome data were screened in the family (Table
2.7), but none of the variants segregated with the disease.

70
Figure 3.4 Clinical analyses of the two affected members in the PCG family GLC 2. i)
Shows an opaque cornea and bulging of the eyes due to an elevated IOP in individual II:3.
ii) Shows an opaque cornea of individual II:4, which also bulges out. Both individuals were
completely blind, iii) showing the B-scans done for II:4. The B-scan of the right eye shows
an integral haze with a total freely mobile fibrotic posterior vitreous detachment. The optic
nerve head shows a markedly deep excavated cup indicated with an arrow. The B-scan of
the left eye also shows a deep excavated cup (indicated with an arrow), but the patient had
normal tomographs.

71
Figure 3.5 Homozygosity Mapper plot of the congenital glaucoma family (GLC 2) (details of regions are given in Appendix 6)

72
Figure 3.6 Homozygous region linked to PCG in two affected individuals (II: 3 and II: 4) of family GLC 2. Both SNP array and
Exome sequencing were performed for both affected individuals.
GLC 2 (Chr.7:139,681,371-141,507,822)

73
3.3.2 Identification of a Homozygous Region in Juvenile Open Angle Glaucoma
Family (GLC 4)
A family with JOAG (GLC 4) with a dominant pattern of inheritance was sampled from
the suburbs of southern Punjab, Pakistan. Six affected individuals and seven unaffected
individuals were sampled from this family for analysis. Among the six affected individuals
four (indicated by * in Fig. 3.8) were not aware of having developed the disease and were
clinically suspected to be suffering from glaucoma based on persistent headaches and
blurred of vision. All family members (affected, glaucoma suspects and unaffected)
underwent diagnostic tests. Gonioscopic findings revealed a CDR> 0.5 in the affected and
individuals suspected of having glaucoma and all of them had visual field defects and a
raised IOP (>30 mmHg). Fundus fluorescein angiography (FFA) was conducted for the 7
normal individuals and 2 affected and 4 glaucoma suspects. The affected individuals as
well as glaucoma suspects had thinning of the nerve fibre layer. All normal individuals also
underwent diagnostic tests such as visual field analysis, IOP measurement, CDR analysis
and RNFL thickness estimation, which were within normal limits in all cases. Individual
V:2 was seven years of age and was most severely affected in the family. The diagnostic
tests helped in confirmation of the affected status of the glaucoma suspects as they all had
damaged optic disc, impaired visual field and thinned nerve fiber layer, all of these
symptoms were similar as in the established affected members of the family (III:3 and V:2).
Known glaucoma genes were excluded in the family and one individual (V:2) was selected
from the family for 250K SNP microarray analysis. The data were analysed by
Homozygosity Mapper, which revealed three homozygous regions in the family located on
chromosomes 1, 3 and 10 (Fig. 3.7, Annexure 6). OPTN, TMCO1, and COL11A1 were
positional candidate genes in these regions and were screened for the presence of
mutations. OPTN screening revealed no novel variant in the family, but SNP rs11258194
(Met98Lys) was found, which had previously been shown to be associated with glaucoma.
However, the Met98Lys variant did not segregate with the disease in the family (Fig. 3.8).
Analysis of the other two genes, TMCO1 and COL11A1, did not reveal any mutation in
this family. Therefore, the family was included in the panel of unsolved families (A;
Annexure 7).

74
Figure 3.7 Homozygosity Mapper plot of homozygous regions in a juvenile open angle glaucoma family GLC 8 (details of regions are
given in Annexure 6)

75
Figure 3.8 Pedigree of a recessive consanguineous Pakistani family with juvenile open angle glaucoma (GLC 4). The polymorphism
Met98Lys in OPTN is indicated with an M, and the ancestral allele with a ‘+’. All affected individuals carry the mutation homozygously
or heterozygously, while some of the unaffected individuals were also heterozygous, demonstrating that the variation did not segregate
with the disease in the family.
GLC 4 (c.293T>A; p.Met98Lys)

76
3.3.3 Identification of Homozygous Region in Juvenile Open Angle Glaucoma
Family GLC 8
A JOAG family with a recessive pattern of inheritance was sampled from KPK province
of Pakistan. Six affected and eight normal individuals were sampled for further analysis
(Fig. 3.9). The proband of the family (V:5) suffered from a raised IOP and blurred vision.
Due to the raised IOP, the individual was suspected to have glaucoma and underwent
additional diagnostic tests. Visual field analysis revealed arcuate defects in vision,
tonometery revealed a raised IOP (>30 mmHg), and gonioscopic findings also supported
the other two tests revealing an increased cup-to-disc ratio (CDR=0.7). The individual had
a family history of the disease and hence all the approachable family members were
screened clinically for glaucoma. There were six individuals in the family who had an
increased CDR (>0.6), an elevated IOP (>30 mmHg) and visual field defects. The normal
individuals had no visual field defects or alterations in the CDR and their IOP was in the
normal range. The symptoms of the disease started appearing at the end of the second
decade of life in all affected individuals. In addition, individual IV:3 (the father of proband)
suffered from diabetic retinopathy. Four affected individuals from the fifth generation (V:1,
V:3, V:5 and V:7) were selected for 250K SNP microarray analysis. Homozygosity
Mapper was used to analyse the data obtained from the array, which revealed 4
homozygous regions on chromosomes 3, 4, 6 and 11 (Fig. 3.10 Annexure 6). The family
(GLC 8, Fig. 3.9) was screened for mutations in known glaucoma genes (MYOC, OPTN,
WDR36 and CYP1B1), and no causative mutation was found in any of these genes. Using
the online UCSC genome browser, two genes known to be involved in anterior segment
defects (PITX2 and FOXC1) and four candidate genes (IFT80, COL25A1, ATXN1,
PLEKHA7) were selected from the homozygous regions, and were screened in the family
for disease-causing variants. No mutation was found in any of these genes. Therefore, this
family was also added to the panel of unsolved families (Annexure 7).

77
Figure 3.9 Pedigree of a consanguineous Pakistani family with juvenile open angle glaucoma (GLC 8), exhibiting an autosomal
recessive inheritance pattern. The sampled family members are indicated by *, and the proband by an arrow.
GLC 8 (Juvenile Open Angle Glaucoma Family)

78
Figure 3.10 Homozygosity Mapper plot of homozygous regions in juvenile open angle glaucoma family GLC 8 (details of regions are
given in Annexure 6)

79
3.4 Next Generation Sequencing Analysis
3.4.1 Identification of Three Variants MYO18A, ENOX1 and COL9A2 in JOAG
Family GLC 1
A large glaucoma family (GLC1) with a dominant mode of inheritance was sampled, but
due to a difference in the age of disease onset in the two loops of the family they were
analysed separately as independent families. GLC 1a had a juvenile onset (mean age 25
years). While GLC 1b had a late onset (mean age 50 years, Fig. 3.11). GLC 1a consisted
of ten sampled members (seven affected and three unaffected). There were two non-
consanguineous loops in GLC 1a, one of which had an early onset of the disease with a girl
(V: 5) being affected in the first decade of life. In the other affected individuals of loop
GLC1a the onset of signs and symptoms was in the mid to late half of the second decade
of life or at the beginning of the third decade. The patients suffered from a raised IOP and
pain in the eyes and forehead region. Ophthalmic examination revealed a raised CDR (0.7-
0.9), and visual field analysis showed loss in the field of vision. In addition, FFA was
conducted, which revealed RNFL thinning in the affected (individual IV:10, Fig. 3.12) and
also in two members of the family (IV:2, IV:4) who were unaware of the onset of
glaucomatic changes and were subsequently categorized as affected members (Fig. 3.11).
Two members of the family from the GLC1a branch (IV:10 and V:5) were selected for
exome sequencing. After filtering of the exome data, only 38 overlapping variants were
left among the two affected individuals. All variants were checked for segregation among
the GLC 1a and GLC 1b loops, and three heterozygous variants 2071G>A; Arg691Cys in
MYO18A, 171C>T; Met57Ile in ENOX1 and 1061C>T; Pro354Leu (rs201772619) in
COL9A2 segregated with the disease in the affected family members of loop GLC 1a.
Hence, all the affected members carry three variants in three genes, which were not present
in any of the normal members in any of the two branches. These three variants were not
present in 200 normal healthy unrelated control individuals. Two of the variants (in
MYO18A and ENOX1) were also present in a normal individual in loop GLC 1b (IV:1) but
of the third variant in COL9A2 was absent in this individual.

80
Figure 3.11 Pedigree of a consanguineous Pakistani family with JOAG (GLC 1a) as well as late onset POAG (GLC 1b) inherited
dominantly. Exome sequencing was performed for individuals IV:10 and V:5. Variants in three genes, MYO18A c. 2071G>A (black),
ENOX1 c.171C>T (blue), and COL9A2 c.1061C>T (red), were found to segregate with the disease in loop GLC1a. The variant allele is
indicated with an M, and the ancestral allele with a ‘+’. All affected individuals in loop GLC 1a carry the mutations heterozygously (IV:
10 carries MYO18A variant homozygously). The proband is indicated by arrow.
GLC 1 (MYO18A c. 2071G>A; p.Arg691Cys, ENOX1 c.171C>T; p.Met57Ile, COL9A2 c.1061C>T; p.Pro354Leu)

81
Figure 3.12 RNFL thickness for the patient IV:10 of JOAG family GLC1a. The figure
shows RNFL thinning in all four quadrants (nasal, temporal, superior and inferior), which
along with measurement of IOP, CDR clearly indicates that the individual is glaucomatic.

82
Exome sequencing revealed only one variant (724C>T; p.Val242Met) in the NCOA7 gene
segregated with the disease in the GLC 1b loop of the family (Fig. 3.13). The variant was
present in heterozygous form among the two affected members (IV:2 and IV:4) of the
family in the fourth generation; all unaffected individuals in this generation had the
homozygous ancestral allele. Of the three sampled individuals in the fifth generation, two
unaffected individuals (V:2 and V:3) carried the variant allele in a heterozygous state.
These two individuals at the time of sampling were in their first decade of life. As the
disease has a late onset in this branch of the family, the symptoms of the disease might not
have surfaced yet in these unaffected individuals. In loop GLC 1a, the variant in NCOA7
was present heterozygously in all affected members, except for one affected individual
(IV:12), while all normal individuals carried the ancestral allele (segregation not shown in
the pedigree). The variant was not identified in 200 unrelated normal unaffected controls.
3.4.2 Identification of a Variant in PHKG1 in JOAG Family GLC 5
Family GLC 5 (Fig. 3.14) was a consanguineous family with a dominantly inherited form
of glaucoma, sampled from the suburbs of southern Multan. This family had early onset of
the disease in two individuals (V:2, V:6) with appearance of symptoms in the middle of
the second decade of life, whereas among all other individuals the symptoms appeared in
the later half of the third decade. Individual V: 6 presented with a raised IOP (>30 mmHg)
as well as increased CDR, which was higher for the vertical diameter than the horizontal
diameter, creating a notch in the neuroretinal rim superiorly. Treatment of the patient with
beta-blockers helped in lowering the IOP to the normal range (18-20 mmHg). The other
affected members of the family (III:1, IV:4, IV:6, IV:7, IV:8) had a late onset of the disease
with the symptoms appearing in the later half of the third decade. Six affected members
and two normal individuals of the family were sampled. All sampled individuals underwent
ophthalmic examination. The visual field test confirmed abnormalities among the affected
members of the family only. They also had a raised IOP (>30 mmHg) and increased CDR
(0.8). All normal individuals of the family had an IOP in the normal range (<20 mmHg)
and normal CDR (0.1-0.3).

83
Figure 3.13 Pedigree of a consanguineous Pakistani family with late onset glaucoma (GLC 1b) inherited dominantly. Segregation of
variant c.724C>T; p.Val242Met in NCOA7 is shown in the figure. The derived allele is indicated with an M, and the ancestral allele
with a ‘+’. All elderly affected individuals in the third generation of loop GLC 1b carry the variant heterozygously, while in the fourth
generation, V: 2 and V:3 carry the varaint heterozygously.
GLC 1b (NCOA7: c.724C>T; p. p.Val242Met)

84
Figure 3.14 Pedigree of a consanguineous Pakistani family with juvenile onset open angle glaucoma inherited dominantly. Exome
sequencing was performed for individuals IV:4, IV:6, IV:7 and V:6. Segregation of a variant (c.125C>T) in the PHKG1 gene is shown
in the figure. The derived allele is indicated with an M, and the ancestral allele with a ‘+’. All affected members of the family are
heterozygous for the variant, and V: 6 was homozygous for the variant. The proband is indicated by an arrow.
GLC 5 (PHKG1: c.125 C>T; p.Thr42Met)

85
No novel or recurrent variants were found in the known glaucoma genes in this family, and
thus the family was further analysed by exome sequencing. Exome data filtering resulted
in forty variants, which were subsequently screened in the family for segregation. Out of
all variants, only one variant, 125C>T (p.Thr42Met) in PHKG1, segregated with the
disease in the family (Fig. 3.14). The variant was present in a heterozygous state in affected
individuals who had an onset of disease in the fourth decade of life, as well as in one normal
individual (V:7) of age below 10 years, and in homozygous form in one affected individual
(V: 6) who had juvenile onset of the disease and a severe phenotype with much raised IOP
and CDR as compared to other affected members of the family as well as severely reduced
visual fields.
3.5 Case-Control Association Studies
3.5.1 Case-Control Association Studies for Glaucoma
Patients and controls included in the case-control association studies for glaucoma were
age- and gender-matched (Table 3.2). The mean age (± standard deviation) of the controls
was 48.1±13.2 years, of patients with POAG 48.3±16.5 years, of patient with PACG
45.5±16.5 years and of patients with PEXG 50.09±14.1 years (Table 3.2). In total 350
healthy subjects (52% males and 48% females), 500 patients with POAG (51% males and
49% females), 200 patients with PACG (49.5% males and 50.5% females) and 300 patients
with PEXG (48% males and 52% females) were enrolled in the study. The majority of the
patients were under treatment by β-blockers, or had undergone surgery (trabeculectomy)
to lower their IOP.
3.5.1.1 Screening BIRC6 and PDIA5 Polymorphisms in Glaucoma Cohort
The allele and genotype frequencies of rs11720822 in PDIA5 were not significantly
different between POAG, PACG and PEXG as compared to the control individuals (Table
3.3). The T allele of rs2754511 in BIRC6 was found in 35% of control alleles, while it was
found in 32% of POAG alleles, 35% of PACG alleles, and 28% of PEXG alleles. The
frequency of the T allele was found to be significantly lower in PEXG

86
Table 3.2 Demographic and clinical features of the control, POAG, PACG and PEXG cohorts
Controls POAG p-
value PACG
p-
value PEXG
p-
value
Age 48.1±13.2 48.3±16.5 >0.05 45.5.±16.5 >0.05 50.09±14.1 >0.05
Gender
>0.05
>0.05
>0.05 Males 52% 51% 49.5% 48%
Females 48% 49% 50.5% 52%
IOP 16.4±2.3 30.5±11.6 <0.05 26.4±10.2 <0.05 28.4±10.5 <0.05
CDR 0.39±0.18 0.85±.63 <0.05 0.67±.27 <0.05 0.76±.23 <0.05

87
Table 3.3 Results of logistic regression analysis for genotype and allele frequencies of SNPs rs11720822 in PDIA5 and rs2754511 in BIRC6 in POAG, PACG and PEXG patients and control individuals
PDIA5
rs11720822
POAG
Est.
Z
value OR (95%CI) P-value/pb
PACG
Est.
Z
value OR (95%CI) p-value/pb
PEXG
Est.
Z
value OR (95%CI) p-value/pb
CC 0.07
17.90
0.16
0.02
0.9 (0.37-2.26) a
5.95(0.00-Inf) a
0.86/1.00b
0.98/1.00b
0.22
12.89
-0.45
0.01
0.79 (0.29-2.13)a
3.69 (0.00-Inf)a
0.64/1.00b
0.98/1.00b
0.60
15.55
1.30
0.01
1.82(0.74-4.48)a
5.68(0.00-Inf)a
0.18/1.00b
0.98/1.00b CT
TT
Allele Frequency
C - - 0.74 (0.41-1.34)c 0.28/1.00b
- - 1.00 (0.51-1.96)c 0.99/1.00b
- - 1.15 (0.60-2.19)c 0.66/1.00b
T - - - - - -
BIRC6
rs2754511
AA 0.39
0.18
-2.53
0.81
0.67 (0.49-0.91)a
0.83 (0.52-1.30)a
0.01/0.06b
0.41/1.00b
0.05
0.18
-0.28
0.59
0.94 (0.62-1.41)a
1.20 (0.65-2.22)a
0.77/1.00
0.54/1.00b
0.35
0.84
-1.87
2.58
0.70 (0.48-1.01)a
0.42 (0.22-0.81)a
0.06/0.36b
0.009/0.05b AT
TT
Allele Frequency
A - - 0.85 (0.68-1.06)c 0.15/0.90b
- - 0.95(0.72-1.26)c 0.28/1.00b
- - 0.72 (0.55-0.94)c 0.01/0.06b
T - - - - - -
a Age- and gender-adjusted OR and (95%CI) from multivariate logistic regression analysis; pb Bonferroni-corrected p values; c OR and (95%CI)
from univariate logistic regression analysis; Est., estimates

88
patients as compared to the controls (p=0.01; OR 0.72 [95% CI 0.55-0.94]) (Table 3.3),
however this association did not remain significant when Bonferroni correction was
applied to the data (p=0.06). Logistic regression analysis was conducted adjusting for age
and gender, which showed that the homozygous TT genotype of the studied BIRC6
polymorphism is protective in the case of PEXG (p=0.009), which remained significant
even after Bonferroni correction was applied (p=0.05).
3.5.1.2 Screening OPTN and MYOC Polymorphisms in Glaucoma Cohort
The genotype and allele frequencies of the SNP rs11258194 in OPTN were not
significantly associated with increased risk of POAG after correction of p values for
multiple testing, (p=0.07, OR=2.85 [95% CI=1.15-7.06]; p=0.06, OR=2.68 [95% CI=1.07-
7.12]; Table3.4). The AA genotype was present in low percentage (0% in controls, and 1%
in cases; data not shown) therefore it was merged into the TA genotype for logistic
regression analysis. Similarly, no significant associations were observed for PACG or
PEXG (PACG; p=0.25, OR=2.05 [95% CI=0.05-7.14]; p=0.22, OR=1.96 [95% CI=0.58-
6.68], PEXG; p=0.33, OR=1.76 [95% CI=0.56-5.51]; p=0.17, OR=1.96 [95% CI=0.67-
6.11]; Table3.4). In addition, rs10906308 in OPTN and rs2234926 in MYOC were not
found to be significantly associated with POAG, PACG, or PEXG (Table 3.4). Moreover,
the mean IOP of POAG patients carrying the variant allele rs11258194 (23.6±9.2 mmHg)
was not significantly different from the mean IOP in POAG patients who had the ancestral
allele (25.2±10.1 mmHg; p>0.05). Haplotype analysis of the two SNPs in OPTN was also
conducted, which showed that the haplotype A-G (rs11258194-rs10906308) was
significantly associated with increased risk of POAG (p=0.019, OR=2.96 [95% CI=1.20-
7.31]; Table 3.5).
3.5.1.3 Screening Oxidative Stress and Apoptotic Pathway Gene Polymorphisms in
Glaucoma Cohort
Polymorphisms in three genes (P21, P53, P450) of the apoptotic pathway were selected
for screening in the glaucoma cohorts. In addition, polymorphisms in the oxidative stress
genes NOS3 and HSP70 were screened in these cohorts. Logistic regression analysis
revealed that the P21 polymorphism rs1801270 is not associated with any type of

89
Table 3.4 Logistic regression analysis for rs11258194 and rs10906308 in OPTN and rs2234926 in MYOC in Pakistani glaucoma
cohorts and controls
Genotype
rs11258194
Estimate
POAG
Z
value OR (95%CI)
p value/
*p-value
Estimate
PACG
Z
value OR (95%CI)
p value/
*p-value
Estimate
PEXG
Z
value OR (95%CI)
p value/
*p-value
TT -- -- 2.85 (1.15-7.06)a 0.02/0.07
-- -- 2.05(0.05-7.14)a 0.25/0.60
-- -- 1.76 (0.56-
5.51)a 0.33/0.72
TA+AA 1.05 2.27 0.71 1.13 0.56 0.97
Allele Frequency
T -- -- 2.68(1.07-7.12)b 0.02/0.06
-- -- 1.96(0.58-6.68)b 0.22/0.66
-- -- 1.96(0.67-
6.11)b 0.17/0.51
A -- -- -- -- -- --
Genotype rs10906308
GG -- --
0.96(0.35-2.62)a
1.16(0.68-1.98)a
0.45/0.92
0.92/0.99
-- --
0.99(0.58-1.68)a
1.04(0.41-2.66)a
0.98/1.00
0.91/0.99
-- --
0.87(0.25-2.99)a
0.99(0.51-1.93)a
0.98/1.00
0.78/0.99
GA 0.15 0.73 -0.003 -0.01 -0.006 -0.02
AA -0.03 -0.08 0.04 0.10 -0.13 -0.27
Allele Frequency
G -- -- 1.10(0.86-1.63)b 0.54/1.00
-- -- 1.10(0.75-1.61)b 0.92/1.00
-- -- 1.00(0.68-
1.47)b 0.71/1.00
A -- -- -- -- -- --
Genotype rs2234926
GG -- --
0.91(0.60-1.38)a
0.75(0.36-1.55)a
0.69/0.99
0.44/0.91
-- --
0.74(0.43-1.26)a
0.88(0.37-2.12)a
0.27/0.72
0.79/0.99
-- --
0.71(0.35-1.43)a
1.23(0.42-3.54)a
0.22/0.64
0.61/0.98
GA -0.08 -0.39 -0.29 -1.09 -0.33 -1.21
AA -0.28 -0.76 -0.11 -0.26 0.20 0.49
Allele Frequency
G -- -- 0.87(0.60-1.26)b 0.49/1.00
-- -- 0.87(0.60-1.26)b 0.47/1.00
-- -- 1.00(0.69-
1.45)b 1.00/1.00
C -- -- -- -- -- --
aAge- and gender-adjusted OR and (95% CI) from multivariate logistic regression analysis, bOR and (95%CI) from univariate logistic regression
analysis, *p Bonferroni corrected p-values,

90
Table 3.5 Haplotype analysis of OPTN SNPs rs11258194 and rs10906308 in Pakistani
POAG cohorts
rs11258194 rs10906308 Freq OR (95%CI) P-value
1 T G 0.6733 1.00 ---
2 T A 0.2789 1.10 (0.80-1.51) 0.55
3 A G 0.0398 2.96 (1.20-7.31) 0.019
Global haplotype association p-value:0.0082

91
glaucoma. The P450 polymorphism c.-2805T>C was found to possibly have a protective role
in patients with PEXG (estimate=-0.81, z value=-3.68, OR=0.44, [95% CI=0.25-0.77], p=8.8e-
04) in the presence of the heterozygous genotype. However, the P450 c.-2805T>C
polymorphism was not found to be associated with POAG or PACG (Table 3.6).
The P53 polymorphism rs1042522 was also not found to be associated with any type of
glaucoma (Table 3.6). When univariate logistic regression analysis was applied to the allele
frequencies (Table 3.7), it was seen that the minor allele ‘C’ of this polymorphism was not
associated with either POAG, PACG or PEXG (POAG: OR=1.01, [95% CI=0.83-1.23],
p=1.00), (PACG: OR=1.25 [95% CI=1.00-1.58], p=0.2), (PEXG: OR=1.26 [95% CI=1.02-
1.57], p=0.15) (Table 3.7).
The HSP70 rs1043618 polymorphism was found to be significantly associated with POAG,
both for the heterozygous genotype (GC) (estimate=0.98, z value= 6.19, OR=2.68 [95%
CI=1.79-4.01], p=2.22e-09) as well as for the homozygous variant genotype (CC)
(estimate=0.60, z value= 3.06, OR=1.83 [95% CI=1.11-3.04], p=0.009) (Table 3.6). It was also
found to be significantly associated with PACG, both in heterozygous (GC) form
(estimate=0.65, z value= 2.87, OR=1.91 [95% CI=1.08-3.39], p=0.01) as well as in
homozygous (CC) form (estimate=0.65, z value= 3.41, OR=1.91 [95% CI=1.18-3.10],
p=0.002). In PEXG only the homozygous variant genotype (CC) of the polymorphism was
significantly associated with the disease (estimate=1.05, z value= 0.19, OR=2.87 [95%
CI=1.75-4.71], p=2.5e-07). Univariate logistic regression analysis showed that the risk allele C
of the HSP70 rs1043618 polymorphism is significantly associated with all three types of
glaucoma; POAG (OR=1.69 [95% CI=1.37-2.09], p=<0.001), PACG (OR=1.60 [95%
CI=1.25-2.05], p=<0.001), and PEXG (OR=2.02 [95% CI=1.61-2.54], p=<0.001) (Table 3.7).
The heterozygous genotype of in 27bp intron 4 VNTR polymorphism in NOS3 was found to
be significantly associated with POAG and PEXG (estimate=0.55, z value= 3.06, OR=1.74,
[95% CI=1.10-2.75], p=0.01) and (estimate=0.51, z value= 2.38, OR=1.68, [95% CI=1.01-
2.74], p=0.04), respectively. However, PACG was found to be significantly associated with
both heterozygous (estimate=0.73, z value= 3.5, OR=2.09, [95% CI=1.23-3.55], p=0.001) as
well as homozygous genotypes (estimate=0.87, z value= 2.46, OR=2.38, [95% CI=1.00-

92
Table 3.6 Logistic regression analysis of genotype frequency distribution of P21 (rs1801270), P450 (c.-2805T>C), P53 (rs1042522),
HSP70 (rs1043618) and NOS3 (27bp intron 4) polymorphisms in Pakistani glaucoma cohorts and controls
Categories POAG
Estimate
Z
value
OR (95%CI) p value/
*p-value
PACG
Estimat
e
Z
Value
OR (95%CI) p value/
*p-value
PEXG
Estimat
e
Z
value
OR (95%CI) p value/
*p-value
P21 (rs1801270) polymorphism
CC -- -- --
0.76 (0.26-2.23)/0.02/0.95
1.55 (0.93-2.57)/0.53/0.12
-- -- --
1.10 (0.58-2.06)/0.68/0.99
0.11 (0.007-1.59)0.03/0.15
-- -- --
0.98 (0.62-1.566)/0.95
1.08 (0.47-2.50)/0.84
CA -0.26 -0.62 0.09 0.40 -0.01 -0.05
AA 0.44 2.18 -2.1 -2.07 0.08 0.19
P450 (rs2567206) polymorphism
CC -- -- --
0.61(0.36-1.03)/0.01/0.07
0.80 (0.47-1.36)/0.031/0.74
-- -- --
0.73 (0.39-1.37)/0.21/0.59
1.03 (0.54-1.94)/0.89/0.99
-- -- --
0.44 (0.25-0.77)/0.0002/8.8 e-
04
0.63 (0.36-1.11)/0.04/0.15
CT -0.49 -2.35 -0.31 -1.25 -0.81 -3.68
TT -0.21 -1.03 0.03 0.12 -0.45 -2.04
P53 (rs1042522) polymorphism
GG -- -- --
1.29 (0.83-1.99)/0.13/0.43
1.05 (0.64-1.70)/0.78/0.99
-- -- --
1.2 (0.74-2.15)/0.26/0.69
1.4 (0.85-2.63)/0.07/0.25
-- -- --
1.23 (0.75-2.01)/0.27/0.71
1.51 (0.89-2.55)/0.04/0.17
GC 0.25 1.50 0.23 1.11 0.21 1.09
CC 0.05 0.26 0.40 1.80 0.41 1.99
HSP70 (rs1043618) polymorphism
GG -- -- --
2.68 (1.79-4.01)/0.000/2.22 e-09
1.83 (1.11-3.04)/0.002/0.009
-- -- --
1.91 (1.08-3.39)/0.0006/0.01
1.91 (1.18-3.10)/0.004/0.002
-- -- --
1.04 (0.64-1.68)/0.81/0.99
2.87 (1.75-4.71)0.000/2.5 e-07
GC 0.98 6.19 0.65 2.87 0.04 0.23
CC 0.60 3.06 0.65 3.41 1.05 0.19
NOS3 (27 bp intron 4 VNTR polymorphism)
Bb -- -- --
1.74 (1.10-2.75)/0.002/0.01
1.34 (0.57-3.13)/0.37/0.86
-- -- --
2.09 (1.23-3.55)/0.0004/0.001
2.38 (1.00-5.82)/0.01/0.05
-- -- --
1.68 (1.01-2.7)/0.009/0.04
1.56 (0.64-3.78)/0.20/0.61
Ba 0.55 3.06 0.73 3.5 0.51 2.38
Aa 0.29 0.88 0.87 2.46 0.44 1.27
*p p-values corrected by simultaneous inference.

93
Table 3.7 Allele frequency distribution of P21 (rs1801270), P450 (c.-2805T>C), P53 (rs1042522), HSP70 (+190G>C), and NOS3
(27bp intron 4) polymorphisms in Pakistani glaucoma cohorts and controls
P21
(rs1801270)
Controls
N=350
POAG
N=518
OR (95%CI) p value/
*p-value
PACG
N=274
OR (95%CI) p value/
*p-value
PEXG
N=348
OR (95%CI) p value/
*p-value
C 636 (91%) 922 (89%) 1.23 (0.88-1.72)
0.20/1.00 510 (93%)
0.74 (0.48-1.15)
0.15/0.75 631 (91%)
1.02 (0.70-1.49)
0.89/1.00
A 64 (9%) 114 (11%) 38 (7%) 65 (9%)
P450 (rs2567206)
C 440 (63%) 643 (62%) 1.03 (0.84-1.27)
0.73/1.00
351 (64%) 0.95 (0.75-1.21)
0.66/1.00
414 (60%) 1.15 (0.92-1.44)
0.19/0.95 T 260 (37%) 393 (38%) 197 (36%) 282 (40%)
P53 (rs1042522 )
G 342 (49%) 503 (49%) 1.01 (0.83-1.23)
0.90/1.00
236 (43%) 1.25 (1.00-1.58)
0.04/0.2
300 (43%) 1.26 (1.02-1.57)
0.03/0.15 C 358 (51%) 533 (51%) 312 (57%) 396 (57%)
HSP70 (rs1043618)
G 500 (71%) 618 (60%) 1.69 (1.37-2.09)
<0.001/<0.001
334 (61%) 1.60 (1.25-2.05)
<0.001/<0.001
385 (55%) 2.02 (1.61-2.54)
<0.001/<0.001 C 200 (29%) 418 (40%) 214 (39%) 311 (45%)
NOS3 (27bp intron 4)
B 616 (88%) 861 (83%) 1.49 (1.12-1.99)
0.005/0.02
432 (79%) 1.97 (1.43-2.71)
<0.001/<0.001
575 (83%) 1.54 (1.13-2.11)
0.004/0.02 A 84 (12%) 175 (17%) 116 (21%) 121 (17%)
*p Bonferroni corrected p-values.

94
5.82], p=0.05). The risk allele of the NOS3 gene polymorphism was also significantly
associated with POAG (OR=1.49, [95% CI=1.12-1.99], p=0.005), PACG cohort
(OR=1.97, [95% CI=1.43-2.71], p=<0.001), as well as the PEXG cohort (OR=1.54, [95%
CI=1.13-2.11], p=0.004) (Table 3.7).
3.5.1.4 Screening PLEKHA7, COL11A1, and PCMTD1 polymorphisms in the
PACG Cohort
PACG-associated SNPs rs11024102 in PLEKHA7, rs3753841 in COL11A1 and rs1015213
in PCMTD1 were screened in 200 PACG patients and 200 age- and gender-matched
unaffected controls. The genotype and allele frequencies of the SNP rs3753841 in
COL11A1 were significantly associated with PACG (homozygous derived genotype;
p=0.05, OR=0.44 [95% CI=0.19-1.00]; derived allele; p<0.001, OR=0.56 [95% CI=0.41-
0.75]; Table3.8), respectively, suggesting a protective role. As opposed to this, no
significant association was observed in the PACG cohort with SNP rs1015213 in
PCMTD1, where the minor genotype (TT) was present at a low percentage, and therefore
it was merged with the CT genotype for logistic regression analysis [genotype; (p=0.15,
OR=0.59 [95% CI=0.31-1.1]; allele frequency; p=1.00, OR=1.00 [95% CI=0.7-1.45];
Table3.8). Moreover, genotype and allele frequencies of the rs11024102 polymorphism in
PLEKHA7 were not found to be significantly associated with PACG (CT: p=0.89,
OR=0.79 [95% CI=0.36-1.7]; CC: p=0.89, OR=0.74 [95% CI=0.33-1.6]; allele frequency;
p=0.19, OR=0.82 [95% CI=0.61-1.1], Table 3.8).
3.6 Results of AMD Families
Two families with AMD were recruited in the current study. Family AMD 1 was sampled
from the federal capital of Pakistan with three affected individuals, but at the time of
sampling only two affected members were alive and hence sampled (Fig. 3.15 A). Family
AMD 2 (Fig. 3.15 B) was a small family consisting of two affected members belonging to
DG Khan in Pakistan. The probands of both families had wet AMD and were treated with
Avastin injections to control neovascularisation. As there were only two affected
individuals from each family available, only analysis of known genes was conducted for
the families. All exons of the CFH gene were screened in the probands of both families,

95
Table 3.8 Logistic regression analysis of genotype and allele frequency distribution of COL11A1 (rs3753841), PCMTD1 (rs1015213),
and PLEKHA7 (rs11024102) polymorphisms in Pakistani PACG cohort and controls
Genotype
COL11A1 (rs3753841) OR (95% CI)
p value/
*p-value
PCMTD 1
(rs1015213) OR (95%
CI)
p value/
*p-value
PLEKHA7
(rs11024102) OR (95% CI) p value/
*p-value Est. Z value Est. Z value Est. Z value
Ancestral allele
genotype -- --
0.65 (0.30- 1.4)
0.44 (0.19-1.0)
0.16/0.49
0.01/0.05
-- --
0.59 (0.31- 1.1)
0.03/0.15
-- --
0.79 (0.36- 1.7)
0.74 (0.33- 1.6)
0.44/ 0.89
0.36/0.82
Heterozygous -0.42 -1.38 0.51** -2.07** -0.23 -0.75
Derived allele
Genotype -0.80 -2.48 -0.29 -0.90
Allele
Frequency Con. PACG Con.
Patient
s Con. Patients
Ancestral allele 126 (32%) 180 (45%)
0.56 (0.41-0.75) <0.001
<0.001
318
(80%)
317
(79%) 1.0 (0.7-
1.45) 1.00/1.00
152
(38%)
171
(43%) 0.82 (0.61-1.1) 0.19/0.57
Derived allele 274 (69%) 220 (55%) 82
(20%)
83
(21%)
248
(62%)
229
(57%)
*p values of genotype frequency corrected by simultaneous inference and p values of allele frequency corrected by Bonferroni method
** Multivariate logistic regression done by merging Heterozygous CT and Homozygous TT genotypes together, Est.; Estimate.

96
Figure 3.15 Pedigrees of non-consanguineous Pakistani families with AMD. A) Segregation of variant c.1204C>T; p.His402Tyr in CFH
is shown in family AMD 1. Derived allele is indicated with an M and the ancestral allele with a ‘+’. B) Segregation of variant
c.2548G>A; p.Glu850Lys in CFH is shown in family AMD 2. The variant allele is indicated with an M2, and the ancestral allele with
a ‘+’.
AMD 2 (CFH: c.2548G>A) AMD 1 (CFH: c.1204C>T)

97
which identified non-synonymous SNPs rs800292 in exon 2, rs1061170 in exon 9 and
rs368670743 in exon 14. Among these SNPs rs1061170 was previously shown to be
associated with AMD and thus its segregation was checked in the respective family
(Fig.3.15). Another variant, c.2548G>A (p.Glu850Lys), was found in the proband of
family AMD 2, which upon segregation analysis showed no linkage with the disease (Fig.3.
15 B).
3.7 Case-Control Studies in AMD
Patients and controls included in the current study were age- and gender-matched. The
mean age (± standard deviation) of the controls was 64.6±10.92 years and of AMD cases
65.9±10.92 years. 300 healthy subjects (52% males and 48% females) and 300 patients
with AMD (51% males and 49% females) were enrolled in the case-control association
studies. The AMD patients were further bifurcated into two categories i.e. wet AMD and
dry AMD. Moreover, the individuals who had stopped smoking at least 3 years ago were
categorised as former smokers and those individuals who had been smoking for the past 5
years were categorized as current smokers. Multivariate logistic regression analysis was
applied to the data keeping age and gender as covariates. The p-values were corrected by
simultaneous inference (test of hypothesis) for multiple testing. Univariate logistic
regression analysis was applied to the allele frequencies to determine the effect of the
variant allele on the disease. The data analysis showed that the current smokers were at a
higher risk of developing AMD as compared to the non-smokers [OR=2.42(95%CI=2.42-
5.01) p=0.004]. Moreover, the former smokers were at higher risk of development of the
disease as compared to the non-smokers [OR=5.34 (95%CI=2.55-11.17) p<0.0001]. The
former smokers with dry and wet AMD were more at risk of development of advanced
stages of AMD [OR=5.42 (95%CI=1.95-15.01) p<0.0001] as compared to the current
smokers with dry or wet AMD [OR=2.76 (95%CI=1.16-6.57) p=0.008].

98
3.7.1 Screening Polymorphisms in Known AMD Gene
3.7.1.1 CFH and ARMS2
Multivariate logistic regression analysis showed that rs1061170 in CFH was not associated
with AMD overall or with wet AMD. The ‘CC’ as well as the ‘TC’ genotype of the
polymorphism rs1061170 was not associated with the risk of having AMD or any subtype
of AMD (Table 3.9) (AMD overall; TC: p=0.77, OR=0.94 [95% CI=0.64-1.38], CC:
p=0.02, OR=2.14 [95% CI=1.08-4.25]; Wet AMD (TC: p=0.53, OR=0.85 [95% CI=0.52-
1.39], CC: p=0.03, OR=2.37 [95% CI=1.06-5.32]; Dry AMD (TC: p=0.80, OR=1.05 [95%
CI=0.68-1.62], CC: p=0.06, OR=2.05 [95% CI=0.96-4.37; Table 3.9]).
Univariate logistic regression analysis showed that the risk allele C was also not associated
with the disease in the combined data (p=0.13, OR=1.24 [95% CI=0.93-1.64]) nor with the
subtypes of the disease (Wet AMD; p=0.22, OR=1.23 [95% CI=0.87-1.76], Dry AMD;
p=0.15, OR=1.24 [95% CI=0.90-1.71]; Table 3.9).
Multivariate logistic regression analysis showed that the derived genotype ‘TT’ of
rs10490924 in ARMS2 was significantly associated with AMD in the overall data as well
as with wet AMD. The ‘GT’ genotype of the polymorphism rs10490924 was not associated
with the risk of developing AMD (AMD overall; GT: p=0.92, OR=1.15 [95% CI=0.69-
1.91], TT: p=0.003, OR=2.61 [95% CI=1.28-5.32] nor with wet AMD (GT: p=0.94,
OR=1.19 [95% CI=0.61-2.32], TT: p=0.0006, OR=3.57 [95% CI=1.52-8.37]). None of the
genotypes were associated with dry AMD (GT: p=0.97, OR=1.12 [95% CI=0.63-1.99],
TT: p=0.06, OR=2.14 [95% CI=0.97-4.37]). Univariate logistic regression analysis showed
that the risk allele T was significantly associated with the disease in the overall data
(p<0.001, OR=1.61 [95% CI=1.22-2.11]) as well as with the subtypes of the disease (wet
AMD; p<0.001, OR=1.89 [95% CI=1.34-2.65], dry AMD; p=0.04, OR=1.43 [95%
CI=1.05-1.95]; Table 3.9).
3.7.1.2 C2/CFB
An AMD-associated SNP (rs429608) near C2 and CFB genes on chromosome 6p21.3 was
screened in AMD cases and controls (Table 3.10). Multivariate logistic regression analysis
adjusted for age, gender and smoking status showed that the genotype and allele frequency

99
Table 3.9 Logistic regression analysis of genotype and allele frequency distribution of polymorphisms rs1061170 in CFH and
rs10490924 in ARMS2 in AMD patients and controls
Genotype
CFH
(rs1061170)
Overall OR (95%CI) p/*p
value Wet AMD OR (95%CI)
p/*p
value
Dry AMD OR (95%CI) p/*p
value
Est. Z value Est. Z
value Est. Z value
TT -- -- -
0.94 (0.64-1.38)
2.14 (1.08-4.25)
-
0.77/0.99
0.02/0.11
- - -
0.85 (0.52-1.39)
2.37 (1.06-5.32)
-
0.53/0.95
0.03/0.13
- - -
1.05 (0.68-1.62)
2.05 (0.96-4.37)
-
**0.80
**0.06
TC -0.05 -0.28 -0.15 -0.62 0.05 0.24
CC 0.76 2.18 0.86 2.10 0.71 1.85
Allele
Frequency Controls Overall
Allele
Frequency
Allele
Frequency
T 281 (70%) 393 (66%) 1.24 (0.93-1.64) 0.13/0.26
164 (66%) 1.23 (0.87-1.76) 0.22/0.4
229 (65%) 1.24 (0.90-1.71)
**0.15/0.3 C 119 (30%) 207 (34%) 86 (34%) 121 (35%)
ARMS2 (rs10490924)
GG - -
-
1.15 (0.69-1.91)
2.61 (1.28-5.32)
-
0.47/0.92
0.0006/
0.003
- -
-
1.19 (0.61-2.32)
3.57 (1.52-8.37)
-
0.50/0.94
0.0001/
0.0006
- -
-
1.12 (0.63-1.99)
2.14 (0.97-4.37)
-
0.60/0.97
0.01/0.06
GT 0.14 0.71 0.17 0.66 0.11 0.51
TT 0.96 3.39 1.27 3.76 0.76 2.42
Allele
Frequency Controls Overall
Allele
Frequency
Allele
Frequency
G 273 (68%) 343 (57%) 1.61 (1.22-2.11)
<0.001/<
0.001
133 (53%) 1.89 (1.34-2.65)
<0.001/<0
.001
210 (60%) 1.43 (1.05-1.95)
0.02/0.0
4 T 127 (32%) 257 (43%) 117 (47%) 140 (40%)
*p values corrected by simultaneous inference, **p value not corrected

100
Table 3.10 Logistic regression analysis of genotype and allele frequency distribution of rs429608 polymorphism near C2/CFB in AMD
patients and controls
Genotype
C2/CFB
(rs429608)
Overall
OR (95% CI) P
value
Wet AMD
OR (95% CI) P
value
Dry AMD
OR (95% CI) P
value Est. Z value Est. Z
value Est.
Z
value
GG
GA -0.03* -0.15* 0.96 (0.63- 1.47) 0.8*
-0.44 -1.50 0.63 (0.35- 1.14) 0.13 0.23 0.93 1.26 (0.77- 2.06) 0.35
AA -0.22 -0.37 0.79 (0.23- 2.65) 0.70 -0.40 -0.61 0.66 (0.18- 2.43) 0.54
Allele
Frequency Controls AMD
Allele
Frequency
Allele
Frequency
A 310 (79%) 400 (79%) 0.97 (0.69-1.36) 0.89
167 (81%) 0.86 (0.55-1.34) 0.52
233 (78%) 0.98 (0.66-1.44) 1.00
G 84 (21%) 106 (21%) 39 (19%) 62 (22%)
Est.; Estimate,

101
of rs4420638 was not associated with AMD. The homozygous genotype AA was present
in a small number of cases. Therefore, the heterozygous and homozygous genotype groups
were merged together in the combined AMD data to conduct multivariate logistic
regression analysis (AMD overall; p=0.8, OR=0.96 [95% CI=0.63-1.47], wet AMD; GA:
p=0.13, OR=0.63 [95% CI=0.35-1.14], AA: p=0.70, OR=0.79 [95% CI=0.23-2.65]; Table
3.10, dry AMD; GA: p=0.35, OR=1.26 [95% CI=0.77-2.06], AA: p=0.54, OR=0.66 [95%
CI=0.18-2.43]; Table 3.10). Univariate logistic regression analysis showed that the risk
allele A was also not associated with the disease in the combined data (p=0.89, OR=0.97
[95% CI=0.69-1.36]) nor with the subtypes of the disease (wet AMD; p=0.52, OR=0.86
[95% CI=0.55-1.34], dry AMD; p=1.00, OR=0.98 [95% CI=0.66-1.44]; Table 3.10).
3.7.1.3 C3
An AMD-associated SNP (rs2230199) in C3 was screened in AMD cases and controls.
Multivariate logistic regression analysis adjusted for age, gender and smoking status
showed that the genotype and allele frequencies of the polymorphism rs2230199 were not
associated with AMD (AMD overall; GC: p=0.17, OR=0.31 [95% CI=0.05-1.70], CC:
p=0.31, OR=0.42 [95% CI=0.08-2.24], wet AMD; GC p=0.32, OR=0.35 [95% CI=0.04-
2.78], CC: p=0.28, OR=0.33 [95% CI=0.04-2.52], dry AMD; GA: p=0.13, OR=0.24 [95%
CI=0.03-1.53], AA: p=0.36, OR=0.44 [95% CI=0.07-2.61]; Table 3.11). Univariate
logistic regression analysis showed that the risk allele C was also not associated with the
disease in the overall data (p=0.62, OR=1.10 [95% CI=0.7-1.64]) nor with the subtypes of
the disease (wet AMD; p=0.5, OR=0.86 [95% CI=0.53-1.3], dry AMD; p=0.18, OR=1.36
[95% CI=0.84-2.19]; Table 3.11).
3.7.2 Screening Polymorphisms in Lipid Metabolism Associated Gene
3.7.2.1 APOE
A previously reported AMD-associated SNP (rs4420638) 14 kb upstream of the APOE
gene was screened in AMD cases and controls. Multivariate logistic regression analysis
adjusted for age-, gender and smoking status showed that the genotype and allele
frequencies of polymorphism rs4420638 were not associated with AMD (Table 3.12). The

102
Table 3.11 Logistic regression analysis of genotype and allele frequencies of the rs2230199 polymorphism near C3 in AMD patients
and controls
Genotype
C3
(rs2230199)
Overall
OR (95% CI) P
value
Wet AMD
OR (95% CI) P
value
Dry AMD
OR (95% CI) P
value Estimate Z value Est. Z
value Est.
Z
value
GG
GC -1.16 -1.34 0.31 (0.05- 1.70) 0.17 -1.04 -0.99 0.35 (0.04- 2.78) 0.32 -1.41 -1.50 0.24 (0.03- 1.53) 0.13
CC -0.84 -1.0 0.42 (0.08- 2.24) 0.31 -1.10 -1.06 0.33 (0.04- 2.52) 0.28 -0.81 -0.90 0.44 (0.07- 2.61) 0.36
Allele
Frequency Controls Overall
Allele
Frequency
Allele
Frequency
G 56 (14%) 69 (13%) 1.10 (0.7-1.64) 0.62
35 (16%) 0.86 (0.53-1.3) 0.5
34 (11%) 1.36 (0.84-2.19) 0.18
C 344 (%) 469 (87%) 185 (84%) 284 (89%)
Est.; Estimate, Con.; Controls

103
Table 3.12 Logistic regression analysis of genotype and allele frequencies of the rs4420638 polymorphism near APOE in AMD
patients and controls
Genotype
APOE
(rs4420638)
Overall
OR (95% CI) p
value
Wet AMD
OR (95% CI) p
value
Dry AMD
OR (95% CI) p value Est. Z value Est.
Z
value Est.
Z
value
GG 1.34 (0.79- 2.28)
0.27
0.99 (0.50- 1.99) 0.99
1.55 (0.86- 2.80) 0.14 GA+AA 0.29 1.08 -0.001 -0.003 0.44 1.46
Allele
Frequency Controls AMD
Allele
Frequency
Allele
Frequency
G 373 (91%) 454 (90%) 1.15 (0.72-
1.84) 0.57
185 (92%) 0.92 (0.48-1.75) 0.88
269 (88%) 1.31 (0.78-2.19) 0.31
A 37 (9%) 52 (10%) 17 (8%) 35 (12%)
, Est.; Estimate,

104
homozygous genotype AA was not present in the patients and only one control individual
was homozygous for the risk allele. Therefore, the heterozygous and homozygous genotype
groups were merged together to conduct the multivariate logistic regression analysis (AMD
overall; p=0.27, OR=1.34 [95% CI=0.79- 2.28], wet AMD; p=0.99, OR=0.99 [95%
CI=0.50-1.99], dry AMD; p=0.14, OR=1.55 [95% CI=0.86-2.80]; Table 3.12). Univariate
logistic regression analysis showed that the risk allele A was also not associated with the
disease in the combined data (p=0.57, OR=1.15 [95% CI=0.72-1.84]) nor with the subtypes
of the disease (wet AMD; p=0.88, OR=0.92 [95% CI=0.48-1.75], dry AMD; p=0.31,
OR=1.31 [95% CI=0.78-2.19]; Table 3.12).
3.7.3 Screening Polymorphisms in Immune System Pathway Genes
3.7.3.1 CX3CR1
Two SNPs, rs3732378 (c.839C>T) and rs3732379 (c.745G>A), in CX3CR1 were
genotyped in the AMD cohort and controls. Multivariate logistic regression analysis
showed that the genotype distribution of rs3732378 was not associated with AMD (AG;
p=0.5, OR=2.04 [95% CI=0.57-7.31]; GG; p=0.6, OR=1.77 [95% CI=0.55-5.69]; Table
3.13), nor with any of the sub-types of AMD (Table 3.13). Univariate logistic regression
analysis showed that the risk allele ‘G’ was also not associated with AMD (p=0.28,
OR=0.76 [95% CI=0.52-1.10]; Table3.13), nor with wet AMD (p=0.60, OR=0.76 [95%
CI=0.46-1.24]; Table 3.13), but was significantly associated with dry AMD (p=0.00,
OR=0.30 [95% CI=0.16-0.55]; Table 3.13) suggesting a protective role in dry AMD.
Multivariate logistic regression analysis showed that the heterozygous genotype ‘CT’ of
rs3732379 in CX3CR1 was significantly associated with AMD (CT; p=0.005, OR=0.26
[95% CI=0.08-0.77], TT; p=0.9, OR=1.59 [95% CI=0.37-6.69]; Table 3.13), and also with
dry AMD (CT; p=0.0008, OR=0.19 [95% CI=0.06-0.60], TT; p=0.9,OR=1.41 [95%
CI=0.30-6.48]; Table 3.13) but not with wet AMD (CT; p=0.5, OR=0.41 [95% CI=0.09-
1.85], TT; p=0.7, OR=2.25 [95% CI=0.35-14.1]; Table 3.13). Univariate logistic
regression analysis showed that the risk allele ‘T’ was not associated with AMD overall
(p=0.64, OR=1.12 [95% CI=0.88-1.44]; Table 3.13), nor with wet AMD (p=0.36, OR=1.23

105
Table 3.13 Logistic regression analysis of genotype and allele frequencies of rs3732378 and rs3732379 polymorphisms in CX3CR1 in
AMD patients and controls
CX3CR1
(rs3732378)
Overall
OR (95%CI) p value/
*p-value
Wet AMD
OR (95%CI) p value/
*p-value
Dry AMD
OR (95%CI) p value/
*p-value Est. Z value Est. Z
value Est.
Z
valu
e
AA -- -- -- -- -- --
AG 0.71 1.47 2.04 (0.57- 7.31) 0.13/0.5 0.30 0.50 1.35 (0.27- 6.57) 0.61/0.9 1.08 1.71 2.95 (0.56- 15.6) 0.08/0.3
GG 0.57 1.30 1.77 (0.55- 5.69) 0.19/0.6 0.28 0.53 1.33 (0.32- 5.54) 0.59/0.9 0.79 1.33 2.21 (0.46- 10.4) 0.18/0.6
Allele
Frequency Con. AMD
Allele
Frequency Allele Frequency
A 429 (86%) 533 (89%) 0.76 (0.52-1.10) 0.14/0.28
222 (89%) 0.76 (0.46-1.24) 0.30/0.60
314 (95%) 0.30 (0.16-0.55)
<0.0001
<0.001 G 71 (14%) 67 (11%) 28 (11%) 16 (5%)
CX3CR1 (rs3732379)
CC -- -- -- --
CT -1.34 -3.28 0.26 (0.08- 0.77) 0.001/
0.005 -0.89 -1.56 0.41 (0.09- 1.85) 0.11/0.5 -1.64
-3.80
0.19 (0.06- 0.60) 0.0001/
0.0008
TT 0.46 0.85 1.59 (0.37- 6.69) 0.39/0.9 0.81 1.17 2.25 (0.35- 14.1) 0.24/0.7 0.34 0.60 1.41 (0.30- 6.48) 0.54/0.9
Allele
Frequency Con. AMD
Allele
Frequency Allele Frequency
C 250 (50%) 282 (47%) 1.12 (0.88-1.44) 0.32/0.64
112 (45%) 1.23 (0.89-1.69) 0.18/0.36
170 (48%) 1.05 (0.79-1.40) 0.72/1.00
T 250 (50%) 318 (53%) 138 (55) 180 (52%)
*p values corrected by simultaneous inference,

106
[95% CI=0.89-1.69], and neither with dry AMD (p=1.00, OR=1.05 [95% CI=0.79-1.40];
Table 3.13).
3.7.4 Screening Vascular System Related Gene Polymorphisms
3.7.4.1 VEGF
Three promoter region polymorphisms of VEGF were screened in 150 AMD samples (50%
wet AMD and 50% dry AMD) and 150 age-matched controls. Multivariate logistic
regression analysis was conducted and the results showed that rs8333061 was not
associated with AMD overall, nor with wet AMD or dry AMD (AMD overall; CT: p=0.80,
OR=1.05 [95% CI=0.68-1.62], TT: p=0.44, OR=2.05 [95% CI=0.96-4.37], wet AMD; CT:
p=0.44, OR=1.34 [95% CI=0.62-2.86], TT: p=0.10, OR=1.89 [95% CI=0.86-4.15), Dry
AMD; CT: p=0.68, OR=0.86 [95% CI=0.43-1.72], TT: p=0.65, OR=0.84 [95% CI=0.39-
1.79]; Table 3.14).
In addition, rs13207351 was also not associated with AMD or any subtype of AMD in the
current cohort (AMD overall; AG: p=0.93, OR=0.97 [95% CI=0.53-1.76], GG: p=0.72,
OR=1.12 [95% CI=0.58-2.17], Wet AMD; AG: p=0.28, OR=1.55 [95% CI=0.69-3.48],
GG: p=0.12, OR=1.96 [95% CI=0.82-4.66), Dry AMD; AG: p=0.28, OR=0.68 [95%
CI=0.34-1.36], GG: p=0.32, OR=0.67 [95% CI=0.30-1.48]; Table 3.14).
Also rs1570360 was not associated with AMD or any subtype of AMD in the current cohort
(AMD overall; GA: p=0.20, OR=1.37 [95% CI=0.87-2.25], AA: p=0.45, OR=1.31 [95%
CI= 0.65-2.64], wet AMD; GA: p=0.30, OR=1.35 [95% CI=0.75-2.45], AA: p=0.46,
OR=0.68 [95% CI=0.25-1.86], dry AMD; GA: p=0.23, OR=1.45 [95% CI=0.78-2.70],
AA: p=0.07, OR=2.08 [95% CI=0.93-4.65]; Table 3.14). Univariate logistic regression
analysis showed that the risk allele C of rs8333061, the risk allele G of rs13207351 as well
as risk allele A of rs1570360 were not associated with AMD [(rs8333061; AMD overall;
T: p=0.41, OR=1.59 [95% CI=0.83-1.62], wet AMD: p=0.08, OR=1.42 [95% CI=0.93-
2.16], dry AMD; p=0.84, OR=0.94 [95% CI=0.62-1.43], rs13207351; AMD overall;
p=1.00, OR=1.01 [95% CI=0.72-1.41], wet AMD: p=0.23, OR=1.27 [95% CI=0.84-1.93],
dry AMD; p=0.31, OR=0.80 [95% CI=0.53-1.21]), (rs1570360; AMD overall; p=0.25,
OR=1.23 [95% CI=0.86-1.76], wet AMD: p=1.00, OR=0.98 [95% CI=0.62-1.54]) but the

107
Table 3.14 Logistic regression analysis of genotype and allele frequencies of VEGF polymorphisms in AMD patients and controls
Genotype
VEGF
rs8333061
Overall OR (95%CI) p
value Wet AMD OR (95%CI)
*p
value Dry AMD OR (95%CI)
*P
value
Est. Z value Est. Z
value Est.
Z
value
CC - -
1.05 (0.68- 1.62)
2.05 (0.96- 4.37)
-
0.86
0.44
- - -
1.34 (0.62- 2.86)
1.89 (0.86-4.15)
-
0.44
0.10
- - -
0.86(0.43- 1.72)
0.84(0.39-1.79)
-
0.68
0.65
CT 0.05 0.24 0.29 0.75 -0.14 -0.40
TT 0.71 1.85 0.64 1.60 -0.17 -0.44
Allele
Frequency Controls AMD
Allele
frequency
Allele
frequency
C 142 (47%) 131 (44%) 1.59 (0.83-1.62) 0.41
58 (39%) 1.42 (0.93-2.16) 0.08
73 (49%) 0.94 (0.62-1.43) 0.84
T 158 (53%) 169 (56%) 92 (61%) 77 (51%)
rs13207351
AA - -
0.97 (0.53- 1.76)
1.12 (0.58-2.17)
-
0.93
0.72
- - -
1.55 (0.69-3.48)
1.96 (0.82- 4.66)
-
0.28
0.12
- - -
0.68(0.34- 1.36)
0.67(0.30- 1.48)
-
0.28
0.32
AG -0.02 -0.08 0.43 1.06 -0.38 -1.07
GG 0.11 0.34 0.67 1.52 -0.39 -0.97
Allele
Frequency Controls AMD
Allele
frequency
Allele
frequency
A 140 (47%) 135 (45%) 1.01 (0.72-1.41) 1.00
59 (39%) 1.27 (0.84-1.93) 0.23
76 (51%) 0.80 (0.53-1.21) 0.31
G 169 (53%) 165 (55%) 91 (61%) 74 (49%)
rs1570360
GG - -
1.37 (0.84- 2.25)
1.31 (0.649- 2.64)
-
0.20
0.45
- - -
1.35 (0.75-2.45)
0.68 (0.25- 1.86)
-
0.30
0.46
- - -
1.45(0.78-2.70)
2.08(0.93- 4.65)
-
0.23
0.07
GA 0.32 1.27 0.30 1.01 0.37 1.19
AA 0.27 0.75 -0.37 -0.73 0.73 1.79
Allele
Frequency Controls AMD
Allele
frequency
Allele
frequency
G 209 (70%) 195 (65%) 1.23 (0.86-1.76) 0.25
105 (70%) 0.98 (0.62-1.54) 1.00
90 (60%) 1.53 (0.99-2.35)
0.04/0
.12 A 91 (30%) 105 (35%) 45 (30%) 60 (40%)
*p values corrected by simultaneous inference, Est.; Estimate

108
risk allele ‘A’ of the SNP rs1570360 was found to be associated with dry AMD; p=0.04,
OR=1.53 [95% CI=0.99-2.35]; Table 3.14) but the association did not remain significant
after the p-values were corrected.
3.7.4.2 Intron 4, 27bp VNTR in NOS3
Multivariate logistic regression analysis of the intron 4, 27 bp VNTR in NOS3 showed that
the genotype frequencies were not associated with AMD (ba; p=0.22, OR=1.59 [95%
CI=0.87-2.90], aa; p=0.07, OR=1.91 [95% CI=0.47-7.66]; Table 3.15), nor with wet AMD
(ba; p=0.1, OR=1.80 [95% CI=0.86-3.73], aa; p=0.8, OR=1.88 [95% CI=0.36-9.56]; Table
3.15) or with dry AMD (ba; p=0.7, OR=1.41 [95% CI=0.69-2.87], aa; p=0.9, OR=1.55
[95% CI=0.31-7.66]; Table 3.15). Univariate logistic regression analysis showed that the
risk allele ‘a’ was associated with AMD in the overall cohort (p=0.01, OR=1.57 [95%
CI=1.00-2.28]; Table 3.15), as well as with wet AMD (p=0.008, OR=1.81 [95% CI=1.15-
2.84], but not with dry AMD (p=0.11, OR=1.40 [95% CI=0.91-2.16]; Table 3.15).
3.7.5 Screening Polymorphisms in Genes Implicated in Oxidative Stress
3.7.5.1 MMPs
Two SNPs, rs17576 and rs243866, in MMP9 and MMP2, respectively, were genotyped in
the AMD cohort and controls. Multivariate logistic regression analysis showed that
rs17576 in MMP9 was significantly associated with AMD (AG; p=0.005, OR=8.47 [95%
CI=1.57-45.5]; GG; p=0.05, OR=5.34 [95% CI=0.97-29.25]; Table 3.16)), but not with
any of the sub-types of AMD (Table 3.16). Univariate logistic analysis showed that the risk
allele ‘G’ was not associated with AMD (p=1.00, OR=1.06 [95% CI=0.8 2-1.38]; Table
3.16), nor any subtype of AMD (Wet AMD; p=1.00, OR=0.97 [95% CI=0.68-1.33]; Dry
AMD; p=0.60, OR=1.15 [95% CI=0.85-1.56]; Table3.16).
For the rs243866 SNP in MMP2, multivariate logistic regression analysis showed that the
homozygous risk genotype ‘AA’ was significantly associated with AMD (AA; p=0.01,
OR=4.98 [95% CI=1.25-19.88]; Table 3.16), and also with dry AMD (AA; p=0.01,
OR=5.55 [95% CI=1.22-25.1]; Table 3.16), but not with wet AMD (AA; p=0.06, OR=4.76

109
Table 3.15 Logistic regression analysis of genotype and allele frequencies of the 27-bp VNTR polymorphism in NOS3 in AMD
patients and controls
Genotype
NOS3
Overall
OR (95% CI) *P
value
Wet AMD
OR (95% CI) *P
value
Dry AMD
OR (95% CI) *P
value Est. Z value Est. Z
value Est.
Z
value
Bb -- -- -- -- -- --
Ba 0.46 2.04 1.59 (0.87- 2.90) 0.04/0.
22 0.58 2.13 1.80 (0.86- 3.73)
0.03/
0.1 0.34 0.26 1.41 (0.69- 2.87)
0.19/0
.7
Aa 0.64 1.23 1.91 (0.47- 7.66) 0.21/0.
76 0.63 1.02 1.88 (0.36- 9.56)
0.30/
0.8 0.44 0.73 1.55 (0.31- 7.66)
0.46/0
.9
Allele
Frequency Con AMD
Allele
Frequency
Allele
Frequency
B 446 (89%) 504 (84%) 1.57 (1.0-2.28) 0.01
205(85%) 1.81 (1.15-2.84) 0.008
299 (85%) 1.40 (0.91-2.16) 0.11
A 54 (11%) 96 (16%) 45 (18%) 51 (15%)
*p values corrected by simultaneous inference, Est.; Estimate, Con.; controls

110
Table 3.16 Logistic regression analysis of genotype and allele frequencies of MMP9 (rs17576) and MMP2 (rs243866) polymorphisms
in AMD patients and controls
Genotype
MMP9
(rs17576)
Overall
OR (95%CI) p value/
*p-value
Wet AMD
OR (95%CI) p value/
*p-value
Dry AMD
OR (95%CI) p value/
*p-value Est. Z value Est. Z value Est. Z
value
AA -- -- -- --
AG 2.13 3.33 8.47 (1.57- 45.5) 00008/
0.005 2.55 2.45 12.92 (0.85- 19.6)
0.01/
0.07 1.90 2.46 6.7 (0.88- 50.4)
0.01/
0.07
GG 1.67 2.58 5.34 (0.97-29.25) 0.009/
0.05 1.78 1.69 5.93 (0.37- 92.5)
0.09/
0.3 1.56 2.00 4.78 (0.62- 36.7)
0.04/
0.22
Allele
Frequency Con. AMD Allele Frequency Allele Frequency
A 175 (35%) 201 (66.5%) 1.06 (0.82-1.38) 0.61/1.00
90(36%) 0.97 (0.68-1.33) 0.8/1.00
111(32%) 1.15 (0.85-1.56) 0.33/0.60
G 325 (65%) 399 (33.5%) 160(64%) 239(68%)
MMP2(rs243866)
GG -- -- -- -- -- --
GA -0.01 -0.05 0.98 (0.57-1.69) 0.95/
1.00 -0.22 -0.85 0.79 (0.39-1.61)
0.39/
0.9 0.09 0.39 1.09 (0.58- 2.04) 0.69/0.9
AA 1.60 3.07 4.98 (1.25-19.88) 0.002/
0.01 1.56 2.54 4.76 (0.94-24.1)
0.01/
0.06 1.71 3.00 5.55 (1.22- 25.1) 0.002/0.01
Allele
Frequency Con. AMD Allele Frequency Allele Frequency
G 421 (84%) 469 (78%) 1.48 (1.08-2.05) 0.01/0.02
202 (81%) 1.26 (0.83-1.91) 0.25/0.5
267 (76%) 1.60 (1.12-2.29) 0.008/0.01
A 79 (16%) 131 (22%) 48 (19%) 83 (24%)
*p values of genotype frequency corrected by simultaneous inference and p values of allele frequency corrected by Bonferroni method,
Est.; Estimate, Con,; Controls,

111
[95% CI=0.94-24.1]; Table 3.16). Similarly, univariate logistic regression analysis showed
that the risk allele ‘G’ was associated with AMD (p=0.02, OR=1.48 [95% CI=1.08-2.05];
Table3.9), as well as with dry AMD (p=0.01, OR=1.65 [95% CI=1.15-2.37]), but not with
wet AMD (p=0.5, OR=1.26 [95% CI=0.83-1.91]; Table 3.16).
3.7.5.2 TIMP3
A previously reported AMD-associated SNP (rs5749482) 100 kb upstream of TIMP3 was
screened in AMD cases and controls. The multivariate logistic regression analysis adjusted
for age, gender and smoking status showed that the genotype and allele frequencies of the
polymorphism rs4420638 were not associated with AMD. As the homozygous genotype
AA was present in in only a few cases, the heterozygous and homozygous genotype groups
were added together in the combined AMD multivariate logistic regression analysis (AMD
overall; p=0.60, OR=1.13 [95% CI=0.70-1.81], wet AMD; p=0.73, OR=1.10 [95%
CI=0.60-2.02], dry AMD; p=0.48, OR=1.21 [95% CI=0.70-2.06]; Table 3.17). Univariate
logistic regression analysis showed that the risk allele C was also not associated with the
disease in the overall data (p=0.69, OR=1.08 [95% CI=0.72-1.63]) nor with the subtypes
of the disease (wet AMD; p=0.80, OR=1.06 [95% CI=0.63-1.78], dry AMD; p=0.65,
OR=1.10 [95% CI=0.69-1.74]; Table 3.17).
3.7.5.3 TNF and ILβ
The SNP rs1800629 in TNF and SNP rs16944 in ILβ were genotyped in the AMD cohort
and controls. Multivariate logistic regression analysis showed that there was no genotype
association between the TNF rs1800629 SNP and the AMD cohort nor with any subtype of
AMD (Table 3.18). For rs16944 in ILβ, multivariate logistic regression analysis showed
that the heterozygous genotype ‘CT’ as well as homozygous risk allele ‘TT’ were
significantly associated with AMD (CT; p=0.01, OR=1.87 [95% CI=1.10-3.18]) TT;
p=0.02, OR=2.38 [95% CI=1.06-5.38]; Table 3.18), and also with wet AMD (CT; p=0.05,
OR=2.01 [95% CI=1.0-4.12], TT; p=0.009, OR=3.23 [95% CI=1.21-8.62]; Table 3.18) as
well as with dry AMD but only with the CT genotype (CT; p=0.006, OR=2.17 [95%
CI=1.16-4.06], TT; p=0.15, OR=2.29 [95% CI=0.85-6.21]; Table 3.18). Univariate logistic

112
Table 3.17 Logistic regression analysis of genotype and allele frequencies of the rs5749482 polymorphism near TIMP3 in AMD patients
and controls
Genotype
TIMP3
(rs5749482)
Overall
OR (95% CI) P
value
Wet AMD
OR (95% CI) P
value
Dry AMD
OR (95% CI) P
value Estimate Z value Est. Z
value Est.
Z
value
GG - - 1.13 (0.70- 1.81) 0.60
- - 1.10 (0.60- 2.02) 0.73
- - 1.21 (0.70- 2.06) 0.48
GC+CC 0.124 0.51 0.10 0.33 0.19 0.69
Allele
Frequency Controls Overall
Allele
Frequency
Allele
Frequency
G 340 (87%) 450 (86%) 1.08 (0.72-1.63) 0.69
185 (86%) 1.06 (0.63-1.78) 0.80
265 (86%) 1.10 (0.69-1.74) 0.65
C 50 (13%) 72 (14%) 29 (14%) 43 (14%)
Est.; Estimate, Con.; Controls

113
Table 3.18 Logistic regression analysis of genotype and allele frequencies of rs1800629 in TNF and rs16944 in ILβ in AMD patients
and controls
Genotype
TNF
rs1800629
Overall
OR (95%CI) *p
value
Wet AMD
OR (95%CI) *p
value
Dry AMD
OR (95%CI) *P
value Estimate Z value Est. Z Est. Z
value
GG -- -- -- -- -- --
GA 0.15 0.62 1.16 (0.60- 2.27) 0.5/0.9 0.33 1.08 1.40 (0.61- 3.18) 0.27/0.8 0.08 0.27 1.08 (0.49- 2.38) 0.78/0.9
AA 0.19 0.20 1.21 (0.09- 15.38) 0.8/0.9 1.21 1.13 3.37 (0.19- 57.9) 0.25/0.8 -0.53 -0.41 0.58 (0.01- 17.4) 0.67/0.9
Allele
Frequency Controls AMD
Allele
Frequency
Allele
Frequency
G 461 (92%) 545 (91%) 1.19 (0.76-1.87)
0.44/0.
88
224 (90%) 1.37 (0.78-2.38)
0.27/0.5
4
321 (92%) 1.06 (0.62-1.81) 0.79/1.00
A 39 (8%) 55 (9%) 26 (10%) 29 (8%)
ILβ rs16944
TT -- -- -- -- -- --
TC 0.62 3.14 1.87 (1.10- 3.18) 0.001/0
.01 0.70 2.5 2.01 (1.00- 4.12)
0.009/0.
05 0.77 3.27 2.17 (1.16- 4.06)
0.001/0.00
6
CC 0.87 2.83 2.38 (1.06- 5.38) 0.004/0
.02 1.17 3.16 3.23 (1.21- 8.62)
0.001/0.
009 0.83 2.21 2.29 (0.85- 6.21) 0.02/0.15
Allele
Frequency Controls AMD
Allele
Frequency
Allele
Frequency
T 348 (70%) 371 (62%) 1.41 (1.09-1.83)
0.008/0
.01
148 (59%) 1.57 (1.13-2.19)
0.005/0.
01
223(64%) 1.30 (0.96-1.76) 0.07/0.14
C 152 (30%) 229 (38%) 102 (40%) 127 (36%)
*p values corrected by simultaneous inference,

114
regression analysis showed that the risk allele ‘T’ was associated with [95% CI=1.09-1.83];
Table3.18), and with wet AMD [p=0.01, OR=1.57 [95% CI=1.13-2.19], but not with dry
AMD (p=0.14, OR=1.30 [95% CI=0.96-1.76]; Table 3.18).
3.8 Summary
The Summarised results of the multivariate logistic regression (OR and 95% CI) are
presented in the forest plots (Fig. 3.16; POAG, Fig. 3.17; PACG and Fig. 3.18;
PEXG, Fig. 3.19; wet AMD and Fig. 3.20; dry AMD).

115
Fig 3.16 Forest plot of the SNPs screened for POAG. Diamond shape represents OR, horizontal lines represent 95% CI, HG;
heterozygous genotype, VG; variant allele genotype, AF; Allele frequency, * the p values were significant before correction for
multiple testing. The vertical line at unit 1 represents the central value of OR. All the horizontal lines that cross this line represent non-
significant association of the SNPs. Those left of this central line are protective (OR<1), and those right of the line are risk-conferring
SNPs (OR>1).

116
Fig 3.17 Forest plot of the SNPs screened for POAG. Diamond shape represents OR, horizontal lines represent 95% CI, HG;
heterozygous genotype, VG; variant allele genotype, AF; Allele frequency. The vertical line at unit 1 represents the central value of
OR. All the horizontal lines that cross this line represent non-significant association of the SNPs. Those left of this central line are
protective (OR<1), and those right of the line are risk-conferring SNPs (OR>1).

117
Fig 3.18 Forest plot of the SNPs screened for POAG. Diamond shape represents OR, horizontal lines represent 95% CI, HG;
heterozygous genotype, VG; variant allele genotype, AF; Allele frequency, * the p values were significant before correction for
multiple testing. The vertical line at unit 1 represents the central value of OR. All the horizontal lines that cross this line represent non-
significant association of the SNPs. Those left of this central line are protective (OR<1), and those right of the line are risk-conferring
SNPs (OR>1).

118
Fig 3.19 Forest plot of the SNPs screened for POAG. Diamond shape represents OR, horizontal lines represent 95% CI, HG;
heterozygous genotype, VG; variant allele genotype, AF; Allele frequency, * the p values were significant before correction for
multiple testing. The vertical line at unit 1 represents the central value of OR. All the horizontal lines that cross this line represent non-
significant association of the SNPs. Those left of this central line are protective (OR<1), and those right of the line are risk-conferring
SNPs (OR>1).

119
Fig 3.20 Forest plot of the SNPs screened for POAG. Diamond shape represents OR, horizontal lines represent 95% CI, HG;
heterozygous genotype, VG; variant allele genotype, AF; Allele frequency. The vertical line at unit 1 represents the central value of
OR. All the horizontal lines that cross this line represent non-significant association of the SNPs. Those left of this central line are
protective (OR<1), and those right of the line are risk-conferring SNPs (OR>1).

Chapter 4
Discussion

121
4 Discussion
Glaucoma and AMD are multifactorial diseases, caused by a combination of genetic and
environmental factors. Some of the features reflecting the complex nature of the diseases
are their heterogeneous nature (different genes causing the same phenotype) and polygenic
involvement (more than one gene interacts to cause the disease). In addition, environmental
factors also influence disease progression (phenocopies), and sometimes the mutation
carriers do not have disease symptoms due to the presence of modifier elements. In
addition, such diseases may also not necessarily follow Mendelian rules of inheritance
(Faucher et al., 2002; Baird et al., 2003; Pang et al., 2002; Lander and Schork 1994). For
such complex diseases, although it is difficult but is very important to ascertain the
pathogenic nature of the variant, penetrance of the disease and age of disease onset.
Moreover another indicator of the pathogenicity of a certain variant is indicated by its
higher presence in affected individuals as compared to an unaffected control population
(Alward et al., 1998).
In an attempt to identify the underlying genetic factors in Pakistani patients implicated in
multifactorial disorders including glaucoma and AMD, genetic screening was carried out
for 20 families with glaucoma and 2 families with AMD. In the glaucoma families, possible
novel disease genes were identified, including a possible novel locus for PCG. The
previously associated glaucoma genes MYOC, OPTN and WDR36 were found not to be
involved in the pathogenesis of glaucoma in the studied Pakistani families. However, a
mutation in CYP1B1 was found to be involved in the pathogenicity of PCG in a Pakistani
family. Of the 20 families studied, in 4 (20%) families of glaucoma a possible genetic cause
was identified in the current study. Along with the screening of the familial cases, case-
control association analysis for both glaucoma and AMD was carried out where 12 SNPs
in 1000 cases with glaucoma (500 POAG, 200 PACG and 300 PEXG) and 300 controls,
and 16 SNPs in 300 cases with AMD and ~300 controls were studied. In the Pakistani
population a few SNPs were found to have a protective role while others had a pathogenic
role and yet others had no role in the pathogenicity of the diseases. The difference in the
association of the SNPs in Pakistani populations as compared to the populations in which
the SNPs are associated with the respective diseases (glaucoma and AMD) might be due

122
to variations in the distribution of the alleles of a particular SNP in various populations of
the world.
4.1 Glaucoma Families
All the glaucoma families were pre-screened for candidate glaucoma genes MYOC OPTN,
WDR36 and CYP1B1. Though MYOC is known to be involved in disease progression in
2.6% to 4.4% of POAG cases (Fingert et al., 1999), no pathogenic variant in the gene was
found in the current cohort with the exception of a non-synonymous SNP (rs2234926).
This variant was identified in 16 probands, and was therefore screened in a panel of
unrelated POAG, PACG and PEXG patients. However, no significant association was
found for rs2234926 with the different types of glaucoma. This polymorphism is a
recurrent SNP among MYOC variations and being the most common SNP it is reported to
be disease-associated in various populations (Lam et al., 2000; Pang et al., 2002). In
addition, mutations in MYOC occur in various populations of the world with varying
frequency; 8% of Italian glaucoma patients carry MYOC variants, whereas in the Finnish
population no MYOC variants were identified (Lam et al., 2000; Pang et al., 2002; Fingert
et al., 1999). In the Indian population, mutations in the gene are reported to be responsible
for 2% of POAG cases (Sripriya et al., 2004). Although no disease-causing mutation was
found in the current cohort, recently the c.1130C>T, p.(Thr377Arg) variant in MYOC has
been reported to be a disease-causing mutation in a Pakistani family (Waryah et al., 2013).
This indicates the possibility that the gene might be involved in the pathogenesis of
glaucoma in the Pakistani population, but is probably a rare cause of the disease. Similarly,
in the current cohort only a known pathogenic SNP, Met98Lys, was found in OPTN in
three probands. The result is not surprising as the association of the SNPs and mutations in
OPTN varies among various populations of the world (Leung et al., 2003; Ayala-Lugo et
al., 2007). The original study that highlighted OPTN as a candidate gene for glaucoma
described the Met98Lys, was found in OPTN in three probands. The result is not surprising
as the variant to be associated with NTG (Rezaie et al., 2002). Although subsequent studies
showed conflicting results about the involvement of the variant in glaucoma, meta-analysis
did indicate association of the Met98Lys, was found in OPTN in three probands. The result
is not surprising as the variant with glaucoma but only a weak association was found in

123
various Asian populations (Ayala-Lugo et al., 2007; Alward et al., 2003; Fuse et al., 2004;
Sripriya et al., 2006). Keeping in view the diversity of the association of this SNP with
different populations, Ayala-Luogo et al (2007) proposed that the involvement of
rs11258194 might be evaluated in glaucoma families as well as in sporadic cases. Thus in
the current study the segregation of rs11258194 was checked in the families of the 3
probands (in whom it was initially identified), as well as its association with sporadic
POAG, PACG and PEXG cohorts. Although the SNP did not segregate in the 3 POAG
families, an interesting pattern of segregation was seen when the overall frequency
distribution of the alleles was calculated in the affected as well as unaffected family
members. In this analysis it was observed that of the total individuals 2 (11%) had the
ancestral TT genotype, 14 (78%) were heterozygous (TA) and 2 (11%) had the
homozygous variant allele (AA). This pattern was not seen in unaffected controls
(TT=96.4%, TA=3.6%, AA=0%), or sporadic cases of POAG (TT=90.8%, TA=9%,
AA=0.2%). Although this variant did not segregate in the families, the preponderance of
the TA genotype in the families suggests a possible role in the progression of the disease.
This genotype may interact with some other unknown gene and thus increase the risk of
glaucoma in the families carrying this variant. In order to preclude the possibility that the
high prevalence in the affected families was by chance, we also analyzed two other POAG
families in which this variant was not found in the probands, but none of the members of
these families were found to carry the variant A allele. This further strengthens our
conjecture that when present, this variant might play a role in the initiation or progression
of the disease in the affected families. In addition, this SNP has previously been reported
to be associated with low IOP, and thus has a modifying effect on the glaucoma phenotype.
OPTN increases the sensitivity of glial neuronal cells to risk factors of glaucoma, even at
normal IOP (Melki et al., 2003). In the current study no difference was detected between
the IOP in patients with and without this variant, which is in agreement with the previous
work of Ayala-Luogo et al. (2007) who also did not find an IOP lowering effect of the
variant allele of this SNP. However, its role in an increased risk due to sensitivity of glial
cells at normal IOP cannot be ruled out, thus studies of NTG patients are required to further
validate this.

124
When WDR36 was screened in the familial cases no mutation was found in any of the cases.
Previously Monemi et al (2005) have shown that WDR36 was associated with Glaucoma,
where they found 4 mutations in this gene present in 11 patients. However, in subsequent
studies of the same gene no association of WDR36 was observed with glaucoma (Fingert
et al., 2007; Footz et al., 2009) thus making it one of the rare genes causing glaucoma in a
select ethnic group.
In the current cohort, there were three families of PCG, and in one family (GLC 2) among
thethem a possible novel locus on chromosome 7 was found to be linked with the disease,
and in another family (GLC 16) a mutation (Arg290Profs*37) in CYP1B1 segregated with
the disease. One family however, remained unsolved. The incidence of PCG worldwide is
1:10,000, which is much higher among populations where the rate of consanguineous
marriages is higher (Papadopoulos et al., 2007). To date the highest incidence of PCG has
been found in Gypsies (1:1,250) (Gencik 1989) and Saudis (1:2500) (Gencik et al., 1982)
whereas in India 1:3300 children suffer from PCG (Dandona et al., 1998). In the Pakistani
population the ratio of consanguineous marriages is much higher (Afzal et al., 1994;
Hussain and Bittles 1998), hence the rate of PCG is expected to be high but due to a lack
of epidemiological studies the exact rate is not known. To date 4 loci (GLC3A to GLC3D)
have been reported to be associated with PCG (Sarfarazi et al., 1995; Akarsu et al., 1996).
Two genes in two of these loci have been found to be involved in the pathogenicity of PCG,
one of which is well established; CYP1B1 in GLC3A (Stoilov et al., 1997) and LTBP2 in
GLC3D. The later still needs to be functionally validated for its involvement in PCG
(Moren et al., 1994). It has been more than a decade that CYP1B1 has been shown to be
causative in PCG patients (Sarfarazi et al., 1995), and screening of POAG and PCG for
CYP1B1 in different populations of the world has revealed various mutations involved in
the pathogenesis of the disease. Mostly these mutations have been identified in
homozygous form in PCG patients owing to the recessive pattern of inheritance of the
disease (Stoilov et al., 1998). Nearly 150 mutations are known in CYP1B1, causing PCG
in various populations while a few of them have been identified to be disease-associated in
the Pakistani population, which include p.Leu177Pro, p.Ile87Val, p.Asp374Asn (Beier and
Fahimi 1985), p.Ala288Pro, p.Asp242Ala (Micheal et al., 2014). This higher prevalence
of mutations in a particular gene resulting in the same phenotype in a population is

125
indicative of its pathogenicity and screening of this gene could be effectively used as a
diagnostic tool for pre-screening of PCG patients before whole genome analysis.
Another interesting result of the current work was the identification of possible trigenic
inheritance in a JOAG family (GLC 1). Novel variants in MYO18A, ENOX1 and COL9A2
segregated with the disease in one loop (GLC1a) of the family, while in the other loop
(GLC1b) a variant in NCOA7 segregated with the disease in the family. The difference in
both loops was the age at which the symptoms of the disease started to appear. In the loop
where the three variants were present the mean age of onset was 25 years, whereas in the
loop where this possible trigenic pattern was absent, the mean age of onset of the disease
was 50 years. The interaction of different genes resulting in variation in the age at which
the symptoms of a particular phenotype appear within the same family has also been
reported previously in glaucoma, where a single mutation in MYOC (Gly399Val) resulted
in disease development among the affected individuals at a mean age of 57 years, and when
this mutation was present in tandem with a mutation in another gene, CYP1B1
(Arg368His), it resulted in a lower mean age of disease onset to 27 years (Vincent et al.,
2002).
Among the three variants, the variant in MYO18A (c.2071C>T; p.Arg691Cys) lies in a
highly conserved region in 12 species (phyloP 4.40) where it is present in the motor head
domain of the protein, resulting in the change of a basic amino acid (Arg) to a hydrophobic
amino acid (Cys), which gave a higher physicochemical difference among the two amino
acids (Grantham distance=180). SIFT analysis revealed the variant as deleterious and
Mutation Taster categorises the variant as disease-causing. The gene MYO18A encodes a
P21 activated kinase (PAK) involved in Golgi localization, cytoskeleton maintenance and
acts as an immunological cell surface protein (Hsu et al., 2010). Moreover, it also plays an
important role in the migration ability of epithelial cells (Taft et al., 2013). The motor
domain of MYO18A has a binding site for ATP and F-actin, and it is localized near the
cell periphery in the lamellar actomyosin bundles (Taft et al., 2013). There is no previous
report of the involvement of the gene in pathogenicity of glaucoma, but in a study
conducted by Thomas et al (2011) on the differential expression of protein phosphorylating
genes in response to increased pressure on the glial cells (astrocytes), the authors found

126
that MYO18A was one of the few genes highly expressed in the region as a result of
increased hydrostatic pressure. Inhibition of the protein kinases can result in the disruption
of the actin filaments, present in the eyes, which can change the TM and as a consequence
alter the ECM matrix composition and aqueous humor outflow (Thomas et al., 2011),
which can result in raising the IOP. High expression of the gene is seen in the mouse eye
(genome.ucsc.edu). All members of the family in the current study carrying the variant had
elevated IOP, which was reduced to the normal range by the use of medicine.
The second variant (c.171G>A, p.Met57Ile) in the family (GLC1) was found in the Ecto
NADH Oxidase (ENOX1) disulphide exchanger 1 gene. This variant also lies in a highly
conserved region of the gene in 12 species (phyloP 5.37), resulting in the change of
methionine (Met) to isoleucine (Ile). As both amino acids are hydrophobic, the
physicochemical difference is low (Grantham distance=10) and the pathogenicity
predicting programme SIFT grades the variant as tolerated, whereas Mutation Taster
identifies it as a disease-causing variant. The ENOX1 exhibits oxidoreductase activity as
well as N disulphide thiol interchange activity (Jiang et al., 2008). It also plays an essential
role in the plasma membrane electron transport pathway, which in turn is involved in
cellular defence, intracellular redox homeostasis and control of cell growth and survival
(Venkateswaran et al., 2014). It has been observed that there are strong interactions
between the plasma membrane and cytosolic redox homeostasis imbalance and oxidative
stress. Once the ratio is imbalanced the induction of Bcl-2 occurs resulting in apoptotic cell
death (Morré and Morré, 2012).
The third variant (c.1061C>T, p.Pro345Leu) segregating with the disease in the family was
located in the collagen, type IX, alpha 2 (COL9A2) gene, present in a highly conserved
region in 11 species (PhyloP 4.48). This change results in incorporation of the amino acid
leucine instead of the normally translated amino acid proline. As both amino acids are
hydrophobic, there is very little physciochemical difference between them (Grantham score
21). The pathogenicity predictor SIFT predicts the variant to be deleterious and the
Mutation Taster grades it as disease-causing. This is a rare variant and has been assigned a
reference SNP number rs201772619. The collagens play an important role in strengthening
and structurally supporting connective tissues (Bruce et al., 2007) such as tendons and

127
ligments. The type 9 collagens are the most flexible collagens among all. Mutations in the
genes coding the protein are known to cause dominant multiple epiphyseal dysplasia
(Villemain et al., 1990), intervertebral disc disease (Higashino et al., 2007) and Stickler’s
syndrome (Baker et al., 2011). The features of Stickler syndrome are distinctive facial
appearance, eye abnormalities, hearing loss and joint problems. The eye abnormalities can
be severe myopia (mostly), increased IOP and glaucoma, retinal detachment as well as
cataract (Nikopoulos et al., 2011; Pagon et al., 2012). Mutations in the gene have
previously been reported to cause severe myopia in Han Chinese (Chen et al., 2014a).
Glaucoma in the above mentioned family may possibly be due to a result of the combined
effect of all the three variants. The combination of these variants may also result in
lowering the age of onset of the disease, as in the patients (GLC1b) where the variant was
not present the age of onset of the disease was much higher. Moreover it was observed that
an individual who had both variants in MYO18A and ENOX1 had no symptoms of the
disease. Therefore, it is hypothesized that the presence of the third variant in COL9A2
interacts with the other two variants and results in the appearance of the phenotype at an
early age. Another possibility is that only one variant among the three is responsible for
the disease pathogenicity and COL9A2 variant is deemed to be the most likely disease
causative variant in this family. However, there is still a need of conducting functional
studies to validate the involvement as well as the interaction of these variants with each
other in the manifestation of disease. As opposed to this, the variant (c.724G>A,
p.Val242Met) in exon 11 of NCOA7 (nuclear receptor coactivator 7) segregated with the
disease in the loop with higher age of onset of the disease. The variant lies in a highly
conserved region (PhyloP 6.18) resulting in a change of valine to methionine in the
peptidoglycan-binding lysin domain. As both amino acids are hydrophobic, there is a small
physiochemical difference between them (Grantham distance=21). The pathogenicity
predicting software SIFT scores the variation deleterious, Mutation Taster categorises it as
disease-causing, and PolyPhen considers the variant as probably damaging. NCOA7
encodes a protein involved in nuclear hormone receptor binding and ligand-dependent
nuclear receptor transcription coactivator activity. It is involved in the enhancement of the
transcriptional activities of several nuclear receptors and coactivation of different nuclear
receptors, such as estrogen receptor 1, thyroid hormone receptor, beta, peroxisome

128
proliferator-activated receptor gamma and retinoic acid receptor, alpha. The gene has been
implicated in reducing oxidative stress, thus lowering its damaging effects (Durand et al.,
2007), in diseases such as neurological diseases. These are regulated by interferons,
moreover the exons 11, 12 and 15 are expressed excessively as compared to other exons in
the neurological disorders (Yu et al., 2014). The variant c.724G>A also lies in the Exon 11
of the gene and thus functional studies are required for the elucidation of disruption in the
function of the gene as a consequence of this change.
Another family with dominant glaucoma (GLC 5) was screened by exome sequencing; the
family had two individuals with early appearance of glaucoma symptoms. Only one variant
(c.125C>T, p.Thr42Met) in PHKG1 segregated with the phenotype in the family in a
heterozygous form, with the exception of the individuals with early appearance of
symptoms in which it was present homozygously. The variant lies in four overlapping
domains; the protein kinase catalytic domain, serine-threonine/tyrosine-protein kinase
catalytic domain, serine/threonine/dual specificity protein kinase catalytic domain and
tyrosine-protein kinase catalytic domain. This variant lies in a highly conserved region in
ten different species (phyloP 5.94), and results in an amino acid change from threonine to
methionine, thus changing a polar uncharged amino acid to a hydrophobic amino acid
(Grantham score= 81). SIFT scores the variation deleterious, Mutation Taster categorises
it as disease-causing, and PolyPhen considers the variant to be probably damaging.
4.2 Case Control Association Analysis: Glaucoma
Previously reported SNPs associated with POAG in various studies including GWAS, were
screened in the current glaucoma cohort. Since recent studies have suggested that common
genetic factors might contribute to various forms of glaucoma, the current study was
extended to PACG and PEXG. A summary of the SNPs genotyped for glaucoma in the
Pakistani cohort and their pathways is given in Figure 4.1. Results indicated association of
SNPs in HSP70 and NOS3 with all three types of glaucoma, whereas an association of
BIRC6 and P450 polymorphisms was observed only with PEXG. No association was
observed for SNPs in PDIA5, P21 and P53 with any type of glaucoma in the current cohort.
Besides these SNPs, three SNPs in genes PLEKHA7, COL11A1 and PCMTD1 were
recently reported to be associated with PACG in the Asian population, therefore the SNPs

129
Figure 4.1 Summary of the SNPs genotyped for glaucoma. ‘*’ represents the SNPs that were genotyped for PACG only, ER;
Endoplasmic Reticulum, TM; Trabecular Meshwork.

130
were studied in the current cohort which identified only the COL11A1 SNP to be associated
with PACG.
Stress and apoptosis induced RGC degeneration is accentuated by the involvement of
multiple factors such as raised intraocular pressure (IOP), vascular abnormalities and
oxidative stress. These genes play an important role in oxidative stress and apoptosis and
one of the mechanisms via which the modification of cells as a result of oxidative stress
are dealt with, is controlled expression and regulation of various genes. NOS3 and HSP70
are two such genes, which are expressed in the cells in response to stress-inducing factors
such as heat, toxic metabolites, high intensity light and free radicals (Fletcher et al., 2008).
These genes have been shown to elicit enhanced transcription levels of the respective
mRNA when the body is under stress (Ishii et al., 2003; Liu and Neufeld 2003). NOS3 is
involved in different processes, such as neurotransmission, the regulation of vascular tone,
vasodilatation and apoptosis. In addition, it also regulates blood flow to the ocular tissues
and has been implicated in the pathogenesis of different neurodegenerative disorders, such
as diabetic retinopathy (Awata et al., 2004), glaucoma (Toda and Nakanishi-Toda 2007)
and migraines (Gruber et al., 2010). Plasma NO levels are regulated by NOS3, thus any
environmental or genetic risk factor that enhances NOS3 expression would contribute to
NO mediated toxicity. It has been previously reported that the VNTR in intron 4
of NOS3 significantly influences the plasma NO levels. Functional studies have shown that
the variant ‘a’ allele (with four 27-bp repeats) in homozygous form is strongly correlated
with increased plasma NO levels, which were found to be twice as high as the level found
in the ‘b/b’ genotype (with five 27-bp repeats), indicating the NOS3 underlying potential
for NO-related pathogenicity (Malek et al., 1999).
The NOS3 expression is regulated at the transcriptional level by microRNAs (Balligand et
al., 2009) that repress NOS3 expression by interfering with the gene transcription
efficiency. Moreover the microRNAs act as an endogenous sequence-specific feedback
regulatory molecule that reversibly inhibited this process and thus enabled the rapid
turnover of NOS3 molecules to minimize the damage associated with stress and hypoxia.
Zang et al. (2005) postulated that the amount of microRNA would vary from individual to
individual. In contrast to the ‘b’ allele with five 27-bp repeats, the variant ‘a’ allele with 4

131
repeats produced fewer microRNAs and hence, reduced transcriptional repression would
occur, correlating with the increased plasma NO.
The current results are in line with the above observations, as in the current study
significant association of the NOS34 a/b genotype was found with all forms of glaucoma
in the Pakistani cohort, which is probably a result of high plasma NO levels that are toxic
to the optic nerve and ultimately cause its degeneration, which is a classic hallmark of
glaucoma. Earlier studies conducted to establish a possible association between glaucoma
and altered NOS expression focused mainly on POAG patients (Galassi et al., 2004;
Karantzoulis-Fegaras et al., 1999) and were able to show a positive correlation between
this polymorphism and the disease, which is in agreement with the current results.
In the current work, the involvement of the intron 4 VNTR polymorphism of NOS3 was
also studied in PACG, as impairment in the NO production might lead to closure of the
angle (Awadalla et al., 2013), which can be partially associated with
altered NOS3 expression and the resultant NO-mediated neurotoxicity. The current results
indicate that there is indeed a correlation between PACG and the polymorphism in NOS3,
as a significantly higher frequency of the variant NOS3 a allele was found in PACG patients
as compared to the unaffected controls. Previously also the 27bp variant allele of the NOS3
intron 4 VNTR polymorphism has been shown to be significantly associated with PACG
in Australians (Awadalla et al., 2013). In the current cohort an association of ‘ba’ and ‘aa’
genotypes of the NOS3 gene polymorphism was also found with PACG. As opposed to this
in the POAG and PEXG cohorts, the heterozygous ‘ba’ genotype was found to be
associated with the disease. The mechanism behind the PACG pathogenicity might be that
NO production in the anterior chamber results in the relaxation of the ciliary muscle and
thus increases the depth of the anterior chamber of the eye (Shi et al., 2014). The site for
the formation of NOS3 lies in excess in the ciliary muscle, and the outflow passageway of
the aqueous humor and thus has been proposed to be involved in the regulation of IOP
(Nathanson and Mckee 1995). The anatomical change induced by NO in PACG is
postulated to be due to its effect on the activity of MMP9, which when down regulated,
might result in the narrowing of the anterior chamber and refractive errors by affecting the
ECM remodelling (Shi et al., 2014). In the presence of the ‘ba’ or ‘aa’ genotype the

132
narrowing of the chamber occurs, which is a characteristic feature of PACG (Shi et al.,
2014). In POAG and PEXG there are other mechanisms such as the accumulation of debris
in the TM for disease pathogenicity as opposed to the narrowing/closing of the angle, which
in the later case remains open.
In glaucoma patients, raised IOP causes stress mediated neuron injury and to overcome
this stress heat shock proteins (HSPs) are recruited. Besides its protective effects one of
the side effects of the HSPs is the stimulation of the immune system and engagement of
the antigen presenting cells. Thus the HSPs not only act as neuroprotective molecules in
the cell but they can also contribute to the progression of the disease by over-activating the
auto-stimulatory immune responses leading to optic nerve neuropathy (Tezel et al., 2004;
Ishii et al., 2003). In glaucoma patients, it has been observed that as a result of activation
of the immune system, there are increased titers of anti-HSP antibodies, which aid in the
progression of the disease by minimising the protective abilities of the native HSPs (Tezel
et al., 2000).
The regulation of HSPs’ expression pattern determines the fate of the cell, the
underexpression leads to an inefficient stress response and overexpression drives
immunodestruction, with the outcome in both cases being damage driven by the oxidative
free radicals in one case and by cytokines in the other. This is supported by the data of
Tezel et al. (2000), who have previously shown HSPs to be significant enhancers of both
the cytoprotective and neurodegenerative functions of the immune system in RGCs and
glial cells, and clearly demonstrated that these proteins were critical in facilitating the
glaucomatous changes resulting in optic nerve damage and neurodegeneration.
The rs1043618 polymorphism in HSP70 screened in the current cohort has previously been
shown to be associated with reduced HSP70 expression, which could result in an inability
of the cell to cope with stress and to perform cytoprotective functions. Functional analyses
of the rs1043618 polymorphism, which maps to the 5′ UTR region of HSP70, has revealed
that compared with the G allele, the variant C allele causes reduced promoter activity and
lower HSP70 protein levels (He et al., 2009). Tosaka et al. (2007) had previously reported
a significant association between the -110A>C polymorphism in HSP70 and POAG
(p=0.026) in the Japanese population. This polymorphism is known to increase HSP70

133
expression, thus supporting the hypothesis that neuropathy is associated with
autoimmunity as a result of the elevated HSP70 levels. However, Tosaka et al. (2007) did
not find any association between glaucoma and the rs1043618 polymorphism. The same
mechanism might be involved in the onset of PEXG seen in the current study, as the raised
IOP-induced stress on the RGCs might recruit the HSPs to overcome the stress. Moreover,
Fung et al. (2005) have reported that lower levels of HSP70 are not able to provide
protection against neurodegeneration in Alzheimer’s disease. On the basis of a higher
frequency of the risk allele “C” in PEXG, POAG and PACG patients it is hypothesized that
this polymorphism might be associated with pathogenesis of all three types of glaucoma.
In both the primary forms of glaucoma the association of the heterozygous ‘GC’ as well as
homozygous ‘CC’ genotype was observed with the disease but in the secondary form i.e.
PEXG, only the homozygous ‘CC’ genotype was found to be associated with the disease.
In different studies different risk factors of POAG and PACG have been established
whereas, there is still limited understanding of the factors responsible for PEXG
predisposition. Raised IOP is the major contributor of OAG in patients with PEXG, but the
contribution of the risk factors such as the dandruff-like flakes that accumulate in all the
aqueous bathed surfaces of the eye in PEXG cannot be ignored (Eagle 2012). Differential
expression of the stress response genes is seen in eyes with PEXG, as seen in the case of
clustrin gene, an efficient extracellular chaperone, which is down regulated in the case of
PEXG, resulting in the aggregate formation and accumulation of PEX material in the TM,
hence clogging it and elevating the IOP (Zenkel et al., 2006). This mechanism might
indicate that the changes in the PEXG patients carrying the ‘CC’ genotype of the HSP70
polymorphism is more severe as compared to those carrying the ‘GC’ genotype.
The current study identified a moderate protective association of the BIRC6 rs2754511
polymorphism with PEXG in the Pakistani population (p=0.05). In agreement with the
previous findings in the Salt Lake City and San Diego populations, which demonstrated a
protective effect of the T allele of rs2754511 on the development of POAG (Carbone et
al., 2011), this allele in the homozygous form (TT) was also found to be protective in
PEXG in the current study. BIRC6 is ubiquitin carrier protein involved in the protection of
the cell against apoptosis and also reduces cellular stress (Carbone et al., 2011; Lamers et

134
al., 2012). Increased intraocular pressure, ROS and free radicals create a stressful
environment in the eye (Sacca et al., 2007; Izzotti et al., 2011). In the ER, stress can be
accompanied by the aggregation of misfolded proteins, which can activate a cytoprotective
signal response known as unfolded protein response (UPR) that triggers the activator
functions such as adaptation, alarm and apoptosis (Xu et al., 2005). When stress is
prolonged and adaptation and alarm fail to pull the cell back towards normal conditions,
the UPR results in activation of apoptosis (Kim et al., 2008) and also elicits an
inflammatory response in order to restore the normal environment of the cell. This
mechanism has been found to be involved in the pathogenesis of many neurodegenerative
disorders such as Alzheimer’s, Parkinson’s and cerebral ischemic insults (Wang and
Kaufman 2012). Apoptosis might be one of the various mechanisms that is involved in the
degeneration of RGCs in PEXG. BIRC6 is an anti-apoptotic protein, which promotes cell
survival by inhibiting caspases (Ren et al., 2005). Association of downregulation of BIRC6
with various polymorphisms and mutations leads to upregulation of P53, resulting in
mitochondrial-mediated apoptotic cell death (Ren et al., 2005).
Another polymorphism in CYP1B1, rs2567206, iwas also screened, which indicated a
strong association of the polymorphism with PEXG only and not with POAG or PACG.
CYP1B1 belongs to the family of cytochrome P450 (Zhao et al., 2013) and is involved in
regulating the metabolic pathways by acting as an intermediate catalyst. This protein also
plays an important role in the proper development and functioning of the iridocorneal angle
of the eye (Sarfarazi 1997). Vasiliou and Gonzalez (2008) observed that CYP1B1 deficient
mice had an abnormal drainage structure, including abnormalities in the trabecular
meshwork; the same phenomenon has been observed in human PACG patients. Mutations
in this gene associated with PACG have been reported in Pakistani (Firasat et al., 2008),
Indian (Kumar et al., 2007) and European families (Reddy et al., 2003; Kakiuchi-
Matsumoto et al., 2001). Polymorphisms in different region of the gene have been reported
to be associated with modified activity of the CYP1B1 enzyme, which has been shown to
cause certain types of cancers and POAG in different populations. The SNP rs2567206 has
previously been found to be associated with PCG but not with primary open angle or angle
closure glaucoma. It has been hypothesized that the variant results in lowering the activity
of the promoter in the TM cells, and regulates the gene in vivo (Chakrabarti et al., 2010).

135
It has also been observed that the polymorphism rs2567206 covers the site of the promoter
region, which contains the binding site of transcription factors and could thus interfere with
this process (Kim et al., 2002; Price et al., 1992).
The association of both BIRC6 and CYP1B1 SNP only with PEXG might be due to the
more aggressive nature of PEXG i.e severe degenerative changes occurring in PEXG as
compared to POAG or PACG. Moreover, in patients with PEXG the damage to the ONH
is more severe than in POAG or PEXG in the current cohort as depicted by the CDRs,
(mean CDR values; PEXG=0.79±0.26, POAG=0.62±0.23, & PACG=0.61±0.27). The
extracellular matrix of the trabecular meshwork is disrupted as a consequence of damage
to the mitochondria, a characteristic mechanism involved in the pathogenicity of POAG
and PEXG (Izzotti et al., 2011). Konstas et al. (1997) have observed excessive
mitochondrial alterations in PEXG. The highest level of mitochondrial damage and
mitochondrial loss per cell was seen in PEXG as compared to POAG, which indicates its
more aggressive nature. Zenkel et al (2005) have reported differential expression of ECM
proteins and stress response genes in the eyes of PEXG patients compared to eyes of normal
healthy controls. The expression of ECM genes is upregulated, resulting in aggregation of
ECM proteins. Glutathione S-transferase 1, which is involved in protection from oxidative
stress, has been reported to be downregulated in these patients. In addition, clusterin, an
efficient extracellular chaperone, is downregulated in PEXG eyes, resulting in aggregation
of pathologic ECM proteins. Consequently, abnormal proteins accumulate, resulting in the
formation of pseudoexfoliative material (Zenkel et al., 2006). In the anterior chamber this
hinders the outflow of aqueous humor by clogging the trabecular meshwork, which results
in elevation of the IOP (Streeten et al., 1992; Streeten et al., 1990). All these stresses result
in severe degenerative changes in PEXG.
The SNP rs1801270 was also screened in the current glaucoma cohort but no association
was found. The SNP is located in a highly conserved region, which encodes the DNA-
binding zinc-finger domain of the protein and results in incorporation of Arg at position 31
instead of Ser (Ressiniotis et al., 2005). Incorporation of Arg results in failure to protect
the RGCs from degeneration in glaucomatous neuropathy. RGC death via apoptosis has
been extensively explored (Nickells 1999) and the major transcription factor in this

136
apoptotic cascade is P53, which is also known as guardian of the genome (Rosenbaum et
al., 1998) and is involved in the transcription of the kinase inhibitor P21 (Ressiniotis et al.,
2005). Damage to the DNA causes the activation of the P21 enzyme, which then causes
cell cycle arrest by inhibiting the cyclin dependent kinases, thus blocking the entry of the
cell cycle from the G1 to S phase and from the S to G2 phase, finally leading the cell
towards apoptosis. In normal ocular tissue a higher expression of P53 is usually observed
(Acharya et al., 2002), therefore it has been speculated that any alteration in its expression
might stimulate P53-induced apoptosis. Tsai et al (2004) concluded that the post-
transcriptional product of rs1801270 was important in the development of POAG.
However, studies conducted on Caucasian (Ressiniotis et al., 2005) and Turkish (Saglar et
al., 2009) populations showed non-significant association of rs1801270 with glaucoma.
The current results are in agreement with the above mentioned studies as there was no
association between the P21 SNP and all the three different types of glaucoma in the
Pakistani population. The distribution of the minor allele of the SNP is highly variable
among populations; according to NCBI, it is 0.02 among Europeans and reaches 0.41
among Asians, while Africans and Hispanics had a frequency distribution in between these
values (Gravina et al., 2009).
Different studies of Chinese (Lin et al., 2002) and Caucasians (Daugherty et al., 2009)
have demonstrated significant association of P53 polymorphism (rs1042522) with POAG.
However, Acharya et al (2002), Saglar et al (2009) and Mabuchi et al (2009) studied P53
polymorphism in Indians, Turks and Japanese, respectively, and found no association
between the P53 alleles and POAG. Another interesting aspect of the polymorphism is that
the presence of Arg is associated with POAG in the Chinese population (Lin et al., 2002)
whereas the presence of the variant amino acid Pro is associated with POAG in Caucasians
(Daugherty et al., 2009). The aim of the current work was to study the role of this SNP in
the Pakistani population and the results of the current study were found to be in agreement
with Dimasi et al (2005) who also did not find any association of this SNP with POAG.
One possible explanation of not finding association in the current cohort could be that P53
might be contributing towards the development of glaucoma as a non-IOP genetic factor
(Mabuchi et al., 2009; Nickells 1999), increasing the susceptibility of NTG patients toward
glaucoma as compared to the patients with high tension glaucoma. Since in the current

137
cohort patients were studied with predominantly higher IOP, no association was observed,
while taking the NTG association under consideration, Dimasi et al (2005) screened their
patients with NTG for the polymorphism but found no association of the SNP with the
disease, which might be due to a smaller cohort of patients (62) of NTG in their study.
In addition a previously associated SNP, rs11720822 in the protein disulphide isomerase
family A member 5 (PDIA5) gene was also screened, but no association was found with
the disease in the Pakistani population. The gene is upregulated in response to endoplasmic
reticulum stress (Hayano and Kikuchi 1995), and the SNP has been shown to be associated
with POAG in San Diego in a GWAS study (Carbone et al., 2011). According to the dbSNP
database, occurrence of the T allele of rs11720822 in PDIA5 is very rare in various
populations of the world including the Asian and African populations
(http://www.ncbi.nlm.nih.gov/projects/SNP/snp_ref.cgi?rs=rs11720822), which supports
the current finding, as in the current study high occurrence of the allele was not observed.
Among the three genes found to be implicated in the pathogenicity of PACG (Vithana et
al., 2012), the polymorphism rs3753841 in COL11A1 was the only one found to be
associated with PACG in the Pakistani population. This polymorphism results in a change
from proline at position 1323 to leucine. The collagen type 11 has two α chains and the
gene COL11A1 transcribes one of them. Mutations in the gene have already been known
to cause Marshall syndrome and Stickler syndrome, both of which have glaucoma as one
of the features, in addition to features such as face flattening, auditory and skeletal
dysfunctioning. Due to aberrations in this gene, abnormality in the fibrillar collagen matrix
in the sclera occurs causing ocular deformities. The gene is also expressed in TM cells and
might be associated with the regulation of aqueous humor drainage, which when aberrant
might predispose the person to ocular anomaly. Vithana et al (2012) propose that common
variants in the gene affect the normal ocular architecture and might result in PACG. The
other two polymorphisms, one in PLEKHA7 (rs11024102) and the other in PCMTD1
(rs1015213), were not found to be associated with PACG in the current Pakistani cohort.
PLEKHA7 is involved in stabilizing the cellular junctions (adherens junctions), which are
essential in the iris, cillary body and aqueous humor outflow and the choroid. The SNP
rs1015213 resides 120 kb upstream of the gene and is in linkage disequilibrium (LD) with

138
PCMTD1, which has lately been found to play an intertermediate role in apoptosis and
inflammation. The differences in the association might be attributed to the smaller sample
size of the current study (200 PACG samples, 200 controls) as compared to the original
study (3771 PACG samples and 18,551 controls) (Vithana et al., 2012). All three SNPs
have also been screened in the Indian PACG cohort, which identified an association of
rs1015213 in PCMTD1 with PACG but not the other two polymorphisms (Duvesh et al.,
2013). The SNPs in COL11A1 and PLEKHA7 have also been reported to be associated
with higher risk of PACG in the Chinese, where the incidence of PACG is twice as high as
compared to other Asian populations (Chen et al., 2014b).
4.3 Familial Screening and Case Control Association Analysis: Age
Related Macular Degeneration
Two families with AMD were screened for the candidate gene CFH, in which no
involvement of the gene variants was found in the current families. Although linkage
studies for AMD using large families and twin studies has helped to identify the AMD
susceptibility genes, it has always been difficult to map the plausible genes mainly due to
the late onset of the disease (Swaroop et al., 2009). The familial studies have helped in the
discovery of disease causing genetic variants in two major AMD causing genetic loci which
harbour CFH and ARMS2/HTRA1. Besides the familial studies, case-control association
studies have contributed tremendously in defining the genetic component of the disease. A
summary of the SNPs genotyped for AMD in the Pakistani cohort and their pathways; is
given in Figure 4.2.
Drusen are the hallmark of AMD in whose formation and accumulation, the components
of the inflammatory pathway and complement system have been shown to be involved
(Seddon et al., 2005; Yucel et al., 2012). Polymorphisms in CFH, C3, C2, CFB and few
other genes have also been reported to be associated with AMD in various populations
around the world (Deangelis et al., 2011). Besides CFH, variants in ARMS2/HTRA1 have
also been found to be associated with AMD (Rivera et al., 2005; Klein et al., 2005b). In
the current AMD cohort no association was found with the CFH polymorphism rs1061170,
which is a well-established AMD causative variation in various populations, especially in

139
Europeans and also Indians (Kaur et al., 2006). These results are suggestive of differences
in the genotype and allele frequency distribution of this polymorphism among and within
various populations (Rodriguez De Cordoba et al., 2004; Chen et al., 2006). The
association of the CFH polymorphism appears to be varied specially among the Asian and
white populations (Tsai et al., 2008). The risk allele of the SNP was found to be lower in
Asians (Chen et al., 2012; Tsai et al., 2008), whereas it is higher in Europeans (Sofat et al.,
2012). It has recently been reported by the AMD Gene Consortium (Fritsche et al., 2013)
that there were great differences in effect sizes of the CFH polymorphism when the data
were stratified on the basis of ethnic background, and the strongest association was found
in Europeans. Other genes of the complement pathway have also been found to be
associated with AMD, including C2/CFB and C3 (Fuse et al., 2006; Yates et al., 2007;
Gold et al., 2006). SNPs that had been previously reported to be significantly associated
with AMD and are located 100kb upstream of the C2/CFB and C3 genes (Fritsche et al.,
2013) were screened in the current study, but these SNPs were not found to be associated
with AMD in the current Pakistani cohort, although the variants in these genes have been
reported to significantly contribute to AMD susceptibility (Swaroop et al., 2009).
A gene other than the complement pathway genes that has been shown to have a major
contribution in AMD is ARMS2 (Swaroop et al., 2009). In the current population, the case-
control association analysis identified that the risk allele (T) of the ARMS2/HTRA1
rs10490924 SNP confers higher risk of developing wet AMD as compared to dry AMD,
which is in agreement with the study of Sobrin et al (2011). In another study conducted by
Schwartz et al (2012), it was observed that the variant allele T conferred higher risk towards
advance bilateral wet AMD. The effect size of the rs10490924 SNP was much higher in
the current wet AMD cohort (OR=3.57) as compared to the multicentre study conducted
by Sobrin et al. (2011) although they obtained similar results the effect size was between
1.34-1.56. ARMS2 is located in the outer mitochondrial membrane and encodes protein
(age-related maculopathy susceptibility protein 2) of mitochondria (Kanda et al., 2007).
An indel polymorphism (372_815del443ins54) in the gene has been reported to remove
the polyadenylation signal, resulting in a higher turnover of the mRNA (Fritsche et al.,
2008). With advancing age, loss in the functional efficiency of the mitochondria occurs,
resulting in the formation and accumulation of ROS, mutations in the mitochondrial DNA

140
Figure 4.2 Summary of the SNPs genotyped for Age Related Macular Degeneration. ECM; Extracellular Matrix

141
and onset of apoptosis (Lin and Beal 2006). It has been observed that in the aging retina
and particularly in the macular region, cytochrome C deficient cones accumulate as well
as a higher rate of mitochondrial deletions are detected (Mcbride et al., 2006). The SNP
rs10490924 has been implicated in mitochondrial dysfunction, which consequently
increases the susceptibility of the photoreceptors to age associated degenerative changes
that might be due to the change in the coding sequence (A69S) of ARMS2, affecting its
conformation and thus interaction of the protein (Kanda et al., 2007).
A SNP, rs4420638, 14 kb upstream of the gene APOC1 and co-inherited with APOE is
previously shown to be significantly associated with AMD in the studied population
(Fritsche et al., 2013) was also screened in the current study, but the SNP was not found to
be associated with AMD in the current cohort. APOE was initially considered as a plausible
gene for AMD for two main reasons. First, it was found to be present in drusen associated
with AMD (Wang et al., 2010) and secondly, due to its involvement in Alzheimer’s (Baird
et al., 2006), which has many common features with AMD such as the presence of β
amyloid in the plaques of patients with Alzheimer’s as well as in drusen of patients with
AMD. In addition, both are diseases that occur at higher age (Ohno-Matsui 2011). The
gene is involved in the transport of lipids and cholesterol metabolism (Schmidt et al.,
2002), which are essential components of drusen (Wang et al., 2010) and hence the
involvement of APOE in AMD cannot be ignored, despite the non-association of
rs4420638 in the current cohort, which could be due to racial differences.
Microglial cells are present in the retina that respond to oxidative stress by the formation
of drusen (Combadiere et al., 2007) by the expression of APOE (Xu et al., 2006), proteins
of the complement system (Bellander et al., 2004), inflammatory components, CX3CR1and
β amyloid precursor protein (Haass et al., 1991). These cells are also found to play a
proangiogenic role in the retina (Checchin et al., 2006), and moreover, in the absence of
CX3CR1, they secrete VEGF which results in neovascularisation (Combadiere et al., 2007)
resulting in wet AMD. The risk allele (A) of the chemokine receptor CX3CR1 (Tuo et al.,
2004) SNP rs3732378, and the heterozygous genotype of SNP rs3732379 confer increased
risk of AMD in the Pakistani population, which is in agreement with previous studies
(Yang et al., 2010). It is postulated that the variation (rs3732378) in CX3CR1 affects the

142
migratory properties of the microglial cells in the retina, and accumulation in the
underlying layers of the retina result in drusenogenesis (Combadiere et al., 2007).
Moreover, lower levels of CX3CR1 have been detected in the macula of patients with
AMD and both variants, rs3732379 and rs3732378, might be responsible for decreased
ligand affinity and receptor binding. It is further postulated by Tuo et al (2004) that
decreased levels of CX3CR1 might be due to the interaction of SNPs present in the
promoter region that are in LD with the above mentioned SNPs and thus the presence of
the variant alleles of these SNPs might affect the transcription activity.
Under stressful conditions, VEGF plays a very important role in the maintenance of the
vasculature and has been found to be extensively expressed in the eyes of the AMD patients
where it induces the formation of new vessels in the retina (Shibuya 2008). Moreover, the
binding of VEGF with its receptor generates a signal cascade that affects NOS3 expression
(Gelinas et al., 2002; Hood et al., 1998). The expression of NOS3 results in the synthesis
of NO, which maintains the vascular tone, inhibits apoptosis (Kota et al., 2012) and is a
key regulator of ocular blood flow (Bhutto et al., 2010). In the promoter region of VEGF
there are eight SNPs (rs833061 [-460C>T], rs833062 [-417T>C], rs59260042 [-
1210C>A], rs79469752 [-1203C/T], C-160T, rs28357093 [-141A>C], rs1570360 [-
116G>A]) which have previously been reported to be associated with diabetic retinopathy
(Churchil et al., 2008), and recently found to be involved in neovascularisation in Pakistani
diabetic patients with retinopathy (unpublished data). Keeping in view the involvement in
the Pakistani diabetic retinopathy patients, the SNPs were also screened in the current
AMD cohort. However, none of the SNPs were found to be associated with AMD in this
cohort, although the risk allele of rs1570360 [-116G>A] showed a trend towards
association (after correction for multiple testing p=0.07) with AMD but did not reach the
level of significance. The 27bp intron 4 VNTR polymorphism of NOS3 was also screened
in the current AMD cohort, and it was observed that the risk allele ‘a’ was significantly
associated with wet AMD. The risk allele of the NOS3 polymorphism has previously been
reported to be associated with macular edema in the Japanese (Awata et al., 2004). The
NO produced results in the vasodilatation of the ocular vessels but free radicals produced
in oxidative stress deactivate the NO function, which further catalyses the lipid
peroxidation resulting in enhancement of stress in the ocular tissue (Beckman et al., 1990).

143
The minor allele ‘a’ has been shown to be associated with lower production of NO, which
under oxidative stress can increase the damage to the cells (Zhang et al., 2008). Previously
NO has been found in lower amounts in the plasma of AMD patients (Totan et al., 2001)
and reported to have an adverse effect on vascular functions (Bhutto et al., 2010).
In the current cohort the SNP rs243866 in MMP2 and SNP rs17576 in MMP9 were also
screened to determine their association with AMD. Both these SNPs were found to be
associated with AMD (wet and dry AMD combined) and with the dry AMD in the
subgroup analysis. However, the association remained significant only for rs243866 after
correction for multiple testing, although SNP rs17576 had a mild association with both wet
AMD and dry AMD, before the correction for multiple testing, which might be the reason
that overall the SNP is strongly associated with AMD. It is hypothesised that the risk allele
(A) and genotype (AA) of MMP2 rs243866 increases the predisposition towards dry AMD.
Both MMPs belong to the subgroup of gelatinases that cleaves the collagenases (Sethi et
al., 2000). The MMPs maintain the balance of extracellular matrix (Birkedal-Hansen et al.,
1993), which in the eyes includes the interphotoreceptor matrix (IPM) and the BM
(Plantner 1992). The MMP2 and MMP9 proteins are abundantly found in the IPM. It is
postulated that disproportion of these MMPs against their tissue inhibitors TIMPs in the
IPM can cause a pathological condition (AMD) in the retina. MMP2 and MMP9 proteins
have been found in higher levels in the RPE associated ECM in patients of AMD (Plantner
et al., 1998b; Plantner et al., 1998a). The SNP rs17579 has also been screened in Chinese
Han, but was not found to be associated with AMD (Zeng et al., 2014). The MMP activity
is controlled by expression of the tissue inhibitors of MMPs and posttranslational
modifications and thus by the control of expression level (Sternlicht and Werb 2001). The
SNP rs243866 is located in the promoter region of MMP2 (-1575 position) and has been
found to be associated with reduced transcriptional activity (Harendza et al., 2003).
Various studies found SNPs near the tissue inhibitor metalloproteinase 3 (TIMP3) gene to
be significantly associated with AMD. The protein remodels the extracellular matrix in the
retina (Francis and Klein 2011). The mutated gene causes Sorby’s fundus dystrophy, which
is an early onset degeneration of the macula (Weber et al., 1994). The previously associated
SNP rs5749482 in TIMP3 was studied in the current AMD cohort, but no association of

144
the SNP was found. Although the variation in the SNP has previously been reported as not
associated with AMD (Stone et al., 2001), Abecasis et al (2004) speculate that the
variations in the gene might be involved in interacting with some other variants in AMD
susceptible genes and also suggest environmental influences to cause the late effects of the
disease (neovascularisation).
Several Interleukins have been reported to play a key role in the pathogenesis of AMD
(Seddon et al., 2005; Klein et al., 2005a). IL-6 was previously shown to be involved in
increasing the risk of AMD independently (Seddon et al., 2005), moreover, IL-10 has been
postulated to suppress neovascularisation in wet AMD by regulating macrophages, which
are known to be anti-angiogenic factors (Apte et al., 2006). This interleukin is suggested
to suppress the influx of macrophages by having inhibitory effect on the cytokines that
attract macrophages (Ferguson et al., 1994). In the current cohort the risk allele ‘C’ and the
homozygous genotype ‘CC’ of the SNP rs16944 in ILβ was found to increase the risk of
wet AMD with an effect size of 1.57 and 3.23, respectively. However, the ‘CT’ genotype
of the SNP is associated with both wet and dry AMD, and the homozygous ‘CC’ genotype
was associated with dry AMD, but the association did not remain significant after the p
value was corrected for multiple testing. In a study conducted by Tsai et al. (2008), it was
postulated that the risk allele of the associated interleukin (IL-8) also increased the risk of
developing wet AMD in the Taiwanese. This SNP (rs16944) has previously been shown to
be associated with schizophrenia (Shirts et al., 2006) and bipolar disorder (Papiol et al.,
2008). The SNP is in the promoter region of the gene (-511) and has been shown to increase
the expression of the gene in combination with another variant in the promoter region of
the gene at -31 position (Hulkkonen et al., 2000; Hall et al., 2004).
SNP rs1800629 located in the promoter region of the ubiquitously expressed cytokine
tumor necrosis factor-alpha (TNF-α) was also screened in the current AMD cohort, but no
association of the polymorphism was found. The protein is involved in various processes
such as inflammation, immune-regulation and apoptosis (Vassalli 1992) and the
polymorphism has been associated with elevated TNF-α production (Wilson et al., 1997),
which has been associated with various complications in the eyes such as diabetic
retinopathy (Yoshioka et al., 2006; Limb et al., 1999) and glaucoma (Huang et al., 2009).

145
This polymorphism was also found to be associated with PEXG in the Pakistani population
(Khan et al., 2009) but the same polymorphism was not associated with PEXG in
Europeans of Caucasian descent (Mossbock et al., 2009). The difference in the associations
might be due to the difference in the distribution of the genotypes among various
populations of the world (Mossbock et al., 2009).
4.4 Conclusion
In the present study the genetic cause of familial and sporadic cases with glaucoma and
AMD were studied in the Pakistani population. This is the first time that a genetic screening
of AMD and whole genome screening of familial glaucoma in Pakistan has been
conducted, which has resulted in the identification of possible novel genes and a possible
novel locus linked to glaucoma. The association analysis of sporadic glaucoma and AMD
was also conducted for various polymorphisms, which were found to be significantly
associated with various populations in GWAS. Some of those polymorphisms were found
to be associated with the current population, either playing a pathogenic or a protective
role; whereas the rest of them were not associated with the disease, indicating genetic
heterogeneity. These differences among different association studies might be due to
geographical and ethnic variations in the studied populations.
4.5 Future Perspective
Glaucoma and AMD are both complex disorders and their complexity is attributed to the
contribution of numerous genes with varying degrees of effects. Although high throughput
techniques like GWAS have resulted in discovery of interesting genes but due to
restrictions such as differences in phenotyping and screening methods, replicating such
studies becomes difficult. Moreover, in the current study several genes could not be
functionally validated. Also genes implicated by functional studies could not be found to
be associated in genetic studies. Therefore the requirement is to characterize these diseases
at the molecular level using high throughput techniques. For such complex disorders,
whole genome sequencing is the method of choice for understanding their genetic etiology.
Functional studies would further be required for the validation of the genetic data, followed
by validation through proteomic approaches, animal models and replication studies in

146
different populations. Only then it would be possible to unravel the causative agents of
these complex disorders and their underlying molecular mechanisms that will further help
in developing better therapeutic interventions.

Chapter 5
References

147
5. References
Abecasis, G. R., Yashar, B. M., Zhao, Y., Ghiasvand, N. M., Zareparsi, S., Branham, K.
E., Reddick, A. C., Trager, E. H., Yoshida, S., Bahling, J., Filippova, E., Elner, S.,
Johnson, M. W., Vine, A. K., Sieving, P. A., Jacobson, S. G., Richards, J. E. &
Swaroop, A. (2004). Age-related macular degeneration: a high-resolution genome
scan for susceptibility loci in a population enriched for late-stage disease. Am J
Hum Genet. 74: 482-494.
Acharya, M., Mitra, S., Mukhopadhyay, A., Khan, M., Roychoudhury, S. & Ray, K.
(2002). Distribution of p53 codon 72 polymorphism in Indian primary open angle
glaucoma patients. Mol Vis. 8: 367-371.
Adatia, F. A. & Damji, K. F. (2005). Chronic open-angle glaucoma. Review for primary
care physicians. Can Fam Physician. 51: 1229-1237.
Afzal, M., Ali, S. M. & Siyal, H. B. (1994). Consanguineous marriages in Pakistan. Pak
Dev Rev. 33: 663-674.
Agarwal, S., Agarwal, A., Buratto, L., Apple, D. J. & Alió, J. L. (2002). Textbook of
Ophthalmology, Lippincott Williams & Wilkins.
Age-Related Eye Disease Study Research Group. (2001). A randomized, placebo-
controlled, clinical trial of high-dose supplementation with vitamins C and E, beta
carotene, and zinc for age-related macular degeneration and vision loss: AREDS
report no. 8. Arch Ophthalmol. 119: 1417-1436.
Age-Related Eye Disease Study 2 Research Group. (2013). Lutein + zeaxanthin and
omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye
Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 309: 2005-2015.
Akarsu, A. N., Turacli, M. E., Aktan, S. G., Barsoum-Homsy, M., Chevrette, L., Sayli, B.
S. & Sarfarazi, M. (1996). A second locus (GLC3B) for primary congenital
glaucoma (Buphthalmos) maps to the 1p36 region. Hum Mol Genet. 5: 1199-1203.
Akiyama, M., Yatsu, K., Ota, M., Katsuyama, Y., Kashiwagi, K., Mabuchi, F., Iijima, H.,
Kawase, K., Yamamoto, T., Nakamura, M., Negi, A., Sagara, T., Kumagai, N.,
Nishida, T., Inatani, M., Tanihara, H., Ohno, S., Inoko, H. & Mizuki, N. (2008).
Microsatellite analysis of the GLC1B locus on chromosome 2 points to NCK2 as a
new candidate gene for normal tension glaucoma. Br J Ophthalmol. 92: 1293-1296.
Ali, M., Mckibbin, M., Booth, A., Parry, D. A., Jain, P., Riazuddin, S. A., Hejtmancik, J.
F., Khan, S. N., Firasat, S., Shires, M., Gilmour, D. F., Towns, K., Murphy, A. L.,
Azmanov, D., Tournev, I., Cherninkova, S., Jafri, H., Raashid, Y., Toomes, C.,

148
Craig, J., Mackey, D. A., Kalaydjieva, L., Riazuddin, S. & Inglehearn, C. F. (2009).
Null mutations in LTBP2 cause primary congenital glaucoma. Am J Hum Genet.
84: 664-671.
Allingham, R. R., Wiggs, J. L., Hauser, E. R., Larocque-Abramson, K. R., Santiago-Turla,
C., Broomer, B., Del Bono, E. A., Graham, F. L., Haines, J. L., Pericak-Vance, M.
A. & Hauser, M. A. (2005). Early adult-onset POAG linked to 15q11-13 using
ordered subset analysis. Invest Ophthalmol Vis Sci. 46: 2002-2005.
Alm, A. & Nilsson, S. F. (2009). Uveoscleral outflow-a review. Exp Eye Res. 88: 760-768.
Alm, A. (2014). Latanoprost in the treatment of glaucoma. Clin Ophthalmol. 8: 1967-1985.
Alvarado, J., Murphy, C. & Juster, R. (1984). Trabecular meshwork cellularity in primary
open-angle glaucoma and nonglaucomatous normals. Ophthalmology. 91: 564-579.
Alvarado, J., Murphy, C., Polansky, J. & Juster, R. (1981). Age-related changes in
trabecular meshwork cellularity. Invest Ophthalmol Vis Sci. 21: 714-727.
Alward, W. L., Fingert, J. H., Coote, M. A., Johnson, A. T., Lerner, S. F., Junqua, D.,
Durcan, F. J., Mccartney, P. J., Mackey, D. A., Sheffield, V. C. & Stone, E. M.
(1998). Clinical features associated with mutations in the chromosome 1 open-
angle glaucoma gene (GLC1A). N Engl J Med. 338: 1022-1027.
Alward, W. L., Kwon, Y. H., Kawase, K., Craig, J. E., Hayreh, S. S., Johnson, A. T.,
Khanna, C. L., Yamamoto, T., Mackey, D. A., Roos, B. R., Affatigato, L. M.,
Sheffield, V. C. & Stone, E. M. (2003). Evaluation of optineurin sequence
variations in 1,048 patients with open-angle glaucoma. Am J Ophthalmol. 136: 904-
910.
Ambati, J., Ambati, B. K., Yoo, S. H., Ianchulev, S. & Adamis, A. P. (2003). Age-related
macular degeneration: etiology, pathogenesis, and therapeutic strategies. Surv
Ophthalmol. 48: 257-293.
Anderson, D. H., Mullins, R. F., Hageman, G. S. & Johnson, L. V. (2002). A role for local
inflammation in the formation of drusen in the aging eye. Am J Ophthalmol. 134:
411-431.
Anderson, D. H., Radeke, M. J., Gallo, N. B., Chapin, E. A., Johnson, P. T., Curletti, C.
R., Hancox, L. S., Hu, J., Ebright, J. N., Malek, G., Hauser, M. A., Rickman, C. B.,
Bok, D., Hageman, G. S. & Johnson, L. V. (2010). The pivotal role of the
complement system in aging and age-related macular degeneration: hypothesis re-
visited. Prog Retin Eye Res. 29: 95-112.

149
Apte, R. S., Richter, J., Herndon, J. & Ferguson, T. A. (2006). Macrophages inhibit
neovascularization in a murine model of age-related macular degeneration. PLoS
Med. 3: e310.
Arakawa, S., Takahashi, A., Ashikawa, K., Hosono, N., Aoi, T., Yasuda, M., Oshima, Y.,
Yoshida, S., Enaida, H., Tsuchihashi, T., Mori, K., Honda, S., Negi, A., Arakawa,
A., Kadonosono, K., Kiyohara, Y., Kamatani, N., Nakamura, Y., Ishibashi, T. &
Kubo, M. (2011). Genome-wide association study identifies two susceptibility loci
for exudative age-related macular degeneration in the Japanese population. Nat
Genet. 43: 1001-1004.
Arthur, L. & Jan, J. (2005). Atlas of Ophthalmology, London, World Scientific Publishers.
Aung, T., Lim, M. C., Wong, T. T., Thalamuthu, A., Yong, V. H., Venkataraman, D.,
Venkatraman, A., Chew, P. T. & Vithana, E. N. (2008). Molecular analysis of
CHX10 and MFRP in Chinese subjects with primary angle closure glaucoma and
short axial length eyes. Mol Vis. 14: 1313-1318.
Aung, T., Ocaka, L., Ebenezer, N. D., Morris, A. G., Krawczak, M., Thiselton, D. L.,
Alexander, C., Votruba, M., Brice, G., Child, A. H., Francis, P. J., Hitchings, R. A.,
Lehmann, O. J. & Bhattacharya, S. S. (2002). A major marker for normal tension
glaucoma: association with polymorphisms in the OPA1 gene. Hum Genet. 110:
52-56.
Awadalla, M. S., Burdon, K. P., Kuot, A., Hewitt, A. W. & Craig, J. E. (2011a). Matrix
metalloproteinase-9 genetic variation and primary angle closure glaucoma in a
Caucasian population. Mol Vis. 17: 1420-1424.
Awadalla, M. S., Thapa, S. S., Burdon, K. P., Hewitt, A. W. & Craig, J. E. (2011b). The
association of hepatocyte growth factor (HGF) gene with primary angle closure
glaucoma in the Nepalese population. Mol Vis. 17: 2248-2254.
Awadalla, M. S., Thapa, S. S., Hewitt, A. W., Craig, J. E. & Burdon, K. P. (2013).
Association of eNOS polymorphisms with primary angle-closure glaucoma. Invest
Ophthalmol Vis Sci. 54: 2108-2114.
Awata, T., Neda, T., Iizuka, H., Kurihara, S., Ohkubo, T., Takata, N., Osaki, M., Watanabe,
M., Nakashima, Y., Sawa, T., Inukai, K., Inoue, I., Shibuya, M., Mori, K., Yoneya,
S. & Katayama, S. (2004). Endothelial nitric oxide synthase gene is associated with
diabetic macular edema in type 2 diabetes. Diabetes Care. 27: 2184-2190.
Ayala-Lugo, R. M., Pawar, H., Reed, D. M., Lichter, P. R., Moroi, S. E., Page, M., Eadie,
J., Azocar, V., Maul, E., Ntim-Amponsah, C., Bromley, W., Obeng-Nyarkoh, E.,
Johnson, A. T., Kijek, T. G., Downs, C. A., Johnson, J. M., Perez-Grossmann, R.
A., Guevara-Fujita, M. L., Fujita, R., Wallace, M. R. & Richards, J. E. (2007).

150
Variation in optineurin (OPTN) allele frequencies between and within populations.
Mol Vis. 13: 151-163.
Ayub, H., Khan, M. I., Micheal, S., Akhtar, F., Ajmal, M., Shafique, S., Ali, S. H., Den
Hollander, A. I., Ahmed, A. & Qamar, R. (2010). Association of eNOS and HSP70
gene polymorphisms with glaucoma in Pakistani cohorts. Mol Vis. 16: 18-25.
Azmanov, D. N., Dimitrova, S., Florez, L., Cherninkova, S., Draganov, D., Morar, B., Saat,
R., Juan, M., Arostegui, J. I., Ganguly, S., Soodyall, H., Chakrabarti, S., Padh, H.,
Lopez-Nevot, M. A., Chernodrinska, V., Anguelov, B., Majumder, P., Angelova,
L., Kaneva, R., Mackey, D. A., Tournev, I. & Kalaydjieva, L. (2011). LTBP2 and
CYP1B1 mutations and associated ocular phenotypes in the Roma/Gypsy founder
population. Eur J Hum Genet. 19: 326-333.
Baird, P. N., Craig, J. E., Richardson, A. J., Ring, M. A., Sim, P., Stanwix, S., Foote, S. J.
& Mackey, D. A. (2003). Analysis of 15 primary open-angle glaucoma families
from Australia identifies a founder effect for the Q368STOP mutation of myocilin.
Hum Genet. 112: 110-116.
Baird, P. N., Foote, S. J., Mackey, D. A., Craig, J., Speed, T. P. & Bureau, A. (2005).
Evidence for a novel glaucoma locus at chromosome 3p21-22. Hum Genet. 117:
249-257.
Baird, P. N., Richardson, A. J., Robman, L. D., Dimitrov, P. N., Tikellis, G., Mccarty, C.
A. & Guymer, R. H. (2006). Apolipoprotein (APOE) gene is associated with
progression of age-related macular degeneration (AMD). Hum Mutat. 27: 337-342.
Baker, S., Booth, C., Fillman, C., Shapiro, M., Blair, M. P., Hyland, J. C. & Ala-Kokko,
L. (2011). A loss of function mutation in the COL9A2 gene causes autosomal
recessive Stickler syndrome. Am J Med Genet A. 155A: 1668-1672.
Balligand, J. L., Feron, O. & Dessy, C. (2009). eNOS activation by physical forces: from
short-term regulation of contraction to chronic remodeling of cardiovascular
tissues. Physiol Rev. 89: 481-534.
Beatty, S., Koh, H., Phil, M., Henson, D. & Boulton, M. (2000). The role of oxidative stress
in the pathogenesis of age-related macular degeneration. Surv Ophthalmol. 45: 115-
134.
Beckman, J. S., Beckman, T. W., Chen, J., Marshall, P. A. & Freeman, B. A. (1990).
Apparent hydroxyl radical production by peroxynitrite: implications for endothelial
injury from nitric oxide and superoxide. Proc Natl Acad Sci U S A. 87: 1620-1624.
Beers, A. P. & Van Der Heijde, G. L. (1994). In vivo determination of the biomechanical
properties of the component elements of the accommodation mechanism. Vision
Res. 34: 2897-2905.

151
Behndig, A., Svensson, B., Marklund, S. L. & Karlsson, K. (1998). Superoxide dismutase
isoenzymes in the human eye. Invest Ophthalmol Vis Sci. 39: 471-475.
Beier, K. & Fahimi, H. D. (1985). Automatic determination of labeling density in protein
A-gold immunocytochemical preparations using an image analyzer. Application to
peroxisomal enzymes. Histochemistry. 82: 99-100.
Bejjani, B. A., Stockton, D. W., Lewis, R. A., Tomey, K. F., Dueker, D. K., Jabak, M.,
Astle, W. F. & Lupski, J. R. (2000). Multiple CYP1B1 mutations and incomplete
penetrance in an inbred population segregating primary congenital glaucoma
suggest frequent de novo events and a dominant modifier locus. Hum Mol Genet.
9: 367-374.
Bellander, B. M., Bendel, O., Von Euler, G., Ohlsson, M. & Svensson, M. (2004).
Activation of microglial cells and complement following traumatic injury in rat
entorhinal-hippocampal slice cultures. J Neurotrauma. 21: 605-615.
Bhutto, I. A., Baba, T., Merges, C., Mcleod, D. S. & Lutty, G. A. (2010). Low nitric oxide
synthases (NOSs) in eyes with age-related macular degeneration (AMD). Exp Eye
Res. 90: 155-167.
Bird, A. C., Bressler, N. M., Bressler, S. B., Chisholm, I. H., Coscas, G., Davis, M. D., De
Jong, P. T., Klaver, C. C., Klein, B. E., Klein, R. & Et Al. (1995). An international
classification and grading system for age-related maculopathy and age-related
macular degeneration. The International ARM Epidemiological Study Group. Surv
Ophthalmol. 39: 367-374.
Birkedal-Hansen, H., Moore, W. G., Bodden, M. K., Windsor, L. J., Birkedal-Hansen, B.,
Decarlo, A. & Engler, J. A. (1993). Matrix metalloproteinases: a review. Crit Rev
Oral Biol Med. 4: 197-250.
Bonnel, S., Mohand-Said, S. & Sahel, J. A. (2003). The aging of the retina. Exp Gerontol.
38: 825-831.
Borish, E. T., Pryor, W. A., Venugopal, S. & Deutsch, W. A. (1987). DNA synthesis is
blocked by cigarette tar-induced DNA single-strand breaks. Carcinogenesis. 8:
1517-1520.
Bruce, A., Alexander, J., Julian, L., Martin, R., Keith, R. & Peter, W. (2007). Molecular
Biology of the Cell, New York, Garland Science.
Buckingham, B. P., Inman, D. M., Lambert, W., Oglesby, E., Calkins, D. J., Steele, M. R.,
Vetter, M. L., Marsh-Armstrong, N. & Horner, P. J. (2008). Progressive ganglion
cell degeneration precedes neuronal loss in a mouse model of glaucoma. J
Neurosci. 28: 2735-2744.

152
Burgoyne, C. F., Quigley, H. A., Thompson, H. W., Vitale, S. & Varma, R. (1995). Early
changes in optic disc compliance and surface position in experimental glaucoma.
Ophthalmology. 102: 1800-1809.
Cai, J., Nelson, K. C., Wu, M., Sternberg, P., Jr. & Jones, D. P. (2000). Oxidative damage
and protection of the RPE. Prog Retin Eye Res. 19: 205-221.
Campochiaro, P. A. (2004). Ocular neovascularisation and excessive vascular
permeability. Expert Opin Biol Ther. 4: 1395-1402.
Cano, M., Thimmalappula, R., Fujihara, M., Nagai, N., Sporn, M., Wang, A. L., Neufeld,
A. H., Biswal, S. & Handa, J. T. (2010). Cigarette smoking, oxidative stress, the
anti-oxidant response through Nrf2 signaling, and Age-related Macular
Degeneration. Vision Res. 50: 652-664.
Cao, S., Ko, A., Partanen, M., Pakzad-Vaezi, K., Merkur, A. B., Albiani, D. A., Kirker, A.
W., Wang, A., Cui, J. Z., Forooghian, F. & Matsubara, J. A. (2013). Relationship
between systemic cytokines and complement factor H Y402H polymorphism in
patients with dry age-related macular degeneration. Am J Ophthalmol. 156: 1176-
1183.
Carbone, M. A., Chen, Y., Hughes, G. A., Weinreb, R. N., Zabriskie, N. A., Zhang, K. &
Anholt, R. R. (2011). Genes of the unfolded protein response pathway harbor risk
alleles for primary open angle glaucoma. PLoS One. 6: e20649.
Center, P. (2007). Glaucoma Medical Therapy : Principles and Management, New York,
Oxford University Press.
Chakrabarti, S., Ghanekar, Y., Kaur, K., Kaur, I., Mandal, A. K., Rao, K. N., Parikh, R. S.,
Thomas, R. & Majumder, P. P. (2010). A polymorphism in the CYP1B1 promoter
is functionally associated with primary congenital glaucoma. Hum Mol Genet. 19:
4083-4090.
Challa, P. (2011). Genetics of adult glaucoma. Int Ophthalmol Clin. 51: 37-51.
Charman, W. N. (2008). The eye in focus: accommodation and presbyopia. Clin Exp
Optom. 91: 207-225.
Checchin, D., Sennlaub, F., Levavasseur, E., Leduc, M. & Chemtob, S. (2006). Potential
role of microglia in retinal blood vessel formation. Invest Ophthalmol Vis Sci. 47:
3595-3602.
Chen, H., Yu, K. D. & Xu, G. Z. (2012). Association between variant Y402H in age-related
macular degeneration (AMD) susceptibility gene CFH and treatment response of
AMD: a meta-analysis. PLoS One. 7: e42464.

153
Chen, L. J., Liu, D. T., Tam, P. O., Chan, W. M., Liu, K., Chong, K. K., Lam, D. S. &
Pang, C. P. (2006). Association of complement factor H polymorphisms with
exudative age-related macular degeneration. Mol Vis. 12: 1536-1542.
Chen, R., Gong, B., Li, Q., Zeng, G., Hao, F., Li, N., Shi, Y. & Zhang, D. (2014a).
[Analysis of COL9A2 gene mutations in a Chinese Han population with
pathological myopia]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 31: 129-133.
Chen, W., Stambolian, D., Edwards, A. O., Branham, K. E., Othman, M., Jakobsdottir, J.,
Tosakulwong, N., Pericak-Vance, M. A., Campochiaro, P. A., Klein, M. L., Tan,
P. L., Conley, Y. P., Kanda, A., Kopplin, L., Li, Y., Augustaitis, K. J., Karoukis,
A. J., Scott, W. K., Agarwal, A., Kovach, J. L., Schwartz, S. G., Postel, E. A.,
Brooks, M., Baratz, K. H., Brown, W. L., Brucker, A. J., Orlin, A., Brown, G., Ho,
A., Regillo, C., Donoso, L., Tian, L., Kaderli, B., Hadley, D., Hagstrom, S. A.,
Peachey, N. S., Klein, R., Klein, B. E., Gotoh, N., Yamashiro, K., Ferris Iii, F.,
Fagerness, J. A., Reynolds, R., Farrer, L. A., Kim, I. K., Miller, J. W., Corton, M.,
Carracedo, A., Sanchez-Salorio, M., Pugh, E. W., Doheny, K. F., Brion, M.,
Deangelis, M. M., Weeks, D. E., Zack, D. J., Chew, E. Y., Heckenlively, J. R.,
Yoshimura, N., Iyengar, S. K., Francis, P. J., Katsanis, N., Seddon, J. M., Haines,
J. L., Gorin, M. B., Abecasis, G. R. & Swaroop, A. (2010a). Genetic variants near
TIMP3 and high-density lipoprotein-associated loci influence susceptibility to age-
related macular degeneration. Proc Natl Acad Sci U S A. 107: 7401-7406.
Chen, Y., Bedell, M. & Zhang, K. (2010b). Age-related macular degeneration: genetic and
environmental factors of disease. Mol Interv. 10: 271-281.
Chen, Y., Chen, X., Wang, L., Hughes, G., Qian, S. & Sun, X. (2014b). Extended
association study of PLEKHA7 and COL11A1 with primary angle closure
glaucoma in a Han Chinese population. Invest Ophthalmol Vis Sci. 55: 3797-3802.
Chintala, S. K., Zhang, X., Austin, J. S. & Fini, M. E. (2002). Deficiency in matrix
metalloproteinase gelatinase B (MMP-9) protects against retinal ganglion cell death
after optic nerve ligation. J Biol Chem. 277: 47461-47468.
Churchill, A.J., Carter, J.G., Ramsden, C., Turner, S.J., Yeung, A., Brenchley, P.E., Ray,
D.W. (2008). “VEGF polymorphisms are associated with severity of diabetic
retinopathy”. Invest Ophthal Vis Sci. 49:3611-3616.
Coleman, A. L. (1999). Glaucoma. Lancet. 354: 1803-1810.
Coleman, H. R., Chan, C. C., Ferris, F. L., 3rd & Chew, E. Y. (2008). Age-related macular
degeneration. Lancet. 372: 1835-1845.
Combadiere, C., Feumi, C., Raoul, W., Keller, N., Rodero, M., Pezard, A., Lavalette, S.,
Houssier, M., Jonet, L., Picard, E., Debre, P., Sirinyan, M., Deterre, P., Ferroukhi,
T., Cohen, S. Y., Chauvaud, D., Jeanny, J. C., Chemtob, S., Behar-Cohen, F. &

154
Sennlaub, F. (2007). CX3CR1-dependent subretinal microglia cell accumulation is
associated with cardinal features of age-related macular degeneration. J Clin Invest.
117: 2920-2928.
Cook, C. & Foster, P. (2012). Epidemiology of glaucoma: what's new? Can J Ophthalmol.
47: 223-226.
Cook, C. (2009). Glaucoma in Africa: size of the problem and possible solutions. J
Glaucoma. 18: 124-128.
Copin, B., Brezin, A. P., Valtot, F., Dascotte, J. C., Bechetoille, A. & Garchon, H. J. (2002).
Apolipoprotein E-promoter single-nucleotide polymorphisms affect the phenotype
of primary open-angle glaucoma and demonstrate interaction with the myocilin
gene. Am J Hum Genet. 70: 1575-1581.
Craig, J. E., Hewitt, A. W., Dimasi, D. P., Howell, N., Toomes, C., Cohn, A. C. & Mackey,
D. A. (2006). The role of the Met98Lys optineurin variant in inherited optic nerve
diseases. Br J Ophthalmol. 90: 1420-1424.
Curcio, C. A. & Millican, C. L. (1999). Basal linear deposit and large drusen are specific
for early age-related maculopathy. Arch Ophthalmol. 117: 329-339.
Curcio, C. A., Johnson, M., Huang, J. D. & Rudolf, M. (2009). Aging, age-related macular
degeneration, and the response-to-retention of apolipoprotein B-containing
lipoproteins. Prog Retin Eye Res. 28: 393-422.
Curcio, C. A., Johnson, M., Huang, J. D. & Rudolf, M. (2010). Apolipoprotein B-
containing lipoproteins in retinal aging and age-related macular degeneration. J
Lipid Res. 51: 451-467.
Dandona, L., Williams, J. D., Williams, B. C. & Rao, G. N. (1998). Population-based
assessment of childhood blindness in southern India. Arch Ophthalmol. 116: 545-
546.
Das, A. & Mcguire, P. G. (2003). Retinal and choroidal angiogenesis: pathophysiology and
strategies for inhibition. Prog Retin Eye Res. 22: 721-748.
Daugherty, C. L., Curtis, H., Realini, T., Charlton, J. F. & Zareparsi, S. (2009). Primary
open angle glaucoma in a Caucasian population is associated with the p53 codon
72 polymorphism. Mol Vis. 15: 1939-1944.
Davis, M. D., Gangnon, R. E., Lee, L. Y., Hubbard, L. D., Klein, B. E., Klein, R., Ferris,
F. L., Bressler, S. B. & Milton, R. C. (2005). The Age-Related Eye Disease Study
severity scale for age-related macular degeneration: AREDS Report No. 17. Arch
Ophthalmol. 123: 1484-1498.

155
De Jong, P. T. (2006). Age-related macular degeneration. N Engl J Med. 355: 1474-1485.
Deangelis, M. M., Silveira, A. C., Carr, E. A. & Kim, I. K. (2011). Genetics of age-related
macular degeneration: current concepts, future directions. Semin Ophthalmol. 26:
77-93.
Dibas, A., Yang, M. H., He, S., Bobich, J. & Yorio, T. (2008). Changes in ocular
aquaporin-4 (AQP4) expression following retinal injury. Mol Vis. 14: 1770-1783.
Dimasi, D. P., Hewitt, A. W., Green, C. M., Mackey, D. A. & Craig, J. E. (2005). Lack of
association of p53 polymorphisms and haplotypes in high and normal tension open
angle glaucoma. J Med Genet. 42: e55.
Ding, X., Patel, M. & Chan, C. C. (2009). Molecular pathology of age-related macular
degeneration. Prog Retin Eye Res. 28: 1-18.
Distelhorst, J. S. & Hughes, G. M. (2003). Open-angle glaucoma. Am Fam Physician. 67:
1937-1944.
Donoso, L. A., Kim, D., Frost, A., Callahan, A. & Hageman, G. (2006). The role of
inflammation in the pathogenesis of age-related macular degeneration. Surv
Ophthalmol. 51: 137-152.
Drance, S. M. (2008). What can we learn from the disc appearance about the risk factors
in glaucoma? Can J Ophthalmol. 43: 322-327.
Dunaief, J. L., Dentchev, T., Ying, G. S. & Milam, A. H. (2002). The role of apoptosis in
age-related macular degeneration. Arch Ophthalmol. 120: 1435-1442.
Durand, M., Kolpak, A., Farrell, T., Elliott, N. A., Shao, W., Brown, M. & Volkert, M. R.
(2007). The OXR domain defines a conserved family of eukaryotic oxidation
resistance proteins. BMC Cell Biol. 8: 13.
Duvesh, R., Verma, A., Venkatesh, R., Kavitha, S., Ramulu, P. Y., Wojciechowski, R. &
Sundaresan, P. (2013). Association study in a South Indian population supports
rs1015213 as a risk factor for primary angle closure. Invest Ophthalmol Vis Sci. 54:
5624-5628.
Eagle, R. C. (2012). Eye Pathology: An Atlas and Text, Philadelphia Wolters Kluwer
Health.
Edwards, A. O., Ritter, R., 3rd, Abel, K. J., Manning, A., Panhuysen, C. & Farrer, L. A.
(2005). Complement factor H polymorphism and age-related macular degeneration.
Science. 308: 421-424.

156
Ehrlich, R., Harris, A., Kheradiya, N. S., Winston, D. M., Ciulla, T. A. & Wirostko, B.
(2008). Age-related macular degeneration and the aging eye. Clin Interv Aging. 3:
473-482.
Ergorul, C., Ray, A., Huang, W., Wang, D. Y., Ben, Y., Cantuti-Castelvetri, I. &
Grosskreutz, C. L. (2010). Hypoxia inducible factor-1alpha (HIF-1alpha) and some
HIF-1 target genes are elevated in experimental glaucoma. J Mol Neurosci. 42: 183-
191.
Fagerness, J. A., Maller, J. B., Neale, B. M., Reynolds, R. C., Daly, M. J. & Seddon, J. M.
(2009). Variation near complement factor I is associated with risk of advanced
AMD. Eur J Hum Genet. 17: 100-104.
Fan, B. J., Leung, Y. F., Wang, N., Lam, S. C., Liu, Y., Tam, O. S. & Pang, C. P. (2004).
Genetic and environmental risk factors for primary open-angle glaucoma. Chin
Med J (Engl). 117: 706-710.
Fan, B. J., Wang, D. Y., Lam, D. S. & Pang, C. P. (2006). Gene mapping for primary open
angle glaucoma. Clin Biochem. 39: 249-258.
Faucher, M., Anctil, J. L., Rodrigue, M. A., Duchesne, A., Bergeron, D., Blondeau, P.,
Cote, G., Dubois, S., Bergeron, J., Arseneault, R., Morissette, J. & Raymond, V.
(2002). Founder TIGR/myocilin mutations for glaucoma in the Quebec population.
Hum Mol Genet. 11: 2077-2090.
Faucher, M., Anctil, J. L., Rodrigue, M. A., Duchesne, A., Bergeron, D., Blondeau, P.,
Cote, G., Dubois, S., Bergeron, J., Arseneault, R., Morissette, J. & Raymond, V.
(2002). Founder TIGR/myocilin mutations for glaucoma in the Quebec population.
Hum Mol Genet. 11: 2077-2090.
Feero, W. G., Guttmacher, A. E. & Collins, F. S. (2008). The genome gets personal--
almost. JAMA. 299: 1351-1352.
Ferguson, T. A., Dube, P. & Griffith, T. S. (1994). Regulation of contact hypersensitivity
by interleukin 10. J Exp Med. 179: 1597-1604.
Ferreira, S. M., Lerner, S. F., Brunzini, R., Evelson, P. A. & Llesuy, S. F. (2004). Oxidative
stress markers in aqueous humor of glaucoma patients. Am J Ophthalmol. 137: 62-
69.
Ferris, F. L., 3rd, Fine, S. L. & Hyman, L. (1984). Age-related macular degeneration and
blindness due to neovascular maculopathy. Arch Ophthalmol. 102: 1640-1642.

157
Fingert, J. H., Heon, E., Liebmann, J. M., Yamamoto, T., Craig, J. E., Rait, J., Kawase, K.,
Hoh, S. T., Buys, Y. M., Dickinson, J., Hockey, R. R., Williams-Lyn, D., Trope,
G., Kitazawa, Y., Ritch, R., Mackey, D. A., Alward, W. L., Sheffield, V. C. &
Stone, E. M. (1999). Analysis of myocilin mutations in 1703 glaucoma patients
from five different populations. Hum Mol Genet. 8: 899-905.
Fingert, J. H., Robin, A. L., Stone, J. L., Roos, B. R., Davis, L. K., Scheetz, T. E., Bennett,
S. R., Wassink, T. H., Kwon, Y. H., Alward, W. L., Mullins, R. F., Sheffield, V. C.
& Stone, E. M. (2011). Copy number variations on chromosome 12q14 in patients
with normal tension glaucoma. Hum Mol Genet. 20: 2482-2494.
Fingert, J. H., Alward, W. L. M., Kwon, Y. H., Shankar, S. P., Andorf, J. L., Mackey, D.
A., Sheffield, V. C., Stone, E. M. (2007). No association between variations in the
WDR36 gene and primary open-angle glaucoma. Arch. Ophthal. 125: 434-436.
Firasat, S., Riazuddin, S. A., Hejtmancik, J. F. & Riazuddin, S. (2008). Primary congenital
glaucoma localizes to chromosome 14q24.2-24.3 in two consanguineous Pakistani
families. Mol Vis. 14: 1659-1665.
Firasat, S., Riazuddin, S. A., Khan, S. N. & Riazuddin, S. (2008). Novel CYP1B1
mutations in consanguineous Pakistani families with primary congenital glaucoma.
Mol Vis. 14: 2002-2009.
Fletcher, A. E., Bentham, G. C., Agnew, M., Young, I. S., Augood, C., Chakravarthy, U.,
De Jong, P. T., Rahu, M., Seland, J., Soubrane, G., Tomazzoli, L., Topouzis, F.,
Vingerling, J. R. & Vioque, J. (2008). Sunlight exposure, antioxidants, and age-
related macular degeneration. Arch Ophthalmol. 126: 1396-1403.
Footz, T. K., Johnson, J. L., Dubois, S., Boivin, N., Raymond, V., Walter, M. A. (2009).
Glaucoma-associated WDR36 variants encode functional defects in a yeast model
system. Hum. Molec. Genet. 18: 1276-1287.
Francis, P. J. & Klein, M. L. (2011). Update on the role of genetics in the onset of age-
related macular degeneration. Clin Ophthalmol. 5: 1127-1133.
Frank, H. A. (1996). Structural determinations and spectroscopic studies of carotenoids
reveal the factors important in controlling their function in biological systems. Eur
J Clin Nutr. 50 Suppl 3: S13-16.
Fraser, S. & Manvikar, S. (2005). Glaucoma- the pathophysiology and diagnosis.
Glaucoma- the pathophysiology and diagnosis. 12: 4.
Fritsche, L. G., Chen, W., Schu, M., Yaspan, B. L., Yu, Y., Thorleifsson, G., Zack, D. J.,
Arakawa, S., Cipriani, V., Ripke, S., Igo, R. P., Jr., Buitendijk, G. H., Sim, X.,
Weeks, D. E., Guymer, R. H., Merriam, J. E., Francis, P. J., Hannum, G., Agarwal,
A., Armbrecht, A. M., Audo, I., Aung, T., Barile, G. R., Benchaboune, M., Bird,

158
A. C., Bishop, P. N., Branham, K. E., Brooks, M., Brucker, A. J., Cade, W. H.,
Cain, M. S., Campochiaro, P. A., Chan, C. C., Cheng, C. Y., Chew, E. Y., Chin, K.
A., Chowers, I., Clayton, D. G., Cojocaru, R., Conley, Y. P., Cornes, B. K., Daly,
M. J., Dhillon, B., Edwards, A. O., Evangelou, E., Fagerness, J., Ferreyra, H. A.,
Friedman, J. S., Geirsdottir, A., George, R. J., Gieger, C., Gupta, N., Hagstrom, S.
A., Harding, S. P., Haritoglou, C., Heckenlively, J. R., Holz, F. G., Hughes, G.,
Ioannidis, J. P., Ishibashi, T., Joseph, P., Jun, G., Kamatani, Y., Katsanis, N., C, N.
K., Khan, J. C., Kim, I. K., Kiyohara, Y., Klein, B. E., Klein, R., Kovach, J. L.,
Kozak, I., Lee, C. J., Lee, K. E., Lichtner, P., Lotery, A. J., Meitinger, T., Mitchell,
P., Mohand-Said, S., Moore, A. T., Morgan, D. J., Morrison, M. A., Myers, C. E.,
Naj, A. C., Nakamura, Y., Okada, Y., Orlin, A., Ortube, M. C., Othman, M. I.,
Pappas, C., Park, K. H., Pauer, G. J., Peachey, N. S., Poch, O., Priya, R. R.,
Reynolds, R., Richardson, A. J., Ripp, R., Rudolph, G., Ryu, E., Sahel, J. A.,
Schaumberg, D. A., Scholl, H. P., Schwartz, S. G., Scott, W. K., Shahid, H.,
Sigurdsson, H., Silvestri, G., Sivakumaran, T. A., Smith, R. T., Sobrin, L., Souied,
E. H., Stambolian, D. E., Stefansson, H., Sturgill-Short, G. M., Takahashi, A.,
Tosakulwong, N., Truitt, B. J., Tsironi, E. E., Uitterlinden, A. G., Van Duijn, C.
M., Vijaya, L., Vingerling, J. R., Vithana, E. N., Webster, A. R., Wichmann, H. E.,
Winkler, T. W., Wong, T. Y., Wright, A. F., Zelenika, D., Zhang, M., Zhao, L.,
Zhang, K., Klein, M. L., Hageman, G. S., Lathrop, G. M., Stefansson, K.,
Allikmets, R., Baird, P. N., Gorin, M. B., Wang, J. J., Klaver, C. C., Seddon, J. M.,
Pericak-Vance, M. A., Iyengar, S. K., Yates, J. R., Swaroop, A., Weber, B. H.,
Kubo, M., Deangelis, M. M., Leveillard, T., Thorsteinsdottir, U., Haines, J. L.,
Farrer, L. A., Heid, I. M. & Abecasis, G. R. (2013). Seven new loci associated with
age-related macular degeneration. Nat Genet. 45: 433-439, 439e431-432.
Fritsche, L. G., Loenhardt, T., Janssen, A., Fisher, S. A., Rivera, A., Keilhauer, C. N. &
Weber, B. H. (2008). Age-related macular degeneration is associated with an
unstable ARMS2 (LOC387715) mRNA. Nat Genet. 40: 892-896.
Fujiwara, N., Matsuo, T. & Ohtsuki, H. (2003). Protein expression, genomic structure, and
polymorphisms of oculomedin. Ophthalmic Genet. 24: 141-151.
Funayama, T., Mashima, Y., Ohtake, Y., Ishikawa, K., Fuse, N., Yasuda, N., Fukuchi, T.,
Murakami, A., Hotta, Y. & Shimada, N. (2006). SNPs and interaction analyses of
noelin 2, myocilin, and optineurin genes in Japanese patients with open-angle
glaucoma. Invest Ophthalmol Vis Sci. 47: 5368-5375.
Fung, H. C., Chen, C. M., Wu, Y. R., Hsu, W. C., Ro, L. S., Lin, J. C., Chang, K. H., Wang,
H. K., Lin, S. J., Chan, H., Lin, Y. Y., Wei, S. L., Hsu, Y., Hwang, J. C., Tung, L.
C. & Lee-Chen, G. J. (2005). Heat shock protein 70 and tumor necrosis factor alpha
in Taiwanese patients with dementia. Dement Geriatr Cogn Disord. 20: 1-7.
Fuse, N. (2010). Genetic bases for glaucoma. Tohoku J Exp Med. 221: 1-10.

159
Fuse, N., Miyazawa, A., Mengkegale, M., Yoshida, M., Wakusawa, R., Abe, T. & Tamai,
M. (2006). Polymorphisms in Complement Factor H and Hemicentin-1 genes in a
Japanese population with dry-type age-related macular degeneration. Am J
Ophthalmol. 142: 1074-1076.
Fuse, N., Takahashi, K., Akiyama, H., Nakazawa, T., Seimiya, M., Kuwahara, S. & Tamai,
M. (2004). Molecular genetic analysis of optineurin gene for primary open-angle
and normal tension glaucoma in the Japanese population. J Glaucoma. 13: 299-
303.
Gabelt, B. T. & Kaufman, P. L. (2005). Changes in aqueous humor dynamics with age and
glaucoma. Prog Retin Eye Res. 24: 612-637.
Gabelt, B. T., Gottanka, J., Lutjen-Drecoll, E. & Kaufman, P. L. (2003). Aqueous humor
dynamics and trabecular meshwork and anterior ciliary muscle morphologic
changes with age in rhesus monkeys. Invest Ophthalmol Vis Sci. 44: 2118-2125.
Gaillard, E. R., Atherton, S. J., Eldred, G. & Dillon, J. (1995). Photophysical studies on
human retinal lipofuscin. Photochem Photobiol. 61: 448-453.
Galassi, F., Renieri, G., Sodi, A., Ucci, F., Vannozzi, L. & Masini, E. (2004). Nitric oxide
proxies and ocular perfusion pressure in primary open angle glaucoma. Br J
Ophthalmol. 88: 757-760.
Gelinas, D. S., Bernatchez, P. N., Rollin, S., Bazan, N. G. & Sirois, M. G. (2002).
Immediate and delayed VEGF-mediated NO synthesis in endothelial cells: role of
PI3K, PKC and PLC pathways. Br J Pharmacol. 137: 1021-1030.
Gemenetzi, M., Yang, Y. & Lotery, A. J. (2012). Current concepts on primary open-angle
glaucoma genetics: a contribution to disease pathophysiology and future treatment.
Eye (Lond). 26: 355-369.
Gencik, A. (1989). Epidemiology and genetics of primary congenital glaucoma in
Slovakia. Description of a form of primary congenital glaucoma in gypsies with
autosomal-recessive inheritance and complete penetrance. Dev Ophthalmol. 16: 76-
115.
Gencik, A., Gencikova, A. & Ferak, V. (1982). Population genetical aspects of primary
congenital glaucoma. I. Incidence, prevalence, gene frequency, and age of onset.
Hum Genet. 61: 193-197.
Godley, B. F., Shamsi, F. A., Liang, F. Q., Jarrett, S. G., Davies, S. & Boulton, M. (2005).
Blue light induces mitochondrial DNA damage and free radical production in
epithelial cells. J Biol Chem. 280: 21061-21066.
Gold, B., Merriam, J. E., Zernant, J., Hancox, L. S., Taiber, A. J., Gehrs, K., Cramer, K.,
Neel, J., Bergeron, J., Barile, G. R., Smith, R. T., Hageman, G. S., Dean, M. &

160
Allikmets, R. (2006). Variation in factor B (BF) and complement component 2 (C2)
genes is associated with age-related macular degeneration. Nat Genet. 38: 458-462.
Gottanka, J., Johnson, D. H., Martus, P. & Lutjen-Drecoll, E. (1997). Severity of optic
nerve damage in eyes with POAG is correlated with changes in the trabecular
meshwork. J Glaucoma. 6: 123-132.
Gravina, S., Lescai, F., Hurteau, G., Brock, G. J., Saramaki, A., Salvioli, S., Franceschi, C.
& Roninson, I. B. (2009). Identification of single nucleotide polymorphisms in the
p21 (CDKN1A) gene and correlations with longevity in the Italian population.
Aging (Albany NY). 1: 470-480.
Green, W. R. & Enger, C. (2005). Age-related macular degeneration histopathologic
studies: the 1992 Lorenz E. Zimmerman Lecture. 1992. Retina. 25: 1519-1535.
Gruber, H. J., Bernecker, C., Lechner, A., Weiss, S., Wallner-Blazek, M., Meinitzer, A.,
Hobarth, G., Renner, W., Fauler, G., Horejsi, R., Fazekas, F. & Truschnig-Wilders,
M. (2010). Increased nitric oxide stress is associated with migraine. Cephalalgia.
30: 486-492.
Haass, C., Hung, A. Y. & Selkoe, D. J. (1991). Processing of beta-amyloid precursor
protein in microglia and astrocytes favors an internal localization over constitutive
secretion. J Neurosci. 11: 3783-3793.
Hageman, G. S. & Mullins, R. F. (1999). Molecular composition of drusen as related to
substructural phenotype. Mol Vis. 5: 28.
Hall, S. K., Perregaux, D. G., Gabel, C. A., Woodworth, T., Durham, L. K., Huizinga, T.
W., Breedveld, F. C. & Seymour, A. B. (2004). Correlation of polymorphic
variation in the promoter region of the interleukin-1 beta gene with secretion of
interleukin-1 beta protein. Arthritis Rheum. 50: 1976-1983.
Harendza, S., Lovett, D. H., Panzer, U., Lukacs, Z., Kuhnl, P. & Stahl, R. A. (2003). Linked
common polymorphisms in the gelatinase a promoter are associated with
diminished transcriptional response to estrogen and genetic fitness. J Biol Chem.
278: 20490-20499.
Hashizume, K., Mashima, Y., Fumayama, T., Ohtake, Y., Kimura, I., Yoshida, K.,
Ishikawa, K., Yasuda, N., Fujimaki, T., Asaoka, R., Koga, T., Kanamoto, T.,
Fukuchi, T. & Miyaki, K. (2005). Genetic polymorphisms in the angiotensin II
receptor gene and their association with open-angle glaucoma in a Japanese
population. Invest Ophthalmol Vis Sci. 46: 1993-2001.
Hayano, T. & Kikuchi, M. (1995). Molecular cloning of the cDNA encoding a novel
protein disulfide isomerase-related protein (PDIR). FEBS Lett. 372: 210-214.

161
He, M., Guo, H., Yang, X., Zhang, X., Zhou, L., Cheng, L., Zeng, H., Hu, F. B., Tanguay,
R. M. & Wu, T. (2009). Functional SNPs in HSPA1A gene predict risk of coronary
heart disease. PLoS One. 4: e4851.
Hernandez, M. R. (2000). The optic nerve head in glaucoma: role of astrocytes in tissue
remodeling. Prog Retin Eye Res. 19: 297-321.
Hewitt, A. W., Craig, J. E. & Mackey, D. A. (2006). Complex genetics of complex traits:
the case of primary open-angle glaucoma. Clin Experiment Ophthalmol. 34: 472-
484.
Heys, J. J., Barocas, V. H. & Taravella, M. J. (2001). Modeling passive mechanical
interaction between aqueous humor and iris. J Biomech Eng. 123: 540-547.
Higashino, K., Matsui, Y., Yagi, S., Takata, Y., Goto, T., Sakai, T., Katoh, S. & Yasui, N.
(2007). The alpha2 type IX collagen tryptophan polymorphism is associated with
the severity of disc degeneration in younger patients with herniated nucleus
pulposus of the lumbar spine. Int Orthop. 31: 107-111.
Hollyfield, J. G., Perez, V. L. & Salomon, R. G. (2010). A hapten generated from an
oxidation fragment of docosahexaenoic acid is sufficient to initiate age-related
macular degeneration. Mol Neurobiol. 41: 290-298.
Holz, F. G., Bindewald-Wittich, A., Fleckenstein, M., Dreyhaupt, J., Scholl, H. P. &
Schmitz-Valckenberg, S. (2007). Progression of geographic atrophy and impact of
fundus autofluorescence patterns in age-related macular degeneration. Am J
Ophthalmol. 143: 463-472.
Holz, F. G., Schutt, F., Kopitz, J., Eldred, G. E., Kruse, F. E., Volcker, H. E. & Cantz, M.
(1999). Inhibition of lysosomal degradative functions in RPE cells by a retinoid
component of lipofuscin. Invest Ophthalmol Vis Sci. 40: 737-743.
Hood, J. D., Meininger, C. J., Ziche, M. & Granger, H. J. (1998). VEGF upregulates ecNOS
message, protein, and NO production in human endothelial cells. Am J Physiol.
274: H1054-1058.
Hsu, R. M., Tsai, M. H., Hsieh, Y. J., Lyu, P. C. & Yu, J. S. (2010). Identification of
MYO18A as a novel interacting partner of the PAK2/betaPIX/GIT1 complex and
its potential function in modulating epithelial cell migration. Mol Biol Cell. 21: 287-
301.
Huang, P., Zhang, S. S. & Zhang, C. (2009). The two sides of cytokine signaling and
glaucomatous optic neuropathy. J Ocul Biol Dis Infor. 2: 78-83.

162
Hulkkonen, J., Laippala, P. & Hurme, M. (2000). A rare allele combination of the
interleukin-1 gene complex is associated with high interleukin-1 beta plasma levels
in healthy individuals. Eur Cytokine Netw. 11: 251-255.
Hussain, R. & Bittles, A. H. (1998). The prevalence and demographic characteristics of
consanguineous marriages in Pakistan. J Biosoc Sci. 30: 261-275.
Inagaki, Y., Mashima, Y., Funayama, T., Ohtake, Y., Fuse, N., Yasuda, N., Fukuchi, T.,
Murakami, A. & Hotta, Y. (2006). Paraoxonase 1 gene polymorphisms influence
clinical features of open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol. 244:
984-990.
Iqbal, Z., Cejudo-Martin, P., De Brouwer, A., Van Der Zwaag, B., Ruiz-Lozano, P.,
Scimia, M. C., Lindsey, J. D., Weinreb, R., Albrecht, B., Megarbane, A., Alanay,
Y., Ben-Neriah, Z., Amenduni, M., Artuso, R., Veltman, J. A., Van Beusekom, E.,
Oudakker, A., Millan, J. L., Hennekam, R., Hamel, B., Courtneidge, S. A. & Van
Bokhoven, H. (2010). Disruption of the podosome adaptor protein TKS4
(SH3PXD2B) causes the skeletal dysplasia, eye, and cardiac abnormalities of
Frank-Ter Haar Syndrome. Am J Hum Genet. 86: 254-261.
Ishii, Y., Kwong, J. M. & Caprioli, J. (2003). Retinal ganglion cell protection with
geranylgeranylacetone, a heat shock protein inducer, in a rat glaucoma model.
Invest Ophthalmol Vis Sci. 44: 1982-1992.
Ishikawa, K., Funayama, T., Ohtake, Y., Kimura, I., Ideta, H., Nakamoto, K., Yasuda, N.,
Fukuchi, T., Fujimaki, T., Murakami, A., Asaoka, R., Hotta, Y., Kanamoto, T.,
Tanihara, H., Miyaki, K. & Mashima, Y. (2005). Association between glaucoma
and gene polymorphism of endothelin type A receptor. Mol Vis. 11: 431-437.
Iwabe, S., Lamas, M., Vasquez Pelaez, C. G. & Carrasco, F. G. (2010). Aqueous humor
endothelin-1 (Et-1), vascular endothelial growth factor (VEGF) and
cyclooxygenase-2 (COX-2) levels in Mexican glaucomatous patients. Curr Eye
Res. 35: 287-294.
Iyengar, S. K., Song, D., Klein, B. E., Klein, R., Schick, J. H., Humphrey, J., Millard, C.,
Liptak, R., Russo, K., Jun, G., Lee, K. E., Fijal, B. & Elston, R. C. (2004).
Dissection of genomewide-scan data in extended families reveals a major locus and
oligogenic susceptibility for age-related macular degeneration. Am J Hum Genet.
74: 20-39.
Izzotti, A., Bagnis, A. & Sacca, S. C. (2006). The role of oxidative stress in glaucoma.
Mutat Res. 612: 105-114.

163
Izzotti, A., Longobardi, M., Cartiglia, C. & Sacca, S. C. (2011). Mitochondrial damage in
the trabecular meshwork occurs only in primary open-angle glaucoma and in
pseudoexfoliative glaucoma. PLoS One. 6: e14567.
Izzotti, A., Sacca, S. C., Cartiglia, C. & De Flora, S. (2003). Oxidative deoxyribonucleic
acid damage in the eyes of glaucoma patients. Am J Med. 114: 638-646.
Jiang, Z., Gorenstein, N. M., Morre, D. M. & Morre, D. J. (2008). Molecular cloning and
characterization of a candidate human growth-related and time-keeping constitutive
cell surface hydroquinone (NADH) oxidase. Biochemistry. 47: 14028-14038.
Johnson, E. C., Deppmeier, L. M., Wentzien, S. K., Hsu, I. & Morrison, J. C. (2000).
Chronology of optic nerve head and retinal responses to elevated intraocular
pressure. Invest Ophthalmol Vis Sci. 41: 431-442.
Johnson, T. V., Fan, S., Camras, C. B. & Toris, C. B. (2008). Aqueous humor dynamics in
exfoliation syndrome. Arch Ophthalmol. 126: 914-920.
Julien, S. & Schraermeyer, U. (2012). Lipofuscin can be eliminated from the retinal
pigment epithelium of monkeys. Neurobiol Aging. 33: 2390-2397.
Junemann, A. G., Von Ahsen, N., Reulbach, U., Roedl, J., Bonsch, D., Kornhuber, J.,
Kruse, F. E. & Bleich, S. (2005). C677T variant in the methylentetrahydrofolate
reductase gene is a genetic risk factor for primary open-angle glaucoma. Am J
Ophthalmol. 139: 721-723.
Juronen, E., Tasa, G., Veromann, S., Parts, L., Tiidla, A., Pulges, R., Panov, A., Soovere,
L., Koka, K. & Mikelsaar, A. V. (2000). Polymorphic glutathione S-transferase M1
is a risk factor of primary open-angle glaucoma among Estonians. Exp Eye Res. 71:
447-452.
Kahn, M. G., Giblin, F. J. & Epstein, D. L. (1983). Glutathione in calf trabecular meshwork
and its relation to aqueous humor outflow facility. Invest Ophthalmol Vis Sci. 24:
1283-1287.
Kakiuchi-Matsumoto, T., Isashiki, Y., Ohba, N., Kimura, K., Sonoda, S. & Unoki, K.
(2001). Cytochrome P450 1B1 gene mutations in Japanese patients with primary
congenital glaucoma. Am J Ophthalmol. 131: 345-350.
Kanda, A., Chen, W., Othman, M., Branham, K. E., Brooks, M., Khanna, R., He, S., Lyons,
R., Abecasis, G. R. & Swaroop, A. (2007). A variant of mitochondrial protein
LOC387715/ARMS2, not HTRA1, is strongly associated with age-related macular
degeneration. Proc Natl Acad Sci U S A. 104: 16227-16232.

164
Kanda, A., Chen, W., Othman, M., Branham, K. E., Brooks, M., Khanna, R., He, S., Lyons,
R., Abecasis, G. R. & Swaroop, A. (2007). A variant of mitochondrial protein
LOC387715/ARMS2, not HTRA1, is strongly associated with age-related macular
degeneration. Proc Natl Acad Sci U S A. 104: 16227-16232.
Karantzoulis-Fegaras, F., Antoniou, H., Lai, S. L., Kulkarni, G., D'abreo, C., Wong, G. K.,
Miller, T. L., Chan, Y., Atkins, J., Wang, Y. & Marsden, P. A. (1999).
Characterization of the human endothelial nitric-oxide synthase promoter. J Biol
Chem. 274: 3076-3093.
Karen, L. (2006). Glaucoma, An insight into disease and therapy, Toronto, Ontario,
Canadian Pharmacists Association.
Kaur, I., Hussain, A., Hussain, N., Das, T., Pathangay, A., Mathai, A., Nutheti, R.,
Nirmalan, P. K. & Chakrabarti, S. (2006). Analysis of CFH, TLR4, and APOE
polymorphism in India suggests the Tyr402His variant of CFH to be a global
marker for age-related macular degeneration. Invest Ophthalmol Vis Sci. 47: 3729-
3735.
Khan, M. I., Micheal, S., Rana, N., Akhtar, F., Den Hollander, A. I., Ahmed, A. & Qamar,
R. (2009). Association of tumor necrosis factor alpha gene polymorphism G-308A
with pseudoexfoliative glaucoma in the Pakistani population. Mol Vis. 15: 2861-
2867.
Kijlstra, A., La Heij, E. & Hendrikse, F. (2005). Immunological factors in the pathogenesis
and treatment of age-related macular degeneration. Ocul Immunol Inflamm. 13: 3-
11.
Kim, I., Xu, W. & Reed, J. C. (2008). Cell death and endoplasmic reticulum stress: disease
relevance and therapeutic opportunities. Nat Rev Drug Discov. 7: 1013-1030.
Kim, S. K., Selleri, L., Lee, J. S., Zhang, A. Y., Gu, X., Jacobs, Y. & Cleary, M. L. (2002).
Pbx1 inactivation disrupts pancreas development and in Ipf1-deficient mice
promotes diabetes mellitus. Nat Genet. 30: 430-435.
Kim, Y. Y. & Jung, H. R. (1997). Clarifying the nomenclature for primary angle-closure
glaucoma. Surv Ophthalmol. 42: 125-136.
Klein, M. L., Schultz, D. W., Edwards, A., Matise, T. C., Rust, K., Berselli, C. B., Trzupek,
K., Weleber, R. G., Ott, J., Wirtz, M. K. & Acott, T. S. (1998). Age-related macular
degeneration. Clinical features in a large family and linkage to chromosome 1q.
Arch Ophthalmol. 116: 1082-1088.
Klein, R. J., Zeiss, C., Chew, E. Y., Tsai, J. Y., Sackler, R. S., Haynes, C., Henning, A. K.,
Sangiovanni, J. P., Mane, S. M., Mayne, S. T., Bracken, M. B., Ferris, F. L., Ott,
J., Barnstable, C. & Hoh, J. (2005). Complement factor H polymorphism in age-
related macular degeneration. Science. 308: 385-389.

165
Klein, R., Klein, B. E., Knudtson, M. D., Meuer, S. M., Swift, M. & Gangnon, R. E. (2007).
Fifteen-year cumulative incidence of age-related macular degeneration: the Beaver
Dam Eye Study. Ophthalmology. 114: 253-262.
Klein, R., Klein, B. E., Knudtson, M. D., Wong, T. Y., Shankar, A. & Tsai, M. Y. (2005a).
Systemic markers of inflammation, endothelial dysfunction, and age-related
maculopathy. Am J Ophthalmol. 140: 35-44.
Ko, M. L., Hu, D. N., Ritch, R. & Sharma, S. C. (2000). The combined effect of brain-
derived neurotrophic factor and a free radical scavenger in experimental glaucoma.
Invest Ophthalmol Vis Sci. 41: 2967-2971.
Konstas, A. G., Mantziris, D. A. & Stewart, W. C. (1997). Diurnal intraocular pressure in
untreated exfoliation and primary open-angle glaucoma. Arch Ophthalmol. 115:
182-185.
Kopitz, J., Holz, F. G., Kaemmerer, E. & Schutt, F. (2004). Lipids and lipid peroxidation
products in the pathogenesis of age-related macular degeneration. Biochimie. 86:
825-831.
Kota, S. K., Meher, L. K., Jammula, S., Krishna, S. V. & Modi, K. D. (2012). Aberrant
angiogenesis: The gateway to diabetic complications. Indian J Endocrinol Metab.
16: 918-930.
Kumar, A., Basavaraj, M. G., Gupta, S. K., Qamar, I., Ali, A. M., Bajaj, V., Ramesh, T.
K., Prakash, D. R., Shetty, J. S. & Dorairaj, S. K. (2007). Role of CYP1B1, MYOC,
OPTN, and OPTC genes in adult-onset primary open-angle glaucoma:
predominance of CYP1B1 mutations in Indian patients. Mol Vis. 13: 667-676.
Lai, E. (2001). Application of SNP technologies in medicine: lessons learned and future
challenges. Genome Res. 11: 927-929.
Lam, D. S., Leung, Y. F., Chua, J. K., Baum, L., Fan, D. S., Choy, K. W. & Pang, C. P.
(2000). Truncations in the TIGR gene in individuals with and without primary
open-angle glaucoma. Invest Ophthalmol Vis Sci. 41: 1386-1391.
Lamers, F., Schild, L., Koster, J., Speleman, F., Ora, I., Westerhout, E. M., Van Sluis, P.,
Versteeg, R., Caron, H. N. & Molenaar, J. J. (2012). Identification of BIRC6 as a
novel intervention target for neuroblastoma therapy. BMC Cancer. 12: 285.
Lander, E. S. & Schork, N. J. (1994). Genetic dissection of complex traits. Science. 265:
2037-2048.
Leske, M. C. (2007). Open-angle glaucoma -- an epidemiologic overview. Ophthalmic
Epidemiol. 14: 166-172.

166
Leung, Y. F., Fan, B. J., Lam, D. S., Lee, W. S., Tam, P. O., Chua, J. K., Tham, C. C., Lai,
J. S., Fan, D. S. & Pang, C. P. (2003). Different optineurin mutation pattern in
primary open-angle glaucoma. Invest Ophthalmol Vis Sci. 44: 3880-3884.
Libby, R. T., Gould, D. B., Anderson, M. G. & John, S. W. (2005). Complex genetics of
glaucoma susceptibility. Annu Rev Genomics Hum Genet. 6: 15-44.
Lichter, P. R. (2002). Impact of intraocular pressure reduction on glaucoma progression.
JAMA. 288: 2607-2608.
Limb, G. A., Webster, L., Soomro, H., Janikoun, S. & Shilling, J. (1999). Platelet
expression of tumour necrosis factor-alpha (TNF-alpha), TNF receptors and
intercellular adhesion molecule-1 (ICAM-1) in patients with proliferative diabetic
retinopathy. Clin Exp Immunol. 118: 213-218.
Lin, H. J., Chen, W. C., Tsai, F. J. & Tsai, S. W. (2002). Distributions of p53 codon 72
polymorphism in primary open angle glaucoma. Br J Ophthalmol. 86: 767-770.
Lin, H. J., Tsai, C. H., Tsai, F. J., Chen, W. C., Chen, H. Y. & Fan, S. S. (2004). Transporter
associated with antigen processing gene 1 codon 333 and codon 637
polymorphisms are associated with primary open-angle glaucoma. Mol Diagn. 8:
245-252.
Lin, H. J., Tsai, F. J., Chen, W. C., Shi, Y. R., Hsu, Y. & Tsai, S. W. (2003a). Association
of tumour necrosis factor alpha -308 gene polymorphism with primary open-angle
glaucoma in Chinese. Eye (Lond). 17: 31-34.
Lin, H. J., Tsai, F. J., Hung, P., Chen, W. C., Chen, H. Y., Fan, S. S. & Tsai, S. W. (2006).
Association of E-cadherin gene 3'-UTR C/T polymorphism with primary open
angle glaucoma. Ophthalmic Res. 38: 44-48.
Lin, H. J., Tsai, S. C., Tsai, F. J., Chen, W. C., Tsai, J. J. & Hsu, C. D. (2003b). Association
of interleukin 1beta and receptor antagonist gene polymorphisms with primary
open-angle glaucoma. Ophthalmologica. 217: 358-364.
Lin, M. T. & Beal, M. F. (2006). Mitochondrial dysfunction and oxidative stress in
neurodegenerative diseases. Nature. 443: 787-795.
Lipton, S. A. (1999). Neuronal protection and destruction by NO. Cell Death Differ. 6:
943-951.
Liu, B. & Neufeld, A. H. (2003). Activation of epidermal growth factor receptor signals
induction of nitric oxide synthase-2 in human optic nerve head astrocytes in
glaucomatous optic neuropathy. Neurobiol Dis. 13: 109-123.

167
Lopez-Garrido, M. P., Medina-Trillo, C., Morales-Fernandez, L., Garcia-Feijoo, J.,
Martinez-De-La-Casa, J. M., Garcia-Anton, M. & Escribano, J. (2013). Null
CYP1B1 genotypes in primary congenital and nondominant juvenile glaucoma.
Ophthalmology. 120: 716-723.
Luibl, V., Isas, J. M., Kayed, R., Glabe, C. G., Langen, R. & Chen, J. (2006). Drusen
deposits associated with aging and age-related macular degeneration contain
nonfibrillar amyloid oligomers. J Clin Invest. 116: 378-385.
Mabuchi, F., Sakurada, Y., Kashiwagi, K., Yamagata, Z., Iijima, H. & Tsukahara, S.
(2009). Lack of association between p53 gene polymorphisms and primary open
angle glaucoma in the Japanese population. Mol Vis. 15: 1045-1049.
Mackey, D. A., Healey, D. L., Fingert, J. H., Coote, M. A., Wong, T. L., Wilkinson, C. H.,
Mccartney, P. J., Rait, J. L., De Graaf, A. P., Stone, E. M. & Craig, J. E. (2003).
Glaucoma phenotype in pedigrees with the myocilin Thr377Met mutation. Arch
Ophthalmol. 121: 1172-1180.
Malek, A. M., Izumo, S. & Alper, S. L. (1999). Modulation by pathophysiological stimuli
of the shear stress-induced up-regulation of endothelial nitric oxide synthase
expression in endothelial cells. Neurosurgery. 45: 334-344; discussion 344-335.
Malek, G., Li, C. M., Guidry, C., Medeiros, N. E. & Curcio, C. A. (2003). Apolipoprotein
B in cholesterol-containing drusen and basal deposits of human eyes with age-
related maculopathy. Am J Pathol. 162: 413-425.
Maller, J. B., Fagerness, J. A., Reynolds, R. C., Neale, B. M., Daly, M. J. & Seddon, J. M.
(2007). Variation in complement factor 3 is associated with risk of age-related
macular degeneration. Nat Genet. 39: 1200-1201.
Mancebo, J. (1992). PEEP, ARDS, and alveolar recruitment. Intensive Care Med. 18: 383-
385.
Mcbride, H. M., Neuspiel, M. & Wasiak, S. (2006). Mitochondria: more than just a
powerhouse. Curr Biol. 16: R551-560.
Mcconnell, V. & Silvestri, G. (2005). Age-related macular degeneration. Ulster Med J. 74:
82-92.
Mckay, G. J., Patterson, C. C., Chakravarthy, U., Dasari, S., Klaver, C. C., Vingerling, J.
R., Ho, L., De Jong, P. T., Fletcher, A. E., Young, I. S., Seland, J. H., Rahu, M.,
Soubrane, G., Tomazzoli, L., Topouzis, F., Vioque, J., Hingorani, A. D., Sofat, R.,
Dean, M., Sawitzke, J., Seddon, J. M., Peter, I., Webster, A. R., Moore, A. T.,
Yates, J. R., Cipriani, V., Fritsche, L. G., Weber, B. H., Keilhauer, C. N., Lotery,
A. J., Ennis, S., Klein, M. L., Francis, P. J., Stambolian, D., Orlin, A., Gorin, M.

168
B., Weeks, D. E., Kuo, C. L., Swaroop, A., Othman, M., Kanda, A., Chen, W.,
Abecasis, G. R., Wright, A. F., Hayward, C., Baird, P. N., Guymer, R. H., Attia, J.,
Thakkinstian, A. & Silvestri, G. (2011). Evidence of association of APOE with age-
related macular degeneration: a pooled analysis of 15 studies. Hum Mutat. 32:
1407-1416.
Melki, R., Belmouden, A., Akhayat, O., Brezin, A. & Garchon, H. J. (2003). The M98K
variant of the OPTINEURIN (OPTN) gene modifies initial intraocular pressure in
patients with primary open angle glaucoma. J Med Genet. 40: 842-844.
Michael, O. H. (2005). Anatomy of the Anterior Eye for Ocularists. Journal of Ophthalmic
Prosthetics. pp. 25-35.
Michael, S., Qamar, R., Akhtar, F., Khan, W. A. & Ahmed, A. (2008). C677T
polymorphism in the methylenetetrahydrofolate reductase gene is associated with
primary closed angle glaucoma. Mol Vis. 14: 661-665.
Micheal, S., Ayub, H., Zafar, S. N., Bakker, B., Ali, M., Akhtar, F., Islam, F., Khan, M. I.,
Qamar, R. & Den Hollander, A. I. (2014). Identification of novel CYP1B1 gene
mutations in patients with primary congenital and primary open-angle glaucoma.
Clin Experiment Ophthalmol. doi: 10.1111/ceo.12369.
Monemi, S., Spaeth, G., Dasilva, A., Popinchalk, S., Ilitchev, E., Liebmann, J., Ritch, R.,
Heon, E., Crick, R. P., Child, A. & Sarfarazi, M. (2005). Identification of a novel
adult-onset primary open-angle glaucoma (POAG) gene on 5q22.1. Hum Mol
Genet. 14: 725-733.
Moren, A., Olofsson, A., Stenman, G., Sahlin, P., Kanzaki, T., Claesson-Welsh, L., Ten
Dijke, P., Miyazono, K. & Heldin, C. H. (1994). Identification and characterization
of LTBP-2, a novel latent transforming growth factor-beta-binding protein. J Biol
Chem. 269: 32469-32478.
Morré, D. J. & Morré, D. M. (2012). ECTO-NOX Proteins: Growth, Cancer, and Aging,
New York, Springer.
Morris, B., Imrie, F., Armbrecht, A. M. & Dhillon, B. (2007). Age-related macular
degeneration and recent developments: new hope for old eyes? Postgrad Med J.
83: 301-307.
Morrison, J. C. & Pollack, I. P. (2011). Glaucoma: Science and Practice, Hongkong,
Thiemes Medical Publishers.
Morrison, J. C., Johnson, E. C., Cepurna, W. & Jia, L. (2005). Understanding mechanisms
of pressure-induced optic nerve damage. Prog Retin Eye Res. 24: 217-240.

169
Mossbock, G., Renner, W., El-Shabrawi, Y., Faschinger, C., Schmut, O., Wedrich, A.,
Zimmermann, C. & Weger, M. (2009). TNF-alpha -308 G>A and -238 G>A
polymorphisms are not major risk factors in Caucasian patients with exfoliation
glaucoma. Mol Vis. 15: 518-522.
Mozaffarieh, M., Grieshaber, M. C. & Flammer, J. (2008). Oxygen and blood flow: players
in the pathogenesis of glaucoma. Mol Vis. 14: 224-233.
Mukesh, B. N., Mccarty, C. A., Rait, J. L. & Taylor, H. R. (2002). Five-year incidence of
open-angle glaucoma: the visual impairment project. Ophthalmology. 109: 1047-
1051.
Nakamura, K., Ota, M., Meguro, A., Nomura, N., Kashiwagi, K., Mabuchi, F., Iijima, H.,
Kawase, K., Yamamoto, T., Nakamura, M., Negi, A., Sagara, T., Nishida, T.,
Inatani, M., Tanihara, H., Aihara, M., Araie, M., Fukuchi, T., Abe, H., Higashide,
T., Sugiyama, K., Kanamoto, T., Kiuchi, Y., Iwase, A., Ohno, S., Inoko, H. &
Mizuki, N. (2009). Association of microsatellite polymorphisms of the GPDS1
locus with normal tension glaucoma in the Japanese population. Clin Ophthalmol.
3: 307-312.
Narooie-Nejad, M., Paylakhi, S. H., Shojaee, S., Fazlali, Z., Rezaei Kanavi, M.,
Nilforushan, N., Yazdani, S., Babrzadeh, F., Suri, F., Ronaghi, M., Elahi, E. &
Paisan-Ruiz, C. (2009). Loss of function mutations in the gene encoding latent
transforming growth factor beta binding protein 2, LTBP2, cause primary
congenital glaucoma. Hum Mol Genet. 18: 3969-3977.
Nathanson, J. A. & Mckee, M. (1995). Identification of an extensive system of nitric oxide-
producing cells in the ciliary muscle and outflow pathway of the human eye. Invest
Ophthalmol Vis Sci. 36: 1765-1773.
Naumann, G. O., Schlotzer-Schrehardt, U. & Kuchle, M. (1998). Pseudoexfoliation
syndrome for the comprehensive ophthalmologist. Intraocular and systemic
manifestations. Ophthalmology. 105: 951-968.
Neale, B. M., Fagerness, J., Reynolds, R., Sobrin, L., Parker, M., Raychaudhuri, S., Tan,
P. L., Oh, E. C., Merriam, J. E., Souied, E., Bernstein, P. S., Li, B., Frederick, J.
M., Zhang, K., Brantley, M. A., Jr., Lee, A. Y., Zack, D. J., Campochiaro, B.,
Campochiaro, P., Ripke, S., Smith, R. T., Barile, G. R., Katsanis, N., Allikmets, R.,
Daly, M. J. & Seddon, J. M. (2010). Genome-wide association study of advanced
age-related macular degeneration identifies a role of the hepatic lipase gene (LIPC).
Proc Natl Acad Sci U S A. 107: 7395-7400.
Ni Dhubhghaill, S. S., Cahill, M. T., Campbell, M., Cassidy, L., Humphries, M. M. &
Humphries, P. (2010). The pathophysiology of cigarette smoking and age-related
macular degeneration. Adv Exp Med Biol. 664: 437-446.

170
Nickells, R. W. (1999). Apoptosis of retinal ganglion cells in glaucoma: an update of the
molecular pathways involved in cell death. Surv Ophthalmol. 43 Suppl 1: S151-
161.
Nikopoulos, K., Schrauwen, I., Simon, M., Collin, R. W., Veckeneer, M., Keymolen, K.,
Van Camp, G., Cremers, F. P. & Van Den Born, L. I. (2011). Autosomal recessive
Stickler syndrome in two families is caused by mutations in the COL9A1 gene.
Invest Ophthalmol Vis Sci. 52: 4774-4779.
Nowak, J. Z. (2006). Age-related macular degeneration (AMD): pathogenesis and therapy.
Pharmacol Rep. 58: 353-363.
Ntim-Amponsah, C. T., Amoaku, W. M., Ofosu-Amaah, S., Ewusi, R. K., Idirisuriya-
Khair, R., Nyatepe-Coo, E. & Adu-Darko, M. (2004). Prevalence of glaucoma in
an African population. Eye (Lond). 18: 491-497.
Ohno-Matsui, K. (2011). Parallel findings in age-related macular degeneration and
Alzheimer's disease. Prog Retin Eye Res. 30: 217-238.
Osborne, N. N., Melena, J., Chidlow, G. & Wood, J. P. (2001). A hypothesis to explain
ganglion cell death caused by vascular insults at the optic nerve head: possible
implication for the treatment of glaucoma. Br J Ophthalmol. 85: 1252-1259.
Owen, C. G., Fletcher, A. E., Donoghue, M. & Rudnicka, A. R. (2003). How big is the
burden of visual loss caused by age related macular degeneration in the United
Kingdom? Br J Ophthalmol. 87: 312-317.
Pagon, R.A., Bird, T.D., Dolan, C.R., Stephens, K., Adam, M.P. (2012). Stickler
Syndrome; Gene Reviews, University of Washington. Last reviewed:13 Janurary
2015, (http://www.ncbi.nlm.nih.gov/books/NBK1302/)
Pang, C. P., Fan, B. J., Canlas, O., Wang, D. Y., Dubois, S., Tam, P. O., Lam, D. S.,
Raymond, V. & Ritch, R. (2006). A genome-wide scan maps a novel juvenile-onset
primary open angle glaucoma locus to chromosome 5q. Mol Vis. 12: 85-92.
Pang, C. P., Leung, Y. F., Fan, B., Baum, L., Tong, W. C., Lee, W. S., Chua, J. K., Fan, D.
S., Liu, Y. & Lam, D. S. (2002). TIGR/MYOC gene sequence alterations in
individuals with and without primary open-angle glaucoma. Invest Ophthalmol Vis
Sci. 43: 3231-3235.
Papadopoulos, M., Cable, N., Rahi, J. & Khaw, P. T. (2007). The British Infantile and
Childhood Glaucoma (BIG) Eye Study. Invest Ophthalmol Vis Sci. 48: 4100-4106.
Papiol, S., Molina, V., Desco, M., Rosa, A., Reig, S., Sanz, J., Palomo, T. & Fananas, L.
(2008). Gray matter deficits in bipolar disorder are associated with genetic
variability at interleukin-1 beta gene (2q13). Genes Brain Behav. 7: 796-801.

171
Parmeggiani, F., Romano, M. R., Costagliola, C., Semeraro, F., Incorvaia, C., D'angelo,
S., Perri, P., De Palma, P., De Nadai, K. & Sebastiani, A. (2012). Mechanism of
inflammation in age-related macular degeneration. Mediators Inflamm. 2012:
546786.
Pasutto, F., Matsumoto, T., Mardin, C. Y., Sticht, H., Brandstatter, J. H., Michels-
Rautenstrauss, K., Weisschuh, N., Gramer, E., Ramdas, W. D., Van Koolwijk, L.
M., Klaver, C. C., Vingerling, J. R., Weber, B. H., Kruse, F. E., Rautenstrauss, B.,
Barde, Y. A. & Reis, A. (2009). Heterozygous NTF4 mutations impairing
neurotrophin-4 signaling in patients with primary open-angle glaucoma. Am J Hum
Genet. 85: 447-456.
Patel, S. J. & Lundy, D. C. (2002). Ocular manifestations of autoimmune disease. Am Fam
Physician. 66: 991-998.
Pauleikhoff, D., Harper, C. A., Marshall, J. & Bird, A. C. (1990). Aging changes in Bruch's
membrane. A histochemical and morphologic study. Ophthalmology. 97: 171-178.
Penfold, P. L., Killingsworth, M. C. & Sarks, S. H. (1985). Senile macular degeneration:
the involvement of immunocompetent cells. Graefes Arch Clin Exp Ophthalmol.
223: 69-76.
Plantner, J. J. (1992). High molecular weight mucin-like glycoproteins of the bovine
interphotoreceptor matrix. Exp Eye Res. 54: 113-125.
Plantner, J. J., Jiang, C. & Smine, A. (1998a). Increase in interphotoreceptor matrix
gelatinase A (MMP-2) associated with age-related macular degeneration. Exp Eye
Res. 67: 637-645.
Plantner, J. J., Smine, A. & Quinn, T. A. (1998b). Matrix metalloproteinases and
metalloproteinase inhibitors in human interphotoreceptor matrix and vitreous. Curr
Eye Res. 17: 132-140.
Price, M., Lazzaro, D., Pohl, T., Mattei, M. G., Ruther, U., Olivo, J. C., Duboule, D. & Di
Lauro, R. (1992). Regional expression of the homeobox gene Nkx-2.2 in the
developing mammalian forebrain. Neuron. 8: 241-255.
Provencio, I., Rodriguez, I. R., Jiang, G., Hayes, W. P., Moreira, E. F. & Rollag, M. D.
(2000). A novel human opsin in the inner retina. J Neurosci. 20: 600-605.
Qui, M. (1990). [Bone histomorphometric study of iliac crest in normal Chinese subjects].
Zhonghua Yi Xue Za Zhi. 70: 685-690, 648.
Quigley, H. A. & Broman, A. T. (2006). The number of people with glaucoma worldwide
in 2010 and 2020. Br J Ophthalmol. 90: 262-267.

172
Quigley, H. A. (1996). Number of people with glaucoma worldwide. Br J Ophthalmol. 80:
389-393.
Quigley, H. A. (1999). Neuronal death in glaucoma. Prog Retin Eye Res. 18: 39-57.
Quigley, H. A. (2011). Glaucoma. Lancet. 377: 1367-1377.
Quigley, H. A., Nickells, R. W., Kerrigan, L. A., Pease, M. E., Thibault, D. J. & Zack, D.
J. (1995). Retinal ganglion cell death in experimental glaucoma and after axotomy
occurs by apoptosis. Invest Ophthalmol Vis Sci. 36: 774-786.
Radu, R. A., Hu, J., Yuan, Q., Welch, D. L., Makshanoff, J., Lloyd, M., Mcmullen, S.,
Travis, G. H. & Bok, D. (2011). Complement system dysregulation and
inflammation in the retinal pigment epithelium of a mouse model for Stargardt
macular degeneration. J Biol Chem. 286: 18593-18601.
Rao, A. (2014). Intraocular Pressure: Is it a Risk Factor in Normal Tension Glaucoma? J
Glaucoma. (Epub ahead of print)
Ratnapriya, R. & Chew, E. Y. (2013). Age-related macular degeneration-clinical review
and genetics update. Clin Genet. 84: 160-166.
Reale, E., Groos, S., Eckardt, U., Eckardt, C. & Luciano, L. (2009). New components of
'basal laminar deposits' in age-related macular degeneration. Cells Tissues Organs.
190: 170-181.
Reddy, A. B., Panicker, S. G., Mandal, A. K., Hasnain, S. E. & Balasubramanian, D.
(2003). Identification of R368H as a predominant CYP1B1 allele causing primary
congenital glaucoma in Indian patients. Invest Ophthalmol Vis Sci. 44: 4200-4203.
Ren, J., Shi, M., Liu, R., Yang, Q. H., Johnson, T., Skarnes, W. C. & Du, C. (2005). The
Birc6 (Bruce) gene regulates p53 and the mitochondrial pathway of apoptosis and
is essential for mouse embryonic development. Proc Natl Acad Sci U S A. 102: 565-
570.
Resnikoff, S., Pascolini, D., Etya'ale, D., Kocur, I., Pararajasegaram, R., Pokharel, G. P. &
Mariotti, S. P. (2004). Global data on visual impairment in the year 2002. Bull
World Health Organ. 82: 844-851.
Ressiniotis, T., Griffiths, P. G., Keers, S. M., Chinnery, P. F. & Birch, M. (2005). A
polymorphism at codon 31 of gene p21 is not associated with primary open angle
glaucoma in Caucasians. BMC Ophthalmol. 5: 5.

173
Rezaie, T., Child, A., Hitchings, R., Brice, G., Miller, L., Coca-Prados, M., Heon, E.,
Krupin, T., Ritch, R., Kreutzer, D., Crick, R. P. & Sarfarazi, M. (2002). Adult-onset
primary open-angle glaucoma caused by mutations in optineurin. Science. 295:
1077-1079.
Riordan-Eva, P., Whitcher, J. & Asbury, T. Vaughan & Asbury's General Ophthalmology.
In “Anatomy & Embriology of the Eye”. McGraw-Hill Education. New York., pp.
12 (2007).
Risch, N. & Merikangas, K. (1996). The future of genetic studies of complex human
diseases. Science. 273: 1516-1517.
Ritch, R. & Schlotzer-Schrehardt, U. (2001). Exfoliation syndrome. Surv Ophthalmol. 45:
265-315.
Rivera, A., Fisher, S. A., Fritsche, L. G., Keilhauer, C. N., Lichtner, P., Meitinger, T. &
Weber, B. H. (2005). Hypothetical LOC387715 is a second major susceptibility
gene for age-related macular degeneration, contributing independently of
complement factor H to disease risk. Hum Mol Genet. 14: 3227-3236.
Rodriguez De Cordoba, S., Esparza-Gordillo, J., Goicoechea De Jorge, E., Lopez-Trascasa,
M. & Sanchez-Corral, P. (2004). The human complement factor H: functional roles,
genetic variations and disease associations. Mol Immunol. 41: 355-367.
Rosenbaum, D. M., Rosenbaum, P. S., Gupta, H., Singh, M., Aggarwal, A., Hall, D. H.,
Roth, S. & Kessler, J. A. (1998). The role of the p53 protein in the selective
vulnerability of the inner retina to transient ischemia. Invest Ophthalmol Vis Sci.
39: 2132-2139.
Rudolf, M., Clark, M. E., Chimento, M. F., Li, C. M., Medeiros, N. E. & Curcio, C. A.
(2008). Prevalence and morphology of druse types in the macula and periphery of
eyes with age-related maculopathy. Invest Ophthalmol Vis Sci. 49: 1200-1209.
Russell, S. R., Mullins, R. F., Schneider, B. L. & Hageman, G. S. (2000). Location,
substructure, and composition of basal laminar drusen compared with drusen
associated with aging and age-related macular degeneration. Am J Ophthalmol.
129: 205-214.
Ryan, S. J., Schachat, A. P., Wilkinson, C. P., Hinton, D. R., Sadda, S. V. R. & Wiedemann,
P. Retina. In “Structure, Function, and Pathology of Bruch’s Membrane”. Elsevier
Health Sciences., pp. 466-478 (2012)
Sacca, S. C., Izzotti, A., Rossi, P. & Traverso, C. (2007). Glaucomatous outflow pathway
and oxidative stress. Exp Eye Res. 84: 389-399.

174
Saglar, E., Yucel, D., Bozkurt, B., Ozgul, R. K., Irkec, M. & Ogus, A. (2009). Association
of polymorphisms in APOE, p53, and p21 with primary open-angle glaucoma in
Turkish patients. Mol Vis. 15: 1270-1276.
Saprunova, V. B., Pilipenko, D. I., Alexeevsky, A. V., Fursova, A., Kolosova, N. G. &
Bakeeva, L. E. (2010). Lipofuscin granule dynamics during development of age-
related macular degeneration. Biochemistry (Mosc). 75: 130-138.
Sarfarazi, M. (1997). Recent advances in molecular genetics of glaucomas. Hum Mol
Genet. 6: 1667-1677.
Sarfarazi, M., Akarsu, A. N., Hossain, A., Turacli, M. E., Aktan, S. G., Barsoum-Homsy,
M., Chevrette, L. & Sayli, B. S. (1995). Assignment of a locus (GLC3A) for
primary congenital glaucoma (Buphthalmos) to 2p21 and evidence for genetic
heterogeneity. Genomics. 30: 171-177.
Sarfarazi, M., Child, A., Stoilova, D., Brice, G., Desai, T., Trifan, O. C., Poinoosawmy, D.
& Crick, R. P. (1998). Localization of the fourth locus (GLC1E) for adult-onset
primary open-angle glaucoma to the 10p15-p14 region. Am J Hum Genet. 62: 641-
652.
Sarfarazi, M., Stoilov, I. & Schenkman, J. B. (2003). Genetics and biochemistry of primary
congenital glaucoma. Ophthalmol Clin North Am. 16: 543-554.
Schmidt, S., Klaver, C., Saunders, A., Postel, E., De La Paz, M., Agarwal, A., Small, K.,
Udar, N., Ong, J., Chalukya, M., Nesburn, A., Kenney, C., Domurath, R., Hogan,
M., Mah, T., Conley, Y., Ferrell, R., Weeks, D., De Jong, P. T., Van Duijn, C.,
Haines, J., Pericak-Vance, M. & Gorin, M. (2002). A pooled case-control study of
the apolipoprotein E (APOE) gene in age-related maculopathy. Ophthalmic Genet.
23: 209-223.
Schutt, F., Davies, S., Kopitz, J., Holz, F. G. & Boulton, M. E. (2000). Photodamage to
human RPE cells by A2-E, a retinoid component of lipofuscin. Invest Ophthalmol
Vis Sci. 41: 2303-2308.
Schwartz, M. & Ziv, Y. (2008). Immunity to self and self-maintenance: a unified theory of
brain pathologies. Trends Immunol. 29: 211-219.
Schwartz, S. G., Agarwal, A., Kovach, J. L., Gallins, P. J., Cade, W., Postel, E. A., Wang,
G., Ayala-Haedo, J., Spencer, K. M., Haines, J. L., Pericak-Vance, M. A. & Scott,
W. K. (2012). The ARMS2 A69S variant and bilateral advanced age-related
macular degeneration. Retina. 32: 1486-1491.
Seddon, J. M., Ajani, U. A., Sperduto, R. D., Hiller, R., Blair, N., Burton, T. C., Farber, M.
D., Gragoudas, E. S., Haller, J., Miller, D. T. & Et Al. (1994). Dietary carotenoids,

175
vitamins A, C, and E, and advanced age-related macular degeneration. Eye Disease
Case-Control Study Group. JAMA. 272: 1413-1420.
Seddon, J. M., George, S., Rosner, B. & Rifai, N. (2005). Progression of age-related
macular degeneration: prospective assessment of C-reactive protein, interleukin 6,
and other cardiovascular biomarkers. Arch Ophthalmol. 123: 774-782.
Sethi, C. S., Bailey, T. A., Luthert, P. J. & Chong, N. H. (2000). Matrix metalloproteinase
biology applied to vitreoretinal disorders. Br J Ophthalmol. 84: 654-666.
Shaarawy, T., Sherwood, M. B. & Crowston, J. G. (2009). Glaucoma: Medical diagnosis
& therapy, Saunders/Elsevier.
Shastry, B. S. (2013). Genetic susceptibility to primary angle closure glaucoma (PACG).
Discov Med. 15: 17-22.
Sheffield, V. C., Stone, E. M., Alward, W. L., Drack, A. V., Johnson, A. T., Streb, L. M.
& Nichols, B. E. (1993). Genetic linkage of familial open angle glaucoma to
chromosome 1q21-q31. Nat Genet. 4: 47-50.
Shi, H., Zhu, R., Hu, N., Shi, J., Zhang, J., Yang, M., Jiang, L., Jiang, H. & Guan, H.
(2014). Association of eNOS polymorphisms with anterior chamber depth in han
chinese: jiangsu eye study. J Ophthalmol. 2014: 164104.
Shibuya, E., Meguro, A., Ota, M., Kashiwagi, K., Mabuchi, F., Iijima, H., Kawase, K.,
Yamamoto, T., Nakamura, M., Negi, A., Sagara, T., Nishida, T., Inatani, M.,
Tanihara, H., Aihara, M., Araie, M., Fukuchi, T., Abe, H., Higashide, T., Sugiyama,
K., Kanamoto, T., Kiuchi, Y., Iwase, A., Ohno, S., Inoko, H. & Mizuki, N. (2008).
Association of Toll-like receptor 4 gene polymorphisms with normal tension
glaucoma. Invest Ophthalmol Vis Sci. 49: 4453-4457.
Shibuya, M. (2008). Vascular endothelial growth factor-dependent and -independent
regulation of angiogenesis. BMB Rep. 41: 278-286.
Shigenaga, M. K., Hagen, T. M. & Ames, B. N. (1994). Oxidative damage and
mitochondrial decay in aging. Proc Natl Acad Sci U S A. 91: 10771-10778.
Shirts, B. H., Wood, J., Yolken, R. H. & Nimgaonkar, V. L. (2006). Association study of
IL10, IL1beta, and IL1RN and schizophrenia using tag SNPs from a comprehensive
database: suggestive association with rs16944 at IL1beta. Schizophr Res. 88: 235-
244.
Sivaprasad, S., Bailey, T. A. & Chong, V. N. (2005). Bruch's membrane and the vascular
intima: is there a common basis for age-related changes and disease? Clin
Experiment Ophthalmol. 33: 518-523.

176
Smith, W., Mitchell, P. & Wang, J. J. (1997). Gender, oestrogen, hormone replacement
and age-related macular degeneration: results from the Blue Mountains Eye Study.
Aust N Z J Ophthalmol. 25 Suppl 1: S13-15.
Sobrin, L., Reynolds, R., Yu, Y., Fagerness, J., Leveziel, N., Bernstein, P. S., Souied, E.
H., Daly, M. J. & Seddon, J. M. (2011). ARMS2/HTRA1 locus can confer
differential susceptibility to the advanced subtypes of age-related macular
degeneration. Am J Ophthalmol. 151: 345-352 e343.
Sofat, R., Casas, J. P., Webster, A. R., Bird, A. C., Mann, S. S., Yates, J. R., Moore, A. T.,
Sepp, T., Cipriani, V., Bunce, C., Khan, J. C., Shahid, H., Swaroop, A., Abecasis,
G., Branham, K. E., Zareparsi, S., Bergen, A. A., Klaver, C. C., Baas, D. C., Zhang,
K., Chen, Y., Gibbs, D., Weber, B. H., Keilhauer, C. N., Fritsche, L. G., Lotery, A.,
Cree, A. J., Griffiths, H. L., Bhattacharya, S. S., Chen, L. L., Jenkins, S. A., Peto,
T., Lathrop, M., Leveillard, T., Gorin, M. B., Weeks, D. E., Ortube, M. C., Ferrell,
R. E., Jakobsdottir, J., Conley, Y. P., Rahu, M., Seland, J. H., Soubrane, G.,
Topouzis, F., Vioque, J., Tomazzoli, L., Young, I., Whittaker, J., Chakravarthy, U.,
De Jong, P. T., Smeeth, L., Fletcher, A. & Hingorani, A. D. (2012). Complement
factor H genetic variant and age-related macular degeneration: effect size,
modifiers and relationship to disease subtype. Int J Epidemiol. 41: 250-262.
Sparrow, J. R., Nakanishi, K. & Parish, C. A. (2000). The lipofuscin fluorophore A2E
mediates blue light-induced damage to retinal pigmented epithelial cells. Invest
Ophthalmol Vis Sci. 41: 1981-1989.
Spencer, K. L., Olson, L. M., Schnetz-Boutaud, N., Gallins, P., Agarwal, A., Iannaccone,
A., Kritchevsky, S. B., Garcia, M., Nalls, M. A., Newman, A. B., Scott, W. K.,
Pericak-Vance, M. A. & Haines, J. L. (2011). Using genetic variation and
environmental risk factor data to identify individuals at high risk for age-related
macular degeneration. PLoS One. 6: e17784.
Sripriya, S., Nirmaladevi, J., George, R., Hemamalini, A., Baskaran, M., Prema, R., Ve
Ramesh, S., Karthiyayini, T., Amali, J., Job, S., Vijaya, L. & Kumaramanickavel,
G. (2006). OPTN gene: profile of patients with glaucoma from India. Mol Vis. 12:
816-820.
Sripriya, S., Uthra, S., Sangeetha, R., George, R. J., Hemamalini, A., Paul, P. G., Amali,
J., Vijaya, L. & Kumaramanickavel, G. (2004). Low frequency of myocilin
mutations in Indian primary open-angle glaucoma patients. Clin Genet. 65: 333-
337.
Stein, J. D., Kim, D. S., Niziol, L. M., Talwar, N., Nan, B., Musch, D. C. & Richards, J. E.
(2011). Differences in rates of glaucoma among Asian Americans and other racial
groups, and among various Asian ethnic groups. Ophthalmology. 118: 1031-1037.

177
Sternlicht, M. D. & Werb, Z. (2001). How matrix metalloproteinases regulate cell behavior.
Annu Rev Cell Dev Biol. 17: 463-516.
Stoilov, I., Akarsu, A. N. & Sarfarazi, M. (1997). Identification of three different truncating
mutations in cytochrome P4501B1 (CYP1B1) as the principal cause of primary
congenital glaucoma (Buphthalmos) in families linked to the GLC3A locus on
chromosome 2p21. Hum Mol Genet. 6: 641-647.
Stoilov, I., Akarsu, A. N., Alozie, I., Child, A., Barsoum-Homsy, M., Turacli, M. E., Or,
M., Lewis, R. A., Ozdemir, N., Brice, G., Aktan, S. G., Chevrette, L., Coca-Prados,
M. & Sarfarazi, M. (1998). Sequence analysis and homology modeling suggest that
primary congenital glaucoma on 2p21 results from mutations disrupting either the
hinge region or the conserved core structures of cytochrome P4501B1. Am J Hum
Genet. 62: 573-584.
Stoilova, D., Child, A., Trifan, O. C., Crick, R. P., Coakes, R. L. & Sarfarazi, M. (1996).
Localization of a locus (GLC1B) for adult-onset primary open angle glaucoma to
the 2cen-q13 region. Genomics. 36: 142-150.
Stone, E. M., Sheffield, V. C. & Hageman, G. S. (2001). Molecular genetics of age-related
macular degeneration. Hum Mol Genet. 10: 2285-2292.
Strauss, O. (2005). The retinal pigment epithelium in visual function. Physiol Rev. 85: 845-
881.
Streeten, B. W., Dark, A. J., Wallace, R. N., Li, Z. Y. & Hoepner, J. A. (1990).
Pseudoexfoliative fibrillopathy in the skin of patients with ocular
pseudoexfoliation. Am J Ophthalmol. 110: 490-499.
Streeten, B. W., Li, Z. Y., Wallace, R. N., Eagle, R. C., Jr. & Keshgegian, A. A. (1992).
Pseudoexfoliative fibrillopathy in visceral organs of a patient with
pseudoexfoliation syndrome. Arch Ophthalmol. 110: 1757-1762.
Sugiyama, T., Moriya, S., Oku, H. & Azuma, I. (1995). Association of endothelin-1 with
normal tension glaucoma: clinical and fundamental studies. Surv Ophthalmol. 39
Suppl 1: S49-56.
Sundaresan, P., Vashist, P., Ravindran, R. D., Shanker, A., Nitsch, D., Nonyane, B. A.,
Smeeth, L., Chakravarthy, U. & Fletcher, A. E. (2012). Polymorphisms in
ARMS2/HTRA1 and complement genes and age-related macular degeneration in
India: findings from the INDEYE study. Invest Ophthalmol Vis Sci. 53: 7492-7497.
Suriyapperuma, S. P., Child, A., Desai, T., Brice, G., Kerr, A., Crick, R. P. & Sarfarazi, M.
(2007). A new locus (GLC1H) for adult-onset primary open-angle glaucoma maps
to the 2p15-p16 region. Arch Ophthalmol. 125: 86-92.

178
Suzuki, Y., Shirato, S., Taniguchi, F., Ohara, K., Nishimaki, K. & Ohta, S. (1997).
Mutations in the TIGR gene in familial primary open-angle glaucoma in Japan. Am
J Hum Genet. 61: 1202-1204.
Swaroop, A., Chew, E. Y., Rickman, C. B. & Abecasis, G. R. (2009). Unraveling a
multifactorial late-onset disease: from genetic susceptibility to disease mechanisms
for age-related macular degeneration. Annu Rev Genomics Hum Genet. 10: 19-43.
Taft, M. H., Behrmann, E., Munske-Weidemann, L. C., Thiel, C., Raunser, S. & Manstein,
D. J. (2013). Functional characterization of human myosin-18A and its interaction
with F-actin and GOLPH3. J Biol Chem. 288: 30029-30041.
Tamm, E. R. (2009). The trabecular meshwork outflow pathways: structural and functional
aspects. Exp Eye Res. 88: 648-655.
Tamm, E. R., Russell, P., Epstein, D. L., Johnson, D. H. & Piatigorsky, J. (1999).
Modulation of myocilin/TIGR expression in human trabecular meshwork. Invest
Ophthalmol Vis Sci. 40: 2577-2582.
Tarongoy, P., Ho, C. L. & Walton, D. S. (2009). Angle-closure glaucoma: the role of the
lens in the pathogenesis, prevention, and treatment. Surv Ophthalmol. 54: 211-225.
Taylor, H. R. & Keeffe, J. E. (2001). World blindness: a 21st century perspective. Br J
Ophthalmol. 85: 261-266.
Taylor, H. R., West, S., Munoz, B., Rosenthal, F. S., Bressler, S. B. & Bressler, N. M.
(1992). The long-term effects of visible light on the eye. Arch Ophthalmol. 110:
99-104.
Terman, A. & Brunk, U. T. (1998). Lipofuscin: mechanisms of formation and increase with
age. APMIS. 106: 265-276.
Tezel, G. (2009). The role of glia, mitochondria, and the immune system in glaucoma.
Invest Ophthalmol Vis Sci. 50: 1001-1012.
Tezel, G., Hernandez, R. & Wax, M. B. (2000). Immunostaining of heat shock proteins in
the retina and optic nerve head of normal and glaucomatous eyes. Arch Ophthalmol.
118: 511-518.
Tezel, G., Yang, J. & Wax, M. B. (2004). Heat shock proteins, immunity and glaucoma.
Brain Res Bull. 62: 473-480.
Thomas, J. L., Pan, D., Haixi, M. & Simon, L. (2011). Differential Effects of Elevated
Hydrostatic Pressure on Gene Expression and Protein Phosphorylation in Optic
Nerve Head Astrocytes. In “The mystery of glaucoma” Croatia, InTech.

179
Tielsch, J. M., Katz, J., Sommer, A., Quigley, H. A. & Javitt, J. C. (1994). Family history
and risk of primary open angle glaucoma. The Baltimore Eye Survey. Arch
Ophthalmol. 112: 69-73.
Toda, N. & Nakanishi-Toda, M. (2007). Nitric oxide: ocular blood flow, glaucoma, and
diabetic retinopathy. Prog Retin Eye Res. 26: 205-238.
Tomany, S. C., Cruickshanks, K. J., Klein, R., Klein, B. E. & Knudtson, M. D. (2004a).
Sunlight and the 10-year incidence of age-related maculopathy: the Beaver Dam
Eye Study. Arch Ophthalmol. 122: 750-757.
Tomany, S. C., Wang, J. J., Van Leeuwen, R., Klein, R., Mitchell, P., Vingerling, J. R.,
Klein, B. E., Smith, W. & De Jong, P. T. (2004b). Risk factors for incident age-
related macular degeneration: pooled findings from 3 continents. Ophthalmology.
111: 1280-1287.
Tosaka, K., Mashima, Y., Funayama, T., Ohtake, Y. & Kimura, I. (2007). Association
between open-angle glaucoma and gene polymorphism for heat-shock protein 70-
1. Jpn J Ophthalmol. 51: 417-423.
Totan, Y., Cekic, O., Borazan, M., Uz, E., Sogut, S. & Akyol, O. (2001). Plasma
malondialdehyde and nitric oxide levels in age related macular degeneration. Br J
Ophthalmol. 85: 1426-1428.
Trifan, O. C., Traboulsi, E. I., Stoilova, D., Alozie, I., Nguyen, R., Raja, S. & Sarfarazi, M.
(1998). A third locus (GLC1D) for adult-onset primary open-angle glaucoma maps
to the 8q23 region. Am J Ophthalmol. 126: 17-28.
Tsai, F. J., Lin, H. J., Chen, W. C., Chen, H. Y. & Fan, S. S. (2003). Insulin-like growth
factor-II gene polymorphism is associated with primary open angle glaucoma. J
Clin Lab Anal. 17: 259-263.
Tsai, F. J., Lin, H. J., Chen, W. C., Tsai, C. H. & Tsai, S. W. (2004). A codon 31ser-arg
polymorphism of the WAF-1/CIP-1/p21/tumour suppressor gene in Chinese
primary open-angle glaucoma. Acta Ophthalmol Scand. 82: 76-80.
Tsai, Y. Y., Lin, J. M., Wan, L., Lin, H. J., Tsai, Y., Lee, C. C., Tsai, C. H., Tsai, F. J. &
Tseng, S. H. (2008). Interleukin gene polymorphisms in age-related macular
degeneration. Invest Ophthalmol Vis Sci. 49: 693-698.
Tunny, T. J., Richardson, K. A. & Clark, C. V. (1998). Association study of the 5' flanking
regions of endothelial-nitric oxide synthase and endothelin-1 genes in familial
primary open-angle glaucoma. Clin Exp Pharmacol Physiol. 25: 26-29.

180
Tunny, T. J., Richardson, K. A., Clark, C. V. & Gordon, R. D. (1996). The atrial natriuretic
peptide gene in patients with familial primary open-angle glaucoma. Biochem
Biophys Res Commun. 223: 221-225.
Tuo, J., Bojanowski, C. M. & Chan, C. C. (2004). Genetic factors of age-related macular
degeneration. Prog Retin Eye Res. 23: 229-249.
Tuo, J., Smith, B. C., Bojanowski, C. M., Meleth, A. D., Gery, I., Csaky, K. G., Chew, E.
Y. & Chan, C. C. (2004). The involvement of sequence variation and expression of
CX3CR1 in the pathogenesis of age-related macular degeneration. FASEB J. 18:
1297-1299.
U.S. Preventive Services Task Force. (2005). Screening for glaucoma: recommendation
statement. Ann Fam Med. 3: 171-172.
Van Der Valk, R., Webers, C. A., Schouten, J. S., Zeegers, M. P., Hendrikse, F. & Prins,
M. H. (2005). Intraocular pressure-lowering effects of all commonly used
glaucoma drugs: a meta-analysis of randomized clinical trials. Ophthalmology.
112: 1177-1185.
Varma, R., Lee, P. P., Goldberg, I. & Kotak, S. (2011). An assessment of the health and
economic burdens of glaucoma. Am J Ophthalmol. 152: 515-522.
Vasiliou, V. & Gonzalez, F. J. (2008). Role of CYP1B1 in glaucoma. Annu Rev Pharmacol
Toxicol. 48: 333-358.
Vassalli, P. (1992). The pathophysiology of tumor necrosis factors. Annu Rev Immunol.
10: 411-452.
Venkateswaran, A., Sekhar, K. R., Levic, D. S., Melville, D. B., Clark, T. A., Rybski, W.
M., Walsh, A. J., Skala, M. C., Crooks, P. A., Knapik, E. W. & Freeman, M. L.
(2014). The NADH oxidase ENOX1, a critical mediator of endothelial cell
radiosensitization, is crucial for vascular development. Cancer Res. 74: 38-43.
Villemain, F. M., Bach, J. F. & Chatenoud, L. M. (1990). Characterization of histamine
H1 binding sites on human T lymphocytes by means of 125I-iodobolpyramine.
Preferential expression of H1 receptors on CD8 T lymphocytes. J Immunol. 144:
1449-1454.
Vincent, A. L., Billingsley, G., Buys, Y., Levin, A. V., Priston, M., Trope, G., Williams-
Lyn, D. & Heon, E. (2002). Digenic inheritance of early-onset glaucoma: CYP1B1,
a potential modifier gene. Am J Hum Genet. 70: 448-460.
Viso, E., Rodriguez-Ares, M. T. & Gude, F. (2010). Prevalence of pseudoexfoliation
syndrome among adult Spanish in the Salnes eye Study. Ophthalmic Epidemiol. 17:
118-124.

181
Vithana, E. N., Khor, C. C., Qiao, C., Nongpiur, M. E., George, R., Chen, L. J., Do, T.,
Abu-Amero, K., Huang, C. K., Low, S., Tajudin, L. S., Perera, S. A., Cheng, C. Y.,
Xu, L., Jia, H., Ho, C. L., Sim, K. S., Wu, R. Y., Tham, C. C., Chew, P. T., Su, D.
H., Oen, F. T., Sarangapani, S., Soumittra, N., Osman, E. A., Wong, H. T., Tang,
G., Fan, S., Meng, H., Huong, D. T., Wang, H., Feng, B., Baskaran, M., Shantha,
B., Ramprasad, V. L., Kumaramanickavel, G., Iyengar, S. K., How, A. C., Lee, K.
Y., Sivakumaran, T. A., Yong, V. H., Ting, S. M., Li, Y., Wang, Y. X., Tay, W. T.,
Sim, X., Lavanya, R., Cornes, B. K., Zheng, Y. F., Wong, T. T., Loon, S. C., Yong,
V. K., Waseem, N., Yaakub, A., Chia, K. S., Allingham, R. R., Hauser, M. A., Lam,
D. S., Hibberd, M. L., Bhattacharya, S. S., Zhang, M., Teo, Y. Y., Tan, D. T., Jonas,
J. B., Tai, E. S., Saw, S. M., Hon Do, N., Al-Obeidan, S. A., Liu, J., Chau, T. N.,
Simmons, C. P., Bei, J. X., Zeng, Y. X., Foster, P. J., Vijaya, L., Wong, T. Y., Pang,
C. P., Wang, N. & Aung, T. (2012). Genome-wide association analyses identify
three new susceptibility loci for primary angle closure glaucoma. Nat Genet. 44:
1142-1146.
Vittitow, J. & Borras, T. (2002). Expression of optineurin, a glaucoma-linked gene, is
influenced by elevated intraocular pressure. Biochem Biophys Res Commun. 298:
67-74.
Vohra, R., Tsai, J. C. & Kolko, M. (2013). The role of inflammation in the pathogenesis of
glaucoma. Surv Ophthalmol. 58: 311-320.
Wand, M., Grant, W. M., Simmons, R. J. & Hutchinson, B. T. (1977). Plateau iris
syndrome. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 83: 122-130.
Wang, D. Y., Fan, B. J., Chua, J. K., Tam, P. O., Leung, C. K., Lam, D. S. & Pang, C. P.
(2006a). A genome-wide scan maps a novel juvenile-onset primary open-angle
glaucoma locus to 15q. Invest Ophthalmol Vis Sci. 47: 5315-5321.
Wang, I. J., Chiang, T. H., Shih, Y. F., Lu, S. C., Lin, L. L., Shieh, J. W., Wang, T. H.,
Samples, J. R. & Hung, P. T. (2006b). The association of single nucleotide
polymorphisms in the MMP-9 genes with susceptibility to acute primary angle
closure glaucoma in Taiwanese patients. Mol Vis. 12: 1223-1232.
Wang, L., Clark, M. E., Crossman, D. K., Kojima, K., Messinger, J. D., Mobley, J. A. &
Curcio, C. A. (2010). Abundant lipid and protein components of drusen. PLoS One.
5: e10329.
Wang, S. & Kaufman, R. J. (2012). The impact of the unfolded protein response on human
disease. J Cell Biol. 197: 857-867.
Waryah, A. M., Narsani, A. K., Sheikh, S. A., Shaikh, H. & Shahani, M. Y. (2013). The
novel heterozygous Thr377Arg MYOC mutation causes severe Juvenile Open
Angle Glaucoma in a large Pakistani family. Gene. 528: 356-359.

182
Wax, M. B., Tezel, G., Yang, J., Peng, G., Patil, R. V., Agarwal, N., Sappington, R. M. &
Calkins, D. J. (2008). Induced autoimmunity to heat shock proteins elicits
glaucomatous loss of retinal ganglion cell neurons via activated T-cell-derived fas-
ligand. J Neurosci. 28: 12085-12096.
Weber, B. H., Vogt, G., Pruett, R. C., Stohr, H. & Felbor, U. (1994). Mutations in the tissue
inhibitor of metalloproteinases-3 (TIMP3) in patients with Sorsby's fundus
dystrophy. Nat Genet. 8: 352-356.
Weeks, D. E., Conley, Y. P., Tsai, H. J., Mah, T. S., Schmidt, S., Postel, E. A., Agarwal,
A., Haines, J. L., Pericak-Vance, M. A., Rosenfeld, P. J., Paul, T. O., Eller, A. W.,
Morse, L. S., Dailey, J. P., Ferrell, R. E. & Gorin, M. B. (2004). Age-related
maculopathy: a genomewide scan with continued evidence of susceptibility loci
within the 1q31, 10q26, and 17q25 regions. Am J Hum Genet. 75: 174-189.
Wiggs, J. L. (2007). Genetic etiologies of glaucoma. Arch Ophthalmol. 125: 30-37.
Wiggs, J. L., Lynch, S., Ynagi, G., Maselli, M., Auguste, J., Del Bono, E. A., Olson, L. M.
& Haines, J. L. (2004). A genomewide scan identifies novel early-onset primary
open-angle glaucoma loci on 9q22 and 20p12. Am J Hum Genet. 74: 1314-1320.
Wilensky, J. T. (1999). The role of medical therapy in the rank order of glaucoma
treatment. Curr Opin Ophthalmol. 10: 109-111.
Wilkinson, C. H., Van Der Straaten, D., Craig, J. E., Coote, M. A., Mccartney, P. J.,
Stankovich, J., Stone, E. M. & Mackey, D. A. (2003). Tonography demonstrates
reduced facility of outflow of aqueous humor in myocilin mutation carriers. J
Glaucoma. 12: 237-242.
Wilson, A. G., Symons, J. A., Mcdowell, T. L., Mcdevitt, H. O. & Duff, G. W. (1997).
Effects of a polymorphism in the human tumor necrosis factor alpha promoter on
transcriptional activation. Proc Natl Acad Sci U S A. 94: 3195-3199.
Wilson, M. R., Hertzmark, E., Walker, A. M., Childs-Shaw, K. & Epstein, D. L. (1987). A
case-control study of risk factors in open angle glaucoma. Arch Ophthalmol. 105:
1066-1071.
Wirtz, M. K., Samples, J. R., Kramer, P. L., Rust, K., Topinka, J. R., Yount, J., Koler, R.
D. & Acott, T. S. (1997). Mapping a gene for adult-onset primary open-angle
glaucoma to chromosome 3q. Am J Hum Genet. 60: 296-304.
Wirtz, M. K., Samples, J. R., Rust, K., Lie, J., Nordling, L., Schilling, K., Acott, T. S. &
Kramer, P. L. (1999). GLC1F, a new primary open-angle glaucoma locus, maps to
7q35-q36. Arch Ophthalmol. 117: 237-241.

183
Wolf, C., Gramer, E., Muller-Myhsok, B., Pasutto, F., Reinthal, E., Wissinger, B. &
Weisschuh, N. (2009). Evaluation of nine candidate genes in patients with normal
tension glaucoma: a case control study. BMC Med Genet. 10: 91.
Wolfs, R. C., Klaver, C. C., Ramrattan, R. S., Van Duijn, C. M., Hofman, A. & De Jong,
P. T. (1998). Genetic risk of primary open-angle glaucoma. Population-based
familial aggregation study. Arch Ophthalmol. 116: 1640-1645.
Xu, C., Bailly-Maitre, B. & Reed, J. C. (2005). Endoplasmic reticulum stress: cell life and
death decisions. J Clin Invest. 115: 2656-2664.
Xu, Q., Bernardo, A., Walker, D., Kanegawa, T., Mahley, R. W. & Huang, Y. (2006).
Profile and regulation of apolipoprotein E (ApoE) expression in the CNS in mice
with targeting of green fluorescent protein gene to the ApoE locus. J Neurosci. 26:
4985-4994.
Yamada, Y., Ishibashi, K., Bhutto, I. A., Tian, J., Lutty, G. A. & Handa, J. T. (2006). The
expression of advanced glycation endproduct receptors in rpe cells associated with
basal deposits in human maculas. Exp Eye Res. 82: 840-848.
Yang, X., Hu, J., Zhang, J. & Guan, H. (2010). Polymorphisms in CFH, HTRA1 and
CX3CR1 confer risk to exudative age-related macular degeneration in Han
Chinese. Br J Ophthalmol. 94: 1211-1214.
Yates, J. R., Sepp, T., Matharu, B. K., Khan, J. C., Thurlby, D. A., Shahid, H., Clayton, D.
G., Hayward, C., Morgan, J., Wright, A. F., Armbrecht, A. M., Dhillon, B., Deary,
I. J., Redmond, E., Bird, A. C. & Moore, A. T. (2007). Complement C3 variant and
the risk of age-related macular degeneration. N Engl J Med. 357: 553-561.
Yildirim, O., Ates, N. A., Tamer, L., Muslu, N., Ercan, B., Atik, U. & Kanik, A. (2004).
Changes in antioxidant enzyme activity and malondialdehyde level in patients with
age-related macular degeneration. Ophthalmologica. 218: 202-206.
Yorio, T., Krishnamoorthy, R. & Prasanna, G. (2002). Endothelin: is it a contributor to
glaucoma pathophysiology? J Glaucoma. 11: 259-270.
Yoshioka, K., Yoshida, T., Takakura, Y., Umekawa, T., Kogure, A., Toda, H. &
Yoshikawa, T. (2006). Relationship between polymorphisms 804C/A and 252A/G
of lymphotoxin-alpha gene and -308G/A of tumor necrosis factor alpha gene and
diabetic retinopathy in Japanese patients with type 2 diabetes mellitus. Metabolism.
55: 1406-1410.
Yu, L., Croze, E., Yamaguchi, K. D., Tran, T., Reder, A. T., Litvak, V. & Volkert, M. R.
(2014). Induction of a Unique Isoform of the NCOA7 Oxidation Resistance Gene
by Interferon beta-1b. J Interferon Cytokine Res. DOI: 10.1089/jir.2014.0115

184
Yu, Y., Bhangale, T. R., Fagerness, J., Ripke, S., Thorleifsson, G., Tan, P. L., Souied, E.
H., Richardson, A. J., Merriam, J. E., Buitendijk, G. H., Reynolds, R.,
Raychaudhuri, S., Chin, K. A., Sobrin, L., Evangelou, E., Lee, P. H., Lee, A. Y.,
Leveziel, N., Zack, D. J., Campochiaro, B., Campochiaro, P., Smith, R. T., Barile,
G. R., Guymer, R. H., Hogg, R., Chakravarthy, U., Robman, L. D., Gustafsson, O.,
Sigurdsson, H., Ortmann, W., Behrens, T. W., Stefansson, K., Uitterlinden, A. G.,
Van Duijn, C. M., Vingerling, J. R., Klaver, C. C., Allikmets, R., Brantley, M. A.,
Jr., Baird, P. N., Katsanis, N., Thorsteinsdottir, U., Ioannidis, J. P., Daly, M. J.,
Graham, R. R. & Seddon, J. M. (2011). Common variants near FRK/COL10A1 and
VEGFA are associated with advanced age-related macular degeneration. Hum Mol
Genet. 20: 3699-3709.
Yucel, D., Yilmaz, M., Durukan, A. H. & Ozgul, R. K. (2012). Association of CFH Y402H
polymorphism with both forms of advanced age-related macular degeneration in
Turkish patients. Ophthalmic Genet. 33: 144-149.
Zareparsi, S., Branham, K. E., Li, M., Shah, S., Klein, R. J., Ott, J., Hoh, J., Abecasis, G.
R. & Swaroop, A. (2005). Strong association of the Y402H variant in complement
factor H at 1q32 with susceptibility to age-related macular degeneration. Am J Hum
Genet. 77: 149-153.
Zeng, R., Zhang, X., Wu, K., Su, Y. & Wen, F. (2014). MMP9 gene polymorphism is not
associated with polypoidal choroidal vasculopathy and neovascular age-related
macular degeneration in a Chinese Han population. Ophthalmic Genet. 35: 235-
240.
Zenkel, M., Kruse, F. E., Junemann, A. G., Naumann, G. O. & Schlotzer-Schrehardt, U.
(2006). Clusterin deficiency in eyes with pseudoexfoliation syndrome may be
implicated in the aggregation and deposition of pseudoexfoliative material. Invest
Ophthalmol Vis Sci. 47: 1982-1990.
Zenkel, M., Poschl, E., Von Der Mark, K., Hofmann-Rummelt, C., Naumann, G. O., Kruse,
F. E. & Schlotzer-Schrehardt, U. (2005). Differential gene expression in
pseudoexfoliation syndrome. Invest Ophthalmol Vis Sci. 46: 3742-3752.
Zhang, K., Zhang, L. & Weinreb, R. N. (2012). Ophthalmic drug discovery: novel targets
and mechanisms for retinal diseases and glaucoma. Nat Rev Drug Discov. 11: 541-
559.
Zhang, M. X., Ou, H., Shen, Y. H., Wang, J., Coselli, J. & Wang, X. L. (2005). Regulation
of endothelial nitric oxide synthase by small RNA. Proc Natl Acad Sci U S A. 102:
16967-16972.
Zhang, M. X., Zhang, C., Shen, Y. H., Wang, J., Li, X. N., Zhang, Y., Coselli, J. & Wang,
X. L. (2008). Biogenesis of short intronic repeat 27-nucleotide small RNA from
endothelial nitric-oxide synthase gene. J Biol Chem. 283: 14685-14693.

185
Zhao, Y., Wang, S., Sorenson, C. M., Teixeira, L., Dubielzig, R. R., Peters, D. M., Conway,
S. J., Jefcoate, C. R. & Sheibani, N. (2013). Cyp1b1 mediates periostin regulation
of trabecular meshwork development by suppression of oxidative stress. Mol Cell
Biol. 33: 4225-4240.
Zheng, W., Reem, R. E., Omarova, S., Huang, S., Dipatre, P. L., Charvet, C. D., Curcio,
C. A. & Pikuleva, I. A. (2012). Spatial distribution of the pathways of cholesterol
homeostasis in human retina. PLoS One. 7: e37926.
Zhou, L., Cheng, E. L., Rege, P. & Yue, B. Y. (2000). Signal transduction mediated by
adhesion of human trabecular meshwork cells to extracellular matrix. Exp Eye Res.
70: 457-465.
Zhou, L., Li, Y. & Yue, B. Y. (1999). Oxidative stress affects cytoskeletal structure and
cell-matrix interactions in cells from an ocular tissue: the trabecular meshwork. J
Cell Physiol. 180: 182-189.
Zimmerman, T. J. & Kaufman, H. E. (1977). Timolol. A beta-adrenergic blocking agent
for the treatment of glaucoma. Arch Ophthalmol. 95: 601-604.

Annexures

187
Annexure 1 Product size and primer sequences used to amplify the exons and intron-exon
junctions of MYOC and OPTN
Gene Exon Primer sequence 5’ to 3’ Product size (bp)
MYOC 1_A F-CAGGCACCTCTCAGCACAG
406 R-AGCCCCTCCTGGGTCTC
MYOC 1_B F-ACCCAACGCTTAGACCTGG
432 R-TGTAGCAGGTCACTACGAGCC
MYOC 2 F-CAACATAGTCAATCCTTGGGC
255 R-AACACAGCACTAGACATGAATAAAGAC
MYOC 3_A F-GCATGATCATTGTCTGTGTTTG
521 R-GCTGTAAATGACCCAGAGGC
MYOC 3_B F-GAGAAGGAAATCCCTGGAGC
500 R-CCAGGAGCCCTGAGCATC
OPTN 4_A F-GGGGGACAGCTCTATTTTCA
224 R-CTGCTCACCTTTCAGCTGGT
OPTN 4_B F-AAACCTGGACACGTTTACCC
146 R-TAGTGCAAAGGGATGGCATT
OPTN 5_A F-TCCACTTTCCTGGTGTGTGA
218 R-TTTTCCAAGCTCTTCCTTCAA
OPTN 5_B F-CAGAAGGAAGAACGCCAGTT
160 R-CATCACAATGGATCGGTCTG
OPTN 6_A F-ATGGTGCCCAGCCTTAGTTT
201 R-CGCTGGAGTTCAGCTTGAG
OPTN 6_B
F-CCAGGTGGTGAGGCTACAAG 219
R-CAATCCTTGGCTTGTGTTGA
OPTN 7
F-TGGGTTGCATGTCACAAAAA 206
R-GACAGCCCGAGTCTTCCTTC
OPTN 8_A
F-TTGGAATTTTTCTGATGAAAACC 154
R-CTGATTCCCTTCCCTTAGGC
OPTN 8_B F-CAGATGGGGCCAAGAATTAC
214 R-CTTTAAATGGGTGAACTGTATGG
OPTN 9 F-CCCAATTGTAAACAATGTTCTTTTT
244 R-GTGTGTGGGTGTGGTAGTGG
Larger exons were split into two amplicons A & B. F; Forward, R; Reverse

188
Annexure 1 cont.
Gene Exon Primer sequence 5’ to 3’ Product
size (bp)
OPTN 10
F-TGGTTCAGCCTGTTTTCTCC 235
R-TCAAAGGAGGATAAAATTGCTCTC
OPTN 11
F-TTAAAAGCCACTGCGACGTA 239
R-GCTGCCCTTCTGACTCAACA
OPTN 12
F-ATTTTCCCCAGGATTCCATT 194
R-AACGTTCAACAGTTTCTGTTCATT
OPTN 13
F-ACTAAAACAGGCAGAATTATTTCAA 242
R-AGCTGGGGTTTTGGAAGGT
OPTN 14
F-CGCATAAACACTGTAAGAATCTGC 236
R-GATGTGAGCTCTGGGTCCTC
OPTN 15
F-TGTCATGTTTCGGGGTTGTA 213
R-TGAAGTGGAATTTTTCTTCAAGC
OPTN 16
F-CGCCATCTGTTCTTCAAGTG 232
R-ACCAACAGTTTTGGGGAGGT
F; Forward, R; Reverse

189
Annexure 2 Product size and primer sequences used to amplify exons and intron-exon
junctions of WRD36 and CYP1B1
Gene Exon Primer sequence 5’to 3’ Product size (bp)
CYP1B1 1_A F-GGAGTCCGGGTCAAAGC
577 R-AAAGTACCTACCACGCCACC
CYP1B1 1_B F-GTCACTGAGCTAGATAGCCT
844 R-GGACAGTTGATTTATGCTCACC
CYP1B1 2 F-AGACCACGCTCCTGCTACTC
168 R-GAGCGAACGAGAGGTGAGC
WDR36 1 F-CTAGGCAACGTGCTGGAGAC
463 R-GAGTTAGAGGCCAAGGAGGG
WDR36 2 F-GAGGTTATATCTTAATCTTCAGGTG
211 R-TTACCTTGGCTTCCTTATATGC
WDR36 3 F-CAAGGTGATTTCCTATCCTTAGTTTG
409 R-TAGTTCCAGAGTGTGCTGGG
WDR36 4 F-AACAGAAGCATCTCAGGATTAGC
321 R-TTTACAGGCAAAATCTCTGGC
WDR36 5 F-AAATTACATTTACAAGTTGCCTCTC
475 R-CCTCTGATACAGGGGACCAAC
WDR36 6 F-TGTAGCTGATATTGTTTTCCTCC
185 R-TCCTGAAACTGAAGGATTTTCC
WDR36 7 F-TTTGATAACACCTAATAATGATGCG
350 R-TTGCCTTTTACTCCAGTATTCATTC
WDR36 8 F-TGAATACTGGAGTAAAAGGCAAAG
492 R-TGCAATCATGTCACCTGCTG
WDR36 9 F-GCTTGCAGATCAGATGGAAC
247 R-CAAACCTCATACTGGGCACC
WDR36 10 F-TTCCCTTTAAAGTGTCCCAAAC
274 R-TTGATGAAACTTCCTCCAGTTG
WDR36 11 F-TTTCTGACTTAAATGGGAATATCTTG
278 R-AAAACAGCATACAGTAGGAAATAAATG
WDR36 12 F-AGTGTCTGAAATATTGGATGCC
375 R-TTTGTGGCTTTGGGTTATGC
WDR36 13 F-GCTTTGGAAAGCATAAAGTGC
306 R-TGATTATAACCCATCTTCAACTTTAG
Exon 1 was split into two amplicons A & B, F; Forward, R; Reverse

190
Annexure 2 cont.
Gene Exon Primer sequence 5’to 3’ Product size (bp)
WDR36 14-15
F-TGTGTATTGTTCAGAGAGAAACACTG 620
R-GGATAACACACCCAAACAAAAG
WDR36 16
F-TGAAGCCTGCATTATCTTTTC 318
R-AAAGCATATAACCCATTAACTATCGG
WDR36 17
F-GACTTTCTGATCAATGCTGGTG 437
R-GCTGTCTACATTATCAAGCAGATG
WDR36 18
F-GCATATTCGCACTCTGACTTACTC 551
R-TGCACTAAACTTTGCCTTTGG
WDR36 19
F-CATTGAAGAAGGTGTTTTGGG 577
R-CATCCAAATGTCTGCTGAGTG
WDR36 20-21
F-GAAATTAAATATGAGAAACTGTTGGC 541
R-TGAGAACGCTGATATTTCCTTC
WDR36 22
F-TCAATTATTTTGGGTTTCATTCTAC 413
R-AGATAGCACTGCCCCAGAAG
WDR36 23
F-TGTCTTTTGTGGTTCCTTGG 326
R-TCACATTGACACTTGGAAAATAAG
F; Forward, R; Reverse

191
Annexure 3 Standard PCR reagent concentrations
Reagent Stock
Concentration
Working
concentration
Reaction
volume (25µl)
Annealing
temperature
dNTPs 25mM 0.2mM 0.2µl
58 oC
Buffer 10X 1X 2.5µl
MgCl2 25mM 1.5mM 1.5µl
Forward Primer 10µM 0.2µM 0.5µl
Reverse primer 10µM 0.2µM 0.5µl
Taq polymerase 5U/µl 1U 0.2µl
gDNA - 100ng/µl 2µl
PCR water - - 17.6µl

192
Annexure 4 Product size and primer sequence and PCR products for candidate genes in the
homozygous regions of GLC 2, GLC 4 and GLC 8
Gene Exon Primer Sequence Product size
(bp)
TMEM74 1 F-CTGGCCTACAACTCCCG
R-ATTCGAGGTACGGATGTGTC 340
2_A F-AGGAGCAACACTCCTGGAAG
R-TCCCCAGGGTGATTATGC 523
2_B F-TGCAGCCAGGAATTAGAAAC
R-AGTTTTGCAGACTCTTTGGAAG 515
2_C F-GGCGTCATCCTGTCCTG
R-AAGAAATAATTTGTAGACTGGGTC 501
2_D F-CAGCCACACCTATCCTTCTG
R-TGACCCTGGCTAATATCTGG 507
2_E F-ATGTTGGGCTTTCCTTATTG
R-TGTGAGTGGGAGGTGAGTTC 616
PXDN 1 F-CCCTCGGGGATTCAGAG
R-TTCGGAGGTTCCCTTCTG 518
2 F-GCAAATGTGTAGCGATGTTTG
R-TGAGTTCTACCTACAGATAAACAATG 212
3 F-AATGTGACCTTTTCCAAGGC
R-CAATAATTCATAAGCAGCACG 260
4 F-TTTCCGTCTGAAGTTTGACC
R-ACTCCACTGGTCCCTACAAG 210
5 & 6 F-TGATATCTGAATTTGAAATGACTAGG
R-GAATCAGATTGTTATCAACATTTCAC 709
7_A F-CTGATGGATGGATGGACAAG
R-TGATGGTTGCCACTGAGC 213
7_B F-CTCAAACACACTTCACTGCG
R-GTCTGTGTCTGCATGTGTGTC 664
8 F-CATCTGTGGTTTCCTTTTGG
R-TGTGGTTTGGGTGTCTGAG 290
9 F-GGGTGAGGTACGTCTTTGTG
R-AGGCAGATAGTGAGGGACG 291
10 F-AAACCATGTCAAACCGGG
R-GCTAGTGGAGGGGTGAGG 388
Larger exons were split into two or more amplicons A, B, C, D & E, F; Forward, R; Reverse

193
Annexure 4 Cont.
Gene Exon Primer Sequence Product size
(bp)
11 F-AGACGTCTGCCAAGACTGTG
R-GTGGAAATGTGTGCTTCCTG 399
12 F-CAGGAGTTCTCCATGCG
R- CAACGCTTTATAACGAAGAGTAAC 319
13 F- GCAGGGGATTTTGTTCTTC
R- CAGCCCGTCTACCTTGTATC 244
14 F- CCCAACCCTAGGTCAGATAAC
R- ACACTAGGGACCTGCGG 297
15 F- ATGCCTTGTGGCTAATGATG
R- TAATCACTCCCACCTTCACC 271
16 F- AGCAATGATTATATTTTGGGG
R- GTTCAACCCCGTTACTCAG 298
17_A F- CCCTCACACATCCTCCAG
R- CTGTCCGTCGGAGAAGC 486
17_B F-GAGAATGGCTTCAACACCC
R-CATAGTAGATGGTGTCGCCG 736
17_C F-TCAACCAGCTCACCTCCTAC
R-TTGCAGTAGACCCTGTAGTCG 826
17_D F-CGGCGACACCATCTACTATG
R-AGGTTCCCATCTTGACCTTC 735
18 F-AGCATTGTGGAGAGATGCAG
R-AGAAGATACCAGGGCCTCAG 465
19 F-GTGACCTGTGAGTCTCCTGC
R-AGCAGTCACCAAAACCAGG 322
20 F-CTTAATTTCCCCGAGGTCAG
R-AGGATGCCGGTCCTACTG 260
21 F-CCAGGAAACCTTGAAATGAG
R-AGGGCTGTGCTGCTGTG 268
22 F-GCCAAGCTGTTACTCTGAAG
R-GGACTCTCGGACTTGCG 225
23 F-GAGCTGACAGGCTTTGCTC
R-ACCCGATCTCACGATGG 243
Exons 17 was split into 4 amplicons A, B, C & D. F; Forward, R; Reverse

194
Annexure 5 Product size and primer sequences for the gene SH3PXD2B
Exon Primer sequence Product
size (bp)
1 F-AGCTCCAGGTTCCCTGC
R-GGAGGCAGAAGTTTTCCAAG 262
2 F-AACCCACGTCTTTCTGACTCT
R-TGGACTCTAAAGCTGTAGTGGAA 266
3 F-AAATGTCCTAGATGATGTTTAGTGC
R-AGGGCTCTGGGAACTGTAAC 206
4 F-CTGAGAGCTTGTCCCTGTTC
R-TTTTATTGTTGAGCATCTTGTAGC 221
5 F-TGGGTTTGCTTTTGTGTTTG
R-GCTAAGTGAAGTGCGGTCTC 452
6 F-TCACGTCAATACATGGCAAG
R-CCTGGTGCACAGTTGGTG 164
7 F-GCTCTGACTCCTGCTCTTTC
R-TTCCAAATGTTTCATGTCCC 270
8 F-ATTCACTGGTACAGTGGCTG
R-AGGCCAAAAGAAGAGATTGG 295
9 F-GGATTACGGCATCCCAAG
R-GTCCCTGTGACCCCAAAC 255
10 F-GTGATTCCCAGTAGGAGCAA
R-TCTGGGCCTCTGTTTTCTTA 445
11 F-ATAGACCCGACCTGGCAC
R-CTAGTGGACACCCCTCACAG 189
12 F-ACAGGGTCGCAGGAGTG
R-GACAGGGGAGAAGTAGGAGG 257
13_A
F-CAAACCATTCCATCTGCTG
R-ATCGGCAAAATCACGCC 564
13_B
F-TCAGCAGGCTACGAGGAG
R-GGCAGGCCTGAGCTTAC 507
13_C
F-GAGAAGCCAGATGCCACTC
R-TGGAGAGAAAAGGTTTGGC 556
13_D
F-AAACCTCTTCGTCATCCAGG
R-AATACGTGGGTAAAGCCAGC 494
Exon 13 was split into 4 amplicons A, B, C & D. F; Forward, R; Reverse

195
Annexure 6 Homozygous regions obtained in the affected members of family GLC 2, GLC
4 and GLC 8
Family GLC 2
Chromosome Flanking SNP Boundaries (Mbs) Size (Mbs)
Chr. 3 rs2372548-rs12715538 43,801,895-58,931,816 15.1
Chr. 7 rs2354332-rs4727933 138,534,971-147,937,132 9.4
Chr. 15 rs1104848-rs12914158 56,112,714-58,070,608 1.9
Chr. 15 rs2970374-rs1816625 60,108,779-61,437,557 1.3
Chr. 15 rs2044029-rs9920103 71,679,959-78,435,527 6.7
Family GLC 4
Chr. 1 rs7512461-rs16861320 102408762-168665346 66.25
Chr. 2 rs4954099-rs6758983 134757957-175192260 40.43
Chr.10 rs4980024-rs10886726 80839269-122386632 41.54
Family GLC 8
Chr. 3 rs17746160-rs2710779 148,533,397-192,100,439 43.56
Chr. 4 rs1315962-rs6535574 111,033,550-148,928,801 37.89
Chr. 6 rs6927090-rs6456313 25,214,5-20,251,699 19.99
Chr.11 rs11602762-rs7121949 116,129,53-312,881,60 19.67
SNP, single nucleotide polymorphism; Mbs, mega bases

196
Annexure 7 Unsolved glaucoma Families A; JOAG family GLC4, B; Late glaucoma onset family GLC6, C; Late glaucoma onset
family GLC7, D; Late glaucoma onset family GLC 9, E; A PACG family GLC10 and F; Late glaucoma onset family GLC11.

197
Annexure 7 Continued. G; Late onset POAG family GLC12, H; A PACG GLC13, I; A PACG family GLC14, J; A JOAG family
GLC15, K; Recessive PCG Family GLC1

Published and Submitted Data

199
1. Association of a polymorphism in the BIRC6 gene with Pseudoexfoliative
Glaucoma. Ayub H., Micheal S., Akhtar F., Khan M.I., Bashir S., Waheed
N.K., Ali M., E-Koller F., Shafique S., Qamar R and Hollander AI. PLoS One.
2014;13;9(8):e105023.
2. Association of known common genetic variants with primary open angle,
primary angle closure, and pseudoexfoliation glaucoma in Pakistani cohorts.
Micheal S., Ayub H., Khan M.I., Bakker B., E-Koller F., Ali M., Akhtar F.,
Khan W., Qamar R and Hollander AI. Mol Vis 2014 20: 1471-1479.
3. Identification of novel CYP1B1 gene mutations in patients with primary
congenital and primary open angle glaucoma. Micheal S., Ayub H., Zafar SN.,
Bakker B., Ali M., Akhtar F., Islam F., Khan MI., Qamar R and Hollander A.I.
Clin Experiment Ophthalmol. doi: 10.1111/ceo.12369.
4. Genetic spectrum of autosomal recessive non-syndromic hearing loss in
Pakistani families. Shafique S., Siddiqi S., Schraders M., Oostrik J., Ayub H.,
Bilal A., Ajmal M., Seco C.Z., Strom T.M., Mansoor A., Mazhar K., Shah S.T.,
Hussain A., Azam M., Kremer H and Qamar R. PLoS One. 2014;
20;9(6):e100146.
5. Exome sequencing identifies three novel candidate genes implicated in
intellectual disability. Agha Z., Iqbal Z., Azam M., Ayub H., Vissers E.L.M.,
Gilissen C., Ali S.H.B., Riaz M., Veltman J.A., Pfundt R., van Bokhoven H and
Qamar R. DOI: 10.1371/journal.pone.0112687.
6. A genetic variant in TMCO1 is strongly associated with primary open angle,
primary angle closure and pseudoexfolation glaucoma. Micheal S., Ayub H.,
Islam F., Khan W.A., Akhtar F., Khan M.I., Qamar R and Hollander I.A. Invest
Ophthalmol Vis Sci 2013;54: E-Abstract 6233.
7. Exome sequencing identifies a novel and a recurrent BBS1 mutation in
Pakistani families with Bardet-Biedl syndrome. Ajmal M., Khan M.I., Neveling

200
K., Tayyab A., Jaffar S., Sadeque A., Ayub H., Abbasi N.M., Riaz M., Micheal
S., Gilissen C., Ali S.H., Azam M., Collin RW., Cremers F.P and Qamar R. Mol
Vis. 2013;19:644-53.
8. The genetic spectrum of familial hypercholesterolemia in Pakistan. Ahmed W.,
Whittall R., Riaz M., Ajmal M., Sadeque A., Ayub H., Qamar R and Humphries
SE. Clin Chim Acta. 2013 Jun 5;421:219-25. doi: 10.1016/j.cca.2013.03.017.
9. Association of eNOS and HSP70 gene polymorphisms with glaucoma in
Pakistani cohorts. Ayub H., Khan M.I., Micheal S., Akhtar F., Ajmal M.,
Shafique S., Ali S.H.B., Hollander A.I, Ahmed A and Qamar R. Mol. Vis. 2010;
16:18-25.
10. Association studies of tumor necrosis factor-alpha -308G/A polymorphism with
primary open-angle and angle closure glaucoma in Pakistani patients Asghar
J., Micheal S., Akhtar F., Ayub H., Khan M.I., Waheed N.K., Khurram R., Ali
M., Ali S.H.B., Hollander A.I and Qamar R. (Submitted).
11. Screening of myocilin and optineurin genes in a cohort of Pakistani glaucoma
families and sporadic cases. Ayub H., Micheal S., Akhtar F., Ali M., Waheed
N.K., Ali S.H.B., Bashir S., Riaz M., Shafique S., Qazi N.A., Hashmi S., Khan
M.I., E-Koller F., Hollander A.I and Qamar R. (Submitted).
12. Homozygosity mapping and targeted Sanger sequencing reveal genetic defects
underlying inherited retinal disease in families from Pakistan. Maria M., Ajmal
M., Azam M., Waheed NK., Siddiqui SN., Mustafa B., Ayub H., Ali L., Ahmad
S., Micheal S., Hussain A., Shah S.T.A., Ali S.H.B., Ahmed W., Khan Y.M.,
Hollander A.I., Haer-Wigman L., Collin R.W.J., Khan M.I, Qamar R and
Cremers F. (Submitted).
13. Variants in the ASB10 gene are associated with primary open angle glaucoma.
Micheal S., Ayub H., Islam F., Khan W.A., Akhtar F., Khan M.I., Qamar R and
Hollander I.A. (Submitted).

201
14. Case control association study relates the Apoptotic and Stress related gene
polymorphisms with glaucoma in Pakistani population. Ayub H., Shafique S.,
Micheal S., Akhtar F., Khan M. I., Ali M., Ali L., Ali S. H. B., Riaz M., Ahmad
S., Hollander A.I and Qamar R. (In preparation).
15. Association of a polymorphism in the HTRA1/ARMS2 with Age Related
Macular Degeneration in Pakistani population. Ayub H., Shafique S., Azam A.,
Qazi N.A., Akhtar F., Khan M.A., Ayub A., Bashir S., Bakker B., E-Koller F.,
Shakil A., Qamar R and Hollander, A.I. (In preparation)
16. Association of a polymorphism in the MMPs with Age Related Macular
Degeneration in Pakistani population. Ayub H., Shafique S., Azam A., Qazi N.
A., Akhtar F., Khan M.A., Ayub A., Bashir S., Ali L., Qamar R and Hollander,
A.I. (In preparation)
17. Association of a polymorphism in the CX3CR1 with Wet AMD in Pakistani
population. Ayub H., Shafique S., Azam A., Qazi N. A., Akhtar F., Khan M.A.,
Ayub A., Bashir S., Qamar R and Hollander, A.I. (In preparation)