Weekly Global COVID-19 Update: Part 3...e.g. diagnostic imaging Wait listed elective cases, e.g....
23
Presented by Vidal Seegobin, Global Forum for Health Care Innovators What you need to know in 30 minutes Weekly Global COVID-19 Update: Part 3 27 April 2020
Transcript of Weekly Global COVID-19 Update: Part 3...e.g. diagnostic imaging Wait listed elective cases, e.g....

Presented by
Vidal Seegobin, Global Forum for Health Care Innovators
What you need to know in 30 minutes
Weekly Global COVID-19 Update: Part 3
27 April 2020

© 2020 Advisory Board • All rights reserved • advisory.com
Today’s Research Expert
Vidal Seegobin
Practice Manager, International Research
Vidal is a practice manager on the Global Forum for Health Care
Innovators—Advisory Board International's health care strategy
programme.
Prior to joining the Advisory Board, he worked as a researcher on
disease surveillance and pandemic response. He holds a master's
degree in international economics from American University and a
bachelor's degree in international business from Carleton University
in Ottawa, Canada.
[email protected] @SeegobiV
Vidal photo

© 2020 Advisory Board • All rights reserved • advisory.com
6
1
10
100
1000
0 5 10 15 20 25 30 35 40 45 50 55 60
Number of days since 3 daily deaths first recorded
Spain
Italy
U.S.
South Korea
U.K.
France
Germany
4000
1. Current as of 04/25/2020.
Source: Bernard S et al., “Coronavirus Tracked: The Latest Figures as the
Pandemic Spreads,” Financial Times, 2020; Roser M et al., “Coronavirus
Disease (COVID-19) – Statistics and Research,” Our World in Data, 2020.
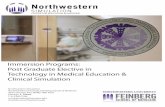
‘Peak’ of curve proving to be a long plateau
Advisory Board interviews and analysis.
Daily coronavirus deaths (rolling 3-day average), by number of days since 3 daily deaths first recorded1
Country Total deaths
per million
Spain 482
Italy 430
France 341
U.K. 287
U.S. 154
Germany 66
South Korea 5

© 2020 Advisory Board • All rights reserved • advisory.com
7
Singapore tightens social distancing measures after recent COVID resurgence
A second surge undermining some initial successes
Advisory Board interviews and analysis.
Missed population leads to resurgence in cases Early action intended to capture entire population
Immediate border closures
Rapid testing in over 1,000
newly-established private clinics
Extensive contact tracing through
TraceTogether phone application
Heavily-enforced social
distancing measures
Source: J Guy and J Griffiths, “Singapore threatens 6 months in jail for breaking social distancing laws”, CNN, 27 March, 2020; M Sullivan, “Singapore Sees Surge in COVID-19 Cases, Now has Highest Number in
Southeast Asia”, NPR, April 20, 2020; R Pung et al., “Investigation of three clusters of COVID-19 in Singapore: implications for surveillance and response measures”, The Lancet, 28 March, 2020; “COVID-19: Cases
in Singapore”, Singaporean Government Agency Website, 23 April, 2020; “Circuit Breaker extension and tighter measures: What you need to know”, Singaporean Government Agency Website, 21 April, 2020.
New COVID-19
cases between
20-24 April
5,487Of new cases are
migrant workers
residing in dormitories
95%
‘Circuit Breaker’ extended and tightened
• Stay-at-home order
extended until 1 June
• Less critical services and
business suspended
• Schools to be
temporarily closed
DATA SPOTLIGHT
• Opticians operate by
appointment only
• Employees expected
to telecommute, if
possible

© 2020 Advisory Board • All rights reserved • advisory.com
8
Source: P Chan-kyong, “South Korean patients who test positive for reactivated coronavirus have ‘little or no infectivity’, officials say”, South
China Morning Post, 23 April, 2020; J Power, “Poor immunity or mutations? South Korea investigates ‘shrewd’ coronavirus as reinfections creep
up”, South China Morning Post, 16 April, 2020; H Shin, “South Korea finds patients testing positive post-recovery from coronavirus barely
infectious”, Reuters, 22 April, 2020; “South Korean firm starts production for rapid antibody testing kits in India”, Times of India, 22 April, 2020.
South Korea highlights knowledge-gap in disease immunity
Advisory Board interviews and analysis.
Questions still to be answered
If patients can be reinfected, how
effective will an antibody vaccine be?
How long will antibodies provide
immunity, if at all?
Can the virus be reactivated after a
period of time?
What we know
207 South Korean patients have tested
positive for COVID-19 after
previously recovering
South Korean experts have found
patients who are ‘reinfected’ to have
little to no infectivity to others
On 19 April, South Korean firm
launches its test kit production, with
a production capacity of 500,000
tests per week
What is the likelihood of being infected
by a different strain of SARS-Cov-2?

© 2020 Advisory Board • All rights reserved • advisory.com
9
Source: “Malaysia turns to coronavirus antibody tests to supplement laboratory checks”, WHBL, April 14, 2020; T You, “Chinese police wear smart helmets equipped with AI-powered infrared cameras to detect
pedestrians with fevers as they patrol the streets amid coronavirus crisis”, Daily Mail, March 4, 2020; “Help speed up contact tracing with TraceTogether”, Singapore Government Website, March 21, 2020.
Focus and solutions needed for three unanswered questions
At minimum, what we need from public health to reopen
Who is immune? How is it spreading?Who has it and doesn’t know?
Antibody tests
To understand community
spread and immunity
levels in the population
What is needed
to reopen,
state-by-state
What’s in the
way of doing
more?
Disease surveillance
To scan populations broadly
for early symptoms and
collect data
Scaled contact tracing
To isolate those who
may have been exposed
to symptomatic people
Singapore
TraceTogether app tracks
contact between people
using Bluetooth
Where it’s
already
happening
China
Chinese police wear smart
helmets equipped to check
pedestrians for fevers
Few commercially available,
government-approved tests
Malaysia
Antibody tests used in
conjunction with PCR1 tests
during quarantine periods
Training and deploying newly
idled government workers
Potential infringement on
personal privacy laws
Advisory Board interviews and analysis.
1. Polymerise chain reaction.

© 2020 Advisory Board • All rights reserved • advisory.com
10
Source: N Evershed et al., “Coronavirus numbers in Australia: how many new cases are there? Covid-19 map, statistics
and graph”, The Guardian, 23 April, 2020; ”Government eases elective surgery restrictions”, Australian Government
Department of Health, 21 April, 2020; “National Cabinet update, media release,” Prime Minister of Australia, 26 March 2020.
Elective surgeries start to reopen as daily new case count dwindles
Australia’s reality soon expected to become the norm
Advisory Board interviews and analysis.
0
50
100
150
200
250
300
350
400
450 Excerpt
Government eases elective
surgery restrictions
The Australian Government will gradually ease restrictions
on elective surgery from Tuesday 28 April 2020.
The easing will cover:
• IVF
• Screening programs (cancer and other diseases)
• Post cancer reconstruction procedures (such as breast
reconstruction)
• Procedures for children under 18 years of age
• Joint replacements (including knees, hips, shoulders)
• Cataracts and eye procedures
• Endoscopy and colonoscopy procedures
Timeline of COVID surgery limits against daily new cases
21 April 2020Excerpt
Temporary suspension of all
semi-urgent elective surgery
26 March 2020

© 2020 Advisory Board • All rights reserved • advisory.com
11
Three patient demand waves moving forward
Advisory Board interviews and analysis.
Assessing potential cases after COVID surge passes
Challenge: Surge in delayed procedures
while productivity dips due to sanitation
requirements and scarce PPE; must treat
all patients as COVID-positive upon
entering
Patient types:
Immediate: COVID demand
Challenge: Sudden influx of COVID
patients requiring isolation and new
pathways; some systems experiencing
consequences without elective revenue
Patient types:
Imminent: Postponed demand
Looming: Complex demand
Challenge: Latent demand growth from
delayed diagnostics, planned, and
unplanned care; chronic patients return;
must treat all patients as COVID-positive
Patient types:
Newly infected COVID patients
ICU-requiring COVID patients
Readmitted COVID patients
Rescheduled non-urgent
cases, e.g. hip replacement
Discontinued care of chronic
condition, e.g. diabetes, COPD
Delayed emergency clinical and
behavioural needs, e.g. PCI
Rescheduled but deteriorated
elective patients, e.g. GI surgery
Delayed diagnosis of long-term
conditions, e.g. breast cancerPlanned semi-urgent cases,
e.g. diagnostic imaging
Wait listed elective cases, e.g.
non-invasive vascular care\

© 2020 Advisory Board • All rights reserved • advisory.com
12
Three shifts in approach to sustain the system
Advisory Board interviews and analysis.
Challenge: Surge in delayed procedures
while productivity dips due to sanitation
requirements and scarce PPE; must treat
all patients as COVID-positive upon
entering
Immediate: COVID demand
Challenge: Sudden influx of COVID
patients requiring isolation and new
pathways; some systems experiencing
consequences without elective revenue
Imminent: Postponed demand
Looming: Complex demand
Challenge: Latent demand growth from
delayed diagnostics, planned, and
unplanned care; chronic patients return;
must treat all patients as COVID-positive
From PPE acquisition to PPE reuse
From hospital reinforcement to continuum reinforcement
From staff expansion to staff resilience

© 2020 Advisory Board • All rights reserved • advisory.com
13
Lack of redundancy across the supply chain prevents flexibility in times of crisis
Why not just make more PPE?
Advisory Board interviews and analysis.
Factors that limit flexibility across the supply chain
ManufacturingProvider
contracting
Providers often
contract with a
limited number of
vendors to secure
preferential pricing
Distribution
Providers favour
just-in-time inventory
management as
opposed to
stockpiling or
holding reserves
Regulators limit
provider use of
certain items by
classifying certain
versions as “medical
grade”; can limit
manufacturers’ ability
to flex production
Regulatory
Suppliers often rely
on the same limited
set of vendors to
source component
parts
Component
parts
Manufacturers
may rely on very
few sources
(often abroad)
for complex or
harvested raw
materials
Raw
materials
Manufacturers
centralise
production (often
in far-away, lower-
cost markets) to
gain economies
of scale
UpstreamDownstream
Shift #1: PPE Reuse

© 2020 Advisory Board • All rights reserved • advisory.com
14
Health systems must balance tradeoffs in ensuring sufficient PPE to reopen
Imperfect solutions to a critical PPE problem
Advisory Board interviews and analysis.
Sustainable
at scale
Major safety and cost considerations
Timeliness
Procure steady stream
of new disposables
Do I have stable,
reliable vendors?
What is the price premium
for guaranteed delivery?
Sanitise and
reuse disposables
Does sanitisation break
down protective materials?
How many times can we
safely reuse?
Spectrum of options for obtaining PPE needed to reopen non-essential services
Use DIY products
from local businesses
and volunteers
Are we compromising on
individual safety?
Can we scale and sustain?
Shift to medical-grade
reusable products
How can we encourage design
and manufacturing of medical-
grade, reusable masks?
What are added costs for
procurement and cleaning?

© 2020 Advisory Board • All rights reserved • advisory.com
15
Source: S Braithwaite, “Almost half of coronavirus deaths in Europe were in care homes, World Health Organization says,” CNN, 23 April, 2020; R Booth and P Duncan, “Coronavirus: England and Wales care home
deaths quadruple in a week,” Guardian, 21 April, 2020; “Fifth death confirmed at Newmarch House aged care home,” Guardian, 24 April, 2020; Stockman F et al., “‘They’re Death Pits’: Virus Claims at Least 7,000
Lives in U.S. Nursing Homes,” New York Times, 17 April, 2020; “Canada: 50% of COVID-19 deaths are aged care residents – Government flags tighter regulation on ownership,” The Weekly Source, 21 April, 2020.
Hotspots emerge across the globe in post-acute, care home facilities
Long-term care now the vulnerable point in the system
Advisory Board interviews and analysis.
DATA SPOTLIGHT
50% Covid-19 deaths in
Europe that occurred in
long-term care facility
residents, according to
estimates from the World
Health Organisation
“Canada: 50% of COVID-
19 deaths are aged care
residents”
The Weekly Source
“Australia coronavirus news: fifth
Covid-19 death at Sydney's
Newmarch House aged care home”
The Guardian
“Coronavirus: England and
Wales care home deaths
quadruple in a week”
The Guardian
“‘They’re Death Pits’: Virus
Claims at Least 7,000 Lives
in US Nursing Homes”
The New York Times
Shift #2: Continuum reinforcement

© 2020 Advisory Board • All rights reserved • advisory.com
16
Sample ways to support long-term care partners
Support post-acute providers to mitigate hotspots
UW Medicine
Collaborating with post-acute partners to:
Advisory Board interviews and analysis.
Set expectations about discharge
strategy and testing capabilities 1
Educate staff on infection
prevention skills and protocols2
Prepare an on-demand team to be
deployed in case of escalation3
We can’t afford the post-acute care providers
to not be ready, that will only create another
surge for us down the line.”
Mary Shepler, CNO
EvergreenHealth
Source: “'Do your planning now': EvergreenHealth CNO's stark warning to American
hospitals,” Advisory Board Daily Briefing, 1 April, 2020; UW Medicine, Washington, US.

© 2020 Advisory Board • All rights reserved • advisory.com
17
1. As of 7 April 2020.
2. The company is called eConsults.
Sources: S Fanel, “Ontario doctors warn of primary care 'crisis' as care shifts to virtual visits,” CTV News, 17 April, 2020; N Bostock, “Millions of patients 'avoiding calls to GP' during COVID-19 pandemic,” GPonline,
25 April, 2020; L Haynes, “Nearly 2,000 GPs self-isolating as BMA demands 'drastic improvement' in testing,” GPonline, 16 April, 2020; L Xing, “As callers wait days to hear from Telehealth Ontario, province says to
call your family doctor,” CBC News, 7 April, 2020; R Browne, “Demand for telemedicine has exploded in the UK as doctors adapt to the coronavirus crisis,” CNBC, 9 April, 2020; Knaus C and McGowan M,
“Australia's small medical practices on brink of collapse amid coronavirus,” Guardian, 8 April, 2020; L Haynes, “Allow GP practices time to regroup after COVID-19, BMA warns NHS chiefs,” GPonline, 22 April 2020.
Influx of complex patients soon to be managed by primary care
As virtual care becomes default, GPs struggling to keep up
Advisory Board interviews and analysis.
Rush to telehealth leaving
demand outpacing supply
Telehealth incentives threatening
primary care economics
‘Cannonball’ of complex GP
visits to hit as wave one eases
Of UK citizens are avoiding
routine GP care because they
are afraid to burden the NHS
during the COVID pandemic
NHSE may need to relax or suspend
primary care network targets to help
general practice cope with a backlog
of work after the coronavirus
pandemic.
40%Estimated UK GPs
self-isolating due to
COVID-19
2,000
Average days1 to respond
to a non-COVID telehealth
inquiry in Ontario
2.5
Increase in monthly
telehealth visits at one2
UK virtual care company
1,200x
Surveyed GPs in Australia
who have lost over 30% of
their expected YTD
revenue amidst national
telehealth boom
How can we keep being
heroes if we’re going to go
bankrupt in our practices?
50%
Family doctor
Ottawa, Canada British Medical Association

© 2020 Advisory Board • All rights reserved • advisory.com
18
Source: “RACE Program provides rapid specialist consults,” Canadian Medical Association Journal ,185, No. 18 (2010).
Formal connection to hospitals gives GPs rapid access to specialist expertise
Specialist knowledge is your most valuable resource
Advisory Board interviews and analysis.
Providence Health Care
8-site health network • Affiliate of Vancouver
Coastal Health • BC, Canada
• Established the RACE telephone
hotline to allow GPs easy access to
needed hospital specialist expertise
• Expanded to 23 specialty areas, each
call to the line saves approximately
$200 in avoided acute care costs
CASE EXAMPLE
Integration Benefits
Better informed GPs provide better care,
often avoiding unnecessary specialist
follow-ups or ED presentations
Quick decision support
Specialists available to speak to GPs and
give treatment advice immediately; majority
of consults happen within 10 minutes
Low-cost infrastructure
Low-tech way for primary care providers to
connect with specialists in over 23 clinical
areas when a difficult patient presents 1/3Of patients avoided
hospital and ED visits
60%Of patients avoided
subsequent
specialist referrals
Tangible benefits
across continuum
hotline’s key pillars:

© 2020 Advisory Board • All rights reserved • advisory.com
19
As surge subsides, staffing challenges will take centre stage
Advisory Board interviews and analysis.
Frontline staffing
shortages
Senior leader
burnout
Negative publicity
as staff speak out
More aggressive
collective bargaining
Anger, distrust
over leadership
surge decisions
Extreme stress,
trauma, and burn out
among frontline staff
Current challenges
Looming
challenges
COVID has eroded staff resilience thus far, but challenges poised to grow
“You know, in combat situations,
soldiers come home and get at
least a few months of R&R. After
COVID, our clinicians are going
to be asked to be even more
productive, with their backlogs
and delayed improvement projects,
and any subsequent COVID
waves. What conclusion is there
other than burnout?"
Director of Workforce,
UK Hospital
Shift #3: Staff resilience

© 2020 Advisory Board • All rights reserved • advisory.com
20
Source: T Hurst and V Reid, “Starter list: How you can support frontline staff during the
Covid-19 crisis,” Advisory Board, 2 April, 2020; A Polyak and M Simmons, “3 ways to meet
the essential needs of your frontline staff during Covid-19,” Advisory Board, 2 April, 2020.
Health systems investing in expanding access to emotional support services
For long-term resilience, focus on staff well-being now
Advisory Board interviews and analysis.
Set up confidential phone line to
navigate staff to behavioural
health support services
Run virtual peer support sessions
once a week to discuss personal
and professional concerns
Leverage local mental health
professionals willing to offer free
virtual therapy to frontline staff
Take care of essential needs,
like meals, transportation,
and childcare
Provide virtual drop-in sessions with
staff who have expertise in providing
mental and emotional support
Create ‘bounce back kits’ with
items like a reflection exercise and
store them in a central location
Partner with local facilities like
YMCAs to provide staff a place to
shower and change after shifts
Widely share open online
resources on coping with
anxiety and stress
Provide onsite or virtual
meditation at various times
across shifts

© 2020 Advisory Board • All rights reserved • advisory.com
21
Source: L Rewers, “The 4 key imperatives for your Covid-19 staffing strategy,” Advisory Board,
17 April, 2020; R Pilling, “Where’s your #WobbleRoom?,” 15 Seconds 30 Minutes, 1 April, 2020.
Embed opportunities in frontline workflow to process grief and moral distress
Opt-in support important, but not sufficient
Advisory Board interviews and analysis.
Establish a peer
accountability system
• Use team meetings to encourage
clinicians to reflect on and plan self-
care habits
• Then, assign each clinician a peer
to periodically check in on their
well-being and ensure they’re
following through on self-care plans
Convert existing meetings
to well-being checks
• Use previously scheduled
meetings, like unit huddles, as
opportunities to facilitate discussion
• Create a safe space with the goal
of helping staff process emotions,
not eliminating emotional distress
Integrate physical space
for staff to decompress
• Establish ‘wobble rooms’ and
encourage staff to take a few
minutes per shift to use the
dedicated space to process difficult
emotions or decompress
• Make sure the spaces are easily
accessible from priority units, and
encourage leaders to model use

© 2020 Advisory Board • All rights reserved • advisory.com
22
Source: M Cornner and V Reid, “How to talk with staff about PPE shortages,” Advisory Board, 20 April, 2020;
R Richmond, “Preventing and responding to staff burnout during the pandemic,” Advisory Board, 9 April, 2020.
Four communication tips for executives
Effective communication vital to staff well-being and trust
Advisory Board interviews and analysis.
Emphasise
transparency
• Communicate the
‘why’ behind difficult
decisions, such as PPE
policies, staff
redeployment, and
postponing non-Covid-
19 care
• Be upfront about what
you don’t know and
share the steps you’re
taking to learn more
1
Give staff a consistent
source of COVID-19 truth
• Send messages from
the same person/email
address
• Regularly publish
answers to FAQs to field
and respond to
rumours
2
Make yourself
virtually accessible
• Establish regular virtual
office hours and use
open-ended questions
to prompt conversation
• Hold virtual town halls
and repeat sessions
across shifts
3
Share your gratitude
personally and often
• Acknowledge the
challenges and
uncertainty staff are
navigating
• Recognise the
sacrifices team
members are making
• Emphasise staff health
and safety as much as
patient/family health
and safety
4

© 2020 Advisory Board • All rights reserved • advisory.com
24
Speed of recovery will vary based on multiple factors
When will hospital utilisation get back to ‘normal’?
High impact Low impactMedium impact
Near-term
Long-term
Medium-term
Centralised decision-making over
health care reopening continues to
delay return of elective procedures
Manufacturers increase availability of
PPE and tests, increasing comfort and
readiness among patients and staff
Backfilled cases lead to bed and
operating room capacity constraints,
shifts to “higher capacity” peers
Lingering consumer anxiety/fear of
exposure to infection results in site of
care shifts or absolute reductions in use
Delays in care lead to exacerbation of
health issues
Referrals from GPs are delayed due to
primary care focus on COVID-19 needs
Positive experiences with telehealth
encourage first-time users to use virtual
care for future needs, possibly with
competing organisations
Lasting negative stigma of long term
care homes leads to longer LOS, less
bed turnover
Loss of clinical workers who are burnt
out or COVID-19 positive
Organisations proactively reach out to
patients to reschedule appointments;
effectively communicate re: safety
The availability of therapeutics and
vaccines reduces the probability of a
second Covid-19 wave—and need for
additional postponements
Reduced travel leads to less accident-
induced trauma
Mortalities in highly affected regions
reduces demand
Increased interest, funding and
focus on population health
management decreases acute care
utilisation
Decreased utilisation Increased utilisation
Advisory Board interviews and analysis.
Greater home health uptake for post-
acute and rehabilitative care
Telehealth becomes the default for
specialty care, reducing reliance on
in-person appointments

© 2020 Advisory Board • All rights reserved • advisory.com
26
Your top resources for COVID-19 readiness
Advisory Board interviews and analysis.
To access the top COVID-19 resources,
visit advisory.com/covid-19
WHO Guidelines
Compiles evidence-based information on
hospital and personnel preparedness, COVID-
19 infection control recommendations, clinical
guidelines, and case trackers
Coronavirus scenario planning
Explores ten situations hospital leaders
should prepare for and helps hospital
leadership teams pressure test the
comprehensiveness of their preparedness
planning efforts and check for blind spots
Managing clinical capacity
Examines best practices for creating flexible
nursing capacity, maximising hospital
throughput in times of high demand, increasing
access channels, deploying telehealth
capabilities, and engaging clinicians as they
deal with intense workloads
How COVID-19 is transforming
telehealth—now and in the future
Explores how telehealth is being deployed
against COVID-19 and essential next steps for
telehealth implementation

LEGAL CAVEAT
Advisory Board has made efforts to verify the accuracy of the information it provides to members. This report relies on data obtained from many sources, however, and
Advisory Board cannot guarantee the accuracy of the information provided or any analysis based thereon. In addition, Advisory Board is not in the business of giving legal,
medical, accounting, or other professional advice, and its reports should not be construed as professional advice. In particular, members should not rely on any legal
commentary in this report as a basis for action, or assume that any tactics described herein would be permitted by applicable law or appropriate for a given member’s situation.
Members are advised to consult with appropriate professionals concerning legal, medical, tax, or accounting issues, before implementing any of these tactics. Neither Advisory
Board nor its officers, directors, trustees, employees, and agents shall be liable for any claims, liabilities, or expenses relating to (a) any errors or omissions in this report,
whether caused by Advisory Board or any of its employees or agents, or sources or other third parties, (b) any recommendation or graded ranking by Advisory Board, or (c)
failure of member and its employees and agents to abide by the terms set forth herein.
Advisory Board and the “A” logo are registered trademarks of The Advisory Board Company in the United States and other countries. Members are not permitted to use these
trademarks, or any other trademark, product name, service name, trade name, and logo of Advisory Board without prior written consent of Advisory Board. All other
trademarks, product names, service names, trade names, and logos used within these pages are the property of their respective holders. Use of other company trademarks,
product names, service names, trade names, and logos or images of the same does not necessarily constitute (a) an endorsement by such company of Advisory Board and its
products and services, or (b) an endorsement of the company or its products or services by Advisory Board. Advisory Board is not affiliated with any such company.
IMPORTANT: Please read the following.
Advisory Board has prepared this report for the exclusive use of its members. Each member acknowledges and agrees that this report and the information contained herein
(collectively, the “Report”) are confidential and proprietary to Advisory Board. By accepting delivery of this Report, each member agrees to abide by the terms as stated herein,
including the following:
1. Advisory Board owns all right, title, and interest in and to this Report. Except as stated herein, no right, license, permission, or interest of any kind in this Report is intended
to be given, transferred to, or acquired by a member. Each member is authorized to use this Report only to the extent expressly authorized herein.
2. Each member shall not sell, license, republish, or post online or otherwise this Report, in part or in whole. Each member shall not disseminate or permit the use of, and shall
take reasonable precautions to prevent such dissemination or use of, this Report by (a) any of its employees and agents (except as stated below), or (b) any third party.
3. Each member may make this Report available solely to those of its employees and agents who (a) are registered for the workshop or membership program of which this
Report is a part, (b) require access to this Report in order to learn from the information described herein, and (c) agree not to disclose this Report to other employees or
agents or any third party. Each member shall use, and shall ensure that its employees and agents use, this Report for its internal use only. Each member may make a
limited number of copies, solely as adequate for use by its employees and agents in accordance with the terms herein.
4. Each member shall not remove from this Report any confidential markings, copyright notices, and/or other similar indicia herein.
5. Each member is responsible for any breach of its obligations as stated herein by any of its employees or agents.
6. If a member is unwilling to abide by any of the foregoing obligations, then such member shall promptly return this Report and all copies thereof to Advisory Board.
27© 2020 Advisory Board • All rights reserved • advisory.com

Tenth Floor, 5 Merchant Square, London W2 1AS, UK
+44-(0)-207-479-1799 │ advisory.com