We still do not know much about it - hkgs.org still do not know much about it (25 Nov).pdf · •...
82
We still do not know much about it Dr. Cheng MF Supervisor : Dr. Wah SH
Transcript of We still do not know much about it - hkgs.org still do not know much about it (25 Nov).pdf · •...

We still do not know much about it
Dr. Cheng MF
Supervisor : Dr. Wah SH
The case
• F/82, NKDA, living with family
• ADL-I
• FU EKLCC, UCH Med and FM
• Past medical history
• HT
• Hyperlipidaemia
• CKD, baseline Cr 280, USG kidney 9.2014 > chronic parenchymal disease
• Old ischaemic CVA with good recovery

• 1st admission to UCH in 22.8.2014-26.8.2014
• Fever, mild cough with not many other symptoms
• Empirical augmentin and discharged
• Physical examination > unremarkable
• Hb 8.9
• OGD > gastritis, HP-ve
• Fe profile > Fe deficiency anaemia
• Fe supplement started
• Blood culture / MSU culture –ve
• Sputum culture -ve

22.8.2014 CXR

• 2nd admission to UCH on 26.8.2014 (the day of discharge)
• Fever again
• Dry cough only
• Mild left chest wall pain, non-anginal
• No trauma or sprain
• No sputum or haemoptysis or hoarseness of voice
• No GI or urinary symptoms
• No joint pain or rash
• No travel history or contact
• No insect bites
• No TCM or OTC meds
• Family well

• HS dual no M
• Chest clear
• Abd soft
• Neck soft
• No focal neurological sign
• No rash
• No insect bite mark
• No tender joint or swollen joint
• No mucosal lesion
• No palpable cervical, axillary, trochlear or groin LN

• FOB +ve
• Colonoscopy declined by patient
• CRP 108
• ESR 126
• WBC 25.6
• LDH 168
• Sputum x AFB smear –ve
• MSU culture > contamination
• Blood culture -ve

1.9.2014 CXR

• Empirical rocephin
• Fever down
• WBC mildly elevated, ~ 12, to tazocin, empirically
• Pending Gallium scan
• To rehab unit on 3.9.2014

To rehab unit to finish the course of antibiotic…




Tazocin finished on 8.9.2014

Other medications


• Repeated sputum culture > oropharyngeal contamination
• EMU x AFB smear –ve
• CRP 168 > 173 > 79
• ESR 126
• C3/4 N
• WBC 16, blood film > neutrophil vacuolation
• SPE no paraprotein

• Patient remained non-septic
• Walking unaided, ADL-I in ward
• Chills during kicks of fever
• Physical examination unremarkable

• Weil felix
• Widal
• Brucellosis all –ve
• Anti-HIV –ve
• T-spot test reactive
• Echocardiogram booked

• Gallium scan on 12.9.2014 (before echocardiogram)

Abnormality ?



Gallium scan report
• Suboptimal scan
• Motion artefacts significant
• Increased uptake at bilateral hila, corresponding to CT-thorax, likely lymphadenopathy
• Prominent right axillary nodes
• No definite breast mass
• Increased tracer uptake at Lt elbow, corresponding to CT showing osteophytes and decreased joint space

• Consulted Resp Team
• Transferred back to acute unit
• Remained afebrile without antibiotic
• Rt axillary LN excisional biopsy
• LN pathology : mycobacterial infection, AFB smear -ve

Review
• Fever of unknown origin
• FDG vs Gallium scan
• Extrapulmonary mycobacterium infection (non-TB and TB)

FUO
• FUO is one of the most vexing clinical conditions for clinicians and patients
• No published guidelines
Am Fam Physicians. 2014;90(2):91-96
What is FUO ?
• FUO was first described in a 1961 case series as prolonged febrile illness (Temp of 101F (38.3C) or higher) for three weeks or longer that did not have an established etiology despite one-week inpatient evaluation
Petersdorf R, Beeson PB. Fever of unexplained origin: report on 100 cases. Medicine(Baltimore). 1961;40:1-30

101F from where ?
• The criterion of range of fever has been challenged
• Most authors and even Petersdorf do not mention the method of temperature measurement (oral, axillar, rectal, etc), nor the timing (morning or evening value)

Evolution of the definition of FUO

Subtypes of FUO

Implications of such classification

• The spectrum of the underlying disease in the latter 3 entities differs from that of classical FUO, with more infections, neoplastic and drug-related causes
• Different clinical approach
• The patients are all at risk for rapid deterioration due to their immune dysfunction
• Prompt empirical antimicrobial therapy, sometimes anti-viral and antifungal therapy, is the cornerstone of the approach in neutropenic FUO
Knockaert DC et al. Fever of unknown origin in adults : 40 years on Journal of Internal Medicine 253:263-75

• Such treatment should also be considered in nosocomial and HIV-associated FUO, be it less mandatory
• There is a sharp contrast to the approach in classical FUO, where most investigators caution against early empirical therapy and prefer a conservative strategy
Knockaert DC et al. Fever of unknown origin in adults: 40 years on Journal of Internal Medicine 253:263-275

• Common causes of PUO
• Infection
• Malignancy
• Non-infectious inflammatory diseases
• Miscellaneous
• Undiagnosed



• A shift in the relative proportion of specific disease categories
• About 15% remain undiagnosed
• The number of infectious causative agents was reduced with every 10 years for the past 4 decades, but the number of autoimmune and neoplastic causative agents of FUO increased
Arce-Salinas CA, et al. Classical fever of unknown origin : curernt causes in Mexico. Rev Invest Clin. 2005; 57(6):762-9

Approach of FUO
• No guidelines
• Most evaluation recommendations are based on expert opinion
• History and physical examination


• If no potentially diagnostic clues are found, a minimum diagnostic workup should be performed
• Infections predominate early in FUO diagnoses, and the longer FUO remains undiagnosed, the less likely it is caused by an infection
• Approximately 12-35% patients die from FUO-related cause (generally malignancy or infection)
• Those remain undiagnosed most recover or have a benign course with a good prognosis
Cunha BA. Fever of unknown origin : focused diagnostic approach based on clinical clues from the history, physical examination, and laboratory tests. Infect Dis Clin North Am. 2007;21(4):1137-1187
Hayakawa K. Fever of unknown origin : an evidence-based review. Am J Med Sci. 2012;344(4):867-915


ESR & CRP
• ESR does not help discriminate between active autoimmune disease and infection
• Malignancies and noninfectious inflammatory diseases can cause an elevated ESR and CRP
• ESR > 100 has a high specificity for malignancy (96%) and infection (97%), and its positive predictive value was 90%
• A normal ESR has a high negative predicative value for temporal arteritis
Fisher RM, et al. Clinical significance of extreme elevation of the erythrocyte sedimentation rate. Arch Intern Med. 186;146(8):1581-1583
Smetana GW, et al. Does this patient have temporal arteritis ? JAMA 2002;287(1):92-101
ESR & CRP
• An ESR that is not elevated has no diagnostic value and does not rule out neoplasm or other disorders
• CRP not sensitive enough to discriminate between infection and inflammation
Cunha BA. Fever of unknown origin: focused diagnostic approach based on clinical clues from the history, physical examination, and laboratory tests. Infect Dis Clin North Am. 2007;21(4):1137-1187
Limper M, et al. The diagnostic role of procalcitonin and other biomarkers in discriminating infectious from non-infectious fever. J Infect. 2010;60(6):409-416

Procalcitonin
• Newer marker specific for bacterial infection
• Specificity ranging from 70-98%
• May be helpful
• Its role in PUO is currently undefined Naito T, et al. Diagnostic workup for fever of unknown origin: a multicenter collaborative retrospective study. BMJ Open. 2013;3(12):e003971

Ferritin level
• Ferritin level of 561ng per ml (1261 pmol per L) seems to be optimal cutoff to predict that FUO was a non-infectious cause, in one study (77 subjects only) (>561 likely infectious)
Hayakawa K, et al. Fever of unknown of origin: an evidence-based review. Am J Med Sci. 2012;344(4):307-316

USG
• Abdominal & pelvic USG often recommended
• Low cost, lack of radiation exposure

CT
• Chest and abdominal CT had high sensitivity (82% & 92%, respectively) and were recommended if the initial evaluation was unrevealing
Bleeker-Rovers CP, et al. A prospective multicenter study on fever of unknown origin: The yield of a structured diagnostic protocol. Medicine (Baltimore). 2007;86(1):26-38

Still no clue…
• Secondary evaluation
• Few algorithms are supported by evidence from prospective studies
• Of the invasive procedures, biopsies have the highest diagnostic yield
• Serologic tests are helpful only if there are potentially diagnostic clues and if the patient lives in or has visited an area where the suspected disease is prevalent
Knockaert DC, et al. Fever of unknown origin in adults: 40 years on. J Intern Med. 2003;253(3):263-275
Gaeta GB, et al. Fever of unknown origin: a systematic review of the literature for 1995-2004. Nucl Med Commun. 2006;27(3):205-211
Bleeker-Rovers CP, et al. A prospective multicenter study on fever of unknown origin: the yield of a structured diagnostic protocol. Medicine (Baltimore). 2007;86(1):26-38

Biopsies
• Liver biopsy, with a diagnostic yield 14-17%, can reveal granulomatous hepatitis, inflammatory, or neoplastic processes
• Lymph node biopsy is most useful
• Bone marrow biopsy is diagnostically useful, particularly with neoplasm and infectious disease, esp TB
• In a study, 25% diagnostic yield
• Bone marrow aspiration and culture have a low diagnostic yield, 0-2%
Hayakawa K, et al. Fever of unknown origin: an evidence-based review. Am J Med Sci. 2012;344(4):307-316
Hot A, et al. Yield of bone marrow examination in diagnosing the source of fever of unknown origin. Arch Intern Med. 2009;169(21):2018-2023

• Empiric trials of antibiotics or steroids rarely establish a diagnosis and are discouraged in the management of patients with FUO, unless there are clinical indications
• Consultation with a subspecialist is appropriate at any point in the evaluation
Mourad O, et al. A comprehensive evidence-based approach to fever of unknown origin. Arch Intern Med. 2003;163(5):545-551

Evidence of key recommendations
Prolonged febrile illlness and Fever of unknown origin in adults Am Fam Physician. 2014;90(2):91-96

FUO in elderly patients
• Are they different ?
Srp Arh Celok Lek. 2011 Jan-Feb;139(1-2);64-68

The study
• > 65 vs < 65
• Retrospective study
• Were treated and were referred to a clinic, within a 3-year period
• 50 : 50 patients
• All patients were taking antibiotics before sampling materials
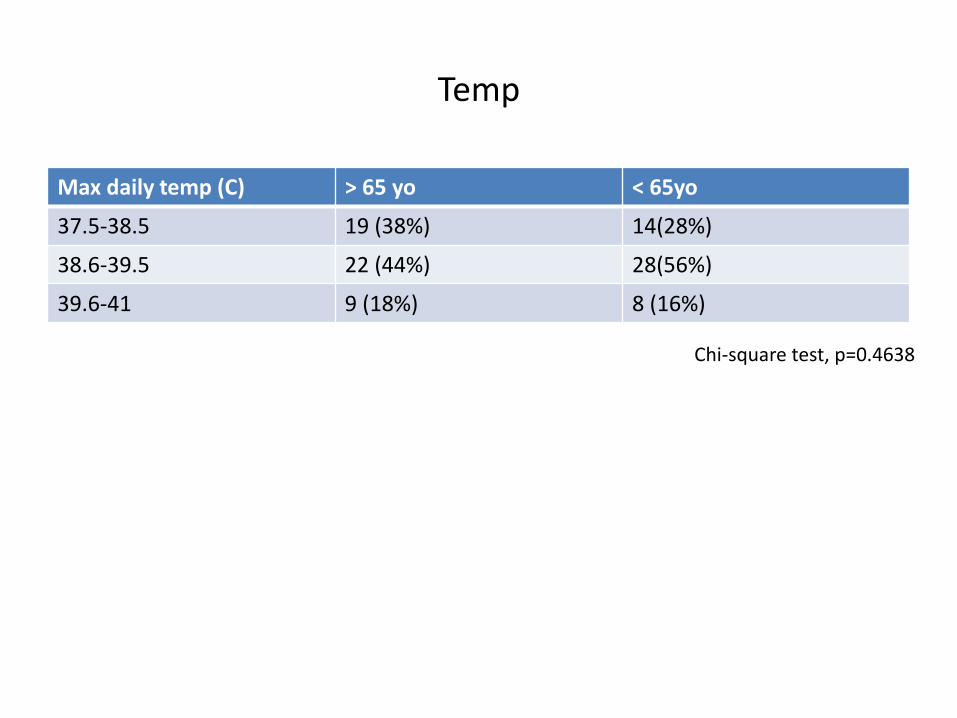
Temp
Max daily temp (C) > 65 yo < 65yo
37.5-38.5 19 (38%) 14(28%)
38.6-39.5 22 (44%) 28(56%)
39.6-41 9 (18%) 8 (16%)
Chi-square test, p=0.4638

Blood culture +ve rate
> 65yo < 65yo
Blood culture +ve 47.5% of samples taken 6% of samples taken
Chi-square test, p=0.0001
Most common : Staphylococcus sp. Enterococcus E.Coli

Leukocytes, ESR, fibrinogen & CRP
There is no statistically significant differences between 2 groups

Final diagnoses
P=0.358
P=0.1212
P=0.007

Outcome in this study
• No fatal outcome in < 65 group
• 12% in > 65 group
• Heterogeneity observed in different studies
• 13.6% elderly vs 14.7% younger patients died in a study of 97 FUO patients
• 5-year death rate in the patients with undiagnosed FUO is around 3.2%
Onal IK, et al. Fever of unknown origin: what is unremarkable in the elderly in a developing country? J Infect. 2006;52(6):399-404
Balcus C, et al. Fever of unknown origin- predictors of outcome (a prospective multicentre study on 164 patients). Eur J Intern Med. 2003;14:249-54

A Chinese study on PUO
• 997 PUO cases hospitalized at Peking Union Medical College Hospital between Jan 2004-Oct 2010
• And compare the results with previous studies of PUO in the same hospital since 1985
Shi Xiao-chun, et al. Major causes of fever of unknown origin at Peking Union Medical College Hospital in the past 26 years. Chin Med J 2013;126(5)


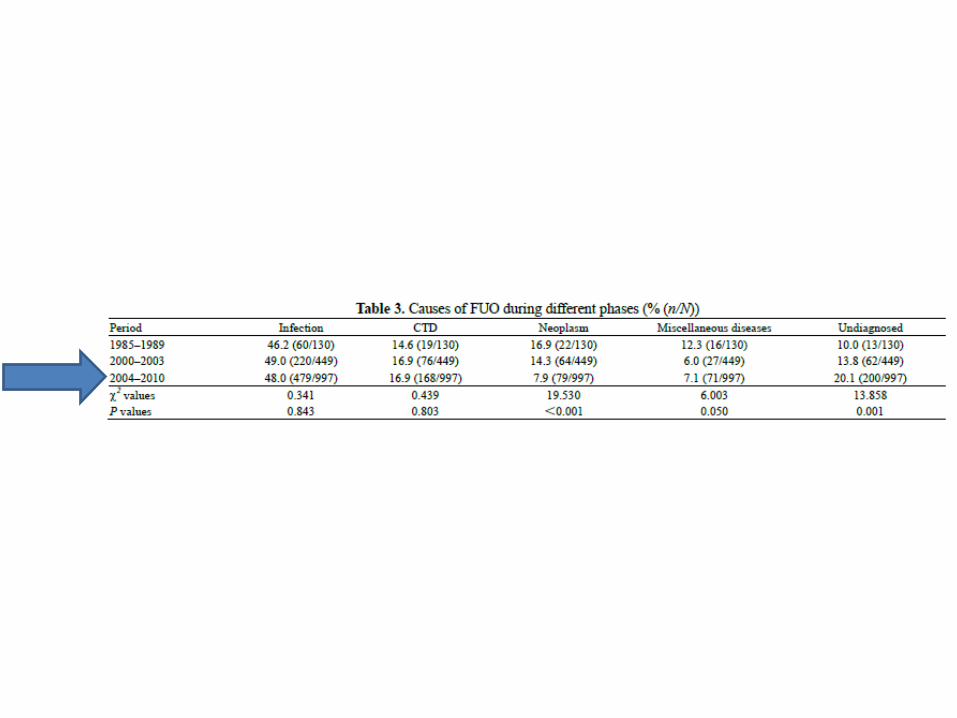

• During different periods, infectious diseases, esp TB, were the leading etiologies of PUO and the proportion of TB had no significant difference
• The frequency of neoplasms was descending
• The proportion of lymphoma in the neoplasm group was ascending
• The frequency of undiagnosed cases was increasing

II. FDG vs Gallium scan
• Gallium-67 citrate
• Can image acute, chronic, and granulomatous inflammation but also various malignant diseases
• Considerable radioactive burden
• Rather poor image quality
• Excreted into the bowel within possible superimposition of pathological foci on planar scans

FDG
• Fluorine-18 2’-deoxy-2-fluoro-D-glucose (FDG)
• Accumulate in malignant tissues and inflammatory processes, owing to their increased glucose metabolism and has been used extensively with positron emission tomography (PET)

The study
• Fever of unknown origin : prospective comparison of 18F-FDG imaging with a double-head coincidence camera and gallium-67 citrate SPET
J Meller, et al. Eur J Nucl Med (2000) 27:1617-1625

• 20-non DM patients
• Between 2.1999-3.2000
• Age 18-67
• Duration of fever 26-54 days
• 4/20 on antibiotics
• 2/20 on immunosuppressant therapy

Discussion
• The purpose of radionuclide imaging in patients with FUO is to localize a potential focal pathology for fever , which can subsequently be evaluated by other diagnostic modalities
• In vitro and in vivo labeled WBCs has been used, but have been found to be sensitive and specific in the diagnosis of pyogenic inflammation only
• Therefore labeled WBCs cannot be considered as the first choice

Summary of the study
• FDG sensitivity 81% and specificity 86%
• Ga scintigraphy sensitivity 67%, specificity 78%
• Antibiotics and immunosuppressive therapy did not seem to influence the results of FDG scanning, as 66% patients (4/6) of the patients who were treated exhibited a pathological uptake that clarified the cause of fever
• The superiority may be explained by the preferable tracer kinetics of the small FDG molecule compared with the relatively large Ga-transferrin complex and by the better spatial resolution of the DHCC system in comparison with a conventional gamma camera

• In the context of screening FUO patients a negative scan is less helpful than a positive one because it cannot contribute to the final diagnosis
• In this study negative studies in conditions such as HCV infection during viraemia, prolonged viral infection, liver haemangiomatosis, haemolysis, PE and drug fever

TB and non-TB related lymphadenopathy
• Non-TB lymphadenopathy
• Most frequently isolated species
• Mycobacterium avium complex
• M. scrofulaceum
• M malmonense
• M hemophilum

HK data
• Of the 5757 patients treated, 13.7% had extra-pulmonary tuberculosis alone and 8.6% had both
• 36.5% of such cases had LN involvement
• Unrelated to HIV infection
Noertjojo, K, et al. The International Journal of Tuberculosis and Lung Disease, Volume 6, No.10, October 2002, pp.879-886(8)

• Generally, an indolent disease
• Usually unilateral and occurs in the cervical, submandibular, or preauricular LNs
• Cultures of draining and ulcerative lesions, eg. Swab, give a lower diagnostic yield than needle aspirate or tissue biopsy samples

NTM lymphadenitis treatment
• Treatment of uncomplicated NTM lymphadenitis is by complete surgical excision
• I and D are discouraged
• Sinus tract formation and chronic discharge
• Chemotherapy may be considered for patients in whom lymphadenitis recur after surgery or for whom all abnormal tissues could not be excised
• Optimal chemotherapy still undetermined
• Duration of pharmacological treatment, still undetermined
• Combination therapy including clarithromycin and RIF, either RIF or rifabutin, and/or EMB, may be beneficial

TB lymphadenitis
• Lymphadenitis most common presentation of EPTB in both children and adults (19%, UK data)
• Most common sites
• Anterior or posterior cervical and submandibular LN Angela Houston, Derek Macallan Medicine 42:1

• Usually painless
• Nodes are firm, may be matted together
• Symptoms depend on site
• Mediastinal TB may present with dysphagia or recurrent laryngeal nerve involvement
• FNA of the affected node is recommended
• Excision biopsy may be considered if the diagnosis is in doubt
• The yield of AFB from a smear is poor, but increases in patients co-infected with HIV

• The > 120 recognized species of NTM share common features
• 1. facultative pathogens
• 2. evidence of human-to-human transmission is lacking
• 3. ubiquitous vs restricted distribution
• 4. treatment may be difficult, according to involved organism and disease site
• 5. pathogenesis is still undefined Claudio Piersimoni and Claudio Scarparo Emerging Infectious Diseases Vol.15, No.9, September 2009
TB-lymphadenitis treatment
• Follows a waxing and waning course, even during Rx
• Worsening on treatment may be attributable to paradoxical reactions (An enhanced immune response to dying mycobacteria)
• Standard quadruple therapy
• Duration same as pulmonary TB
• Role of steroid, under debate


Our patient
• HRZM
• Off M x visual acuity deterioration
• Await LN culture report