(VTE) prophylaxis in pregnancy and the puerperium
25
Maternity and Neonatal Clinical Guideline Great state. Great opportunity. Department of Health
Transcript of (VTE) prophylaxis in pregnancy and the puerperium

Maternity and Neonatal Clinical Guideline
Great state. Great opportunity.
Department of Health

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 2 of 25
Document title: Venous thromboembolism (VTE) prophylaxis in pregnancy and the puerperium
Publication date: February 2014
Document number: MN14.9-V5-R19
Document supplement:
The document supplement is integral to and should be read in conjunction with this guideline.
Amendments: Full version history is supplied in the document supplement.
Amendment date: Amendment October 2014. Full review of 2009 publication occurred in February 2014.
Replaces document: MN14.9-V4-R19
Author: Queensland Clinical Guidelines
Audience: Health professionals in Queensland public and private maternity services
Review date: February 2019
Endorsed by: Queensland Clinical Guidelines Steering Committee Statewide Maternity and Neonatal Clinical Network (Queensland)
Contact: Email: [email protected] URL: www.health.qld.gov.au/qcg
Disclaimer These guidelines have been prepared to promote and facilitate standardisation and consistency of practice, using a multidisciplinary approach. Information in this guideline is current at time of publication. Queensland Health does not accept liability to any person for loss or damage incurred as a result of reliance upon the material contained in this guideline. Clinical material offered in this guideline does not replace or remove clinical judgement or the professional care and duty necessary for each specific patient case. Clinical care carried out in accordance with this guideline should be provided within the context of locally available resources and expertise. This Guideline does not address all elements of standard practice and assumes that individual clinicians are responsible to:
• Discuss care with consumers in an environment that is culturally appropriate and which enables respectful confidential discussion. This includes the use of interpreter services where necessary
• Advise consumers of their choice and ensure informed consent is obtained • Provide care within scope of practice, meet all legislative requirements and maintain
standards of professional conduct • Apply standard precautions and additional precautions as necessary, when delivering care • Document all care in accordance with mandatory and local requirements
© State of Queensland (Queensland Health) 2014
This work is licensed under a Creative Commons Attribution Non-Commercial No Derivatives 3.0 Australia licence. In essence, you are free to copy and communicate the work in its current form for non-commercial purposes, as long as you attribute Queensland Clinical Guidelines, Queensland Health and abide by the licence terms. You may not alter or adapt the work in any way. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/3.0/au/deed.en
For further information contact Queensland Clinical Guidelines RBWH Post Office, Herston Qld 4029, email [email protected], phone (07) 3131 6777. For permissions beyond the scope of this licence contact: Intellectual Property Officer, Queensland Health, GPO Box 48, Brisbane Qld 4001, email [email protected], phone (07) 3234 1479.

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 3 of 25
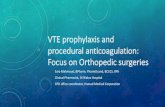
Flow Chart: Antenatal assessment and management for VTE prophylaxis
High Risk Factors• Single prior unprovoked VTE• Single prior VTE pregnancy or COCP related • Single prior VTE + thrombophilia• Single prior VTE + family history of thrombophilia• Prior recurrent VTE (>1)• Family history VTE (but no personal history VTE)
+ antithrombin deficiency
Antenatal VTE assessment and management • Evidence correlating risk factors and the occurrence of VTE is limited• Assess each woman individually for VTE risk. The flowchart does not replace clinical judgement• Assess risk early in pregnancy, repeat if hospitalised and if there is a change in clinical circumstances• Assess the risks associated with VTE prophylaxis (guideline section 1.4)• Discuss options for VTE prophylaxis with the woman• Document a plan of care• Liaise with a team experienced in prophylactic assessment/management as required• Refer to the full text of the guideline for detailed prophylaxis assessment and management
High Risk • Discuss GCS• #LMWH prophylaxis • Consider IPC if hospitalised
Lower Risk
Que
ensl
and
Clin
ical
Gui
delin
e: V
enou
s th
rom
boem
bolis
m (V
TE) p
roph
ylax
is in
pre
gnan
cy a
nd th
e pu
erpe
rium
. Gui
delin
e N
o: M
N14
.9-V
5-R
19
Abbreviations: COCP: Combined oral contraceptive pill GCS: Graduated compression stockings HIT: Heparin induced thrombocytopenia IPC: Intermittent pneumatic compression LMWH: Low molecular weight heparin ≥: Greater than or equal to >: Greater than
Moderate Risk• Discuss GCS• Consider IPC if hospitalised• Consider #LMWH prophylaxis
Pre-pregnancy therapeutic anticoagulation Antenatal therapeuticanticoagulation
Socio-demographic• Age ≥ 35 years • BMI ≥ 30 kg/m2 • Cigarette smoker
(>10/day)
Medical history• Systemic lupus
erythematosus• Cardiac or lung
disease• Sickle cell disease• Gross varicose veins • Inflammatory
conditions• Nephrotic syndrome• Cancer• Pre-existing diabetes• Ovarian
hyperstimulation
Pregnancy related• Immobility (e.g. bed rest,
long distance travel)• Preeclampsia/eclampsia• Artificial reproductive
therapy• Gestational diabetes• Multiparity (> 2)• Multiple pregnancy• Intrauterine growth
restriction• Hyperemesis/dehydration• Current systemic infection
(requiring antibiotics or hospitalisation)
• Antepartum haemorrhage• Surgical procedure in
pregnancy
Known Risk Factors
• Single prior provoked VTE (not COCP related)• Asymptomatic thrombophilia (inherited or acquired) • Family history VTE• Family history VTE (but no personal history VTE) +
thrombophilia (excluding antithrombin deficiency)• No personal or family history of VTE but significant
laboratory thrombophilia• Antiphospholipid antibodies
VTE/Thrombophilias
Hospitalised + ≥ 2 risk factors or ≥ 3 risk factors
0 - 2 risk factors
All Risk• Clinical surveillance• Encourage mobilisation• Avoid dehydration
# Determine dose (standard, intermediate or therapeutic) based on individual assessment Refer to full guideline - Section 5: Specific patient groups and Appendix A: Drug information.

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 4 of 25
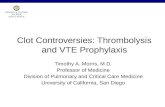
Flow Chart: Postnatal assessment and management for VTE prophylaxis
High Risk Factors• Antenatal LMWH prophylaxis (refer to
antenatal VTE prophylaxis flow chart)• Any previous personal history of VTE (not
current pregnancy#)
Postnatal VTE assessment and management • Evidence correlating risk factors and the occurrence of VTE is limited• Assess each woman individually for VTE risk. The flowchart does not replace clinical judgement• Assess risk at birth and if there is a change in clinical circumstances• Assess the risks associated with VTE prophylaxis (guideline section 1.4)• Discuss options for VTE prophylaxis with the woman• Document a plan of care• Liaise with a team experienced in prophylactic assessment/management as required• Refer to the full text of the guideline for detailed prophylaxis assessment and management
High Risk• GCS• #LMWH prophylaxis for
6 weeks• Consider IPC if
hospitalised
Lower Risk• Discuss GCS• Consider #LMWH
prophylaxis until discharge or fully mobile
Queensland Clinical Guideline: Venous thromboembolism (VTE) prophylaxis in pregnancy and the puerperium. Guideline No: MN14.9-V5-R19
Moderate Risk• Discuss GCS• #LMWH prophylaxis for
5 days • Consider IPC if
hospitalised
Antenatal therapeutic anticoagulation Postnatal therapeutic anticoagulation
Socio-demographic• Age ≥ 35 years • BMI ≥ 30 kg/m2 • Cigarette smoker
(>10/day)
Medical history• Asymptomatic
thrombophilia (inherited or
acquired)• Family history VTE +
weak thrombophilia • Systemic lupus
erythematosus• Cardiac or lung
disease• Sickle cell disease• Gross varicose veins • Inflammatory
conditions• Nephrotic syndrome• Cancer• Pre-existing diabetes• Antiphospholipid
antibodies
Birth• Emergency CS in
labour• Elective CS• Prolonged labour (>
24 hrs)• Operative vaginal birth• Stillbirth• Preterm birth• Postpartum
haemorrhage (> 1L)
Postpartum• Immobility (long
distance travel, prolonged bed rest)
• Preeclampsia/eclampsia
• Gestational diabetes • Infection• Any surgical
procedure
Known Risk Factors
All Risk• Clinical surveillance• Early mobilisation• Avoid dehydration
Abbreviations: CS: Caesarean section GCS: Graduated compression stockings HIT: Heparin induced thrombocytopenia IPC: Intermittent pneumatic compression LMWH: Low molecular weight heparin ≥: Greater than or equal to >: Greater than
Emergency CS in labour
≥ 3 risk factors
1-2 risk factors
No risk factors
# Determine dose (standard, intermediate or therapeutic) based on individual assessment Refer to full guideline - Section 5: Specific patient groups and Appendix A: Drug information.

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 5 of 25
Abbreviations
AOR Adjusted odds ratio APCR Activated protein C resistance APPT Activated partial thromboplastin time bd Twice daily BMI Body mass index CI Confidence interval COCP Combined oral contraceptive pill CS Caesarean section DVT Deep vein thrombosis GCS Graduated compression stockings GI Gastrointestinal HIT Heparin induced thrombocytopenia INR International normalised ratio IPC Intermittent pneumatic compression IV Intravenous LMWH Low molecular weight heparin PE Pulmonary embolism PPH Postpartum haemorrhage stat Immediately Subcut subcutaneous UFH Unfractionated heparin VTE Venous thromboembolism > Greater than ≥ Greater than or equal to
2BTerminology
Term Definition Family history of VTE
Family history is considered positive if one or more first degree relatives are affected.1,2
Informed choice
When a woman has the autonomy and control to make decisions about her care after a process of information exchange that involves providing her with sufficient, evidence-based information about all options for her care, in the absence of coercion by any party and without withholding information about any options.3
Informed consent
When a woman consents to a recommendation about her care after a process of information exchange that involves providing her with sufficient, evidence-based information about all the options for her care so that she can make a decision, in the absence of coercion by any party, that reflects self-determination, autonomy and control.3
Obstetrician
Local facilities may as required, differentiate the roles and responsibilities assigned in this document to an ‘Obstetrician’ according to their specific practitioner group requirements; for example to General Practitioner Obstetricians, Specialist Obstetricians, Consultants, Senior Registrars and Obstetric Fellows.
Provoked VTE VTE occurring where risk factors can be identified.1
Recurrent VTE Two or more VTE.
Significant thrombophilia
Significant laboratory thrombophilia includes antithrombin deficiency, protein C and S deficiency, homozygous factor V Leiden or multiple thrombophilic defects. All other thrombophilia are considered weak.1
Unprovoked VTE VTE occurring where there are no identified risk factors.1
Woman centred care
Woman centred care includes the affordance of respect and dignity by supporting the woman to be central and active in her own care4 through5:
• Holistic care taking account of the woman’s physical, psychosocial, cultural, emotional and spiritual needs
• Focussing on the woman’s expectations, aspirations and needs, rather than the institutional or professional needs
• Recognising the woman’s right to self-determination through choice, control and continuity of care from a known or known caregivers
• Recognising the needs of the baby, the woman’s family and significant others

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 6 of 25
Table of Contents
1 Introduction ..................................................................................................................................... 7 1.1 Incidence................................................................................................................................ 7 1.2 Communication ...................................................................................................................... 7 1.3 Risk and benefit of VTE prophylaxis ...................................................................................... 7 1.4 Risks associated with VTE prophylaxis ................................................................................. 8 1.5 Signs and symptoms of VTE ................................................................................................. 9 1.6 Transfer of care ..................................................................................................................... 9 1.7 Clinical standards .................................................................................................................. 9
2 Risk assessment .......................................................................................................................... 10 2.1 High risk factors for VTE ...................................................................................................... 10 2.2 Known risk factors for VTE .................................................................................................. 11 2.3 Criteria for assessment of risk ............................................................................................. 12 2.4 Additional assessments ....................................................................................................... 12
3 Options for thromboprophylaxis ................................................................................................... 13 3.1 Other pharmaceutical agents............................................................................................... 14
4 Prophylactic management of VTE ................................................................................................ 15 4.1 Specific patient group management .................................................................................... 15 4.2 Antenatal prophylaxis .......................................................................................................... 15 4.3 Intrapartum prophylaxis ....................................................................................................... 15 4.4 Postnatal prophylaxis ........................................................................................................... 16 4.5 Neuraxial blockade .............................................................................................................. 17
5 Specific patient groups ................................................................................................................. 18 6 Discharge ..................................................................................................................................... 19 References .......................................................................................................................................... 20 Appendix A: Drug information .............................................................................................................. 22 Appendix B: Adjusted odds ratio (AOR) for risk of VTE ...................................................................... 23 Appendix C: Risk of VTE with Thrombophilia ...................................................................................... 24 Acknowledgements .............................................................................................................................. 25 List of Tables
Table 1. Risks associated with VTE prophylaxis ................................................................................... 8 Table 2. Signs and symptoms of VTE ................................................................................................... 9 Table 3. High risk factors for VTE ........................................................................................................ 10 Table 4. Known risk factors ................................................................................................................. 11 Table 5. Criteria for assessment of risk ............................................................................................... 12 Table 6. Additional risk assessment .................................................................................................... 12 Table 7. Options for thromboprophylaxis ............................................................................................. 13 Table 8. Other pharmaceutical agents ................................................................................................ 14 Table 9. Antenatal prophylaxis ............................................................................................................ 15 Table 10. Prophylaxis postpartum by assessment of risk ................................................................... 16 Table 11. Management of LMWH, UFH and neuraxial blockade ........................................................ 17 Table 12. Antenatal and postnatal management of specific patient groups ........................................ 18 Table 13. Preparation for discharge .................................................................................................... 19

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 7 of 25
1 Introduction Pulmonary embolism (PE) and deep vein thrombosis (DVT) are the two components of a single disease called venous thromboembolism (VTE).6,7 Pregnant women have an increased risk (4–5 fold1,7) of developing a VTE, in comparison to non-pregnant women due to hypercoagulability, increased venous stasis, decreased venous outflow and compression of the inferior vena cava and pelvic veins by the enlarging uterus.1
1.1 Incidence • Thromboembolism is a leading cause of maternal deaths in the developed world8,9
o Second most common cause of direct maternal death in Australia1 o Maternal mortality is reported to be 0.4–1.6 per 100,000 pregnancies1
• The risk of VTE is greater postpartum than during the antenatal period1,2,10 o 40–60% of antenatal VTE occur in the first trimester11
• Rates of VTE are estimated at no more than 2 per 1000 pregnancies1,2 but vary considerably o 75–80% of events are caused by DVT and 20–25% by PE7 - of which 1 in 40 is fatal1 o 43–60% of pregnancy related episodes of PE occur in the 4–6 weeks after birth2
• DVT is more likely to occur in the left lower extremity7
1.2 Communication • Share and discuss information with the woman in a manner that enables informed choice
and consent and supports woman centred care [Refer to definition of terms] • Discuss the woman’s preferences for management2 • Provide the woman at increased risk of VTE, culturally appropriate information about
VTE12, the risks of VTE prophylaxis and the symptoms suggestive of DVT and PE to facilitate early recognition and management1 [Refer to Table 2. Signs and symptoms of VTE]
1.3 Risk and benefit of VTE prophylaxis Explain the risks and benefits of VTE prophylaxis as appropriate to the individual circumstances. Including2:
• Risk of VTE and consequences for the woman and her baby if no prophylaxis • Relative effectiveness of treatment:
o Despite receiving low molecular weight heparin (LMWH), VTE occurred in 0.86% of pregnancies(n=2777 pregnancies)13
• Burden of prolonged compliance with treatment option • Cautions and contraindications to prophylactic options
o Refer to Table 1. Risks associated with VTE prophylaxis o Risk of significant bleeding
Antepartum 0.43% (95% CI 0.22–0.75%) with LMWH2 Postpartum 0.94% (95% CI 0.61–1.37%) with LMWH2
o With LMWH, the risk of (n=2777)13: Allergic skin reactions (1.80%) Thrombocytopenia (0.11%) Osteoporotic fractures (0.04%) Heparin Induced Thrombocytopenia (HIT) (0%)
• The woman with very high risk conditions (mechanical heart valves, chronic thromboembolic pulmonary hypertension, history of myocardial infarction, permanent occlusion of a major vessel or a history of recurrent thrombosis while fully anticoagulated) requires counselling and advice from a medical specialist as she is at increased risk of maternal mortality14

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 8 of 25
1.4 Risks associated with VTE prophylaxis
Table 1. Risks associated with VTE prophylaxis
Aspect Risk
Patient-related risk factors for bleeding15
• Active antenatal or postpartum bleeding (requiring at least two units of blood/products to be transfused in 24 hours or PPH greater than 1 L)
• Chronic clinically significant and measurable bleeding over 48 hours • Women at risk of major haemorrhage (e.g. placenta previa) • Acquired or inherited bleeding disorders (e.g. acute liver failure,
haemophilia) • Recent central nervous system bleeding • Intracranial or spinal lesion • Abnormal blood coagulation • Thrombocytopenia • Severe platelet dysfunction • Active peptic ulcer or active ulcerative gastrointestinal disease • Obstructive jaundice or cholestasis • Recent major surgical procedure of high bleeding risk • Concomitant use of medications that may affect the clotting process • Regional axial or recent lumbar puncture
Cautions for pharmacological prophylaxis15
• *Contraindications to pharmacological therapy o Known hypersensitivity o History of or current HIT o Creatinine clearance less than 30 mL/minute
• *Cautions to pharmacological therapy o Renal impairment o Hepatic impairment
Mechanical prophylaxis15
• Recommend with caution where there is: o Morbid obesity and correct fitting stocking cannot be achieved o Inflammatory conditions of the lower legs o Severe peripheral neuropathy o Severe oedema of the legs o Diabetic neuropathy o Severe lower limb deformity
• Intermittent pneumatic compression device (IPC) can exacerbate ischaemic disease
*Consult an Australian pharmacopeia for complete drug information

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 9 of 25
1.5 Signs and symptoms of VTE
Table 2. Signs and symptoms of VTE
Type Clinical presentation
Pulmonary embolism11
• Dyspnoea (most common symptom of PE) • Palpitations • Chest pain • Haemoptysis • Hypoxia/Cyanosis • Tachycardia • Tachypnoea • Hypotension • Collapse
Deep Vein Thrombosis
• DVT in pregnancy is often proximal and may not present with usual features of distal DVT16
• Unilateral leg pain • Swelling in an extremity7,9 • Increase in calf/thigh circumference7 • Increased temperature11 • Prominent superficial veins11 • Pitting oedema11
1.6 Transfer of care • Provide care in accordance with local service capabilities17 • Consult with, refer or transfer care to higher level services as appropriate18 • Document processes for referral and transfer appropriate to the local facility
1.7 Clinical standards • Educate clinicians about VTE risk assessment • Document VTE risk assessment of the pregnant woman in the health record
o Develop a written plan of care to manage identified risks o Document completion of the inpatient risk assessment on the National Inpatient
Medication Chart • Measure and document observations consistent with the clinical situation and at a
minimum, the Australian Commission on Safety and Quality in Health Care requirements19 • Consider use of Queensland Maternity Early Warning Tools to detect deterioration of
pregnant patients8 • Use standard administration forms for prophylactic and therapeutic medications (e.g.
Heparin intravenous infusion order and administration form)20,21 o For Dalteparin, write the brand name in addition to the generic name to reduce
ambiguity22

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 10 of 25
2 Risk assessment Failure to recognise and/or treat personal or pregnancy specific risk factors has been identified as a significant contributing factor to maternal mortality and morbidity arising from thrombosis.1,10 However, there is limited high level evidence from randomised trials or among evidence based/consensus guidelines23 about which women require thromboprophylaxis during pregnancy and postpartum.1,9,15
• Assess all women for VTE risk factors in early pregnancy or before conception1,10 • Repeat the assessment when there is a change in risk status and following birth11
o Ask about VTE symptoms o Commencing prophylaxis at times of additional VTE risk is clinically important and
appropriate1 • Assess the woman’s risk of bleeding and/or contraindications to pharmacological or
mechanical prophylaxis15,24 before offering VTE prophylaxis [refer to Table 1] • Formulate an overall risk assessment with consideration of risk of thromboprophylaxis
against the benefits15 [Refer to Section 1.2] • Refer to Section 5 Specific patient group for management if identified risk factor(s) include
any of the following: o Significant personal history of VTE o Thrombophilia o Antiphospholipid syndrome o Pre-pregnancy anticoagulation
2.1 High risk factors for VTE The strongest personal risk factor for VTE in pregnancy is a history of thrombosis - 15–25% of VTE in pregnancy are recurrent events, followed by thrombophilia - present in 20–50% of women who experience VTE during pregnancy and postpartum.14
Table 3. High risk factors for VTE
Period High risk factors
Antenatal
• Single prior unprovoked VTE • Single prior VTE pregnancy or combined oral contraceptive pill (COCP)
related • Single prior VTE and thrombophilia • Single prior VTE and family history of thrombophilia • Prior recurrent VTE (>1) • Family history VTE (but no personal history VTE) and antithrombin
deficiency
Postnatal • Antenatal LMWH • Any personal history of VTE

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 11 of 25
2.2 Known risk factors for VTE The evidence correlating risk factors and the occurrence of VTE is imprecise with wide and sometimes contradictory estimates of risk1 [Refer to Appendix B]. The presence of multiple risk factors may have additive or synergistic effects1,10,15 but the combinations with the greatest risk are unknown. It is unclear from the evidence whether particular risk factors are more likely to be associated with antenatal or postnatal VTE (or both).
Table 4. Known risk factors
Risk factors
Socio-demographic
• Age (greater than 35 years)25-29 • BMI ≥ 30 kg/m2,26,27,30-33 • Cigarette smoker26,28,30,31 (>10/day)
Medical history
• Single previous VTE with no family history VTE or thrombophilia26,29,33 • Thrombophilia and no previous VTE26 • Family history VTE1 • Antiphospholipid syndrome1 • Thrombophilia (inherited or acquired)10 • Systemic lupus erythematosus26 • Cardiac or lung disease26,31 • Sickle cell disease26 • Ovarian hyperstimulation syndrome10 • Gross varicose veins31,32 • Inflammatory conditions24,32 • Nephrotic syndrome32 • Cancer24 • Pre-existing diabetes32
Pregnancy related
• Immobility30 (e.g. bed rest, long distance travel) • Preeclampsia/eclampsia25,28-30,34 • Artificial reproductive therapy (ART)25,30,34 • Gestational diabetes25,30 • Multiparity (greater than 2 27,28,31 or 329) • Multiple pregnancy25,26,28,30,34 • Intrauterine growth restriction30 • Hyperemesis/dehydration26 • Current systemic infection (requiring antibiotics or hospitalisation)32 • Antepartum haemorrhage25,26 • Surgical procedure in pregnancy24
Birth/ Postpartum
• Prolonged labour (greater than 24 hours)10 • Caesarean section26,28,29,31-34 (emergency25,30 and elective25) • Operative vaginal birth10 • Stillbirth32 • Preterm birth31,32,35 • PPH (> 1L)26,30,32,35 • Transfusion26 • Any surgical procedure in the puerperium24 • Postpartum infection26,30

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 12 of 25
2.3 Criteria for assessment of risk Consider the potential for additive effects of multiple risk factors. Refer to Appendix B Adjusted odds ratio (AOR) for risk of VTE.
Table 5. Criteria for assessment of risk
Risk assessment Antenatal criteria Postnatal criteria
All risk • All pregnant women are at increased risk for VTE
• All postnatal women are at increased risk for VTE
Therapeutic anticoagulation
• Pre-pregnancy therapeutic anticoagulation
• Antenatal therapeutic anticoagulation
High risk • One or more antenatal high risk factors
• One or more postnatal high risk factors
Moderate risk • 3 or more known risk factors • If hospitalised, 2 or more known
risk factors
• Emergency caesarean birth in labour
• 3 or more known risk factors
Lower risk • 0-2 antenatal known risk factors • 1-2 postnatal known risk factors
2.4 Additional assessments
Table 6. Additional risk assessment
Aspect Consideration
Previous VTE
• A positive family history of VTE has been shown to increase the risk of VTE two-fold1
• Refer the woman with a positive personal or family history of VTE to an obstetrician or physician experienced in VTE prophylaxis management
• All women with previous VTE require a full thrombophilia screen including10: o *Activated protein C resistance (APCR) o Factor V Leiden mutation will be done if APCR is detected o Prothrombin gene mutation o *Antithrombin III deficiency o *Protein C deficiency o *Protein S deficiency o Antiphospholipid antibodies:
Lupus anticoagulant *Anticardiolipin antibodies Beta 2 Glycoprotein 1 (B2GP1)
Note: High risk thrombophilia include: Homozygous Factor V Leiden mutation, Antithrombin III deficiency and the presence of multiple thrombophilia are associated with a higher risk for VTE1 *Test in non- pregnant state as range affected by pregnancy
Pre-existing medical conditions
• Liaise with an obstetrician and physician experienced in prophylactic management of VTE where the woman has a history of: o Cerebral haemorrhage o Gastrointestinal haemorrhage o HIT/Thrombocytopenia o Renal insufficiency
• Ensure a multidisciplinary approach to care • Thromboprophylaxis may need to be individualised • Ensure referral to anaesthetics team to discuss management plan
peripartum

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 13 of 25
3 Options for thromboprophylaxis Table 7. Options for thromboprophylaxis
Method Considerations
Non-pharmacological
• Encourage and educate the pregnant woman about the importance of: o Mobilisation o Avoidance of dehydration
Mechanical
• There is limited high quality evidence about the use of graduated elastic compression stockings (GCS) during pregnancy and the puerperium
• GCS are effective in diminishing the risk of DVT in non-pregnant hospitalised patients when used alone, with increased benefit when used in conjunction with another method of prophylaxis36
• There is limited high quality evidence about the effectiveness of knee length versus thigh length GCS37
• GCS o Patient compliance is essential – encourage to wear as much as
possible o Contraindicated in critical limb ischemia o Should be measured and fitted for each woman o A health professional trained in garment sizing and application can
assist with GCS selection and fitting o Check skin integrity regularly
• Intermittent pneumatic compression device (IPC) in combination with other prophylactic modalities has been shown to reduce the incidence of DVT in high-risk non-pregnant patients38
Pharmacological
• Low molecular weight heparin (LMWH) o Agent of choice for antenatal thromboprophylaxis2 o Does not cross placenta2,9 o No evidence of teratogenicity or increased risk of fetal bleeding2 o Associated with fewer bleeding episodes compared with
Unfractionated Heparin (UFH)13 o Risk of HIT lower with LMWH than with UFH2 o Risk of osteoporosis lower with LMWH than UFH2 o Refer to Department of Health: Anticoagulation and prophylaxis using
LMWH in adult inpatients39 • Unfractionated heparin • Warfarin:
o Contraindicated antenatally for thromboprophylaxis o Consider postnatal only for prolonged thromboprophylaxis or treatment o If warfarin used pre-pregnancy recommence postpartum o Refer to Appendix A for pharmacological information
• Note: LMWH, UFH and Warfarin are safe for breastfeeding mothers2

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 14 of 25
3.1 Other pharmaceutical agents
Table 8. Other pharmaceutical agents
Agents Considerations
Newer agents
• There is limited information about the use of newer pharmacological agents (e.g. Rivaroxaban) during pregnancy and their safety while breastfeeding16,40
• The American College of Chest Physicians recommend2: o Pregnant women: limit the use of Fondaparinux to those with severe
allergic reactions to Heparin who cannot receive Danaparoid o Pregnant women: avoid the use of oral direct thrombin (e.g. Dabigatran
and Factor-Xa inhibitors (e.g. Rivaroxaban, Apixaban) o Breastfeeding women: use alternative anticoagulants rather than
Fondaparinux and Factor Xa inhibitors (e.g. Rivaroxaban) • Not recommended in conjunction with neuraxial blockade41 • Discuss newer agents with a team experienced in their use • Refer to Department of Health: Guideline for managing patients on a factor
Xa inhibitor - Apixaban (Eliquis®) or Rivaroxaban (Xarelto®)42
Aspirin
• There are no controlled trials on the use of aspirin for thromboprophylaxis in pregnancy10
• The American College of Physicians recommend against the use of aspirin for VTE in any patient group2
• No adverse fetal outcomes were reported in a meta-analysis of large randomised controlled trials of low-dose aspirin for the prevention of preeclampsia in pregnancy43
• There is insufficient evidence to recommend routine use of aspirin for thromboprophylaxis in the antenatal and postnatal period at this stage

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 15 of 25
4 Prophylactic management of VTE Regardless of risk for VTE, minimise immobilisation and dehydration.
• Routine laboratory thrombophilia screening of pregnant women is not recommended1,2 • If anticoagulation is required peripartum a multidisciplinary team approach is essential
o Develop a plan for the peripartum management of anticoagulation (prophylactic or therapeutic)
• Determine dose of prophylaxis (standard, intermediate or therapeutic) based on the assessment of an individual’s risk for VTE
4.1 Specific patient group management If identified risk factor(s) include any of the following, refer to Section 5 for specific patient group antenatal and postnatal management:
o Significant personal history of VTE o Thrombophilia o Antiphospholipid syndrome o Long-term therapeutic coagulation
4.2 Antenatal prophylaxis UFH may be substituted for LMWH at the discretion of the obstetrician/physician in anticipation of birth.
Table 9. Antenatal prophylaxis
Risk assessment Antenatal prophylaxis
All risk (all antenatal women)
• Clinical surveillance • Encourage mobilisation • Avoid dehydration
High risk
• Recommend GCS • Consider IPC if hospitalised • Recommend prophylaxis with #LMWH • Liaise with a treating team experienced in prophylactic management
Moderate risk
• Discuss GCS • Consider IPC if hospitalised • Consider prophylaxis with #LMWH • Liaise with a treating team experienced in prophylactic management as
required Lower risk • As for all risk women
#Determine dose (standard, intermediate or therapeutic) based on individual assessment
4.3 Intrapartum prophylaxis For the woman receiving intermediate or high risk antenatal thromboprophylaxis:
• Document a plan of care that considers individual risk factors and clinical circumstances o Discuss the plan with the woman prior to labour and birth
• Liaise with a multidisciplinary team regarding: o Timing of anticoagulation cessation prior to established labour/planned birth o Timing for recommencement of thromboprophylaxis following birth
• Consider precautions related to neuraxial blockade [Refer to Section 4.5]

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 16 of 25
4.4 Postnatal prophylaxis • The risk of VTE is greater after caesarean section than after vaginal birth however, the
woman with multiple risk factors giving birth vaginally may still require specific VTE prophylaxis
• Postpartum prophylaxis should begin as soon as possible after birth15 • UFH may be substituted for LMWH at the obstetrician/physician’s discretion [refer to
Appendix A] • Consider precautions regarding neuraxial blockade management [Refer to Section 4.5]
Table 10. Prophylaxis postpartum by assessment of risk
Risk Assessment Clinical care
All risk (all postnatal women)
• Clinical surveillance • Early mobilisation • Avoid dehydration
High risk
• GCS until mobilising • Consider IPC • Recommend prophylaxis with #LMWH for 6 weeks • Refer to Section 5 Specific patient groups • Liaise with a treating team experienced in prophylactic management
Moderate risk
• Discuss GCS (until mobilising) • Recommend prophylaxis with #LMWH:
o Commence within 4 hours after giving birth10,15 o Continue until day 5 postpartum o If not fully mobile at day 5, then continue prophylaxis until fully mobile
Lower risk
• Discuss GCS • Consider prophylaxis with #LMWH
o Commence within 4 hours after giving birth10,15 o Continue until discharge or until fully mobile
• If hospitalised more than 5 days, medical staff review required regarding continuation/cessation of prophylaxis
#Determine dose (standard, intermediate or therapeutic) based on individual assessment

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 17 of 25
4.5 Neuraxial blockade
Table 11. Management of LMWH, UFH and neuraxial blockade
Aspect Clinical care
Context
• Safety of a neuraxial blockade in patients receiving anticoagulation depends on: o Anticoagulant used o Timing of insertion o Whether catheter is left in situ o Timing of removal
• Spinal haematoma, the most serious complication, is a clinical emergency1 o Tends to occur at either insertion or removal of a neuraxial catheter
• Consider risk and benefit relative to the clinical circumstances o Provide information to the woman to support informed decision making
Plan care
• Formulate a written plan of care • Refer to and discuss with the anaesthetic team • Monitor for evidence of neuraxial haematoma for 24 hours after insertion or
removal of a neuraxial block
LMWH prophylactic dose41
• Wait at least 12 hours after LMWH dose before performance of neuraxial block or removal of catheter
• Wait at least 4 hours following neuraxial blockade or neuraxial catheter removal before giving subsequent LMWH dose
LMWH therapeutic dose41
• Avoid therapeutic dosing with catheter in situ if possible • Wait at least 24 hours after the last therapeutic dose LMWH before
performing neuraxial blockade or removing catheter • Wait at least 4 hours after performing neuraxial blockade or removing
catheter before giving subsequent LMWH dose
UFH prophylactic dose41
• Wait at least 4 hours after last dose of UFH (doses ≤ 10,000 U) before performing neuraxial blockade or removing catheter
• Wait at least 1 hour after performing neuraxial blockade or removing a catheter before giving subsequent UFH dose
UFH therapeutic dose41
• Stop intravenous UFH at least 4 hours prior to performing neuraxial blockade or removing catheter
• Document normal activated partial thromboplastin (APTT) (3–4 hours after stopping infusion)
• Wait at least 4 hours after performing neuraxial blockade or removing catheter before giving subsequent UFH dose
Newer agents • There is limited data on the safety of newer drugs (e.g. Fondaparinux,
Rivaroxaban) and they are therefore not currently recommended in conjunction with neuraxial blockade41

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 18 of 25
5 Specific patient groups There is limited evidence to determine best practice. Each woman should be assessed on an individual basis and referred to a physician experienced in this area. Where pharmacological prophylaxis is indicated, also consider mechanical methods of prophylaxis (e.g. GCS, IPC) [refer to Table 7. Options for thromboprophylaxis] and Appendix A: Drug Information for dosing.
Table 12. Antenatal and postnatal management of specific patient groups
Liaise with a team experienced in this area regarding prophylaxis management Patient group Antenatal management Postpartum management • Single previous unprovoked VTE • Single previous pregnancy
associated VTE • Previous recurrent VTE • Single previous VTE and
thrombophilia • Single previous VTE associated
with combined oral contraceptive pill (COCP)
• Prophylaxis recommended (standard dose)
• Prophylaxis for 6 weeks (standard dose)
• Single previous provoked VTE (excluding those associated with COCP)
• Clinical surveillance unless other risk factors
• Prophylaxis for 6 weeks (standard dose)
• Any previous VTE and antithrombin deficiency
• Recurrent unprovoked VTE
• These women may be on long term anticoagulants
• Therapeutic anticoagulation required throughout pregnancy
• Therapeutic anticoagulation for 6 weeks or longer
• Long term anticoagulation any indication
• Therapeutic anticoagulation • Monitor in high risk clinic
• Return to pre-pregnancy therapeutic anticoagulation
• Administer therapeutic intravenous UFH or LMWH until therapeutic anticoagulation achieved
• Refer to usual treating healthcare team at discharge
• Antenatal VTE current pregnancy
• Therapeutic anticoagulation • Discuss duration with an
experienced team
• Management depends on timing of antenatal VTE
• Discuss with an experienced team
• Positive family history VTE but no personal history VTE, with antithrombin deficiency
• Consider intermediate dose prophylaxis or therapeutic anticoagulation
• Therapeutic anticoagulation for 6 weeks
• Positive family history VTE but no personal history VTE with significant laboratory thrombophilia (excluding antithrombin deficiency)
• Prophylaxis favoured especially if other risk factors (standard dose)
• Prophylaxis for 6 weeks (standard dose)
• No personal or family history of VTE but significant laboratory thrombophilia
• Clinical surveillance • Consider prophylaxis
(standard dose)
• Consider prophylaxis for 6 weeks (standard dose)
• Positive family history VTE but no personal history VTE and/or weak laboratory thrombophilia
• Clinical surveillance unless other risk factors
• Consider prophylaxis for 6 weeks especially if other risk factors (standard dose)
• Antiphospholipid syndrome and previous VTE
• Prophylaxis required • Discuss dose with an
experienced team
• Prophylaxis for 6 weeks • Discuss dose with an
experienced team • Antiphospholipid antibodies and
no previous VTE • Clinical surveillance • Prophylaxis 5-7 days
postpartum Adapted from: McLintock C ,Brighton T ,Chunilal S ,Dekker G ,McDonnell N ,McRae S, et al. Recommendations for the prevention of pregnancy-associated venous thromboembolism. Aust N Z J Obstet Gynaecol. 2012; 52(1):3-13

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 19 of 25
6 Discharge Table 13. Preparation for discharge
Aspect Considerations
Discharge information24
• Offer women and their families verbal and written information on12: o Signs and symptoms of VTE [Refer to Table 2] o How to reduce the risk of VTE (e.g. keep well hydrated and mobilise
frequently) o Risks and possible consequences of VTE o Importance of VTE prophylaxis [Refer to Section 1.2] o Correct use/application and duration of recommended treatment
including onset of action, monitoring requirements, and side effects of recommended treatment
o The importance of seeking help and who to contact if concerned o Discuss future anti-coagulation needs for subsequent pregnancies o The risk of VTE with prolonged periods of immobility (e.g. long
distance travel)
Follow-up • Complete a discharge summary/referral to the women’s local medical officer and if appropriate to the treating specialist

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 20 of 25
References 1. McLintock C, Brighton T, Chunilal S, Dekker G, McDonnell N, McRae S, et al. Recommendations for the prevention of pregnancy-associated venous thromboembolism. Aust N Z J Obstet Gynaecol. 2012; 52(1):3-13.
2. Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141(2 Suppl):e691S-736S.
3. National Health and Medical Research Council (NHMRC), Department of Health and Ageing, Australian Government. National guidance on collaborative maternity care. Canberra: NHMRC; 2010.
4. NHS, Quality Improvement Scotland. Pathways for maternity care. Keeping Childbirth Natural and Dynamic Programme. 2009.
5. Homer C, Brodie P, Leap N. Midwifery continuity of care: a practical guide. Sydney: Elsevier; 2008.
6. Marik PE, Plante LA. Venous thromboembolic disease and pregnancy. New England Journal of Medicine. 2008; 359(19):2025-33.
7. The American College of Obstetricians and Gynecologists. Practice Bulletin Number 123. Thromboembolism in pregnancy. Obsetrics and Gynecology. 2011; 118(3):718-29.
8. Centre for Maternal and Child Enquiries (CMACE). Saving mothers' lives: reviewing maternal deaths to make motherhood safer. 2006-2008. The eighth report on confidential enquiries into maternal deaths in the United Kingdom. BJOG. 2011; 118 (Suppl. 1):1-203.
9. Tooher R, Gates S, Dowswell T, Davis LJ. Prophylaxis for venous thromboembolic disease in pregnancy and the early postnatal period. Cochrane Database Syst Rev. 2010; (5):CD001689.
10. Royal College of Obstetricians and Gynaecologists. Reducing the risk of thrombosis and embolism during pregnancy and the puerperium. Green-top Guideline No.37a. 2009.
11. Scottish Intercollegiate Guidelines Network (SIGN). Prevention and management of venous thromboembolism: a national clinical guideline. 2010 [cited 2013 July 25]; SIGN publication no. 122. Available from: http://www.sign.ac.uk.
12. National Health and Medical Research Council (NHMRC). Blood Clots: Reducing your risk. 2010 [cited 2013 October 22]. Available from: http://www.nhmrc.gov.au/_files_nhmrc/file/nics/material_resources/stop_the_clot_patient_brochure_crop.pdf.
13. Wu P, Poole TC, Pickett JA, Bhat A, Lees CC. Current obstetric guidelines on thromboprophylaxis in the United Kingdom: evidence based medicine? Eur J Obstet Gynecol Reprod Biol. 2013; 168(1):7-11.
14. James AH. Prevention and treatment of venous thromboembolism in pregnancy. Clinical Obstetrics and Gynecology. 2012; 55(3):774-787.
15. Australian Government. National Health and Medical Research Council. Clinical practice guideline for the prevention of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to Australian hospitals. 2009. Available from: www.nhmrc.gov.au.
16. Lussana F, Coppens M, Cattaneo M, Middeldorp S. Pregnancy-related venous thromboembolism: risk and the effect of thromboprophylaxis. Thromb Res. 2012; 129(6):673-80.
17. Queensland Government. Maternity services. In: Clinical services capability framework for public and licensed private health facilities v3.1. Brisbane: Queensland Government Department of Health; 2012 [cited 2014 October 14]. Available from: http://www.health.qld.gov.au/cscf/default.asp.
18. Australian College of Midwives. National midwifery guidelines for consultation and referral. 3rd edition. 2013.
19. Australian Commission on Safety and Quality in Healthcare. National consensus statement: essential elements to recognising and responding to clinical deterioration. 2010 [cited 2013 August 12]. Available from: http://www.safetyandquality.gov.au.
20. Queensland Health. Heparin intravenous infusion order and administration form (SW034). Health Services Support Agency. 2013 [cited 2013 August 12]. Available from: http://qheps.health.qld.gov.au/hssa/home.htm.
21. Queensland Health. Guidelines for anticoagulation using warfarin. Health Services Support Agency. 2013 [cited 2013 August 12]. Available from: http://qheps.health.qld.gov.au/hssa/medicines/guidelines/home.htm.
22. Queensland Government. Patient Safety Communique No. 03/2013. Patient Safety Unit. [cited 2013, September 03]. Available from: http://qheps.health.qld.gov.au/psu/alerts/alerts.htm.

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 21 of 25
23. Okoroh E, Azonobi I, Grosse S, Grant A, Atrash H, James AH. Prevention of venous thromboembolism in pregnancy: a revew of guidelines, 2000-2011. Journal of Women's Health. 2012; 21(6):611-5.
24. National Institute for Health and Clinical Excellence. Venous thromboembolism: reducing the risk. London: National Institute of Clinical Excellence; 2010.
25. Jacobsen AF, Skjeldestad FE, Sandset PM. Incidence and risk patterns of venous thromboembolism in pregnancy and puerperium--a register-based case-control study. Am J Obstet Gynecol. 2008; 198(2):233 e1-7.
26. James AH, Jamison MG, Brancazio LR, Myers ER. Venous thromboembolism during pregnancy and the postpartum period: incidence, risk factors, and mortality. Am J Obstet Gynecol. 2006; 194(5):1311-5.
27. Knight M. Antenatal pulmonary embolism: risk factors, management and outcomes. BJOG. 2008; 115(4):453-61.
28. Lindqvist P, Dahlback B, Marsal K. Thrombotic risk during pregnancy: a population study. Obstet Gynecol. 1999; 94(4):595-9.
29. Kane EV, Calderwood C, Dobbie R, Morris C, Roman E, Greer IA. A population-based study of venous thrombosis in pregnancy in Scotland 1980-2005. Eur J Obstet Gynecol Reprod Biol. 2013; 169(2):223-9.
30. Jacobsen AF, Skjeldestad FE, Sandset PM. Ante- and postnatal risk factors of venous thrombosis: a hospital-based case-control study. J Thromb Haemost. 2008; 6(6):905-12.
31. Simpson EL, Lawrenson RA, Nightingale AL, Farmer RD. Venous thromboembolism in pregnancy and the puerperium: incidence and additional risk factors from a London perinatal database. BJOG. 2001; 108(1):56-60.
32. Sultan AA, Tata LJ, West J, Fiaschi L, Fleming KM, Nelson-Piercy C, et al. Risk factors for first venous thromboembolism around pregnancy: a population-based cohort study from the United Kingdom. Blood. 2013; 121(19):3953-61.
33. Sharma S, Monga D. Venous thromboembolism during pregnancy and the post-partum period: incidence and risk factors in a large Victorian health service. Aust N Z J Obstet Gynaecol. 2008; 48(1):44-9.
34. Won HS, Kim do Y, Yang MS, Lee SJ, Shin HH, Park JB. Pregnancy-induced hypertension, but not gestational diabetes mellitus, is a risk factor for venous thromboembolism in pregnancy. Korean Circ J. 2011; 41(1):23-7.
35. Danilenko-Dixon DR, Heit JA, Silverstein MD, Yawn BP, Petterson TM, Lohse CM, et al. Risk factors for deep vein thrombosis and pulmonary embolism during pregnancy or post partum: a population-based, case-control study. Am J Obstet Gynecol. 2001; 184(2):104-10.
36. Sachdeva A, Dalton M, Amaragiri SV, Lees T. Elastic compression stockings for prevention of deep vein thrombosis. Cochrane Database Syst Rev. 2010; (7):CD001484.
37. Sajid MS, Desai M, Morris RW, Hamilton G. Knee length versus thigh length graduated compression stockings for prevention of deep vein thrombosis in postoperative surgical patients. Cochrane Database Syst Rev. 2012; 5:CD007162.
38. Kakkos SK, Caprini JA, Geroulakos G, Nicolaides AN, Stansby GP, Reddy DJ. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism in high-risk patients. Cochrane Database Syst Rev. 2008; (4):CD005258.
39. Department of Health. Anticoagulation and prophylaxis using LMWH in adult inpatients. Document Number # QH-GDL-951:2014. 2014 [cited 2104 September 01]. Available from: http://www.health.qld.gov.au/qhpolicy/docs/gdl/qh-gdl-951.pdf.
40. Hale L. Medications and Mothers' Milk. 2013 [cited 2013, August 08]. Available from: https://www-medsmilk-com.cknservices.dotsec.com/
41. Harrop-Griffiths W, Cook T, Gill H, Hill D, Ingram M, Makris M, et al. Regional anaesthesia and patients with abnormalities of coagulation: The Association of Anaesthetists of Great Britain & Ireland The Obstetric Anaesthetists' Association Regional Anaesthesia UK. Anaesthesia. 2013.
42. Department of Health. Guideline for managing patients on a factor Xa inhibitor - Apixaban (Eliquis®) or Rivaroxaban (Xarelto®). Document Number # QH-GDL-950:2014. 2014 [cited 2014 September 01]. Available from: http://www.health.qld.gov.au/qhpolicy/docs/gdl/qh-gdl-950.pdf.
43. Duley L, Henderson-Smart DJ, Meher S, King JF. Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database Syst Rev. 2007; (2):CD004659.

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 22 of 25
Appendix A: Drug information The choice of drug is dependent on availability, clinical circumstances, patient preferences, and clinician familiarity. Note: Although there is limited data on the dosing of LMWH in pregnant women, obese women and women with renal impairment, the current doses are determined on standard practice worldwide. Liaise with an experienced team and/or pharmacist regarding LMWH dosing and monitoring for women greater than 100 kg (actual weight) or with renal impairment.
Caution: refer to Australian Medicine Handbook for complete drug information Dose Prophylactic STANDARD dose Prophylactic INTERMEDIATE dose THERAPEUTIC dose
for weight 50-100 kg
Liaise with experienced team if actual weight less than 50 kg or more than 100 kg
Dalteparin (Fragmin)
Less than 50 kg: 2500 units subcut once daily 50–100 kg: 5000 units subcut once daily Greater than 100 kg: 7500 units subcut once daily
5000 units subcut twice daily 100 units/kg twice daily
Enoxaparin (Clexane)
Less than 50 kg: 20 mg subcut once daily 50–100 kg: 40 mg subcut once daily Greater than 100 kg: 60–80 mg subcut once daily
40 mg subcut twice daily
Antenatal: 1mg/kg subcut twice daily Postnatal: 1.5 mg/kg subcut daily • Check renal function prior to initiating • If weight greater than 100 kg liaise with
experienced physician regarding dose
Sodium Heparin
Less than 50 kg: Consider reduced dose 50-100 kg: 5000 units subcut twice daily More than 100 kg: 7500 units subcut twice daily
7500 units subcut twice daily
Loading Dose: 80 units/kg IV stat Infusion: 18 units/kg/hour IV infusion • Monitor APTT as per Queensland Health’s
Heparin Intravenous Infusion Order and Administration - Adult form
Warfarin (postnatal) Do not use Do not use
Variable oral dose • Aim for INR 2-3 unless specified otherwise • Refer to Queensland Health’s guidelines for
anticoagulation using Warfarin* *Queensland Health, Health Services Support Agency http://qheps.health.qld.gov.au/hssa/home.htm Adapted from: Royal College of Obstetricians and Gynaecologists. Reducing the risk of thrombosis and embolism during pregnancy and the puerperium. Green-top Guideline No.37a. 2009.
Determine dose (standard, intermediate or therapeutic) based on assessment of an individual’s risk for VTE. Refer to Section 5: Specific patient groups

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 23 of 25
Appendix B: Adjusted odds ratio (AOR) for risk of VTE in pregnant and postpartum women compared with pregnant and postpartum women without these risk factors Risk Factor AOR 95%CI Comment Previous VTE 24.8 17.1–36 n=603 Age >35 1.3 1.0–1.7 pn=256 1.4 1.0–2.0 n=143 an PE BMI >30 mg/kg2 2.65 1.09–6.45 n=129 5.3 2.1–13.5 4.4 3.4–5.7 1.7 1.2–2.4 pn=256 BMI >25 mg/kg2 1.8 1.3–2.4 an=268 2.4 1.7–3.3 pn=291 1.7 1.2–2.4 pn=256 Parity 1 4.03 1.6–9.84 n=143 an PE Parity 2 1.5 1.1–1.9 n=603 Parity 3 2.4 1.8–3.1 n=603 Smoking 2.1 1.3–3.4 an=268 Smoking 10–30/day 3.4 2.0–5.5 pn=291 1.4 1.1–1.9 n=603 2.5 1.3–4.7 n=90 Current smoker 2.7 1.5–4.9 n=129 Sickle cell 6.7 4.4–10.1 2.5 1.5–4.1 DVT 1.7 0.9–3.1 PE Heart disease 7.1 6.2–8.3 5.4 2.6–11.3 pn=256 SLE 8.7 5.8–13 Anaemia 2.6 2.2–2.9 Varicose veins 2.4 1.04–5.4 Immobility 7.7 3.2–19 an 10.8 4.0–28.8 pn Preeclampsia 2.9 2.1–3.9 3.1 1.8–5.3 Preeclampsia + fetal growth restriction 5.8 2.1–16 Hyperemesis 2.5 2–3.2 Assisted reproductive technology 4.3 2.0–9.4 an Twins 2.6 1.1–6.2 an Multiple pregnancy 4.2 1.8–9.7 n=603 Preterm delivery <36 weeks 2.4 1.6–3.5 an=109 Antepartum haemorrhage 2.3 1.8–2.8 pn=256 Emergency caesarean section 2.7 1.8–4.1 Any caesarean section 3.6 3.0–4.3 pn=256 Postpartum haemorrhage >1 L 4.1 2.3–7.3 Postpartum haemorrhage + surgery 12 3.9–36.9 Obstetric haemorrhage 9 1.1–71 Postpartum infection 4.1 2.9–5.7 Postpartum infection + caesarean section 6.2 2.4-16.2 Transfusion 7.6 6.2–9.4 an=antenatal; pn=postnatal; n=number of cases in case-control study; Source: Royal College of Obstetricians and Gynaecologists. Reducing the risk of thrombosis and embolism during pregnancy and the puerperium. Green-top Guideline No.37a. 2009.

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 24 of 25
Appendix C: Risk of VTE with Thrombophilia Adjusted odds ratio for risk of VTE in pregnancy and/or postpartum with different thrombophilia
Thrombophilia Risk of VTE Odds Ratio Odds Ratio 95% CI
Antithrombin deficiency 10–unknown 4.7 1.3–17.0 Protein C deficiency 2–unknown 4.8 2.2–10.6 Protein S deficiency – 3.2 1.5–6.9 Factor V Leiden (heterozygous) 5–7 8.3 5.4–12.7 Prothrombin G20210A (heterozygous) 3–10 6.8 2.5–18.8 Factor V Leiden (homozygous) 10–41 34.4 9.9–120.1 Prothrombin G20210A (homozygous) – 26.4 1.2–559.2 Compound heterozygote (Factor V Leiden and prothrombin G20210A) 9–107 – –
Source: Royal College of Obstetricians and Gynaecologists. Reducing the risk of thrombosis and embolism during pregnancy and the puerperium. Green-top Guideline No.37a. 2009. Estimated absolute risk of VTE with different thrombophilic defects in women with one or more symptomatic first degree relatives Thrombophilic defect Pregnancy Antenatal Postpartum
%/pregnancy 95% CI %/pregnancy 95% CI %/pregnancy 95% CI Antithrombin, Protein C, Protein S deficiency 4.1 1.7–8.3 1.2 0.3–4.2 3.0 1.3–6.7
Antithrombin deficiency type 1* 15–50 (range) – 0–40 – 11–28 –
Factor V Leiden (heterozygous) 2.1 0.7–4.9 0.4 0.1–2.4 1.7 0.7–4.3
Prothrombin G20210A (heterozygous) 2.3 0.8–5.3 0.5 0.1–2.6 1.9 0.7–4.7
Factor V Leiden (homozygous) or Compound heterozygote (Factor V Leiden and prothrombin G20210A)
1.8–15.8 (range) – 0–5 – 1–10 –
*Population-based not family study Source: Royal College of Obstetricians and Gynaecologists. Reducing the risk of thrombosis and embolism during pregnancy and the puerperium. Green-top Guideline No.37a. 2009.

Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium
Refer to online version, destroy printed copies after use Page 25 of 25
Acknowledgements Queensland Clinical Guidelines gratefully acknowledges the contribution of Queensland clinicians and other stakeholders who participated throughout the guideline development process particularly:
Working Party Clinical Lead
Dr Karin Lust, Obstetric Physician, Royal Brisbane and Women’s Hospital, Brisbane
Working Party Members
Ms Noor Aladhami, Pharmacist, Royal Brisbane and Women’s Hospital Mrs Anne Bousfield, Midwifery Unit Manager, Roma Hospital Dr Stephen Elgey, Staff Specialist, Obstetrics and Gynaecology, Logan Hospital Dr Hasthika Ellepola, Staff Specialist, Obstetrics and Gynaecology, Logan Hospital Ms Sandra Gosley, VTE Coordinator, RBWH Safety and Quality Unit, Royal Brisbane and Women's Hospital Ms Debbie Humbley, Midwife, Maternity Unit, Dalby-Jandowae Health Service Associate Professor Rebecca Kimble, Director Obstetric Services, Royal Brisbane and Women's Hospital Dr Alka Kothari, Staff Specialist, Obstetrics and Gynaecology, Redcliffe Hospital Associate Professor, Kassam, Mahomed, Staff Specialist, Obstetrics and Gynaecology, Ipswich Hospital Dr Bruce Maybloom, Resident Medical Officer, Queensland Ms Jody Paxton, Coordinator, Statewide Intensive Care Network, Clinical Access and Redesign Unit, Queensland Health Mrs Bernice Ross, Midwife, Lactation Consultant, Private Sector Ms Meredith Shallcross, Perinatal Information Midwife, Redcliffe Hospital Mrs Robyn Sharpe, Team Leader Physiotherapy Women's Health, Royal Brisbane and Women's Hospital Dr Makarla Stead, Staff Specialist, Anaesthesiology and Perioperative Services, Royal Brisbane and Women’s Hospital Dr Agnes Wilson, Guideline Developer/Women’s Health Coordinator, Royal Australian and New Zealand College of Obstetricians and Gynaecologists Ms Latisha Ryder, Consumer Representative, Maternity Coalition
Queensland Clinical Guidelines Team
Associate Professor Rebecca Kimble, Director Ms Jacinta Lee, Program Manager Ms Lyndel Gray, Clinical Nurse Consultant Dr Brent Knack, Program Officer Ms Jeanette Tyler, Clinical Nurse Consultant Queensland Clinical Guidelines Steering Committee
Funding
This clinical guideline was funded by Queensland Health, Health Systems Innovation Branch.