
VP Shunt Case Report
46
I. Introduction Hydrocephalus or "water on the brain." is a build-up of fluid inside the skull, leading to brain swelling, and ventriculoperitoneal shunt is a basic part of its treatment. Hydrocephalus is due to a problem with the flow of cerebrospinal fluid (CSF), the liquid that surrounds the brain and spinal cord. The fluid brings nutrients to the brain, takes away waste from the brain, and acts as a cushion. CSF normally moves through areas of the brain called ventricles, then around the outside of the brain and the spinal cord. It is then reabsorbed into the bloodstream. Buildup of CSF can occur in the brain if its flow or absorption is blocked or if too much CSF is produced. This build-up of fluid puts pressure on the brain, pushing the brain up against the skull and damaging or destroying brain tissues. Hydrocephalus may start while the baby is growing in the womb. It is commonly present with myelomeningocele , a birth defect involving incomplete closure of the spinal column. Genetic defects and certain infections that occur during pregnancy may also cause hydrocephalus. In young children, hydrocephalus may also be associated with the following conditions: Infections that affect the central nervous system (such as meningitis or encephalitis), especially in infants, bleeding in the brain during or soon after delivery (especially in premature babies), injury before, during, or after childbirth, including subarachnoid hemorrhage, tumors of the central nervous system, including the brain or spinal cord, Injury or trauma. The goal of ventriculoperitoneal shunting is to reduce or prevent brain damage by improving the flow of CSF. 1
-
Upload
dhei-dayrit -
Category
Documents
-
view
888 -
download
3
Transcript of VP Shunt Case Report

I. Introduction
Hydrocephalus or "water on the brain." is a build-up of fluid inside the skull,
leading to brain swelling, and ventriculoperitoneal shunt is a basic part of its
treatment. Hydrocephalus is due to a problem with the flow of cerebrospinal fluid
(CSF), the liquid that surrounds the brain and spinal cord. The fluid brings nutrients
to the brain, takes away waste from the brain, and acts as a cushion.
CSF normally moves through areas of the brain called ventricles, then around
the outside of the brain and the spinal cord. It is then reabsorbed into the
bloodstream. Buildup of CSF can occur in the brain if its flow or absorption is
blocked or if too much CSF is produced. This build-up of fluid puts pressure on the
brain, pushing the brain up against the skull and damaging or destroying brain
tissues.
Hydrocephalus may start while the baby is growing in the womb. It is
commonly present with myelomeningocele, a birth defect involving incomplete
closure of the spinal column. Genetic defects and certain infections that occur
during pregnancy may also cause hydrocephalus. In young children, hydrocephalus
may also be associated with the following conditions: Infections that affect the
central nervous system (such as meningitis or encephalitis), especially in infants,
bleeding in the brain during or soon after delivery (especially in premature babies),
injury before, during, or after childbirth, including subarachnoid hemorrhage,
tumors of the central nervous system, including the brain or spinal cord, Injury or
trauma.
The goal of ventriculoperitoneal shunting is to reduce or prevent brain
damage by improving the flow of CSF.
The blockage may be surgically removed, if possible. If the blockage cannot
be removed, a shunt (flexible tube) may be placed within the brain to allow CSF to
flow around the blocked area. The shunt tubing travels to another part of the body,
such as the abdomen, where the extra CSF can be absorbed. This procedure is done
in the operating room under general anaesthesia. It takes about 1 1/2 hours. The
child's hair behind the ear is shaved off. A surgical cut in the shape of a horseshoe
1

(U-shape) is made behind the ear. Another small surgical cut is made in the child's
belly. A small hole is drilled in the skull. A small thin tube called a catheter is passed
into a ventricle of the brain. Another catheter is placed under the skin behind the
ear and moved down the neck and chest, and usually into the abdominal
(peritoneal) cavity. Sometimes, it goes to the chest area. The doctor may make a
small cut in the neck to help position the catheter. A valve (fluid pump) is placed
underneath the skin behind the ear. The valve is attached to both catheters. When
extra pressure builds up around the brain, the valve opens, and excess fluid drains
out of it into the belly or chest area. This helps decrease intracranial pressure. The
valves in newer shunts can be programmed to drain more or less fluid from the
brain.
As Nurses, one should always be updated with current procedures, treatment,
and management applied in the clinical setting. One should be well informed in
advances in the field since this can be used in fulfilling the role of a Nurse as a
Health Educator. An In-depth study of this procedure should be advocated by the
Nurses since they are also involved in the Procedure. As a member of the Health
team and a member of the sterile team, it is important to be well educated and well
informed not only in skills but also in theory during practice since one is dealing
with life. . Research in this area can help shed light into the workings of the disease,
the predisposing factors, impact on the morbidity and mortality rates and the
measures taken by the health care team in the treatment and control of the
condition.
2
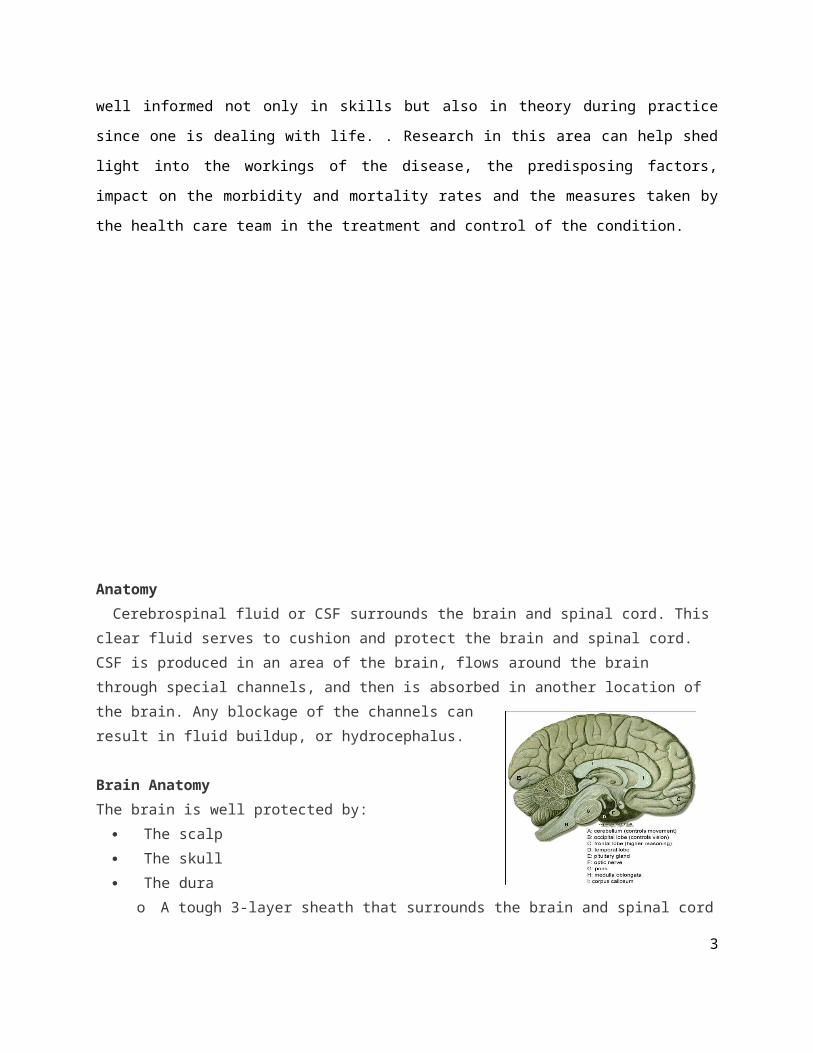
Anatomy
Cerebrospinal fluid or CSF surrounds the brain and spinal cord. This clear fluid
serves to cushion and protect the brain and spinal cord. CSF is produced in an area
of the brain, flows around the brain through special channels, and then is absorbed
in another location of the brain. Any blockage of the channels can result in fluid
buildup, or hydrocephalus.
Brain Anatomy
The brain is well protected by:
The scalp
The skull
The dura
o A tough 3-layer sheath that surrounds the
brain and spinal cord
o Layers include the dura mater (strongest layer), arachnoid mater (middle
layer), and pia mater (closest to the brain)
The brain is a complicated structure containing many parts. These include:
The cerebrum:
o Made up of two cerebral hemispheres that are connected in the middle
o It is the largest part of the brain
o Each area of the cerebrum performs an important function, such as
language or movement
o Higher thought (cognition) comes from the frontal cortex (front portion of
the cerebrum)
o Outside of the cerebrum are blood vessels
o There are fluid-filled cavities and channels inside the brain
o
The cerebellum:
o Located in the lower, back part of the skull
3

o Controls movement and coordination
The brainstem and pituitary gland:
o Responsible for involuntary functions such as breathing, body temperature,
and blood pressure regulation
o Pituitary gland is the "master gland" that controls other endocrine glands in
the body, such as the thyroid and adrenal glands
The cranial nerves:
o Twelve large nerves exit the bottom of the brain
to supply function to the senses such as hearing,
vision, and taste
The cerebral blood vessels:
o A complicated system that supplies oxygenated
blood and nutrients to the brain
The blood supply to the brain is divided into two main parts:
Anterior cerebral circulation:
o The front of the brain is supplied by the paired carotid arteries in the neck.
Posterior cerebral circulation:
The back portion of the brain is supplied by the paired vertebral arteries in
the spine.
4

Hydrocephalus is a condition caused by an imbalance in the production and absorption of CSF in the ventricular system. When production exceeds absorption, CSF accumulates, usually under pressure, producing dilation of the ventricles.
It is a term derived from the Greek words “hydro” meaning water, and “cephalus” meaning head, and this condition is sometimes known as “water on the brain”.
People with hydrocephalus have abnormal accumulation of cerebrospinal fluid (CSF) in the ventricles, or cavities, of the brain. This may cause increased intracranial pressure inside the skull and progressive enlargement of the head, convulsion, and mental disability.
Usually, hydrocephalus does not cause any intellectual disability if recognized and properly treated. A massive degree of hydrocephalus rarely exists in typically functioning people, though such a rarity may occur if onset is gradual rather than sudden.Hydrocephalus occurs with a number of anomalies, such as NTD’s.
Etiology:Congenital hydrocephalus usually results from defects, such as Chairi
malformations. It is also associated with spina bifida.Acquired hydrocephalus usually results from space-occupying lesions,
hemorrhage, intracranialinfections or dormant development defects.
People with hydrocephalus have abnormal accumulation of cerebrospinal fluid (CSF) in the ventricles, or cavities, of the brain. This may cause increased
5

intracranial pressure inside the skull and progressive enlargement of the head, convulsion, and mental disability.Usually, hydrocephalus does not cause any intellectual disability if recognized and properly treated. A massive degree of hydrocephalus rarely exists in typically functioning people, though such a rarity may occur if onset is gradual rather than sudden.Hydrocephalus occurs with a number of anomalies, such as NTD’s.
6

PATHOPHYSIOLOGY
7
Choroid Plexuses of the Lateral Ventricles
CSF Formation
Impaired Absorption of CSF within the Arachnoid Space
(communicating hydrocephalus)
Obstruction to the flow of CSF through the ventricular system
(non-communicating hydrocephalus)
Increased ICP
Dilation of the pathways proximal to the site of obstruction
Abnormal increase in volume of CSF
Enlargement of the head in infancy

III. CLINICAL INTERVENTION
1.1 Description of prescribed surgical treatment performed
Ventriculoperitoneal shunting is surgery to relieve increased pressure inside the skull due to excess cerebrospinal fluid (CSF) on the brain (hydrocephalus).
Description
This procedure is done in the operating room under general anesthesia. It takes about 1 1/2 hours.
The child's hair behind the ear is shaved off. A surgical cut in the shape of a horseshoe (U-shape) is made behind the ear. Another small surgical cut is made in the child's belly.
A small hole is drilled in the skull. A small thin tube called a catheter is passed into a ventricle of the brain.
8

Another catheter is placed under the skin behind the ear and moved down the neck and chest, and usually into the abdominal (peritoneal) cavity. Sometimes, it goes to the chest area. The doctor may make a small cut in the neck to help position the catheter.
A valve (fluid pump) is placed underneath the skin behind the ear. The valve is attached to both catheters. When extra pressure builds up around the brain, the valve opens, and excess fluid drains out of it into the belly or chest area. This helps decrease intracranial pressure.
The valves in newer shunts can be programmed to drain more or less fluid from the brain.
THE PROCEDURE
Position of the child is important to correctly implant the shunt. The head is
turned sharply to the left to accommodate a right occipital placement. The burr hole is
placed approximately 4 cm up from the inion and 3-4 cm off the mid-line. This occipital
placement allows a relatively straight shot into the body of the ventricle so that the shunt
catheter is mostly within it. This trajectory avoids the risk of going too low, through the
internal capsule, which can happen with shunt placement sites that are more lateral and
inferior.
An adequate length of ventricular catheter needs to be selected to place the tip anterior
to the foramen of Munroe, where there is less choroid plexus. This is to lessen the risk
of occlusion. Generally, a 6 cm catheter is used in a small newborn; an 8 cm catheter in
an older infant and young child; and a 10 cm catheter is used in a children 18 months or
older. Perioperative antibiotics can be used, though definitive data showing that this is
mandatory is lacking.
The shoulder blades should be raised to elevate the chest and neck, and allow for a
straight passage of the shunt passer with no secondary incisions between the head and
the abdomen. The abdominal incision is a horizontal incision, either just below the rib
cage or just lateral to the umbilicus. Once the shunt is laid in position, the dura is
opened with a pinpoint cautery to have just a big enough opening to allow the passage
of the catheter (a large dural opening can allow CSF to flow around the shunt and cause
a subcutaneous fluid collection). The ventricle is tapped using a rigid brain cannula and,
once a good flow of CSF has been obtained, the ventricular catheter is fed into the
ventricle through this tract. This is done without a stylette.
9

Fluid should then be aspirated from the lower end of the shunt, to insure that the valve
system is opened, and then it should then be placed into the peritoneal cavity. A large
amount of tubing can be placed in the peritoneal cavity, even enough to allow for full
growth of the child. 15-20" of peritoneal catheter is usually inserted at the same time as
the initial shunt placements.
Risks
Risks for any anesthesia are:
Reactions to medications Problems breathing
Changes in blood pressure or breathing rate
Risks for any surgery are:
Bleeding Infection
Possible risks of ventriculoperitoneal shunt placement are:
Blood clot or bleeding in the brain Brain swelling
The shunt may stop working and fluid will begin to build up in the brain again.
The shunt may become infected.
Infection in the brain
Damage to brain tissue
Seizures
1.2 Indication of prescribed surgical treatment
10

The procedure is indicated for people with hydrocepahalus. In hydrocephalus, there is a buildup of fluid of the brain and spinal cord (cerebrospinal fluid or CSF). This buildup of fluid causes higher than normal pressure on the brain. Too much pressure, or pressure that is present too long, will damage the brain tissue.
A shunt helps to drain the excess fluid and relieve the pressure in the brain. A shunt should be placed as soon as hydrocephalus is diagnosed.
1.3 Required instruments, devices, supplies, equipment and facilities
The Operating Room
Surgical Drill
11

Used to created a burr hole.
Dissecting Instruments
In the first part of the surgery, incisions are made with dissectors, which are either sharp
or and are used to make precise incisions, the most well know example being the
scalpel. Blunt instruments, such as the elevator or the curette are mostly used to scrape
tissues.
Clamps
12

After the incision is made, the surrounding skin is clamped with the use of forceps or
clips. These instruments are also used to hold not only tissues, but also other
instruments.
Cauterization
An electrocautery machine is used to remove lesions and tissues that are highly
vascularized. The machine reduces the risk of bleeding, sealing off blood vessels by
using high frequency electric currents to instantly stop bleeding.
e. Suction
13

Oozing of blood and other fluids are inevitable in a surgical procedure, including
a ventriculoperitoneal shunt procedure. The suction machine is tied to a container
where the loss of fluid can be measured and monitored during the procedure.
f. Sutures, Staples, Needles
Closure of the incision site occurs after the procedure. The needles, along with the
sutures are used to properly close the site. Sutures can be absorbable or non-
absorbable. Staples, however, are used frequently nowadays to speed up the surgery
and reduce the chance of infection due to an open wound
g. Drains
Before surgical closure, a drain is attached to the site to remove the remaining fluid left
over from the procedure. It also allows the medical personnel to monitor the amount of
bleeding during the post-operative phase. Its drainage also helps a physician determine 14

if an infection is developing or healing. Removal of the drains is the prerogative of the
surgical team, which usually leave it in place for five to six post-operative days.
1.4 Perioperative tasks and responsibilities of the Nurse
PRE-OPERATIVE CARE
Preparing the operating theatre
Ensure that:
the operating theatre is clean (it should be cleaned after every procedure)
necessary supplies and equipment are available, including drugs and an oxygen
cylinder
emergency equipment is available and in working order
there are adequate supply of theatre dress for the anticipated members of the
surgical team
clean linens are available
sterile supplies (gloves, gauze, instruments) are available and not beyond expiry
date
Surgical handscrub
15

Remove all jewelry.
Hold hands above the level of the elbow, wet hands thoroughly and apply soap
(preferably an iodophre, e.g. betadine).
Begin at the fingertips and lather and wash, using a circular motion:
Wash between all fingers;
Move from the fingertips to the elbows of one hand and then repeat for the
second hand.
Wash for three to five minutes
Rinse each arm separately, fingertips first, holding hands above the level of the
elbows.
Dry hands with a clean or disposable towel, wiping from the fingertips to the
elbows, or allow hands to air dry.
Ensure that scrubbed hands do not come into contact with objects (e.g.
equipment, protective gown) that are not high-level disinfected or sterile. If the
hands touch a contaminated surface, repeat surgical handscrub.
INTRA OPERATIVE CARE
Assist in the sterile gowning and gloving of the surgeon and his or her assistant.
Prevent injury to the patient by removing heavy or sharp instruments from the
operative site as soon as the surgeon has finished using them.
Constantly be alert to any intraoperative dangers to the patient.
Take part in sponge, needle, and instrument counts, as needed. All of these
items must be accounted for during the procedure. The technologist takes part in
counting the items before, during, and after surgery to ensure that they are not
left in the wound. The count is done in an orderly way and is performed using
accepted technique.
16

Properly identify and preserve specimens received during surgery. The
technologist is responsible for maintaining the specimens in a prescribed manner
so that the material can be subsequently examined by the pathologist.
Anticipate the needs of the surgeon by watching the progress of the surgery and
knowing the various steps of the procedure. He or she passes instruments and
other supplies in an acceptable manner so that the surgeon does not have to turn
away from the wound site to receive them.
Assist the surgeon by tissue retraction, suture cutting, fluid evacuation, or
sponging the wound when asked to do so.
At the end of the procedure, assemble all instruments and supplies and prepare
them for decontamination and resterilization and assist in the safe clean-up of the
operating suite following Universal Precautions.
POST OPERATIVE CARE
At the recovery room, the nurse will monitor the blood pressure, pulse and
breathing of the patient
Place a dressing (bandage) over the surgery site
Provide instructions on how to care for the patient at home, including taking care
of the incision and drains, recognizing signs of infection and understanding
activity restrictions
Talk to the patient about when to resume wearing a bra or wearing a breast
prosthesis
Give prescriptions for pain medication and possibly an antibiotic
Remind the patient to meet with her doctor a week or two after surgery. The
drainage tubes will likely be removed at that time.
17

1.5 Expected outcomes of surgical treatment performed
Shunt placement is usually successful in reducing pressure in the brain. But if hydrocephalus is related to other conditions, such as spina bifida, brain tumor, meningitis, encephalitis, or hemorrhage, these conditions could affect the prognosis. The severity of hydrocephalus present before surgery will also affect the outcome.
Support groups for families of children with hydrocephalus or spina bifida are available in most areas.
The major complications to watch for are an infected shunt and a blocked shunt.
The patient will need to lie flat for 24 hours the first time a shunt placed. After that your child will be helped to sit up.
The usual stay in the hospital is 3 to 4 days.The doctor will check vital signs and neurological status often. Your child may get medication for pain. Intravenous fluids and antibiotics are given. The shunt will be checked to make sure it is working properly.
1.6 Medical management of physiologic outcomes
Pain Management
People experience different types and amount of pain or discomfort after surgery.
The goal of pain management is to assess the level of discomfort and to take
medication as needed. The patient will be given a prescription for analgesics for the
management of moderate pain. It is recommended to take medication for pain when
pain is experienced on a regular schedule. Ibuprofen (Advil) can be added to or replace
18

the analgesic. Everyone is different and if one plan to decrease pain is not working, it
will be changed. Healing and recovery improve with good pain control.
An icepack may also be helpful to decrease discomfort and swelling.
Incision and Dressing Care
Incision, or scar, has both stitches and steri-strips, which are small white strips of
tape, and is covered by a gauze dressing and tape or a plastic dressing. Advise the
patient not to remove the dressing, steri-strips or stitches. The nurse will remove the
dressing in seven to 10 days. The nurse will also remove the sutures in one to two
weeks unless they absorb on their own. If the dressing or steri-strips fall off, tell the
patient not to attempt to replace them.
Educate patient that bruising and some swelling are common after surgery. Also,
a low-grade fever that is below 100 degrees Fahrenheit is normal the day after surgery.
A home care nurse may be assigned to check your progress at home.
Activity
Inform patient to avoid strenuous activity, heavy lifting and vigorous exercise until
the stitches are removed. Walking is a normal activity that can be restarted right away.
Recommend exercises to regain movement and flexibility. Most people return to work
within three to six weeks.
Diet
The patient may resume regular diet as soon as you can take fluids after
recovering from anesthesia. Encourage to drink eight to 10 glasses of water and non-
caffeinated beverages per day, plenty of fruits and vegetables as well as lower fat
foods.
19

20

NURSING CARE PLAN
Deficient knowledge related to client and family understanding of the preoperative, operative, and
postoperative phases of ventriculoperitoneal shunt
Assessment Nursing
Diagnosi
s
Scientific
Explanation
Planning Nursing
Interventions
Rationale Evaluation
S>
“Napansin
ko na
hindi
normal ang
laki ng ulo
ng
anak ko” as
verbalized
by the
mother.
O> the
patient may
manifest:
Deficient
knowled
ge
related
to client
and
family
understa
nding of
the
preopera
tive,
operativ
e, and
postoper
Due to its
complicated
procedure,
the parents
of such
patients who
undergo this
surgery may
have many
misconceptio
n and lack of
information
which leads
to deficient
knowledge of
After 4
hours of
nursing
intervention
s, the family
will be able
to
participate
in learning
process and
exhibit
increased
interest/
assume
responsibilit
>Establish rapport
>Assess patient’s
general condition
>Monitor and record
vital signs
>Obtain baseline
neurologic
assessment:
a. Motor and sensory
>To gain the trust and
cooperation of the
patient
>To obtain base line
data
>To obtain baseline
data
>Establishes baseline
motor and sensory
function for later
comparisons,
determines level of
Short-
term:
The family
shall have
participate
d in
learning
process
and
exhibited
increased
interest/
assumed
responsibil
21

-
Restlessnes
s
Irritability
-Changes in
VS
-
verbalizatio
n of
misconcepti
ons about
the
surgery of
So
ative
phases
of
ventricul
operiton
eal
shunt
the family. y for own
learning by
beginning to
look for
information
and ask
questions
Long-term:
After 3-5
days of
nursing
intervention
s, the client
and family
will be able
to have
sufficient
knowledge
regarding
the surgical
procedure,
preoperativ
function
b. Psychological
readiness
>Discuss activity
limitation
>Review pain
management
>Discuss proper
wound care
ability and knowledge
>Prevents damage to
surgical site
>To gain knowledge
on treating / managing
postoperative pain
> to provide non
pharmacologic
interventions to
alleviate pain
>To prevent
ity for own
learning
by
beginning
to look for
informatio
n and ask
questions
Long-term:
The family
shall have
sufficient
knowledge
regarding
the
surgical
procedure,
preoperati
ve
preparatio
ns, and
22

e
preparations
, and the
postoperativ
e
precautions
and needs
to be able to
prevent the
developmen
t of
complicatio
ns
>Discuss changes in
home environment:
occurrence of infection
>Anticipate home care
needs
the
postoperat
ive
precaution
s and
needs to
be able to
prevent
the
developm
ent of
complicati
ons
23

Risk for infection secondary to surgical incision
Assessment Nursing
Diagnosis
Scientific
Explanation
Planning Nursing
Interventions
Rationale Evaluation
S> Ø
O>the
patient may
manifest:
-increased
body
temperature
-increased
WBC
-
inflammatio
n in the
surgical
Risk for
infection
secondar
y to
surgical
incision
The skin
considered as
the first line
of defense
against any
foreign
organism
when surgical
procedure
impaired the
skin, possible
entry of
microorganis
m therefore
may cause
infection
Short term:
After 4 hours of
nursing
interventions,
the patient will
identify and
demonstrate
intervention to
prevent
infection
Long term:
After 3-5 days
of nursing
intervention the
patient will
>Establish
rapport
>Monitor V.S.
>Note signs and
symptoms of
sepsis
>Provide wound
healing such as
cleaning of
wound
>Provide care,
change dressing
as needed
>To gain trust
>To obtain
baseline data
>To reduce
complication and
monitor for
infection
>To reduce risk
for infection
>To promote
healing to the
incision
>to prevent
occurrence of
Short term:
The patient
identified and
demonstrated
interventions to
prevent risk of
infection
Long-term:
the patient shall
have achieved
timely wound
healing without
developing
infections
24

incision
-bleeding in
the surgical
incision
achieve timely
wound healing
without
developing
infections
Prevent stress on
incision line,
cleanse site daily
as ordered, and
apply dry, sterile
dressing
> emphasize
importance of
proper hygiene
and wound care
>Encourage
ongoing
nutritional needs
> Emphasize
necessity of
taking antibiotics
to s.o as directed
infection
>To prevent
infection to
increase immune
resistance
>To increase
healing of wound
> Premature
discontinuation
of treatment
when client
begins to feel
well may result
in return of
infection
>To prevent
occurrence of
25

> Administer
prophylactic
antibiotics as
ordered
infection
Decreased Intracranial Adaptive Capacity r/t Space- Occupying Lesion secondary to reoccurrence of fluid accumulation due to shunt defect.
Assessment Diagnosis Scientific
Explanation
Planning Nursing
Interventions
Rationale Expected
Outcome
S>Ø Decreased Complications Short term: >Establish >To gain the client The SO shall
26

O> the pt.
manifested
the ff.
-Altered
mental
status
-Speech
abnormaliti
es
-
Restlessnes
s
-Changes in
mental
state AEB
(-) pupil
reaction to
light,
flexion on
pain, no
verbal
Intracrani
al
Adaptive
Capacity
r/t Space-
Occupying
Lesion
secondary
to
reoccurre
nce of
fluid
accumulat
ion due to
shunt
defect.
of
ventriculoperi
toneal
shunting can
occur. Some
patients may
experience
blood clot or
bleeding in
the brain,
swelling and
infection in
the brain,
brain tissue
damage,
reoccurrence
of fluid build
up in the
brain because
the shunt
may also stop
working, the
shunt may
After 1-2° of NI
the SO will be
able to
understand the
client’s
condition and
be able
perform
actively in
promoting the
clients
condition
having now a
higher level of
understanding
of the client’s
condition and
complications
that may occur.
rapport
>Monitor VS.
>Monitor/
document
changes in ICP
waveform and
responses to
stimuli.
>Assess eye
opening and
position/movem
ent, Pupils (size,
equality, light
reactivity),
purposeful and
non-purposeful
motor response
comparing left
and right sides,
presence of
and SO’s trust.
>To obtain data
for comparison.
>To alter care
appropriately.
> To note degree
of impairment
>To increase SO’s
understanding of
have
understand
the client’s
condition and
be able
perform
actively in
promoting the
clients
condition
having now a
higher level of
understanding
of the client’s
condition and
complications
that may
occur.
The client shall
have
demonstrated
stable ICP AEB
27

response. also become
infected and
seizures may
occur.
Intracranial
pressure,
(ICP), is the
pressure
exerted by
the cranium
on the brain
tissue,
cerebrospinal
fluid (CSF),
and the
brain's
circulating
blood volume.
ICP is a
dynamic
phenomenon
constantly
fluctuating in
Long term:
After 6-7 days
of NI the client
will be able to
demonstrate
stable ICP AEB
normalization
of pressure
waveforms/res
ponse to
stimuli.
reflexes, nuchal
rigidity,
consciousness
and mental
state.
>Provide
information
about the
client’s
condition
including the
complications
which may arise
once untreated
>Elevate HOB
and maintain
head/neck in
midline/neutral
position
>Decrease
the client’s
condition and will
be able to decide
properly for the
client’s care.
>To promote
circulation/venous
drainage
>To reduce CNS
stimulation and
promote
relaxation.
>To decrease
factors which may
contribute in
further increasing
ICP.
>To
pharmacologically
manage client’s
normalization
of pressure
waveforms/res
ponse to
stimuli.
28

response to
activities such
as exercise,
coughing,
straining,
arterial
pulsation, and
respiratory
cycle. An
increase in
pressure,
most
commonly
due to head
injury leading
to intracranial
hematoma or
cerebral
edema can
crush brain
tissue, shift
brain
structures,
extraneous
stimuli/provide
comfort
measures
>Limit activities
that increases
intrathoracic/ab
dominal
pressure
>Administer
medications as
ordered (e.g.
antihypertensiv
es, diuretics,
analgesics,
antipyretics,
vasopressors,
antiseizure,
neuromuscular
blocking agents,
and
condition and
maintain
homeostasis
>To reduce ICP
and enhance
circulation
>To have a
continuous client’s
care
29

contribute to
hydrocephalu
s, cause the
brain to
herniate, and
restrict blood
supply to the
brain, leading
to an
ischemic
cascade. If
left untreated
the patient
may result to
coma or worst
death.
corticostreiods)
>Prepare pt. for
surgery as
indicated (Space
Occupying
Lesion)
>Refer
accordingly
Impaired skin integrity related to surgical incision 2˚ ventriculoperitoneal shunting
30
ASSESSMENTNURSING
DIAGNOSIS
SCIENTIFIC
EXPLANATIONOBJECTIVES
INTERVENTIO
NSRATIONALE
EXPECTED
OUTCOME
S: Ø
O: The
patient
manifests:
>Surgical
incision on
head
The patient
may
manifest:
>redness
>heat on
incision
>inflammator
y process
Impaired skin
integrity related to
surgical incision 2˚
ventriculoperitone
al shunting
Ventriculoperitone
al shunting is
surgery to relieve
increased pressure
inside the skull due
to excess
cerebrospinal fluid
(CSF) on the brain
(hydrocephalus).
The procedure is
done by shaving
the hair behind the
ear, then a surgical
cut in the shape of
a horseshoe (U-
shape) is made
behind the ear and
another small
surgical cut is
made in the child's
belly. A small hole
SHORT
TERM:
After 4
hours of
nursing
intervention
s, patient’s
SO will be
able to
understand
and
participate
in
prevention
measures
and
treatment
program for
the pt
>Establish
rapport
>Assess vital
signs
>Monitor
Intake
and output.
Weigh as
indicated.
Note
skin turgor,
status, and
mucous
membrane.
> Maintain
head or
>To gain
trust
>To obtain
baseline
data
>Useful
indicators of
body water,
which is an
integral part
of
tissue
perfusion.
> Turning
bed to
one side
compresses
SHORT
TERM:
The
patient’s SO
shall have
understand
and
participated
in
prevention
measures
and
treatment
program for
the pt.
LONG
TERM:
31

is drilled in the
skull and a
catheter is passed
into a ventricle of
the brain. Another
catheter is placed
under the skin
behind the ear and
moved down the
neck and chest,
and usually into
the abdominal
(peritoneal) cavity.
LONG TERM:
After 6 days
of nursing
intervention
s, the
patient will
be able to
achieve
timely
healing of
surgical
incision.
neck in
midline or
in neutral
position,
support
with small
towel
rolls and
pillows.
Avoid placing
head on large
pillows.
>Identify
underlying
condition
involved
>Periodically
assess skin
and observe
the jugular
veins and
inhibits
cerebral
venous
drainage
that
may cause
ONCREASE
D icp
>To
determine
cause of
impairment
>To
monitor
progress of
wound
healing
The patient
shall have
achieved
timely
healing of
surgical
incision.
32

for possible
complications
>Keep the
area
clean/dry,
perform
proper wound
care, support
incision
>Use
appropriate
barrier
dressings and
wound
coverings,
skin-
protective
agents for
open/draining
>To assist
body’s
natural
process of
repair
>To protect
the wound
and/or
surrounding
tissues
33

wounds and
stomas
>Encourage
to increase
oral fluid
intake
>Promote
importance of
proper
nutrition of pt
>To boost
immune
system and
enhance
skin turgor
>To boost
immune
system and
address
ongoing
nutritional
needs of
pt .For
tissue
repair to
achieve
timely
healing
>Promotes
34
> Elevate the
head
of bed
gradually
to 15-30
degrees
as tolerated or
indicated.
venous
drainage
from
head,
reducing
cerebral
congestion
and
edema and
increased
ICP.
35

CONCLUSION:
Ventriculoperitoneal shunting is surgery to relieve increased pressure inside
the skull due to excess cerebrospinal fluid (CSF) on the brain (hydrocephalus).
Hydrocephalus may start while the baby is growing in the womb. It is
commonly present with myelomeningocele, a birth defect involving incomplete
closure of the spinal column. Genetic defects and certain infections that occur
during pregnancy may also cause hydrocephalus. In hydrocephalus, there is a build-
up of fluid of the brain and spinal cord (cerebrospinal fluid or CSF). This build-up of
fluid causes higher than normal pressure on the brain. Too much pressure, or
pressure that is present too long, will damage the brain tissue
A shunt helps to drain the excess fluid and relieve the pressure in the brain. A
shunt should be placed as soon as hydrocephalus is diagnosed. The procedure is
done by shaving the hair behind the ear, then a surgical cut in the shape of a
horseshoe (U-shape) is made behind the ear and another small surgical cut is made
in the child's belly. A small hole is drilled in the skull and a catheter is passed into a
ventricle of the brain. Another catheter is placed under the skin behind the ear and
moved down the neck and chest, and usually into the abdominal (peritoneal) cavity.
Sometimes, it goes to the chest area. The doctor may make a small cut in the neck
to help position the catheter. A valve (fluid pump) is placed underneath the skin
behind the ear. This will be attached to both catheters. When extra pressure builds
up around the brain, these valve opens, and excess fluid drains out of it into the
belly or chest area which then helps in decreasing intracranial pressure.
Complications can occur. Some patients may experience blood clot or
bleeding in the brain, swelling and infection in the brain, brain tissue damage,
reoccurrence of fluid build up in the brain because the shunt may also stop working,
the shunt may also become infected and seizures may occur.
After the procedure the patient will need to lie flat for 24 hours the first time
a shunt placed then the patient will be helped to sit up. The usual stay in the
hospital is 3 to 4 days. Recording vital signs and neurological status often is
36

needed. The patient may be given medications for pain. Intravenous fluids and
antibiotics are given to maintain hydration and prevent the occurrence of infection.
The shunt will be checked regularly to make sure it is working properly.
37


















