Von willebrand disease
20
Von Willebrand Disease
-
Upload
iqra-yasin -
Category
Health & Medicine
-
view
106 -
download
0
Transcript of Von willebrand disease
Von Willebrand Disease
What is VWD?
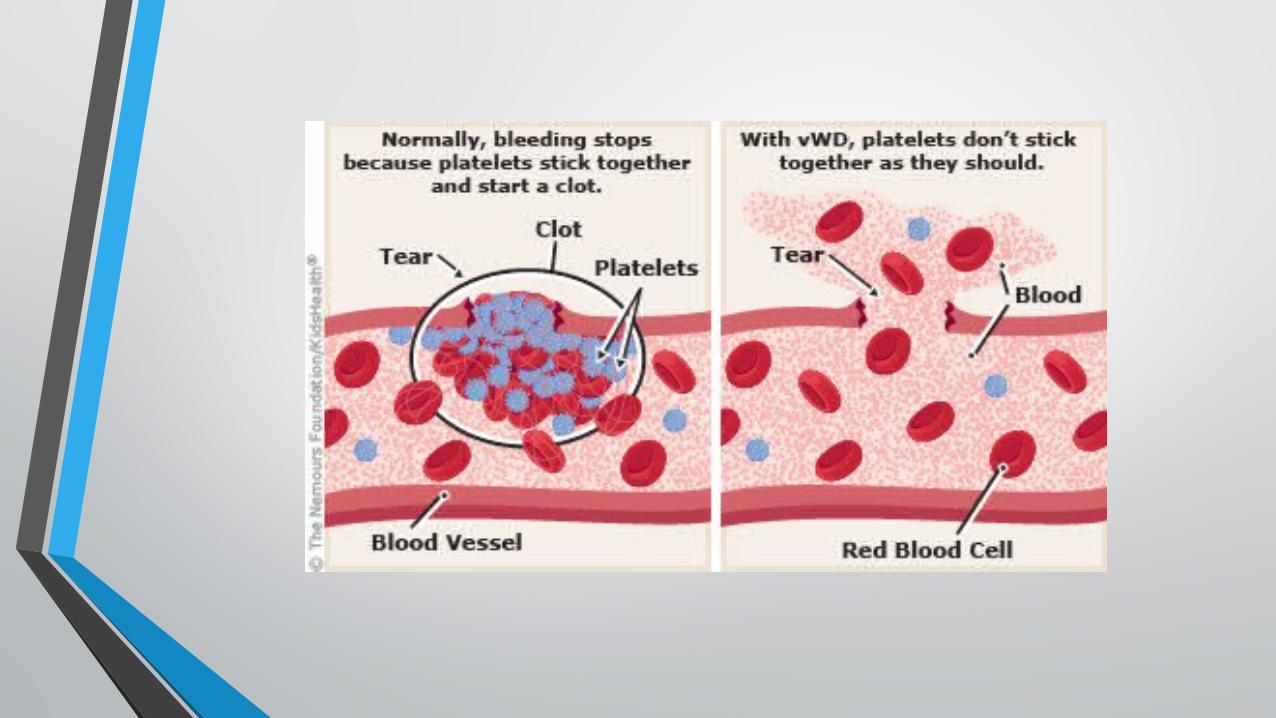
• Von Willebrand disease (VWD) is a genetic disorder caused by missing or defective Von Willebrand factor (VWF), a clotting protein. VWF binds factor VIII, a key clotting protein, and platelets in blood vessel walls, which help form a platelet plug during the clotting process.
• VWD is the most common bleeding disorder
• It is carried on chromosome 12 and occurs equally in men and women.
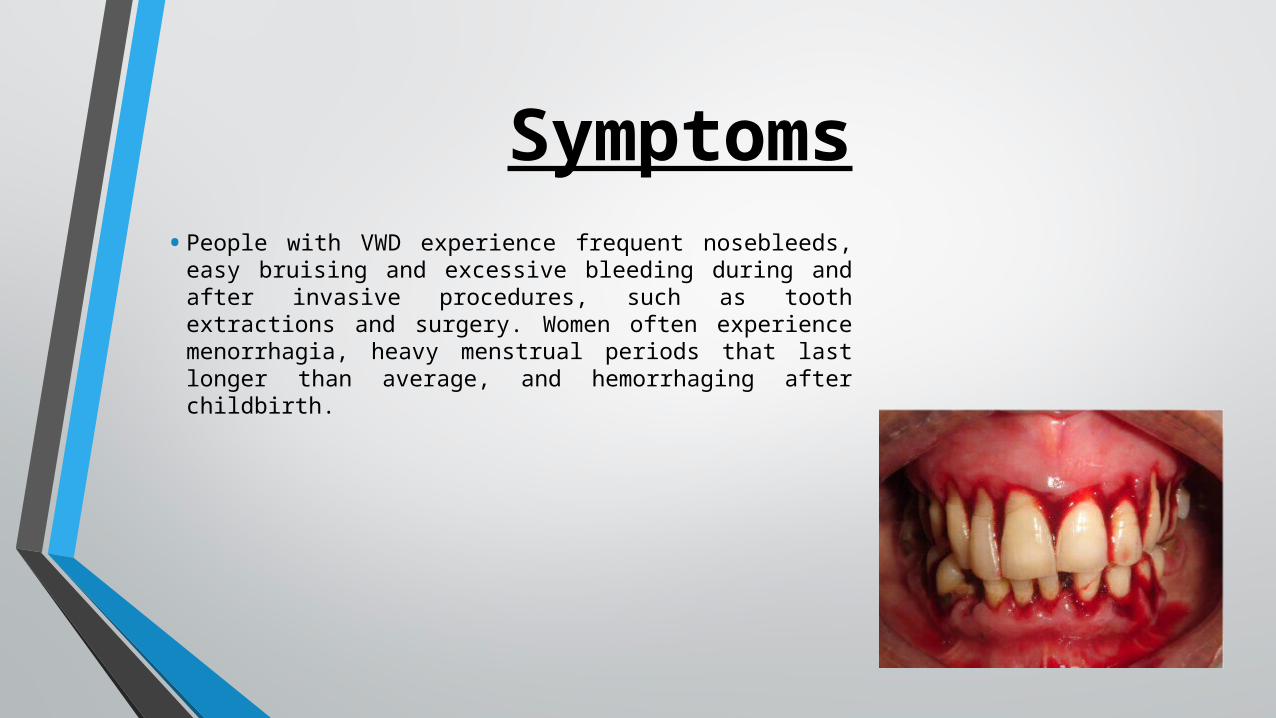
Symptoms• People with VWD experience frequent nosebleeds, easy
bruising and excessive bleeding during and after invasive procedures, such as tooth extractions and surgery. Women often experience menorrhagia, heavy menstrual periods that last longer than average, and hemorrhaging after childbirth.
Clinical Screening for an Underlying Disorder of Hemostasis in the Adult Patient With
Excessive Menstrual Bleeding*• Initial screening for an underlying disorder of hemostasis in patients with excessive menstrual bleeding
should be structured by the medical history. A positive screening result* comprises the following circumstances:
• Heavy menstrual bleeding since menarche
• One of the following conditions: Postpartum hemorrhage
Surgery-related bleeding
Bleeding associated with dental work
• Two or more of the following conditions: Epistaxis, one to two times per month
Frequent gum bleeding
Family history of bleeding symptoms
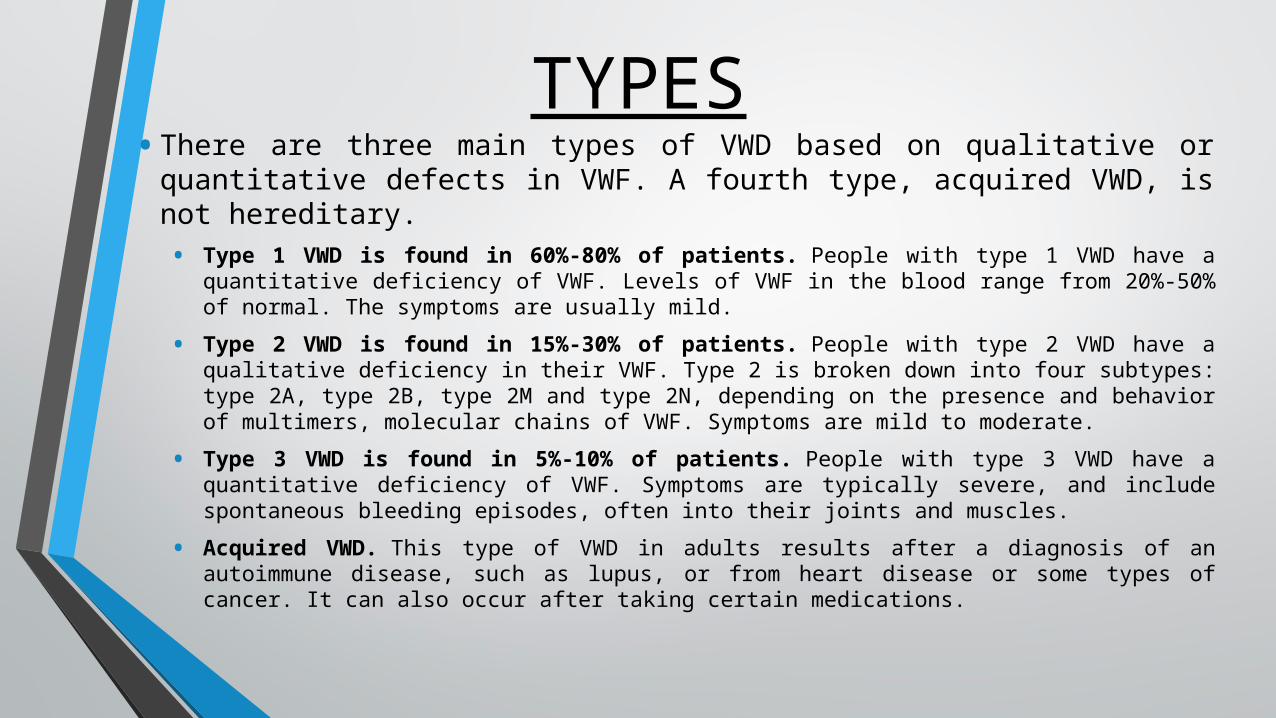
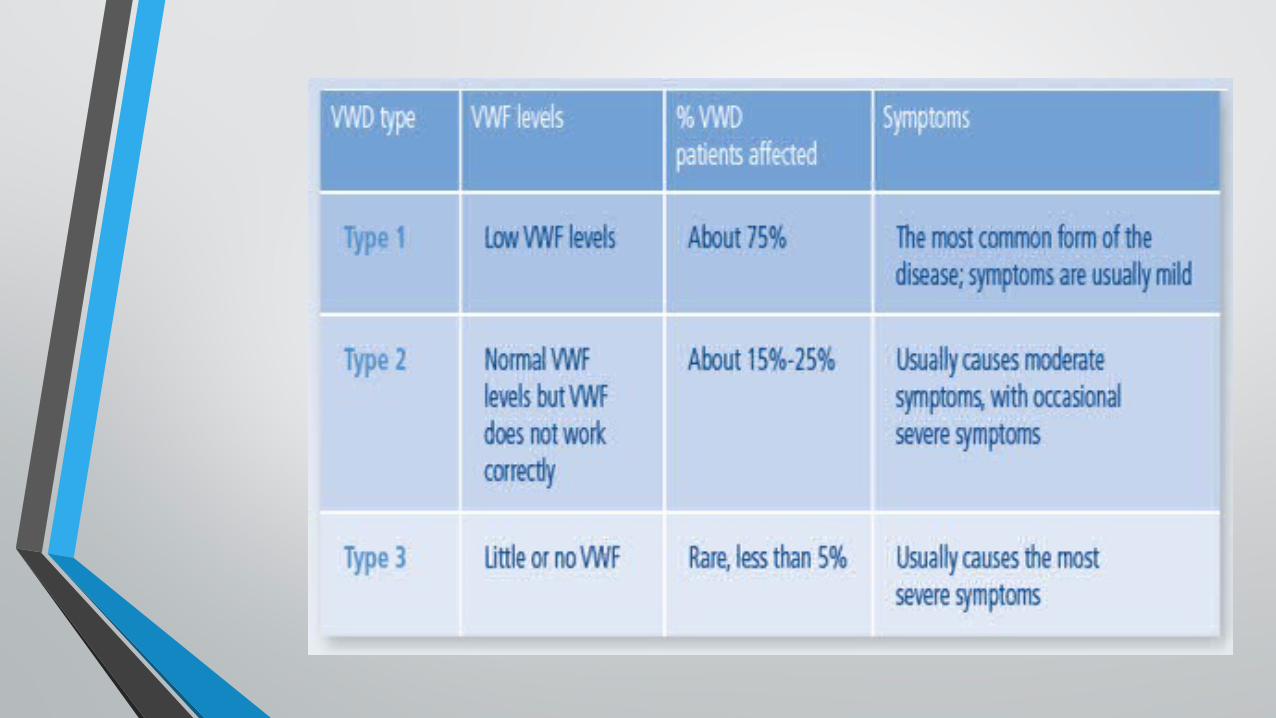
TYPES• There are three main types of VWD based on qualitative or
quantitative defects in VWF. A fourth type, acquired VWD, is not hereditary.• Type 1 VWD is found in 60%-80% of patients. People with type 1 VWD have a quantitative deficiency
of VWF. Levels of VWF in the blood range from 20%-50% of normal. The symptoms are usually mild.
• Type 2 VWD is found in 15%-30% of patients. People with type 2 VWD have a qualitative deficiency in their VWF. Type 2 is broken down into four subtypes: type 2A, type 2B, type 2M and type 2N, depending on the presence and behavior of multimers, molecular chains of VWF. Symptoms are mild to moderate.
• Type 3 VWD is found in 5%-10% of patients. People with type 3 VWD have a quantitative deficiency of VWF. Symptoms are typically severe, and include spontaneous bleeding episodes, often into their joints and muscles.
• Acquired VWD. This type of VWD in adults results after a diagnosis of an autoimmune disease, such as lupus, or from heart disease or some types of cancer. It can also occur after taking certain medications.
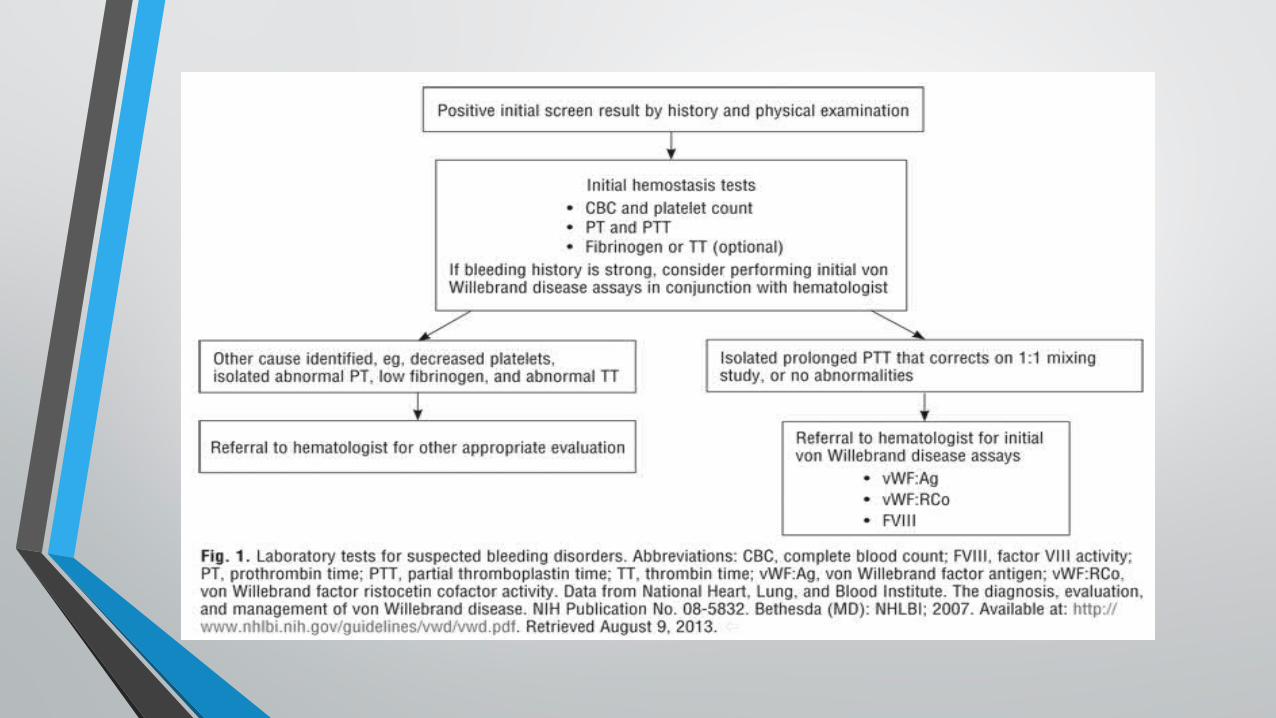

DIAGNOSIS• When VWD is suspected, blood plasma of a patient must be investigated for quantitative and
qualitative deficiencies of VWF. This is achieved by measuring the amount of VWF in a VWF antigen assay and the functionality of VWF with a glycoprotein (GP)Ib binding assay, a collagen binding assay, or a ristocetin cofactor activity (RiCof) or ristocetin induced platelet agglutination (RIPA) assays.
• Factor VIII levels are also performed because factor VIII is bound to VWF which protects the factor VIII from rapid breakdown within the blood. Deficiency of VWF can then lead to a reduction in factor VIII levels, which explains the elevation in PTT time. Normal levels do not exclude all forms of VWD, particularly type 2, which may only be revealed by investigating platelet interaction with subendothelium under flow, a highly specialized coagulation study not routinely performed in most medical laboratories. A platelet aggregation assay will show an abnormal response to ristocetin with normal responses to the other agonists used. A platelet function assay may give an abnormal collagen/adrenaline closure time, and in most cases, a normal collagen/ADP time. Type 2N may be considered if factor VIII levels are disproportionately low, but confirmation requires a "factor VIII binding" assay. Detection of VWD is complicated by VWF being an acute phase reactant with levels rising in infection, pregnancy, and stress.
• Other tests performed in any patient with bleeding problems are a complete blood count (especially platelet counts), activated partial thromboplastin time, prothrombin time, thrombin time, and fibrinogen level. Testing for factor IX may also be performed if hemophilia B is suspected. Other coagulation factor assays may be performed depending on the results of a coagulation screen. Patients with von Willebrand disease typically display a normal prothrombin time and a variable prolongation of partial thromboplastin time.
Gynecologic Considerations
• The association of von Willebrand disease with other gynecologic problems—including ovarian cysts, endometriosis, and leiomyoma—is uncertain. Heavy menstrual bleeding or hemorrhagic ovarian cysts may be managed with combined hormonal contraceptives, which can address both the bleeding and the development of hemorrhagic cysts. For the acute presentation of a ruptured ovarian cyst, patients with von Willebrand disease may require surgical intervention for hemostasis.
Hormonal Treatments• Levonorgestrel-releasing intrauterine system may be effective for this population. Use of
progestin-only contraceptives, such as medroxyprogesterone acetate; progestin-only pills; and the progestin implant, also may reduce menstrual flow in the setting of bleeding disorders.
• For women without bleeding disorders, use of combined oral contraceptives or the levonorgestrel-releasing intrauterine system reduce menstrual bleeding. Limited studies in women with von Willebrand disease and heavy menstrual bleeding suggest these treatments also may be effective for this population. Although oral progestins (taken for 21 days of the cycle) and depot medroxyprogesterone acetate are effective for women with heavy menstrual bleeding without bleeding disorders and may be effective for women with bleeding disorders as well.
Nonhormonal Treatments
• Nonhormonal treatment options include antifibrinolytic agents, such as tranexamic acid and ε-aminocaproic acid .Therapies generally prescribed in conjunction with a hematologist once a diagnosis of von Willebrand disease is established include desmopressin acetate, recombinant factor VIII, and VWF complex infusion. Desmopressin acetate is a synthetic derivative of the antidiuretic hormone vasopressin and works by stimulating the release of VWF from endothelial cells. Recombinant factor VIII and VWF complex infusion are plasma-derived concentrates used to replace factor VIII and VWF, respectively.
Obstetric Considerations
• Obstetric concerns regarding patients with bleeding disorders include spontaneous abortion, mode of delivery, epidural management, operative delivery techniques, and postpartum hemorrhage. Patients with an underlying bleeding disorder are at a high risk of epidural or spinal hematoma. Many experts advocate that women with von Willebrand disease may have a vaginal delivery safely, with cesarean delivery reserved for standard indications. Because von Willebrand disease can be transmitted as an autosomal dominant or recessive trait, the fetus can have up to a 50% risk of being affected. Procedures, such as fetal scalp electrode or fetal scalp sampling, are better avoided, and circumcision should be postponed until the newborn’s VWD status is determined. Operative vaginal deliveries, in which there may be an increased risk of trauma to the newborn, should be avoided because of the potential risk of intracranial hemorrhage.
Safety steps to take during pregnancy
• For prenatal care and delivery, consider using a medical center that specializes in high-risk obstetrics and has a hematologist on staff.
• preventing serious blood loss before any invasive procedure, such as amniocentesis.• During third trimester,blood tests to measure von Willebrand factor and factor VIII again to
help plan for delivery.• anesthesiologist consultation before delivery to review choices for anesthesia and to discuss
taking medicine to reduce bleeding risk.• Consultation with pediatric hematologist regarding the evaluation of the baby after delivery. If
there is boy and plan for circumcision, consider waiting until he has been tested and it is deemed safe to perform the procedure.
Treatment
• Treatment for VWD depends on the diagnosis and severity. The mainstay of treatment is DDAVP (desmopressin acetate), the synthetic version of a natural hormone vasopressin,. It stimulates the release of VWF from cells, which also increases FVIII.DDAVP comes in two forms: injectable and nasal spray. Because DDAVP is an antidiuretic, causing the body to retain water, fluid restrictions are important so patients don’t develop hyponatremia, reduced sodium in the bloodstream.
• There are a few clotting factor concentrates that are rich in VWF, and are recommended for patients with VWD. These therapies are given by intravenous infusion.