Larry R. Squire- The History of Neuroscience in Autobiography: Volume 1

Progressive NeuroscienceA publication for physicians produced by the Institute for Neurosciencesat Winthrop-University Hospital
Volume 8 No. 1 l Fall 2015
• Effects of Dust from the World TradeCenter on Peripheral Nerves
• Minimally Invasive Total Stereotactic Resection of GiantIntraventricular Meningioma
• Resection of Lumbar Giant Cell Tumor

To Our Colleagues:Attacking the essence of a person, neurological diseases often cause life-altering transformations in the
lives of patients and their families. However, given the epic upsurge in our knowledge of the nervous
system — coupled with the development of revolutionary technology, progressive techniques and
ground-breaking treatments — we are responding to the challenge of caring for these patients with
increasingly impressive results.
In this issue of Progressive Neuroscience, we focus on some notable patient outcomes directly related
to the use of sophisticated technologies and treatments, including:
• Minimally invasive total stereotactic resection of a giant intraventricular meningioma
• Image-guided spine surgery
• Resection of a lumbar giant cell tumor and reconstruction that obviated the need
for adjuvant therapy
• State-of-the-science monitoring of cardiac output and fluid management in the NeuroICU
In addition, we highlight important research currently underway at Winthrop-University Hospital’s
Institute for Neurosciences. Neurology and environmental medicine experts are collaborating in an
exciting study to expand our understanding of the effects of dust from the World Trade Center disaster
on peripheral nerves.
Our objective continues to be to provide the most advanced, collaborative and world-class care for
your patients.
Mark M. Stecker, MD, PhD Michael H. Brisman, MDChairman Chief Department of Neuroscience Division of Neurosurgery
Co-Director Institute for Neurosciences
Michael H. Brisman, MDMark M. Stecker, MD, PhD

Table of Contents
Progressive Neuroscience l Fall 2015 l 1
Winthrop-UniversityHospital’s Institute forNeurosciences specializes in the latest and most effective neurological procedures for:
• Acoustic Neuroma• Astrocytoma• Arteriovenous Malformation
of Brain & Spine • Back Pain• Brain Aneurysms• Brain & Spinal Traumas • Brain Tumors• Carotid Stenosis• Cerebral Aneurysms • Cerebrovascular &
Endovascular Diseases• Chiari Malformation • Chronic Pain • Degenerative Scoliosis • Epilepsy• Facial Pain • Glioblastoma• Hemifacial Spasm• Herniated Discs• Hydrocephalus• Intracranial Atherosclerotic
Disease • Intracranial Hemorrhage• Memory Disorders• Meningiomas• Metastatic Tumors• Movement Disorders• Moyamoya Disease• Multiple Sclerosis• Neck Pain• Neurological Cancers• Neuromuscular Diseases• Normal Pressure
Hydrocephalus• Ossification of Posterior
Longitudinal Ligament• Parkinson’s Disease • Pediatric Neurological
Conditions • Peripheral Nerve Disorders• Phantom Limb Pain• Pinched Nerve• Pituitary Adenoma• Post Herpetic Neuralgia • Sciatica• Seizure Disorder • Spasticity• Spina Bifida• Spinal Cord Injury • Spinal Stenosis • Spine Fractures • Spine Tumors • Stroke• Subarachnoid Hemorrhage• Subdural Hematoma • Syringomyelia• Trigeminal Neuralgia
Progressive Neuroscience is produced by the Institute for Neurosciences at Winthrop-University Hospital, 259 First St., Mineola, NY 11501, 516-663-0333, www.winthrop.org.
Charles M. StrainChairman of the Board
John F. CollinsPresident & CEO
Mark M. Stecker, MDChairman, Neuroscience
Michael H. Brisman, MDChief, Neurosurgery
Co-Director, Institute for Neurosciences
Phyllis AbramsWriter/Editor
Charles WalshGraphic Designer
Solomon A. Torres Vice President, Administration
J. Edmund KeatingVice President
Marketing & Advertising
ResearchEffects of Dust from World Trade Center Disaster on Peripheral Nerves l 2
Minimally invasive Total Stereotactic Resection of a Giant Intraventricular Meningioma l 4
Case ReportResection of Lumbar Giant Cell Tumor l 6
Image-Guided Spine SurgeryRevolutionizes Visualization l 8
State-of-the-Science Cardiac Output Monitoring and Fluid Management in the NeuroICU l 10
Contributing Clinicians l 12

The World Trade Center (WTC) disaster of 9/11/2001 was associated with anumber of health problems for those exposed.1-3 Although research is beingconducted to understand the full extent of these problems, the National
Institute of Occupational Safety and Health (NIOSH) includes asthma, chroniclaryngitis, chronic respiratory disorder, interstitial lung diseases, reactive airwaydisease, sleep apnea, upper airway hyper-reactivity, and WTC-exacerbated chronicobstructive pulmonary disease among the conditions linked to the catastrophe.Major depression, post-traumatic stress disorder (PTSD) and generalized anxietydisorder are also included.
The chemical compounds present in the dust produced by the WTC disaster arecontributors to these medical disorders. Paul Lioy, PhD, an eminent environmentalscientist and Vice Chair of the Department of Environmental Medicine UMDNJ -Robert Wood Johnson Medical School, demonstrated that the dust contained manyvery complex hydrocarbons and hexacarbons that may be neurotoxic, as well aslead and arsenic, which certainly are.4
ByMark M. Stecker, MD, PhDChairman, Neuroscience
Marc Wilkenfeld, MDChief, Occupational &Environmental Medicine
Winthrop-University Hospital
2
Effects of Dust from the World Trade Center on Peripheral Nerves
Research

We are still learning about the fulleffects of the WTC disaster on thoseexposed. Since some WTC respondersand survivors have experienced neuro-pathic symptoms, we have undertakena study of the effect of WTC site dust
on peripheral nerves, using the invitrosciatic nerve preparation. The dust wasobtained from Dr. Lioy.4
Method
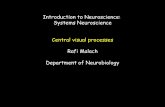
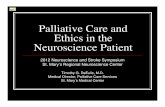
In the invitro sciatic nerve model,5
(Fig.1) sciatic nerves from a rat are har-vested and then placed in a perfusionapparatus, where the solution bathingthe nerve can be well controlled. Inthese experiments, the temperature ofthe perfusate is maintained at bodytemperature (37°C) and consists of asalt solution similar to that of the cere-brospinal fluid.
Each experiment lasts 16 hours, duringwhich the nerve action potential (NAP)is recorded every four seconds. Fromeach nerve action, we determine itsamplitude, velocity, duration andresponse to paired pulses (conditionedstimulus response-CSR). Normally,during the course of the experiment,the amplitude of the NAP drops slight-ly, as does the velocity.
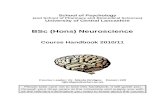
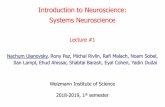
We have been able to compare theeffects of WTC dust on peripheralnerves under two conditions: First,
1gm of dust was extracted with salineand injected into the fluid bathing thenerve. Second, 10gms of dust wereextracted with methanol and injectedinto the bathing fluid. Infusion of 1gmof dust extract had no effect. However,
the nerve exposed to10gms of dust extractedwith methanol demon-strated reduced conduc-tion velocity in compari-son to nerves exposedto the same amount ofmethanol without dust.(Fig.2)
It has been shown thatWTC dust containstoxic substances thathave caused disease inthose exposed. The dustmay have a direct toxiceffect on myelin.However, it is difficultto apply these datadirectly to determinewhether WTC dust may
produce neuropathy in humans.
First, this an acute model, and inhumans it is more likely that damagedue to lower levels accumulates overtime. Second, although the conductionstudies performed in the invitro sciaticnerve system are similar to those pro-duced in humans for the assessment of neuropathy, these studies are not
associated with any assessment ofphysiological changes. Thus, althoughmore physiologic measurements areindicated, and may be helpful in identi-fying the nature of the toxic substance,it is important to assess humans who were exposed.
For more information, call the Institutefor Neurosciences at 1-866-WINTHROPor visit www.winthrop.org
REFERENCES1. Solan S, Wallenstein S, Shapiro M, et al. Cancer
incidence in world trade center rescue andrecovery workers, 2001-2008.EnvironHealthPerspect 2013Jun;121(6):699-704.PMCID: PMC3672914.
2. Jordan HT, Brackbill RM, Cone JE, et al.Mortality among survivors of the sept 11, 2001,world trade center disaster: results from theworld trade center health registry cohort.Lancet 2011Sep 3;378(9794):879-887.
3. Liu B, Tarigan LH, Bromet EJ, et al. World tradecenter disaster exposure-related probable post-traumatic stress disorder among respondersand civilians: a meta-analysis. PLoS One2014Jul 21;9(7):e101491. PMCID: PMC4105417.
4. Lioy PJ, Weisel CP, Millette JR, et al.Characterization of the dust/smoke aerosol thatsettled east of the world trade center (WTC) inlower manhattan after the collapse of the WTC11 september 2001. Environ Health Perspect.2002Jul;110(7):703-714. PMCID: PMC1240917.
5. Stecker MM, Stevenson M. Anoxia inducedchanges in optimal substrate for peripheralnerve. Neuroscience 2015;284:653-657.
6. Stecker M, Segelnick J, Wilkenfeld M. Analysisof short-term effects of world trade center duston rat sciatic nerve. JOccupEnvironMed2014Oct;56(10):1024-1028.
Progressive Neuroscience l Fall 2015 l 3
Oxygen Computer
Constant CurrentStimulator
Perfusate(Saline)
RecyclingPump
Amplifier
Nerve
Stimulus Artifact
NAP = Nerve Action PotentialCSR = Amp2/Amp 1Velocity = Distance/Latency Voltage
NAP1 NAP2
Latency
Time
Amp1 Amp2} }
Effect of WTC Dust on Nerve Conduction Velocity1.05
1.00
0.95
0.90
0.85
0.80
0.75
Nor
mal
Vel
ocity
Time (From Onset of Experiment-Hours)1-2.5 4-5.5 7-8.5 10-11.5 13-14.5
WTC DustNo Dust
Fig. 2
Fig. 1

Awoman in her 60s presented with gaitinstability and a history of memorydisturbance. She was neurologically
nonfocal, and after ruling out the possibilityof a middle ear problem, a diagnosticMRI/MRA of the brain was performed. Itrevealed the existence of multiple menin-giomas, including one very large intraventic-ular mass filling the lateral ventricle, withdownward displacement of the deep andinternal cerebral veins. In addition toobstructive hydrocephalus, which was causing her symptoms, there was evidence ofincreased vascularity fed mostly by the pos-terior choroidal artery (PCA) branches andconsistent with a diagnosis of meningioma.
To keep intracranial pressure from increas-ing and to treat the hydrocephalus, surgerywas recommended. The goal was to preventfurther neurologic deterioration and help thepatient recover neurologic function.
Incidence, Symptoms, Diagnosis
Intraventricular meningiomas are slowgrowing, benign tumors that generallydevelop into large masses prior to detection.Considered rare, they account for 0.5%-5%
of all intracranial meningiomas, generallypresenting in the fourth-to-sixth decades oflife, and occurring twice as often in womenthan men.1,2
Since the brain’s ventricles provide spacefor expansion, patients are usually asympto-matic until the mass grows large enough to
cause compression of the adjacent neuralstructures or hydrocephalus increasesintracranial pressure. Symptoms mayinclude headache, imbalance, visual disturbances, memory difficulties, languagefunction impairment, seizures and mood orpersonality changes.
Minimally Invasive Total Stereotactic Resection ofa Giant Intraventricular Meningioma
Interview with Jonathan L. Brisman, MDDirector, Cerebrovascular &Endovascular Neurosurgery
Michael H. Brisman, MDChief, Neurosurgery
Winthrop-University Hospital
4
“Intraventricular surgery is high risk and involves meticulous navigationaround the critical thalamostriate veinand the fornices.”
Michael Brisman, MD Chief, Neurosurgery
Post-contrast coronal MRI preoperative, showing large intraventicular menimgioma
Post-contrast axial MRI preoperative showing large intraventricular meningioma.

Depending on the patient’s age, specific tumor site and radiologicalcharacteristics, deep-seated masses inthe ventricles can have significant differential diagnoses, including low-grade gliomas, astrocytomas,metastases and lymphoma, as well assarcoidosis, arteriovenous malforma-tions and cavernous hemangiomas.
“Accurate diagnosis is crucial so thesurgeon is aware of the type of tumorand its possible complications,”explained Jonathan Brisman, MD,Winthrop’s Director of Cerebrovascularand Endovascular Neurosurgery. Withdual training in microneurosurgery andendovascular techniques, he performedthe digital subtraction diagnosticangiography to evaluate the vascularityof the tumor.
Treatment
Excising a large intraventricular menin-gioma burrowed into the middle of the brain requires a complex and chal-lenging surgical procedure. It involvespassing through essential and eloquentcortical areas with minimal manipula-tion of the neural structures encirclingthe ventricles. Retraction must be mini-mized, functional cortical areas avoidedand feeder vessels controlled early.
Dr. Jonathan Brisman collaborated withWinthrop’s Chief of Neurosurgery,Michael Brisman, MD, in this carefullyplanned effort. Several surgicalapproaches to meningiomas of the
lateral ventricle have been developed inorder to reduce the risk to vital neuro-logical structures and the potential forcreating speech and cognitive deficits.They elected to use a transcorticalapproach, considered least invasive and most direct.
“Intraventricular surgery is high riskand involves meticulous navigationaround the critical thalamostriate veinand the fornices,” explained Dr. MichaelBrisman. “Tumors located in the lateralventricle are more easily accessedthrough a cortical incision. The tech-nique also provides superior workingspace and flexibility.”
In this case, MRI images helped guidethe proposed corticectomy tract fortumor excision. To obviate the need formultiple retractors, obtain safe access tothe deeply embedded tumor and reduce
the risk of retraction-related complica-tions, they used a recently developedtransparent plastic tubular retractor. Thecompletely clear cylindrical device pro-vided excellent visualization — as it wascarefully guided toward the lesion —and facilitated the evacuation of themeningioma, which was completelyremoved through the retractor’s lumenwithout placing extra pressure on thebrain tissue.
“After the rim of the tumor was coagu-lated, we debulked the mass, rolling itonto itself and ultimately achievinggross total resection,” Dr. MichaelBrisman reported. “The patient returnedhome after several days of hospitaliza-tion and remains symptom-free withoutneurological deficits.”
For more information, call the Institutefor Neurosciences at 1-866-WINTHROPor visit www.winthrop.org
REFERENCES1. Erman T, Gocer AL. Erdogen E, et al.
Intraventricular meningiomas: a review andreport of eight cases. NeurosurgQuartly2004;14:154-160.
2. Koeller KK, Sandberg GD. From the archives ofthe AFIP. Cerebral intraventricular neoplasms:radiologic-pathologic correlation. Radiographics22(6)1475-1505. doi:10.1148/rg.226025118.
Progressive Neuroscience l Fall 2015 l 5
Post-contrast axial MRI postoperativeshowing complete removal of tumor
Post-contrast sagittal MRI postoperativeshowing complete removal of tumor
Post-contrast coronal MRI postoperativeshowing complete removal of tumor

After failing all means of conservativetreatment for back pain, a man inhis 40s presented with intractable,
worsening pain that traveled from his righthip and buttock down the posterolateralaspect of his right leg to the foot. The leftlower and upper extremities were normal.
He complained of difficulty walking andepisodes of right lower extremity paralysis,as well as being unable to function inde-pendently because of the pain and neuro-logical problems.
An MRI of the lumbar spine showed a lyticlesion consuming the body of L4 withextradural extension and compression ofthe thecal sac. The remaining L4 vertebralbody had deteriorated to nothing more thanan “egg shell.”
A needle biopsy confirmed that the lesionwas a benign giant cell tumor (GCT) thatneeded to be excised in order to address thepatient’s neurological deficits and spinalinstability.
Angiogram & Embolization
Given the vascular nature of most GCTs, apreoperative angiogram was conducted,revealing a hypervascular mass at L4.Embolization was performed to reduce thetumor’s vascularity and the potential forextensive blood loss during surgery. Usingthe right transfemoral approach, a catheter
6
By Benjamin R. Cohen, MDNeurosurgeonWinthrop-University Hospital
Resection ofLumbar Giant Cell Tumor
The surgery consisted of an intricatetwo-stage procedure conducted overtwo days.
Case Report
Pre-op sagittal and axial MRI with gadolinium showing mass in the L4 vertbral body, epidural extension and thecal sac compression
Postoperativeangiogram showingvasularity of L4 tumor

was placed in the L4 lumbar artery,where a small amount of polyvinyl alco-hol (PVA) glue was instilled to achievedevascularization of the tumor.
Resection & Stabilization
The surgery consisted of an intricatetwo-stage procedure conducted overtwo days. Stage one involved a com-plete posterior laminectomy from thebottom of L3 to the top of L5, with sta-bilization and fusion. The procedureresulted in the removal of a good por-tion of the L4 vertebral body, a widesurgical resection of the tumor anddecompression of the nerves.
Stage two involved an anterior corpectomy at L4 for resection of theremaining tumor with reconstructionusing an expandable cage. Near-complete resection of the tumor wascompleted. Since the lesion was con-tained in one area and near total resec-tion was achieved, adjuvant therapywas not recommended.
Two weeks postoperatively, the patientreported significant improvement of hissymptoms, with the preoperative rightlower extremity pain, weakness anddysfunction completely resolved.
To help determine this patient’s futurecare and ensure timely treatmentshould the GCT recur, postoperativemonitoring will involve regular exami-
nations with interval X-rays, CT scansand MRI studies.
For more information call the Institutefor Neurosciences at 1-866NEURO-RXor visit www.winthrop.org.
REFERENCES1. Mendenhall WM, Zlotecki RA, Scarborough
MT, et al. Giant cell tumor of bone. AJCOnc2006;29:96-99.
2. Abbas AK, Kumar V, Fausto N, et al. Robbinsand Cotran Pathologic Basis of Disease,Professional Edition E-Book, W.B. SaundersCo. 2010 ISBN:1437721826.
3. Turcotte RE. Giant cell tumor of bone.OrthoClinNorthAm 2006;37:35-51.
4. Martin C, McCarthy EF. Giant cell tumor of thesacrum and spine:series of 23 cases and areview of the literature. IowaOrthoJ2006;30:69-75.
Giant cell tumors (GCT) of the spine are uncommon, accounting for approximately2%-4% of bone neoplasms.1 While technically benign, these lesions can be aggressive, resulting from over-proliferation of osteoclasts.
With a high rate of recurrence,2 GCTs are typically seen in men and women betweenages 20-45. Most patients present with debilitating back pain. However, the conditionis usually diagnosed after development of a neurological deficit caused by the tumor’scompression of the spinal cord or nerve roots at the site of involvement.
Given the complicated structure of the spine, diagnosis can be challenging, requiringthe exclusion of degenerative disease, infections, muscular strains and neurologicimpingements. In addition to pain, symptoms can range from slight weakness or anabnormal reflex to complete paraplegia, as well as bladder and bowel incontinence.
MRI imaging studies are critical to pinpointing the tumor’s size, location, local extension and extent of neurological compression. For histological confirmation —and to exclude the leading differential diagnosis of aneurysmal bone cyst — a CT-guided needle biopsy is necessary.
While management of long bone GCTs usually involves curettage and filling thedefect with bone cement,3 the treatment of choice for spinal GCTs is complex surgery,requiring careful preoperative planning and a multidisciplinary approach. The proce-dure — en bloc resection — offers the greatest chance for a cure.4 The role of adju-vant chemotherapy and/or radiation is controversial.
Since tumors in this region frequently do not present until the mass has grown verylarge, surgery carries the potential for mechanical and neurological complications.Moreover, GCTs can be hypervascular, often mandating preoperative arterialembolization to reduce the potential for hemorrhaging during surgery.
Ongoing multidisciplinary follow-up care — with routine X-rays and MRI studies — iscrucial to monitoring for recurrence.
Progressive Neuroscience l Fall 2015 l 7
Postoperative AP and lateral X-rays showing removal of the L4 vertebrae and posterior elements with reconstruction using an anterior “expandable” cage and posterior pedicle screws

8
Viewing the intricate, multifaceted anatomy of the spine during surgery has always been challenging. However, with the development of microsurgery, advanced imaging
technology and — most recently — image-guided spine surgery, visualization of the complexstructure has reached new heights.
Now, instead being restricted to traditionalinvasive spine surgery — where only the partof the anatomy that is exposed can be seen —spine surgeons have more treatment optionsto offer select patients. Because they canobtain a full view of the spine with the newvisualization technology, they can perform lessinvasive, safer surgery percutaneously,through small incisions.
A 70-year-old man with a history of laminectomy using instrumentation and fusion, was expe-riencing uncontrollable back and leg pain that was worsening steadily and preventing himfrom walking or standing for more than 30 seconds.
Artem Vaynman, MD, a Board-Certified neurosurgeon, recently employed image-guidedsurgery to treat this patient, who was diagnosed with postlaminectomy syndrome at L3-L4 and L4-L5. He also had residual stenosis at that site and developmental stenosis at
Interview with Artem Y. Vaynman, MDNeurosurgeonWinthrop-University Hospital
Because they can obtain a full view of the spine with the new visualizationtechnology, they can perform lessinvasive, safer surgery percutaneously,through small incisions.
Image-Guided Spine SurgeryRevolutionizes Visualization
Cage navigation
Probe postion

L2-L3, as well as bilateral radiculopathyand instability.
“After his first surgery at another insti-tution seven years earlier, the patientnever improved,” reported Dr.Vaynman, who specializes in complexand minimally invasive spine surgery,“When he presented recently, he was insevere pain, had great difficulty walking,and his symptoms were growing pro-gressively worse, reducing his inde-pendence substantially.”
Revision spinal surgery carries addi-tional risks, including poor healing,increased incidence of wound infectionsand cerebrospinal fluid leaks. Since thispatient needed decompression of hisnerve roots, fusion would be necessaryto re-establish spinal alignment and sta-bility. This made him an ideal candidatefor a combination of minimally invasiveand open surgery.
Dr. Vaynman recommended a complextwo-stage surgical procedure: Stage oneconsisted of a minimally invasiveanterolateral diskectomy with interbodyfusion from L2-L3 and L3-L4. The sec-ond stage comprised revision of the L3-L4 and L4-L5 laminectomy, and an L2-L3laminectory with bilateral facetectomyand foraminotomy, as well as L4-L5diskectomy with interbody fusion.
Image-guided technology includes aninfrared navigation camera that tracksthe movement and position of Smartinstruments with LEDs in the surgicalfield. However, at its core is specializedcomputer software that correlates pre-operative CT scans with intraoperativeanatomy, providing the surgeon withreal-time guidance during the operationwhen visibility with the human eye isproblematic.
First, the patient’s CT scan was down-loaded into the surgical navigationcomputer, which converted the 2-Dimages into a virtual 3-D model of his unique spinal anatomy. Then, onthe day of the surgery, he was fittedwith a special probe carrying theLEDs. A camera, hooked to thecomputer, tracked the LEDs as Dr. Vaynman moved.
During the operation, image registration matched pre-definedpoints on the computer model tothe patient’s real-time anatomy, creating a digital road map of thespine, and enabling Dr. Vaynman toavoid potential damage to surroundingtissue and structures. The surgery wassuccessful and the recovery uneventful.Two days postoperatively, the patienthad only incisional pain, which wascontrolled with small doses of pain
medication. He no longer felt the pre-operative pain and was walking with-out difficulty.
“In the past, such complicated proce-dures were extraordinarily long andwould necessitate taking multiple X-rayimages to guide us and verify the loca-tion of instruments, placement ofimplants and alignment,” Dr. Vaynmanexplained. “Today, we can work withunprecedented precision, safety andaccuracy without exposure to radiationor the need for open surgery.Additionally, in spinal fusion, image-guided surgery helps us plan the posi-tion, length and diameter of the pediclescrews, and then plant instrumentsexactly as planned.”
Image-guided surgery not onlyenhances visibility, reduces use of radia-tion in the OR and shortens the lengthof the procedure, it also allows for aspeedier recovery, and provides imme-diate quality control, as well as the abili-ty to check progress before concludingthe operation.
For more information, call the Institutefor Neurosciences at 1-866-WINTHROPor visit www.winthrop.org
Progressive Neuroscience l Fall 2015 l 9
Final fluoro
Probe position

Besides treating the underlying disease,critical care specialists focus on opti-mizing brain perfusion and fluid man-
agement. It has been demonstrated that suf-ficient brain perfusion, which secures oxy-gen delivery to the cells of the body, decreas-es morbidity and mortality.1
“Oxygen delivery is a blood-flow issue vital to the well-being of NeuroICU patients,and effective fluid management is crucial,”said Elzbieta Wirkowski, MD, MedicalDirector of Winthrop’s NeuroICU andDirector of the Cerebrovascular Disordersand Stroke Program.
In fact, the literature suggests that accuratemeasurement of fluid status and subsequentappropriate treatment remain unmet needsin neurological intensive care units, sinceonly 50% of all hemodynamically unstablepatients are considered fluid responsive.2
“Our goal is to optimize cardiac output byincreasing the amount of fluid or by increas-ing blood pressure or heart rate. Properassessment of fluid responsiveness canimprove prognosis and prevent complica-tions of fluid overload,” Dr. Wirkowskiexplained.
Traditionally, hemodynamic assessmentshave relied heavily on blood pressure andECG measurements. For decades, the use of
10
State-of-the-Science Cardiac Output Monitoringand Fluid Management in the NeuroICU
Interview withElzbieta Wirkowski, MDCo-Director, Neuroscience ICUDirector, CerebrovascularDisorders & Stroke ProgramWinthrop-University Hospital
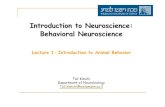
Winthrop’s NeuroICU utilizes NICOM, acompletely noninvasive novel techniqueto establish objective parameters thatdetermine fluid responsiveness.
An 85-year-old woman with a medical history of atrial fibrillation, hypertension, hypercholes-terolemia, anxiety and arthritis presented with right-sided weakness and difficulty speaking.She was admitted to Winthrop-University Hospital’s Neuroscience Intensive Care Unit(NeuroICU) to rule out a cerebrovascular accident and seizures. While hospitalized, thepatient grew progressively delirious with increased tachypnea. A chest X-ray and oxygenationwere normal. Over time, her urine output and blood pressure decreased. She was not intubated and had no central line. However, hemodynamic monitoring was indicated, and noninvasive cardiac output measurement (NICOM) was instituted in order to monitor cardiacoutput and fluid-requirement status.
Fig. 1

invasive intravascular catheters (Swann-Ganz) has been the monitoring methodof choice for accurate evaluation ofhemodynamic status. However, while itprovides essential real-time data, thepractice carries significant risk, andbenefits in patient outcomes have notbeen reported.
Winthrop’s NeuroICU utilizes NICOM —a completely noninvasive novel tech-nique — to establish objective parame-ters that determine fluid responsiveness.(Fig. 1) The technology, which providesan immediate and continuous flow ofinformation, is based upon the fact thatthe electrical impedance of the chestvaries with the amount of blood present.Thus, when an alternating current isapplied to the chest, the resulting volt-age changes with the pulsatile bloodflow in the large thoracic arteries.
The data are delivered to a computer foranalysis, storage and future recall.“We’ve long known that the cardiovas-cular system forms a new dynamic forevery heartbeat,” said Dr. Wirkowski.“Therefore, hemodynamically significantblood flow is not cardiac output flowper minute, but rather an indexed bloodflow per beat.”
Monitoring cardiac output with NICOMbegins with the placement of four dualsensors on the outside of the patient’schest or back, with two sensors posi-tioned above and two below the heart.(Fig. 2) An electric current of known frequency is applied across the thoraxbetween the outer pair of electrodes.Then, a signal is recorded between theinner pairs of the sensors.
The change in phase of the voltage andcurrent waveforms is analyzed with thehelp of a highly sensitive phase detectorthat can sense tiny phase shifts pro-duced by changes in impedance, which
are closely correlated with aortic bloodvolume. The signal is translated intoflow. Ventricular outflow drives changesin the phase shift of radiofrequencywaves as they cross the chest, and
measuring the difference in phasebetween the current and voltage wave-forms enables the calculation of bloodflow. “With the ECG leads built into themedical censors, we can detect heartrate and measure cardiac output,” Dr.Wirkowski said.
NICOM permits users to obtain a hemo-dynamic profile for differential diagnosisand baseline assessment. If oxygen
perfusion needs to be improved, thetechnology first assesses fluid status. Iffluid is optimized, but oxygen perfusionremains inadequate, the available dataguide the practitioner to the next step intreatment, which could be drug inter-
vention to increase contractility of theheart or reduce afterload. Continuedmonitoring with NICOM also quicklyassesses the intervention’s effectiveness.In addition to fluid management and
optimization of oxygen delivery, NICOMcan also help reduce over or underresuscitation, prevent unnecessary intubations or delayed extubations, andavoid unwarranted fluid removal orfluid overload.
“Our data show that NICOM is safe anduseful in cases of intubated patients with sepsis, hypotension, hypertensivetherapy in subarachnoid hemorrhage orduring hypothermia therapy,” reportedDr. Wirkowski. “It is also useful in non-intubated and alert patients where fluidstatus must be monitored closely.”
For more information, call the Institutefor Neurosciences at 1-866-WINTHROPor visit www.winthrop.org
REFERENCES1. Bland RD, Shoemaker WS. Probability of sur-
vival as a prognostic and severity of illness scorein critically ill surgical patients. CritCareMed1985. 13:2.
2. Michard F, Teboul JL. Predicting fluid respon-siveness in ICU patients. Chest 2002;121:2000-2008.
Progressive Neuroscience l Fall 2015 l 11
Ideal Hemodynamic Monitoring
• Provides Relevant & Accurate Data• Delivers Reproducible &
Interpretable Data• Is Easy to Use• Is Noninvasive• Can Guide Therapy
Hemodynamic Data Captured Noninvasively
• Stroke Volume • Stroke Volume Variation• Thoracic Fluid Content • Total Peripheral Resistance • Ventricular Ejection Time• Cardiac Index
Fig. 2

12
Mark M. Stecker, MD, PhD Chairman, Department of Neuroscience516.663.4852
Dr. Mark Stecker isBoard Certified by theAmerican Board ofPsychiatry andNeurology in Neurologyand Clinical Neuro-physiology, as well asby the American Boardof Clinical Neuro-
physiology in EEG and by the AmericanBoard of Neurophysiologic Monitoring inIntraOperative Neurophysiology. Hisspecial clinical interests are EEG/epilepsyand intraoperative neurophysiologicmonitoring. His research interests centeron the response of peripheral nerve toischemia, the properties of electrodes andinformation theory. Prior to his appoint-ment as Chairman of Neuroscience atWinthrop, he was Associate Chair forNeurology in the Department ofNeuroscience at Marshall University inHuntington, West Virginia, where he wasalso a Professor of Neuroscience. Hispostgraduate training includes a DanaFellowship in Neuroscience/Epilepsy/EEGat the University of Pennsylvania andGraduate Hospital in Philadelphia. Hecompleted a residency in neurology at theHospital of the University of Pennsylvaniaand an internship in medicine atLankenau Hospital in Philadelphia. Dr.Stecker earned his medical degree fromthe Harvard Medical School/MIT HSTProgram and a PhD in physics from theUniversity of Pennsylvania. He is a pastpresident and a Fellow of the AmericanSociety of Neurophysiologic Monitoringand a Fellow of the American ClinicalNeurophysiology Society. Dr. Stecker is asenior member of the IEEE (Institute of Electrical and Electronics Engineers)and has authored over 100 papers and articles.
Michael H. Brisman, MDChief, Division of NeurosurgeryCo-Director, Institute for Neurosciences516.255.9031
Dr. Michael Brisman specializes in stereotac-tic surgery and radio-surgery for braintumors and trigeminalneuralgia. He is BoardCertified by theAmerican Board ofNeurological Surgeons
and is a Fellow of the American Collegeof Surgeons. His postgraduate trainingincludes a neurosurgical residency andsurgical internship at The Mount SinaiMedical Center in New York, where hewas Chief Resident. He received his med-ical degree from Columbia University’sCollege of Physicians and Surgeons. Dr.Brisman has published numerous articlesin professional journals. He is pastPresident of the Nassau County MedicalSociety and President of the New YorkState Neurosurgical Society.
Jonathan L. Brisman, MD Director, Cerebrovascular & EndovascularNeurosurgery516.255.9031
Dr. Jonathan Brismanspecializes in cebro-vascular and endovas-cular surgery for dis-eases of the centralnervous system. As oneof fewer than 100 neu-rosurgeons nationwidewith dual training in
microneurosurgery and endovasculartechniques (and the first on Long Island),he is skilled in aneurysm clipping andendovascular coiling for brain aneurysms,as well as in advanced procedures to treatbrain arteriovenous malformations(AVM), carotid stenosis and acute stroke.His postgraduate training includes anInterventional Neuroradiology Fellowshipat Roosevelt Hospital in New York and aMicrovascular Neurosurgical Fellowshipat Swedish Hospital in Seattle. He com-pleted a neurosurgical residency and sur-gical internship at Massachusetts GeneralHospital, where he was Chief Neuro-surgery Resident. Dr. Brisman receivedhis medical degree from ColumbiaUniversity’s College of Physicians andSurgeons. He has published over 40
articles in peer-reviewed neurosurgeryjournals, including “Medical Progress:Cerebral Aneurysms” in the New EnglandJournal of Medicine and one on strokemanagement in Lancet Neurology.
Benjamin R. Cohen, MDNeurosurgeon516.255.9031
Dr. Benjamin Cohen isa Board CertifiedNeurosurgeon special-izing in spinal surgery.His practice includesrevision spine surgery,adult scoliosis and thetreatment of spinalinfection and metasta-
sis. Fully versed in standard laminectomyand fusion techniques, Dr. Cohen has aspecial interest in minimally invasive pro-cedures, including kyphoplasty andmicrodiscectomy, as well as surgery forspinal tumors. His postgraduate trainingincludes a Fellowship in Complex SpinalSurgery at the University of Alabama, aswell as a neurosurgical residency andgeneral surgery internship at the AlbanyMedical Center, where he also receivedthe House Staff Scholarly ResearchAward. Dr. Cohen earned his medicaldegree from The Chicago Medical School,where he was elected to Alpha OmegaAlpha, the medical honor society. He hasauthored and co-authored numerousmanuscripts and articles in the fields ofneurosurgery and the spine, and hasgiven many presentations on these topics.
Contributing Clinicians

Artem Vaynman, MDNeurosurgeon516.255.9031
Dr. Artem Vaynmanspecializes in complexspinal surgery, minimal-ly invasive spinal sur-gery and 3D spinal navi-gation. He treats a vari-ety of spine problems,including degenerativescoliosis, spinal stenosis,
compression fractures, back pain, herniat-ed disc and sciatica. His postgraduatetraining includes a Fellowship in ComplexSpine Surgery at the Cleveland ClinicFoundation and residencies in general sur-gery and neurosurgery at the New JerseyMedical School, University Hospital inNewark, where he served as ChiefResident in Neurosurgery. He obtained hismedical degree at SUNY DownstateCollege of Medicine in Brooklyn. Dr.Vaynman has authored “Spinal CordInjury and Paralysis” a chapter inEssentials of Orthopedic Surgery: Spine.
Marc Wilkenfeld, MDChiefDivision of Occupational & Environmental Medicine516.663.8890
Dr. Marc Wilkenfeld — arecognized expert inenvironmental medicineand the impact of 9/11on victims, first respon-ders and individualsnear the site at the timeof the disaster — hasmore than 20 years of
clinical and teaching experience in thespecialty. Board Certified in OccupationalMedicine, Dr. Wilkenfeld served on anexpert review panel of the EnvironmentalProtection Agency’s Technical AdvisoryTask Force following the 9/11 terroristattacks. He also consulted with corpora-tions, community groups and governmentagencies on the disaster’s impact onhealth, assisting in the development ofscreening protocols for individualsexposed to the site. Dr. Wilkenfeld hasevaluated hundreds of patients with ill-nesses related to the disaster, continuingto treat many of them. His postgraduatetraining includes a residency in occupa-tional medicine at The Mount SinaiMedical Center in New York. He earned
his medical degree from the University of Vermont College of Medicine. Dr.Wilkenfeld has authored several articlesand book chapters on environmental medicine and has lectured extensively onthe topic throughout the U.S., Europe,Canada and the Middle East.
Elzbieta Wirkowski, MDMedical Director, Neuroscience IntensiveCare UnitDirector, Cerebrovascular Disorders andStroke Program516.663.4525
Dr. Elzbieta Wirkowskispecializes in cere-brovascular neurologyand neurocritical care.She is Board Certifiedin Neurology, VascularNeurology andNeurocritical Care. Herpostgraduate training
includes a Cerebrovascular Fellowship atLong Island Jewish Medical Center (LIJ),where she participated in multipleresearch trials dealing with neurocriticaland cerebrovascular problems. She alsocompleted a residency and internship inneurology at LIJ. Dr. Wirkowski earnedher medical degree with honors fromWarsaw University in Poland, where shealso studied molecular biology. She is theauthor of many publications dealing withneurocritical care and stroke, and pres-ents regularly at national and internation-al meetings.

Non-Profit Org.US PostageP A I D
Permit #13Mineola, NY
Institute for Neurosciences259 First Street, Mineola, NY 115011-866-NEURO-RX
www.winthrop.org
Winthrop-University Hospital is a 591-bed teaching hospital located on LongIsland in Mineola, NY. A major regionalhealthcare resource, the Hospital has been a leading healthcare provider formore than a century, dedicated to theintegrity, dignity and well-being of every individual. Winthrop offers a fullcomplement of advanced inpatient andoutpatient services with a deep commit-ment to medical education and research.
Physicians and surgeons in Winthrop’sInstitute for Neurosciences are pioneer-ing the use of technologically advancedapproaches for the diagnosis and treatment of diseases of the brain andspine, including computerized imagingsystems, state-of-the-art surgical inter-ventions and the latest generation of medication therapies.
The Institute’s interdisciplinary teamincludes neurologists; neurosurgeons; neurointensivists; pediatric neurologistsand neurosurgeons; neuroradiologists;vascular surgeons; orthopaedic spine surgeons; neuro-oncologists; neuro-pathologists; neurophysiologists; and specially trained nurse practitioners,physician assistants and nurses. Special-ized physical and occupational therapy,social work and other supportive servicesare also key components of the Institute.The Institute’s experts are up to date onthe latest developments in neuroscienceand help pave the way for new discoveriesthrough participation in clinical researchtrials, which enable them to providepatients with access to tomorrow’s mostpromising therapies.
Winthrop-University Hospital’s Institute for Neurosciences
Programs & Services Offered by the Institute for Neurosciences
Neuroscience Intensive Care UnitThe 14-bed acute care NeuroICU is reserved for patients with serious, complex neurological issues.The focus is on providing continuous monitoring and instantaneous results of critical values, allowing the expert staff, experienced in using advanced technology and providing neurocritical care,to employ aggressive interventions that treat neurological deterioration.
For more information, call the Institute for Neurosciences at 1-866-NEURO-RX.
Comprehensive Level 4 Epilepsy CenterMovement Disorders ProgramMultiple Sclerosis Care CenterNeurodiagnostic Laboratory
Neuromuscular/Peripheral Neuropathy ProgramNeuroscience Intensive Care UnitNYS Designated Stroke Center with AHA and ASA “Gold” Level Status
Aneurysm TreatmentCT Perfusion ScanningInterventional NeuroradiologyNeuroangiography
Positron Emission Tomography (PET) ScanningUltrafast Computed Tomography (CT) & Magnetic Resonance Imaging (MRI)
Attention Disorders & Learning Disabilities Treatment
Craniosynostosis SurgeryBrain Tumor TreatmentEvaluation & Treatment of Children with Headaches
Evaluation & Treatment of Neurological DisordersMyelomeningocele Surgery
Neuro Developmental Screening & Early Intervention
Pediatric Intensive Care UnitSeizure Disorders ManagementSurgery for Pediatric Neurovascular DisordersTreatment for Hydrocephalus & Other CNS Anomalies
Aneurysm Coiling & ClippingDisc ReplacementBrain Aneurysm ProgramBrain Tumor ProgramBrain & Skull Base SurgeryCarotid Stenting & EndarterectomyCerebrovascular & Endovascular SurgeryChiari Decompression SurgeryComplex & Minimally Invasive Spinal Surgeries Complex Cranial Surgery Computer-Assisted Resection of Brain TumorsCyberKnife® RadiosurgeryEndoscopic Pituitary SurgeryEpilepsy Surgery ProgramFacial Pain/Trigeminal Neuralgia ProgramImage-Guided Spine SurgeryKyphoplasty
Merci®/Penumbra® Clot Retrieval Microdiscectomy Microneurosurgical Techniques Microvascular Decompression for Trigeminal Neuralgia & Hemifacial Spasm
Neuro-oncologyParkinson’s Disease Surgery ProgramPosterior Lumbar Interbody Fusion Prestige® Cervical Disc Programmable Shunt PlacementSpinal StimulationSpine Revision SurgeryStereotactic Radiosurgery Traumatic Brain & Spine Injury Diagnosis & Treatment
X-Stop® for Spinal Stenosis
Pediatric Neurology & Neurosurgery
Neuroradiology
Neurosurgery
Neurology