Volume 28 – Number 4 July/August 2019
16
Pharmacology Updates: 2019 FDA Approved Drugs Safe Bedside Practice: Patient Safety Alert INSIDE 10 12 OFFICIAL NEWSLETTER Volume 28 – Number 4 July/August 2019 Michele D. Blakely H Healthcare workers face daily stressors that are known to negatively impact their efficiency as well as physical and mental health. Mokhtar, El Shikieri, Taha, and Rayan (2016) note that the higher than normal levels of workplace stress faced by nurses is not unique to Western cultures but is an international concern. Literature in recent years highlights that simply practicing gratitude, intention- ally shifting thoughts and mindfully focusing on positive experiences, can reap benefits in mental health. More research into positive psychology within the context of health care is emerging. This information is especially important to nursing staff in medical-surgical areas where work-related stress can be high. Each nursing specialty offers its own diverse set of stressors and challenges to the staff that practice there. Medical-surgical nursing in particular is a specialty arena with high expectations that require nurses to possess a diverse skillset to manage a wide array of disease states, procedures, and patient populations – all in a given shift. Recognizing the growing intensity and diverse needs of the population being managed in today’s acute care environments, nurses must be prepared and supported with strategies to enhance coping and manage resilience to remain healthy throughout the span of their nursing careers. Coping strategies that nurses choose are often predictive of their physical and mental health. For example, emotional strategies, such as binge eating, excessive alcohol consumption, prolonged sleeping, or even ‘marathon’ television watching can be negative or damaging when compared to healthier coping behaviors such as exercise, reflection, journaling, art, or other hobbies. Many researchers are finding that employing positivity strategies that may be perceived as superficial or simple in the workplace may have profound impacts on the wellbeing of the nurse. If borrowing les- sons from the positive psychology playbook has the potential to lessen workplace stress in nurses, those options should be explored more deeply. Clauss and colleagues (2018) noted basic daily pos- itive reflection practices were beneficial in reducing fatigue and exhaustion in caregivers. Similarly, Cheng,Tsui, and Lam (2015) reported a decline in stress and depressive symptoms using a reflective diary approach. Strategies such as positive reflection, journaling, and ending a shift change huddle with praise, positive thoughts, or gratitude (asking staff to express what they are grateful for), are all free techniques that can be easily implemented on nursing units. The financial and health benefits gained by utilizing simple positive psychological strategies in health care far outweigh the grim con- sequences of workplace stress facing nurses and their employers.To retain and attract nursing talent, Caring for a Patient with a Small Bowel Obstruction Complicated by Functional Somatic Syndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 Joining Forces: Actualizing Veteran-Centered Nursing Practice in the Medical-Surgical Setting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 Legislative Issues: Engagement is a Choice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 CNE PLUS
Transcript of Volume 28 – Number 4 July/August 2019

Pharmacology Updates: 2019 FDA Approved Drugs
Safe Bedside Practice: Patient Safety Alert
INSIDE
1012
OFFICIAL NEWSLETTER
Volume 28 – Number 4 July/August 2019
Michele D. Blakely
HHealthcare workers face daily stressors that are known to negatively impact their efficiency as well as physical and mental health. Mokhtar, El Shikieri, Taha, and Rayan (2016) note that the higher than normal levels of workplace stress faced by nurses is not unique to Western cultures but is an international concern. Literature in recent years highlights that simply practicing gratitude, intention-ally shifting thoughts and mindfully focusing on positive experiences, can reap benefits in mental health. More research into positive psychology within the context of health care is emerging. This information is especially important to nursing staff in medical-surgical areas where work-related stress can be high. Each nursing specialty offers its own diverse set of stressors and challenges to the staff that practice there. Medical-surgical nursing in particular is a specialty arena with high expectations that require nurses to possess a diverse skillset to manage a wide array of disease states, procedures, and patient populations – all in a given shift. Recognizing the growing intensity and diverse needs of the population being managed in today’s acute care environments, nurses must be prepared and supported with strategies to enhance coping and manage resilience to remain healthy throughout the span of their nursing careers.
Coping strategies that nurses choose are often predictive of their physical and mental health. For example, emotional strategies, such as binge eating, excessive alcohol consumption, prolonged sleeping, or even ‘marathon’ television watching can be negative or damaging when compared to healthier coping behaviors such as exercise, reflection, journaling, art, or other hobbies. Many researchers are finding that employing positivity strategies that may be perceived as superficial or simple in the workplace may have profound impacts on the wellbeing of the nurse. If borrowing les-sons from the positive psychology playbook has the potential to lessen workplace stress in nurses, those options should be explored more deeply. Clauss and colleagues (2018) noted basic daily pos-itive reflection practices were beneficial in reducing fatigue and exhaustion in caregivers. Similarly, Cheng, Tsui, and Lam (2015) reported a decline in stress and depressive symptoms using a reflective diary approach. Strategies such as positive reflection, journaling, and ending a shift change huddle with praise, positive thoughts, or gratitude (asking staff to express what they are grateful for), are all free techniques that can be easily implemented on nursing units. The financial and health benefits gained by utilizing simple positive psychological strategies in health care far outweigh the grim con-sequences of workplace stress facing nurses and their employers. To retain and attract nursing talent,
Caring for a Patient with a Small Bowel Obstruction Complicated by Functional Somatic Syndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 Joining Forces: Actualizing Veteran-Centered Nursing Practice in the Medical-Surgical Setting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 Legislative Issues: Engagement is a Choice. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
CNE
PLUS

Healthy PRACTICE ENVIRONMENTS
employers must acknowledge the burden of workplace stress and act proactively to reduce it in nursing.
Maintaining a healthy nursing workforce requires collaboration between the nurse, leadership, and employing organization. The nurse must be accountable for their own wellbeing, seeking healthy coping strategies, or asking for help when needed. Nurse leaders need to advocate, engage, and train staff in effective, healthy coping mechanisms. By identifying and intervening when additional resources are warranted to improve the work environment, nurse leaders can positively impact the level of workplace stress. Finally, organizations employing nurses must be com-mitted to initiatives that transparently acknowledge, teach, support, and identify when resources are needed to promote the most effective techniques for manag-ing workplace stress. For our nurses to remain healthy and resilient enough to meet the continually increasing healthcare demands, workplace stress must stay in the forefront of leaders’ minds.
Michele D. Blakely, DNP, RN, NEA-BC, is Program Director for Nursing Professional Practice, Wake forest Baptist Health, Winston-Salem, NC. She may be con-tacted at [email protected]
References Cheng, S.T., Tsui, P.K., Lam, J.H. (2015). Improving mental health in health care practitioners:
Randomized controlled trial of a gratitude intervention. Journal of Consulting and Clinical Psychology, 83(1), 177-186. doi:10.1037/a0037895
Clauss, E., Hoppe, A., O’Shea, D., González Morales, M.G., Steidle, A., & Michel, A., (2018). Promoting personal resources and reducing exhaustion through positive work reflection among caregivers. Journal of Occupational Health Psychology, 23(1), 127-140. doi:10.1037/ocp0000063
Mokhtar, K., El Shikieri, A., Taha, E., & Rayan, A. (2016). The relationship between occupational stressors and performance amongst nurses working in pediatric and intensive care units. American Journal of Nursing Research, 4(2), 34-40. doi:10.12691/ajnr-4-2-2
2
Volume 28 – Number 4 July/August 2019
Reader Services MedSurg Matters! Academy of Medical-Surgical Nurses East Holly Avenue, Box 56 Pitman, NJ 08071-0056 (856) 256-2300 • (866) 877-AMSN (2676) Fax (856) 589-7463 [email protected] www.amsn.org
MedSurg Matters! is owned and published bimonthly by the Academy of Medical-Surgical Nurses (AMSN). The newsletter is distributed to members as a direct benefit of membership.
Advertising Contact Rick Gabler, Advertising Representative, (856) 256-2314.
Back Issues To order, call 866-877-AMSN (2676).
Editorial Content AMSN encourages the submission of news items and photos of interest to AMSN members. By virtue of your submission, you agree to the usage and editing of your submission for possible publica-tion in the AMSN newsletter, online, and in other promotional and educational materials.
To send comments, questions, or article sugges-tions, or if you would like to write for us, contact the Editor at [email protected].
AMSN Publications and Products To order, call 866-877-AMSN (2676), or visit www.amsn.org.
Reprints For permission to reprint an article, call 866-877-AMSN (2676).
Indexing MedSurg Matters! is indexed in the Cumulative Index to Nursing and Allied Health Literature (CINAHL).
© Copyright 2019 by AMSN. All rights reserved. Reproduction in whole or part, electronic or mechanical without written permission of the pub-lisher is prohibited. The opinions expressed in MedSurg Matters! are those of the contributors, authors and/or advertisers, and do not necessarily reflect the views of AMSN, MedSurg Matters!, or its editorial staff.
Publication Management is provided by Anthony J. Jannetti, Inc., which is accredited by the Association Management Company
Institute.
For our nurses to remain healthy and resilient enough to meet
the continually increasing healthcare demands, workplace stress must stay in the forefront
of leaders’ minds.
If you have any questions or comments regarding the “Healthy Practice Environments” column, or if you are interested in writing, please contact Column Editor Michele Blakely at [email protected].
Did You Know?AMSN has a
Member-Get-A-Member Program!
You can earn discounts by
bringing more people
into AMSN’s community
of med-surg nurses.
Learn more at www.amsn.org/ mgm

Instructions for Continuing Nursing Education Contact Hours Caring for a Patient with a Small Bowel Obstruction Complicated
by Functional Somatic Syndromes
Deadline for Submission: August 31, 2021
MSNN1904
To Obtain CNE Contact Hours 1. For those wishing to obtain CNE contact hours,
you must read the article and complete the evaluation through the AMSN Online Library. Complete your evaluation online and print your CNE certificate immediately, or later. Simply go to www.amsn.org/library
2. Evaluations must be completed online by August 31, 2021. Upon completion of the evaluation, a certificate for 1.3 contact hour(s) may be printed.
Fees Member: FREE Regular: $20
Learning Outcome After completing this learning activity, the
learner will be able to discuss the role that an interdisciplinary team and palliative care team plays in advocating for and managing the care of patients with the ‘silent diseases’ of functional somatic syndrome (FSS).
Learning Engagement Activity Review Table 1 to identify the best practices to
incorporate into a multifactoral treatment plan for patients with FSS.
The author(s), editor, editorial committee, con-tent reviewers, and education director reported no actual or potential conflict of interest in relation to this continuing nursing education article.
This educational activity is jointly provided by Anthony J. Jannetti, Inc. and the Academy of Medical-Surgical Nurses (AMSN).
Anthony J. Jannetti, Inc. is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Anthony J. Jannetti, Inc. is a provider approved by the California Board of Registered Nursing, provider number CEP 5387. Licensees in the state of California must retain this certificate for four years after the CNE activity is completed.
This article was reviewed and formatted for con-tact hour credit by Michele Boyd, MSN, RN-BC, AMSN Education Director.
4
Caring for a Patient with a Small Bowel Obstruction Complicated by Functional Somatic Syndromes
CNECONTINUING
NURSINGEDUCATION
Kaléi Kowalchik, Michael M. Evans, Kiernan Riley, and Theresa Baker
Mr. E., a 38-year-old-male, arrived in the emergency department complaining of abdominal pain, nausea, and vomiting. He lives at home with his wife and young son and is a U.S. Army veteran, having served time in Afghanistan and Iraq. Mr. E. was honorably discharged fol-lowing a gunshot wound to the abdomen which required several sur-geries. He is currently disabled and has a past medical history of hypertension, gastroesophageal reflux disease, bowel obstructions, fibromyalgia, chronic fatigue syndrome (CFS), and bowel adhesions. His past surgical history includes a loop colostomy with reversal of colostomy 6 months later. On admis-sion to the emergency department, Mr. E. vomited approximately 300 mL of green fluid. Vital signs were temperature of 100.2 Fahrenheit (F) tympanic, pulse of 108, respirations of 24, blood pres-sure of 160/90 mmhg, and a pulse oximetry reading of 97% on room air with a generalized pain level of 8/10. Home medications included: Lisinopril 40 mg PO daily, Prilosec 20 mg PO daily, Lyrica 300 mg PO daily, Lexapro 20 mg PO daily, and Tylenol 650 mg PO every 6 hours as needed for pain.
Upon assessment, Mr. E. was awake, alert, and oriented but ill-appearing. His abdomen was distended and tender to touch with high pitched bowel sounds noted. He received Zofran 4 mg intravenously (IV) for the nausea and vomiting after a 22-guage IV catheter was started in his left hand without incident. An IV of Normal Saline Solution (NSS) was started at 100 mL/hr for hydration, and Mr. E. was made NPO. Labs ordered by the emer-gency department physician included a complete blood cell count (CBC) and a comprehensive metabolic panel (CMP), along with an abdominal x-ray. The x-ray showed dilated loops of small bowel consistent with a small bowel
obstruction, most likely related to bowel adhesions from previous surger-ies. The CBC revealed a white blood cell count (WBC) of 14.2 K/ul; all other labs were within normal limits. Based on these findings, the emergency department physician admitted him to the medical-surgical floor for further evaluation and treatment.
Upon admission to the medical-surgical unit, he vomited two more times for a total of 400 mL of green fluid. His abdominal assessment and vital signs remained unchanged. When questioned where it hurts, the patient stated that he had tender, aching pain to the touch located throughout his entire body, but worse in the abdomen. He stated, “I’m sick of no one believing [me] that the pain hurts so bad.” After being seen by the hospitalist, Mr. E. was kept NPO, and his IV fluids were changed to NSS with 20 meq of KCL at 125 mL/hr. In addition, Mr. E. was started on Morphine 2 mg IV every 4 hours as needed for pain. A nasogastric tube (NGT) was ordered to be inserted and started on low intermit-tent suction to help with nausea and vomiting. Home medications were ordered to continue with a small sip of water and the NGT turned off for 1-hour post medication administration. Lastly, a follow-up CBC, CMP, and abdominal X-ray was ordered for the next morning.
Background of Functional Somatic Syndromes
Functional somatic syndromes (FSSs) are a category of illnesses that are characterized by a plethora of unexplained medical symptomology (Henningsen, Zipfel, Sattel, & Creed, 2018). They are sometimes referred to as ‘invisible diseases,’ which can be fur-ther defined as diseases that limit a person’s physical, mental, or neuro-

5
866-877-2676 Volume 28 – Number 4
logical abilities internally and are invis-ible to onlookers. This is an umbrella term for diseases such as fibromyalgia, CFS, and psychological disorders. These diseases cause debilitating symptoms for patients which are invisible to healthcare providers and subsequently difficult to recognize and treat (Amigues, 2019). Graver (2017) suggests that nearly 30% of general medical patients may be experiencing one or more of these syndromes.
Fibromyalgia is a chronic condi-tion which is characterized by wide-spread pain and tenderness with peri-ods of exacerbations and remissions. While fibromyalgia does not develop from immune dysfunction or inflam-mation, rheumatic disease is a known predecessor to it. In addition to wide-spread pain, patients may have trouble sleeping, experience chronic fatigue, and develop memory problems (Lewis, Dirksen, Heitkemper, Bucher, & Harding, 2014). There is no definitive diagnosis for fibromyalgia. It is typically diagnosed based off of symptomology and rule-out of other possible causes. There is no cure for fibromyalgia. Treatment typically consists of non-pharmacologic measures, such as exercise and physi-cal therapy, combined with pharmacologic therapies, such as anti-depressants or gamma-aminobutyric acid analogues (Amigues, 2019).
Chronic fatigue syndrome, also known as myalgic encephalomyelitis or post-exertional malaise, is a chronic and debilitating condition that can affect multiple body systems. The most common manifestation is an extreme reduction in energy to the point where activities of daily living can no longer be performed. In severe cases, patients can be con-fined to a bed. The disease process and associated symptoms are unpredictable making disease management for FSSs diffi-cult to plan for. There is no definitive diagnosis for CFS, and treatment is largely palliative towards symptom manifesta-tions (Centers for Disease Control and Prevention, 2018).
Barriers to Care Arnold, Gebke, and Choy (2016) have identified the fol-
lowing as barriers to care for patients with FSSs: Lack of a clear pathway for diagnosis and management of •pain. Multiple practitioners prescribing multiple medications. •Cultural differences related to patient expectations of •treatment outcomes.
These barriers can lead to patient and healthcare provider dissatisfaction and possible distrust (Arnold et al., 2016).
Skepticism often surrounds patients with FSSs as their symptoms may vary from day to day. Patients with FSSs received a higher bias from healthcare workers when com-pared to patients with a clear disease trajectory (Cohen, 2009). Pain and fatigue are often dismissed as emotional problems, although they are legitimate physical problems, just not yet explained by modern medicine. Dismissal of symp-toms as emotional problems causes a fear of reporting symp-toms by patients and a lack of appropriate symptom pallia-tion, further contributing to a decreased quality of life (Graver, 2017).
Patients who feel healthcare professionals do not believe or accept their symptoms may disengage from primary care (Bayliss et al., 2014). Disengagement may lead to medical complications requiring a need for emergency care and resulting in continuation of the dysfunctional cycle. This, in turn, can lead to more disabling complications, increased medical costs, and, most importantly, negative mental, physi-cal, and social outcomes (Arnold et al., 2016). Patients caught up in this dysfunctional cycle may experience decreased workplace productivity, social isolation, depression, and anxiety (Cohen, 2009).
Best Practices There are few evidence-based treatments available for
providers caring for patients with FSSs due to the limited access to specialized care plans for these diverse pathological issues and the trend to care for patients with determined dis-
eases (Bayliss et al., 2014). Due to the vast differences between patient experiences and perceptions when dealing with FSSs, there is not one best treatment utilized for this population. Therefore, with the help of palliative care special-ists, medical-surgical nurses and healthcare providers in gen-eral can provide person-centered care that addresses the many symptoms faced by persons suffering from a FSS. Palliative care teams can provide specialized medical treat-ment which focuses on alleviating suffering of chronic and debilitating diseases. These teams consist of a variety of healthcare team members, including physicians, nurses, physi-cal and occupational therapists, spiritual counselors, and more, who focus on a patient’s physical, psychosocial, and spir-itual health (World Health Organization [WHO], 2019). The case study below breaks down some of the best practices that could be utilized when caring for patients with FSSs.
Case Study Update Mr. E.’s small bowel obstruction was resolved without
surgical intervention through bowel rest and decompression with the NGT. After 2 days, the NGT was discontinued and the patient was started on a clear liquid diet which was tol-erated well. However, while his abdominal pain was better, he still complained of generalized pain and extreme fatigue; therefore, the medical-surgical nurse consulted the palliative care team to evaluate the patient for these complaints. After assessing the patient, the palliative care team – in conjunction with the hospitalist and the patient’s medical-surgical nurses – decided to add ibuprofen 600 mg PO every 6 hours as needed for mild pain (taken with food), Tramadol 50 mg PO every 6 hours as needed for moderate to severe pain, and Cymbalta 30 mg PO daily for 1 week and then increase to twice a day, along with the patient’s routine medications. These medications were added to assist Mr. E. with his con-stant struggles with pain and fatigue. In addition, physical ther-apy was consulted to evaluate Mr. E. and outpatient exercises were recommended to assist him with his FSSs, fibromyalgia, and CFS (Mayo Clinic, 2017).
Two days later, Mr. E. tolerated a regular diet, complained of less pain and fatigue, and was discharged home. He was instructed to follow-up with the palliative care team on an outpatient basis to assist with the management of his fibromyalgia and CFS. When receiving his discharge instruc-tions, Mr. E. said to the medical-surgical nurse, “Thank you for believing me. You are the first person to get me help.” The nurse smiled and let him know that it was her pleasure to care and advocate for him to get the treatment he deserves.
Conclusion As discussions for silent diseases such as fibromyalgia
and CFS become more prevalent in society, it is important that healthcare professionals become educated on the com-plexities associated with the nature of each syndrome. It can be frustrating and difficult for healthcare workers to under-stand and care for patients experiencing FSSs due to each patient’s internal, individual, and complex symptom experi-ence. The multifaceted symptoms that patients experience can make it challenging for them to be accepted by the healthcare community while obtaining proper symptom management which causes a decline in these patients’ quality of life. By incorporating aspects of palliative care and inter-professional team-based approaches, healthcare providers will be able to better manage their patients suffering with FSSs. The best practices section noted above should be uti-lized as a resource for nurses and other healthcare providers caring for a patient with any type of FSS in the medical-sur-gical setting to ensure better outcomes and overall health-care experiences for the patient. Kaléi Kowalchik is a Senior Honor’s Nursing Student and Undergraduate and Graduate Research Assistant, The Pennsylvania State University, College of Nursing, Scranton Campus, Dunmore, PA. She may be contacted [email protected]
Academy of Medical-Surgical Nurses www.amsn.org
6
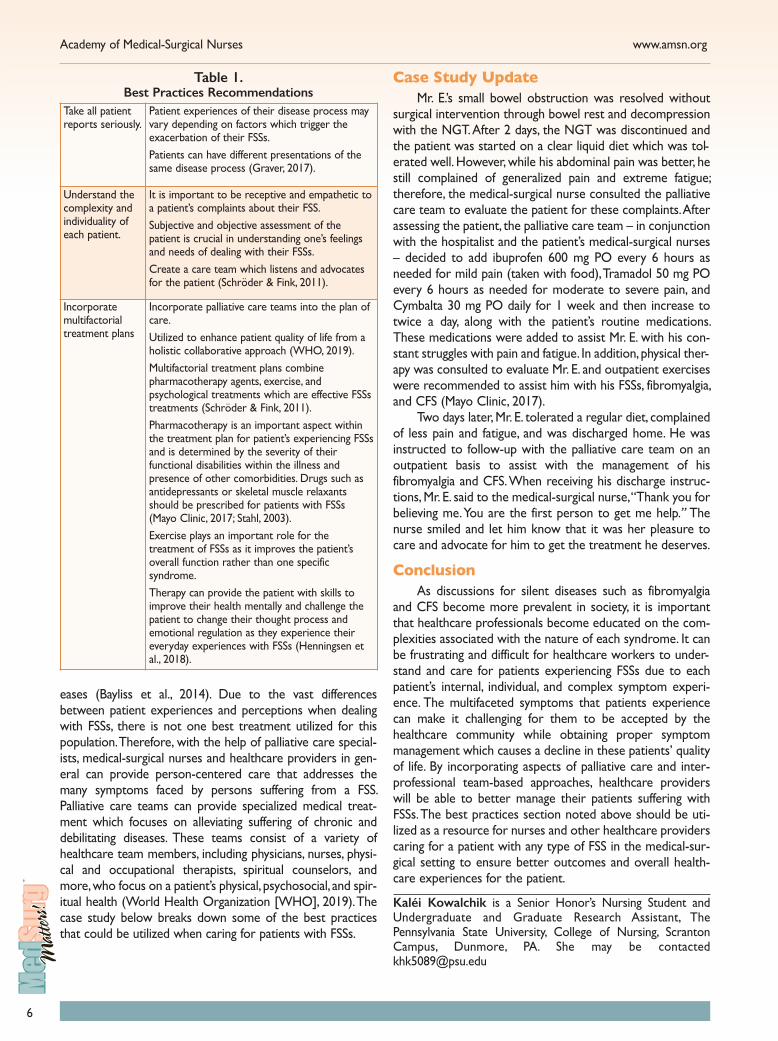
Take all patient reports seriously.
Patient experiences of their disease process may vary depending on factors which trigger the exacerbation of their FSSs. Patients can have different presentations of the same disease process (Graver, 2017).
Understand the complexity and individuality of each patient.
It is important to be receptive and empathetic to a patient’s complaints about their FSS. Subjective and objective assessment of the patient is crucial in understanding one’s feelings and needs of dealing with their FSSs. Create a care team which listens and advocates for the patient (Schröder & Fink, 2011).
Incorporate multifactorial treatment plans
Incorporate palliative care teams into the plan of care. Utilized to enhance patient quality of life from a holistic collaborative approach (WHO, 2019). Multifactorial treatment plans combine pharmacotherapy agents, exercise, and psychological treatments which are effective FSSs treatments (Schröder & Fink, 2011). Pharmacotherapy is an important aspect within the treatment plan for patient’s experiencing FSSs and is determined by the severity of their functional disabilities within the illness and presence of other comorbidities. Drugs such as antidepressants or skeletal muscle relaxants should be prescribed for patients with FSSs (Mayo Clinic, 2017; Stahl, 2003). Exercise plays an important role for the treatment of FSSs as it improves the patient’s overall function rather than one specific syndrome. Therapy can provide the patient with skills to improve their health mentally and challenge the patient to change their thought process and emotional regulation as they experience their everyday experiences with FSSs (Henningsen et al., 2018).
Table 1. Best Practices Recommendations

7
866-877-2676 Volume 28 – Number 4
Michael M. Evans, PhD, MSEd, RN, ACNS, CMSRN, CNE, is an Associate Teaching Professor of Nursing, The Pennsylvania State University, College of Nursing, Scranton Campus, Dunmore, PA. Kiernan Riley, BSN, RN, is a BSN to PhD Student and University Fellow, The Pennsylvania State University, College of Nursing, University Park Campus, University Park, PA. Theresa Baker, MSN, RN, is an Instructor of Nursing, The Pennsylvania State University, College of Nursing, Scranton Campus, Dunmore, PA.
References Amigues, I. (2019). Fibromyalgia. Retrieved from https://www.rheuma
tology.org/ I-Am-A/Patient-Caregiver/Diseases-Conditions/Fibromyalgia
Arnold, L.M., Gebke, K.B., & Choy, E.H.S. (2016). Fibromyalgia: Management strategies for primary care providers. The International Journal of Clinical Practice, 70(2), 99-112. doi:10.1111/ijcp.12757
Bayliss, K., Goodall, M., Chisholm, A., Fordham, B., Chew-Graham, C., Riste, L. … Wearden, A. (2014). Overcoming the barriers to the diagnosis and management of chronic fatigue Syndrome/ME in pri-mary care: A meta synthesis of qualitative studies. BMC Family Practice,15. doi:10.1186/1471-2296-15-44
Centers for Disease Control and Prevention. (2018). Treatment of ME/CFS. Retrieved from https://www.cdc.gov/me-cfs/treatment/index.html
Cohen, S.P. (2009). Overcoming obstacles: Barriers to care in fibromyal-gia treatment. John Hopkins Advanced Studies in Medicine, 9(4), 115-121.
Graver, C.J. (2017). Functional somatic syndrome: Assessment and man-agement. The Journal of the American Osteopathic Association, 117, 511-519. doi:10.7556/jaoa.2017.101
Henningsen, P., Zipfel, S., Sattel, H., & Creed, F. (2018). Management of functional somatic syndromes and bodily distress. Psychotherapy and Psychosomatics, 87(1), 12-31. doi:10.1159/000484413
Lewis, S.L., Dirksen, S.R., Heitkemper, M.M., Bucher, L., & Harding, M.M. (2014). Medical-surgical nursing: Assessment and management of clin-ical problems (9th Edition). St. Louis, MI: Elsevier.
Mayo Clinic. (2017). Fibromyalgia. Retrieved from https://www.mayoclinic.org/diseases-conditions/fibromyalgia/diagnosis-treatment/drc-20354785
Schröder, A., & Fink, P. (2011). Functional somatic syndromes and somatoform disorders in special psychosomatic units: Organizational aspects and evidence-based treatment. The Psychiatric Clinics of North America, 34(3), 673-687. doi:10.1016/j.psc.2011.05.008
Stahl, S.M. (2003). Antidepressants and somatic symptoms: Therapeutic actions are expanding beyond affective spectrum disorders to functional somatic syndromes. The Journal of Clinical Psychiatry, 64(7), 724-726. doi:10.4088/jcp.v64n0701
World Health Organization (WHO). (2019). WHO definition of pallia-tive care. Retrieved from http://www.who.int/cancer/palliative/definition/en/
MED-SURGMOMENTS
AN AMSN PODCAST
Topics and guests you care about, hosted by med-surg nurses!Listen, subscribe, and download on Apple Music, Spotify,
Google Music, and everywhere you get your podcasts!
www.medsurgmoments.org
Academy of Medical-Surgical Nurses www.amsn.org
8
Joining ForcesVisit amsn.org/joiningforces for more information on caring for the unique needs of members of the military.
If you have questions or comments regarding the “Joining Forces” column, or if you are interested in writing, please contact Column Editor Brenda Elliott at [email protected].
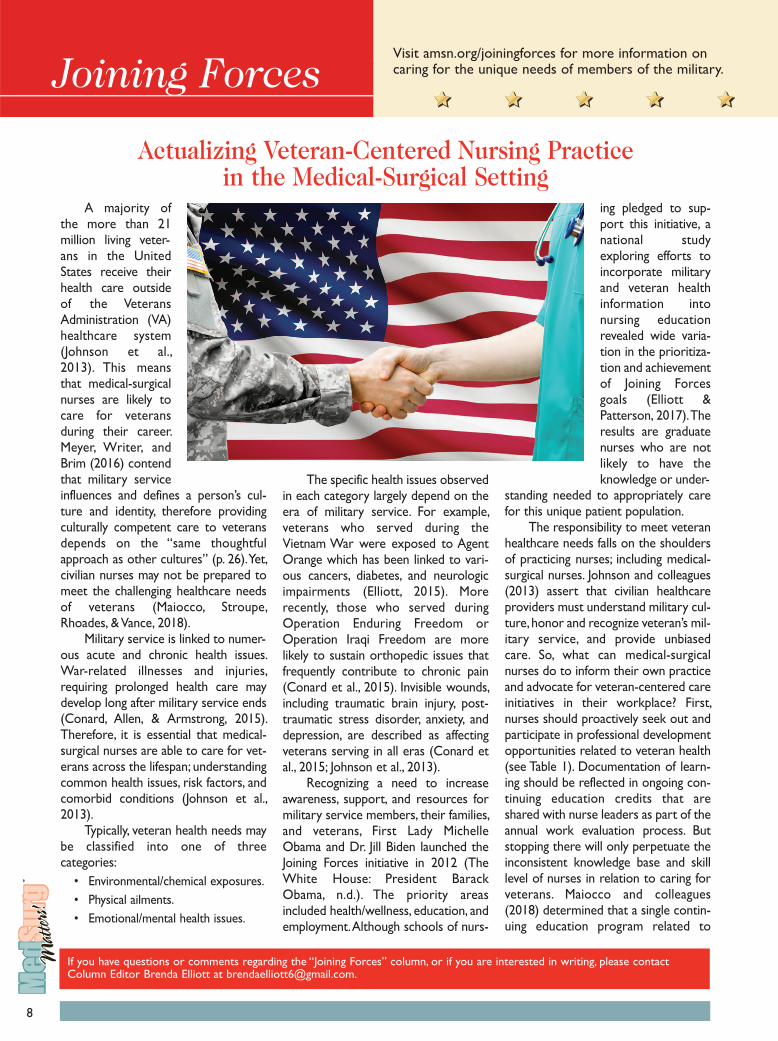
Actualizing Veteran-Centered Nursing Practice in the Medical-Surgical Setting
A majority of the more than 21 million living veter-ans in the United States receive their health care outside of the Veterans Administration (VA) healthcare system (Johnson et al., 2013). This means that medical-surgical nurses are likely to care for veterans during their career. Meyer, Writer, and Brim (2016) contend that military service influences and defines a person’s cul-ture and identity, therefore providing culturally competent care to veterans depends on the “same thoughtful approach as other cultures” (p. 26). Yet, civilian nurses may not be prepared to meet the challenging healthcare needs of veterans (Maiocco, Stroupe, Rhoades, & Vance, 2018).
Military service is linked to numer-ous acute and chronic health issues. War-related illnesses and injuries, requiring prolonged health care may develop long after military service ends (Conard, Allen, & Armstrong, 2015). Therefore, it is essential that medical-surgical nurses are able to care for vet-erans across the lifespan; understanding common health issues, risk factors, and comorbid conditions (Johnson et al., 2013).
Typically, veteran health needs may be classified into one of three categories:
Environmental/chemical exposures. •Physical ailments. •Emotional/mental health issues. •
The specific health issues observed in each category largely depend on the era of military service. For example, veterans who served during the Vietnam War were exposed to Agent Orange which has been linked to vari-ous cancers, diabetes, and neurologic impairments (Elliott, 2015). More recently, those who served during Operation Enduring Freedom or Operation Iraqi Freedom are more likely to sustain orthopedic issues that frequently contribute to chronic pain (Conard et al., 2015). Invisible wounds, including traumatic brain injury, post-traumatic stress disorder, anxiety, and depression, are described as affecting veterans serving in all eras (Conard et al., 2015; Johnson et al., 2013).
Recognizing a need to increase awareness, support, and resources for military service members, their families, and veterans, First Lady Michelle Obama and Dr. Jill Biden launched the Joining Forces initiative in 2012 (The White House: President Barack Obama, n.d.). The priority areas included health/wellness, education, and employment. Although schools of nurs-
ing pledged to sup-port this initiative, a national study exploring efforts to incorporate military and veteran health information into nursing education revealed wide varia-tion in the prioritiza-tion and achievement of Joining Forces goals (Elliott & Patterson, 2017). The results are graduate nurses who are not likely to have the knowledge or under-
standing needed to appropriately care for this unique patient population.
The responsibility to meet veteran healthcare needs falls on the shoulders of practicing nurses; including medical-surgical nurses. Johnson and colleagues (2013) assert that civilian healthcare providers must understand military cul-ture, honor and recognize veteran’s mil-itary service, and provide unbiased care. So, what can medical-surgical nurses do to inform their own practice and advocate for veteran-centered care initiatives in their workplace? First, nurses should proactively seek out and participate in professional development opportunities related to veteran health (see Table 1). Documentation of learn-ing should be reflected in ongoing con-tinuing education credits that are shared with nurse leaders as part of the annual work evaluation process. But stopping there will only perpetuate the inconsistent knowledge base and skill level of nurses in relation to caring for veterans. Maiocco and colleagues (2018) determined that a single contin-uing education program related to

9
866-877-2676 Volume 28 – Number 4
veteran mental health failed to improve nurses’ documentation of military serv-ice and improve confidence to adjust care to meet veterans’ needs.
Healthcare systems and state boards of nursing must share the obli-gation to advance the Joining Forces goals and do so on an on-going basis. Currently, only two state boards of nursing require continuing education related to veteran health for licensure and both are limited to mental health (Connecticut State Department of Public Health, 2019; West Virginia RN Board, 2019). It is proposed that contin-uing education requirements are expanded to include veteran-related competencies in all states. Recommendations for increasing awareness of veteran health needs in the acute care environment could be accomplished by appraising veteran-related health research in a journal club, sharing articles about veterans, participation in high fidelity simulations, and attending in-services dedicated to veteran-centered care. Further, it is rec-ommended that clinical educators and staff nurses collaborate to integrate veteran health information and cultur-ally-sensitive bedside care practices into annual competency assessments. It is not enough to merely acknowledge that veteran health care is important; medical-surgical nurses are called to spearhead efforts to enhance evidence-
based, veteran-centered care by com-mitting to professional development, advocating for resources, and partici-pating in care improvement processes needed to meet Joining Forces goals.
Katie A. Chargualaf, PhD, RN, CMSRN, is an Assistant Professor, University of South Carolina Aiken, Aiken, SC. She may be contacted at [email protected]
References Conard, P.L., Allen, P.E., & Armstrong, M.L.
(2015). Preparing staff to care for veter-ans in a way they need and deserve. Journal of Continuing Education in Nursing, 46(3), 119-120. doi:10.3928/00220124-20150220-15
Connecticut State Department of Public Health. (2019). Continuing education. Retrieved from https://portal.ct.gov/D P H / P r a c t i t i o n e r- L i c e n s i n g —Invest igat ions/APRN/Continuing-Education
Elliott, B. (2015). Caring for Vietnam veterans. Home Healthcare Now, 33(7), 358-365. doi:10.1097/NHH.0000000000000261
Elliott, B., & Patterson, B. (2017). Joining forces: The status of military and veteran health care in nursing curricula. Journal of Professional Nursing, 33(2), 145-152. doi:10.1016/j.profnurs.2016.06.006
Johnson, B.S., Boudiab, L.D., Freundl, M., Anthony, M., Gmerek, G.B., & Carter, J. (2013). Enhancing veteran-centered care: A guide for nurses in non-VA settings. The American Journal of Nursing, 113(7), 24-39. doi:10.1097/01.NAJ.0000 431913.50226.83
The White House: President Barack Obama. (n.d.). Joining forces. Retrieved from
National League for Nurses (NLN)
Resources for Veterans http://www.nln.org/professional-development-programs/teaching-resources/veterans-ace-v/joining-forces/resources-for-veterans
VA: National Center for PTSD Free Continuing Education Courses https://www.ptsd.va.gov/professional/continuing_ed/all_offerings.asp
American Association of Colleges of Nursing
Enhancing Veterans’ Care Toolkit https://www.aacnnursing.org/Teaching-Resources/Tool-Kits/Enhancing-Veterans-Care-Tool-Kit/Student-Resources
Academy of Medical-Surgical Nurses
Scholarly Papers, Government Guidelines, Websites, and Videos https://www.amsn.org/practice-resources/patient-care/ joining-forces
Jonas Philanthropies Jonas Philanthropies: Jonas Center for Nursing and Veterans Healthcare http://jonasphilanthropies.org/nursing-and-veterans-healthcare/
Table 1. Veteran Related Continuing Education Sources for Staff Nurses and
Clinical Educators
https://obamawhitehouse.archives.gov/joiningforces/about
Maiocco, G., Stroupe, L.M., Rhoades, A., & Vance, B. (2018). Care of veterans in a non-veteran health administration hospi-tal: What is the status of nursing practice after continuing education? Journal of Clinical Nursing, 28(3-4), 520-527. doi:10.1111/jocn.14641
Meyer, E.G., Writer, B.W., & Brim, W. (2016). The importance of military cultural com-petence. Current Psychiatry Reports, 18(3), 1-8. doi:10.1007/s11920-016-0662-9
West Virginia RN Board. (2019). Education. Retrieved from https://wvrnboard.wv.gov/education/Pages/default.aspx
Improve more lives in more waysWith more than 90,000 nurses at
over 1,800 sites of care in 21 states
across the country - HCA Healthcare
colleagues are raising the bar and
impacting healthcare everywhere -
today and tomorrow.
HCA Healthcare’s nurses improve
more lives in more ways and unlock
possibilities for their own career
growth. Be a part of a team that exists
to bring people a healthier tomorrow.
For more information, visit
careers.HCAhealthcare.com

10
If you have any questions or comments regarding the “Pharmacology Updates” column, or if you are interested in writing, please contact Column Editor Jane F. Marek at [email protected]
Pharmacology Updates
2019 FDA Approved Drugs The United States leads the world
in per capita prescription drug costs accounting for 30-40% of the global market. In 2016, the U.S.’s retail pre-scription drug costs reached $329 bil-lion, an estimated 10% of total national health expenditures (American Aca-demy of Actuaries, 2018). The Centers for Medicare and Medicaid Services predict prescription drug spending will increase an average of 6.3% annually during the years 2016 through 2025 (Olson & Sheiner, 2017). This year, Americans will fill an estimated 4.25 bil-lion retail prescriptions (Shahbandeh, 2019). Before a drug reaches the U.S. market, it must undergo a lengthy approval process by the U.S. Food & Drug Administration (FDA) to ensure its safety (you can view the drug approval process summary by visiting www.fda.gov/media/ 82381/download). After testing by the pharmaceutical company, the FDA’s Center for Drug Evaluation and Research (CDER) reviews the evidence from drug testing, evaluates its safety and efficacy for the intended use, and determines if the proposed benefits outweigh potential risks. Many drugs never reach the FDA and some developed to treat a specific disease may eventually be used to treat a different disease. For example, zidovu-dine (Retrovir or AZT), was initially researched in the 1960s as a drug to treat cancer, but in 1987 it was approved by the FDA to treat AIDS (FDA, 2017).
Nurses practicing in acute care set-tings administer an average of 10 med-ication doses per day for every patient (Durham, 2015). Many patients, particu-larly older adults and those with chronic disease, take more than one prescrip-tion medication. Keeping abreast of medications is an ongoing challenge with new drugs appearing on the mar-ket every year. In 2018, the FDA approved 59 new drugs, exceeding the
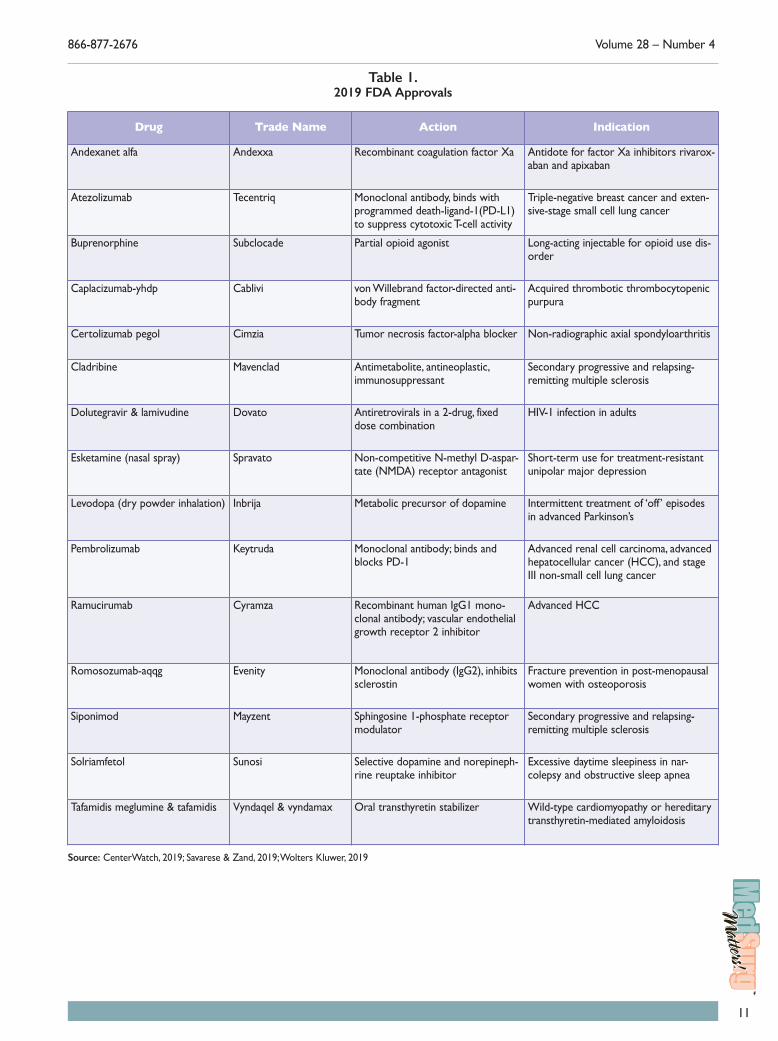
record for the number of medications approved yearly by the CDER (Mezher, 2019). The FDA also approved new indi-cations and new dosage forms for already approved drugs. To date, in this year alone, the FDA has approved 65 drugs, including new indications and new dosages for existing drugs (CenterWatch, 2019). Table 1 highlights some of the 2019 FDA approvals.
Jane F. Marek, DNP, MSN, RN, is an Assistant Professor, Frances Payne Bolton School of Nursing, Case Western Reserve University, Cleveland, OH. She may be contacted at [email protected]
References American Academy of Actuaries. (2018).
Prescription drug spending in the U.S. health care system: An actuarial perspective [Issue brief]. Retrieved from https://www.actu-ary.org/content/prescription-drug-spending-us-health-care-system
CenterWatch. (2019). 2019 FDA approved drugs. Retrieved from https://www.cen-terwatch.com/drug-information/fda-approved-drugs/year/2019
Durham, B. (2015). The nurse’s role in medica-tion safety. Nursing, 45(4), 1-4. doi:10.1097/01.nurse.0000461850.24153.8b
Mezher, M. (2019). FDA’s record year: A look at 2018 new drug approvals. Regulatory
Focus™, 2019(1). Retrieved from https : / /www.raps .org /news-and-articles/news-articles/2019/1/fdas-record-year-a-look-at-2018-new-drug-approva
Olson, P. & Sheiner, L. (2017). The Hutchins Center explains: Prescription drug spending. Brookings. Retrieved from https://www.brookings.edu/blog/up-front/2017/04/26/the-hutchins-center-explains-prescription-drug-spending/
Savarese, D.M.F., & Zand, J.M. (2019). What’s new in drug therapy. Retrieved from https://www.uptodate.com/contents/whats-new-in-drug-therapy
Shahbandeh, M. (2019). Total number of retail prescriptions filled Annually in the United States from 2013 to 2024 (in billions)*. Retrieved from https://www.statista.com/statistics/261303/total-number-of-retail-prescriptions-filled-annually-in-the-us/
U.S. Food & Drug Administration. (2017). The FDA’s drug review process: Ensuring drugs are safe and effective. Retrieved from https://www.fda.gov/drugs/drug-informa-tion-consumers/fdas-drug-review-process-ensuring-drugs-are-safe-and-effective
Wolters Kluwer. (2019). Clinical notices. Retrieved from https://www.wolter-skluwercdi.com/clinical-notices/new-drugs/
11
866-877-2676 Volume 28 – Number 4
Drug Trade Name Action Indication
Andexanet alfa Andexxa Recombinant coagulation factor Xa Antidote for factor Xa inhibitors rivarox-aban and apixaban
Atezolizumab Tecentriq Monoclonal antibody, binds with programmed death-ligand-1(PD-L1) to suppress cytotoxic T-cell activity
Triple-negative breast cancer and exten-sive-stage small cell lung cancer
Buprenorphine Subclocade Partial opioid agonist Long-acting injectable for opioid use dis-order
Caplacizumab-yhdp Cablivi von Willebrand factor-directed anti-body fragment
Acquired thrombotic thrombocytopenic purpura
Certolizumab pegol Cimzia Tumor necrosis factor-alpha blocker Non-radiographic axial spondyloarthritis
Cladribine Mavenclad Antimetabolite, antineoplastic, immunosuppressant
Secondary progressive and relapsing-remitting multiple sclerosis
Dolutegravir & lamivudine Dovato Antiretrovirals in a 2-drug, fixed dose combination
HIV-1 infection in adults
Esketamine (nasal spray) Spravato Non-competitive N-methyl D-aspar-tate (NMDA) receptor antagonist
Short-term use for treatment-resistant unipolar major depression
Levodopa (dry powder inhalation) Inbrija Metabolic precursor of dopamine Intermittent treatment of ‘off’ episodes in advanced Parkinson’s
Pembrolizumab Keytruda Monoclonal antibody; binds and blocks PD-1
Advanced renal cell carcinoma, advanced hepatocellular cancer (HCC), and stage III non-small cell lung cancer
Ramucirumab Cyramza Recombinant human IgG1 mono-clonal antibody; vascular endothelial growth receptor 2 inhibitor
Advanced HCC
Romosozumab-aqqg Evenity Monoclonal antibody (IgG2), inhibits sclerostin
Fracture prevention in post-menopausal women with osteoporosis
Siponimod Mayzent Sphingosine 1-phosphate receptor modulator
Secondary progressive and relapsing-remitting multiple sclerosis
Solriamfetol Sunosi Selective dopamine and norepineph-rine reuptake inhibitor
Excessive daytime sleepiness in nar-colepsy and obstructive sleep apnea
Tafamidis meglumine & tafamidis Vyndaqel & vyndamax Oral transthyretin stabilizer Wild-type cardiomyopathy or hereditary transthyretin-mediated amyloidosis
Table 1. 2019 FDA Approvals
Source: CenterWatch, 2019; Savarese & Zand, 2019; Wolters Kluwer, 2019
12
Patient Safety Alert: What to Know About Infiltration, Vesicants, and Extravasation
Peripheral Intravenous Catheters Ubiquitous in Nursing Care
Medical-surgical nurses commonly care for peripheral intravenous (PIV) catheters used for the delivery of fluids, medications, and chemotherapeutic agents. While some insti-tutions have dedicated IV teams, the bedside nurse is respon-sible for assessing and maintaining the IV site, identifying irri-tating medications, and adhering to the institution’s medication administration policies and guidelines. When an IV team is unavailable, bedside nurses also require education and practice in PIV placement, securement principles, and IV flushing protocols. In addition, nurses need to be aware of patient characteristics often associated with extravasation injuries:
Neonates and geriatric patients. •Diabetics. •Dialysis patients. •Limbs of patients with known vascular impairment and •edema. Mastectomy with axillary surgery and node dissection. •Raynaud’s Syndrome (Lateef, 2017). •
A PIV may seem like a routine device to facilitate nursing care, however, the nurse must be alert and use caution when delivering medications through a PIV to minimize the risk of infiltration and extravasation which may necessitate surgical intervention.
Infiltration versus Extravasation An infiltration and extravasation occur when fluid leaks
outside the vessel into the tissue. An extravasation can be more serious than an infiltration because the substance that has leaked is a vesicant. Vesicants are medications that have a pH that is outside the range compatible with a blood pH, either an acid (< 5.5) or a base (> 8.5) (Lateef, 2017). Vesicants are also defined as infusions with osmolarity > 290 mmol/L. Examples of hyperosmolar solutions include > 10% dextrose and 15% mannitol (Lateef, 2017).
Infiltration Injury An infiltration of a non-vesicant, such as normal saline,
may still cause serious patient injury. In the case of rapid infusion of large volumes, such as a resuscitation in an emer-
gency department or surgical procedure in the operating room, an infiltrate can lead to compartment syndrome due to increased extravascular pressure. The mechanical pres-sure caused by the large fluid infiltrate can weaken pulses, cause pain and edema at the site and surrounding tissues resulting in compartment syndrome. The patient may require a fasciotomy to alleviate compartment syndrome (AQI-AIRS Steering Committee, 2013). The AQI-AIRS Steering Committee (2013) recommends the use of clear or peeking below sterile drapes in the operating room to ensure the integrity of the PIV during surgery. The stakes can be high for the patient when an ‘out of sight, out of mind’ mentality is present in the operating room or other areas.
Continuum of an Extravasation Injury While a fasciotomy for an infiltration is certainly a seri-
ous event, extravasation injuries can result in loss of function and possible amputation. The mechanism of action in extrava-sation involves direct cellular toxicity and vasoconstriction (Lateef, 2017). The continuum of extravasation typically begins with leakage of the vesicant medication into surround-ing tissue first causing skin necrosis at the epidermal and der-mal layers, and then tissue necrosis at the subcutaneous level. Eventually, ulceration, gangrene, limb ischemia, and amputa-tion of the limb or digit can occur (Loubani & Green, 2015). Extravasation can extend to nerves, tendons, and joints and continue to cause pain and dysfunction for months after hos-pitalization.
Most extravasations occur in areas where there is min-imal soft tissue protection such as the dorsum of the hand, antecubital fossa, and near joints. According to a review of the National Extravasation Information Service in the United Kingdom, 44% of extravasations occurred on the evening shift, 38% on day shift, and 10% on night shift (Al-Benna, O’Boyle, & Holley, 2013). Many new post-operative patients are being admitted to nursing units on the evening shift after typically receiving liters of fluid in the operating room. It is essential that nurses know how to assess and monitor for extravasation and access institutional policies on extravasa-tion management.
Extravasation Identification The early stages of a PIV extravasation can be subtle,
leading to an effort to formalize extravasation identification
Safe Bedside Practice
If you have questions or comments regarding the “Safe Bedside Practice” column, or if you are interested in writing, please contact Column Editor Patricia J. Bartzak at [email protected]

13
through the use of a staging system. In general, the key parameters to consider when assessing potential extravasa-tion include patient discomfort, swelling, redness, pulses, blanching, coolness, induration, discoloration, skin break-down, and capillary refill greater than 3 seconds (Al-Benna et al., 2013). When a vesicant is infusing, the nurse should be monitoring the following symptoms and considering extrava-sation if any of the following develop:
Flare reaction: Itchy and blotchy skin at the PIV site. •Vessel irritation: Skin tightness. •Vessel shock: Muscular vessel wall spasms. •Hypersensitivity reaction: Hives (Lateef, 2017). •
Emergent Vasopressor Medications and Treatment
In the emergency room, the patient presenting with vol-ume depletion or sepsis with severe hypotension refractory to fluid repletion will likely need vasopressor support. Vasopressor medications that are known vesicants include norepinephrine, epinephrine, and dopamine (Lateef, 2017). Loubani and Green (2015) suggest that vasopressors infuse via PIV for less than 2 hours as a stop-gap measure while a central venous catheter (CVC) is started. Although vesicants infused through a CVC can cause injury, one study demon-strated vasopressors that run through PIVs were implicated in 204 local tissue injuries, while only four local injuries occurred when a CVC was used (Loubani & Green, 2015).
According to Plum and Moukhachen (2017), phento-lamine is the current standard treatment for vasopressor extravasation; however, this drug has been in short supply. Alternative medications to phentolamine include topical nitroglycerin and subcutaneous terbutaline. Symptom resolu-tion is best achieved when the antidote medications are administered within 2 hours of extravasation.
Vesicant Medication in the Medical-Surgical Setting
The nurse must take care when administering medica-tions characterized as vesicants and be knowledgeable about the associated antidote protocols. Vesicant medications com-monly used in the medical-surgical setting include van-comycin, phenytoin, gentamicin, and cefotaxime. In addition, the medical-surgical nurse will likely encounter calcium chlo-ride, calcium gluconate, and potassium chloride (Lateef, 2017). When an extravasation injury occurs with these med-ications, Lateef (2017) suggests that the nurse take the fol-lowing actions:
Stop the infusion. •Press over the site to express exudate. •Mark the area. •Document the time of injury, drug name, concentration, •and amount delivered. Elevate the limb. •A cold pack can be used for the medications listed above •but not for some chemotherapeutic medications, specifi-cally the vinca alkaloids. Begin neurovascular checks. •Follow institutional protocols and notifications. •
Medical-surgical nurses may also need to prepare the patient for a CT or MRI scan requiring contrast media that can extravasate when infused. It’s important for the nurse to check the catheter and determine if power injection of con-trast media is possible. Mohammed (2015) describes a case in which a patient had a #18 external jugular catheter that was injected with contrast media. Swelling was noted in the patient’s neck and upper thorax. The cannula was removed and the radiological procedure was terminated. A CT was performed without contrast and showed a large amount of contrast media in the retropharyngeal area that resulted in

Academy of Medical-Surgical Nurses www.amsn.org
14
shifting the trachea. The patient subsequently underwent excision and drainage to remove the contrast and release the tracheal compression (Mohammed, 2015).
Chemotherapeutic Medications on the Oncology Unit
Nurses who work on oncology units are well aware of the hazards of vesicant medications and often have compe-tency standards to meet. In addition, many oncology units have extravasation kits for chemotherapy (Lateef, 2017). Cytotoxic agents that can cause serious extravasation injuries include doxorubicin, mitomycin, vincristine, and vin-blastine. It is essential that oncology nurses know and follow their institutional protocols. The use of cold and heat are important for the nurse to distinguish in this setting. The vinca alkaloids, specifically vincristine and vinblastine, should be dispersed after an extravasation – hence the use of a warm pack. Whereas doxorubicin and mitomycin often
utilize a dry, cool compress after extravasation. Many oncol-ogy patients may have a CVC, but until one is placed, patients may receive chemotherapeutic agents via PIV in the interim.
Implications for Nursing A multi-pronged policy approach to prevent extravasation •can heighten awareness of extravasation injury that can occur in the everyday use of PIVs. Nurses can utilize their practice councils and best practice •committees to develop and enhance their extravasation toolkit. Development of an education competency, which identi-•fies offending medications, assessment criteria and treat-ment plans, may help minimize extravasation injuries. Education delivered during nursing orientation and •throughout employment provides essential updates as the science evolves and new drug treatments become avail-able.
Patricia J. Bartzak, DNP, RN, CMSRN, is a Nurse Educator, Milford Regional Medical Center, Milford, MA. She is also an Expert Nurse Witness.
References Al-Benna, S., O’Boyle, C., & Holley, J. (2013). Extravasation injuries in
adults. ISRN Dermatology, 1-8. doi:10.1155/2013/856541201906020008141105631471
AQI-AIRS Steering Committee. (2013). A case report from the Anesthesia Incident Reporting System. American Society of Anesthesiologists, 77(3), 28-3120190602000539694411516
Lateef, F. (2017). Extravasation: There could be more than meets the eye! Journal of Trauma and Critical Care, 1(1), 1-4.
Loubani, O.M., & Green, R.S. (2015). A systematic review of extravasation and local tissue injury from administration of vasopressors through peripheral intravenous catheters and central venous catheters. Journal of Critical Care, 30(3), e9-e17. doi:10.1016/j.jcrc.2015.01.014201906020018531082936406
Mohamed, M. (2015). Case report: Management of unusual site for contrast media extravasation in right external jugular vein. The Egyptian Journal of Radiology and Nuclear Medicine, 46(4), 1033-1035. doi:10.1016/j.ejrnm.2015.08.011
Plum, M., & Moukhachen, O. (2017). Alternative pharmacological management of vasopressor extravasation in the absence of phentolamine. P&T, 42(9), 581-585. 201906021507521165328264
AMSN Corporate Sponsors
www.philips.com/healthcare
www.wolterskluwer.com/www.lww.com
www.hcahealthcare.com/nurses
www.gehealthcare.com
www.dalemed.com
Gold Level
Silver Level
www.hillrom.com
15
Legislative Issues
The “Legislative Issues” column (formerly known as “Health Care Reform”) is a place to convey the voice of the nurse on issues surrounding health care policy, bills and laws impacting patients and professionals, and other governmental develop-ments. These articles are for you. Your voice matters.
If you have questions or comments regarding the “Legislative Issues” column, or if you are interested in writing, please contact Column Editor Yalanda Comeaux at [email protected].
Today, nursing professionals are called to be innovators, change makers, and leaders while delivering excellent nursing care; a calling designed to pave the way to healthcare reform (Institute of Medicine [IOM], 2010). Almost a decade since the IOM identified the nursing profes-sion as essential to healthcare reform, I wonder if nurses really understand the magnitude of this calling. Are nurses prepared to stand up and meet these expectations? Nursing engagement is fundamental to suc-cessful process improve-ment in healthcare, and Academy of Medical-Surgical Nurses (AMSN) membership is one method of promoting nursing engagement to meet the IOM’s calling for nurses “to lead change and advance health” (IOM, 2010, p.1).
AMSN membership elevates medical-surgical nursing care delivery by offering tools for certification, scholarship initiatives, professional development opportunities, grant funding, and medical-surgical nursing networking. As a clinical nurse leader (CNL) on a medical oncology telemetry unit, my effectiveness as a nurse leader and clinical expert is directly related to promoting nursing engagement. AMSN membership supports my efforts to lead and encourage engagement of bedside nurses focused on delivering up-to-date evidence-based nursing practices that promote improved patient outcomes and safety. Being certified in a specialty area formally recognizes clinical expertise based on knowledge, skills, and experience (American Board of Nursing Specialties, 2005). Through certification, I serve as a role model and demonstrate to nurses the benefits of being certified. The AMSN Hub communities are excellent resources for medical-surgical nurses to discuss common challenges, barriers, interventions, knowledge, etc. specific to medical-surgical units. The AMSN annual convention provides numerous opportunities for professional development by networking as well as sharing nursing innovations and quality improvement projects.
I made the choice to become certified and get involved in AMSN to elevate my nursing practice and develop my nursing leadership skills. As an AMSN member, I have had the
opportunity to build coalitions with other nursing legislative members, net-
work with nursing profes-sionals involved in devel-oping effective health policy, and disseminate my new legislative per-spectives and awareness to my work environ-ment. The opportunities I have had as a legislative team member helped transform me both pro-fessionally and person-ally. In my CNL role, I
utilize the resource tools available to me as an
AMSN member for up-to-date clinical knowledge, quality improvement processes, and leadership development.
Engagement is a choice; successful nurse leadership as a change agent hinges on promoting and empowering nursing engagement. A nurse leader must look beyond point of care issues to develop a global view on the interconnections, envi-ronments, and stakeholders within the existing complex healthcare system. AMSN membership captures this critical opportunity to encourage nursing engagement and promote professional development. Nurses who use AMSN member-ship as a method to be engaged have made the choice to ele-vate their nursing practice; they are meeting the IOM’s (2010) calling to lead change.
Chatty O’Keeffe, MSN-CNL, RN, CMSRN, is a Clinical Nurse Leader, VA Puget Sound Health Care System, Seattle, WA. She is also a Legislative Team Member. References American Board of Nursing Specialties. (2005). A position statement on
the value of specialty nursing certification. Birmingham, AL: Author. Institute of Medicine (IOM). (2010). The Future of nursing: Leading change,
advancing health. Retrieved from http://iom.national academies.org/~/media /F i les /Repor t%20Fi les /2010/The-Future-of -Nursing/Future%20of%20Nursing%202010%20Report% 20Brief.pdf
Engagement is a choice: What Every Medical Surgical Nurse Should Know About Advocacy and Leadership

AMSN BOARD OF DIRECTORS
President Robin A. Hertel, EdS, MSN, RN, CMSRN
Immediate Past President Linda Yoder, PhD, MBA, RN, AOCN, FAAN
Treasurer Summer Bryant, DNP, MSN, RN, CMSRN
Secretary Andie Melendez, MSN, RN, CHTP, HTCP, HSMI, RM
Director Marisa Streelman, MSN, RN, CMSRN
Director Michele George, MBA, BSN, RN
Director Jennifer Kennedy, MS, RN-BC, CMSRN
Director Kristi Reguin-Hartman, MSN, APRN, ACNS-BC
Chief Executive Officer Terri Hinkley, EdD, MBA, BScN, RN
Director, Association Services Suzanne Stott, BS
MedSurg Matters!
Editor Heather Craven, PhD, RN, CMSRN
Editorial Committee Millicent G. De Jesus, PhD, RN-BC
Deidra B. Dudley, DNS, MN, MS, RN-BC, NEA-BC
Dianne J. Gibbs, DNP, RN Stephanie Huckaby, MSN, RN-BC
Sally S. Russell, MN, RN, CMSRN Elizabeth Thomas, MSN, RN, ACNS-BC
Managing Editor Kaytlyn Mroz
Layout and Design Specialist Robert Taylor, AS
Education Director Michele Boyd, MSN, RN-BC
The purpose of MedSurg Matters! is to disseminate information that will provide or enhance nursing
knowledge, practice, and professional development related to medical-surgical nurses.
Box 56, Pitman, NJ 08071-0056 • 866-877-AMSN (2676) [email protected] • www.amsn.org
Volume 28 – Number 4 • July/August 2019
Please think GREEN and recycle!
www.twitter.com/MedSurgNurses
www.facebook.com/MedSurgNurses
AMSN is a dynamic community of medical-surgical nurses that are committed to quality patient care through professional development, certification, scholarship, and advocacy.