
Volume 24 • Number 3 In This Issue
20
Volume 24 • Number 3 November 2009 In This Issue Lesson 5 Nontraumatic Acute Increased Intracranial Pressure Page 2 The Drug Box Page 8 The LLSA Literature Review Page 9 Lesson 6 Evaluation and Treatment of Status Epilepticus Page 10 The Critical Image Page 17 CME Questions Page 18 The Critical ECG Page 20 Contributors Arleen Allen, MD, and Bernard L. Lopez, MD, MS, FACEP, wrote “Nontraumatic Acute Increased Intracranial Pressure.” Dr. Allen is a resident in emergency medicine at Thomas Jefferson University Hospital, Philadelphia, Pennsylvania. Dr. Lopez is vice chair of Academic Affairs, residency program director, and professor of emergency medicine at Thomas Jefferson University Hospital, Department of Emergency Medicine, in Philadelphia. George L. Sternbach, MD, FACEP, reviewed “Nontraumatic Acute Increased Intracranial Pressure.” Dr. Sternbach is a clinical professor of surgery at Stanford University Medical Center in Stanford, California, and an emergency physician at Seton Medical Center in Daly City, California. Julie J. Cooper, MD, and Michael A. Gisondi, MD, FACEP, wrote “Evaluation and Treatment of Status Epilepticus.” Dr. Cooper is a resident in emergency medicine at Northwestern University, Chicago, Illinois. Dr. Gisondi is associate residency director in the Department of Emergency Medicine at Northwestern University in Chicago. George L. Sternbach, MD, FACEP, reviewed “Evaluation and Treatment of Status Epilepticus.” Dr. Sternbach is a clinical professor of surgery at Stanford University Medical Center in Stanford, California, and an emergency physician at Seton Medical Center in Daly City, California. Frank LoVecchio, DO, MPH, FACEP, reviewed the questions for these lessons. Dr. LoVecchio is research director at the Maricopa Medical Center Emergency Medicine Program and medical director of the Banner Poison Control Center, Phoenix, Arizona, and a professor at Midwestern University/Arizona College of Osteopathic Medicine in Glendale, Arizona. Louis G. Graff IV, MD, FACEP, is Editor-in-Chief of Critical Decisions. Dr. Graff is professor of traumatology and emergency medicine at the University of Connecticut School of Medicine in Farmington, Connecticut. Contributor Disclosures In accordance with ACCME Standards and ACEP policy, contributors to Critical Decisions in Emergency Medicine must disclose the existence of significant financial interests in or relationships with manufacturers of commercial products that might have a direct interest in the subject matter. Authors and editors of these Critical Decisions lessons reported no such interests or relationships. Method of Participation This educational activity consists of two lessons with a posttest and should take approximately 5 hours to complete. To complete this educational activity as designed, the participant should, in order, review the learning objectives, read the lessons, and complete the online posttest. Release date May 1, 2009. Expiration date April 30, 2012. Accreditation Statement The American College of Emergency Physicians (ACEP) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. ACEP designates this educational activity for a maximum of 5 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity. Approved by ACEP for 5 Category I credits. Approved by the American Osteopathic Association for 5 hours of AOA Category 2-B credit (requires passing grade of 70% or better). Target Audience This educational activity has been developed for emergency physicians. n Next Month Fever in Returning Travelers • High-Altitude Illness •
Transcript of Volume 24 • Number 3 In This Issue

Volume 24 • Number 3
November
2009
In This IssueLesson 5 Nontraumatic Acute Increased Intracranial Pressure . . . . . . . . . Page 2 The Drug Box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Page 8 The LLSA Literature Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Page 9 Lesson 6 Evaluation and Treatment of Status Epilepticus . . . . . . . . . . . . Page 10 The Critical Image . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Page 17 CME Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Page 18 The Critical ECG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Page 20
ContributorsArleen Allen, MD, and Bernard L. Lopez, MD, MS, FACEP, wrote “Nontraumatic Acute Increased
Intracranial Pressure.” Dr. Allen is a resident in emergency medicine at Thomas Jefferson University Hospital, Philadelphia, Pennsylvania. Dr. Lopez is vice chair of Academic Affairs, residency program director, and professor of emergency medicine at Thomas Jefferson University Hospital, Department of Emergency Medicine, in Philadelphia.
George L. Sternbach, MD, FACEP, reviewed “Nontraumatic Acute Increased Intracranial Pressure.” Dr. Sternbach is a clinical professor of surgery at Stanford University Medical Center in Stanford, California, and an emergency physician at Seton Medical Center in Daly City, California.
Julie J. Cooper, MD, and Michael A. Gisondi, MD, FACEP, wrote “Evaluation and Treatment of Status Epilepticus.” Dr. Cooper is a resident in emergency medicine at Northwestern University, Chicago, Illinois. Dr. Gisondi is associate residency director in the Department of Emergency Medicine at Northwestern University in Chicago.
George L. Sternbach, MD, FACEP, reviewed “Evaluation and Treatment of Status Epilepticus.” Dr. Sternbach is a clinical professor of surgery at Stanford University Medical Center in Stanford, California, and an emergency physician at Seton Medical Center in Daly City, California.
Frank LoVecchio, DO, MPH, FACEP, reviewed the questions for these lessons. Dr. LoVecchio is research director at the Maricopa Medical Center Emergency Medicine Program and medical director of the Banner Poison Control Center, Phoenix, Arizona, and a professor at Midwestern University/Arizona College of Osteopathic Medicine in Glendale, Arizona.
Louis G. Graff IV, MD, FACEP, is Editor-in-Chief of Critical Decisions. Dr. Graff is professor of traumatology and emergency medicine at the University of Connecticut School of Medicine in Farmington, Connecticut.
Contributor DisclosuresIn accordance with ACCME Standards and ACEP policy, contributors to Critical Decisions in Emergency Medicine must
disclose the existence of significant financial interests in or relationships with manufacturers of commercial products that might have a direct interest in the subject matter. Authors and editors of these Critical Decisions lessons reported no such interests or relationships.Method of Participation
This educational activity consists of two lessons with a posttest and should take approximately 5 hours to complete. To complete this educational activity as designed, the participant should, in order, review the learning objectives, read the lessons, and complete the online posttest. Release date May 1, 2009. Expiration date April 30, 2012.Accreditation Statement The American College of Emergency Physicians (ACEP) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. ACEP designates this educational activity for a maximum of 5 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity. Approved by ACEP for 5 Category I credits. Approved by the American Osteopathic Association for 5 hours of AOA Category 2-B credit (requires passing grade of 70% or better).Target Audience This educational activity has been developed for emergency physicians.
n Next MonthFever in Returning Travelers•
High-Altitude Illness•

Critical Decisions in Emergency Medicine
2
Lesson 5
Arleen Allen, MD, and Bernard L. Lopez, MD, MS, FACEP
Nontraumatic Acute Increased Intracranial Pressure
n ObjectivesOn completion of this lesson, you should be able to:
Discuss causes and presentations of 1. nontraumatic increased intracranial pressure (ICP).
Describe the pathophysiology of 2. increased ICP as it relates to the disease entities.
Detail the diagnosis of increased 3. ICP and its different entities.
Discuss the role of neuroimaging 4. in evaluating ventriculoperitoneal shunts.
Discuss management of increased 5. ICP.
Discuss the major complication of 6. idiopathic intracranial hypertension.
n From the EM Model12.0 Nervous System Disorders
12.4 Hydrocephalus
Disorders of acute elevations in increased intracranial (ICP) offer a challenge for emergency physicians and require an understanding of the physiology behind the disorders, the diagnostic modalities, and the nuances of management. Patients with elevated ICP can rapidly deteriorate and are at significant risk for vision loss, brain herniation, and death.
This lesson will review three causes of nontraumatic increased ICP: idiopathic intracranial hypertension (formerly pseudotumor cerebri), shunt malfunction, and acute hydrocephalus. It will examine the major complications and some of the controversies in diagnosis and management, including the utility of neuroimaging in shunt malfunction and alterations in rapid sequence intubation.
Case Presentations
n Case OneA 35-year-old woman presents to
the emergency department because she has been having intermittent headaches for 6 months to a year. The headaches usually resolve with acetaminophen, ibuprofen, or rest. She has noticed that in the past 3 months the headaches have been increasing in intensity, the medications are not as helpful, and she will occasionally get a ringing in her ears. What concerns her most, however, is that she is often seeing double and feels like there is a haze in the corners of her vision.
On physical examination, the patient is mildly obese, alert, and in no distress. Head is normocephalic and atraumatic. She has mild horizontal nystagmus with extraocular movements intact. Her neck is supple. Neurologically, the patient has intact cranial nerves, sensation, and cerebellar function, with full strength throughout.
Results of her laboratory evaluation, including a CBC and electrolyte panel, are within normal limits. A urine pregnancy test is negative. A noncontrast computed tomography (CT) scan of the head shows no intracranial hemorrhage or mass effect.
The patient is given 1 liter of intravenous normal saline, prochlorperazine, and ketorolac, with subsequent resolution of her headache. She is discharged home with a diagnosis of headache of unknown origin and told to follow up with her primary physician.
n Case TwoA 54-year-old man with a history
of subarachnoid hemorrhage (SAH) complicated by hydrocephalus presents to the emergency department because he “passed out.” He had a ventriculoperitoneal (VP) shunt placed 2 years ago. He reports that 1 hour prior to presentation he was walking to the bathroom when he felt a posterior headache, not as intense as when he had SAH, but “pretty bad.” He called out to his daughter and slid to the floor, landing on his buttocks.

November2009•Volume24•Number3
3
He did not hit his head and had no loss of consciousness; the headache is now lessening in intensity.
On physical examination, the patient is alert and resting comfortably. Vital signs are blood pressure 148/85, pulse rate 75, respiratory rate 16, and temperature 36.6°C (97.9°F). The head is normocephalic and atraumatic. The neck is supple. Mucous membranes are dry. Breath sounds are clear. Heart sounds are normal, without murmur, rub, or gallop. The patient is alert and oriented to person, time, and place; cranial nerves II through XII are intact, without focal neurologic deficits. Motor strength is 5/5 throughout, sensation is intact to light touch, and cerebellar function is intact.
Results of the laboratory evaluation, including a CBC and electrolyte panel, are normal. An ECG is unremarkable, with normal sinus rhythm and no ischemic changes. A noncontrast CT scan of the head shows an unchanged enlarged ventricle size, no intracranial hemorrhage, and no mass effect. A shunt survey shows no disconnection, migration, or kinking of tubing.
After receiving 1 liter of normal saline intravenously and acetaminophen, 1,000 mg, the patient reports that his headache has resolved. He has called his wife to pick him up and wants to leave the emergency department.
n Case ThreeA 51-year-old man with a history
of hypertension and squamous cell carcinoma of the tongue and
larynx who recently had surgical resection, chemotherapy, and radiation is brought in via ambulance accompanied by his wife and son. For the past 2 weeks the patient has had fever and headaches. He was seen by his family physician who prescribed an unknown antibiotic and analgesics. For the past few days he has not been acting like himself and his speech has been incoherent; today he stopped speaking. This morning he was found lying on the floor after an unwitnessed fall.
On physical examination, the patient is awake, alert, and nonverbal. Vital signs are blood pressure 230/95, pulse rate 90, respiratory rate 12, and oral temperature 38.9°C (102°F). The head is normocephalic and atraumatic. Pupils are equal, round, and reactive to light. There is minimal tracking for extraocular movements. The patient does not follow commands but is moving all extremities, with strength testing 3/5 throughout.
Laboratory evaluation is significant for a WBC count of 39,000 and lactate of 30 mg/dL (normal is 4.5-19.8 mg/dL). The electrolyte panel results are within normal limits. A noncontrast CT scan of the brain shows new hydrocephalus with dilation of the lateral ventricles, the third ventricle, and possibly the fourth ventricle.
During the course of the emergency department evaluation, the patient has further neurologic deterioration, becoming unresponsive.
An understanding of changes in ICP stems from an understanding of intracranial mechanics. The brain,
blood, and cerebrospinal fluid (CSF) are housed in the fixed spaces of the cranium and vertebral column. Any increases in the volume of the brain, blood, or CSF causes an increase in the ICP. Pressures greater than 25 mm Hg are considered “increased,” although adequate cerebral perfusion can be maintained at an ICP of up to 40 mm Hg if blood pressure remains normal.1 If CSF flow is impaired within the ventricular system (eg, mass lesions, stenotic lesions, or intraventricular hemorrhage), this can result in hydrocephalus, defined as an increase in volume and subsequent pressure. Alternatively, hydrocephalus can also occur with CSF impairment outside the ventricular system at the level of the arachnoid granulations or basal cisterns (eg, resulting from bacterial meningitis, SAH, spinal cord tumors).
The most common cause of acute hydrocephalus is infection, most often bacterial meningitis.2 It often occurs several weeks after initial presentation but has been known to develop within days. Cerebellar encephalitis and neurocysticercosis can also be infectious causes. The second most common cause of hydrocephalus is intracranial hemorrhage, most often subarachnoid hemorrhage.
Finally, idiopathic intracranial hypertension (also known as pseudotumor cerebri) is the term used to describe increased ICP in the absence of an identifiable cause such as tumor or infection. Idiopathic intracranial hypertension can have various etiologies or associations including medications such as tetracycline and retinoids,
What findings suggest increased ICP?•How useful are shunt series and brain computed •tomography in assessing patients with ventriculoperitoneal shunt malfunctions?
What role do lumbar punctures, shunt taps, and •ventriculostomy have in the emergent management of increased ICP? How does the management of idiopathic intracranial •hypertension differ from the management of other causes of increased ICP?
Critical Decisions

Critical Decisions in Emergency Medicine
4
vitamin A toxicity, and diseases of endocrinology, including thyroid disease. There are several theories explaining the development of this entity; a common theory is that obstruction of flow through the arachnoid villi or venous sinuses causes an increase in pressure without an increase in volume.3
CRITICAL DECISIONWhat findings suggest increased ICP?
How a patient presents clinically depends both on the patient’s age and the mechanism of the intracranial hypertension. Infants with acute hydrocephalus often present with head enlargement greater than 97th percentile, bulging or tense fontanelles, nausea and vomiting, poor feeding and failure to thrive, failure of upward gaze (“sunset eyes”), irritability, and a depressed level of consciousness. In a study by Piatt and Gorton,4 bulging fontanelles had the highest association with increased ICP in the setting of shunt malfunction, followed by depressed level of consciousness and irritability. Furthermore, the absence of irritability, headache, and nausea/vomiting greatly reduces the likelihood of shunt failure. In children and adults, clinical manifestations of increased ICP include headache, nausea and vomiting, sleepiness, confusion, ataxia, ocular palsies, tinnitus, and papilledema. The Cushing triad of hypertension, bradycardia, and irregular respirations is a late finding indicating impending herniation or marked intracranial hypertension. Decerebrate or decorticate posturing is an even later sign.
In idiopathic intracranial hypertension, the classic patient is an obese woman of childbearing age who presents with headaches and visual symptoms. However, it can affect children, men, and thin individuals. The headache varies considerably and can be a frontal, retro-ocular, or pressure headache, and it can
have migrainous features (throbbing, photophobia, phonophobia, nausea) or a presentation suggestive of SAH (worst headache of one’s life). Vision obscurations (partial or complete visual loss lasting seconds at a time) occur in 75% of patients and tinnitus in 50%. But the hallmark of the condition is papilledema, which is often bilateral but can be unilateral.5
The physical examination should include an assessment of the external head to rule out suspected traumatic causes of elevated ICP. The eyes must be examined thoroughly, including assessing pupil reactivity, shape, and equality; extraocular movements should be checked for palsies and visual field constrictions; and finally the fundi should be examined for papilledema. A thorough neurologic examination should be performed, including assessment of mentation, cranial nerves, motor and sensation, and cerebellar function. In life-threatening situations, the evaluation should be narrowed to an assessment of mental status using the Glasgow Coma Scale (GCS) and a pupillary assessment.6
Laboratory evaluation is nonspecific for the etiology or diagnosis of elevated ICP. A noncontrast CT scan of the brain is the initial imaging recommended. It is helpful in examining ventricle size, intracranial hemorrhage, masses, and mass effect. In the case of shunt malfunction, a radiographic shunt series can reveal shunt migration, disconnection, or kinking. The shunt series comprises views of the anterior, posterior, and lateral skull; anterior and posterior chest; and anterior and posterior abdomen.
CRITICAL DECISIONHow useful are shunt series and brain CT in assessing patients with shunt malfunctions?
In a retrospective study of 280 children with shunts presenting to a Toronto emergency department, Mater and colleagues7 looked at the utility of shunt series and brain CT
in identifying shunt malfunction by correlating these studies with subsequent shunt revision. They found that abnormal shunt series readings had a sensitivity of 30%, a specificity of 95.8%, a positive predictive value (PPV) of 72.3%, and a negative predictive value (NPV) of 75.1%. Abnormal brain CT readings had a sensitivity of 61%, a specificity of 82.7%, a PPV of 64.5%, and an NPV of 80.5%. These findings suggest that neuroimaging, which is routinely performed to exclude life-threatening complications, is insensitive and has poor predictive value.
Zorc and colleagues8 retrospectively studied 140 children with shunts presenting to a Philadelphia emergency department, looking at the shunt series, brain CT, and both in combination. Results again showed poor sensitivity (20% in shunt series, 83% in brain CT, and 88% in combination) and predictive value (75%, 55%, and 55% respectively). In adults, Griffey and colleagues9 performed a retrospective review of 192 patients presenting to a Boston emergency department. Again, these studies were found to have poor sensitivity (11% shunt series, 52% brain CT, and 57% combination) and predictive value (56%, 33%, and 33%, respectively).
In both children and adults, both shunt series and brain CT, in isolation or in combination, have been shown to have poor correlative characteristics with shunt malfunction. These findings bring into question whether these expensive and potentially harmful imaging studies are useful for emergency physicians. However, evaluating a shunt clinically is often difficult as well. Isaacman and Poirer10 presented three case studies of children with shunts with varied symptoms of headache, vomiting, and neck stiffness and asked three emergency physicians to discuss management. They conclude that results of the history and physical examination are often inconclusive. Despite

November2009•Volume24•Number3
5
various studies that have looked at clinical findings in relation to shunt malfunction, no set of clinical factors reliably predicts shunt malfunction.10 Thus, because both clinical findings and radiological studies are unreliable in identifying shunt malfunction, neurosurgical consultation should be sought when there is persistent clinical concern despite a negative workup.
ManagementIn general, once the diagnosis
of elevated ICP has been made, the goal of management is to prevent secondary insult (eg, herniation and death in acute shunt malfunction and hydrocephalus and vision loss in idiopathic intracranial hypertension). In milder cases (headache, normal level of consciousness, no neurologic deficit), management centers on analgesia and diagnostic studies. In more severe cases in which consciousness is altered or neurologic deficits are present, airway control and ventilator management must be considered.
Early endotracheal intubation and controlled ventilation are important—hypoxia and hypercarbia adversely affect cerebral perfusion pressure. Induction agents are important even in patients with GCS scores lower than 8, because induction agents blunt hemodynamic fluctuations that come with laryngoscopy and intubation. Meyer and colleagues6 recommend rapid sequence induction (RSI) with thiopental and succinylcholine/rocuronium in the hemodynamically stable patient and etomidate/ketamine and succinylcholine/rocuronium in unstable patients. Thiopental, propofol, and etomidate all reduce ICP. Although succinylcholine can cause a transient increase in ICP, the clinical relevance of this has not been established, and its use is not contraindicated.11 Furthermore, Clancy et al in a literature search could find no evidence that succinylcholine caused a detectable
change in ICP in patients with acute trauma or bleeds.12
There is conflicting evidence about whether lidocaine should be used as pretreatment in RSI for patients with elevated ICP. Lidocaine is a fast sodium channel blocker whose exact mechanism for preventing increases in blood pressure is unclear, but when it is given at a dose of 1.5 mg/kg it is known to suppress the cough reflex, preventing elevation in ICP. One set of authors13 opposes its use given the lack of direct evidence (its use is often inferred from studies with tracheal suctioning rather than endotracheal intubation). Moreover, they note that lidocaine takes several minutes to provide its blunting effect, which can be deleterious in a rapidly decompensating patient who needs an emergent airway. And, when it does take it effect, it can cause a sustained decreased in mean arterial pressure and subsequent perfusion pressure. Caro and Bush continue to recommend its use based on its cough suppression effect and especially when no neuromuscular blockade is given.14 Fentanyl, 1 to 3 mcg/kg, is also recommended as possible pretreatment to blunt ICP. Routine use of atropine in children and a defasciculating small dose of a competitive neuromuscular blocker in conjunction with succinylcholine administration are no longer recommended.
With respect to ventilation, there is debate about the utility of hyperventilation therapy in decreasing ICP. Hyperventilation reduces ICP by causing vasoconstriction and a reduction in cerebral blood flow, which in turn can cause ischemic consequences. A Cochrane review15 concluded that data are inadequate to assess either potential harm or benefit. A recent neurosurgical workgroup16 details guidelines for using hyperventilation in elevated ICP. It should not be used routinely or prophylactically. If hyperventilation is used, it should only be a temporizing measure,
but not in the first 24 hours after intubation, as the brain is more subject to insult during that period.
To further decrease ICP, mannitol or hypertonic saline solution is used. Mannitol is given in a 20% rapid infusion. It acts by inducing water transfer and decreasing total brain water content and volume. Mannitol also acts by a reflex vasoconstriction to reduce ICP.
CRITICAL DECISIONWhat role do lumbar punctures, shunt taps, and ventriculostomy have in the emergent management of increased ICP?
All of these procedures act to measure and reduce ICP. The lumbar puncture can be a fatal procedure in a patient with increased ICP because of the risk for cerebral herniation. It should only be performed in neurologically intact patients with no papilledema and a brain CT showing no mass effect. There are four radiographic findings indicative of increased ICP: midline shift, obstructive hydrocephalus, compression of basilar cisterns, and compression of fourth ventricle.17
The lumbar puncture is useful in chronic VP shunt patients with communicating hydrocephalus and concern for meningitis. Patients with VP shunts can have compartmentalization of CSF, allowing infection to occur in the ventricles but not in the meninges, and vice versa. With communicating hydrocephalus, pressures between intracranial compartments are equal and lumbar puncture is thought to be safe. However, herniation has occurred in patients with meningitis who had “normal” CT scans.17 Therefore, following lumbar puncture, such patients should be closely monitored for signs of neurologic deterioration. The lumbar puncture is also the definitive diagnostic modality in idiopathic intracranial hypertension; CSF analysis will be normal except for an elevated opening pressure (above 20 cm H2O in a thin

Critical Decisions in Emergency Medicine
6
patient, above 25 cm H2O in an obese patient).
A shunt tap is a percutaneous needle aspiration of ventricular CSF. It is indicated in patients with VP shunts and concern for ventriculitis, and more importantly it is decompressive therapy in the setting of increased ICP. The main risks of the procedure are introduction of infection, brain edema, and intraparenchymal bleeding. The first can be prevented by strict aseptic procedure, the last two by avoiding rapid removal of CSF.
Ventriculostomy is indicated for the critical, rapidly declining patient with increased ICP from acute hydrocephalus or massive intraventricular hemorrhage. It offers a temporizing measure for diversion of fluid or blood until definitive surgical intervention can take place. Its major complication is infection, most often secondary to skin flora contamination.
CRITICAL DECISIONHow does the management of idiopathic intracranial hypertension differ from the management of other causes of increased ICP?
Once the diagnosis of idiopathic intracranial hypertension has been made (ie, elevated opening pressure with normal neuroimaging), the goal of management is to preserve vision. Papilledema can occur early in the course of idiopathic intracranial hypertension—even before the patient becomes symptomatic with visual obscurations.5 Papilledema is often difficult to detect with direct ophthalmoscopy, and ophthalmology consultation is often needed. Visual changes include constriction of field (central vision is usually involved late), blind spots, diplopia, and blurred vision. The major concern is that papilledema can lead to optic nerve atrophy and blindness. Spontaneous recovery is common (70%), but optic nerve atrophy and blindness can also recur (10% in 1 year, 40% in 6 years, 15% in 13
years).3 Blindness occurs in 5% to 10%—unilateral or bilateral. The risk of blindness is related to the duration of papilledema and the rate of developing optic atrophy. Rarely does blindness occur within a few days.3
Once emergencies such as meningitis and subarachnoid hemorrhage have been excluded, a patient with idiopathic intracranial hypertension can be managed in an outpatient setting. Medical management includes weight loss counseling, acetazolamide, and corticosteroids. Acetazolamide is first-line drug treatment. It is a carbon anhydrase inhibitor that acts to reduce CSF production and thus ICP. Furosemide can be an adjunct if the effects of acetazolamide are insufficient or the side effects are intolerable. Oral corticosteroids are often considered in the short term (1 to 2 mg/kg for 2 to 6 weeks) for acute severe cases, but there is a risk of weight gain.
Surgery (shunt procedure or optic nerve fenestration) is indicated when visual deterioration and disabling headaches persist despite medical treatment. It is not recommended for headaches alone. Shunting is usually lumboperitoneal rather than ventriculoperitoneal. Shunting carries the risk of overdrainage, which can result in low-pressure headaches, tonsillar herniation, lumbar radiculopathy, and shunt failure.
Optic nerve sheath fenestration is thought to work by immediate lowering of the CSF pressure in the subarachnoid space surrounding the optic nerve. Later, scarring of the fenestration can protect against transfer of the increased ICP from the sheath to the optic nerve. Most patients (two thirds) will achieve initial relief of headache and improvement or stabilization of visual function. There is a risk, however, of later deterioration of visual function and central retinal artery occlusion.3
Emergency department management is based on symptoms. If patients are asymptomatic,
PearlsCushing triad is a late •sign of elevated ICP.
The hallmark of idiopathic •intracranial hypertension is papilledema.
The shunt series and brain CT •have been shown over several studies to have poor sensitivity and predictive value for identifying shunt malfunction.
Even in the obtunded patient, •rapid sequence intubation should be performed to blunt elevations in ICP.
Routine atropine and •defasciculating doses of a competitive paralytic are no longer recommended to blunt ICP elevation.
Hyperventilation should •not be used routinely or prophylactically in elevated ICP, and it should never be used acutely in the first 24 hours.
PitfallsNot doing an ophthalmoscopic •examination.
Assuming that negative •shunt series and negative brain CT rule out shunt malfunction; half of patients with a shunt malfunction requiring shunt revision will not have a positive test.
Not involving specialists when •clinical concern persists for shunt malfunction or idiopathic intracranial hypertension.
Performing a lumbar •puncture in a patient with increased ICP can result in cerebral herniation.

November2009•Volume24•Number3
7
they should be educated and referred to a specialist (neurology or ophthalmology). Symptomatic headache patients should be given analgesics, and initiation of acetazolamide should be considered in consultation with a neurologist or ophthalmologist. Patients with severe or rapid optic neuropathy should be admitted with specialist consultation and attempts at reduction of ICP (acetazolamide, mannitol).
Case Resolutions
n Case OneOne month later, this patient
returned with worsening headaches and vision changes. The morning of this visit she noticed that she could not see anything for several seconds before her vision returned. She made an appointment to see her primary physician but he was not available for 2 months. On this visit, the emergency physician detected papilledema on ophthalmoscopic examination. A lumbar puncture was performed and revealed an opening pressure of 28 cm H2O, but results of CFS analysis were otherwise normal. The on-call neurologist was consulted by phone, and the patient was started on topiramate for analgesia and acetazolamide and given an appointment to see the neurologist in 2 days for further neuroimaging. On discharge, the patient’s headache had improved and her visual obscurations had not returned. She was given instructions on idiopathic intracranial hypertension, counseled on the benefits of weight loss, and informed of the risk of permanent visual changes and possible loss of vision with her condition.
n Case TwoThe patient agreed to wait until the
emergency physician could discuss the case with his neurosurgeon. The neurosurgeon had several concerns—syncope, shunt malfunction, and new subarachnoid hemorrhage. The patient and his wife agreed to hospital admission. Results of a cardiac
workup (serial cardiac enzymes, echocardiogram, and neuroimaging [including magnetic resonance imaging, magnetic resonance angiography, and magnetic resonance venography of the brain and neck]) were normal. The VP shunt was tapped and revealed normal opening pressure and CSF analysis; a shunt revision was not performed. The patient was discharged home 2 days later with a diagnosis of vasovagal syncope.
n Case ThreeThis patient was presumed to
have acute obstructive hydrocephalus secondary to meningitis. Rapid sequence intubation was performed with etomidate and succinylcholine. No lidocaine or fentanyl was used for pretreatment. No hyperventilation was performed. The patient was started on broad-spectrum antibiotics. Neurosurgery was called for emergent ventriculostomy for decompression and CSF analysis. The opening pressure was more than 50 cm H2O, and CSF analysis revealed a WBC count of 540 with a neutrophilic predominance of 82%, an RBC count of 6, normal glucose, and normal protein. In the neurosurgical ICU, the patient, who had initially been hypertensive, became hypotensive, requiring vasopressors. Magnetic resonance imaging of the brain showed extensive leptomeningeal, parenchymal, and bone enhancement with concern for ventriculitis, osteomyelitis of the skull, and multiple areas of infarction in the cerebellum and midbrain. Two sets of blood cultures grew out after only 2 days with Streptococcus intermedius. Despite antibiotics guided by consultation with an infectious disease specialist and vasopressor support, the patient’s neurologic status and prognosis continued to remain poor. The patient was placed under comfort care by his family, and 2 days after presentation to the emergency department he died.
SummaryAcute elevations in ICP can cause
significant morbidity and mortality. Emergency physicians must have an understanding of the different diagnostic modalities and their utility. An ophthalmoscopic examination is vital in diagnosis and should not be forgotten in the workup of patients with increased ICP. A noncontrast brain CT is the appropriate imaging starting point. Specialist consultation and involvement are important, especially when clinical concern persists despite negative neuroimaging or negative direct ophthalmoscopy.
Emergency physicians must also be aware of the alterations in management with respect to rapid sequence intubation, ventilation, and decompressive therapy in patients with elevated ICP. There is on-going debate in the literature about pretreatment with lidocaine; but succinylcholine is considered safe, and hyperventilation is no longer recommended in acute management. The lumbar puncture is to be deferred with findings of mass effect on neuroimaging. Finally, for patients with confirmed or suspected idiopathic intracranial hypertension, appropriate, close, outpatient followup arrangements should be made.
ReferencesRopper AH, Brown RH. Disturbances of cerebrospinal 1. fluid and its circulation, including hydrocephalus, pseudotumor cerebri, and low-pressure syndromes. In: Adams and Victor’s Principles of Neurology. 8th ed. New York, NY: McGraw-Hill; 2005:529-545.
Nasr FF, Honeycutt JH. Management of acute 2. hydrocephalus. In Loftus CM, ed: Neurosurgical Emergencies. 2nd ed. New York, NY: Theime; 2008:27-33.
Skau M, Brennum J, Gjerris F, Jensen R. What is 3. new about idiopathic intracranial hypertension? An updated review of mechanism of treatment. Cephalalgia. 2006;26:384-399.
Piatt JH, Garton HJL. Clinical diagnosis of 4. ventriculoperitoneal shunt failure among children with hydrocephalus. Pediatr Emerg Care. 2008;24(4):201-210.
Friedman DI. Idiopathic intracranial hypertension. 5. Curr Pain Headache Rep. 2007;11:62-68.
Meyer PG, Ducrocq S, Carli P. Pediatric neurologic 6. emergencies. Curr Opin Crit Care. 2001;7:81-87.
Mater A, Shroff M, Al-Farsi S, et al. Test characteristics 7. of neuroimaging in the emergency department evaluation of children for cerebrospinal fluid shunt malfunction. CJEM. 2008;10:131-135.

Critical Decisions in Emergency Medicine
8
Zorc J, Krugman S, Ogborn J, Benson J. Radiographic 8. evaluation for suspected cerebrospinal fluid shunt obstruction. Pediatr Emerg Care. 2002;18:337-340.
Griffey R, Ledbetter S, Khorasani R. Yield and utility 9. of radiographic “shunt series” in the evaluation of ventriculo-peritoneal shunt malfunction in adult emergency patients. Emerg Radiol. 2007;13:307-311.
Isaacman DJ, Poirier MP, Hegenbarth M, et al. 10. Ventriculoperitoneal shunt management. Pediatr Emerg Care. 2003;19:119-125.
Danzl DF, Vissers RJ. Tracheal intubation and 11. mechanical ventilation. In: Tintinalli JE, Kelen GD, Stapczynski JS, eds. Emergency Medicine: A Comprehensive Study Guide. 6th ed. New York, NY: McGraw-Hill; 2004:108-119.
Clancy M, Halford S, Walls RM, Murphy M. In patients 12. with head injuries who undergo rapid sequence intubation using succinylcholine, does pretreatment with a competitive neuromuscular blocking agent improve outcome? A literature review. Emerg Med J. 2001;18(5):373–375.
Salhi B, Stettner E. In defense of the use of lidocaine 13. in rapid sequence intubation. Ann Emerg Med. 2007;49(1):84-86.
Caro DA, Bush S. Pretreatment agents. In: Walls RM, 14. Murphy MF, Luten RC, eds. Manual of Emergency Airway Management. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:222-232.
Roberts IG, Schierhout G. Hyperventilation therapy 15. for acute traumatic brain injury. Cochrane Database of Systematic Reviews. 1997, Issue 4. Art. No.: CD000566. DOI: 10.1002/14651858.CD000566.
Brain Trauma Foundation, American Association of 16. Neurological Surgeons, Congress of Neurological Surgeons, et al. Guidelines for the management of severe traumatic brain injury. XIV. Hyperventilation. J Neurotrauma. 2007;24(1):S87-S90.
Schwartz DT. Hydrocephalus—use of CT before LP. In: 17. Emergency Radiology: Case Studies. New York, NY: McGraw-Hill; 2007:487-497.
Additional ReadingsLueck C, McIllwaine G. Interventions for idiopathic
intracranial hypertension. Cochrane Database of Systematic Reviews. 2005, Issue 3.
Rangwala L, Liu G. Pediatric idiopathic intracranial hypertension. Surv Ophthalmol. 2007;52:597-612.
Shah SM, Kelly KM, eds. Increased intracranial pressure, Chapter 26; Normal pressure hydrocephalus, Chapter 28; Hydrocephalus and shunts in children, Chapter 34. Emergency Neurology Principles and Practice. New York, NY: Cambridge University Press; 1999:378-380.
Shah VA, Kardon RH, Lee AG, et al. Long-term follow-up of idiopathic intracranial hypertension: the Iowa experience. Neurology. 2008;70:634-640.
Tabassi K, Silvestre CG. Management of increased intracranial pressure and intracranial shunts. In: Roberts JR, Hedges JR, eds: Clinical Procedures in Emergency Medicine. 4th ed. Philadelphia, PA: Elsevier Science; 2004:1185-1196.
AcknowledgmentThe authors would like to thank Dr. H. Edward Seibert and Dr. Timberly Booker for the use of case three. It informed this lesson greatly on the significant morbidity and mortality that can arise with increased intracranial pressure.
The Drug Box
Phenytoin
Mechanism of Action Limits seizure spread and propagation via sodium channels in the neuronal cell membrane
Indications Treatment of active seizure or status epilepticus; seizure prophylaxis
Dosing Children and adults: 15-20 mg/kg IV; repeat 5-10 mg/kg IV if seizure persistsMaximum loading dose: 30 mg/kg PO or IV*Nonemergent loading dose: 15-20 mg/kg PO given as 400 mg PO every 2-3 hours30-mg, 50-mg, and 100-mg tablets available*Never exceed an IV administration rate of 50 mg/minute
Side Effects Dizziness, drowsiness, suicidal ideation, mood changes, hypoglycemia
Estimated Cost to Hospital and Patient
Oral form available through most $4 prescription plansIV: $1 to $10 depending on dose
Contraindication/Precautions Hypersensitivity to barbituratesSecreted in breast milk (avoid when breastfeeding)Pregnancy category DDiscontinue immediately if rash develops
Phenytoin
By Amy Niertit, MD; Summa Health System Emergency Medicine Residency
Although most seizures encountered in the emergency department can be easily controlled by benzodiazepines, emergency physicians should also be familiar with phenytoin . In addition to its use in status epilepticus, it is frequently encountered on a patient’s medication list, and emergency physicians should be able to recognize signs of phenytoin toxicity . Common signs of toxicity are nystagmus, vertigo, vomiting, confusion, tremor, and hypotension . Most emergency department laboratories are able to provide a phenytoin level from a simple blood sample .
Feature Editor: Michael S . Beeson, MD, FACEP

November2009•Volume24•Number3
9
The LLSA Literature Review“The LLSA Literature Review” summarizes articles from ABEM’s “2010 Lifelong Learning and Self-Assessment Reading List.”
Many of these articles are available online in the ACEP LLSA Resource Center (www.acep.org/llsa) and on the ABEM web site.
Assessment of Patients’ Competence to Consent to TreatmentReviewed by Kalpana Narayan, MD, MSc, and J. Stephen Bohan, MD, MS, FACEP
Appelbaum PS. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-840.
Competence (or capacity) is the critical component in a patient’s ability to understand and make decisions regard-ing his or her medical care. A patient’s competence could be compromised by illness, by the effects of medication or hospitalization, or by mental disorders such as delirium, de-mentia, or major depression. Physicians must be able to as-sess a patient’s decision-making capacity in an organized and structured manner.
Between 3% and 25% of all requests for psychiatric con-sultation in hospital settings involve questions about patients’ competence to make treatment-related decisions. Lack of in-sight has been reported to be the strongest predictor of in-capacity, as well as older age, fewer years of education, and cognitive impairment. Although medical conditions such as dementia, depression, and schizophrenia can induce impair-ment, the presence of these conditions is not invariably pre-dictive of incapacity.
Capacity is presumed for all adults unless there is a reason to question it. If there is doubt, capacity should be assessed by those who best know the patient; a psychiatric consulta-tion can help in particularly complex cases or when mental illness is present. When deciding to perform a competence assessment, it is important to weigh the seriousness of the likely consequences of the patient’s decisions against the se-riousness of declaring the patient incompetent.
Criteria for the assessment of decision-making capacity in-clude the ability to communicate a choice, to understand the relevant information, to appreciate the medical consequences of the situation, and to reason about treatment choices. Stud-ies show that using a structured approach, such as specific legal standards or a systematic set of questions, can lead to a
high rate of agreement with expert judgments. Exams such as the Mini-Mental State Examination (5-minute duration) and the MacArthur Competence Assessment Tool for Treat-ment (20-minute duration) are useful and correlate well with incapacity based on their respective scores. Unfortunately, neither test can identify a threshold score at which a patient’s ability to make a decision is inadequate. Moreover, there are no formal practice guidelines to assess capacity, and all the instruments differ in their identification of patients who are impaired.
In nonurgent situations, try to reverse specific causes of incapacity, if possible (eg, fever, hypoxia, uremia, sedation); when fear or anxiety is interfering with the patient’s capacity, a trusted confidant or adviser could be helpful in the con-sent process. In an emergency in which an advance directive or surrogate decision maker is unavailable, a physician can provide care under the presumption that a reasonable per-son would consent to such treatment. Alternatively, if time is available, contacting family members can help; the preferred family member to contact, in order of preference, is generally the spouse, adult child, parents, sibling, and other relatives.
Highlights Physicians should assess competence in an organized and •structured manner.
Competence is assumed until the patient proves otherwise.•
Structured exams like the Mini-Mental State Exam and the •MacArthur Competence Assessment tools are useful, but there is no one approach that is most valid, and there are no clear boundaries at which capacity ends and incapacity begins.
In emergency situations, an advance directive or surrogate •decision maker should be used to determine treatment. Alternatively, a physician can contact family members or provide appropriate care under the presumption that a reasonable person would consent to treatment.
Article 9

Critical Decisions in Emergency Medicine
10
n ObjectivesOn completion of this lesson, you
should be able to:
1. Describe presentations of status epilepticus in both adult and pediatric populations.
2. Discuss appropriate first- and second-line medications for seizure termination in status epilepticus.
3. Select appropriate medications for rapid-sequence intubation and postintubation infusion therapy in status epilepticus patients requiring airway management.
4. Describe an appropriate diagnostic evaluation for a patient presenting with status epilepticus.
5. Explain how to differentiate simple from complex febrile seizures in children, and describe effective treatments for children with febrile status epilepticus.
n From the EM Model12.0 Nervous System Disorders
12.9 Seizure Disorders
Julie J. Cooper, MD, and Michael A. Gisondi, MD, FACEP
Evaluation and Treatment of Status Epilepticus
Lesson 6
Seizures affect over three million Americans of all ages at an estimated $15.5 billion in direct and indirect health care costs.1 Seizure-related emergencies are a common reason for emergency department visits; approximately 1.2% of all emergency department patients present with complaints related to seizures.2 The annual incidence of status epilepticus in adults is estimated to be between 18 and 40 per 100,000 in the United States,3 and in children the incidence is about 31,600 per year.4 Status epilepticus is a medical emergency responsible for up to 42,000 deaths annually in the United States; it occurs in a wide spectrum of patients including those with no prior history of seizure.5
The traditional definition of status epilepticus is continuous seizure activity lasting 30 minutes or a succession of seizures without an intervening return to baseline mental status. This definition uses 30 minutes as a threshold duration based mainly on animal data demonstrating that neurons undergo irreversible damage after 30 minutes of continually induced seizures.6 This definition is problematic in the clinical setting, however, because the type of seizure and the time to neuronal damage will vary from patient to patient. There are no readily available laboratory or imaging tests to quantify this ongoing brain damage. Some experts suggest that 5 to 10 minutes of continuous seizure activity is a more practical definition
of status epilepticus, recognizing that more than 90% of tonic-clonic seizures will spontaneously terminate within 2 minutes.3 Pediatric data show that once a seizure has lasted for 5 to 10 minutes it is unlikely to terminate without pharmacologic intervention, and the longer a seizure lasts the more difficult it is to control despite medical therapy.7 Operationally, status epilepticus must be presumed in any patient who presents to the emergency department with persistent seizure activity, because most prehospital transport times will easily exceed 5 minutes.
Case Presentations
n Case OneA 67-year-old man is brought
to the emergency department by ambulance after having a generalized tonic-clonic seizure. According to his wife, the patient was in his usual state of health until this morning. He was in the kitchen when she heard a loud noise and found him on the floor having a generalized seizure. When EMS arrived, the seizure had stopped, and the patient was noted to appear postictal, with a depressed mental status. There was no obvious trauma. He has a history of hypertension, hyperlipidemia, and prior prostatectomy for prostate cancer. The paramedics were not able to establish intravenous access in the ambulance, and only 100% oxygen by face mask was given as he was transported to the emergency department. Shortly after being placed in an examination

November2009•Volume24•Number3
11
Which medications should be used in the emergency •department management of status epilepticus?What additional therapies may be used to treat refractory •status epilepticus?What are the special considerations in airway •management for status epilepticus?
What diagnostic testing in the emergency department •can help reveal the causes of status epilepticus?What are the unique considerations in pediatric status •epilepticus?
Critical Decisions
room, he begins to have tonic-clonic seizure activity. Initial vital signs are blood pressure 140/80, pulse rate 110, respiratory rate 12, temperature 37.3°C (99.1°F), and oxygen saturation of 99% on 100% oxygen via face mask. Physical examination reveals a well-developed, well-nourished elderly man having a tonic-clonic seizure. He is unresponsive to voice or painful stimulus. A cervical collar is in place, and no trauma is noted to the head or face. Pupils are equal, round, and reactive to light. There is scant bright red blood noted in the oropharynx. Heart, lung, and abdominal examinations are unremarkable. Peripheral intravenous access is obtained, and an initial point-of-care blood glucose level is 143.
n Case TwoAn 18-month-old otherwise
healthy girl is brought to the emergency department after a seizure witnessed by her babysitter. She had upper respiratory symptoms over the past 2 days and had two episodes of nonbloody, nonbilious emesis after breakfast. This morning she was interactive and playful. She lay down for a nap and about 45 minutes later was noted to have a generalized seizure of at least 5 minutes’ duration. EMS was called and found a lethargic toddler who aroused to voice and was irritable. In the ambulance she slowly returned to her baseline mental status. The babysitter states that the child has no known prior history of seizure. Initial vital signs are blood pressure 90/palpable, pulse rate 130, respiratory rate 12, temperature
39.7°C (103.5°F), and oxygen saturation 99% on room air. Physical examination reveals an alert toddler who is irritable and cries when examined. No trauma is noted. Pupils are equal, round, and reactive to light. Mucous membranes are moist. The oropharynx is clear. No cervical lymphadenopathy is noted. She has a normal heart, lung, and abdominal examination with no organomegaly. A peripheral intravenous line is established. About 10 minutes after arriving in the emergency department, the child experiences another generalized seizure.
Classification of Status Epilepticus
Status epilepticus can be classified as convulsive or nonconvulsive. Generalized tonic-clonic status epilepticus is the most common and serious form and might represent cortical generalization of a precipitating partial seizure. Other convulsive forms are simple partial seizures (focal motor seizures, focal sensory symptoms, or cognitive symptoms without impaired consciousness) and complex partial seizures (with impaired consciousness). Nonconvulsive status epilepticus can present a diagnostic challenge because its manifestations are subtle and can include absence status and myoclonic status (repeated myoclonic jerks in the setting of altered mental status).
Psychogenic status epilepticus (or psychogenic nonepileptic status epilepticus, PNESE) presents with generalized motor features of seizure without true epileptiform activity
on electroencephalograph (EEG). Features that can help distinguish psychogenic status epilepticus include gradual onset of undulating motor activity, variable motor activity, or partially preserved consciousness with a lack of a postictal period. Response to noxious stimuli in these patients is often preserved even during “seizure” activity.8
Assessment and Management of Status Epilepticus
Seizure patients can present to an emergency department in dramatic fashion and require a rapid and organized diagnostic assessment in parallel with early and aggressive anticonvulsant therapy.9
Status epilepticus is a medical emergency and requires mobilization of resources and rapid diagnostic assessments similar to those required for cardiac arrest or an ST-elevation myocardial infarction. As with any life-threatening illness, the standard considerations of airway, breathing, and circulation apply in status epilepticus. Endotracheal intubation is not routinely indicated solely for seizure activity but is frequently necessitated during anticonvulsant infusion therapy.
Place all actively seizing patients on supplemental oxygen by face mask and monitor oxygen saturation continuously via pulse oximetry. If feasible, establishing a nasopharyngeal airway could facilitate improved oxygenation.3 Initial vital signs and intravenous access should be obtained with the goal of rapid administration of a benzodiazepine

Critical Decisions in Emergency Medicine
12
in conjunction with the ongoing diagnostic evaluation. Place the patient on continuous telemetry monitoring and obtain an ECG when possible. Obtain a point-of-care blood glucose level. If dextrose is indicated, consider pretreatment with 100 mg of intravenous thiamine, especially if there is concern for alcoholism or malnutrition.
CRITICAL DECISIONWhich medications should be used in the emergency department management of status epilepticus?
There are four categories of anticonvulsant drugs used to treat status epilepticus, and they are generally initiated and titrated rapidly in a stepwise fashion. These categories are the benzodiazepines, phenytoin, barbiturates, and propofol. Levetiracetam and valproate have recently been added to this list as alternatives to phenytoin, given emerging data for their effectiveness in status epilepticus. Table 1 summarizes these medications, their dosages, and considerations for their use.
First-Line Therapy: Benzodiazepines
Benzodiazepines remain the first-line treatment for all seizure emergencies and status epilepticus. Their mechanism of action is enhancement of chloride conduction through central nervous system (CNS) -aminobutyric acid type A (GABAA) receptors, decreasing overall neuronal excitability.10 In the largest pediatric clinical trial to date, lorazepam alone (0.1 mg/kg) terminated seizure activity in 64.9% of patients with overt convulsive activity.11 A 2005 Cochrane review12 of anticonvulsant therapy also found parenteral lorazepam to be the initial therapy of choice in adults presenting with status epilepticus. Additionally, benzodiazepines have been shown to be safe when given in the prehospital setting with the goal of aborting seizure activity prior to emergency department arrival. Of note, patients
who were still in status epilepticus at the time of emergency department arrival were more than twice as likely to require ICU admission as those whose seizures were successfully terminated prehospital.13
Lorazepam is familiar to emergency department providers, fast acting, easy to use, and offers a longer therapeutic effect and lower risk of respiratory suppression than diazepam. There is no upper limit to the amount of benzodiazepine that can be administered. Dosing may be limited by respiratory suppression in some settings, but in the emergency department the physician should secure the airway and continue repeating benzodiazepine administration until seizure termination; cessation of seizure activity should supercede the concern for respiratory depression.
Second-Line Therapy: Phenytoin, Fosphenytoin, Levetiracetam, Valproate
Phenytoin acts to terminate seizure activity through modulation of neuronal voltage-dependent sodium and calcium channels. Phenytoin is a familiar anticonvulsant drug in the emergency department that is widely used as a second-line agent when seizures are not controlled with benzodiazepines, although this strategy has yet to be rigorously clinically tested.3 Phenytoin has some well-recognized limitations as a parenteral therapy; side effects include hypotension, cardiac arrhythmias (similar in mechanism to class IA antiarrhythmic drugs), pain at the infusion site, and local toxicity if it extravasates (purple glove syndrome). All of the systemic toxicities are infusion-rate related and largely due to the propylene glycol used as a diluent. Given the cardiovascular side effects, patients should be on a telemetry monitor, and phenytoin should be infused at a rate to limit side effects, generally no faster than 50 mg/min. Phenytoin cannot be administered by intravenous
push. It is often ineffective in status epilepticus caused by alcohol withdrawal or toxicologic etiologies.
Fosphenytoin is a prodrug of phenytoin that is not diluted in propylene glycol; thus it causes fewer adverse reactions and can be infused much faster. Fosphenytoin must undergo first-pass metabolism in the liver, where it is converted to phenytoin; therefore its overall time to onset of action is similar to that of slowly infused phenytoin. It is frequently cited as a less desirable parenteral therapy for seizures in the emergency department because of its higher cost; however, the more favorable side-effect profile of fosphenytoin and its ease of rapid infusion can make it a better choice.14
Levetiracetam is an anticonvulsant drug with a poorly defined mechanism of action that has become widely used in the outpatient setting for the treatment of seizure disorders because of its efficacy and favorable side-effect profile. A parenteral formulation was approved in 2006. Although animal studies of intravenous levetiracetam for status epilepticus have been equivocal, there are case reports of refractory status epilepticus that has responded to levetiracetam in the ICU setting. There are no studies of intravenous levetiracetam in the emergency department setting, but as it becomes more widely used it may have a role as a lower-toxicity second-line therapy.15
Three small trials of intravenous sodium valproate have demonstrated its efficacy in refractory status epilepticus. Studies have shown a benefit of valproate over phenytoin as a first-line anticonvulsant drug for status epilepticus,16 equivalence of valproate and phenytoin in patients who did not respond to first-line diazepam (approximately 85% of these patients had termination of seizure activity with a second-line agent),17 and similar response of pediatric status epilepticus to both diazepam infusion and valproate as

November2009•Volume24•Number3
13
first-line therapy (with a reduction in respiratory depression in children who received valproate).18 Some authors advocate that levetiracetam or valproate be recommended as third-line therapies before barbiturates.3
Refractory Status EpilepticusA critical juncture in the
management of status epilepticus occurs when a patient continues to seize after an adequate dose of benzodiazepine has been administered. Second-line
anticonvulsant drugs often take some time to be prepared and have an onset of action of 10 to 30 minutes. In one study, only 7% of patients who did not respond to appropriate doses of a benzodiazepine and phenytoin or
Table 1.Medications commonly used in the emergency department management of status epilepticus
Benzodiazepines – First-Line Therapy
Medication Routes of Administration, Dosage Considerations
Lorazepam IV or IM Adults: 0 .02-0 .03 mg/kg IV every 5 min, maximum single dose 4 mg Children: 0 .1 mg/kg IV, maximum single dose 4 mg
First-line agent for status epilepticus
Diazepam IV, IM, rectal Adults: 0 .05-0 .1 mg/kg IV every 5 min; Children: 0 .3-0 .5 mg/kg IV or PR, maximum, 10 mg
Can be given as a rectal gel when prompt intravenous access is not possible Fast effect (3 min IV, 5-7 min rectal)
Midazolam IV, IM, rectal, buccal, intranasal, or continuous infusionInfusion: 0 .05 mg/kg;Adults: 0 .1-0 .2 mg/kg IV; Buccal in children: 0 .5 mg/kg
The benzodiazepine of choice in hemodynamically unstable or ICU patients; used in infusion therapy
Anticonvulsant Drugs – Second-Line Therapy
Medication Routes of Administration, Dosage Considerations
Phenytoin IV only for status epilepticus 20 mg/kg loading dose; goal concentration 15-25 mcg/mL Infuse at a rate of up to 50 mg/min, titrate down if cardiovascular toxicity; give at 25 mg/min if patient is older than 50 years or ectopy is noted on monitor
Traditional second-line anticonvulsant drug after the benzodiazepines; can cause hypotension, drug rashes, irritation on infusion, purple-hand syndrome if it extravasates; draw serum level about 10 min after infusion ends and administer an extra 5 mg/kg if serum levels are subtherapeutic
Fosphenytoin IV or IM Prescribed as “phenytoin equivalent” dose
Given more rapidly, less likely to cause hypotension, more expensive than phenytoin, IM absorption can be erratic
Sodium Valproate IV or rectal 20-30 mg/kg loading dose at a rate of up to 10 mg/kg/min
Frequently used when phenytoin/fosphenytoin are contraindicated; adverse effects include hyperammonemia, pancreatitis, thrombocytopenia (contraindicated in preexisting thrombocytopenia)
Levetiracetam No established IV dose for use in status epilepticus, small studies used doses of 1,000-6,000 mg; may also be given orally through a nasogastric tube
No human controlled trials of its use in status epilepticus
Barbiturates
Medication Routes of Administration, Dosage Considerations
Phenobarbital IV or IM 20 mg/kg loading dose at a rate of 30-50 mg/min
Many patients need intubation after loading dose; long half-life with slow emergence
Pentobarbital IV 10 mg/kg of pentobarbital infused at a rate up to 100 mg/min; may follow with continuous infusion
Mandatory central venous pressure monitoring makes barbiturate coma appropriate only in the ICU setting
Infusion Therapy
Medication Routes of Administration, Dosage Considerations
Propofol IV bolus then infusion (off-label) 1-2 mg/kg bolus followed by 1 .5-10 mg/kg/hr infusion
Excellent postintubation infusion therapy; can be titrated to effect (cessation of seizure clinically or, if paralyzed, by EEG)

Critical Decisions in Emergency Medicine
14
fosphenytoin responded to any third-line agent.10
Barbiturates are frequently cited as an appropriate third-line agent in the ICU setting. Their mechanism of action is similar to benzodiazepines in that they enhance CNS GABA activity and decrease neuronal excitability. Phenobarbital, thiopental, and its metabolite pentobarbital are of limited utility in the emergency department because of their slow onset of action and because they induce profound hypotension requiring continuous central venous pressure monitoring.6
CRITICAL DECISIONWhat additional therapies may be used to treat refractory status epilepticus?
Given the low rate of success of third-line agents, many clinicians now prefer proceeding directly to continuous infusion therapy rather than using a third-line anticonvulsant drug.3 Continuous infusions used in the management of status epilepticus include midazolam, which is preferred in hemodynamically unstable patients for its ease of titration and short half-life,3 and propofol, an intravenous anesthetic agent that is familiar to most emergency department providers and has very effective anticonvulsant properties. Propofol is used off-label as an infusion therapy for status epilepticus.
CRITICAL DECISIONWhat are the special considerations in airway management for status epilepticus?
Most of the medications used in the management of status epilepticus have the potential to cause respiratory depression. Adequate dosing of anticonvulsant drugs should never be withheld for a competing goal of avoiding intubation, as refractory seizures must be stopped as quickly as possible to limit neuronal damage.
Most patients with status epilepticus that require intubation will not yet have a clear etiology of their seizures, so rapid sequence
intubation should be performed with consideration for potential intracranial pathology. Consider pretreatment with lidocaine if there is a concern for increased intracranial pressure and time allows. Most of the anticonvulsant drugs cause some degree of hypotension and sedation; if an additional induction agent is required for intubation, consider using etomidate as it has a favorable hemodynamic profile. Use a nondepolarizing paralytic agent such as rocuronium to avoid increases in intracranial pressure.
Paralyzing status epilepticus patients will convert convulsive status epilepticus to an iatrogenic nonconvulsive status epilepticus, as motor activity is blunted while neuronal stimulation is on-going. Infusion therapy should begin immediately after intubation either with midazolam or propofol to treat presumed nonconvulsive status epilepticus. Continuous EEG monitoring should be arranged as quickly as possible in order to titrate infusion therapy to seizure termination.
CRITICAL DECISIONWhat diagnostic testing in the emergency department can help reveal the causes of status epilepticus?
Ongoing management of status epilepticus requires a search for correctable underlying causes of seizure activity. In adults, the most common factors leading to status epilepticus are subtherapeutic anticonvulsant drug levels (34%), history of prior CNS insult (25%), cerebrovascular accident (22%), metabolic derangements (15%), and alcohol-related seizures (13%).5 In pediatric populations, the most common etiologies are infection outside the CNS (febrile status epilepticus, 52%), prior CNS disease (most commonly congenital malformations, 38%), and subtherapeutic anticonvulsant drug levels in children with known epilepsy (21%).5
The diagnostic evaluation for the etiology of status epilepticus should begin in parallel with anticonvulsant therapy. There are few rigorously studied guidelines for the diagnostic evaluation of status epilepticus, and most recommendations represent expert opinion. Routine blood testing, including bedside glucose, electrolyte levels, creatine phosphokinase to evaluate ongoing muscle breakdown, and a toxicology screen, should be performed in all adult patients presenting with status epilepticus.3,6,19 Serum anticonvulsant drug levels should be drawn if the patient’s anticonvulsant medication regimen is known. Although status epilepticus seldom has a surgically correctable intracranial etiology,5 computed tomography scanning of the head remains an important screening tool in cases of suspected trauma and for patients who cannot undergo a complete neurologic examination because of depressed or altered mental status and could go on to require lumbar puncture. Head computed tomography should not delay initiation of anticonvulsant drug therapy. Lumbar puncture is indicated in patients with preceding illness, fever, or other signs of CNS infection but is not routinely indicated in status epilepticus. Consider blood cultures in the febrile seizure patient only; the diagnostic yield of blood cultures in an afebrile patient is unclear.4
CRITICAL DECISIONWhat are the unique considerations in pediatric status epilepticus?
Febrile status epilepticus is the cause of approximately 22% of childhood status epilepticus.4 Febrile seizures are the most common form of seizures, affecting 2% to 5% of all children and usually appearing when children are between 3 months and 5 years of age. Febrile seizures are classified as simple or complex. A simple febrile seizure lasts less than 15 minutes and is self-limited, with tonic-clonic features. Children with simple febrile seizures have

November2009•Volume24•Number3
15
no recurrence within 24 hours and no postictal pathology. In contrast, a complex febrile seizure is of longer duration (>15 minutes), or it can present as a series of shorter seizures recurring within 24 hours. Focal febrile seizures (such as partial seizures with secondary generalization or deviation of the head or eyes) are considered complex febrile seizures.20
Although only supportive care is routinely required for simple febrile seizures, febrile status epilepticus is treated using the same medication algorithm as outlined for adults. Benzodiazepines are highly effective as first-line therapy in febrile status epilepticus, with rare cases necessitating the addition of second-line anticonvulsant drugs. Despite the association between seizure and fever, antipyretic medications have not been shown to be beneficial in febrile seizures or status epilepticus.20 Status epilepticus, whether febrile or afebrile, is the first seizure presentation in 12% of children with epilepsy.21
Unique to the pediatric population is the widespread use of rectal and buccal benzodiazepines when intravenous access is difficult to obtain.22 Prehospital benzodiazepine use for children with status epilepticus has been shown to be associated with shorter seizure duration compared to those whose treatment was delayed until emergency department arrival.13
Case Resolutions
Case OneThis 80-kg patient received
an initial dose of 4 mg lorazepam intravenously (standard dose 0.02-0.03 mg/kg IV in adults). He continued to have tonic-clonic seizure activity, and a second dose of lorazepam was administered 5 minutes later; fosphenytoin was ordered from the pharmacy. After a third dose of lorazepam, his respiratory rate decreased to 8 with intermittent oxygen desaturations to 88% on 100% oxygen via face mask.
PearlsAny patient presenting to an emergency department with •an active seizure should be considered to be in status epilepticus, because most hospital transport times exceed the 5-minute operational definition of status epilepticus.
Simple febrile seizures in children should be treated supportively, •but complex febrile seizures and febrile status epilepticus should be treated with anticonvulsant drugs.
Consider nonconvulsive status epilepticus in the differential diagnosis of •patients presenting with altered mental status or reduced responsiveness.
Potential systemic complications of status epilepticus include rhabdomyolysis, •aspiration, disseminated intravascular coagulation, neurocardiogenic pulmonary edema, arrhythmia, cardiac arrest, endocrinopathies, electrolyte disturbances, and cerebral edema. These complications should be actively sought out and aggressively treated in the emergency department.
PitfallsWithholding adequate doses of anticonvulsant drugs out of concern •for respiratory depression. “Time is brain,” and stopping the seizure is the priority; intubate for airway protection and ventilation.
In cases of refractory seizures, failing to search for uncommon, •but reversible causes of status epilepticus such as hypoglycemia, isoniazid toxicity, hyponatremia, and postpartum eclampsia.
Failing to remember that dosing of phenytoin is weight-based—18 •to 20 mg/kg (or 1,400 mg in a 70-kg adult); it is easy to underdose patients when not taking their weight into consideration. Infuse phenytoin at a rate of no more than 50 mg/minute in order to avoid cardiovascular side effects. Never give phenytoin as an intravenous push. If ectopy is observed, halve the infusion rate.
The decision was made to intubate for airway protection and to facilitate diagnostic workup. Rocuronium, 80 mg, was administered, and the patient was endotracheally intubated on the first attempt. Neurology was consulted for continuous EEG monitoring and ICU admission. His seizure activity on EEG terminated with initiation of propofol infusion. Magnetic resonance imaging later revealed a left middle cerebral artery distribution cerebrovascular accident.
Case TwoThe emergency physician
recognized the events as a complex febrile seizure in this toddler. During the second seizure, a dose of 0.1 mg/kg of lorazepam was administered
intravenously with prompt cessation of seizure activity. Empiric antibiotics for meningitis were ordered, and a lumbar puncture revealed a pleocytosis. No further seizures were observed in the emergency department. The child was admitted to the pediatric ICU for observation and antibiotic therapy.
SummaryStatus epilepticus is a time-
sensitive medical emergency that can present in a dramatic fashion. Emergency department management requires rapid recognition and early administration of appropriate anticonvulsant drug therapy to help prevent neuronal damage and long-term sequelae. The longer a
Critical Decisions in Emergency Medicine
16
seizure continues, the more difficult it becomes to control. Most status epilepticus seizures will terminate with early administration of a benzodiazepine and phenytoin or fosphenytoin, but emergency physicians should be prepared to treat refractory cases after endotracheal intubation with infusion therapy using midazolam or propofol. Treatment of status epilepticus should occur in parallel with an appropriate diagnostic evaluation, early neurology service consultation, and ICU admission.
References1. Epilepsy foundation. Epilepsy and seizure statistics.
Available online at: http://www.epilepsyfoundation.org/about/statistics.cfm. Accessed June 8, 2009.
2. Huff JS, Morris DL, Kothari RU, et al, Emergency Medicine Seizure Study Group. Emergency department management of patients with seizures: a multicenter study. Acad Emerg Med. 2001;8:622-628.
3. Costello DJ, Cole AJ. Treatment of acute seizures and status epilepticus. J Intensive Care Med. 2007;22(6):319-347.
4. Riviello JJ, Ashwal S, Hirtz D, et al. Practice parameter: diagnostic assessment of the child with status epilepticus (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2006;67:1542-1550.
5. DeLorenzo RJ, Pellock JM, Towne AR, et al. Epidemiology of status epilepticus. J Clin Neurophysiol. 1995;12(4):316-325.
6. García Peñas JJ, Molins A, Salas Puig J. Status epilepticus: evidence and controversy. Neurologist. 2007;13(6 Suppl 1):S62-S73.
7. Shinnar S, Berg AT, Moshe SL, et al. How long do new-onset seizures in children last? Ann Neurol. 2001;49:659-664.
8. Reuber M, Baker GA, Gill R, et al. Failure to recognize psychogenic nonepileptic seizures may cause death. Neurology. 2004;62:834-835.
9. Tarabar AF, Ulrich AS, D’Onofrio G. Seizures. In: Adams JG, Barton ED, Collings JL, et al, eds. Emergency Medicine. Philadelphia, PA: Saunders Elsevier; 2008.
10. Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998;339:792-798.
11. Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatments for generalized convulsive status epilepticus. New Engl J Med. 1998;339:792-798.
12. Prasad K, Al-Roomi K, Krishnan PR, Sequeira R. Anticonvulsant therapy for status epilepticus. Cochrane Database of Systematic Reviews 2005. Issue 4. CD003723.
13. Alldredge BK, Gelb AM, Isaacs SM, et al. A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med. 2001;345:631-637.
14. Rudis MI, Touchette DR, Swadron SP, et al. Cost-effectiveness of oral phenytoin, intravenous phenytoin and intravenous fosphenytoin in the emergency department. Ann Emerg Med. 2004;43(3):386-397.
15. Misra UK, Kalita J, Patel R. Sodium valproate vs. phenytoin in status epilepticus: a pilot study. Neurology. 2006;67:340–342.
16. Agarwal P, Kumar N, Chandra R, et al. Randomized study of intravenous valproate and phenytoin in status epilepticus. Seizure. 2007;16:527–532.
17. Mehta V, Singhi P, Singhi S. Intravenous sodium valproate versus diazepam infusion for the control of refractory status epilepticus in children: a randomized controlled trial. J Child Neurol. 2007;22:1191–1197.
18. Wheeles JW, Traiman DM. The role of newer antiepileptic drugs in the treatment of generalized convulsive status epilepticus. Epilepsia. 2008;49(suppl 9):74-78.
19. Pellock JM. Overview: definitions and classifications of seizure emergencies. J Child Neurol. 2007;22(5):9s-13s.
20. Fetveit A. Assessment of febrile seizures in children. Eur J Pediatr. 2008;167:17-27.
21. Haut SR, Shinnar S, Moshe SL, et al. The association between seizure clustering and convulsive status epilepticus in patients with intractable complex partial seizures. Epilepsia. 1999;40:1832-1834.
22. McIntyre J, Robertson S, Appleton R, et al. Safety and efficacy of buccal midazolam versus rectal diazepam for emergency treatment of seizures in children: a randomized controlled trial. Lancet. 2005;366:205-210.
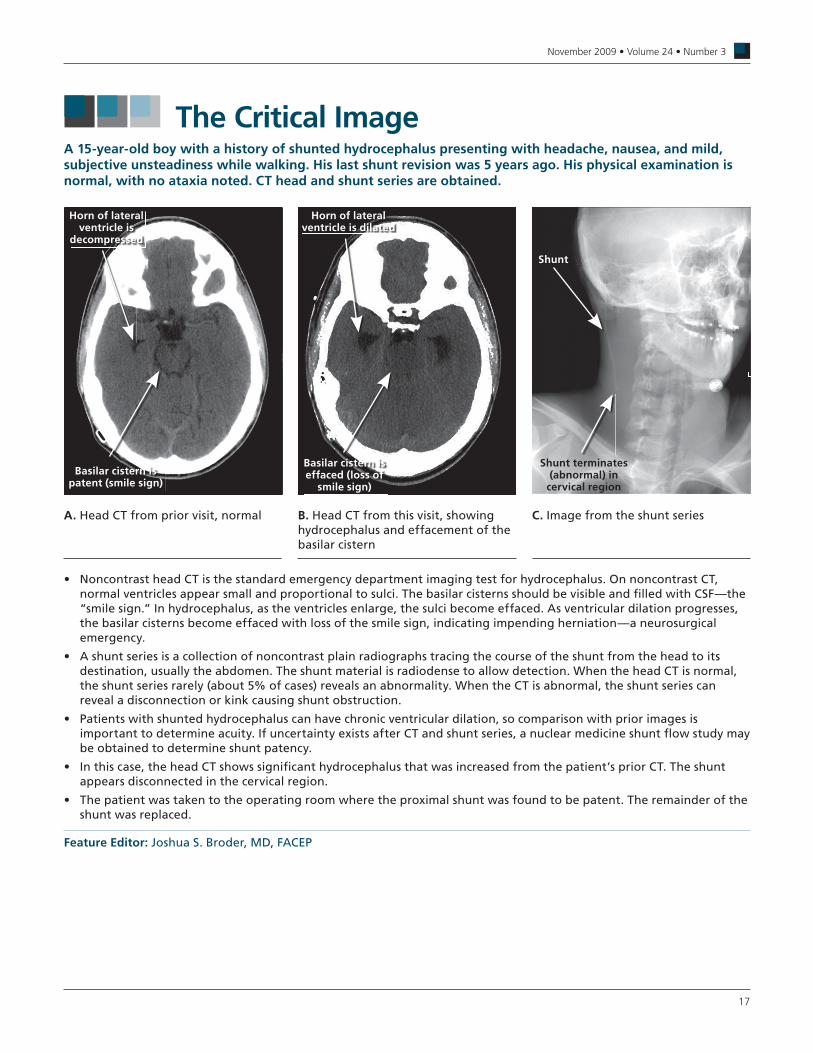
November2009•Volume24•Number3
17
The Critical ImageA 15-year-old boy with a history of shunted hydrocephalus presenting with headache, nausea, and mild, subjective unsteadiness while walking. His last shunt revision was 5 years ago. His physical examination is normal, with no ataxia noted. CT head and shunt series are obtained.
Noncontrast head CT is the standard emergency department imaging test for hydrocephalus . On noncontrast CT, • normal ventricles appear small and proportional to sulci . The basilar cisterns should be visible and fi lled with CSF—the “smile sign .” In hydrocephalus, as the ventricles enlarge, the sulci become effaced . As ventricular dilation progresses, the basilar cisterns become effaced with loss of the smile sign, indicating impending herniation—a neurosurgical emergency .
A shunt series is a collection of noncontrast plain radiographs tracing the course of the shunt from the head to its • destination, usually the abdomen . The shunt material is radiodense to allow detection . When the head CT is normal, the shunt series rarely (about 5% of cases) reveals an abnormality . When the CT is abnormal, the shunt series can reveal a disconnection or kink causing shunt obstruction .
Patients with shunted hydrocephalus can have chronic ventricular dilation, so comparison with prior images is • important to determine acuity . If uncertainty exists after CT and shunt series, a nuclear medicine shunt fl ow study may be obtained to determine shunt patency .
In this case, the head CT shows signifi cant hydrocephalus that was increased from the patient’s prior CT . The shunt • appears disconnected in the cervical region .
The patient was taken to the operating room where the proximal shunt was found to be patent . The remainder of the • shunt was replaced .
Feature Editor: Joshua S . Broder, MD, FACEP
A. Head CT from prior visit, normal B . Head CT from this visit, showing hydrocephalus and effacement of the basilar cistern
C . Image from the shunt series
Horn of lateral ventricle is
decompressed
Basilar cistern is patent (smile sign)
Horn of lateral ventricle is dilated
Basilar cistern is effaced (loss of
smile sign)
Shunt
Shunt terminates (abnormal) in
cervical region

Critical Decisions in Emergency Medicine
18
Qualified, paid subscribers to Critical Decisions in Emergency Medicine may receive CME certificates for up to 5 ACEP Category I credits, 5 AMA PRA Category I Credits™, and 5 AOA Category 2-B credits for answering the following questions . To receive your certificate, go to www .acep .org/criticaldecisionstesting and submit your answers online . You will immediately receive your score and printable CME certificate . You may submit the answers to these questions at any time within 3 years of the publication date . You will be given appropriate credit for all tests you complete and submit within this time . Answers to this month’s questions will be published in next month’s issue .
CME Questions
1 . Which of the following findings is most suggestive of increased intracranial pressure (ICP) in an infant?A. bulging or tense fontanellesB. drowsinessC. failure to thriveD. headacheE. sunset eyes
2 . For patients with suspected acutely increased ICP, which of the following is the first-line imaging study?A. brain CT with contrastB. brain CT without contrastC. magnetic resonance angiography of the brainD. magnetic resonance imaging of the brain with and without
gadoliniumE. magnetic resonance imaging of the brain without gadolinium
3 . What is the leading cause of acute hydrocephalus?A. infections such as bacterial meningitisB. ischemic strokeC. neurocysticercosisD. subarachnoid hemorrhageE. subdural hemorrhage
4 . Elevated cerebrospinal fluid (CSF) opening pressure is defined as a value greater than:A. 5 cm H2OB. 10 cm H2OC. 15 cm H2OD. 20 cm H2O in an obese patientE. 25 cm H2O in an obese patient
5 . Treatment of idiopathic intracranial hemorrhage is aimed at preventing which of the following?A. herniationB. optic nerve atrophyC. retinal hemorrhageD. strokeE. subarachnoid hemorrhage
6 . Which of the following is the first-line drug treatment for lowering ICP for stable patients with idiopathic intracranial hypertension?A. acetazolamideB. furosemideC. glucagonD. mannitolE. topiramate
7 . Which of the following is no longer routinely recommended during induction in patients with elevated ICP?A. atropineB. etomidateC. fentanylD. lidocaineE. succinylcholine
8 . Which of the following induction agents has been associated with a transient increase in ICP?A. etomidateB. fentanylC. propofolD. succinylcholineE. thiopental
9 . Which of the following interventions should be delayed 24 hours after intubation in a patient with increased ICP for whom the intervention would otherwise be indicated?A. hypertonic salineB. hyperventilationC. mannitolD. rapid sequence intubationE. ventriculostomy
10 . It is relatively safe to perform a lumbar puncture in a patient with suspected meningitis who has which of the following findings?A. communicating hydrocephalusB. compression of basal cisternsC. midline shiftD. obstructive hydrocephalusE. obtunded mental status without focal neurologic deficit
11 . A man arrives by ambulance having a generalized tonic-clonic seizure . No past history is available, and the bystanders who called EMS are not present . His airway is intact, and his vital signs are stable . What is the most appropriate initial action?A. 18-mg/kg loading dose of phenytoinB. airway control with rapid sequence intubationC. immediate administration of 0.02 mg/kg of lorazepamD. neurologic consultationE. observation for cessation of seizure activity within 30 minutes

November2009•Volume24•Number3
19
Answer key for October 2009, Volume 24, Number 2
The American College of Emergency Physicians makes every effort to ensure that contributors to College-sponsored publications are knowledgeable authorities in their fields. Readers are nevertheless advised that the statements and opinions expressed in this series are provided as guidelines and should not be construed as College policy unless specifically cited as such. The College disclaims any liability or responsibility for the consequences of any actions taken in reliance on those statements or opinions. The materials contained herein are not intended to establish policy, procedure, or a standard of care.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20B B A A C B B E B E B C C A D B E B D D
12 . A 60-year-old man presents in status epilepticus . During treatment he develops hypotension refractory to intravenous fluid; QT prolongation with frequent premature ventricular contractions is noted . Which of the following most likely caused these findings?A. fosphenytoinB. levetiracetamC. lorazepamD. midazolamE. phenytoin
13 . A 65-year-old man with refractory status epilepticus is intubated for respiratory depression . He is still actively seizing after receiving three doses of lorazepam and initiation of a fosphenytoin load . Rapid sequence intubation is performed using lidocaine, etomidate, and rocuronium . A continuous EEG shows ongoing seizure activity . Which is the most appropriate next action?A. continue to push 0.1-mg/kg doses of lorazepam every 5
minutes until seizure cessationB. initiate a propofol infusion and titrate upward until cessation of
seizure on EEG monitorC. initiate a rocuronium infusion to continue to suppress
convulsionsD. repeat the fosphenytoin load via an intramuscular routeE. wait for rocuronium to wear off to determine if convulsive
seizures will continue
14 . What is the most common cause of status epilepticus in adults with a history of epilepsy?A. alcohol withdrawalB. central nervous system infectionC. cerebrovascular accidentD. electrolyte abnormalitiesE. subtherapeutic anticonvulsant drug level
15 . In which of the following children are supportive care and observation appropriate emergency department management strategies?A. 12-day-old infant with fever to 38.3°C (101°F) and a
generalized seizure lasting 4 minutes followed by an apneic spell, who now looks well
B. 9-month-old baby boy with known otitis media on amoxicillin, fever to 38.3°C (101°F), and 4-minute tonic-clonic seizure that terminated spontaneously at home; he now looks well
C. 14-month-old toddler with three febrile seizures today, the longest of which lasted 3 minutes, who appears septic
D. 5-year-old girl with fever, lethargy, and witnessed seizure involving head and eye deviation to the left for 10 minutes, now postictal
E. 15-year-old boy with known epilepsy who had a witnessed, 4-minute-long tonic-clonic seizure at school; no trauma is noted; his heart rate is 130 beats per minute, and he is neurologically intact
16 . Which of the following rapid sequence intubation drugs should theoretically be avoided when intubating an undifferentiated patient with status epilepticus?A. etomidateB. lidocaineC. midazolamD. rocuroniumE. succinylcholine
17 . Which of the following statements is true regarding the use of benzodiazepines in status epilepticus?A. benzodiazepines are less effective than phenytoin or
fosphenytoin for seizures from toxicologic causesB. benzodiazepines should be titrated to respiratory depressionC. most patients have termination of seizure activity with a
benzodiazepine aloneD. most patients require endotracheal intubation after the first
dose of benzodiazepineE. only intravenous administration of benzodiazepines should be
considered
18 . Which of the following anticonvulsant medications is contraindicated for a patient with idiopathic thrombocytopenic purpura? A. levetiracetamB. lorazepamC. phenytoinD. propofolE. sodium valproate
19 . A man is brought in with status epilepticus . He appears to be about 40 years old . His seizures are refractory to multiple doses of intravenous lorazepam and fosphenytoin . After rapid sequence intubation and initiation of propofol infusion therapy, a chest radiograph is obtained that shows a right upper lobe cavitary infiltrate . His glucose is normal, and he has a severe metabolic acidosis . What is the most appropriate empiric treatment for this 80-kg adult?A. enoxaparin, 80 mg subcutaneouslyB. magnesium sulfate, 6 g IVC. piperacillin/tazobactam, 4.5 g IV, and vancomycin, 1 g IVD. pyridoxine, 5 g IVE. thiamine, 100 mg IV, and 50 mL of 50% dextrose IV
20 . Which of the following is true regarding fosphenytoin?A. the adverse effect profile for fosphenytoin is similar to that for
intravenous phenytoinB. the cost per dose for fosphenytoin is about the same as for
intravenous phenytoinC. the diluent for fosphenytoin is similar to that for phenytoinD. fosphenytoin must be given at the same rate as intravenous
phenytoinE. intravenous fosphenytoin can safely be administered faster
than intravenous phenytoin
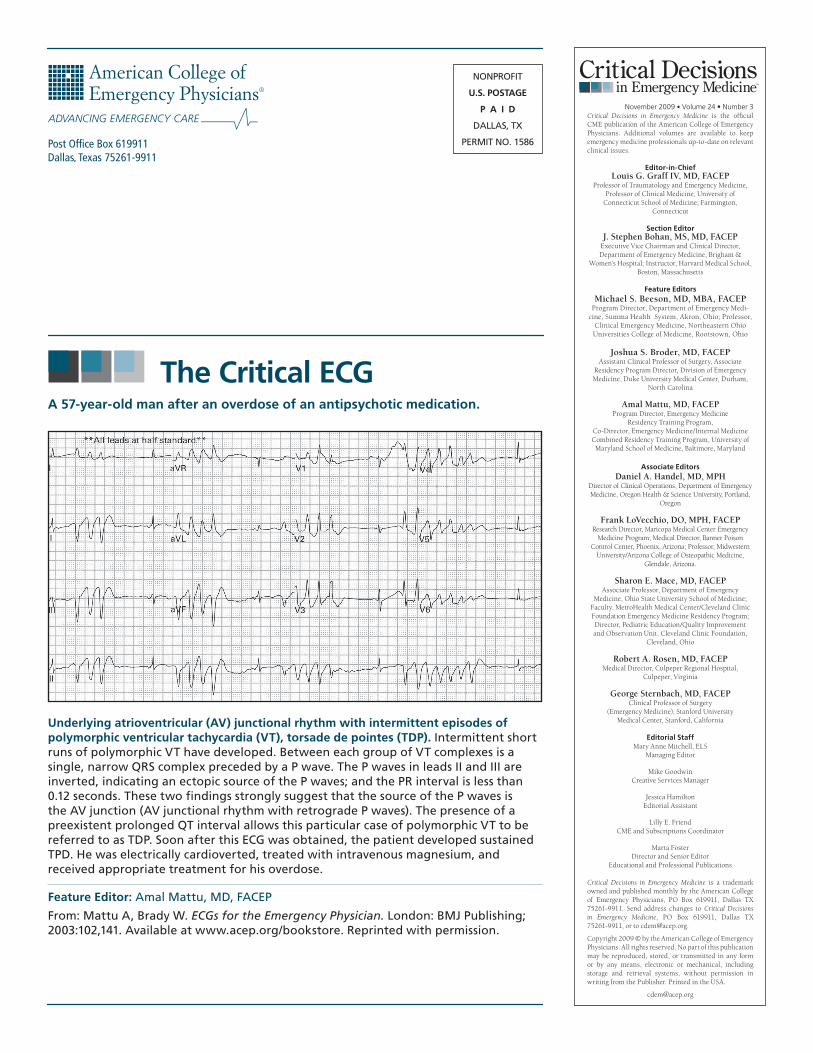
NONPROFIT
U.S. POSTAGE
P A I D
DALLAS, TX
PERMIT NO . 1586
The Critical ECG
November 2009 • Volume24•Number3Critical Decisions in Emergency Medicine is the official CME publication of the American College of Emergency Physicians. Additional volumes are available to keep emergency medicine professionals up-to-date on relevant clinical issues.
Editor-in-ChiefLouis G. Graff IV, MD, FACEP
Professor of Traumatology and Emergency Medicine, Professor of Clinical Medicine, University of
Connecticut School of Medicine; Farmington, Connecticut
Section EditorJ. Stephen Bohan, MS, MD, FACEP
Executive Vice Chairman and Clinical Director, Department of Emergency Medicine, Brigham &
Women’s Hospital; Instructor, Harvard Medical School,Boston, Massachusetts
Feature EditorsMichael S. Beeson, MD, MBA, FACEP
Program Director, Department of Emergency Medi-cine, Summa Health System, Akron, Ohio; Professor,
Clinical Emergency Medicine, Northeastern Ohio Universities College of Medicine, Rootstown, Ohio
Joshua S. Broder, MD, FACEP Assistant Clinical Professor of Surgery, Associate
Residency Program Director, Division of Emergency Medicine, Duke University Medical Center, Durham,
North Carolina
Amal Mattu, MD, FACEPProgram Director, Emergency Medicine
Residency Training Program,Co-Director, Emergency Medicine/Internal Medicine Combined Residency Training Program, University of Maryland School of Medicine, Baltimore, Maryland
Associate EditorsDaniel A. Handel, MD, MPH
Director of Clinical Operations, Department of Emergency Medicine, Oregon Health & Science University, Portland,
Oregon
Frank LoVecchio, DO, MPH, FACEPResearch Director, Maricopa Medical Center Emergency
Medicine Program; Medical Director, Banner Poison Control Center, Phoenix, Arizona; Professor, Midwestern
University/Arizona College of Osteopathic Medicine, Glendale, Arizona.
Sharon E. Mace, MD, FACEPAssociate Professor, Department of Emergency
Medicine, Ohio State University School of Medicine; Faculty, MetroHealth Medical Center/Cleveland Clinic Foundation Emergency Medicine Residency Program; Director, Pediatric Education/Quality Improvement and Observation Unit, Cleveland Clinic Foundation,
Cleveland, Ohio
Robert A. Rosen, MD, FACEPMedical Director, Culpeper Regional Hospital,
Culpeper, Virginia
George Sternbach, MD, FACEPClinical Professor of Surgery
(Emergency Medicine), Stanford University Medical Center, Stanford, California
Editorial StaffMary Anne Mitchell, ELS
Managing Editor
Mike GoodwinCreative Services Manager
Jessica HamiltonEditorial Assistant
Lilly E. FriendCME and Subscriptions Coordinator
Marta FosterDirector and Senior Editor
Educational and Professional Publications
Critical Decisions in Emergency Medicine is a trademark owned and published monthly by the American College of Emergency Physicians, PO Box 619911, Dallas TX 75261-9911. Send address changes to Critical Decisions in Emergency Medicine, PO Box 619911, Dallas TX 75261-9911, or to [email protected].
Copyright 2009 © by the American College of Emergency Physicians. All rights reserved. No part of this publication may be reproduced, stored, or transmitted in any form or by any means, electronic or mechanical, including storage and retrieval systems, without permission in writing from the Publisher. Printed in the USA.
Underlying atrioventricular (AV) junctional rhythm with intermittent episodes of polymorphic ventricular tachycardia (VT), torsade de pointes (TDP). Intermittent short runs of polymorphic VT have developed . Between each group of VT complexes is a single, narrow QRS complex preceded by a P wave . The P waves in leads II and III are inverted, indicating an ectopic source of the P waves; and the PR interval is less than 0 .12 seconds . These two findings strongly suggest that the source of the P waves is the AV junction (AV junctional rhythm with retrograde P waves) . The presence of a preexistent prolonged QT interval allows this particular case of polymorphic VT to be referred to as TDP . Soon after this ECG was obtained, the patient developed sustained TPD . He was electrically cardioverted, treated with intravenous magnesium, and received appropriate treatment for his overdose .
Feature Editor: Amal Mattu, MD, FACEP
From: Mattu A, Brady W . ECGs for the Emergency Physician. London: BMJ Publishing; 2003:102,141 . Available at www .acep .org/bookstore . Reprinted with permission .
A 57-year-old man after an overdose of an antipsychotic medication.


















