
Volume 1 Issue 19 KG Medi News - kghospital.com · Volume 1 Issue 19 Retail ... 612 elements in 120...
8
1 KG Medi News (English Monthly) May, 2016 Coimbatore Volume 1 Issue 19 Retail Price : Rs. 5 Annual Subscription : Rs. 50.00 Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore Dr G.Bakthavathsalam speaks... A hospital is generally considered to be a safe place for patients to get treatment for various kinds of ailments and diseases and to get back health and life. An ill equipped hospital would pose health hazards to patients and the visitors as there would be quite a number of causes for contracting “hospital acquired infections,” known in medical parlance as “Iatrogenic diseases.” Iatrogenic diseases can be defined as man- made diseases caused either by error or negligence or through infection caused by the presence of micro-organisms that might abound in a hospital. Negligence by a physician can happen in the form of leaving behind scissors or a piece of gauze inside the operated area or performing operation on the wrong side or carrying out mismatched blood transfusion or administering wrong dosage of drugs. Sources of Infection An otherwise healthy person can get infections when he/she comes in contact with a patient having bouts of cough or sneezing. Those who eat junk foods, addicted to smoking and drinking alcohol (whatever be the quality of liquor consumed) too are exposed to the risk of infection and develop physical conditions that might lead to morbidity and mortality. Iatrogenic diseases are not uncommon even in the highly civilized societies. For instance, 25 per cent of patients admitted in US “The Most Dangerous Place in Town is the Hospital,” said an American Doctor! It may be true in India as well?! hospitals are victims of one or other kind of infections. Therefore, it is advisable for the patients to get treatment at the right kind of hospitals that pay attention to their safety and facilitate early cure. Therefore, for standardizing the health care delivery system the European countries and the US have formulated stringent norms for the hospitals and healthcare providers to follow. Standardization of medical treatment is being stressed upon with the laudable objective of giving the best possible care to patient so as to improve their quality of life. Indian Scenario As far as India is concerned there exists the National Accreditation Board for Hospitals and Healthcare Providers (NABH) that grants quality certification to those hospitals which fulfill the rigorous norms set by the NABH. Of the 10,000 odd hospitals across the country, only 400 hospitals, including KG Hospital, have voluntarily sought to get NABH certification. Before granting accreditation the unbiased team of assessors of the NABH usually inspects a hospital for the duration of three days to look into as many as 612 elements in 120 measurable quality indicators. Thus, only those hospitals that fulfill all these criteria are eligible to get accreditation. It can be said for sure that KG Hospital has done extremely well in this regard. KG Hospital had got its first NABH accreditation way back in 2010, and the second NABH accreditation in 2013. Hat-Trick Now, KG Hospital is all set to get its third NABH accreditation and such a voluntary initiative has so far borne fruits owing to the committed hospital staff, right from the specialists to the housekeeping workers who constantly work towards accomplishing the Mission and Vision set by the hospital. In KG Hospital the doctors are dedicated, the nurses are like angels and all the supporting staff are superb. KG Hospital is unique in this aspect as it would soon be one among the 76 hospitals that have the honour of getting NABH accreditation for more than two times. KG Hospital could clinch such an honour because it has built up a wonderful team whose members have passion to deliver health care services in the best possible manner. It is a patient-centric hospital known for its accessibility, affordability, affability, adaptability and accountability. And of course, these sterling qualities has made KG Hospital “one above the crowd.” Rightly, the NABH team that visited KG Hospital recently, as part of assessment for granting third accreditation, had complemented stating that “KG Hospital stands out in terms of cohesive work culture, and, excellent infrastructure and patient care.”
Transcript of Volume 1 Issue 19 KG Medi News - kghospital.com · Volume 1 Issue 19 Retail ... 612 elements in 120...

1
KG Medi News(English Monthly)
May, 2016 Coimbatore
Volume 1 Issue 19
Retail Price : Rs. 5
Annual Subscription : Rs. 50.00
Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore
Dr G.Bakthavathsalam speaks...
A hospital is generally considered to be a safe
place for patients to get treatment for various
kinds of ailments and diseases and to get
back health and life. An ill equipped hospital
would pose health hazards to patients and
the visitors as there would be quite a number
of causes for contracting “hospital acquired
infections,” known in medical parlance as
“Iatrogenic diseases.”
Iatrogenic diseases can be defined as man-
made diseases caused either by error or
negligence or through infection caused by
the presence of micro-organisms that might
abound in a hospital.
Negligence by a physician can happen in the
form of leaving behind scissors or a piece of
gauze inside the operated area or performing
operation on the wrong side or carrying out
m i s m a t c h e d b l o o d t r a n s f u s i o n o r
administering wrong dosage of drugs.
Sources of Infection
An otherwise healthy person can get
infections when he/she comes in contact with
a patient having bouts of cough or sneezing.
Those who eat junk foods, addicted to
smoking and drinking alcohol (whatever be
the quality of liquor consumed) too are
exposed to the risk of infection and develop
physical conditions that might lead to
morbidity and mortality.
Iatrogenic diseases are not uncommon even
in the highly civilized societies. For instance,
25 per cent of patients admitted in US
“The Most Dangerous Place in Town is the Hospital,”
said an American Doctor!
It may be true in India as well?!
hospitals are victims of one or other kind of
infections. Therefore, it is advisable for the
patients to get treatment at the right kind of
hospitals that pay attention to their safety and
facilitate early cure.
Therefore, for standardizing the health care
delivery system the European countries and
the US have formulated stringent norms for
the hospitals and healthcare providers to
follow. Standardization of medical treatment
is being stressed upon with the laudable
objective of giving the best possible care to
patient so as to improve their quality of life.
Indian Scenario
As far as India is concerned there exists the
National Accreditation Board for Hospitals
and Healthcare Providers (NABH) that grants
quality certification to those hospitals which
fulfill the rigorous norms set by the NABH.
Of the 10,000 odd hospitals across the
country, only 400 hospitals, including KG
Hospital, have voluntarily sought to get
NABH cer t i f icat ion. Before granting
accreditation the unbiased team of assessors
of the NABH usually inspects a hospital for the
duration of three days to look into as many as
612 elements in 120 measurable quality
indicators.
Thus, only those hospitals that fulfill all these
criteria are eligible to get accreditation. It can
be said for sure that KG Hospital has done
extremely well in this regard. KG Hospital
had got its first NABH accreditation way back
in 2010, and the second NABH accreditation
in 2013.
Hat-Trick
Now, KG Hospital is all set to get its third
NABH accreditation and such a voluntary
initiative has so far borne fruits owing to the
committed hospital staff, right from the
specialists to the housekeeping workers who
constantly work towards accomplishing the
Mission and Vision set by the hospital.
In KG Hospital the doctors are dedicated, the
nurses are like angels and all the supporting
staff are superb. KG Hospital is unique in this
aspect as it would soon be one among the 76
hospitals that have the honour of getting
NABH accreditation for more than two times.
KG Hospital could clinch such an honour
because it has built up a wonderful team
whose members have passion to deliver
health care services in the best possible
manner. It is a patient-centric hospital known
for its accessibility, affordability, affability,
adaptability and accountability.
And of course, these sterling qualities has
made KG Hospital “one above the crowd.”
Rightly, the NABH team that visited KG
Hospital recently, as part of assessment for
g r a n t i n g t h i r d a c c re d i t a t i o n , h a d
complemented stating that “KG Hospital
stands out in terms of cohesive work culture,
and, excellent infrastructure and patient
care.”

2
KG Hospital received appreciation from the
National Accreditation Board for Hospitals
and Healthcare Providers (NABH) team that
recently carried out assessment of the hospital
for giving quality certification for the third
time.
The three-member NABH team has termed
KG Hospital as “an excellent hospital having
good infrastructure, offering good patient care
and adopting good management practices. At
the helm of affairs is its Chairman Dr
G.Bakthavathsalam who has astounding
passion and involvement in the field of
medical care and obviously, in the hospital,
quality percolates from the top.”
Above all, the team has likened KG Hospital
to “a cohesive family unit” that is working in
unison to achieve the common goal of
rendering health care services to the
satisfaction of patients.
The team comprising Principal Assessor
Dr Jayadeep M.Gadhavi and two Assessors
Dr R.K.Ranyal and Ms M.M.Leessamma
examined the medical equipment and the
kind of services provided by al l the
departments, including the Intensive Care
Unit, in the hospital for three days, ie., from
May 12 to 14, 2016.
Unique Hospital
After completing the assessment, Dr Jayadeep
M.Gadhavi told the formal gathering of
doctors, the heads of departments and
managers of the hospital that “overall I am
very much satisfied with the performance of
KG Hospital.” He further said that so far he
had inspected over 75 hospitals across the
coun t r y f o r t he pu rpose o f g i v i ng
accreditation.
But he found KG Hospital to be the first one to
pro-act ive ly put in p lace necessary
infrastructure and adopt the best hospital
management practices. In his opinion the
ambulance service, blood bank, bio-medical
engineering department, endoscopy
department, pharmacy, Central
Sterile Service Department, main
reception, stores, medical records
department and human resource
department were doing good work.
Dr Gadhavi had a special word of
praise for KG Hospital Chairman
Dr G.Bakthavathsalam who he said
remained dedicated to medical
profession even at the age of 73. “If all
the physicians show the same kind of
involvement and passion, KG Hospital can do
wonders and such a situation would help the
hospital in case of litigation too,” he said.
Dr Gadhavi praised the nurses of KG Hospital
for their excellent services which he attributed
to the good training imparted to them.
However, he said that training was not just a
one-time affair but a continuous process. He
was thankful to the medical fraternity, para-
medical staff and all other employees of KG
Hospital for extending their “kind co-
operation” to the NABH team during its visit.
Facilitators as Appreciators
Dr R.K.Ranyal, one of the Assessors, clarified
that “the visit of the NABH is not intended to
be a fault-finding one, but a fact finding one.
The NABH team has come down here as
facilitators to bring out the best in what you
have and also to learn from you.”
He said, “Hats off to the ambulance drivers of
KG Hospital who are well aware of the Code
Blue procedures (medical emergency), Basic
Life Support System (BLS) and the Advanced
Cardiac Life Support System (ACLS).”
It was an indication as to how knowledge
about health care exigencies had percolated
down the line in KG Hospital. Dr Ranyal
suggested that during an emergency situation
or a disaster the hospital staff should remain
alert to locate the patients by calling out “who
is the patient?” as the patients need not
necessar i ly be ly ing down for easy
identification. It would enable the staff to
render timely medical aid to the affected
people.
Dr Ranyal said that the areas of conflict
identified by the team did not mean that it
would take up AK-46 or AK 47 to sort them
out. It held healthy discussions with the
hospital management on how to get things
right. He emphasized the point that quality
assessment was an ongoing process and did
not stop with a single visit.
Appreciating the total involvement of KG
Hospital Chairman Dr Bakthavathsalam and
his passion for rendering health care services,
Dr Ranyal called upon each and every staff of
the hospital to emulate the Chairman.
Assessor Ms Leessamma thanked the
management for i t s hospi ta l i ty and
appreciated the hard work being put in by the
nursing and housekeeping staff.
Good Work Culture
Chairman Dr Bakthavathsalam in his
introductory speech profusely thanked all
doctors, managers, nurses and employees of
the hospital for their tireless efforts in the past
many years to comply with the NABH norms.
Dr Bakthavathsalam emphatically said that
for KG Hospital patients’ interests and safety
came first and in the 42 years of its existence it
had been successfully implementing its
Mission, thanks to the right work culture the
hospital had evolved.
KG Hospital gets kudos from NABH team
Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore

3Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore
4Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore
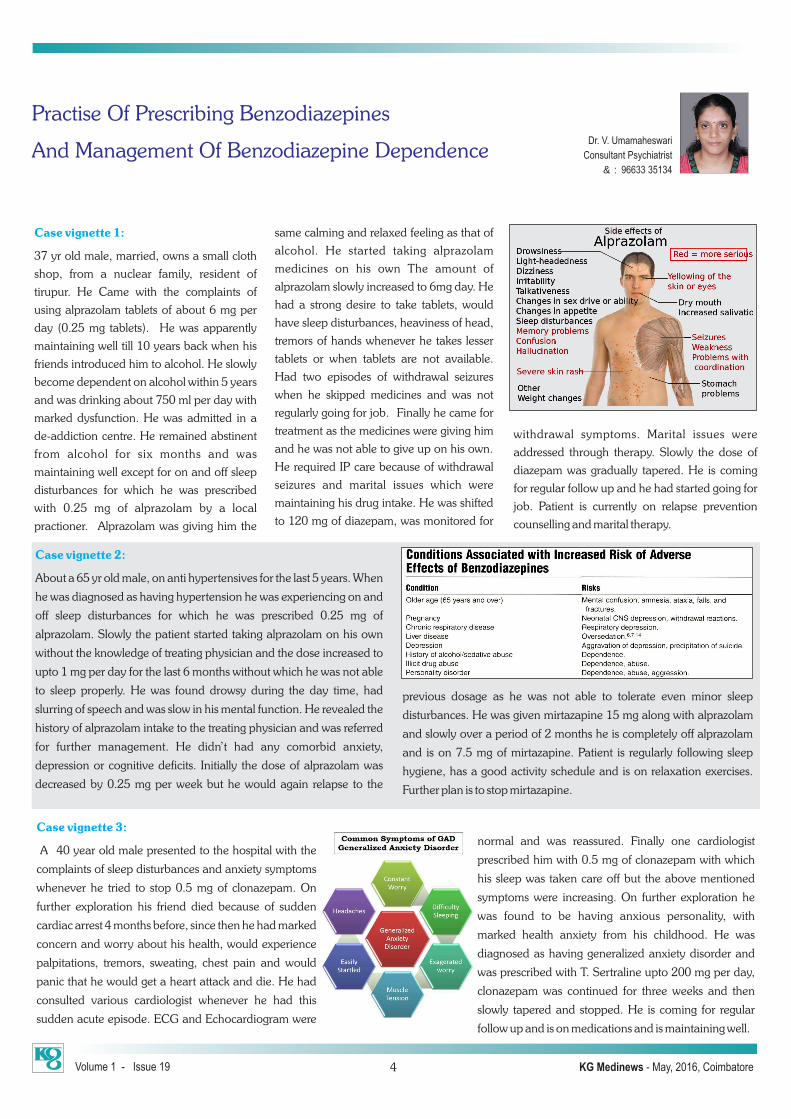
Case vignette 1:
37 yr old male, married, owns a small cloth
shop, from a nuclear family, resident of
tirupur. He Came with the complaints of
using alprazolam tablets of about 6 mg per
day (0.25 mg tablets). He was apparently
maintaining well till 10 years back when his
friends introduced him to alcohol. He slowly
become dependent on alcohol within 5 years
and was drinking about 750 ml per day with
marked dysfunction. He was admitted in a
de-addiction centre. He remained abstinent
from alcohol for six months and was
maintaining well except for on and off sleep
disturbances for which he was prescribed
with 0.25 mg of alprazolam by a local
practioner. Alprazolam was giving him the
same calming and relaxed feeling as that of
alcohol. He started taking alprazolam
medicines on his own The amount of
alprazolam slowly increased to 6mg day. He
had a strong desire to take tablets, would
have sleep disturbances, heaviness of head,
tremors of hands whenever he takes lesser
tablets or when tablets are not available.
Had two episodes of withdrawal seizures
when he skipped medicines and was not
regularly going for job. Finally he came for
treatment as the medicines were giving him
and he was not able to give up on his own.
He required IP care because of withdrawal
seizures and marital issues which were
maintaining his drug intake. He was shifted
to 120 mg of diazepam, was monitored for
withdrawal symptoms. Marital issues were
addressed through therapy. Slowly the dose of
diazepam was gradually tapered. He is coming
for regular follow up and he had started going for
job. Patient is currently on relapse prevention
counselling and marital therapy.
Practise Of Prescribing Benzodiazepines
And Management Of Benzodiazepine DependenceDr. V. Umamaheswari
Consultant Psychiatrist
& : 96633 35134
Case vignette 2:
About a 65 yr old male, on anti hypertensives for the last 5 years. When
he was diagnosed as having hypertension he was experiencing on and
off sleep disturbances for which he was prescribed 0.25 mg of
alprazolam. Slowly the patient started taking alprazolam on his own
without the knowledge of treating physician and the dose increased to
upto 1 mg per day for the last 6 months without which he was not able
to sleep properly. He was found drowsy during the day time, had
slurring of speech and was slow in his mental function. He revealed the
history of alprazolam intake to the treating physician and was referred
for further management. He didn’t had any comorbid anxiety,
depression or cognitive deficits. Initially the dose of alprazolam was
decreased by 0.25 mg per week but he would again relapse to the
previous dosage as he was not able to tolerate even minor sleep
disturbances. He was given mirtazapine 15 mg along with alprazolam
and slowly over a period of 2 months he is completely off alprazolam
and is on 7.5 mg of mirtazapine. Patient is regularly following sleep
hygiene, has a good activity schedule and is on relaxation exercises.
Further plan is to stop mirtazapine.
Case vignette 3:
A 40 year old male presented to the hospital with the
complaints of sleep disturbances and anxiety symptoms
whenever he tried to stop 0.5 mg of clonazepam. On
further exploration his friend died because of sudden
cardiac arrest 4 months before, since then he had marked
concern and worry about his health, would experience
palpitations, tremors, sweating, chest pain and would
panic that he would get a heart attack and die. He had
consulted various cardiologist whenever he had this
sudden acute episode. ECG and Echocardiogram were
normal and was reassured. Finally one cardiologist
prescribed him with 0.5 mg of clonazepam with which
his sleep was taken care off but the above mentioned
symptoms were increasing. On further exploration he
was found to be having anxious personality, with
marked health anxiety from his childhood. He was
diagnosed as having generalized anxiety disorder and
was prescribed with T. Sertraline upto 200 mg per day,
clonazepam was continued for three weeks and then
slowly tapered and stopped. He is coming for regular
follow up and is on medications and is maintaining well.
5Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore
Lessons Learnt From These Patients:
The first case is an example of illicit drug
abuse. He had strong history for addiction.
Had alcohol dependence and prescription of
benzodiazepine made him to switch over to
b e n z o d i a z e p i n e d e p e n d e n c e a n d
unresolved marital discord was the
maintaining factor for his dependence.
The second case is an example of therapeutic
drug over dose, where the pat ient
continuous to abuse the medicine prescribed
to him by a physician and slowly became
dependent on it and had side effects with the
medicines.
The third patient is an example for anxiety
disorder, which was not recognised and
treated promptly.
Dont’s
Avoid prescr ib ing benzodiazepines
particularly in elderly as there is high chance
for sedation, falls, fracture and memory
disturbances.
Avoid benzodiazepines in individuals with
history of addiction / family history of
addiction.
Avoid using psychiatric medicines like
anxiolytic and antidepressants which comes
in combination with benzodiazepines as
people would abuse them.
Low dose of benzodiazepines mask
underlying depression and anxiety, and
prescribing benzodiazepines in such
individuals’ results in increase in severity of
the underlying illness and it becomes difficult
to treat in the long run.
Avoid benzodiazepines in patient with
delirium as it would worsen delirium.
(Benzodiazepines need to be given only in
a l c o h o l w i t h d r a w a l d e l i r i u m a n d
benzodiazepine dependence).
Avoid benzodiazepines in patients with
dementia and head injury as it would worsen
cognitive deficits.
Do’s
Use benzodiazepines only when required.
Make sure that the patient gets medicines only
for the prescribed duration and not more than
that.
Medicines need to be supervised by the family
members.
Risk of continued usage without the treating
physician’s knowledge needs to be explained.
S l e e p d i s t u r b a n c e s a re t h e i n i t i a l
manifestations of majority of the psychiatric
disorders like depression and anxiety disorder.
So all patients presenting with sleep
disturbances and unexplained pain need to be
assessed for underlying psychiatric disorders
and require proper psychiatric help.
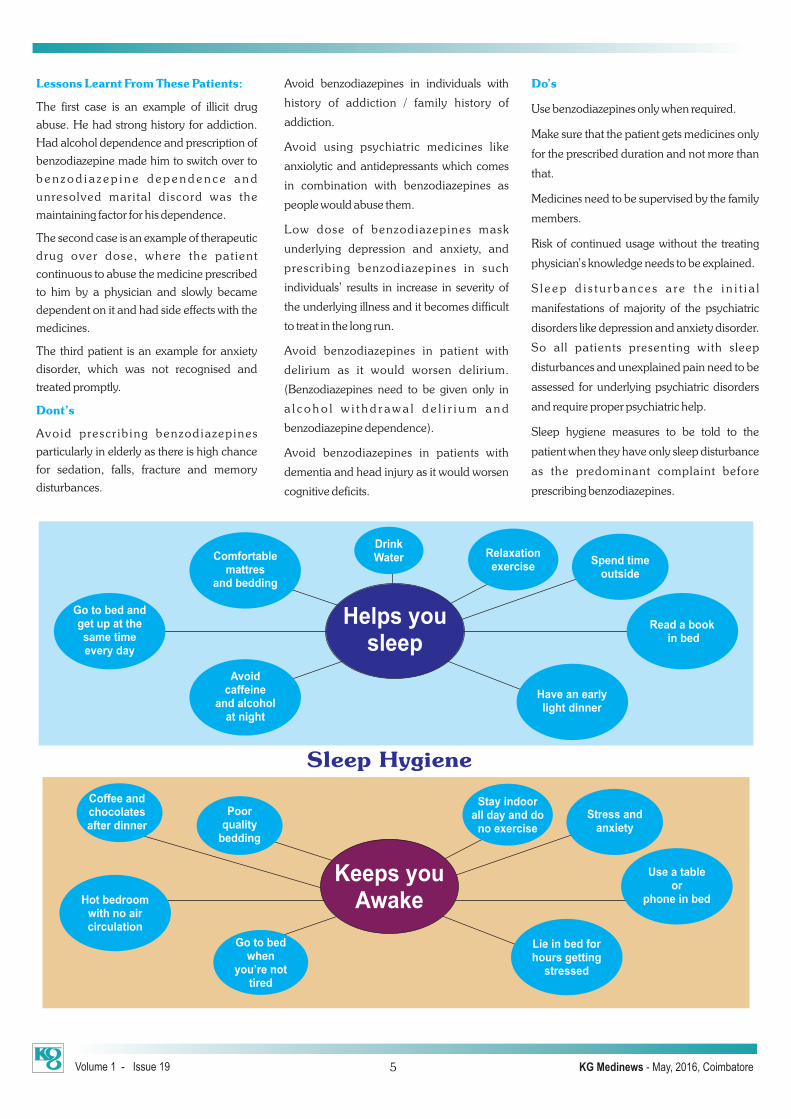
Sleep hygiene measures to be told to the
patient when they have only sleep disturbance
as the predominant complaint before
prescribing benzodiazepines.
DrinkWaterComfortable
mattresand bedding
Go to bed and get up at the same time every day
Avoidcaffeine
and alcoholat night
Spend time outside
Read a book in bed
Relaxation exercise
Have an early light dinner
Helps yousleep
Poor quality
bedding
Coffee andchocolatesafter dinner
Hot bedroomwith no aircirculation
Go to bedwhen
you’re nottired
Stress andanxiety
Use a tableor
phone in bed
Stay indoorall day and do
no exercise
Lie in bed for hours getting
stressed
Keeps youAwake
Sleep Hygiene

Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore6
‘Hare Krishna’
Stapedotomy at 68
Stapedotomy is the surgical treatment of
choice of Otosclerosis for the ear.
Mr. Ramalingam, 68 years male from Ooty
was suffering from hearing loss and mild
tinnitus both ears for the past 45 years. He has
consulted many ENT doctors at Chennai and
Coimbatore. He was afraid of the ear surgery
since the prognosis of the surgery –
Stapedotomy is ALL (or) None law. He was
told that either he may get back the normal
hearing or may lose the remaining hearing
after the surgery.
He came to us (KG Hospital) to consult me
regarding the treatment. I examined him and
diagnosed as otosclerosis both ears. I
explained him in detail the pros and cons and
the prognosis of the surgery - Stapedotomy
and convinced him for the surgery.
He underwent right Stapedotomy and Teflon
Piston with vein graft interposition. He has
regained his normal hearing during the
surgery on the table itself. He was able to hear
the sounds and noise of the world and the first
sound he heard was HARE KRISHNA, HARE
RAMA Nama Sangeerthan in the recovery
room. He was very much excited and very
happy to hear lord Krishna’s sangeerthan. He
feels he has got a second life with good
hearing at the age of 68 years.
The age 68 with presbyacusis is not an
absolute contraindication for Stapedotomy.
“We dress the wound. He who heals it”
Caution:
Root canal treatment (Dental) with high
intensity drill sound may produce accustic
trauma and sudden sensory normal hearing
in stapedotomy patients.
Result & Conclusion:
Long term followup of 10 years in 500 cases
with vein graft interposition technique
Air bone gap before surgery (AB gap) – 45db
Air bone gap after surgery– 10db (average)
Tinnitus – 50% relieved, 30% remain the
same, 5% increased.
Highly respected and revered Dr G.Bakthavathsalam Sir,
My loveable greetings to you.
I recently read the Tamil book “Idhayam Oru Koil” (“Heart is a Temple”) authored by you
from cover to cover, without leaving even a single sentence. I have read quite a lot of literary
works, including poetry, essays, novels and story books. This is the first time that I have read a
book related to medicine and thoroughly enjoyed it.
The book gives an interesting and tasteful reading on how to lead a healthy life. The Koran,
Holy Book of Islam, says:
“One who does not have the mind to say ‘No’ has got unparalleled kindness;
One who listens to and heeds the distress call of others looks into the thinking and
heart of the sufferer;
One who looks at the external appearance is a human;
But, one who looks at the heart is God.”
The Koran is considered to be a panacea for all ailments and this truth can be understood
from the following lines: “It is but natural for man to fall sick--in such cases, it is the
responsibility of the sick to approach physicians to get medicines—but it is God’s grace that
makes the medicines work.”
The title of each chapter in your book conveys brilliant ideas in a crisp manner. The significant
aspect of the book is the foreword given by my best friend and Health Secretary
Mr V.K.Subburaj, I.A.S, and its release by honourable former President Dr A.P.J.Abdul
Kalam, who was the guiding star of the young generation.
I deem it a pleasure to quote from the book some of the shining lines which have greatly
impressed me:
“If you don’t take proper care of the heart that is beating lakhs of time, you will
lose lakhs (of money).”
“Like a confined air, stuffing the heart with very many unwanted thoughts will
lead to complications.”
“Today’s youth in the name of searching Heaven are heading to Hell.”
“The classic songs would lose their rhythm if re-mixing is improperly done;
similarly, if the rhythm of heart changes the heart will get spoiled.”
Former Chief Minister Doctor Kalaignar (Mr M.Karunanidhi) has stated that: “One who takes
preventive measure is intelligent and one who struggles after getting ailment is unwise.”
You have mentioned in your book how an actor earned crores of rupees by stylishly puffing
cigarettes in movies and how such a mannerism has spoiled the health of many youths who
copied him. It clearly shows that you are not after money but are sincerely propagating health
aspects.
You have stressed the importance of having whole body test and examining the condition of
the heart through the 128 Slice CT Scan.
Therefore, the “Idhayam Oru Koil” book, replete with healthy tips, should be read by every
citizen of India. Though I have a lot more to say, for the sake of brevity I conclude with the
following sentence:
“May Allah bless you with long life and let your health care services grow further.”
V.M.A.Shalappha
Film Director and Script Writer
“All Glory to God” —A Film Director’s encomiums for Dr G.B’s book
Dr. S. Kaliannan
ENT Surgeon
& : 9443425136
Appreciation

Case No.1:
55 years old male, smoker came with complaints of chronic cough with
expectoration for 3 months. He denied history of haemoptysis, fever,
shortness of breath, weight loss or loss of appetite. Chest X-ray showed
left upper zone homogenous opacification suggestive of
consolidation. Blood biochemistry were normal. ECG was normal.
Further evaluation with CT chest revealed left upper lobe complete
collapse consolidation with a mass lesion in the left hilar region
extending to left subcarinal region and engulfing left pulmonary artery
suggestive of bronchogenic carcinoma. Bronchoscopy showed
complete occlusion of left upper lobe bronchus by the extincic mass
with mucosal invasion. No endo bronchial mass lesion was visible.
Hence a transbronchial needle aspiration was done with a special
needle (size 22 G) which can pass through bronchoscope from
subcarinal and left hilar region with a special attention not to puncture
the pulmonary vessels which were very close to the puncture site. Even
though there was a minimal bleed which could be controlled with local
hemostat, no major bleed encountered. The needle aspirate was
prepared in to s l ides and the cy tof ixed s l ides showed
adenocarcinomatous cells on HPE.
TBNA is a minimally invasive procedure that provides a nonsurgical
means to diagnose and stage bronchogenic carcinoma by sampling
the mediastinal lymph nodes. The procedure allows for sampling
tissue through the trachea or bronchial wall, and sampling of tissue
beyond the vision of the dedicated operator. In addition to the
equipment needed for bronchoscopy, the equipment needed
specifically for TBNA include TBNA needles, which are designed to
pass through a bronchoscope without causing damage and to be
flexible enough to facilitate the positioning of the bronchoscope, yet
rigid enough to penetrate the airway wall. Two types of TBNA needles,
cytology needles and histology needles, should be available for the
procedure. The most common potential complications are bleeding,
pneumothorax, or pneumomediastinum. Significant bleeding rarely
occurs even after a major vessel puncture. Fever and bacteremia have
been reported following TBNA, although this may be related to the
bronchoscopic procedure itself rather than this specific technique.
IBNA:
Case No.2:
75 year old male, smoker, was hospitalized with acute respiratory
failure. He had underlying severe LV dysfunction (ejection fraction
25%) and ischaemic cardiomyopathy. He had fever for 1 week along
with cough with expectoration. He had severe hypoxia and
hypercarbia on admission. He was stabilized with non-invasive
ventilation and diuretics along with antibiotics. Chest X-ray showed
features of pulmonary oedema with left upper lobe consolidation with
cavitation. Further CT chest confirmed the above findings. Even
though the patient had an initial improvement, he required continuous
non-invasive ventilation support and oxygen without which he
desaturated significantly down to 75% on room air. An infective focus
was strongly suspected which could be the cause for acute worsening
of LVD and pulmonary oedema. His sputum examination did not
show AFB or any gram stained organisms as he could not bring out
sputum properly. Hence Bronchoscopy with BAL was planned. The
risks of bronchoscopy in hypoxic patient with severe LVD including
sudden cardiorespiratory arrest, cardiac arrhythmias, pulmonary
oedema, pneumothorax and airway bleed were discussed with the
family in detail. Family consented for bronchoscopy with NIV support.
Bronchoscopy under NIV support was successfully done under local
anaesthesia and IV sedation and BAL sample obtained and procedure
was uneventful.
Bronchoscopy in patients with respiratory disorders can be
challenging. The bronchoscope occupies 10 –15% of the normal
tracheal lumen and can increase the work of breathing and decrease
PaO2 by 10 – 20 mm Hg, which can cause respiratory complications
and cardiac arrhythmia. Hypoxemia occurs with insertion of the
bronchoscope through the glottis into the trachea, and becomes worse
when local anesthetics or saline solution is instilled into the lower
airways. Bronchoalveolar lavage is associated with worse oxygen
desaturation than when lavage is not done. Furthermore, suction
Interesting BronchoscopiesDr. S. Santhakumar
Pulmonologist
& : 99946 52670
7Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore
LUL Complete Occlusion TBNABronchoscopy with NIV support.

RNI No. TNENG/2014/59720
Published by Dr. G. Bakthavathsalam, on behalf of K. Govindaswamy Naidu Medical Trust (KG Hospital), Published from 5, Govt. Arts College Road, Coimbatore - 641 018. Tamil Nadu and printed by A. Dhanasekaran, at The Safire Offset Printers, Vembakkottai Road, Ayyanar Colony, Sivakasi - 626123. Editor : Dr. G. Bakthavathsalam
Registration No : CB/127/2015-17
8
Volume 1 - Issue 19 KG Medinews - May, 2016, Coimbatore
For the benefit of the poor people who
might need surgeries for various diseases,
KG Hospital has organized a two month-
long “General surgery camp” in the
hospital premises here Started on May
1st. It will go on till June 30, according to
Dr G.Bakthavathsalam, Chairman of the
hospital.
I n a s t a t e m e n t r e l e a s e d h e r e
Dr Bakthavathsalam has stated that
during the camp period free consultation
would be given to the patients. And those
patients who would be identified as the
probable candidates for surgeries, the
diagnosis and operation would be
performed at concessional rates ranging
from 25 to 50 per cent.
Dr. Bakthavathsalam has further stated
that “the 500-bedded multi-specialty
tertial care KG Hospital is equipped with
ultra modern medical equipment for
doing perfect diagnosis for all kinds of
diseases. The specialists in the respective
fields of medicine/surgery would attend
on the patients and perform the surgeries
with utmost clinical precision.”
A team of experts headed by leading
surgeon Dr V. P. Shanmugasundaram,
who is Chief of the General Surgery
Department and Chief Laparoscopic and
KG Hospital performs General Surgeries at 50 % concessional rate
Transplantation Surgeon of the hospital,
would screen the patients and organise the
required surgeries.
The concess ional scheme would be
applicable to the following surgeries
Ÿ Advanced laparoscopic hysterectomy
Ÿ Tumour in the neck
Ÿ Tumour in the uterus
Ÿ Gall bladder
Ÿ Pancreas and liver surgeries
Ÿ Gastroenterology
Ÿ Varicose vein
Ÿ Appendicitis
Ÿ Hernia
Ÿ Piles and Intestinal problems
Ÿ Family planning
Ÿ Tonsillitis
Ÿ Circumcision and surgery for torsion
testicles
and any cancerous growth in the body
during bronchoscopy reduces the end-
expiratory volume and positive end-
expiratory pressure and thus causes alveolar
closure. Though hypoxemia is associated
with cardiac arrhythmias in 11– 40% of
p a t i e n t s w h o u n d e r g o f i b e r o p t i c
bronchoscopy, these cardiac rhythm
disturbances are rarely clinically important.
The American Thoracic Society, however,
recommends avoiding flexible bronchoscopy
and bronchoalveolar lavage in patients with
hypoxemia that cannot be corrected to at
least a PaO2 of 75 mm Hg or to an arterial
oxygen saturation of 90% with supplemental
oxygen. In these higher-risk patients the
traditional alternatives are avoidance of
bronchoscopy and empirical treatment, or
intubation and mechanical ventilation to
assure adequate vent i la t ion dur ing
bronchoscopy.
Endotracheal intubation and mechanical
vent i la t ion have potent ia l ly severe
complications, however, and in many
patients NIV is a valid alternative to
intubation, especially in immuno suppressed
patients and in critically ill patients with
pneumonia. Single and multi center
randomized studies found, however, that in a
heterogeneous group of patients with a
history of cardiac or respiratory disease and
who developed respiratory distress during the
first 48 hours after extubation, the addition of
NIV to standard medical therapy did not
improve re-intubation rate, hospital mortality,
intensive-care-unit stay, or hospital stay. In
fact, in that patient population NIV may be
harmful and increase the risk of death from
cardiac ischemia, respiratory muscle fatigue,
aspiration pneumonitis, or complications of
emergency intubation.
D. Rajesh. &�:� 98433 21803
P. Sheeba &�:� 90476 55121
For details contact :


















