Quantitative History and Historical Numeracy Margo Anderson History Department margo.

VOL XXX NO 2 APRIL 2009
ACCESS
IN THIS ISSUE:bUILdINg A CULTURE Of PRIVACy • NATIONAL NURSINg wEEk 2009 •LAbOUR mObILITy • CONTINUINg COmPETENCy UPdATE • CLINICAL CORNER • NURSES Of NOTE and more!

CounCil
Front Row L-R: bev white (President - Elect), kathy watkins, Peggy O’brien-Connors, Jim feltham (President), Janice brennan, Cathy burke. Second Row L-R: Pegi Earle (Ed), kathy fitzgerald, Sandra gear, bea Courtney, Sandra Evans. Missing from photo: Ray frew, Lynn miller, beverly Pittman, margo Cashin, Joan downey
ACCESS VOL XXX NO 2 APRIL 2009
ARnnl STAFF
Advertise in the next issue of ACCESS Contact Janice lockyer, Director of Communications, ARnnl [email protected] 753-6198
55 military Road St. John’s, NL A1C 2C5Ph: (709) 753-6040 fax: (709) 753-4940 Toll free: 1-800-563-3200email: [email protected] www.arnnl.ca
©Association of Registered Nurses of Newfoundland and Labrador (ARNNL). All rights reserved. for editorial matters, please contact the editor. The views and opinions expressed in the articles and advertisements are those of the authors or advertisers and do not necessarily represent the policies of ARNNL.
Executive director
director of Regulatory Services
director of Policy & Practice
director of Communications
director of Corporate Services
Nursing Consultant – Policy & Practice
Nursing Consultant – Regulatory Services &Advanced Practice
Project Consultant QPPE
Research Analyst & ARNNL Trust
Administrative Assistant to Executive director & Council
Administrative Assistant to Consultants & workplace Representative Program
Administrative Assistant to Consultants, ACCESS & QPPE & Registration
Administrative Assistant to Consultants & Professional Conduct Review Administrative Assistant toConsultants
Pegi Earle
michelle Osmond
Lynn Power
Janice Lockyer
Elizabeth dewling
Siobhainn Lewis
beverley mcIsaac
JoAnna bennett (part-time)
Julie wells
Christine fitzgerald
Jeanette gosse
Jennifer Rideout
Colleen Jones
Nicole ghaney
1 |
2 |
3 |
4 |
5 |
6 |
8 |
9 |
10 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
18 |
19 |
20 |
message from the President
Cameron Inquiry: Improving Patient Safety
duty to Report: Advocacy in Action
Tribute to John Pelley
Personal Health Information Act: building a Culture of Privacy
Labour mobility
Continuing Competence Program Update
Nurses of Note
NATIONAL NURSINg wEEk 2009
greening Health Care & ‘7 Acts of green’
making the Connection
Vietnam Nurses Association
‘Just a Nurse’
workplace Rep Profiles
ARNNL TRUST
goings On
ARNNL Announces
Clinical Corner
A New way to Teach Nursing Skills
ACCESS is the official publication of the Association of Registered Nurses of Newfoundland and Labrador.
ACCESS is published three times a year in January, may and September. Subscriptions are available for $25.00 per year.
ON THE COVER: The CNA board of directors. front Row L to R: Paula bilton, yRNA; kathy doerksen, CRNm; Val Cartmel, CRNbC; kristy feltham, RNANT/NU; margaret Hadley, CARNA; Rachel bard, Chief Executive Officer; Judith Shamian, CNA President-Elect. back Row L to R: wendy fucile, RNAO; monique Cormier-daigle, NANb/AIINb; Sandra Easson-bruno, Associate member Representative; Colleen Toye, SRNA; Hubert gauthier, Public Representative; Jim feltham, ARNNL; kaaren Neufeld, CNA President; mary Hughes, ARNPEI.
for more information on the Coat of Arms visit www.cna-aiic.ca/CNA/about/history/centennial/coat_of_arms/default_e.aspx
Photo by: Teckles Photography Inc. CNA Coat of Arms march 2009 board meeting Ottawa, ON
Janice Lockyer, director of Communications
Vanessa Stockley, granite Studios
Jennifer Rideout, ARNNL
EDiToR |
CREATivE DESign |
ADminiSTRATion |
Jim Feltham, President 2008 – 2010Bev White, President-Elect 2008 – 2010Ray Frew, Public Representative 2007 – 2010Bea Courtney, Public Representative 2008 – 2011 (February)Kathy Watkins, St. John’s Region 2006 – 2009Lynn Miller, Labrador Region 2008 – 2011Janice Brennan, Western Region 2007 – 2010Sandra Evans, Central Region 2008 – 2011Sandra Gear, Eastern Region 2007 – 2010Beverly Pittman, Northern (Grenfell) Region 2007 – 2010Peggy O’Brien-Connors, Advanced Practice 2006 – 2009Kathy Fitzgerald, Practice 2006 – 2009Margo Cashin, Practice 2007 – 2010Joan Downey, Nursing Education/Research 2008 – 2011Cathy Burke, Administration 2007 – 2010

1
James w. feltham , RN, bN, CNCC(C)
Message from the President
A s we prepare another edition of Access for print, a number of issues have captured the minds of nurses in the province. from contract negotiations,
to the new budget, to the ongoing nursing shortage, these are challenging times for our profession. but in as much as we have challenges to face, we are lucky – lucky to have the opportunity to move ahead with our lives and enjoy the benefits of being highly educated, qualified professionals. As recent events surrounding the crash of Cougar flight 491 have served to remind us, yet
again, we must see the positive and live life to the fullest.As I write this, we are getting ready to celebrate National Nursing week. The theme this year -
Nursing: you Can’t Live without It! - focuses on how nursing is very important to the lives of people in our communities and to the overall health of the population. After hearing Suzanne gordon speak at the CNA Leadership Conference in Toronto in february, I have a new appreciation for our profession. According to gordon, “Nurses save lives, prevent suffering and save money. Canadians need a nursing profession that wears its brain on its sleeve not its heart. Caring is a knowledge not a virtue. both patients and registered nurses need the four ‘R’s’ respect, recognition, rewards and resources especially if we want to avoid turning nurses into patients.”
The four ‘R’s’ are more important now than ever before. As I write this, the outcome of contract negotiations is unknown. while the ARNNL is not involved in the negotiation process, it is still my hope that the issue will be settled in a respectful manner so we can return our focus to the task at hand - providing a publicly funded, not for profit health care system.
during the Leadership Conference, I was also struck by The Seven Ethics of Effective Leadership. These Ethics are something we should keep in mind at all times:
I would also like to take a few moments to tell you about some of the discussion at the march CNA board meeting. The CNA is an active and important part of nursing in this country and we should all endeavour to understand the work it does. At the meeting, the board approved position statements on global Health and Equity and another on Peace and Security. It was also decided that the issues of the increasing utilization of unregulated health workers, and utilizing nurses as solution providers for a sustainable public health system would be discussed at the 2009 CNA Annual meeting.
I also attended the unveiling of the magnificently sculpted CNA Coat of Arms, the culminating activity of the CNA’s Centennial Celebrations. One of the striking images on this Coat of Arms is the lion holding the Canada Health Act which I saw as nurses defending the principles of the Canada Health Act as fundamental to the health of all Canadians.
I would like to conclude by discussing the Cougar Helicopter crash of march 12th. I know a number of RN’s have been affected by this accident through the loss of a husband, uncle or classmate. for me, the crash brought home the reality of the danger people of our province often face in earning a living and how surprisingly small the degree of separation is in our province when 18 people are involved in a tragedy.
you will notice in this edition, we have a tribute to John Pelley, RN, who died as a result of the crash. The tribute was written with the cooperation of John’s close friend Shane fudge, RN, and the permission of his wife, Lori. ARNNL sent condolences to the family and friends of all involved and received a number of condolences from other Nursing organizations across the country – including the CNA, the College of Registered Nurses of manitoba, the Registered Nurses’ Association of Ontario, the Nurses Association of New brunswick, the College of Registered Nurses of british Columbia, Victorian Order of Nurses, western Health and government of NL to mention a few. John Pelley was a young man who loved his career, his work, and most of all his friends and family, his lasting legacy is the positive manner in which he lived his life.
Until next time, I wish you all a safe, healthy and happy summer.
Treat others as they would like to be treated• be just when seeking justice• fight “fire” with “fire prevention”• Understand two rights often make a wrong•
If you have nothing nice to say, find a nice way of saying it• be yourself, but be your best self• If you can’t beat them, learn from them•

ACCESS VOL XXX NO 2 APRIL 2009
2
T hose of us who work in the health care system know that our system is prone to error, and
adverse events, preventable or otherwise, occur. In 2004 the landmark Canadian Adverse Events Study estimated that 7.5% of patients admitted to acute care hospitals in Canada experience one or more adverse events (baker and Norton et al., 2004). Large scale studies have shown that errors result in system inefficiencies, increased costs and most importantly, can lead to avoidable patient complications and even deaths. It was during this time, as safety concerns were being brought out from behind closed doors, that the problems with estrogen and progesterone receptor (ER/PR) testing performed at Eastern Health came to light.
On march 1, 2009 The Honourable margaret Cameron, Commissioner, released her Report of the Commission of Inquiry on Hormone Receptor Testing. The ‘Cameron Inquiry’, established in 2007, attempted to provide an understanding of what went wrong with the ER/PR testing from 1997 to 2005 and how to avoid such errors in the future. I will not attempt an in-depth analysis of the Commissioner’s comprehensive 495 page report and 60 recommendations in this column. However, suffice it to say that the Commissioner’s harsh indictment, “The whole of the health system, to varying degrees can be said to have failed the ER/PR patients. There is a failure of both accountability and oversight at all levels,” is the main message for those of us who work in the health care system. Accepting the ‘whole’ of the system failed the ER/PR patients, my initial read of the report was through ARNNL’s lens- from the perspective of a regulatory body/professional association.
what struck me as I studied the recommendations was the importance of the work of regulatory bodies/professional associations, such as ARNNL, in supporting quality initiatives and improving safety in our health care system. Justice Cameron recognized the role regulation, accreditation and licensure plays in raising standards of practice when she recommended that laboratories be licensed and accredited and that laboratory technologists be regulated and registered. She also recognized the importance of high standards of basic education, mandatory continuing education and annual competency assessment in ensuring highly skilled professionals as she made a number of recommendations for laboratory technologists and physicians in this regard. Justice Cameron supported the need for evidence informed decision making and quality assurance systems that reflect ‘best practices’ in laboratory practice and the process for disclosure of adverse
events. Regulators/associations drive many best practices and are a source for current information to guide safe, competent and ethical practice. The Commissioner also addressed the importance of system supports to improve quality controls and adverse event disclosure, such as, the need for province-wide information management systems including an electronic health record, apology legislation and sufficient funding to implement her recommendations. Regulators/associations have an important role to advocate for supportive policy and legislation and to support system implementation of these broad patient safety initiatives. finally, regulators have an important role in assisting members to understand their specific obligations and accountabilities related to patient safety.
So what are my initial impressions of the report on the Cameron Inquiry?
first, regulatory bodies/professional associations are essential partners in efforts to improve patient safety. Our role in setting
standards for education and practice and promoting the continued competence of members helps to ensure the quality of our practitioners and therefore, the safety and quality of patient care. Professional standards must be upheld.
Secondly, The Cameron Inquiry aired the issue of safety in the public: The ‘adverse event door’ is wide open. Our profession, and the health system, needs to understand the inevitable increased public scrutiny of health care and to find better ways to involve the public in creating the ‘culture of safety’
the system is striving to achieve. Public scrutiny will help us improve patient safety.
finally, the report reinforced the need for system-wide accountability for patient safety. while the Commissioner directs many recommendations to Eastern Health in order “to avoid such errors in the future,” action is required at all levels and with all stakeholders - practitioners, regulators, unions, health care authorities, government and the public. All of us have a role in improving the safety of OUR health care system.
Everyone feels the impact when our health care system fails and patients’ health and lives are affected. The Commission of Inquiry on Hormone Receptor Testing helps to better understand the changes needed to improve the safety and quality of health care in our province. Thank you to all the courageous people who participated in the Inquiry; especially, to the patients and relatives who gave evidence. I have every confidence that your participation will improve OUR health care system.
Imp oving Patient SafetyMARGAREt (PEGi) EARLE, RN, MScNExECutivE DiRECtOR
CAmERon inquiRy
OuR ROLE iN SEttiNG StANDARDS FOR
EDuCAtiON AND PRACtiCE AND PROMOtiNG thE
CONtiNuED COMPEtENCE OF MEMBERS hELPS tO
ENSuRE thE quALity OF OuR PRACtitiONERS AND
thEREFORE, thE SAFEty AND quALity OF PAtiENt CARE.

3
Imp oving Patient Safety By ChRiStiNE CRAWLEy, BSCN, RN
Nurses have always had an ethical and professional obligation to ensure that clients are appropriately cared for as outlined in the Code of Ethics for Registered Nurses (CNA, 2008) and Standards for Nursing Practice (2007). These obligations apply to all domains (practice, research, education, administration, and policy) and in all settings. The Registered Nurses Act (2008) goes beyond these ethical and professional obligations by establishing a legal duty for nurses to report situations where they have “knowledge through direct observation or possess objective evidence of conduct deserving of a sanction of another registered nurse” (Section 20). All registered nurses are now legally obligated to report conduct deserving of a sanction of another registered nurse. This new provision in the legislation reflects the primary responsibility of RNs and the ARNNL to ensure public protection. Reporting must be seen as a positive means of ensuring excellence in nursing practice.
Section 20 also stipulates that employers have a legal obligation to report to the ARNNL the termination or restrictions on the employment of a registered nurse for reasons related to direct knowledge of the registered nurse’s conduct deserving of sanction. A report from an employer, the public, or an RN gives the regulatory body the authority to initiate the process to intervene to address the nurses’ practice or conduct that is in question. without cooperation and input from everyone the problem cannot be addressed appropriately, and members of the public could be at risk. If you don’t know if the registered nurse’s conduct is deserving of sanction, the best thing to do is ask the ARNNL.
This new provision is not without challenges. most health care providers function as part of a tight-knit community, and thus confronting incidences of conduct deserving of a sanction
by a colleague presents a difficult situation. Referred to in the literature as a “conspiracy of silence”, nurses who encounter inappropriate behaviour by other nurses are oftentimes at a loss of how to respond (Lowell & massey, 1997). Research suggests that the most common ways nurses respond to problems with other nurses are: doing nothing, trying to help their colleague privately, or requesting intervention from a manager or alternate authority (Lucken-brett & Stuler-Schlag, 1987; Orbe & king, 2000). while the intentions of the nurse are usually good, the results may not be and the problems may continue. A cited advantage of duty to report requirements are that they
clarify who is responsible for what and thus help alleviate some of the ethical distress such an action can evoke (Lucken-brett & Stuler-Schlag, 1987).
The duty to Report requirements are extremely important to nursing practice. Section 20 provides nurses with an avenue to voice their concerns in a professional manner. The literature tells us that organizations which provide clear and proper channels for disclosure encourage health care workers to use those channels (Lucken-brett & Stuler-
Schlag, 1987; Orbe & king, 2000). Client advocacy is a hallmark of the nursing profession. The
duty to report provision strengthens RNs’ ability to be true advocates; to speak out for what is in the best interest of those we serve (Hamric, 2000). Therefore, it is important for every registered nurse to be familiar with the RN Act. Over the next few months the ARNNL will be initiating discussion about the RN Act and the duty to report. we invite all interested nurses to actively participate in these upcoming events.
References available upon request
How would you respond if a colleague were to ask, “What does a nurse do when another nurse’s practice does not meet professional standards?” If you are not sure how to answer this question then read on to learn what you need to know about changes to the Registered Nurses Act, 2008 (RN Act) and the duty to report.
thE Duty tO REPORt REquiREMENtS ARE
ExtREMELy iMPORtANt tO NuRSiNG PRACtiCE. SECtiON 20 PROviDES
NuRSES With AN AvENuE tO vOiCE
thEiR CONCERNS iN A PROFESSiONAL MANNER.
Editor’s note: Christine is a Master of Nursing Student at Memorial university who is assisting the ARNNL Director of Regulatory Services to develop policy and educational material for the duty to report provision in the new RN Act. Special acknowledgement to Alice Gaudine.
ACCESS VOL XXX NO 2 APRIL 2009
4
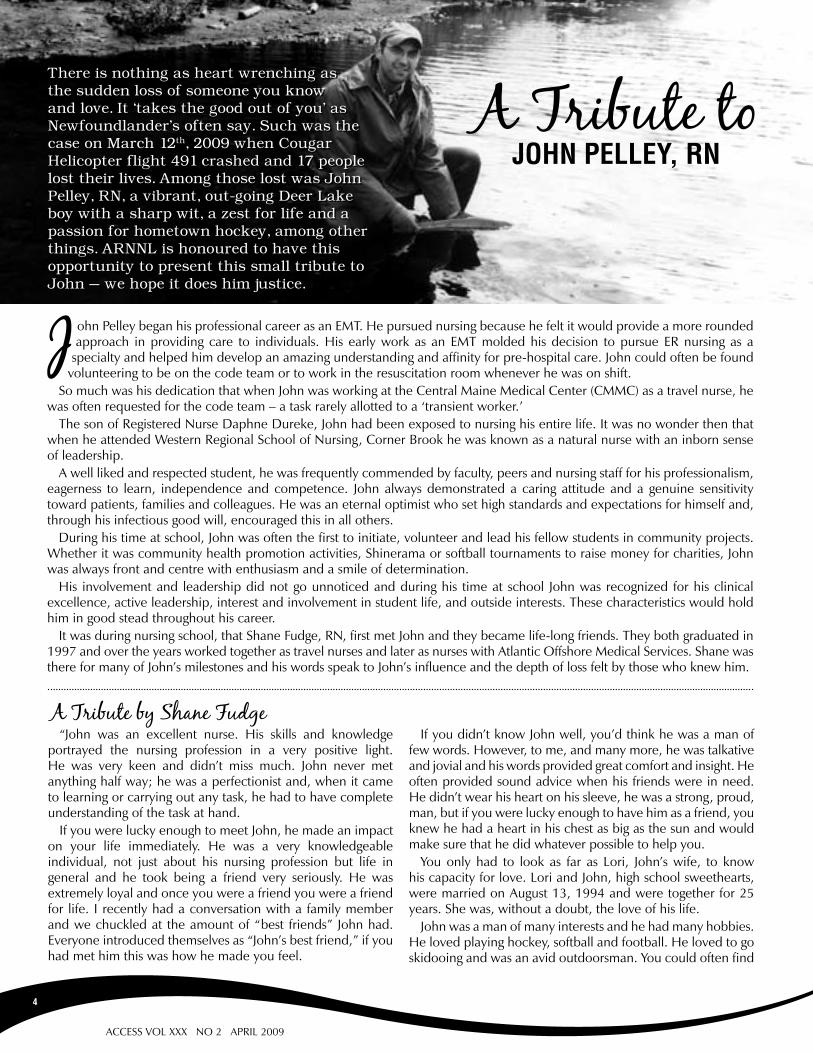
ohn Pelley began his professional career as an EmT. He pursued nursing because he felt it would provide a more rounded approach in providing care to individuals. His early work as an EmT molded his decision to pursue ER nursing as a
specialty and helped him develop an amazing understanding and affinity for pre-hospital care. John could often be found volunteering to be on the code team or to work in the resuscitation room whenever he was on shift.
So much was his dedication that when John was working at the Central maine medical Center (CmmC) as a travel nurse, he was often requested for the code team – a task rarely allotted to a ‘transient worker.’
The son of Registered Nurse daphne dureke, John had been exposed to nursing his entire life. It was no wonder then that when he attended western Regional School of Nursing, Corner brook he was known as a natural nurse with an inborn sense of leadership.
A well liked and respected student, he was frequently commended by faculty, peers and nursing staff for his professionalism, eagerness to learn, independence and competence. John always demonstrated a caring attitude and a genuine sensitivity toward patients, families and colleagues. He was an eternal optimist who set high standards and expectations for himself and, through his infectious good will, encouraged this in all others.
during his time at school, John was often the first to initiate, volunteer and lead his fellow students in community projects. whether it was community health promotion activities, Shinerama or softball tournaments to raise money for charities, John was always front and centre with enthusiasm and a smile of determination.
His involvement and leadership did not go unnoticed and during his time at school John was recognized for his clinical excellence, active leadership, interest and involvement in student life, and outside interests. These characteristics would hold him in good stead throughout his career.
It was during nursing school, that Shane fudge, RN, first met John and they became life-long friends. They both graduated in 1997 and over the years worked together as travel nurses and later as nurses with Atlantic Offshore medical Services. Shane was there for many of John’s milestones and his words speak to John’s influence and the depth of loss felt by those who knew him.
“John was an excellent nurse. His skills and knowledge portrayed the nursing profession in a very positive light. He was very keen and didn’t miss much. John never met anything half way; he was a perfectionist and, when it came to learning or carrying out any task, he had to have complete understanding of the task at hand.
If you were lucky enough to meet John, he made an impact on your life immediately. He was a very knowledgeable individual, not just about his nursing profession but life in general and he took being a friend very seriously. He was extremely loyal and once you were a friend you were a friend for life. I recently had a conversation with a family member and we chuckled at the amount of “best friends” John had. Everyone introduced themselves as “John’s best friend,” if you had met him this was how he made you feel.
If you didn’t know John well, you’d think he was a man of few words. However, to me, and many more, he was talkative and jovial and his words provided great comfort and insight. He often provided sound advice when his friends were in need. He didn’t wear his heart on his sleeve, he was a strong, proud, man, but if you were lucky enough to have him as a friend, you knew he had a heart in his chest as big as the sun and would make sure that he did whatever possible to help you.
you only had to look as far as Lori, John’s wife, to know his capacity for love. Lori and John, high school sweethearts, were married on August 13, 1994 and were together for 25 years. She was, without a doubt, the love of his life.
John was a man of many interests and he had many hobbies. He loved playing hockey, softball and football. He loved to go skidooing and was an avid outdoorsman. you could often find
John PEllEy, RnA Tribute to
There is nothing as heart wrenching as the sudden loss of someone you know and love. It ‘takes the good out of you’ as Newfoundlander’s often say. Such was the case on March 12th, 2009 when Cougar Helicopter flight 491 crashed and 17 people lost their lives. Among those lost was John Pelley, RN, a vibrant, out-going Deer Lake boy with a sharp wit, a zest for life and a passion for hometown hockey, among other things. ARNNL is honoured to have this opportunity to present this small tribute to John – we hope it does him justice.
There is nothing as heart wrenching as the sudden loss of someone you know and love. It ‘takes the good out of you’ as Newfoundlander’s often say. Such was the case on March 12th, 2009 when Cougar Helicopter flight 491 crashed and 17 people lost their lives. Among those lost was John Pelley, RN, a vibrant, out-going Deer Lake boy with a sharp wit, a zest for life and a passion for hometown hockey, among other things. ARNNL is honoured to have this opportunity to present this small tribute to John – we hope it does him justice.
A Tribute by Shane Fudge
5
Privacy is Everyone’s Responsibility. For more information on the Personal Health Information Act contact Legislative & Regulatory Affairs, Department of Health and Community Services at 729-7007. the Act is available on the Government of Newfoundland & Labrador website at: www.assembly.nl.ca/legislation/sr/statutes/p07-01.htm
ARNNL iS PLEASED tO PRESENt thE FiRSt iN A SERiES OF ARtiCLES OutLiNiNG thE NEW PERSONAL hEALth iNFORMAtiON ACt AND itS iMPACt ON CuStODiANS iN thE PROviNCE
PERSonAl hEAlTh inFoRmATion ACT: quESTionS & AnSwERS FoR CuSToDiAnSthis overview is presented for the convenience of reference only. Nothing in this overview should be construed as legal advice. you should consult the Act and your own solicitors for all purposes of interpretation.
A PRivACy CuLtuRE iNvOLvES “AWARENESS AND SENSitivity By EACh PERSON WithiN AN ORGANizAtiON WhEN PROCESSiNG PERSONAL iNFORMAtiON iN thEiR DAy-tO-DAy-ACtivitiES” (POWER, 2008). EACh EMPLOyEE ACCEPtS RESPONSiBiLity FOR PROtECtiNG thE PERSONAL iNFORMAtiON iN thE ORGANizAtiON’S CuStODy.
Personal HealtH InformatIon act: BuIldIng a culture of PrIvacy
him hunting, fly fishing, or any number of other activities. He was a member of various men’s sporting teams and he was an avid deer Lake Red wings fan and I’d even venture to say that if he was off shift he didn’t miss a game.
He was also an amazing musician with a great voice and an uncanny knack for the guitar and the mandolin.
He was an individual who seemed to get the most out of everything he was involved in. If he was fly fishing, you would have to literally beg him to leave the river and there were many nights I sat my truck after dark waiting for him to call it a day. It didn’t matter, if he was playing guitar or tying flies, he was the same - dedicated and devoted to the task at hand.
John was first and foremost a Newfoundlander. He never saw permanently leaving the province as an option. Even when we worked almost 2 years in the US, he saw working away only as a stepping stone to a better career and life back in Newfoundland. I don’t recall ever hearing him say that he would like to move from Newfoundland. Newfoundland provided him with the opportunity to do everything he wanted.
John and I were friends for 15 years, and during that time there wasn’t much we didn’t talk about or do. John was a great confidant and always had his own theories on most things, which usually ended in a chuckle. I will miss our conversations and his guidance. John was a great nurse and a better friend – he will be missed by all who knew and loved him.”
What is the Personal Health Information act?
the Personal health information Act is a provincial law that governs the collection, use and disclosure of personal health information. it also gives individuals the right to access and request correction of their own health information.
Why is the Personal Health Information act needed?
the Personal health information Act applies to all personal health information held by custodians regardless of the format of the information, or whether it is held in the public or private system. Without this Act, personal health information in this province would be subject to different legislation depending on the setting. the federal Personal information Protection and Electronic Documents Act (PiPEDA) currently regulates private practitioners while public bodies, such as regional health authorities, are subject to the provincial legislation, Access to information and Protection of Privacy Act (AtiPPA).
When will the act become law?
the Personal health information Act is expected to be proclaimed in early 2010. Prior to proclamation, resources will be developed and shared with custodians. Work is currently underway for the development of these resources.
Who does the act affect? the Personal health information Act affects everyone including custodians who have custody or control of personal health information, their employees, agents, volunteers, and individuals with practice privileges within the organization, as well as the general public.
Who are custodians?
Custodians are defined in the Personal health information Act as a person having custody or control of personal health information. included in this list of custodians are the following:• Regionalhealthauthorities(RHA);• Aboard,council,committee,commission,corporationor
agencythatisestablishedbytheRHA;• AdepartmentcreatedbytheExecutiveCouncilAct;• TheMinisterresponsiblefortheAct;• Ahealthcareprofessional;• Ahealthcareprovider;• A person who operates a health care facility, pharmacy,
ambulance service or a centre, program or service for communityormentalhealth;
• TheProvincialPublicHealthLaboratory;• TheCentreforHealthInformation• Memorial University’s Faculty of Medicine, School of
Nursing, School of Pharmacy and School of human KineticsandRecreation;
• TheCentreforNursingStudies;• WesternRegionalSchoolofNursing;• A person who under law obtains custody or control of
healthrecordsasaresultofbankruptcyorinsolvency;• ArightsadvisorundertheMentalHealthCareandTreatment
Act;• The Workplace Health, Safety and Compensation
Commission;and• Apersondesignatedasacustodianintheregulations.

ACCESS VOL XXX NO 2 APRIL 2009
6
Since 1995, the federal and provincial governments have
been working to improve labour mobility in Canada. On January 16, 2009, Prime minister Stephen Harper and Canada’s Premiers signed a new Agreement on Internal Trade (AIT) that allows, within the labour mobility chapter (Chapter 7), regulated professionals who are licensed in one province or territory to have access to employment opportunities elsewhere in Canada without having to complete additional training, experience, examinations or assessments as part of the registration procedure. This includes health professionals such as registered nurses and nurse practitioners. The new AIT came into effect on April 1st 2009 and the Association of Registered Nurses of Newfoundland and Labrador (ARNNL), as the regulatory body for registered nurses and nurse practitioners, is required to comply with this agreement.
what is labour mobility and how does it affect the nursing profession?
Labour mobility allows workers, registered in one province, the freedom to practice their profession throughout Canada, wherever job opportunities exist and without having to complete additional training, experience, examinations or assessments. Encouraging the recognition of qualifications across Canada benefits workers and employers alike and allows for a greater resource pool of skilled workers (Human Resources and Skills development Canada, 2007). workers have a wider range of opportunities and employers have a broader selection of candidates. Allowing nurses, nurse practitioners and other professionals to move freely within the country may help recruitment and movement of nurses into positions where they are most needed.
All nursing regulators, including the ARNNL, have expressed concerns with respect to the full impact and outcomes of the AIT. The AIT is relevant to the mandate of regulatory bodies that develop the requirements for entry to the profession, standards of education and determining the scope of practice for nursing. while Canadian regulatory bodies have the responsibility of protecting the public and ensuring that
registered nurses and nurse practitioners are competent, they are concerned that the AIT can overrule these responsibilities and thereby compromise public safety.
Under AIT, ARNNL will be required to license registered nurses and nurse practitioners who hold a license in another province or territory, unless there are demonstrated differences in standards or scope of practice. In circumstances where a regulator, such as ARNNL, identifies a difference in standards or scope of practice, the regulator has the option to submit a “legitimate objective” to their provincial government. A “legitimate objective” must demonstrate that compliance with AIT endangers public safety or endangers social and health programs. The government determines if the legitimate objective is accepted or not and thereby becomes the final adjudicator of regulatory standards and not the ARNNL.
A regulator can refuse or restrict a license under specific circumstances. A nurse who has a disciplinary action or criminal proceedings against him/her in another province related to competency, conduct or character of the worker and where such action may endanger public safety, can be refused licensure by the regulator. In situations where a nurse or nurse practitioner has not practiced for an extended period of time, the regulatory body can refuse licensure.
In Canada, there is a mutual Recognition Agreement (mRA) for registration and licensure of registered nurses among all provinces and territories. There are no barriers for registered nurses applying for licensure and registration from other jurisdictions. However, there are some differences in legislation, regulations and scope of practice for nurse practitioners
LABOUR MOBILITY
What does it mean for registered nurses and nurse
practitioners in Newfoundland & Labrador?
By BEvERLEy MciSAAC, RN, NP, MN (ANP)

7
the province lost a legendary health care leader March 31 with the passing of Sister Mary (hennebury) Fabian.
Fabian’s leadership in health care encompassed not only the care of patients and their families, but also the concern for staff members and their families. She had an outstanding career in nursing and hospital administration at St. Clare’s Mercy hospital. She was primarily responsible for the expansion of the hospital facilities, the founding of a detoxification centre and the establishment of a palliative care unit. For her work, and the impact she had on the community, she was named St. John’s Citizen of the year in 1982.
Born in Bonavista, Fabian entered the congregation of the Sisters of Mercy in 1935 and graduated from St. Clare’s School of Nursing in 1942, the first Sister of Mercy to receive a nursing degree from a Newfoundland nursing school.
While she officially retired almost three decades ago, in 1981, Fabian remained an active volunteer on boards and accreditation teams until late into her eighties. She was an honorary member of the ARNNL and was also honorary Patron of the ARNNL trust. in her later years she lived at McAuley Convent in St. John’s where she continued to minister to sick and elderly Sisters of Mercy.
The Passing of a Health Care Leader
Sister mary fabian
across Canada. for example, Quebec and british Columbia require nurse practitioners to complete both a written and a clinical examination prior to registration. Regulators from all jurisdictions are working to achieve common standards and scope of practice competencies for nurse practitioners.
The AIT does not mean nurses can move to a province or territory and start working without first registering with the nursing regulatory body. while the AIT may facilitate nurses who are registered in another province or territory to register in Newfoundland & Labrador, they are required to provide verification of their current registration from the other jurisdiction, proof of legal identity and satisfactory references.
The ARNNL supports labour mobility for Registered Nurses (RNs) and Nurse Practitioners (NPs) and is working with other jurisdictions and government to enable labour mobility and ensure compliance with the agreement, without compromising nursing standards.
References available upon request

ACCESS VOL XXX NO 2 APRIL 2009
8
continuing competence program:a Plan for safe, comPetent nursIng PractIce and lIfe-long learnIng
what we do know is that the CC Program toolkit will include: Reflection: you will look back at the previous year to
identify what continuing education sessions you participated in (formal and Self –directed)
A Self Assessment guide• A Learning Plan• Evaluation of the Learning Plan• An Online Tutorial to assist with completing • the CC Tools
continuing competence program: faQs
Does this replace the requirement for hours of practice? No, you will still be required to practice 1,125 hours of
registered nursing practice in the past five (5) years or have completed an approved education program in addition to the CC Program requirements.
what documents do i have to submit with my registration renewal?
None. you will only need to provide your documentation if requested by ARNNL. beginning in 2012, ARNNL will randomly select members each year to take part in an auditing process. you are required to keep your documentation for three (3) years.
i have not practiced this year, but am planning to go back to work soon. how can i complete the Program?
you will need to reflect on both your last nursing experience and your needs in relation to the area you will be working in. what orientation will your employer provide? what else will you need to know to feel comfortable working in that area? do you need to enhance on your knowledge of the care of patients with specific diseases? what about the procedures, skills, and equipment you will need to be proficient in? All of these needs can be incorporated into your self-assessment and learning plan so that as you return to work, you can be prepared and the transition will go smoothly.
Wanted:continuing competency champions
Continuing Competency Champions are nurses who are passionate about lifelong learning, improving nursing practice and patient care.
Champions influence colleagues, groups and committees.
if you would like to join ARnnl’s Continuing Competency Champions, send me an email.
Bev mcisaac, nursing Consultant [email protected]
ARNNL is currently in the early stages of developing the tools required for implementation of the Continuing Competence (CC) Program. The CC framework was approved by ARNNL Council in february 2009. Two members of the CC Advisory Committee co-hosted the first teleconference session to review the CC Program framework. The session was well attended with 77 RNs and NPs present. ARNNL will be scheduling further teleconference sessions to review the CC framework and introduce the CC Tools.
A series of province-wide education sessions are planned for fall 2009. The schedule will be posted on the ARNNL website in the coming months.
nuRSE PRACTiTionER REgulATionS uPDATE
ARNNL wishes to inform members that new NP Regulations (2009) will be coming into effect shortly.
ARNNL Council approved a new Regulatory Framework for Nurse Practitioner Practice in Newfoundland and Labrador, April 2008, which required amendments to the 1998 NP Regulations before implementation. The Nurse Practitioner Regulations (2009) have been drafted by Legislative Council, government of Newfoundland and Labrador and were brought to ARNNL Council on April 14th and will now be brought to the NP Standards Committee for approval as required by the RN Act (2008).
following this, the regulations will go to the minister of Health & Community Services (mOH) for final approval and signature.
The NP Regulations (2009), once approved, will allow for implementation of the Regulatory Framework for Nurse Practitioner Practice in Newfoundland and Labrador. The new NP Regulations (2009) will significantly expand the Scope of Practice for NPs in the province and will take effect immediately upon signing by the mOH. After signing, NPs will no longer be able to use the 1998 regulations as guidelines.
further information and updates will be ongoing - keep checking ARNNL’s website for updates or contact beverley mcIsaac at [email protected] or 753-6174.

9
The Association of occupational health nurses of newfoundland and labrador
The Association of Occupational Health Nurses of Newfoundland and Labrador (AOHNNL) began with 11 eager members in the early 1980’s. On march 31, 1982, the ARNNL adopted the bylaws and Constitution of the AOHNNL, granting it special interest group status. Since the early 1980’s, provincial educational conferences have been an annual event for the AOHNNL and continue to this day. membership grew to 15-20 members in the early 1990’s and today there are 30 registered members.
“The membership numbers have only grown, and we have been able to remain an active special interest group for over 27 years,” said AOHNNL President denise maher, RN, dOHN, manager of multidisciplinary/medical Services with fIT for work. when asked how the group has been sustained over so many years, denise replied that they have “developed a strong network of committed professionals who are interested in developing their knowledge and in providing the most current, evidence-based practice.”
Occupational Health Nurses practice in the specialty of occupational health and safety delivering integrated services to individuals and worker populations. “Occupational Health Nursing encompasses the promotion, maintenance and restoration of health and the prevention of illness and injury” (Canadian Occupational Health Nursing Association, 2009). According to Cathy bradbury, RN, bN, COHN (C), Association Treasurer, “the Association of Occupational Health Nurses of Newfoundland and Labrador believes in promoting and maintaining the physical, social and psychological well-being of all individuals in their work environment.” Cathy has been a long time member of the Occupational Health Nurses special interest group and currently works as an Occupational Health Nurse in the Safety and Health department with Nalcor Energy – NL Hydro.
members of the AOHNNL are also members of the Canadian Occupational Health Nurses Association, a national group of Occupational Health Nurses. National membership has
provided opportunities for networking with colleagues and making sure that standards that are applied in this province are consistent with national standards.
when asked how things have changed over the years for occupational health nursing, Cathy said that valuing and understanding the role of the occupational health nurse has probably been the biggest change.
“more and more occupational health nurses are being introduced in industry and businesses as people see the asset that occupational health nurses can provide in the workplace – from disability management to wellness promotion, to attendance management and workplace health and safety monitoring. Occupational Health Nurses function as independent practitioners, providers of care, consultants, teachers and researchers,” said Cathy, adding that “the role improves health and safety of workers thus contributes to the health of the community.”
The AOHNNL special interest group meets every 6 weeks or so, with many members attending via teleconference. They discuss current issues and concerns and share forms or processes that have been developed. denise stated that this opportunity to know how others are carrying out their work allows people to benefit from the knowledge and skills of their counterparts. members are more aware of available resources now and a strong evidence base for practice has been established. Every meeting is not all business, though, denise pointed out. “we host social events throughout the year and we have retired members who meet for lunch regularly – a sign that lifelong friendships have been formed.”
The CNA offers a certification in Occupational Health Nursing, identified by the initials COHN (C). details about obtaining this certification are available on the CNA website www.cna-aiic.ca. Information about Occupational Health Nursing is available on the Canadian Association of Occupational Health Nurses website at www.cohna-aciist.ca. Locally the AOHNLL annual spring conference is scheduled for June 5, 2009 in St. John’s. for more information, contact Provincial President of AOHNLL, denise maher via e-mail at [email protected] or by phone at 722-7676 ext 316.
Special Interest groups (SIgs) bring together registered nurses who share a common concern for professional development in a defined area of nursing practice, education, administration or research. They serve to promote the profession, enhance quality of care and standards of practice, as well as develop knowledge and competency through sharing with peers.
Special Interest groups provide their expertise to the ARNNL and provide input into decision-making on relevant issues.There are currently 18 ARNNL SIgs. details around developing a special interest group, as well as a list of current special
interest groups are outlined on our webpage www.arnnl.ca. To highlight the work of these groups, we have chosen the Association of Occupational Health Nurses of Newfoundland and Labrador (AOHNNL) as this edition’s Nurse(s) of Note.
If you would like to nominate an RN you know for our Nurse of Note, please contact Janice Lockyer via e-mail at [email protected]
Nurses of Note

ACCESS VOL XXX NO 2 APRIL 2009
10
ARnnl AnD SRnA iSSuE A nATionAl nuRSing wEEk ChAllEngE greening health Care“REDuCE thE AMOuNt OF GARBAGE WE GENERAtE”…”RECyCLE BEvERAGE CONtAiNERS”… “ChANGE yOuR LiGht BuLBS tO ENERGy EFFiCiENt ONES”...
we’ve all heard the promotions. It seems so manageable and practical at home. but how can we make these environmental changes in our workplaces? So many things are out of our control. Or are they? “greening health care” has never been more important or more possible. but what is a registered nurses role in this? “Nurses are influential contributors to building design, institutional procedures and purchasing decisions” (Canadian Nurses Association (CNA), 2008, p.13). Nurses are key team members, working within health facilities with an opportunity to reduce a buildings environmental footprint (CNA, 2008). Environmental health issues go beyond institutions to the community, schools and industry. Nurses in all roles have a part to play. If we are going to have a sustainable future, health care needs to be a part of it.
but where do we start? we can start with committing one act of green in the workplace. Throughout National Nursing week, may 11 – 17th, 2009, Registered Nurses in Newfoundland and Labrador will be called upon to commit one act of green every day. Each day brings a new challenge and a meaningful way to make a difference. we have been asked to partner with our colleagues in Saskatchewan who will be carrying out the same acts of green during nursing week. with the 6000 RN’s in NL and the 10,000 RN’s in Saskatchewan every small act has a big impact.
ARNNL workplace reps in Newfoundland and Labrador and SRNA workplace reps in Saskatchewan will distribute posters throughout both provinces outlining an activity for each day. monday will see registered nurses sharing a ride to work to reduce green house gases. Tuesday finds registered nurses asking about the equipment in their areas and determining if any mercury containing products remain. wednesday cautions registered nurses to only place appropriate items in the sharps containers. biomedical waste is incinerated and inappropriate items can add to toxic emissions. fuel usage also increases when heavy sharps containers are shipped
away for incineration. Agency policies should address these issues. Thursday encourages discussions about environmentally friendly practices and brings about a sharing of knowledge. friday involves reducing waste by bringing lunch in reusable containers. Saturday calls for a reduction in the amount of paper we print by only printing what is required. Sunday challenges registered nurses to reduce power usage by turning off unnecessary lights and taking the stairs where appropriate.
Throughout the week, let each other know how many acts of green you have committed. Together with our colleagues in Saskatchewan, we can show ourselves and others how registered nurses in two different provinces are able to affect change.
References available upon request
11
N urses work in a variety of practice areas and all of us have a role to play in promoting health of the
communities in which individuals live, work, worship and play (Health Canada, 1999). Thinking about health in an “outside the box” approach requires that nurses view health from a multi-faceted perspective. It’s not enough to simply provide care for clients while they are ill, what can we as nurses do for the community and the bigger picture at large?
Reflecting on your own practice, how can you as a nurse make an impact on “Jason’s” health? who is “Jason” in your area of expertise? How can you ensure that when administering chemotherapy, you consider all the factors that may be impacting on your client’s health in a positive or negative manner? does your client have an issue with transportation? Is family support available when he returns home?
How often have we termed clients as non-compliant when really they have no control over what we ask them to do. A client instructed to follow a diabetic diet may have no funds to buy the healthier foods. maybe she lives in a rural area with no access to fruits and vegetables. maybe she is dependant on a neighbour for travel to the outpatient diabetes clinic appointment.
working from an “upstream” approach requires that no matter what nursing practice area we work in, consideration is given to the root cause of illness (Health Canada, 2001). why is it that our province’s population has such a high rate of increased blood pressure and early death from cardiovascular disease? How does the closure of the local paper mill affect health and well-being? why should I be concerned with mr. X’s income, he is only here for inpatient treatment of a diabetic ulcer? These questions, and the forthcoming answers, all contribute to the mosaic of individual, community, and provincial health, as a whole. Overall, the information obtained from an assessment of the determinants of health encourage [nurses] to initiate
population led activities that promote health and prevent risk of disease before individuals present with mild to moderate symptoms (Horsburgh, Smith & yallop, 2007).
DETERMINANTS OF HEALTHdeterminants of health are known as
the key factors that influence health. These influences can be considered a benefit to health, or can have a detrimental effect on health and the social environment (wilkinson & marmot, 2003). These factors include:
Education Level• Income • Social Support• genetics• Culture• Personal Health Practices • and Coping SkillsHealth Services • gender• Physical Environment• working Conditions and • EmploymentHealthy Child development•
Nurses have a responsibility to be cognizant of the determinants when providing holistic care to clients. Nurses must ask themselves how these factors can influence client health, and how personal nursing practices may need to change in public health, obstetrics, discharge planning, coronary care, etc…in order to impact the greater good for the client. Acknowledging the determinants not only allows for effective team work, it also supports the capacity of clients to participate in their own care (Horsburgh, Smith, & yallop. 2007). Taking this lens allows the opportunity for clients to tell us their concerns, their barriers to achieving health, and what they might envision as potential solutions.
Providing a holistic approach to care, which includes an assessment of the determinants of health, can facilitate improved health outcomes for all “Jasons” and in turn, create a healthier population for Newfoundland and Labrador!
nATio
nAl n
uR
Sing
wEEk 2009
“WHy IS JASON IN THE HOSpITAL?Because he had an infection in his leg.
BuT WHy DOES HE HAvE AN INFEcTION?Because he had a bad cut on his leg.
BuT WHy DOES HE HAvE A BAD cuT ON HIS LEg?Because he was playing in the junk yard next to his apartment building and he fell on a sharp piece of steel. BuT WHy WAS HE pLAyINg IN THE JuNk yARD?Because his neighbourhood is run down. A lot of kids play in the junk yard, with no one to keep an eye on them.
BuT WHy DOES HE LIvE IN THAT NEIgHBOuRHOOD?Because his parents can’t afford to live in a nicer place. BuT WHy cAN’T HIS pARENTS AFFORD A NIcER pLAcE?Because his Dad has no job and his Mom is sick. BuT WHy IS HIS DAD OuT OF WORk?Because he doesn’t have much education and he can’t find a job.
BuT WHy…?”
(Health canada, 1999).
By JOANNE PELLEy, BN, RN, MN PROGRAMhEALth PROMOtiON AND WELLNESS MANAGER, CENtRAL hEALth

ACCESS VOL XXX NO 2 APRIL 2009
12
for over 30 years, the work of the Canadian Nurses Association (CNA) with nursing associations
from developing countries has been based on the premise that strong and vibrant professional associations can play an important leadership role in the health sector. CNA believes that nurses can be leaders and partners working to advance health for all. Through the International Health Partnerships Program, CNA’s department for International Policy and development has sought to enhance collaboration between nurses from Canada and developing countries. These international partnerships both increase Canadian nurses’ understanding of global health issues, and build the capacity of nursing organizations in developing countries to be leaders in improving their own health systems and health outcomes.
The Association of Registered Nurses of Newfoundland and Labrador (ARNNL) has participated in this process through CNA’s Strengthening Nurses, Nursing Networks and Associations Program (SNNNAP), which is supported with funding from the Canadian International development Agency (CIdA). Since 2002, CNA has been working through SNNNAP with national nursing associations in burkina faso, El Salvador, Ethiopia, Indonesia, Nicaragua, Senegal, Vietnam and SANNAm, a regional nursing network in southern Africa. The program focuses on developing the capacity of its partners to contribute to health policy and health system strengthening, improve nursing practice and care through regulation of the profession, and build the leadership capacity of nurses, increasing public recognition of the contribution nursing makes to the health system and population health.
The Vietnam Nurses Association (VNA) was founded in 1990. with a membership of 48,000 in 59 out of 64 provinces, they now represent about 90 per cent of the professional nurses in the country. with CNA support since 1999 they have built their profile and capacity to be one of the most representative and respected health professional associations in the country. VNA successfully facilitates nursing leadership in health system policy development and is routinely consulted by government and included in policy consultations. The association has also established a leadership role in promoting primary health care and care for people living with HIV/AIdS.
SNNNAP provides technical assistance and targeted skills-building to support international partners’ work, including making global linkages and sharing expertise. Canadian nurses play a key role in the delivery of technical assistance through mentoring, providing ongoing advice and assistance to international partners on issues of regulation, policy advocacy, leadership and organizational governance. ARNNL has been mentoring VNA since 2003. during this time, ARNNL staff has worked with VNA in Vietnam and in Canada on regulatory issues such as developing a scope of practice and membership registration.
ARNNL’s board and members recognize the importance of this work. Over the years ARNNL leadership, staff and members have contributed to building the partnership with VNA and supporting their development into one of the country’s foremost health professional associations. Lan gien and Consie Howley provided important professional support to VNA as they developed a program to strengthen the contribution of nurses to caring for people living with HIV/AIdS.
Lynn Power of ARNNL has visited Vietnam four times under the SNNNAP program. Over this time Lynn has witnessed VNA grow in both strength and numbers. “They have developed a reputation amongst the nurses in Vietnam from the ground up. for example, they have developed and offered numerous educational events on topics ranging from therapeutic communications to research. They created newsletters, journals and a web site. They have designed and implemented community programs and written policy papers such as the national scope of practice which successfully advanced the quality of nurse’s lives and client services in Vietnam. Their dedication and commitment is truly remarkable.”
Vietnamese nurses still face many challenges, in particular in the area of nursing education – there are very few programs offered at the bachelor and masters levels, and most nursing instructors are medical doctors. VNA must now work to consolidate their gains from the past by further addressing nursing education, building their membership, and strengthening the visibility and public image of nurses and nursing.
ARnnl mEnToRS ThE viETnAm nuRSES ASSoCiATion, PART oF CnA’S inTERnATionAl hEAlTh PRogRAm
viETnAm – FAST FACTS: hEAlThtotal population: 86 millionLife expectancy at birth m/f (years): 69 / 75As of 2002, there were 52,145 nurses in vietnamMaternal mortality rate (per 100 000 live births): 160under 5 infant mortality rate (per 1000 live births): 17
Figures are for 2006 unless indicated. Source: World health Statistics 2008, World health Organization www.who.int/countries/bfa/en
By tANyA SALEWSKi

13
Vietnam is long and narrow, with an extensive coastline on the South China Sea. It is a densely-populated developing country that in the last 30 years has had to recover from the ravages of war, the loss of financial support from the old Soviet bloc, and the rigidities of a centrally-planned economy. Thanks to significant economic reforms started in the late 1980s, Vietnam has experienced positive economic change in recent years, including rapid growth of the private sector and an ongoing shift to fiscal decentralisation. Along with its strengthening economy, Vietnam’s health system is undergoing dramatic transformation, leading to the diversification and expansion of health care services and better health service provision to people across the country.
despite impressive progress and gains in health, many Vietnamese continue to live on the edge of the poverty line and are at risk of being propelled back due to vulnerability to illness, natural disaster and environmental degradation. maternal and child mortality and malnutrition remain high and the burden of health care costs is increasingly being borne by households through user-fees and out-of-pocket expenditures, contributing to inequitable access to health care. Additional population health issues include the re-emergence of potential pandemics such as the avian flu, SARS, dengue fever and a rapid increase in HIV infections.
ARNNL is both proud and grateful to be able to assist yet also learn from our colleagues in Vietnam as they move forward with initiatives to improve the quality of nursing services for the population of Vietnam.
nATio
nAl n
uR
Sing
wEEk 2009
Are you protected?Every nurse should have professional liability protection.
www.cnps.ca 1-800-267-3390Log in to Members Only
Username: ARNNL Password: assist
Canadian Nurses Protective Society
1-10 copies $10.00 each 11-99 copies $7.50 each100-200 copies $5.00 each above 200 contact the author
Price does not include postage which varies depending on how many copies are purchased.
Post
er is
Cou
rtes
y of
Suz
anne
Gor
don
and
can
be p
urch
ased
by
vis
iting
ww
w.s
uzan
nego
rdon
.com
/?pa
ge_i
d=28
.

ACCESS VOL XXX NO 2 APRIL 2009
14
Alexandra CodnerAlexandra Codner is a workplace
representative at St. Clare’s Hospital in St. John’s. Alexandra graduated from the Centre of Nursing Studies in 2004 and now works on 6 west at St. Clare’s, a busy 32 bed adult orthopedic/surgery unit. Alexandra is actively involved in several committees including the delirium Protocol development Committee, the Scheduling Committee of 6 west and the Acute Pain Committee of St. Clare’s. with four years of experience under her belt, Alexandra says “nursing to me is being able to reach out and help a person when they are at their lowest and most desperate times of their lives. The satisfaction of knowing that you make these difficult times a little easier is very gratifying and special.”
Karen Morriskaren morris is a workplace representative for
the Emergency department at the Carbonear general Hospital. A graduate of the grace School of Nursing (1980), karen has 26 years experience in nursing, 8 of which have been spent in Emergency which serves a population of 40-50,000 and sees an average of 1700 patients monthly. karen enjoys being an ER nurse because “it fulfils my desire to help people in need.” karen says she sees many aspects of the nursing profession in her position including healing, counseling, resuscitating, prevention, grieving, tragedy and recovery and believes that “on most days, when my shift is done, I can say I have seen and touched humanity.” karen has completed the Health Assessment Course, ACLS, PALS, CTAS and attained her T.N.C.C. in 2005. karen is a member of the Newfoundland and Labrador Emergency Nursing Association (NLENA) and is an active volunteer who has served on the planning committee for the Provincial ER Symposium and as a participant in a QPPE pilot project. when she isn’t nursing, karen is a busy wife and mother. Having just celebrated her 25th anniversary, karen says she has ‘been blessed with 2 beautiful daughters and a wonderful husband. Life is very busy, but also very satisfying.”
Peggy HancockPeggy Hancock is a workplace representative
at western memorial Hospital where she works as a float pool nurse, mostly in the very busy maternal/newborn unit which has 13 beds, including 5 birthing rooms and a nursery. Peggy, who has worked as a nurse for 6 years, enjoys “knowing that [she] is having a positive impact on a family’s experience, that every day is different and there is always something new to learn.” Peggy is a graduate of the western Regional School of Nursing (2003) and has completed her CNA Certification in Perinatal Nursing (PNC(C)) and will be starting her masters in fall 2009. Peggy is also a member of the Association of women’s Health, Obstetric and Neonatal Nurses (AwHONN) and an Associate RN member of the Society of Obstetricians and gynecologists of Canada (SOgC). when she isn’t at work, Peggy loves to spend time with her family, especially her one-year-old Robbie. She also enjoys many outdoor activities, including geocaching.
Barbara Elliottbarbara Elliott is a workplace representative
at the John m. gray Centre in St. Anthony. A 23 year nursing veteran, barbara has worked on a medical unit, in the ER and is now working in long term care. barbara works as a Staff Nurse at the John m. gray Centre which provides Level 3 and 4 care to 48 residents. barbara graduated from the general Hospital School of Nursing in 1985 and is certified in IV Therapy, IV Push meds, Venipuncture, Pap Smears and Suturing. barbara is also a Certified medivac Trained Nurse and has completed a Nursing Health Assessment Course from Athabasca University. In June 2008, barbara completed a post-grad Nursing and Healthcare Leadership/management Program through mcmaster University. barbara is an active volunteer serving on the Unit Council at the John m. gray Centre, on the Stroke Strategy Committee, the Privacy Committee and the documentation committee with the Labrador-grenfell Regional Health Authority. barbara says she “like(s) the challenge of new programs” and is “looking forward to becoming an active participant in workplace Rep initiatives.”
Workplace Repsworkplace Representatives (wPRs) volunteer to represent ARnnl by supporting a professional nursing practice and communicating information in their workplaces. Reps complete an orientation and a workshop on leadership in Professional Practice to prepare for the role. ongoing support and development is provided through regular meetings and education sessions. our Reps are introduced in Access so you will get to know these important volunteers!

15
ADvAnCED noTiCEthe ARNNL Education and Research trust will be accepting applications for the Fall 2009 funding competition in June 2009. Online applications in the following categories will be available on the new ARNNL website:
ConTinuing EDuCATion AwARDSBursaries for Conference Registration & Post Basic Courses (up to $1000)Florrie Penney RN Physical Rehabilitation Bursary ($500)Nancy Llewellyn RN Pediatric Nursing Bursary ($500)Canadian Cancer Society harry Lake Memorial Scholarship (up to $1000)Nursing Leadership Awards ($500-$3000)NL Gerontological Nurses Association Bursary ($750)
Bn SCholARShiPSBN years 2, 3, 4 ($1000 each)BN Fast track year 2 ($1000)Flo hillyard Memorial Scholarship ($1000)Mona Fisher Cancer Nursing Scholarship ($1000)
Bn (PoST Rn) SCholARShiPSBNPostRN(FT-$1500;PT-$750)St.Clare’sAlumniAssociationScholarship(FT-$1500;PT-$750)
Rn RE-EnTRy SCholARShiP ($500)
ARnnl BAy ST. gEoRgE ChAPTER SCholARShiPAvailable to RNs from the Bay St. George area ($750)
gRADuATE SCholARShiPSMasters/PhDNursing(FT-$2000;PT-$1000)ARNNL 50thAnniversary(FT-$2000;PT-$1000)Masters/PhDNon-Nursing(FT-$2000;PT-$1000)Marcella Linehan Scholarship ($2000)
violET D. RuElokkE PRimARy hEAlTh CARE AwARD(2 at $500 or 1 at $1000)
nuRSing RESEARCh AwARDS (up to $2500 each)
Check out the new and improved online application forms in June 2009 on www.arnnl.ca
DEADLiNE FOR APPLiCAtiONS iS OCtOBER 15th
Late or incomplete applications will not be accepted.
ARnnl EDuCATion AnD RESEARCh TRuST Agmthe Annual Meeting of the ARNNL Education and Research trust will be held in Corner Brook on tuesday June 23rd at 1230. Location to be announced. For more information please contact [email protected] or Julie Wells at [email protected]
Call for nominations for Trust Board of DirectorsNominations are sought for the following positions:
Western Regional Director•Labrador-Grenfell Regional Director•Northern Regional Director•Eastern Rural Director•
the ARNNL Education and Research trust is a registered charitable foundation, established in 1986, to promote, support and assist basic nursing education, continuing nursing education and nursing research. As a member of the Board of Directors you will set the direction of the trust and participate in its administration.
term of office: Directors can serve a maximum of 2 consecutive terms. Each term is for two years.
For more information contact the trust at709-753-6040 or [email protected]
DEADLiNE FOR NOMiNAtiONS iS JuNE 1St, 2009.

ACCESS VOL XXX NO 2 APRIL 2009
16
CnA AnnounCES ThE nuRSing innovATionS ExChAngE
CNA has launched the Nursing innovation Exchange, an easy-to-use online database where nurses can improve Canada’s health-care system through the exchange, and ultimately the implementation, of innovations related to workforce redesign, practice environment education and other areas.
At the Nursing innovation Exchange, nurses can share information about the solutions, be they small or big, that they have successfully implemented or will be implementing in their workplace or educational setting. it is the place for clinical nurses, educators, administrators, policymakers and anyone interested in improving the health-care system to learn about innovative practices implemented by nurses. CNA hopes the exchange will become a widely used resource — and one that other health-care professionals, employers, governments, industry and the public will respond to.
For more information on the Exchange, visit: www.cna-aiic.ca/cna/nursing/innovations/default_e.aspx
Goings on...Goings on...
the Public Consultations on the Display and Promotion of tobacco Products are officially underway. if you would like to make your voice heard about this very important issue please visit: www.health.gov.nl.ca/health/tobacco/default.htm
Remember – every action counts!
AnnuAl nuRSing ChARiTy BAllin benefit of the nl Down Syndrome SocietyOn Saturday, March 28th, the 11th Annual Nursing Charity Ball in benefit of the Newfoundland and Labrador Down Syndrome Society was held at the holiday inn and Suites. During the evening, which raised $7000 in support of the NLDSS, Spirit Awards were presented to Laura Downing from the MuN School of Nursing and Robyn Power of the Centre for Nursing Studies.
Pictured(LefttoRight):PegiEarle,ExecutiveDirector;ARNNL,LauraDowning,MUNSchoolofNursing;KristaBlake,CharityBallCoordinator,CentreforNursingStudies;andRobynPower,CentreforNursingStudies
ARNNL President Jim Feltham meets with Community health Nurses from Eastern health in St. John’s April 7, 2009 to discuss challenges facing ChNs in their practice today and in the future.
CAnADiAn PATiEnT SAFETy wEEk: november 2-6, 2009 Ask. listen. Talk.
the Canadian Patient Safety institute (CPSi) is pleased to announce Canadian Patient Safety Week (CPSW) with a theme focused on communication - Ask. Listen. Talk
Are you a mental health nurse? Are you interested in professional development?would you like to talk to other mental health nurses?PSiGNAL wants you as a member.to find out how to get involved contact Karen Whitehorne at [email protected]
ARnnl Council links-to-listen
ConSulTATionS unDERwAy
17
Goings on...Goings on...
Goings on...Goings on...
ConFEREnCES & woRkShoPS
uRologiCAl ExCEllEnCE ConFEREnCE: Sept 24-26, 2009 Westin hotel, Edmonton Alberta - hosted by Edmonton ChapterEvidence and Caring: Spanning the Ages in Urologic NursingContact: [email protected]
nuRSing 2990: Spiritual Dimensions of nursing Practice
have you ever encountered clients in your practice who have spiritual needs and you did not know what to do about it, except perhaps refer them to pastoral care? Would you know how to assess a person’s spiritual needs? Do you know what spiritual needs are? if you do not know the answer to these questions, this course is for you!
Nursing 2990 is an elective course in the post-RN program (distance education mode) at the School of Nursing, Memorial university. however, you do not need to be in the post-RN program to take this course. it was developed to provide nurses with the knowledge and skills to attend to the spiritual needs and concerns of clients.
the course will be offered in Winter semester, 2010, pending sufficient enrollment. if you are interested in finding out more information about this course, please contact Doreen Westera attheSchoolofNursing,MemorialUniversity:777-7259;[email protected] or visit www.ucs.mun.ca/~dwestera
National Nursing Week is an opportunity to promote and show appreciation for the vital role nursing plays in the health system and in the life of every Canadian.
Let’s celebrate the nursing profession and encourage others to take part in the festivities.
CNA is pleased to provide you with National Nursing Week resources and tools to ensure your celebrations are a true success.
Log on to www.cna-aiic.ca for more details.
3RD AnnuAl nEwFounDlAnD & lABRADoR ACCESS & PRivACy woRkShoP "Paving the Way" hosted by the NFL Office of the Chief information Officer, health and Community Services, ARMA, and Newfoundland and Labrador Offshore Petroleum Board will be held at the holiday inn Government Centre in St. John's, NL on May 27, 2009. Website: www.verney.ca/nlapw2009Contact information: [email protected] | 613-226-8317
inAuguRAl nEwFounDlAnD & lABRADoR inFoRmATion mAnAgEmEnT DAy 2009"Managing for Today, Preparing for Tomorrow"holiday inn Government Centre in St. John's, NL on May 25th, 2009. Website: http://www.verney.ca/nlim2009/Contact information: [email protected] | 613-226-8317
21ST oPERATing Room nuRSing ASSoCiATion oF CAnADA (oRnAC) Conference to be held June 7-12, 2009, St. John’s NL For further information contact registration co-chairs, val tilley [email protected] or Jo Moss [email protected]

ACCESS VOL XXX NO 2 APRIL 2009
18
wElComEARNNL is pleased to welcome Siobhainn
lewis Rn, Bn to the position of Nursing Consultant, Policy and Practice. Siobhainn graduated with her RN diploma from the
general Hospital School of Nursing and subsequently completed her bN at memorial University in 2003 and is due to complete her master of Nursing from Athabasca University in April 2009. before joining the ARNNL, Siobhainn worked as the Regional Nursing Recruitment Consultant with Eastern Health and as division manager for the medicine Program with Eastern Health. Siobhainn also worked in a variety of roles within the former Health Care Corporation of St. John’s including manager of discharge Planning, Admission-discharge facilitator, Site Clinical Coordinator and as a Staff Nurse with the Surgery program.
Siobhainn is an active volunteer and served as the Chair of the ARNNL Education and Research Trust Awards Committee for five years. She has also volunteered with the SPCA and served as both Treasurer and President of the general Hospital School of Nursing Alumni Association. Siobhainn is also a member of the Newfoundland and Labrador Nurses Respiratory Society.
In her role as Nursing Consultant – Policy and Practice, Siobhainn will provide strategic leadership on current issues, emerging trends and future directions in nursing practice and health policy. Siobhainn’s skills are ideally suited for building strong networks and programs that support safe, competent and ethical nursing practice. we welcome Siobhainn to the ARNNL team and we look forward to working with her as we continue to shape the future of the nursing profession in the province.
ARnnl lAunChES nEw liCEnCE STATuS SEARCh Tool
ARNNL is pleased to announce the launch of a new Licence Status Search tool through our website www.arnnl.ca. The search tool will allow all stakeholder groups (the public, employers, members etc) to access the list of nurses who currently hold membership with the Association.
A complete, searchable, list is provided to help locate members with current registration. Confirmation of current registration of a Registered Nurse, a Nurse Practitioner or a nurse with an interim/temporary licence can be viewed by simply entering the name or registration number of a member in the status search feature. Complete instructions for the Licence Status Search Tool can be found by visiting: www.arnnl.nf.ca/practicing, www.arnnl.nf.ca/nonpracticing and www.arnnl.nf.ca/nursepractitioner
we hope you find this new service helpful and welcome your feedback on the process. for further information contact michelle Osmond, director of Regulatory Services at [email protected] or Janice Lockyer, director of Communications at [email protected]
ConTACTing mEmBERS FoR RESEARCh PuRPoSES
ARNNL is often approached to assist with nursing research studies. before we agree to do so, researchers must provide an outline of their proposal and a copy of their ethical approval. Typically ARNNL will receive requests to provide contact information for potential research participants. Once we have approved such a request, there are two ways that we do this. first, if the researcher wants to send their questionnaire or recruit RNs themselves, we provide the contact information of those RNs who meet the study inclusion criteria and who indicate on their registration form that they consent to release of that information for research purposes (see Question 15 on the ARNNL registration form). If you do not check the consent box, your name is not released to researchers. Second, we will distribute questionnaires on behalf of a researcher to all RNs who meet their study inclusion criteria. In this case, the questionnaires are mailed from ARNNL and the researcher does not receive any contact information.
If you have any questions about this or other research questions, please contact Julie wells, Research Analyst at [email protected] or michelle Osmond, director of Regulatory Services at [email protected]
oPPoRTuniTy FoR FEEDBACkARNNL wishes to advise members that the following
documents are coming up for review:The documentation Standards• The Position Statement on Nursing Leadership. •
we invite feedback from interested members. The documents can be viewed at: www.arnnl.nf.ca/menu/opportunity_for_input.shtml.

19
The Jury is out!Have you heard the discussion… pre-testing the
balloon for indwelling catheters could increase the risk of urethral trauma. Experts are indicating that this is no longer necessary as it can cause an irregularity (the balloon wrinkles) on the outside of the catheter which can cause friction, mucosal irritation and sometimes bleeding upon insertion.
Reference: Perry, A & Potter, P., (2010). Clinical Nursing Skills and Techniques (7th edition) Mosby; Society of Urologic Nurses andAssociates (SuNA).
new 2008 guidelines for the management of high Blood Pressure
The new Canadian bP guidelines warn that approximately one million Canadians with “high-normal” blood pressure will develop full-blown high blood pressure over the next four years - putting them at a higher risk for heart attack and stroke - unless they are diagnosed and treated.
The new guidelines, developed and updated annually by the Canadian Hypertension Education Program (CHEP) in association with the Heart and Stroke foundation and other organizations, are a wake-up call for health care providers caring for patients with this borderline condition. www.heartandstroke.pe.ca/site/c.inklkRowhqE/b.5019121/k.A298/new_2008_guidelines_for_the_management_of_high_blood_pressure.htm
heart and Stroke Foundation, 2008
making a list and Checking it Twice….medication Reconciliation actually works. An
elderly gentleman was admitted to acute care from a personal care home with a diagnosis of hyponatremia. The physician was unable to determine the cause of the low sodium. during the medication reconciliation process it was discovered that the patient had been started on hydrochlorthiazide a week before and this was determined to be the cause of the problem. The hospital had not been informed of this new medication by the personal care home but when the nurse verified the medication information with a second source (as part of the medication reconciliation process) the cause of the diagnosis was confirmed. without this information the cause of the hospitalization would not have been determined and the gentleman would have resumed his medication once he returned to the home; potentially leading to further adverse events.
By Maxine Power-Murrin RN MEd, Project Coordinator Medication Reconciliation initiative, Eastern health
EDitOR’S NOtE: Clinical Corner is designed for nurses to share information that they have found in their experience to be practical, safe, and effective. ARNNL requires that the information provided reflect good nursing judgment. We do not confirm the validity of the submitter’s tip in the literature. ARNNL does not endorse any products identified in the submissions to this column.
SAFETY TIPout of the Box: Storage of open insulin vialsReplacing open insulin bottles back into the manufacturer’s box can lead to errors. This is especially true if you are using different types of Insulin. It is easy to absentmindedly slip the bottle back into a wrong box and in a rush someone may inadvertently not double check the inside label especially if the labels are similar and give the wrong insulin. By Annette Morgan BN, MN GNC(C) Professional Practice Consultant- LtC, Eastern health
Clinical CornerClinical Corner
Can you Read this Progress note??Called b2 pt’s room. Pt. z “itigbs”. Pt. assisted ax d
room n b2 bed. denied any pain. Offered antiemetic Im o po. gravol 50 mg’s po given. Pt. stated he felt “vri c%l”. Temp 36.8c. On reassessment 10 minutes l8r, pt. zzzz.
Reference: www.swalk.com/sms1.htmThe use of approved abbreviations, symbols or
acronyms can improve efficiencies in documentation if their meaning is well understood by everyone. Abbreviations and symbols that are obscure, obsolete, poorly defined or have multiple meanings can lead to errors, cause confusion and waste time. (ARNNL, documentation Standards draft, 2009.)
ANSWER: Called back to patients room. Patient said “i think i’m going to be sick”. Patient assisted across room and back to bed. Denied any pain. Offered antiemetic iM or po. Gravol 50mg’s po given. Patient stated he felt “very cool”. temp 36.8c. On reassessment 10 minutes later, patient was sleeping.

ACCESS VOL XXX NO 2 APRIL 2009
20
A new way to teach nursing skillsST
uDEn
T Co
RnER
The nursing student washes his hands, walks into the patient’s room, introduces himself and then assesses the patient’s
knowledge and perspective. For five mun fast track students in the Fall 2008, this experience differed from contact with a human patient only because it involved
human patient simulation (hPS).
HPS makes use of a computerized life-size simulator mannequin that is programmed to provide interactive clinical situations for caregivers in a safe learning environment. This unique and innovative teaching tool is currently being incorporated into health care service and education, including national and international schools of nursing.
Eastern Health acquired a HPS mannequin in 2002 through a donation from the give to feel good campaign and entered into a joint agreement with the faculty of medicine to integrate its use with both groups.
mUN School of Nursing saw the value in using the simulation. with funding from the Vice–President’s Innovative Teaching grant, dr. Sandra macdonald, ms. brenda Oldford, ms. Christine Castagné, and ms. April manuel were able to explore the possibility of integrating HPS into the bN (Collaborative) curriculum through simulated clinical experiences. The grant provided funding for educational opportunities to prepare faculty to implement HPS modules.
Though, HPS has implications for use across the curriculum, for this project the faculty members developed one module related to the nursing care of a medical surgical patient requiring a blood transfusion and subsequently experiencing an adverse reaction. five third-year nursing students in the course N3111: Nursing Care of middle and Older Adults, volunteered to take part. during the three-hour HPS session, the students had to assess and treat this patient in the same manner as they would have in the ‘real’ clinical setting. during the implementation of the module faculty were able to explore the impact of participation on student’s psychomotor skill acquisition and their satisfaction with the simulated clinical experience.
“The evaluation tool developed for this HPS indicated that students had met all of the objectives set out for the experience,” said dr. Sandra macdonald. “The students performed a very thorough baseline assessment, even documenting a slight difference between left and right pupil dilation, which was not a planned portion of the session.”
dr. macdonald also reports that the students were extremely professional in their conduct towards each other, the patient and the other professionals they had to call during the session. “The students were able to follow the current institutional policy to safely check and administer the blood product–packed red blood cells. They were able to pick up on subtle verbal cues from the patient and physiologic changes in the vital signs to successfully assess and respond to a transfusion reaction. during the final debriefing, all of the students enthusiastically agreed that they felt much better prepared to administer blood in the clinical setting and monitor their patients for any adverse reaction.”
Nursing students simulator: From left: Dee Ann Belbin, Rebecca Duffy, Geoff Shinkle, Sherry Nelson, and Matthew hand and nursing faculty member April Manuel.
Nursing students healing touch: From left: Rebecca Duffy, Dee Ann Belbin, Sherry Nelson, Geoff Shinkle and Matthew hand
EDitED FROM A GAzEttE ARtiCLE By ShARON GRAy

21
Projet : Annonce MMI 2009
Client : Meloche Monnex
No de dossier : L-MM7712-09_MMI (7.5x10)•cnanurses_EN
Province : Newfoundland
Publication : ACCESS
Format : 7.5 x 10
Couleur : BLK
Épreuve # : 1
Date de tombée : 9/02/09
Graphiste : Marie-Josée Proulx
Hamelin Martineau • 505, boul. de Maisonneuve O. Bureau 300 • Montréal (Québec) H3A 3C2 • T : 514 842 4416 F : 514 844 9343ATTENTION : Merci de vérifi er attentivement cette épreuve afi n d’éviter toute erreur.
GROUP HOME AND AUTO INSURANCE for members of the Canadian Nurses Association
PROTECTION MADE EASY...GROUP RATES MADE EASIER! As a member of the Canadian Nurses Association, you can SAVE on your home and auto insurance through preferred group rates, while enjoying high-quality insurance products and outstanding service.
As the leading provider of group home and auto insurance, we offer a wide range of innovative products, so you are sure to get the coverage that is right for your particular needs…and the peace of mind that goes with it!
Insurance program supported by
The TD Insurance Meloche Monnex home and auto insurance program is underwritten by SECURITY NATIONAL INSURANCE COMPANY and distributed by Meloche Monnex Insurance and Financial Services Inc. in Québec and by Meloche Monnex Financial Services Inc. in the rest of Canada.
Due to provincial legislation, our auto insurance program is not offered in British Columbia, Manitoba or Saskatchewan. *No purchase required. Contest ends on January 16, 2010. Skill-testing question required. Odds of winning depend on number of entries received. Complete contest rules available at MelocheMonnex.com.Meloche Monnex® is a trade-mark of Meloche Monnex Inc. TD Insurance is a trade-mark of The Toronto-Dominion Bank, used under license.
MelocheMonnex.com/cnanurses
1 866 269 1371
ENJOY SAVINGS THROUGH PREFERRED GROUP RATES
Monday to Friday, 8 a.m. to 8 p.m. (ATLANTIC)Monday to Friday, 8:30 a.m. to 8:30 p.m. (NEWFOUNDLAND)
Request a quote and you could