
Vol. Printed in U.S.A. Technique Intraperitoneal Injection of
2
APPLIED MICROBIOLOGY, Sept. 1968, p. 1418-1419 Copyright 1968 American Society for Microbiology Errors in the Technique of Intraperitoneal Injection of Mice JOHN P. STEWARD, E. P. ORNELLAS,' K. D. BEERNINK,' AND WILLIAM H. NORTHWAY Department of Medical Microbiology and the Fleischmann Laboratories of the Medical Sciences, and Department- of Radiology, Stanford University School of Medicine, Palo Alto, California 94304 Received for publication 2 July 1968 Injection of drugs, chemicals, or infectious agents into the peritoneal cavity of the mouse is used by investigators in a variety of disciplines for presumably reliable and safe placement of an inoculum into a known anatomical location. However, we have found no descriptions of the distribution of intraperitoneal inocula, nor of the possible errors in their initial placement. Recently, we attempted to recover radioactively labeled bacteria from the peritoneal cavities of mice previously injected intraperitoneally with a suspension of the radioactive bacteria. Infre- quently, we recovered levels of radioactivity far below that expected. It seemed likely that in these cases the injection had been mistakenly placed into a site other than the peritoneal cavity. To confirm this, we used the same technique to inject into the peritoneal cavities of B1oD2, CF #1 (Carworth Farms, New York, N.Y.) and B Alb C mice the same volume (0.2 ml) of Ethiodol (Guer- bet Laboratories), a nonabsorbable radiological contrast material with a viscosity near that of water. The mice were sacrificed 15 to 30 min after injection, and anteroposterior and lateral X-rays were taken of each mouse. The injections were performed with a 25-gauge, 5A-inch (1.59 cm) dis- posable needle. The investigator held the mouse by the skin of the back and neck in his left hand. With the syringe in his right hand, he injected through the wall of the abdomen into one of the lower abdominal quadrants. The techniques of five experienced investigators were sampled and the results are summarized in Table 1. Of 150 mice injected, 21 (14%) showed all or part of the inoculum in a site other than the peritoneal cavity. In 13 cases, this site was the lumen of the stomach or the small bowel, al- though 4 subcutaneous, 3 retroperitoneal, and 1 intravascular injection occurred. All other inoc- ulae were very well dispersed throughout the peritoneal cavity, and, in every male mouse, con- trast material could be seen in the scrotum. Typi- 'Public Health Service Predoctoral Fellow (GM 30280). 2Postdoctoral Fellow, supported by the Aron Foundation. cal radiographs of successful and unsuccessful injections are shown in Fig. 1. The reason for the more accurate placement of the inoculum by one investigator (F. A. F.) was not immediately ap- parent. The techniques in all cases were similar. The results show that the well-placed inoculum quickly distributes uniformly throughout the peritoneal cavity. In the male, this distribution invariably includes the peritesticular space, and it seems likely that this compartment is less accessi- ble to procedures for recovery of the inoculum from the peritoneal cavity. In studies where re- TABLE 1. Anatomical location in mice of supposedly intraperitoneal injections of 0.2 ml of a radi- ological contrast medium determined by X-ray No. of Injector inoculaa/ Anatomical location of inoculab Inetr total mice injected J. P. S. 3/12 2 SB; 1 RP E. P. O. 3/20 2 SB; 1 SC V. K. 3/18 2 SC; 1 IV K. D. B. 11/75 8 SB; 2 RP; I SC F. A. F. 1/25 1 SB Total 21/150 13 SB; 3 RP 4 SC; 1 IV a Wholly or partly outside the peritoneal cavity. bNot in the peritoneal cavity. SB, lumen of stomach and/or small bowel; RP, retroperitoneal; SC, subcutaneous; IV, intravascular. covery of the inoculum is important, females should be used. Attempts were made to improve the injection procedure by using one investigator to hold the mouse while the other investigator injected through a fold of abdominal wall. The incidence of error remained the same. It is probable that placement of the inoculum into a site other than the peritoneal cavity, al- though infrequent, is an error inherent in the tech- nique and cannot be minimized by simple modifi- cations of procedure. This error may explain the occasional failure of a mouse to show a predicted effect when this failure is most unlikely to have resulted from other causes. The possibility of the 1418 Vol. 16, No. 9 Printed in U.S.A. on December 20, 2018 by guest http://aem.asm.org/ Downloaded from
Transcript of Vol. Printed in U.S.A. Technique Intraperitoneal Injection of
APPLIED MICROBIOLOGY, Sept. 1968, p. 1418-1419Copyright 1968 American Society for Microbiology
Errors in the Technique of IntraperitonealInjection of Mice
JOHN P. STEWARD, E. P. ORNELLAS,' K. D. BEERNINK,' AND WILLIAM H. NORTHWAY
Department of Medical Microbiology and the Fleischmann Laboratories of the Medical Sciences, and Department-ofRadiology, Stanford University School of Medicine, Palo Alto, California 94304
Received for publication 2 July 1968
Injection of drugs, chemicals, or infectiousagents into the peritoneal cavity of the mouse isused by investigators in a variety of disciplines forpresumably reliable and safe placement of aninoculum into a known anatomical location.However, we have found no descriptions of thedistribution of intraperitoneal inocula, nor of thepossible errors in their initial placement.
Recently, we attempted to recover radioactivelylabeled bacteria from the peritoneal cavities ofmice previously injected intraperitoneally with a
suspension of the radioactive bacteria. Infre-quently, we recovered levels of radioactivity farbelow that expected. It seemed likely that in thesecases the injection had been mistakenly placedinto a site other than the peritoneal cavity.To confirm this, we used the same technique to
inject into the peritoneal cavities of B1oD2, CF #1(Carworth Farms, New York, N.Y.) and B Alb Cmice the same volume (0.2 ml) of Ethiodol (Guer-bet Laboratories), a nonabsorbable radiologicalcontrast material with a viscosity near that ofwater. The mice were sacrificed 15 to 30 min afterinjection, and anteroposterior and lateral X-rayswere taken of each mouse. The injections wereperformed with a 25-gauge, 5A-inch (1.59 cm) dis-posable needle. The investigator held the mouseby the skin of the back and neck in his left hand.With the syringe in his right hand, he injectedthrough the wall of the abdomen into one of thelower abdominal quadrants.The techniques of five experienced investigators
were sampled and the results are summarized inTable 1. Of 150 mice injected, 21 (14%) showedall or part of the inoculum in a site other than theperitoneal cavity. In 13 cases, this site was thelumen of the stomach or the small bowel, al-though 4 subcutaneous, 3 retroperitoneal, and 1intravascular injection occurred. All other inoc-ulae were very well dispersed throughout theperitoneal cavity, and, in every male mouse, con-
trast material could be seen in the scrotum. Typi-
'Public Health Service Predoctoral Fellow (GM30280).
2Postdoctoral Fellow, supported by the AronFoundation.
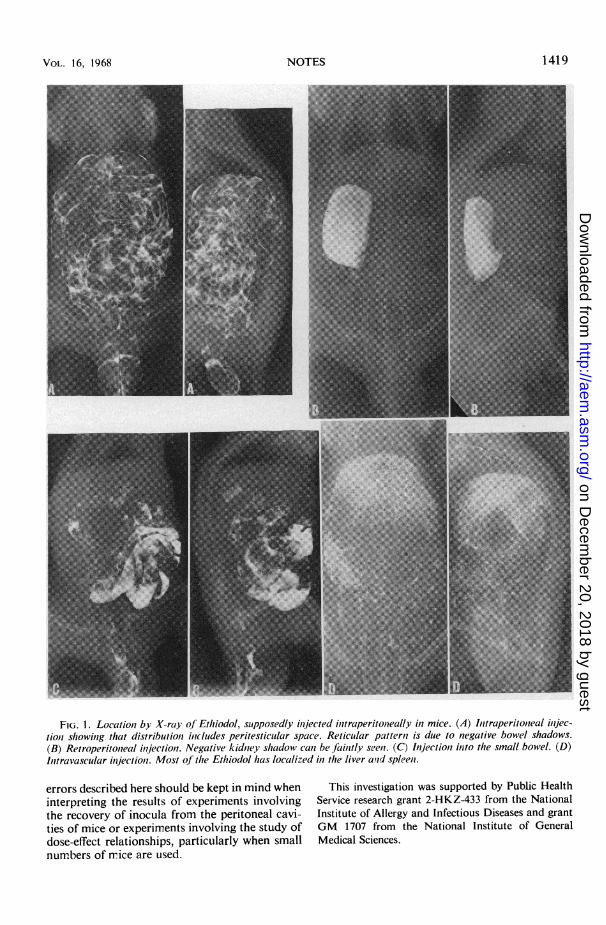
cal radiographs of successful and unsuccessfulinjections are shown in Fig. 1. The reason for themore accurate placement of the inoculum by oneinvestigator (F. A. F.) was not immediately ap-parent. The techniques in all cases were similar.The results show that the well-placed inoculum
quickly distributes uniformly throughout theperitoneal cavity. In the male, this distributioninvariably includes the peritesticular space, and itseems likely that this compartment is less accessi-ble to procedures for recovery of the inoculumfrom the peritoneal cavity. In studies where re-
TABLE 1. Anatomical location in mice ofsupposedlyintraperitoneal injections of 0.2 ml of a radi-ological contrast medium determinedby X-ray
No. ofInjector inoculaa/ Anatomical location of inoculabInetr total mice
injected
J. P. S. 3/12 2 SB; 1 RPE. P. O. 3/20 2 SB; 1 SCV. K. 3/18 2 SC; 1 IVK. D. B. 11/75 8 SB; 2 RP; I SCF. A. F. 1/25 1 SBTotal 21/150 13 SB; 3 RP
4 SC; 1 IV
a Wholly or partly outside the peritoneal cavity.bNot in the peritoneal cavity. SB, lumen of
stomach and/or small bowel; RP, retroperitoneal;SC, subcutaneous; IV, intravascular.
covery of the inoculum is important, femalesshould be used.
Attempts were made to improve the injectionprocedure by using one investigator to hold themouse while the other investigator injectedthrough a fold of abdominal wall. The incidenceof error remained the same.
It is probable that placement of the inoculuminto a site other than the peritoneal cavity, al-though infrequent, is an error inherent in the tech-nique and cannot be minimized by simple modifi-cations of procedure. This error may explain theoccasional failure of a mouse to show a predictedeffect when this failure is most unlikely to haveresulted from other causes. The possibility of the
1418
Vol. 16, No. 9Printed in U.S.A.
on Decem
ber 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from
VOL. 16, 1968
FIG. 1. Location by X-ray of Ethiodol, suipposedly ilnjected ilitraperitoneally in mice. (A) Initraperitonieal inijec-tioci showinig. that distributionI inlcluldes peritesticlllar space. Reticular patternl is due to negative bowel shadows.(B) Retroperitoneal inijectiont. Negative kidntey shadow can be faintly seen. (C) Injectiont into thle small bowel. (D)Inttravascular injection1. Most of the Ethiodol has localized in the liver and spleeni.
errors described here should be kept in mind wheninterpreting the results of experiments involvingthe recovery of inocula from the peritoneal cavi-ties of mice or experiments involving the study ofdose-effect relationships, particularly when smallnumbers of nmice are used.
This investigation was supported by Public HealthService research grant 2-HKZ-433 from the NationalInstitute of Allergy and Infectious Diseases and grantGM 1707 from the National Institute of GeneralMedical Sciences.
1419NOTES
on Decem
ber 20, 2018 by guesthttp://aem
.asm.org/
Dow
nloaded from


















